
Submitted:
17 July 2024
Posted:
18 July 2024
You are already at the latest version
Abstract
Clinical academics experience dual workplaces; the clinical and the research environment. However, working in two workplaces leads to difficulty in forming an integrated identity, and hence affects a person’s work environment and well-being. The aim was to explore how clinical academics experience the psychosocial work environment and their suggestions for improving and changing work well-being.
A multicenter qualitative approach with group interviews inspired by participatory action de-sign was used. A purposeful criterion sampling strategy was used, selecting researchers affiliat-ed with the university's research network (n=12). Data were analyzed by thematic analysis and the consolidated criteria for reporting qualitative research was applied. The main finding “lack of integration of research in clinical practice”, revealed how clinical academics balanced between the two practices, how their need for belonging in both work environments were established by fellowship, and how motivational factors and role models could be enhanced through a joint commitment of responsibility in research units and clinical practice.
This study provides a contemporary understanding of the challenges that clinical academics en-counter and what solutions they would offer. This study adds to knowledge on psychological work well-being and provides solutions on how clinical academics can achieve integration of research in clinical practice.
Keywords:
Well-being
; Psychosocial
; Work environment
; Clinical academics
; Participatory action research
1. Introduction
Globally, there has been advocacy for clinical academic positions for health care professionals due to their positive impact on care quality and their role in supporting recruitment and retention [1,2]. Clinical academics (CAs) can be described as individuals with any health professional background who work in both clinical and research roles and play a key role in the academic and healthcare workforce with a clinical and academic work environment [1]. CAs have any background and their research and teaching commitments are dependent on various individual factors as well as the systems in which they operate [1]. The Physician-Scientist Workforce Working Group Report [3], details the unique perspective of physician-scientists: a two-way process, where clinical observations can be translated into research, and the findings can be implemented in care [3,4]. Due to the duality of the position, Denmark has politically prioritized that clinical work takes precedence in the healthcare system, where clinical work may in periods give way for research and Ph.D. [5].
CAs’ work environment at the hospital is complex in terms of workload, individual responsibility, pressure due to lack of time, and the scarcity of human resources [6,7]. This can result in stress and burnout among physicians leading to career and job dissatisfaction and profession change [8]. Occupational stress is also reported high in academia [9]. A good working environment leads to high-quality patient care [7,10]. Well-being at work refers to a psychosocial work environment as a combination of health, safety, and well-being concerns including organization of work and workplace culture [11]. A good and healthy work environment is influenced by knowledgeable management, collaboration amongst colleagues, good physical conditions, and psychological well-being (e.g. flexibility, and autonomy) [12,13]. The psychosocial work environment has been used in different job strain models (e.g., the job demands-resources and self-determination theory) to explain why psychosocial factors and resources might lead to negative (e.g., stress, dissatisfaction, and burnout) and positive outcomes (e.g., engagement, motivation, and commitment) [14,15,16].
A healthy work environment promotes well-being, which influences work performance and leads to retention, health disparities, and care delivery [17,18,19,20]. Ng and colleagues (2019) found that the integration of clinical work and research, especially during a Ph.D. program, is poorly defined [21]. Moreover, since there are no defined competencies for a CAs position, this can lead to uncertain expectations from the management [19]. CAs often work on short-term contracts, develop as independent researchers, apply for funding, navigate a competitive environment, and aim to increase their research publication output [22,23,24]. The majority of research has used questionnaires and interviews for quantifying and understanding CAs work well-being [3,4,13,17,18,20,24], but none have actively engaged CAs in investigating their challenges and the possible solutions to improve their work well-being. Therefore, is the aim of this study to explore how clinical academics experience the psychosocial work environment and their suggestions for changing work well-being.
2. Materials and Methods
2.1. Design
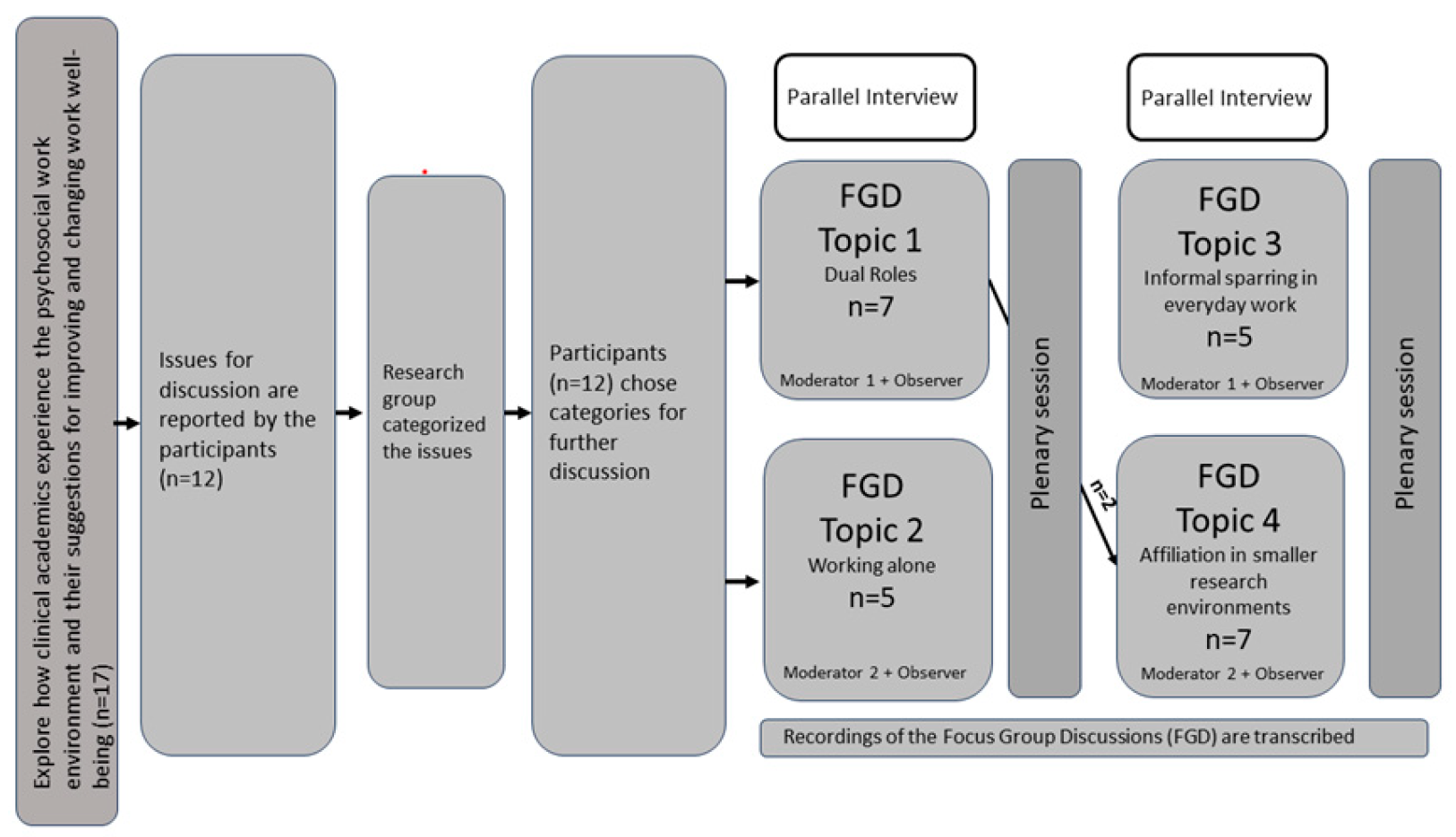
The study used a qualitative approach with virtual focus group discussions inspired by participatory action design [25,26]. The consolidated criteria for reporting qualitative research (COREQ) was applied [27]. Participatory action design encouraged participants to emphasize their solutions based on their problems and challenges experienced as CAs in different hospital settings [28]. Participatory action design was based on participants submitting issues of importance and participating in workshop with group discussions of challenges and achievable solutions. It reinforced critical dialogue about their experiences of work well-being [25,26]. At subsequent theme days by the Institute for Regional Health Research suggestions and actions were a part of the discussions on how to improve work well-being in practice, Figure 1.
2.2. Setting and Participants
The participants of the study, as well as four of the authors, were researchers associated with the University of Southern Denmark (SDU), Institute for Regional Health Research (IRS). IRS is a network of health research environments and educational activities anchored at SDU covering 12 different hospital settings in the regions of Southern Denmark, Zealand, and the Capital Region of Denmark. Therefore, researchers at the IRS are dually affiliated with SDU and clinical departments at hospitals. The IRS network of young researchers consists of Ph.D. students (n=110), postdoctoral researchers (n=15), and adjuncts (n=5). They were all invited to participate via email by a secretary. A purposeful criterion sampling strategy was used based on participants’ affiliation to IRS to capture the experiences of researchers’ dual affiliation and to explore solutions to improve work well-being [29]. In total, 17 researchers volunteered to participate in the study, however, some were absent due to unexpected work (n=5) leaving the final sample with 12 participants, Figure 1.
2.3. Procedures
The week prior to the focus group interviews, participants submitted 15 daily challenges by email, which could be discussed in the group interviews [30]. These were organized into topics, Table 1. Participants selected four topics in two parallel group interviews, which they found most crucial for further discussions. These were: 1) Dual roles; 2) Working alone; 3) Informal sparring in everyday work; and 4) Affiliation in smaller research environments. After each parallel interview, a plenary session with all participants were conducted to summarize the findings from each focus group interview [30,31]. The interview guide consisted of two ‘grand tour’ questions covering ‘What is the problem?’ and ‘How can it be resolved?’. All four focus group interviews were audio recorded, transcribed, and used for the analysis. Interview lasted 45 minutes (Range 42-47 minutes).
2.4. Data Analysis
Each group interview was facilitated by an experienced moderator (first and last author) accompanied by an observer (a consultant and third author). The moderator and observer took notes during the interviews. All data was analyzed using a qualitative thematic analysis, which identifies, analyzes, and reports themes within the qualitative data [31]. A theme is identified as something significant about the data in relation to exploring how the work environment can support work well-being and possible solutions, which symbolizes a patterned response or meaning within the data set [31]. Data was collected inductively, where the focus group interviews had predefined topics, that were designed to explore the work environment and possible solutions [31]. A narrative listening to the interviews, notes during the interviews, and summaries were used to initiate the analysis. The next step was to search, sort, and categorize codes into themes. These themes were then revised and sorted into distinct themes with corresponding subthemes. Critical statements were sought in the collected data material, about the participants' experiences of challenges in the work environment and their suggestions for changes. Throughout the process, the authors made sure to agree on all themes, subthemes, and quotes. Audio recordings of the interviews were transcribed and verified by a third party. Three authors completed the thematic analysis (first, second and last author). Finally, the themes were named in the ongoing analysis of each theme and their relation to the study's overall story. The data analysis was performed using Excel software. The authors’ interest in researching the work environment was due to the assumption that our work environment influences our performance, and how the psychosocial work environment could be improved.
2.5. Ethical Approvals
The Helsinki Declaration was followed, and participants were included after oral and written informed consent had been obtained. The study was presented to the National Committee on Health Research Ethics, and according to Danish law, no formal approval was needed (J. no EMN-2023-02212). The local Ethical committee at the Hospital and relevant hospital- and department managers approved the study protocol (EMN-2023-04115). Participants were informed that participating in this study was confidential and did not have any influence on their work or terms of employment.
3. Results
3.1. Participants Characteristics
Participants were affiliated with five hospitals located in the Southern Region of Denmark. This included two adjuncts, one associate professor, and nine Ph.D. students, of whom five were males and seven were female, all aged 29-62 (mean 38 years) with current employment in the department between 6-140 months (mean 39). In total, seven had combined positions between research and clinical work (n=5), or between research and teaching (n=2), Table 2.
3.2. Main Theme: Lack of Integration of Research in Clinical Practice
The main theme structured the meaning of CAs’ well-being in their psychosocial work environment, and their suggestions for change. This was ‘Lack of integration of research in clinical practice’. It emerged after identifying three themes: I) ‘The fine line between research and clinical practice’; II) ‘A wish to belong; and III) ‘The impact of motivational factors and role models’. The analytical process is abstracted in Table 3 and selected quotations are presented in Table 4.
3.3. Theme I: The Fine Line between Research and Clinical Practice
Participants spoke of a vision that clinical work and research should complement each other. The participants assumed that their colleagues considered research in clinical practice the same way. However, participants experienced being stuck between the consideration for the clinical- and patient-related work and the consideration for progressing their research projects. The feeling of being caught in both positions was reinforced by expectations from both positions to perform at 110%. Few participants were concerned about missing a new procedure or guideline, which could potentially harm patients and result in legal complaints. Most participants experience being in a double role, where the role as clinician is led by the concern for patient care. In contrast, their role as a researcher is driven by need to a continuously advance in both research, publications, and other academic tasks. Participants challenges was about time for research, as patient care and clinical tasks often are acute, and will be prioritized. Some expressed that research was consumed by clinical tasks, and an obligation towards timely quality patient care, which was driven by their consciousness. Some participants spoke of the importance of having dedicated time for both positions and being strict with their time to fulfill each function.
All participants believed delegation of time to research should be a manager’s and research leader’s responsibility. It can be stressed that the department management, might not always have a full overview of all the details of the research projects, however, acceptance and support from both the research and the department management is equally important. In addition to time delegation, boundaries between functions and the associated tasks and roles were also unclear. This made the navigation between the two professional roles difficult. Unclear content of functions, tasks, and time structure were areas that added to the burden of research in clinical practice and pushed research to be secondary. Participants experienced structuring their work life, as a challenge that requires special attention due to unclear roles and content. Some stated that several of the challenges they experienced, could be resolved by having a guide of the daily work, with updates on crucial changes in patients’ guidelines, but also having a journal of guidelines in the department. Most participants highlighted that structure in a written journal allows for an overview, with clear task delegation. Additionally, it allows for an overview of the clinical tasks, for example when test results are available for check up in the clinical work. It is a motivational factor for participants to have management’s visible support and recognition.
3.4. Theme II: A Wish to Belong
It was essential for participants to feel a sense of belonging in both working environments. Conducting research can be lonely, but is dependent on collaboration, network, and social relationships to succeed. Participants felt alone in research on two levels; on the physical level by having single offices or working from home; and on the research level in their individual projects, due to having different research areas compared to other researchers in the research unit.
Being visible was experienced to be of importance, for example by including the departments’ staff in the current research projects. It permits a sense that a researcher is not remote, but rather one, who is carrying out research in clinical practice. It encouraged a sense of community beyond patient care, allowing us to celebrate research victories together. Participants elaborated on having clinical obligations in addition to research as stressful, but some also considered it as a break with the opportunity to be a part of a broader fellowship. Some regarded being affiliated with clinical practice as a place to have casual chats, and the fellowship was enhanced by physical presence to share knowledge in clinical practice. Others used face-to-face contact with their professor or research colleagues in a more formal approach to create fellowship. The need for fellowship along with their responsibility in clinical practice generated a struggle to say no to their colleagues or other health professionals. It created an inner conflict between clinical duty with fellowship and personal interest to progress with one’s research project. It leads to an experience of putting your own needs aside to strengthen your research, which will benefit the overall research unit. It requires a unique kind of person with high self-discipline and a focus on progression in research. Sometimes participants had to accept that not everything is manageable within the timeframe or resources they have.
3.5. Theme III: The Impact of Motivational Factors and Role Models
Competition is a premise of research. It can be motivational or destructive factors, which either provide energy and engagement or stress people out. The competitive aspect affects the priority of themes, within the research unit, based on the head of the research unit and/or supervisors’ interests. The focus on specific topics of research influences the opportunities for funding applications, how much attention the topic gets within and outside the research unit, including how much information staff receive about present research activities. The expectations and ambitions in the research unit is to be the first to publish in high-impact journals. Both clinicians and research supervisors have expectations, which can be incongruent in terms of how participants should prioritize their time and tasks. Contrastingly, some have zero expectations due to repeatedly neglect from either the research unit or the clinical practice.
Participants expressed being simultaneously responsible for creating progress and flow in the research, which allows for great job satisfaction when succeeded. However, it is also emphasized that participants must set clear and realistic goals in the daily workload and avoid procrastination. Clinical work can be a legitimate way to procrastinate, which in turn disturbs the expected progress of the research. Academic sparring supported young as well as senior researchers to grow. However, senior researchers, who were supervisors had a dual role in both assisting young researchers and seek out support in their own network. As a supervisor, one has a great responsibility to support others. Few Ph.D. candidates spoke of their relationship with their supervisor as a parent/child or like an apprenticeship. The learning process was influenced by the support of the supervisor and the surrounding environment. Senior researchers also mentioned network sparring as necessary for moving forward in their projects. Many found academic sparring outside their research unit due to two reasons; the research unit was too small; or lack of confidence to be safe in the fellowship within the unit. That way, they have people around them, who they trust and feel safe enough to ask even the most obvious questions. It was all about having unprejudiced and constructive feedback in the research environment.
Some participants experienced a lack of joint commitment and a sense of responsibility toward each other. One of the solutions were doing activities together to enhance a sense of responsibility. Activities could be going on a walk or eating lunch with both researchers and clinicians. Participants pointed out that it would be obvious to make a network across research units, preferably virtual and in close association with the current research unit. Some also had great experience with joint research meetings, which offered a shared space that it is necessary to create and cultivate relationships across research areas and hospitals. It is important to have versatility in one’s social circle, people to rely on for help, and a place to talk about things that take up a lot of space mentally.
4. Discussion
This is one of the few studies that used participatory design to explored how work environment can support work well-being among CAs, and their suggestions for changes. Applying this approach to clinical academics’ psychosocial work environment, we showed how researchers in clinical practice struggled with promoting and inhibiting aspects of their jobs that affected their work well-being. The main finding “lack of integration of research in clinical practice” describes how researchers balanced between research obligations and clinical responsibilities; their need for belonging in both work environments are established by fellowship; and how motivational factors and role models should be enhanced through a joint commitment of responsibility in research units and clinical practices.
The importance of integrating research in clinical practice has been to combine expertise from both roles to advocate for cost-effective patient care [1,32,33]. A significant investment in joint CA positions has been made to bridge the gap between academia and the clinical field [5,32]. Lack of integration might be explained by findings from a systematic review [1] evaluating interventions intended to increase recruitment, retention, and career progression within CA careers [1]. These findings indicated the benefits of supportive relationships for CAs, including peer and senior mentors [1]. A significant barrier was having dedicated time, particularly to moderate the negative impact of competing clinical demands and research-related activity for both nurses and physicians [1,34]. However, maintaining dedicated time was reported to be difficult in practice [1], as participants in the present study also experienced. According to Raine et al. (2021), a committed and experienced program staff were key facilitators of success [1], which is related to the solutions suggested in this study. It is possible that interventions to integrate research in clinical practice successfully should add supportive relationships for CAs, secure dedicated time for research in clinical practice, and enroll committed and experienced program staff in future studies. This might increase work well-being but also have a positive effect on the recruitment and retention of CA careers, as highlighted by others [1]. Surprisingly, only one of the participants spoke of incorporating physical activity as a work place intervention. Other work place interventions might be mindfulness, which have indicated an increased effectiveness on well-being and optimal time management in academia compared to a control group [9]. However, protected time for research in clinical practice is somewhat controversial because clinical work has been politically stated to have superiority in the healthcare system [5].
The lack of integration can also be explained through differences between the clinical and academic worlds, which might be the disconnect between the two that has been called the “theory-practice gap” within the nursing literature [32,34]. Support from leadership for participating in research activities is essential if research-based nursing care is to succeed [35]. Success is determined by clear expectations, roles, and how to integrate CAs among the staff to avoid competition, isolation, and blurring of roles [35]. Blurring roles also affected participants’ work well-being in this study, which matches a qualitative study with senior researchers (n=13) [36]. Trusson & Rowley (2022) described difficulties in making the role of the CA clear and hence, adjusting expectations from colleagues [36]. Participants described the work environment in two different cultures where direct patient care is a priority for clinical staff and manager leaders, hence implying that research is not [36]. Another similar qualitative study (n=14) indicated that these issues arise from CA nurses feeling under-appreciated and were victims of negative reactions from the clinical team [37]. In this study, the priority on patient care was experienced by physicians as well as nurses. The solution from participants in this study was a higher degree of leadership support, as found by others [38]. Oostveen et al. (2017) suggest that leaders' lack of commitment may stem from a lack of clear vision and mission at the strategic level [37]. Additionally, nursing directors should take a frontline role in promoting CA’s work [37]. However, managers and directors reported personally inadequate academic knowledge and competencies for integrating clinical and academic work [37]. To achieve a higher degree of integration of clinical and academic work, leaders also need clear roles, expectations, and content to the individual employee [35]. Additionally, mentoring, peer support, and having role models aids in academic skills and establishing an academic identity [39,40]. Moreover, according to the job demands-resources theory, resources can serve as buffer between job demands and strain [15]. Resources such as social support, performance feedback, and opportunities for development can diminish the experience of job demand and aid the individual in managing job demands better [15]. This shows the importance of adding resources to increase resilience and improve well-being.
Work well-being can be increased with simple low-cost suggestions that can be incorporated into future interventions. These suggestions included structuring everyday work life, having academic sparring, being a part of a network, and doing activities together. Self-determination theory focuses on the effect of social-contextual factors on human motivation, behavior, and personality [16]. The self-determination theory can be used to understand how to support people's motivation at work [16]. Some of the findings can be explained by the self-determination theory and shows how to facilitate extrinsic rewards on the participants’ motivation. In the self-determination theory, there are three crucial psychological needs equally central to optimizing development, functioning, and increasing well-being [16]. These needs are competence, autonomy, and relatedness, and can help explain our findings [16]. Competencies can be related to the fine line between clinical and research practice, autonomy as the impact of motivational factors and role models, and relatedness in terms of the theme of a wish to belong. According to World Health Organization (2010) managing mental health at work offers an opportunity for growth and sustainable development [11]. Future studies are recommended to investigate some of the suggestions the participants pointed out as a base for interventional frameworks. These interventions can be seen from the multilevel perspective of an integrated approach like the Individual, Group, Leader, Organizational, and Overarching context model (IGLOO) [41,42]. The interventions should incorporate the psychological needs from the self-determination theory, and address demands and resources seen from the job demands-resources theory [15,16] to ensure effective prevention, promotion, and support for mental health at work [11]. The next step of this study is to develop implementation strategies based on participants’ suggestions for change at various levels within the organization (e.g., within the IGLOO framework). Another important unanswered question is the psychosocial work environment experienced by senior CAs, including professors. A future examination that includes senior CAs would bring another perspective and provide insight into issues and solutions regarding their work environment.
Methodological Considerations
This study was limited by uneven seniority presentation, which was uncontrollable with volunteer-based participation. Additionally, while this study involved a selected group affiliated diverse group of CAs from different hospital settings with varying experience, these individuals do not represent all CAs from their hospitals and were mostly PHD students. However, the study included 12 participants, and found adequate informational power and hereby achieving data saturation [43]. We could have held the interviews outside normal working hours or conducted the interviews in a continuation of the annual seminar held at the IRS. However, this might have decreased the sample size and affect the analysis and data transformation. The credibility and trustworthiness of our findings were increased by adapting well-established research methods and by investigator triangulation [44,45]. The findings emerged from participants also employed at different hospitals and provide equivalent results as other studies, which increased the transferability of our findings. No studies, to our knowledge, have explored the work environment of CAs including which factors is changeable to improve their work well-being. One major strength of this study is the triangulation of methods combining elements from participatory action design with interview techniques [44,45]. This method actively engaged participants in selecting the issues, and allowed participants to voice their own opinions on solutions, and even solutions in their specific workplace to increase their work well-being [25]. Lastly, authors openly discussed their predispositions to maintain objectivity during analysis and interpretation [44,45].
5. Conclusions
This study provides a contemporary understanding of the challenges that clinical academics encounter and what solutions they would offer. These findings could guide the development of future interventions based on participants' suggestions for change at different levels within the organization. Lack of integration of research in clinical practice affected CA’s work well-being differently depending on their specific context. To accomplish integration, several issues, must be addressed at different levels: 1) Overarching level with a clear CA work-related national policy; 2) organizationally with a clear vision and mission; 3) the leaders level with the support of management and leaders, and having clear expectations, defined roles, and plans for integration of CA’s within the staff; 4) the group and relational level by creating peer, mentor and network support; and 5) the individual level to help to structure everyday work and secure work-life balance. Addressing some of the many solutions suggested to change the work environment might increase work well-being and simultaneously improve retention, reduce sick leave, and long-term stress to benefit both patients, and the healthcare system, and enhance care delivery. This section is not mandatory but can be added to the manuscript if the discussion is unusually long or complex.
Author Contributions
Authors contributed different to this work. Conceptualization, J.F.J., M.P.R., and D. H.; methodology, J.F.J., D.H. and M.V., acquisition of data J.F.J., and D.H., validation, C.F.J., R.L.L., and M.C.; formal analysis, J.F.J., D.H., C.F.J.; writing—original draft preparation, C.F.J., J.F.J.; writing—review and editing, R.L.L., M.R.P., and M.C.; visualization, C.F.J.; project administration, J.F.J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethic Committee of The National Committee on Health Research Ethics (J.no EMN-2023-02212) and the local Ethical committee at Zealand University Hospital (J.no. EMN-2023-04115).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, but the anonymous data can be available on request to first author.
Acknowledgments
We wish to thank all participants who shared their experience of their work environment. We wish to thank the managers of Department of Neurology, Zealand University Hospital for their support to publish this study. The authors would like to acknowledge institute of Regional Health Research at University of Southern Denmark for their participation and support in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Raine, G.; Raine, G.; Evans, C.; Evans, C.; Uphoff, E.P.; Uphoff, E.P.; Brown, J.V.E.; Brown, J.V.E.; Crampton, P.E.S.; Crampton, P.E.S.; et al. Strengthening the clinical academic pathway: a systematic review of interventions to support clinical academic careers for doctors and dentists. BMJ Open 2022, 12, e060281. [Google Scholar] [CrossRef] [PubMed]
- Aspinall, C.; Slark, J.; Parr, J.; Pene, B.; Gott, M. The role of healthcare leaders in implementing equitable clinical academic pathways for nurses: An integrative review. J. Adv. Nurs. 2024. [Google Scholar] [CrossRef] [PubMed]
- Feldman, A.M. The National Institutes of Health Physician-Scientist Workforce Working Group Report: A Roadmap for Preserving the Physician-Scientist. Clin. Transl. Sci. 2014, 7, 289–290. [Google Scholar] [CrossRef] [PubMed]
- Health NIo. Physician-scientist workforce working group report. 2014. Bethesda, MD: National Institutes of Health 2021.
- Health MotIa. The government is launching several initiatives in the emergency plan for the healthcare system [Regeringen lancerer flere initiativer i akutplan for sundhedsvæsenet]. Website of the Ministry of the Interior and Health of Denmark, 2023:1-2.
- Labrague, L.J.; McEnroe-Petitte, D.M.; Leocadio, M.C.; Van Bogaert, P.; Cummings, G.G. Stress and ways of coping among nurse managers: An integrative review. J. Clin. Nurs. 2018, 27, 1346–1359. [Google Scholar] [CrossRef] [PubMed]
- Eva, G.; Amo-Setién, F.; César, L.; Concepción, S.; Roberto, M.; Jesús, M.; Carmen, O. Effectiveness of intervention programs aimed at improving the nursing work environment: A systematic review. Int. Nurs. Rev. 2023, 71, 148–159. [Google Scholar] [CrossRef] [PubMed]
- Silistraru, I.; Olariu, O.; Ciubara, A.; Roșca. ; Alexa, A.-I.; Severin, F.; Azoicăi, D.; Dănilă, R.; Timofeiov, S.; Ciureanu, I.-A. Stress and Burnout among Medical Specialists in Romania: A Comparative Study of Clinical and Surgical Physicians. Eur. J. Investig. Heal. Psychol. Educ. 2024, 14, 311–323. [Google Scholar] [CrossRef]
- Marais, G.A.B.; Lantheaume, S.; Fiault, R.; Shankland, R. Mindfulness-Based Programs Improve Psychological Flexibility, Mental Health, Well-Being, and Time Management in Academics. Eur. J. Investig. Heal. Psychol. Educ. 2020, 10, 1035–1050. [Google Scholar] [CrossRef] [PubMed]
- Aiken, L.H.; Sermeus, W.; Smith, H.L.; Kutney-Lee, A.; van den Heede, K.; Sloane, D.M.; Busse, R.; McKee, M.; Bruyneel, L.; Rafferty, A.M.; et al. Patient safety, satisfaction, and quality of hospital care: cross sectional surveys of nurses and patients in 12 countries in Europe and the United States. BMJ 2012, 344, e1717. [Google Scholar] [CrossRef]
- World Health Organization & Burton, J. WHO healthy workplace framework and model: background and supporting literature and practices. Geneva: World Health Organization 2010:93 p.
- Buch A, Andersen V, Sørensen OH. Knowledge work and stress: between excitement and strain [Videnarbejde og stress: mellem begejstring og belastning]: Jurist-og Økonomforbundets Forlag 2009.
- Fisher, CD. Conceptualizing and measuring wellbeing at work. In: Cooper PYCaCL, ed. Work and wellbeing Wiley Blackwell 2014:9-93.
- Hobfoll, S.E. Conservation of resources: A new attempt at conceptualizing stress. Am. Psychol. 1989, 44, 513–524. [Google Scholar] [CrossRef]
- Bakker AB, Demerouti E. Job demands-resources theory. Work and wellbeing, Vol III. Hoboken, NJ, US: Wiley Blackwell 2014:37-64.
- Deci EL, Ryan RM. Self-determination theory. Handbook of theories of social psychology, Vol 1. Thousand Oaks, CA: Sage Publications Ltd 2012:416-36.
- Berndt, J.D.; Ortelli, T.A.P. Creating a Healthy Work Environment. AJN, Am. J. Nurs. 2023, 123, 59–60. [Google Scholar] [CrossRef]
- Copanitsanou, P.; Fotos, N.; Brokalaki, H. Effects of work environment on patient and nurse outcomes. Br. J. Nurs. 2017, 26, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Suliman, M.; Aljezawi, M. Nurses’ work environment: indicators of satisfaction. J. Nurs. Manag. 2018, 26, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Sinsky, C.A.; Biddison, L.D.; Mallick, A.; Dopp, A.L.; Perlo, J.; Lynn, L.; Smith, C.D. Organizational Evidence-Based and Promising Practices for Improving Clinician Well-Being. NAM Perspect. 2020, 2020. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.; Jones, A.A.; Sivapragasam, M.; Nath, S.; Mak, L.E.M.; Rosenblum, N.D.M. The Integration of Clinical and Research Training: How and Why MD–PhD Programs Work. Acad. Med. 2019, 94, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Chatzea, V.-E.; Mechili, E.A.; Melidoniotis, E.; Petrougaki, E.; Nikiforidis, G.; Argyriadis, A.; Sifaki-Pistolla, D. Recommendations for young researchers on how to better advance their scientific career: A systematic review. Popul. Med. 2022, 4, 1–17. [Google Scholar] [CrossRef]
- Bazeley, P. Defining 'Early Career' in Research. High. Educ. 2003, 45, 257–279. [Google Scholar] [CrossRef]
- Hermann, K.J. , Wichmann-Hansen G., T.K. J. Quality in Ph.D. courses [Kvalitet i ph.d.-forløb]. Aarhus: Aarhus University, 2014:1-144.
- Chevalier JM, Buckles D. Participatory Action Research: Theory and Methods for Engaged Inquiry: Routledge 2013.
- Holden, R.J.; Scott, A.M.M.; Hoonakker, P.L.T.; Hundt, A.S.; Carayon, P. Data collection challenges in community settings: insights from two field studies of patients with chronic disease. Qual. Life Res. 2015, 24, 1043–1055. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- McIntyre, A. Participatory Action Research: SAGE Publications 2008.
- Patton, MQ. Choosing a Sample: The Logic of Purposeful Sampling. In: MQ P, ed. Program evaluation Kit How to Use Qualitative Methods in Evaluation. Newbury Park, California: Sage Publications, Inc. 1987:44-70.
- Halkier, B. Focus groups as social enactments: integrating interaction and content in the analysis of focus group data. Qual. Res. 2010, 10, 71–89. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Happell, B. Clinical-academic partnerships research: converting the rhetoric into reality. . 2005, 11, 1218–26. [Google Scholar] [PubMed]
- Jones, S.; Bradbury, A.; Shortland, S.; Hewett, F.; Storey, K. Clinical academic careers for general practice nurses: a qualitative exploration of associated barriers and enablers. J. Res. Nurs. 2021, 26, 704–715. [Google Scholar] [CrossRef] [PubMed]
- Haase, K.R.; Strohschein, F.J.; Horill, T.C.; Lambert, L.K.; Powell, T.L. A survey of nurses' experience integrating oncology clinical and academic worlds. Nurs. Open 2021, 8, 2840–2849. [Google Scholar] [CrossRef]
- Hølge-Hazelton, B.; Kjerholt, M.; Berthelsen, C.B.; Thomsen, T.G. Integrating nurse researchers in clinical practice - a challenging, but necessary task for nurse leaders. J. Nurs. Manag. 2016, 24, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Trusson, D.; Rowley, E. Qualitative study exploring barriers and facilitators to progression for female medical clinical academics: interviews with female associate professors and professors. BMJ Open 2022, 12, e056364. [Google Scholar] [CrossRef]
- van Oostveen, C.J.; Goedhart, N.S.; Francke, A.L.; Vermeulen, H. Combining clinical practice and academic work in nursing: A qualitative study about perceived importance, facilitators and barriers regarding clinical academic careers for nurses in university hospitals. J. Clin. Nurs. 2017, 26, 4973–4984. [Google Scholar] [CrossRef]
- Pedersen, M.V. What motivates radiographers to start working with research? Radiography 2022, 29, 215–220. [Google Scholar] [CrossRef]
- Logan, P.A.; Gallimore, D.; Jordan, S. Transition from clinician to academic: an interview study of the experiences of UK and Australian Registered Nurses. J. Adv. Nurs. 2016, 72, 593–604. [Google Scholar] [CrossRef]
- Robichaud-Ekstrand, S. New Brunswick nurses' views on nursing research, and factors influencing their research activities in clinical practice. Nurs. Heal. Sci. 2016, 18, 246–255. [Google Scholar] [CrossRef]
- Nielsen, K.; Christensen, M. Positive Participatory Organizational Interventions: A Multilevel Approach for Creating Healthy Workplaces. Front. Psychol. 2021, 12, 696245. [Google Scholar] [CrossRef]
- Nielsen, K.; Yarker, J.; Munir, F.; Bültmann, U. IGLOO: An integrated framework for sustainable return to work in workers with common mental disorders. Work. Stress 2018, 32, 400–417. [Google Scholar] [CrossRef]
- Malterud, K.; Siersma, V.D.; Guassora, A.D. Sample Size in Qualitative Interview Studies: Guided by Information Power. Qual. Heal. Res. 2016, 26, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Malterud, K. The art and science of clinical knowledge: evidence beyond measures and numbers. Lancet 2001, 358, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Malterud, K. Qualitative research: standards, challenges, and guidelines. Lancet 2001, 358, 483–488. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Overall design.

| Organized Topics | Submitted Issues |
| Dual roles | Motivation Work life balance |
| Working alone | Loneliness Working from home versus working at the office (pros & cons) Structuring administrative tasks, emails, and research tasks. |
| Employment conditions | Terms of employment (Part time/temporary employment) Insecurities towards future employment |
| Informal sparring in everyday work | Collaboration Cooperation Missing/lack of recognition Colleagueship |
| Affiliation in smaller research environments | Competitive environment Sharing knowledge Chemistry between main supervisor and PHD student New employees’ experiences of inclusion in the research environment |
Table 1.
Interview guide: Participants’ issues organized into five clustered topics.
| Organized Topics | Submitted Issues |
| Dual roles |
Motivation Work life balance |
| Working alone | Loneliness Working from home versus working at the office (pros & cons) Structuring administrative tasks, emails, and research tasks. |
| Employment conditions | Terms of employment (Part time/temporary employment) Insecurities towards future employment |
| Informal sparring in everyday work |
Collaboration Cooperation Missing/lack of recognition Colleagueship |
| Affiliation in smaller research environments | Competitive environment Sharing knowledge Chemistry between main supervisor and PHD student New employees’ experiences of inclusion in the research environment |
Table 2.
Participants characteristics.
| Participants (P#)1 | Age (years) | Sex | Education | Position | Focus Group (#) | Employed2 (Months) | ||
| P1 | 33 | Male | Physician | PHD student | 1 | 3 | 36 | |
| P2 | 53 | Female | Nurse | Adjunct | 2 | 4 | 48 | |
| P3 | 30 | Female | Nurse | PHD student | 2 | 4 | 15 | |
| P4 | 29 | Male | Physician | PHD student | 2 | 4 | 6 | |
| P5 | 39 | Male | Physician | PHD student | 1 | 3 | 15 | |
| P6 | 62 | Male | Nurse | Adjunct | 1 | 3 | 108 | |
| P7 | 31 | Female | Pharmacist | PHD student | 1 | 4 | 14 | |
| P8 | 44 | Female | Radiographer | Associated professor | 1 | 4 | 140 | |
| P9 | 32 | Female | Physician | PHD student | 2 | 4 | 24 | |
| P10 | 36 | Female | Physician | PHD student | 1 | 3 | 25 | |
| P11 | 38 | Female | Physician | PHD student | 2 | 4 | 24 | |
| P12 | 36 | Male | Physician | PHD student | 1 | 3 | 14 | |
1 All participants were dual affiliated to the University and the hospital, 2 Employed in the same hospital department.
Table 3.
Analytical process.
| Codes | Sub-Themes | Theme | Main Theme |
|---|---|---|---|
| Double workload Time management is hard with unpredictable tasks and cloudy functions The researcher’s choice has consequences and risks for individuals and patients Focus on the positive in combining research and clinic to manage stress Leadership responsibilities |
Dissolved boundaries between the two functions makes navigation necessary. Unclear task functions results in potential consequences, self-management strategies, and a need for support from leaders |
The fine line between research and clinical practice |
Lack of integration of research in clinical practice |
| Need of fellowship ‘No’ generates an internal conflict. Difficult choices affect work well-being It takes a certain someone who has certain skills |
Loneliness is decreased by sparring and collaboration Dilemmas emerge between duty and personal interest |
A wish to belong | |
| Competition drives effort and pushes to keep you going Incongruent expectations and interests Progression, workflow, and autonomy are motivational factors Structure and fellowship maintain motivation Sparring, reaching out and connecting in a broader network can be difficult, but is needed Companionship increases motivation to succeed |
Competition is a killer and a driver Reinforce motivational factors Impact of role models |
The impact of role models and motivational factors |
Table 4.
Quotations by themes.
| Themes | Quotes (samples) |
|---|---|
| The fine line between research and clinical practice | P6: Some believe that those in research and clinic go hand in hand - and that there is not much of a difference P1: I think it can be rather stressful, even though you don’t physically have to be in the clinic, you still need to do the patient work, such as their tests, and all of my patients get bloodwork done and the results end up in my mailbox. So, if you have somewhat of a conscience, then you have to be in control of the test. Even though you actually are in the middle of a week delegated for research P4: You have obligations, which applies to all with clinical research, the issue is, that we have an additional job, which has nothing to do with the clinic. P5: … It (research) should not affect the patients. P9: Time – for the clinic, those days disappear, and you cannot continue with funding application and project. On the other hand, the clinic affects research days, because there is something with a patient, which cannot wait. So, if I am not strict with time, then you are easily absorbed P5: It’s hard to say no - I frequently find myself in departments where numerous studies are incorporated into everyday practice. This blurs the distinction between being solely a clinician; suddenly, one becomes involved in research P12: It is a management task to tell the hospital department what the researcher should use their time on, and that they should not plan other tasks for the person P11: Tips could be to make a bullet journal, which clearly illustrates when to do what, but also allows for marking the tasks as completed or removing them once finished. It grants the experience of momentum |
| A wish to belong | P7: It is hard even though you are physically together – it is a feeling of loneliness, it can be lonely to sit with your own when you research different things… you sit with your own challenges P9, P3: If you are barely in the clinic, then you will not be a part of the fellowship they already have P9: I have been there two days, but I have no clue what is going on. You become an outsider P5: … That it is not just me who is researching, but it is the whole department who is researching. Everyone is part of the research – and that we remember to celebrate all our victories P3: Being in the clinic is a breather - being together with others, having one's colleagues again P5: It's important to have others whom I can casually chat with, informally discussing issues I face P2: We should not underestimate the relational aspect of formal as well as informal meetings P4: … If you want a research unit to work, then you have to put aside your own needs P3: I have accepted the fact that, even when you do it as well as you possibly can, then you still cannot do it on time P8: ... But you must be able to endure the environment |
| The impact of role models and motivational factors | P4: I believe that within the medical field, competition is everywhere, however, it is the level of competition that changes across each field of research. I worked incredibly much, also more than what I thought was comfortable, I knew I was controlled by the competition in my daily work. … Being first in the field is our goal; we aim for the highest impact. It should be the first thing published. … When I have a combined position, there are expectations from both sides regarding the clinical part and the research part P3: There is also a prioritization of what is most important in the themes one researches. It is controlled by the main supervisor's interests and the competition regarding which focus is emphasized. It would be nice if everyone had equal opportunities, including those who were not highlighted as much P8: Our positioning is at stake; we thrive on being involved and being present, and it is really tough P4: Personally, I would like a work life where I thrive, and if I keep ending up in situations where I need to say yes and no because I want to succeed with my research, then I do not think one publication can weigh up for it. It is important that I have others who I can small talk with, talk informally about the problems I face P2: Something, which I need, is constructive feedback. I do not need to hear that I am a clown. I approach people best if I feel like I have a good relationship P7: We have a fine work environment. It is the projects, i.e. advising, sparring, where we have a common ground P6: We must have a binding sense of responsibility towards each other, which is currently missing |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



