
Submitted:
17 July 2024
Posted:
17 July 2024
You are already at the latest version
Abstract
An efficacious treatment of H. pylori infection is cornerstone for the global control of the diseases caused by this bacterium. Continuous epidemiologic surveillance of susceptibility of H. pylori to the antibiotics recommended for its eradication is highly recommended. This study aimed to determine the antimicrobial susceptibility pattern of 651 isolates from five different collections isolated between 1996 to 2008 in México City. The susceptibility profile of H. pylori isolates was determined by the E-test strips for each antibiotic (amoxicillin, clarithromycin, metronidazole, and tetracycline). Antimicrobial susceptibility testing showed a very high proportion of H pylori strains susceptible to amoxicillin, clarithromycin, and tetracycline (94.5%, 95%, and 99.5 %, respectively). In contrast, a high proportion (95%) of isolates was resistant to metronidazole. Notably, the proportion of susceptible/resistant strains to the 4 antibiotics over 5 consecutive time periods remained stable over time. Despite a wide use of amoxicillin and clarithromycin in the general population, the H pylori high susceptibility to these 2 antibiotics has been preserved during more than a decade. The high prevalence of resistance to metronidazole in H. pylori strains in our population compromises its use in the empirical treatment of H. pylori infection.
Keywords:
Helicobacter pylori
; E-test
; Resistance to antibiotics
; Isolates collections
1. Introduction
One of the most prevalent infections worldwide, with approximately 50% of the population, is caused by the Gram-negative bacillus H. pylori, which has been associated with pathologies such as non-ulcer dyspepsia, chronic gastritis, peptic ulcer, duodenal ulcer, malt lymphoma, and gastric adenocarcinoma [1]. For this reason, worldwide consensus on the treatment and antimicrobials to be used are the most important for the eradication of the infection caused by H. pylori. Of these consensuses, Maastricht’s is the one that compiles the experiences of world research groups, but although Maastricht sets the strategy to be followed [2,3,4,5] regional consensuses adapt them according to the needs and behavior of microorganisms to the antimicrobials accepted worldwide for H. pylori eradication [6,7,8,9,10]. Treatment and eradication are indicated as signs and symptoms of infection and if the patient belongs to the high-risk group as having first-degree relatives with a history of gastric cancer, habits like excessive smoking, presence of the mutation CDH-1 or live-in high-risk area of gastric cancer, likewise, patients with Pangastritis, dominant gastritis gastric body atrophy and intestinal metaplasia [5].
These consensuses determined the use of globally accepted first-line therapy, which includes several antimicrobials such as clarithromycin, amoxicillin, metronidazole, and tetracycline [2,3,4,5]. Due to the difficulty of obtaining a gastric biopsy and its processing and culture to obtain the H. pylori strain, it is common to perform antimicrobial susceptibility tests (Epsilometer Test, or E-Test) and thus obtain the resistance pattern to define the treatment to be followed. However, empirical treatment predominates, which has led to its failure and a significant increase in resistance to these antimicrobials [2,11]. Therefore, the aim of this study was to analyses the trend over time of the patterns of susceptibility to antimicrobials used in the first line therapy for the eradication of H. pylori in 651 isolates obtained during a 12-year period in Mexico City.
2. Results
2.1. H. pylori Isolate Collections
Table 1 describes the demographic data of the five collections analysed. Collection I is made up of 83 isolates, obtained from 50 men and 33 women whose average age was 57.4 years with an interval between 30 and 72 years and in a period of two years (from 1996 to 1998). From collection II, 24 isolates were obtained from 3 men and 21 women with an average age of 42.7 years with an interval from 19 to 71, and a period from 1999 to 2000. Collection III, which was obtained from July 2000 to December 2001, had 338 isolates corresponding to 135 men and 203 women whose average age was 48.1 years in a range of 15 to 87 years. Collection IV had 24 isolates, 7 from men and 17 from women whose average age was 55.5 years and an interval of 29 to 79 years, in a period from 2003 to 2005. Finally, Collection V was made up of 182 isolates, 54 of which were acquired from men and the remaining 128 were from women, whose average age was 46.9, with an interval of 15 to 87 years, in a period from May 2007 to January 2008.
2.2. Antimicrobial Breakpoints
The breakpoints that were considered for the determination of the resistance by the E-test, in the studied collections, were taken mainly from the studies published by Mexican groups. This is based on the differences in treatments and use of antimicrobials and resistances reported worldwide since each region has its characteristics and different antimicrobial resistances. Thus, amoxicillin remained resistant to a concentration greater than 2 µg/mL, clarithromycin > 2 µg/mL, metronidazole > 8 µg/mL, and tetracycline > 4 µg/mL. In Figure 1, we present the strains of the various pathologies and their growth in the various antimicrobial concentrations that were used. The decision was made to take a dilution before resistance as an intermediate zone, in such a way that any dilution before this would be considered susceptible.
2.3. Determination of The Antimicrobial Susceptibility Profile
All 651 strains were studied for the antimicrobial agents, except 83 strains that were not tested for tetracycline; these were part of the first collection, in the remaining four collections tetracycline was included. The results obtained showed that 94.47% (615/651) of the H. pylori strains were susceptible to amoxicillin, 2.92% (19/651) showed intermediate susceptibility, and 2.61% (17/651) were resistant. For clarithromycin 95.08% (619/651) were susceptible, 1.08% (7/651) with intermediate susceptibility, and 3.84% (25/651) were resistant. In the case of metronidazole, we observed that 15.98% (104/651) were susceptible, 1.38% (9/651) with intermediate susceptibility, and 82.64% (538/651) were resistant. Finally, for tetracycline, 99.47% (565/568) were susceptible, and 0.53% (3/568) were resistant, Figure 2. Being untested, for the latter 12.75% (83/651) of isolates (Collection I).
2.4. Secular Trend of Drug Resistance
Table 2 and Figure 3 show the proportion of H. pylori isolates susceptible to the 4 studied antimicrobials according to 5 different consecutive time periods of isolation. Antimicrobial susceptibility testing showed a very high proportion of H. pylori strains susceptible to amoxicillin, clarithromycin, and tetracycline (94.5%, 95% and 99.5%, respectively). In contrast, a high proportion (84%) of isolates was resistant to metronidazole. Notably, the proportion of susceptible/resistant strains to the 4 antibiotics over the 5 consecutive time periods remained stable over time. Estimated slopes of the association of antibiotic susceptibility prevalence and period was estimated through a simple linear regression analysis; these slopes were of low magnitude (less than one percentual point) and statistically not different form zero.
On the other hand, when we analyze the antimicrobial resistant profiles of the H. pylori isolates (Table 2), we observe that for the collection I, 83 isolates were performed only for amoxicillin, clarithromycin and metronidazole. Antimicrobial resistant for metronidazole was 72.3% (60/83 isolates). We found one isolate resistant to amoxicillin and clarithromycin (1.2%), and a second H. pylori isolate was found clarithromycin and metronidazole resistant (1.2%). Amoxicillin, clarithromycin and metronidazole resistant were observed in 8.43% (7/83 isolates). In this collection, high clarithromycin resistance (≥ 256 µg/mL) was found in two isolates. Collection II, with 24 isolates tested, we found 22 isolates metronidazole resistant (91.67%), and 87.5% (21/24) strains showed high resistance to metronidazole (≥ 256 mg/mL). We only found three isolates clarithromycin and metronidazole resistant (12.5%). For collection III, with 338 isolates tested, we found that metronidazole resistant was 81.36% (275/338). Amoxicillin and metronidazole resistant we found in four isolates (1.18%); and 2 clarithromycin-metronidazole resistant (0.59%). All H. pylori isolate from collection III were tetracycline susceptible. In the case of collection IV, with 24 isolates tested, 19 out of 21 isolates showed high metronidazole resistance (≥ 256 µg/mL). All isolates tested were amoxicillin and tetracycline susceptible. In relation to collection V, with 182 H. pylori isolates tested, 2.19% (4/182) isolates were amoxicillin and metronidazole resistant, and 2.75% were clarithromycin-metronidazole resistant (2.75%). Six H. pylori isolate showed a profile clarithromycin intermediate and metronidazole resistant; and 10 isolates were amoxicillin intermediate and metronidazole resistant (data not shown).
When we analyze the behavior of antibiotics of each one of the collections by the geometric mean of their MIC, we observe similar behavior for amoxicillin, clarithromycin, and tetracycline, which trends to maintain very low resistance in collections II to V. In the case of metronidazole is upward in the different collections, except in collection IV, in which there is a decrease in resistance (Figure 4).
2.5. Dual Resistance to Clarithromycin-Metronidazole
Table 2 shows the percentage of H. pylori isolates resistant to clarithromycin-metronidazole. We found only 2% (13/651) of the isolates with this resistance profile.
2.6. Analysis of Resistance By Gastric Pathology
In Table 3 the percentage of H. pylori isolates resistant to one, two, three, and four antibiotics, according to the gastric disease, is shown.
3. Discussion
In the present study, we shown the results of five isolate collections, covering a 12-year follow-up period of H. pylori susceptibility in Mexico City, in which the E-Test was used as the method to determine the antimicrobial susceptibility of H. pylori, according to Li et al, and Mégraud and Lehours, the susceptibility agreement between E-test and agar dilution method (“gold standard”) for amoxicillin, clarithromycin and tetracycline is excellent, but not for metronidazole where it has been shown that the resistance rate is higher than that of agar dilution method [12,13]. In this study, we did not find a significant increase in metronidazole resistance, although it was sustained over the 12-year follow-up. Metronidazole is an antibiotic widely used for parasitic infections of the gastrointestinal tract and in the treatment of female genital tract infections. Quite the opposite is for amoxicillin, clarithromycin, and tetracycline whose susceptibility remain above 90%. Therefore, the use of these three antimicrobials is still used as the first choice for the treatment of infection by H. pylori, but it is not for metronidazole. Due to the lack of clinical MIC breakpoints for determining antibiotic resistance for H. pylori [13]. We prefer adopted those described by CLSI [14], López-Vidal, et al. [15], Torres et al. [16], Garza-González et al. [17], Chihu et al. [18], to define resistance to clarithromycin, amoxicillin, metronidazole, and tetracycline, probably due to this the resistance profile during the five periods in our study remains stable. However, it is possible that MIC breakpoints will change over time as more data become available in our population. On the other hand, according to Boyanova et al., the absence of an increase in antibiotic resistance is often associated with a decrease in the national antibiotic consumption, compliance with guidelines for infection treatment, and strict application of antibiotic [19]. However, in Mexico, the guidelines to which the sale and dispensing of antibiotics is subject came into force in August 2010 (Diario Oficial de la Federación; May 7, 2010. Available in: http://www.dof.gob.mx/nota_detalle.php?codigo=5144336&fecha=27/05/2010&print=true), so in our study we do not know why the use of amoxicillin, clarithromycin and tetracycline did not have an impact on the increase in antimicrobial resistance; but we can deliberate that is due to the breakpoints we used in the study.
We also corroborated the reports by Garza et al. regarding the geographical behavior of H. pylori to the susceptibility of amoxicillin and tetracycline antibiotics, showing greater resistance of metronidazole in the CDMX (center of the country) that in the northeastern (Nuevo León) [17]. This can be in part explained based on different schedule treatment used or the consumption of antibiotics.
In general, the antimicrobials used as first line such as amoxicillin, clarithromycin, and tetracycline are still used. Thus, treatment with metronidazole, clarithromycin, amoxicillin, and sometimes tetracycline is still valid to prescribe. This can be explained the are no changes observed on resistance to these antimicrobials, which in some countries reached alarming levels of resistant. Thus, the amplitude of antimicrobial pattern is very wide in Latin America, the resistance to clarithromycin goes from 0 to 60%, metronidazole from 12.5 to 95%, amoxicillin from 0 to 39%, and tetracycline from 0 to 86% [20]. In Mexico, there are several published studies on the susceptibility of H. pylori to first-line antimicrobials, this previous studies showed a clear difference in metronidazole resistance among isolates from the north and the center Mexico as previously described that are strong association with geographic differences may be explained for increased use of this antibiotic prescription [15,16,17,18]. However, recently in the Masstricht VI/Florence consensus report it is suggested that “The absence of significant amoxicillin resistance among H. pylori strains after decades of treatment indicates the inability of the pathogen to adapt to penicillin exposure,……. compared to increasing rates of resistance after previous unsuccessful H. pylori eradication therapies with quinolones, macrolides, and metronidazole in different cohorts” [21].
Although resistance in the antimicrobial first-line treatment is maintained does not correlates with therapeutic success. Therefore, the need for prescription of metronidazole, or levofloxacin used in rescue treatments, only impacts in decrease in the eradication rate of approximately 50%, 25%, and between 20 to 40%, respectively. Hence, it is recommended, especially if there have already been two treatment failures, that an endoscopy be performed to be able to isolate the microorganism and be able to perform an antibiogram or perform molecular determinations to be able to demonstrate antimicrobial resistance [22,23,24,25]. Fortunately, it has been found that resistance to amoxicillin, tetracycline, and rifampicin is below 5% and has not increased in this study among other studies [23].
Although in the past has been described geographic differences of that clarithromycin in this study, we did not find such differences of resistance. In the case of metronidazole, the high rate of resistance can be explained by the time intervals between the preparation of the test medium and the performance of the susceptibility test, which determines the redox potential, an important parameter for the reduction of metronidazole [12,13]. Therefore, high in vitro resistance should not always be used as a predictor of treatment failure, so if the dose is increased considering side effects, or it is changed to another nitroimidazole such as tinidazole, it can continue being used. In case of resilience of H. pylori infection is strong recommendation that clarithromycin and levofloxacin not be used once more [22,23,24,25].
Regarding dual resistance to clarithromycin-metronidazole, we did not find significant dual resistance (2%), the recommendation by Dehesa et al. in 2002 for patients with peptic ulcer and non-ulcer dyspepsia, where they observed resistance to metronidazole of 68.2% and clarithromycin of 24.3%, while the dual resistance (clarithromycin-metronidazole) was 16.8% is not in this study plausible. Due to this, we recommend prior knowledge of susceptibility patterns before using the recommended treatments to eradicate H. pylori [26]. Besides, Ayala et al. in 2011, found that resistant to metronidazole was 19%, while for clarithromycin it was 5.5%. In the case of dual resistant, they reported 3.3% for isolates from the corpus and 4.4% for those from the antrum. Suggesting to determine the susceptibility patterns of the different gastric regions can occurred [27]. Camargo et al. in 2014 conducted a meta-analysis of results compiled from Latin American publications on antimicrobial resistance patterns of H. pylori, finding that for clarithromycin the average resistance was 12%, while for metronidazole it was 53%, the dual resistance found was 8%. In the case of Mexico specifically, this resistance was 13%. In this meta-analysis, they concluded that the pattern of resistance varies between the different countries, and recommended be careful with clarithromycin is used as empirical treatment [20], the use of clarithromycin is not recommended when resistance is greater than 15% [22]. In our collection II we observed this condition, which found resistance to clarithromycin of 12.5% (3/24 isolates), where clarithromycin should discard its use. Among these isolates, it is one that was sequenced and showed the presence of regions that match that multidrug resistance [28].
In contrast of our data, Camorlinga et al. in 2019, found a significant increase in the levels of resistance to clarithromycin and levofloxacin in isolates over a period of 20 years, which leads us to a scenario where their use is not recommended for the treatment of H. pylori [29]. Whenever standard triple therapy fails, the Maastricht Consensus VI guidelines [21] recommend the use of levofloxacin as rescue therapy. However, in Mexico, resistance rates of 9 to 58% have been reported over a period of 20 years, this resistant can be explained as due to its use for the treatment of urinary tract infections and other types of infections. They also showed that resistance metronidazole and levofloxacin was 32%, that increased the suggested limit of 10% [29]. Therefore, for this study clarithromycin has no plausible consideration for inclusion in the treatment of H. pylori infection. Contreras-Omaña et al. 2021, found, when analyzing 51 publications from the previous 10 years, resistance to metronidazole from 50 to 80%, to clarithromycin from 20 to 40%, and levofloxacin from 30 to 35% [30]. Based on the above, both clarithromycin and fluoroquinolones cannot be used empirically, since the dose used cannot be increased. In contrast to metronidazole since the increase in its dosage resolves the resistance problem and can combined with bismuth-based quadruple therapy [25].
Recently, with the increasing resistance of H. pylori to antibiotics and their adverse effects, the use of probiotics in conjunction with H. pylori eradication therapy has been proposed [27,31,32,33,34], rather than through direct effects on H. pylori [21,22], with substantial success in eradicating the bacteria.
4. Materials and Methods
4.1. H. pylori Strains
The 651 strains of the present study were obtained from five different collections isolated between 1996 to 2008 in México City. The strains were isolated from patients that presented different pathologies associated with the infection H. pylori, such as acid peptic disease (APD), chronic gastritis (CG), non-ulcerous dyspepsia (NUD), bleeding peptic ulcer (BPU), gastric cancer (GC), and peptic ulcer (PU). The strains were preserved in aged Brucella broth added with 20% glycerol and 20% Fetal Bovine Serum, at -70˚C.
4.2. Susceptibility Test for H. pylori
The strains were grown-up for 3 days on Casman agar medium supplemented with 10% defibrinated horse blood in a microaerophilic environment at 37˚C and inoculated again and incubated for 72 hours to guarantee the presence of 90% of bacillary forms. According to the guidelines of the Clinical and Laboratory Standard Institute (CLSI) [14], we used Mueller Hinton medium, but in this case, supplemented with 5% horse blood. The inoculum size was 3.0 McFarland turbidity standard (9.0x108 UFC/mL), and quality control strain H. pylori ATCC 43504 was used. The inocula were adjusted and dispensed onto the media. The Epsilometer test (E-test) strips contain 15 double dilutions of each antibiotic [amoxicillin (AMX), clarithromycin (CLR), metronidazole (MTZ), and tetracycline (TE)], and all concentrations range from 0.016 to 256 µg/mL (Biomerieux) were applied, and plates were incubated at 37˚C in the microaerophilic environment during 72 h. The results were obtained by reading the MICs. Antimicrobial resistance was defined by cutoff points consistent with work already published by various groups, such as CLSI [14], López-Vidal, et al. [15], Torres et al. [16], Garza-González et al. [17], Chihu et al. [18]. The breakpoints for resistance to clarithromycin ≥ 2 µg/mL, amoxicillin ≥ 2 µg/mL, metronidazole ≥ 8 µg/mL, and tetracycline ≥ 4 µg/mL.
4.3. Statistical Methods
The comparison of the proportion of H pylori isolates susceptible to the studied antimicrobials among the 5 consecutive time periods was statistically tested by a simple linear regression modelling. A p value less than 5% was considered as statistically significant.
5. Conclusions
In conclusion, despite a wide use of amoxicillin and clarithromycin in the general population, the H pylori presented high susceptibility to these 2 antibiotics has been preserved for more than a decade. The 0.5% resistance to tetracycline in our isolates suggests that the use of this antibiotics in quadruple therapy is an appropriate option. H. pylori isolate resistant to three or four antibiotics was found in less than 5% of infected persons. We found high resistance to metronidazole in H. pylori strains in our population, which can be explained when we increased doses its successful use for the rescue treatment of H. pylori infection. Even our contrast data in antimicrobial resistant in México it is mandatory keep going on in continuous surveillance is necessary to prevent treatment failures and meanwhile, continues the experience by introduction of probiotics for the development of new treatment protocols to minimize further spread of resistant H. pylori isolates.
Author Contributions
Conceptualization, CM-M, GA-V, GC-R, YL-V; methodology, GA-V, RIA-F, CM-M; analyzed the data, RIA-F, JJC; writing-original draft preparation, RIA-F, GC-R; writing-review and editing, JJC, YL-V, GC-R. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Dirección General de Asuntos del Personal Académico-Programa de Apoyo a Proyectos de Investigación e Innovación Tecnológica (DGAPA-PAPIIT) IN217823 and operating budget of the Facultad de Medicina, Universidad Nacional Autónoma de México. No funding bodies played any role in the study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Malfertheiner, P.; Camargo, M.C.; El-Omar, E.; Liou, J.M.; Peek, R.; Schulz, C.; Smith, S.I.; Suerbaum, S. Helicobacter pylori infection. Nat. Rev. Dis. Primers 2023, 9, 19. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Mégraud, F.; OʼMorain, C.; Bell, D.; Porro, B.G.; Deltenre, M.; Forman, D.; Gasbarrini, G.; Jaup, B.; Misiewicz, J.J.; Pajares, J.; Quina, M.; Rauws, E. Current European concepts in the management of Helicobacter pylori infection - the Maastricht Consensus Report. Eur. J. Gastroenterol. Hepatol. 1997, 9, 1–2. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Mégraud, F.; O’Morain, C.; Hungin, A.P.S.; Jones, R.; Axon, A.; Graham, D.Y.; Tytgat, G.; European Helicobacter pylori Study Group (EHPSG). Current concepts in the management of Helicobacter pylori infection -The Maastricht 2-2000 Consensus Report. Aliment. Pharmacol. Ther 2002, 16, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.; Bazzoli, F.; El-Omar, E.; Graham, D.; Hunt, R.; Rokkas, T.; Vakil, N.; Kuiper., E.J. Current concepts in the management of Helicobacter pylori infection: the Maastricht III Consensus Report. Gut 2007, 56, 772–781. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Atherton, J.; Axon, A.T.R.; Bazzoli, F.; Gensini, G.F.; Gisbert, J.P.; Graham, D.Y.; Rokkas, T.; El-Omar, E.M.; Kuipers, E.J.; European Helicobacter Study Group. Management of Helicobacter pylori infection—the Maastricht IV/ Florence Consensus Report. Gut 2012, 61, 646–664. [Google Scholar] [CrossRef] [PubMed]
- Coelho, L.G.; León-Barúa, R.; Quigley, E.M. Latin-American Consensus Conference on Helicobacter pylori infection. Latin-American National Gastroenterological Societies affiliated with the Inter-American Association of Gastroenterology (AIGE). Am. J. Gastroenterol. 2000, 95, 2688–2691. [Google Scholar] [CrossRef] [PubMed]
- Coelho, L.G.; Coelho, M.C. Clinical Management of Helicobacter pylori: The Latin American Perspective. Dig. Dis. 2014, 32, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Abdo-Francis, J.M.; Uscanga, L.; Sobrino-Cossio, S.; Rivera-Ramos, J.F.; Huerta-Iga, F.; Tamayo de la Cuesta, J.L. [III Mexican Consensus on Helicobacter pylori]. Rev. Gastroenterol. Mex. 2007, 72, 323–338. [Google Scholar] [PubMed]
- Rollan, A.; Arab, J.P.; Camargo, M.C.; Candia, R.; Harris, P.; Ferreccio, C.; Rabkin, C.S.; Gana, J.C.; Cortés, p.; Herrero, R.; Durán, L.; García, A.; Toledo, C.; Espino, A.; Lusting, N.; Sarfatis, A.; Figueroa, C.; Torres, J.; Riquelme, A. Management of Helicobacter pylori infection in Latin America: A Delphi technique-based consensus. World J. Gastroenterol. 2014, 20, 10969–10983. [Google Scholar] [CrossRef]
- Zagari, R.M.; Romano, M.; Ojetti, V.; Stockbrugger, R.; Gullini, S.; Annibale, B.; Farinati, F.; Ierardi, E.; Maconi, G.; Rugge, M.; Calabrese, C.; Di Mario, F.; Luzza, F.; Pretolani, S.; Savio, A.; Gasbarrini, G.; Caselli, M. Guidelines for the management of Helicobacter pylori infection italy: The III Working Group Consensus Report 2015. Dig. Liver Dis. 2015, 47, 903–912. [Google Scholar] [CrossRef]
- Graham, D.Y.; Fischbach, L. Helicobacter pylori treatment in the era of increasing antibiotic resistance. Gut 2010, 59, 1143–1153. [Google Scholar] [CrossRef] [PubMed]
- Mégraud, F.; Lehours, P. Helicobacter pylori detection and antimicrobial susceptibility testing. Clin. Microbiol. Rev. 2007, 20, 280–322. [CrossRef]
- Li, H.; Shen, Y.; Song, X.; Tang, X.; Hu, R.; Marshall, B.J.; Tang, H.; Benghezal, M. Need for standardization and harmonization of Helicobacter pylori antimicrobial susceptibility testing. Helicobacter 2022, 27, e12873. [CrossRef] [PubMed]
- CLSI M100; Performance Standards for Antimicrobial Susceptibility testing. 32nd Ed. CLSI supplement M100. Clinical and Laboratory Standards Institute, 2022.
- López-Vidal, Y.; Rangel-Frausto, M.S.; Calva, J.J. Antibiotic resistance of Helicobacter pylori in an infectious disease referral center. Rev. Investig. Clin. 1998, 50, 19–24. [Google Scholar]
- Torres, J.; Camorlinga-Ponce, M.; Pérez-Pérez, G.; Madrazo-De la Garza, A.; Dehesa, M.; González-Valencia, G.; Muñoz, O. Increasing Multidrug Resistance in Helicobacter pylori Strains Isolated from Children and Adults in Mexico. J. Clin. Microbiol. 2001, 39, 2677–2680. [Google Scholar] [CrossRef] [PubMed]
- Garza-González, E.; Pérez-Pérez, G.I.; Alanís-Aguilar, O.; Tijerina-Menchaca, R.; Maldonado-Garza, H.J.; Bosques-Padilla, F.J. Antibiotic Susceptibility Patterns of Helicobacter pylori Strains Isolated from Northeastern Mexico. J. Chemother. 2002, 14, 342–345. [Google Scholar] [CrossRef]
- Chihu, L.; Ayala, G.; Mohar, A.; Hernández, A.; Herrera-goepfert, R.; Fierros, G.; González-Márquez, H.; Silva, J. Antimicrobial Resistance and Characterization of Helicobacter pylori Strains Isolated from Mexican Adults with Clinical Outcome. J. Chemother. 2005, 17, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Boyanova, L.; Hadzhiyski, P.; Gergova, R.; Markovska, R. Evolution of Helicobacter pylori Resistance to Antibiotics: A Topic of Increasing Concern. Antibiotics 2023, 12, 332. [Google Scholar] [CrossRef] [PubMed]
- Camargo, C.M.; García, A.; Riquelme, A.; Otero, W.; Camargo, C.A.; Hernandez-García, T.; Candia, R.; Bruce, M.G.; Rabki, C.S. The Problem of Helicobacter pylori Resistance to Antibiotics: A Systematic Review in Latin America. Am. J. Gastroenterol. 2014, 109, 485–495. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; Rokkas, T.; Gisbert, J.P.; Liou, J.-M.; Schulz, C.; Gasbarrini, A.; Hunt, R.; Leja, M.; O’Morain, C.; Rugge, M.; Suerbaum, S.; Tilg, H.; Sugano, K.; El-Omar, E.M.; On behalf of the European Helicobacter and Microbiota Study Group. Management of Helicobacter pylori infection: the Maastricht VI/Florence Consensus Report. Gut 2022, 0, 1–39. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; Hunt, R.; Moayyedi, P.; Rokkas, T.; Rugge, M.; Selgrad, M.; Suerbaum, S.; Sugano, K.; El-Omar, E.M.; European Helicobacter and Microbiota Study Group and Consensus panel. Management of Helicobacter pylori infection—the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.C.; Iyer, P.G.; Moss, S.F. AGA Clinical Practice Update on the Management of Refractory Helicobacter pylori Infection: Expert Review. Gastroenterology 2021, 160, 1831–1841. [Google Scholar] [CrossRef] [PubMed]
- Bosques-Padilla, F.J.; Remes-Troche, J.M.; González-Huezo, M.S.; Pérez-Pérez, G.; Torres-López, J.; Abdo-Francis, J.M.; Bielsa-Fernandez, M.V.; Camargo, M.C.; Esquivel-Ayanegui, F.; Garza-González, E.; Hernández-Guerrero, A.I.; Herrera-Goepfert, R.; Huerta-Iga, F.M.; Leal-Herrera, Y.; Lopéz-Colombo, A.; Ortiz-Olvera, N.X.; Riquelme-Pérez, A.; Sampieri, C.L.; Uscanga-Domínguez, L.F.; Velarde-Ruiz, V.J.A. IV consenso mexicano sobre Helicobacter pylori. Rev. Gastroenterol. Mex. 2018, 83, 325–341. [Google Scholar] [CrossRef] [PubMed]
- Dehesa, M.; Larisch, J.; Dibildox, M.; Di Silvio, M.; Lopez, L.H.; Ramirez-Barba, E.; Torres, J. Comparison of Three 7-Day Pantoprazole-Based Helicobacter pylori Eradication Regimens in a Mexican Population with High Metronidazole Resistance. Clin. Drug Investig. 2002, 22, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Ayala, G.; Galván-Portillo, M.; Chihu, L.; Fierros, G.; Sánchez, A.; Carrillo, B.; Román, A.; López-Carrillo, L.; Silva-Sánchez, J. , Study Group. Resistance to Antibiotics and Characterization of Helicobacter pylori Strains Isolated from Antrum and Body from Adults in Mexico. Microb. Drug Resist. 2011, 17, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Mucito-Varela, E.; Castillo-Rojas, G.; Calva, J.J.; López-Vidal, Y. Integrative and Conjugative Elements of Helicobacter pylori Are Hypothetical Virulence Factors Associated with Gastric Cancer. Front. Cell. Infect. Microbiol. 2020, 10, 525335. [Google Scholar] [CrossRef] [PubMed]
- Camorlinga-Ponce, M.; Gómez-Delgado, A.; Aguilar-Zamora, E.; Torres, R.C.; Giono-Cerezo, S.; Escobar-Ogaz, A.; Torres, J. Phenotypic and Genotypic Antibiotic Resistance Patterns in Helicobacter pylori Strains From Ethnically Diverse Population in México. Front. Cell. Infect. Microbiol. 2021, 10, 539115. [Google Scholar] [CrossRef] [PubMed]
- Contreras-Omaña, R.; Escorcia-Saucedo, A.E.; Velarde-Ruiz, V.J.A. Prevalence and impact of antimicrobial resistance in gastrointestinal infections: A review. Rev. Gastroenterol. Mex. 2021, 86, 265–275. [Google Scholar] [CrossRef]
- Ladrón-de-Guevara, L.; Bornstein-Quevedo, L.; González-Huezo, S.; Castañeda-Romero, B.; Costa, F.G.; di Silvio-López, M. Helicobacter pylori erradication in México with a levofloxacin-base scheme versus standard triple therapy: Results from an open-label, randomized, noninferiority phase iiib trial. Rev. Gastroenterol. Mex. 2019, 84, 274–283. [Google Scholar] [CrossRef]
- Lesbros-Pantoflickova, D.; Corthésy-Theulaz, I.; Blum, A.L. Helicobacter pylori and Probiotics. J. Nutr. 2007, 137, 812S–818S. [Google Scholar] [CrossRef] [PubMed]
- Valdovinos, M.A.; Montijo, E.; Abreu, A.T.; Heller, S.; González-Garay, A.; Bacarreza, D.; Bielsa-Fernández, M.; Bojórquez-Ramos, M.C.; Bosques-Padilla, F.; Burguete-García, A.I.; Carmona-Sánchez, R.; Consuelo-Sánchez, A.; Coss-Adame, E.; Chávez-Barrera, J.A.; de Ariño, M.; Flores-Calderón, J.; Gómez-Escudero, O.; González-Huezo, M.S.; Icaza-Chávez, M.E.; Larrosa-Haro, A.; Morales-Arámbula, M.; Murata, C.; Ramírez-Mayans, J.A.; Remes-Troche, J.M.; Rizo-Robles, T.; Peláez-Luna, M.; Toro-Monjaraz, E.M.; Torre, A.; Urquidi-Rivera, M.E.; Vázquez, R.; Yamamoto-Furusho, J.K.; Guarner, F. The Mexican consensus on probiotics in gastroenterology. Rev. Gastroenterol. Mex. 2017, 82, 156–178. [Google Scholar] [CrossRef]
- Eslami, M.; Yousefi, B.; Kokhaei, P. , Moghadas, A.J.; Moghadam, B.S.; Arabkari, V.; Niazi, Z. Are probiotics useful for therapy of Helicobacter pylori diseases? Comp. Immunol. Microbiol. Infect. Dis. 2019, 64, 99–108. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Minimum inhibitory concentrations due to pathology; A) Amoxicillin, B) Clarithromycin, C) Metronidazole, and D) Tetracycline.
Figure 1.
Minimum inhibitory concentrations due to pathology; A) Amoxicillin, B) Clarithromycin, C) Metronidazole, and D) Tetracycline.
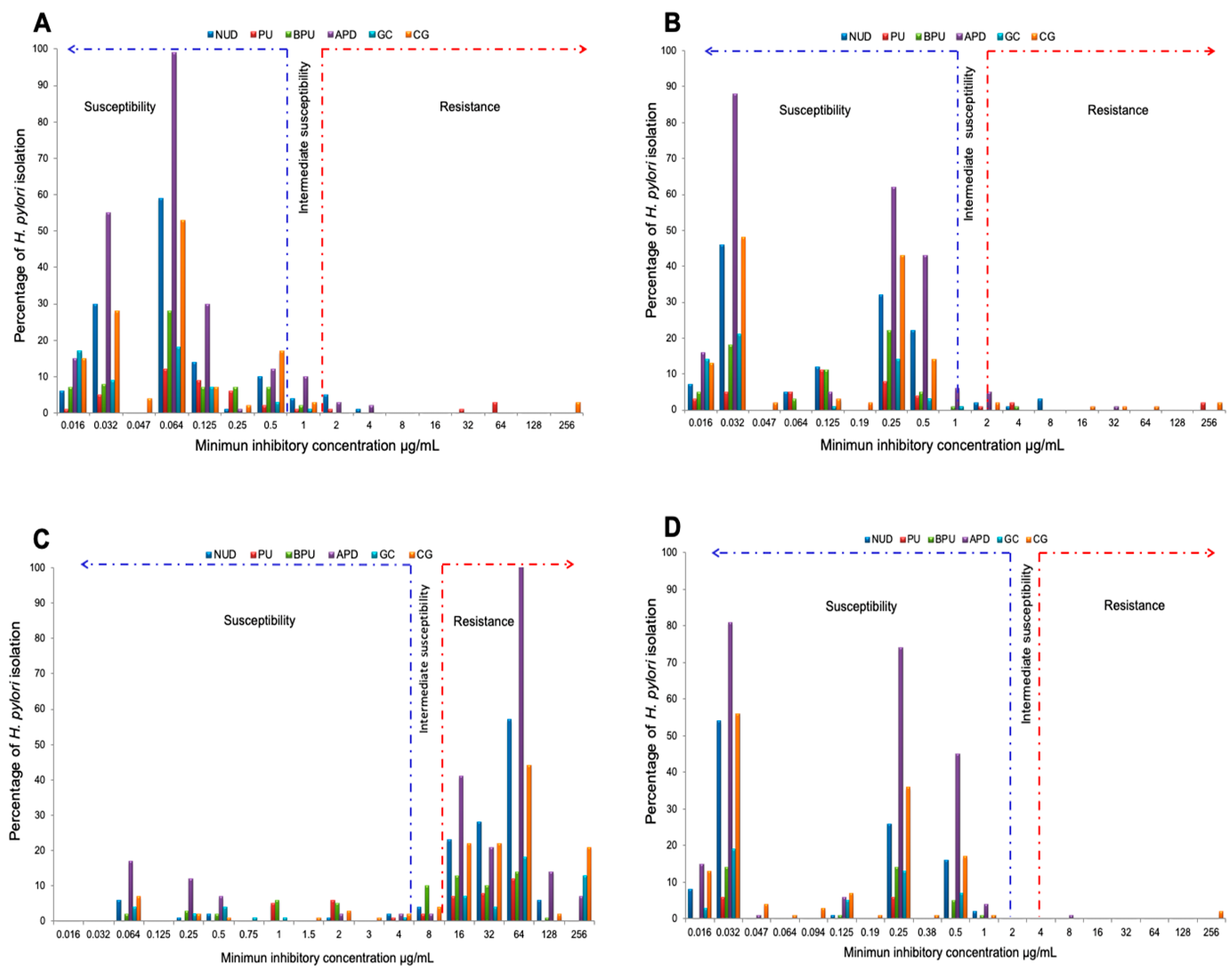
Figure 2.
Percentage of H. pylori isolate susceptible, with intermediate susceptibility and resistant to 4 antibiotics susceptibility in 651 isolates.
Figure 2.
Percentage of H. pylori isolate susceptible, with intermediate susceptibility and resistant to 4 antibiotics susceptibility in 651 isolates.
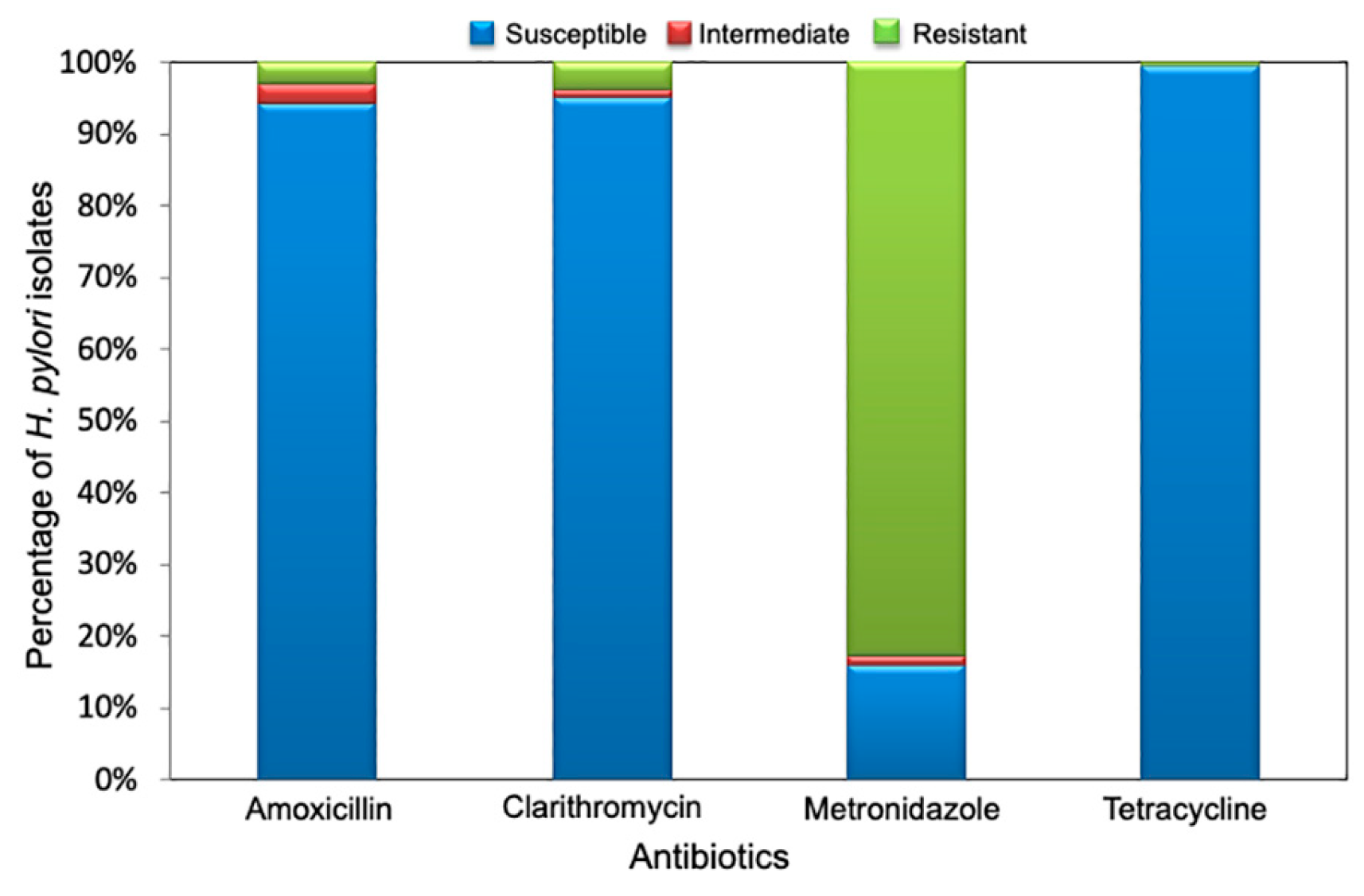
Figure 3.
Percentage of H. pylori isolate susceptible, with intermediate susceptibility and resistant to 4 antibiotics, according to the period of isolation.
Figure 3.
Percentage of H. pylori isolate susceptible, with intermediate susceptibility and resistant to 4 antibiotics, according to the period of isolation.
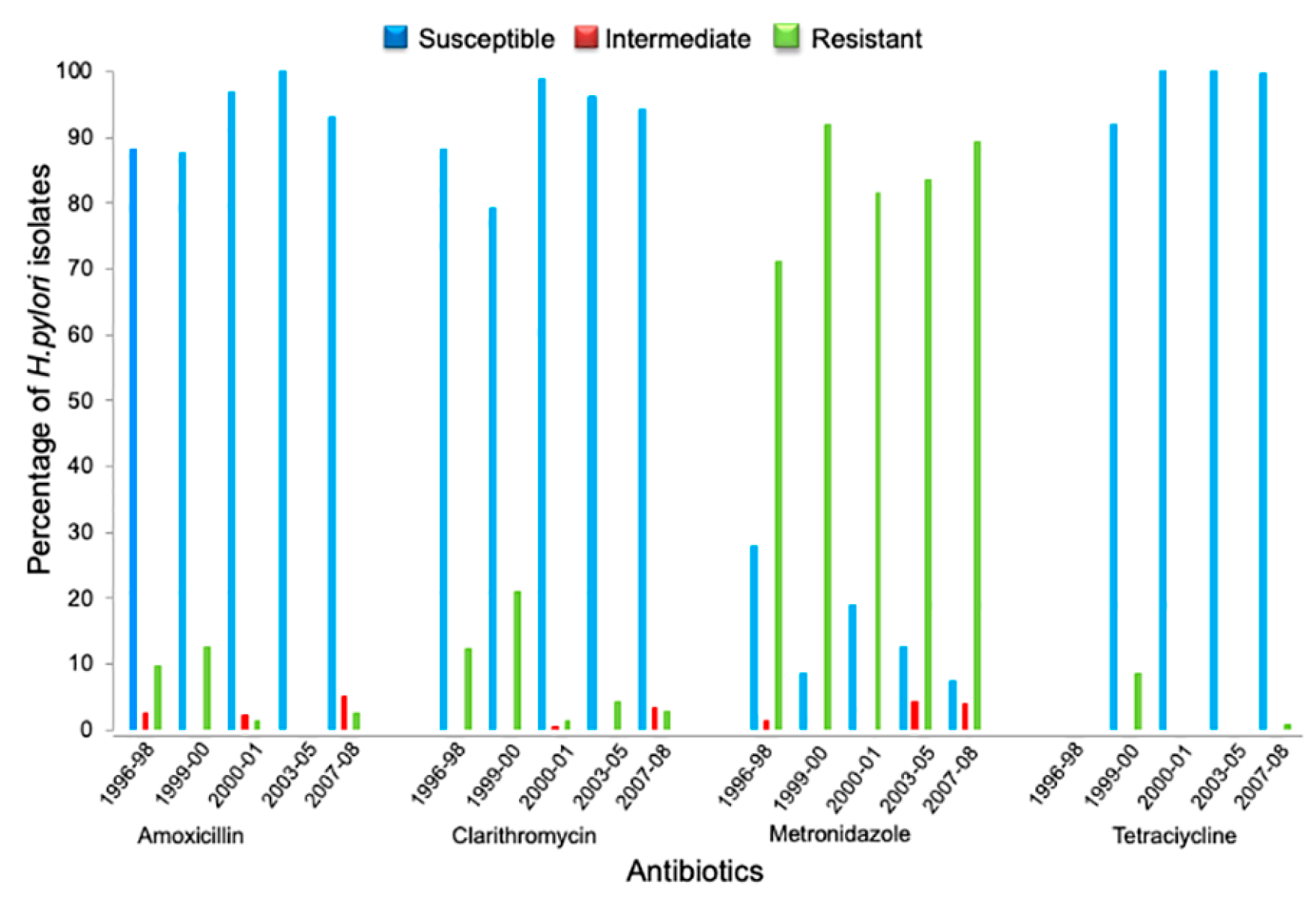
Figure 4.
The geometric mean of MIC for 4 antibiotics according to the period of isolation of H. pylori.
Figure 4.
The geometric mean of MIC for 4 antibiotics according to the period of isolation of H. pylori.
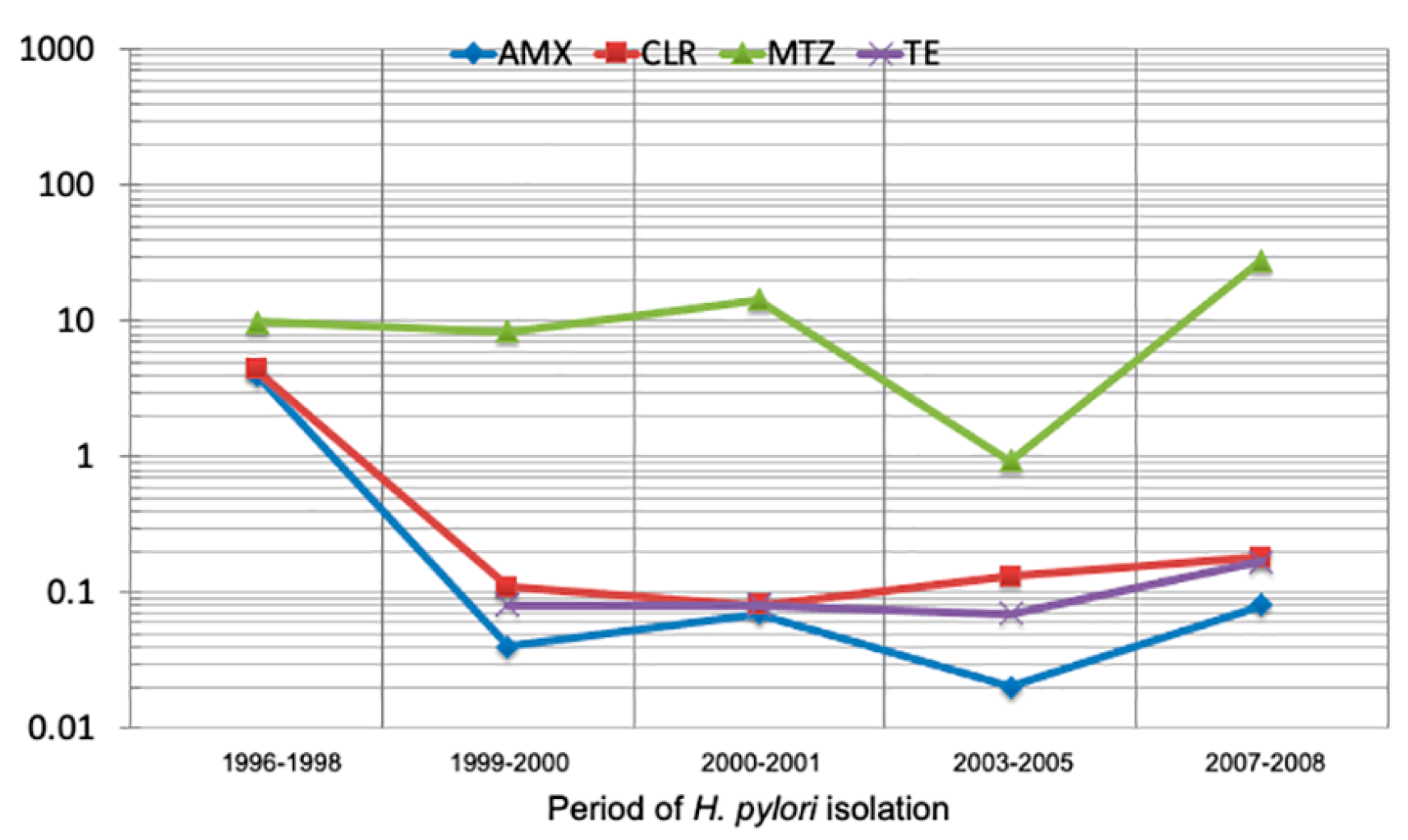

Table 1.
Participants’ demographic data according to the period of isolation of Helicobacter pylori.
Table 1.
Participants’ demographic data according to the period of isolation of Helicobacter pylori.
| Collection | n | Gender | Age | Period | |
| M | F | Mean (min -max value ) | |||
| I | 83 | 50 | 33 | 57.4 (30 – 72) | 1996 to 1998 |
| II | 24 | 3 | 21 | 42.7 (19 – 71) | 1999 to 2000 |
| III | 338 | 135 | 203 | 48.1 (15 – 87) | July 2000 to December 2001 |
| IV | 24 | 7 | 17 | 55.5 (29 – 79) | 2003 to 2005 |
| V | 182 | 54 | 128 | 46.9 (15 – 87) | May 2007 to January 2008 |
| TOTAL | 651 | 249 | 402 | ||
M = Male, F = Female, min = minimum, max = maximum.
Table 2.
Percentage of isolates resistant to 4 antibiotics according to the period of isolation of H. pylori.
Table 2.
Percentage of isolates resistant to 4 antibiotics according to the period of isolation of H. pylori.
| Collection | Period | Isolates n |
Isolates resistant to | ||||
|---|---|---|---|---|---|---|---|
| AMX n (%) |
CLR n (%) |
MTZ n (%) |
TE n (%) |
CLR-MTZ n (%) |
|||
| I | 1996 to 1998 | 83 | 10 (12.05) | 10 (12.05) | 60 (72.29) | NT | 1 (1.2) |
| II | 1999 to 2000 | 24 | 3 (12.5) | 5 (20.83) | 22 (91.67) | 2 (8.33) | 3 (12.5) |
| III | July 2000 to December 2001 | 338 | 11 (3.25) | 5 (1.48) | 275 (81.36) | 0 (0.0) | 2 (0.59) |
| IV | 2003 to 2005 | 24 | 0 (0.0) | 1 (4.17) | 21 (87.5) | 0 (0.0) | 2 (8.33) |
| V | May 2007 to January 2008 | 182 | 12 (7.15) | 11 (6.05) | 169 (92.86) | 1 (0.53) | 5 (2.75) |
| Total | 651 | 36 (5.53) | 32 (4.9) | 547 (84.02) | 3 (0.46) | 13 (1.99) | |
AMX=amoxicillin, CLR=clarithromycin, MTZ=metronidazole, TE=tetracycline, CLR-MTZ=clarithromycin-metronidazole. NT=not tested.
Table 3.
Percentage of Helicobacter pylori isolate resistant to one, two, three, and four antibiotics, according to the gastric disease.
Table 3.
Percentage of Helicobacter pylori isolate resistant to one, two, three, and four antibiotics, according to the gastric disease.
|
Pathology (n) |
Antibiotic resistance* | |||
|
1 n (%) |
2 n (%) |
3 n (%) |
4 n (%) |
|
| APD (227) | 168 (74) | 24 (10.57) | - | - |
| CG (132) | 107 (81.06) | 8 (6.06) | - | 2 (1.52) |
| NUD (130) | 108 (83.08) | 9 (6.92) | 4 (3.08) | - |
| BPU (66) | 46 (69.7) | 3 (4.55) | - | - |
| GC (55) | 41 (74.55) | 2 (3.64) | - | - |
| PU (41) | 25 (60.98) | 3( 7.32) | 4 (9.76) | - |
APD = acid peptic disease, CG = chronic gastritis, NUD = non-ulcerous dyspepsia, BPU = bleeding peptic ulcer, GC = gastric cancer, and PU = peptic ulcer. *Include intermediate isolations and intermediate/resistant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



