
Submitted:
22 July 2024
Posted:
24 July 2024
You are already at the latest version
Abstract
Introduction: Management of hypoxic-ischemic encephalopathy (HIE) has been the subject of international recommendations. However, some aspects remain within the realm of service practices and appear to vary greatly from one center to another. Objectives: To achieve a multidisciplinary consensus in France regarding management of HIE newborns that are not covered by international and national guidelines. Methods: This is a prospective, multicenter study using the Delphi method from April 21, 2021, to July 15, 2021. Perinatal professionals were contacted through professional societies. Participants received a questionnaire in three successive rounds. Each proposal was rated using a Likert scale from 1 (completely disagree) to 8 (completely agree). An item was considered consensual if at least 70% of responses were in agreement or disagreement. Results: 58 french neonatal professionals participated. A consensus was reached in the first round concerning the use of passive hypothermia in maternity ward, with 84% agreement and to define the target temperature between 35.0°C and 35.5°C at the third round. Regarding hypoglycemia in the delivery room, 79.2% agreed in the first round to correct blood glucose levels below a threshold of <2.2 mmol/l. Parenteral route was the preferred correction method for 91.4% of respondents, while enteral route via nasogastric tube did not reach consensus. Conclusion: This study highlights the variability in definitions and practices among professionals in the management of HIE. Consensus was found regarding certain care practices performed without formal guidelines. The work to harmonize definitions and practices for the management of HIE likely needs to continue.
Keywords:
neonatal encephalopathy
; perinal asphyxia
; passive hypothermia
; therapeutic hypothermia
; hypoglycemia
; delphi method
; cardiopulmonary resuscitation
; consensus
1. Introduction
It often occurs suddenly and can lead to a hypoxic ischemic encephalopathy (HIE), resulting in irreversible brain injuries or death. [3,5,6,7].Management of hypoxic-ischemic encephalopathy (HIE) has been the subject of national and international recommendations (ILCOR, ERC, SFN) [12,13] for resuscitation in the delivery room and in the first hours of life. However, some aspects remain within the realm of service practices and appear to vary greatly from one center to another [1,14,15,16], such as the modalities of clinical and biological monitoring of the newborn with HIE [15,16,17,18]. For example, the definition of hypoglycemia lacks uniformity in the international literature and it is generally agreed that a single blood glucose value cannot accurately define this clinical entity [16,17]. Questions about care of hypoxic-ischemic encephalopathy newborns, its organization and many perinatal cares that are not guided by international and national recommendations need to be discussed in order to improve the management of HIE.
The Delphi method is a validated tool of reaching a consensus with an expert committee on a specific topic and is useful to identify and analyze empirical data on a specific question that are currently limited or controversial in the literature [20,21,22].Thus, our work was to achieve a multidisciplinary consensus regarding different perinatal care for newborns with HIE in France.
2. Materials and Methods
Population and Methods
Study Design
Figure 1.
Three-phase study design.
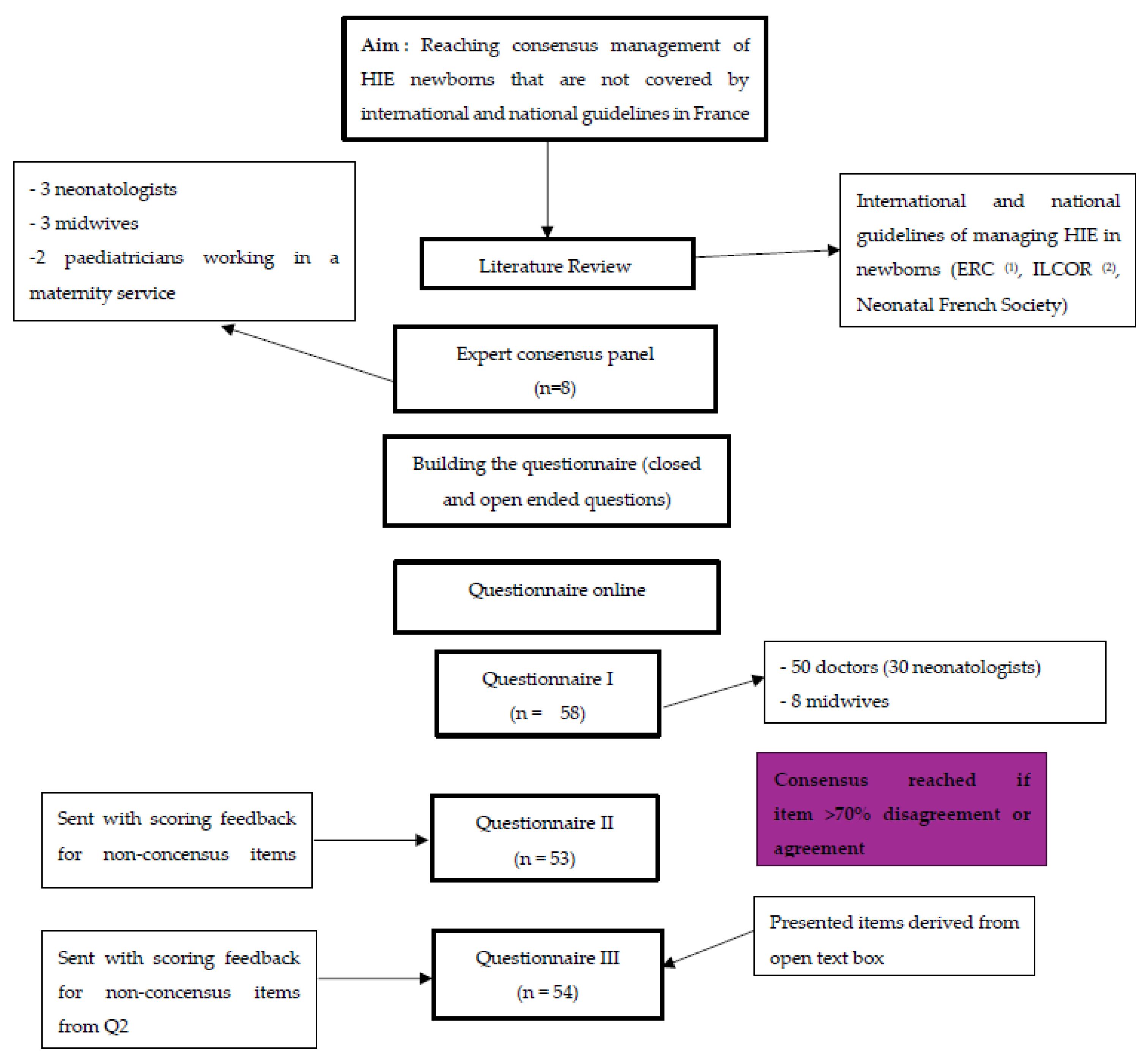
This study constitutes a prospective multicenter investigation, conducted utilizing the Delphi method from April 21st, 2021 to July 15th, 2021, across 10 regions in France (excluding overseas territories, Burgundy, and the Great-East region). Participants were solicited via email through learned societies in France, where they were apprised that participation in the study was voluntary, anonymous, and unpaid.
Informations Sources
The questionnaire was elaborated from December 2020 to April 2021. We first looked into international and national guidelines concerning the neonatal managing of severe perinatal asphyxia and neonatal encephalopathy in newborns. Our search strategy involved the guidelines by the Neonatal French Society, French legislative texts concerning birth rooms, perinatal decrees and international recommendations (ERC, ILCOR) [12,13]. We searched in two databases (PubMed - Cochrane Library) using the following keywords, separately and combined, in as many stages as necessary: hypoxic-ischemic encephalopathy; neonatal encephalopathy; birth asphyxia; Fetal distress; birth management; neonatal resuscitation; neonatal guidelines; therapeutic hypothermia; neonatal neuroprotection; first hours of life; neonatal protocol
Building the Questionary
Based on the literature review, 8 perinatal professionals (midwives, pediatricians, neonatologists and epidemiologists) contributed to the development of the questionnaire during two collectives’ sessions. Subsequently, the questionnaire underwent testing by a sample group consisting of epidemiologists and neonatologists before being distributed to our expert panel. For enhanced accessibility, the questionnaire was made available online through the LimeSurvey® platform.
The survey was structured into the following sub-topics:
Characteristics of the participants,
Equipment in birthing rooms,
Management strategies for perinatal asphyxia in birthing rooms,
Resuscitation protocols during the first hour of life,
Neurological assessment procedures in birthing rooms,
Transfer protocols to neonatal intensive care units,
Organization of primary care within neonatal intensive care units,
Strategies for preventing secondary brain injuries,
Assessment of neurodevelopmental outcomes,
Management of medical files.
Due to the specialized nature of part 7, focusing on neonatal intensive care units, only statements relevant to this area were dispatched to experts working within neonatal intensive care units.
Consensus Process
The consensus process employed a Delphi approach consisting of three iterative questionnaire rounds. Following each round, open feedback sessions were conducted with the entire panel to encourage further input. This iterative process allowed the reviewal of items that did not initially reach consensus, fostering reflection and reconsideration among expert stakeholders until a consensus was ultimately achieved. For each statement, participants were afforded the opportunity to express their level of agreement using a Likert scale, ranging from 1 (strongly disagree) to 10 (strongly agree). Responses were classified into three categories: negative agreement (scores 1-3), neutral (scores 4-6), and positive agreement (scores 7-10). Consensus was then defined as a positive or negative agreement percentage surpassing 70%.
During each round, participants were given a period of 7 days to complete the survey online. If a participant did not complete the questionnaire within a week, two reminder emails were sent. After ten days, the online survey was closed.
Statistical Analysis: Data analysis was conducted after each round and concluded two months after the third round. Data were initially extracted from the LimeSurvey® Software and subsequently analyzed using Stata13® Software. Quantitative analysis involved calculating central tendencies (mean, median, lower and upper limits) and agreement percentages.
Ethical and Legal Considerations
Ethical approval was obtained from the ethics committee of the French Pediatric Society on March 23rd, 2021 (Number CERSFP_2021_130). Participation in the questionnaire was voluntary and anonymous, requiring no prior authorization. Panel experts were informed that data would be retained for one year following the study's publication and might be utilized for subsequent research endeavors.
The computer file adhered to French (Law of Computing and Freedom) and European (Data Protection Act) regulations, and was compliant with the CNIL (French data protection authority, number 2221393 v0). This study was conducted by INSERM UMR1153 Team Epopé and funded by the Human Safety Net Foundation.
3. Results
3.1. Characteristics
The questionnaire was distributed and in the initial round, out of 60 initial registrations, 58 respondents completed the questionnaire. The panel composition comprised 86% physicians and 14% midwives. Within the physician category, 64% identified as neonatologists 12% of whom worked in private establishments. Regarding care facility types, 67% operated in type 3 care, 22% in type 2, and 5% in type 1. This distribution remained consistent throughout all three rounds.
3.2. Equipment in the Delivery Room
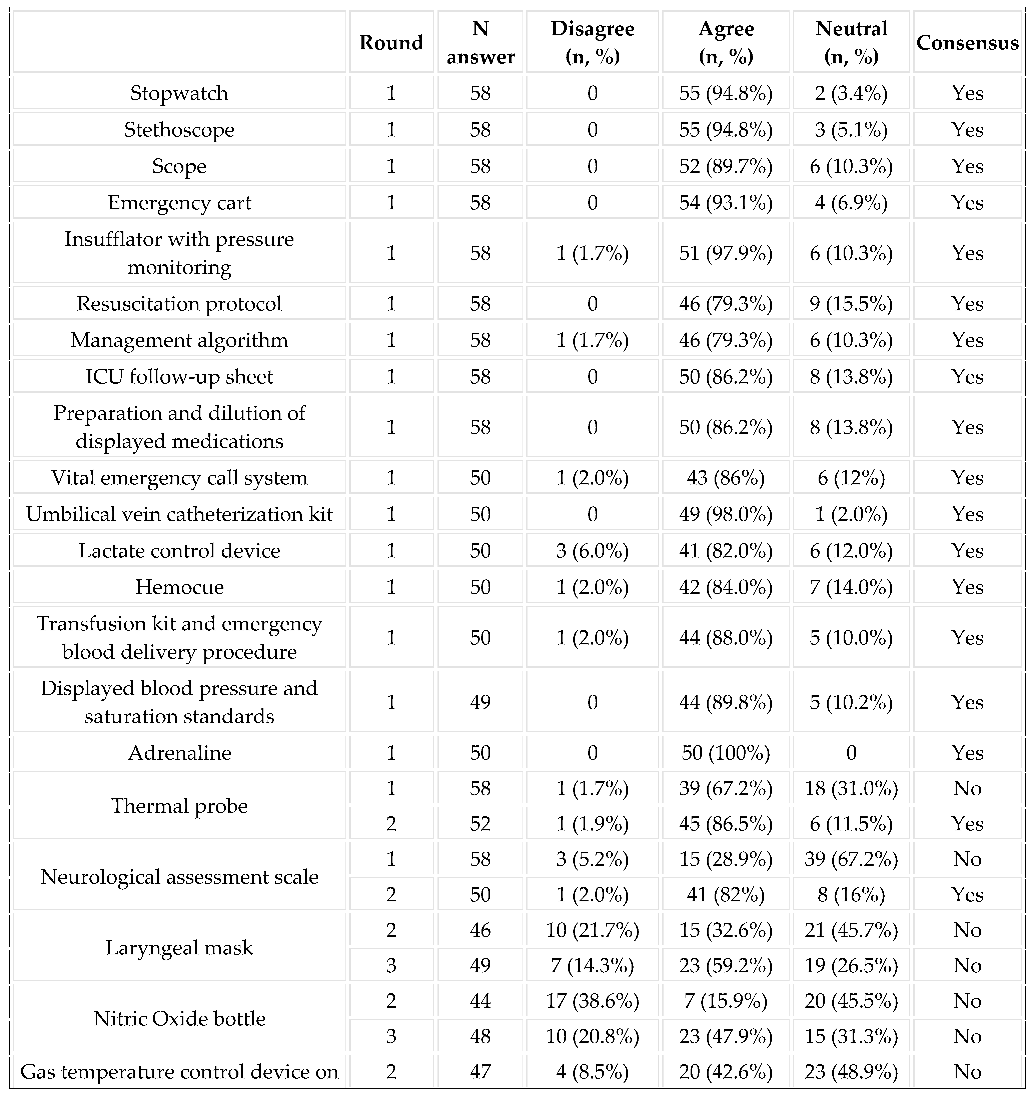
During the first round, consensus was reached on several items, including the necessity for a timer, stethoscope, scope, crash cart, neonatal resuscitation protocol, and adrenaline. (Table 1)
3.3. Implementation of Resuscitation:
Participants were asked to opine on the duration, in minutes from onset, at which they considered the performance of these procedures to be delayed. The response intervals varied considerably, ranging from 1 to 60 minutes for acceptable tracheal intubation timing (Table 2).
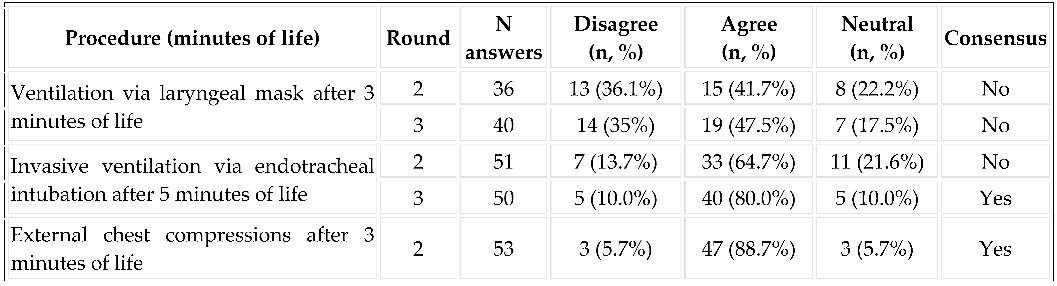
Consensus was reached in the second round for the initiation of external chest compressions (before 3 minutes), the placement of an umbilical vein catheter (10 minutes), and the administration of adrenaline (10 minutes). Consensus was achieved in the third round for intubation and invasive ventilation (5 minutes). However, no consensus was reached among the respondents for the use of laryngeal mask ventilation and the timing of vascular filling (Table 3).
3.4. Calling the Pediatrician by the Midwife
In cases where severe perinatal asphyxia is presumed prenatally, there was a strong consensus in the first round (80.4% agreement) for a systematic call to the pediatrician to be present at birth. In cases of a poor neonatal adaptation, a consensus was reached in the second round with the arrival of the pediatrician which was considered late if he arrived after five minutes after the call.
3.5. Care in the Delivery Room during the First Hours of Life
3.5.1. Systematic Sedation and Analgesia in the Delivery Room
The responses were overall non-consensual, with 57.1% agreement to initiate it in the delivery room, 24.5% disagreement, and 18.4% neutral. Regarding the use of paracetamol in this context, a consensus was reached for its use in the third round (76.5% agreement).
3.5.2. Passive Hypothermia in the Delivery Room and during Transport:
A consensus was reached in the first round regarding the initiation of passive hypothermia in the delivery room (85.7% agreement). The target temperature was initially non-consensual, with responses ranging from 33.0°C to 36.5°C. Finally, a consensus was reached in the third round (85.4% agreement) for a target temperature between 35°C and 35.5°C. Consensus was also reached for the use of a dermal thermal probe for temperature monitoring (92.4% agreement in the second round), but no consensus was reached for the use of a rectal thermal probe) (Figure 2).
3.5.3. Regarding the Management of Glycemia:
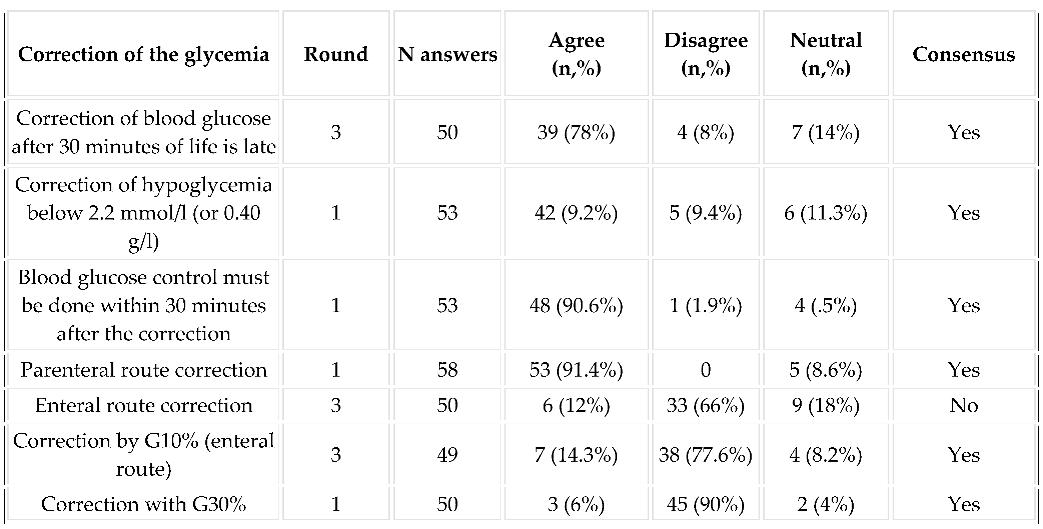
The answers to the question ‘When do you think the first blood sugar check is necessary’ ranged from 5 to 60 minutes of life, with an average and median of 30 minutes. In the third round, consensus was achieved that testing and correcting blood glucose after 30 minutes of life was considered late (78% agreement). Regarding the correction of hypoglycemia, a consensus emerged against oral correction (84% agreement) and in favor of parenteral correction 53/58 (91% agreement). No consensus was reached regarding the correction by enteral route via nasogastric tube. The post-correction control of hypoglycemia was consensual at 30 minutes after correction (90,6% of agreement) (Table 4).
4. Discussion
The aim of this study was to establish a consensus concerning the management during the first hours of life of a newborn presenting HIE for care not covered by French legislation or national and international recommendations. A consensus has been reached among 58 experts working in neonatology on the organization of care, the use of passive hypothermia and the monitoring and correction of glycemic disorders.
The international recommendations concerning the resuscitation procedures in newborns follow the ILCOR 2020’s and the ERC 2021’s guidelines [12,13], but the recent version does not precise the right timing of the procedures in practice. This question is important to guide resuscitation but also to judge a posteriori the quality of the resuscitation performed [14]. In our study, a consensus was reached for many resuscitations procedures timing, such as the tracheal intubation which was considered too late after five minutes of life, with 80% level of agreement in the third round, or the set-up of a UVC which was considered late after ten minutes of life. This timing was very similar to that described in previous versions of ILCOR [13].
The 1998 decree concerning safety standards for maternity wards, staff, and facilities defines three types of maternity wards. Type I facilities cater to low-risk pregnancies. Type II facilities provide neonatology care with some intensive care units where pediatricians may be present 24/7 but are not exclusively dedicated to the neonatology unit (they also cover the emergency unit). Type III facilities handle high-risk pregnancies, including maternal-fetal pathologies requiring multidisciplinary care. In Type III facilities, pediatricians are present and dedicated to neonatal care 24/7. Depending on the type of unit, the first professional to take care of an asphyxiated newborn may be a midwife, and pediatricians could be called in ante or postnatal, as he is not systematically present. The midwife could be the first perinatal professional who initiates the neonatal resuscitation. Their skills are well detailed in the Public Health Code, Article 4127. According to the French decree on the 12th October 2011, their skills in a delivery room vary from taking the vital signs, ventilate and performed chest compressions or drugs administration. In our study, a consensus was reached that if asphyxia was presumed antenatally, the pediatrician should be called to be present before birth. It was also agreed that a delay of more than 5 minutes after birth for the pediatrician's arrival, if called postnatally, was considered too late, regardless of the type of maternity unit in which the resuscitation took place. This contradicts the legal requirements in France for type 1 maternity units to have a pediatrician on call and usually available within 20 minutes of the call. This question of the presence and timing of the arrival of a dedicated pediatrician in the maternity unit is a key point concerning the management of resuscitations in the delivery room and the potentially associated medico-legal consequences [24]. Despite the results of this study, there is no legal or regulatory definition specifying a maximum arrival time for the pediatrician after being called by the midwife.
Neonatal hypoglycemia affects up to 15% of all newborns [16,17]. Despite the high prevalence there is currently no uniform definition of neonatal hypoglycemia, and existing guidelines differ significantly in terms of screening for hypoglycemia, and where to set interventional thresholds and treatment goals [25]. In the context of severe perinatal asphyxia, hypoglycemia is recognized as a risk factor for poor long-term neurodevelopmental outcomes [5,6]. Clinical studies seem to define a “low glucose” concentration <3.0 mmol/l as neuroglycopenic symptoms are known to occur, but with high intra- and interindividual variability [25]. Managing hypoglycemia is especially challenging in newborns, considering that there is a physiological transient drop of blood glucose levels during the first hours and days of life [25]. Some guidelines recommend blood glucose testing before the second feed but not later than 3 to 4 hours of age. In our study, there was a consensus about the first blood glucose testing in the third round with a median of 30 minutes of life suggested by the participants. A consensus was reached in the first round of correcting the glycemia below 2.2 mmol/L, by parenteral route (91.4% level of agreement), but no consensus for the enteral route, even if it is the simplest way in maternity ward. These results may be explained by the lack of guidelines regarding nutritional and metabolic practices for newborns with HIE especially during therapeutic hypothermia [15].
Currently, controlled hypothermia represents the only specific treatment validated for HIE [27,28,29]. In the management of moderate to severe HIE, controlled hypothermia has proven its efficacy in reducing the combined rate of death and major disability at 12 to 18 months of age [7,8]. One challenge is initiating therapeutic hypothermia within the first 6 hours of life. Thus, managing a safe and an optimal perinatal care before and during the transport for newborns with HIE is a priority for each maternity ward. Some units recommend passive hypothermia prior to admission to intensive care, in order to ‘save’ time in the neuroprotection of the newborn baby [35]. In our study, a consensus was reached on the use of passive hypothermia in the first round. However, when we tried to get our panel to define the temperature they considered to be cible during passive hypothermia, the responses varied widely, between 33.5°C and 36°C. The definition of passive hypothermia is not consensual in the literature [32,33]. In practice, passive cooling involves turning off the radiant warmers, early removal of wet blankets and pre-warming surfaces. In our study, a consensus was reached in the third round (84.3% level of agreement) for a target temperature between 35.0°C and 35.5°C during passive hypothermia. In moderately asphyxiated newborns, the rectal temperature spontaneously drops to 35.5°C within 30 minutes [33]. This suggests that passive hypothermia could be enough when initiated before and during the transport, with a target temperature between 33.0°C and 35.0°C [32]. Moreover, passive hypothermia could be to avoid hyperthermia, which has been shown to be associated with a poorer prognosis [36].
However, passive hypothermia is not without side effects and an increase in brain damage has been reported in patients treated with passive hypothermia who have experienced overcooling [37]. Another study reported that overcooling (<33.0°C) was associated with a higher incidence of multiorgan compromise and death [32]. The monitoring of core temperature is important. In cases of hypothermia, the skin temperature does not correlate with the rectal temperature, and there is a 1 to 2 °C difference between the axillary and rectal temperatures [31]. Despite this scientific data, consensus was also reached for the use of a dermal thermal probe for temperature monitoring, but not for the use of a rectal thermal probe. The use of servo-controlled devices during neonatal transport improves the ability to maintain the infant's temperature within the target range (33-34°C) with less overcooling [31]. However, future research is needed to investigate its impact on mortality and neurological impairment [31,32].
The Delphi method is a consensus-building approach involving a panel of experts on a specific topic who complete a structured questionnaire iteratively and anonymously [21,22]. The results are statistically analyzed using tools such as the Likert scale, which allows participants to express their degree of agreement, disagreement, or neutrality. Results are sent back to participants after each round to give the opportunity for participants to add anonymous comments. This means that a participant may change their opinion based on the responses of other experts, aiming to converge towards a common consensus. Each participant's response carries equal weight in achieving consensus [23]. The Delphi method also facilitates the gathering of diverse expert opinions on a given question. Participants can independently complete the questionnaire without organizational constraints, overcoming geographical limitations (such as team meetings, email or phone consultations, or multidisciplinary meetings). In our study, our panel remained stable throughout the different rounds of the study, resulting in a low dropout rate. It may require a long process in terms of recruitment and participation, especially if the questionnaire needs to be repeated many times until a consensus is reached. In our study, the estimated time per expert needed to complete each round was 2 full hours, i.e. a total of 6 hours per participant, not including the time spent consulting the results of the previous round. Few data were missing among respondents and our panel remained stable throughout the different rounds of the study, resulting in a low dropout rate. Additionally, forming an expert group requires recruitment that must be varied and of high quality, as the results will directly depend on their collective opinion [21,22]. In our study, we were able to recruit a diverse panel of experts, ranging from midwives to emergency physicians and epidemiologists, allowing for varied perspectives on the issues. The large number of professionals represented (> 50), the variety of their practices, and the diversity of the French regions in which they worked allowed us to consider the group as relatively representative of birth room care in France. Lastly, there is likely a conformity effect, wherein the responses of each participant, despite being anonymized, may be influenced by the responses of others. Indeed, the initial viewpoint of an expert may no longer be maintained and may change to converge towards the response that garners the most consensus, especially when their response is part of a minority [21,22].
5. Conclusions
Our work using the Delphi method has led to consensus on common practices in the management of neonatal HIE at the national level. Some items, not covered by national or international recommendations, did not achieve consensus, highlighting a real heterogeneity of perinatal care in France. A continued effort towards harmonizing care and definitions is likely necessary to facilitate the practice of perinatal professionals.
Author Contributions
Dr Isabelle Guellec, Dr Nguyen Thulan conceptualized and designed the study, drafted the initial manuscript, and critically reviewed and revised the manuscript.Dr Isabelle Guellec and Elisabeth Lyonnais designed the data collection instruments, collected data, carried out the initial analyses, and critically reviewed and revised the manuscript. Thulan N’Guyen, Manon Michaud, Prof Pierre-Yves Ancel, Dr Paola Sikias, Pr Gauthier Loron, Dr Beatrice Harvey, Dr Priscille Sauvegrain, Dr Anne Chantry critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Data Availability Statement
Data can be shared on request and upon authorization of the institution.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Vega-Del-Val, C.; Arnaez, J.; Caserío, S.; Gutiérrez, E.P.; Castañón, L.; Benito, M.; et al. Adherence to hypothermia guidelines in newborns with hypoxic-ischemic encephalopathy. An Pediatr. 2022, 97, 30–39. [Google Scholar] [CrossRef]
- Lundgren, C.; Brudin, L.; Wanby, A.S.; Blomberg, M. Ante- and intrapartum risk factors for neonatal hypoxic ischemic encephalopathy. J Matern-Fetal Neonatal Med Off J Eur Assoc Perinat Med Fed Asia Ocean Perinat Soc Int Soc Perinat Obstet. 2018, 31, 1595–1601. [Google Scholar] [CrossRef]
- Zupan Simunek, V. Définition de l’asphyxie intrapartum et conséquences sur le devenir. J Gynécologie Obstétrique Biol Reprod. 2008, 37, S7–S15. [Google Scholar] [CrossRef] [PubMed]
- Palsdottir, K.; Dagbjartsson, A.; Thorkelsson, T.; Hardardottir, H. [Birth asphyxia and hypoxic ischemic encephalopathy, incidence and obstetric risk factors]. Laeknabladid. 2007, 93, 595–601. [Google Scholar] [PubMed]
- Zupan Simunek, V. Asphyxie périnatale à terme : Diagnostic, pronostic, éléments de neuroprotection. Arch Pédiatrie. 2010, 17, 578–582. [Google Scholar] [CrossRef]
- McKinlay, C.J.D.; Alsweiler, J.M.; Anstice, N.S.; Burakevych, N.; Chakraborty, A.; Chase, J.G.; et al. Association of Neonatal Glycemia With Neurodevelopmental Outcomes at 4. 5 Years. JAMA Pediatr. 2017, 171, 972–983. [Google Scholar] [CrossRef] [PubMed]
- Edwards, A.D.; Brocklehurst, P.; Gunn, A.J.; Halliday, H.; Juszczak, E.; Levene, M.; Strohm, B.; Thoresen, M.; Whitelaw, A.; Azzopardi, D. Neurological outcomes at 18 months of age after moderate hypothermia for perinatal hypoxic ischaemic encephalopathy: Synthesis and meta-analysis of trial data. BMJ. 2010, 340, c363. [Google Scholar] [CrossRef]
- van Handel, M.; Swaab, H.; de Vries, L.S.; Jongmans, M.J. Long-term cognitive and behavioral consequences of neonatal encephalopathy following perinatal asphyxia: A review. Eur J Pediatr. 2007, 166, 645–654. [Google Scholar] [CrossRef]
- Goswami, I.; Guillot, M.; Tam, E.W.Y. Predictors of Long-Term Neurodevelopmental Outcome of Hypoxic-Ischemic Encephalopathy Treated with Therapeutic Hypothermia. Semin Neurol. 2020, 40, 322–334. [Google Scholar] [CrossRef]
- Armstrong-Wells, J.; Bernard, T.J.; Boada, R.; Manco-Johnson, M. Neurocognitive outcomes following neonatal encephalopathy. NeuroRehabilitation. 2010, 26, 27–33. [Google Scholar] [CrossRef]
- Lou, H.C. Etiology and pathogenesis of attention-deficit hyperactivity disorder (ADHD): Significance of prematurity and perinatal hypoxic-haemodynamic encephalopathy. Acta Paediatr Oslo Nor 1992. 1996, 85, 1266–1271. [Google Scholar] [CrossRef] [PubMed]
- Madar, J.; Roehr, C.C.; Ainsworth, S.; Ersdal, H.; Morley, C.; Rüdiger, M.; et al. European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation. 2021, 161, 291–326. [Google Scholar] [CrossRef] [PubMed]
- Perlman, J.M.; Wyllie, J.; Kattwinkel, J.; Wyckoff, M.H.; Aziz, K.; Guinsburg, R.; et al. Part 7: Neonatal Resuscitation: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science With Treatment Recommendations. Circulation. 2015, 132 (Suppl. 1), S204–241. [Google Scholar] [CrossRef] [PubMed]
- Berglund, S.; Norman, M.; Grunewald, C.; Pettersson, H.; Cnattingius, S. Neonatal resuscitation after severe asphyxia--a critical evaluation of 177 Swedish cases. Acta Paediatr. 2008, 97, 714–719. Acta Paediatr. 2008, 97, 714–719. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gale, C.; Longford, N.T.; Jeyakumaran, D.; Ougham, K.; Battersby, C.; Ojha, S.; et al. Feeding during neonatal therapeutic hypothermia, assessed using routinely collected National Neonatal Research Database data: A retrospective, UK population-based cohort study. Lancet Child Adolesc Health. 2021, 5, 408–416. [Google Scholar] [CrossRef] [PubMed]
- The International Hypoglycaemia Study Group. Glucose concentrations of less than 3.0 mmol/l (54 mg/dl) should be reported in clinical trials: A joint position statement of the American Diabetes Association and the Europian Association for the Study of Diabetes. Diabetologia. 2017, 60, 3–6.
- Roeper, M.; Hoermann, H.; Kummer, S.; Meissner, T. Neonatal hypoglycemia: Lack of evidence for a safe management. Front Endocrinol. 2023, 14, 1179102. [Google Scholar] [CrossRef]
- Giouleka, S.; Gkiouleka, M.; Tsakiridis, I.; Daniilidou, A.; Mamopoulos, A.; Athanasiadis, A.; et al. Diagnosis and Management of Neonatal Hypoglycemia: A Comprehensive Review of Guidelines. Child Basel Switz. 2023, 10, 1220. [Google Scholar] [CrossRef]
- Pinchefsky, E.F.; Schneider, J.; Basu, S.; Tam, E.W.Y.; Gale, C. , Newborn Brain Society Guidelines and Publications Committee*. Nutrition and management of glycemia in neonates with neonatal encephalopathy treated with hypothermia. Semin Fetal Neonatal Med. 2021, 26, 101268. [Google Scholar]
- Cornblath, M.; Ichord, R. Hypoglycemia in the neonate. Semin Perinatol. 2000, 24, 136–149. [Google Scholar] [CrossRef]
- Taze, D.; Hartley, C.; Morgan, A.W.; Chakrabarty, A.; Mackie, S.L.; Griffin, K.J. Developing consensus in Histopathology: The role of the Delphi method. Histopathology. 2022, 81, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Humphrey-Murto, S.; Varpio, L.; Gonsalves, C.; Wood, T.J. Using consensus group methods such as Delphi and Nominal Group in medical education research. Med Teach. 2017, 39, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Romero-Collado, A. Essential elements to elaborate a study with the (e)Delphi method. Enferm Intensiva. 2021, 32, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Fanaroff, J.M.; Ross, M.G.; Donn, S.M. , Newborn Brain Society Guidelines and Publications Committee*. Medico-legal considerations in the context of neonatal encephalopathy and therapeutic hypothermia. Semin Fetal Neonatal Med. 2021, 26, 101266. [Google Scholar] [PubMed]
- Srinivasan, G.; Pildes, R.S.; Cattamanchi, G.; Voora, S.; Lilien, L.D. Plasma glucose values in normal neonates: A new look. J Pediatr. 1986, 109, 114–117. [Google Scholar] [CrossRef]
- Hoermann, H.; Mokwa, A.; Roeper, M.; Salimi Dafsari, R.; Koestner, F.; Hagenbeck, C.; et al. Reliability and Observer Dependence of Signs of Neonatal Hypoglycemia. J Pediatr. 2022, 245, 22–29.e2. [Google Scholar] [CrossRef] [PubMed]
- Warchoł, A.; Kwinta, P. Nutrition of Newborns with Hypoxic-Ischaemic Encephalopathy during Therapeutic Hypothermia - A Survey of Practice in Polish Neonatal Care Units. J Mother Child. 2024, 28, 8–13. [Google Scholar] [PubMed]
- Wassink, G.; Gunn, E.R.; Drury, P.P.; Bennet, L.; Gunn, A.J. The mechanisms and treatment of asphyxial encephalopathy. Front Neurosci. 2014, 8, 40. [Google Scholar] [CrossRef]
- Chiang, M.C.; Jong, Y.J.; Lin, C.H. Therapeutic hypothermia for neonates with hypoxic ischemic encephalopathy. Pediatr Neonatol. 2017, 58, 475–483. [Google Scholar] [CrossRef]
- Russ, J.B.; Simmons, R.; Glass, H.C. Neonatal Encephalopathy: Beyond Hypoxic-Ischemic Encephalopathy. NeoReviews. 2021, 22, e148–e162. [Google Scholar] [CrossRef]
- Torre Monmany, N.; Behrsin, J.; Leslie, A. Servo-controlled cooling during neonatal transport for babies with hypoxic-ischaemic encephalopathy is practical and beneficial: Experience from a large UK neonatal transport service. J Paediatr Child Health. 2019, 55, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Troncoso, G.; Agudelo-Pérez, S.; Maldonado, N.T.; Becerra, M.P. Relationship of passive hypothermia during transport with the incidence of early multiorgan compromise in newborns with perinatal asphyxia. Early Hum Dev. 2023, 187, 105902. [Google Scholar] [CrossRef] [PubMed]
- Bellini, C.; Ramenghi, L.A.; Gente, M. Effective Passive Cooling During Neonatal Transport. Ther Hypothermia Temp Manag. 2022, 12, 168–170. [Google Scholar] [CrossRef] [PubMed]
- Kendall, G.S.; Kapetanakis, A.; Ratnavel, N.; Azzopardi, D.; Robertson, N.J. ; Cooling on Retrieval Study Group. Passive cooling for initiation of therapeutic hypothermia in neonatal encephalopathy. Arch Dis Child Fetal Neonatal Ed. 2010, 95, F408–F412. [Google Scholar] [CrossRef] [PubMed]
- Momin, S.; Thomas, S.; Zein, H.; Scott, J.N.; Leijser, L.M.; Vayalthrikovil, S.; Yusuf, K.; Paul, R.; Howlett, A.; Mohammad, K. Comparing Three Methods of Therapeutic Hypothermia Among Transported Neonates with Hypoxic-Ischemic Encephalopathy. Ther Hypothermia Temp Manag. 2023, 13, 141–148. [Google Scholar] [CrossRef]
- Laptook, A.; Tyson, J.; Shankaran, S.; McDonald, S.; Ehrenkranz, R.; Fanaroff, A.; et al. Elevated temperature after hypoxic-ischemic encephalopathy: Risk factor for adverse outcomes. Pediatrics. 2008, 122, 491–499. [Google Scholar] [CrossRef]
- Troncoso, G.; Agudelo-Pérez, S.; Thorin, N.; Diaz, C.; Vargas, A. Corrigendum correcting the paper "Short-term neurological injury in newborns infants with overcooling in passive hypothermia and transferred to reference hospital in Colombia". Acta Paediatr. 2024, 113, 366–367. [Google Scholar] [CrossRef]
Figure 2.
Definition of passive hypothermia.
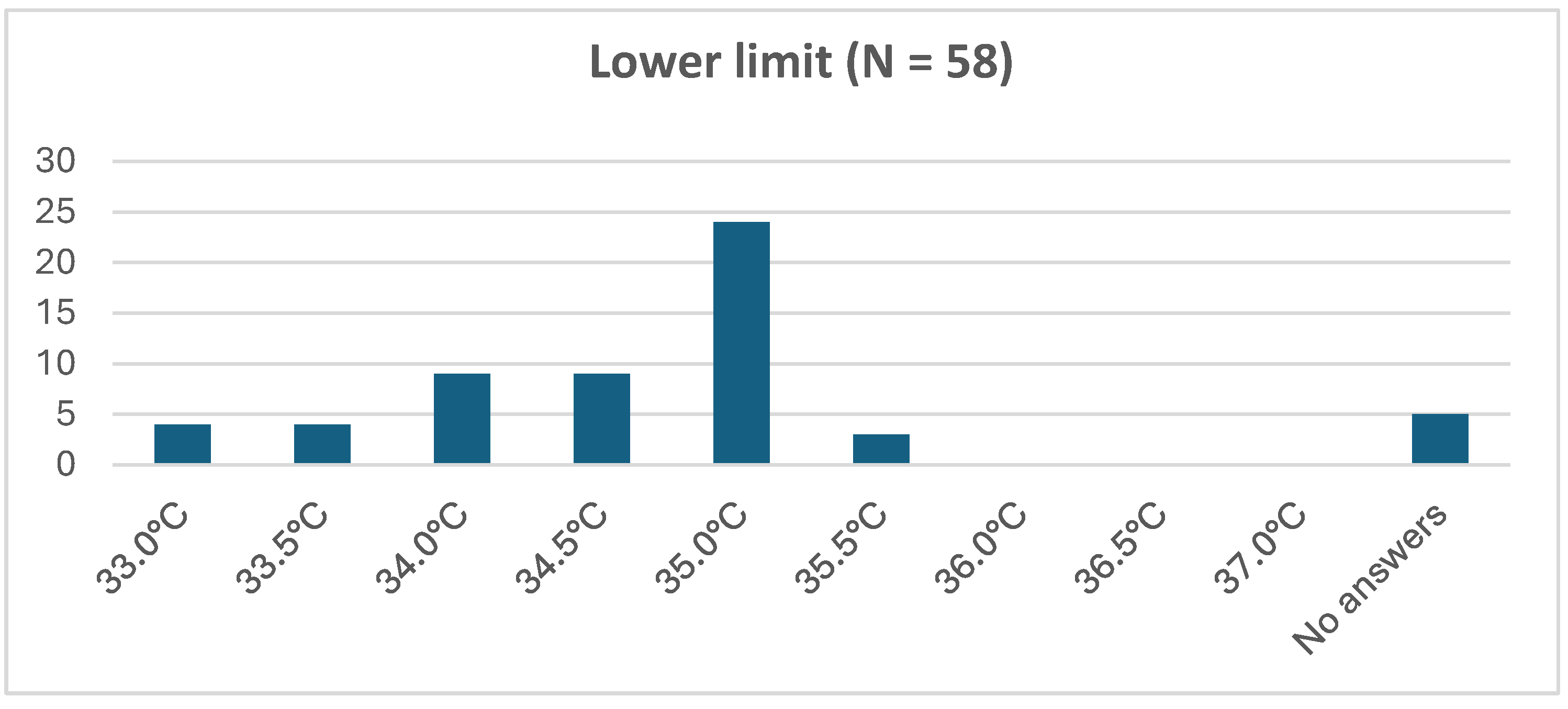
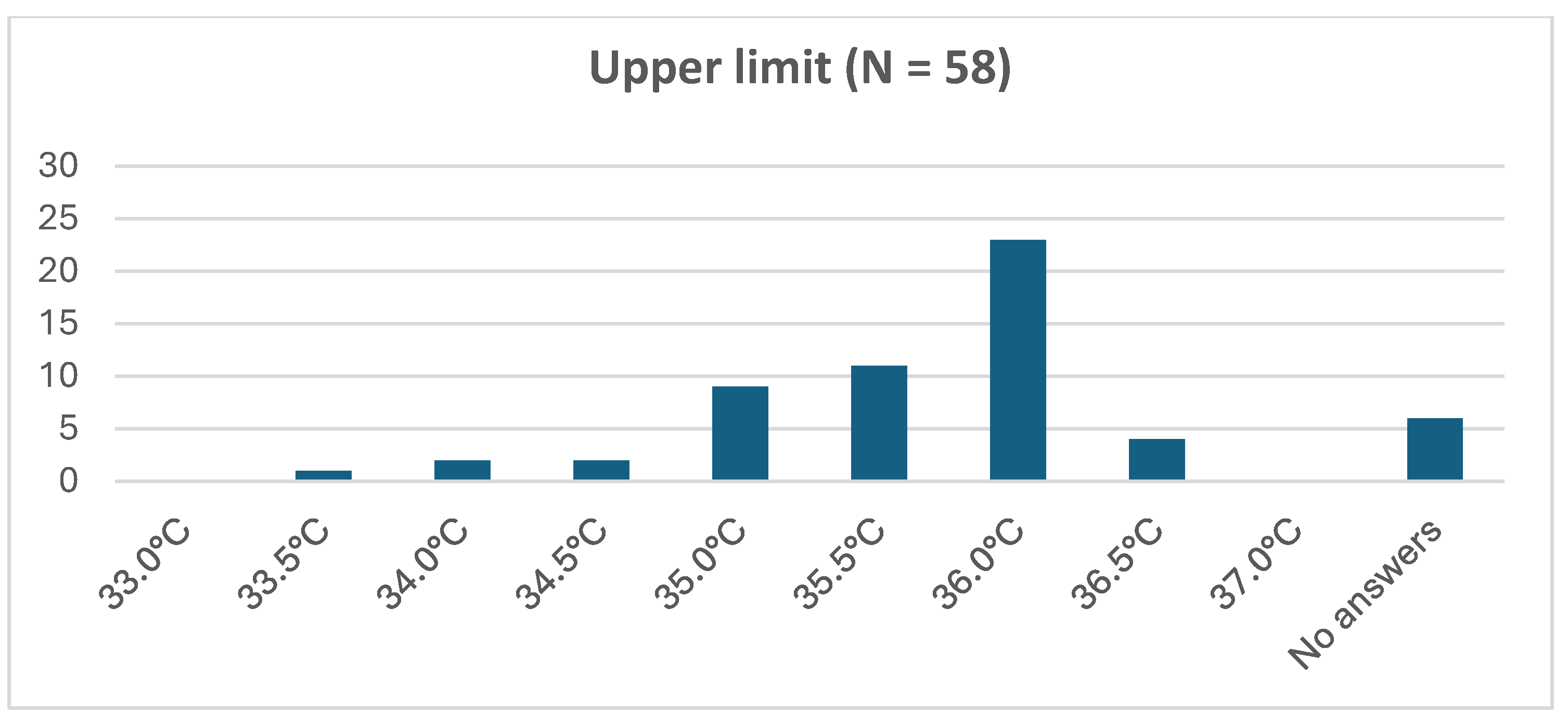

Table 1.
Equipment in the delivery room consensus responses.
 |
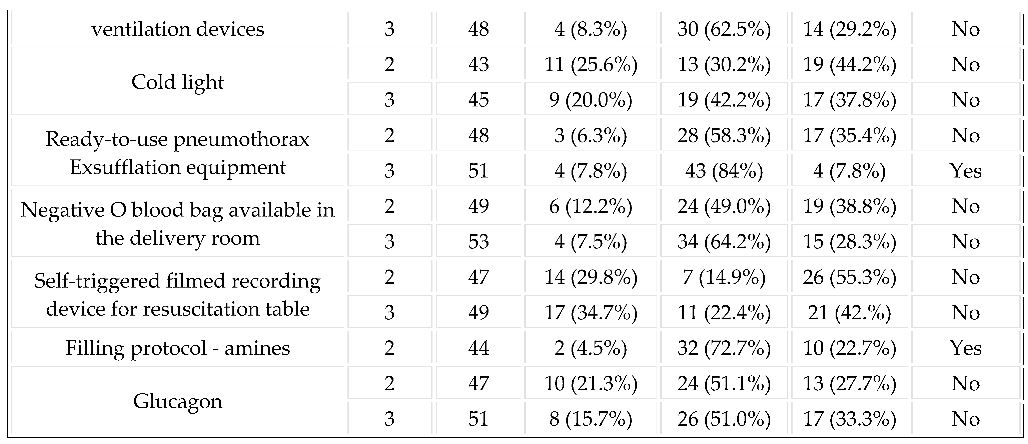 |
Table 2.
Implementation delays of resuscitation procedures (open answers).
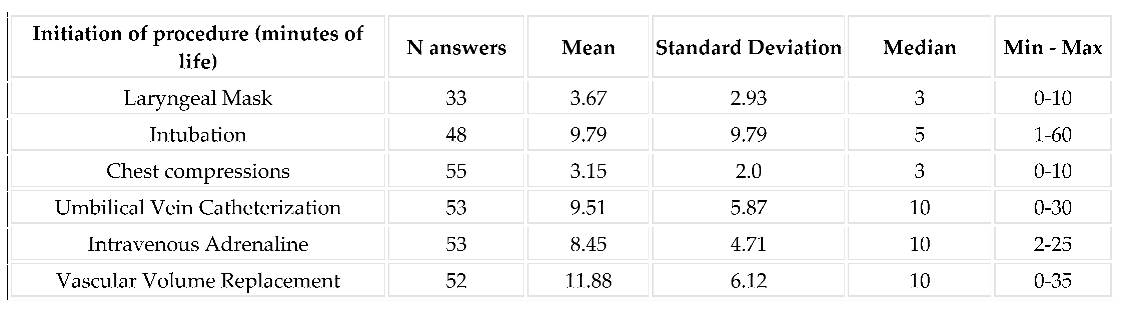 |
Table 3.
How late do you think it is to initiate these resuscitation procedures ?
 |
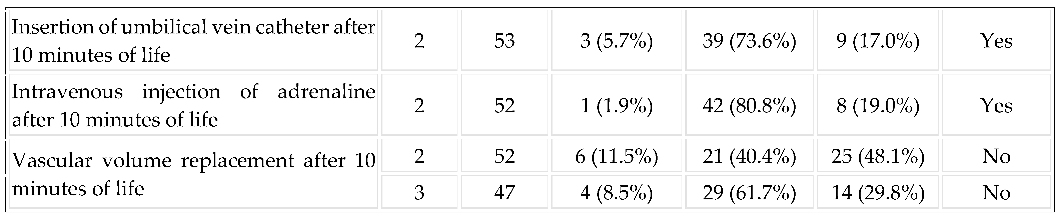 |
Table 4.
First control and correction of the blood glucose in the first hour of life in newborns with HIE (Hypoxic ischemic encephalopathy).
Table 4.
First control and correction of the blood glucose in the first hour of life in newborns with HIE (Hypoxic ischemic encephalopathy).
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



