
Submitted:
17 July 2024
Posted:
18 July 2024
You are already at the latest version
Abstract
The primary objective of this systematic review study was to investigate the effectiveness, durability, and adverse events of PLLA treatment for aesthetic indications. The search strategy was performed in MEDLINE (Ovid). The electronic literature search of five databases was performed, from the inception of the databases until 12th of February 2024. This was to identify randomized clinical trials that assessed PLLA treatment in adult individuals exhibiting facial aging and/or facial lipoatrophy. Risk of bias was assessed using the Cochrane Risk-of-Bias Tool for Randomized Trials (RoB 2). Eleven RCTs out of 1467 identified citations were included. Four studies showed increased dermal thickness, significant improvement in facial lipoatrophy severity and aesthetic clinical scores, after PLLA treatment with its effects sustained for at least 25 months. Two studies demonstrated the superiority of PLLA over injectable human collagen. Also, three studies showed positive results favoring PLLA when compared with PH gel in lipoatrophy severity, trans epidermal water loss, skin quality, elasticity, and patient satisfaction. All adverse events were mild-to-moderate in intensity, and the main ones worth noting were bruising, hematoma, tenderness, nodules, and edema. Five out of 11 studies were considered as high risk of bias. The evidence on the effectiveness and safety of PLLA for facial rejuvenation is of low quality; thus, the reported high effectiveness, safety, and long-lasting effects for this purpose, should be further investigated.
Keywords:
Poly-L-lactic Acid
; Facial Aesthetics
; Biostimulador
; Systematic review
1. Introduction
With the growing interest in facial rejuvenation and the consequent advancement in understanding the aging process, collagen bio-stimulators such us Poly-L-lactic Acid (PLLA) have been prominent in the aesthetic market[1]. PLLA is a synthetic, biodegradable, biocompatible, and immunologically inert polymer belonging to the family of alpha hydroxy acids polymers[2]. Its mechanism of action occurs through the stimulation of neo-collagenases, by triggering a foreign body reaction to the injected material, resulting in a controlled cellular inflammatory response, which consequently activate fibroblast to produce autologous collagen[3]. This results in a natural and semi-permanent correction of facial volume loss associated with aging[4].
Historically, PLLA was first approved in Europe as a filler in 1999, under the trade name New-Fill® (Biotech Industry SA). Then, in 2004, it was approved as Sculptra® (Dermik Laboratories, Sanofi Aventis, USA) by the FDA (Food and Drug Administration) as a lipoatrophy treatment for people with human immunodeficiency virus (HIV), presenting high efficacy in the restoration of facial volume loss[5,6,7]. In 2009, it was also approved for correction of deep nasolabial folds and other wrinkles in HIV population and recently, in 2023, an extension of the indications was approved for the correction of fine wrinkles in the cheek region.[8,9]. In addition, PLLA (Sculptra Aesthetic®), has also been used for aesthetic indications in healthy patients, showing an extensive track record of efficacy and safety[3,8,10].
Therefore, PLLA is a recommended treatment for enhancing skin tightness due to aging. It is also effective for improving wrinkles, creases, scars, and other changes caused by aging and volume loss. Application in various layers like supraperiosteal, subcutaneous, and subdermal is advised for optimal results in facial rejuvenation by improving skin quality, firmness, and facial contour [11,12].
In addition, numerous clinical trials assessing its safety, effectiveness, and durability have been published. These studies included not only HIV populations, but also healthy individuals and reported that the majority of the studied volunteers were satisfied or very satisfied with the clinical results of PLLA treatment[6,8]. Notwithstanding, it is important to assess the aforementioned studies, since most of them used different PLLA treatment protocols, mainly regarding the dilution process and the quantity of PLLA applied, factors that certainly influence the efficacy, durability and adverse events of this bio-stimulator[13]. Thus, there is a necessity of a systematic synthesis of PLLA literature for aesthetic indications, to enhance its uses in clinical practice and to provide a guideline protocol. Based on this, the aim of this systematic review was to investigate the effectiveness, durability, and adverse events of PLLA treatment for aesthetic indications.
2. Materials and Methods
Protocol and Research Question
This systematic review was registered beforehand in PROSPERO (the International Prospective Register of Systematic Reviews, #CRD42023472405). The research question was formed using the PICO framework[14], being an acronym for: P = Patients, I = Intervention, C = Comparison, O = Outcome. The population comprised of patients (P) with signs of facial aging and/or lipoatrophy, while the investigated intervention (I) was treatment with Poly-L-Lactic Acid for the restoration of tissue volume and facial aging. The outcomes (O) were the efficacy, durability and safety of PLLA and the comparison (C) were no treatment, placebo or another treatments for the aging face and/or lipoatrophy. The present systematic review followed the Preferred Reporting Items for The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-Analyses of Health Care Interventions (the PRISMA-P checklist)[15] (Supplemental file 1).
The inclusion criteria were a) Randomized clinical trials; b) adult individuals (over the age of 18) exhibiting of facial aging; c) adult individuals (over the age of 18) presenting facial lipoatrophy. The following exclusion criteria were applied: a) Studies that cannot be found in other languages other than English, Portuguese and Spanish; b) publications irrelevant to the research question; c) cross-sectional, case-control, and observational studies, editorials, letters, legal cases, interviews, case-series, case reports and reviews.
Search Strategy and Selection Criteria
The search strategy was created and executed in MEDLINE (Ovid) with the assistance of the librarians (LL) and (ELS) at the University Library at Karolinska Institutet. The search methods were reviewed by another librarian before the final searches. Together with authors RS and GDC, each search concept was identified using Medical Subject Headings (MeSH-terms) and free text terms. The Polyglot Search Translator[16] was utilized to translate the search into other databases. The final electronic search covered databases such as MEDLINE, EMBASE, CINAHL, and Web of Science from the inception of each database up to the 12th of February 2024. The duplication was carried out following the method by Bramer et al. (2016)[17]. Additionally, a step was included to compare digital object identifiers (DOI) and search the reference-lists of the included studies. The complete search strategy for all databases is provided in Supplemental file 2.
Selection of Studies
To mitigate any potential bias during the study screening process, we utilized the web-based tool Rayyan[18]. This screening was conducted independently and in a blinded fashion by authors RS and FCS. In instances of disagreement regarding eligibility, these were resolved through discussions with author GDC, who took the final decisions. Once all discrepancies were resolved, authors RS and FS endeavored to obtain the full texts of the included and potentially eligible studies. Subsequently, these retrieved studies were thoroughly reviewed in full text by authors RS and FCS to ascertain their alignment with the inclusion criteria. Any disagreements were addressed through discussions with author GDC, as before. Additionally, we identified supplementary articles through citation searches. The full texts of the identified studies were then retrieved and reviewed in the same manner as previously described.
Analysis of Risk of Bias
Risk of bias and quality assessment of the included articles were performed using the Cochrane Risk-of-Bias Tool for Randomized Trials (RoB 2)[19]. This tool is composed of five domains: randomization process (D1), deviations from the intended interventions (D2), missing outcome data (D3), measurement of the outcome (D4) and selection of the reported results (D5). Each domain can be judged for risk of bias into three categories: low risk, some concerns or high risk. Two authors (AB and AC) evaluated the risk of bias for each study blinded and independently. In cases where conflict arose it was resolved by discussion with the author RP, serving as a judge. The individual quality assessment of each included study is presented in Table 1.
Extraction of Data
Following the risk of bias and quality assessment, data extraction was carried out. A data extraction form was devised, created (by authors RS, GDC), and pilot-tested independently on three randomly chosen studies by authors RS and MCS to ensure extraction consistency. The extracted data encompassed information on the characteristics of the included studies and participants, including author details, study type, diagnosis/criteria utilized, participant numbers, average age, gender distribution, doses of PLLA, dilution protocol, regions in which PLLA was injected, and details of randomized studies. Any discrepancies in the data extraction process were resolved by author GDC, acting as an adjudicator.
3. Results
Literature Search Outflow
The entire literature search from all databases provided 2,586 citations, of which 1,119 were overlaps (Figure 1). Thus, 1467 citations were evaluated for eligibility. The title and abstracts of those articles were then screened which resulted in an exclusion of 1412 articles, leaving 55 full text that were sought for retrieval, of which all of them were successfully retrieved. Out of this 55 full-texts, 44 full-texts did not meet the inclusion criteria and were excluded. Then, 11 full texts were included in this systematic review, all randomized controlled studies (RCTs) (Table 1).
Studies Results
Efficacy and Durability of PLLA: Immediate x Delayed Protocol
Some studies used an immediate or delayed protocol for PLLA injection. As for short follow-up (up to 12 weeks), some studies found a significant increase of dermal thickness in injected regions and in self-assessment scores for the immediate group, compared to the delayed[6], but no differences at week 24. The severity score of lipoatrophy was declined in both groups after 2 years[6], as well as patients’ self-perceived facial thinness was significantly more positive for both groups, leading to less depression and anxiety; moreover, PLLA’s positive psychological and physical effects persisted for at least 18 months[20] .Conversely, some studies found a significant improvement in facial lipoatrophy severity[5], MBSRQ-AS scores[5], aesthetic improvement[21], and SS scores[21] for the participants in the immediate group protocol. In addition, Brown et al.21 found that individuals receiving injectable PLLA maintained aesthetic improvement for up to 25 months.
PLLA x Human Collagen
Two studies compared the use of PLLA with injectable human collagen. In both, the PLLA demonstrated statistically significant improvements from baseline in WAS score2 and in IGE through all the follow-ups[10], being superior to human collagen.
Other Comparisons
PLLA was compared with polyacrylamide hydrogel (PH) gel by Lafaurie et al (2012)[22]. A significant improvement from baseline in lipoatrophy severity was found in both groups at week 48 and 96, with no significant differences in patients satisfaction scores[22]. When compared to saline solution (placebo), participants receiving PLLA had significantly improved skin quality at the 12month-visit, and greater reduction in trans epidermal water loss, higher elasticity, and higher satisfaction through all the follow-ups[3]. Moreover, this improvement was also found when comparing PLLA with no treatment[8]. Participants receiving PLLA had higher GCWS scores at rest and dynamic, increased GAIS scores, and significant increased FACE-Q scores in all follow-up[8].
Adverse Events
Most studies reported mild-to-moderate intensity adverse events, such as bruising, bleeding, tenderness, firmness, injection-site hematoma, erythema, pain, pigmentation and pruritus, limited superficial local cellulitis, headache, rhinorrhea, perioral hypoesthesia, dizziness, vagal hypertonia during injections, and edema post-injections[5,6,8,21,22,23,24]. Additionally, Moyle et al.[20] reported that 7% of adverse events were severe in intensity: one case of injection-site induration and nine cases of injection-site nodules, which were noted at the 2 years recall. Subcutaneous papules and nodules were also reported in shorter follow-ups in some studies[5,10,21], being presented in 41% of the studied population in the study conducted by Lafaurie et al.[22].
Studies comparing PLLA and human collagen concluded that higher incidence of adverse events were reported on the collagen groups compared with the injectable PLLA groups[2,10]. Further, only one study reported no adverse events related to the treatment[3], stating that just three patients had temporary mild swelling.
Dilution Protocol
Only one study tested dilution protocol for PLLA (Sculptra). Palm et al.[23] evaluated two protocols to dilute PLLA: 8mL/sterile water + 1 mL of 2% lidocaine hydrochloride, totaling 9 ml of product, with no standing time was required (experimental – G1). The control group (G2) received PLLA diluted in 5ml of sterile water only, with a standing time from 2 to 72 h. The amount of product injected was also different: for G1, 4.5mL per nasolabial fold; as for G2, 2.5 mL per nasolabial fold. In the last follow-up (48 weeks), both groups presented similar results for WAS, GAIS, and satisfaction with results. The remaining studies presented varied protocols according to what was prescribed by manufacturers by the time of data collection (which has changed over the years).
Quality Assessment
None of the included studies were considered as having low risk of bias. Five articles were considered as having high risk of bias as not fulfilling the criteria for the topic “deviation from intended intervention” (D2)[5,6,8,20,23]. The risk of bias of the remained six articles was considered as some concerns [2,3,10,21,22,24]. Further, most of the studies presented some concerns regarding the “randomization process” (D1) and for “selection of the reported of results” (D5) all manuscripts were considered as presenting “some concerns” related to the risk of bias (Table 2).
4. Discussion
The primary findings of this systematic review indicate that PLLA is a highly effective and long-lasting treatment for facial aesthetics. Its effectiveness surpasses all other substances it was compared to, being a safe treatment, as most adverse effects were mild to moderate and resolved spontaneously. However, it is important to note that these results are mainly based on low-quality evidence.
The reported high efficacy of PLLA in all the included studies could be explained by its composition and mechanism of action that favors neocollagenesis. PLLA is an enantiomeric polymer of lactic acid, that is part of the alpha-hydroxy acids family, being biocompatible and biodegradable in nature. Its particles have an average size of 52 µm (40 µm to 63 µm), plate-shaped, non-porous, which accounts for their lower degradation rate when injected into tissues[25,26]. This slower degradation favors the process of neocollagenesis for a longer period. This process begins with the immune cells recognizing PLLA particles as foreign bodies resulting in a controlled cellular inflammatory response, in which monocytes are recruited and transform into macrophages, then fuse to form giant cells, recruit fibroblasts, and increase the levels of TGF-β1 and tissue inhibitor of metalloproteinase 1 (TIMP1), promoting the deposition of type I and III collagen. This process contributes to increase collagen production in the area treated with PLLA, resulting in firmer, thicker, and more elastic skin[25,26].
PLLA is made available in the form of a lyophilized powder in a sterile vial also containing non-pyrogenic mannitol (which improves the lyophilization of the particles), croscarmellose (an emulsifying agent that maintains particle distribution after reconstitution)[26]. Over the years, the process of reconstituting PLLA particles has been revisited[27]. In addition, most of studies included in this review presented varied reconstitution protocols. However, it is important to highlight that the reconstitution instructions of PLLA have changed according to the time of which the studies were performed, following the manufacturer’s instructions at each specific time. Initially, with NewFill®/Sculptra®, reconstitutions were carried out with a total volume of 5 mL[27]. In the present study, the most common reconstitution protocols were using 5 mL or 8 mL of sterile water. Notwithstanding, when these reconstitution protocols were compared no significant differences were found in the efficacy of PLLA[23]. Additionally, the efficacy remains unchanged whether reconstituted immediately or 24 to 72 hours before the procedure[27]. The resting period of 24 to 72 hours was considered necessary to hydrate the PLLA molecules, forming a homogeneous suspension with carboxymethylcellulose (CMC) without the formation of lumps. However, recent studies have shown no statistical differences between performing the reconstitution at 72 hours and immediately, without altering clinical efficacy. Therefore, based on the results of the included studies, we might confirm that the efficacy of PLLA is not altered by both the reconstituted volume and reconstitution time before injection procedure[27].
Since PLLA particles are not amorphous, they easily agglomerate with the excipient CMC, commonly leading to needle and cannula blockages making injection process difficult and the formation of nodules after applications, which was one of the most common adverse effects related to the product found in this study. To prevent nodules formation, post-application massages were recommended to avoid these complications, as the mechanical process dissolves potential nodules that may form[3]. The chance of nodule dissolution is higher when performed after application, even though a proper protocol has not been reported. Importantly, the most prevalent adverse effects reported in this review are related with the injection procedure and patients’ following post-injection recommendations, and not to PLLA per se. Furthermore, despite the fibroplasia process caused by PLLA influencing aesthetic outcomes, there is no evidence of residual fibrosis[4], insignificant amounts of degradation residues are found in vital organs, and the product is completely eliminated within 18 months, which demonstrates its safety[28]. However, only one study was considered free of treatment-related adverse events[3].
The global market for PLLA is undergoing substantial growth. In 2023, the market size for PLLA fillers was estimated to be approximately $268.1 million, with Scultra® being the front leader in the market[29]. In addition, among the included studies, all were conducted with the commercial PLLA product Sculptra®/NewFill®, confirming the predominance of these products in the available data. Only one study used a different product, GANA V®, to verify non-inferiority, compared with Sculptra®[24]. Although both products are composed of PLLA, they have different physicochemical properties, resulting in distinct particle shapes which can influence their clinical responses, durability, and adverse effects. Due to the limited literature on GANA V®, more studies are needed to prove its efficacy, durability, and safety, as well as to evaluate its polymeric chemical composition.
The quality of the evidence presented in this systematic review should be carefully considered when interpreting the results. Although PLLA has demonstrated significant efficacy and an acceptable safety profile compared to other substances, most of the included studies were classified as having high or moderate concerns regarding the risk of bias. Additionally, the lack of consistency in evaluation methods and clinical protocols limit the robustness of the conclusions. Therefore, even though PLLA treatment for facial aesthetic is increasing in clinical practice, it is essential to develop higher-quality clinical trials including objective and subjective assessments to confirm the findings presented in this systematic review.
Study Strengths and Limitations
The following measures were taken in order to minimize bias. The literature search was performed in several databases with the help of search experts. The article selection process and the risk of bias assessment was performed by two blinded authors independently to prevent bias, ensuring that each other’s decisions would not be a factor of influence. Another strength of this systematic review is the inclusion of only RCTs. However, this could also be seen as a limitation, as the included RCTs exhibit methodological flaws that prevent them from being considered high quality. Also, a quantitative analysis was not feasible since the outcomes and assessment of the included studies were diverse. In addition, there were substantial variations in PLLA reconstitution and administration protocols, which impacted the comparability of results. Also, the relatively low number of included studies (11) could be considered a limitation for this review.
Clinical Implications and Generalizability
The results of this study indicate that the clinical response to PLLA in both HIV patients and general patients for aesthetic purposes seems to be high. Both professional and patient evaluations are positive in almost all studies, indicating a significant improvement in dermal thickness and aesthetic perception. However, it is necessary to interpret these results with caution since all studies demonstrate gaps that reveal strong risks of bias, preventing a rigorous assessment of the real effects of PLLA-based biopolymers and complete recommendations for clinical practice.
Future Applications
To confirm the efficacy and safety of PLLA in facial aesthetic treatments, future high-quality studies should be conducted with high methodological rigor and impartiality. These studies should adopt standardized methodologies and ensure proper randomization and blinding processes, which were the major limitations of the included studies. These recommendations are necessary to reduce the risks of bias in future RCTs, and to stablish validated clinical protocols to provide robust and reliable evidence base on the clinical effects of PLLA.
5. Conclusions
PLLA demonstrated to be a highly effective and long-lasting treatment for facial aesthetics with a reasonable safety profile. However, all findings are supported by low-quality evidence.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, S1: Prisma Checklist; S2: Search strategy in different databases.
Author Contributions
R.S. and G.D.C had the main idea for the article. However, all authors contributed to the study conception and design. B.B.S.N, S.V. and M.B.B performed the literature search with help from the university library at Karolinska Institutet. Selection of papers was performed by R.S. and F.C.S. and double checked by G.D.C. Analysis of risk of bias was performed by A.C. C. and A.P.B. R.L.P double checked all parts of the assessment of risk of bias. G.D.C., M.B.C.S., and S.V. drafted the first manuscript that was critically revised by all authors that commented on previous versions of the manuscript. All authors read and approved the final version manuscript.
Funding
This research was financed by national funds through the FCT - Foundation for Science and Technology, I.P., under the project UIDB/04585/2020.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Acknowledgments
We would like to thank the librarians Sabina Gillsund & Narcisa Hannerz who performed and develop the search of the articles.
Conflicts of Interest
Authors A.C.C and A.P.B. are speakers for GALDERMA S.A. Brazil. All other authors declare that they have no conflicts of interest that might be relevant to the contents of this manuscript.
References
- Christen, M.-O. Collagen stimulators in body applications: a review focused on poly-L-lactic acid (PLLA). Clinical, cosmetic and investigational dermatology, 1019. [Google Scholar]
- Narins, R.S.; Baumann, L.; Brandt, F.S.; Fagien, S.; Glazer, S.; Lowe, N.J.; Monheit, G.D.; Rendon, M.I.; Rohrich, R.J.; Werschler, W.P. A randomized study of the efficacy and safety of injectable poly-L-lactic acid versus human-based collagen implant in the treatment of nasolabial fold wrinkles. Journal of the American Academy of Dermatology 2010, 62, 448–462. [Google Scholar] [CrossRef]
- Bohnert, K.; Dorizas, A.; Lorenc, P.; Sadick, N.S. Randomized, controlled, multicentered, double-blind investigation of injectable poly-L-lactic acid for improving skin quality. Dermatologic Surgery 2019, 45, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, R.; Vleggaar, D. Facial volume restoration of the aging face with poly-l-lactic acid. Dermatologic therapy 2011, 24, 2–27. [Google Scholar] [CrossRef] [PubMed]
- Carey, D.L.; Baker, D.; Rogers, G.D.; Petoumenos, K.; Chuah, J.; Easey, N.; Machon, K.; Cooper, D.A.; Emery, S.; Carr, A. A randomized, multicenter, open-label study of poly-L-lactic acid for HIV-1 facial lipoatrophy. JAIDS Journal of Acquired Immune Deficiency Syndromes 2007, 46, 581–589. [Google Scholar] [CrossRef]
- Moyle, G.; Lysakova, L.; Brown, S.; Sibtain, N.; Healy, J.; Priest, C.; Mandalia, S.; Barton, S. A randomized open-label study of immediate versus delayed polylactic acid injections for the cosmetic management of facial lipoatrophy in persons with HIV infection. HIV medicine 2004, 5, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.M.; Azizzadeh, B.; Graivier, M. Injectable poly-L-lactic acid (Sculptra): technical considerations in soft-tissue contouring. Plastic and reconstructive surgery 2006, 118, 55S–63S. [Google Scholar] [CrossRef]
- Fabi, S.; Hamilton, T.; LaTowsky, B.; Kazin, R.; Marcus, K.; Mayoral, F.; Joseph, J.; Hooper, D.; Shridharani, S.; Hicks, J. Effectiveness and Safety of Sculptra Poly-L-Lactic Acid Injectable Implant in the Correction of Cheek Wrinkles. Journal of Drugs in Dermatology: JDD 2024, 23, 1297–1305. [Google Scholar] [CrossRef]
- Food and Drug Administration FDA (2023). Summary of Safety and effectiveness Data (SSES). Available online: https://www.accessdata.fda.gov/cdrh_docs/pdf16/P160035B.pdf.
- Brandt, F.S.; Cazzaniga, A.; Baumann, L.; Fagien, S.; Glazer, S.; Kenkel, J.M.; Lowe, N.J.; Monheit, G.D.; Narins, R.S.; Rendon, M.I. Investigator global evaluations of efficacy of injectable poly-L-lactic acid versus human collagen in the correction of nasolabial fold wrinkles. Aesthetic surgery journal 2011, 31, 521–528. [Google Scholar] [CrossRef]
- Haddad, A.; Kadunc, B.V.; Guarnieri, C.; Noviello, J.S.; da Cunha, M.G.; Parada, M.B. Conceitos atuais no uso do ácido poli-l-láctico para rejuvenescimento facial: revisão e aspectos práticos. Surgical & cosmetic dermatology 2017, 9, 60–71. [Google Scholar]
- Akinbiyi, T.; Othman, S.; Familusi, O.; Calvert, C.; Card, E.B.; Percec, I. Better results in facial rejuvenation with fillers. Plastic and Reconstructive Surgery–Global Open 2020, 8, e2763. [Google Scholar] [CrossRef]
- Butterwick, K.; Lowe, N.J. Injectable poly-L-lactic acid for cosmetic enhancement: learning from the European experience. Journal of the American Academy of Dermatology 2009, 61, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Riva, J.J.; Malik, K.M.; Burnie, S.J.; Endicott, A.R.; Busse, J.W. What is your research question? An introduction to the PICOT format for clinicians. The Journal of the Canadian Chiropractic Association 2012, 56, 167. [Google Scholar] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Annals of internal medicine 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.M.; Sanders, S.; Carter, M.; Honeyman, D.; Cleo, G.; Auld, Y.; Booth, D.; Condron, P.; Dalais, C.; Bateup, S. Improving the translation of search strategies using the Polyglot Search Translator: a randomized controlled trial. Journal of the Medical Library Association: JMLA 2020, 108, 195. [Google Scholar] [CrossRef] [PubMed]
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. Journal of the Medical Library Association: JMLA 2016, 104, 240. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Systematic reviews 2016, 5, 1–10. [Google Scholar] [CrossRef]
- Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V. Cochrane handbook for systematic reviews of interventions. Hoboken: Wiley 2019.
- Moyle, G.J.; Brown, S.; Lysakova, L.; Barton, S.E. Long-term safety and efficacy of poly-L-lactic acid in the treatment of HIV-related facial lipoatrophy. HIV Med 2006, 7, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.A.; Rohrich, R.J.; Baumann, L.; Brandt, F.S.; Fagien, S.; Glazer, S.; Kenkel, J.M.; Lowe, N.J.; Monheit, G.D.; Narins, R.S.; et al. Subject global evaluation and subject satisfaction using injectable poly-L-lactic acid versus human collagen for the correction of nasolabial fold wrinkles. Plast Reconstr Surg 2011, 127, 1684–1692. [Google Scholar] [CrossRef] [PubMed]
- Lafaurie, M.; Dolivo, M.; Girard, P.M.; May, T.; Bouchaud, O.; Carbonnel, E.; Madelaine, I.; Loze, B.; Porcher, R.; Molina, J.M. Polylactic acid vs. polyacrylamide hydrogel for treatment of facial lipoatrophy: a randomized controlled trial [Agence Nationale de Recherches sur le SIDA et les Hépatites Virales (ANRS) 132 SMILE]. HIV Med 2013, 14, 410–420. [Google Scholar] [CrossRef]
- Palm, M.; Weinkle, S.; Cho, Y.; LaTowsky, B.; Prather, H. A Randomized Study on PLLA Using Higher Dilution Volume and Immediate Use Following Reconstitution. J Drugs Dermatol 2021, 20, 760–766. [Google Scholar]
- Han, W.Y.; Kim, H.J.; Kwon, R.; Kang, S.M.; Yon, D.K. Safety and efficacy of Poly-L-Lactic acid filler (Gana V vs. Sculptra) injection for correction of the nasolabial fold: a double-blind, non-inferiority, randomized, split-face controlled trial. Aesthetic Plastic Surgery 2023, 47, 1796–1805. [Google Scholar] [CrossRef]
- Oh, S.; Lee, J.H.; Kim, H.M.; Batsukh, S.; Sung, M.J.; Lim, T.H.; Lee, M.H.; Son, K.H.; Byun, K. Poly-L-lactic acid fillers improved dermal collagen synthesis by modulating m2 macrophage polarization in aged animal skin. Cells 2023, 12, 1320. [Google Scholar] [CrossRef]
- Sedush, N.G.; Kalinin, K.T.; Azarkevich, P.N.; Gorskaya, A.A. Physicochemical characteristics and hydrolytic degradation of polylactic acid dermal fillers: A comparative study. Cosmetics 2023, 10, 110. [Google Scholar] [CrossRef]
- Baumann, K.; Alm, J.; Norberg, M.; Ejehorn, M. Immediate Use After Reconstitution of a Biostimulatory Poly-L-Lactic Acid Injectable Implant. Journal of Drugs in Dermatology: JDD 2020, 19, 1199–1203. [Google Scholar] [CrossRef]
- Gupta, A.; Kumar, V. New emerging trends in synthetic biodegradable polymers–Polylactide: A critique. European polymer journal 2007, 43, 4053–4074. [Google Scholar] [CrossRef]
- Riddhesh, D. Global Poly-L-lactic Acid (PLLA) Filler Market. 2023. Available online: https://dataintelo.com/report/global-poly-l-lactic-acid-plla-filler-market/.
Figure 1.
The figure illustrates the PRISMA flow-chart of the database search strategy.
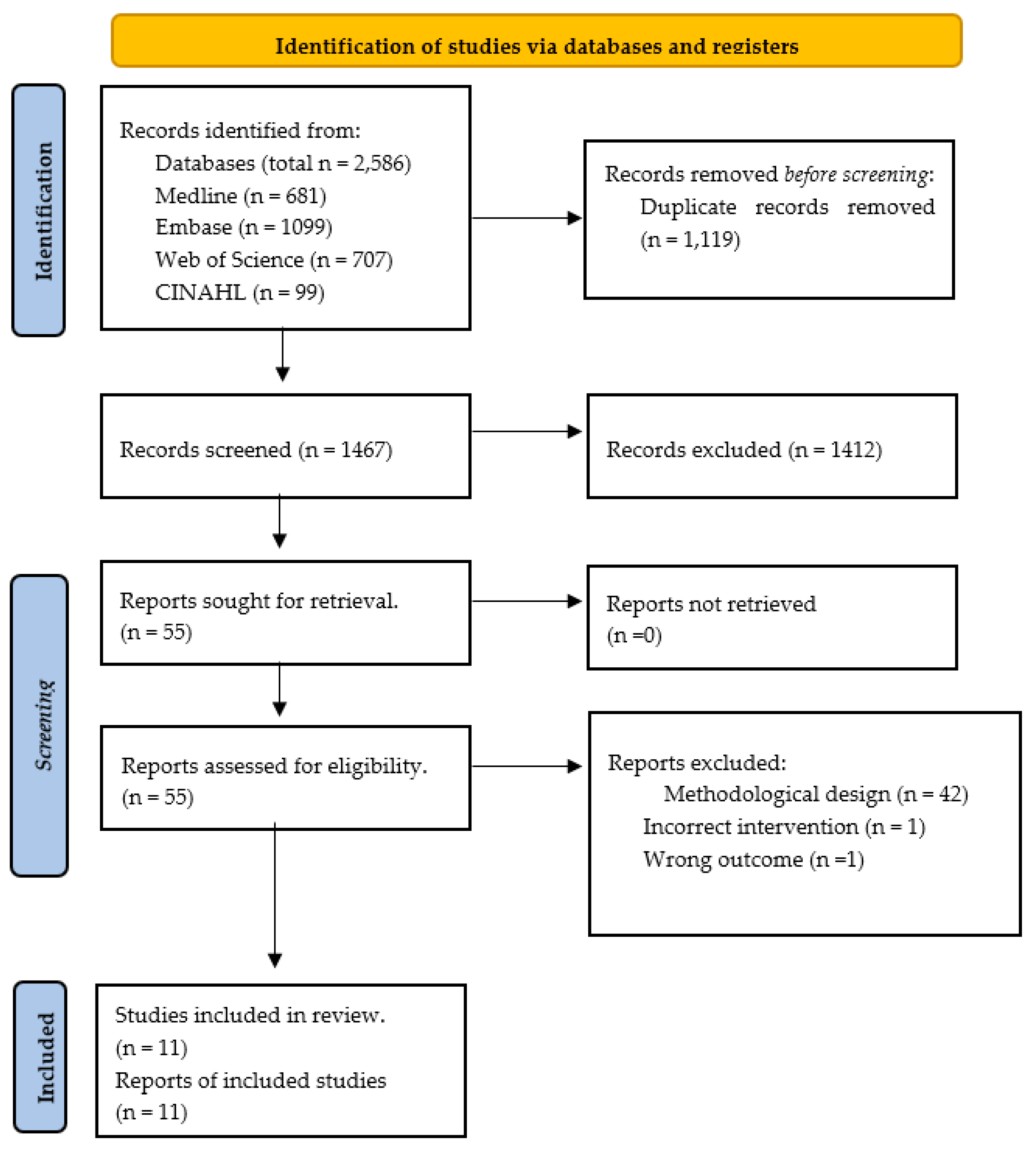

Table 1.
Table illustrating the extracted study characteristics of the eleven included studies.
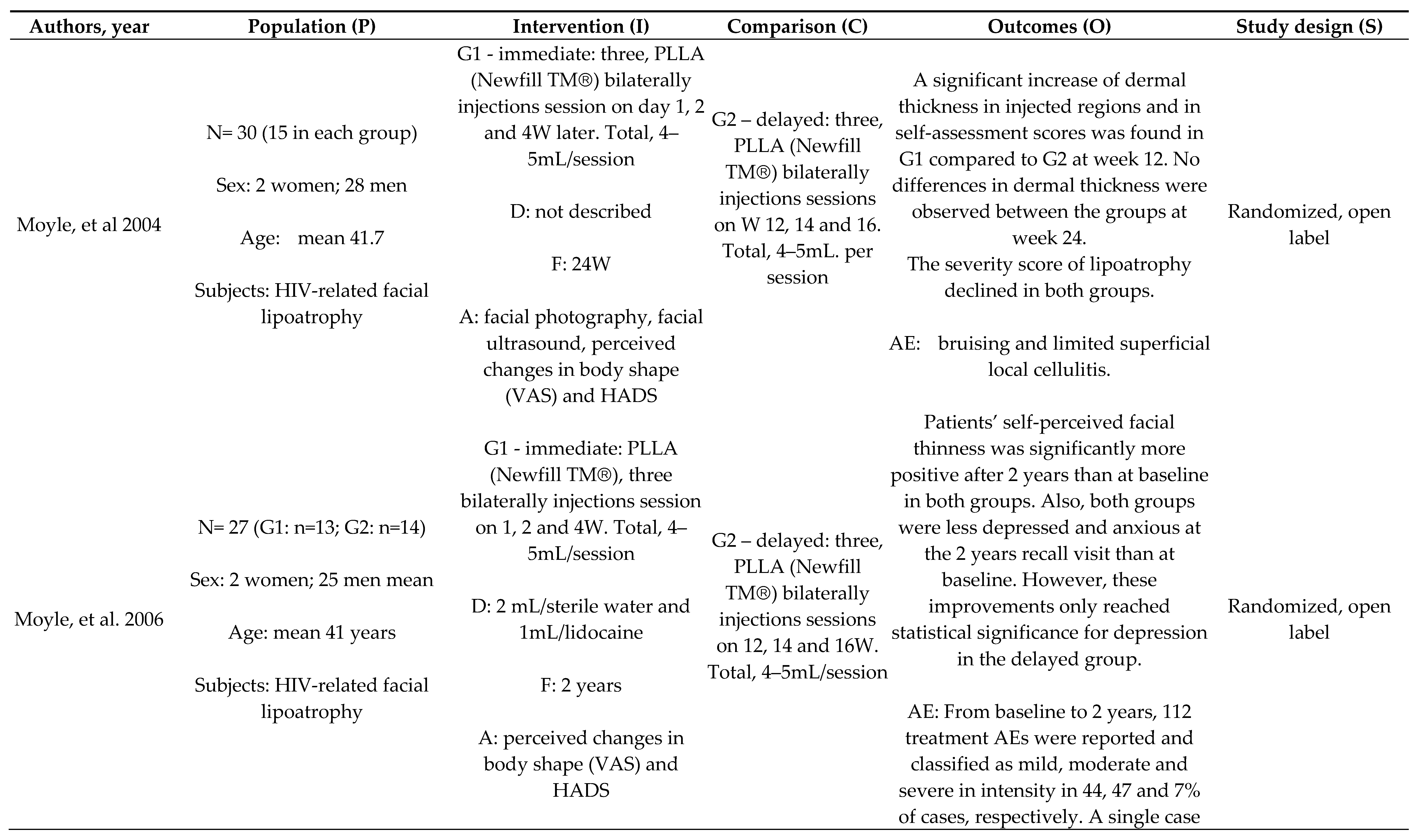
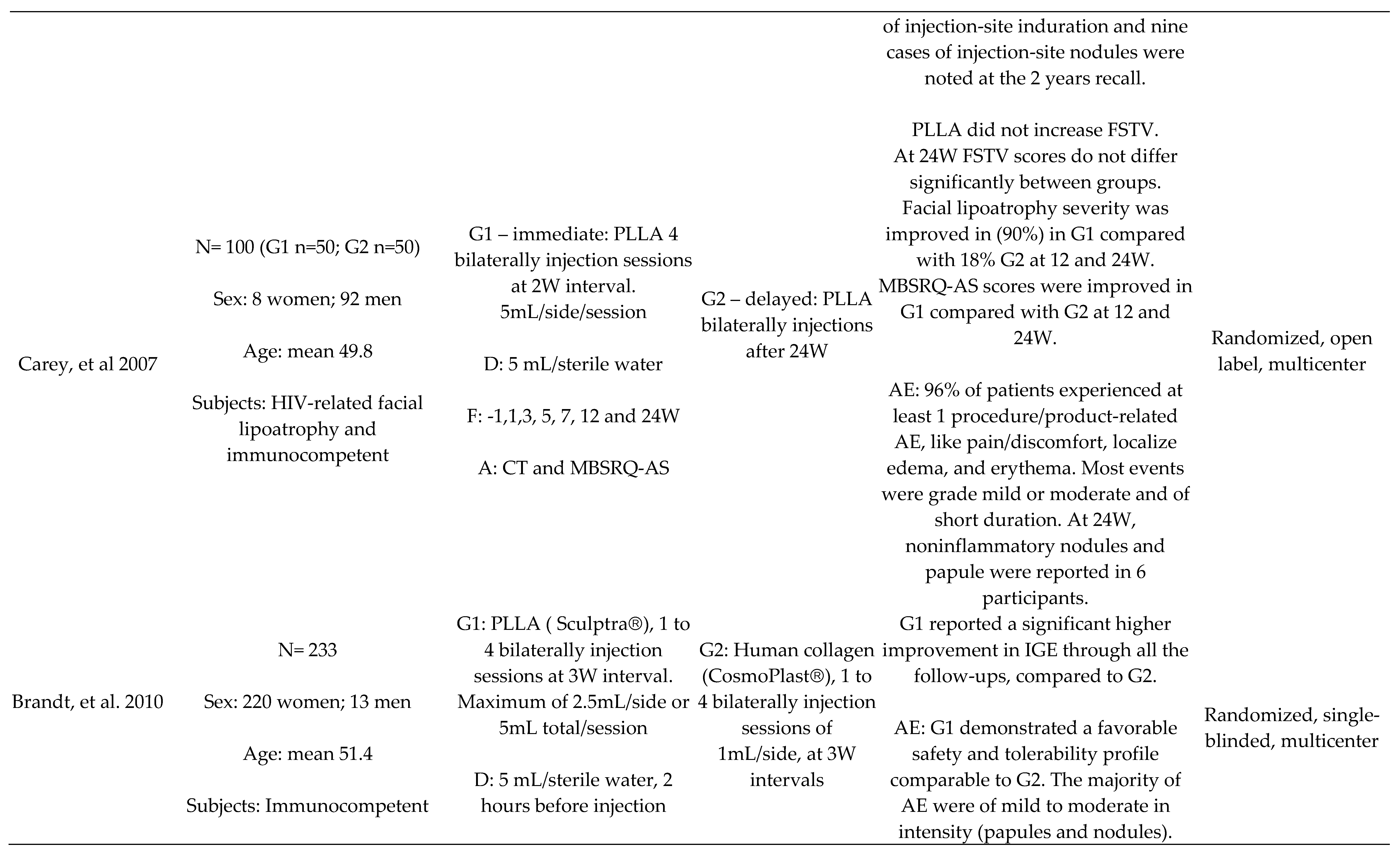
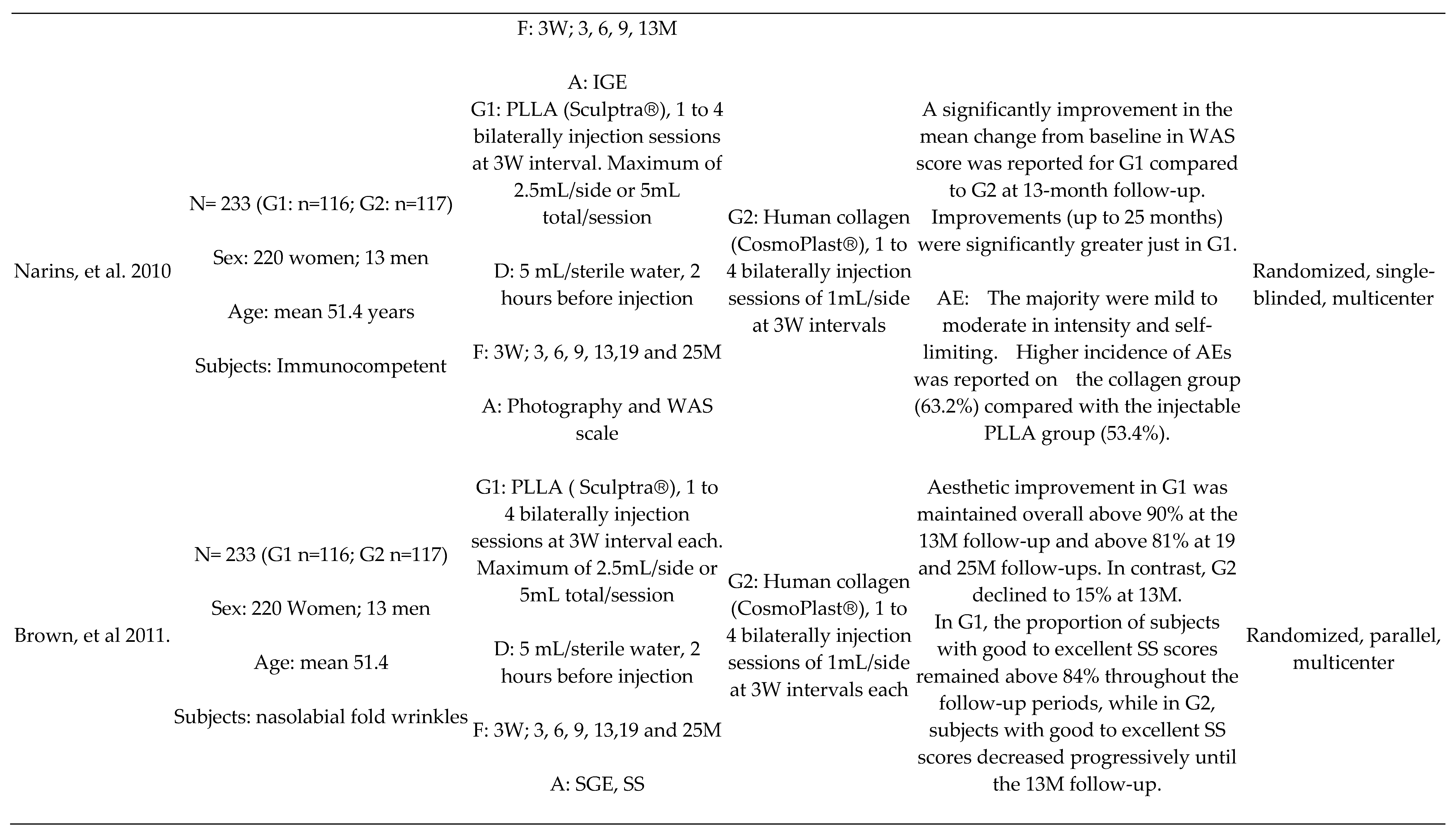
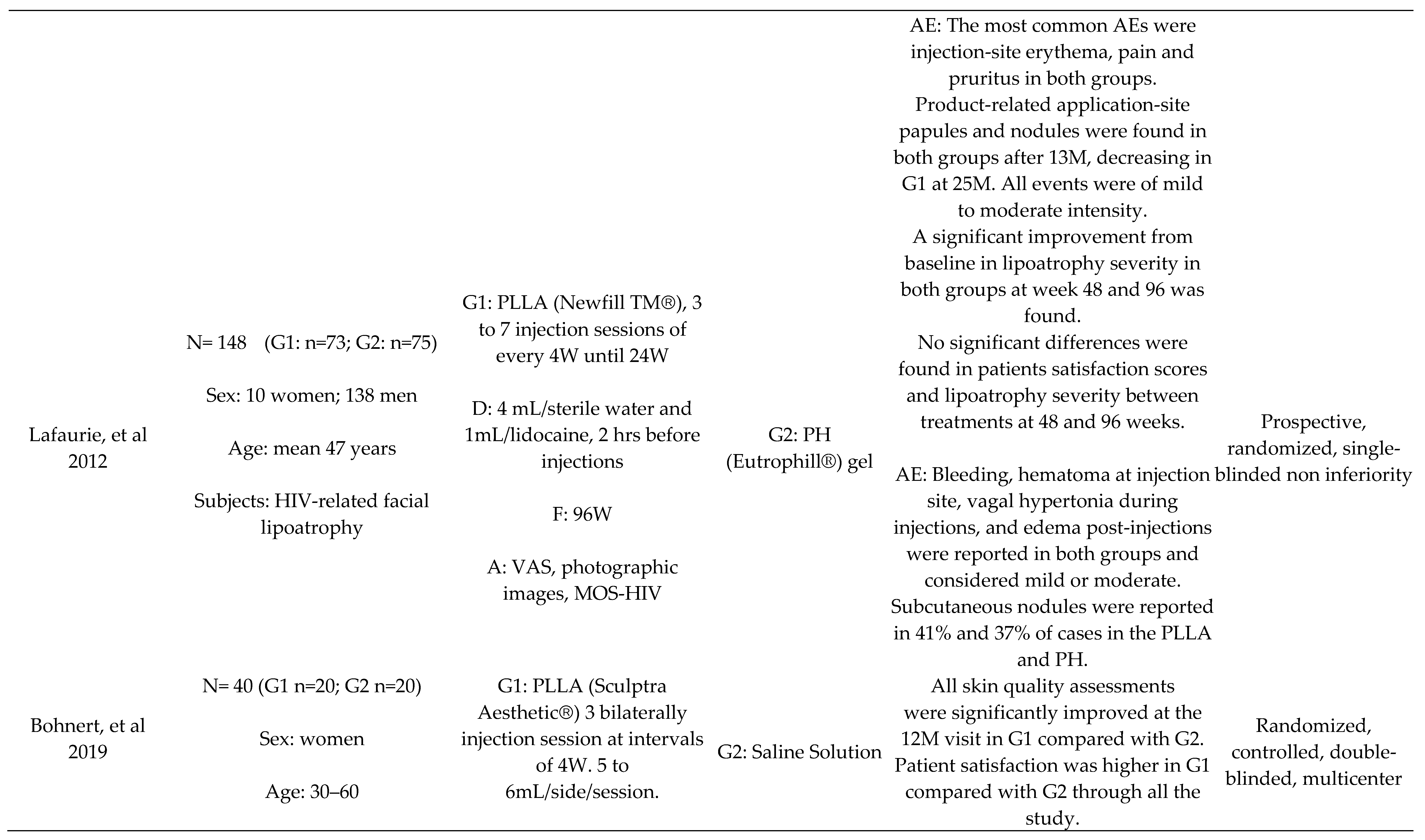
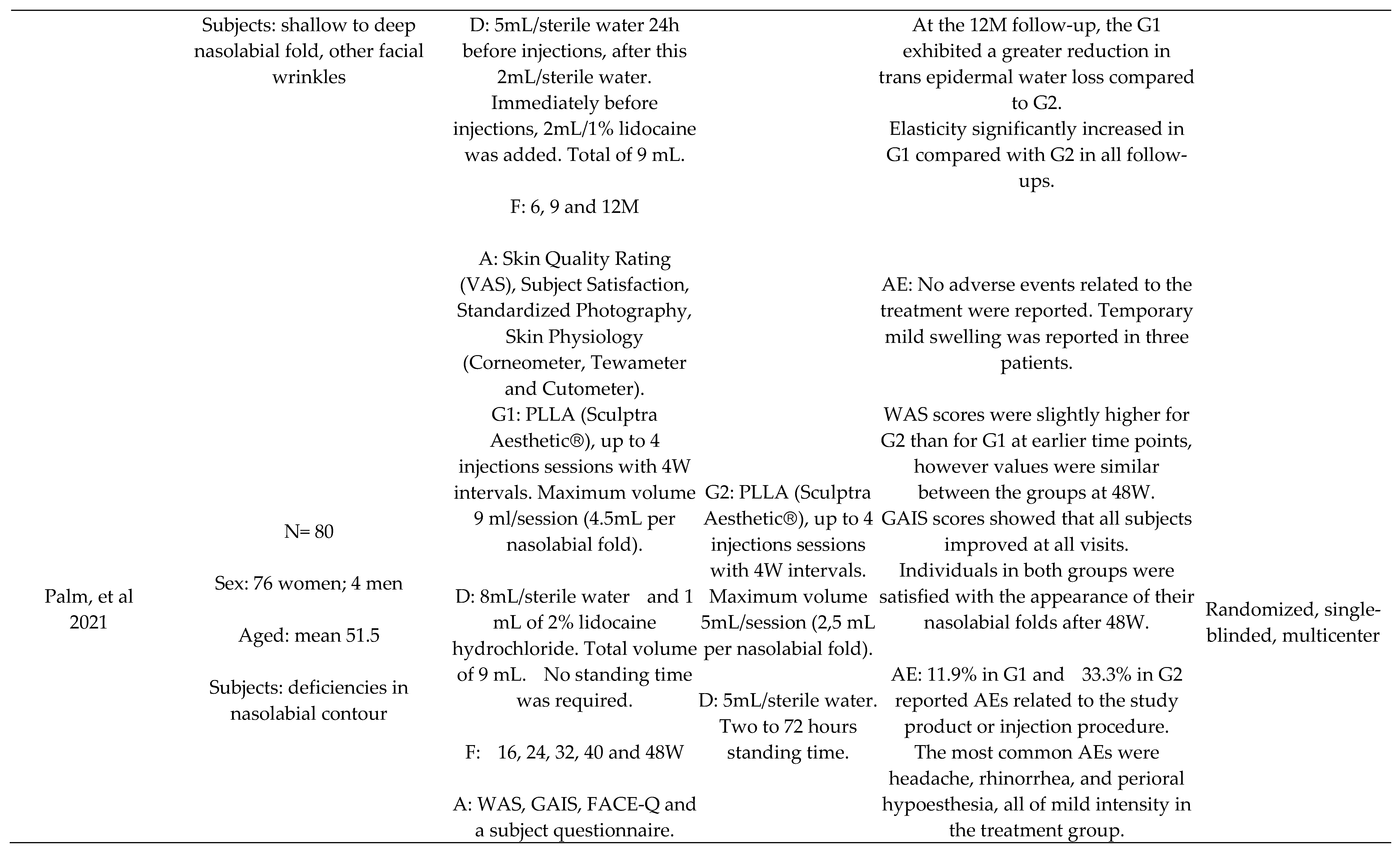
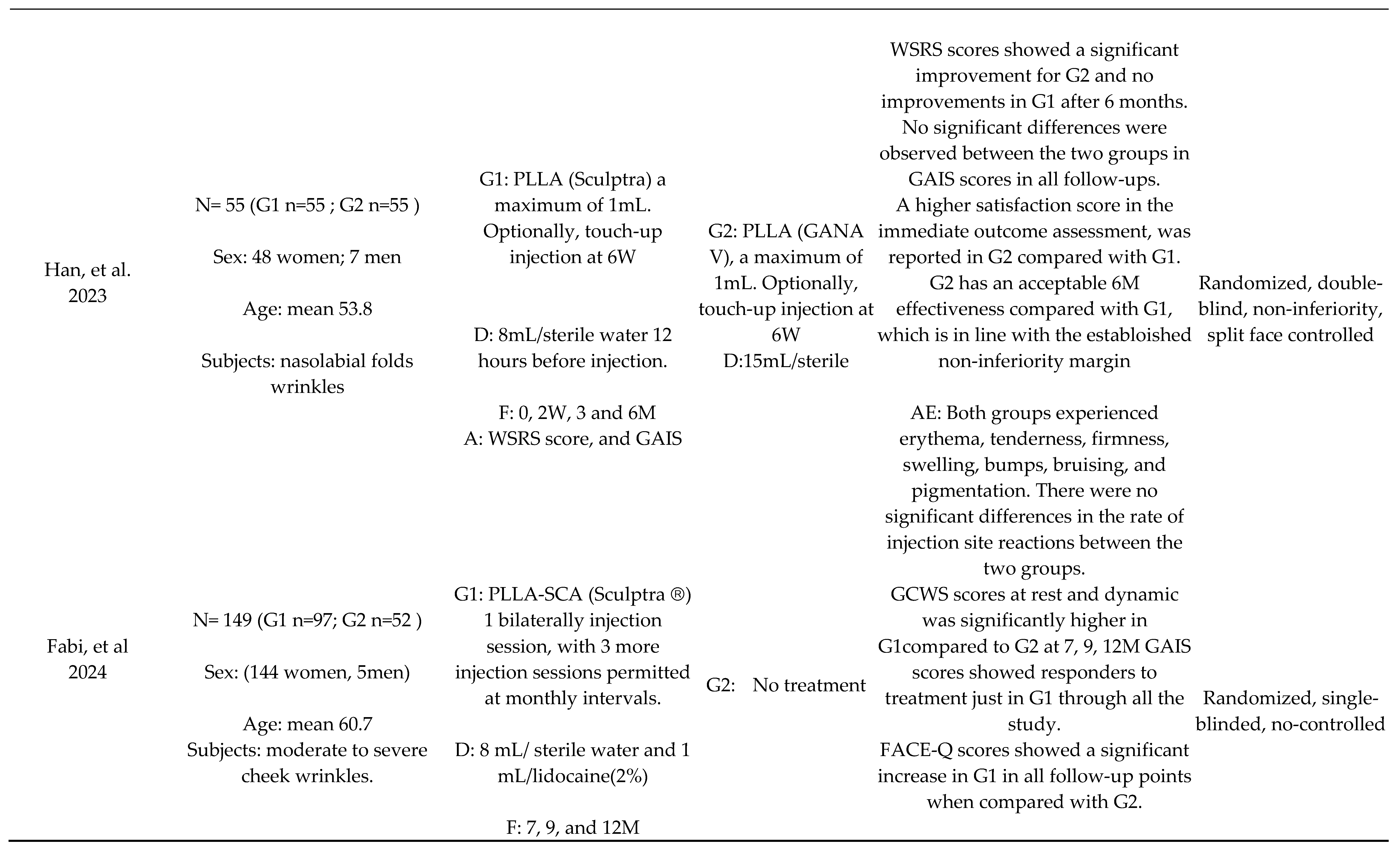

Table 2.
Table summarizing quality assessment and risk of bias.
| Author, year |
Randomization Process |
Deviations from Intended Interventions |
Missing Outcome Data |
Measurement of the Outcome |
Selection of the Reported Results | Overall |
|---|---|---|---|---|---|---|
| Moyle et al., 2004 | Some concerns | High risk | Low risk | Low risk | Some concerns | High risk |
| Moyle et al., 2006 | Some concerns | High risk | Some concerns | Some concerns | Some concerns | High risk |
| Carey et al., 2007 | Some concerns | High risk | Low risk | Low risk | Some concerns | High risk |
| Brandt et al., 2010 | Some concerns | Low risk | Some concerns | Some concerns | Some concerns | Some concerns |
| Narins et al., 2010 | Some concerns | Some concerns | Low risk | Low risk | Some concerns | Some concerns |
| Brown et al., 2011 | Low risk | Some concerns | Some concerns | Some concerns | Some concerns | Some concerns |
| Lafaurie et al., 2013 | Low risk | Some concerns | Some concerns | Some concerns | Some concerns | Some concerns |
| Bohnert et al., 2019 | Low risk | Low risk | Some concerns | Low risk | Some concerns | Some concerns |
| Palm et al., 2021 | Some concerns | High risk | Low risk | Low risk | Some concerns | High risk |
| Han et al., 2023 | Low risk | Low risk | Some concerns | Low risk | Some concerns | Some concerns |
| Fabi et al., 2024 | Some concerns | High risk | Low risk | Low risk | Some concerns | High risk |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



