Submitted:
11 July 2024
Posted:
15 July 2024
You are already at the latest version
Abstract
Our study aimed to identify predictors for the effectiveness of tumor regression in lung cancer patients undergoing neoadjuvant treatment and cancer resections. Patients admitted between 2016 and 2022 were included in the study. Based on the histology of the tumor, patients were categorized into lung adenocarcinoma group (LUAD), and squamous cell carcinoma group (SQCA). Ninety-five patients with non-small cell lung cancer were included in the study. Fifty-eight (61.1%) and 37 (38.9%) patients were included in the LUAD and SQCA groups, respectively. Nine (9.5%), 56 (58.9%), and 30 (31.6%) patients were categorized with a tumor regression score of I, II, and III respectively. In multivariable analyses, histology of the primary tumor (SQCA), lymph node size in the preoperative CT scan (>1.7cm) and absolute tumor size reduction after neoadjuvant treatment (>2.6 cm) independently predict effectiveness of tumor regression (OR, [95% Confidence interval, p-value] of 6.88 [2.40-19.77, p70 years, extended resection >one lobe, and tumor recurrence or metastasis were identified as significant independent predictors of reduced overall survival. Assessment of tumor size before and after neoadjuvant treatment might help to identify high-risk patients with decreased survival and to improve patient management and care.
Keywords:
lung cancer
; PET/CT-scan
; lymph node staging
; neoadjuvant therapy
; pathological response
; tumor regression
; overall survival
1. Introduction
Non-small cell lung cancer (NSCLC) continues to be the leading cause of cancer-related deaths worldwide [1]. Patients with early stages of NSCLC can usually be cured with surgery alone with a 5-year overall survival (OS) rate of 92 % in Stage IA [2]. Unfortunately, many patients with NSCLC present advanced disease at the time of the diagnosis [1]. Patients with locally advanced NSCLC who receive surgery alone show poor OS [2]. The neoadjuvant therapy to reduce the tumor stage, followed by surgery, is the routine treatment of choice in clinical practice by advanced NSCLC [3]. This therapeutical approach aims to reduce the tumor stage, improve operability, and possibly eradicate microscopic metastases, in that way offering a complete curative approach [4]. However, there are no established common standards for neoadjuvant therapy yet [5,6,7]. It is suggested that different neoadjuvant therapy modalities can lead to different tumor regressions.
The assessment of tumor regression grade (TRG) has emerged as a valuable prognostic indicator in evaluating the efficacy of neoadjuvant therapies [8]. TRG reflects the degree of pathological response to therapy and holds the potential to guide clinical decisions, improve patient outcomes, and enhance treatment methods [9]. Thus, understanding the complex relationship between neoadjuvant therapy and TRG is critical for optimizing therapeutic approaches and establishing suitable treatment strategies for individual patients.
By examining the perioperative parameters (laboratory, radiological, histological, and clinical comorbidities), we aim to identify in our recent study the predictors for the effectiveness of tumor regression in lung cancer patients undergoing neoadjuvant treatment and major lung cancer resections to improve the perioperative risk stratification and optimizing patient management. The second goal of our study was to analyze the OS of the patients included in this study and find the relationship between survival and tumor regression.
2. Materials and Methods
2.1. Study Population
This single institution retrospective cohort study was performed after approval by the Ethics Committee of the Ludwig Maximilian University of Munich (LMU), Germany, file number 24-0114 by the Declaration of Helsinki and STROBE recommendations for clinical studies. Patients’ recruitment and treatment were performed at the Department of Thoracic Surgery of the Robert Bosch Hospital (Stuttgart, Germany) between 01.01.2016 and 31.12.2022.
All patients with resectable malignant primary lung tumors undergoing neoadjuvant therapy and major surgical resections (lobectomy, bilobectomy, or pneumonectomy) with histologically reported lung adenocarcinoma (LUAD group) and squamous cell carcinoma (SQCA group) in the intraoperative histological specimens were included in the study. Patients undergoing similar treatment experiencing rare histological subtypes in the intraoperative specimens (e.g. adenosquamous carcinoma (n=2), synovial sarcoma (n=2), sarcomatoid lung carcinoma (n=2), low-grade differentiated sarcoma of the lung (n=1), neuroendocrine/ small cell lung cancer (n=2), and not otherwise specified tumors (NOS, n=4) were excluded (Figure 1).
2.2. Data Assessments/Sources
Clinical data were collected from medical reports and patients’ files stored in the hospital and the Onkostar database of the Baden-Wuerttemberg Cancer Registry. Primary lung tumors were categorized according to the 7th edition of the TNM staging system [10], and histopathological analysis according to the World Health Organization Classification of lung tumors [11].
Clinical data included patients’ demographics (age, sex, BMI, smoking status, nicotine, and alcohol consumption, comorbidities), laboratory (blood counts, C-reactive protein (CRP), creatinine, lactate dehydrogenase (LDH), and albumin), respiratory (FVC: functional vital capacity; FEV1: forced expiratory volume in one second; DLCO: diffusing capacity of the lung for carbon monoxide), radiological (cTNM) parameters with tumor and lymph node size as tumor and lymph node size was chosen the largest distance in transverse, coronal and sagittal plane in CT imaging. Histological parameters and pTNM. Data on patient treatment including neoadjuvant regimen ((combined) chemotherapy, immunotherapy, radiation therapy)), intraoperative approach (minimally invasive or open surgery, surgical time), adjuvant regimen ((combined) chemotherapy, immunotherapy, radiation therapy), as well as postoperative morbidity (complications, in hospital and ICU stay, tumor recurrence/ metastasis) and mortality were collected.
2.3. Outcome
The correlation between the abovementioned clinical parameters and the intraoperative tumor regression score was analyzed concerning the histological subtype of the primary tumor (LUAD or SQCA). Tumor regression grade (TRG) was defined according to the initial study of Junker et al. (TRG_I: >95% vital tumor cells, TRG_IIa: >10% vital tumor cells, TRG_IIb: <10% vital tumor cells, TRG_III: absent vital tumor cells in the intraoperative histological specimens), respectively [8]. TRG_III was also defined as complete pathologic response (CPR) according to Travis et al [12].
2.4. Data Analysis
Parametric variables are presented as median and interquartile range. Comparisons between groups were performed using the Mann-Whitney U-test (for continuous variables, e.g. laboratory parameters, age, BMI, Pack years, lung function parameters, lymph node size, tumor size) or by Chi-square test statistics and Fisher’s exact test (for binary variables). Tumor size reduction values after neoadjuvant treatment were given as absolute values (absolute delta= tumor size before neoadjuvant treatment – tumor size after neoadjuvant treatment, values given in CM). To assess the percentual decrease of the tumor size, relative values were calculated as follows: (relative delta = ((tumor size before neoadjuvant treatment – tumor size after neoadjuvant treatment) / tumor size before neoadjuvant treatment) x 100), values given in %. Multivariable analysis was performed by binary logistic regression analysis validated by three methods (enter, forward LR, and backward LR). Odds ratios (OR) with 95% confidence intervals (CI) were assessed for independent predictors. Optimal cut-off values were evaluated using receiver-operator characteristics (ROC) and the Youden criterion. Survival data were generated by Kaplan Meier analysis (log-rank test) and the independent predictive value of the significant variables by stratified Cox proportional hazard regression analysis. Overall survival is defined as the time interval between lung cancer surgery and event (death) or census (last recorded follow-up). Analyses were performed after excluding the missing values (under 10% for selected variables), by using SPSS (Version 26, IBM, Armonk, New York, USA). P Values <0.05 were considered statistically significant.
3. Results
3.1. Study Population
Of 892 patients admitted for thoracic surgery between 01.01.2016 and 31.12.2022, 95 patients fulfilled the inclusion criteria. The analyzed cohort (n= 32/95 female patients, 33.7 %) included patients with a median age of 64.20 [57.90; 69.06] years (n=42, 44.2% older than 65 years) and a median BMI of 24.54 [22.16; 27.04] kg/m2 (n=49, 51.6%. with a BMI between 18.5 and 25 kg/m2).
Based on the histology of the primary tumor, 58 patients (61.1%) and 37 patients (38.9%) patients were included in the LUAD and SQCA groups, respectively.
The inclusion process and groups of patients categorized by the histology of the primary tumor are illustrated in Figure 1.
Overall, 13 patients (13.7%) were never smokers, 50 patients (52.6%) were current smokers, and 32 patients (33.7%) were ex-smokers at the time of diagnosis.
LUAD group comprised significantly more female patients (27/58 (46.6 %) vs 5/37 (13.5 %, p=0.0009), overweighted patients (29/58 (50.0 %) vs 10/37 (27.0 %), p=0.0264), as well as smokers reporting a lower nicotine consumption (30.0 [4.25; 45.0] vs 40.0 [22.5; 52.5], p=0.0288).
SQCA group encompasses significantly more patients aged 65 years or older (21/37 (56.8 %) vs 21/58 (36.2 %), p=0.0492) and with a normal BMI range (24/37 (64.9 %) vs 25/58 (43.1 %), p=0.0385).
Patients with SQCA were admitted with significantly lower lung function parameters in comparison to the LUAD patients (FEV1: 69.00 [55.50-85.00] vs 80.50 [67.00-90.25] % predicted, p=0.0103; DLCO: 48.00 [42.00-62.00] vs 62.50 [50.50-70.50] % predicted, p=0.0023 and Tiffeneau Index 88.00 [78.00-95.00] vs 95.00 [87.00-102.00] %, p=0.0014, respectively). The patients’ demographics and comorbidities are summarized in Table 1.
Specific comorbidities (Table 1) were not significantly associated with the histology of the primary tumor.
Laboratory parameters on admission day (routinely 1 - 5 days before surgery) showed a low hemoglobin level in all patients upon neoadjuvant therapy. There was no significant difference in the sex-specific hemoglobin level (< 12g/dl in females and < 13g/dl in males) between LUAD and SQCA groups (p=0.7246). Patients from LUAD group were admitted with lower serum C-reactive protein levels (CRP 0.20 [0.10; 0.60] vs 0.50 [0.10; 1.30], p=0.0206) and higher serum albumin levels (4.27 [3.90; 4.46] vs 4.00 [3.60; 4.35], p=0.0281). The standard laboratory parameters on admission day stratified by the histological subtypes of the primary tumor are illustrated in Table 2.
No significant differences regarding tumor side, localization, and lymph node involvement were reported between groups. LUAD group comprised significantly more patients with cT1 tumors (11/58 (19.0 %) vs 0/37 (0 %), p=0.0048) and fewer patients with cT4 tumors (23/58 (39.7 %) vs 24/37 (64.9 %), p= 0.0166).
Upon neoadjuvant therapy, significantly more patients with yT0 tumors were reported in the SQCA group (22/37 (59.5 %) vs 10/58 (17.2 %), p <0.0001). The tumor characteristics are presented in Table 3.
The characteristics of the surgical procedures are illustrated in Table 4.
No significant differences on the tumor resection side (p=0.7521), surgical approach (open vs minimally invasive surgery, p=0.1939), and operative time (p=0.6333) were reported. Whereas the LUAD group included more patients undergoing lobectomies upon neoadjuvant treatment (50/58 (86.2 %) vs 25/37 (67.6%), p=0.0298), the SQCA group comprised more patients undergoing multilobar resections (pneumonectomy, 8/37 (21.6%) vs 4/58 (6.9 %), p= 0.0351).
Regarding the neoadjuvant regimen, 18 patients (18.9%) underwent chemotherapy alone, 7 patients (7.4%) chemoimmunotherapy, one patient (1.1%) radiation therapy, 64 patients (67.4%) chemoradiation and 5 patients (5.3%) a combination of all three approaches. Patients with combined neoadjuvant chemo- and radiation therapy were significantly more frequent in the SQCA group (30/37 (81.1 %) vs 34/58 (58.6 %), p=0.0228, Table 4).
The median in-hospital stay upon surgery was significantly longer in patients with SQCA (13.0 [9.5; 24.5] vs 11.0 [8.0; 14.0] days, p= 0.0458). Proportionally, the stay in the intensive care unit was longer in the SQCA group (3.0 [1.0; 5.0] vs 1.0 [1.0; 2.0] days, p=0.0039).
The analysis of the intraoperative histological specimens revealed significantly more patients experiencing >10% vital tumor cells (TRG_IIa) in the LUAD group (27/58 (46.6 %) vs 5/37 (13.5%), p= 0.0009) and more patients with no vital tumor cells (TRG_III) in the SQCA group (20/37 (54.1%) vs 10/58 (17.2 %), p=0.0002). This was under the significantly higher incidence of yT0 tumors in the SQCA group (22/37 (59.5%) vs 10/58 (17.2 %), p<0.0001) and lower incidence of yT4 tumors in the SQCA group (1/37 (2.7%) vs 8/58 (13.8 %), p= 0.0719, Table 5).
The tumor size before and after neoadjuvant treatment was larger in the SQCA group in comparison to the LUAD group (Table 5).
3.2. Logistic Regression Analysis of Risk Factors
Since TRG_III, which is defined by the absence of the vital tumor cells (CPR) in the histological specimens, occurred significantly more frequently in the SQCA group (20/37 (54.1%) vs 10/58 (17.2 %), p=0.0002), it is of particular interest to characterize this patient subgroup to identify meaningful parameters that independently predict tumor regression.
For this reason, a univariate analysis considering two groups (TRG I_II and TRG_III) was performed, considering the histological classification of the primary tumor (LUAD, SQCA). Intraoperative histology, lymph node size, as well as tumor size after neoadjuvant treatment were significantly associated with tumor regression grade (p<0.05 each). To assess easily available continuous parameters for clinical routine, optimal cut-off values derived by ROC analysis were computed as binary variables and incorporated in a multivariable binary regression analysis. The following parameters were further confirmed as statistically significant: intraoperative histology (SQCA), lymph node size > 1.7cm, and absolute delta tumor size before-after neoadjuvant therapy >2.6 cm. The corresponding odds ratios (OR) in predicting TPG_III and their 95% confidence intervals were 6.88 (2.40-19.77, p=0.0003), 3.13 (1.11-8.83, p=0.0310) and 3.76 (1.20-11.81, p=0.0233). The robustness of the regression analysis was confirmed by three independent methods (Enter, Forward LR, and Backward LR). The results were also reproduced by using absolute values instead of binary variables (derived from cut-off values) with qualitatively unchanged results.
The logistic regression model is summarized in Table 6.
To assess easily available parameters for clinical routine, relative delta values ((tumor size before neoadjuvant treatment - tumor size after neoadjuvant treatment/tumor size before neoadjuvant treatment) x 100) were also calculated. By using ROC Analysis and the Youden criterion we identified a relative delta value >30%, which coincides with a 30% tumor reduction after neoadjuvant treatment, as an independent predictor of complete pathologic response. The multivariable analysis was reproduced as sensitivity analysis when using relative delta values for tumor reduction (>30%), with qualitatively unchanged results (Table 7). This result was consistently verified with three selection methods (Enter, Forward, and Backward).
3.3. Survival Analysis
To assess the overall survival (OS) of the patients included in the study, we further analyzed each clinical parameter presented in Table 1, Table 2, Table 3, Table 4 and Table 5 with the Kaplan–Meier method. Median overall survival for the whole cohort was 71 [47.0-95.0] months. Forty-six death events were recorded in the whole cohort during 330 cumulative follow-up years (Figure 2A).
Patients aged 70 years or older experienced a reduced OS (n= 21, 5-year OS 38.1%) in comparison to younger patients (n=74, 5-year OS=55.9%, p=0.0325, Figure 2B)
No significant difference was noted in the OS of patients when considering BMI, smoking status, alcohol consumption, and comorbidities. Patients with FEV1, FVC, and DLCO >70% have a slightly improved OS (without statistical significance) in comparison to those patients with reduced lung function parameters. Patients suffering from LUAD (n=58) had an almost similar OS (5-year OS=49.4%) when compared to SQCA patients (n= 37, 5-year OS=53.5%, p=0.5041, Figure 2C).
Tumor side, lobe localization, and surgical approach (open vs. minimally invasive surgery) were not significantly associated with OS. An extended resection (>1 lobe, n=20) was significantly associated with a worse prognosis (5-year OS =30.0%) in comparison with patients undergoing standard lobectomies (n=75, 5-year OS 58.3%, p=0.0070, Figure 2D).
A tumor stage >yT3 (n=20) had a significantly decreased OS (5-year OS=26.8%) in comparison to smaller tumor stages (<yT3, n=75, 5-year OS 60.1%, p=0.0251, Figure 2E). The lymph node involvement after neoadjuvant therapy was not significantly associated with OS. No significant differences in OS could be reported when considering comparisons between tumor regression scores (TRG I vs II vs III, Figure 3A).
An absolute tumor size reduction > 2.6 cm after neoadjuvant therapy (absolute delta > 2.6cm) was significantly associated with an improved OS (n=24, 5-year OS=81.8% vs. n=71, 5-year OS=43.1%, p=0.0122, Figure 3B). Qualitatively unchanged results were obtained when using relative delta values (tumor size reduction > 30%). Accordingly, an improved OS was observed in the patient`s group experiencing a relative tumor size reduction> 30% (n=52, 5-year OS=65.1% vs. n=43, 5-year OS=38.8%, p=0.0415).
Patients experiencing a tumor recurrence or metastasis during follow-up had a significantly worse prognosis in comparison to those patients without (n=39, 5-year OS=26.0% vs. n=54, 5-year OS=77.3%, p=0.0017, Figure 3C).
To assess the independent predictive value of the abovementioned parameters on OS, a multivariate Cox regression analysis was performed. Here, we identified age (>70 years), extended resections (>1 lobe), and tumor recurrence or metastasis during follow-up as independent negative predictors of long-term OS. These predictors increased the risk of death by 2.70-, 2.11-, and 2.41-fold, respectively (Exp(B) OR 2.70 [1.37-5.36], p=0.0043, 2.11 [1.10-4.08], p=0.0257; 2.41 [1.27-4.54], p=0.0068. On the contrary, the tumor size reduction after neoadjuvant therapy (> 2.6 cm) was an independent parameter of improved OS (Exp(B) 3.82 [1.33-10.92], p=0.0126. Figure 3D, Table 8.
4. Discussion
The findings of our study shed light on the predictive value of histological and radiological parameters, including primary tumor histology, lymph node size, and tumor size upon neoadjuvant treatment initiation, in determining the effectiveness of tumor regression in patients undergoing major lung cancer resections. These insights have significant implications for treatment planning, prognostic assessment, and therapeutic decision-making in the management of advanced lung cancer.
In our cohort 30 patients (31.57%) experience CPR upon neoadjuvant therapy. Interestingly CPR was significantly higher in the SQCA group, by previous published data (4%-33%) [13,14,15].
Histological assessment of the primary tumor emerges as a critical determinant of treatment response in patients undergoing neoadjuvant therapy. In contrast to our results, Zens et al. showed that the major pathological response after neoadjuvant treatment was more observed in lung adenocarcinoma patients, where only 11% of SQCA had a complete pathological response [9]. In the retrospective analyses from Schreiner et al. CPR was more observed in patients with adenocarcinoma also [16].
Furthermore, various anatomical measurements of changes in tumor size and lymph node size on CT or PET/CT scans were analyzed to improve the preoperative CPR prediction. CT scan delivers anatomical information based on morphological tumor alterations. However, even after dramatic tumor downstaging, vital cells may still be present. Therefore, the morphological evaluation may be misleading in some patients. Despite this, we identified the rate of reduction in the primary tumor size on CT or PET/CT scans as an independent predictor of CPR. This result is in line with existing literature [17,18]. In contrast, a lack of correlation between CT-based volume reduction and pathologic response was identified by Cerfolio et al. and Pöttgen et al. [19,20]. The inconsistency might have resulted from the small sample size of these studies. Moreover, we identified the lymph node size > 1.7 cm at the time of diagnosis also as an independent predictor of CPR. Coroller et al. could also identify radiological features of lymph nodes as predictors of CPR after neoadjuvant treatment in NSCLC patients [21].
In our study, OS estimates were reduced in patients aged over 70 years, in resections of more than one lobe group, and in patients experiencing recurrence or metastasis during the follow-up period. Pilotto et al. developed a scoring system for squamous cell carcinoma patients of the lung, where the age of patients was also one of the risk factors in predicting OS in adjuvant and neoadjuvant therapy groups [22].
Patients with a tumor size reduction of more than 2.6 cm after neoadjuvant therapy could show better OS in our cohort. In contrast to our findings, Tanahashi et al. couldn’t find any survival benefits in patients with tumor size reduction after neoadjuvant therapy [17]. This could be explained by the difference in study population heterogeneity, cohort size, and chosen therapy regimens.
Surprisingly in our cohort, we couldn’t identify any significant benefit of OS in patients with pathological complete response in comparison to CheckMate 816 and Keynote 671 studies [23,24]. It can also be explained by the heterogeneity of patient populations and treatment regimens. Another reason for this may be the shorter follow-up periods in above mentioned studies.
While our study provides valuable insights into the predictive factors of tumor regression effectiveness in neoadjuvant-treated lung cancer patients, several limitations warrant consideration. The retrospective nature of our analysis may introduce inherent biases and confounding variables that could impact the interpretation of results. Additionally, the heterogeneity of patient populations and treatment regimens may limit the generalizability of our findings.
5. Conclusions
Prospective studies incorporating larger patient cohorts and standardized treatment protocols are needed to validate the prognostic utility of these histological parameters and refine predictive models for treatment response in neoadjuvant-treated lung cancer patients.
In summary, our study elucidates the predictive value of histological parameters, including primary tumor histology, lymph node involvement, and tumor size upon neoadjuvant treatment initiation, in determining the effectiveness of tumor regression in patients undergoing major lung cancer resections. These findings have significant implications for personalized treatment planning and prognostic assessment in the management of advanced lung cancer, ultimately guiding therapeutic decisions and improving patient outcomes.
Author Contributions
Conceptualization: F.D., M.G.S., F.M., and G.P.; Data curation: G.P.; Formal analysis: M.G.S. and R.A.H.; Investigation: F.D.; Methodology: F.D., M.G.S., F.M., R.A.H. and G.P; Resources: F.D., E.B., S.D., S.G., E.S. and G.O.; Software: M.G.S.; Supervision: G.P.; Validation: F.D. and G.P.; Visualization: M.G.S.; Writing – original draft: F.D. and M.G.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Ludwig Maximilian University of Munich (LMU), Munich, Germany, file number 24-0114.
Informed Consent Statement
Patient consent was waived due to retrospective and anonymized nature of the study by the Ethics Committee of the Ludwig Maximilian University of Munich (LMU).
Data Availability Statement
The datasets of the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank all colleagues from the Thoracic Surgery, Oncology, and Radiology Departments of the Robert Bosch Hospital Stuttgart for excellent clinical patient care, clinical expertise, and support in the data collection.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Siegel, R.L., et al., Cancer statistics, 2023. CA Cancer J Clin, 2023. 73(1): p. 17-48.
- Goldstraw, P., et al., The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol, 2016. 11(1): p. 39-51. [CrossRef]
- Liang, W., et al., Expert consensus on neoadjuvant immunotherapy for non-small cell lung cancer. Transl Lung Cancer Res, 2020. 9(6): p. 2696-2715. [CrossRef]
- Kalvapudi, S., et al., Neoadjuvant therapy in non-small cell lung cancer: basis, promise, and challenges. Front Oncol, 2023. 13: p. 1286104. [CrossRef]
- Blumenthal, G.M., et al., Current Status and Future Perspectives on Neoadjuvant Therapy in Lung Cancer. J Thorac Oncol, 2018. 13(12): p. 1818-1831. [CrossRef]
- Liu, X., et al., Current status and future perspectives on immunotherapy in neoadjuvant therapy of resectable non-small cell lung cancer. Asia Pac J Clin Oncol, 2022. 18(4): p. 335-343. [CrossRef]
- Xu, Z., et al., Adjuvant and neo-adjuvant immunotherapy in resectable non-small cell lung cancer (NSCLC): Current status and perspectives. Cancer Innov, 2023. 2(1): p. 65-78. [CrossRef]
- Junker, K., et al., Grading of tumor regression in non-small cell lung cancer : morphology and prognosis. Chest, 2001. 120(5): p. 1584-91.
- Zens, P., et al., A prognostic score for non-small cell lung cancer resected after neoadjuvant therapy in comparison with the tumor-node-metastases classification and major pathological response. Mod Pathol, 2021. 34(7): p. 1333-1344. [CrossRef]
- Goldstraw, P., et al., The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol, 2007. 2(8): p. 706-14. [CrossRef]
- Travis, W.D., et al., The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J Thorac Oncol, 2015. 10(9): p. 1243-1260.
- Travis, W.D., et al., IASLC Multidisciplinary Recommendations for Pathologic Assessment of Lung Cancer Resection Specimens After Neoadjuvant Therapy. J Thorac Oncol, 2020. 15(5): p. 709-740. [CrossRef]
- Gilligan, D., et al., Preoperative chemotherapy in patients with resectable non-small cell lung cancer: results of the MRC LU22/NVALT 2/EORTC 08012 multicentre randomised trial and update of systematic review. Lancet, 2007. 369(9577): p. 1929-37.
- Eberhardt, W.E., et al., Phase III Study of Surgery Versus Definitive Concurrent Chemoradiotherapy Boost in Patients With Resectable Stage IIIA(N2) and Selected IIIB Non-Small-Cell Lung Cancer After Induction Chemotherapy and Concurrent Chemoradiotherapy (ESPATUE). J Clin Oncol, 2015. 33(35): p. 4194-201. [CrossRef]
- Albain, K.S., et al., Radiotherapy plus chemotherapy with or without surgical resection for stage III non-small-cell lung cancer: a phase III randomised controlled trial. Lancet, 2009. 374(9687): p. 379-86. [CrossRef]
- Schreiner, W., et al., Pathologic complete response after induction therapy-the role of surgery in stage IIIA/B locally advanced non-small cell lung cancer. J Thorac Dis, 2018. 10(5): p. 2795-2803. [CrossRef]
- Tanahashi, M., et al., Role of fluorodeoxyglucose-positron emission tomography in predicting the pathological response and prognosis after neoadjuvant chemoradiotherapy for locally advanced non-small-cell lung cancer. Interact Cardiovasc Thorac Surg, 2022. 35(2). [CrossRef]
- Agrawal, V., et al., Radiologic-pathologic correlation of response to chemoradiation in resectable locally advanced NSCLC. Lung Cancer, 2016. 102: p. 1-8. [CrossRef]
- Cerfolio, R.J., et al., Repeat FDG-PET after neoadjuvant therapy is a predictor of pathologic response in patients with non-small cell lung cancer. Ann Thorac Surg, 2004. 78(6): p. 1903-9; discussion 1909. [CrossRef]
- Pottgen, C., et al., Value of 18F-fluoro-2-deoxy-D-glucose-positron emission tomography/computed tomography in non-small-cell lung cancer for prediction of pathologic response and times to relapse after neoadjuvant chemoradiotherapy. Clin Cancer Res, 2006. 12(1): p. 97-106. [CrossRef]
- Coroller, T.P., et al., Radiomic-Based Pathological Response Prediction from Primary Tumors and Lymph Nodes in NSCLC. J Thorac Oncol, 2017. 12(3): p. 467-476. [CrossRef]
- Pilotto, S., et al., Risk Stratification Model for Resected Squamous-Cell Lung Cancer Patients According to Clinical and Pathological Factors. J Thorac Oncol, 2015. 10(9): p. 1341-1348. [CrossRef]
- Forde, P.M., et al., Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. N Engl J Med, 2022. 386(21): p. 1973-1985. [CrossRef]
- Wakelee, H., et al., Perioperative Pembrolizumab for Early-Stage Non-Small-Cell Lung Cancer. N Engl J Med, 2023. 389(6): p. 491-503. [CrossRef]
- Remark, R., et al., Immune contexture and histological response after neoadjuvant chemotherapy predict clinical outcome of lung cancer patients. Oncoimmunology, 2016. 5(12): p. e1255394. [CrossRef]
- Betticher, D.C., et al., Prognostic factors affecting long-term outcomes in patients with resected stage IIIA pN2 non-small-cell lung cancer: 5-year follow-up of a phase II study. Br J Cancer, 2006. 94(8): p. 1099-106. [CrossRef]
Figure 1.
Study flow chart illustrating patient enrollment at study entry. Of 892 patients undergoing oncological thoracic surgery between 01.2016 and 12.2022, 108 (12.1%) patients with resectable primary lung tumors underwent neoadjuvant treatment and primary lung cancer resections. Thirteen (12.04%) patients experiencing rare histological tumor subtypes (e.g. adenosquamous carcinoma, synovial sarcoma, sarcomatoid carcinoma, low-grade differentiated sarcoma of the lung, neuroendocrine/ small cell lung cancer, and not otherwise specified tumors) were excluded from the study, thus 95 of 108 patients (87.96%) with primary resectable lung tumors of the lung were included. Based on the histology of the primary tumor, patients were categorized into two groups: lung adenocarcinoma group (LUAD, 58 patients, 61.1%), and squamous cell carcinoma group (SQCA, 37 patients, 38.9%). Based on the tumor regression grade (TRG) of the intraoperative specimens, patients were further stratified in TRG_I (LUAD:10.3%, SQCA:8.1%), TRG_II (LUAD:72.4%, SQCA:37.8%) and TRG_III (LUAD:17.2%, SQCA: 54.1%), respectively.
Figure 1.
Study flow chart illustrating patient enrollment at study entry. Of 892 patients undergoing oncological thoracic surgery between 01.2016 and 12.2022, 108 (12.1%) patients with resectable primary lung tumors underwent neoadjuvant treatment and primary lung cancer resections. Thirteen (12.04%) patients experiencing rare histological tumor subtypes (e.g. adenosquamous carcinoma, synovial sarcoma, sarcomatoid carcinoma, low-grade differentiated sarcoma of the lung, neuroendocrine/ small cell lung cancer, and not otherwise specified tumors) were excluded from the study, thus 95 of 108 patients (87.96%) with primary resectable lung tumors of the lung were included. Based on the histology of the primary tumor, patients were categorized into two groups: lung adenocarcinoma group (LUAD, 58 patients, 61.1%), and squamous cell carcinoma group (SQCA, 37 patients, 38.9%). Based on the tumor regression grade (TRG) of the intraoperative specimens, patients were further stratified in TRG_I (LUAD:10.3%, SQCA:8.1%), TRG_II (LUAD:72.4%, SQCA:37.8%) and TRG_III (LUAD:17.2%, SQCA: 54.1%), respectively.
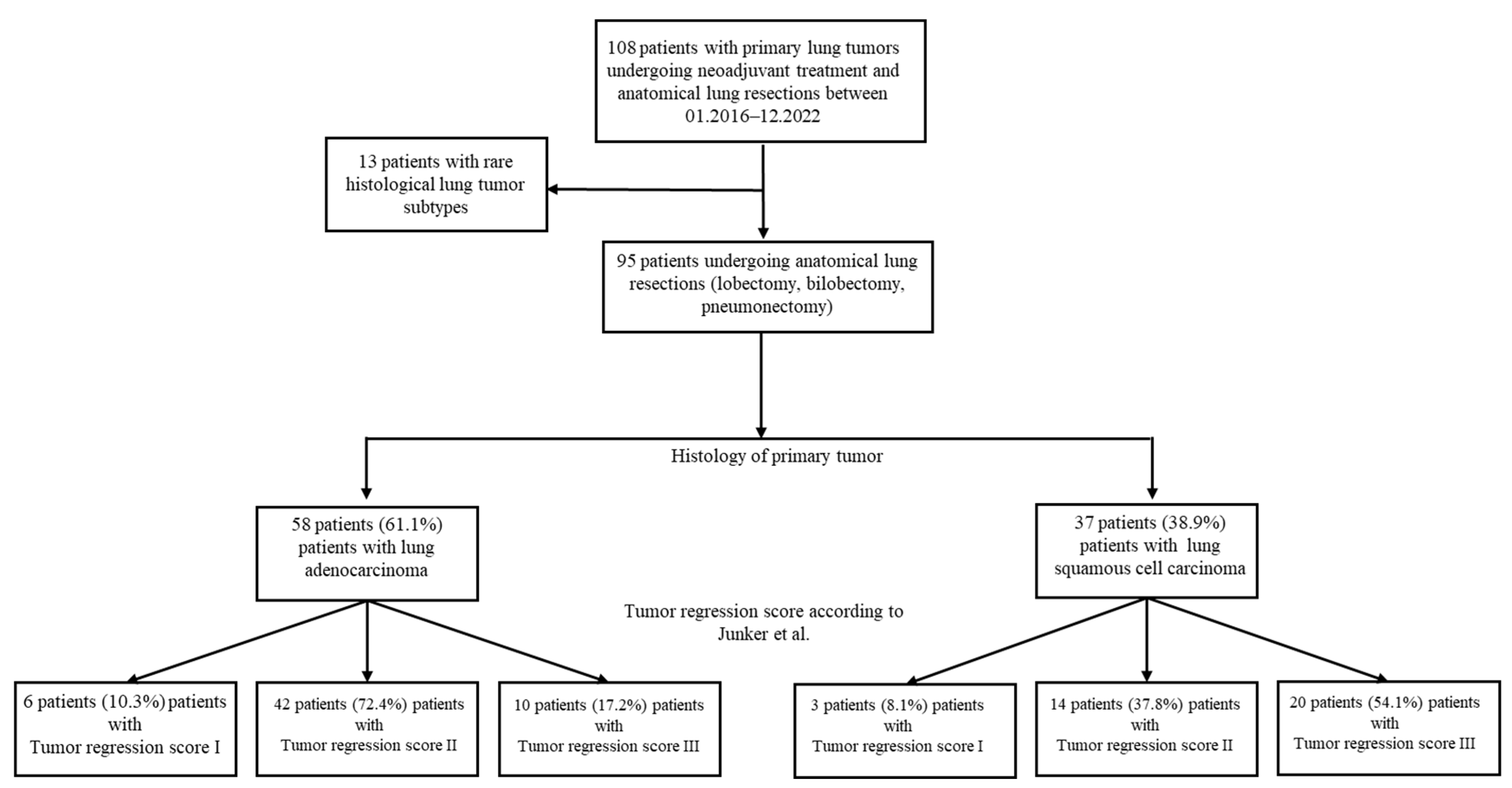
Figure 2.
Survival analysis. Kaplan-Meier curves depicting overall survival (A), OS according to age (B), OS according to histology (C), OS according to the extent of resection (D), and OS according to tumor size (TNM).
Figure 2.
Survival analysis. Kaplan-Meier curves depicting overall survival (A), OS according to age (B), OS according to histology (C), OS according to the extent of resection (D), and OS according to tumor size (TNM).
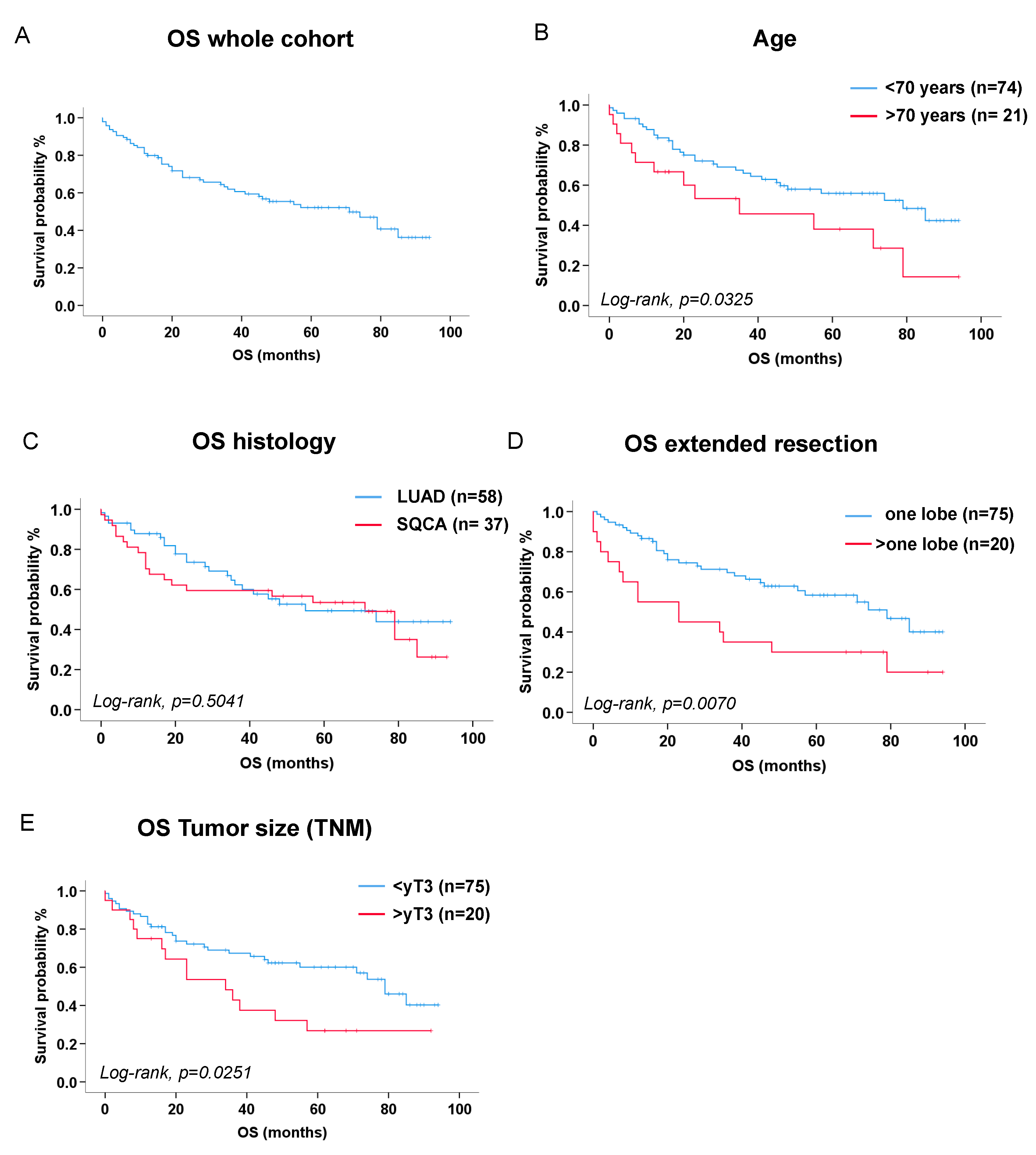
Figure 3.
Survival analysis. Kaplan-Meier curves depicting OS according to tumor regression grade (A), OS according to tumor size reduction after neoadjuvant therapy (B), OS according to tumor recurrence and metastasis (C), Cox proportional hazard regression analysis depicting independent predictors of OS (D).
Figure 3.
Survival analysis. Kaplan-Meier curves depicting OS according to tumor regression grade (A), OS according to tumor size reduction after neoadjuvant therapy (B), OS according to tumor recurrence and metastasis (C), Cox proportional hazard regression analysis depicting independent predictors of OS (D).
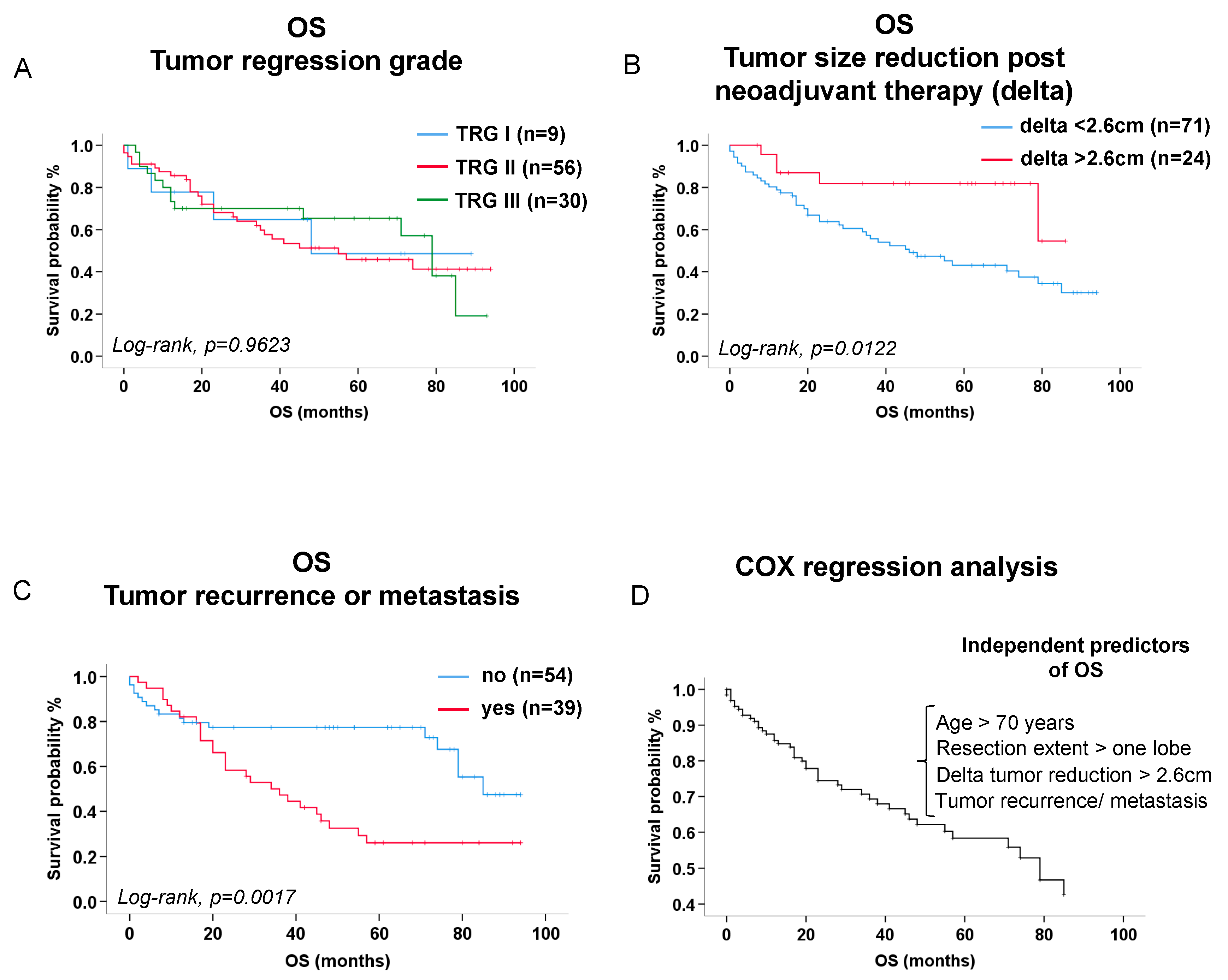

Table 1.
Demographics of patients undergoing neoadjuvant chemotherapy and surgical resection of primary lung tumors classified by histology of primary tumor.
Table 1.
Demographics of patients undergoing neoadjuvant chemotherapy and surgical resection of primary lung tumors classified by histology of primary tumor.
| Patient demographics at study entry | LUAD n=58 |
SQCA n=37 |
P-value |
|---|---|---|---|
|
Age (median, quartiles [1st; 3rd]) years Age > 65 (n, %) Age > 70 (n, %) Age > 80 (n, %) |
60.73 [54.5; 69.0] 21/58 (36.2 %) 11/58 (19.0 %) 0/58 (0 %) |
65.6 [60.5; 70.3] 21/37 (56.8 %) 10/37 (27.0 %) 0/37 (0 %) |
0.0687 0.0492 0.3558 |
|
Sex (n, %) Female Male |
27/58 (46.6 %) 31/58 (53.4 %) |
5/37 (13.5 %) 32/37 (86.5 %) |
0.0009 |
|
BMI (median, quartiles [1st; 3rd]) BMI < 18.5 kg/m2 (n, %) BMI > 18.5, < 25 kg/m2 (n, %) BMI > 25, < 30 kg/m2 (n, %) BMI > 30 kg/m2 (n, %) |
25.3 [23.0; 27.2] 0/58 (0 %) 25/58 (43.1 %) 29/58 (50.0 %) 4/58 (6.9 %) |
23.8 [21.8; 26.6] 0/37 (0 %) 24/37 (64.9 %) 10/37 (27.0 %) 3/37 (8.1 %) |
0.1842 0.0385 0.0264 1.0000 |
|
Pack years (median, quartiles [1st; 3rd]) Never smokers (n, %) Current smokers (n, %) Ex-smokers (n, %) |
30.0 [4.25; 45.0] PY 10/58 (17.2 %) 32/58 (55.2 %) 16/58 (27.6 %) |
40.0 [22.5; 52.5] PY 3/37 (8.1 %) 18/37 (48.6 %) 16/37 (43.2 %) |
0.0288 0.2066 0.5346 0.1143 |
| Alcohol (n, %) |
10/58 (17.2 %) |
6/37 (16.2 %) |
0.8964 |
|
Comorbidities (n, %) Respiratory Cardiovascular Renal Liver Neurological/ psychiatric Diabetes mellitus Non-pulmonary malignancies |
21/58 (36.2 %) 9/58 (15.5 %) 2/58 (3.4 %) 3/57 (5.3 %) 8/58 (13.8 %) 5/58 (8.6 %) 12/58 (20.7 %) |
18/37 (48.6 %) 2/37 (5.4 %) 3/37 (8.1 %) 3/37 (8.1 %) 3/37 (8.1 %) 7/37 (18.9 %) 4/37 (10.8 %) |
0.4546 0.1331 0.3744 0.6769 0.3984 0.1407 0.2096 |
|
Lung function parameters (median, quartiles [1st; 3rd]) FVC (absolute values, L) FEV1 (absolute values, L) DLCO (absolute values, L) |
3.18 [2.76-3.79] 2.25 [1.97-2.92] 5.29 [4.23-6.25] |
3.37 [2.84-4.19] 2.24 [1.64-3.07] 4.40 [3.31-6.05] |
0.2476 0.4897 0.0393 |
|
Lung function parameters (median, quartiles [1st; 3rd]) FVC (predicted, %) FEV1 (predicted, %) DLCO (predicted, %) FEV1/ FVC(%) |
82.50 [72.75-98.00] 80.50 [67.00-90.25] 62.50 [50.50-70.50] 95.00 [87.00-102.00] |
79.00 [71.50-91.00] 69.00 [55.50-85.00] 48.00 [42.00-62.00] 88.00 [78.00-95.00] |
0.2903 0.0103 0.0023 0.0014 |
Abbreviations: BMI: body mass index; PY: pack years; FVC: functional vital capacity; FEV1: forced expiratory volume in one second; DLCO: diffusing capacity of the lung for carbon monoxide.
Table 2.
Preoperative laboratory tests in patients undergoing neoadjuvant chemotherapy and surgical resection of primary lung tumors classified by histology of primary tumor.
Table 2.
Preoperative laboratory tests in patients undergoing neoadjuvant chemotherapy and surgical resection of primary lung tumors classified by histology of primary tumor.
| Parameters preoperatively (median, quartiles [1st; 3rd]) |
LUAD n=58 |
SQCA n=37 |
P-value |
|---|---|---|---|
|
Blood counts Leukocytes (/nL) Erythrocytes (/pL) Hemoglobin (g/dL) Thrombocytes (/nL) Clinical chemistry CRP (mg/dL) Creatinine (mg/dL) Albumin (g/dL) LDH (IU/L) |
6.15 [4.58; 7.30] 3.74 [3.48; 3.91] 11.9 [11.10; 12.43] 240.5 [204.0; 288.25] 0.20 [0.10; 0.60] 0.90 [0.78; 1.00] 4.27 [3.90; 4.46] 200.0 [169.8; 244.0] |
5.60 [4.35; 7.90] 3.56 [3.33; 4.01] 11.6 [10.85; 12.60] 221.0 [198.5; 268.5] 0.50 [0.10; 1.30] 1.0 [0.80; 1.10] 4.00 [3.60; 4.35] 188.0 [174.0; 211.0] |
0.7923 0.7688 0.8396 0.3046 0.0206 0.1304 0.0281 0.2323 |
Abbreviations: CRP: C-reactive protein; eGFR: estimated glomerular filtration rate; LDH: lactate dehydrogenase.
Table 3.
Tumor characteristics in patients undergoing neoadjuvant chemotherapy and surgical resection of primary lung tumors classified by histology of primary tumor.
Table 3.
Tumor characteristics in patients undergoing neoadjuvant chemotherapy and surgical resection of primary lung tumors classified by histology of primary tumor.
| Tumor characteristics | LUAD n=58 |
SQCA n=37 |
P-value |
|---|---|---|---|
|
Tumor side (n, %) Left Right |
27/58 (46.6 %) 31/58 (53.4 %) |
16/37 (43.2 %) 21/37 (56.8 %) |
0.7521 |
|
Tumor localization (n, %) Left upper lobe Left lower lobe Right upper lobe middle lobe Right lower lobe |
17/58 (29.3 %) 10/58 (17.2 %) 22/58 (37.9 %) 2/58 (3.4 %) 7/58 (12.1 %) |
13/37 (35.1 %) 3/37 (8.11 %) 11/37 (29.7 %) 2/37 (5.4 %) 8/37(21.6 %) |
0.5515 0.2066 0.3521 0.6432 0.2131 |
|
TNM7 classification (n, %) cT1 cT2 cT3 cT4 Lymph node involvement (n, %) cN0 cN1 cN2 cN3 |
11/58 (19.0 %) 10/58 (17.2 %) 14/58 (24.1 %) 23/58 (39.7 %) 9/58 (15.5 %) 11/58 (19.0 %) 35/58 (60.3 %) 3/58 (5.2 %) |
0/37 (0 %) 4/37 (10.8 %) 9/37 (24.3 %) 24/37 (64.9 %) 4/37 (10.8 %) 7/37 (18.9 %) 22/37 (59.5 %) 4/37 (10.8 %) |
0.0048 0.3886 0.9830 0.0166 0.5151 0.9955 0.9315 0.3050 |
| Pleura visceralis infiltration (n, %) |
21/58 (36.2 %) |
4/37 (10.8 %) |
0.0061 |
|
TNM7 classification (n, %) yT0 yT1 yT2 yT3 yT4 Lymph node involvement (n, %) yN0 yN1 yN2 yN3 |
10/58 (17.2 %) 20/58 (34.5 %) 11/58 (19.0 %) 9/58 (15.5 %) 8/58 (13.8 %) 34/58 (58.6 %) 6/58 (10.3 %) 17/58 (29.3 %) 1/58 (1.7 %) |
22/37 (59.5 %) 10/37 (27.0 %) 2/37 (5.4 %) 2/37 (5.4 %) 1/37 (2.7 %) 33/37 (89.2 %) 4/37 (10.8 %) 0/37 (0 %) 0/37 (0 %) |
<0.0001 0.4459 0.0608 0.1331 0.0719 0.0014 0.9425 0.0003 0.4220 |
cT1-4: tumor stage 1-4 according to the TNM7 (tumor node metastasis staging system 7, [10]) assessed on computed tomography, cN0-3: lymph node involvement N0-3 according to the TNM7 on computed tomography. yT0-4: tumor stage 0-4 according to the TNM7 upon neoadjuvant therapy assessed from the intraoperative histology; yN0-3: lymph node involvement N0-3 according to the TNM7 upon neoadjuvant therapy assessed from the intraoperative histology.
Table 4.
Technical aspects of the tumor resection in patients undergoing neoadjuvant chemotherapy and surgical resection classified by histology of primary tumor.
Table 4.
Technical aspects of the tumor resection in patients undergoing neoadjuvant chemotherapy and surgical resection classified by histology of primary tumor.
| Features of the surgical procedures | LUAD n=58 |
SQCA n=37 |
P-value |
|---|---|---|---|
|
Resection side (n, %) Left Right |
27/58 (46.6 %) 31/58 (53.4 %) |
16/37 (43.2 %) 21/37 (56.8 %) |
0.7521 |
|
Surgical approach (n, %) Open (thoracotomy) Minimally invasive (VATS) Conversion to open |
50/58 (86.2 %) 5/58 (8.6 %) 3/58 (5.2 %) |
35/37 (94.6%) 2/37 (5.4%) 0/37 (0.0%) |
0.1939 0.7017 0.2791 |
|
Resection extent (n, %) Lobectomy Multilobar -Bilobectomy -Pneumonectomy |
50/58 (86.2 %) 4/58 (6.9 %) 4/58 (6.9 %) |
25/37 (67.6%) 4/37 (10.8%) 8/37 (21.6%) |
0.0298 0.7071 0.0351 |
|
Topographical resection (n, %) Sleeve resection Thoracic wall |
11/58 (19.0 %) 4/58 (6.9 %) |
9/37 (24.3%) 2/37 (5.4%) |
0.5321 1.000 |
| Surgery time (median, quartiles [1st; 3rd]) (minutes) |
213.0 [171.5; 262.5] |
216.0 [165.5;275.0] |
0.6333 |
|
Neoadjuvant therapy Chemotherapy Chemo- and Immunotherapy Radiation therapy Chemo- and Radiation therapy Chemo-, Immuno, and Radiation therapy |
14/58 (24.1 %) 5/58 (8.6 %) 0/58 (0.0 %) 34/58 (58.6 %) 5/58 (8.6 %) |
4/37 (10.8 %) 2/37 (5.4 %) 1/37 (2.7 %) 30/37 (81.1 %) 0/37 (0.0 %) |
0.1060 0.7017 0.3895 0.0228 0.1527 |
|
Adjuvant therapy Chemotherapy Immunotherapy Chemo- and Immunotherapy Radiation therapy Chemo-, Immuno, and Radiation therapy |
1/57 (1.8 %) 9/57 (15.8 %) 0/57 (0.0 %) 8/57 (14.0 %) 1/57 (1.8 %) |
0/36 (0.0 %) 0/36 (0.0 %) 1/36 (2.8 %) 1/36 (2.8 %) 1/36 (2.8 %) |
1.0000 0.0121 0.3871 0.0737 1.0000 |
|
Length of stay (median, quartiles [1st; 3rd]) (days) In-hospital stay ICU stay ICU > 3 days (n, %) ICU > 7 days (n, %) Readmission within 30 days (n, %) |
11.0 [8.0; 14.0] 1.0 [1.0; 2.0] 10/58 (17.2 %) 3/58 (5.2 %) 4/58 (6.9 %) |
13.0 [9.5; 24.5] 3.0 [1.0; 5.0] 12/37 (32.4%) 4/37 (10.8%) 4/37 (10.8%) |
0.0458 0.0039 0.0870 0.4255 0.7071 |
| Primary Tumor relapse or metastasis (n, %) |
31/57 (54.4 %) |
8/36 (22.2%) |
0.0022 |
|
Mortality (n, %) During maximal follow-up Within 30 days postoperatively |
25/58 (43.1 %) 2/58 (3.5 %) |
21/37 (56.8%) 2/37 (5.4%) |
0.5041 1.0000 |
|
Overall survival (estimate [lower bound; upper bound], months) |
55.00 [17.06; 92.94] |
71.00 [44.89; 97.11] |
0.5041 |
Abbreviations: ABT: allogenic blood transfusion; VATS: video-assisted thoracoscopic surgery.
Table 5.
Characterization of tumor regression proportion score according to Junker et al. in patients undergoing neoadjuvant therapy and major surgical resections classified by histology of the primary tumor.
Table 5.
Characterization of tumor regression proportion score according to Junker et al. in patients undergoing neoadjuvant therapy and major surgical resections classified by histology of the primary tumor.
| Characterization of Tumor regression score | LUAD n=58 |
SQCA n=37 |
P-value |
|---|---|---|---|
|
TNM7 classification (n, %) yT0 yT1 yT2 yT3 yT4 Lymph node involvement (n, %) yN0 yN1 yN2 yN3 |
10/58 (17.2 %) 20/58 (34.5 %) 11/58 (19.0 %) 9/58 (15.5 %) 8/58 (13.8 %) 34/58 (58.6 %) 6/58 (10.3 %) 17/58 (29.3 %) 1/58 (1.7 %) |
22/37 (59.5%) 10/37 (27.0%) 2/37 (5.4%) 2/37 (5.4%) 1/37 (2.7%) 33/37 (89.2%) 4/37 (10.8%) 0/37 (0.0%) 0/37 (0.0%) |
<0.0001 0.4459 0.0608 0.1331 0.0719 0.0014 0.9425 0.0003 1.0000 |
|
Tumor Regression Score (Junker et al) (n, %) TRG_I (> 95% vital tumor cells) TRG_IIa (> 10% vital tumor cells) TRG_IIb (< 10% vital tumor cells) TRG_III (no vital tumor cells) |
6/58 (10.3 %) 27/58 (46.6 %) 15/58 (25.9 %) 10/58 (17.2 %) |
3/37 (8.1%) 5/37 (13.5%) 9/37 (24.3%) 20/37 (54.1%) |
0.7166 0.0009 0.8664 0.0002 |
|
Tumor size in CT (median, quartiles [1st; 3rd]) (cm) Before neoadjuvant treatment After neoadjuvant treatment before surgery Delta (before-after) neoadjuvant treatment before surgery (absolute) Delta (before-after) neoadjuvant treatment before surgery (relative) Lymph node size in CT (median, quartiles [1st; 3rd]) (cm) Before neoadjuvant treatment |
3.95 [2.40; 6.68] 2.55 [1.50; 4.60] 1.15 [0.55; 2.50] 30.73 [14.95; 53.55] 1.60 [1.20; 2.03] |
5.50 [3.60; 6.35] 3.30 [1.85; 4.35] 1.70 [0.60; 3.10] 32.14 [14.17; 51.05] 1.60 [1.00; 2.20] |
0.2105 0.3758 0.4248 0.8397 0.9299 |
yT0-4: tumor stage 0-4 according to the TNM7 staging system upon neoadjuvant therapy assessed from the intraoperative histology; yN0-3: lymph node involvement N0-3 according to the TNM7 upon neoadjuvant therapy assessed from the intraoperative histology: TRG: tumor regression grade according to the classification of Junker et al [8]. Absolute delta values = tumor size before neoadjuvant treatment - tumor size after neoadjuvant treatment. Relative delta values = ((tumor size before neoadjuvant treatment - tumor size after neoadjuvant treatment) / tumor size before neoadjuvant treatment) x 100.
Table 6.
Binary logistic regression model predicting complete pathologic response in primary lung cancer patients undergoing neoadjuvant chemotherapy and major surgical resections.
Table 6.
Binary logistic regression model predicting complete pathologic response in primary lung cancer patients undergoing neoadjuvant chemotherapy and major surgical resections.
| Covariates for tumor regression | Exp(B) [95% CI] | P-value |
|---|---|---|
| Intraoperative histology (LUAD vs SQCA) | 6.88 [2.40-19.77] | 0.0003 |
| Lymph node size in preoperative PET > 1.7cm | 3.13 [1.11-8.83] | 0.0310 |
| Absolute Delta tumor size post neoadjuvant Therapy > 2.6cm | 3.76 [1.20-11.81] | 0.0233 |
Abbreviations: SQCA: squamous cell lung cancer; LUAD: Lung adenocarcinoma; Exp(B) = Odds ratio, 95% Confidence interval [lower bound-upper bound]. Absolute delta values = tumor size before neoadjuvant treatment - tumor size after neoadjuvant treatment.
Table 7.
Binary logistic regression model predicting complete pathologic response in primary lung cancer patients undergoing neoadjuvant chemotherapy and major surgical resections.
Table 7.
Binary logistic regression model predicting complete pathologic response in primary lung cancer patients undergoing neoadjuvant chemotherapy and major surgical resections.
| Covariates for tumor regression | Exp(B) [95% CI] | P-value |
|---|---|---|
| Intraoperative histology (LUAD vs SQCA) | 6.81 [2.34-19.77] | 0.0004 |
| Lymph node size in preoperative PET > 1.7cm | 3.86 [1.35-11.10] | 0.0119 |
| Relative delta (tumor size post neoadjuvant Therapy) > 30% | 4.54 [1.49-13.84] | 0.0079 |
Abbreviations: SQCA: squamous cell lung cancer; LUAD: Lung adenocarcinoma; Exp(B) = Odds ratio, 95% Confidence interval [lower bound-upper bound]. Relative delta values = ((tumor size before neoadjuvant treatment - tumor size after neoadjuvant treatment) / tumor size before neoadjuvant treatment) x 100.
Table 8.
Binary logistic regression model predicting overall survival in primary lung cancer patients undergoing neoadjuvant chemotherapy and major surgical resections.
Table 8.
Binary logistic regression model predicting overall survival in primary lung cancer patients undergoing neoadjuvant chemotherapy and major surgical resections.
| Independent predictors of overall survival | Exp(B) [95% CI] | P-value |
|---|---|---|
| Age (>70 years) | 2.70 [1.37-5.36] | p=0.0043 |
| Extended resections (>one lobe) | 2.11 [1.10-4.08] | p=0.0257 |
| Absolute tumor size reduction >2.6 cm after neoadjuvant therapy (absolute delta) | 3.82 [1.33-10.92] | p=0.0126 |
| Tumor recurrence or metastasis during follow-up | 2.41 [1.27-4.54] | p=0.0068 |
Abbreviations: Exp(B) = Hazard ratio, 95% Confidence interval [lower bound-upper bound]. Absolute delta values = tumor size before neoadjuvant treatment - tumor size after neoadjuvant treatment.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



