Submitted:
23 July 2024
Posted:
30 July 2024
You are already at the latest version
Abstract
Lymphadenopathy is a common manifestation of both reactive and malignant diseases, and fine needle aspiration (FNA) is an effective and inexpensive screening method. It can prevent unnecessary invasive surgery and excisional biopsy, especially in benign cases. Unfortunately, the lack of universally accepted terminology for reporting results has hindered its widespread support. The Sydney system proposal for lymph node cytopathology categorization and reporting introduced five diagnostic categories to address the lack of universally accepted terminology for reporting results in lymphadenopathy. Our study analyzed 188 lymph node FNC samples from King Abdulaziz University Hospital, Saudi Arabia, examining clinical follow-up data, pathology records, patient information, and final diagnosis from January 2019 to December 2022. Most specimens were from axillary LNs, with 99.5% tissue correlation. The Sydney System Category classification identified 56.9% of cases as malignant, while 26.1% were benign. The final surgical specimen diagnosis revealed a higher percentage of malignant diagnoses, with the highest ROM in malignant/Category V. In conclusion, our study demonstrates that LN-FNAC offers high diagnostic accuracy for LN aspirates, with the Sydney approach potentially aiding risk stratification and achieving consistency in cytologic diagnosis, but further multi-centric research is needed.
Keywords:
Lymph node cytology
; fine needle aspiration
; Sydney reporting system
; risk of malignancy
1. Introduction
Lymphadenopathy is a prevalent manifestation of both reactive and malignant diseases. When it comes to screening for and, to a lesser degree, diagnosing lymphadenopathy, fine needle aspiration (FNA) is still an effective and inexpensive option[1,2,3]. While tissue biopsies are often necessary for lymphoma diagnosis, fine-needle aspiration (FNA) is also a useful method for obtaining material for further ancillary tests such as flow cytometry, microbiological cultures, and molecular analysis[4]. Although it remains a subject of debate, fine needle aspiration is a valuable screening technique that can assist prevent unnecessarily invasive surgery and excisional biopsy, particularly in instances with a low likelihood of lymphoma in benign lymphadenopathy cases[2].
Moreover, this procedure is straightforward and can be performed at modest healthcare facilities with little resources.Even a general practitioner can perform it with the aid of ultrasound guidance[5]. It also remains a valuable tool in situations where surgical biopsies cannot be conducted due to the patient's severe illness or the potential for secondary surgery-related complications.
One of the biggest obstacles in lymph node cytology is the lack of a universally accepted terminology for reporting lymph node FNA cytology results[6]. This is among the reasons for lymph node FNA has not gained widespread support from medical practitioners and oncologists, despite its minimum invasiveness, low cost, and quickness[1,3,7,8].
At the 20th International Congress of Cytology in Sydney in May 2019, an expert group released the Sydney system proposal for lymph node cytopathology categorization and reporting[9]. With the introduction of five diagnostic categories as follows: category I/L1 represents inadequate or nondiagnostic results, category II/L2 indicates benign findings, category III/L3 refers to atypical cells of unknown significance or atypical lymphoid cells of uncertain significance, category IV/L4 suggests suspicious results, and category V/L5 represents malignant results[10,11,12].
Nevertheless, there is a lack of data in the literature and the Sy ney method has yet to be utilized enough. For that, this study aimed to fill that knoweledge gap by comparing the ROM for each diagnostic category, the accuracy of the diagnosis, and the efficacy of the Sydney reporting system for lymph node FNA[7,9].
2. Materials and Methods
2.1. Study Design
This study conducted a retrospective analysis on 188 lymph node fine needle aspiration cytology (FNC) samples received from the Department of Pathology at King Abdulaziz University Hospital (KAUH) in Jeddah, Saudi Arabia. The samples were collected between January 1, 2019, and December 31, 2022. The clinical follow-up data and glass slides were examined. The pathology records were obtained and information on the patients' age, gender, location of lymph nodes, clinical history, further testing, and ultimate diagnosis were documented.
2.2. Diagnostic Criteria
Two cytopathologists conducted an independent evaluation and categorization of the smears according to the suggested classification scheme. They were unaware of the final histological diagnosis. All inconsistencies in the categorization were resolved by agreement. The diagnostic criteria for each group are based on the proposed Sydney reporting system and are outlined in provided Table 1.
2.3. Histopathological Correlation
The histopathologic diagnoses, where available, were then compared with the cytopathologic diagnoses. The examples that exhibited discordance were examined and the likely causes for the lack of agreement were determined. Both the histology and fine needle aspiration cytology (FNC) diagnosis of all included cases were found to be consistent and in agreement. The ROM (Risk of Malignancy) was evaluated for each diagnostic group based on histopathologic correlation and the likelihood of malignant outcomes.
2.4. Statistechal Analysis
Data were statistically analyzed using the (SPSS) application version 26. To investigate the association between the variables, the Chi-squared test (χ2) was applied to qualitative data that was expressed as numbers and percentages. Quantitative data were expressed as mean and standard deviation (Mean ± SD). The diagnostic accuracy of Sydney system Category for the prediction of malignant outcomes was assessed in terms of sensitivity, specificity, positive and negative predictive values. Sensitivity was the ability of the test to correctly identify those who has the disease = (true +ve / true +ve + false –ve). Specificity was the ability of the test to correctly identify those who do not have the disease = (True –ve/ false +ve + true –ve). The predictive value (+ ve) (PPV) was the proportion of individuals screened positive by the test who actually have the disease = (PPV)= (true +ve / true +ve +false +ve) and the negative predictive value (- ve) (NPV) was the same for negatives = true –ve / true –ve + false –ve)[13].
The accuracy rate was the fraction of predictions the used modality model got right (Accuracy = Number of correct predictions Total number of predictions) and it equals: (true +ve + true -ve/ true +ve + true -ve +false +ve + fale -ve) (1). The true positive cases were those diagnosed as malignant in the final surgical specimen diagnosis and also had class L5: Malignant in the Sydney system Category, and the true negative cases were those diagnosed as benign in the final surgical specimen diagnosis and had class L 1,2,3, or 4 in the Sydney system Category. The False positive cases were those diagnosed having class L5: Malignant in the Sydney system Category but were benign in the final surgical specimen diagnosis. While the false negatives were those having class L 1,2,3, or 4 in the Sydney system Category but were malignant in the final surgical specimen diagnosis. A p-value of less than 0.05. was considered statistically significant.
3. Results
Of the studied 188 patients, 58% had an age more than 50 years with a mean age of 51.22 ± 16.4 years. Of them, 62% were females (Table 2).
As for the specimen source, most of specimens were from the axillary LNs and 99.5% had tissue correlation. According to the Sydney system Category, most of cases 56.9% were classified as Category V (L5): Malignant and 26.1% were classified as Category II (L2): Benign. After the final surgical specimen diagnosis, 64.4% of specimens were malignant (Table 3 and Figure 1).
(Table 4) demonstrates that on comparing the Sydney System Category classification with the final surgical specimen diagnosis, the sensitivity of the Sydney System Category classification was 78.5% and its specificity was 82%. The PPV was 88.7% and the NPV was 67.9%. The Accuracy rate of the Sydney System Category classification was 79.7%.
The correlation between the final surgical specimen diagnosis and the Sydney System Categories revealed that malignant diagnosis had a significant higher percent of having the L5: Malignant the Sydney System Category (p=<0.05) (Table 5).
The detailed list of malignant cases in different diagnostic categories and the associated ROM in each category are presented in (Table 5). The ROM was least (14.2%) for the benign Category II (L2), and highest (88.76%) for the malignant/ Category V (L5). The χ2 test revealed that this difference was statistically significant (χ2 = 13.95, p-value = <0.001).
4. Discussion
Fine needle aspiration (FNA) remains an important technique used as a first line diagnostic approach for most lymphadenopathy of unknown etiology[5]. Its broad applicability in the assessment of lymphadenopathy is facilitated by its minimal invasiveness, rapidity, cost-effectiveness, and the ability to provide material for multiple ancillary techniques[4]. Nevertheless, the traditional, currently used method of reporting lymph node smears lacks a consistent diagnostic categorization, a shared language of reporting among cytopathologists, and unambiguous communication to physicians regarding the risk of malignancy and subsequent therapy[3,6,14].
In the last decades with the introduction of the Bethesda reporting system for the cervical cytology[15], the implementation of standardized reporting methods in cytopathology has been seen to decrease intra-observer variability in reporting. It also facilitates the communication in the clinical world and helped to transfer the clinically important data in a consistent and replicable way. In addition, it will guide the clinical team in regards the management and risk stratification.
In May 2019, During the International Congress of Cytology in Sydney, a systems approach was proposed for the classification, reporting, and execution of lymph node cytology[8,9,16,17]. Their main aim was to develop a common language and to help cytopathologists, hematopathologists, physicians, surgeons, and other medical professionals communicate more effectively, establish consensus criteria and a reference framework. Moreover, offer management suggestions associated with the reporting categories, which may involve utilizing clinical and imaging follow-up, supplementary testing, and potential requirement for LN excision. This will ultimately enhance the accuracy of LN-FNAC and raise awareness among clinicians on its diagnostic capabilities[9,16,18].
Before a newly proposed classification system can be recommended for everyday use, it is necessary to establish its validity, repeatability, and clinical value. For this purpose, several research studies have been conducted at various academic institutions throughout various geographical areas. In this series, we demonstrated the Sydney system's capacity to classify lymph node FNCs into groups with progressively greater ROMs[3,12,19].
In our study included a total of 188 cases. The number of cases falling into each category were as follows: L1 (inadequate/nondiagnostic) - 6 cases (33.3%), L2 (benign) - 49 cases (14.2%), L3 (atypical cells of undetermined significance/atypical lymphoid cells of uncertain significance) - 15 cases (66.6%), L4 (suspicious) - 11cases (63.6%), and L5 (malignant) - 107cases (88.7%). Therefore, L5 was the category that was utilized most frequently. Remarkably, the ROM (Rate of Metastasis) for the L5 category was very high at 56.1%. The fact that our hospital is a tertiary care facility means that we treat a disproportionately large number of cancer patients, which may explain why our results are so above of the average in many published data.
The ROM for category I (L1) was shown to be rather low at 33.2%. Of the 6 cases on this category, we did find that most of these smears showed blood and necrosis which may be related to the expertise of the clinician or the radiologist, as most of the FNA at our institute performed by the non-cytopathologist. This rate was similar to the reported results by Parikshaa Gupta. Et al and much lower than what reported by Elena Vigliar. et al as they reported L1 category to be higher at 26.5% and 50%, respectively[17,20]. For the L2 (benign) category in our study, it was comparable to their data at 14.2%. After further surgical biopsy, 7 of the 49 cases in this group proved to be malignant. Reviewing these cases, we did find that in a small number of cases with Hodgkin lymphoma, the RS cells were spared, and the cytology sample did not accurately represent the disease. Furthermore, three cases comprised metastatic breast ductal carcinoma, in which no carcinoma cells were detected in the cytology specimens and no cell block was conducted.
The L3 category, also known as atypia of indeterminate significance, was implemented by the Sydney reporting systems to ensure high accuracy in identifying benign and malignant cases by maintaining high negative and positive predictive values, respectively. In our data analysis, we discovered that the rate of malignancy (ROM) for category L3 is somewhat higher than the given value of 66.6%, with a comparison to 50% with false positive rate of 7.5%[9,16,20]. Careful analysis of the cytology smear and the subsequent surgical specimen of these cases showed that two of these 5 cases had prominent follicular hyperplasia and the smear showed many larger cells which was reported as atypical cells. Simillar observation was reported by Ankita Shibu Robert, et al in their cohort of cases[21]. In our opinion, flow cytometry is highly valuable in reducing the occurrence of false positive cytology results by effectively demonstrating the characteristics of follicular hyperplasia through the strong expression of CD20 and CD10 by the population of interest.
In this research, each of the L4 (suspected to be malignant) and L5 (malignant) groups had a very high ROM of 63.6% and 88.7%, respectively. Interestingly, the L4 ROM that we observed in our sample is somewhat lower than what has been reported in several investigations[9,16,18,22]. This is due to the use of ancillary methods like flow cytometry in their research which was not done in a good number of our cases in this category. A second diagnostic level based on supplementary procedures, as proposed in the categorization system, might further reduce the frequency of false negative results in this category.
Ancillary methods like as flow cytometry, immunocytochemistry (ICC), and molecular assays are crucial in providing a precise diagnosis, as well as for categorizing and subtyping lymph nodal aspirates[20,22]. We advocate for their utilization wherever possible. These tests have a crucial role in confirming diagnosis for category IV and V aspirates, while their relevance is restricted for categories I, II and III. It is recommended to use these methods when dealing with patients that have questionable clinical characteristics, and the results should be analyzed along with clinical and cytomorphologic aspects. However, it is not possibel to assessed it is role in our chochort of cases as it was not done on all cases.
5. Conclusions
In conclusion, when it comes to diagnosing LN aspirates, LN-FNAC provides a high degree of diagnostic accuracy. The suggested Sydney approach, if implemented, has the potential to aid in risk-stratification using cytology and to achieve consistency and repeatability in cytologic diagnosis. It seems like a strong and promising method for reporting and categorization, but to determine its validity and reliability, bigger multicentric research are needed.
Author Contributions
Formal analysis and supervision, Doaa Alqaidy.; investigation and resources, Amal Magrabi and Hind Al-Thumali.; writing, reviewing and editing, Doaa Alqaidy. All authors have read and agreed to the published version of the manuscript.”
Funding
“This research received no external funding”.
Institutional Review Board Statement
The study was conducted in accordance an approval by the Institutional Ethics Committee of Research Ethics Committee (REC)
(protocol code 705-23 and date of approval: 12/27/2023).”
Informed Consent Statement
“Not applicable.”
Data Availability Statement
Not applicable.
Conflicts of Interest
“The authors declare no conflicts of interest.”
References
- Gupta, R.; Naran, S.; Lallu, S.; Fauck, R. The diagnostic value of fine needle aspiration cytology (FNAC) in the assessment of palpable supraclavicular lymph nodes: a study of 218 cases. Cytopathology 2003, 14, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Hafez, N.H.; Tahoun, N.S. Reliability of fine needle aspiration cytology (FNAC) as a diagnostic tool in cases of cervical lymphadenopathy. Journal of the Egyptian National Cancer Institute 2011, 23, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Makarenko, V.V.; DeLelys, M.E.; Hasserjian, R.P.; Ly, A. Lymph node FNA cytology: diagnostic performance and clinical implications of proposed diagnostic categories. Cancer Cytopathology 2022, 130, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Cordero, R. Challenges and opportunities in lymph node FNA: Insights from the DELYCYUS study. Cancer Cytopathology 2023, 131, 677–678. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, R.; Wilkinson, A. Utility of fine needle aspiration cytology of lymph nodes. IOSR J Dent Med Sci 2013, 8, 13–18. [Google Scholar] [CrossRef]
- Zhou, J.; Li, F.; Meng, L.; Hao, F.; Liu, X.; Zhao, C.; Zhang, K.; Dong, A. Fine needle aspiration cytology for lymph nodes: a three-year study. British Journal of Biomedical Science 2016, 73, 28–31. [Google Scholar] [CrossRef] [PubMed]
- Caputo, A.; Ciliberti, V.; D'Antonio, A.; D'Ardia, A.; Fumo, R.; Giudice, V.; Pezzullo, L.; Sabbatino, F.; Zeppa, P. Real-world experience with the Sydney system on 1458 cases of lymph node fine needle aspiration cytology. Cytopathology 2022, 33, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Kanhe, R.; Tummidi, S.; Kothari, K.; Agnihotri, M. Utility of the proposed Sydney system for classification of fine-needle aspiration cytopathology of lymph node: a retrospective study at a tertiary care center. Acta Cytologica 2023, 67, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Al-Abbadi, M.A.; Barroca, H.; Bode-Lesniewska, B.; Calaminici, M.; Caraway, N.P.; Chhieng, D.F.; Cozzolino, I.; Ehinger, M.; Field, A.S.; Geddie, W.R. A proposal for the performance, classification, and reporting of lymph node fine-needle aspiration cytopathology: the Sydney system. Acta Cytologica 2020, 64, 306–322. [Google Scholar] [CrossRef] [PubMed]
- Saradva, N.; Trivedi, D.P. Lymph node fine needle aspiration cytology reporting using Sydney system at tertiary care center.
- Sreelekshmi, J.R.; Joseph, T. Structured reporting of lymph node cytopathology using the 2020 sydney system guidelines-a retrospective study. National Journal of Laboratory Medicine 2023, 12, 39–44. [Google Scholar] [CrossRef]
- Zeppa, P.; Cozzolino, I.; Caraway, N.P.; Al-Abbadi, M.A.; Barroca, H.; Bode-Lesniewska, B.; Calaminici, M.; Chhieng, D.F.; Ehinger, M.; Geddie, W.R. Announcement: the international system for reporting lymph node cytopathology. Acta Cytologica 2020, 64, 299–305. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: the kappa statistic. Biochemia medica 2012, 22, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Paul, P.; Goswami, B.; Chakrabarti, S.; Giri, A.; Pramanik, R. Fine needle aspiration cytology of lymph nodes-An institutional study of 1448 cases over a five year period. Journal of Cytology 2004, 21, 187–190. [Google Scholar] [CrossRef]
- Pangarkar, M.A. The Bethesda System for reporting cervical cytology. Cytojournal 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, S.; Aziz Khan, A.; Ahuja, R.; Ahuja, P.; Zaheer, S. Systematic Review and Meta-Analysis of the Diagnostic Accuracy of the Sydney System for Reporting Lymph Node Fine-Needle Aspiration Biopsy in Diagnosing Malignancy. Acta Cytologica 2024, 68, 13–25. [Google Scholar] [CrossRef]
- Vigliar, E.; Acanfora, G.; Iaccarino, A.; Mascolo, M.; Russo, D.; Scalia, G.; Della Pepa, R.; Bellevicine, C.; Picardi, M.; Troncone, G. A novel approach to classification and reporting of lymph node fine-needle cytology: application of the proposed Sydney system. Diagnostics 2021, 11, 1314. [Google Scholar] [CrossRef] [PubMed]
- Torres Rivas, H.E.; Villar Zarra, K.; Pérez Pabón, L.A.; González Gutierréz, M.d.l.P.; Zapico Ortiz, N.; Olmo Fernández, M.d.M.; Nieto Llanos, S.; Antoranz Álvarez, N.; Gómez Martín, Á.; Fernández Fernández, L.M. Ultrasound-guided fine-needle aspiration of superficial lymphadenopathy performed by interventional pathologists: the applicability of the Sydney system from 2 years of experience and 363 cases. Acta Cytologica 2021, 65, 453–462. [Google Scholar] [CrossRef] [PubMed]
- GV, N.; Indoria, P.; Bijjaragi, S. Application of the proposed Sydney system of reporting lymphnode cytopathology: A retrospective study in a tertiary institute. Onkologia i Radioterapia 2023, 17. [Google Scholar]
- Gupta, P.; Gupta, N.; Kumar, P.; Bhardwaj, S.; Srinivasan, R.; Dey, P.; Rohilla, M.; Bal, A.; Das, A.; Rajwanshi, A. Assessment of risk of malignancy by application of the proposed Sydney system for classification and reporting lymph node cytopathology. Cancer Cytopathology 2021, 129, 701–718. [Google Scholar] [CrossRef] [PubMed]
- Robert, A.S.; Saldanha, C. An approach to classification and reporting lymph node cytopathology using Sydney system and evaluating the likelihood of malignancy. Biomedicine 2023, 43, 701–705. [Google Scholar] [CrossRef]
- Juanita, J.; Ikram, D.; Sungowati, N.K.; Purnama, I.P.; Amalia, A.; Ningrati, A.F.; Miskad, U.A. Diagnostic accuracy of lymph nodes fine needle aspiration biopsy based on the Sydney system for reporting lymph node cytology. Asian Pacific Journal of Cancer Prevention: APJCP 2023, 24, 1917. [Google Scholar] [CrossRef]
Figure 1.
Percentage distribution of the Sydney System Category classification.
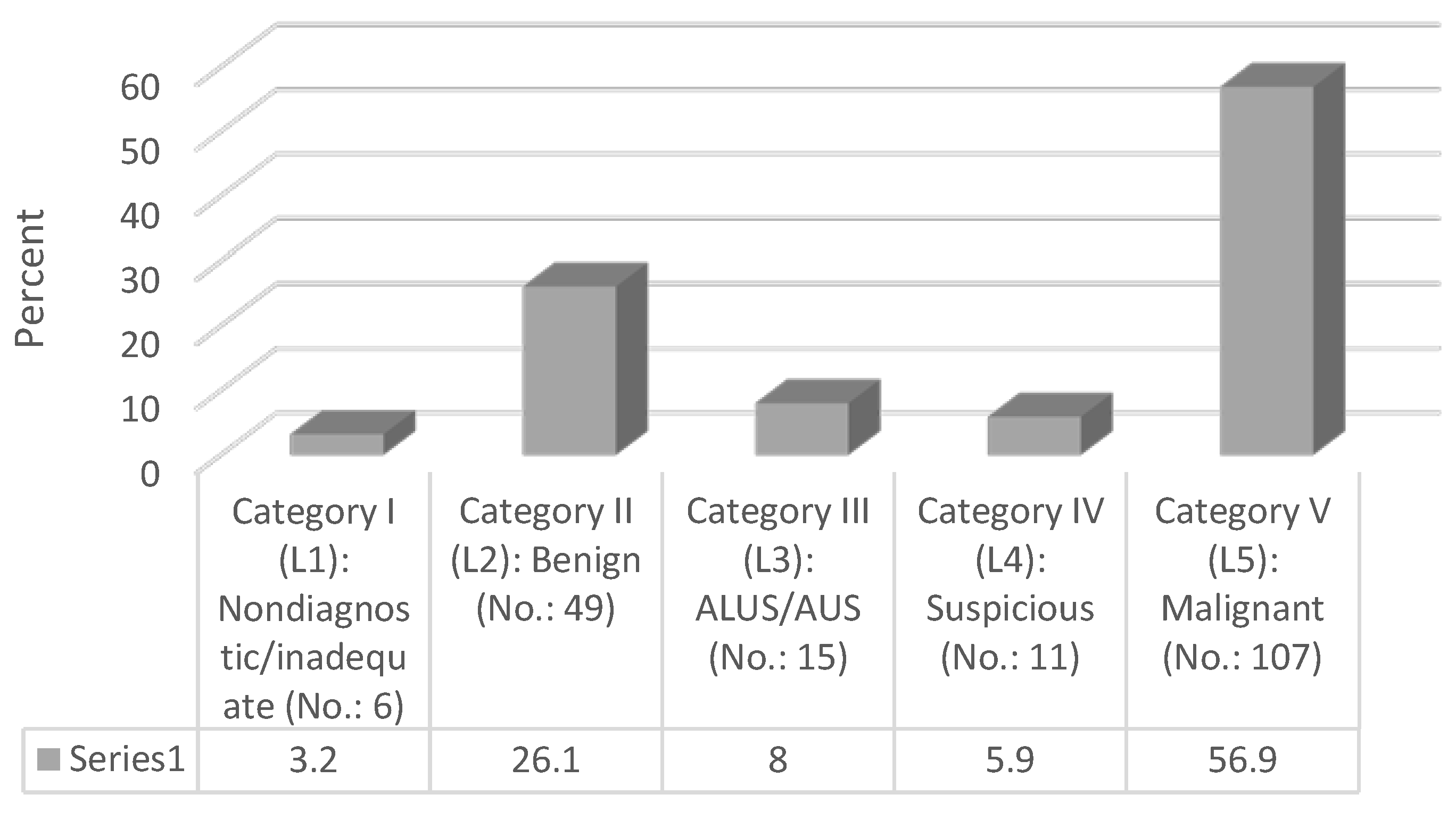

Table 1.
The cytological characteristics of each group in the Sydney System for reporting lymph node cytology.
Table 1.
The cytological characteristics of each group in the Sydney System for reporting lymph node cytology.
| Category | The cytomorphologic features |
|---|---|
| L1: Inadequate/Insufficient | Scant cellularity; Extensive necrosis; Technical limitations that cannot be overcome |
| L2: Benign | Suppurative and granulomatous inflammation; Heterogeneous lymphoid population with small lymphocytes predominating, and often germinal centers with dendritic cells and tingible body macrophages |
| L3: Atypical (Cells) Undetermined Significance/Atypical Lymphoid (Cells) of Uncertain Significance (ALUS/AUS) | Heterogeneous lymphoid population, features suggest a reactive process, follicular lymphoma cannot be excluded; Excess of large cells (centroblasts or immunoblasts) or immature small lymphoid cells or cases where the atypical cells are not lymphoid cells. |
| L4: Suspicious | Small and/or medium-sized, monomorphic atypical lymphoid cells suspicious of lymphoma, but the cytomorphology alone is not sufficient; Polymorphous lymphoid smears, few Hodgkin- or Reed-Sternberg-like cells are detected; Large cell or Burkitt lymphomas scantly cellular; Smears in which atypical cells suspicious for metastasis are detected, but are too scant to be diagnostic |
| L5: Malignant | NHL; HL: Appropriate cellular background and diagnostic Hodgkin and Reed-Sternberg cells; Metastatic neoplasms. |
Table 2.
Distribution of studied patients according to their demographic characters ,No.: 188
| Variable | No. (%) |
|---|---|
| Age | |
| ≤ 50 years | 79 (42) |
| > 50 years | 109 (58) |
| Age (years) (Mean ± SD) | 51.22 ± 16.4 |
| Gender | |
| Female | 117 (62.2) |
| Male | 71 (37.8) |
Table 3.
Distribution of patients according to specimen source, tissue correlation, Sydney system Category and final surgical specimen diagnosis (No.: 188) (No.: 188).
Table 3.
Distribution of patients according to specimen source, tissue correlation, Sydney system Category and final surgical specimen diagnosis (No.: 188) (No.: 188).
| Specimen source | |
|---|---|
| Axillary LN | 72 (38.3) |
| Cervical LN | 20 (10.6) |
| Hilar mass | 9 (4.8) |
| Inguinal LN | 2 (1.1) |
| Neck LN | 2 (1.1) |
| Paratracheal LN | 18 (9.6) |
| Peripancreatic LN | 1 (0.5) |
| Subcarinal LN | 22 (11.7) |
| Submandibular LN | 8 (4.3) |
| Supraclavicular LN | 3 (1.6) |
| Thyroid | 1 (0.5) |
| NA | 30 (16) |
| Tissue correlation | |
| No | 1 (0.5) |
| Yes | 187 (99.5) |
| Sydney system Category | |
| Category I (L1): Nondiagnostic/inadequate | 6 (3.2) |
| Category II (L2): Benign | 49 (26.1) |
| Category III (L3): ALUS/AUS | 15 (8) |
| Category IV (L4): Suspicious | 11 (5.9) |
| Category V (L5): Malignant | 107 (56.9) |
| Final surgical specimen diagnosis | |
| Benign | 67 (35.6) |
| Malignant | 121 (64.4) |
N.B.: ALUS/AUS = atypical lymphoid cells of uncertain significance/atypical cells of undetermined significance.
Table 4.
Validity and precision of the Sydney System Category classification when compared to the final surgical specimen diagnosis.
Table 4.
Validity and precision of the Sydney System Category classification when compared to the final surgical specimen diagnosis.
| Variable | Parameter | Estimate |
|---|---|---|
| Sydney System Category classification results compared to the final surgical specimen diagnosis | True positive | 95 (50.5) |
| True negative | 55 (29.3) | |
| False positive | 12 (6.4) | |
| False negative | 26 (13.8) | |
| Sensitivity | 78.5% | |
| Specificity | 82% | |
| Positive predictive value (PPV) | 88.7% | |
| Negative predictive value (NPV) | 67.9% | |
| Accuracy rate | 79.7% |
Table 5.
Correlation between the final surgical specimen diagnosis and the Sydney System Categories Validity.
Table 5.
Correlation between the final surgical specimen diagnosis and the Sydney System Categories Validity.
|
Cytologic category as per the proposed Sydney system for reporting lymph node cytopathology |
Total | Final surgical specimen diagnosis | χ2 | p-value | |
|---|---|---|---|---|---|
| No. (%) | Benign No. (%) |
Malignant No. (%) |
|||
| L1: Inadequate/Insufficient | 6 (3.2) | 4 (6) | 2 (1.7) | 13.95 | <0.001 |
| L2: Benign | 49 (26.1) | 42 (62.7) | 7 (5.8) | ||
| L3: Atypical (Cells) Undetermined | 15 (8) | 5 (7.5) | 10 (8.3) | ||
| L4: Suspicious | 11 (5.9) | 4 (6) | 7 (5.8) | ||
| L5: Malignant | 107 (56.9) | 12 (17.9) | 95 (78.5) | ||
Table 6.
Risk of Malignancy (ROM) Associated with each cytologic diagnostic category of the proposed Sydney System for Reporting Lymph Node Cytopathology.
Table 6.
Risk of Malignancy (ROM) Associated with each cytologic diagnostic category of the proposed Sydney System for Reporting Lymph Node Cytopathology.
| Cytologic category as per the proposed Sydney system for reporting lymph node Cytopathology |
Total no. of cases with histopathologic diagnosis in each diagnostic category (No.:188) | Total no. of cases reported as malignant on histopathology (No.: 121) | Overall risk of malignancy (ROM) (%) |
|---|---|---|---|
| Category I (L1): Nondiagnostic/inadequate | 6 (3.2) | 2 | 33.3 |
| Category II (L2): Benign | 49 (26.1) | 7 | 14.2 |
| Category III (L3): ALUS/AUS | 15 (8) | 10 | 66.6 |
| Category IV (L4): Suspicious | 11 (5.9) | 7 | 63.6 |
| Category V (L5): Malignant | 107 (56.9) | 95 | 88.7 |
N.B.: ROM = Risk of Malignancy
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



