
Submitted:
22 July 2024
Posted:
23 July 2024
You are already at the latest version
Abstract
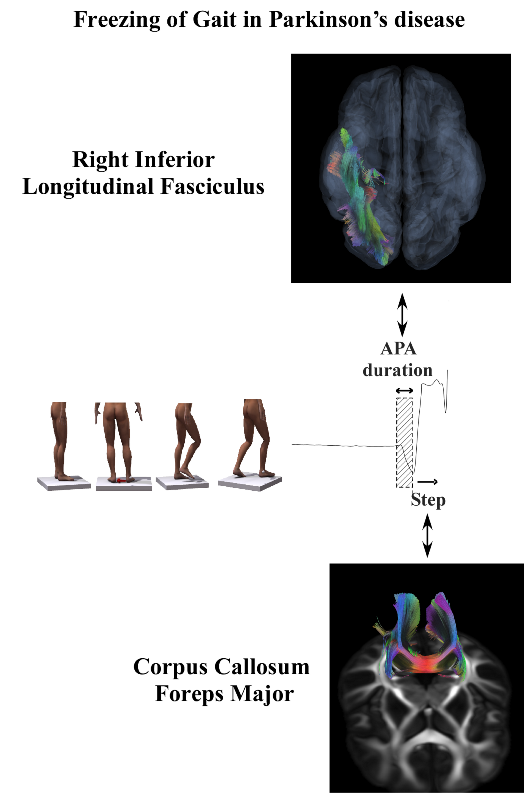
Freezing of Gait (FoG) is a disabling motor complication in Parkinson’s disease (PD), affecting approximately 50% of advanced PD patients. It is characterized by sudden and transient inability to initiate or maintain walking, leading to falls and reduced quality of life. This study investigates the relationship between white matter integrity and step initiation impairments in FoG. Forty-three PD patients (26 with FoG) underwent diffusion-weighted imaging to assess white matter DTI metrics and kinematic analysis during step initiation tasks. Multiple regression analyses were conducted to explore the connection between white matter tract integrity and step initiation behavior. The multiple regression analysis shows that (1) Right Inferior Longitudinal Fasciculus RD explained 31% of APA duration’s variance; (2) Corpus Callosum Forceps Major explained 25% of the step length's variance. There was a positive correlation between the Right Inferior Longitudinal Fasciculus RD and APA duration and a negative correlation between Corpus Callosum Forceps Major RD and step length. The findings suggest that compromised white matter integrity in RILF and CC contributes to impaired motor control during step initiation in FoG. These regions are critical for inhibitory control and interhemispheric coordination, crucial for APA execution and step length regulation.
Keywords:
movement disorders
; step initiation
; white matter integrity
; diffusion tensor imaging
1. Introduction
Freezing of gait (FoG) is a debilitating movement disorder [1,2] present in roughly 50% of individuals with advanced Parkinson’s disease (PD) [3]. It is characterized as a “brief, episodic absence or marked reduction of forward progression of the feet despite the intention to walk” [2], leading to falls, increased dependence [4], and reduced quality of life [5]. FoG is associated with levodopa off-state [6] and longer disease duration [7]. Several factors can trigger FoG, including step initiation, changing direction and environment contexts, narrow doorways, anxiety, walking under temporal constraints, or stress [2]. On the other hand, some situations relieve FoG symptoms: sensory cues and attentional focus on gait [8]. Factors that trigger and relieve FoG depend highly on cortical mechanisms (emotion, attention, executive, and visuospatial functions), which can be explained by compensating cortical circuits on the affected subcortical regions [9].
Recent studies found functionally deficient prefrontal areas in PD individuals with FoG, such as the anterior cingulate (error monitoring, inhibition, and volition); the orbitofrontal cortex (decision making, sensory integration, reward expectation); and the dorsolateral prefrontal cortex (motor planning, organization and changing of context) compared to individuals without PD (nFoG) [10,11]. Current evidence from radiological studies addresses FoG to structural disorders in gray and white matter. Voxel-based morphometry studies have shown atrophy in frontal [10,12] and parietal [10,13] cortices, with some studies also reporting gray matter loss in temporal [12] and occipital [12,14] cortices. Tractography, utilizing diffusion tensor imaging (DTI), allows for the visualization and analysis of white matter tracts, providing insights into the integrity of neural pathways critical for motor control. Alterations in white matter tracts, such as the corpus callosum (CC), right inferior longitudinal fasciculus (RILF), and superior longitudinal fasciculus (SLF), have also been consistently observed in individuals with FoG [15,16,17].
Given FoG’s complexity, it is imperative to explore the role of white matter integrity in step initiation and overall gait performance. The periventricular white matter, comprising longitudinal, thalamic, and callosal fibers, has been implicated in various studies as crucial for motor control and coordination. However, the specific contributions of these tracts to FoG, particularly during the anticipatory postural adjustments (APA) required for step initiation, still need to be explored. Step initiation requires APAs to shift the center of mass to the support leg, releasing the moving leg to take a step. Studies have shown that individuals with FoG have disorders of APA (lower amplitude and longer latency) compared to PD individuals without FoG [18], which are related to disorders in cortical functioning [19]. Recent studies demonstrated potential gray matter regions linked to impaired APA in step initiation in FoG [19,20,21,22]. The involvement of white matter integrity in step initiation behavior in individuals with FoG remains unclear. In the present study, we aim to investigate the integrity of the white matter and its relationship with the step initiation behavior in individuals with FoG.
2. Materials and Methods
2.1. Participants
Forty-three individuals with moderate idiopathic PD (Hoehn & Yahr = 3; 26 with FoG; age: 62.97 ± 10.59 years; disease duration: 10.03 ± 5.94 years; equivalent dose of levodopa: 611.54 ± 429.23 mg·day−1; motor score Unified Parkinson’s Disease Rating Scale - UPDRS: 31.09 ± 10.39; Montreal Cognitive Assessment - MoCA: 18.25 ± 2.51) participated in this study. The individuals were recruited in the Movement Disorders Division of the Medical School of the University of São Paulo. All individuals were diagnosed by neurologists and were submitted to the Unified Parkinson’s Disease Rating Scale - UPDRS on the day of the exam. Inclusion criteria were: (1) Hoehn & Yahr score of 3; (2) availability to engage in task training, brain imaging, and neuropsychological assessments; (3) capacity to walk independently, without assistance devices; (4) ability to understand instructions to perform the experimental motor tasks; (5) absence of neurological diseases other than PD; (6) absence of musculoskeletal impairments possibly affecting the performance of the experimental tasks. The exclusion criteria were as follows: (1) difficulty performing the experimental motor tasks; (2) drop out of any assessment; (3) poor quality of the brain volumes acquired during the fMRI: head motion above 1 mm [23]. Individuals were classified as having FoG if they answered affirmatively the first question of the New Freezing of Gait Questionnaire (nFoGq) following a video showing examples of individuals experiencing FoG. All the FoG individuals scored 3 or 4 in the NFoGq question: “How frequently do you experience freezing episodes when initiating the first step?” indicating moderate or severe FoG during step initiation. All evaluations were taken during the ON state of dopaminergic medications. All participants provided informed consent, and the University of São Paulo Institutional Review Board approved the experimental procedures.
2.2. Behavioral Task: Step Initiation
The individuals performed 30 trials of a step initiation task with the right leg. Once on the platform, the position of their feet was marked with tape on the floor to keep the same initial position in each trial. Firstly, the individual was to gaze at a cross on a TV monitor placed 3 m ahead and relax. The following command displayed was to prepare (a circle that could be open or closed, depending on the randomization of the trials), then an open or closed circle (if the first was closed, the second was open, and vice-versa) to take a step (Figure 1).
The participants performed the task on a force platform (AMTI OR6-6). For kinematic analysis, we placed a reflective marker on the lateral malleolus of both subjects’ legs. Twelve optoelectronic cameras (Vicon, model T10) tracked the markers. Kinematic and kinetic data were acquired at a sampling frequency of 200 Hz using a motion capture system (Vicon Nexus). A trigger synchronizes the motion capture system and the fNIRS system.
The anticipatory postural adjustment (APA) began with the initial lateral displacement of the center of pressure (CoP) toward the leading limb. The end of the APA, and therefore the start of the step, occurred when the free vertical moment changed direction (i.e., became negative when initiating with the right limb) [24]. The following variables were analyzed: (a) APA duration, the time between the beginning of the APA and the beginning of the step; (b) APA amplitude normalized, the maximum amplitude of the last peak of mediolateral displacement of the CoP before the start of the step normalized by the distance between the malleoli; (c) Step length normalized by each individual’s foot size.
2.3. Magnetic Resonance Imaging
To acquire diffusion images, the individuals underwent a Magnetic Resonance Imaging exam in a 3.0 T scanner (Intera Achieva, Philips Healthcare, Best, The Netherlands) in which every individual used a thirty-two-channel head coil (Philips Healthcare, Best, The Netherlands). T1-weighed axial 3D images were acquired with isotropic voxel size 1 mm, FOV 256 × 256, 180 sagittal slices, 60 mm thick each, covering the whole brain, phase encoding anterior-posterior, TR = 7 ms, TE = 3.2ms, TI = 1120 ms, flip angle 8°, acquisition time 4 min 12 s. FLAIR (Axial Fluid-Attenuated Inversion Recovery) images were acquired with isotropic voxel size 1 mm, FOV 256 × 256, 176 sagittal slices, phase encoding anterior-posterior, TR = 5,000 ms, TE = 397 ms, TI = 1,800 ms, flip angle 120°, acquisition time 4 min 42 s. Diffusion-weighted imaging (DWI) was obtained using a single-shot spin echo EPI sequence. Whole brain diffusion images received b = 700 s/mm2 with 32 directions. The repetition time (TR) and echo time (TE) were 13 and 101 ms for this image. Extra brain volumes received four no diffusion weighting (b = 0 s/mm2) with opposing phase-encode directions (Anterior-Posterior and opposite). The structural images consisted of single-shot T1-weighed axial 3D images containing 180 slices, 60 mm thick each, and covering the whole brain. They followed the parameters: flip angle = 8°, TR/TE = 7/3.2 s, FOV = 740 mm², NSA = 1, Fast Imaging Mode = TSE, needing a total of 58.7 s to be taken. DWI images consisted of 72 transversal slices covering the whole brain, with 2 mm³ voxels, 128 x 128 mm matrix, 256 x 256 mm field of view and no gap between slices, following the parameters: TR/TE = 8705/30 ms, NSA = 1, 844 volumes, 90-degree flip angle, b-factor = 2, max b-factor = 1000, diffusion gradient = 31.4/16.3 and EPI factor = 67. The total length of DWI acquisition was 6 minutes 11.5 seconds.
2.4. Image Data Processing
Subcortical segmentation and fiber tracking of the SLF were automated and obtained using FreeSurfer (https://surfer.nmr.mgh.harvard.edu, software package version). Next, TRACULA, a tool available on FreeSurfer, was used to reconstruct the SLF tract based on each of the images obtained. The tool calculated the tract’s likelihood to be next to (or in) each of the cortical and subcortical segmentation labels from FreeSurfer, using manually labeled tracts on training subjects and an MNI 152 template as a reference.
The automated cortical and subcortical segmentation and parcellation were processed using the multimodal recon-all processing stream option, combining both the high-resolution T1 3D-weighted and T2-FLAIR images intended to improve dural surface segmentation [25], which includes motion correction, skull-stripping, registration, segmentation, smoothing, and parcellation mapping in FreeSurfer 6.0 (https://surfer.nmr.mgh.harvard.edu/fswiki). Segmentation results for each subject were manually inspected and edited for accuracy by the first author (MPN), per Freesurfer guidelines. For global probabilistic tractography analyses, diffusion tensor images (DTI) were processed using Freesurfer’s TRActs Constrained by UnderLying Anatomy (TRACULA) tool [26], using a standard pipeline, including eddy-current correction via affine registration, rotation of the gradients to match eddy-current correction, extraction of the brain mask, registration from individual DTI to the individual T1 image (intra-subject registration), registration to MNI space (inter-subject registration), cortical and white matter mask creation, tensor fitting for the extraction of tensor-based measures, and computing anatomical priors for tracts form the TRACULA atlas.
This method reconstructs probabilistic distributions of 18 major white matter tracts for every individual. It computes the following DTI metrics: fractional anisotropy (FA), mean diffusivity (MD), radial diffusivity (RD), and axial diffusivity (AD).
The tract of interest consisted of commissural tracts (Forceps Major and Minor), anterior thalamic radiation, cingulum-angular (infracallosal) bundle, cingulum-cingulate (supracallosal) bundle, corticospinal tract, inferior longitudinal fasciculus, superior longitudinal fasciculus [temporal part, parietal part], and the uncinate fasciculus (UF) in each hemisphere. We checked all reconstructed pathways visually; no failed tracts had aberrant trajectories. At the end of the processing, the software’s output is the FA, AD, RD, and MD values of the most probable voxels in the bundle.
2.5. Statistical Analyses
Shapiro-Wilk and Levene’s tests were used to assess data normality and homogeneity of variance, respectively. For the two groups (FoG and nFoG) separately, we performed linear multiple regressions using the stepwise method to explain the variance of dependent variables (measurements of step initiation: APA duration, APA amplitude normalized, Step length normalized). First, the univariate analyses were used to test which tracts (Forceps Major and Minor, ATR, CAB, CCG, CST, SLFt, SLFp, UF in each hemisphere) would be associated with the dependent variables (APA duration, APA amplitude normalized, Step length normalized). Afterward, to explain the variance of the dependent variables, we included the factors in the linear multivariate analysis using the stepwise model if they presented a P value ≤0.10 and a correlation of lower than 0.6 between them to avoid collinearity [27]. The association between dependent and independent variables was assessed through the Spearman test. Statistical procedures were performed using the software SAS 9.4 (Institute Inc., Cary, NC, USA), and the significance level was set at P≤0.05.
3. Results
Table 1 shows each group’s anthropometric, clinical, biomechanical, and DTI characteristics. There was a significant difference between the groups regarding age, disease duration, L-Dopa dose, and UPDRS score. Patients with FOG were younger, with longer disease duration, higher L-Dopa dose, and had more severe Parkinson’s disease. Regarding biomechanical variables, the FoG group presented lower APA amplitude than nFoG.
Table 2 shows the statistically significant DTI metrics in explaining the measurements of step initiation. For the FoG group, the multiple regression analysis shows that (1) Right Inferior Longitudinal Fasciculus RD explained 31% of APA duration’s variance; (2) Corpus Callosum Forceps Major explained 25% of the step length’s variance. There was a positive correlation between the Right Inferior Longitudinal Fasciculus RD and APA duration (rho = 0.38, p = 0.050) and a negative correlation between Corpus Callosum Forceps Major RD and step length (rho = -0.50, p = 0.010) (Figure 2B). Information about the location of RIFL and CC Forceps Major is in the Supplementary Material.
For the nFoG group, the multiple regression analysis showed that DTI variables were not statistically significant in explaining step initiation.
4. Discussion
Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
This study investigates whether white matter integrity can predict step initiation behavior in individuals with PD and FoG. To address this question, we included the tracts involved in the pathophysiology of PD and FoG in our regression model. This is the first investigation into the relationship between tract integrity and step initiation impairment in individuals with FoG. Our results show that the radial diffusivity in the RILF explained 31% of the variance in APA duration, while the RD in the CC Forceps Major explained 25% in step length in FoG.
Our study provides insights into the role of white matter tracts in modulating step initiation in FoG. These results align with previous research highlighting the importance of white matter tracts in motor control and cognitive functions in PD [15,16,17]. Radial diffusivity (RD) refers to the water diffusion perpendicular to the main axis of the white matter fibers. Changes in RD provide insights into the microstructural integrity of white matter. Increased RD is generally interpreted as losing myelin integrity [28] and is associated with motor and cognitive decline in PD [29]. Specifically, increased RD in extensive white matter circuitry has been suggested to play a role in the pathophysiology of FoG [30,31,32]. The results of Iseki et al. [30] indicated a significant positive correlation between the nFoGq scores and RD values, suggesting that increases in RD reflect a degradation of myelin integrity. This increase in RD was interpreted as indicative of damage to both myelin and axons, which may contribute to the motor difficulties observed in PD, particularly those related to FoG. The analysis also demonstrated that changes in RD were more closely associated with FoG than with other cognitive or gait parameters, highlighting the specificity of these white matter abnormalities to the symptom of FoG in PD.
Step initiation impairments have also been linked with the pathophysiology of FoG. During step initiation, intact inhibitory control allows timely coordination between the interruption of the planning phase associated with the APA and the release of the step [33]. This process is reflected in the APA duration. A longer time to transition from the automatic APA phase to the release of the voluntary step has been associated with FoG [34,35]. A noteworthy finding in our study is the association of the right hemisphere with increased APA duration in the FoG. Prior studies have also reported predominantly right hemisphere impairments in FoG patients, including white matter [20,36,37,38]. Functional brain imaging studies have shown that individuals with FoG often exhibit right-sided deficits [39]. These regions are crucial for integrating sensory information necessary for gait control. Additionally, metabolic imaging studies have revealed lower glucose metabolism in the right parietal cortex [39], suggesting impaired neural activity in this region among FoG. This right-hemisphere predominance highlights the importance of lateralized brain functions in the neural control of gait. It suggests that targeted interventions might need to consider these asymmetries to address FoG effectively.
The RILF’s association with APA duration in our study underscores its involvement in the preparatory phase of the movement, likely reflecting its role in integrating sensory and motor information crucial for step initiation. The RILF connects the occipital and temporal lobes and has been identified as one of the tracts involved in inhibitory circuitry [40]. This finding aligns with existing literature that emphasizes the RILF’s connectivity with regions involved in visuospatial processing and inhibitory control, which are essential for planning and executing movements. Damage to the RILF can lead to difficulties integrating these sensory inputs, disrupting the initiation and smooth continuation of gait. This disruption is particularly evident in PD during movement initiation, where the inability to effectively process visual and spatial cues can result in FoG [41]. Monaghan et al. [42] investigated the association between white matter integrity and improvements in reactive stepping following a training program for individuals with PD. Improvements in step behavior were correlated with greater integrity of RILF and CC. Therefore, the RILF connection highlights how deficits in these areas can exacerbate FoG symptoms by impairing the coordination necessary for step initiation.
Regarding the CC, our results showed that those with smaller step lengths had higher RD in the FoG group. The CC’s role in step length regulation points to its importance in interhemispheric communication and coordination of bilateral motor activities. The step length depends on the integrity of the supporting and stepping leg coordination, which may be controlled by the CC [43]. Dale et al. [44] showed that lesions in the CC led to FoG, possibly due to disrupted callosal connections between the right and left pre-SMA. Accordingly, Wang et al. [45] (2016) showed that FoG patients had more white matter abnormalities in the CC compared to controls. The correlation between reduced step length and RD in the FoG group underscores the importance of CC integrity in maintaining proper leg coordination.
Similar to our results, other studies found that RILF and CC were associated with gait disorders. Tan et al. [46] showed that RILF and CC are more affected in individuals with PD and postural instability gait disorders (PIGD). Wen et al. [47] found strong correlations of motor severity with higher RD of RILF and CC in PIGD compared to the tremor subtype of PD. Pietracupa [37] showed that white matter changes in FoG compared with healthy subjects were prevalent in the RILF and the frontal radiations of the CC, and these abnormalities correlated with cognitive measures, including inhibitory control.
The current study’s results must be interpreted cautiously due to a relatively small sample size, limiting the findings’ generalizability. Also, the cross-sectional design limits the ability to infer causal relationships between white matter integrity and step initiation impairments. Although we controlled for some variables, we did not account for age, disease duration, L-dopa equivalent, and UPDRS, which differed between the groups. However, the FoG group participants were younger than those in the nFoG group, so the regression results cannot be attributed to brain aging. Despite the lack of covariate control, our results remain robust and trustworthy. The methodologies employed were rigorous, with precise measurements of white matter integrity and step initiation impairments, ensuring high reliability.
Our study also reinforces the potential utility of advanced neuroimaging techniques, such as DTI, in elucidating the microstructural changes associated with PD and FoG. DTI metrics provide a sensitive measure of white matter integrity that can reveal subtle but clinically significant changes in neural pathways. This approach not only enhances our understanding of the pathophysiological basis of FoG but also offers a valuable tool for monitoring disease progression and the effects of therapeutic interventions. By identifying specific biomarkers associated with motor impairments, we can improve the precision of clinical assessments and develop more targeted and effective treatment strategies.
Our findings are consistent with previous research, reinforcing their validity. This study underscores the critical role of white matter integrity in the pathophysiology of step initiation impairments in FoG. By demonstrating that increased RD in the RILF and CC significantly correlates with longer APA and reduced step length, respectively, the research highlights the importance of these white matter tracts in motor control. These findings provide valuable insights into the neural mechanisms underlying FoG, suggesting that targeting white matter integrity could be a potential therapeutic avenue. Furthermore, our results underscore the necessity for early detection of white matter deterioration in PD, which could allow for timely and more effective therapeutic interventions. By improving our understanding of the neural underpinnings of FoG, this study lays the groundwork for developing novel diagnostic tools and treatment modalities that specifically address the microstructural changes associated with this debilitating phenomenon. Future studies should focus on validating these findings across diverse populations and exploring the longitudinal impact of therapeutic interventions on white matter integrity and FoG symptoms.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1 - Diffusion tensor imaging (DTI)-based on the Right Inferior Longitudinal Fasciculus. Figure S2 - Diffusion tensor imaging (DTI)-based on the Corpus Callosum Forceps Major.
Author Contributions
Conceptualization, A.C.L.P. and D.B.C.; methodology, A.C.L.P., M.P.N. and D.B.C.; software, A.C.L.P., M.P.N. and D.B.C.; validation, A.C.L.P.; formal analysis, A.C.L.P., M.P.N. and D.B.C.; investigation, A.C.L.P.; writing—original draft preparation, A.C.L.P. and C.E.N.O.; writing—review and editing, E.J.L.A. and D.B.C. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
None.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of University of São Paulo.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lewis, S.J.; Barker, R.A. A Pathophysiological Model of Freezing of Gait in Parkinson’s Disease. Parkinsonism & Related Disorders 2009, 15, 333–338. [Google Scholar] [CrossRef]
- Nutt, J.G.; Bloem, B.R.; Giladi, N.; Hallett, M.; Horak, F.B.; Nieuwboer, A. Freezing of Gait: Moving Forward on a Mysterious Clinical Phenomenon. The Lancet Neurology 2011, 10, 734–744. [Google Scholar] [CrossRef] [PubMed]
- Giladi, N.; Treves, T.A.; Simon, E.S.; Shabtai, H.; Orlov, Y.; Kandinov, B.; Paleacu, D.; Korczyn, A.D. Freezing of Gait in Patients with Advanced Parkinson’s Disease. Journal of Neural Transmission 2001, 108, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Heremans, E.; Nieuwboer, A.; Vercruysse, S. Freezing of Gait in Parkinson’s Disease: Where Are We Now? Curr Neurol Neurosci Rep 2013, 13, 350. [Google Scholar] [CrossRef]
- Moore, O.; Peretz, C.; Giladi, N. Freezing of Gait Affects Quality of Life of Peoples with Parkinson’s Disease beyond Its Relationships with Mobility and Gait. Mov Disord 2007, 22, 2192–2195. [Google Scholar] [CrossRef]
- Schaafsma, J.D.; Balash, Y.; Gurevich, T.; Bartels, A.L.; Hausdorff, J.M.; Giladi, N. Characterization of Freezing of Gait Subtypes and the Response of Each to Levodopa in Parkinson’s Disease. European Journal of Neurology 2003, 10, 391–398. [Google Scholar] [CrossRef]
- Giladi, N.; McDermott, M.P.; Fahn, S.; Przedborski, S.; Jankovic, J.; Stern, M.; Tanner, C. ; The Parkinson Study Group Freezing of Gait in PD: Prospective Assessment in the DATATOP Cohort. Neurology 2001, 56, 1712–1721. [Google Scholar] [CrossRef]
- Snijders, A.H.; Nijkrake, M.J.; Bakker, M.; Munneke, M.; Wind, C.; Bloem, B.R. Clinimetrics of Freezing of Gait. Mov. Disord. 2008, 23, S468–S474. [Google Scholar] [CrossRef] [PubMed]
- Fonoff, E.T.; De Lima-Pardini, A.C.; Coelho, D.B.; Monaco, B.A.; Machado, B.; Pinto De Souza, C.; Dos Santos Ghilardi, M.G.; Hamani, C. Spinal Cord Stimulation for Freezing of Gait: From Bench to Bedside. Front. Neurol. 2019, 10, 905. [Google Scholar] [CrossRef]
- Brugger, F.; Abela, E.; Hägele-Link, S.; Bohlhalter, S.; Galovic, M.; Kägi, G. Do Executive Dysfunction and Freezing of Gait in Parkinson’s Disease Share the Same Neuroanatomical Correlates? Journal of the Neurological Sciences 2015, 356, 184–187. [Google Scholar] [CrossRef]
- Fling, B.W.; Cohen, R.G.; Mancini, M.; Carpenter, S.D.; Fair, D.A.; Nutt, J.G.; Horak, F.B. Functional Reorganization of the Locomotor Network in Parkinson Patients with Freezing of Gait. PLoS One 2014, 9, e100291. [Google Scholar] [CrossRef] [PubMed]
- Kostić, V.S.; Agosta, F.; Pievani, M.; Stefanova, E.; Ječmenica-Lukić, M.; Scarale, A.; Špica, V.; Filippi, M. Pattern of Brain Tissue Loss Associated with Freezing of Gait in Parkinson Disease. Neurology 2012, 78, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Herman, T.; Rosenberg-Katz, K.; Jacob, Y.; Giladi, N.; Hausdorff, J.M. Gray Matter Atrophy and Freezing of Gait in Parkinson’s Disease: Is the Evidence Black-on-white? Movement Disorders 2014, 29, 134–139. [Google Scholar] [CrossRef]
- Tessitore, A.; Amboni, M.; Cirillo, G.; Corbo, D.; Picillo, M.; Russo, A.; Vitale, C.; Santangelo, G.; Erro, R.; Cirillo, M.; et al. Regional Gray Matter Atrophy in Patients with Parkinson Disease and Freezing of Gait. AJNR Am J Neuroradiol 2012, 33, 1804–1809. [Google Scholar] [CrossRef] [PubMed]
- Canu, E.; Agosta, F.; Sarasso, E.; Volonte, M.A.; Basaia, S.; Stojkovic, T.; Stefanova, E.; Comi, G.; Falini, A.; Kostic, V.S.; et al. Brain Structural and Functional Connectivity in Parkinson’s Disease with Freezing of Gait. Hum Brain Mapp 2015, 36, 5064–5078. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.-L.; Ng, K.-M.; Rumpel, H.; Fook-Chong, S.; Li, H.-H.; Tan, E.-K. Transcallosal Diffusion Tensor Abnormalities in Predominant Gait Disorder Parkinsonism. Parkinsonism & Related Disorders 2014, 20, 53–59. [Google Scholar] [CrossRef]
- Gu, Q.; Huang, P.; Xuan, M.; Xu, X.; Li, D.; Sun, J.; Yu, H.; Wang, C.; Luo, W.; Zhang, M. Greater Loss of White Matter Integrity in Postural Instability and Gait Difficulty Subtype of Parkinson’s Disease. Can. J. Neurol. Sci. 2014, 41, 763–768. [Google Scholar] [CrossRef]
- Schlenstedt, C.; Mancini, M.; Nutt, J.; Hiller, A.P.; Maetzler, W.; Deuschl, G.; Horak, F. Are Hypometric Anticipatory Postural Adjustments Contributing to Freezing of Gait in Parkinson’s Disease? Frontiers in Aging Neuroscience 2018, 10, 36. [Google Scholar] [CrossRef]
- de Lima-Pardini, A.C.; Coelho, D.B.; Nucci, M.P.; Boffino, C.C.; Batista, A.X.; de Azevedo Neto, R.M.; Silva-Batista, C.; Barbosa, E.R.; Cohen, R.G.; Horak, F.B.; et al. Brain Networks Associated with Anticipatory Postural Adjustments in Parkinson’s Disease Patients with Freezing of Gait. NeuroImage. Clinical 2020, 28, 102461. [Google Scholar] [CrossRef]
- Fling, B.W.; Cohen, R.G.; Mancini, M.; Nutt, J.G.; Fair, D.A.; Horak, F.B. Asymmetric Pedunculopontine Network Connectivity in Parkinsonian Patients with Freezing of Gait. Brain: A Journal of Neurology 2013, 136, 2405–2418. [Google Scholar] [CrossRef]
- Moreira-Neto, A.; Ugrinowitsch, C.; Coelho, D.B.; De Lima-Pardini, A.C.; Barbosa, E.R.; Teixeira, L.A.; Amaro, E.; Horak, F.B.; Mancini, M.; Nucci, M.P.; et al. Freezing of Gait, Gait Initiation, and Gait Automaticity Share a Similar Neural Substrate in Parkinson’s Disease. Human Movement Science 2022, 86, 103018. [Google Scholar] [CrossRef]
- Silva-Batista, C.; Lira, J.; Coelho, D.B.; De Lima-Pardini, A.C.; Nucci, M.P.; Mattos, E.C.T.; Magalhaes, F.H.; Barbosa, E.R.; Teixeira, L.A.; Amaro Junior, E.; et al. Mesencephalic Locomotor Region and Presynaptic Inhibition during Anticipatory Postural Adjustments in People with Parkinson’s Disease. Brain Sciences 2024, 14, 178. [Google Scholar] [CrossRef]
- Seto, E.; Sela, G.; McIlroy, W.E.; Black, S.E.; Staines, W.R.; Bronskill, M.J.; McIntosh, A.R.; Graham, S.J. Quantifying Head Motion Associated with Motor Tasks Used in fMRI. NeuroImage 2001, 14, 284–297. [Google Scholar] [CrossRef] [PubMed]
- Moineau, B.; Boisgontier, M.P.; Barbieri, G.; Nougier, V. A New Method to Assess Temporal Features of Gait Initiation with a Single Force Plate. Gait & Posture 2014, 39, 631–633. [Google Scholar] [CrossRef]
- Lindroth, H.; Nair, V.A.; Stanfield, C.; Casey, C.; Mohanty, R.; Wayer, D.; Rowley, P.; Brown, R.; Prabhakaran, V.; Sanders, R.D. Examining the Identification of Age-Related Atrophy between T1 and T1 + T2-FLAIR Cortical Thickness Measurements. Sci Rep 2019, 9, 11288. [Google Scholar] [CrossRef]
- Yendiki, A. Automated Probabilistic Reconstruction of White-Matter Pathways in Health and Disease Using an Atlas of the Underlying Anatomy. Front. Neuroinform. 2011, 5. [Google Scholar] [CrossRef]
- Dormann, C.F.; Elith, J.; Bacher, S.; Buchmann, C.; Carl, G.; Carré, G.; Marquéz, J.R.G.; Gruber, B.; Lafourcade, B.; Leitão, P.J.; et al. Collinearity: A Review of Methods to Deal with It and a Simulation Study Evaluating Their Performance. Ecography 2013, 36, 27–46. [Google Scholar] [CrossRef]
- Winklewski, P.J.; Sabisz, A.; Naumczyk, P.; Jodzio, K.; Szurowska, E.; Szarmach, A. Understanding the Physiopathology Behind Axial and Radial Diffusivity Changes—What Do We Know? Front. Neurol. 2018, 9, 92. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.; Wu, Z.; Long, J.; Li, W.; Wang, X.; Hu, N.; Zhao, X.; Sun, T. White Matter Changes in Parkinson’s Disease. npj Parkinsons Dis. 2023, 9, 150. [Google Scholar] [CrossRef]
- Iseki, K.; Fukuyama, H.; Oishi, N.; Tomimoto, H.; Otsuka, Y.; Nankaku, M.; Benninger, D.; Hallett, M.; Hanakawa, T. Freezing of Gait and White Matter Changes: A Tract-Based Spatial Statistics Study. J Clin Mov Disord 2015, 2, 1. [Google Scholar] [CrossRef]
- Kou, W.; Wang, X.; Zheng, Y.; Zhao, J.; Cai, H.; Chen, H.; Sui, B.; Feng, T. Freezing of Gait in Parkinson’s Disease Is Associated with the Microstructural and Functional Changes of Globus Pallidus Internus. Front. Aging Neurosci. 2022, 14, 975068. [Google Scholar] [CrossRef] [PubMed]
- Lench, D.H.; Keith, K.; Wilson, S.; Padgett, L.; Benitez, A.; Ramakrishnan, V.; Jensen, J.H.; Bonilha, L.; Revuelta, G.J. Neurodegeneration of the Globus Pallidus Internus as a Neural Correlate to Dopa-Response in Freezing of Gait. JPD 2022, 12, 1241–1250. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.G.; Nutt, J.G.; Horak, F.B. Errors in Postural Preparation Lead to Increased Choice Reaction Times for Step Initiation in Older Adults. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 2011, 66A, 705–713. [CrossRef]
- Coelho, D.B.; Ribeiro De Souza, C.; De Lima-Pardini, A.C.; Treza, R.D.C.; Shida, T.K.F.; Silva-Batista, C.; Teixeira, L.A. Is Freezing of Gait Correlated with Postural Control in Patients with Moderate-to-severe Parkinson’s Disease? Eur J of Neuroscience 2021, 53, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Peterson, D.S.; Van Liew, C.; Stuart, S.; Carlson-Kuhta, P.; Horak, F.B.; Mancini, M. Relating Parkinson Freezing and Balance Domains: A Structural Equation Modeling Approach. Parkinsonism & Related Disorders 2020, 79, 73–78. [Google Scholar] [CrossRef]
- Bartels, A.L.; Leenders, K.L. Brain Imaging in Patients with Freezing of Gait. Mov. Disord. 2008, 23, S461–S467. [Google Scholar] [CrossRef] [PubMed]
- Pietracupa, S.; Suppa, A.; Upadhyay, N.; Giannì, C.; Grillea, G.; Leodori, G.; Modugno, N.; Di Biasio, F.; Zampogna, A.; Colonnese, C.; et al. Freezing of Gait in Parkinson’s Disease: Gray and White Matter Abnormalities. J Neurol 2018, 265, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Youn, J.; Lee, J.-M.; Kwon, H.; Kim, J.S.; Son, T.O.; Cho, J.W. Alterations of Mean Diffusivity of Pedunculopontine Nucleus Pathway in Parkinson’s Disease Patients with Freezing of Gait. Parkinsonism & Related Disorders 2015, 21, 12–17. [Google Scholar] [CrossRef]
- Bartels, A.L.; De Jong, B.M.; Giladi, N.; Schaafsma, J.D.; Maguire, R.P.; Veenma, L.; Pruim, J.; Balash, Y.; Youdim, M.B.H.; Leenders, K.L. Striatal Dopa and Glucose Metabolism in PD Patients with Freezing of Gait. Movement Disorders 2006, 21, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Tsapanou, A.; Qolamreza, R.R.; Gazes, Y. White Matter Integrity Mediates Decline in Age-Related Inhibitory Control. Behavioural Brain Research 2018, 339, 249–254. [Google Scholar] [CrossRef]
- Almeida, Q.J.; Lebold, C.A. Freezing of Gait in Parkinson’s Disease: A Perceptual Cause for a Motor Impairment? J Neurol Neurosurg Psychiatry 2010, 81, 513–518. [Google Scholar] [CrossRef]
- Monaghan, A.S.; Ofori, E.; Fling, B.W.; Peterson, D.S. Associating White Matter Microstructural Integrity and Improvements in Reactive Stepping in People with Parkinson’s Disease. Brain Imaging and Behavior 2024. [CrossRef] [PubMed]
- Richmond, S.B.; Peterson, D.S.; Fling, B.W. Bridging the Callosal Gap in Gait: Corpus Callosum White Matter Integrity’s Role in Lower Limb Coordination. Brain Imaging and Behavior 2022, 16, 1552–1562. [Google Scholar] [CrossRef] [PubMed]
- Dale, M.L.; Mancini, M.; Curtze, C.; Horak, F.B.; Fling, B.W. Freezing of Gait Associated with a Corpus Callosum Lesion. J Clin Mov Disord 2016, 3, 2. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Jiang, S.; Yuan, Y.; Zhang, L.; Ding, J.; Wang, J.; Zhang, J.; Zhang, K.; Wang, J. Alterations of Functional and Structural Connectivity of Freezing of Gait in Parkinson’s Disease. J Neurol 2016, 263, 1583–1592. [Google Scholar] [CrossRef]
- Tan, S.Y.Z.; Keong, N.C.H.; Selvan, R.M.P.; Li, H.; Ooi, L.Q.R.; Tan, E.K.; Chan, L.L. Periventricular White Matter Abnormalities on Diffusion Tensor Imaging of Postural Instability Gait Disorder Parkinsonism. AJNR Am J Neuroradiol 2019, ajnr;ajnr.A5993v1. [CrossRef]
- Wen, M.-C.; Heng, H.S.E.; Lu, Z.; Xu, Z.; Chan, L.L.; Tan, E.K.; Tan, L.C.S. Differential White Matter Regional Alterations in Motor Subtypes of Early Drug-Naive Parkinson’s Disease Patients. Neurorehabil Neural Repair 2018, 32, 129–141. [Google Scholar] [CrossRef]
Figure 1.
Stepping initiation task on a force plate. (A) command to relax; (B) command to prepare; (C) command to step; (D) Biomechanical variables at the step initiation were analyzed based on the signal from the mediolateral center of pressure (CoPml).
Figure 1.
Stepping initiation task on a force plate. (A) command to relax; (B) command to prepare; (C) command to step; (D) Biomechanical variables at the step initiation were analyzed based on the signal from the mediolateral center of pressure (CoPml).
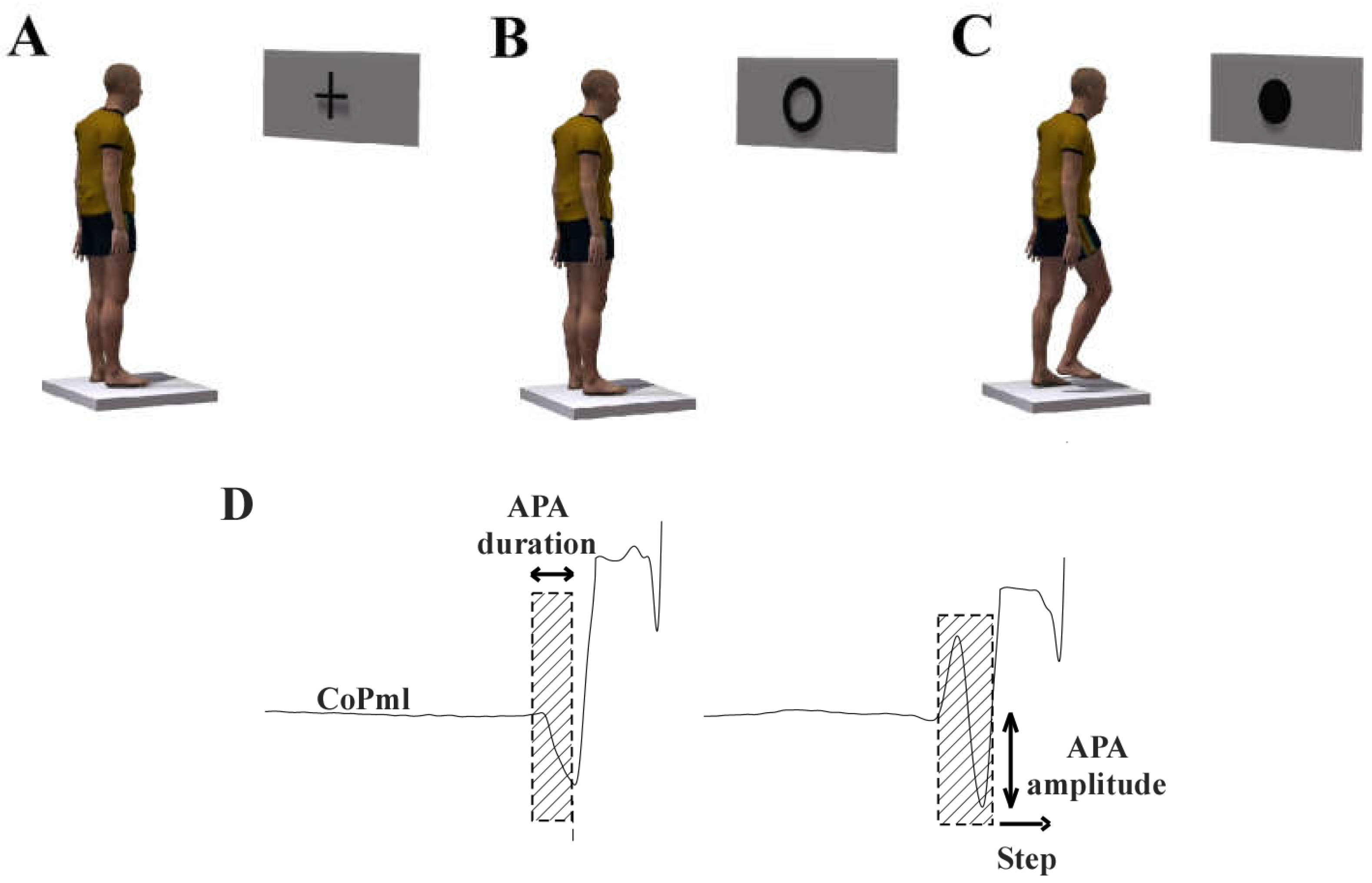
Figure 2.
For the FoG group, scatter plot between the (A) APA duration and Right Inferior Longitudinal Fasciculus RD. (B) Step length normalized and Corpus Callosum Forceps Major RD. APA: anticipatory postural adjustment. FoG: freezing of gait.
Figure 2.
For the FoG group, scatter plot between the (A) APA duration and Right Inferior Longitudinal Fasciculus RD. (B) Step length normalized and Corpus Callosum Forceps Major RD. APA: anticipatory postural adjustment. FoG: freezing of gait.
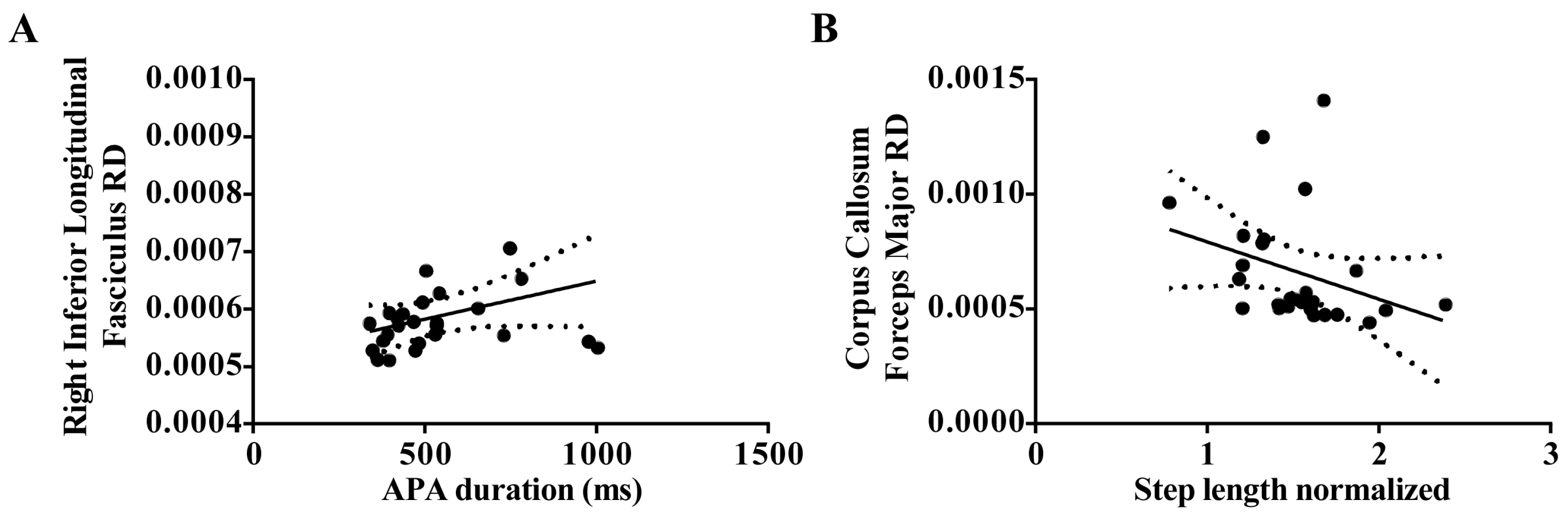

Table 1.
Average (standard deviation) of anthropometric, clinical, and biomechanical in the FoG and nFoG groups.
Table 1.
Average (standard deviation) of anthropometric, clinical, and biomechanical in the FoG and nFoG groups.
| FoG (n = 26) | nFoG (n = 17) | p-value | |
|---|---|---|---|
| Age (years) | 60.23 ± 11.21 | 67.35 ± 6.19 | 0.011 * |
| Disease duration (years) | 13.00 ± 5.72 | 6.55 ± 4.09 | 0.001 * |
| L-Dopa equivalent units (mg•day-1) | 760.71 ± 476.88 | 437.50 ± 291.07 | 0.014 * |
| MoCA | 18.07 ± 2.84 | 18.41 ± 2.27 | 0.709 |
| UPDRS-III (score) | 34.92 ± 9.74 | 27.53 ± 10.55 | 0.027 * |
| nFoGq (score) | 18.92 ± 5.56 | - | - |
| APA duration (ms) | 543.74 ± 186.02 | 488.60 ± 93.76 | 0.266 |
| APA amplitude | 0.44 ± 0.12 | 0.55 ± 0.14 | 0.009 * |
| Step length normalized | 1.53 ± 0.32 | 1.72 ± 0.33 | 0.074 |
APA = anticipatory postural adjustment; ML force = mediolateral force; UPDRS-III = Unified Parkinson’s Disease Scale motor part; nFoGq = Freezing of Gait Questionnaire. MoCA = Montreal Cognitive Assessment.
Table 2.
Stepwise multiple regression analysis results with DTI variables and step initiation as dependent variables.
Table 2.
Stepwise multiple regression analysis results with DTI variables and step initiation as dependent variables.
| Group | Step initiation | DTI variables | Partial (r2) | p-value |
|---|---|---|---|---|
| FoG | APA duration | Right Inferior Longitudinal Fasciculus RD | 0.31 | 0.009 |
| FoG | Step length | Corpus Callosum Forceps Major RD | 0.25 | 0.02 |
APA = anticipatory postural adjustment.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



