
Submitted:
19 July 2024
Posted:
23 July 2024
You are already at the latest version
Abstract
Functional neurological disorder, or FND, is widely misunderstood, particularly when considering recent research that suggests that the illness has a biological rather than a psychiatric basis. Nonetheless, the long-held view that FND is a purely psychiatric disorder without biological basis, or even a contrived (malingered) illness, remains pervasive both in modern medical care and general society. This is because FND involves an intermittent course of involuntary disability that rapidly alternates with improved neurological control. This has in turn caused shaming, low self-efficacy, and social isolation of the patients. Little research has examined the numerous biomarkers that are shared between FND and canonical neurological disorders and the encouraging outcomes that can follow conventional neurological rehabilitation, modified for this disorder. This review summarizes current research on FND biomarkers and physical rehabilitation results. General healthcare providers would benefit their care for their patients through their improved understanding the illness and recourses for support and treatment that are provided in this review.
Keywords:
functional neurological disorder
; MRI
; rehabilitation
1. Introduction
Functional neurological disorder (FND) involves involuntary, intermittent neurological symptoms or signs that vary in relation to the extent of the patient’s self-attention to the symptoms or emotional excitation. Although “FND” is the term that was most recently professionally adopted for this illness, for centuries it was addressed by many other names (hysteria, conversion disorder, psychogenic disorder, among them [1]). The recent name change was recommended in 2014 by specialists who treat FND to allay patients’ concerns for their being inappropriately diagnosed with mental disease [2]. (“Functional neurological symptom disorder” is a widely used but much less frequent synonym.)
This review will show that FND can share characteristics with canonical neurological disorders. As a result, FND itself should be considered as a neurological disorder as well. Although some reviews have stated that FND has a poor prognosis, recent rehabilitation trials have shown more favorable outcomes, which will be reviewed here. The author, a practicing and investigational neurologist, has been the medical director for the FND Clinic at the University of Alabama at Birmingham, Spain Rehabilitation Center, Birmingham, USA, for the past 7 years, having evaluated and treated more than 400 individuals with FND. This review, drawn from the author’s clinical experiences as well as current literature review, may revise the public and professional views of FND and thus help to demystify this vexing disabling illness.
2. Clinical Characteristics of FND
Although FND has been noted to have a peak age of onset at about 40 years [3,4], it can begin anytime between childhood all the way to geriatric age [5,6,7,8,9]. Any voluntary activity can be affected by FND, including limb or facial movement, speech, cutaneous or muscular perception, and vision. The patients’ self-attention to their symptoms or emotional excitement can aggravate them, while distraction from them may reduce their severity [10]. FND symptoms can be provoked by direct medical examination and subside when the patient believes not to be observed or undergoing formal evaluation [11,12,13]. The intermittent dysfunction is not apparently caused by epileptic brain discharges, transient cerebral ischemia, medication side effects, intoxication, metabolic or endocrinological diseases, systemic infection, or fatigue. As many as 18% of patients who are seen on neurological hospital wards can have FND [14].
FND has a high incidence of comorbid mood disorder, though this does not occur with all patients [9,15,16,17,18]. The disturbances are frequently considered to “mimic” canonical neurological disorders [19,20,21,22], which may lead to falsely infer that the patients contrive their symptoms. FND lacks characteristic abnormalities on clinical structural brain or spinal imaging [23,24]. Psychological care, particularly Cognitive Behavioral Therapy (CBT), can attenuate the symptoms [25]. The “conversion disorder” hypothesis for FND was postulated by the noted Austrian psychiatrist Sigmund Freud (1856-1939), in which early life trauma becomes unintentionally mentally repressed and resurfaces later as involuntary somatic complaints [26]. This perspective remains widely accepted by clinicians [27], even though the hypothesis is untestable and unproven [28]. There is consequent common stigmatization and social isolation for persons with FND [29,30]. For these reasons, FND has long been viewed by the public and clinicians as a psychiatric illness in which the patients’ mood disorder is at the root of the disturbance [31], or the symptoms are intentionally produced (malingering) [32], and it lacks a biological cause.
As far back as the 1880s, the eminent French neurologist Jean-Martin Charcot (1825-1893) considered FND (then termed hysteria) as a neurological disorder [33]. Because the fluctuating manifestation of FND led Charcot to consider that a structural brain lesion could not be responsible, the view that FND was a neurological disorder fell by the wayside for most of the 20th century because of Freud’s demonstration that FND can improve with psychoanalysis or hypnosis. However, starting nearly 30 years ago, the findings of distinct regional cerebral metabolic changes in physiological brain imaging studies in persons with FND, not found in neurologically healthy individuals [34,35], invigorated neuroscientific investigations in FND. These continue at an accelerating pace, as shown by the annual rate of publications for FND that are listed in the public registry of medical research publications, PubMed (https://pubmed.ncbi.nlm.nih.gov; Figure 1). These studies as well as those that tested other biomarkers imply, instead, that FND has a biological basis. As will be shown here, many of these biomarkers are in common with canonical neurological disorders. Moreover, rehabilitative techniques that are commonly practiced with canonical neurological disorders (e.g., stroke, spinal cord injury, traumatic brain injury) have been shown similarly to benefit FND and are detailed later.
3. Biomarkers for FND
3.1. Advanced Structural Brain Imaging Findings in FND
Structural brain MRI analysis, primarily using voxel-based morphometry, has indicated significant structural changes in brain grey areas. These findings are evident only with advanced statistical processing of brain MRI data at the patient group level and not in individuals with standard clinical brain MRI. As of now, 21 studies have evaluated morphological brain abnormalities in persons with FND (Table 1). The preponderance of volumetric brain studies in FND found reduced focal cortical or subcortical grey tissue areas when compared to individuals without FND. There was no pattern of volume loss that characterized FND.
Similarly, there has been no characteristic volume loss pattern in patients with Parkinson disease, a common neurodegenerative disease [57], even though numerous voxelwise brain grey matter analyses consistently have shown cortical atrophy [58].
As shown by Table 1, alternative, less frequent patterns also occurred: (1) both volumetric focal decrease and increase in the same study group, (2) only focal volume increase, and finally (3) no difference in brain regional volume compared to non-FND participants. Of note also is that for dystonia, for which there is evidence that it is a neurodegenerative disease [59], and Alzheimer disease, a leading neurodegenerative disease [60], quantitative brain morphological assessment has shown both focal decreased and increased volumes in the same populations [61,62]. Thus, strictly focal brain regional volume decrease is not characteristic of canonical neurodegenerative illness.
3.2. Genetic Analyses
Genetic bases for several neurodegenerative disorders have been identified, although these diseases more often are sporadic than familial. In Parkinson disease 90 genetic risk factors have been identified [63]. Hereditability for multiple sclerosis has been well described [64]; the HLA DRB1*1501 haplotype has been most significantly associated with increased risk for the disease, among more than 200 other genes [65]. The finding of numerous genetic mutations in forms of dystonia in the later 20th century changed the neuroscientific view of dystonia from earlier decades that it had a psychiatric etiology to being a neurological disorder [66,67].
In contrast to this considerable body of study, research for specific genotypes in FND has markedly lagged. A tryptophan hydroxylase 2 gene polymorphism—G703T—has been shown to predict early age onset of FND [68]. Functional seizures, also called paroxysmal or psychogenic nonepileptic seizures, are generally considered to be a kind of FND. Such seizures are associated with polymorphisms of the FKBP5 gene, but only when co-occurring with depression [69].
3.3. Low-Grade Inflammatory Biomarkers
Inflammatory biomarkers have been identified in diverse neurodegenerative disorders. Recurrent inflammation of the central nervous system is well known to be a major determinant of disability in multiple sclerosis [65]. Chronic inflammation in the central nervous system in this disease contributes to neurodegeneration through impairing remyelination [70]. Evidence of low-grade nervous system inflammation has been recently found in other neurodegenerative diseases, including Parkinson disease, Huntington disease, and amyotrophic lateral sclerosis, based on either measuring serum pro-inflammatory cytokines or identifying increased microglial activation in the brain on positron emission tomography [71,72].
Recent research has identified elevated serum cytokines as well in persons with FND, in particular, IL6, IL12, IL17A, IFNg, TNFa and VEGF-a [73]. Elevated serum C-reactive protein levels have been identified in children and adolescents with FND [74]. These findings thus far have not led to successful pharmacological trials for inflammatory modifiable agents for FND.
3.3. Autonomic Disturbance in Canonical Neurological Disease and FND
In some canonical neurological disorders, specific autonomic disturbances have been found that are shared with FND, which are discussed here.
3.3.1. Increased Cardiac Contraction Rate
Tachycardia has been rarely characteristic in specific canonical neurological disorders. Mitochondrial membrane-associated neurodegeneration (MPAN) is a rare disorder that has been described only in the 21st century. It is typified by iron accumulation in the basal ganglia, progressive cognitive decline, spasticity, dysarthria, dystonia, and optic atrophy [75]. Mean onset is at age 10 years. Cerebral atrophy has been described in a subset of the patients. About 30% of MPAN patients have cardiac disease, including cardiomyopathy, arrhythmia, and sustained tachycardia [76]. Orthostatic tachycardia has been found in patients with multiple system atrophy, another neurodegenerative disorder (described further below) [77]. A subset of patients with functional movement disorder are found also to have elevated heart rate at rest, including the Postural Orthostatic Tachycardia Syndrome (POTS), compared to neurologically healthy control subjects [78,79,80]. Several patients in the present author’s FND clinic have been diagnosed with POTS by their cardiologists.
3.3.2. Superficial Tissue Blood Flow and Temperature Changes
Cool and dusky appearance of the distal limbs (the “cold hand sign”) is a characteristic of multiple system atrophy and less often in other neurodegenerative disorders [81,82,83,84,85]. On clinical examination, multiple system atrophy is diagnosed by combined limb rigidity, bradykinesia, postural instability, ataxia, and autonomic nervous system disturbance. Average age of onset is 53 years. Longitudinal structural MRI studies of patients with multiple system atrophy demonstrate progressive degeneration in the putamen or the pons [86]. Longitudinal follow-up on clinical examination demonstrates progression on the Unified Multiple System Atrophy Rating Scale; mean interval between diagnosis and death is 69 months [87].
FND has been reported not to occur in multiple system atrophy [88]. However, in his FND clinic, in recent years patients have brought to this author’s attention of acute, intermittent distal limb dusky discoloration. The author began prospectively to evaluate the color of the patients’ limbs in the clinic with photography. In a preliminary report at the 2022 meeting of the Functional Neurological Disorder Society in Boston, the author observed “purple feet” in 17% of 89 consecutive patients diagnosed with FND [89]. Since that time, the author has observed the phenomenon to be even more frequent, and it is under further study.
The phenomenon resembles closely the “cold hand sign” of multiple system atrophy, as vividly illustrated by Klein et al [83]. The disturbance in the author’s FND patients is more evident in the feet than in the hands; it can be recognized in some cases at the forearms and the knees as well. The patients seldom volunteer the notice of this disturbance and usually are not bothered by it. The discoloration increases after a few minutes at repose with the lower extremities in a dependent position. There is usually no edema and only rarely somatosensory discomfort. In functional hemiparesis the disturbance is unilateral and ipsilateral to the paretic limbs. Often the distal limbs are cool to touch, and in some cases, they have hyperhidrosis. After mild manual compression of the dorsal surfaces of the hands or the feet, the blanching may require as much as 10 seconds to return to baseline. The phenomenon suggests delayed capillary refilling, which also was observed in multiple system atrophy [90]. There is no age dependency for the phenomenon in the author’s FND clinic.
Figure 2 shows purple feet in a young patient seen in the author’s FND clinic. The 18-year-old woman had been followed in the clinic since the prior year. She and her father reported frequent episodic loss of consciousness and staring, with unremarkable EEG; also episodes of poor concentration, partial ptosis of the right eye, and sense of ocular vibration. Her 40-year-old mother had been followed in the same clinic for two years, for the 12-year-history of episodic sense of head vibrating, visual loss, limb paresthesias, bilateral ankle intorsion, and diplopia, with on examination episodic facial flushing, leg tremor only during examination, and prolonged capillary refilling in the feet after light digital compression.
There have been no published instances of this phenomenon in FND. Of note, the distinguished British neurologist Samuel Alexander Kinnier Wilson (1878-1937), who rejected the psychiatric basis for FND, described a patient with functional paraplegia and lower extremity analgesia [91]. Not only did the patient fail to sense the pushing of a needle through the calf, but also no bleeding followed. But when the patient regained skin sensation after the examiner applied a wire brush to the leg, bleeding followed from pin prick. This phenomenon has not been replicated.
Rarely the phenomenon is painful. Figure 3 shows self-taken photographs by a second patient from the author’s FND clinic. The 20-year-old woman had been followed in the FND clinic for the prior year for the four-year complaint of episodic loss of consciousness of uncertain etiology, induced by emotional upset and variable paraparesis. The brain MRI scan was unremarkable. After a year of follow-up, she urgently notified the author of the acute painful and stiff left hand, along with discoloration (Figure 3A). The phenomenon was self-photographed and forwarded to the author. The author urged that the patient to be seen by her local emergency department to rule-out peripheral vascular insufficiency. Work-up in the emergency department demonstrated normal peripheral arterial flow as evaluated by ultrasonic evaluation, and the patient was advised to return to home. The disturbance subsided after a day without specific treatment.
The patient subsequently e-mailed to the author of complaint of another peculiar finding that co-occurred with the hand complaint, which was an elongated roughly linear area of depigmentation that was vertically oriented along her abdomen and not painful (Figure 3B). This also dissipated after a day. The author forwarded the images to the chairman of the section of rheumatology at his university for an opinion, who could not recognize the etiology. The patient continues to be followed for variable paraparesis and sustained delayed pedal capillary refilling after manual compression.
3.3.3. Gastrointestinal Motility Disturbances
Irritable bowel syndrome (IBS) refers to motility difficulties that can include irregular defecation and abdominal pain, without finding structural tissue abnormalities on standard imaging or scoping procedures after excluding inflammatory bowel disease [92]. IBS is common in FND [93,94]. Many patients in the author’s practice complain of reduced ease of esophageal passage of food or pills, which is termed “globus pharyngeus,” formerly called “globus hystericus” [95]. Similarly, various forms of functional (physiological) gastrointestinal motility impairments occur commonly in Parkinson disease, as much as 65% of patients, and the symptoms often long precede the onset of limb motor disturbances [96]. A similar proportion occurs in multiple sclerosis [97].
3.3.4. Joint Hypermobility Disturbances
In recent years this author has noted that many clinic patients diagnosed with FND have hypermobile upper extremity joints (Figure 4), and less often in the hips and distal lower extremity limbs. In the upper limbs, these findings have not disturbed their activities in the patients encountered in this clinic. When these patients were referred for formal orthopedic or rheumatologic evaluation for possible Ehlers-Danlos syndrome, a multiple organ disorder that includes excess joint laxity, these were generally ruled out.
Concurrent with these observations, an unusually high prevalence (55%) of joint hypermobility was reported in a sample of 20 FND patients in a separate investigation [98].
The association between joint hypermobility and other neurological disorders has not been comprehensively examined, most likely in part because joint hypermobility is given little attention in formal medical training, and the finding is widely regarded as benign [99]. This latter view may overlook multiple organ dysfunction that frequently accompanies joint hypermobility, including gastrointestinal motility and cardiovascular autonomic disturbances.
Although general laxity of connective tissues could mechanically contribute to neurological disturbances due to compression of central nervous tissue, including from low-lying cerebellar tonsils in the type I Chiari malformation [100] and spinal instability [101], as have been identified, other neurological disturbances have no clear relationship to mechanical tissue disturbances. A case report of Ehlers-Danlos syndrome identified co-existing limb myopathy on electromyography and ophthalmoplegia [102]. A sample of 90 individuals who scored abnormally high on a joint mobility assessment were found to have significantly reduced visual-evoked potentials latencies and amplitudes compared to individuals without excess hypermobility [103]. Joint hypermobility therefore can be a biomarker for extensive multiple organ dysfunctions.
3.3.5. Behavioral Biomarkers of FND Shared With Canonical Neurodegenerative Disorders
Clinical Blending between FND and Canonical Neurological Disease
Compelling research suggests that functional movement disorder can often evolve to canonical neurodegenerative disease. In medical chart review, 26% of patients who were diagnosed with Parkinson disease (n = 53 total) had earlier developed FND [104]. An additional 8% of Parkinson disease patients had concurrent FND, and most of the Parkinson disease patients (57%) later developed FND. Similarly, Onofrj et al as well as Pareés et al in many instances observed FND to progress to either Parkinson disease or dementia with Lewy bodies [88,105,106]. Elsewhere, three cases of Creutzfeldt-Jakob disease were reported to have initially presented with functional movement disorder [107]. The present author had observed this as well in a 62-year-old man in his clinic, diagnosed initially with functional movement disorder, and then Creutzfeldt-Jakob disease was diagnosed a few months later. He succumbed to the disease two months after the latter diagnosis was made, following rapid neurological decline. In another patient from the clinic, an 18-year-old woman diagnosed with FND has shown in serial photography over 12 months progression to fixed unilateral intorsion ankle dystonia (Figure 4). When most recently seen, the patient wanted to defer a trial of botulinum toxin administration, pending evaluation by her orthopedic surgeon.
Figure 4.
Progressive dystonia resulting in involuntary, fixed ankle intorsion of the right foot. Note also rubor of the same extremity, unlike the other foot. Bandage was worn because dystonia induced chafing with her customary footwear.
Figure 4.
Progressive dystonia resulting in involuntary, fixed ankle intorsion of the right foot. Note also rubor of the same extremity, unlike the other foot. Bandage was worn because dystonia induced chafing with her customary footwear.

Emotional Upset Effects on Symptoms
Emotional upset often provokes symptoms in FND [108]. Similarly, motor symptoms in Parkinson disease can be aggravated by anxiety or other emotional upset [109,110]. Anxiety or depression have been associated with worse performance on a standard test of visual information processing speed among persons with multiple sclerosis [111,112,113,114,115]. Fear of falling can aggravate postural control and gait control among persons with multiple sclerosis [116,117]. High anxiety is a risk factor for dystonic progression that starts with blepharospasm (involuntary contraction of eyelids) to other parts of the body [118].
Exaggeration of Symptoms
In a study by Pareés et al, persons with FND (n = 8) were noted to self-report limb tremor more often than was captured by objective recordings of wrist-worn accelerometers worn in the home [119]. This finding suggests that persons with FND are prone to accentuated self-attention to their bodies, leading to their increased somatic complaints. This mismatch was greater than in a group of patients with “organic” tremor (not otherwise specified; n = 8) who wore the same instruments. Nonetheless, the latter group also exaggerated their time with tremor when compared to the accelerometry data, thus showing that there is not an absolute difference between persons with FND compared to those with “organic” tremor with regard to symptom reporting.
A subsequent, slightly larger study by Kramer et al, using similar methods, found that while persons with FND reported more tremor disturbance than did persons with “organic” tremor, the self-reported “symptom burden” between persons with FND (n = 14) and those specifically with Parkinson disease (n = 6) did not differ [120]. The persons with “organic” tremor (including those with essential tremor, Parkinson disease, and other forms) were objectively recorded to have spent more time in tremor than in those with FND, but the differences were slight. Though the findings did not support symptom exaggeration differences between persons with FND and those with other forms of tremor, it should be noted that the study was based on a small subject sample. These results, however, suggest that the differences between persons with FND vs those with Parkinson disease are minimal with respect to subjective motor symptom impact.
Expectation Effects on Symptoms
The research literature on FND extensively suggests that it is sensitive to suggestibility, i.e., placebo effects, though the studies appear to have had poor experimental design [121]. As far back as 1880, Charcot applied hypnotic suggestion to modify symptoms in persons with FND [122]. Nonetheless, such suggestibility effects are by no means restricted to FND. Placebo effects (expectation to improve) and the obverse, nocebo effects (expectation to worsen), are widely demonstrated in persons with Parkinson disease in reaction to treatments [123]. Low expectation can deter persons with Parkinson disease from pursuing physical exercise [124]. Similar effects are noted in many other involuntary movement disorders, including restless legs syndrome, Huntington disease, tics, amyotrophic lateral sclerosis, and multiple system atrophy [125,126,127].
Context-Specific Changes on Walking Ability
Patients with FND can improve their mobility during their formal rehabilitation by changing the method of locomotion. For example, an FND patient with impaired walking can improve by gliding the feet across the floor instead of lifting, as if moving across a slippery surface [128]. Starting with a more stable form of locomotion, more complex activities can be gradually introduced as part of rehabilitation, which is described further below. Persons with Parkinson disease likewise can change their ability of locomotion by adopting different movement approaches or patterns. Walking backwards or running can improve motor control in Parkinson disease, Huntington disease, or dystonia [129]. Freezing of gait in Parkinson disease can be improved with shoes that project laser points of light in front of the wearer or crawling on all four limbs [130,131]. Rhythmic auditory cues can improve voluntary movement in both Parkinson disease and FND [132,133]. Parkinson disease patients with freezing of gait may easily locomote by pedaling a bicycle on a street [134].
Competing Voluntary Activities that Can Reduce Symptoms
As noted under Section 2, Clinical characteristics of FND above, redirecting attention in persons with FND can ameliorate their symptoms [10]. Similar effects may occur with canonical neurological disorders. Classically, dystonia includes brief amelioration of the motor symptom through a self-initiated voluntary action by the patient, most often, touching a specific part of the body. This behavior is commonly referred to as a “sensory trick” or “geste antagoniste” [135]. Although most often such gestes are simple, an inventory of such gestes shows that they can involve a wide variety of actions, including bending forward, yawning, wearing a scarf, cap, turban, or tight goggles, leaning on one’s elbows, picking at one’s teeth, singing, humming, drinking, kissing, whistling, chewing gum, laughing, piano playing, thinking about talking, running in a counterclockwise direction, listening to a loud radio, mirror viewing, or voluntary eye closure [136]. Such diversity raises consideration that these ameliorative actions may reflect the beneficial effect of redirecting attention from the predominant symptom, as suggested in the overviews of FND and Parkinson disease above.
Cognitive Impairments
Cognitive impairments are common following canonical brain disease, as can be expected. These can also occur with FND. Among them are impaired memory [137], reduced processing speed [138,139,140,141], abnormal executive function [141,142,143,144,145], and impaired Theory of Mind (social cognition) [146,147].
Positive Response to Psychotherapy on Motor Symptoms
CBT, a form of psychotherapy, is a leading treatment for FND [148]. The treatment identifies events that trigger symptoms, diminishes attention to the impairment, redirects attention to better retained voluntary activities, cultivates self-efficacy, reduces emotional upset, and develops mindfulness (concentrating on current emotions and not focusing on events in the past or the future) [108]. The approach can reduce tremor severity and other motor symptoms in FND [149,150]. Although CBT is provided to persons with Parkinson disease mainly to control their mood disorders, preliminary findings indicate that the approach can also improve their walking [151].
Lower Extremity Dysesthesia and Compulsion To Move The Limbs
Restless legs syndrome involves annoying leg sensations (pain, tightness), most often while the patient is recumbent, and the compulsion to move the legs for relief. Increased leg movements also can occur in restless legs syndrome without leg discomfort, particularly during sleep. The worldwide prevalence is about 3% [152]. In a minority of patients with restless legs syndrome (10%), symptoms worsen over 5 years [153]. Restless legs syndrome considerably occurs in canonical neurological movement disorders, including Parkinson disease, multiple system atrophy, and multiple sclerosis [154,155]. Recent quantitative brain MRI studies of restless legs syndrome have shown significant thinning of the cerebral cortex and regional white matter atrophy [156,157], suggesting that it is a neurodegenerative disorder.
Until the quantitative neuroimaging studies referred to above were published, restless legs syndrome was regarded primarily to be a “functional” (that is, physiological) disorder [158]. In a recent study of 96 individuals with functional movement disorder, the incidence of restless legs syndrome according to formal screening criteria was 44%, compared to 8% in neurologically healthy controls [159]. The complaint of restless legs (either nocturnal dysesthesia or the urge to move the legs, confirmed by overnight sleep study) is common in the patients who are seen in the present author’s FND clinic.
4. Rehabilitation for FND
Until recent years, the long-term prognosis for FND was considered to be dismal [160,161,162]. Although numerous biomarkers for FND have been identified, these findings have not thus far indicated a consistently efficacious medical treatment for its impaired voluntary activities.
However, neurological rehabilitation has shown promise for controlling the symptoms of FND. In recent years there has been increasing interest, developing, and testing neurological rehabilitation for FND, and moving from case series reports to larger clinical trials.
The greatest advances have been in applying neurological rehabilitation toward controlling motor symptoms. Table 2 summarizes trials in chronological order up to the present that applied physical rehabilitation techniques for >5 patients with functional movement disorders. This summary encompasses more than 1300 individuals (mostly adults, but also children) who were treated and followed for the durations of the trials.
The published studies generally had favorable outcomes, and in many cases, gains retained over months or years. A considerable limitation among the studies has been the common lack of comparing one treatment to another in groups that were matched for the degree of disability. In addition, in most reports patient groups had diverse symptoms that were targeted for treatment, leaving unclear whether treatment outcomes depended on the individual symptoms treated.
Although the approaches somewhat differed from each other, a common approach was to start with having patients practice voluntary movements that can be performed with little difficulty, and then advance gradually through more complicated movements, with praise at every stage of accomplishment [194]. This is subsumed under the term “shaping” [170,187,195,196,197], which has been used in specific forms of physical rehabilitation (e.g., Constraint-Induced Movement therapy) for canonical neurological disorders, including stroke, cerebral palsy, traumatic brain injury, and multiple sclerosis [198,199,200,201]. In addition, because FND symptoms are affected by self-attention to the deficits, the rehabilitation techniques emphasized increasing general physical activity without drawing attention to the particular part of the body or context, which could aggravate the symptoms. An example for the effect of attention on an FND deficit is the Hoover sign [202]. This involves the inability to extend a hemiparetic leg following direct command while supine or seated, but can occur when the patient is asked to redirect self-attention to the opposite leg and elevate it. In that case, the affected leg’s extension is necessary to stabilize the pelvis during the maneuver. Such a demonstration of retained movement capability when self-attention is redirected can serve as a foundation for rehabilitation.
5. Other Treatments
To a lesser extent, other treatments for FND have been investigated. Because these methods are early in their development, the treatment results are not provided here. The methods have included CBT alone [149], hypnosis [203], and transcranial magnetic stimulation [204]. Although various psychotropic medications have been tried for FND and can help to manage mood disorder, there is thus far no leading efficacious pharmacological treatment for the FND symptoms themselves [205,206].
6. Discussion
The purpose of this review is to amply demonstrate that FND, a much misunderstood illness, shares many objective laboratory and clinical characteristics with canonical neurological disease. Moreover, conventional neurological rehabilitation techniques can ameliorate FND symptoms. This review thus intends to demystify the illness and encourage clinical practitioners to approach FND patients empathetically and supportively. This evidentiary foundation allows practitioners to indicate to their patients that (1) the illness is not a psychiatric disorder, and thus to discard the unsupported implication that it can corrupt reality testing, and (2) the illness can respond positively to rehabilitation techniques that are similarly applied to other neurological disorders. In doing so, this review aims to bring FND into mainstream neurological care, to regard it as a neurological disease, and not to treat it as a fringe, exotic, or mysterious illness.
Even more important, the many biomarkers that FND shares with multiple other neurological disoders should prompt clinicians who evaluate and treat FND to be aware of and routinely evaluate for its multiple organ comorbidities. The constellation of autonomic, cardiovascular, immunological, gastroenterological, and orthopedic disturbances are not unique to FND. In recent research, this pattern also was found to be common in patients who presented with gastrointestinal motility disturbances that lacked observable tissue pathology, who were not noted to have FND [207]. Consequently, treating an FND patient warrants investigating these possible other disturbances and consult specialists in these areas as needed. The diverse biomarkers also suggest that FND may not strictly be a neurological disorder. As yet, although there is no clear physiological or developmental process in common with these disturbances that may also underlie FND, these findings should encourage further hypothesis development and clinical investigation to clarify the pathological process that is involved with FND.
Evaluating and directing treatment for FND requires the expertise of a neurologist, owing to the complexity of the symptoms [208,209,210,211]. The optimal management of FND would start with accurate diagnosis. However, there are many difficulties with doing so:
- There is no gold standard for diagnosing FND. In our review of studies of FND biomarkers [212], we found that there are three main rival methods: the Fahn-Williams method and its variants [192], the method outlined in the various editions of the Diagnostic and Statistical Manual of Mental Disorders [213], and the referring physician’s personal judgement. Without a consensus diagnostic method for FND, rapid progress in research for treatment will likely be hindered.
- Seldom considered has been the extensive list of alternate paroxysmal neurological disorders that are not known to be affected by self-attention or emotional excitation, and which lack distinctive features on conventional clinical neuroimaging. These include frontal lobe epilepsy, paroxysmal dyskinesia, and autoimmune encephalitis [214]. This list obliges the involvement of a neurologist who is highly experienced with assessing FND (indicated above) vs. the alternate neurological disorders, thus to direct the patient to appropriate management.
- Even when a neurologist with expertise in FND may be involved, current clinical practice often limits the time to evaluate new patients to 30 minutes, due to economic pressures and meeting the demands of a large practice [214]. In contrast, as much as an hour is necessary to conduct a thorough historical intake and comprehensive neurological evaluation, and provide empathetic patient and family education and care planning. Furthermore, the patient’s concurrent cognitive limitations (described in section 3.3.5.7) can limit or slow these steps. As a result, the modern medical practice milieu may prolong evaluating and ultimately arranging care for persons who may have FND or other paroxysmal disorders.
- Even with involving a neurologist who is expert with FND, optimal care, including treatment by a neuropsychologist and rehabilitative physical therapists, occupational therapists, or speech-language pathologists, can be limited because of the relatively few medical centers that can provide these services with commensurate expertise with FND. Consequently, there can be a considerable waitlist for patients to be seen, along with the hardship for arranging travel to such places.
To assist the management by the clinician who initially sees persons who may have FND, the web site FND Hope - FND Hope International (https://fndhope.org) lists such centers that have the available expertise. In addition, referring the patient and family to the web site https://neurosymptoms.org/en/ can acquaint them with the diverse appearances and complexities of FND. Doing so can equip them with the knowledge to better understand the illness, which in turn could help to reduce the time for evaluation and allay concerns that the illness is not a mental disorder or a different neurological disorder with episodic symptoms, such as multiple sclerosis [215,216].
7. Conclusions
This overview of the biomarkers and responses to conventional neurological rehabilitation for FND demonstrates that it is a neurological disorder. Consequently, the patient should be approached with this in mind, following appropriate diagnosis. Becoming familiar with the content of this review can prepare the clinician to approach the patient with confidence that FND is not an unknowable, enigmatic disorder, and that optimism should be conveyed to guide patients to improved self-control of their symptoms with competent rehabilitation.
Funding
This research was funded by the National Institute of Health, grant number AG070049.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the University of Alabama at Birmingham, protocol 300009775, approved 1 March 2023.
Informed Consent Statement
Informed consent was obtained from all subjects whose photographs were included in this article, including agreement for such images that are to be published for this paper.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Hassan, J.; Taib, S.; Yrondi, A. Structural and functional changes associated with functional/dissociative seizures: a review of the literature. Epilepsy Behav 2024, 152, 109654. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.J.; Stone, J.; Lang, A.E. From psychogenic movement disorder to functional movement disorder: it's time to change the name [review]. Mov Disord 2014, 29, 849–852. [Google Scholar] [CrossRef] [PubMed]
- Gilmour, G.S.; Jenkins, J.D. Inpatient treatment of functional neurological disorder: a scoping review. Can J Neurol Sci 2021, 48, 204–217. [Google Scholar] [CrossRef] [PubMed]
- Lidstone, S.C.; Costa-Parke, M.; Robinson, E.J.; Ercoli, T.; Stone, J. Functional movement disorder gender, age and phenotype study: a systematic review and individual patient meta-analysis of 4905 cases. J Neurol Neurosurg Psychiatry 2022, 93, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Snijders, A.H.; van de Warrenburg, B.P.; Giladi, N.; Bloem, B.R. Neurological gait disorders in elderly people: clinical approach and classification [review]. Lancet Neurol 2006, 6, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Cuénod, P.; Smaga, D.; Degive, C.; Della Santa, D.R. La main spastique psychogène. Ann Chir Main Memb Super 1996, 15, 100–108, [in French]. [Google Scholar] [CrossRef]
- LaFrance, W.C.; Baker, G.A.; Duncan, R.; Goldstein, L.H.; Reuber, M. Minimum requirements for the diagnosis of psychogenic nonepileptic seizures: a staged approach: a report from the International League Against Epilepsy Nonepileptic Seizures Task Force. Epilepsia 2013, 54, 2005–2018. [Google Scholar] [CrossRef] [PubMed]
- Geroin, C.; Petracca, M.; Di Tella, S.; Marcuzzo, E.; Erro, R.; Cuoco, S.; Ceravolo, R.; Mazzucchi, S.; Pilotto, A.; Padovani, A.; et al. Elderly onset of functional motor disorders: clinical correlates from the Italian registry. Mov Disord Clin Pract 2024, 11, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Perjoc, R.S.; Roza, E.; Vladacenco, O.A.; Teleanu, D.M.; Neacsu, R.; Teleanu, R.I. Functional neurological disorder—old problem new perspective [review]. Int J Environ Res Public Health 2023, 20, 1099. [Google Scholar] [CrossRef] [PubMed]
- Mark, V.W. Functional neurological disorder: extending the diagnosis to other disorders, and proposing an alternate disease term—Attentionally-modifiable disorder. NeuroRehabilitation 2022, 50, 179–207. [Google Scholar] [CrossRef] [PubMed]
- Araújo, R.; van de Warrenburg, B.; Lang, A.; Lees, A.; Bloem, B.R. The Waiting Room: neurological observations made outside the movement disorder specialist's consulting office. Pract Neurol 2019, 19, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.P.; Teasell, R.W. Behavioural interventions in the rehabilitation of acute v. chronic non-organic (conversion/factitious) motor disorders. Br J Psychiatry 2004, 185, 140–146. [Google Scholar] [CrossRef]
- Gooch, J.L.; Wolcott, R.; Speed, J. Behavioral management of conversion disorder in children. Arch Phys Med Rehabil 1997, 78, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Ramsay, N.; Stone, J.; Fadiloglu, K.; Baxter, M.; Hutchison, C.; Bennett, K.; Moullaali, T.; Mathur, J.; Bridson, J.; Hoeritzauer, I. Functional neurological disorder: a common reason for a neurology inpatient referral. Eur J Neurol 2023, 30, 3886–3889. [Google Scholar] [CrossRef] [PubMed]
- Kathol, R.G.; Cox, T.A.; Corbett, J.J.; Thompson, H.S. Functional visual loss. Follow-up of 42 cases. Arch Ophthalmol 1983, 101, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Tinazzi, M.; Geroin, C.; Marcuzzo, E.; Cuoco, S.; Ceravolo, R.; Mazzucchi, S.; Pilotto, A.; Padovani, A.; Romito, L.M.; Eleopra, R.; et al. Functional motor phenotypes: to lump or to split? J Neurol 2021, 268, 4737–4743. [Google Scholar] [CrossRef] [PubMed]
- van der Hoeven, R.M.; Broersma, M.; Pijnenborg, G.H.; Koops, E.A.; van Laar, T.; Stone, J.; van Beilen, M. Functional (psychogenic) movement disorders associated with normal scores in psychological questionnaires: a case control study. J Psychosom Res 2015, 79, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Asadi-Pooya, A.A.; Farazdaghi, M.; Asadi-Pooya, H.; Fazelian, K. Depression, anxiety, stress, and suicide risk in patients with functional seizures vs. those with epilepsy. Acta Neurol Belg in press.
- Simhan, S.; Thijs, V.; Mancuso, S.; Tsivgoulis, G.; Katsanos, A.; Alexandrov, A.V.; Kanaan, R.A. The outcome of acute functional neurological disorder: a meta-analysis of stroke-mimic presentations [review]. J Neurol 2020, 267, 1353–1357. [Google Scholar] [CrossRef] [PubMed]
- Ryznar, E.; Wilcox, D. Functional coma: two case reports and a review of the literature. Psychosomatics 2019, 60, 343–351. [Google Scholar] [CrossRef]
- Trimble, M.; Reynolds, E.H. A brief history of hysteria: from the ancient to the modern. Handb Clin Neurol 2016, 139, 3–10. [Google Scholar] [PubMed]
- Stone, J.; Reuber, M.; Carson, A. Functional symptoms in neurology: mimics and chameleons [review]. Pract Neurol 2013, 13, 104–113. [Google Scholar] [CrossRef]
- Keane, J.R. Hysterical gait disorders. 60 cases. Neurology 1989, 39, 586–589. [Google Scholar] [CrossRef] [PubMed]
- Heruti, R.J.; Reznik, J.; Adunski, A.; Levy, A.; Weingarden, H.; Ohry, A. Conversion motor paralysis disorder: analysis of 34 consecutive referrals. Spinal Cord 2002, 40, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Gutkin, M.; McLean, L.; Brown, R.; Kanaan, R. Systematic review of psychotherapy for adults with functional neurological disorder. J Neurol Neurosurg Psychiatry 2021, 92, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Freud, S. Über den psychischen Mechanismus hysterische Phänomene: vorläufige Mittelung. In Studien über Hysterie und anderen Werke aus den Jahren 1892-1899; S. Fischer Verlage: Frankfurt, 1899; pp. 81–98, [in German]. [Google Scholar]
- Kanaan, R.A.; Armstrong, D.; Wessely, S.C. Neurologists' understanding and management of conversion disorder. J Neurol Neurosurg Psychiatry 2011, 82, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Carson, A.; Ludwig, L.; Welch, K. Psychologic theories in functional neurologic disorders [review]. Handb Clin Neurol 2016, 139, 105–120. [Google Scholar] [PubMed]
- Milano, B.A.; Moutoussis, M.; Convertino, L. The neurobiology of functional neurological disorders characterised by impaired awareness [review]. Front Psychiatry 2023, 14, 1122865. [Google Scholar] [CrossRef] [PubMed]
- McLoughlin, C.; McGhie-Fraser, B.; Carson, A.; Olde Hartman, T.; Stone, J. How stigma unfolds for patients with Functional Neurological Disorder. J Psychosom Res 2024, 181, 111667. [Google Scholar] [CrossRef]
- Joos, A.; Herrmann, C.; Lahmann, C.; Flottman, M.; Jansen, T.; Schede, C.; Maner, P.; Schorner, K.; von Husen, D.K.; Jobges, M.; et al. Biopsychosocial complexity in functional neurological disorder. Gen Hosp Psychiatry 2023, 84, 44–46. [Google Scholar] [CrossRef] [PubMed]
- MacDuffie, K.E.; Grubbs, L.; Best, T.; LaRoche, S.; Mildon, B.; Myers, L.; Stafford, E.; Rommelfanger, K.S. Stigma and functional neurological disorder: a research agenda targeting the clinical encounter. CNS Spectr 2021, 26, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Raynor, G.; Baslet, G. A historical review of functional neurological disorder and comparison to contemporary models. Epilepsy Behav Rep 2021, 16, 100489. [Google Scholar] [CrossRef] [PubMed]
- Varma, A.R.; Moriarty, J.; Costa, D.C.; Gaćinovic, S.; Schmitz, E.B.; Ell, P.J.; Trimble, M.R. HMPAO SPECT in non-epileptic seizures: preliminary results. Acta Neurol Scand 1996, 94, 88–92. [Google Scholar] [CrossRef] [PubMed]
- Vuilleumier, P.; Chicherio, C.; Assal, F.; Schwartz, S.; Slosman, D.; Landis, T. Functional neuroanatomical correlates of hysterical sensorimotor loss. Brain 2001, 124, 1077–1090. [Google Scholar] [CrossRef] [PubMed]
- Atmaca, M.; Aydin, A.; Tezcan, E.; Poyraz, A.K.; Kara, B. Volumetric investigation of brain regions in patients with conversion disorder. Prog Neuropsychopharmacol Biol Psychiatry 2006, 30, 708–713. [Google Scholar] [CrossRef] [PubMed]
- Atmaca, M.; Baykara, S.; Mermi, O.; Yildirim, H.; Akaslan, U. Pituitary volumes are changed in patients with conversion disorder. Brain Imaging Behav 2015, 10, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Labate, A.; Cerasa, A.; Mula, M.; Mumoli, L.; Gioia, M.C.; Aguglia, U.; Quattrone, A.; Gambardella, A. Neuroanatomic correlates of psychogenic nonepileptic seizures: a cortical thickness and VBM study. Epilepsia 2012, 53, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Weber, S.; Bühler, J.; Vanini, G.; Loukas, S.; Bruckmaier, R.; Aybek, S. Identification of biopsychological trait markers in functional neurological disorders. Brain 2023, 146, 2627–2641. [Google Scholar] [CrossRef]
- Perez, D.L.; Matin, N.; Williams, B.; Tanev, K.; Makris, N.; LaFrance, W.C.; Dickerson, B.C. Cortical thickness alterations linked to somatoform and psychological dissociation in functional neurological disorders. Hum Brain Mapp 2018, 39, 428–439. [Google Scholar] [CrossRef] [PubMed]
- Perez, D.L.; Matin, N.; Barsky, A.; Costumero-Ramos, V.; Makaretz, S.J.; Young, S.S.; Sepulcre, J.; LaFrance, W.C.; Keshavan, M.S.; Dickerson, B.C. Cingulo-insular structural alterations associated with psychogenic symptoms, childhood abuse and PTSD in functional neurological disorders J Neurol Neurosurg Psychiatry 2017, 88, 491-497.
- Nicholson, T.R.; Aybeck, S.; Kempton, M.J.; Daly, E.M.; Murphy, D.G.; David, A.S.; Kanaan, R. A structural MRI study of motor conversion disorder: evidence of reduction in thalamic volume. J Neurol Neurosurg Psychiatry 2014, 85, 227–229. [Google Scholar] [CrossRef]
- Tomic, A.; Agosta, F.; Sarasso, E.; Petrovic, I.; Basaia, S.; Pesic, D.; Kostic, M.; Fontana, A.; Kostic, V.S.; Filippi, M. Are there two different forms of functional dystonia? A multimodal brain structural MRI study. Mol Psychiatry 2020, 25, 3350–3359. [Google Scholar] [CrossRef] [PubMed]
- Espay, A.J.; Maloney, T.; Vannest, J.; Norris, M.M.; Eliassen, J.C.; Neefus, E.; Allendorfer, J.B.; Lang, A.E.; Szaflarski, J.P. Impaired emotion processing in functional (psychogenic) tremor: a functional magnetic resonance imaging study. Neuroimage: Clinical 2018, 17, 179–187. [Google Scholar] [CrossRef]
- Tatekawa, H.; Kerr, W.T.; Savic, I.; Engel, J.; Salamon, N. Reduced left amygdala volume in patients with dissociative seizures (psychogenic nonepileptic seizures). Seizure 2020, 75, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Liu, X.; Zhao, X. Neuroimaging studies in peristent postural-perceptual dizziness and related disease: a systematic review. J Neurol 2022, 269, 1225–1235. [Google Scholar] [CrossRef] [PubMed]
- Kerr, W.T.; Tatekawa, H.; Lee, J.K.; Karimi, A.H.; Sreenivasan, S.S.; O'Neill, J.; Smith, J.M.; Hickman, L.B.; Savic, I.; Nasrullah, N.; et al. Clinical MRI morphological analysis of functional seizures compared to seizure-naive and psychiatric controls. Epilepsy Behav 2022, 134, 108858. [Google Scholar] [CrossRef]
- Maurer, C.W.; LaFaver, K.; Limachia, G.S.; Capitan, G.; Ameli, R.; Sinclair, S.; Epstein, S.A.; Hallett, M.; Horovitz, S.G. Gray matter differences in patients with functional movement disorders. Neurology 2018, 91, e1870–e1879. [Google Scholar] [CrossRef] [PubMed]
- Mcsweeney, M.; Reuber, M.; Hoggard, N.; Levita, L. Cortical thickness and gyrification patterns in patients with psychogenic non-epileptic seizures. Neurosci Lett 2018, 678, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Labate, A.; Martino, I.; Caligiuri, M.E.; Fortunato, F.; Bruni, A.; Segura-Garcia, C.; Arcuri, P.; De Fazio, P.; Cerasa, A.; Gambardella, A. Orbito-frontal thinning together with a somatoform dissociation might be the fingerprint of PNES. Epilepsy Behav 2021, 121, 108044. [Google Scholar] [CrossRef] [PubMed]
- Aybek, S.; Nicholson, T.R.; Draganski, B.; Daly, E.; Murphy, D.G.; David, A.S.; Kanaan, R.A. Grey matter changes in motor conversion disorder. J Neurol Neurosurg Psychiatry 2014, 85, 236–238. [Google Scholar] [CrossRef] [PubMed]
- Ristić, A.J.; Daković, M.; Kerr, M.; Kovačević, M.; Parojčić, A.; Sokić, D. Cortical thickness, surface area and folding in patients with psychogenic nonepileptic seizures. Epilepsy Res 2015, 112, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Kozlowska, K.; Griffiths, K.R.; Foster, S.L.; Linton, J.; Williams, L.M.; Korgaonkar, M.S. Grey matter abnormalities in children and adolescents with functional neurological symptom disorder. Neuroimage Clin 2017, 15, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Perez, D.L.; Williams, B.; Matin, N.; LaFrance, W.C.; Costumero-Ramos, V.; Fricchione, G.L.; Sepulcre, J.; Keshavan, M.S.; Dickerson, B.C. Corticolimbic structural alterations linked to health status and trait anxiety in functional neurological disorder. J Neurol Neurosurg Psychiatry 2017, 88, 1052–1059. [Google Scholar] [CrossRef]
- Sojka, P.; Slovák, M.; Vechetová, G.; Jech, R.; Perez, D.L.; Serranová, T. Bridging structural and functional biomarkers in functional movement disorder using network mapping. Brain Behav 2022, 12, e2576. [Google Scholar] [CrossRef] [PubMed]
- Zelinski, L.; Diez, I.; Perez, D.L.; Kotz, S.A.; Wellmer, J.; Schlegel, U.; Popkirov, S.; Jungilligens, J. Cortical thickness in default mode network hubs correlates with clinical features of dissociative seizures. Epilepsy Behav 2022, 128, 108605. [Google Scholar] [CrossRef] [PubMed]
- Maiti, B.; Perlmutter, J. Imaging in movement disorders [review]. Continuum 2023, 29, 194–218. [Google Scholar] [PubMed]
- Xu, X.; Han, Q.; Lin, J.; Wang, L.; Wu, F.; Shang, H. Grey matter abnormalities in Parkinson's disease: a voxel-wise meta-analysis. Eur J Neurol 2020, 27, 653–659. [Google Scholar] [CrossRef] [PubMed]
- Gorno-Tempini, M.L.; Murray, R.C.; Rankin, K.P.; Weiner, M.W.; Miller, B.L. Clinical, cognitive and anatomical evolution from nonfluent progressive aphasia to corticobasal syndrome: a case report. Neurocase 2004, 10, 426–436. [Google Scholar] [CrossRef] [PubMed]
- Scheltens, P.; Blennow, K.; Breteler, M.M.; de Strooper, B.; Frisoni, G.B.; Salloway, S.; Van der Flier, W.M. Alzheimer's disease [review]. Lancet 2016, 388, 505–517. [Google Scholar] [CrossRef]
- MacIver, C.L.; Tax, C.M.W.; Jones, D.K.; Peall, K.J. Structural magnetic resonance imaging in dystonia: a systematic review of methodological approaches and findings. Eur J Neurol 2022, 29, 3418–3448. [Google Scholar] [CrossRef] [PubMed]
- Phan, T.X.; Baratono, S.; Drew, W.; Tetreault, A.M.; Fox, M.D.; Darby, R.R. Increased cortical thickness in Alzheimer's disease. Ann Neurol 2024, 95, 929–940. [Google Scholar] [CrossRef] [PubMed]
- Nalls, M.A.; Blauwendraat, C.; Vallerga, C.L.; Heilbron, K.; Bandres-Ciga, S.; Chang, D.; Tan, M.; Kia, D.A.; Noyce, A.J.; Xue, A.; et al. Identification of novel risk loci, causal insights, and heritable risk for Parkinson's disease: a meta-analysis of genome-wide association studies. Lancet Neurol 2019, 18, 1091–1102. [Google Scholar] [CrossRef] [PubMed]
- Patsopoulos, N.A. Genetics of multiple sclerosis: an overview and new directions [review]. Cold Spring Harb Perspect Med 2018, 8, a028951. [Google Scholar] [CrossRef] [PubMed]
- Reich, D.S.; Lucchinetti, C.F.; Calabresi, P.A. Multiple sclerosis [review]. N Engl J Med 2018, 378, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Munts, A.G.; Koehler, P.J. How psychogenic is dystonia? Views from past to present [review]. Brain 2010, 133, 1552–1564. [Google Scholar] [CrossRef] [PubMed]
- Frucht, L.; Perez, D.L.; Callahan, J.; MacLean, J.; Song, P.C.; Sharma, N.; Stephen, C.D. Functional dystonia: differentiation from primary dystonia and multidisciplinary treatments [review]. Front Neurol 2021, 11, 605262. [Google Scholar] [CrossRef] [PubMed]
- Spagnolo, P.A.; Norato, G.; Maurer, C.W.; Goldman, D.; Hodgkinson, C.; Horovitz, S.; Hallett, M. Effects of TPH2 gene variation and childhood trauma on the clinical and circuit-level phenotype of functional movement disorders. J Neurol Neurosurg Psychiatry 2020, 91, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Asadi-Pooya, A.A.; Simani, L.; Asadollahi, M.; Rashidi, F.S.; Ahmadipour, E.; Alavi, A.; Roozbeh, M.; Akbari, N.; Firouzabadi, N. Potential role of FKBP5 single-nucleotide polymorphisms in functional seizures. Epilepsia Open 2023, 8, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Faissner, S.; Plemel, J.R.; Gold, R.; Yong, V.W. Progressive multiple sclerosis: from pathophysiology to therapeutic strategies [review]. Nat Rev Drug Discov 2019, 18, 905–922. [Google Scholar] [CrossRef] [PubMed]
- Frank-Cannon, T.C.; Alto, L.T.; McAlpine, F.E.; Tansey, M.G. Does neuroinflammation fan the flame in neurodegenerative diseases? [Review.]. Mol Neurodegener 2009, 4, 47. [Google Scholar] [CrossRef] [PubMed]
- Yacoubian, T.A.; Fang, Y.D.; Gerstenecker, A.; Amara, A.; Stover, N.; Ruffrage, L.; Collette, C.; Kennedy, R.; Zhang, Y.; Hong, H.; et al. Brain and systemic Inflammation in de novo Parkinson's disease. Mov Disord 2023, 38, 743–754. [Google Scholar] [CrossRef] [PubMed]
- van der Feltz-Cornelis, C.; Brabyn, S.; Ratcliff, J.; Varley, D.; Aligar, V.; Gilbody, S.; Clarke, C.; Lagos, D. Assessment of cytokines, microRNA and patient related outcome measures in conversion disorder/functional neurological disorder (CD/FND): the CANDO clinical feasibility study. Brain Behav Immun-Health 2021, 13, 100228. [Google Scholar] [CrossRef]
- Kozlowska, K.; Chung, J.; Cruickshank, B.; McLean, L.; Scher, S.; Dale, R.C.; Mohammad, S.S.; Singh-Grewal, D.; Prabhuswamy, M.Y.; Patrick, E. Blood CRP levels are elevated in children and adolescents with functional neurological symptom disorder. Eur Child Adolesc Psychiatry 2019, 28, 491–504. [Google Scholar] [CrossRef] [PubMed]
- Hartig, M.; Prokisch, H.; Meitinger, T.; Klopstock, T. Mitochondrial membrane protein-associated neurodegeneration (MPAN) [review]. Int Rev Neurobiol 2013, 110, 73–84. [Google Scholar] [PubMed]
- Skowronska, M.; Buksinska-Lisik, M.; Kmiec, T.; Litwin, T.; Kurkowska-Jastrzębska, I.; Czlonkowska, A. Is there heart disease in cases of neurodegeneration associated with mutations in C19orf12? Parkinsonism Relat Disord 2020, 80, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.M.; Diedrich, A.; Biaggioni, I.; Robertson, D. The nature of the autonomic dysfunction in multiple system atrophy [review]. J Neurol Sci 2002, 200, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Aboudrar, S.; Benjelloun, H.; Benazzouz, A.; Bendahmanne, S.; Coghlan, L.; Kanouni, N.; Abouqal, R.; Benomar, M. Évaluation de l’activité vagale par le test de la respiration profonde (Deep-Breathing). Neurophysiol Clin 2007, 37, 41–46, [in French]. [Google Scholar] [CrossRef] [PubMed]
- Paredes-Echeverri, S.; Maggio, J.; Begue, I.; Pick, S.; Nicholson, T.R.; Perez, D.L. Autonomic, endocrine, and inflammation profiles in functional neurological disorder: a systematic review and meta-analysis. J Neuropsychiatry Clin Neurosci 2022, 34, 30–43. [Google Scholar] [CrossRef] [PubMed]
- Chudleigh, C.; Savage, B.; Cruz, C.; Lim, M.; McClure, G.; Palmer, D.M.; Spooner, C.J.; Kozlowska, K. Use of respiratory rates and heart rate variability in the assessment and treatment of children and adolescents with functional somatic symptoms. Clin Child Psychol Psychiatry 2019, 24, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Santens, P.; Crevits, L.; van Der Linden, C. Raynaud's phenomenon in a case of multiple system atrophy. Mov Disord 1996, 11, 586–588. [Google Scholar] [CrossRef] [PubMed]
- Pietzarka, K.; Reimann, M.; Schmidt, C.; Herting, B.; Schöls, L.; Reichmann, H.; Berg, D.; Schrader, C.; Ziemssen, T. The cold hand sign in multiple system atrophy: skin perfusion revisited. J Neural Transm 2010, 117, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Klein, C.; Brown, R.; Wenning, G.; Quinn, N. The "cold hands sign" in multiple system atrophy. Mov Disord 1997, 12, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Asahina, M.; Kikkawa, Y.; Suzuki, A.; Hattori, T. Cutaneous sympathetic function in patients with multiple system atrophy. Clin Auton Res 2003, 13, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Köllensperger, M.; Geser, F.; Seppi, K.; Stampfer-Kountchev, M.; Sawires, M.; Scherfler, C.; Boesch, S.; Mueller, J.; Koukouni, V.; Quinn, N.; et al. Red flags for multiple system atrophy. Mov Disord 2008, 23, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Horimoto, Y.; Aiba, I.; Yasuda, T.; Ohkawa, Y.; Katayama, T.; Yokokawa, Y.; Goto, A.; Ito, Y. Longitudinal MRI study of multiple system atrophy - when do the findings appear, and what is the course? J Neurol 2002, 249, 847–854. [Google Scholar] [CrossRef]
- Carmona-Abellan, M.; Del Pino, R.; Murueta-Goyena, A.; Acera, M.; Tijero, B.; Berganzo, K.; Gabilondo, I.; Gomez-Esteban, J.C. Multiple system atrophy: clinical, evolutive and histopathological characteristics of a series of cases. Neurología 2023, 38, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Onofrj, M.; Bonanni, L.; Manzoli, L.; Thomas, A. Cohort study on somatoform disorders in Parkinson disease and dementia with Lewy bodies. Neurology 2010, 74, 1598–1606. [Google Scholar] [CrossRef]
- Mark, V.W. Purple feet. 2022 Available online at 2022FNDSAbstracts.pdf (fndsociety.org).
- Reich, S.G. The cold hands sign in MSA. Neurology 2003, 60, 719. [Google Scholar] [CrossRef] [PubMed]
- Kinnier Wilson, S.A. The approach to the study of hysteria [review]. J Neurol Psychopathol 1931, 11, 193–206. [Google Scholar] [CrossRef]
- Lacy, B.E.; Mearin, F.; Chang, L.; Chey, W.D.; Lembo, A.J.; Simren, M.; Spiller, R. Bowel disorders [review]. Gastroenterology 2016, 150, 1393–1407. [Google Scholar] [CrossRef]
- Hallett, M.; Aybek, S.; Dworetzky, B.A.; McWhirter, L.; Staab, J.P.; Stone, J. Functional neurological disorder: new subtypes and shared mechanisms [review]. Lancet Neurol 2022, 21, 537–550. [Google Scholar] [CrossRef] [PubMed]
- Charney, M.; Foster, S.; Shukla, V.; Zhao, W.; Jiang, S.H.; Kozlowska, K.; Lin, A. Neurometabolic alterations in children and adolescents with functional neurological disorder. Neuroimage Clin 2023, 41, 103557. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Baudoin, R.; Hans, S.; Akst, L.M. History of otolaryngology: globus pharyngeus as "globus hystericus". Otolaryngol Head Neck Surg 2023, 168, 889–892. [Google Scholar] [CrossRef] [PubMed]
- Talman, L.; Safarpour, D. An overview of gastrointestinal dysfunction in Parkinsonian syndromes [review]. Semin Neurol 2023, 43, 583–597. [Google Scholar] [PubMed]
- Annaházi, A.; Schemann, M. Contribution of the enteric nervous system to autoimmune diseases and irritable bowel syndrome [review]. Adv Exp Med Biol 2022, 1383, 1–8. [Google Scholar] [PubMed]
- Nisticò, V.; Iacono, A.; Goeta, D.; Tedesco, R.; Giordano, B.; Faggioli, R.; Priori, A.; Gambini, O.; Demartini, B. Hypermobile spectrum disorders symptoms in patients with functional neurological disorders and autism spectrum disorders: a preliminary study. Front Psychiatry 2022, 13, 943098. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.; Grahame, R. Joint hypermobility syndrome [review]. BMJ 2011, 342, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Ellington, M.; Francomano, C.A. Chiari I malformations and the deritable disorders of connective tissue [review]. Neurosurg Clin N Am 2023, 34, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.A.; Greenberg, J.K.; Steinmetz, M.P.; Vorster, S.; Nevzati, E.; Spiessberger, A. C1-2 hypermobility and its impact on the spinal cord: a finite element analysis. J Neurosurg Spine in press.
- Al-Harbi, T.M.; Al-Rammah, H.; Al-Zahrani, N.; Liu, Y.; Sleiman, P.M.A.; Dridi, W.; Hakonarson, H. Rare neurological manifestations in a Saudi Arabian patient with Ehlers-Danlos syndrome and a novel homozygous variant in the TNXB gene. Am J Med Genet A 2022, 188, 618–623. [Google Scholar] [CrossRef] [PubMed]
- Jahromi, L.S.M.; Sayyadi, A.; Askarian, A.; Dabbaghmanesh, A.; Roshanzamir, S. Visual evoked potential in generalized joint hypermobility: a case-control study. Brain Behav 2024, 14, e3493. [Google Scholar] [CrossRef]
- Wissel, B.D.; Dwivedi, A.K.; Merola, A.; Chin, D.; Jacob, C.; Duker, A.P.; Vaughan, J.E.; Lovera, L.; LaFaver, K.; Levy, A.; et al. Functional neurological disorders in Parkinson disease. J Neurol Neurosurg Psychiatry 2018, 89, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Onofrj, M.; Russo, M.; Carrarini, C.; Delli Pizzi, S.; Thomas, A.; Bonanni, L.; Espay, A.J.; Sensi, S.L. Functional neurological disorder and somatic symptom disorder in Parkinson's disease. J Neurol Sci 2022, 433, 120017. [Google Scholar] [CrossRef]
- Pareés, I.; Saifee, T.A.; Kojovic, M.; Kassavetis, P.; Rubio-Agusti, I.; Sadnicka, A.; Bhatia, K.P.; Edwards, M.J. Functional (psychogenic) symptoms in Parkinson's disease. Mov Disord 2013, 28, 1622–1627. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Mayordomo, V.; Kojović, M.; López-Valdés, E.; ALonso-Frech, F.; Horga, A.; Fernández-Rodríguez, R.; Pareés, I. Functional neurological symptoms as initial presentation of Creutzfeldt-Jakob disease: case series [letter]. J Neurol 2023, 270, 1141–1146. [Google Scholar] [CrossRef]
- Carson, A.J.; McWhirter, L. Cognitive behavioral therapy: principles, science, and patient selection in neurology [review]. Semin Neurol 2022, 42, 114–122. [Google Scholar] [CrossRef]
- Lieberman, A. Are freezing of gait (FOG) and panic related? J Neurol Sci 2006, 248, 219–222. [Google Scholar] [CrossRef]
- Weiss, H.D.; Pontone, G.M. "Pseudo-syndromes" associated with Parkinson disease, dementia, apathy, anxiety, and depression [review]. Neurol Clin Pract 2019, 9, 354–359. [Google Scholar] [CrossRef]
- Marrie, R.A.; Patel, R.; Bernstein, C.N.; Bolton, J.M.; Graff, L.A.; Marriott, J.J.; Hitchon, C.A.; Figley, C.R.; Kornelsen, J.; Fisk, J.D. Anxiety and depression affect performance on the symbol digit modalities test over time in MS and other immune disorders. Mult Scler J 2021, 27, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Soto, E.; Cruz-Gómez, Á.J.; Gutiérrez, R.; González, M.; Sanmartino, F.; Rashid-Lopez, R.; Espinosa-Rosso, R.; Forero, L.; González-Rosa, J.J. Predicting neuropsychological impairment in relapsing remitting multiple sclerosis: the role of clinical measures, treatment, and neuropsychiatry symptoms. Arch Clin Neuropsychol 2021, 36, 475–484. [Google Scholar] [CrossRef]
- Leavitt, V.M.; Brandstadter, R.; Fabian, M.; Sand, I.K.; Klineova, S.; Krieger, S.; Lewis, C.; Lublin, F.; Miller, A.; Pelle, G.; et al. Dissociable cognitive patterns related to depression and anxiety in multiple sclerosis. Mult Scler J 2020, 26, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.P.; Feinstein, A. The link between depression and performance on the Symbol Digit Modalities Test: mechanisms and clinical significance. Mult Scler J 2019, 25, 118–121. [Google Scholar] [CrossRef]
- Landrø, N.I.; Celius, E.G.; Sletvold, H. Depressive symptoms account for deficient information processing speed but not for impaired working memory in early phase multiple sclerosis (MS). J Neurol Sci 2004, 217, 211–216. [Google Scholar] [CrossRef]
- Perrochon, A.; Holtzer, R.; Laidet, M.; Armand, S.; Assal, F.; Lalive, P.H.; Allali, G. Postural control is associated with cognition and fear of falling in patients with multiple sclerosis. J Neural Transm 2017, 124, 495–500. [Google Scholar] [CrossRef] [PubMed]
- Laidet, M.; Herrmann, F.R.; Armand, S.; Assal, F.; Lalive, P.H.; Allali, G. Does fear of falling predict gait variability in multiple sclerosis? J Neurol Sci 2017, 380, 212–214. [Google Scholar] [CrossRef]
- Xing, Z.; Hu, Y.; Teng, F.; Song, Y.; Wu, Z.; Hong, R.; Zhang, Z.; Gu, H.; Peng, K.; He, Y.; et al. A prediction rule for the dystonic spread of blepharospasm: a 4-year prospective cohort study. Ann Neurol in press.
- Pareés, I.; Saifee, T.A.; Kassavetis, P.; Kojovic, M.; Rubio-Agusti, I.; Rothwell, J.C.; Bhatia, K.P.; Edwards, M.J. Believing is perceiving: mismatch between self-report and actigraphy in psychogenic tremor. Brain 2012, 135, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Kramer, G.; Dominguez-Vega, Z.T.; Laarhoven, H.S.; Brandsma, R.; Smit, M.; van der Stouwe, A.M.; Elting, J.W.J.; Maurits, N.M.; Rosmalen, J.G.; Tijssen, M.A. Similar association between objective and subjective symptoms in functional and organic tremor. Parkinsonism Relat Disord 2019, 64, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Rommelfanger, K.S. The role of placebo in the diagnosis and treatment of functional neurologic disorders [review]. Handb Clin Neurol 2016, 139, 607–617. [Google Scholar]
- Bogousslavsky, J. Jean-Martin Charcot and his legacy [review]. Front Neurol Neurosci 2014, 35, 44–55. [Google Scholar] [PubMed]
- Witek, N.; Stebbins, G.T.; Goetz, C.G. What influences placebo and nocebo responses in Parkinson's disease? [Review.]. Mov Disord 2018, 33, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Ellis, T.; Boudreau, J.K.; DeAngelis, T.R.; Brown, L.E.; Cavanaugh, J.T.; Earhart, G.M.; Ford, M.P.; Foreman, K.B.; Dibble, L.E. Barriers to exercise in people with Parkinson disease. Phys Ther 2013, 93, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.J.; Trenkwalder, C.; Mestre, T.A. Placebo and nocebo responses in other movement disorders besides Parkinson's disease: how much do we know? [Review.]. Mov Disord 2018, 33, 1228–1235. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.X.; Zhang, N.N.; Zhao, H.X.; Song, J. Nocebo effect in multiple system atrophy: systematic review and meta-analysis of placebo-controlled clinical trials [review]. Neurol Sci 2022, 43, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Shafiq, F.; Mitsikostas, D.D.; Zis, P. Nocebo in motor neuron disease: systematic review and meta-analysis of placebo-controlled clinical trials [review]. Amyotroph Lateral Scler Frontotemporal Degener 2017, 18, 576–582. [Google Scholar] [CrossRef] [PubMed]
- McKee, K.; Glass, S.; Adams, C.; Stephen, C.D.; King, F.; Parlman, K.; Perez, D.L.; Kontos, N. The inpatient assessment and management of motor functional neurological disorders: an interdisciplinary perspective. Psychosomatics 2018, 59, 358–369. [Google Scholar] [CrossRef] [PubMed]
- Paramanandam, V.; Lizarraga, K.J.; Soh, D.; Algarni, M.; Rohani, M.; Fasano, A. Unusual gait disorders: a phenomenological approach and classification. Expert Rev Neurother 2019, 19, 119–132. [Google Scholar] [CrossRef] [PubMed]
- An, E.J.; Sim, W.S.; Kim, S.M.; Kim, J.Y. Suitability of visual cues for freezing of gait in patients with idiopathic Parkinson's disease: a case-control pilot study. J Neuroeng Rehabil 2023, 20, 91. [Google Scholar] [CrossRef] [PubMed]
- García Ruiz, P.J.; Rojo, A.; Sánchez Bernardos, V.; Romero, A.; Cubo, E.; Aguilar, M. Bloqueo (freezing) del gateo o bloqueo de la marcha cuadrúpeda. Neurología 2004, 19, 77–79, [in Spanish]. [Google Scholar]
- Huang, X.; Dong, K.; Gan, C.; Xu, Z.; Lei, D.; Dong, X.; Liu, H.; Chen, X. Effect of rhythmically cued exercise interventions on functions in patients with Parkinson disease: a meta-analysis [review]. Phys Ther in press.
- Hebb, C.; Raynor, G.; Perez, D.L.; Nappi-Kaehler, J.; Polich, G. The use of rhythmic auditory stimulation for functional gait disorder: a case report. Neurorehabilitation 2022, 50, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Snijders, A.H.; Bloem, B.R. Cycling for freezing of gait. N Engl J Med 2010, 362, e46. [Google Scholar] [CrossRef] [PubMed]
- Albanese, A.; Di Giovanni, M.; Lalli, S. Dystonia: diagnosis and management [review]. Eur J Neurol 2019, 26, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Ramos, V.F.M.L.; Karp, B.I.; Hallett, M. Tricks in dystonia: ordering the complexity [review]. J Neurol Neurosurg Psychiatry 2014, 85, 987–993. [Google Scholar] [CrossRef]
- Butler, M.; Shipston-Sharman, O.; Seynaeve, M.; Bao, J.; Pick, S.; Bradley-Westguard, A.; Ilola, E.; Mildon, B.; Golder, D.; Rucker, J.; et al. International online survey of 1048 individuals with functional neurological disorder. Eur J Neurol 2021, 28, 3591–3602. [Google Scholar] [CrossRef]
- Sadnicka, A.; Daum, C.; Meppelink, A.M.; Manohar, S.; Edwards, M. Reduced drift rate: a biomarker of impaired information processing in functional movement disorders. Brain 2020, 143, 674–683. [Google Scholar] [CrossRef] [PubMed]
- Věchetová, G.; Nikolai, T.; Slovák, M.; Forejtová, Z.; Vranka, M.; Straková, E.; Teodoro, T.; Růžička, E.; Edwards, M.J.; Serranová, T. Attention impairment in motor functional neurological disorders: a neuropsychological study. J Neurol in press.
- Roivainen, E.; Peura, M.; Patsi, J. Cognitive profile in functional disorders. Cogn Neuropsychiatry 2023, 28, 424–436. [Google Scholar] [CrossRef] [PubMed]
- de Vroege, L.; Koppenol, I.; Kop, W.J.; Riem, M.M.E.; der Feltz-Cornelis, C.M. Neurocognitive functioning in patients with conversion disorder/functional neurological disorder. J Neuropsychol 2021, 15, 69–87. [Google Scholar] [CrossRef] [PubMed]
- van Wouwe, N.C.; Mohanty, D.; Lingaiah, A.; Wylie, S.A.; LaFaver, K. Impaired action control in patients with functional movement disorders. J Neuropsychiatry Clin Neurosci 2020, 32, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Kozlowska, K.; Palmer, D.M.; Brown, K.J.; Scher, S.; Chudleigh, C.; Davies, F.; Williams, K.M. Conversion disorder in children and adolescents: a disorder of cognitive control. J Neuropsychol 2015, 9, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Pareés, I.; Kassavetis, P.; Saifee, T.A.; Sadnicka, A.; Bhatia, K.P.; Fotopoulou, A.; Edwards, M.J. 'Jumping to conclusions' bias in functional movement disorders. J Neurol Neurosurg Psychiatry 2012, 83, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Voon, V.; Ekanayake, V.; Wiggs, E.; Kranick, S.; Ameli, R.; Harrison, N.A.; Hallett, M. Response inhibition in motor conversion disorder. Movement Disorders 2013, 28, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Silveri, M.C.; Di Tella, S.; Lo Monaco, M.R.; Petracca, M.; Tondinelli, A.; Antonucci, G.; Pozzi, G.; Di Lazzaro, G.; Calabresi, P.; Bentivoglio, A.R. Theory of mind: a clue for the interpretation of functional movement disorders. Acta Neurol Scand 2022, 145, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Silveri, M.C.; Lo Monaco, M.R.; Tondinelli, A.; Petracca, M.; Zinzi, P.; Fragapane, S.; Pozzi, G.; Pagnini, F.; Bentivoglio, A.R.; Di Tella, S. Social cognition in Parkinson's disease and functional movement disorders. Neurol Sci 2024, 45, 3775–3784. [Google Scholar] [CrossRef] [PubMed]
- Sauer, K.S.; Witthoft, M.; Rief, W. Somatic symptom disorder and health anxiety: assessment and management [review]. Neurol Clin 2023, 41, 745–758. [Google Scholar] [CrossRef] [PubMed]
- Espay, A.J.; Ries, S.; Maloney, T.; Vannest, J.; Neefus, E.; Dwivedi, A.K.; Allendorfer, J.B.; Wulsin, L.R.; LaFrance, W.C.; Lang, A.E.; et al. Clinical and neural responses to cognitive behavioral therapy for functional tremor. Neurology 2019, 93, e1787–e1798. [Google Scholar] [CrossRef] [PubMed]
- O'Connell, N.; Watson, G.; Grey, C.; Pastena, R.; McKeown, K.; David, A.S. Outpatient CBT for motor functional neurological disorder and other neuropsychiatric conditions: a retrospective case comparison. J Neuropsychiatry Clin Neurosci 2020, 32, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Rawson, K.S.; Cavanaugh, J.T.; Colon-Semenza, C.; DeAngelis, T.; Duncan, R.P.; Fulford, D.; LaValley, M.P.; Mazzoni, P.; Nordahl, T.; Quintiliani, L.M.; et al. Design of the WHIP-PD study: a phase II, twelve-month, dual-site, randomized controlled trial evaluating the effects of a cognitive-behavioral approach for promoting enhanced walking activity using mobile health technology in people with Parkinson-disease. BMC Neurology 2020, 20, 146. [Google Scholar] [CrossRef] [PubMed]
- Broström, A.; Alimoradi, Z.; Lind, J.; Ulander, M.; Lundin, F.; Pakpour, A. Worldwide estimation of restless legs syndrome: a systematic review and meta-analysis of prevalence in the general adult population. J Sleep Res 2023, 32, e13783. [Google Scholar] [CrossRef] [PubMed]
- Mitterling, T.; Heidbreder, A.; Stefani, A.; Fritz, J.; Ulmer, H.; Poewe, W.; Högl, B. Natural course of restless legs syndrome/Willis-Ekbom disease: long-term observation of a large clinical cohort. Sleep Med 2015, 16, 1252–1258. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Navarro, H.; García-Martín, E.; Agúndez, J.A.G.; Jiménez-Jiménez, F.J. Association between restless legs syndrome and other movement disorders [review]. Neurology 2019, 92, 948–964. [Google Scholar] [CrossRef] [PubMed]
- Lebrato Hernández, L.; Prieto León, M.; Cerdá Fuentes, N.A.; Uclés Sánchez, A.J.; Casado Chocán, J.L.; Díaz Sánchez, M. Restless legs syndrome in patients with multiple sclerosis: evaluation of risk factors and clinical impact. Neurología 2022, 37, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Connor, J.R.; Ponnuru, P.; Lee, B.Y.; Podskalny, G.D.; Alam, S.; Allen, R.P.; Earley, C.J.; Yang, Q.X. Postmortem and imaging based analyses reveal CNS decreased myelination in restless legs syndrome. Sleep Med 2011, 12, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.Y.; Kim, J.; Connor, J.R.; Podskalny, G.D.; Ryu, Y.; Yang, Q.X. Involvement of the central somatosensory system in restless legs syndrome: a neuroimaging study. Neurology 2018, 90, e1834–e1841. [Google Scholar] [CrossRef] [PubMed]
- Mano, T.; Thomas, R.J. Anatomo-functional basis of restless legs syndrome [comment]. Neurology 2018, 90, 945–946. [Google Scholar] [CrossRef] [PubMed]
- Serranová, T.; Slovák, M.; Kemlink, D.; Šonka, K.; Hallett, M.; Růžička, E. Prevalence of restless legs syndrome in functional movement disorders: a case-control study from the Czech Republic. BMJ Open 2019, 9, e024236. [Google Scholar] [CrossRef] [PubMed]
- Mace, C.J.; Trimble, M.R. Ten-year prognosis of conversion disorder. Br J Psychiatry 1996, 169, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Gelauff, J.; Stone, J. Prognosis of functional neurologic disorders [review]. Handb Clin Neurol 2016, 139, 523–541. [Google Scholar] [PubMed]
- Schrag, A.; Trimble, M.; Quinn, N.; Bhatia, K. The syndrome of fixed dystonia: an evaluation of 103 patients. Brain 2004, 127, 2360–2372. [Google Scholar] [CrossRef] [PubMed]
- Weiser, H.I. Motor sensory dysfunction of upper limb due to conversion syndrome. Arch Phys Med Rehabil 1976, 57, 17–19. [Google Scholar]
- Delargy, M.A.; Peatfield, R.C.; Burt, A.A. Successful rehabilitation in conversion paralysis. Br Med J 1986, 292, 1730–1731. [Google Scholar] [CrossRef] [PubMed]
- Leslie, S. Diagnosis and treatment of hysterical conversion reactions. Arch Dis Child 1988, 63, 506–511. [Google Scholar] [CrossRef] [PubMed]
- Speed, J. Behavioral management of conversion disorder: retrospective study. Arch Phys Med Rehabil 1996, 77, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Moene, F.C.; Spinhoven, P.; Hoogduin, K.A.L.; van Dyck, R. A randomised controlled clinical trial on the additional effect of hypnosis in a comprehensive treatment programme for in-patients with conversion disorder of the motor type. Psychother Psychosom 2002, 71, 66–76. [Google Scholar] [CrossRef]
- Schwingenschuh, P.; Pont-Sunyer, C.; Surtees, R.; Edwards, M.J.; Bhatia, K.P. Psychogenic movement disorders in children: a report of 15 cases and a review of the literature. Mov Disord 2008, 23, 1882–1888. [Google Scholar] [CrossRef] [PubMed]
- Dallocchio, C.; Arbasino, C.; Klersy, C.; Marchioni, E. The effects of physical activity on psychogenic movement disorders. Mov Disord 2010, 25, 421–425. [Google Scholar] [CrossRef] [PubMed]
- Czarnecki, K.; Thompson, J.M.; Richard Seime, R.; Geda, Y.E.; Duffy, J.R.; Ahlskog, J.E. Functional movement disorders: successful treatment with a physical therapy rehabilitation protocol. Parkinsonism Relat Disord 2012, 18, 247–251. [Google Scholar] [CrossRef]
- Saifee, T.A.; Kassavetis, P.; Pareés, I.; Kojovic, M.; Fisher, L.; Morton, L.; Foong, J.; Price, G.; Joyce, E.M.; Edwards, M.J. Inpatient treatment of functional motor symptoms: a long-term follow-up study. J Neurol 2012, 259, 1958–1963. [Google Scholar] [CrossRef] [PubMed]
- Demartini, B.; Batla, A.; Petrochilos, P.; Fisher, L.; Edwards, M.J.; Joyce, E. Multidisciplinary treatment for functional neurological symptoms: a prospective study. J Neurol 2014, 261, 2370–2377. [Google Scholar] [CrossRef] [PubMed]
- Espay, A.J.; Edwards, M.J.; Oggioni, G.D.; Phielipp, N.; Cox, B.; Gonzalez-Usigli, H.; Pecina, C.; Heldman, D.A.; Mishra, J.; Lang, A.E. Tremor retrainment as therapeutic strategy in psychogenic (functional) tremor. Parkinsonism Relat Disord 2014, 20, 647–650. [Google Scholar] [CrossRef] [PubMed]
- Jordbru, A.A.; Smedstad, L.M.; Klungsøyr, O.; Martinsen, E.W. Psychogenic gait disorder: a randomized controlled trial of physical rehabilitation with one-year follow-up. J Rehabil Med 2014, 46, 181–187. [Google Scholar] [CrossRef]
- Nielsen, G.; Ricciardi, L.; Demartini, B.; Hunter, R.; Joyce, E.; Edwards, M.J. Outcomes of a 5-day physiotherapy programme for functional (psychogenic) motor disorders. J Neurol 2015, 262, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Dallocchio, C.; Tinazzi, M.; Bombieri, F.; Arnó, N.; Erro, R. Cognitive Behavioural Therapy and adjunctive physical activity for functional movement disorders (conversion disorder): a pilot, single-blinded, randomized study [letter]. Psychother Psychosom 2016, 85, 381–383. [Google Scholar] [CrossRef]
- Matthews, A.; Brown, M.; Stone, J. Inpatient physiotherapy for functional (psychogenic) gait disorder: a case series of 35 patients. Mov Disord Clin Pract 2016, 3, 603–606. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, G.; Buszewicz, M.; Stevenson, F.; Hunter, R.; Holt, K.; Dudziec, M.; Ricciardi, L.; Marsden, J.; Joyce, E.; Edwards, M.J. Randomised feasibility study of physiotherapy for patients with functional movement symptoms. J Neurol Neurosurg Psychiatry 2017, 88, 484–490. [Google Scholar] [CrossRef]
- Jacob, A.E.; Kaelin, D.L.; Roach, A.R.; Ziegler, C.H.; LaFaver, K. Motor retraining (MoRe) for functional movement disorders: outcomes from a 1-week multidisciplinary program. PM&R 2018, 10, 1164–1172. [Google Scholar]
- Jimenez, X.F.; Aboussouan, A.; Johnson, J. Functional neurological disorder responds favorably to interdisciplinary rehabilitation models. Psychosomatics 2019, 60, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Bullock, K.; Won, A.S.; Bailenson, J.; Friedman, R. Virtual reality-delivered mirror visual feedback and exposure therapy for FND: a midpoint report of a randomized controlled feasibility J Neuropsychiatry Clin Neurosci 2020, 32, 90-94.
- Demartini, B.; Bombieri, F.; Goeta, D.; Gambini, O.; Ricciardi, L.; Tinazzi, M. A physical therapy programme for functional motor symptoms: a telemedicine pilot study. Parkinsonism Relat Disord 2020, 76, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Maggio, J.B.; Ospina, J.P.; Callahan, J.; Hunt, A.L.; Stephen, C.D.; Perez, D.L. Outpatient physical therapy for functional neurological disorder: a preliminary feasibility and naturalistic outcome study in a U.S. cohort. J Neuropsychiatry Clin Neurosci 2020, 32, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Petrochilos, P.; Elmalem, M.S.; Patel, D.; Louissaint, H.; Hayward, K.; Ranu, J.; Selai, C. Outcomes of a 5-week individualised MDT outpatient (day-patient) treatment programme for functional neurological symptom disorder (FNSD). J Neurol 2020, 267, 2655–2666. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.; Riello, M.; Bellamoli, V.; Bombieri, F.; Geroin, C.; Di Vico, I.A.; Tinazzi, M. Motor and non-motor outcomes after a rehabilitation program for patients with Functional Motor Disorders: a prospective, observational cohort study. NeuroRehabilitation 2021, 48, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Hebert, C.; Behel, J.M.; Pal, G.; Kasi, R.; Kompoliti, K. Multidisciplinary inpatient rehabilitation for Functional Movement Disorders: a prospective study with long term follow up. Parkinsonism Relat Disord 2021, 82, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Callister, M.N.; Klanderman, M.C.; Boddu, S.P.; Moutvic, M.A.; Geissler, E.N.; Traver, K.J.; Staab, J.P.; Hassan, A. Outpatient motor retraining for functional movement disorder: predictors of a favorable short-term response. Mov Disord Clin Pract 2023, 10, 1377–1387. [Google Scholar] [CrossRef] [PubMed]
- Guy, L.; Caceres, G.A.; Jackson, T.; Gorman, S.; Wilson, J.; Hsieh, Y.; Petty, D.; Harrison, S.; Pick, S. Routine outcomes and evaluation of an 8-week outpatient multidisciplinary rehabilitative therapy program for functional neurological disorder. J Neurol 2024, 271, 1873–1884. [Google Scholar] [CrossRef] [PubMed]
- McCombs, K.E.; MacLean, J.; Finkelstein, S.A.; Goedeken, S.; Perez, D.L.; Ranford, J. Sensory processing difficulties and occupational therapy outcomes for functional neurological disorder. Neurol Clin Pract 2024, 14, e200286. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, G.; Stone, J.; Lee, T.C.; Goldstein, L.H.; Marston, L.; Hunter, R.M.; Carson, A.; Holt, K.; Marsden, J.; Le Novere, M.; et al. Specialist physiotherapy for functional motor disorder in England and Scotland (Physio4FMD): a pragmatic, multicentre, phase 3 randomised controlled trial. Lancet Neurol 2024, 23, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Polich, G.; Zalanowski, S.; Lewis, S.M.; Sugarman, S.; Christopolous, K.; Hebb, C.; Perez, D.L.; Baslet, G.; Shah, P.; Herman, S. Inpatient rehabilitation for acute presentation of motor functional neurological disorder (FND): a retrospective cohort study. Am J Phys Med Rehabil 2024, 103, 99–104. [Google Scholar] [CrossRef]
- Fahn, S.; Williams, D.T. Psychogenic dystonia [review]. Adv Neurol 1988, 50, 431–455. [Google Scholar] [PubMed]
- Gupta, A.; Lang, A.E. Psychogenic movement disorders [review]. Curr Opin Neurol 2009, 22, 430–436. [Google Scholar] [CrossRef]
- Trieschmann, R.B.; Stolov, W.C.; Montgomery, E.D. An approach to the treatment of abnormal ambulation resulting from conversion reaction. Arch Phys Med Rehabil 1970, 51, 198–206. [Google Scholar] [PubMed]
- Ness, D. Physical therapy management for conversion disorder: case series. J Neurol Phys Ther 2007, 31, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Silver, F.W. Management of conversion disorder. Am J Phys Med Rehabil 1996, 75, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Cardenas, D.D.; Larson, J.; Egan, K.J. Hysterical paralysis in the upper extremity of chronic pain patients. Arch Phys Med Rehabil 1986, 67, 190–193. [Google Scholar] [CrossRef] [PubMed]
- Morris, D.M.; Taub, E.; Mark, V.W.; Liu, W.; Brenner, L.; Pickett, T.; Stearns-Yoder, K.; Bishop-McKay, S.; Taylor, A.; Reder, L.; et al. Protocol for a randomized controlled trial of CI therapy for rehabilitation of upper extremity motor deficit: the Bringing Rehabilitation to American Veterans Everywhere project. J Head Trauma Rehabil 2019, 34, 268–279. [Google Scholar] [CrossRef]
- Mark, V.W.; Taub, E. Constraint-induced movement therapy for chronic stroke hemiparesis and other disabilities [review]. Restor Neurol Neurosci 2004, 22, 317–336. [Google Scholar] [PubMed]
- Taub, E.; Ramey, S.L.; DeLuca, S.; Echols, K. Efficacy of Constraint-Induced Movement Therapy for children with cerebral palsy with asymmetric motor impairment. Pediatrics 2004, 113, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Mark, V.W.; Taub, E.; Uswatte, G.; Morris, D.M.; Cutter, G.R.; Adams, T.L.; Bowman, S. Phase II randomized controlled trial of CI therapy in MS. Part I: effects on real-world function. Neurorehabil Neural Repair 2018, 32, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Hoover, C.F. A new sign for the detection of malingering and functional paresis of the lower extremities. JAMA 1908, 51, 746–747. [Google Scholar] [CrossRef]
- Tibben, M.I.; van Opdorp, A.; Bialek, W.; Schaap, J.; Tijssen, M.A.J.; Merkx, M.J.M. Efficacy of hypnosis and catalepsy induction in functional neurological disorders. Mov Disord Clin Pract 2024, 11, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Taib, S.; Ory-Magne, F.; Brefel-Courbon, C.; Moreau, Y.; Thalamas, C.; Arbus, C.; Simonetta-Moreau, M. Repetitive transcranial magnetic stimulation for functional tremor: a randomized, double-blind, controlled study. Mov Disord 2019, 34, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Perez, D.; Edwards, M.J.; Nielsen, G.; Kozlowska, K.; Hallett, M.; LaFrance, W.C. Decade of progress in motor functional neurological disorder: continuing the momentum [review]. J Neurol Neurosurg Psychiatry 2021, 92, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Marcolini, E.; Tolchin, B. Functional seizures [review]. Emerg Med Clin N Am 2021, 39, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Pasricha, P.J.; McKnight, M.; Villatoro, L.; Barahona, G.; Brinker, J.; Hui, K.; Polydefkis, M.; Burns, R.; McMahan, Z.H.; Gould, N.; et al. Joint hypermobility, autonomic dysfunction, gastrointestinal dysfunction and autoimmune markers (JAG-A): clinical associations and response to intravenous immunoglobulin therapy. Am J Gastroenterol in press.
- Serranová, T.; Di Vico, I.; Tinazzi, M. Functional movement disorder. Assessment and treatment [review]. Neurol Clin 2023, 41, 583–603. [Google Scholar] [CrossRef] [PubMed]
- Bennett, K.; Diamond, C.; Hoeritzauer, I.; Gardiner, P.; McWhirter, L.; Carson, A.; Stone, J. A practical review of functional neurological disorder (FND) for the general physician. Clin Med 2021, 21, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Joos, A. Ätiopathogenese und Behandlung von Funktionellen Neurologischen Störungen mit Fokus auf Funktionelle (Dissoziative) Anfälle [review]. Swiss Arch Neurol Psychiatry Psychother 2020, 171, w03081, [in German]. [Google Scholar]
- Gilmour, G.S.; Nielsen, G.; Teodoro, T.; Yogarajah, M.; Coebergh, J.A.; Dilley, M.D.; Martino, D.; Edwards, M.J. Management of functional neurological disorder [review]. J Neurol 2020, 267, 2164–2172. [Google Scholar] [CrossRef] [PubMed]
- Kirkwood, B.; Mark, V.W. Consistency of inclusion criteria for functional movement disorder clinical research studies: a systematic review. NeuroRehabilitation 2022, 50, 169–178. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR); American Psychiatric Association: Washington, USA, 2022. [Google Scholar]
- Stone, J. Lessons from a neurologist after 25 years of functional neurological disorder subspeciality practice [review]. Neurol Clin 2023, 41, 569–582. [Google Scholar] [CrossRef] [PubMed]
- Aybek, S.; Chan, A. The borderland of multiple sclerosis and functional neurological disorder: a call for clinical research and vigilance. Eur J Neurol 2023, 30, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Boissy, A.R.; Ford, P.J. A touch of MS: therapeutic mislabeling. Neurology 2012, 78, 1981–1985. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Yearly total of publications appearing in PubMed that included the terms “functional neurological disorder,” “functional neurological symptom disorder,” or “conversion disorder.” The alternate terms “hysteria” and “psychogenic disorder” are not included in this graph because they include other disorders that are not FND in addition to FND.
Figure 1.
Yearly total of publications appearing in PubMed that included the terms “functional neurological disorder,” “functional neurological symptom disorder,” or “conversion disorder.” The alternate terms “hysteria” and “psychogenic disorder” are not included in this graph because they include other disorders that are not FND in addition to FND.
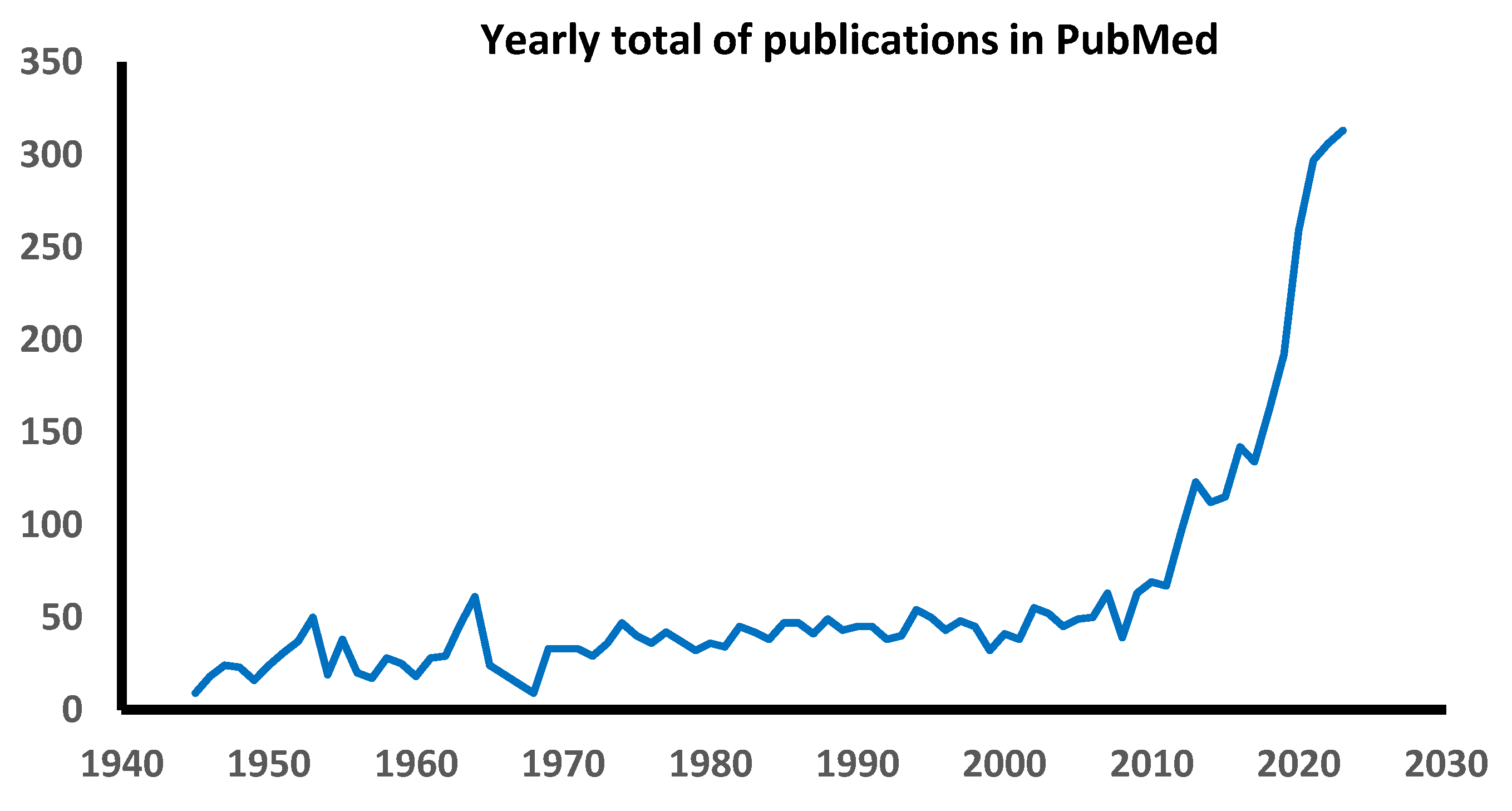
Figure 2.
The examiner leaves blanched “fingerprints” after gentle digital compression on both feet of an 18-year-old woman in the author’s FND clinic with eight years of FND. Note also the purple discoloration of her feet, compared to the areas with delayed capillary refilling immediately after compression.
Figure 2.
The examiner leaves blanched “fingerprints” after gentle digital compression on both feet of an 18-year-old woman in the author’s FND clinic with eight years of FND. Note also the purple discoloration of her feet, compared to the areas with delayed capillary refilling immediately after compression.

Figure 3.
Self-photographed acute dermal changes in a 20-year-old woman with FND. (A) Erythema of fingertips and cyanosis of the thenar eminence, diffuse hand pain and stiffness. (B) Painless right paramedian linear depigmentation of the abdomen.
Figure 3.
Self-photographed acute dermal changes in a 20-year-old woman with FND. (A) Erythema of fingertips and cyanosis of the thenar eminence, diffuse hand pain and stiffness. (B) Painless right paramedian linear depigmentation of the abdomen.
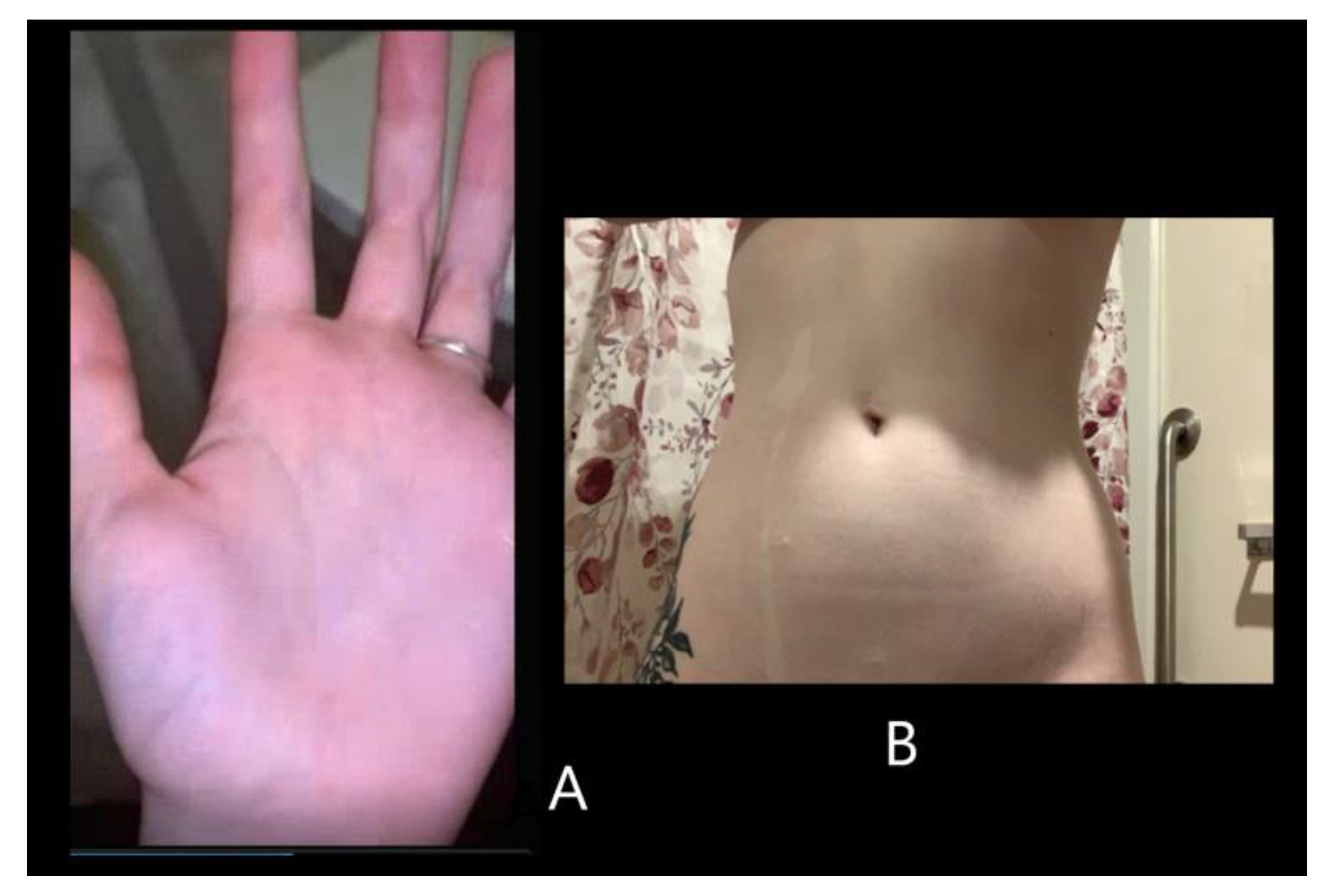
Figure 4.
Hypermobility at the metacarpal joints in an FND clinic patient from the author’s practice.
Figure 4.
Hypermobility at the metacarpal joints in an FND clinic patient from the author’s practice.
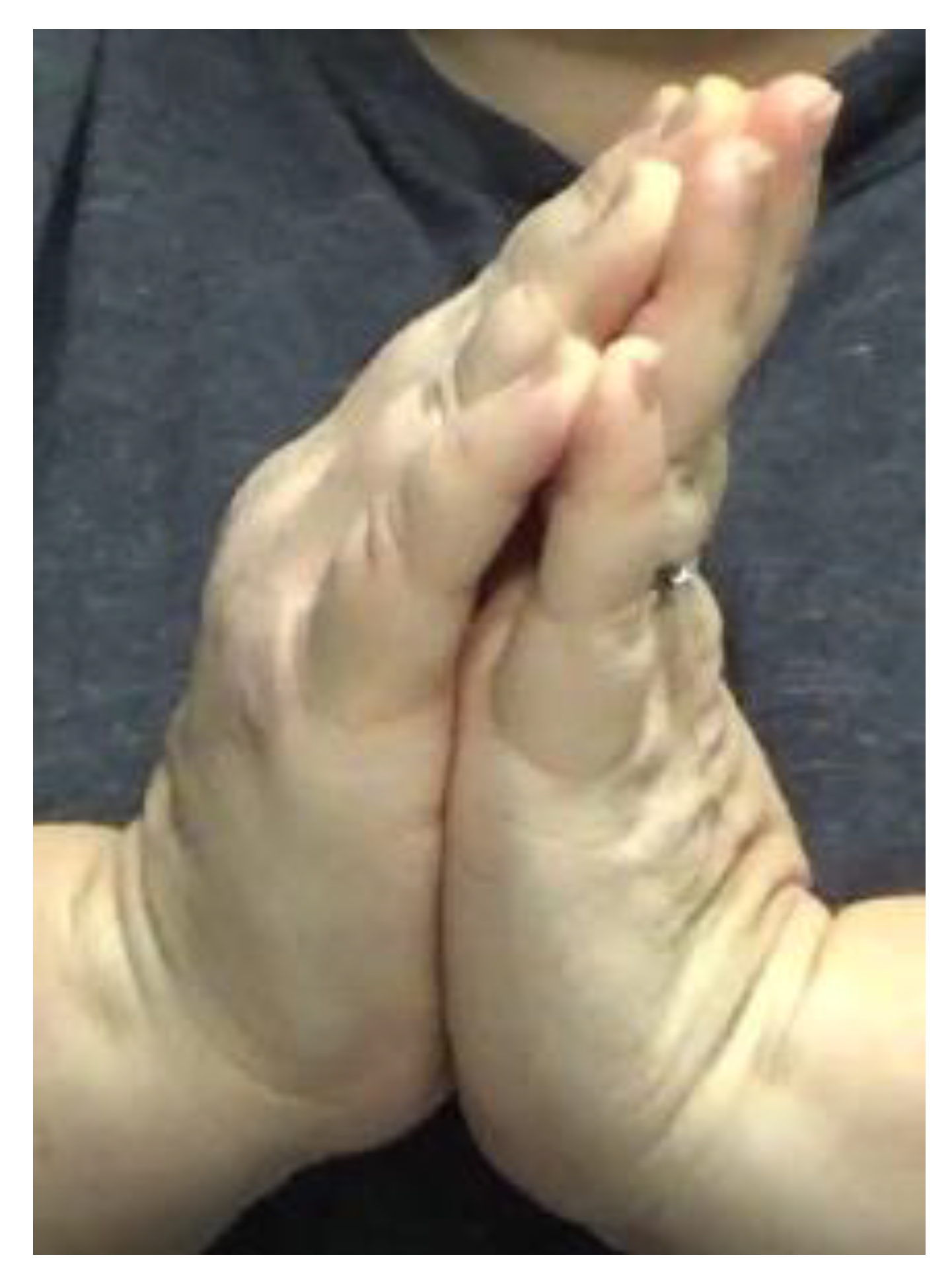

Table 1.
Summary of volumetric grey area changes on structural brain imaging in FND.
| Volume Findings | Number of Studies | References |
|---|---|---|
| Focal decrease | 11 | [36,37,38,39,40,41,42,43,44,45,46] |
| Focal decrease and increase in different areas | 4 | [47,48,49,50] |
| Focal increase | 3 | [51,52,53] |
| No difference compared to non-FND subjects | 3 | [54,55,56] |
Table 2.
Summary of physical therapies for FND.
| Study [Reference] | N* | Diagnostic Method** | Intervention† | Dose (Months) | Setting†† | Motor Symptoms Targeted‡ |
|---|---|---|---|---|---|---|
| Weiser, 1976 [163] | 7 | MD referral | PT, counseling | 0.25-2 | Out | paresis |
| Delargy, 1988 [164] | 6 | MD referral | PT | 0.36-2.5 | In | walking |
| Leslie, 1988 [165] | 20 | MD referral | PT | 1-3 | In or Out | walking, paresis |
| Speed, 1996 [166] | 10 | MD referral | PT | 0.14-0.8 | In | walking |
| Heruti, 2002 [24] | 30 | MD referral | PT | Not stated | In | paresis |
| Moene, 2002 [167] | 45 | DSM-III |
PT + hypnosis vs PT |
3 | In | dystonia, walking, tremor, paresis |
| Schrag, 2004 [162] | 26 | Fahn-Williams | PT + CBT | Not stated | Not stated | dystonia, tremor |
| Schwingenschuh, 2008 [168] | 12 | Fahn-Williams | PT + CBT | Not stated | Out | dystonia, walking, tremor |
| Dallochio, 2010 [169] | 16 | Fahn-Williams | Walking therapy | 3 | Out | dystonia, walking, tremor |
| Czarnecki, 2012 [170] | 80 | Fahn-Williams | PT vs TAU | 0.25 | Out | walking, tremor, paresis |
| Saifee, 2012 [171] | 26 | MD referral | PT + CBT | 0.75 | In | dystonia, tremor, paresis |
| Demartini, 2014 [172] | 36 | MD referral |
Multidisciplinary rehab |
1 | In | dystonia, walking, tremor, paresis |
| Espay, 2014 [173] | 10 | MD referral |
Entrainment with biofeedback device |
0.03 | Out | tremor |
| Jordbru, 2014 [174] | 40 | MD referral |
PT + CBT vs waitlist |
0.75 | In | walking |
| Nielsen, 2015 [175] | 47 | Gupta-Lang | PT | 0.25 | Out | dystonia, walking, tremor, paresis |
| Dallochio, 2016 [176] | 29 | Fahn-Williams |
CBT vs CBT + PT vs TAU |
3 | Out | dystonia, walking, tremor |
| Matthews, 2016 [177] | 35 | MD referral | PT | ≤ 2 | In | walking |
| Nielsen, 2017 [178] | 57 | Fahn-Williams | PT vs nonspecific PT | 0.25 | Out | dystonia, walking, tremor |
| Jacob, 2018 [179] | 32 | Fahn-Williams | PT | 0.25 | In | dystonia, walking, tremor |
| Jimenez, 2019 [180] | 49 | DSM-5 | Pain multidisciplinary rehab | 0.25 | Out | FMD |
| Bullock, 2020 [181] | 12 | DSM-5 |
VR motor rehab + mirror feedback |
2 | Out | FMD or sensory symptoms |
| Demartini, 2020 [182] | 18 | Gupta-Lang | PT | 5.25 | Home | dystonia, walking, tremor, paresis |
| Maggio, 2020 [183] | 50 | DSM-5 | PT, CBT, goal setting | 1.5-3 | Out | dystonia, walking, tremor, paresis |
| Petrochilos, 2020 [184] | 78 | MD referral | PT, Multidisciplinary rehab, CBT | 1.4 | Out | dystonia, walking, tremor, paresis |
| Gandolfi 2021 [185] | 33 | Gupta-Lang | PT | 0.25 | Home | dystonia, walking, tremor, paresis |
| Hebert, 2021 [186] | 13 | Fahn-Williams | PT | 0.25-0.5 | In | dystonia, walking, tremor, paresis |
| Callister, 2023 [187] | 201 | Gupta-Lang | PT | 0.25 | In | walking, tremor, paresis |
| Guy, 2024 [188] | 31 | DSM-5 | PT + CBT | 2 | Out | dystonia, tremor, paresis |
| McCombs, 2024 [189] | 77 | MD referral | Sensory-oriented OT | 4 | Out | dystonia, walking, tremor, paresis |
| Nielsen, 2024 [190] | 241 | Gupta-Lang | PT vs TAU | 0.75 | Out | dystonia, walking, tremor, paresis |
| Polich, 2024 [191] | 22 | MD referral | PT | 0.5 | In | walking, paresis |
Table 2.
Summary of physical therapies for FND (continuation).
| Study | Outcome Measure‡‡ |
Immediate Results |
Follow-up (Months) ¶ |
RESULTS¶¶ |
|---|---|---|---|---|
| Weiser, 1976 [163] | Neurol exam | 100% improved | 1-96 | 86% retained gains |
| Delargy, 1988 [164] | Neurol exam | 100% improved | 8-14 | 100% retained gains |
| Leslie, 1988 [165] | Neurol exam | 85% improved | NA | |
| Speed, 1996 [166] | FIM | 100% improved | 7-36 | 78% retained gains |
| Heruti, 2002 [24] | Neurol exam | 55% improved | NA | |
| Moene, 2002 [167] | Neurol exam | 65% improved; no difference between groups | 6 | 84% retained gains; no difference between groups |
| Schrag, 2004 [162] | Neurol exam | 33% improved | NA | |
| Schwingenschuh, 2008 [168] | Neurol exam | 80% improved | NA | |
| Dallochio, 2010 [169] | PMDRS | 70% improved | NA | |
| Czarnecki, 2012 [170] | Neurol exam | 73% improved | 25-33 | Experimental group 60% self-rated improved vs 22% control treatment |
| Saifee, 2012 [171] |
Nonspecific self-assessment |
58% improved | NA | |
| Demartini, 2014 [172] | COPM, CGI | 67% improved | 12 | COPM: 100% retained gains; CGI: 33% retained gains |
| Espay, 2014 [173] | PMDRS | 100% improved | 3-6 | 50% retained gains, the other measures declined |
| Jordbru, 2014 [174] |
Functional Mobility Scale, FIM |
Experimental group generally improved | 12 | 100% gains retained |
| Nielsen, 2015 [175] | CGI | 96% improved | 3 | 85% retained gains |
| Dallochio, 2016 [176] | PMDRS |
Experimental groups improved, unlike TAU |
NA | |
|
Matthews, 2016 [177] |
Modified Rivermead Mobility Index |
Generally improved | NA | |
| Nielsen, 2017 [178] | CGI |
Assessment delayed until 6 m |
6 | Experimental group > control group gains |
| Jacob, 2018 [179] | CGI, PMDRS | 87% improved | 6 | 67% retained (only CGI assessed) |
| Jimenez, 2019 [180] |
In-lab movement measures |
Generally improved | NA | |
| Bullock, 2020 [181] |
Oxford Handicap Scale |
Improved experimental group only | NA | |
| Demartini, 2020 [182] | PMDRS, CGI | Improved (67%) | 6 | 72% retained gains |
| Maggio, 2020 [183] | Subjective change | Improved (34%) | NA | |
| Petrochilos, 2020 [184] | CGI, COPM | Generally improved | 6 | 100% retained gains |
| Gandolfi 2021 [185] | S-FMDRS, other in-lab measures | Generally improved | 3 | Gains lost |
| Hebert, 2021 [186] | CGI | 93% improved | 12 | 77% retained gains on CGI |
| Callister, 2023 [187] |
COPM ability subscale |
84% improved | NA | |
| Guy, 2024 [188] | Lab assessments | Generally improved | 3 | 100% retained gains |
| McCombs, 2024 [189] | Clinician judgement | 62% improved | NA | |
| Nielsen, 2024 [190] | SF-36; CGI | Not reported | 12 | No difference between groups on SF-36; results favored CGI, but statistics not stated |
|
Polich, 2024 [191] |
PT, OT judgement (ordinal scales) Berg Balance Scale |
95% improved | NA |
*N, number of patients who remained to the conclusion of the study. **Diagnostic method: DSM, Diagnostic and Statistical Manual of Mental Disorders (various editions); Fahn-Williams [192]; Gupta-Lang [193]; MD referral, clinician referral. †Intervention: CBT, Cognitive Behavioral Therapy; OT, occupational therapy; PT, physical therapy; TAU, treatment as usual; VR, virtual reality. ††Setting: In, inpatient; Out, outpatient; Home, home-based therapy. ‡Motor symptoms targeted: FMD, functional movement disorder not otherwise specified. ‡‡Outcome measure: CGI, Clinical Global Impression self-rated scale; COPM, Canadian Occupational Performance Measure; FIM, Functional Independence Measure; Neurol exam, neurological examination; PMDRS, Psychogenic Movement Disorder Rating Scale; S-FMDRS, Simplified Functional Movement Disorder Rating Scale. ¶ Follow-up: NA, not reported. ¶¶ Results: SF-36, 36-item Short Form Health Survey.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



