
Submitted:
17 July 2024
Posted:
18 July 2024
You are already at the latest version
Abstract
Candida spp. is rarely found in the etiology of neonatal early-onset sepsis (EOS). However, candidemia is associated with increased mortality and morbidity, as in late-onset sepsis. Congenital candidiasis may present as mucocutaneous infection or, more rarely, as a systemic infection in term and preterm infants. Material and methods: Case reports of two cases of congenital systemic candidiasis (CSC) produced by Candida albicans and a review of the data in the literature. Results: Both neonates were male, born vaginally, with risk factors for congenital candidiasis. One of the infants was born at term and presented with an almost generalized maculopapular rash at birth; C. albicans grew in the blood culture sampled at 36 hours; parenteral fluconazole was started immediately, and no complications were noted. The other infant was born preterm, at 28 weeks of gestation, and presented signs of respiratory distress on the 4th day of life after initial successful treatment of the respiratory distress syndrome with surfactant and non-invasive respiratory support. C. albicans was present in the neonatal blood and gastric aspirate cultures, and in the maternal vaginal cultures (all sampled at birth); parenteral fluconazole therapy was administered for 30 days as investigations revealed both liver and renal involvement and the infant development bronchopulmonary dysplasia. Conclusion: As data in the literature suggests, despite occurring at any gestational age, CSC may present various clinical pictures, the rash may mimic many other neonatal conditions, and the systemic dissemination cannot be distinguished from bacterial EOS. Careful anamnesis and a high index of suspicion are important for the prompt recognition and treatment of CSC, optimizing the short- and long-term outcomes.
Keywords:
congenital systemic candidiasis
; candidemia
; Candida albicans
; congenital cutaneous candidiasis
; invasive candidiasis
; newborn
; neonate
; preterm infant
; fluconazole
1. Introduction
Neonatal sepsis is the third most common cause of neonatal death after prematurity and complications at birth [1]. Both early-onset sepsis (EOS) (occurring in the first 72 hours of life) and late-onset sepsis (LOS) (occurring after 72 hours after delivery) are associated with increased morbidity and mortality in neonates. The reported incidence of culture-proven neonatal EOS varies between 0.77-5/1000 live births [2,3,4,5,6]. Bacterial infections are the most common cause of neonatal EOS and LOS; however, despite playing a minor role in the etiology of neonatal sepsis, fungal infections may significantly impact neonatal morbidity and mortality.
Candida spp. represent the leading cause of invasive fungal infections in infants admitted to neonatal intensive units (NICUs). They are more commonly seen in LOS etiology than EOS (10-12% versus 2.4-4.6% [7,8,9]). Neonatal EOS produced by Candida spp., also referred to in the literature as congenital candidiasis, is rarely seen. Its incidence is unknown but most probably underestimated as the localized, cutaneous form is probably frequently mistaken with other neonatal dermatoses, and a recent meta-analysis found less than 50 reports of generalized systemic candidiasis published in the literature in more than 50 years [10] since the first report in 1958 [11]. C. albicans was isolated in blood, urine, and cerebrospinal fluid or identified by histological exams in various tissues or cultures sampled postmortem in most reported cases of congenital systemic candidiasis (CSC) [10,12]. The incidence of invasive Candida spp. infections was estimated at 5-10/100.000 live neonates [13,14,15]; an increased incidence of 5-15% is reported in very low birth weight infants (VLBW) as compared to 0.2-2% in the general population of infants admitted to NICU [16]. Despite its rarity, CSC is a critical condition occurring both in term and preterm infants, associated with increased morbidity and mortality if not recognized and treated in a timely manner [17]. Conversely, increased awareness and prompt initiation of antifungal treatment in suspected cases, pending confirmation of the etiology, is associated with improved outcomes.
We present two rare cases of congenital systemic candidiasis with C. albicans. The parents of the patients have given written consent for the publication of these case reports and associated images.
2. Case Reports
2.1. Case Report 1
The first case involves a full-term male newborn (39 gestational weeks) with a birth weight of 3600 g, a length of 52 cm, and a head circumference of 34 cm. The infant was delivered vaginally, in cranial presentation, and received an Apgar score of 10 at 1 minute in a Level I Maternity Hospital. The parents, both elementary school graduates, have no significant personal or family medical history and live in rural areas. The pregnancy progressed physiologically without any interventions; the mother did not undergo any treatments during her pregnancy. Approximately a week before delivery, the mother experienced leucorrhea and genital itching, untreated. The amniotic membrane ruptured during childbirth. The newborn is the fourth live birth of a mother with seven pregnancies. At birth, the infant presented diffuse, generalized erythematous maculopapular rash, including the palms and the soles, rare pustules; the buttocks, penis, scrotum, and perianal were spared and fewer lesions were noted on the posterior trunk and the extension surfaces of the legs (Figure 1). Investigations were started, and the infant was transferred to our hospital with a diagnosis of maternal-fetal infection with staphylococcus, suspected abdominal tumor (on abdominal ultrasound), and congenital heart defect (cardiac murmur on auscultation).
The infant was admitted to our NICU at 38 hours of life. Upon admission, the newborn presented in good general condition; the infant was breathing spontaneously, maintaining a peripheral oxygen saturation over 90% in room air, respiratory rate of 46/minute, heart rate of 145 beats/minute, cardiac murmur grade II/6 on the left parasternal area, normal urine output, transitional stools, mild facial jaundice, good sucking reflex, normal tone and reflexes, and persistence of the above described cutaneous rash.
Abdominal point of care ultrasound revealed mirrored abdominal organs suggesting incomplete abdominal situs inversus, confirmed by the thoracoabdominal radiography (Figure 2. A); no pathological changes in the abdominal parenchymal organs were noted, even on the repeated abdominal scan. The head ultrasound was normal; the echocardiography revealed the presence of a small patent ductus arteriosus, patent foramen ovale, and a right-sided aortic arch. Partial parenteral nutrition was initiated via the umbilical vein. Intravenous administration of antibiotics (Penicillin G and Amikacin) was initiated for three days as C-reactive protein decreased rapidly to normal values (from 19.4 mg/L), and the infant showed no other signs or symptoms of infection. The maternal vaginal culture upon admission yielded negative results (Table 1). However, C. albicans grew in the blood culture sampled at admission, and yeasts were seen with Gram stain on microscopy; systemic fluconazole treatment (6 mg/kg/day) was initiated in the 4th day of life (DOL) and continued for 21 days as the isolated strain of C. albicans showed sensitivity to this drug. Subsequent blood culture after 14 days yielded negative results, indicating treatment efficacy. No other peripheral cultures were positive – nasal, pharyngeal swabs, gastric aspirate - except the cultured tip of the umbilical line (in situ for two days), which was positive for the same Candida strain (Table 2). Candida isolate was sensitive to fluconazole, voriconazole, amphotericine B, flucytosine, caspofungin, and micafungin.
Concurrently, the patient's rash faded gradually by DOL 7, followed by fine, squamous desquamation, and ultimately resolved by 13th DOL (Table 1). The good general status, hemodynamic and respiratory stability, and efficient breastfeeding of the infant allowed the transfer, monitoring, and treatment of the infant in rooming-in from the 5thDOL. Repeated investigations during hospitalization did not reveal any involvement of other organ systems (Table 2). The infant was discharged after 24 days. Discharge recommendations encompassed scheduled follow-up and cardiologic monitoring to address the persistence of ductus arteriosus and patent foramen ovale. Up to the age of 2 years, no significant health problems were noted, and the growth and development of the child are within normal limits for the age.
2.2. Case Report 2
The second case pertains to a premature male newborn delivered at 28 weeks gestation, with a birth weight of 1250 g (25-50th percentile on the Fenton growth chart), length of 43 cm, and head circumference of 25 cm (50th centile). The infant was delivered vaginally in our level III maternity unit and received an Apgar score of 8 at 1 and 5 minutes (color and tone, each noted with 1 point). The parents, colledge graduates, have no significant personal or family medical history and live in a rural area. The pregnancy progressed normally until the premature rupture of membranes (PROM) occurred 136 hours prenatally when the mother, gestations IV, parity IV, was admitted for delivery. Under tocolysis with hexoprenaline, a complete prenatal corticosteroid course was administered therapy for fetal lung maturation; she also received intravenous ampicillin for five days in association with ceftriaxone for one day. A vaginal culture was sampled from the mother at admission was negative; another vaginal culture was sampled at birth (Table 1).
Immediately after birth, the preterm infant presented respiratory distress syndrome (tachypnea, 60 breaths/minute, grunting, intercostal retractions) and peripheral oxygen saturations of 75-80% in room air. Continuous positive airway pressure (Bubble CPAP) on the nasal cannula was used to support breathing, but the oxygen need increased gradually in the next 2 hours up to 40%, and non-invasive replacement therapy with surfactant (LISA) (200 mg/kg) was administered. According to the unit protocol, intravenous caffeine citrate (loading dose of 20 mg/kg), empiric antibiotic therapy (penicillin and amikacin), and parenteral nutrition were started. Immediately after surfactant administration, the oxygen need decreased to 21% in 24 hours, and normal blood and transcutaneous gases allowed a gradual decrease of the positive expiratory end pressure and complete weaning of the respiratory support after 72 hours. The initial thoracic radiography showed a reticular pattern and air bronchogram consistent with respiratory distress syndrome due to surfactant deficiency. The first investigations showed normal values of the C-reactive protein (Table 2); therefore, the antibiotic therapy was stopped after 48 hours.
However, on the 4th DOL, the preterm infant experienced several episodes of desaturation, increased respiratory effort, and tachypnea; free-flow oxygen supplementation at 0.6 L/min was used to increase the oxygen saturation. A rapid C-reactive protein test indicated elevated levels, and the gastric aspirate culture collected at birth was positive for C. albicans. Discussing with the mother the newborn’s condition, she revealed that she was already receiving antifungal treatment (fluconazole) due to the positive vaginal culture for C. albicans sampled at birth. Therefore, antifungal therapy was started with intravenous fluconazole (12 mg/kg) associated with intravenous antibiotic therapy with colistin and amikacin. The next day, the newborn's blood culture collected at birth also showed positive results, the fungi gram indicating sensitivity to fluconazole, voriconazole, amphotericin B, flucytosine, caspofungin, and micafungin. As the respiratory effort of the infant continued to increase in association with prolonged desaturations and a tendency to apnea, the Bubble CPAP support on the nasal cannula was reinitiated, with minimal settings and oxygen concentration, adjusted according to the blood and transcutaneous gases and functional respiratory syndrome. The thoracic radiography performed at this moment showed a slightly pronounced bilateral reticular, micronodular lung interstitium (Figure 2B). Intravenous antibiotic therapy was maintained for 12 days. The respiratory support was de-escalated to humidified heated high-flow nasal cannula (HHHFNC) on DOL 15, again adjusted according to blood gases and peripheral oxygen saturations. A follow-up blood culture after 7 days of antifungal treatment yielded again positive results. C. albicans also grew in the pharyngeal specimens and gastric aspirates sampled in the 4th DOL but not in the nasal swab culture sampled on the same day. Only the third blood culture, sampled 18 days after treatment initiation, yielded negative. At that moment, the gastric aspirate, pharyngeal, and nasal swab cultures were also negative (Table 2).
Abdominal ultrasound performed in the 9th DOL revealed hepatic involvement, characterized by generalized inflammatory changes – increased gross granular, hyperechoic patchy structure (Figure 3A), restricted after five days to the hepatic segment IV as a fine granular structure and altered echogenicity (Figure 3B,C), gradually fading towards a normal smooth hypoechoic structure at discharge. Concurrently, at that moment, blood tests indicated a transient mild increase in serum transaminases and renal markers (creatinine and urea), which were subsequently normalized by DOL 15. Fluconazole systemic therapy was maintained for 30 days. No other parenchymal sonographic changes were noted on the abdominal ultrasound. Head ultrasound was repeatedly normal for the age. Heart ultrasound scans demonstrated only a small persistent ductus arteriosus and persistent foramen ovale (Table 2).
The infant's respiratory status gradually improved, and she was switched to free low-flow oxygen by the 27th DOL and weaned off by DOL 41. In the context of prematurity, EOS with C. albicans, and respiratory support for more than 28 days, this was interpreted as mild bronchopulmonary dysplasia. The preterm infant was discharged recently at 58 DOL, corrected postmenstrual age of 36 weeks, healthy, hemodynamically stable, oxygen-independent, partially breastfed, weight 3020 g (25-50th centile, Fenton’s growth chart), cranial circumference 32 cm (50th centile), normal neurological exam, and recommendations for monitoring grade I retinopathy on the right eye and follow consultations up to the age of 2 years.

Table 1.
Maternal history, clinical characteristics, and clinical course of the two patients.
| Patient 1 | Patient 2 | |
| Gestational age | 39 weeks | 28 weeks |
| Birth weight | 3600 g | 1250 g |
| Maternal history | Vaginal discharge and genital itching one week before delivery | 132 hours of membrane rupture, intravenous ampicillin for 5 days, associated with ceftriaxone at birth |
| Maternal vaginal cultures | No pathogen growth at admission in our unit (2nd day after delivery) | No pathogen growth 5 days before delivery, C. albicans was isolated in cultures sampled at birth |
| Onset | At birth, with characteristic rash | The 4th day, respiratory distress syndrome |
| Antibiotic therapy (newborn) | Penicillin plus amikacin, 3 days after admission, intravenous | Penicillin plus amikacin, 2 days intravenous, empiric therapyColistin plus amikacin for 10 days, starting DOL1 5, intravenous |
| Clinical course | No other signs or symptoms suggestive of sepsis, rash entirely resolved by DOL1 13 | Re-initiated respiratory support (after initial treatment for respiratory distress syndrome due to surfactant deficiency with Bubble CPAP2 and surfactant), gradually decreased pressure and oxygen concentration, weaned on HHHFNC3 on DOL1 15, free low flow oxygen starting DOL1 27, oxygen-independent at DOL1 41 |
| Complications | None | Hepatic and renal involvementGrade I retinopathy of prematurity |
| Discharge | DOL1 24 | DOL1 58 |
| Follow up | Normal growth and development at the age of 2 | Recently discharged, follow-up scheduled |
Legend: 1DOL – day of life, 2CPAP – continuous positive airway pressure, 3 – humidified heated high-flow nasal cannula.
Table 2.
Laboratory and imaging investigations of the two patients.
| Patient 1 | Patient 2 | ||||||||||||
| 12 h | Day 1 | Day 3 | Day 12 | Day 17 | 12 h | Day 1 | Day 2 | Day 4 | Day 5 | Day 10 | Day 15 | Day 20 | |
| Blood count and differential | |||||||||||||
| Hemoglobin (g/dL) | 14 | 11.8 | 11.4 | 11,2 | - | 16.1 | 18.1 | 16.7 | 17.9 | 17.8 | 14.7 | 13.5 | 11.9 |
| Platelets (103/µL) | 434 | 412 | 389 | 354 | - | - | 374 | - | - | 331 | 356 | - | - |
| Leucocytes (/µL) | 17,440 | 14,430 | 11,280 | 9,760 | - | - | 23,300 | - | - | 21,240 | 15,050 | - | - |
| Neutrophils (/µL) | 10,580 | 7,540 | 6,820 | 5,730 | - | - | 15,090 | - | - | 14,350 | 9,030 | - | - |
| Bands (%) | - | 5 | 6 | 1 | - | - | 3.4 | - | - | 6.5 | 2 | - | - |
| I/T1 ratio | - | 0.09 | 0.09 | 0.017 | - | - | 0.05 | - | - | 0.088 | 0.032 | - | - |
| Monocytes (%) | 1.4 | 12 | 12.5 | 4.1 | - | - | 8.4 | - | - | 9.5 | 5 | - | - |
| Inflammatory markers | |||||||||||||
| C-RP2 (mg/L) | 19.38 | 8.3 | 7.4 | 1,6 | 3,1 | 2.1 | 1.3 | <1 | 41.4 | 36.6 | 14.3 | 12.5 | 2.9 |
| Biochemistry | |||||||||||||
| Blood glucose (mg/dL) | 63.1 | 74 | 85 | - | - | 59 | 77 | 57 | 123 | 49 | 87 | 89 | 78 |
| AST3 (U/L) | 38.4 | 34 | 29 | 27 | 15 | 29 | 29 | 114 | 107 | 87 | 20 | 27 | 28 |
| ALT4 (U/L) | 13.3 | 16 | 18 | 15 | 14 | <7 | <7 | 14 | 21 | 22 | 9 | 8 | 9 |
| Creatinine (mg/dL) | 1.01 | 0.61 | 0,52 | 0.54 | 0.45 | 0.52 | 0.85 | 0.97 | 1.15 | 1.25 | 0.91 | 0.75 | 0.54 |
| BUN5 (mg/dL) | 30.5 | 12 | 13 | 15 | 24 | 24 | 63 | 83 | 79 | 74 | 37 | 26 | 19 |
| Total bilirubin (mg/dL) | 3.4 | 4.3 | 5.5 | 1.2 | 0.17 | 2.3 | 4.6 | 6.8 | 6.9 | 6.9 | 1.7 | - | - |
| Conjugated bilirubin (mg/dL) | 0.24 | 0.31 | 0,35 | - | - | 0.28 | 0.31 | 0.26 | 0.35 | 0.33 | 0.6 | - | - |
| Blood gases and electrolytes | |||||||||||||
| Blood gases (arterial) | - | Normal | Normal | - | - | Normal | Normal | Normal | Normal | Normal | Normal | Normal | Normal |
| Electrolytes | - | Normal | - | - | Normal | Normal | Normal | Normal | Normal | Normal | Normal | Normal | |
| Imaging | |||||||||||||
| Thoraco-abdominal radiography | No lung or abdominal involvement | Suggestive of respiratory distress syndrome due to surfactant deficiency on DOL6 0; pronounced reticular, micronodular bilateral lung interstitium on DOL6 5 | |||||||||||
| Abdominal ultrasound | Suspected neuroblastoma on DOL6 1; abdominal situs inversus on DOL6 2; no abdominal parenchymal involvement on DOL6 2 and 10 | Gross, inhomogenous, patchy echogenic areas disseminated, almost throughout the entire liver on DOL6 9; fine granular echogenic areas limited to the fourth hepatic segment by DOL6 14; normal hepatic ultrasound structure on DOL6 45 | |||||||||||
| Head ultrasound | Normal at admission and on follow up | Normal for the gestational or corrected age at DOL6 3, 7, and at discharge | |||||||||||
| Doppler echocardiography | Small PDA7, PFO8, right-sided aortic arch (DOL6 1) | Small PDA7, PFO8 on DOL6 4 and 14 | |||||||||||
| Microbiology | |||||||||||||
| Blood culture | Positive for C. albicans at admission, no growth at 14 days | Positive for C. albicans on DOL6 0 and 11, negative on DOL6 18 | |||||||||||
| Nasal swab culture | No pathogen identified | No pathogen identified on DOL6 4 and 18 | |||||||||||
| Gastric aspirate | No pathogen identified | C. albicans isolated on DOL6 0, and 4, no pathogen growth on DOL6 18 | |||||||||||
| Pharyngeal culture | No pathogen identified | C. albicans isolated on DOL6 4, no pathogen growth on DOL6 18 | |||||||||||
| Umbilical line tip culture | C. albicans (in situ for 2 days) | C. albicans (in situ for 5 days) | |||||||||||
Legend: 1I/T – immature to total neutrophils ratio; 2C-RP – C-reactive pprotein; 3AST – aspartate aminotransferase; 4ALT – alanine aminotransferase; 5BUN – blood urea nitrogen; 6DOL – day of life; 7PDA – persistent ductus arteriosus; 8PFO – persistent foramen ovale.
3. Discussion
3.1. General Aspects - Epidemiology, Etiology
Neonatal sepsis is a critical condition associated with increased morbidity and mortality if not recognized and correctly treated in a timely manner. Although more frequently reported as an etiologic agent in neonatal sepsis, fungal infections are rarely identified in neonatal EOS [12,16,18,19,20,21,22,23,24,25]. Neonatal fungal infections represent a challenge for clinicians due to their unique epidemiological aspects in the neonatal period, unspecific and variable clinical presentation, limited performance of the diagnostic tools, limited pharmacological data of antifungal therapies, increasing fungal resistance to drugs, and increased morbidity and mortality [18,26]. Most of the reported cases occur as LOS, associated with prematurity, low birth weight, and NICU hospitalization [7,21,27,28]. Candida spp. are responsible for most neonatal fungal sepsis [12,17,18,21]. According to data in the literature, the incidence of neonatal EOS produced by Candida spp. varies between 2.4-4.6% compared to the incidence of 10-12% reported for neonatal LOS caused by Candida spp. [7,[7–9].
Two types of EOS or congenital candidiasis are described: a) localized, also called congenital cutaneous candidiasis (CCC), and b) generalized, also described as congenital systemic candidiasis (CSC) (or invasive candidiasis), defined by positive blood, or urine, or cerebrospinal fluid culture for Candida spp. or isolation of fungus in histopathological or cultures sampled au autopsy [10,12]. As for any other neonatal EOS, there is no consensus as regards defining early fungal sepsis; some authors refer to the occurrence of sepsis in the first 72 hours of life [4,6,18,29], some use an extended frame of 7 days [25,30,31]. According to Gudjónsdottir et al. [6], defining neonatal sepsis as occurring after 72 hours of life as EOS would not be appropriate as the etiology changes significantly as, for example, all cases with Group B Streptococcus, one of the main etiological agents producing EOS [4,6], are diagnosed before in the first 72 hours of life. Most of the sepsis cases occurring after 72 hours of life are more probably associated with vascular access and invasive procedures performed in the NICU.
C. albicans is recognized most often as a causal agent in fungal neonatal EOS [10,16,27,32,33,34,35,36,37], although CCC produced by C. parapsilosis [33,38.39], C. glabrata [40], C. Kefyr [41], and C. tropicalis [42] are also signaled in the literature [12,30,43]. Multiple risk factors for congenital candidiasis were reported, including prematurity, prolonged rupture of membranes, Candida vaginosis, and chorioamnionitis being the most frequent [10,12,22,28,35,36,37,41,43,44,45,46,47,48,49,50]. In preterm infants, the risk of congenital candidiasis increases as the gestational age and birth weight decrease [22,43,44]. A report from Canada [12] identifies an increased risk for congenital candidiasis in preterm infants < 25 weeks and birth weight <750 g. Increased permeability of the immature epidermis, immature defense to fungal invasion (antimicrobial peptides, phagocytosis, oxygen reactive species and inflammatory mediators synthesis, complex cellular signaling systems), reduced opsonization and complement function, and immunoglobulin deficiency are increasing the risk for congenital candidiasis and for invasive candidiasis [16,50,51,52,53]. On the other side, Candida’s adherence and slow growth facilitate its ability to colonize and disseminate in the blood and tissues even before clinical signs occur [16]. Even though most of the described cases of congenital candidiasis are associated with prolonged rupture of membranes, there are reports of neonatal Candida infection without amniotic membrane rupture prior to delivery [13]. C. albicans can penetrate the amniotic sac without evident membrane rupture [13,20,41,44,54], and the fetal infection can even develop without signs of vaginitis [55]. Also, many of the reported cases occurred in infants born vaginally but also in association with cesarean section delivery [7,13,36,56].
Candida spp. are, in general, opportunistic, commensal fungi on the skin and reproductive and gastrointestinal tract. However, some Candida spp., including C. albicans and C. parapsilosis, may produce candidiasis, increasing the risk of complications in pregnancy [45,47,48,54,57,58,59]. Up to 40-50% of the pregnant women are colonized with Candida spp. [12,45,60], 13-20% of them presenting Candida vaginitis [46,48,61,62], C. albicans accounting for 90% of the cases [47]. According to Disha et al. [47], three types of factors increase the risk of Candida vaginitis in pregnancy: a) factors related to pregnancy – weakened immune system, high levels of estrogens and progesterone, low vaginal pH, decreased cellular-mediated immunity, increased glycogen content of the vaginal tissue; b) clinical factors – diabetes, HIV infection, prior Candida infections; c) behavioral factors – antibiotic or contraceptive use, intrauterine devices, synthetic and tight clothes, deficient personal hygiene, inappropriate feeding, stress. In these conditions, Candida may take advantage of the abnormal vaginal microbiome, microscopic breaches of the mucosa, or immune defense to invade the amniotic membrane and uterine cavity [10,20,48]. Despite the high incidence of fungal and Candida vaginitis, chorioamnionitis occurs rarely and the fetal and neonatal infection even more infrequently [10,35,36,37,46,48,50], usually limited to chorion and umbilical cord [10]. Intrauterine infection development is rare, with fewer than 100 reported cases of congenital candidiasis associated with Candida [54]. However, the risk of neonatal congenital candidiasis increases in the rare event of systemic maternal fungal infection [41].
The presence of intrauterine devices [10,20,35,36,37,41,43,44,45,49,63], cerclage [20,49], obstetrical procedures as assisted reproductive techniques [46], amniocentesis [10,20], embrioreduction [43] or chorionic villous sampling [48], invasive maneuvers at birth [44] were also associated with an increased risk of congenital candidiasis of the offspring. Prior maternal antibiotic treatment, therapies producing an imbalance of the maternal vaginal microbiome (specifically destroying Lactobacillus spp.), glucocorticosteroids, oral contraceptives, hormonal substitution treatments, immunosuppressive conditions, maternal diabetes are also cited in the literature in association with neonatal congenital candidiasis [10,37,48,49,52,56,64,65]. A genetic predisposition was also cited as a risk factor for Candida infection during pregnancy [37,52,56]. Also, an increased incidence of congenital candidiasis in male infants was reported [66,67], possibly due to a gene on chromosome X involved either in thymus functioning or immunoglobulin synthesis, as proposed by Prinsloo et al. [68].
Neonatal EOS produced by Candida spp. is reported both in term and preterm infants, although the incidence is greater in preterm infants [10,49,50,67,69]. Despite the localized nature of CCC, experts are warning about its potential risk of dissemination, especially in preterm infants [13,20,35,70], favored by a more immature epidermal barrier [49,51] and immature innate and adaptative responses to pathogens [16,50,51,52]. The increased risk for invasive and extensive neonatal congenital candidiasis is linked to epidermal and immune system immaturity in preterm infants, low birth weight, pathogen virulence, magnitude of the inoculum, and invasive procedures [10,35,50,51,71].
We presented 2 male infants with CCC admitted in our unit in the last two years, yielding an incidence of 0.31/1000 live newborns admitted in the maternity ward (2/6513 live births) and 2.89/1000 NICU admissions (2/691) betwee 2022-2024, higher compared to data in the literature - 0.1% [16]. A recent meta-analysis reported a significantly higher occurrence of neonatal candidemia in preterm infants (79.55%) compared to full-term neonates (9.09%) [10]. Both infants were delivered vaginally, patient 1 with amniotic membranes ruptured at birth, and patient 2 after 132 hours of spontaneously prolonged preterm rupture of membranes. A history of vaginal discharge and itching was found in the mother of patient 1, but no fungi grew in her vaginal cultures; the mother of the second patient had no history suggestive of vaginitis, and her vaginal culture sampled five days before birth was negative for fungi. However, another vaginal culture sampled at birth was positive for C. albicans. A recent history of broad-spectrum antibiotic treatment and prophylactic dexamethasone for fetal lung maturation may have been associated with Candida transmission from the mother to the fetus in the second case presented above. It has been shown that a longer duration of membrane rupture increases the risk of CSC [54], and this, along with prematurity and low birth weight, was found in association with patient 2. Both mothers lived in rural areas, in larger families, with limited access to health care. None of them reported significant health problems nor any obstetrical evaluation during pregnancy. We presume that the low educational, social, and economic status of these families may have affected the outcome of the pregnancies.
3.2. Physiopathology
Congenital infection with C. albicans is rarely acquired horizontally by hematogenous spread of Candida spp. from maternal circulation to the fetus through placenta [10,16,20,34,37,41,43,46,48,52,72,73,74,75,76]; this pathway is universally associated with invasive visceral involvement, mainly affecting the liver [10,77] but any organ can be invaded – kidneys, spleen, brain – due to the immaturity of the neonatal immune responses [10,51]. A retrograde hematogenous seeding from the peritoneal cavity through the fallopian tubes was also described [48]. More frequently, C. albicans reaches the fetus using the ascending route and penetrates through the amniotic membranes into the amniotic fluid; inflammatory processes of the membranes, placenta, and umbilical cord occur as a result [10,11,20,34,37,43,44,48,50,78,52,77]. The rupture of the amniotic membranes, the presence of intrauterine devices or any foreign body in the uterus, and diagnostic or therapeutic obstetrical procedures are associated with the ascending route of transmission in congenital candidiasis [46,48,73,74,75]. Inhalation or ingestion of the infected amniotic fluid is proposed as a pathogenic mechanism for lung and gastrointestinal involvement in congenital candidiasis [10]. After vertical transmission, C. albicans often colonizes the neonatal skin and mucous membranes. Prompt and adequate immune innate responses may prevent the excessive spreading of the fungus and subsequent infection of the newborn [79]. It can explain why congenital candidiasis usually presents as CCC in term infants while preterm infants have an increased risk for invasive, disseminated disease, even if presenting initially as CCC [50,51]. The presence of filamentous forms of C. albicans (hyphae, pseudohyphae, germ tubes) is associated with fungal virulence, and other experts are associating this characteristic with the increased severity of congenital candidiasis in preterm infants [16].
The ascending transmission route seems more plausible in our patient 1; penetration of C. albicans through intact amniotic membranes, favored by maternal vaginosis symptoms reported the week before delivery, was already reported in association with congenital candidiasis [11]. In the second case, ascending access to chorion, placenta, amniotic fluid, umbilical cord, and the fetus was favored by prolonged rupture of membranes, treatment with broad-spectrum antibiotics and dexamethasone, all risk factors for fungal infection; also, the vaginal culture sampled at birth was positive for C. albicans. Still, the hepatic and renal involvement in patient 2 cannot exclude the horizontal transmission; prematurity and umbilical line placement could also contribute to the hematogenous spread of C. albicans.
3.3. Clinical Aspects
Recognition of congenital candidiasis is a challenge irrespective of the clinical type, cutaneous or systemic, as the cutaneous rash may present differently from one patient to another, and CSC presents, like most neonatal EOS, with unspecific signs and symptoms [22,34,36,50].
Congenital cutaneous candidiasis rarely occurs [19,20,22,23]; its incidence is estimated at 0.1% of infants admitted to NICUs [13]. The cutaneous involvement is often apparent at birth or occurs in the first days of life [13,44], no later than the sixth DOL [10,80]. In a series of CCC cases, Kaufman et al. [13] reported that the rash occurred in the first DOL in 71% of the patients at a median age of 0 days (0-6). The eruption varies and may be diffuse erythematous, maculopapular, sometimes associating vesicles, bullae, or pustules, and is localized on the face, trunk, extension surfaces of the extremities, and intertriginous, often on the palms and soles [10,13,24,35,36,44,50,70,72,81,82,83]. The rash evolves in days with cutaneous desquamation, and different eruption stages can be seen simultaneously [22,70,72,82]; the genital area and oral mucosa are usually not affected in CCC [81]. Keratin degradation, scaling, hyperkeratosis, parakeratosis, spongiosis, and vesiculation were demonstrated in an in vitro model of CCC in 72 hours [84], another possible pathway for C. albicans dissemination. Rarely does CCC associate onychia and paronychia. Burn-like dermatitis has been reported, usually in preterm infants, and is associated with invasive fungal disease [44,81,85]. Mucocutaneous candidiasis is reported both in term and preterm infants; it most often has a benign, auto-limited course in term infants [10,44,81], resolving in 5 to 20 days [44], but is associated with risk of dissemination in preterm infants, especially the profound epidermal lesions, as burn-like dermatitis [70,81,86]. Recognition of CCC may be difficult as the rash may mimic various dermatologic conditions presenting in the neonatal period [13,37,72]. Still, prompt recognition of CCC is important as delayed treatment is associated with increased rates of dissemination and death [13,72].
Congenital systemic candidiasis is even less often seen compared to CCC [10], especially in term infants [49], associated with a high mortality rate of 39-94% if untreated [10,72,87,88]. Various clinical manifestations were reported in association with CSC, but the disease often presents with signs of respiratory distress due to lung involvement [10,19,27,38,81,89] and gastrointestinal manifestations [10,27,90]. Presentation similar to neonatal bacterial EOS was also reported with candidemia [34,50]. Pneumonia, cardiovascular, renal, liver, and ocular involvement were reported in EOS cases with C. albicans in extremely low birth weight infants in a study from Canada [12,34]. Meningitis, brain abscesses, septic shock, intrauterine and perinatal death were also reported in CSC [10,41,91,92]. The liver and spleen are affected in 1-3%of the cases of candidemia [8,50,93]. Most of the cases diagnosed with hepatic abscess due to Candida spp. were identified in preterm infants with LOS with Candida spp. in association with broad-spectrum antibiotherapy, umbilical vein catheterization, and prolonged parenteral nutrition [94]. Early diagnosis of CSC is, therefore, a real challenge as CSC may occur in the absence of risk factors, has an unspecific clinical picture, with a plethora of clinical signs, and sometimes the eruption is absent [10,12,34,50]; CSC severity also varies, from subacute, indolent course to severe disease, with cardiorespiratory and multiple organ failure [50].
According to data in the literature, the first of our patients, born at term, presented the typical rash in terms of onset (at birth), lesions (maculopapular, erythematous, rare pustule), extension and localization (almost generalized, with rare lesions on the buttocks, flexion face of the extremities, palms and soles, sparing the oral mucosa and genital and perianal areas), course (fading, in days, with furfuraceous desquamation), and resolution. No other involvement was found in this patient. Conversely, the preterm infant, patient 2, had no cutaneous eruption and presented in the 4th DOL with respiratory distress, desaturations imposing reinstitution of the respiratory support and oxygen therapy. Investigations also revealed hepatic and renal involvement due to delayed recognition of the infection. Prematurity, respiratory distress syndrome due to surfactant deficiency, and normal initially C-reactive protein values had an important contribution in delaying CSC diagnosis.
3.4. Diagnosis
The first step in recognizing and diagnosing congenital candidiasis is a high index of suspicion in the presence of the risk factors [20,95] and in cases suspected of neonatal sepsis with an unsatisfactory clinical course despite adequate therapeutic approach [89]. Also, even though most neonatal EOS cases are produced by Group B Streptococcus and Escherichia Coli infections, clinicians must be continuously aware that EOS may also be due to viruses, fungi, and parasites [4,6,18,50]. Therefore, when congenital candidiasis is suspected at birth, a meticulous examination of the placenta and the umbilical cord is mandatory. In the case of Candida spp. infection, yellow-white or red small nodules may be spotted on the umbilical cord (funisitis); on microscopic examination, these lesions are small subchorionic microabscesses with fungi and pseudohyphae [10,48,96]. Similarly, pseudohyphae, microabscesses, and/or granulomas may be found in the placenta [13,22,36,97]. Laboratory tests and imaging are helpful but have limited performance in diagnosing congenital candidiasis [24].
Due to its increased specificity, blood culture is recognized as the gold standard for diagnosing invasive candidiasis and CSC [10,12,16,22,28,34,35,50], although its sensitivity is limited [34,98,99,100,101]. Blood cultures may also take time; with rapid tests, the results come in around 48-72 hours [16,35,102], while classic methods may take 5-7 days for fungal growth [100,101,102]. At least 1 mL of neonatal blood is required to reduce the rate of false negative results [8,34,100,101,102,103]. Failure to identify pathogens in the blood culture may also be associated with reduced pathogen inoculum, prior antibacterial and antifungal therapy, and viral or parasitic infections, and does not exclude infection in the presence of signs and symptoms suggestive of infection [103]. Experts are also warning that a positive blood culture for Candida should not be casually dismissed as a contaminant but instead recognized as indicative of a potentially more profound systemic infection [101,104]. Modern technologies based on real-time polymerase chain reaction (PCR), such as multiplex PCR assays using a panel of Candida spp., may improve Candida spp. identification and offer a more rapid result [34,103,105,106]. Studies are limited, panfungal tests are not yet standardized, do not offer information on fungal sensitivity, and, despite high sensitivity and negative predictive value, specificity and positive predictive value are unsatisfactory [34,35]). Also, a sensitivity of 90% and specificity of 93% were reported for molecular tests in diagnosing neonatal sepsis [107]. However, studies report a high contamination rate and a potential risk of errors in interpreting the results [103]. Metagenomic sequencing allows simultaneous sequencing of billions of nucleic acid fragments in the same time and rapid identification of bacteria, viruses, and fungi without distinction between pathogens and commensals; data is limited in neonates, and these tests take time and are expensive [34,108].
Urine cultures may also be helpful for Candida spp. identification; cerebrospinal fluid cultures are indicated in the presence of signs of neurological infection [22,35,43,50]. A high suspicion of maternal Candida vaginitis or chorioamnionitis should prompt culture from maternal vagina, placenta, amniotic fluid, and sampling nasopharyngeal, gastric aspirates, cutaneous lesions in the newborn [13,22,40,41,43,44,50] as their results may help in early recognition of congenital candidiasis. Microscopic evaluation of the cutaneous lesions (e.g., Gram stain) may confirm fungal presence; potassium hydroxide preparations should be avoided if, for sampling, scraping the skin is necessary [13]. A complete laboratory evaluation is recommended if blood culture yields positive results for Candida, searching for systemic involvement. Term newborns with mucocutaneous infection must also be evaluated thoroughly if there are concerns regarding other systemic infectious diseases [50].
1,3-β-D-glucan test (BDG) was proposed as an alternative diagnostic tool in congenital candidiasis. BDG is a constituent part of the cellular membranes of multiple fungi; this polysaccharide can be detected in serum only in invasive fungal infections [34,109]. The cut-off values of BDG are not yet established in neonates [26,110]; the test can be used for treatment monitoring as it has an acceptable sensitivity (89%) but low specificity (60%) [34]. Better diagnostic accuracy may be achieved by combining BDG with clinical and imaging aspects and other laboratory data [16,109]. Serum mannan (an abundant constituent of the Candida cellular wall – acting as antigen) or anti-mannan (antibodies) levels have minimal sensitivity and specificity of Candida spp. prevalence is low but may improve diagnostic accuracy in combination with blood culture [34].
Blood count and differential parameters have a limited value for congenital candidiasis diagnosis. Leukocytosis has often been reported in CSC [22,23,25,27,34,44,72,81,111]. Extreme leukemoid reactions associated with hyperglycemia and burn-like dermatitis were reported in 3 cases of CSC, all asymptomatic in the first 24 hours of life by Pradeepkumar et al. [25]. Leukemoid reaction and increased number of immature neutrophils were found primarily on disseminated congenital candidiasis, associated with respiratory distress [22,112]. Thrombocytopenia was also found in association with CSC [16,27,34,35], but similarly to neonatal, bacterial sepsis cannot be considered a specific sign of sepsis [34,90,113]. Other authors also reported persistent hyperglycemia [22,25,34,41]. Recently, Ratridewi et al. [114] proposed a cut-off value of >5% monocytes as indicative of Candida spp. infection in preterm infants based on the important role played by monocytes in Candida invasion prevention.
Imaging – thorax, abdomen x-rays, abdominal and head ultrasound, Doppler echocardiography – are helpful in the identification of fungal dissemination within lungs, liver, spleen, kidneys, cardiovascular system, and brain [16,41,44,50,93]. Other biochemical investigations may help clarify the extension of Candida infection: aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase, bilirubin, triglycerides, gamma-glutamyl transferase (assessing liver function), creatinine, blood urea nitrogen (renal function), electrolytes, inflammatory markers (most often use is C-reactive protein) [16,50].
Differential diagnosis of CCC and CSC rash (if present) comprises various neonatal cutaneous eruptions (toxic allergic erythema, milium, miliaria, transient neonatal pustular melanosis) or systemic conditions associated with rashes (neonatal EOS with Listeria monocytogenes, impetigo, cutaneous/systemic staphylococcal infections, congenital varicella, herpes virus congenital infection, epidermolysis bullosa, Langerhans cell histiocytosis) or toxic cutaneous reactions generated by drugs [10,13,22,23,63].
Laboratory tests, imaging, and the uneventful course suggested limited cutaneous infection with C. albicans in the term infant (patient 1) with positive blood culture at birth. All peripheral cultures sampled proved negative for C. albicans. C-reactive protein value decreased rapidly with empiric antibiotic therapy (penicillin and amikacin for three days). No abnormalities were seen on his blood count and differential except an increased number of monocytes (12-12.5%) in the first two DOLs. Based on the maternal pregnancy and delivery history and tests, clinical aspects, imaging, and laboratory results, the patient was diagnosed with CSC with no other organ involvement except the skin. Patient 2, born preterm, cumulated two positive blood cultures for C. albicans (DOL 0 and 11), positive cultures from the gastric aspirate (DOL 0 and 4), pharynx (DOL 4), maternal vagina (day of birth), all indicating CSC. Persistent positive blood cultures were mentioned in the literature in most newborns presenting with candidemia [8,115]. Delayed clinical onset of CSC (DOL 4) was suggestive of lung involvement and associated with leukocytosis, monocytosis (DOL 1 and 4), hyperglycemia (DOL 4), increased AST (DOL 2-5), and creatinine (DOL 3-5). The abdominal ultrasound performed on the 9th day evidenced the hepatic involvement. All the data gathered on this patient suggested CSC with hepatic and renal dissemination. The initial respiratory distress was attributed to surfactant deficiency associated with prematurity, as it quickly resolved with surfactant therapy and non-invasive respiratory support.
3.5. Treatment
Prompt initiation of antifungal therapy is associated with increased rates of survival in CSC [10,25,76]. There is no consensus as regards the best management in CCC. Some authors suggest conservative treatment in all newborns presenting CCC and good general condition and recommend antifungal therapy in those with altered general condition [22,44,49,81] while continuing evaluation for neonatal sepsis [81]. Continuous monitoring of well-appearing newborns with CCC without any sign of systemic infection and topical or oral antifungal therapy is advised by Salusti-Simpson et al. [49]. In order to prevent Candida dissemination, others suggest systemic antifungal treatment for more than 14 days initiated at the rash onset [13,24,43,72,95]. Systemic antifungal treatment is also recommended in infants with CCC associated with signs of respiratory distress, clinical or laboratory aspects suggestive of EOS, birth weight <1500 g, broad-spectrum antibiotic therapy, extensive instrumentation at birth, weak immune system [10,22,44,49], in VLBW infants, and the presence of burn-like dermatitis lesions [13,22,31,49].
A more considerable consensus exists regarding empiric systemic antifungal treatment when clinicians suspect Candida spp. infections in newborns at risk or with clinical signs of neonatal sepsis associated with recent thrombocytopenia or more than 50% reduction of the platelet count, gestational age <26 weeks, or birth weight <750 g [16,43,72].
All authors agree that systemic antifungal therapy must be urgently administered if candidemia is present [10,16,17,25,26,34,43,44,72,76] as the moment when specific antifungal therapy is initiated has been proved crucial for the infants' outcome [43]. Three classes of antifungal drugs are available and have been used to treat neonatal candidiasis: a) polyenes; b) echinocandins (caspofungin, micafungin); and c) azoles (fluconazole, itraconazole, voriconazole, posaconazole), each with various limitations in the treatment of invasive fungal infections [16,17]. Nephrotoxicity may limit polyenes usage; the limited antifungal spectrum and high costs limit echinocandis use [17]. Most authors recommend amphotericin B or fluconazole as first-line antifungal treatment [10,17,26,27,34,36,43,46,49,72,116,117,118,119].
Amphotericin B, a polyene-producing pores in the fungal cell membrane due to interaction with ergosterol, may be used as amphotericin B deoxycholate (5 mg/kg) or liposomal amphotericin B (1 mg/kg) [34,44]; it is excreted in urine, but its use in urinary tract infections with Candida spp. is limited due to nephrotoxicity. Parenteral infusions are frequently associated with reactions and hypokalemia [17,34,120]. Amphotericin B can be used in Candida spp. infections resistant to fluconazole and to prevent resistance to fluconazole [121]. 5-flucytosine has been recommended as a second-line therapy in Candida spp. in infections not responding to amphotericin B [116].
Fluconazole acts as a fungistatic by inhibiting the CYP450 enzyme and, consequently, ergosterol synthesis [34]. Fluconazole (6-12 mg/kg) has an impressive safety profile, is efficient, especially on C. albicans (some authors even recommend fluconazole as the first line treatment in C. albicans candidemia [36]), can be used parenterally but also has an excellent enteral absorption of 90% [13,122], and has an accessible cost [16,17,123]. Its use is limited by the increased risk of tolerance and association with persistent candidemia [124,125], increased resistance of Candida isolates, and recurrence risk [123,124]. Fluconazole has a limited efficiency against C. glabrata [46] and C. parapsilosis [27]. Both amphotericin B and fluconazole have good penetrance into the cerebrospinal fluid, being recommended in central nervous system fungal infections [34,36] as compared to caspofungin and micafungin, echinocandins with reduced penetrance in the cerebrospinal fluid and urine [16,117,118]. Caspofungin has been used in neonates with refractory and invasive fungal infections, but data in newborns is still limited [10,55,80].
Supportive treatment is mandatory, according to the symptoms of each newborn with CCC; respiratory support and oxygen therapy must be used for those presenting with lung involvement; cardio-vascular support if the infection is disseminated to the heart and blood vessels; antibiotic therapy, if necessary must be tailored to pathogen resistance; careful monitoring of the liver and renal function and electrolytes may impose changes of the fluids, nutrition, and electrolytes intake, mainly if hepatic or renal involvement is associated; monitoring for signs of antifungal toxicity is also important. Repeated blood cultures and fungigrams may help identify Candida isolates resistant to the administered antifungal drug. In preterm infants, reducing or stopping humidification is advised if they are cared for in incubators with humidity [13]. Topical antifungal therapy has been used and is recommended in cases evolving with CCC, usually nystatin or clotrimazole [13,44,81].
Parenteral fluconazole was immediately instituted once C. albicans infection was suspected and successfully used to treat CSC in both our patients without any side effects; fluconazole course was prolonged (30 days) due to multiple organ involvement (lung, liver, kidneys), persistent candidemia after eight days of antifungal treatment, and prolonged need of respiratory support and oxygen-dependency, as development of mild bronchopulmonary dysplasia was attributed to CSC. According to the study published by Benjamin et al. [126], 10% of the neonates 320 infants in the study had multiple positive blood cultures and candidemia for more than 14 days.
3.6. Clinical Course and Complications
Dissemination of CCC, more frequently seen in preterm infants, is associated with septicemia, meningitis, bronchopneumonia, arthritis, endocarditis, and increased mortality [10,13,25,30,55,76]. In 2017, Kaufman et al. [13] reported a dissemination rate of CCC of 66% in preterm infants weighing <1000 g associated with a mortality rate of 40%; dissemination rate was appreciated at 33% in preterm infants with a birth weight between 1000 and 2500 g and their mortality rate was 14%; in infants weighing over 2500 g at birth dissemination rate dropped to 11% while the fatality rate decreased to 3.8%, underlying the need for systemic antifungal therapy of CCC in infants at risk for invasive fungal infections. Worse outcomes are cited for CSC with multiorgan involvement [20,23,44]. A meta-analysis on CSC published in 2020 reported mortality rates as high as 39 to 94%, higher in developing countries, associated with lower gestational age and birth weight and clinical onset at birth, especially with early-onset respiratory distress [10]. Although results may vary according to the level of intensive care, mortality in C. albicans infections is increased compared to C. parapsilosis and other non-C. albicans sepsis (approximately 40% versus 15%) [16].
Like bacterial neonatal EOS, fungal EOS may be associated with increased hospitalization costs and poorer developmental outcomes, especially in preterm infants – increased risk for cerebral palsy, blindness, and deafness [16,34,127].
Both our patients had a favorable short-term outcome; the first patient was monitored for two years, had no significant health problems, and was appropriate for age growth and development at the age of 2 years. Prematurity, multiorgan involvement, and persistent candidemia may have contributed to bronchopulmonary dysplasia in patient 2; long-term follow-up was scheduled for this infant, too, but the good clinical status and growth and resolution of all organ involvement up to discharge at 36 weeks corrected age is encouraging regarding a good long-term prognosis.
3.7. Prevention
Recognizing the important contribution of maternal Candida spp. colonization and vaginitis, and the important impact of congenital candidiasis on neonatal morbidity and mortality, some have implemented screening programs for prenatal fungi detection [37]. Also, maternal prenatal treatment in the last trimester of pregnancy, even in asymptomatic colonization, has substantially reduced Candida transmission from the mother to the offspring and oral and genital candidosis in neonates [128,129].
4. Study Limitations
We are aware of the limitations of our study, as it is based on the report of two cases and a review of the most important information in the literature. Congenital cutaneous candidiasis is a rare neonatal EOS infection, and the systemic form occurs even more rarely but is associated with severe outcomes if it is not promptly recognized and treated. In presenting our cases, we focused more on the practical management of the patients. For the first patient, an infant, all the data is presented in this paper. As for the preterm infant, a very low birth weight infant, we have chosen to present only the clinical and paraclinical information relevant for the first month of life, as the rest of the hospitalization period was uneventful, and the prolonged hospital stay was due to prematurity and bronchopulmonary dysplasia. Regarding the investigations performed in both cases, we followed the unit protocol for neonatal sepsis and used the limited resources of our laboratory. According to our protocol, lumbar puncture is performed only if clinical signs and symptoms or head ultrasound suggest central nervous system involvement. If blood culture is positive, serial head ultrasounds are performed at least every 3-5 days, more often if needed, at the clinician's discretion. Additionally, our protocols limit blood sampling for tests in well-appearing infants unless a condition is highly suspected. Unfortunately, our laboratory cannot perform BDG, measurements of serum mannan or anti-mannan levels, modern rapid molecular tests for pathogen identification or any genomic sequencing; if needed, the parents must cover the costs. All these practical shortcomings are reasons to present our experience with these two recent cases. In searching the literature to adopt the most appropriate management, we realized the rarity of this condition, with only 43 cases found in the meta-analysis published four years ago, and no more than two additional cases since then [27,72], totaling less than 50 cases since 1958 when the first case of congenital systemic candidiasis [11] was published. We acknowledge that our review was not systematic, but we gathered the most relevant information for every day clinical practice.
5. Conclusions
We presented two cases of C. albicans CSC, both with some particularities. The full-term infant presented with CSC (confirmed by a positive blood culture sampled in the first DOL); investigations diagnosis was prompted by the occurrence of the characteristic rash at birth, suspected neuroblastoma, and congenital heart defect; successful treatment with fluconazole was achieved, and both the short- and long-term outcome was favorable.
In the case of the preterm infant, CSC diagnosis was slightly delayed by the presentation at birth with respiratory distress syndrome attributed to surfactant deficiency due to prematurity, quickly resolved by surfactant therapy, non-invasive respiratory support, and oxygen therapy, normal C-reactive protein values in the first two days of life, initially negative maternal vaginal culture, and delayed result of the infant's blood culture sampled at birth. Most probably, all these circumstances have favored C. albicans dissemination to the liver and kidney, with minimal clinical impact on the infant's condition; however, lung tissue infection most probably contributed to bronchopulmonary dysplasia development. A longer systemic fluconazole therapy was deemed due to the persistent presence of C. albicans in the blood. A favorable short-term outcome was achieved as the infant was discharged after an uneventful course, growing and developing within normal limits at 36 weeks of corrected age. Interestingly, both infants presented monocytosis at the time of the clinical onset of CSC. Machine learning or artificial intelligence may help evaluate the integration of the monocyte count into a diagnostic algorithm for congenital candidiasis.
The review of the literature and our recent experience with the reported cases allows us to support some important observations expressed by other authors: 1) a high index of suspicion in the presence of risk factors for congenital candidiasis is important for early recognition, prompt and appropriate antifungal treatment and outcome optimization; 2) CCC are rare events and CSC even less; even if in well-appearing term infants CCC has a benign, auto-limited course, there are multiple circumstances in which CCC can disseminate, leading to invasive fungal infection with multiorgan imvolvement and high mortality rate; such cases must be considered for systemic antifungal treatment; 3) variable and unspecific clinical aspects are challenging the clinical recognition of congenital candidiasis; 4) multiple limitations are associated with routine tests used for neonatal candidiasis; negative blood culture – the gold standard test for neonatal sepsis - does not exclude candidemia; rapid, newer tests and technologies may help rapid diagnosis but in the presence of prenatal risk factors, placenta, amniotic membranes and umbilical cord examination may offer a clue for diagnosis; 5) both amphotericine B and fluconazole are effective in CCC and CSC treatment but long-term therapy is needed, increasing the hospitalization costs. However, a standardized approach is needed to diagnose and manage congenital candidiasis, a rare disease posing an increased burden of morbidity and mortality on patients and their families, clinicians, and healthcare systems [12,13,22,23,43,72,88].
Supplementary Materials
The original contributions and all relevant data regarding the cases presented in the study are included in the article; further inquiries can be directed to the corresponding author.
Author Contributions
Conceptualization, M.L.O., M.C., D.A.Te., R.C.C., D.A.To. and L.S.; methodology, M.L.O., M.C., D.P., D.A.Te., R.C.C. and D.A.To.; software, D.P., E.D.C., R.G. and L.S.; validation, M.L.O., L.S., M.C., R.G., D.P. and A.G.B.; formal analysis, M.L.O., M.C., R.C., A.G.B., R.C.C. and D.A.To.; investigation, D.A.Te., R.C.C., D.A.To., I.M., D.P. and E.D.C.; resources, E.D.C., A.G.B. and R.G..; data curation, M.L.O.; writing—M.L.O., D.A.Te., R.C.C., D.A.To., M.C. and R.C.; original draft preparation, M.L.O., D.A.Te., R.C.C., D.A.To., M.C. and I.M.; writing—M.L.O., R.C., A.G.B. and L.S., review and editing, M.L.O., D.A.Te. and M.C.; visualization, R.C., A.G.B. and D.P.; supervision, M.L.O., M.C. and R.G.; project administration, M.L.O. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
All relevant data regarding the cases presented in the study are included in the article; further inquiries can be directed to the corresponding author. Restrictions may apply due to institutional policies.
Acknowledgments
The authors express their gratitude to the patient’s parents for granting consent to publish the two case reports.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Liu, L.; Johnson, H.L; Cousens, S.; Perin, J.; Scott, S.; Lawn, J.E.; Rudan, I.; Campbell, H.; Cibulskis, R.; Li, M.: Mathers, C.; Black, R.E.; Child Health Epidemiology Reference Group of WHO and UNICEF. Global, regional, and national causes of child mortality: An updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379(9832):2151-61. [CrossRef]
- Odabasi, I.O.; Bulbul, A. Neonatal Sepsis. Sisli Etfal Hastan Tip Bul. 2020;54(2):142-158. [CrossRef]
- Cohen-Wolkowiez, M.; Moran, C.; Benjamin, D.K.; Cotten, C.M.; Clark, R.H.; Benjamin, D.K. Jr; Smith, P.B. Early and late onset sepsis in late preterm infants. Pediatr Infect Dis J. 2009;28(12):1052-6. [CrossRef]
- Stoll, B.J.; Hansen, N.I.; Sánchez, P.J.; Faix, R.G.; Poindexter, B.B.; Van Meurs, K.P.; Bizzarro, M.J.; Goldberg, R.N.; Frantz, I.D. 3rd; Hale, E.C.; Shankaran, S.; Kennedy, K.; Carlo, W.A.; Watterberg, K.L.; Bell, E.F.; Walsh, M.C.; Schibler, K.; Laptook, A.R.; Shane, A.L.; Schrag, S.J.; Das, A.; Higgins, R.D.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Early onset neonatal sepsis: The burden of group B Streptococcal and E. coli disease continues. Pediatrics. 2011;127(5):817-26. [CrossRef]
- Turhan, E.E.; Gürsoy, T.; Ovalı, F. Factors which affect mortality in neonatal sepsis. Turk Pediatri Ars. 2015;50(3):170-5. [CrossRef]
- Johansson Gudjónsdóttir, M.; Elfvin, A.; Hentz, E.; Adlerberth, I.; Tessin, I.; Trollfors, B. Changes in incidence and etiology of early-onset neonatal infections 1997-2017 - a retrospective cohort study in western Sweden. BMC Pediatr. 2019;19(1):490. [CrossRef]
- Pfaller, M.A.; Diekema, D.J. Epidemiology of invasive candidiasis: A persistent public health problem. Clin Microbiol Rev. 2007;20(1):133-63. [CrossRef]
- Benjamin, D.K. Jr.; Stoll, B.J.; Gantz, M.G.; Walsh, M.C.; Sánchez, P.J.; Das, A.; Shankaran, S.; Higgins, R.D.; Auten, K.J.; Miller, N.A.; Walsh, T.J.; Laptook, A.R.; Carlo, W.A.; Kennedy, K.A.; Finer, N.N.; Duar,a S.; Schibler, K.; Chapman, R.L.; Van Meurs, K.P.; Frantz, I.D. 3rd.; Phelps, D.L.; Poindexter, B.B.; Bell, E.F.; O'Shea, T.M.; Watterberg, K.L.; Goldberg, R.N.; Eunice Kennedy Shriver National Institute of Child Health and Human Development Neonatal Research Network. Neonatal candidiasis: Epidemiology, risk factors, and clinical judgment. Pediatrics. 2010;126(4):e865-73. [CrossRef]
- Al-Taiar, A.; Hammoud, M.S.; Thalib, L.; Isaacs, D. Pattern and etiology of culture-proven early-onset neonatal sepsis: A five-year prospective study. Int J Infect Dis. 2011;15(9):e631-4. [CrossRef]
- Georgescu, T.A.; Lisievici, A.C.; Munteanu, O.; Furtunescu, F.L.; Bratu, O.G.; Berceanu, C.; Bohîlţea, R.E. Congenital systemic candidiasis: A comprehensive literature review and meta-analysis of 44 cases. Rom J Morphol Embryol. 2020;61(3):673-680. [CrossRef]
- Benirschke, K.; Raphael, S.I. Candida albicans infection of the amniotic sac. Am J Obstet Gynecol. 1958;75(1):200-2. [CrossRef]
- Barton, M.; Shen, A.; O'Brien, K.; Robinson, J.L.; Davies, H.D.; Simpson, K.; Asztalos, E.; Langley, J.; Le Saux, N.; Sauve, R.; Synnes, A.; Tan, B.; de Repentigny, L.; Rubin, E.; Hui, C.; Kovacs, L.; Yau, Y.C.; Richardson, S.E; Paediatric Investigators Collaborative Network on Infections in Canada (PICNIC). Early-Onset Invasive Candidiasis in Extremely Low Birth Weight Infants: Perinatal Acquisition Predicts Poor Outcome. Clin Infect Dis. 2017;64(7):921-927. [CrossRef]
- Kaufman, D.A. Challenging issues in neonatal candidiasis. Curr Med Res Opin. 2010;26(7):1769-78. [CrossRef]
- Chitnis, A.S.; Magill, S.S.; Edwards, J.R.; Chiller, T.M.; Fridkin, S.K.; Lessa, F.C.; Trends in Candida central line-associated bloodstream infections among NICUs, 1999-2009. Pediatrics. 2012;130(1):e46-52. [CrossRef]
- Kaufman, D.A. "Getting to Zero": Preventing invasive Candida infections and eliminating infection-related mortality and morbidity in extremely preterm infants. Early Hum Dev. 2012;88 Suppl 2:S45-9. [CrossRef]
- Kaufman, D.A; Springe,r SC. Fungal Infections in Preterm Infants. https://emedicine.medscape.com/article/980487-overview?st=fpf&scode=msp&socialSite=google&form=fpf&icd=login_success_gg_mismatch_fpf, Updated: Dec 27, 2020; accessed on 10 July 2024.
- Feng, Y.; Lu, H.; Whiteway, M.; Jiang, Y. Understanding fluconazole tolerance in Candida albicans: Implications for effective treatment of candidiasis and combating invasive fungal infections. J Glob Antimicrob Resist. 2023;35:314-321. [CrossRef]
- Năstase, L., Rădulescu, L., Luminos, M.L., Merisescu, M.M., Jugulete, G., Stoicescu, S.M., Severe Modifications of Biological Markers in Late Neonatal Sepsis in a Very Low Birth Weight Due to Candida lusitaniae, Rev. Chim., 2019, 70(2): 393-397. Corpus ID: 214480005. [CrossRef]
- Nouri-Merchaoui, S.; Mahdhaoui, N.; Fekih, M.; Adouani, M.; Zakhama, R.; Methlouthi, J.; Ghith, A.; Seboui, H. Candidose congénitale systémique, forme rare de candidose néonatale : À propos d'une observation chez un nouveau-né prématuré [Systemic congenital candidiasis, a rare condition in neonates: Case report in a premature infant]. Arch Pediatr. 2011;18(3):303-7. French. [CrossRef]
- Fernández-Ruiz, M.; Mosqueda-Peña, R.; Pérez-Ayala, A.; Blázquez-Gamero, D. Congenital cutaneous candidiasis associated with maternal peripartum candidemia. Rev Iberoam Micol. 2020;37(2):68-71. [CrossRef]
- Hammoud, M.S.; Al-Taiar, A.; Fouad, M.; Raina, A.; Khan, Z. Persistent candidemia in neonatal care units: Risk factors and clinical significance. Int J Infect Dis. 2013;17(8):e624-8. [CrossRef]
- Wang, S.M.; Hsu, C.H.; Chang, J.H. Congenital candidiasis. Pediatr Neonatol. 2008;49(3):94-6. [CrossRef]
- Aruna, C.; Seetharam, K. Congenital candidiasis. Indian Dermatol Online J. 2014;5(Suppl 1):S44-7. [CrossRef]
- Shope, C.; Ritter, A.; Karlin, S.; Lee, L.W.; Cotton, C.H. Congenital Cutaneous Candidiasis in Preterm Infants. Neoreviews. 2023;24(3):e175-e180. [CrossRef]
- Pradeepkumar, V.K.; Rajadurai, V.S.; Tan, K.W. Congenital candidiasis: Varied presentations. J Perinatol. 1998;18(4):311-6. PMID: 9730205. [PubMed]
- Ferreras-Antolín, L.; Sharland, M.; Warri,s A. Management of Invasive Fungal Disease in Neonates and Children. Pediatr Infect Dis J. 2019;38(6S Suppl 1):S2-S6. [CrossRef]
- Sanni, U.A.; Lawal, T.O.; Na'uzo, A.M.; Audu, L.I. Invasive Fungal Infection Presenting as Early-Onset Neonatal Sepsis: A Case Report from Northern Nigeria. Journal of Clinical Neonatology. 2023; 12(1):p 38-41. [CrossRef]
- Jung, Y.J. Early- and late-onset candidemia in very low birth weight infants in the Korean neonatal network, 2013-2017. Pediatr Neonatol. 2024;S1875-9572(24)00084-6. [CrossRef]
- Shane, A.L.; Sánchez, P.J.; Stoll, B.J. Neonatal sepsis. Lancet. 2017;390(10104):1770-1780. [CrossRef]
- Melville, C.; Kempley, S.; Graham, J.; Berry, C.L. Early onset systemic Candida infection in extremely preterm neonates. Eur J Pediatr. 1996;155(10):904-6. [CrossRef]
- Aldana-Valenzuela, C.; Morales-Marquec, M.; Castellanos-Martínez, J.; Deanda-Gómez, M. Congenital candidiasis: A rare and unpredictable disease. J Perinatol. 2005;25(10):680-2. [CrossRef]
- Sousa. R.A.; Martins Oliveira Diniz, L.; Lapa Marinho, F.E.; Gonçalves Rezende, L.; Machado Carelos, E.; de castro Romanelli R.M. Risk factors for candidemia in neonates: Systematic review and meta-analysis Journal of Neonatal Nursing. 2022; 28:83–92. [CrossRef]
- Trofa, D.; Gácser, A.; Nosanchuk, J.D. Candida parapsilosis, an emerging fungal pathogen. Clin Microbiol Rev. 2008;21(4):606-25. [CrossRef]
- Daniel, K.; Greenberg, R.G.; Boutzoukas, A.; Katakam, L. Updated Perspectives on the Diagnosis and Management of Neonatal Invasive Candidiasis. Research and Reports in Neonatology. 2023;13:45-63. [CrossRef]
- Weimer, K.E.D.; Smith, P.B.; Puia-Dumitrescu, M.; Aleem, S. Invasive fungal infections in neonates: A review. Pediatr Res. 2022;91(2):404-412. [CrossRef]
- Simonsen, K.A.; Anderson-Berry, A.L.; Delair, S.F.; Davies, H.D. Early-onset neonatal sepsis. Clin Microbiol Rev. 2014;27(1):21-47. [CrossRef]
- Messina, A.; Mariani, A.; Brandolisio, R.; Tavella, E.; Germano, C.; Lipari, G.; Leo, L.; Masturzo, B.; Manzoni, P. Candidiasis in Pregnancy: Relevant Aspects of the Pathology for the Mother and the Fetus and Therapeutic Strategies. Trop Med Infect Dis. 2024;9(5):114. [CrossRef]
- Waguespack-LaBiche, J., Chen, S.H.; Yen. A. Disseminated congenital candidiasis in a premature infant. Arch Dermatol. 1999;135(5):510-2. [CrossRef]
- Krallis, N.; Tzioras, S.; Giapros, V.; Leveidiotou, S.; Paschopoulos, M.; Stefanou, D.; Andronikou, S. Congenital candidiasis caused by different Candida species in a dizygotic pregnancy. Pediatr Infect Dis J. 2006;25(10):958-9. [CrossRef]
- Arai, H.; Goto, R.; Matsuda, T.; Saito, S.; Hirano, H.; Sanada, H.; Sato, A.; Takada, G. Case of congenital infection with Candida glabrata in one infant in a set of twins. Pediatr Int. 2002;44(4):449-50. [CrossRef]
- Pineda, C.; Kaushik, A.; Kest, H.; Wickes, B.; Zauk, A. Maternal sepsis, chorioamnionitis, and congenital Candida kefyr infection in premature twins. Pediatr Infect Dis J. 2012;31(3):320-2. [CrossRef]
- Nichols, A.; Khong, T.Y.; Crowther, C.A. Candida tropicalis chorioamnionitis. Am J Obstet Gynecol. 1995;172(3):1045-7. [CrossRef]
- Chen, W.Y.; Chen, S.J.; Tsai, S.F.; Tsao, P.C.; Tang, R.B.; Soong, W.J. Congenital Systemic Fungus Infection in Twin Prematurity-A Case Report and Literature Review. AJP Rep. 2015;5(1):e46-50. [CrossRef]
- Ruiz-Cabrera, J.R.; Meléndrez-Vásquez, D.; Moreno, D.M.; Prieto-Jure. R. Congenital cutaneous candidiasis in a premature neonate: A case report. Clin Case Rep. 2022;10(5):e05773. [CrossRef]
- Kumar, M.; Saadaoui, M.; Al Khodor. S. Infections and Pregnancy: Effects on Maternal and Child Health. Front Cell Infect Microbiol. 2022;12:873253. [CrossRef]
- Maki, Y.; Fujisaki, M.; Sato, Y.; Sameshima, H. Candida Chorioamnionitis Leads to Preterm Birth and Adverse Fetal-Neonatal Outcome. Infect Dis Obstet Gynecol. 2017;2017:9060138. [CrossRef]
- Disha, T.; Haque, F. Prevalence and Risk Factors of Vulvovaginal Candidosis during Pregnancy: A Review. Infect Dis Obstet Gynecol. 2022;2022:6195712. [CrossRef]
- Shazniza Shaaya, E.; Halim, S.A.A.; Leong, K.W.; Ku, K.B.P.; Lim, P.S.; Tan, G.C.; Wong, Y.P. Candida Chorioamnionitis in Mothers with Gestational Diabetes Mellitus: A Report of Two Cases. Int J Environ Res Public Health. 2021;18(14):7450. [CrossRef]
- Salusti-Simpson, M.; Marghoob, N.; Greene, L.; Morley. K. Congenital cutaneous candidiasis in a full-term neonate. Pediatr Dermatol. 2022;39(6):952-954. Epub 2022 Jul 25. [CrossRef]
- Pammi, M. Candida infections in neonates: Epidemiology, clinical manifestations, and diagnosis. Last updated: May 22, 2024. https://www.uptodate.com/contents/candida-infections-in-neonates-epidemiology-clinical-manifestations-and-diagnosis.
- Suárez, J.A.G.; Calumby, R.J.N.; Silva, D.P.; Barbosa, V.T.; Maranhão, F.C.A.; Moreira, I.F.; Melhem, M.S.C.; Moreira, R.T.F. Neonatal innate immunity response in invasive candidiasis. Braz J Biol. 2024;84:e275155. [CrossRef]
- Michalski, C.; Kan, B.; Lavoie, P.M. Antifungal Immunological Defenses in Newborns. Front Immunol. 2017;8:281. [CrossRef]
- Mahieu, L.M.; Van Gasse, N.; Wildemeersch, D.; Jansens, H.; Ieven, M. Number of sites of perinatal Candida colonization and neutropenia are associated with nosocomial candidemia in the neonatal intensive care unit patient. Pediatr Crit Care Med. 2010;11(2):240-5. [CrossRef]
- Roqué, H.; Abdelhak, Y.; Young, B.K. Intra amniotic candidiasis. Case report and meta-analysis of 54 cases. J Perinat Med. 1999;27(4):253-62. [CrossRef]
- Jagtap, S.A.; Saple, P.P.; Dhaliat, S.B. Congenital cutaneous candidiasis: A rare and unpredictable disease. Indian J Dermatol. 2011;56(1):92-3. [CrossRef]
- Blomberg, L.; Backman, K.; Kirjavainen, P.V.; Karvonen, A.M.; Harju, M.; Keski-Nisula, L. Vulvovaginal yeast infections, gestational diabetes and pregnancy outcome. BMC Pregnancy Childbirth. 2023;23(1):70. [CrossRef]
- Rasti, S.; Asadi, M.A.; Taghriri, A.; Behrashi, M.; Mousavie, G. Vaginal candidiasis complications on pregnant women. Jundishapur J Microbiol. 2014;7(2):e10078. [CrossRef]
- Drummond, R.A.; Lionakis, M.S. Candidiasis of the Central Nervous System in Neonates and Children with Primary Immunodeficiencies. Curr Fungal Infect Rep. 2018;12(2):92-97. [CrossRef]
- Bider, D.; Ben-Rafael, Z.; Barkai, G.; Mashiach, S. Intrauterine fetal death apparently due to Candida chorioamnionitis. Arch Gynecol Obstet. 1989;244(3):175-7. [CrossRef]
- Guzel, A.B.; Ilkit, M.; Burgut, R.; Urunsak, I.F.; Ozgunen, F.T. An evaluation of risk factors in pregnant women with Candida vaginitis and the diagnostic value of simultaneous vaginal and rectal sampling. Mycopathologia. 2011;172(1):25-36. [CrossRef]
- Roberts, C.L.; Rickard, K.; Kotsiou, G.; Morris, J.M. Treatment of asymptomatic vaginal candidiasis in pregnancy to prevent preterm birth: An open-label pilot randomized controlled trial. BMC Pregnancy Childbirth. 2011;11:18. [CrossRef]
- Stronati, M.; Decembrino, L. Neonatal invasive candidiasis. Minerva Pediatr. 2006;58(6):537-49. PMID: 17093376. [PubMed]
- Torres-Alvarez, B.; Hernandez-Blanco, D.; Ehnis-Perez, A.; Castanedo-Cazares, J.P. Cutaneous congenital candidiasis in a full-term newborn from an asymptomatic mother. Dermatol Online J. 2013;19(7):18967. PMID: 24010513. [PubMed]
- Gonçalves, B.; Ferreira, C.; Alves, C.T.; Henriques, M.; Azeredo, J.; Silva, S. Vulvovaginal candidiasis: Epidemiology, microbiology and risk factors. Crit Rev Microbiol. 2016;42(6):905-27. [CrossRef]
- He, Y.; Tang, R.; Deng, J.; Cai, T.; He, P.; Wu, J.; Cao, Y. Effects of oestrogen on vulvovaginal candidosis. Mycoses. 2022;65(1):4-12. [CrossRef]
- Kumar, S.; Vasant, B.; Mathur, A.; De, M. A study of neonatal sepsis due to Candida species. Bombay Hospital Journal. 2011;53: 524-528.
- Saiman, L.; Ludington, E.; Pfaller, M.; Rangel-Frausto, S.; Wiblin, R.T.; Dawson, J.; Blumberg, H.M.; Patterson, J.E.; Rinaldi, M.; Edwards, J.E.; Wenzel, R.P.; Jarvis, W. Risk factors for candidemia in Neonatal Intensive Care Unit patients. The National Epidemiology of Mycosis Survey study group. Pediatr Infect Dis J. 2000;19(4):319-24. [CrossRef]
- Prinsloo, B.; Weldhagen, G.F.; Blaine, R.W. Candida famata central nervous system infection. S Afr Med J. 2003;93(8):601-2. PMID: 14531119. [PubMed]
- Manzoni, P.; Farina, D.; Galletto, P.; Leonessa, M.; Priolo, C.; Arisio, R.; Gomirato, G. Type and number of sites colonized by fungi and risk of progression to invasive fungal infection in preterm neonates in neonatal intensive care unit. J Perinat Med. 2007;35(3):220-6. [CrossRef]
- Darmstadt, G.L.; Dinulos, J.G.; Miller, Z. Congenital cutaneous candidiasis: Clinical presentation, pathogenesis, and management guidelines. Pediatrics. 2000;105(2):438-44. [CrossRef]
- Arsenault, A.B.; Bliss, J.M. Neonatal Candidiasis: New Insights into an Old Problem at a Unique Host-Pathogen Interface. Curr Fungal Infect Rep. 2015;9(4):246-252. [CrossRef]
- Zhao, H.H.; Zhe-Zhou, Lu L.; Zhao, Y.Z.; Yang, L.J.; Ding, Y.X. Congenital candidiasis in a full-term infant: A case report. J Int Med Res. 2023;51(4):3000605231158015. [CrossRef]
- Ito, F.; Okubo, T.; Yasuo, T.; Mori, T.; Iwasa, K.; Iwasaku, K.; Kitawaki, J. Premature delivery due to intrauterine Candida infection that caused neonatal congenital cutaneous candidiasis: A case report. J Obstet Gynaecol Res. 2013;39(1):341-3. [CrossRef]
- Ganer Herman, H.; Mevorach Zussman. N.; Krajden Haratz, K.; Bar, J.; Sagiv, R. Candida glabrata Chorioamnionitis following in vitro Fertilization: Review of the Literature. Gynecol Obstet Invest. 2015;80(3):145-7. [CrossRef]
- Obermair, H.M.; Bhagwanani, G.; Caldas, R.; Doyle, H.; Smoleniec, J.; Adno, A. Candida chorioamnionitis associated with late stillbirth: A case report. Case Rep Womens Health. 2020;27:e00239. [CrossRef]
- Diana, A.; Epiney, M.; Ecoffey, M.; Pfister, R.E. "White dots on the placenta and red dots on the baby": Congential cutaneous candidiasis--a rare disease of the neonate. Acta Paediatr. 2004;93(7):996-9. [CrossRef]
- Blanc, W.A. Pathways of fetal and early neonatal infection. Viral placentitis, bacterial and fungal chorioamnionitis. J Pediatr. 1961;59:473-96. [CrossRef]
- Jin, Y.; Endo, A.; Shimada, M.; Minato, M.; Takada, M.; Takahashi, S.; Harada, K. Congenital systemic candidiasis. Pediatr Infect Dis J. 1995;14(9):818-20.
- Paul, A.A.; Hoffman, K.L.; Hagan, J.L.; Sampath, V.; Petrosino, J.F.; Pammi, M. Fungal cutaneous microbiome and host determinants in preterm and term neonates. Pediatr Res. 2020;88(2):225-233. [CrossRef]
- Miras, I.; Vierge, E.; García, M.; Arruza, L.; Criado, E.; Ramos, J.T.; Martínez-Orgado, J. Congenital Cutaneous Candidiasis With Systemic Dissemination in a Preterm Infant. Pediatr Infect Dis J. 2021;40(6):e230-e233. [CrossRef]
- Colantonio, S.; Hedin, E.; Li, H.O.; Gavigan, G. Management of congenital cutaneous candidiasis in a healthy term baby: A case report. SAGE Open Med Case Rep. 2019;7:2050313X19876707. [CrossRef]
- Almeida Santos, L.; Beceiro, J.; Hernandez, R.; Salas, S.; Escriba, R.; Garcia Frias, E.; Perez Rodriguez, J.; Quero, J. Congenital cutaneous candidiasis: Report of four cases and review of the literature. Eur J Pediatr. 1991;150(5):336-8. [CrossRef]
- Kucinskiene, V.; Sutkute, A.; Valiukeviciene, S. Cutaneous fungal infection in a neonatal intensive care unit patient: A case report and literature review. Pediatr Dermatol. 2014;31(3):267-70. [CrossRef]
- Korting, H.C.; Patzak, U.; Schaller, M.; Maibach, H.I. A model of human cutaneous candidosis based on reconstructed human epidermis for the light and electron microscopic study of pathogenesis and treatment. J Infect. 1998;36(3):259-67. [CrossRef]
- Scheffler, E.; Miller, G.G.; Classen, D.A. Zygomycotic infection of the neonatal upper extremity. J Pediatr Surg. 2003;38(7):E16-7. [CrossRef]
- Smolinski, K.N.; Shah, S.S.; Honig, P.J.; Yan, A.C. Neonatal cutaneous fungal infections. Curr Opin Pediatr. 2005;17(4):486-93. [CrossRef]
- Smith, P.B.; Steinbach, W.J.; Benjamin, D.K. Jr.; Neonatal candidiasis. Infect Dis Clin North Am. 2005;19(3):603-15. [CrossRef]
- Ng, P.C.; Siu, Y.K.; Lewindon, P.J.; Wong, W.; Cheung, K.L.; Dawkins, R. Congenital Candida pneumonia in a preterm infant. J Paediatr Child Health. 1994;30(6):552-4. [CrossRef]
- Carmo, K.B.; Evans, N.; Isaacs, D. Congenital candidiasis presenting as septic shock without rash. Arch Dis Child. 2007;92(7):627-8. [CrossRef]
- Tezer, H.; Canpolat, F.E.; Dilmen, U. Invasive fungal infections during the neonatal period: Diagnosis, treatment and prophylaxis. Expert Opin Pharmacother. 2012;13(2):193-205. [CrossRef]
- Barone, S.R.; Krilov, L.R. Neonatal candidal meningitis in a full-term infant with congenital cutaneous candidiasis. Clin Pediatr (Phila). 1995;34(4):217-9. [CrossRef]
- Baradkar, V.P.; Taklikar, S.M. Meningitis caused by Candida albicans in a premature neonate. J Pediatr Neurosci, 2007,2(2):90–91. [CrossRef]
- Liu, S.H.; Mitchell, H.; Nasser Al-Rawahi, G. Epidemiology and associated risk factors for candidemia in a Canadian tertiary paediatric hospital: An 11-year review. J Assoc Med Microbiol Infect Dis Can. 2023;8(1):29-39. [CrossRef]
- Kopanou Taliaka P, Tsantes AG, Konstantinidi A, Houhoula D, Tsante KA, Vaiopoulos AG, Piovani D, Nikolopoulos GK, Bonovas S, Iacovidou N, Tsantes AE, Sokou R. Risk Factors, Diagnosis, and Treatment of Neonatal Fungal Liver Abscess: A Systematic Review of the Literature. Life (Basel). 2023 Jan 6;13(1):167. [CrossRef] [PubMed] [PubMed Central]
- Meizoso, T.; Rivera, T.; Fernández-Aceñero, M.J.; Mestre, M.J.; Garrido, M.; Garaulet, C. Intrauterine candidiasis: Report of four cases. Arch Gynecol Obstet. 2008;278(2):173-6. [CrossRef]
- Qureshi, F.; Jacques, S.M.; Bendon, R.W.; Faye-Peterson, O.M.; Heifetz, S.A.; Redline, R.; Sander, C.M. Candida funisitis: A clinicopathologic study of 32 cases. Pediatr Dev Pathol. 1998;1(2):118-24. [CrossRef]
- Aliaga, S.; Clark, R.H.; Laughon, M.; Walsh, T.J.; Hope, W.W.; Benjamin, D.K.; Kaufman, D.; Arrieta, A.; Benjamin, D.K. Jr.; Smith, P.B. Changes in the incidence of candidiasis in neonatal intensive care units. Pediatrics. 2014;133(2):236-42. [CrossRef]
- Ellepola, A.N.; Morrison, C.J. Laboratory diagnosis of invasive candidiasis. J Microbiol. 2005;43 Spec No:65-84. [PubMed]
- Clancy, C.J.; Nguyen, M.H. Finding the "missing 50%" of invasive candidiasis: How nonculture diagnostics will improve understanding of disease spectrum and transform patient care. Clin Infect Dis. 2013;56(9):1284-92. [CrossRef]
- Fleiss, N.; Schwabenbauer, K.; Randis, T.M.; Polin, R.A. What's new in the management of neonatal early-onset sepsis? Arch Dis Child Fetal Neonatal Ed. 2023;108(1):10-14. [CrossRef]
- Celik, I.H.; Hanna, M.; Canpolat, F.E.; Pammi, M. Diagnosis of neonatal sepsis: The past, present and future. Pediatr Res. 2022;91(2):337-350. [CrossRef]
- Schelonka, R.L.; Moser, S.A. Time to positive culture results in neonatal Candida septicemia. J Pediatr. 2003;142(5):564-5. [CrossRef]
- Oeser, C.; Pond, M.; Butcher, P.; Bedford Russell, A.; Henneke, P.; Laing, K.; Planche, T.; Heath, P.T.; Harris, K. PCR for the detection of pathogens in neonatal early onset sepsis. PLoS ONE. 2020;15(1):e0226817. [CrossRef]
- Greenberg, R.G.; Benjamin, D.K. Jr. Neonatal candidiasis: Diagnosis, prevention, and treatment. J Infect. 2014;69 Suppl 1(0 1):S19-22. [CrossRef]
- Stein, A.; Soukup, D.; Rath, P.M.; Felderhoff-Müser, U. Diagnostic Accuracy of Multiplex Polymerase Chain Reaction in Early Onset Neonatal Sepsis. Children (Basel). 2023;10(11):1809. [CrossRef]
- Aittakorpi, A.; Kuusela, P.; Koukila-Kähkölä, P.; Vaara, M.; Petrou, M.; Gant, V.; Mäki, M. Accurate and rapid identification of Candida spp. frequently associated with fungemia by using PCR and the microarray-based Prove-it Sepsis assay. J Clin Microbiol. 2012;50(11):3635-40. [CrossRef]
- Innings, A.; Ullberg, M.; Johansson, A.; Rubin, C.J.; Noreus, N.; Isaksson, M.; Herrmann, B. Multiplex real-time PCR targeting the RNase P RNA gene for detection and identification of Candida species in blood. J Clin Microbiol. 2007;45(3):874-80. Erratum in: J Clin Microbiol. 2007;45(6):2104. [CrossRef] [PubMed] [PubMed Central]
- Kosmeri, C.; Giapros, V.; Serbis, A.; Baltogianni, M. Application of Advanced Molecular Methods to Study Early-Onset Neonatal Sepsis. Int J Mol Sci. 2024;25(4):2258. [CrossRef]
- Shabaan, A.E.; Elbaz, L.M.; El-Emshaty, W.M.; Shouman, B. Role of serum (1,3)-β-d-glucan assay in early diagnosis of invasive fungal infections in a neonatal intensive care unit. J Pediatr (Rio J). 2018;94(5):559-565. [CrossRef]
- Warris, A.; Lehrnbecher, T. Progress in the Diagnosis of Invasive Fungal Disease in Children. Curr Fungal Infect Rep. 2017;11(2):35-44. [CrossRef]
- Manzoni, P.; Mostert, M.; Galletto, P.; Gastaldo, L.; Gallo, E.; Agriesti, G.; Farina, D. Is thrombocytopenia suggestive of organism-specific response in neonatal sepsis? Pediatr Int. 2009;51(2):206-10. [CrossRef]
- Wolach, B.; Bogger-Goren, S.; Whyte, R. Perinatal hematological profile of newborn infants with candida antenatal infections. Biol Neonate. 1991;59(1):5-12. [CrossRef]
- Tasneem, F.; Hossain, M.M.; Mahmud, S, Ahmed, S.S.;. Clinical profile of fungal sepsis in new born: A tertiary centre experience from Bangladesh. J Pediatr Neonatal Care. 2020;10(6):170-173. [CrossRef]
- Ratridewi, I.; Amalia, K.; Huwae, T.E.; Putera, M.A.; Sulistijono, E. Systemic Candidosis Diagnostic Test with Candida Score and Monocyte Count in Premature Infants with Late-Onset Sepsis: Research in Low Resources Country // Russian Journal of Infection and Immunity. 2023; 13(1): 133-140. [CrossRef]
- Noyola, D.E.; Fernandez, M.; Moylett, E.H.; Baker, C.J. Ophthalmologic, visceral, and cardiac involvement in neonates with candidemia. Clin Infect Dis. 2001;32(7):1018-23. [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; Zaoutis, T.E.; Sobel, J.D. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62(4):e1-50. [CrossRef]
- Ruhnke, M.; Rickerts, V.; Cornely, O.A.; Buchheidt, D.; Glöckner, A.; Heinz, W.; Höhl, R.; Horré, R.; Karthaus, M.; Kujath, P.; Willinger, B.; Presterl, E.; Rath, P.; Ritter, J.; Glasmacher, A.; Lass-Flörl, C.; Groll, A.H; German Speaking Mycological Society; Paul-Ehrlich-Society for Chemotherapy. Diagnosis and therapy of Candida infections: Joint recommendations of the German Speaking Mycological Society and the Paul-Ehrlich-Society for Chemotherapy. Mycoses. 2011;54(4):279-310. [CrossRef]
- Hope, W.W.; Castagnola, E.; Groll, A.H.; Roilides, E.; Akova, M.; Arendrup, M.C.; Arikan-Akdagli, S.; Bassetti, M.; Bille, J.; Cornely, O.A.; Cuenca-Estrella, M.; Donnelly, J.P.; Garbino, J.; Herbrecht, R.; Jensen, H.E.; Kullberg, B.J.; Lass-Flörl, C.; Lortholary, O.; Meersseman, W.; Petrikkos, G.; Richardson, M.D.; Verweij, P.E.; Viscoli, C.; Ullmann, A.J; ESCMID Fungal Infection Study Group. ESCMID* guideline for the diagnosis and management of Candida diseases 2012: Prevention and management of invasive infections in neonates and children caused by Candida spp. Clin Microbiol Infect. 2012;18 Suppl 7:38-52. [CrossRef]
- Vasileiou, E.; Apsemidou, A.; Vyzantiadis, T.A.; Tragiannidis, A. Invasive candidiasis and candidemia in pediatric and neonatal patients: A review of current guidelines. Curr Med Mycol. 2018;4(3):28-33. [CrossRef]
- Robbins, N.; Caplan, T.; Cowen, L.E. Molecular Evolution of Antifungal Drug Resistance. Annu Rev Microbiol. 2017;71:753-775. [CrossRef]
- Gharaghani, M.; Taghipour, S.; Halvaeezadeh, M.; Mahmoudabadi, A.Z. Candiduria; a review article with specific data from Iran. Turk J Urol. 2018;44(6):445-452. [CrossRef]
- Wade, K.C.; Benjamin, D.K. Jr.; Kaufman, D.A.; Ward, R.M.; Smith, P.B.; Jayaraman, B.; Adamson, P.C.; Gastonguay, M,R.; Barrett, J.S. Fluconazole dosing for the prevention or treatment of invasive candidiasis in young infants. Pediatr Infect Dis J. 2009;28(8):717-23. [CrossRef]
- Lu, H.; Shrivastava, M.; Whiteway, M.; Jiang, Y. Candida albicans targets that potentially synergize with fluconazole. Crit Rev Microbiol. 2021;47(3):323-337. [CrossRef]
- Berman, J.; Krysan, D.J. Drug resistance and tolerance in fungi. Nat Rev Microbiol. 2020;18(6):319-331. Erratum in: Nat Rev Microbiol. 2020;18(9):539. Erratum in: Nat Rev Microbiol. 2020;18(9):539. doi: 10.1038/s41579-020-0415-y. [CrossRef]
- Rosenberg, A.; Ene, I.V.; Bibi, M.; Zakin, S.; Segal, E.S.; Ziv, N.; Dahan, A.M.; Colombo, A.L.; Bennett, R.J.; Berman, J. Antifungal tolerance is a subpopulation effect distinct from resistance and is associated with persistent candidemia. Nat Commun. 2018;9(1):2470. [CrossRef]
- Benjamin, D.K. Jr.; Stoll, B.J.; Fanaroff, A.A.; McDonald, S.A.; Oh, W.; Higgins, R.D.; Duara, S.; Poole, K.; Laptook, A.; Goldberg, R; National Institute of Child Health and Human Development Neonatal Research Network. Neonatal candidiasis among extremely low birth weight infants: Risk factors, mortality rates, and neurodevelopmental outcomes at 18 to 22 months. Pediatrics. 2006;117(1):84-92. [CrossRef]
- de Haan, T.R.; Beckers, L.; de Jonge, R.C.; Spanjaard, L.; van Toledo, L.; Pajkrt, D.; van Wassenaer-Leemhuis, A.G.; van der Lee, J.H. Neonatal gram negative and Candida sepsis survival and neurodevelopmental outcome at the corrected age of 24 months. PLoS ONE. 2013;8(3):e59214. [CrossRef]
- Mendling, W.S.H. Antimykotische Therapie der Vaginalen Hefepilz-Kolonisation von Schwangeren zur Verhutung von Kandidamykosen beim Neugeborenen. AMWF 2008;15:S1.
- Mantadakis, E.; Pana, Z.D.; Zaoutis, T. Candidemia in children: Epidemiology, prevention and management. Mycoses. 2018;61(9):614-622. [CrossRef]
Figure 1.
Cutaneous rash – aspects in the first 30 hours of life.

Figure 2.
(A) Small bilateral perihilar interstitial foci; left-sided distended stomach, right-sided liver opacity, normal heart position in patient 1. (B) Slightly pronounced reticular, micronodular lung interstitium, bilateral.
Figure 2.
(A) Small bilateral perihilar interstitial foci; left-sided distended stomach, right-sided liver opacity, normal heart position in patient 1. (B) Slightly pronounced reticular, micronodular lung interstitium, bilateral.
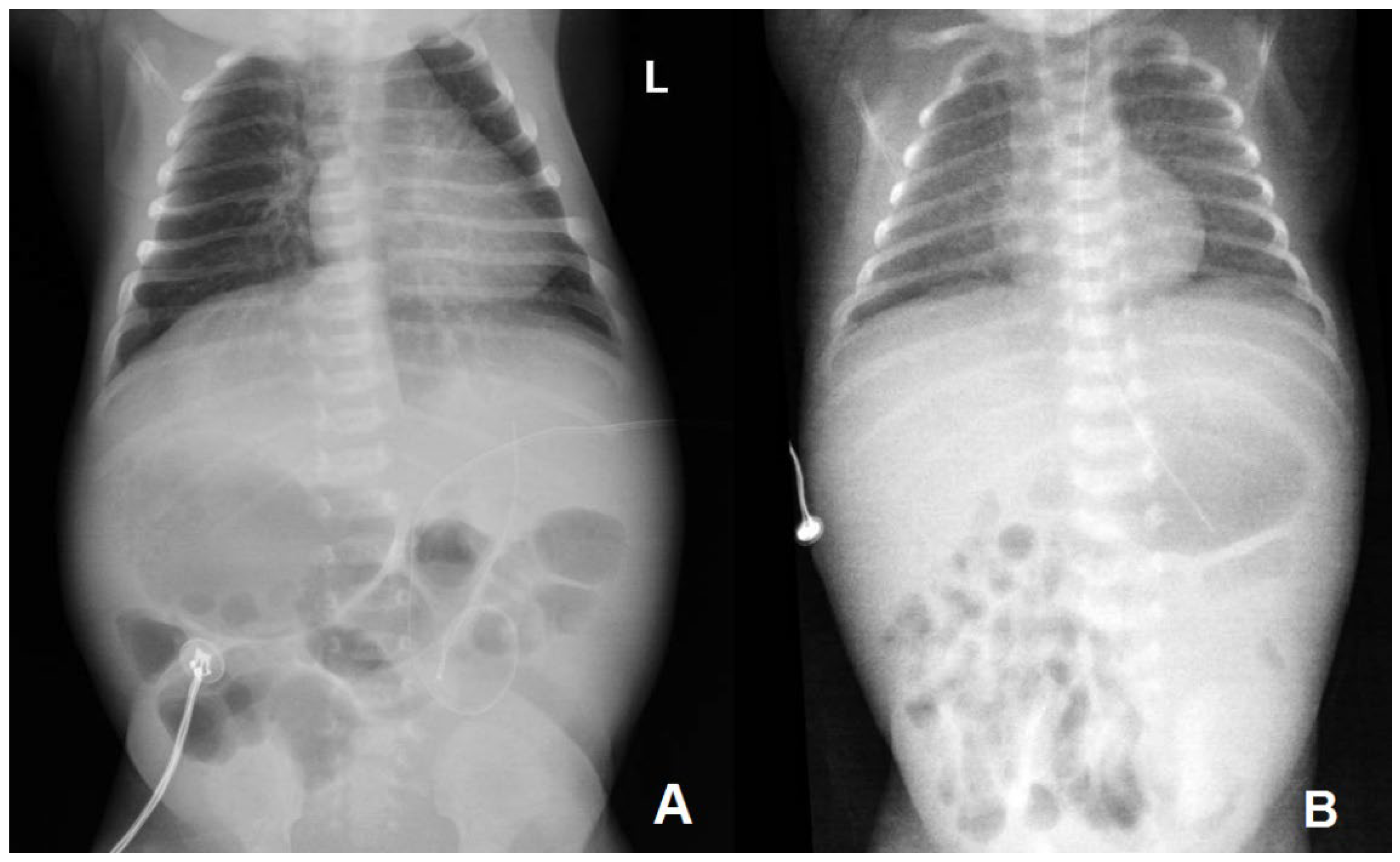
Figure 3.
A – Almost generalized gross, nodular, hyperechoic structure of the liver; B and C – limited areas of fine granular echogenic hepatic structure.
Figure 3.
A – Almost generalized gross, nodular, hyperechoic structure of the liver; B and C – limited areas of fine granular echogenic hepatic structure.
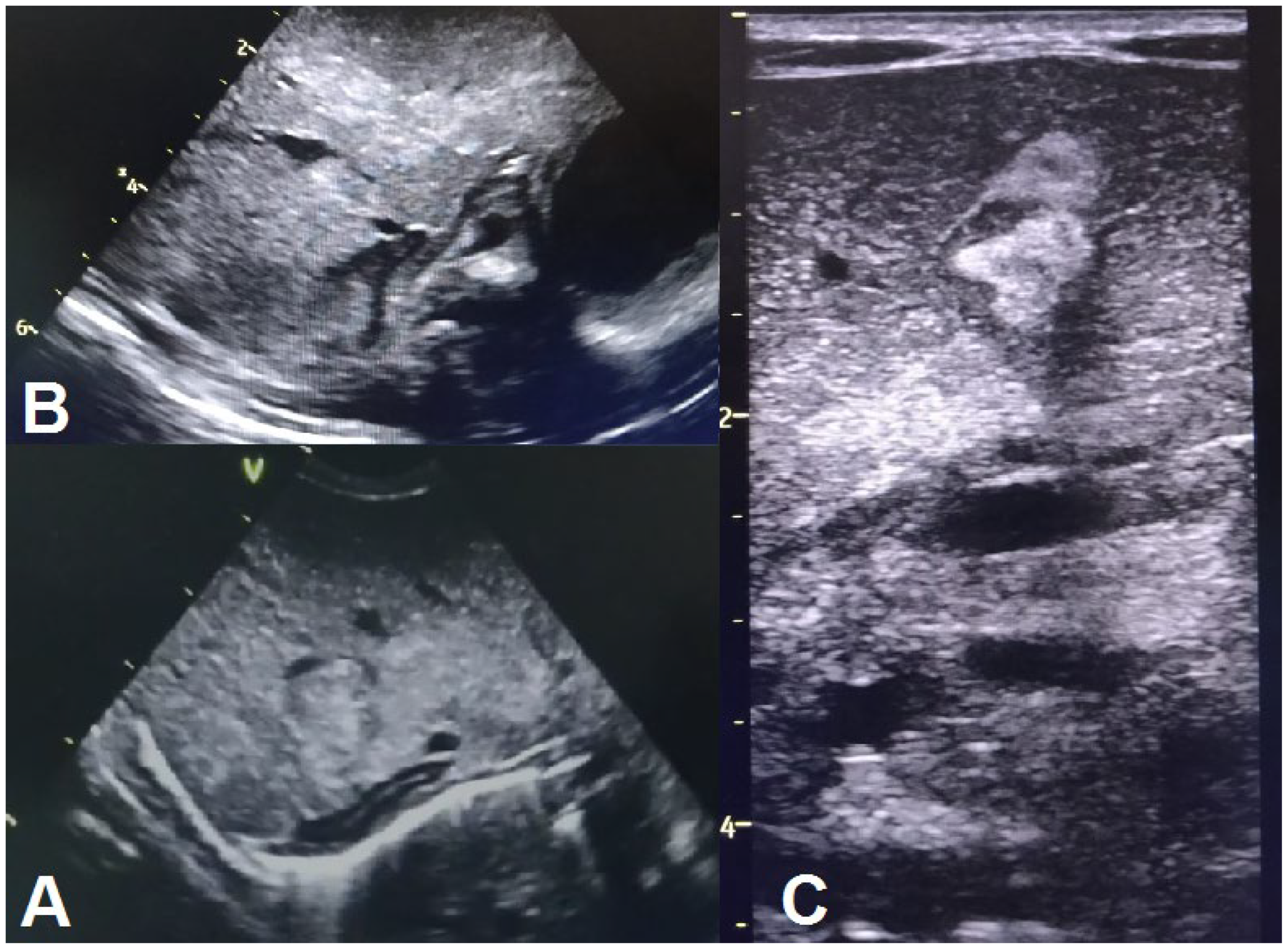
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



