
Submitted:
12 July 2024
Posted:
15 July 2024
You are already at the latest version
Abstract
In Thailand, thousands of children living with perinatal HIV have been exposed to HIV-related stigma/discrimination but its frequency and expressions have been little studied. Our objective was to assess stigma/discrimination prevalence, associated risks factors and its expressions among adolescents. All caregivers of adolescents aged 12-19 years living with perinatal HIV and receiving antiretrovirals in 20 hospitals throughout Thailand were invited to complete a face-to-face questionnaire on their adolescent’s life and medical history. Of the 572 adolescents living in family settings, 464 had their HIV-status known in the community. The overall stigma/discrimination prevalence was 46%. Factors associated included living in the north-east region (OR: 2.80, 95%CI: 1.19-4.96), having a low intellectual ability (OR:2.68, 95%CI: 1.45-5.16), a lower Body Mass Index (BMI) (OR BMI > 18.5: 0.61, 95%CI: 0.37-0.98), conflicts with caregivers (OR: 1.86, 95%CI: 1.26-2.76) and caregivers being members of a support group (OR: 2.34, 95%CI: 1.58-3.48). Expressions of stigma/discrimination included bullying, social isolation, behavioral discrimination and public disclosure. The prevalence of stigma/discrimination among adolescents living with perinatal HIV is high. Despite existing policies, stigma eradication remains necessary to normalize their life as they grow into adulthood.
Keywords:
perinatal HIV
; stigmatization
; discrimination
; Thailand
; bullying
1. Introduction
Recognized by the United Nations General Assembly in 2006 as “a critical element in combating the global HIV/AIDS pandemic”[1], HIV-related stigma or discrimination has been defined as negative beliefs, feelings and attitudes towards people living with HIV, groups associated with people living with HIV and other key populations at high risk of HIV infection [2]. In addition, UNAIDS has characterized discrimination as the unfair and unjust action taken against an individual or group because of their real or perceived status or attributes, such as a health condition (e.g. HIV), socioeconomic status, gender, race, sexual identity or age [3]. HIV-related stigma or discrimination is recognized as an important cause of inequality [4], leading to poorer resources, socio-emotional skills and access to prevention and healthcare [5]. However, the extent of stigma/discrimination is difficult to assess because people may keep their HIV status secret for fear of being stigmatized or discriminated against.
Stigma/discriminations in perinatally infected children and adolescents comprises specific elements. First, orphanhood has been associated with child stigmatization [6,7]. Indeed, in hard-hit communities, if a parent dies, HIV is generally suspected of being the cause of death, and the HIV-stigma towards parents can be passed on to their children. Second, HIV-stigma could impede an adolescent’s education and cognitive development [8,9]. A lower intellectual capacity could be a cause of stigmatization in itself, and reinforce HIV-stigma. [10] Third, poor health has been found to be in itself a cause of stigma [4], notably when associated with visible symptoms of HIV [11,12]. Fourth, an early age at antiretroviral treatment initiation is an indicator of a long treatment history, usually using suboptimal antiretroviral combinations, which are associated with side-effects such as lipodystrophy. Although lipodystrophy is less common in children than in adults, it has been described as being associated with stigma [13]. Fifth, it has been shown that fear of stigma or discrimination can lead to poor access to HIV diagnosis [14] and reduced adherence to antiretroviral treatment, which can lead to disease progression and health problems and, in turn, stigma [15]. Sixth, adolescence is known to be a period of conflict with caregivers. For adolescents living with perinatal HIV, conflicts with caregivers may indicate resentment towards parents who transmitted the virus perinatally, or towards caregivers who may view them as a burden [16]. The hypothesis is that, in these circumstances, adolescents may be more sensitive to stigmatization [2] and have a lower perception of their happiness and mental health problems [6,17]. Seven, adolescents who do not know their HIV status may not perceive any social isolation [18,19]. As for caregivers, their participation in support groups would enable them to be better informed about HIV and to be more sensitive to stigma and discrimination [20]. Finally, a poor financial situation of the caregivers may reinforce stigma, as several studies have shown in [6,21,22]. Food accessibility has been specifically mentioned as a priority need for adolescents’ caregivers, as good nutritional status would reduce the visibility of the disease [23].
According to the Thai Ministry of Public health, in the early 2010s there were more than 12,000 HIV-infected adolescents aged 12-19 years old in the country, of whom at least 9,000 were receiving antiretroviral therapy [24]. In addition, according to UNAIDS, there were approximatively 520 000 people living with HIV in Thailand in 2021. Of these, around 2,000 were under 15 years of age [25], a dramatic reduction reflecting the success of the national Prevention of mother-to-child transmission (PMTCT) program [26].
While there is literature on HIV-related stigma in adults in Thailand [22,27,28,29,30], little is known about the specific population of children and adolescents living with perinatally HIV. To our knowledge, only one survey conducted at Chiang Mai University Hospital in northern Thailand has assessed stigma from the perspectives of caregivers [31] and adolescents [32]. It shows that discriminatory attitudes were most prevalent among caregivers themselves, and that HIV-related stigma/discrimination was identified in all aspects of adolescents’ lives.
To better understand the circumstances and expressions of stigma among children and adolescents living with perinatal HIV, we analyzed data from a multicenter cross-sectional study conducted among adolescents and their caregivers in Thailand [33]. The aim of this analysis was to assess the prevalence of stigma/discriminations and its associated factors among children/adolescents living with perinatal HIV in Thailand, as reported by their caregivers. We also conducted a qualitative description of the experiences of stigma/discrimination during childhood or adolescence as reported by their caregivers.
2. Materials and Methods
We used the quantitative and qualitative information obtained from caregivers of adolescents living with perinatal HIV who participated in the Teens Living With Antiretrovirals (TEEWA) study [33]. Briefly, the TEEWA study is a cross-sectional study conducted in 2011-2012 to examine the living conditions of adolescents living with perinatal HIV in Thailand compared with a control group from the general population. Caregivers (or legal guardians) of adolescents aged 12-19 years who were receiving antiretrovirals (ART) in 20 public hospitals across Thailand were invited to participate in the study with their adolescent child. At the hospital, the adolescents completed a detailed self-administered questionnaire about their daily lives. Because some adolescents did not know their HIV status, the adolescent questionnaire did not include questions about HIV. In a face-to-face interview conducted in the hospital, caregivers were asked about the adolescent's sociodemographic status, life and medical history, including HIV diagnosis and treatment history, experiences of stigma/discrimination, caregivers’ perception of their adolescent’s well-being, and their relationship. Clinical, virological and immunological information was extracted from medical records by the attending hospital nurse. Written informed consent was obtained from caregivers and assent was obtained from adolescents. Details regarding the TEEWA study have been published elsewhere [33].
The study was approved by the Faculty of Associated Medical Sciences of Chiang Mai University (ref: AF02-014) and by the ethics committees of the participating hospitals. All data were pseudo-anonymized using unique identifiers. Data are available upon request.
2.1. Inclusion Criteria
Only adolescents living in a family environment were included, as the question on stigma/discrimination was not asked for those living in orphanages. In fact, they usually live in a separate environment where they have limited interaction with the community. Moreover, these children/adolescents may not talk to orphanage staff about their experiences of stigma/discrimination.
2.2. Variables of interest: Stigma or Discrimination
Experiences of stigma/discrimination were recorded by asking caregivers whether they knew that the adolescent in their care had ever experienced stigma or social discrimination because of their HIV status. The settings in which these experiences of stigma or discrimination had occurred were also recorded: family, friends, school, hospital, village/neighborhood. Within each setting, the frequency of occurrence was also recorded.
2.3. Quantitative analysis
Covariates
The TEEWA questionnaire was build to assess the living situation of the adolescents living with perinatal HIV, but not specifically to address the question of stigma. Characteristics obtained from the caregiver interviews included the adolescent’s gender; age; region of residence (center, north, northeast, or south); orphan status (at least one parent alive versus both parents known to be dead); school delay (i.e. having repeated a grade); caregiver’s perceived intellectual ability of the adolescent (good/very good versus fair/low/very low); perceived adolescent’s health (very good/good versus fair/poor/very poor); perceived happiness (very happy/happy/fair versus unhappy/very unhappy); presence of conflicts with the adolescent (yes or no); caregiver’s knowledge of the adolescent’s awareness of his/her HIV status (yes versus no or unsure) ; age at ART initiation (0-6, and > 7 years old); adherence to ART (very good/good versus fair/poor/very poor).
Clinical characteristics of adolescents obtained from medical records included the adolescent’s most recent height and weight, CD4 cell count (≥ 500/mm3 versus <500/mm3), and HIV-1 RNA viral load (considered undetectable if less than 50 copies/mL). The body mass index (BMI) was calculated, and underweight was defined as less than 18.5 kg/m2.
Information about the adolescent’s caregiver included sex; age; relationship with the adolescent (parent, grandparent or sibling, aunt or uncle, and other); perceived financial situation (very good/good/fair versus difficult/very difficult); perceived current health status (very good/good versus fair/poor/very poor); and membership in a support group for people living with HIV/AIDS (yes or no).
Rationale for selecting the covariates included in the analysis
Among all the variables available, we considered those, which were mentioned in the literature on HIV in children and adults as associated with stigma. In addition to the socio-demographic factors to be taken into account, we focused on the variables listed in Table 1, bearing in mind that it is sometimes difficult to know whether these factors are the causes or consequences of stigmatization.
Statistical analyses
Only adolescents whose HIV-status was known in the community (as reported by their caregivers) were included in the analysis, as HIV-related stigma/discrimination attitudes require knowledge of HIV-status.
Adolescents and caregiver characteristics were tabulated and compared according reported experience of stigma and discrimination. Characteristics of adolescents and caregivers whose HIV-status had been disclosed to the community were compared with those whose status had been kept secret. The chi-square test was used to assess differences between groups, with statistical significance set at p<0.05.
Logistic regression was used to identify factors associated with any experience of discrimination and was carried out in two stages: Covariates with statistical significance <0.15 in the univariable analysis were included in the multivariable analysis [34]. Two additional logistic regressions were performed to assess the factors associated with “repeated stigma/discrimination”, i.e. when it was reported to occur regularly in at least one circumstance, and “diverse stigma/discrimination”, i.e. when it was reported in at least two circumstances. Statistical analyses were performed using R software (version 4.1.2).
3. Results
3.1. Characteristics of the study population
A total of 712 adolescents living with perinatal HIV and their caregivers were interviewed as part of the TEEWA study between March 2010 and July 2012 (Figure 1).
The text continues here.
Among them, those living in orphanages (n=136), those not currently receiving ART (n=3) and one with missing information on stigma were excluded, leaving a total of 572 adolescents. Adolescents whose HIV status was known in the community (n=464) were less likely to be from central Thailand (18% versus 52%, p<0.01), more likely to have lost both parents (47% versus 23%, p<0.01), and more likely to know their HIV status (90% versus 76%, p<0.01). Their caregivers were more often grand-parents (39.7% vs 30.6, p<0.01), older (52 versus 46 years, p<0.01), less likely to be in a good financial situation (60% versus 78%, p<0.01) and more likely to be members of a support group (45% versus 29%, p<0.01) than those whose status was kept secret (Table 1).
Of the 464 adolescents whose HIV status was known in the community and who were therefore exposed to stigma or discrimination, 58% were girls, with a median age of 14.5 years (IQR: 13.2-16.0). A detailed description of the adolescents and their caregivers is provided in Table 1.
The text continues here.
3.2. Quantitative Analysis
A total of 212 (46%) caregivers reported at least one occurrence of stigma/discrimination experienced by their child/adolescent (Table 1). Stigma/discrimination was more prevalent among those living in the Northeast region (16% versus 8%, p<0.01), those perceived by the caregiver to have an intellectual disability (22% versus 10%, p<0.01), those in conflicts with their caregiver (49% versus 35%, p<0.01), and if the caregiver reported being a member of a support group (56% versus 35%, p<0.01).
Stigma/discrimination had primarily occurred at school in 64% of reports (from classmates, teachers or staff), from friends in 59% of the cases, and from family members in 10% of the cases (Table 3). Stigmatization in hospital was reported in less than 1% of the cases s. Fifty-one percent of the caregivers reported repeated stigma/discrimination in the same context, and 52% in multiple contexts (Table 2).
The text continues here.
3.3. Multivariable Analysis
After adjustment for age and sex, the following covariates were included in the multivariable analysis: region, awareness of HIV status, perception of adolescent’s intellectual abilities, conflicts with caregivers, age at ART initiation, BMI, CD4 count and caregivers’ being membership of support groups. The factors that remained significantly associated with any experience of stigma/discrimination were: living in the northeast region (OR: 2.93, 95%CI: 1.36-6.45), having a low intellectual ability as perceived by caregivers (OR: 3.35, 95%CI: 1.66-7.10), conflicts with caregivers (OR: 1.81, 95%CI: 1.17-2.79), and caregivers being members of a support group (OR: 2.28, 95%CI: 1.48-3.53). Having a BMI > 18.5 was associated with less stigma/discrimination (OR: 0.61, 95%CI: 0.37-0.98).
After adjustment for age and gender, the factors that remained associated with “repeated stigma/discrimination” and with “diverse stigma/discrimination” are shown in Table 3. Awareness of the adolescent’s HIV status (OR: 3.55, 95%CI: 1.30-12.6) was also associated with experience of “diverse stigma/discrimination”.

Table 3.
Factors associated with stigma or discrimination after adjustment on age and gender.
| Any experience of stigma/discrimination | Diverse stigma/discrimination | Repeated stigma/discrimination | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Univariable | Multivariable | Univariable | Multivariable | Univariable | Multivariable | |||||||
| Factors | OR (95%CI) | p | aOR (95%CI) | p | OR (95%CI) | p | aOR (95%CI) | p | OR (95%CI) | p | aOR (95%CI) | p |
| Age | >0.99 | 0.15 | 0.90 | 0.99 | 0.48 | 0.09 | ||||||
| 12-13 | Ref | Ref | Ref | Ref | Ref | Ref | ||||||
| 14-15 | 1.02 (0.67-1.57) | 1.51(0.91-2.53) | 0.94 (0.57-1.54) | 0.99 (0.58-1.70) | 1.05 (0.63-1.75) | 1.28 (0.74-2.22) | ||||||
| 16-19 | 1.00 (0.61-1.65) | 1.73(0.92-3.27) | 1.14 (0.64-2.06) | 0.98 (0.51-1.84) | 1.57 (0.90-2.72) | 2.13 (1.14-3.95) | ||||||
| Sex Female |
Ref | 0.72 | Ref | 0.74 | Ref | 0.89 | Ref | 0.24 | Ref | 0.87 | Ref | 0.39 |
| Male | 1.07 (0.74-1.55) | 0.93 (0.59-1.45) | 0.97 (0.63-1.49) | 0.75 (0.45-1.22) | 0.93 (0.60-1.44) | 0.80 (0.49-1.31) | ||||||
| Region | 0.07 0.03 | 0.02 | 0.06 | 0.01 | 0.01 | |||||||
| Center | Ref | Ref | Ref | Ref | Ref | Ref | ||||||
| North | 1.38 (0.84-2.28) | 1.46 (0.84-2.56) | 1.07 (0.60-1.99) | 1.21 (0.65-2.34) | 0.80 (0.46-1.45) | 0.75 (0.41-1.39) | ||||||
| North-East | 2.64 (1.31-5.40) | 2.93 (1.36-6.45) | 2.67 (1.25-5.78) | 2.70 (1.21-6.13) | 2.17 (1.04-4.58) | 2.25 (1.04-4.94) | ||||||
| South | 1.68 (0.49-5.81) | 3.31 (0.77-15.5) | 1.94 (0.47-6.97) | 2.29 (0.52-8.89) | 0.63 (0.09-2.65) | 0.54 (0.08-2.46) | ||||||
| School delay | 0.38 | 0.16 | 0.19 | |||||||||
| No | Ref | Ref | Ref | |||||||||
| Yes | 1.25 (0.76-2.04) | 1.48 (0.85-2.53) | 1.46 (0.83-2.50) | |||||||||
| Orphan | 0.30 | 0.72 | 0.79 | |||||||||
| No | Ref | Ref | Ref | |||||||||
| Yes | 0.82 (0.57-1.19) | 0.93 (0.60-1.42) | 0.94 (0.61-1.45) | |||||||||
| Adolescent aware of his status | 0.03 | 0.15 | <0.01 | 0.01 | 0.35 | |||||||
| No | Ref | Ref | Ref | Ref | Ref | |||||||
| Yes | 1.98 (1.04-3.95) | 1.79 (0.81-4.12) | 3.52 (1.38-11.9) | 3.55 (1.30-12.6) | 1.45 (0.69-3.44) | |||||||
| Perception of adolescent’s health | 0.54 | 0.24 | 0.87 | |||||||||
| Good | Ref | Ref | Ref | |||||||||
| Very good | 0.87 (0.56-1.36) | 0.74 (0.45-1.23) | 1.04 (0.62-1.79) | |||||||||
| Perception of adolescent’s happiness | 0.50 | 0.50 | 0.87 | |||||||||
| Happy | Ref | Ref | Ref | |||||||||
| Unhappy | 0.70 (0.24-1.93) | 1.47 (0.45-4.13) | 1.10 (0.30-3.24) | |||||||||
| Perception of adolescent’s intellectual ability | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | ||||||
| Good | Ref | Ref | Ref | Ref | Ref | Ref | ||||||
| Low | 3.10 (1.69-5.91) | 3.35 (1.66-7.10) | 2.45 (1.32-4.45) | 2.99 (1.52-5.88) | 2.40 (1.29-4.39) | 2.92 (1.49-5.66) | ||||||
| Conflicts with adolescents | <0.01 | <0.01 | 0.01 | 0.07 | 0.15 | 0.53 | ||||||
| No | Ref | Ref | Ref | Ref | Ref | Ref | ||||||
| Yes | 1.83 (1.26-2.66) | 1.81 (1.17-2.79) | 1.73 (1.12-2.66) | 1.54 (0.96-2.49) | 1.38 (0.89-2.13) | 1.17 (0.72-1.89) | ||||||
| Age at ART initiation (years) | 0.07 | 0.06 | 0.47 | 0.68 | ||||||||
| 0-6 | Ref | Ref | Ref | Ref | ||||||||
| 7-19 | 0.69 (0.46-1.02) | 0.64 (0.40-1.02) | 0.76 (0.48-1.20) | 0.91 (0.57-1.45) | ||||||||
| Adherence to treatment | 0.30 | 0.94 | 0.79 | |||||||||
| Good | Ref | Ref | Ref | |||||||||
| Very good | 1.43 (0.72-2.92) | 0.97 (0.46-2.24) | 1.11 (0.52-2.69) | |||||||||
| BMI | 0.09 | 0.04 | 0.92 | 0.98 | ||||||||
| <18.5 | Ref | Ref | Ref | Ref | ||||||||
| >18.5 | 0.71 (0.48-1.05) | 0.61 (0.37-0.98) | 0.94 (0.60-1.47) | 0.99 (0.63-1.55) | ||||||||
| CD4 cell count (cells/mm3) | 0.08 | 0.06 | 0.97 | 0.87 | ||||||||
| <500 | Ref | Ref | Ref | Ref | ||||||||
| >500 | 1.43 (0.96-2.14) | 1.57 (0.98-2.55) | 0.98 (0.62-1.56) | 1.04 (0.66-1.67) | ||||||||
| Viral load | 0.74 | 0.03 | 0.07 | 0.50 | ||||||||
| Detectable | Ref | Ref | Ref | Ref | ||||||||
| Undetectable | 0.92 (0.57-1.48) | 1.78 (1.05-2.96) | 1.63 (0.89-2.93) | 1.20 (0.69-2.05) | ||||||||
| Caregiver member of a support group | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | <0.01 | ||||||
| No | Ref | Ref | Ref | Ref | Ref | Ref | ||||||
| Yes | 2.34 (1.61-3.42) | 2.28 (1.48-3.53) | 2.08 (1.35-3.21) | 1.88 (1.18-3.04) | 2.25 (1.46-3.51) | 1.99 (1.24-3.23) | ||||||
*OR = Odds Ratios ; aOR = adjusted Odds Ratio ; 95%CI: 95% confidence intervals ; p-value significant when <0.15 in the univariable analysis; <0.05 in the multivariable analysis.
The text continues here.
3.4. Qualitative Analysis : Experiences of Stigma or Social Discrimination
All caregivers who reported experiences of stigma/discrimination towards their adolescents (N=212) provided comments. In addition, 5 caregivers provided comments related to the fear of discrimination without having experienced it, and finally 9 caregivers reported discrimination from siblings (a category not considered separately in the questionnaire).
Inductive analysis of the verbatims identified four main themes of stigma: bullying or moral harassment was reported in 61% of cases, social isolation in 42% of cases, behavioral discrimination in 19% of cases, and public disclosure in 7% of cases (Table 2).
- Bullying or moral harassment
School was the main setting for bullying, where children/adolescents were mistreated by administrative staffs, teachers or friends. One of the most common forms of bullying was calling children “Pen AIDS”, i.e. “you have AIDS”. Such bullying sometimes led to temporary or permanent voluntary withdrawal from school. For three children who didn’t know their HIV status, this was a way of finding out they were HIV-positive. Sometimes the bullying was also related to the health or HIV status of the parents.
Grand-father: “The child said that her friends often bullied her, “Pen AIDS”, so that she refused to go to school for one year”
Aunt: “When the child was young, his friends always teased him that his parents got HIV and died from AIDS and that it will be the same for him. He came to me and asked what is AIDS?”
Bullying also occurred when children showed visible physical symptoms.
Aunt: “My niece could not go to school because the director said the other parents don’t want a child who has skin wounds on her body.
- Social isolation
Another major issue raised by caregivers was the social isolation resulting from the children’s HIV status. This isolation occurred at school, in the community and even within the family. The main reason given was the fear of infection.
Grand-mother: “The teacher didn’t pay attention when my grand-daughter was asking permission to go out of the classroom in order to take her medication. Also when she was sick at school, she had to manage to call home on her own”
Mother: “The school director refused to enroll my son, because in that year, his own child was attending the school and he feared that they may be close”
Mother: “In kinder-garden, nobody dare to sit near my daughter”
In the community, parents of other children or neighbors also tended to forbid their children from playing with children who were known to be living with HIV.
Grand-mother: “My grand-daughter was always told that as having AIDS she was not allowed to play with other children at school and in the community”
Finally, in the family context, some comments were made about discrimination due to fear of contamination.
Aunt: “Some cousins were disgusted and feared that my niece might transmit the disease to other children. They warned her not to get close to other children”
- Behavioral discrimination
Another common discrimination behavior was to avoid sharing the same food or water with children living with HIV, whether at school, in the children’s home or in any other place where the children might be invited.
Grand-mother: “My grand-daughter went to other people’s house and ask them to drink water, but they refused”
Beyond not sharing food or water, some children were unable to access services or help because of their status.
Grand-mother: “Between age 8 and 9 years, when my grand-son was going for a haircut, the barber refused to do”
- Public Disclosure
Some caregivers commented on how the child’s HIV status was disclosed to the community.
Father: “I was angry at the teacher because she (the teacher) told the students that my child had HIV infection in front of the whole classroom”
Aunt: “The neighbor said that my niece had AIDS, and asked why she wasn’t dying already. We both felt angry”
4. Discussion
Our study showed that, from the perspective of their caregivers, almost half of adolescents living with perinatal HIV had experienced stigma or discrimination. This occurred mainly at school, more often in the north-east region, was more likely to affect those perceived as mentally retarded, those in conflict with their caregivers, those with a BMI < 18.5, and those whose caregivers were members of support groups. It was not significantly associated with other factors such as gender, age, orphan status, health status including virological or immunological status, self-awareness of the HIV status, or adherence to ART.
In our study, 19% of caregivers reported that their child’s HIV status was not known to the community. In the study in Northern Thailand of adolescents living with perinatal HIV followed in Chiang Mai University hospital, about 40% of caregivers reported keeping their adolescent’s HIV status secret, a percentage twice as high as in our study [31]. The lack of disclosure in the community is likely related to anticipated stigma [35], as caregivers or adolescents may have chosen not to disclose their status [36].
It is difficult to compare our findings with those of other studies conducted in Thailand, as the populations and approaches used to study stigma/discrimination against adolescents are different. Similar to our study, a qualitative study conducted in Bangkok among 33 adolescents and young adults 15-24 years (more than half of whom were infected perinatally) indicates that the educational context was the main setting in which they encountered stigma/discrimination [37]. In contrast with the study in Chiang Mai University hospital [31] where almost half of the caregivers had discrimination attitudes towards their adolescents, caregivers in our study reported relatively few (10%) experiences of stigma/discrimination in the family context. It is possible that this frequency is underestimated, as specific questions about discriminatory attitudes in the family were not asked, and that caregivers may not consider these attitudes to be discriminatory. Finally, experience of stigma/discrimination in the health care setting were almost never reported (<1%). This contrasts with the situation in the United States, where a study of adolescents and young adults found that 38% had experienced HIV-related stigma/discrimination when accessing sexual health services, particularly women [38].
In our study, the most common expression of stigma/discrimination against children was teasing or bullying, reported by about a quarter of all caregivers. In the Chiang Mai study, 23% of caregivers reported that their adolescents had been teased and 11% bullied at school [31], a similar percentage to our findings. In our study, social isolation was mentioned by almost a fifth of all caregivers and was reinforced in case of physical symptoms. The word “rangkiat”, meaning “disgust”, was often used by caregivers to express how HIV-infected people were perceived by others.
We found that the prevalence of stigma/discrimination was highest in the Northeast region. This is consistent with the results of successive surveys on stigmatizing attitudes towards people living with HIV among the Thai adult population [29,30], and highlights the need to prioritize this region for interventions. Our study also shows a strong association between stigma/discrimination and lower intellectual ability among adolescents. In a previous analysis, it was found that adolescents who had experienced stigmatization at school were almost twice as likely to have a disrupted academic trajectory [10]. However, it is difficult to distinguish between HIV-related stigma and stigma associated with mental disability. Negative consequences of stigma on mental health have also been documented [39,40,41,42]. Finally, we found that reports of stigma/discrimination were more frequent when caregivers were member of an HIV support group. Through their participation in these groups, caregivers are better informed about HIV and may be more sensitive to stigma and discrimination.
We found no difference in the experience of stigma/discrimination according to gender. This is in contrast to findings in adults, where women were more likely to experience stigma/discrimination than men [27]. Similarly, unlike in adults, HIV-related stigma/discrimination was not associated with poor adherence [15]. In fact, during childhood, adherence depends primarily on the caregivers who provide ART and directly observe its intake [43,44]. There was also no association between stigma/discrimination and the viral load level or CD4 count. It should be noted that the virological and immunological response to ART was very good in both groups. As encouraging results in medical settings are found both in our population and other populations [45], stigma remains a factor that can facilitate the spread of HIV [46]. The transition to adulthood remains complex and should be manage in a multidisciplinary way [47].
Our findings may not be representative of the situation in the country as a whole, as the majority of adolescents were recruited from the northern region. However, it was conducted on a relatively large sample of adolescents living with perinatal HIV recruited in 20 hospitals of different size across Thailand. In addition, the study was carried out more than 10 years ago, and stigma is known to have decreased with the widespread use of ART [48].
The 46% prevalence of stigma/discrimination obtained from interviews with caregivers is likely to be an underestimate, as children/adolescents do not always report their experiences to their caregivers, and direct testimonies from adolescents’ were not available. Also, given the frequent change in caregivers due to parental separation or death, the caregiver at the time of the interview may not be aware of past experiences of child stigma or discrimination. However, our approach of interviewing caregivers rather than the adolescents themselves, while reducing the number of reports of stigma/discrimination, respected the fact that some adolescents had not been informed of their HIV status and also prevented them from recalling painful events in their lives. The age of the children/adolescents at the time they experienced stigma, and internalized self-stigma were not available. A specific Thai internalized HIV-stigma scale for adults was developed in 2023 [49]. However, the mixed methods used, with a life-history approach in which the adolescent’s life was reconstructed by the caregiver, alongside a qualitative questioning, enabled us to obtain detailed information about stigma/discrimination experiences in childhood and adolescence.
Thanks to the successful implementation of PMTCT, the number of adolescents living with perinatal HIV is decreasing significantly [50] and may no longer be considered a key population. However, as they reach adulthood, they may face the consequences of past discrimination in terms of access to university studies or certain jobs, and may face discrimination at work, in the community or in their romantic life [51]. We are currently conducting a follow-up study, TEEWA-2, in which the same ypung people will be asked directly about their current experiences of stigma/discrimination, as young adults [52].
In its National Strategy to End AIDS 2017-2030, Thailand has committed to reducing HIV-related discrimination by 90% [53]. While Thailand can be considered a success story in its fight against HIV/AIDS, in terms of prevention of sexual transmission, PMTCT, scaling up ART and combating stigma/discrimination among adults [54], our study highlights the vulnerability of children and adolescents for whom school-based interventions should be targeted.
Author Contributions
Conceptualization, S.L., validation, S.L., Y.Y. and Z.Z.; formal analysis, A.G.; investigation, W.S., P.J, W.C, C.R, M.K, U.S, S.S, S.T, T.K; writing—original draft preparation, A.G.; writing—review and editing, W.S., P.J, W.C, C.R, M.K, U.S, S.S, S.T, T.K, S.L ..; supervision, S.L.; funding acquisition, S.L. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by Sidaction, Grant AI22-1/01855 and OXFAM Great Britain, Grant THAA51.
Institutional Review Board Statement
“The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Faculty of Associated Medical Sciences of Chiang Mai University (ref: AF02-014) and by the ethics committees of the participating hospitals.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request..
Acknowledgments
We would like to thank Julie Pannetier, Aurore Camier, Marc Lallemant and Aboubakari Nambiema for reviewing and providing valuable suggestions to the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- United Nations General Assembly. Political Declaration on HIV/AIDS (Resolution 60/262), 2006. Accessed February 26th 2024 https://www.unaids.org/sites/default/files/sub_landing/files/20060615_hlm_politicaldeclaration_ares60262_en.pdf.
- UNAIDS, Evidence for eliminating HIV-related stigma and discrimination, 2020. Accessed February 26th, 2024. https://www.unaids.org/sites/default/files/media_asset/eliminating-discrimination-guidance_en.pdf.
- United Nations Agency for International Development (UNAIDS). Protocol for identification of discrimination against people living with HIV. 2000. Accessed February 26th, 2024. https://data.unaids.org/publications/irc-pub01/jc295-protocol_en.pdf.
- Hatzenbuehler, M.L.; Phelan, J.C.; Link, B.G. Stigma as a Fundamental Cause of Population Health Inequalities. Am. J. Public Heal. 2013, 103, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Relf, M.V.; Holzemer, W.P.L.; Holt, L.M.; Nyblade, L.; Caiola, C.P.E. A Review of the State of the Science of HIV and Stigma: Context, Conceptualization, Measurement, Interventions, Gaps, and Future Priorities. J. Assoc. Nurses AIDS Care 2021, 32, 392–407. [Google Scholar] [CrossRef] [PubMed]
- Cluver, L.; Orkin, M. Cumulative risk and AIDS-orphanhood: Interactions of stigma, bullying and poverty on child mental health in South Africa. Soc. Sci. Med. 2009, 69, 1186–1193. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Wu, Q.; Zhao, J.; Zhao, G.; Li, X.; Du, H.; Chi, P. Enacted Stigma Influences Bereavement Coping Among Children Orphaned by Parental AIDS: A Longitudinal Study with Network Analysis. Psychol. Res. Behav. Manag. 2023, ume 16, 4949–4958. [Google Scholar] [CrossRef]
- Horsakulchai, W.; Sermprasartkul, T.; Sumetchoengprachya, P.; Chummaneekul, P.; Rungruang, N.; Uthis, P.; Sripan, P.; Srithanaviboonchai, K. Factors associated with internalized HIV-related stigma among people living with HIV in Thailand. AIDS Care 2024, 1–10. [Google Scholar] [CrossRef]
- Lowther, K.; Selman, L.; Harding, R.; Higginson, I.J. Experience of persistent psychological symptoms and perceived stigma among people with HIV on antiretroviral therapy (ART): A systematic review. Int. J. Nurs. Stud. 2014, 51, 1171–1189. [Google Scholar] [CrossRef] [PubMed]
- Merville, O.; Puangmala, P.; Suksawas, P.; Kliangpiboon, W.; Keawvilai, W.; Tunkam, C.; Yama, S.; Sukhaphan, U.; Sathan, S.; Marasri, S.; et al. School trajectory disruption among adolescents living with perinatal HIV receiving antiretroviral treatments: a case-control study in Thailand. BMC Public Heal. 2021, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Logie, C.; Gadalla, T. Meta-analysis of health and demographic correlates of stigma towards people living with HIV. AIDS Care 2009, 21, 742–753. [Google Scholar] [CrossRef] [PubMed]
- Kimera, E.; Vindevogel, S.; Reynaert, D.; Justice, K.M.; Rubaihayo, J.; De Maeyer, J.; Engelen, A.-M.; Musanje, K.; Bilsen, J. Experiences and effects of HIV-related stigma among youth living with HIV/AIDS in Western Uganda: A photovoice study. PLOS ONE 2020, 15, e0232359. [Google Scholar] [CrossRef]
- Brener, L.; Callander, D.; Slavin, S.; de Wit, J. Experiences of HIV stigma: The role of visible symptoms, HIV centrality and community attachment for people living with HIV. AIDS Care 2013, 25, 1166–1173. [Google Scholar] [CrossRef]
- Katz, I.T.; E Ryu, A.; Onuegbu, A.G.; Psaros, C.; Weiser, S.D.; Bangsberg, D.R.; Tsai, A.C. Impact of HIV-related stigma on treatment adherence: systematic review and meta-synthesis. J. Int. AIDS Soc. 2013, 16, 18640. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Munir, K.; Kanabkaew, C.; Le Coeur, S. Factors influencing antiretroviral treatment suboptimal adherence among perinatally HIV-infected adolescents in Thailand. PLOS ONE 2017, 12, e0172392. [Google Scholar] [CrossRef] [PubMed]
- Rutakumwa, R.; Zalwango, F.; Richards, E.; Seeley, J. Exploring the Care Relationship between Grandparents/Older Carers and Children Infected with HIV in South-Western Uganda: Implications for Care for Both the Children and Their Older Carers. Int. J. Environ. Res. Public Heal. 2015, 12, 2120–2134. [Google Scholar] [CrossRef] [PubMed]
- Amuri, M.; Mitchell, S.; Cockcroft, A.; Andersson, N. Socio-economic status and HIV/AIDS stigma in Tanzania. AIDS Care 2011, 23, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Wiener, L.S.; Battles, H.B.; Heilman, N.; Sigelman, C.K.; A Pizzo, P. Factors associated with disclosure of diagnosis to children with HIV/AIDS. 1996, 7, 310–24. [Google Scholar] [PubMed]
- Robinson, A.; Cooney, A.; Fassbender, C.; McGovern, D.P. Examining the Relationship Between HIV-Related Stigma and the Health and Wellbeing of Children and Adolescents Living with HIV: A Systematic Review. AIDS Behav. 2023, 27, 3133–3149. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, S.C.; Sikkema, K.J.; Somlai, A. People living with HIV infection who attend and do not attend support groups: A pilot study of needs, characteristics and experiences. AIDS Care 1996, 8, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Tzemis, D.; Forrest, J.I.; Puskas, C.M.; Zhang, W.; Orchard, T.R.; Palmer, A.K.; McInnes, C.W.; Fernades, K.A.; Montaner, J.S.; Hogg, R.S. Identifying self-perceived HIV-related stigma in a population accessing antiretroviral therapy. AIDS Care 2012, 25, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Rayanakorn, A.; Ong-Artborirak, P.; Ademi, Z.; Chariyalertsak, S. Predictors of Stigma and Health-Related Quality of Life Among People Living with HIV in Northern Thailand. AIDS Patient Care STDs 2022, 36, 186–193. [Google Scholar] [CrossRef]
- Chem, E.D.; Ferry, A.; Seeley, J.; Weiss, H.A.; Simms, V. Health-related needs reported by adolescents living with HIV and receiving antiretroviral therapy in sub-Saharan Africa: a systematic literature review. J. Int. AIDS Soc. 2022, 25, e25921. [Google Scholar] [CrossRef]
- National Health Statistical Office (NHSO), National Statistical Office (NSO) the 2010 Population and Housing Census.
- UNAIDS, Thailand country factsheet, 2022. Accessed February 26th, 2024. https://www.unaids.org/en/regionscountries/countries/thailand.
- Lolekha, R.; Boonsuk, S.; Plipat, T.; Martin, M.; Tonputsa, C.; Punsuwan, N.; Naiwatanakul, T.; Chokephaibulkit, K.; Thaisri, H.; Phanuphak, P.; et al. Elimination of Mother-to-Child Transmission of HIV — Thailand. Mmwr. Morb. Mortal. Wkly. Rep. 2016, 65, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Pannetier, J.; Lelièvre, E.; Le Cœur, S. HIV-related stigma experiences: Understanding gender disparities in Thailand. AIDS Care 2015, 28, 170–178. [Google Scholar] [CrossRef]
- Zhang, H. Intersectional stigma and coping strategies of single mothers living with HIV in Thailand. Cult. Heal. Sex. 2022, 25, 336–351. [Google Scholar] [CrossRef]
- Srithanaviboonchai, K.; Chariyalertsak, S.; Nontarak, J.; Assanangkornchai, S.; Kessomboon, P.; Putwatana, P.; Taneepanichskul, S.; Aekplakorn, W. Stigmatizing attitudes toward people living with HIV among general adult Thai population: Results from the 5th Thai National Health Examination Survey (NHES). PLoS ONE 2017, 12, e0187231–e0187231. [Google Scholar] [CrossRef]
- Chautrakarn, S.; Ong-Artborirak, P.; Naksen, W.; Thongprachum, A.; Wungrath, J.; Chariyalertsak, S.; Stonington, S.; Taneepanichskul, S.; Assanangkornchai, S.; Kessomboon, P.; et al. Stigmatizing and discriminatory attitudes toward people living with HIV/AIDS (PLWHA) among general adult population: the results from the 6th Thai National Health Examination Survey (NHES VI). J. Glob. Heal. 2023, 13, 04006. [Google Scholar] [CrossRef]
- Oberdorfer Perceived and Experienced Stigma and Discrimination among Caregivers of Perinatally HIV-Infected Adolescents in Thailand. J. Ther. Manag. HIV Infect. 2013. [CrossRef]
- Charles H. Washington, Peninnah Oberdorfer. Stigma and Discrimination among Perinatally HIV-Infected Adolescents Receiving HAART in Thailand. International Journal of Sociology Study; 2014 2, 33-41.
- Le Coeur S, Lelièvre E, Kanabkaew C, Sirirungsi W. A Survey of Adolescents Born with HIV: The TEEWA project in Thailand. Population (English edition) 2017, 72: 333-356. [CrossRef]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Aurpibul, L.; Tangmunkongvorakul, A.; Detsakunathiwatchara, C.; Masurin, S.; Srita, A.; Meeart, P.; Chueakong, W. Social effects of HIV disclosure, an ongoing challenge in young adults living with perinatal HIV: a qualitative study. Front. Public Heal. 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Hogwood, J.; Campbell, T.; Butler, S. I wish I could tell you but I can’t: Adolescents with perinatally acquired HIV and their dilemmas around self-disclosure. Clin. Child Psychol. Psychiatry 2012, 18, 44–60. [Google Scholar] [CrossRef]
- Mathew, R.S.; Boonsuk, P.; Dandu, M.; Sohn, A.H. Experiences with stigma and discrimination among adolescents and young adults living with HIV in Bangkok, Thailand. AIDS Care 2019, 32, 530–535. [Google Scholar] [CrossRef]
- Fair, C.D.; Berk, M. Provider perceptions of stigma and discrimination experienced by adolescents and young adults with pHiV while accessing sexual and reproductive health care. AIDS Care 2017, 30, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Thai, T.T.; Tran, V.B.; Nguyen, N.B.T.; Bui, H.H.T. HIV-related stigma, symptoms of depression and their association with suicidal ideation among people living with HIV in Ho Chi Minh City, Vietnam. Psychol. Heal. Med. 2022, 28, 1263–1274. [Google Scholar] [CrossRef]
- Aurpibul, L.; Kosalaraksa, P.; Kawichai, S.; Lumbiganon, P.; Ounchanum, P.; Songtaweesin, W.N.; Sudjaritruk, T.; Chokephaibulkit, K.; Rungmaitree, S.; Suwanlerk, T.; et al. Alcohol use, suicidality and virologic non-suppression among young adults with perinatally acquired HIV in Thailand: a cross-sectional study. J. Int. AIDS Soc. 2023, 26, e26064. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.V.; Abramowitz, S.; Koenig, L.J.; Chandwani, S.; Orban, L. Negative life events and depression in adolescents with HIV: a stress and coping analysis. AIDS Care 2015, 27, 1265–1274. [Google Scholar] [CrossRef] [PubMed]
- Aurpibul, L.; Sophonphan, J.; Malee, K.; Kerr, S.J.; Sun, L.P.; Ounchanum, P.; Kosalaraksa, P.; Ngampiyaskul, C.; Kanjanavanit, S.; Chettra, K.; et al. HIV-related enacted stigma and increase frequency of depressive symptoms among Thai and Cambodian adolescents and young adults with perinatal HIV. Int. J. STD AIDS 2020, 32, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Aurpibul, L.; Detsakunathiwatchara, C.; Khampun, R.; Wongnum, N.; Chotecharoentanan, T.; Sudjaritruk, T. Quality of life and HIV adherence self-efficacy in adolescents and young adults living with perinatal HIV in Chiang Mai, Thailand. AIDS Care 2022, 35, 406–410. [Google Scholar] [CrossRef] [PubMed]
- Fair, C.D.; Jutras, A. “I have hope, but I'm worried”: Perspectives on parenting adolescents and young adults living with perinatally-acquired HIV. Fam. Syst. Heal. 2022, 40, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P.; Spire, B.; Obadia, Y.; Moatti, J.-P. ; for the VESPA Group Discrimination against HIV-Infected People and the Spread of HIV: Some Evidence from France. PLOS ONE 2007, 2, e411–e411. [Google Scholar] [CrossRef] [PubMed]
- Mofenson, L.M.; Cotton, M.F. The challenges of success: adolescents with perinatal HIV infection. J. Int. AIDS Soc. 2013, 16, 18650. [Google Scholar] [CrossRef]
- Siraprapasiri, T.; Srithanaviboonchai, K.; Chantcharas, P.; Suwanphatthana, N.; Ongwandee, S.; Khemngern, P.; Benjarattanaporn, P.; Mingkwan, P.; Nyblade, L. Integration and scale-up of efforts to measure and reduce HIV-related stigma: the experience of Thailand. AIDS 2020, 34, S103–S114. [Google Scholar] [CrossRef]
- Dollfus, C.; Le Chenadec, J.; Faye, A.; Blanche, S.; Briand, N.; Rouzioux, C.; Warszawski, J. Long-Term Outcomes in Adolescents Perinatally Infected with HIV-1 and Followed Up since Birth in the French Perinatal Cohort (EPF/ANRS CO10). Clin. Infect. Dis. 2010, 51, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Uthis, P.; Suktrakul, S.; Wiwatwongwana, R.; Tangmunkongvorakul, A.; Sripan, P.; Srithanaviboonchai, K. The Thai Internalized HIV-related Stigma Scale. Front. Psychol. 2023, 14, 1134648. [Google Scholar] [CrossRef] [PubMed]
- Desmonde, S.; Lolekha, R.; Costantini, S.; Siraprapasiri, T.; Frank, S.; Bakkali, T.; Benjarattanaporn, P.; Hou, T.; Jantaramanee, S.; Kuttiparambil, B.; et al. A focused multi-state model to estimate the pediatric and adolescent HIV epidemic in Thailand, 2005–2025. PLOS ONE 2022, 17, e0276330. [Google Scholar] [CrossRef] [PubMed]
- Fernet, M.; Wong, K.; Richard, M.-E.; Otis, J.; Lévy, J.J.; Lapointe, N.; Samson, J.; Morin, G.; Thériault, J.; Trottier, G. Romantic relationships and sexual activities of the first generation of youth living with HIV since birth. AIDS Care 2011, 23, 393–400. [Google Scholar] [CrossRef]
- Le Coeur S, Hoang Ngoc Minh P, Sriphetcharawut S, Jongpaijitsakul P, Lallemant M, Puangmala P. The Teens Living with Antiretrovirals (TEEWA) study group. Mortality among adolescents living with perinatal HIV (APHIV) receiving antiretroviral therapy (ART): the Teens Living with Antiretrovirals (TEEWA) study in Thailand. 23rd Intl AIDS Conference (Aids 2020), 6-10 July 2020, San Francisco, USA.
- National Committee for the Prevention and Response to AIDS. Thailand National Strategy to End AIDS 2017-2030. April 2017.
- Harris, J.; Thaiprayoon, S. Common factors in HIV/AIDS prevention success: lessons from Thailand. BMC Heal. Serv. Res. 2022, 22, 1–10. [Google Scholar] [CrossRef]
Figure 1.
Flow chart describing the selection of the study population within the TEEWA study.
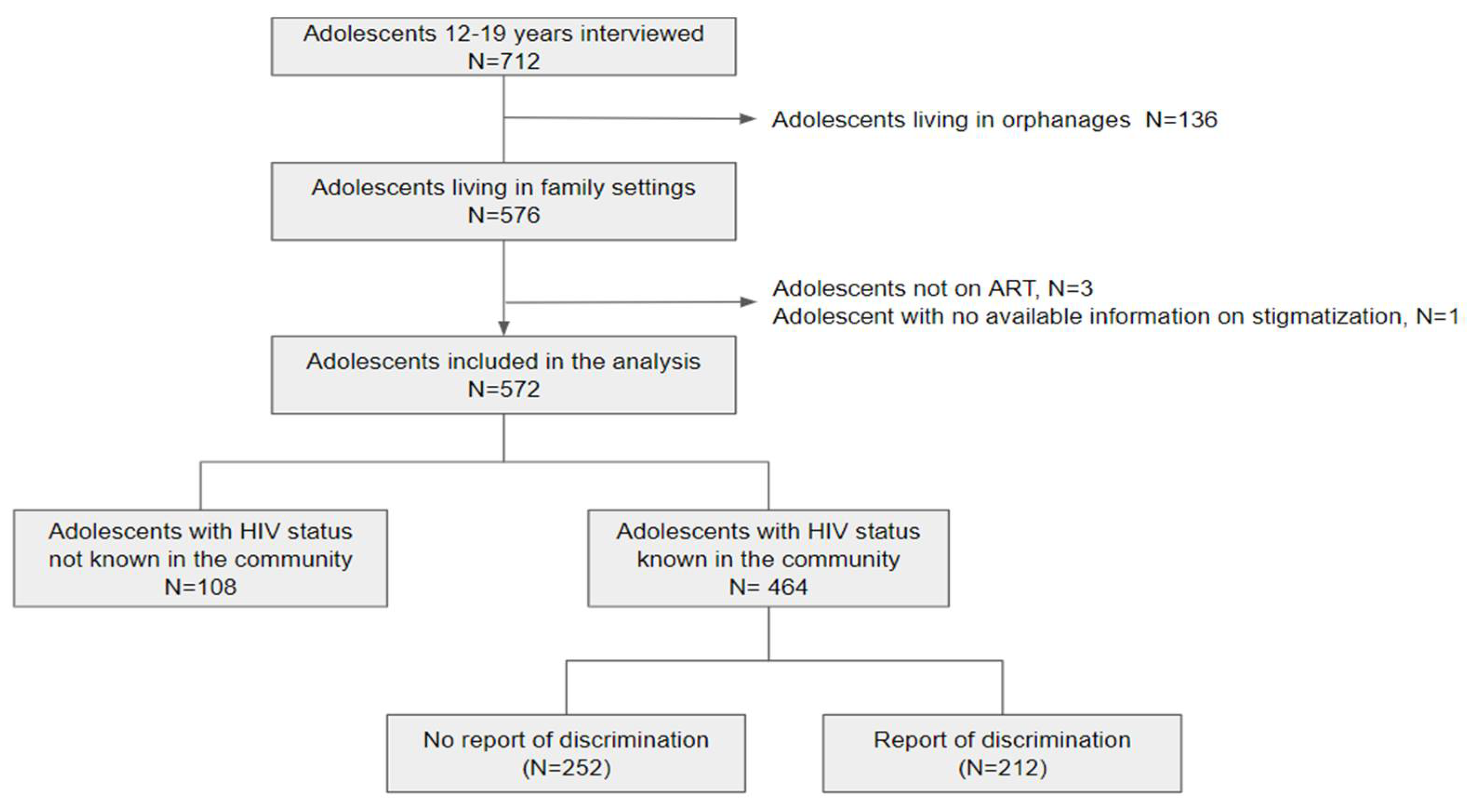
Table 1.
Characteristics of participants included in the analysis, overall and by knowledge of the adolescent’s HIV status in the community, and by report of stigma/discrimination among those whose status in known in the community.
Table 1.
Characteristics of participants included in the analysis, overall and by knowledge of the adolescent’s HIV status in the community, and by report of stigma/discrimination among those whose status in known in the community.
| Characteristics of adolescents, (from caregivers, % | Total | Knowledge of the HIV status in the community | Report of stigma/discrimination | ||||
|---|---|---|---|---|---|---|---|
| Yes | No | p | Yes | No | p | ||
| All | 572 (100) | 464 (81.1) | 108 (18.9) | 212 (45.7) | 252 (54.3) | ||
| Sex (female) | 334 (58.4) | 269 (57.8) | 65 (60.1) | 0.70 | 121 (57.0) | 148 (58.7) | 0.70 |
| Age (years) | 14.4 | 14.5 | 14.2 | 0.40 | 14.5 | 14.4 | 0.80 |
| Median [IQR] | 13.1, 16.0 | 13.2- 16.0 | 12.9-15.4 | 13.3-15.9 | 13.1, 16.2 | ||
| 12-13 | 203 (35.4) | 159 (34.2) | 44 (40.7) | 74 (34.9) | 85 (33.7) | ||
| 14-15 | 195 (34.1) | 159 (34.2) | 36 (33.3) | 75 (35.3) | 84 (33.3) | ||
| 16-19 | 174 (30.4) | 146 (31.4) | 28 (25.9) | 63 (29.7) | 83 (32.9) | ||
| Region | <0.01 | <0.01 | |||||
| Center | 139 (24.3) | 83 (17.8) | 56 (51.9) | 31 (14.6) | 52 (20.6) | ||
| North | 336 (58.7) | 315 (67.7) | 21 (19.4) | 142 (67.0) | 173 (68.6) | ||
| North-East | 66 (11.5) | 54 (11.6) | 12 (11.1) | 33 (15.6) | 21 (8.3) | ||
| South | 31 (5.4) | 12 (2.6) | 19 (17.6) | 6 (2.8) | 6 (2.4) | ||
| Orphan from both parents | 245 (42.8) | 220 (47.4) | 25 (23.1) | <0.01 | 95 (44.8) | 125 (49.6) | 0.30 |
| School delay (repeated a school year) | 87 (15.2) | 76 (16.3) | 11 (10.2) | 0.10 | 38 (17.9) | 38 (15.1) | 0.40 |
| Perception of adolescent’s intellectual capacity: low | 82 (14.4) | 72 (15.7) | 10 (9.3) | 0.20 | 47 (22.2) | 25 (10.0) | <0.01 |
| Perception of adolescent’s health: good or very good | 445 (77.8) | 357 (76.8) | 88 (81.4) | 0.40 | 161 (75.9) | 196 (77.8) | 0.60 |
| Perception of adolescents happiness: fair, happy or very happy | 554 (96.9) | 448 (96.3) | 106 (98.1) | 0.50 | 206 (97.1) | 242 (96.0) | 0.50 |
| Conflicts with adolescents | 235 (41.1) | 191 (41.1) | 44 (40.7) | 0.90 | 104 (49.1) | 87 (34.5) | <0.01 |
| Adolescent aware of his/her HIV status | 501 (87.6) | 419 (90.1) | 82 (75.9) | <0.01 | 198 (93.3) | 221 (87.7) | 0.10 |
| Age at ART initiation | 0.40 | 0.06 | |||||
| 0-6 | 180 (31.5) | 144 (31.0) | 36 (33.3) | 75 (35.3) | 69 (27.4) | ||
| 7-12 | 321 (56.1) | 258 (55.5) | 63 (58.3) | 115 (54.2) | 143 (56.7) | ||
| >12 | 55 (9.6) | 48 (10.3) | 7 (6.5) | 16 (7.5) | 32 (12.7) | ||
| Adherence to treatment: good or very good | 519 (90.7) | 421 (90.5) | 98 (90.7) | 0.70 | 196 (92.4) | 225 (89.3) | 0.60 |
| Information obtained from the medical records | |||||||
| BMI>18.5 | 206 (36.0) | 163 (35.1) | 43 (39.8) | 0.40 | 66 (25.0) | 97 (26.2) | 0.08 |
| CD4 cell count >500/cell/mm3 | 386 (67.5) | 318 (68.5) | 68 (63.0) | 0.30 | 154 (72.6) | 164 (65.1) | 0.07 |
| Undetectable viral load (<50 copies/mL) | 467 (81.6) | 378 (81.3) | 89 (82.4) | 0.90 | 174 (82.1) | 204 (81.0) | 0.70 |
| Characteristics of the caregivers | |||||||
| Sex (female) | 445 (77.8) | 354 (76.1) | 91 (84.2) | 0.07 | 167 (78.7) | 187 (74.2) | 0.20 |
| Age (median, IQR) | 50 (41, 60) | 52 (42, 61) | 46 (39, 57) | <0.01 | 52 (42, 61) | 50 (41, 60) | 0.50 |
| Relationship with the adolescent | 0.01 | 0.30 | |||||
| Parents | 77 (13.5) | 53 (11.4) | 24 (22.2) | 23 (10.8) | 30 (11.9) | ||
| Grandparents or siblings | 217 (37.9) | 184 (39.7) | 33 (30.6) | 86 (40.6) | 98 (38.9) | ||
| Aunt or uncle | 138 (24.1) | 117 (25.2) | 21 (19.4) | 46 (21.7) | 71 (28.2) | ||
| Other relatives | 140 (24.5) | 110 (23.7) | 30 (27.8) | 57 (26.9) | 53 (21.0) | ||
| Caregiver’s financial situation: good or very good | 363 (63.5) | 279 (60.0) | 84 (77.8) | <0.01 | 120 (56.6) | 159 (63.1) | 0.20 |
| Caregiver own’s health perception: good or very good | 528 (92.3) | 427 (91.8) | 101 (93.5) | 0.60 | 193 (91.0) | 234 (92.9) | 0.50 |
| Member of a support group | 239 (41.8) | 208 (44.7) | 31 (28.7) | <0.01 | 119 (56.1) | 89 (35.3) | <0.01 |
*Chi-square or student’s test. Significance is met when p<0.05 ** at least one parent alive vs. both parents known to be dead.
Table 2.
Context, frequency and types of the reported experiences of stigma and discrimination by adolescents living with perinatal HIV.
Table 2.
Context, frequency and types of the reported experiences of stigma and discrimination by adolescents living with perinatal HIV.
| N (%) | |
| Adolescents whose HIV status is known in the community | 464 (100.0) |
| Any experience of stigma/discrimination | 212 (45.6) |
| Circumstances of stigma/discrimination* (N=212) | |
| At school | 136 (64.2) |
| From friends | 125 (59.0) |
| From people in the village | 91 (42.9) |
| From family | 22 (10.4) |
| At the hospital | 5 (0.02) |
| Type of stigma/discrimination* (N=212) | |
| Bullying/moral harassment | 130 (61.3) |
| Social isolation | 90 (42.4) |
| Behavioral discrimination | 40 (18.9) |
| Public disclosure | 16 (7.5) |
| Repeated stigma/discrimination experiences** (N=464) | 108 (23.3) |
| Among adolescents with stigma/discrimination experience (N=212) | 108 (50.9) |
| Diverse stigma/discrimination experiences** (N=464) | 111 (23.9) |
| Among adolescents with stigma/discrimination experience (N=212) | 111 (52.3) |
*The denominator is the total number of stigma/discrimination affected children (212) **The denominator is the total number of adolescents with their HIV status known in the community (464).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



