
Submitted:
23 July 2024
Posted:
24 July 2024
You are already at the latest version
Abstract
Background: This is a propensity matched, single centre study of limited versus extended resections for Type A acute aortic dissections (AAAD). Methods: Retrospective data for 440 patients with acute Type A aortic dissection repairs (Limited Resection, LR-215, Extended Resection, ER-225). 109 pairs were propensity matched to LR versus ER. Multivariate analysis was performed for inpatient death, long term survival and composite of inpatient death/TIA/stroke. Kaplan Meier survival curves were compared at 1, 3, 5, 10 and 15 years using the log-rank test. Results: Mean age was 66.9±13 years and mean follow up was 5.3±4.7 years. 48.9% had LR. In-hospital mortality was 10% (LR;6% vs ER;13.8%, p<0.01). ER, NYHA class, salvage surgery and additional procedures were predictors of increased mortality in unmatched data. Propensity matched data showed no difference in TIA/stroke rates, LOS, in-patient mortality or composite outcomes. LR had better survival (LR; 77.1% vs ER; 51.4%, p<0.001). ER (OR; 1.97, 95%CI; 1.27, 3.08, p=0.003) was a significant predictor of worse long term survival. At 15 years, aortic re-operation was 17% and freedom from re-operation and death was 42%. Conclusions: Type A aortic dissection repair has high mortality and morbidity although results have improved over two decades. ER was predictor of worse perioperative results and long term survival.
Keywords:
acute aortic dissection
; type A
; stanford type A
1. Introduction
Stanford type A acute aortic dissection (AAAD) represents a life-threatening surgical emergency. The surgical mortality remains high despite several advances in the operative techniques, neuro-cerebral monitoring, neuroprotection and postoperative care [1,2].
Clinical presentation and extent of surgery remain the major determinants of early and late outcomes in addition to operator experience and surgical volumes. Data on medium and long term survival however remains scarce even in large international databases. There remain several controversies regarding cannulation strategies, neuroprotection, identification and resection of tears, closed versus open distal anastomosis, extent of resection and fate of residual ‘downstream’ aorta and its impact on late re-interventions and survival.
There has been further proliferation of devices recently that enable a single stage stabilization of the downstream aorta with an extended resection with an open hybrid stent graft at the time of the primary repair of AAAD. This also facilitates resection and/or stabilization of difficult tears especially in the arch and proximal descending thoracic aorta. Extended resections with resection of the arch and reattachment of the head and neck vessels are technically much more challenging than limited resections of the ascending aorta. The role and indications for extended resections for AAAD remain undefined. Guidelines suggest that should be undertaken by aortic surgeons in high volume aortic centers only.
Extended resections are associated with longer cross clamp times, bypass times and operative times. The periods of deep hypothermic circulatory arrest and cerebral perfusion are also longer contributing to increased morbidity of adverse neurological outcomes. The long term neurological sequelae of extended resections including those on memory and motor function are not well known.
Our working hypothesis based on conventional wisdom was that extended resections have greater morbidity and mortality in the perioperative period and worse long term survival compared to limited resections.
The aims of this study were
- evaluate peri-operative outcomes and late survival of AAAD repair
- compare limited versus extended resections.
2. Materials and Methods
Population
The study was conducted as per the STROBE (Strengthening the reporting of observational studies in epidemiology) guidelines. Data for AAAD repairs was retrospectively collected (January 2000 – January 2019) from PAS (Patient Administration System). AAAD was defined as any dissection that involved the ascending aorta and presenting within 2 weeks of symptoms. Patients who refused the operation, underwent a conservative management or died before the operation were excluded. Data was processed in compliance with institutional data policies (SEV/0697). Consent for individual use was waived due to nature of study and prior approval at the time of consent. Long term survival statistics were collected from Patient Administration System (e-CAMIS) and the National Healthcare Service Spine Portal Summary Care Records (SCR). Baseline demographics included age, sex, New York Heart Association (NYHA) class, Canadian Cardiovascular Society (CCS) class, prior cardiac surgery, diabetes, hypertension, smoking status, renal and pulmonary disease, obesity (BMI>28), peripheral vascular disease, left ventricular ejection fraction, emergent or salvage surgery, aortic arch procedure, additional cardiac procedure, unstable status and EuroSCORE. Emergency surgery was defined as that done before the next day after decision for surgery was made. Salvage was defined as requiring cardiopulmonary resuscitation en route to theatre or prior to induction of anesthesia.
Operative Techniques
All operations were performed through a median sternotomy. Cannulation site was chosen according to aortic CT findings, technical feasibility of access and surgeons preference for techniques [3]. Cold blood cardioplegia was used for myocardial protection. The ascending aorta was replaced with an interposition graft. Extent of aortic resection (ascending aorta, hemi-arch or arch with conventional or frozen elephant trunk operation) and aortic root repair or replacement and any other additional procedures were based on preoperative scans, trans-oesophageal echocardiogram, intraoperative inspection, location of tears and surgeon’s preference.
Limited resections (LR) included ascending aorta resection and interposition grafts with a closed distal anastomosis. Extended resections (ER) included resections of distal ascending aorta, hemi-arch or arch with/without re-implantation of neck vessels or variations of frozen elephant trunk operation. An open distal aortic reconstruction or frozen elephant trunk operation under deep hypothermic circulatory arrest (DHCA) was usually performed in presence of an intimal tear extending into the aortic arch or crossing the clamp area. Cerebral protection for open anastomosis was achieved with either DHCA, or DHCA with antegrade/retrograde cerebral perfusion. Near infrared spectroscopy was used after 2010 for noninvasive, continuous cerebral oxygen saturation monitoring of balance between oxygen delivery and extraction of the cerebral cortex. Infrared light emitting diode sensors were bilaterally placed on the forehead for measurement. Bilateral similar values above 60% were maintained. These correlate with venous cerebral saturations. Higher perfusion pressures or selective perfusion with cannulation of the left carotid ostium from inside the arch was used for persist low levels.
Statistical and Propensity Score Analysis
Distributions were visually inspected and normality was tested by a Shapiro-Wilcoxon W test. Continuous variables were compared using Mann-Whitney test (or student’s t-test for normal distributions) and categorical variables by Fisher’s exact test or chi-squared test. Sixteen preoperative variables (Table 3). Variables with p<0.2 on univariate analysis were entered in multivariate analysis to identify independent predictors of in-patient death and composite of in-patient death/TIA/stroke. The arbitrary p<0.2 value provides enough predictive value even without statistical significance to warrant further investigation in the multivariate analysis. A more stringent lower value would make the model too exacting at risk of excluding clinically relevant variables that are known to affect outcomes from experience and review of literature. The clinically relevant non-intercorrelated variables that have been known to predict adverse perioperative outcomes and worse survival in literature were included in the multivariable analysis to test their predictive value in addition to statistical significance.
Kaplan Meier survival curves were compared at 1, 3, 5, 10 and 15 years using log-rank test. Cox proportional hazards model was used to determine predictors of long term survival. Proportionality assumption was tested with Schoenfeld residuals. Propensity scores were calculated using logistic regression and ER patients were posteriorly matched in a 1:1 ratio with LR by the nearest neighbor method with caliper width of 0.2 of the standard deviation of propensity score logit. Means, standard deviations and proportions of baseline demographic were compared to assure appropriate balance; statistical significance was tested using a Wilcoxon signed-rank paired test and McNemar’s test for continuous and categorical variables, respectively. Standardized differences were used for appropriate balance for bias <10% (Supplementary Figure S1).
3. Results
AAAD repair was performed in 440 patients [LR – 215 (48.7%), ER – 225 (51.3%)] (Supplementary Table S1). Mean age was 66.9±13 years and mean follow up was 5.3±4.7 years. 48.9% patients had LR. 16.8% were unstable at presentation and 8% needed a salvage operation. 20% had an additional cardiac procedure. A fifth of the patients had an arch procedure (hemiarch, total arch or a frozen elephant trunk operation). One hundred nine patients with ER were propensity matched to LR (Supplementary Table S2).
3.1. Operative Results
There was no significant difference in the bypass times (LR; 173 min vs ER; 191 min, p=0.225) and cross clamp times (LR; 99 min vs ER; 99 min, p= 0.862) (Table 1). Mean total circulatory arrest time for ER was 27 min (IQR; 18-33.5 min). Overall, TIA/stroke rate was 18.4%. There was no difference in perioperative TIA/stroke (LR; 16.3% vs ER; 20.4%, p=0.474). Overall length of stay was 12 days (IQR – 8-20 days, LR; 12 days vs ER; 11 days, p=0.012). In-hospital mortality was 10% (LR; 6% vs ER; 13.8%, p<0.01).
After propensity matching, there was no difference between LR and ER in TIA/stroke rates, length of stay, in-patient mortality or composite outcomes (Table 1).
ER (OR; 2.92, 95%CI; 1.36, 6.29, p=0.006), NYHA class (OR; 2.49, 95%CI; 1.10, 5.63, p=0.029), salvage surgery (OR; 3.60, 95%CI; 1.27, 10.17, p=0.016) and additional cardiac procedures (OR; 2.23, 95% CI;1.01, 4.92, p=0.047) were predictors of increased inpatient mortality (Supplementary Table S3). Salvage surgery, bypass time and age > 70yrs were predictors of worse composite outcomes (Table 2). Operative mortality for salvage and non-salvage cases was 25.7% vs 8.6% (p=0.001).
ER was a predictor of increased in-patient mortality (OR; 2.92, CI; 1.36, 6.29, p=0.006), worse composite outcomes (OR; 1.44, CI; 0.91, 2.29, p=0.12) and reduced long term survival (OR; 1.97, CI; 1.27, 3.08, p=0.003).
Cox regression identified ER (OR; 1.97, 95% CI; 1.27, 3.08, p=0.003), NYHA class (OR; 2.08, 95% CI; 1.30 to 3.33, p=0.002), prior cardiac surgery (OR;1.75, 95% CI; 1.02 to 2.99, p=0.041) and age>70 years (OR;2.00, 95% CI; 1.34 to 3.00, p=0.001) as significant predictors of worse long term survival (Table 3).
Survival in propensity matched pairs was better for LR (LR; 77.1% vs ER; 51.4%, p<0.001) (Table 3, Figure 1). Patients with DHCA and cerebral perfusion had worse long term survival (Supplementary Figure S2). Age >75 did not have worse survival (supplementary Figure S3).
3.2. Comment
Institutional studies and registries have reported mortality of 17-28% for AAAD repair (GERAADA (2006-14); 19.5%, JCSD (2008-15); 9.5%, IRAD (2010-13); 18.4%, NORCAAD (2005-14); 17.6%)) [4,5,6,7]. The overall mortality in our series was 10% (2000-19) with changes in operative techniques, use of ante-flow cannulation, antegrade cerebral perfusion and use of near infrared spectroscopy. Stroke remains a devastating complication. STS NACSD (2014-17) reported stroke rate of 13% [8]. Axillary cannulation was associated with lower risk of stroke versus femoral (odds ratio, 0.60; P < .001). Retrograde cerebral perfusion (odds ratio, 0.75; P = 0.008) was associated with reduced risk compared with no cerebral perfusion or antegrade cerebral perfusion. Total arch replacement, longer circulatory arrest time, cerebral perfusion time, and cardiopulmonary bypass time were all related to higher risk of postoperative stroke. Critical status, preoperative hypotension, shock or cardiopulmonary resuscitation, malperfusion syndrome and neurologic deficit have been associated with a poor operative outcomes.
Age>70 years was an independent risk for mortality in IRAD registry. Surgery was significantly better than medical management even in > 80 yrs. In JCSD registry (mean age 69 yrs), age was a significant risk factor for both limited and extended resections involving the arch. GERAADA showed a significantly higher in-hospital mortality for octogenarians (OR; 3.23, 34.9% vs 15.8%, p < 0.001). In our experience, age >70 years was not a predictor of inpatient death but adversely affected the composite outcome of TIA/stroke/inpatient death (OR; 1.69, 95% CI; 1.05, 2.71, p=0.031). Age >70 years was also a strong predictor of poor late survival.
Our results are striking for the following reasons:
- a)
- propensity matched in-hospital mortality and composite outcomes were similar for ER and LR.
- b)
- long term survival for extended resections was worse than limited resections.
- c)
- risk of aortic re-operation was very low at 10% at 10 years and 17% at 15 years.
Evidence for extent of resection remains conflicting and results differ for specialist and non-specialist units. Between 2004 and 2016, the STS Adult Cardiac Surgery Database reported that AAAD repairs involved the ascending aorta only in 54% of patients and arch interventions in 46% [9]. Early mortality remained high regardless of extent of aortic resection (30-day mortality was 18.9% for ascending only operations vs 19.8% for arch resections, p=0.09). However Japanese experience with more extensive resections and arch intervention in AAAD repair especially with frozen elephant trunk (FET) operations has shown consistently better results. In 426 AAAD repairs, Asakura et al. had no difference in thirty-day mortality and neurological dysfunction between the FET and no FET groups (1.4% vs 2.4%, p = 0.50 and 5.0% vs 6.3%, p = 0.61, respectively) [10]. Long-term survival was better with FET (p = 0.008). Freedom from distal thoracic re-intervention was similar (p=0.74). After propensity matching, freedom from aortic-related death was better with FET (p=0.044). In the ARCH database, 978 patients who underwent total aortic arch replacement for AAAD with or without FET showed significant differences for permanent neurologic deficits (11.9% vs 10.1%, p=0.59) and spinal cord injury (4.0% vs 6.3%, p=0.52). After post-hoc propensity-score stratification, FET was associated with a significantly lower mortality risk (odds ratio, 0.47; P = .03). In a pooled meta-analysis of 38 studies by Smith et al., hospital mortality for extended arch techniques was 8.6% (95% CI 7.2-10.0) (11.9% for total arch, 8.6% total arch and frozen stented elephant trunk, 6.3% hemiarch and frozen stented elephant trunk and 5.5% total arch and ‘warm’ stent graft) [11]. Stroke was 5.7% (95% CI 3.6-8.2) and spinal cord ischemia was 2.0% (95% CI 1.2-3.0). There is an emerging expert consensus for the safety of concomitant repair of the downstream aorta in specialist aortic centers [12]. Extended resections have been shown to be safe with excellent mid and long term outcomes of ‘downstream aortic re-modelling’ with various modifications of FET in AAAD repair for specialist aortic units.
Guidelines and consensus papers favour an open distal repair in AAAD repair [13]. Despite technical advantages in constructing the distal anastomosis with an excellent visualization while providing a more radical resection of pathological wall, there is no evidence that this technique carries lower mortality or morbidity. 50% of the dissection repairs in this series were done with a closed distal technique compared to 14-41% in literature. The choice between these two approaches for distal aortic repair was based mainly on anatomical factors associated with the dissection (i.e., extension beyond the ascending aorta, primary intimal tear located in the aortic root or the ascending aorta and need for arch intervention) but was influenced mainly by surgeon preferences and idiosyncrasies of individual techniques. The limited resections have advantages of a quicker operation, avoiding prolonged hypothermic circulatory arrest and its attendant complications [14]. Disadvantages include cross clamping the dissected aorta with risk of rupture and malperfusion, inability to evaluate for additional tears, limited resection of the ascending aorta and technically more difficult distal anastomosis. AAAD dissection repair is essentially a lifesaving procedure that should be done without increasing the complexity of the operation. Proponents of conservative resection argue that most emergency AAADs are referred to peripheral non-aortic referral centers, where the treating surgeons have limited proficiency and experience in complex emergency resections [15]. The need for re-interventions for ‘downstream problems’ of re-entry tears and growth of distal aorta is less than 10-15% in a safe, elective setting with low mortality. This ‘less is more’ approach of limited ascending aortic resection is primarily aimed at preventing the life threatening detumescence and rupture of the dissected aorta. A meta-analysis of 9 studies found lower early mortality (RR = 0.69, p=0.005) but higher incidence of postoperative aortic events including re-operation of distal aorta (RR = 3.14, p<0.001) with limited proximal aortic resections [16]. The extent of aortic resection did not adversely affect perioperative stroke (RR; 0.73, 95% CI 0.30-1.78, p=0.50) or long-term survival (HR = 1.02, 95% CI 0.51-2.06, p=0.96).
Is it necessary to identify and resect additional tears and does the false lumen patency affect long term survival? Kim et al. identified re-entry tears in proximal descending thoracic aorta (38.5%), distal DTA (25.2%) and abdominal aorta (41.7%) in 309 non-syndromic AAAD repairs [17]. Multivariate analysis showed proximal DTA re-entry tear was an independent risk factor for aortic re-intervention (HR; 4.955;p<0.01) and significant aortic expansion (HR; 4.214p= 0.002). Lin et al. noted that persistent false lumen presents faster expansion of aortic diameter (B=5.935, 95% CI; 0.35, 11.52; p=0.038) and growth rate>5mm/year (P=0.029) [18]. However, persistent false lumen did not predict post-discharge mortality (P=0.479). Multiple other studies have shown that the number of distal tears adversely affect the rate of aortic growth and false lumen patency is associated with late events and adverse long term survival [19,20]. Open distal anastomosis is associated with a higher rates of distal false lumen thrombosis. However, despite this presumed better evolution of the downstream aorta, survival benefit of open distal anastomosis is not superior to closed distal anastomosis.
Long term survival data is one of the strengths of our study. This compares favorably with other large single institutional studies. Mid and long term survival data even in multicenter studies and registries are still scarce. GERAADA has not yet provided mid-term data, while IRAD investigators reported only 3-years survival rate for a minority of the patients enrolled in the registry.
In our experience, surgical re-interventions for ‘downstream aorta’ were rare. Despite indications for surgery, some of these patients may have been managed conservatively, especially during the earlier periods of the study. The single most important determining factor for the extent of resection and survival is the surgeon. These arguments for lesser resection probably do not apply to high volume, specialist aortic centres with The text continues here.
4. Limitations
This was a singe center, retrospective analysis. Vicissitudes and idiosyncrasies of operative techniques with multiple surgeons in this series spanning a period of 2 decades remains an uncorrected confounder. There were significant improvements in operative monitoring and perioperative care in the latter decade. This is historical data over 2 decades before the advances with covered and noncovered hybrid open stents. Information regarding cause of death during follow-up was not available so cardiovascular and non-cardiovascular deaths could not be separated. Radiological follow up for false lumen patency, additional tears and ‘downstream problems’ was not available for much of our historical data.
5. Conclusions
AAAD repair remains a procedure with high mortality and morbidity, needing prolonged hospitalization and recuperation. Operative results have improved with changes in operative techniques and cerebral monitoring. Age is not a risk factor for early mortality although stroke rates and late survival is worse. Salvage surgery has poor outcomes. Limited aortic resections have improved early and long term survival.
6. Future Directions
The registry data remains sparse on long term outcomes. Possibly lifelong follow up is required for registries. This could be achieved by linking to national death registries to capture long term survival including specific cause of death whether aortic or non-aortic. Data fields to capture extent of resection and further details contributing to detailed analysis of peri-operative outcomes are also lacking in the databases. These would need to be updated with increasing trends for extended resections especially with the use of hybrid open stent grafts. These would also inform decisions about re-interventions for delayed complications and progression of disease. There is also a lack of uniformity of datafields and definitions of datapoints in different national and international aortic databases and registries for inter-registry comparison and meaningful meta-analysis of results. Further research is needed in cerebral perfusion and protection strategies to reduce the high morbidity of adverse neurological outcomes in the peri-operative period. Salvage surgery still has very high operative morbidity and mortality for AAAD. Further research in operative techniques and open/ percutaneous stent grafts may be needed to improve these results.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
References
- Conzelmann LO, Weigang E, Mehlhorn U, Abugameh A, Hoffmann I, Blettner M, Etz CD, Czerny M, Vahl CF; GERAADA Investigators. Mortality in patients with acute aortic dissection type A: analysis of pre- and intraoperative risk factors from the German Registry for Acute Aortic Dissection Type A (GERAADA). Eur J Cardiothorac Surg. 2016, 49, e44–e52. [Google Scholar] [CrossRef] [PubMed]
- Pape LA, Awais M, Woznicki EM, Suzuki T, Trimarchi S, Evangelista A, Myrmel T, Larsen M, Harris KM, Greason K, Di Eusanio M, Bossone E, Montgomery DG, Eagle KA, Nienaber CA, Isselbacher EM, O’Gara P. Presentation, Diagnosis, and Outcomes of Acute Aortic Dissection: 17-Year Trends From the International Registry of Acute Aortic Dissection. J Am Coll Cardiol. 2015, 66, 350–8. [Google Scholar]
- Malvindi PG, Modi A, Miskolczi S, Kaarne M, Velissaris T, Barlow C, Ohri SK, Tsang G, Livesey S. Open and closed distal anastomosis for acute type A aortic dissection repair. Interact Cardiovasc Thorac Surg. 2016, 22, 776–83. [Google Scholar] [CrossRef] [PubMed]
- Evangelista A, Isselbacher EM, Bossone E, Gleason TG, Eusanio MD, Sechtem U, Ehrlich MP, Trimarchi S, Braverman AC, Myrmel T, Harris KM, Hutchinson S, O’Gara P, Suzuki T, Nienaber CA, Eagle KA; IRAD Investigators. Insights From the International Registry of Acute Aortic Dissection: A 20-Year Experience of Collaborative Clinical Research. Circulation. 2018, 137, 1846–1860. [Google Scholar] [CrossRef] [PubMed]
- Pape LA, Awais M, Woznicki EM, Suzuki T, Trimarchi S, Evangelista A et al. Presentation, diagnosis, and outcome of acute aortic dissection: 17-year trends from the International Registry of Acute Aortic Dissection. J Am Coll Cardiol, 2015; 66, 350–358.
- Reutersberg B, Salvermoser M, Trenner M, Geisbüsch S, Zimmermann A, Eckstein HH, Kuehnl A. Hospital Incidence and In-Hospital Mortality of Surgically and Interventionally Treated Aortic Dissections: Secondary Data Analysis of the Nationwide German Diagnosis-Related Group Statistics From 2006 to 2014. J Am Heart Assoc. 2019, 8, e011402.
- Abe T, Yamamoto H, Miyata H, Motomura N, Tokuda Y, Tanemoto K, Usui A, Takamoto S. Patient trends and outcomes of surgery for type A acute aortic dissection in Japan: an analysis of more than 10 000 patients from the Japan Cardiovascular Surgery Database. Eur J Cardiothorac Surg. 2020, 57, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Ghoreishi M, Sundt TM, Cameron DE, et al. Factors associated with acute stroke after type A aortic dissection repair: An analysis of the Society of Thoracic Surgeons National Adult Cardiac Surgery Database. J Thorac Cardiovasc Surg. 2020, 159, 2143–2154.e3. [Google Scholar] [CrossRef] [PubMed]
- Helder MRK, Schaff HV, Day CN, Pochettino A, Bagameri G, Greason KL, Lansman SL, Girardi LN, Storlie CB, Habermann EB. Regional and Temporal Trends in the Outcomes of Repairs for Acute Type A Aortic Dissections. Ann Thorac Surg. 2020, 109, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Yoshitake A, Tochii M, Tokunaga C, Hayashi J, Takazawa A, Yamashita K, Chubachi F, Hori Y, Nakajima H, Iguchi A, Gatate Y, Nakano S, Asakura T. Early and long-term results of total arch replacement with the frozen elephant trunk technique for acute type A aortic dissection. Eur J Cardiothorac Surg. 2020, 58, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Smith HN, Boodhwani M, Ouzounian M, Saczkowski R, Gregory AJ, Herget EJ, Appoo JJ. Classification and outcomes of extended arch repair for acute Type A aortic dissection: a systematic review and metaanalysis. Interact Cardiovasc Thorac Surg. 2017, 24, 450–459. [Google Scholar]
- Luthra S, Tsang GM. Concurrent stabilization of “downstream” aorta during acute type A aortic dissection repair. J Thorac Cardiovasc Surg. 2023, 165, 586–588. [Google Scholar] [CrossRef] [PubMed]
- Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, Evangelista A, Falk V, Frank H, Gaemperli O, Grabenwöger M, Haverich A, Iung B, Manolis AJ, Meijboom F, Nienaber CA, Roffi M, Rousseau H, Sechtem U, Sirnes PA, Allmen RS, Vrints CJ; ESC Committee for Practice Guidelines. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J. 2014, 35, 2873–926. [Google Scholar]
- Dib B, Seppelt PC, Arif R, Weymann A, Veres G, Schmack B, Beller CJ, Ruhparwar A, Karck M, Kallenbach K. Extensive aortic surgery in acute aortic dissection type A on outcome - insights from 25 years single center experience. J Cardiothorac Surg. 2019, 14, 187. [Google Scholar] [CrossRef] [PubMed]
- Lansman, SL. Commentary: Is more always better? J Thorac Cardiovasc Surg. 2019, 158, 1282. [Google Scholar] [CrossRef] [PubMed]
- Yan Y, Xu L, Zhang H, Xu ZY, Ding XY, Wang SW, Xue X, Tan MW. Proximal aortic repair versus extensive aortic repair in the treatment of acute type A aortic dissection: a meta-analysis. Eur J Cardiothorac Surg. 2016, 49, 1392–401. [Google Scholar] [CrossRef] [PubMed]
- Kim JH, Lee SH, Lee S, Youn YN, Yoo KJ, Joo HC. The Impact of a Reentry Tear After Open Repair of Nonsyndromic Acute Type I Aortic Dissection. Ann Thorac Surg. 2019 Dec 17. pii: S0003-4975(19)31876-4.
- Lin FY, Tseng YH, Huang JW, Hsieh CC, Chen HM, Chiu CC, Chen YF. Fate of distal aorta after acute type A aortic dissection repair: Change and persistency of postoperative false lumen status. Int J Cardiol. 2018, 266, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Halstead JC, Meier M, Etz C, Spielvogel D, Bodian C, Wurm M, et al. The fate of the distal aorta after repair of acute type A aortic dissection. J Thorac Cardiovasc Surg. 2007, 133, 127–35. [Google Scholar] [CrossRef] [PubMed]
- Kimura N, Itoh S, Yuri K, Adachi K, Matsumoto H, Yamaguchi A, Adachi H. Reoperation for enlargement of the distal aorta after initial surgery for acute type A aortic dissection. J Thorac Cardiovasc Surg. 2015, 149, S91–S98. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Survival by extent of resection (Limited versus Extended). (A) Unmatched, (B) Matched.
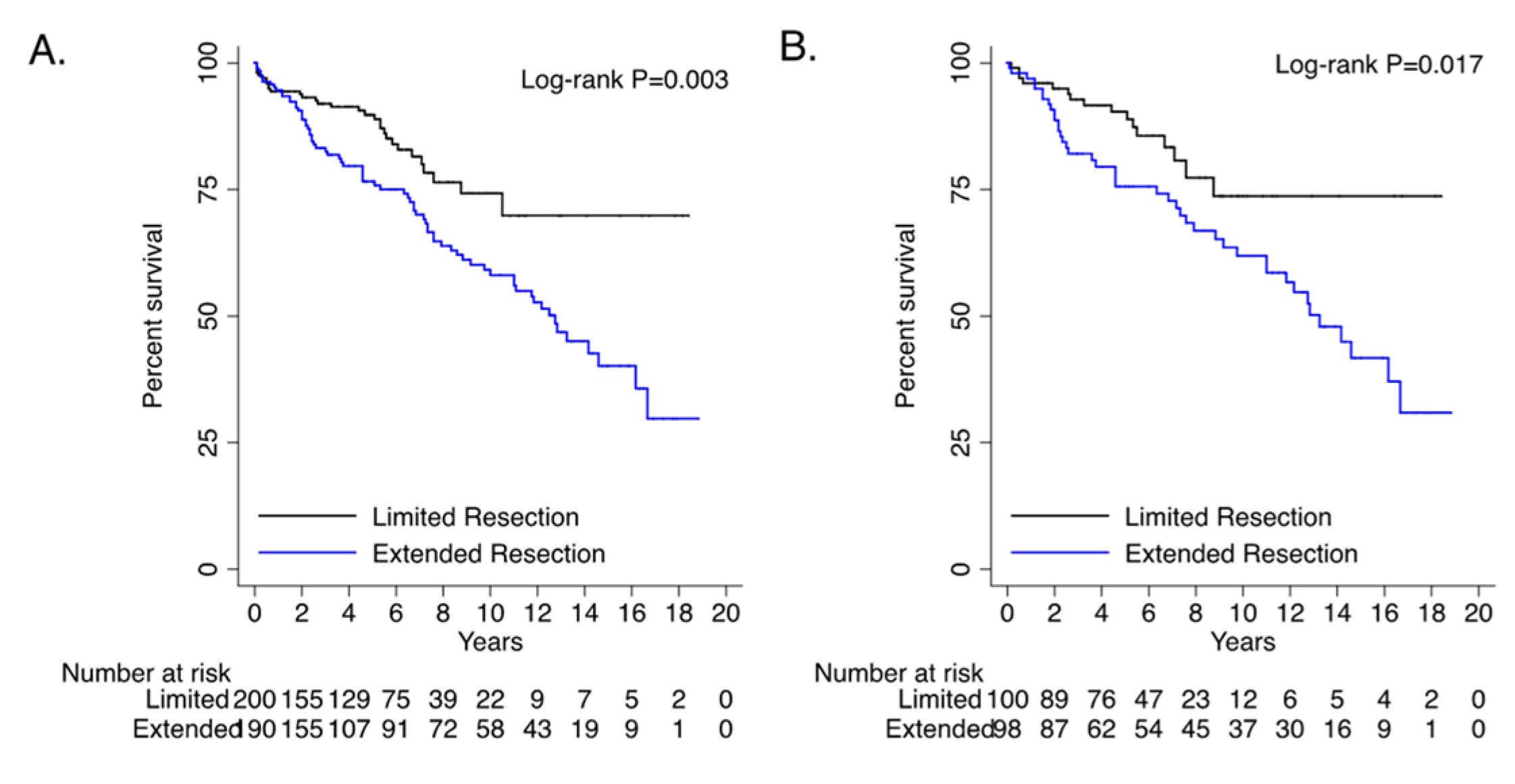
Figure 2.
A - Risk of re-operation (%) on any part of aorta after acute aortic dissection repair. B – Freedom from composite of death and aortic re-operation (%) after acute aortic dissection repair.
Figure 2.
A - Risk of re-operation (%) on any part of aorta after acute aortic dissection repair. B – Freedom from composite of death and aortic re-operation (%) after acute aortic dissection repair.
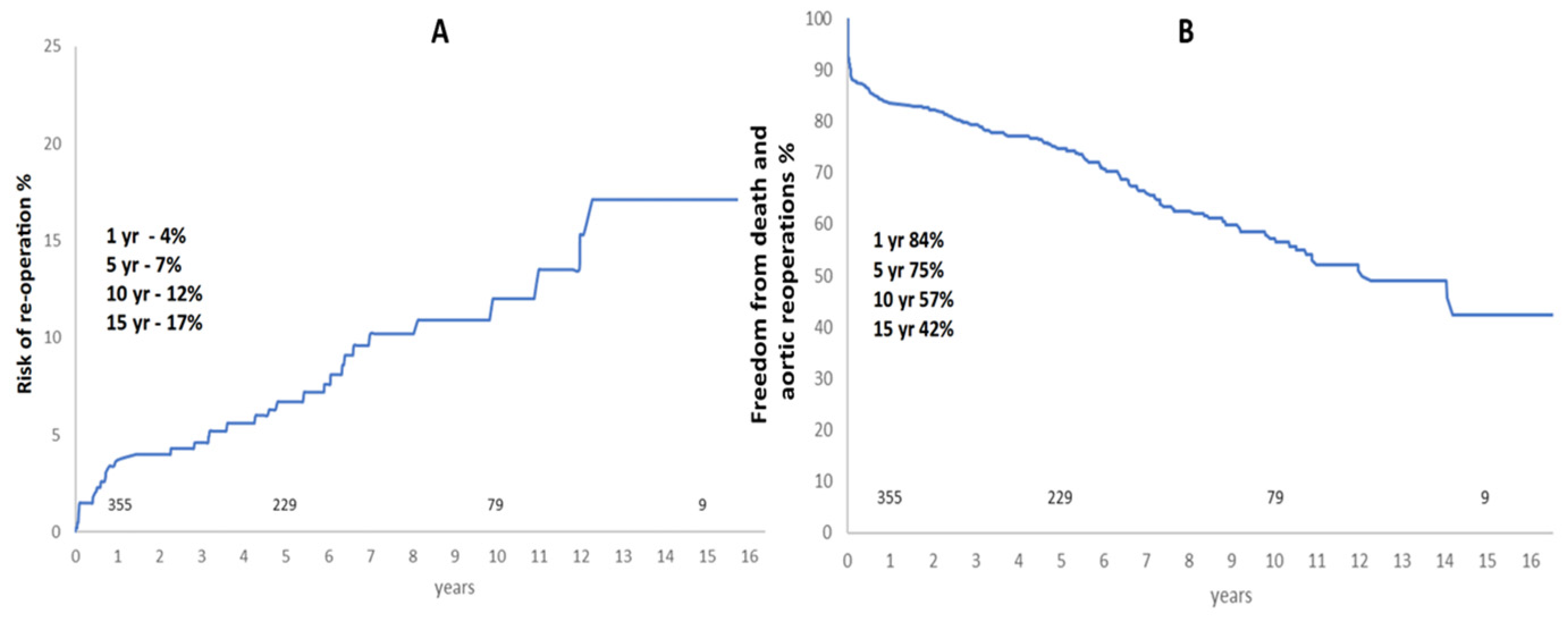

Table 1.
Operative and postoperative outcomes for unmatched and propensity matched data.
| UNMATCHED | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall (n=440) |
Limited Resection (n=215) |
Extended Resection (n=225) | ||||||||||||
| n | % or IQR | N | % or IQR | N | % or IQR | P value | ||||||||
| Bypass time | 187 | [130-249] | 173 | [121-256] | 191 | [145.5-245.5] | 0.225 | |||||||
| Cross clamp time | 99 | [75-130] | 99 | [74-131] | 99 | [76-128] | 0.862 | |||||||
| Circulatory arrest time | 27 | [75-130] | 26 | [19-33] | 27 | [18-33.5] | 0.545 | |||||||
| LOS days[IQR] | 12 | [8-20] | 12 | [8-20] | 11 | [7-17] | 0.012 | |||||||
| 30-day survival | 390 | 88.6 | 200 | 93.0 | 190 | 84.4 | 0.005 | |||||||
| Composite outcome | 126 | 28.6 | 53 | 24.7 | 73 | 32.4 | 0.071 | |||||||
| Stroke/TIA | 81 | 18.4 | 35 | 16.3 | 46 | 20.4 | 0.474 | |||||||
| In-hospital death | 44 | 10.0 | 13 | 6.0 | 31 | 13.8 | 0.007 | |||||||
| Overall survival | 286 | 65.0 | 169 | 78.6 | 117 | 52.0 | <0.001 | |||||||
| LOS: length of stay, TIA: transient ischemic attack | ||||||||||||||
| PROPENSITY MATCHED | ||||||||||||||
|
Overall (n=218) |
Limited Resections (n=109) | Extended Resection (n=109) | ||||||||||||
| N | % or IQR | n | % or IQR | N | % or IQR | P value | ||||||||
| Bypass time | 188 | [125-249] | 172 | [119-254] | 192 | [129-240] | 0.828 | |||||||
| Cross clamp time | 97 | [76-130] | 97 | [76-130] | 97 | [78-132] | 0.994 | |||||||
| Circulatory arrest time | 26 | [17-35] | 26 | [17-36] | 27 | [18-34] | 0.848 | |||||||
| LOS days [IQR] | 12 | [8-18] | 12 | [9-20] | 11 | [8-17.5] | 0.537 | |||||||
| 30-day mortality | 20 | 9.2 | 9 | 8.3 | 11 | 10.1 | 0.815 | |||||||
| Composite outcome | 58 | 26.6 | 24 | 22.0 | 34 | 31.2 | 0.133 | |||||||
| Stroke/TIA | 34 | 15.6 | 12 | 11.0 | 22 | 20.2 | 0.064 | |||||||
| In-hospital death | 16 | 7.3 | 8 | 7.3 | 8 | 7.3 | 1.000 | |||||||
| Overall survival | 140 | 64.2 | 84 | 77.1 | 56 | 51.4 | <0.001 | |||||||
| LOS: length of stay, TIA: transient ischemic attack | ||||||||||||||
Table 2.
Univariate and multivariate analysis for composite of TIA/stroke/in-hospital death.
| OR | 95% CI (lower, upper) |
P value | OR | 95% CI (lower, upper) |
P value | |||
|---|---|---|---|---|---|---|---|---|
| Extended Resection | 1.47 | 0.97 | 2.23 | 0.071 | 1.52 | 0.92 | 2.49 | 0.101 |
| Male gender | 1.04 | 0.67 | 1.59 | 0.868 | ||||
| CCS III-IV | 1.37 | 0.77 | 2.43 | 0.282 | ||||
| NYHA III-IV | 1.33 | 0.75 | 2.36 | 0.326 | ||||
| Prior cardiac surgery | 1.28 | 0.65 | 2.51 | 0.48 | ||||
| Diabetes | 1.03 | 0.42 | 2.54 | 0.953 | ||||
| Hypertension | 1.29 | 0.84 | 1.98 | 0.246 | 1.38 | 0.83 | 2.31 | 0.217 |
| Smoking history | 0.96 | 0.63 | 1.47 | 0.859 | ||||
| Renal disease | 1.40 | 0.46 | 4.26 | 0.553 | ||||
| Pulmonary disease | 1.37 | 0.73 | 2.58 | 0.321 | ||||
| PVD | 1.27 | 0.47 | 3.46 | 0.641 | ||||
| LVEF moderate/poor | 1.58 | 0.94 | 2.64 | 0.081 | 1.49 | 0.81 | 2.75 | 0.203 |
| Hemodynamically unstable | 1.47 | 0.86 | 2.51 | 0.159 | 1.40 | 0.74 | 2.65 | 0.299 |
| Salvage surgery | 2.26 | 1.12 | 4.55 | 0.023 | 2.94 | 1.22 | 7.08 | 0.016 |
| Obese (BMI >28) | 0.84 | 0.54 | 1.31 | 0.451 | ||||
| Bypass time | 1.00 | 1.00 | 1.01 | <0.001 | 1.01 | 1.00 | 1.01 | 0.001 |
| Cross clamp time | 1.00 | 1.00 | 1.01 | 0.044 | 1.00 | 0.99 | 1.00 | 0.724 |
| Circulatory arrest time | 1.01 | 0.99 | 1.92 | 0.471 | ||||
| Additional cardiac procedures | 1.19 | 0.72 | 1.96 | 0.51 | ||||
| Aortic arch procedure | 1.41 | 0.87 | 2.30 | 0.167 | 1.03 | 0.56 | 1.91 | 0.928 |
| Log euroscore | 1.03 | 0.99 | 1.07 | 0.163 | 1.01 | 0.97 | 1.06 | 0.632 |
| Age >70 | 1.63 | 1.07 | 2.48 | 0.023 | 1.85 | 1.11 | 3.07 | 0.017 |
| OR: odds ratio, CI: confidence interval, CCS: Canadian cardiovascular score, NYHA: New York Heart Association, PVD: peripheral vascular disease, LVEF: left ventricular ejection fraction, BMI: body mass index | ||||||||
Table 3.
Cox proportional hazards analysis for long term survival.
| HR |
95% CI (lower, upper) |
P value | HR |
95% CI (lower, upper) |
P value | |||
| Extended Resection | 1.90 | 1.24 | 2.92 | 0.003 | 2.06 | 1.31 | 3.25 | 0.002 |
| Male gender | 1.22 | 0.82 | 1.81 | 0.323 | ||||
| CCS III-IV | 1.38 | 0.80 | 2.38 | 0.253 | ||||
| NYHA III-IV | 2.03 | 1.28 | 3.22 | 0.003 | 2.07 | 1.28 | 3.35 | 0.003 |
| Prior cardiac surgery | 1.66 | 0.99 | 2.79 | 0.057 | 2.01 | 1.17 | 3.45 | 0.012 |
| Diabetes | 0.69 | 0.28 | 1.69 | 0.411 | ||||
| Hypertension | 1.59 | 1.05 | 2.40 | 0.027 | 1.45 | 0.94 | 2.22 | 0.092 |
| Smoking history | 1.10 | 0.75 | 1.62 | 0.628 | ||||
| Renal disease | 1.72 | 0.70 | 4.23 | 0.238 | 1.89 | 0.75 | 4.76 | 0.175 |
| Pulmonary disease | 0.84 | 0.44 | 1.62 | 0.613 | ||||
| PVD | 1.13 | 0.46 | 2.77 | 0.796 | ||||
| LVEF moderate/poor | 1.34 | 0.84 | 2.12 | 0.22 | 1.42 | 0.88 | 2.30 | 0.153 |
| Hemodynamically unstable | 0.85 | 0.48 | 1.50 | 0.574 | ||||
| Salvage surgery | 0.79 | 0.32 | 1.94 | 0.602 | ||||
| Obese (BMI >28) | 0.92 | 0.61 | 1.39 | 0.682 | ||||
| Bypass time | 1.00 | 0.99 | 1.00 | 0.707 | ||||
| Cross clamp time | 0.99 | 0.99 | 1.00 | 0.136 | 1.00 | 0.99 | 1.00 | 0.341 |
| Circulatory arrest time | 0.99 | 0.98 | 1.01 | 0.343 | ||||
| Additional cardiac procedures | 0.68 | 0.35 | 1.31 | 0.245 | 0.76 | 0.37 | 1.57 | 0.459 |
| Aortic arch procedure | 1.21 | 0.76 | 1.93 | 0.415 | ||||
| Log euroscore | 1.02 | 0.98 | 1.06 | 0.283 | ||||
| Age >70 | 2.10 | 1.42 | 3.12 | <0.001 | 2.00 | 1.32 | 3.03 | 0.001 |
| OR: odds ratio, CI: confidence interval, CCS: Canadian cardiovascular score, NYHA: New York Heart Association, PVD: peripheral vascular disease, LVEF: left ventricular ejection fraction, BMI: body mass index | ||||||||
Table 4.
Reoperations after acute aortic dissection repair.
| Aortic procedures after AAAD repair | ||
| Aortic valve and root | (47.2%) | |
| Aortic root repair/replacement | 10 | |
| Aortic valve replacement +/- redo Interposition graft | 7 | |
| Arch | (13.9%) | |
| Arch resection +/- Frozen elephant trunk | 5 | |
| Descending thoracic aorta | (27.8%) | |
| Descending thoracic aortic aneurysm repair | 8 | |
| Thoracic endovascular aneurysm repair | 2 | |
| Abdominal aortic aneurysm repair | (8.3%) | |
| Abdominal aortic aneurysm repair (open) | 2 | |
| Endovascular aneurysm repair (EVAR) | 1 | |
| Total | 36 | (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



