
Submitted:
12 July 2024
Posted:
15 July 2024
You are already at the latest version
Abstract
Detecting and evaluating pain in people with cognitive impairment, especially dementia, is a challenge. Their ability to accurately report pain and comprehend related questions decreases the reliability of their self-report. This has contributed to the fact that pain is underdiagnosed and undertreated in this population, which can lead to involuntary ageism. The design and assessment of this training capsule under the context of the European COST-Action TD1005 responds to the need for education and training in "Pain Assessment In Cognitive Impairment, especially dementia" and the development of the internationally agreed observational PAIC15 scale. The 3-hour capsule, intended for healthcare workers and caregivers, consists of theoretical-practical levels: 1) basic concepts and challenges in pain in aging, cognitive impairment/dementia, 2) available scales and PAIC15, 3) video presentation of clinical cases illustrating a 3×2 matrix of situations (rest, transfer and experimental pain) and stages of disease (mild and moderate). The objectives focused on training the ability to observe, detect, and assess the signs of pain using PAIC15 and its feasibility. The pre-post analysis in a Master educational setting showed agreement with the results obtained in the Spanish national survey on 1) scarce knowledge of observational tools and their use, and 2) uncertainty in the identification of signs of pain and feasibility in moderate/severe scenarios. The capsule improved the ability to identify and evaluate the pain items, especially facial expressions, and their confidence on observational tools. Debriefings highlighted the relevance of observational scales in dementia and the gain obtained using the new observational instrument.
Keywords:
pain
; pain assessment
; cognitive impairment
; dementia
; PAIC15
; COST-Action
1. Introduction
Global population ageing and gains in life expectancy are also associated with a growing prevalence of (co)morbidity and functional decline resulting in increased burden of disease, demands for care and access to long-term care (LTC) [1]. In this UN Decade of Healthy Ageing [2] the most recent report proposes three-core LTC interventions to meet older people’s complex care needs [3]. The first one refers to screening-assessment-management of priority health conditions (such as pain and cognitive decline, among others) associated with decreased physical and mental capacities and functional ability. The second points at palliative care needs to prevent and relieve suffering. These two interventions encompass the third one on social care and support needs. Interestingly, programs and courses for carers and LTC workers aimed to increase their knowledge, skills, attitudes, and competence to provide safe and quality interventions are presented as important tools to build and strengthen human resources in these scenarios. However, the report also warns that, with few exceptions, care workers have limited access to specialized or relevant training [3].
Pain is common in many diseases and, in nursery homes (NH), its prevalence in older people can range from 22 to 85% [4]. In some chronic conditions, the prevalence of pain can be higher than the cardinal symptoms of these diseases [5]. According to recent systematic reviews, impairment of activities of daily living (ADL), arthritis, depression and cognitive impairment present the strongest association with pain in NH residents [4]. Longitudinal studies assessing the association between self-reported pain and ADL are already aware of the significant impact of pain leading to a decline in overall quality of life (QoL) in older people [4,6]. On the other hand, since age is the main risk factor for dementia and pain, the number of patients experiencing this ‘double jeopardy’ will also grow in the coming decades [7]. In a population-based investigations, dementia was associated with a lower incidence of pain reporting (4-43%) and analgesic usage (33%) among home-dwelling older people than in those without dementia (13-69% and 47%, respectively) [8]. In the case of NH, were about 67% of residents have cognitive impairment [9], their prevalence of pain is in the range of 8.6% to 79.6% [7,10]. Yet, chronic pain patients with dementia are undermedicated [11,12]. In this scenario, their QoL worsens with the progressive deterioration and loss of the ability to express pain orally [13,14,15]. Among these patients, pain is not only a source of discomfort and distress but it is frequently the underlying cause of behavioral symptoms [9,16]. Thus, pain in dementia usually manifests itself as irritability, agitation and sometimes even aggressiveness, which not only contribute to further complications in care but can lead to inappropriate treatment with antipsychotics [17,18,19] and medications aimed to counteract neuropsychiatric symptoms [9,16]. Therefore, a worrisome scenario derives from pain being under-detected and under or inappropriately treated in dementia [14,15,18,20].
One of the most probable reasons for the under-detection of pain and its deficiencies when doing so in patients with dementia, is because the diagnostic tools of pain, its classification and evaluation depend on a great extent on the intact cognitive and communication skills [14,15]. Both requirements are difficult to meet in dementia, since patients lose them throughout the course of the disease until they are completely absent in the more advanced stages [14,15]. For this reason, starting early 1990’s, a series of specialized tools were developed to assess pain in homes and residences for older people. Two decades after, through COST-Action TD1005 ‘Assessment of pain, in cognitive impairment, especially dementia’ (http://www.cost-td1005.net), basic and clinical researchers from 16 European countries joined efforts to study various aspects of pain in different subtypes of dementia, including pain diagnosis and pain cognitive examination, as well as a road map and guidelines for the appropriate assessment of pain in dementia. [19]. The European consortium developed a comprehensive and internationally agreed toolkit for assessing pain in older adults called PAIC [22] The PAIC15 scale is already available in 10 languages (German, French, English, Dutch, Italian, Spanish, Chinese, Arabic, Danish and Portuguese (Brazil)) and has been internationally validated in different clinical scenarios [i.e. 23,24]
Despite various factors contributing to it, the current inadequate assessment and management of pain in this group of patients can lead to involuntary double ageism based on age and mental health condition. Translational basic research on pain in Alzheimer’s disease (AD) also provides evidence of the preservation of pain and vulnerability of these populations [25,26] supporting consensus clinical reports that agree that a comprehensive approach for pain management in patients with dementia is needed [14,15,20,27]. Four key perspectives on pain in dementia are proposed: 1) the impact of neuropathological changes in dementia on pain, 2) assessment of pain in dementia, 3) efficient treatments, and 4) organizational and educational aspects that challenge pain management in dementia. [15,20,27]. In this latter respect, while evidence-based guidance is urgently needed, difficulties in pain management due to the lack of sufficient training and education for healthcare professionals at all levels and across all settings have been reported in our two COST-Action TD1005 surveys [15,28,29]. Here, it is interesting to note that, in addition to the relevance of education and training for LTC for older people discussed in the recent UN report [3], educational activities are the second of the four strategies tackling ageism from different disciplines and perspectives promoted by the Global Campaign after the UN Global Report on Ageism [30] and the global strategy and action plan on this decade of healthy aging [31].
Therefore, the present work aims to create a ‘training capsule’ for health professionals attending and caring people with cognitive impairment, especially dementia, which would later also be transferable to informal caregivers. The capsule should focus on knowing how to recognize the signs of pain in this clinical population, thus allowing them to improve their skills in the detection and assessment of pain, while becoming familiar with the use of the new PAIC scale [22].
2. Materials and Methods
2.1. Participants
As described in the next sections, participants were involved in the design of the training capsule (see 2.2.) and others in the assessment of it (see 2.3.). The first group consisted of older people with mild cognitive impairments (MCI) or dementia included in the research project COST-Action Spain [see 23,24]. The degree of cognitive impairment was mild to moderate so that verbal report could be assessed in all the participants. Selected clinical cases were chosen to illustrate the complexity of pain assessment in cognitive impairment/dementia. The second group of participants refers to the target recipients, master students with professional nursing experience with vulnerable populations (intensive care units, day centers, nursing homes, rehabilitation centers, etc) who would learn about the observational instruments to decode pain, particularly the PAIC instrument.
2.2. Design of the Training Capsule
The procedure of development of the capsule included three sections:
1) Bibliographic search: Exploration of articles, books and scientific reviews relevant to the topic at hand.
2) Preparation of teaching materials: Based on the bibliography and research, theoretical and practical content was prepared to be taught in the capsule.
The theoretical part aimed to cover 1) basic concepts and challenges in pain in aging and cognitive impairment, especially dementia, 2) the use of regulations/guidelines and available scales, 3) the PAIC15 scale [22].
With regards of the observational instrument, the key observation items of PAIC15 are the following: facial expression (frowning, narrowing eyes, raising upper lip, opening mouth, looking tense), body movements (freezing, guarding, resisting care, rubbing, restlessness) and vocalization (using pain-related words, shouting, groaning, mumbling, complaining). These items can be assessed with a 5 scoring system (0, not at all; 1, slight degree; 2 moderate degree; 3, great degree, x, not scorable) at rest, during an ADL, during guided movement or other specific conditions. Initial evidence suggests that PAIC15 test scores of >3 indicate “probable” pain and >5 indicate “mild” pain.
For the practical material, cases to illustrate the clinical scenarios were obtained from COST Action TD1005 Spain research materials [23,24]. In those previous occasions, all the families of people with cognitive impairment or dementia and healthy controls provided informed consent for the use of videos for academic and research purposes within the context of the COST Action TD1005. Relevant scenarios focusing on the assessment of pain in dementia were selected, these being easily transferable to those in the professional activity of the participants. Hence, cases were analyzed in conditions of rest but also of transfer, and experimental pain.
3) Design of the session: After several positive pilot experiences as workshops in psychogeriatric meetings (IPA, International Psychogeriatric Association) and continuous formation in clinical institutions, the session was designed. The present work included postgraduate students who received training on vulnerable groups in adulthood and old age as part of the University Master’s Degree in Nursing Innovation Applied to Vulnerability and Health at the Universitat Autònoma de Barcelona, which is relevant to various practical areas of professional nursing.
2.3. Assessment of the Training Capsule
In the practicum, participants learned to observe, detect and assess the different items of the PAIC scale through trial-and-error method, with direct expert feedback. On the other hand, the training process included a pre-post evaluation, that is, a knowledge test prior to the delivery of the capsule and a subsequent one that measured the changes achieved after the theoretical and practical sessions. A selection of questions from the self-administered “Questionnaire about the use of standards/guidelines, assessment of pain in cognitive impairment, especially dementia’ [29] was used. The pre-post test was part of the self-assessment of their academic achievements, it was submitted anonymously, and only the results of those who gave consent for its use to assess the capsule were included in the present analysis.
2.4. Statistical Analysis
Data are expressed as the frequency (%) or mean ± SEM. Chi-square analysis or Fisher exact test were performed with GraphPad QuickCalcs Web site https://www.graphpad.com/quickcalcs/contingency1/ San Diego, CA, USA (accessed on 25 June 2024) by Dotmatics was used. Chi-square, in all cases, p < 0.05 was considered statistically significant.
3. Results
3.1. Bibliographic Search
For the selection and prioritization of the contents, relevant articles of the COST-Action TD1005 consortium referred to in the PAIC15.org [https://paic15.com/en/leu-en/] that respond to the theoretical and practical needs were selected and provided as key references.
3.2. Preparation of Teaching Materials
In this training capsule, we developed didactic tools based on our current scientific research and recommendations of the literature [10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,27,28,29]. These tools were designed to conduct theoretical practical sessions under clinical scenarios involving the rest and transfer of older adults with cognitive impairment, especially dementia. The sessions would be carried out in two common clinical settings: the day hospital and a day center.
The training capsule was taught orally, supported by video presentations, which made it easily feasible for trial-and-error method, but also adaptable to videoconferencing and other digital formats.
The didactic material and clinical scenarios of this training capsule allowed to cover several dimensions:
3.2.1. Basic Introduction of Theoretical Concepts
Scenarios / clinical cases: Selected videos (about 1-3 minutes duration) of female and male patients (mean age: 78.0 ± 6.8 years old, GDS 3-5) participants in our research studies [23,24] were presented. The scenarios were real, exemplifying situations of rest and habitual transfer of older adults with dementia within the clinical environment of a day hospital and a day center) but that can be easily applied later to home settings.
Audiovisual support: Videos of older adults with dementia a resting and a transfer situation from our own research work [23,24] were used to demonstrate their applicability in these different cases according to the parameters studied. The video recording allowed trial-and-error until reaching criteria.
Observational instrument: The instrument consisted of the Spanish version of the extended PAIC scale [22], that contained the 35 items or key observation points for the recognition of 1. Facial expressions, 2, body movements and 3, vocalizations of older people with dementia. Once the training was completed, the brief version PAIC 15 was presented (https://paic15.com/wp-content/uploads/paic15_spanish.pdf).
Assessment of the ‘training capsule’: Based on the Spanish survey [29], an evaluation sheet considered several of the key aspects that must be reached once the training was completed. At the end of the session, during a debriefing session, the participants could verify their own results with those of the participants and the Delphi Panel published in the surveys [28,29] and discuss about the observational tools in dementia.
3.3. Design of the Session
The session was carried out in 3 consecutive steps, developed through a total of 3 hours that started with a get-to-know (15 min) and a pre-test (15 min), followed by the theoretical (45 min) section. After a 15 min break, the practical part (1 h) started and ended with a post-test (15 min) and a final debriefing (15 min). In detail, the main sections were as follows:
3.3.1. Step 1. Who Is Who and Clinical Settings (15 Minutes)
The instructor of the training capsule started the session with a ‘Who is who’ presentation to know the degree of mastery and knowledge of the participants, their clinical settings as well as the occupation or training they had. This was also used to give greater importance and depth to those aspects that are relevant, adjusting the discourse as much as possible to the contents of the participants. Spaces to answer questions, clarify concepts, and above all, create practical scenarios where the audience was the protagonist of their training.
3.3.2. Step 2. Theory (45 Minutes)
The theoretical part was developed within 6 conceptual frames (A to F):
A) Conceptual distinction between pain and nociception.
B) Objectives of the study and treatment of pain according to IPA, International Pain Association.
C) Basic criteria and use of unidimensional and multidimensional pain scales.
D) Determinants of pain management in aging and in people with different levels of cognitive impairment, especially dementia.
E) Prevalence, needs and assessment challenges of pain in these clinical populations.
F) COST-Action TD1005 and PAIC scale (https://paic15.com/en/start-en/).
3.3.3. Step 3. Practicum (1 Hour)
After a break, clinical cases illustrating a 3 × 2 matrix of situations (rest, transfer, experimental assessment) and stages of disease (mild and moderate) were presented to achieve 10 key aspects: acquisition, identification and applicability of the observational items (OI) and 7 key learning points of this training capsule. The different aspects would help to improve the participants’ criteria and skills to observe, detect and evaluate the signs of pain of PAIC 35 and PAIC-15 and the detection and correction of distracting/confounding intrinsic/extrinsic factors.
Key aspects:
- 1)
- The acquisition and unification of recognition criteria of the three elements of non-verbal communication on which the PAIC scale is based: facial expressions, body movements and vocalizations.
- 2)
- The identification of these components in clinical cases demonstrates their validity for differential diagnosis, overcoming confounding intrinsic/extrinsic factors (i.e., facial expression and posture in old age, environmental noises, etc).
- 3)
- The applicability in the clinical environment in a situation of rest and transfer (chair-to-chair or chair-to-bed displacements, for example).
- 4)
- Specific observation 1: Pain assessment in cognitive impairment can be challenging: To observe the difficulty in detecting pain (when it is present, but not obvious), also assessing the degree of reliability of the verbal response given by the patient. Using the PAIC 35 can help to gain skills for this type of assessment.
- 5)
- Specific observation 2: Incongruence between verbal self-report and non-verbal response: To contrast the non-verbal response (measure with the PAIC observational scale, in its three components) and the verbal response (VAS scale, the most used, as the standard).
- 6)
- Specific observation 3: PAIC 35 intersubject validity with/without pain in a situation of rest: To recognize the observable changes in the facial and body components and the vocalizations in the same patient in two rest situations, one in which it is known that there is pain and a second one where it is known that there is no pain.
- 7)
- Specific observation 4: PAIC 35 intersubject validity with/without pain during a transfer: To recognize the observable changes in the facial and body components and the vocalizations in the same patient in a new situation that implies transfer and possible elicitation of pain.
- 8)
- Specific observation 5: Rest and transfer conditions comparison: To contrast the changes in PAIC 35 observed in one situation (resting) and another (transfer) and assess whether there is a correlation between them.
- 9)
- Specific observation 6: PAIC 35 in experimental pain: To observe that in front of mild pressure stimuli (2 Kpa) in the shoulder administered with an algesimeter, the verbal and non-verbal response can be of null perception, hyperalgesia or normal, as compared to healthy controls.
- 10)
- Simplification to PAIC 15. Once the criteria and skills were trained, the PAIC 15 brief version was presented to the participants, to highlight the most important items of observation and the time feasibility of its use. Thereafter, students were informed that they could further increase the reliable handling of the PAIC 15 scale through a 30-minute free online training available at https://paic15.com/e-training/
3.4. Assessment of the ‘Training Capsule’
The ability to observe, detect and assess the different observation items of the PAIC scale in the clinical cases presented in the practicum was successfully achieved by all participants through the trial-and-error method with expert feedback for a good interrater reliability. The results of the pre- and post-training on observational scales (confidence, difficulty, feasibility) administered before and after the theoretical and practical sections are presented here:
3.4.1. Confidence on Observational Items (OI) to Assess Pain in People with Mild Cognitive Impairment/Dementia and Those with Moderate Impairment (Figure 1):
The reliability given to the scales to assess pain (Figure 1A) was 1 point lower in moderate/severe (min 1, median 6, max 8) than in mild cognitive impairment/dementia (min 2, median 7, max 8). The training session increased the confidence, with a median of 8 and a maximum of 10 in both clinical scenarios. The pre-post analysis also showed an overall increase in Self-confidence (Figure 1B) with 9.1% (1/11), 45.5% (5/11) and 73.7% (8/11) of participants increasing their confidence in their professional criteria, and the gain of confidence increased with the severity of the impairment/dementia to be judged. Contrarily, some participants experienced reduced confidence levels: 27.3% (3/11) showed no impairment, 18.2% (3/11) had mild impairment, and 9.1% (1/11) had moderate impairment. However, the impact on confidence was minimal relative to cognitive impairment severity.
3.4.2. Professional Preference About How to Register Pain (Figure 2):
There was not a clear preference on the way to register pain, with a present/absent dichotomic question or categoric scale (each, 27.3%, 3/11), followed by a numeric scale or open question (18.2, 2/11) and other ways (9.1%, 1/11). After the training capsule, participants indicated open question (36.4%, 3/11) and present/absent (27.3%, 3/11) as preferred, categoric scale was not mentioned (0%, 0/11) and other participants referred to other or mixed (each, 9.1%, 1 participant) depending on the clinical scenario.
3.4.3. Feasibility and Conditioning Factors for the Use of Observational Instruments (Figure 3):
The pre-test indicated that the feasibility, in terms of difficulty (Figure 3A), on the use of observational instruments was mainly constricted by the poor knowledge the participants had on them (27.3% reports, 3/11) or the difficulty to be used (very difficult, 9.1%, 1/11; difficult, 27.3% reports, 3/11), as compared to the 18.2% (2/11) that considered them easy to use or those that don’t use them (18.2%, 2/11). After the training capsule, answers were dichotomic, with about half of the participants considering they were easy to use (45.5%, 5/11) and the other half considering they were difficult to use (54.5%, 6/11).
With respect to the moment when the assessment of pain should be done (Figure 3B), there was a clear coincidence that should be while attending the old person (81.8%, x/11). This consideration changed after the training capsule, since other temporal scenarios, such as at the end (18.2%, 2/11) or after a session (18.2%, 2/11), or specific situations (9.1% each, 1/11) were also considered appropriate.
The answers about the situation of the old person (rest or moving) when doing the pain assessment (Figure 3C) showed a majoritarian consideration that ‘while resting and moving’ was the most suitable (90.9%, 10/11) and one referred to specific conditions as the one that should be considered (9.1%, 1/11). After the training session, the answers to ‘resting and moving’ diminished as some participants also considered that ‘only at rest’ could be a more suitable scenario for the assessment (rest and moving, 72.7%, 8/11; at rest 18.2%, 2/11; specific, 9.1%, 1/11).
Finally, when participants were asked about how long the pain assessment should take (Figure 3D), half of them (55.6%, 7/11) considered short intervals, with intervals ‘less than 1 minute’ being majoritarian (‘less than 1 min, 36.4%, 4/11; ‘1-2 min, 18.2%, 3/11). Oppositely, the second most frequent answer was the longest period of ‘more than 10 minutes’ (27.3%, 3/11), whereas the other two participants considered other in between intervals (‘3-5 min’, 9.1%, 1/11; ‘6-10 min’, 9.1%, 1/11). After the training capsule, about half of the participants (45.5%, 5/11) considered that an interval of ‘3-5 min’ would be the most suitable, in detriment of the ‘less than 1 min’ (18.2%, 2/11) and ‘more than 10 min’ (9.1%, 1/11) answers.
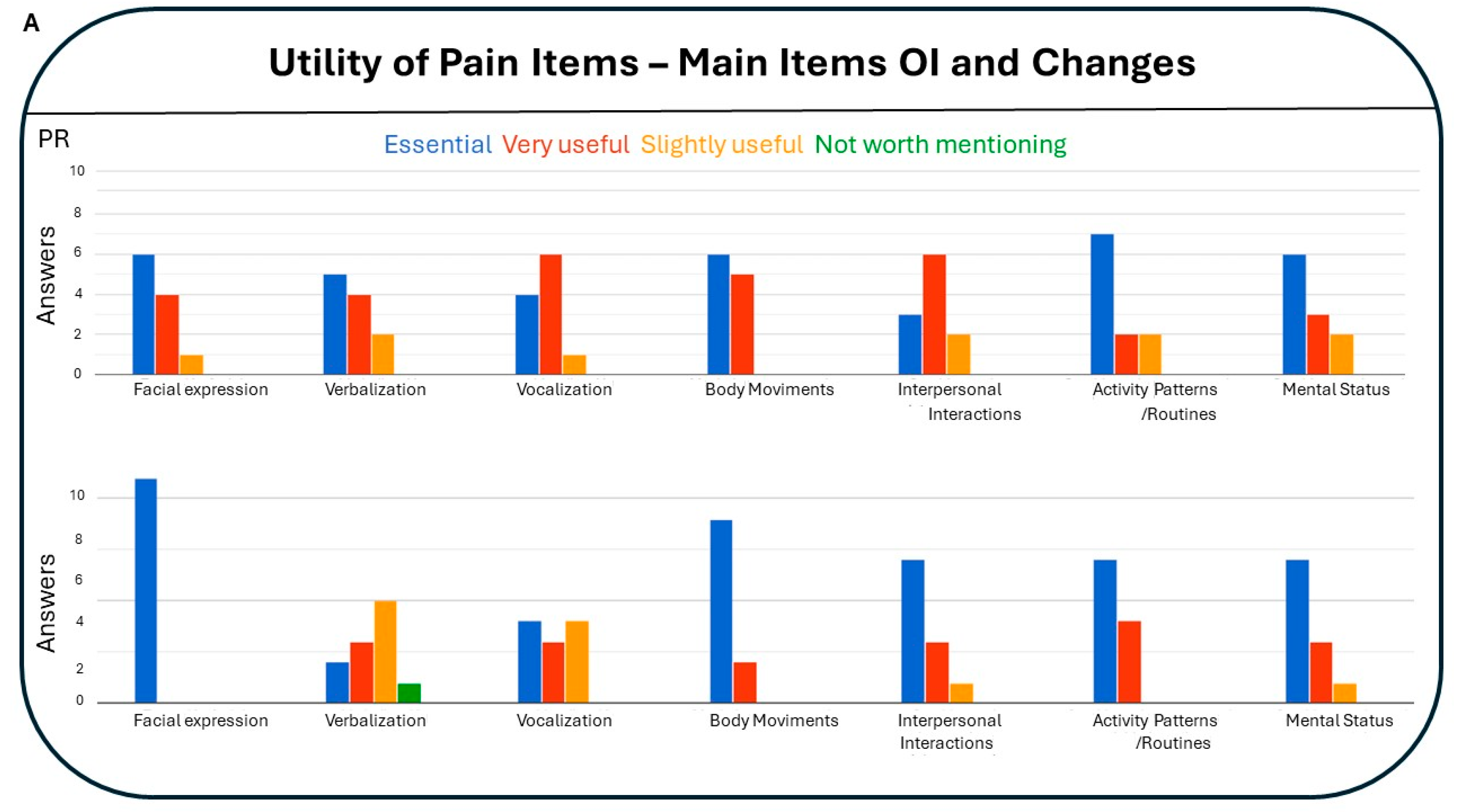
3.4.4. Utility of Pain Items: Main Items of Observational Instruments and Changes (Figure 4):
The utility of the main pain items and changes improved after the training capsule. There was an overall increase in the consideration of their relevance (total answers ‘essential’ and ‘very useful’, pre-post, ChiSquare = 2.667, 1df, one tailed p = 0.05) and in the discrimination of level of relevance (total answers ‘essential’ vs. total answers ‘very useful’, pre-post, ChiSquare = 4.161, p = 0.04) mostly due to a decrease the ‘very useful’ category in the main items of observational instruments (total answers ‘very useful’ to main items, pre-post, ChiSquare, 5.162, 1gf, p = 0.02).
Considering particular pain items, while in the pre-test ‘changes in activity patterns and routines’ was considered for more than half of participants (63.6%, 7/11) an essential item, closely followed by ‘changes in mental status’ (45.5%, 5/11) and ‘facial expression’ (45.5%, 5/11), after the intervention there was an absolute agreement on the prominence of ‘facial expression’ (100%, 11/11) (pre-post, Fisher exact test, p = 0.035). Also, a trend of overall consideration of the different levels of utility of verbalization and vocalization (reduction), body movement and changes in interpersonal interactions (increase) were recorded.
4. Discussion
On the needs and relevance - Among the reasons that explain the under-dection and insufficient treatment of pain in dementia there is not only the difficulty in detecting pain in patients with the poor or absent ability to verbally express it but also the scarcity of activities for professional training in this regard [15]. This second reason is a consistently reported regret from social and health science professionals when they refer to their dissatisfaction around the scarce training offer, especially in specific continuous training for the assessment of pain in dementia [20,32] as well as in our surveys [28,29].
In the Spanish survey [29], difficulties related to observational instruments were identified at three levels, namely, the patient, the professional knowledge and the tools themselves. Thus, pain management in severe cognitive impairment was the problem raising more concern. Other challenges described by participants in the Spanish survey included: 1) the absent or poor verbal communication and level of comprehension in such severe conditions; 2) The scarce time availability for pain assessment and monitoring confronted to low feasible and time-consuming tools; 3) The lack of specialized pain education and poor knowledge of specific tools for this population; 4) The poor standardized tools and their poor reliability mostly for severe cognitive impairment. In addition, the presence of confounding factors, a general lack of guidelines and recommendations, and low awareness among health professionals were identified in agreement with the international healthcare community [32]. Future directions to help professionals to improve pain assessment in these populations were foreseen by Spanish professionals aligned with those advised from other EU countries [28,29,32]. Pain education, specialized for older people with dementia was prioritized by one-third of participants in the survey. That is why professional training is considered one of the fundamental pillars for improving the detection and treatment of pain in the older population with dementia [33]. With this, pain management in these patients, especially in those phases in which verbal communication is very deficient or already impossible, could be improved with the use of behavioral scales with specific validity for such clinical scenarios, as would be the case with the PAIC scale. Progress would be greater if the knowledge about the existence of these tools would be accompanied by good professional training for their use [20].
When self-reports are not reliable, it is preferable to also use scales based on the evaluations of observers. The scales for specific types of pain require not only general knowledge about pain, but also specific experience, which must be provided together with the assessment instrument. That is why this training module, with the basic principles and practical training to detect, observe and assess facial expressions, vocalizations and body movements is a feasible proposal to start addressing the training needs of the professional group that cares for and attends this old population.
Finally, it is important to note that in the current WHO Long-term care for older people report [3] pain can be found in several topics for education and training for carers and also for LTC workers (see Annex 6, Tables A6.1. and A6.2., respectively), involving training in care of people living with dementia, management of pain and palliative care, including end-of life care. Among the summary descriptions providing arguments, clear statements are given as follows: “Carers encounter numerous challenges when managing pain due to complex chronic conditions common in older people and the various interventions to decrease pain. They should be able to understand the multidimensional, subjective nature of pain, which can influence a positive dyad relationship, and improve their knowledge and self-efficacy for pain management, particularly in palliative care and end-of-life situations”. Also, “Carers should be trained to recognize the sources of suffering, which involves understanding issues beyond physical symptoms. They can learn to help older people to live as actively as possible until death, paying attention to their specific needs and priorities (e.g. pain relief)”. Key points and action for the education and training for carers and that for LTC workers are also detailed. Interestingly, the document refers to pain as one of the sources of behavioral symptoms in dementia “Carers can participate in the multidisciplinary team by describing symptoms and looking for the causes of behavioural symptoms, such as pain, illness, discomfort, hunger and loneliness.”
On the training capsules - In parallel to the validation and implementation of tools, in our case, the PAIC observational scale [23,24], the need to develop units of continuous training that allow improving the professional skills of health teams is a simple and fast way, given their strong time constraints. On the other hand, these training units must be active and have specific objectives that can be measurable with respect to their results. To achieve this, planning based on the identified professional needs is required in order to improve the knowledge, skills and attitudes of professionals in the face of the advancement of knowledge [34]. These measures are approached in a flexible way, with training itineraries that break space-time barriers and, thus, make it possible for the contents to be accessible to a greater number of people. The teaching methods and tools lay the foundation for micro and meso learning, as proposed by Hug [35,36]. This approach involves using 'training capsules' to address immediate training needs in caring for older people with dementia. The training is initially conducted face-to-face but can also be adapted for digital formats, including online or blended teaching. Thus, the ‘training capsules’ constitute short, highly focused and practical training activities that aim to be immediately applicable in a clear and direct way. The ‘training capsule’ is planned based on a specific topic on which one wants to consolidate knowledge and practices, for the subsequent generation of key competencies that can be used on a day-to-day basis [35,36].
On the design - Based on the micro-learning guidelines proposed by Hug [35,36], the didactic tools were developed to carry out a theoretical-practical session in the form of a ‘training capsule’ for the assessment of ‘pain in dementia’ cases to achieve quickly and efficiently:
- 1)
- The acquisition and unification of recognition criteria of the three elements of non-verbal communication on which the PAIC scale is based: Facial expressions, body movements and vocalizations.
- 2)
- The identification of these components in clinical cases that demonstrate their validity for differential diagnosis, overcoming confounding intrinsic/extrinsic factors (i.e., facial expression and posture in old age, environmental noises, etc).
- 3)
- The applicability in the clinical environment in a situation of rest and transfer (chair-to-chair or chair-to-bed displacements, for example).
The training capsule was taught orally, supported by video presentations, which made it easily adaptable to videoconferencing and other digital formats. The key elements to support the training process were identified and structured in a format that was flexible to carry out and it was also adaptable to different health care professional profiles. In the practicum, through trial-and-error, participants learned to observe, detect and assess the different items of the PAIC scale. In addition, the pre-post evaluation enabled the professional to immediately and autonomously have tangible evidence of the level of achievement of acquired competencies in different scopes. The training capsule allowed, in a 3-hour session, to know the current use of pain assessment scales, their limitations in patients with cognitive impairment and the care needs in different geriatric settings. Training in the use of observational scales through the visualization of clinical cases in a real context and when participating in an experimental pain study, allowed acquiring skills and competencies aimed at knowing how to identify and assess the signs of pain, as well as guidelines for proper evaluation of pain in dementia.
On the participants - To assess a homogeneous sample of participants, the academic scenario of the master was used. The results of the current work refer to the answers of a specific composition of participants (in this case, professional nurses) and their professional experience with this specific group of vulnerable patients. A gender bias was also evident due to preponderance of females among participants, both patients and nursing participants. Therefore, gender-dependent sensitivity to decode emotions could also exert an influence in the results [37]. In this sense, gender has been suggested to play a critical role in how facial expressions of pain are perceived by others. However, recent work of our German team [38] showed that the observer's gender (nursing professional) appears to be less important in the decoding of facial expressions of pain than the expressor's (patient’s) gender alone. Thus, more research is necessary to determine the causes of the trend to see more suffering in female faces, which may be related to psychosocial issues like gender stereotypes.
Despite the above and other conditionings, the pre-post results of the present work showed a change and improvement in most questions, in agreement with previous pilot experiences in workshops with psychogeriatricians (IPA) and continuous education in clinical institutions with a myriad of health professionals attending people with cognitive impairment. The pre-test, reporting uncertainty and poor confidence in observational tools for pain assessment in the most demanding clinical scenarios, agrees with that reported in the Spanish survey [29]. The main explanation for the low confidence, as referred to during the debriefing session, was that competencies in non-verbal communication are not as usual or trained as others. In this respect, efforts at the academic level are currently made in our and other schools of medicine to introduce and instruct young students in such a sort of communicative abilities as a key part of the doctor-patient relationship [37,39]. In these academic contexts, it is considered that students, but also teachers and professionals in the field of health sciences, should discover the relevance of non-verbal communication in the healthcare context and to improve their observation skills and non-verbal behavior in clinical practice. In this respect, a second study on the administration and assessment of this training capsule for young medical students is in preparation and shows similar positive results.
On the pre-post assessment – A number of specific questions from the Spanish survey [29] were selected for the assessment of the training capsule. At a pragmatic level, and due to the short duration of training capsules, the pre-post assessment was done about aspects with strong application in clinical practice (such as difficulty of the tool, when/how long and the level of confidence) and that would meet the demands expressed by health professionals in the previous survey [29]. Still, the feasibility in terms of time to administer the pre-post test within the time frame of the master session was redefined thanks to previous pilot experiences.
In agreement with the Spanish survey [29] the reliability given to the scales to assess pain was lower in moderate/severe impairment/dementia than in mild clinical scenarios. Interestingly, the training session increased the confidence on these tools, and, in both cases, the median was 8 and the maximum of 10. Also, the training capsule had an impact on self-confidence since percentages increased and, most importantly, did so with the severity of the clinical scenarios. In a few cases, self-confidence decreased, because a greater knowledge increased self-demand and awareness of one's own limitations. In addition, the preferences for pain registration also changed after the training capsule with open questions receiving more followers than other categories mentioned before.
After the theoretical introduction of observational scales, and particularly the PAIC instrument, the learning about which items of facial expressions, body movements and vocalizations scientifically validated for pain assessment in these clinical populations were determinants for the achievement of the practicum. During the development and validation of the PAIC scale, this knowledge about the ‘validity of certain items’ was already reported by Spanish nurses as a useful tool helping to focus professional efforts and gain efficiency in terms of accuracy and time, resulting in an increase of their confidence on pain assessment [40]. In the practical part, the trial-and-error method facilitated efficient learning to observe, detect and assess the different items of the PAIC scale, achieving a good interrater reliability. Most importantly, there was a gain in the perception of feasibility in terms of difficulty (easy) and temporal scenarios (when, when she, how long).
Despite the small size of the student’s group - inherent of specialized masters- limited the statistical power to detect the significance of the pre-post analysis, the changes in the relevance of observational items were salient and reached statistical significance. This is interesting to note for several reasons, but basically here we can refer to its implications for a day-to-day professional practice and for educational and training purposes. First, the main effect of the training capsule was to increase the utility assigned to facial expression that reached absolute preponderance with respect to the other items. This is important since many tools rely on facial expressions [41] and facial descriptors are used by Care Home nurses to infer whether a person in dementia is in pain [42]. Nurses' total pain ratings are significantly predicted by the physically based descriptors "frowning," "narrowed eyes," and the indicators of emotional arousal "looking tense," "looking scared," which account for around 45% of the variance [41]. In their study, authors aware that development of observational pain tools and nurse training in their use should take into account the preconceptions that nurses have about how to interpret pain and their potential bias. Therefore, in the present work, the pre-test and the strong coincidence with the Spanish survey [29] were an important part of the results. In fact, it is also important to note that Spanish health professionals already expressed their predilection for this item in the Spanish survey [29] in contrast to the European [28]. There, clinical staff from Austria, Belgium, Denmark, Germany, The Netherlands, Switzerland and the United Kingdom considered facial expression to be the least useful in comparison to other items, and also found interpreting facial expressions in relation to pain more difficult. This is interesting since facial expressions in older people as considered more difficult to be decoded due to age-related structural changes [43] or due to a general trend to be less expressive [43,44]. On the other hand, and second, in the design of training abilities in other educational scenarios, where content and time restrictions may occur, it is important to include specific observational items where training has been proven to have an impact. For example, in practicums of pain assessment for general population, where a brief focus on pain assessment in dementia wants to be included but cannot last only a few minutes of the whole session. In this respect, also with the aim to reinforce their knowledge and training, master students are informed about the chance to increase the reliable handling of the PAIC15 scale through a 30-minute free online training (in English) available at https://paic15.com/e-training/. This e-training is focused on individual items of the PAIC scale, based on a few training video clips depicting various pain situations that must be rated using the PAIC scale, receiving direct expert feedback and a testing phase to achieve a good interrater (with the expert ratings) reliability.
5. Conclusions
In summary, the ‘training capsule’ allowed reaching a basic level of training on PAIC15 observational scale in a professional group of nurses from different clinical settings interested in vulnerable old populations. The capsule changed their self-confidence in assessing pain in people with cognitive impairment, especially dementia, and in observational tools to do so, improving their criteria on their use and feasibility. The session significantly enhanced the prior perception they had on the utility of facial expression items. Education and training of healthcare professionals can be a first step that contributes to improving the well-being and quality of life of the older people with cognitive impairment/dementia who have pain but have lost a good part of their ability to express it.
Author Contributions
Conceptualization, L.G-L.; Methodology, L.G.-L., M.K.; Data curation, L.G.L.; Formal analysis, L.G.-L.; Resources, M.S., A.B., Investigation, L.G.L., L.M.P.G., I.M.dO.,A.M. and M.K.; writing—original draft preparation, L.G.L.; writing—review and editing, L.G.-L, M.K.; supervision, A.B.; Project administration, L.G.-L., M.S., A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board, Ethics Committee, Comité ëtico de Investigación Clínica Hermanas Hospitalarias del Sagrado Corazón de Jesus (CEIC protocol code PR-2015-04 and date of approval April, 30, 2015).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The descriptive data of the study (assessment) can be provided by contacting the corresponding author of the study.
Acknowledgments
We thank the patients and their families, and all the master students for their participation to make it possible.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Vollset, S.E.; Ababneh, H.S.; Abate, Y.H.; Abbafati, C.; Abbasgholizadeh, R.; Abbasian, M.; Abbastabar, H.; Magied, A.H.A.A.A.; ElHafeez, S.A.; Abdelkader, A.; et al. Burden of disease scenarios for 204 countries and territories, 2022–2050: a forecasting analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2204–2256. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Aflatoxins; WHO: Geneva, Switzerland, 2018. Available online: https://www.who.int/ foodsafety/FSDigest_Aflatoxins_EN.pdf (accessed on 19 December 2021).
- World Health Organization. Long-term care for older people: package for universal health coverage. World Health Organization. Available online: https://iris.who.int/handle/10665/376585 (accessed May 22 2024).
- Cole, C.S.; Carpenter, J.S.; Chen, C.X.; Blackburn, J.; Hickman, S.E. Prevalence and Factors Associated with Pain in Nursing Home Residents: A Systematic Review of the Literature. J. Am. Med Dir. Assoc. 2022, 23, 1916–1925. [Google Scholar] [CrossRef] [PubMed]
- Viderman, D.; Tapinova, K.; Aubakirova, M.; Abdildin, Y.G. The Prevalence of Pain in Chronic Diseases: An Umbrella Review of Systematic Reviews. J. Clin. Med. 2023, 12, 7302. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Akkala, S.; Nayak, M.; Kotlo, A.; Poondla, N.; Raza, S.; Stankovich, J.; Antony, B. Impact of Pain on Activities of Daily Living in Older Adults: A Cross-Sectional Analysis of Korean Longitudinal Study of Aging (KLoSA). Geriatrics 2024, 9, 65. [Google Scholar] [CrossRef] [PubMed]
- Zwakhalen, S.M.; Koopmans, R.T.; Geels, P.J.; Berger, M.P.; Hamers, J.P. The prevalence of pain in nursing home residents with dementia measured using an observational pain scale. Eur. J. Pain 2009, 13, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Zwakhalen, S.M.; Koopmans, R.T.; Geels, P.J.; Berger, M.P.; Hamers, J.P. The prevalence of pain in nursing home residents with dementia measured using an observational pain scale. Eur. J. Pain 2009, 13, 89–93. [Google Scholar] [CrossRef]
- Mäntyselkä, P.; Hartikainen, S.; Louhivuori-Laako, K.; Sulkava, R. Effects of dementia on perceived daily pain in home-dwelling elderly people: a population-based study. Age and Ageing 2004, 33, 496–499. [Google Scholar] [CrossRef] [PubMed]
- Björk, S.; Juthberg, C.; Lindkvist, M.; Wimo, A.; Sandman, P.-O.; Winblad, B.; Edvardsson, D. Exploring the prevalence and variance of cognitive impairment, pain, neuropsychiatric symptoms and ADL dependency among persons living in nursing homes; a cross-sectional study. BMC Geriatr. 2016, 16, 154. [Google Scholar] [CrossRef]
- Helvik, A.-S.; Bergh, S.; Tevik, K. A systematic review of prevalence of pain in nursing home residents with dementia. BMC Geriatr. 2023, 23, 1–21. [Google Scholar] [CrossRef]
- Scherder EJ, Bouma A. Is decreased use of analgesics in Alzheimer disease due to a change in the affective component of pain? Alzheimer Dis Assoc Disord. 1997;11(3):171–174. [CrossRef]
- Achterberg, W.P.; Erdal, A.; Husebo, B.S.; Kunz, M.; Lautenbacher, S. Are Chronic Pain Patients with Dementia Being Undermedicated? J. Pain Res. 2021, ume 14, 431–439. [Google Scholar] [CrossRef]
- Anderson, C.M. Pain relief at the end-of-life: a clinical guide. 2003, 99, 556–9. [Google Scholar]
- Corbett, A.; Husebo, B.; Malcangio, M.; Staniland, A.; Cohen-Mansfield, J.; Aarsland, D.; Ballard, C. Assessment and treatment of pain in people with dementia. Nat. Rev. Neurol. 2012, 8, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Corbett, A.; Husebo, B.; Malcangio, M.; Staniland, A.; Cohen-Mansfield, J.; Aarsland, D.; Ballard, C. Assessment and treatment of pain in people with dementia. Nat. Rev. Neurol. 2012, 8, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Achterberg, W.; Pieper, M.J.; van Dalen-Kok, A.H.; de Waal, M.W.; Husebo, B.S.; Lautenbacher, S.; Kunz, M.; Scherder, E.J.; Corbett, A. Pain management in patients with dementia. Clin. Interv. Aging 2013, 8, 1471–82. [Google Scholar] [CrossRef] [PubMed]
- Ballard, C.; Smith, J.; Corbett, A.; Husebo, B.; Aarsland, D. The role of pain treatment in managing the behavioural and psychological symptoms of dementia (BPSD). Int. J. Palliat. Nurs. 2011, 17, 420–424. [Google Scholar] [CrossRef]
- Ballard, C.; Smith, J.; Corbett, A.; Husebo, B.; Aarsland, D. The role of pain treatment in managing the behavioural and psychological symptoms of dementia (BPSD). Int. J. Palliat. Nurs. 2011, 17, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, H.A.; Jarland, M. Are nursing home patients with dementia diagnosis at increased risk for inadequate pain treatment? Int. J. Geriatr. Psychiatry 2005, 20, 730–737. [Google Scholar] [CrossRef]
- Briesacher, B.A.; Limcangco, M.R.; Simoni-Wastila, L.; Doshi, J.A.; Levens, S.R.; Shea, D.G.; Stuart, B. The Quality of Antipsychotic Drug Prescribing in Nursing Homes. Arch. Intern. Med. 2005, 165, 1280–1285. [Google Scholar] [CrossRef]
- Briesacher, B.A.; Limcangco, M.R.; Simoni-Wastila, L.; Doshi, J.A.; Levens, S.R.; Shea, D.G.; Stuart, B. The Quality of Antipsychotic Drug Prescribing in Nursing Homes. Arch. Intern. Med. 2005, 165, 1280–1285. [Google Scholar] [CrossRef]
- Lipori, J.P.; Tu, E.; Shireman, T.I.; Gerlach, L.; Coe, A.B.; Ryskina, K.L. Factors Associated with Potentially Harmful Medication Prescribing in Nursing Homes: A Scoping Review. J. Am. Med Dir. Assoc. 2022, 23, 1589–e1. [Google Scholar] [CrossRef]
- Corbett, A.; Husebo, B.S.; Achterberg, W.P.; Aarsland, D.; Erdal, A.; Flo, E. The importance of pain management in older people with dementia. Br. Med Bull. 2014, 111, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Corbett, A.; Achterberg, W.; Husebo, B.; Lobbezoo, F.; de Vet, H.; Kunz, M.; Strand, L.; Constantinou, M.; Tudose, C.; Kappesser, J.; et al. An international road map to improve pain assessment in people with impaired cognition: the development of the Pain Assessment in Impaired Cognition (PAIC) meta-tool. BMC Neurol. 2014, 14, 229. [Google Scholar] [CrossRef] [PubMed]
- Kunz, M.; de Waal, M.W.M.; Achterberg, W.P.; Gimenez-Llort, L.; Lobbezoo, F.; Sampson, E.L.; van Dalen-Kok, A.H.; Defrin, R.; Invitto, S.; Konstantinovic, L.; et al. The Pain Assessment in Impaired Cognition scale (PAIC15): A multidisciplinary and international approach to develop and test a meta-tool for pain assessment in impaired cognition, especially dementia. Eur. J. Pain 2019, 24, 192–208. [Google Scholar] [CrossRef] [PubMed]
- de Waal, M.W.M.; van Dalen-Kok, A.H.; de Vet, H.C.W.; Gimenez-Llort, L.; Konstantinovic, L.; de Tommaso, M.; Fischer, T.; Lukas, A.; Kunz, M.; Lautenbacher, S.; et al. Observational pain assessment in older persons with dementia in four countries: Observer agreement of items and factor structure of the Pain Assessment in Impaired Cognition. Eur. J. Pain 2019, 24, 279–296. [Google Scholar] [CrossRef] [PubMed]
- Kunz, M.; Crutzen-Braaksma, P.; Giménez-Llort, L.; Invitto, S.; Villani, G.; Detommaso, M.; Petrini, L.; Vase, L.; Matthiesen, S.T.; Gottrup, H.; et al. Observing Pain in Individuals with Cognitive Impairment: A Pilot Comparison Attempt across Countries and across Different Types of Cognitive Impairment. Brain Sci. 2021, 11, 1455. [Google Scholar] [CrossRef]
- Baeta-Corral, R.; Defrin, R.; Pick, C.G.; Giménez-Llort, L. Tail-flick test response in 3×Tg-AD mice at early and advanced stages of disease. Neurosci. Lett. 2015, 600, 158–163. [Google Scholar] [CrossRef]
- Cañete, T.; Giménez-Llort, L. Preserved Thermal Pain in 3xTg-AD Mice With Increased Sensory-Discriminative Pain Sensitivity in Females but Affective-Emotional Dimension in Males as Early Sex-Specific AD-Phenotype Biomarkers. Front. Aging Neurosci. 2021, 13. [Google Scholar] [CrossRef]
- Defrin, R.; Amanzio, M.; de Tommaso, M.; Dimova, V.; Filipovic, S.; Finn, D.P.; Gimenez-Llort, L.; Invitto, S.; Jensen-Dahm, C.; Lautenbacher, S.; et al. Experimental pain processing in individuals with cognitive impairment. Pain 2015, 156, 1396–1408. [Google Scholar] [CrossRef] [PubMed]
- Zwakhalen, S.; Docking, R.E.; Gnass, I.; Sirsch, E.; Stewart, C.; Allcock, N.; Schofield, P. Pain in older adults with dementia. Der Schmerz 2018, 32, 364–373. [Google Scholar] [CrossRef] [PubMed]
- Giménez-Llort, L.; Bernal, M.L.; Docking, R.; Muntsant-Soria, A.; Torres-Lista, V.; Bulbena, A.; Schofield, P.A. Pain in Older Adults With Dementia: A Survey in Spain. Front. Neurol. 2020, 11. [Google Scholar] [CrossRef]
- Global report on ageism. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis, 2016–2021: Towards Ending Viral Hepatitis. 2016. Available online: http://apps. who.int/iris/bitstream/10665/246177/1/WHO-HIV-2016.06-eng.pdf (accessed on).
- Liao, Y.-J.; Jao, Y.-L.; Berish, D.; Hin, A.S.; Wangi, K.; Kitko, L.; Mogle, J.; Boltz, M. A Systematic Review of Barriers and Facilitators of Pain Management in Persons with Dementia. J. Pain 2023, 24, 730–741. [Google Scholar] [CrossRef] [PubMed]
- Bravell, M.E. Pain-related palliative care challenges in people with advanced dementia call for education and practice development in all care settings. Évid. Based Nurs. 2017, 20, 118–119. [Google Scholar] [CrossRef] [PubMed]
- Domingo-Coscollola, M.; Marquès-Graells, P. Classroom 2.0 Experiences and Building on the Use of ICT in Teaching. Comunicar 2011, 19, 169–175. [Google Scholar] [CrossRef]
- Hug, T. Hug, T. (2005). Micro learning and narration: Exploring possibilities of utilization of narrations and storytelling for the designing of “micro units” and didactical micro-learning arrangements. MiT4: The Work of Stories, Proceedings of the fourth Media in Transition conference, May 6-8, 2005, MIT, Cambridge (MA), USA.
- Hug, T. (2012). Microlearning. In: Seel, N.M. (eds) Encyclopedia of the Sciences of Learning. Springer, Boston, MA. [CrossRef]
- Molinuevo, B. (2017) Molinuevo, B. La comunicación no verbal en la relación médico-paciente [The non-verbal communication in the doctor-patient relationship]. Editorial UOC, ISBN: 9788491169734.
- Göller, P.J.; Reicherts, P.; Lautenbacher, S.; Kunz, M. How gender affects the decoding of facial expressions of pain. Scand. J. Pain 2022, 23, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Weiss, T.; Swede, M.J. Transforming Preprofessional Health Education Through Relationship-Centered Care and Narrative Medicine. Teach. Learn. Med. 2016, 31, 222–233. [Google Scholar] [CrossRef] [PubMed]
- Moriana de la Olla, I. , Pajuelo González, L.M. & Giménez-Llort. Mejora de las competencias profesionales en la enfermería geriátrica en la detección y evaluación de dolor en pacientes con demencia [Improvement of professional skills in geriatric nursing in the detection and evaluation of pain in patients with dementia ] In: Conocimientos, investigación y prácticas en el campo de la salud [Knowledge, research and practices in the field of health]. Editor 1, Pérez-Fuentes, M.C., Editor 2, Gázquez, J.J., Editor 3, Molero, M.M., Editor 4, Simón, M.M., Editor 5, Martos, A. Editor 6, Barragán, A.B. Volumen II. Publisher: ASUNIVEP, Almería, Spain, 2017; Volume 2, pp. 933-938.
- Lautenbacher, S.; Sampson, E.L.; Pähl, S.; Kunz, M. Which Facial Descriptors Do Care Home Nurses Use to Infer Whether a Person with Dementia Is in Pain? Pain Med. 2016, 18, 2105–2115. [Google Scholar] [CrossRef] [PubMed]
- Lautenbacher, S.; Walz, A.L.; Kunz, M. Using observational facial descriptors to infer pain in persons with and without dementia. BMC Geriatr. 2018, 18, 88. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J.; Carstensen, L.L.; Pasupathi, M.; Tsai, J.; Skorpen, C.G.; Hsu, A.Y.C. Emotion and aging: Experience, expression, and control. Psychol. Aging 1997, 12, 590–599. [Google Scholar] [CrossRef]
- Malatesta, C.Z.; Izard, C.E.; Culver, C.; Nicolich, M. Emotion communication skills in young, middle-aged, and older women. Psychol. Aging 1987, 2, 193–203. [Google Scholar] [CrossRef]
Figure 1.
Pre-post analysis of educational intervention on confidence to assess pain: (A) Pre and post levels of the confidence on observational instruments (OI) for pain assessment in people with mild cognitive impairment/dementia (left) and moderate/severe cognitive impairment/dementia (right); (B) Pre-post analysis on self-confidence to assess pain in people without cognitive impairment (top), mild cognitive impairment/dementia (middle) or moderate/severe cognitive impairment/dementia (bottom).
Figure 1.
Pre-post analysis of educational intervention on confidence to assess pain: (A) Pre and post levels of the confidence on observational instruments (OI) for pain assessment in people with mild cognitive impairment/dementia (left) and moderate/severe cognitive impairment/dementia (right); (B) Pre-post analysis on self-confidence to assess pain in people without cognitive impairment (top), mild cognitive impairment/dementia (middle) or moderate/severe cognitive impairment/dementia (bottom).
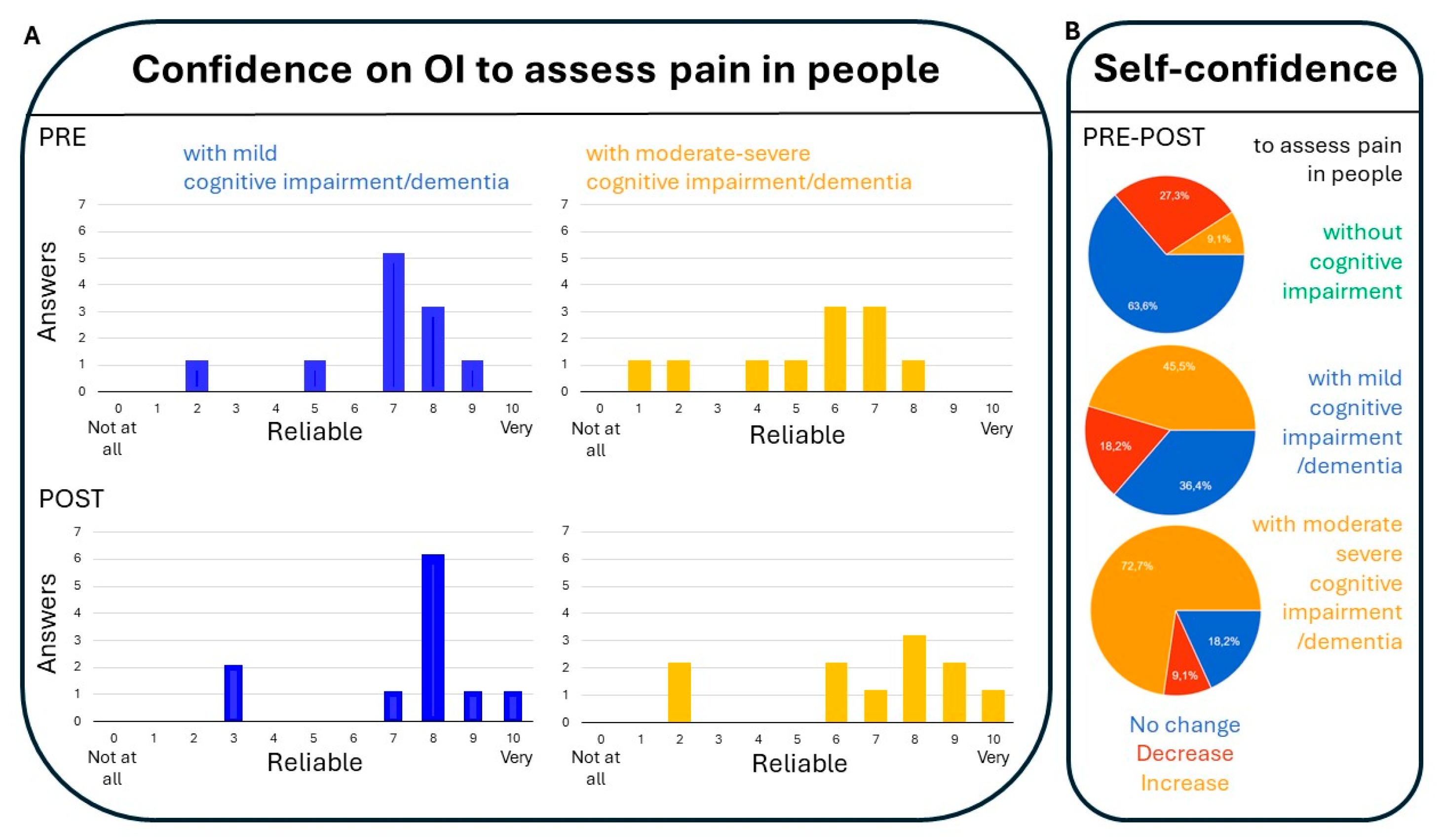
Figure 2.
Pre-post analysis of educational intervention on the professional preference about how to register pain. Participants were requested to indicate their preference for present/absent, numeric scale, categoric scale, open question, other, mixed methods to register pain in patients with cognitive impairment, especially dementia.
Figure 2.
Pre-post analysis of educational intervention on the professional preference about how to register pain. Participants were requested to indicate their preference for present/absent, numeric scale, categoric scale, open question, other, mixed methods to register pain in patients with cognitive impairment, especially dementia.
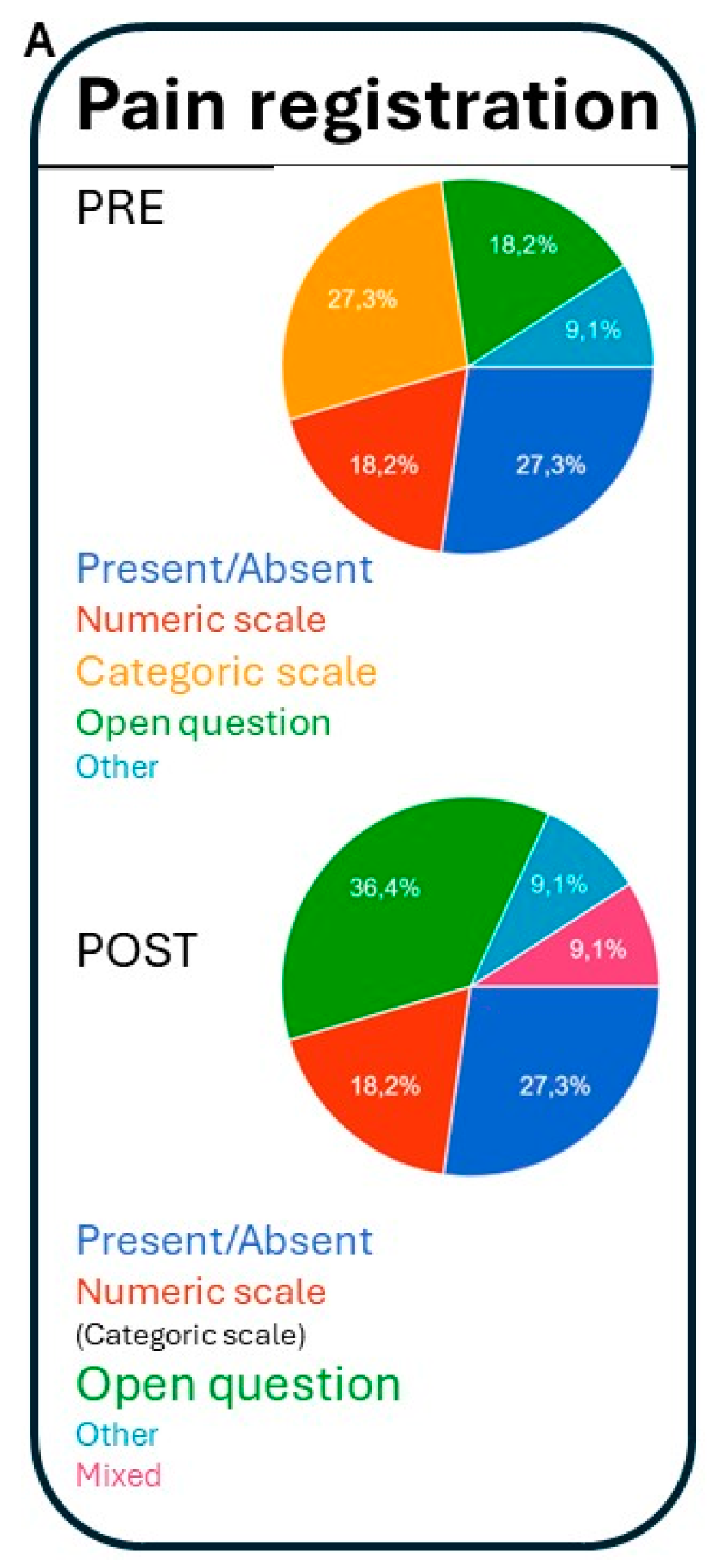
Figure 3.
Pre-post analysis of educational intervention on the use of observational instruments (OI): Feasibility in terms of difficulty (A), and the different conditioning factors on the use of observational instruments for pain assessment in people with dementia (B, When; C, the activity of the patient; D, time needed for the assessment), before (PRE) and after (POST) the training capsule.
Figure 3.
Pre-post analysis of educational intervention on the use of observational instruments (OI): Feasibility in terms of difficulty (A), and the different conditioning factors on the use of observational instruments for pain assessment in people with dementia (B, When; C, the activity of the patient; D, time needed for the assessment), before (PRE) and after (POST) the training capsule.
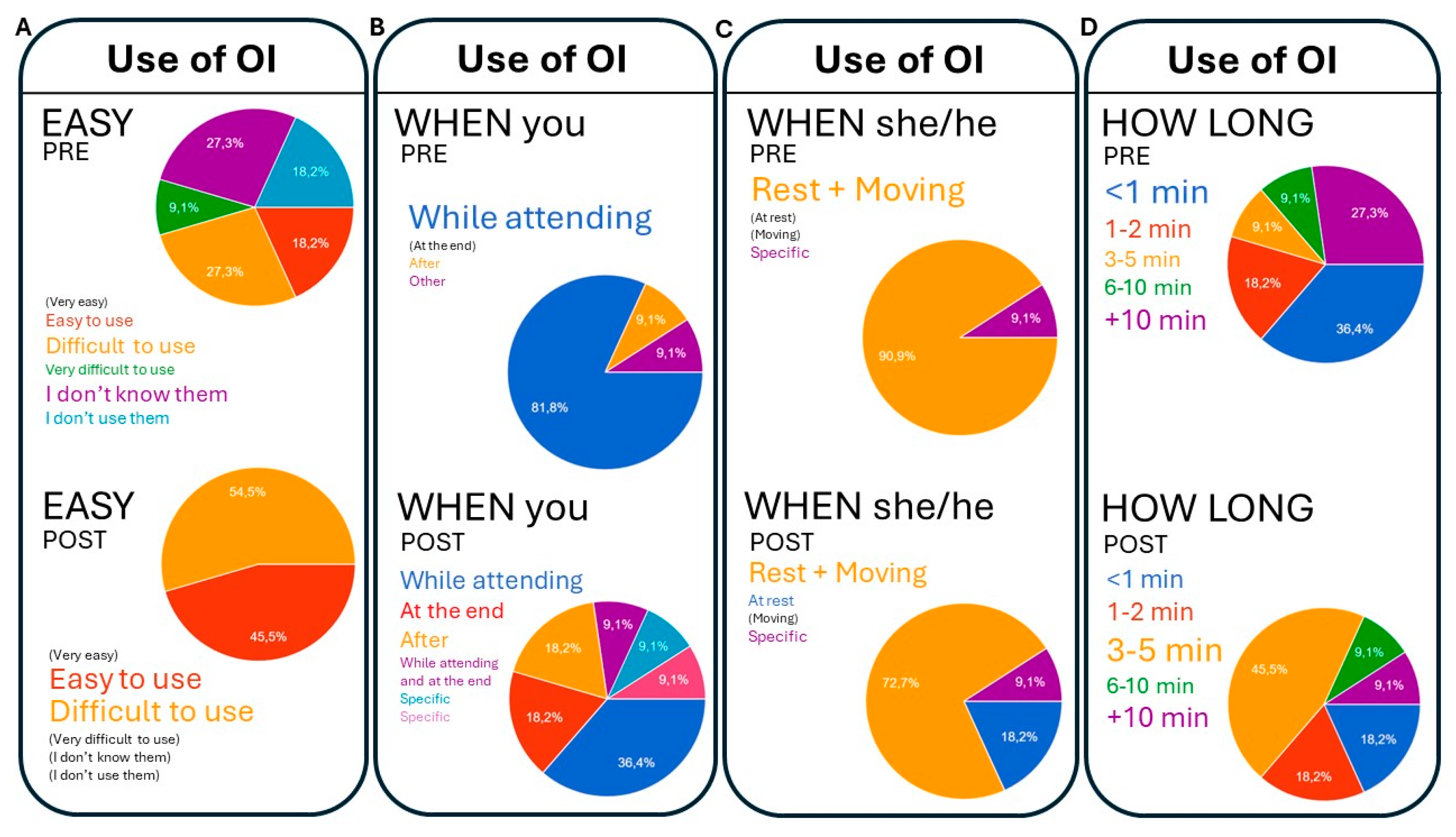
Figure 4.
Pre-post analysis of educational intervention on the utility of pain items: Utility of main pain items of observational scales for pain assessment in people with dementia (A, main items: facial expression, verbalization, vocalization, body movements; Changes in interpersonal interactions, activity patterns/routine, mental status)
Figure 4.
Pre-post analysis of educational intervention on the utility of pain items: Utility of main pain items of observational scales for pain assessment in people with dementia (A, main items: facial expression, verbalization, vocalization, body movements; Changes in interpersonal interactions, activity patterns/routine, mental status)
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



