
Submitted:
04 September 2024
Posted:
09 September 2024
You are already at the latest version
Abstract
Multiple sclerosis (MS) is an immune-mediated disease characterized by inflammation, demyelination, and neurodegeneration within the central nervous system. Brain plasticity, the brain's ability to adapt its structure and function, plays a crucial role in mitigating MS's impact. This paper explores the potential benefits of lifestyle changes and nutraceuticals on brain plasticity in MS population. Lifestyle modifications, including physical activity and dietary adjustments, can enhance brain plasticity by upregulating neurotrophic factors, promoting synaptogenesis, and reducing oxidative stress. Nutraceuticals, such as vitamin D, omega-3 fatty acids, and antioxidants like alpha-lipoic acid, have shown promise in supporting brain health through anti-inflammatory and neuroprotective mechanisms. Regular physical activity has been linked to increased levels of brain-derived neurotrophic factor and improved cognitive function. Dietary interventions, including caloric restriction and the intake of polyphenols, can also positively influence brain plasticity. Integrating these lifestyle changes and nutraceuticals into the management of MS could provide a complementary approach to traditional therapies, potentially improving neurological outcomes and enhancing the quality of life for MS population.
Keywords:
multiple sclerosis
; neurodegeneration
; neurorehabilitation
; nutraceuticals
; obesity
Introduction
Multiple sclerosis (MS) is the most common form of immune-mediated pathology affecting the central nervous system (CNS) [1]. It is characterized by neuronal degeneration caused by inflammation, which, together with demyelination and axonal degeneration, represents the basis of the pathogenic mechanisms but also of the clinical manifestations [2]. The characteristic of the lesions detected in population with MS is represented by multifocal areas of demyelination that produce the destruction of oligodendrocytes in the affected areas and the appearance of glial scars. Axonal injury that appears later in the course of the disease is another pathological change characteristic of MS [3]. The symptomatology of this pathology is varied and is most frequently manifested by visual disturbances (especially changes in the visual field/visual acuity, the appearance of scotomas), paresthesia, urinary incontinence, intestinal incontinence, focal weakness, or cognitive dysfunctions. These symptoms are more common in young adults and are characterized by acute relapses, varying both in intensity and manifestation depending on the location of the lesions [4].
Regarding the immunopathology of MS, it has been observed that cellular immunology is dominated by altered interactions between T and B cells and myeloid cells. Additionally, a series of alleles of the major histocompatibility complex, especially from class I and II, seem to be involved in increasing the susceptibility to MS. In addition to these immunological changes and interactions, antibodies directed against myelin oligodendrocyte glycoprotein, a protein that is part of the myelin structure, have been discovered [3]. Molecular mimicry is another immunological mechanism. This mimicry occurs secondary to either bacterial or viral infection, which can trigger a cross antigenic response between viral antigens and myelin components [3].
In conclusion, immunopathology of MS involves complex interactions between B and T lymphocytes, playing crucial roles in disease initiation and progression. Here's a summary of their involvement:
This complex interplay between B and T lymphocytes underscores the multifaceted nature of MS immunopathology, suggesting that targeting both cell types may be necessary for effective treatment strategies [1,2,3,4].
MS can be categorized into different stages depending on its progression. About 65% of cases are relapsing-remitting MS (RRMS), marked by neurological symptoms that worsen over days to weeks and last 24-48 hours. Primary progressive MS (PPMS), representing 15% of cases, involves gradual deterioration without relapses. Secondary progressive MS (SPMS) follows RRMS and is characterized by steady neurological decline. MS with progressive relapses features ongoing relapses with progressive deterioration, while an isolated clinical syndrome represents a single CNS inflammatory demyelination episode. Fulminant MS, the most severe form, rapidly leads to functional impairment, whereas the benign form is mild with infrequent relapses [1,3,5].
The most common clinical pattern is RRMS, where in most cases relapses are followed by periods of partial or complete recovery, often without treatment. However, in the case of partial recovery, residual symptomatology contributes to progressive deterioration leading to general disability [1,3,5]. The McDonald criteria are the most widely accepted diagnostic guidelines for MS, focusing on key aspects such as Dissemination in Space (DIS) and Time (DIT). DIS involves lesions in different areas of the central nervous system (CNS), while DIT refers to the development of new lesions over time. Revisions in 2010 and 2017 emphasized the use of MRI to demonstrate these criteria, enabling earlier diagnosis. Additionally, the 2017 revision reintroduced cerebrospinal fluid (CSF) analysis, particularly highlighting the presence of oligoclonal bands (OCBs). These criteria are mainly applied to populations presenting with a typical clinically isolated syndrome (CIS), ensuring that alternative diagnoses are carefully excluded.
The goals of long-term treatment are to reduce the risk of developing permanent disability and to reduce the rates of relapse [7].
Risk Factors for Development and Progression of MS
The exact cause of the development of MS is unknown, but several studies have highlighted some risk factors that could increase the susceptibility to the development of this pathology [10]. Some studies showed that populations diagnosed with an autoimmune pathology such as type 1 diabetes mellitus present a double risk to develop MS compared to the population without the disease [8,9,10].
Genetic susceptibility is an important risk factor. After numerous studies conducted on this topic, more than two hundred polymorphisms involved and associated with multiple sclerosis were discovered. Although the mechanism by which these polymorphisms increase the risk of disease onset is unclear, it has been found that they are present in the regulatory regions of the genes involved in immunological functions, thus being associated with other autoimmune pathologies [11,12,13].
Several external risk factors have been identified that may influence the likelihood of developing MS, including viral infections, geographical factors, sunlight exposure, variations in vitamin D3 levels, smoking, obesity, and vaccination status [14,15]. Research suggests that viral infections, particularly the Epstein-Barr virus (EBV), may act as infectious stimuli for the immune system, potentially triggering an exaggerated immune response that could lead to the onset of MS, although the role of other viruses in this process has not been entirely ruled out [16,17]. Sunlight exposure, which either directly through ultraviolet radiation or indirectly by raising serum levels of vitamin D3, is believed to offer some protection against the development of MS, thereby linking it to geographical factors such as latitude, altitude, and geographical area [18]. Additionally, tobacco use, known for increasing the risk of numerous chronic diseases with significant morbidity and mortality, is also associated with a higher risk of MS. While nicotine itself may not be directly harmful, the byproducts of combustion are thought to be responsible, potentially due to the increased oxidative stress observed in smokers, although the exact mechanism remains unclear [19,20].
Acknowledging risk factors in MS is important for several reasons:
- Research direction: Identifying risk factors guides future research efforts, helping to elucidate MS pathogenesis and develop new therapeutic strategies [12].
By acknowledging and addressing these risk factors, we can potentially reduce MS incidence, improve population outcomes, and advance our understanding of this complex disease.
Brain Plasticity
Brain plasticity refers to the brain's ability to change its structure and function in response to experiences, learning, and environmental stimuli [21]. It is a fundamental process that allows the brain to adapt, learn, and recover from injuries or diseases [22]. Plasticity can occur at the cellular and molecular levels, leading to changes in neuronal properties, synaptic connections, and neural networks [23]. Research has shown that brain plasticity is present throughout the lifespan, although the efficiency of plasticity may decline with age [24]. Genetic factors also play a role in brain plasticity, with heritability estimates suggesting that genetic variations contribute to interindividual variability in plasticity [25].
The mechanisms of brain plasticity refer to the processes by which the brain can reorganize and modify its neural connections in response to numerous factors such as experience, learning, injury, and disease. These mechanisms include the following (Figure 1):
- Brain plasticity involves modifications in the strength and number of connections between neurons, known as synapses. This can occur through processes such as long-term potentiation and long-term depression, which are activity-dependent changes in synaptic transmission.
- Plasticity can also involve the creation of new synapses between neurons. This process, known as synaptogenesis, allows for the establishment of new connections and the rewiring of neural circuits.
- Plasticity can lead to alterations in the structure and function of individual neurons. This can include changes in dendritic branching, axonal sprouting, and the generation of new neurons through neurogenesis.
- Plasticity can be influenced by changes in the levels and activity of various neurotransmitters and neuromodulators. These substances can affect synaptic transmission and neuronal excitability, thereby influencing the plasticity of neural circuits.
Brain plasticity has important implications in various contexts, including neurodevelopmental disorders, addiction, stroke recovery, and neurodegenerative diseases [22,29,30].
Physical activity has a significant impact on brain plasticity, which refers to the brain's ability to reorganize and modify its neural connections. Several studies have shown that physical activity can enhance brain plasticity and promote various neuroadaptive processes.
One study found that voluntary exercise in rats increased both precursor and mature forms of brain-derived neurotrophic factor (BDNF) in the hippocampus, a region important for learning and memory [31]. BDNF is a neurotrophic factor that plays a crucial role in synaptic plasticity and neuronal survival. Exercise also increased the activity of tissue-type plasminogen activator (tPA), an enzyme involved in the cleavage of proBDNF into mature BDNF. Blocking tPA activity reduced the exercise-induced effects on BDNF and its downstream signaling pathways [31].
Regular physical activity has also been shown to enhance brain plasticity in humans. Studies have demonstrated that aerobic exercise, anaerobic exercise, and resistance exercise can positively influence brain plasticity and cognitive function [32]. These exercise modalities can lead to changes in the expression of neurotrophic factors, such as BDNF, lactate, and vascular endothelial growth factor, which promote neurogenesis and synaptic plasticity [32].
Furthermore, physical activity can reduce short interval intracortical inhibition, a measure of cortical inhibition, and create a more optimal environment for plasticity [33]. Exercise-induced reductions in SICI may contribute to enhanced neuroplasticity and improved motor learning [33].
Overall, physical activity has been shown to promote brain plasticity through various mechanisms, including the upregulation of neurotrophic factors, modulation of synaptic activity, and reduction of cortical inhibition. These findings highlight the importance of regular physical activity for maintaining and enhancing brain health and function [31,32,33,34,35,36].
There is limited information available specifically addressing the adverse effects of MS medications on brain plasticity. However, some studies suggest that certain medications used to treat MS may have a positive impact on brain plasticity by reducing inflammation and promoting recovery. One study found that treatment with interferon beta-1a, a commonly used MS medication, improved cortical function and cognitive deficits in newly diagnosed MS populations with gadolinium-enhancing lesions [37]. Another study showed that reduction of inflammation with interferon beta was associated with the restoration of brain plasticity in MS populations, as evidenced by improvements in task performance and synaptic plasticity [38].
It is important to note that the studies mentioned above focused on the positive effects of MS medications on brain plasticity, rather than adverse effects. Adverse effects of MS medications can vary depending on the specific medication and individual risk factors. It is recommended to consult with a healthcare professional for a comprehensive understanding of the potential adverse effects of specific MS medications on brain plasticity.
Overall, while there is limited research specifically addressing adverse effects, current evidence suggests that some MS medications may have a positive impact on brain plasticity by reducing inflammation and promoting recovery. Further research is needed to fully understand the relationship between MS medications and brain plasticity.
Different diets can have an impact on brain plasticity, which refers to the brain's ability to change and adapt in response to experiences and environmental factors. Several studies have investigated the effects of various dietary interventions on brain plasticity markers and cognitive function.
Caloric restriction and intermittent fasting have been shown to enhance brain plasticity in animal studies. These dietary interventions have been associated with increased expression of neurotrophic factors, synaptic function, and adult neurogenesis in the hippocampus, a brain region important for learning and memory [39]. However, more research is needed to understand the mechanisms underlying these effects and to determine their translatability to humans.
Dietary supplementation with polyphenols and polyunsaturated fatty acids (PUFA) has also been found to impact brain plasticity. For example, docosahexaenoic acid (DHA), an omega-3 fatty acid found in fatty fish, has been shown to influence protein levels related to metabolic homeostasis and synaptic plasticity in the hypothalamus and hippocampus of rats [40]. Additionally, DHA supplementation has been associated with improved spatial memory ability in mice [41].
Furthermore, the consumption of dark chocolate, which contains flavonoids and other bioactive compounds, has been shown to have positive effects on brain functions. In a rat study, different dietary patterns of dark chocolate were found to reverse the harmful effects of chronic isolation stress on synaptic potency, plasticity, learning, and memory in the hippocampus [42].
Overall, these studies suggest that different diets can modulate brain plasticity markers and cognitive function. However, more research is needed to fully understand the specific mechanisms and to determine the optimal dietary interventions for promoting brain health and function in humans.
Neurodegeneration in MS
Neurodegeneration in MS is a key factor in disease progression and disability. Several mechanisms have been proposed to contribute to neurodegeneration in MS, as shown in the following image (Figure 2).
- Chronic inflammation in MS leads to the activation of microglia, which releases inflammatory mediators and generates oxidative stress. This can result in damage to neurons and axons [43,44,45]. Neuroinflammation, characterized by the infiltration of immune cells into the central nervous system, can contribute to neurodegeneration in MS. Immune-mediated mechanisms, such as the release of inflammatory cytokines and autoantibodies, can cause neuronal damage [46].
- Glutamate, an excitatory neurotransmitter, can accumulate in the extracellular space during inflammation and demyelination in MS. Excessive glutamate can lead to excitotoxicity, causing damage to neurons and axons [45].
-
Additional mechanisms:
- a.
- Altered sodium and calcium homeostasis contributes to axonal injury [44].
- b.
- Activated microglia release neurotoxic factors [45].
- c.
- Myelin debris accumulation impairs neurorepair and plasticity.
- d.
- Increased TNF signaling in neurons leads to programmed cell death [50].
- e.
- Impaired astrocytic support may contribute to axonal degeneration [49].
- f.
Clinical and lifestyle predictors for MS progression can help identify individuals at risk for worsening disease outcomes. Younger age at onset of MS has been associated with a higher risk of disease progression [51]. Men with MS have been found to have an increased risk of disease progression compared to women [52]. Population with progressive forms of MS, such as SPMS, are more likely to experience disease progression [52]. A higher number of relapses during the disease has been associated with an increased risk of progression [52]. Higher levels of disability at baseline have been linked to a greater likelihood of disease progression [51]. Smoking has been identified as a lifestyle factor that is associated with subsequent disability worsening in individuals with MS [53]. Higher levels of physical activity, both premorbid and current, have been found to be associated with a reduced risk of disability progression in MS [54]. A high-quality diet, including the avoidance of meat and dairy, has been associated with better fatigue and disability trajectories in MS [55]. Lower sun exposure during childhood and adolescence has been linked to an increased risk of disease progression [51].
The most important modifiable factors which act as a risk/protective factor in MS are summarized in the following table (Table 1).
Vascular and psychiatric comorbidities have also been associated with subsequent disability worsening in individuals with MS [53].
Nutraceuticals in MS
Nutraceuticals are natural or bioactive compounds found in food or dietary supplements that have potential health benefits beyond basic nutrition. They are often used as adjunctive treatments to support overall health and well-being.
In MS, several nutraceuticals have been studied for their potential benefits. The most used nutraceuticals in MS include:
- Alpha lipoic acid (ALA) is an antioxidant that has shown promise in improving clinical and biological outcomes in MS, such as reducing fatigue and improving brain volume [59].
- Ginkgo biloba has been reported to improve clinical and biological outcomes in MS, including fatigue and antioxidant capacity [59].
- Biotin supplementation has shown potential in improving clinical outcomes in MS, such as reducing disability progression and improving walking ability [59].
- Omega-3 fatty acids, found in fish oil, have anti-inflammatory properties and may help reduce inflammation in MS [58].
A study found no significant evidence for drug interactions between conventional MS drugs and several nutraceuticals, including ginger, cranberry, vitamin D, fatty acids, turmeric, probiotics, or glucosamine [60].
The presumed mechanisms of action of nutraceuticals in MS involve their ability to target various pathways involved in the pathogenesis of the disease (Figure 3). Some of these mechanisms are:
- Nutraceuticals such as polyunsaturated fatty acids (PUFAs), green tea flavonoids (epigallocatechin-3-gallate), curcumin, and scorpion toxins have been found to possess anti-inflammatory properties and can modulate the immune response in MS. They can inhibit pro-inflammatory signaling pathways, such as NF-κB or toll-like receptors and reduce the activity of auto-aggressive immune cells. These effects may help reduce inflammation and immune-mediated damage in MS [56].
- Oxidative stress is implicated in the pathogenesis of MS. Nutraceuticals like green tea, curcumin, and resveratrol have antioxidative properties and can scavenge free radicals, reducing oxidative damage. By reducing oxidative stress, these compounds may protect against neuronal damage and inflammation in MS [61].
- Nutraceuticals such as flavonoids, terpenoids, and polyphenols have shown potential in promoting neuroprotection and myelin repair in animal models of MS. They may support the survival and function of neurons, promote remyelination, and enhance endogenous repair processes [62].
- Epigenetic modifications play a role in MS. Some nutraceuticals, such as plant polyphenols, Ω-3 and Ω-6 polyunsaturated fatty acids, and sulfur-containing compounds, can influence gene expression through epigenetic mechanisms. These compounds may regulate the production of pro-inflammatory proteins and modulate immune responses in MS [63].
Vitamin D3
Vitamin D3, also known as cholecalciferol, is a form of vitamin D that is synthesized in the skin when exposed to sunlight or obtained through dietary sources. It plays a crucial role in maintaining calcium and phosphate balance in the body, which is essential for bone health. However, emerging research suggests that vitamin D3 also has important roles in brain plasticity and MS [64].
Vitamin D3 has been found to have immunomodulatory and neuroprotective effects within the central nervous system. It acts through its receptors in glial cells, such as astrocytes and microglia, to influence the production of proinflammatory cytokines and antioxidants. This modulation of neuroinflammation may help mitigate the cascade of events leading to neuronal damage. Vitamin D3 also contributes to neurogenesis and synaptic plasticity, which are important processes for brain plasticity [65].
In the context of MS, vitamin D3 has been investigated for its potential therapeutic effects. Studies have shown that vitamin D3 supplementation may reduce disease activity and demyelination in animal models of MS. Clinical studies have also suggested that vitamin D3 deficiency is associated with an increased risk of developing MS and that supplementation may have beneficial effects on disease progression and activity [66].
In a study on mice with experimental autoimmune encephalomyelitis (EAE), an animal model of MS, early intervention with the active form of vitamin D3 (1,25-dihydroxyvitamin D3) was found to control neuroinflammation and reduce inflammation, demyelination, and oxidative stress. This suggests that vitamin D3 may have potential as an adjunct therapy for MS population [64].
Vitamin D3's role in modulating neuroinflammation and its potential neuroprotective effects make it an interesting target for further research and therapeutic strategies in neurodegenerative and neuropsychiatric disorders. However, more clinical studies are needed to validate these findings and fully understand the mechanisms and benefits of vitamin D3 supplementation in these conditions.
In summary, vitamin D3 plays a role in brain plasticity and has been investigated for its potential therapeutic effects in multiple sclerosis. It has immunomodulatory and neuroprotective properties that may help reduce neuroinflammation and promote neurogenesis and synaptic plasticity. However, further research is needed to fully understand the benefits and mechanisms of vitamin D3 in brain health and disease.
Immunoglobulin Y
Immunoglobulin Y (IgY) is a type of immunoglobulin, or antibody, found in the blood of birds, reptiles, and amphibians. It is the avian equivalent of mammalian immunoglobulin G (IgG). IgY is produced by specialized cells called B lymphocytes in these animals and plays a crucial role in their immune defense against pathogens. One unique characteristic of IgY is that it is actively transported from the bloodstream into the egg yolk during egg formation. As a result, IgY is present in copious quantities in the egg yolk, providing passive immunity to the developing embryo or offspring. This is an evolutionary adaptation that allows birds and reptiles to pass on immune protection to their young before they have fully developed their own immune systems. IgY has gained attention in biomedical research and applications due to its potential as an alternative to mammalian antibodies, such as IgG. It offers several advantages, including ethical considerations (no need for animal bleeding as antibodies are extracted from eggs), cost-effectiveness (production from egg yolks), and potential therapeutic applications. Research on IgY has explored its use in various fields, including immunodiagnostics, immunotherapy, and antimicrobial applications. Studies have investigated its effectiveness in detecting and treating infectious diseases, as well as its potential in modulating immune responses and targeting specific pathogens [67,68].
There is limited research specifically investigating the role of IgY in MS. However, a study mentioned that IgY supplements derived from chicken egg yolk have shown potential in modulating gut microbiota and immune responses and have been effective against various infections [69]. In terms of MS, the study mentioned that clinical trials using IgY supplements in MS are limited but have shown positive outcomes, including reduced symptoms and altered immune responses [69]. However, further research is needed to understand the mechanisms of IgY's interaction with gut microbiota, determine optimal dosage, and assess long-term safety [69].
Homeopathy and Alternative Medicine
Homeopathy is a form of complementary and alternative medicine (CAM) that is sometimes used by people with MS. It is relatively cheap, and some find relief in it. While there is no definitive treatment for MS, management is largely focused on symptom relief. Conventional therapies may not be effective for everyone or may cause unacceptable side effects. As a result, some individuals with MS turn to CAM, including homeopathy, to help manage their symptoms. Homeopathy is a whole-person approach that allows for individualized treatment based on the specific symptoms and needs of the person with MS. It aims to stimulate the body's self-healing mechanisms by administering highly diluted substances that would produce similar symptoms in a healthy person. Homeopathic treatments for MS symptoms such as urinary incontinence, sexual dysfunction, cramps and spasms, tremor, and trigeminal neuralgia have shown some benefit in certain individuals [70,71,72]. However, it is important to note that the evidence supporting the effectiveness of homeopathy in treating MS is limited. Studies on the use of homeopathy in MS have mainly focused on individual cases or small groups of populations, making it difficult to draw definitive conclusions. Additionally, the placebo effect may play a role in the perceived benefits of homeopathic treatments [70,71,72].
Ginkgo Biloba
Ginkgo biloba extract (GBE) is a plant extract derived from the leaves of the Ginkgo biloba tree. It has been used for centuries in traditional medicine and is now commonly consumed as a dietary supplement. The presumed effects of GBE on brain plasticity are based on its potential neuroprotective and neuroregenerative properties. GBE has been shown to have antioxidant and anti-inflammatory effects, which can help protect neurons from damage and promote their survival [74]. It has also been found to enhance cerebral blood flow and improve vascular function, which is important for delivering oxygen and nutrients to the brain [74]. In terms of brain plasticity, GBE has been studied for its effects on synaptic plasticity, which is the ability of synapses to change and adapt in response to experience. Some studies have suggested that ginkgo biloba extract can enhance synaptic plasticity by modulating neurotransmitter pathways and promoting the release of endogenous relaxing factors [74]. These effects may contribute to improved cognitive function and memory.
There is limited evidence on the specific effects of Ginkgo biloba on brain plasticity in MS. However, some studies have investigated the effects of GBE on cognitive function and neuroprotection in MS.
One study evaluated the effects of GBE on cognitive function in individuals with MS and found that treatment with GBE did not improve cognitive performance [75]. Another study investigated the effects of GBE on cognitive performance in MS and found that GBE did not show a statistically significant improvement in cognitive function, except for a trend towards improvement on the Stroop test [76].
While these studies focused on cognitive function, they did not specifically examine brain plasticity. However, GBE has been shown to have neuroprotective effects in various neurological diseases. It has been found to promote myelin generation, regulate the balance of microglia and astrocytes, and induce the generation of oligodendrocyte precursor cells, which are important for remyelination [77]. These effects may indirectly contribute to brain plasticity in MS.
Overall, the evidence on the effects of GBE on brain plasticity in MS is limited. Further research is needed to determine the specific effects of Ginkgo biloba on brain plasticity in individuals with MS.
Alpha Lipoic Acid
Alpha lipoic acid (ALA) is a natural compound with antioxidant and anti-inflammatory properties. It acts as a cofactor for mitochondrial enzymes involved in energy production and has various biological functions, including scavenging reactive oxygen species, regenerating other antioxidants, and modulating signal transduction pathways [78].
In terms of brain plasticity, ALA has been studied for its potential neuroprotective effects after brain injury. Animal studies have shown that ALA can stimulate the synthesis of glutathione, decrease cell death, promote angiogenesis, and reduce the formation of glial scars, which allows for the formation of new neural tissue [79]. These findings suggest that ALA may have a role in promoting brain repair and regeneration after injury.
Regarding MS, ALA has shown promise in preclinical and clinical studies. In animal models of MS, ALA has been found to reduce nerve damage, inhibit the migration of inflammatory cells, and decrease the activity of matrix metalloproteinases, which are involved in the breakdown of the blood-brain barrier [80]. Clinical trials have demonstrated positive effects of ALA on cellular and physical outcomes in people with MS. However, more research is needed to determine the effectiveness of ALA as a therapy for MS, and it is not currently approved for this purpose [80].
In summary, ALA has potential roles in brain plasticity by promoting neuroprotection and repair after injury. In the context of multiple sclerosis, ALA has shown promising effects in preclinical and clinical studies, but further research is needed to establish its efficacy as a therapy for MS.
Biotin
Biotin, also known as vitamin B7 or vitamin H, is a water-soluble vitamin that plays a crucial role in various metabolic processes in the body. It acts as a cofactor for several carboxylase enzymes involved in energy production, fatty acid synthesis, and amino acid metabolism.
In the context of MS, there is growing interest in the potential role of high-dose biotin in preventing brain neurodegeneration.
Several studies have investigated the effects of high-dose biotin (MD1003) in populations with progressive MS. These studies have shown promising results, suggesting that biotin may have a beneficial effect on disease progression and disability improvement [4,81,82,83]. The exact mechanisms by which biotin exerts its neuroprotective effects are not fully understood, but several hypotheses have been proposed.
It is important to note that while some studies have shown positive effects of high-dose biotin in MS, not all studies have reported significant benefits [84].
Further research is needed to fully understand the potential role of biotin in preventing brain neurodegeneration in MS and to determine the optimal dosage and treatment duration.
In summary, biotin is a vitamin that plays a role in various metabolic processes in the body. High-dose biotin has shown promise in preventing brain neurodegeneration in multiple sclerosis, potentially through its effects on energy production and myelin synthesis. However, more research is needed to confirm these findings and determine the optimal use of biotin in MS treatment.
Flavonoids
Flavonoids are a large group of plant polyphenols that are widely distributed in the human diet. They are found in various fruits, vegetables, nuts, and beverages. Flavonoids have been studied for their potential health benefits and are believed to have several presumed effects in the human body. Flavonoids can reduce free radical formation and scavenge free radicals, which can help protect cells from oxidative damage [85]. They can also increase the plasma antioxidant status and preserve the levels of antioxidants like vitamin E [85]. Flavonoids have been shown to possess anti-inflammatory effects. They can modulate intracellular signaling cascades and inhibit enzymes involved in cellular activation, leading to a reduction in inflammation [86]. Flavonoids have been associated with a lower risk of cardiovascular diseases. They have been shown to have vasodilating actions, reduce lipid peroxidation, and protect against oxidative stress, which are all beneficial for heart health [87]. Flavonoids have immunomodulatory properties and can influence immune responses. They have been reported to possess anti-allergenic and anti-viral activities [85]. Flavonoids have been studied for their pro-cognitive effects. They can interact with major signal transduction cascades in the brain and impact transcription factors involved in neuronal function [88].
It's important to note that the effects of flavonoids can vary depending on their specific chemical structure and concentration. Further research is needed to fully understand the mechanisms of action and potential health benefits of different flavonoids [89].
There is limited direct evidence on the effects of flavonoids on brain plasticity specifically in MS. However, flavonoids have been shown to have neuroprotective and neuroplasticity-promoting effects in various neurological conditions.
- Flavonoids have been found to exert neuroprotective effects by reducing oxidative stress and inflammation, which are key factors in MS [90,91]. They have also been shown to promote synaptogenesis and neurogenesis, which are important processes for brain plasticity [90]. Additionally, flavonoids have been found to modulate signaling pathways involved in neuronal survival and synaptic plasticity [92,93].
- In animal models of MS, flavonoids have demonstrated positive therapeutic effects. For example, flavonoid luteolin has been shown to suppress clinical symptoms, reduce inflammation, and prevent relapse in rats with EAE [94]. A systematic review of studies on EAE and MS also reported positive outcomes for the therapeutic effect of flavonoids on these conditions [95].
While the direct effects of flavonoids on brain plasticity in MS are not well-studied, their neuroprotective and neuroplasticity-promoting properties suggest that they may have potential benefits for enhancing brain plasticity in MS. Further research is needed to explore the specific effects of flavonoids on brain plasticity in MS and to determine optimal dosages and treatment strategies [90,91,92,95].
Polyunsaturated Fatty Acids
Polyunsaturated fatty acids (PUFA) are a type of fat that is essential for human health and cannot be produced by the body, so they must be obtained through diet. PUFA can be further classified into two main groups: omega-3 (n-3) and omega-6 (n-6) fatty acids.
The presumed effects of PUFA in humans are diverse and have been extensively studied. PUFA, particularly omega-3 fatty acids, have been associated with a reduced risk of cardiovascular diseases. They can help lower blood triglyceride levels, reduce inflammation, improve blood vessel function, and prevent the formation of blood clots. Omega-3 fatty acids, especially docosahexaenoic acid (DHA), play a crucial role in brain development and function. They are important for cognitive function, memory, and mood regulation. Adequate intake of omega-3 fatty acids has been linked to a lower risk of neurodegenerative diseases and improved mental health. They also provide anti-inflammatory properties. They can help reduce chronic inflammation in the body and modulate immune responses. This can be beneficial for conditions such as rheumatoid arthritis, inflammatory bowel disease, and asthma. Some studies suggest that omega-3 fatty acids may have a protective effect against certain types of cancer, such as breast, colorectal, and prostate cancer. However, more research is needed to fully understand the relationship between PUFA and cancer prevention. PUFA can influence metabolic processes, including lipid metabolism, insulin sensitivity, and glucose regulation. They may help improve insulin resistance, reduce the risk of type 2 diabetes, and prevent fatty liver disease.
It's important to note that the effects of PUFA can vary depending on the specific type and ratio of omega-3 to omega-6 fatty acids consumed, as well as individual factors such as genetics, overall diet, and health status. Therefore, it is recommended to maintain a balanced intake of both omega-3 and omega-6 fatty acids for optimal health benefits [96,97,98,99,100,101,102,103].
The effects of PUFA on brain plasticity in MS population have been investigated in several studies. Their main effects can be concluded in:
- A study on mice with induced CNS demyelination found that an increased n-3 PUFA status promoted remyelination after toxic injury to CNS oligodendrocytes. This effect may be mediated by n-3 PUFA-derived lipid metabolites [104].
- Omega-3 PUFAs, such as docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA), have been shown to modulate microglial responses to myelin pathology. They can inhibit inflammation while enhancing beneficial immune responses, such as microglial phagocytosis. In a mouse model of MS, n-3 PUFA supplementation reduced demyelination and shifted microglial polarization towards a beneficial phenotype [105].
- In vitro studies using oligodendroglia cells and primary oligodendrocytes have shown that supplementation with n-3 and n-6 PUFAs can promote oligodendrocyte differentiation. This was evidenced by increased expression of markers of oligodendroglia differentiation and enhanced myelin sheet formation [106].
- A study on healthy older adults found that omega-3 PUFAs were associated with individual differences in functional brain connectivity. Specifically, they were linked to connectivity within regions supporting executive function, memory, and emotion. These regions were also found to predict general, fluid, and crystallized intelligence [107].
It's important to note that while these studies provide insights into the potential effects of PUFA on brain plasticity in MS populations, more research is needed to fully understand the mechanisms and clinical implications. Additionally, the optimal dosage and duration of PUFA supplementation for MS populations are still being explored.
Curcumin
Curcumin is a natural compound found in turmeric, which is a spice commonly used in cooking. It has been extensively studied for its potential health benefits. Curcumin is known for its antioxidant, anti-inflammatory, and anticancer properties. It has been shown to have diverse pharmacological effects, including neuroprotective, cardioprotective, and immunomodulatory activities. Curcumin has been investigated for its potential in the prevention and treatment of various diseases, such as cancer, cardiovascular diseases, diabetes, arthritis, neurological diseases, and gastrointestinal disorders. However, curcumin's low bioavailability has been a challenge in harnessing its full therapeutic potential [108,109,110,111,112,113].
There is limited research specifically investigating the effect of curcumin on brain plasticity in MS populations. However, curcumin has been shown to have beneficial effects on brain health through various mechanisms, including its antioxidant, anti-inflammatory, and neuroprotective properties. These effects may potentially contribute to the modulation of brain plasticity in MS populations. Curcumin has been studied in animal models of MS, where it has demonstrated neuroprotective effects, reduced demyelination, and improved cognitive function. Further research is needed to determine the specific impact of curcumin on brain plasticity in MS populations [114,115,116].
Resveratrol
Resveratrol is a natural compound found in various plants, including grapes, berries, peanuts, and red wine. It is a polyphenol with antioxidant, anti-inflammatory, and anti-cancer properties. Resveratrol has been studied for its potential health benefits in several areas. Resveratrol may have cardioprotective effects by improving inflammatory markers, atherogenic profile, glucose metabolism, and endothelial function [117,118]. It has shown promising results in preventing or delaying the development of various types of cancer, including prostate cancer by inhibiting proliferation, promoting apoptosis, and enhancing sensitivity to radiation [119]. Also, it has been investigated for its potential in neurodegenerative diseases such as Alzheimer's Disease (AD), Parkinson's Disease (PD), and Huntington's disease (HD). It has shown effects in in vitro models, but further research is needed [120]. Resveratrol has been associated with improved insulin sensitivity, increased energy expenditure, and a decrease in body fat [121]. It may also have anti-obesity effects by inhibiting adipogenesis and increasing lipid mobilization [122]. Also, it has been shown to reduce inflammation and oxidative stress in various tissues and organs [118]. It may also have anti-angiogenic effects [119].
It's important to note that while resveratrol has shown promising results in preclinical studies and some clinical trials, there is still a need for more research, especially in human subjects, to fully understand its effects and determine optimal doses [123,124]. Additionally, the bioavailability of resveratrol and its potential interactions with medications should be considered [122].
There is limited research specifically investigating the effects of resveratrol on brain plasticity in MS populations. In an EAE mouse model of MS, resveratrol treatment was found to improve clinical outcomes and protect against optic nerve and spinal cord degeneration [125]. Another study in cuprizone-intoxicated mice, a model of demyelination/remyelination like MS, showed that resveratrol enhanced motor coordination, reversed demyelination, and increased the expression of genes associated with active remyelination [126].
While these studies suggest potential neuroprotective effects of resveratrol in MS models, it is important to note that the effects of resveratrol on brain plasticity in human MS populations have not been extensively studied. Further research is needed to determine the specific effects of resveratrol on brain plasticity in MS populations and its potential as a therapeutic intervention for MS-related neurodegenerative processes [125].
Terpenoids
Terpenoids are a class of naturally occurring compounds that are derived from terpenes. They are found in various plants, animals, and microorganisms. Terpenoids have diverse biological activities and are known for their pharmacological effects on the human body.
Terpenoids have been studied for their potential therapeutic benefits in various chronic illnesses. They have been found to have anti-inflammatory, antimicrobial, antifungal, antiviral, antitumor, and antioxidant properties [127,128,129,130,131,132,133,134]. They can also act as skin penetration enhancers and have been used in the prevention and treatment of inflammatory diseases [129]. In the context of specific diseases, terpenoids have shown promise in the treatment of non-alcoholic fatty liver disease. They regulate lipid metabolism disorder, insulin resistance, oxidative stress, and inflammation, and target pathways such as AMPK, PPARs, Nrf-2, and SIRT 1 [127]. Additionally, terpenoids have been explored for their potential antiviral efficacy against SARS-CoV-2, the virus responsible for COVID-19 [15].
Furthermore, terpenoids have been investigated for their effects on psychiatric disorders. Preclinical studies have demonstrated their neuropharmacological effects and their potential as alternative therapeutic options for psychiatric disorders [131].
Two studies provide insights into the effects of terpenoids on brain plasticity in MS populations. In a study by Tomassini et al., it was found that inflammation in MS interferes with brain plasticity [135]. However, pharmacological reduction of inflammation, such as with Interferon beta treatment, can restore brain plasticity. The study used a visuomotor adaptation task and functional MRI to assess brain plasticity in MS populations. The results showed that reduced inflammation with IFN beta treatment led to a restoration of brain plasticity, suggesting that modulation of inflammation can enhance recovery-oriented strategies that rely on brain plasticity. Similarly, Shin et al. investigated the effects of terpenes on neuronal health in Drosophila AD models. They found that certain terpenes, including limonene, had neuroprotective effects against the neurotoxicity of beta amyloid 42 (Aβ42), a protein associated with AD. Limonene treatment decreased cell death, inflammation, and oxidative stress in the brains of the AD model flies. While this study was not conducted specifically in MS populations, it provides insights into the potential neuroprotective effects of terpenes on brain health [130].
These findings suggest that terpenoids, including terpenes like limonene, may have the potential to modulate brain plasticity in MS populations by reducing inflammation, promoting neuroprotection, and enhancing recovery processes. However, it is important to note that these studies were conducted in animal models and further research is needed to determine the specific effects of terpenoids on brain plasticity in MS populations.
Polyphenols
Polyphenols are a group of natural compounds found in a variety of plant-based foods, such as fruits, vegetables, nuts, seeds, whole grains, tea, coffee, and red wine. They are characterized by the presence of phenol structural units and are known for their antioxidant properties. The presumed effects of polyphenols in the human body are diverse and have been the subject of extensive research. Some of their potential benefits include:
- Polyphenols can scavenge and neutralize harmful free radicals, reducing oxidative stress and protecting cells from damage [136].
- Polyphenols have been investigated for their potential anti-carcinogenic effects. They may inhibit tumor growth, induce apoptosis in cancer cells, and have anti-mutagenic properties [140].
- Some polyphenols, such as resveratrol and epigallocatechin-3-gallate, have shown promise in protecting against neurodegenerative disorders by reducing mitochondrial dysfunction and oxidative stress [141].
There is evidence that the use of plant polyphenols may have beneficial effects on brain plasticity in MS. For example, grape seed extract has been shown to have neuroprotective properties and can improve brain plasticity in an EAE mouse model of MS. GSE treatment in EAE mice resulted in the correction of oxidative stress damage, restoration of antioxidant capacities, normalization of myelin protein expression, and modulation of astroglial and microglial proliferation. These effects suggest that GSE may have a positive impact on brain plasticity in MS [142].
Sulphur-Containing Compounds
Sulphur-containing compounds play important roles in the human body and have various effects. Methionine, cysteine, homocysteine, and taurine are sulfur-containing amino acids. They are essential for protein synthesis and are involved in antioxidant defense mechanisms. They contribute to the synthesis of intracellular antioxidants like glutathione, which helps protect cells from oxidative damage [143].
Glutathione and N-acetylcysteine are derivatives of sulfur-containing amino acids and act as powerful antioxidants. They help neutralize free radicals and protect cells from oxidative stress. They are also used in chelation therapy to eliminate toxic metals from the body [143]. Naturally occurring sulfur-containing ligands can act as detoxifying agents, preventing the toxic effects of heavy and transition metal ions and aiding in their elimination from the body [143]. Exposure to malodorous sulfur compounds has been associated with respiratory symptoms such as cough, respiratory infections, and nasal symptoms. Reduction in sulfur compound exposure has been shown to decrease the frequency of these symptoms [144,145]. Some sulfur compounds, such as diallyl sulfide and diallyl disulfide, have immunomodulatory effects. They can enhance white blood cell count, antibody production, and bone marrow cellularity, suggesting potential immunostimulant effects [146]. Sulphur-containing antioxidants, such as N-acetylcysteine and lipoic acid, have been shown to reduce oxidative stress induced by substances like lead. They can help protect against oxidative damage and maintain cellular health [147].
One study investigated the therapeutic effects of hydrogen sulfide (H2S) in a cuprizone-induced MS model in mice. The study found that treatment with a hydrogen sulfide donor improved locomotor coordination, reduced neuronal inflammation and demyelination, and decreased oxidative stress in the brain. These effects were associated with the downregulation of miR-146a expression and the regulation of the miR-146a/NF-κB/IL-1β axis [148].
Another study examined the effects of sulfur dioxide exposure on synaptic plasticity in the hippocampus of rats. The study found that exposure to SO2 at different concentrations and durations resulted in the inhibition of synaptic plasticity markers and memory-related proteins in the hippocampus. The effects of SO2 on synaptic plasticity were dependent on the duration and concentration of exposure [149].
While these studies provide insights into the effects of sulfur compounds on brain plasticity in MS-related models, further research is needed to fully understand the mechanisms and potential therapeutic applications of sulfur compounds in MS.
Several dietary nutraceuticals have been tested in MS; while some have potential to aid the process of neuroregeneration, some still need research. A summary of the key current knowledge is found in Table 2.
Obesity
Obesity is considered both a risk for MS development and the progression of the disease [150,151]. Obesity is a medical condition characterized by excessive accumulation of body fat, which can have negative effects on health. Obesity is defined using the body mass index (BMI), which is calculated by dividing a person's weight in kilograms by the square of their height in meters. A BMI of 30 or higher equals obesity. The prevalence of obesity varies across different populations and countries. In developed countries, such as the United States, Europe, and Australia, the average prevalence of obesity is estimated to be around 15-20% [152]. However, there are significant variations within and between countries.
A study conducted in the Nurses' Health Study and Nurses' Health Study II found that obesity at age 18 was associated with a more than twofold increased risk of MS [150] . Another study using Mendelian randomization analysis found that genetically BMI was associated with a 41% increased risk of MS [153]. Furthermore, a meta-analysis of observational studies reported that excess body weight during childhood and adolescence increased the risk of MS, particularly in females [154]. Another study found that obese adolescents had a higher risk of developing MS compared to non-obese individuals, even after adjusting for other factors [155,156]. Another study found that a common polymorphism in the fat-mass obesity gene, associated with obesity, was linked to being overweight/obese in MS populations [157].
In terms of disease progression, a study showed that overweight or obese MS populations had higher MRI activity and were less likely to achieve no evidence of disease activity status compared to normal-weight populations [158]. Additionally, obesity was associated with a higher risk of disability accumulation in MS populations [159].The mechanisms underlying the association between obesity and MS that were suggested are chronic inflammation, altered gut microbiota, and vitamin D deficiency [160,161].
In conclusion, obesity, particularly during adolescence and early adulthood, is associated with an increased risk of developing MS and may also impact disease progression and disability accumulation. Obesity prevention in adolescence may reduce the risk of developing MS [155,156,162,163].
Obesity has been found to have an impact on brain plasticity. A study conducted on adult volunteers with a wide range of BMI found that the effect of short-term monocular deprivation, a measure of early visual plasticity, decreased with increasing BMI. Morbidly obese individuals also showed altered binocular rivalry dynamics compared to normal-weight individuals, indicating impaired sensory processing and plasticity [164,165].
Another study investigated the plasticity of the motor cortex in obese individuals compared to those with a healthy weight. It found that obese individuals had an impaired capacity for plasticity in the motor cortex, as measured by the suppression of cortical excitability following brain stimulation. This suggests that the ability of the motor cortex to change and adapt is reduced in obesity [166].
Furthermore, obesity has been associated with alterations in synaptic plasticity in the hippocampus, a brain region involved in learning and memory. Studies have shown that obese individuals, particularly males, exhibit deficits in hippocampal synaptic plasticity, which may contribute to cognitive impairments [167].
The underlying mechanisms linking obesity and impaired brain plasticity are not fully understood. However, factors such as chronic inflammation, oxidative stress, altered gut-brain hormonal functionality, and insulin resistance have been proposed as potential contributors [167,168].
Obese populations with MS may experience neurodegeneration through several mechanisms, as shown in the following image (Figure 4):
- Obesity and high-calorie diets are associated with disturbances in gut microbiota. Emerging evidence suggests that gut dysbiosis may play a role in the development and progression of MS. Altered gut microbiota can influence immune responses and neuroinflammation, contributing to neurodegeneration in obese MS populations [161,173].
- Obesity is characterized by insulin and leptin resistance, which can impair neuroprotective signaling pathways. Insulin and leptin resistance may weaken the protective effects of these molecules in the CNS, leading to increased neurodegeneration in MS [174].
Fighting against obesity is hard for all populations, and nevertheless for MS populations. Some possibilities include:
Regular exercise is crucial for weight management and overall health. The American College of Sports Medicine recommends between 150-250 minutes per week of moderate-intensity physical activity for preventing weight gain and between 225-420 minutes per week for weight loss in people with MS [175].
When designing exercise programs for individuals with MS, it is important to consider their specific needs and limitations. Exercise programs should exceed energy expenditure recommendations to effectively counteract weight gain [175].
- Intermittent fasting has shown beneficial effects on weight loss and lipid profile in people with obesity and type 2 diabetes. Although limited data is available for its effects on MS, intermittent fasting may be a safe and feasible intervention for individuals with MS [180].
- Tailored dietary change strategies, nutrition education, and counseling can play a significant role in managing metabolic comorbidities in MS. Addressing barriers and facilitators to dietary changes through behavior change techniques can help individuals achieve sustainable and tailored dietary behavior changes [181].
Obesity, particularly during adolescence and early adulthood, significantly increases the risk of developing MS and worsens disease progression and disability accumulation. Studies have identified mechanisms such as chronic inflammation, altered gut microbiota, and vitamin D deficiency that link obesity with MS. Additionally, obesity impairs brain plasticity, affecting sensory processing, motor cortex adaptability, and hippocampal synaptic plasticity, which may contribute to cognitive impairments. Obesity-induced chronic inflammation, adipokine dysregulation, blood-brain barrier permeability, and insulin resistance exacerbate neurodegeneration in MS populations. Effective management strategies include regular exercise, behavioural weight loss interventions, bariatric surgery, intermittent fasting, and tailored dietary changes, which can help mitigate obesity's impact on MS progression and overall health.
Conclusions
MS presents a complex interplay of immune-mediated pathology, characterized by inflammation, demyelination, and neurodegeneration. The CNS undergoes significant changes due to the disease's progression, leading to varied symptoms and disability levels among populations [1,2,3,4,5,6,7]. Enhancing brain plasticity offers a promising avenue for mitigating these effects and improving population outcomes [21,22,23].
Brain plasticity, the capacity of the brain to reorganize its structure and function, is vital for learning, memory, and recovery from injuries. In the context of MS, promoting brain plasticity can help counteract the neurological damage caused by the disease. Several mechanisms underpin brain plasticity, including synaptic modification, neurogenesis, and the activation of complex signalling pathways that support neuronal connectivity and survival [26,27,28].
Physical exercise is a potent modulator of brain plasticity. Aerobic exercise, resistance training, and even simple activities like walking have been shown to enhance synaptic plasticity, neurogenesis, and cognitive functions [29,30]. The increased production of BDNF is one key mechanism through which physical activity exerts its beneficial effects. BDNF supports the survival of existing neurons and encourages the growth and differentiation of new neurons and synapses [31,32].
Diet plays a crucial role in modulating brain health. Caloric restriction and intermittent fasting have been associated with increased expression of neurotrophic factors and enhanced synaptic function [175–181]. Additionally, specific nutrients, such as omega-3 fatty acids found in fish oil, have anti-inflammatory properties that can help reduce CNS inflammation and promote brain plasticity [96,97,98,99,100,101,102,103,104,105,106,107,108]. Polyphenols, present in foods like dark chocolate and certain fruits, also contribute to neuroprotection and cognitive enhancement [117,118,119].
Obesity is a known risk factor for MS progression. Controlling body weight through diet and exercise can reduce inflammation and oxidative stress, thereby supporting brain plasticity. Nutraceuticals like ALA and resveratrol have been shown to reduce oxidative damage and support metabolic homeostasis, further aiding in the control of obesity-related impacts on brain health [150–180].
Nutraceuticals are bioactive compounds that provide health benefits beyond basic nutrition. They play a significant role in supporting brain plasticity and overall brain health in MS populations.
Vitamin D3 has immunomodulatory and neuroprotective effects. It influences the production of pro-inflammatory cytokines and antioxidants, aiding in the reduction of neuroinflammation and promoting neurogenesis and synaptic plasticity. Studies have shown that vitamin D3 supplementation can reduce disease activity and progression in MS [64,65,66].
Omega-3 fatty acids, particularly DHA, have been shown to support brain plasticity by modulating synaptic function and promoting neurogenesis. They also have anti-inflammatory properties that can help mitigate CNS inflammation in MS populations [96,97,98,99,100,101,102,103,104,105,106,107].
Antioxidants like ALA and flavonoids found in green tea and dark chocolate can scavenge free radicals, reducing oxidative stress and supporting neuroprotection. These compounds have shown potential in improving clinical outcomes in MS, including reducing fatigue and supporting cognitive functions [78,79,80].
GBE has been reported to improve cognitive functions and reduce fatigue in MS populations. Its antioxidant capacity supports brain plasticity by protecting neurons from oxidative damage and enhancing synaptic function [74,75,76,77].
Integrating lifestyle changes and nutraceuticals into the management of MS provides a holistic approach that complements traditional pharmacological treatments. By addressing modifiable risk factors and supporting brain plasticity, populations can experience improved neurological outcomes and quality of life. Regular physical activity, a balanced diet rich in neuroprotective nutrients, and the strategic use of nutraceuticals can form a comprehensive strategy for managing MS [170–180].
Future research should focus on the long-term effects of these lifestyle modifications and nutraceuticals on brain plasticity and MS progression. Large-scale, randomized controlled trials are needed to establish definitive evidence and provide clear guidelines for clinicians. Understanding the individual variability in response to these interventions can also help tailor personalized treatment plans for MS populations.
In conclusion, the synergistic effects of lifestyle changes and nutraceuticals hold great promise for enhancing brain plasticity and improving the lives of those living with MS. By adopting these strategies, populations can take an active role in managing their condition and optimizing their neurological health.
Abbreviation list
AD = Alzheimer’s disease; ALA = alpha lipoic acid; BDNF = Brain derived neurotrophic factor; CAM = Complementary and alternative medicine; CIS = Clinically isolated syndrome; CNS = Central nervous system; CSF = Cerebrospinal fluid; DHA = docosahexaenoic acid; DIS = Dissemination in Space; DIT = Dissemination in Time; EBV = Epstein-Barr virus; EAE = Experimental autoimmune encephalomyelitis; EPA = eicosapentaenoic acid; GBE = Ginkgo biloba extract; HD = Huntington’s disease; MS = Multiple sclerosis; OCBs = Oligoclonal bands; PD = Parkinson’s disease; PPMS = Primary progressive multiple sclerosis; PUFA = Polyunsaturated fatty acids; RRMS = Relapsing-remitting multiple sclerosis; SPMS = Secondary progressive multiple sclerosis; tPA = tissue-type plasminogen activator.
References
- Ward, M., & Goldman, M. D. (2022). Epidemiology and Pathophysiology of Multiple Sclerosis. Continuum (Minneapolis, Minn.), 28(4), 988–1005. https://doi.org/10.1212/CON.0000000000001136 Weiner HL. Multiple sclerosis is an inflammatory T-cell-mediated autoimmune disease. Arch Neurol. 2004 Oct;61(10):1613–5. [CrossRef]
- Dendrou CA, Fugger L, Friese MA. Immunopathology of multiple sclerosis. Nat Rev Immunol. 2015 Sep;15(9):545–58. [CrossRef]
- Cree BAC, Gourraud P-A, Oksenberg JR, Bevan C, Crabtree-Hartman E, Gelfand JM, et al. Long-term evolution of multiple sclerosis disability in the treatment era. Ann Neurol. 2016 Oct;80(4):499–510.
- Tarlinton RE, Martynova E, Rizvanov AA, Khaiboullina S, Verma S. Role of Viruses in the Pathogenesis of Multiple Sclerosis. Viruses. 2020 Jun;12(6). [CrossRef]
- Vattoth S, Kadam GH, Gaddikeri S. Revised McDonald Criteria, MAGNIMS Consensus and Other Relevant Guidelines for Diagnosis and Follow Up of MS: What Radiologists Need to Know? Curr Probl Diagn Radiol. 2021 May-Jun;50(3):389-400. doi: 10.1067/j.cpradiol.2020.06.006. Epub 2020 Jun 29. PMID: 32665060.Noyes K, Weinstock-Guttman B. Impact of diagnosis and early treatment on the course of multiple sclerosis. Am J Manag Care. 2013 Nov;19(17 Suppl):s321-31. [CrossRef]
- Marrie RA, Reider N, Cohen J, Stuve O, Sorensen PS, Cutter G, et al. A systematic review of the incidence and prevalence of autoimmune disease in multiple sclerosis. Mult Scler. 2015 Mar;21(3):282–93. [CrossRef]
- Nielsen NM, Westergaard T, Frisch M, Rostgaard K, Wohlfahrt J, Koch-Henriksen N, et al. Type 1 diabetes and multiple sclerosis: A Danish population-based cohort study. Arch Neurol. 2006 Jul;63(7):1001–4.
- Gupta G, Gelfand JM, Lewis JD. Increased risk for demyelinating diseases in populations with inflammatory bowel disease. Gastroenterology. 2005 Sep;129(3):819–26.
- Goris A, Vandebergh M, McCauley JL, Saarela J, Cotsapas C. Genetics of multiple sclerosis: lessons from polygenicity. Lancet Neurol. 2022 Sep;21(9):830–42. [CrossRef]
- Barac IS, Iancu M, Văcăraș V, Cozma A, Negrean V, Sâmpelean D, et al. Potential Contribution of IL-27 and IL-23 Gene Polymorphisms to Multiple Sclerosis Susceptibility: An Association Analysis at Genotype and Haplotype Level. J Clin Med. 2021 Dec;11(1). [CrossRef]
- Vacaras V, Paraschiv A-C, Iluț S, Vacaras C, Nistor C, Marin G-E, et al. Brain-Derived Neurotrophic Factor in Multiple Sclerosis Disability: A Prospective Study. Brain Sci. 2024 Feb;14(3). [CrossRef]
- Cusick MF, Libbey JE, Fujinami RS. Multiple sclerosis: Autoimmunity and viruses. Curr Opin Rheumatol. 2013;25(4):496–501.
- Taan M, Al Ahmad F, Ercksousi MK, Hamza G. Risk Factors Associated with Multiple Sclerosis: A Case-Control Study in Damascus, Syria. Mult Scler Int. 2021;2021:8147451. [CrossRef]
- Jacobs BM, Giovannoni G, Cuzick J, Dobson R. Systematic review and meta-analysis of the association between Epstein-Barr virus, multiple sclerosis and other risk factors. Mult Scler. 2020 Oct;26(11):1281–97.
- Xu Y, Smith KA, Hiyoshi A, Piehl F, Olsson T, Montgomery S. Hospital-diagnosed infections before age 20 and risk of a subsequent multiple sclerosis diagnosis. Brain. 2021 Sep;144(8):2390–400. [CrossRef]
- Jacobs BM, Noyce AJ, Giovannoni G, Dobson R. BMI and low vitamin D are causal factors for multiple sclerosis: A Mendelian Randomization study. Neurol Neuroimmunol neuroinflammation. 2020 Mar;7(2).
- Manouchehrinia A, Tench CR, Maxted J, Bibani RH, Britton J, Constantinescu CS. Tobacco smoking and disability progression in multiple sclerosis: United Kingdom cohort study. Brain. 2013 Jul;136(Pt 7):2298–304. [CrossRef]
- Ramanujam R, Hedström A-K, Manouchehrinia A, Alfredsson L, Olsson T, Bottai M, et al. Effect of Smoking Cessation on Multiple Sclerosis Prognosis. JAMA Neurol. 2015 Oct;72(10):1117–23. [CrossRef]
- Sale A, Berardi N, Maffei L. Environment and brain plasticity: towards an endogenous pharmacotherapy. Physiol Rev. 2014 Jan;94(1):189–234. [CrossRef]
- Chandler LJ. Ethanol and brain plasticity: receptors and molecular networks of the postsynaptic density as targets of ethanol. Pharmacol Ther. 2003 Sep;99(3):311–26. [CrossRef]
- Kolb B, Whishaw IQ. Brain plasticity and behavior. Annu Rev Psychol. 1998;49:43–64. [CrossRef]
- Pascual-Leone A, Freitas C, Oberman L, Horvath JC, Halko M, Eldaief M, et al. Characterizing brain cortical plasticity and network dynamics across the age-span in health and disease with TMS-EEG and TMS-fMRI. Brain Topogr. 2011 Oct;24(3–4):302–15.
- Missitzi J, Gentner R, Geladas N, Politis P, Karandreas N, Classen J, et al. Plasticity in human motor cortex is in part genetically determined. J Physiol. 2011 Jan;589(Pt 2):297–306. [CrossRef]
- Tzounopoulos T, Kraus N. Learning to encode timing: mechanisms of plasticity in the auditory brainstem. Neuron. 2009 May;62(4):463–9. [CrossRef]
- Travaglia A, Bisaz R, Cruz E, Alberini CM. Developmental changes in plasticity, synaptic, glia and connectivity protein levels in rat dorsal hippocampus. Neurobiol Learn Mem. 2016 Nov;135:125–38. [CrossRef]
- Johnston M V. Plasticity in the developing brain: implications for rehabilitation. Dev Disabil Res Rev. 2009;15(2):94–101. [CrossRef]
- Strettoi E, Di Marco B, Orsini N, Napoli D. Retinal Plasticity. Int J Mol Sci. 2022 Jan;23(3).
- Pearson-Fuhrhop KM, Kleim JA, Cramer SC. Brain plasticity and genetic factors. Top Stroke Rehabil. 2009;16(4):282–99. [CrossRef]
- Ding Q, Ying Z, Gómez-Pinilla F. Exercise influences hippocampal plasticity by modulating brain-derived neurotrophic factor processing. Neuroscience. 2011 Sep;192:773–80. [CrossRef]
- Ben-Zeev T, Shoenfeld Y, Hoffman JR. The Effect of Exercise on Neurogenesis in the Brain. Isr Med Assoc J. 2022 Aug;24(8):533–8.
- Smith AE, Goldsworthy MR, Garside T, Wood FM, Ridding MC. The influence of a single bout of aerobic exercise on short-interval intracortical excitability. Exp brain Res. 2014 Jun;232(6):1875–82. [CrossRef]
- Dishman RK, Berthoud H-R, Booth FW, Cotman CW, Edgerton VR, Fleshner MR, et al. Neurobiology of exercise. Obesity (Silver Spring). 2006 Mar;14(3):345–56.
- Achiron A, Kalron A. [Physical activity: positive impact on brain plasticity]. Harefuah. 2008 Mar;147(3):252-255,276.
- Cirillo J, Lavender AP, Ridding MC, Semmler JG. Motor cortex plasticity induced by paired associative stimulation is enhanced in physically active individuals. J Physiol. 2009 Dec;587(Pt 24):5831–42. [CrossRef]
- Mori F, Kusayanagi H, Buttari F, Centini B, Monteleone F, Nicoletti CG, et al. Early treatment with high-dose interferon beta-1a reverses cognitive and cortical plasticity deficits in multiple sclerosis. Funct Neurol. 2012;27(3):163–8.
- Parry AMM, Scott RB, Palace J, Smith S, Matthews PM. Potentially adaptive functional changes in cognitive processing for populations with multiple sclerosis and their acute modulation by rivastigmine. Brain. 2003 Dec;126(Pt 12):2750–60.
- Murphy T, Dias GP, Thuret S. Effects of diet on brain plasticity in animal and human studies: mind the gap. Neural Plast. 2014;2014:563160. [CrossRef]
- Gomez-Pinilla F, Ying Z. Differential effects of exercise and dietary docosahexaenoic acid on molecular systems associated with control of allostasis in the hypothalamus and hippocampus. Neuroscience. 2010 Jun;168(1):130–7. [CrossRef]
- Xu B-L, Wang R, Ma L-N, Dong W, Zhao Z-W, Zhang J-S, et al. Effects of Caloric Intake on Learning and Memory Function in Juvenile C57BL/6J Mice. Biomed Res Int. 2015;2015:759803. [CrossRef]
- Kalantarzadeh E, Radahmadi M, Reisi P. The impact of different dark chocolate dietary patterns on synaptic potency and plasticity in the hippocampal CA1 area of the rats under chronic isolation stress. Nutr Neurosci. 2023 Aug;26(8):756–65. [CrossRef]
- Libner CD, Salapa HE, Levin MC. The Potential Contribution of Dysfunctional RNA-Binding Proteins to the Pathogenesis of Neurodegeneration in Multiple Sclerosis and Relevant Models. Int J Mol Sci. 2020 Jun;21(13). [CrossRef]
- Dong Y, D’Mello C, Pinsky W, Lozinski BM, Kaushik DK, Ghorbani S, et al. Oxidized phosphatidylcholines found in multiple sclerosis lesions mediate neurodegeneration and are neutralized by microglia. Nat Neurosci. 2021 Apr;24(4):489–503. [CrossRef]
- Gonsette RE. Neurodegeneration in multiple sclerosis: the role of oxidative stress and excitotoxicity. J Neurol Sci. 2008 Nov;274(1–2):48–53. [CrossRef]
- Vyshkina T, Kalman B. Autoantibodies and neurodegeneration in multiple sclerosis. Lab Invest. 2008 Aug;88(8):796–807. [CrossRef]
- Kalman B, Leist TP. A mitochondrial component of neurodegeneration in multiple sclerosis. Neuromolecular Med. 2003;3(3):147–58. [CrossRef]
- Mahad DH, Trapp BD, Lassmann H. Pathological mechanisms in progressive multiple sclerosis. Lancet Neurol. 2015 Feb;14(2):183–93. [CrossRef]
- Barnett MH, Mathey E, Kiernan MC, Pollard JD. Axonal damage in central and peripheral nervous system inflammatory demyelinating diseases: common and divergent pathways of tissue damage. Curr Opin Neurol. 2016 Jun;29(3):213–21.
- Zoupi L, Booker SA, Eigel D, Werner C, Kind PC, Spires-Jones TL, et al. Selective vulnerability of inhibitory networks in multiple sclerosis. Acta Neuropathol. 2021 Mar;141(3):415–29. [CrossRef]
- Chapman C, Lucas RM, Ponsonby A-L, Taylor B. Predictors of progression from a first demyelinating event to clinically definite multiple sclerosis. Brain Commun. 2022;4(4):fcac181. [CrossRef]
- Alroughani RA, Akhtar S, Ahmed SF, Al-Hashel JY. Clinical predictors of disease progression in multiple sclerosis populations with relapsing onset in a nation-wide cohort. Int J Neurosci. 2015;125(11):831–7.
- Simmons SB, Schippling S, Giovannoni G, Ontaneda D. Predicting disability worsening in relapsing and progressive multiple sclerosis. Curr Opin Neurol. 2021 Jun;34(3):312–21. [CrossRef]
- Motl RW, Dlugonski D, Pilutti L, Sandroff B, McAuley E. Premorbid physical activity predicts disability progression in relapsing-remitting multiple sclerosis. J Neurol Sci. 2012 Dec;323(1–2):123–7. [CrossRef]
- Lin X, Zarghami A, Jelinek GA, Simpson-Yap S, Neate S, Nag N. Diet and omega-3 and vitamin D supplement use predict five-year fatigue and disability trajectories in people with multiple sclerosis. Mult Scler Relat Disord. 2024 Jun;86:105615. [CrossRef]
- Schmitz K, Barthelmes J, Stolz L, Beyer S, Diehl O, Tegeder I. “Disease modifying nutricals” for multiple sclerosis. Pharmacol Ther. 2015 Apr;148:85–113.
- O’Connor K, Weinstock-Guttman B, Carl E, Kilanowski C, Zivadinov R, Ramanathan M. Patterns of dietary and herbal supplement use by multiple sclerosis populations. J Neurol. 2012 Apr;259(4):637–44.
- Bergien SO, Petersen CM, Lynning M, Kristiansen M, Skovgaard L. Use of natural medicine and dietary supplements concomitant with conventional medicine among people with Multiple Sclerosis. Mult Scler Relat Disord. 2020 Sep;44:102197. [CrossRef]
- Marx W, Hockey M, McGuinness AJ, Lane M, Christodoulou J, van der Mei I, et al. The effect of emerging nutraceutical interventions for clinical and biological outcomes in multiple sclerosis: A systematic review. Mult Scler Relat Disord. 2020 Jan;37:101486. [CrossRef]
- Spagnuolo P. Interactions Between Nutraceutical Supplements and Standard Acute Myeloid Leukemia Chemotherapeutics. J Pharm Pharm Sci a Publ Can Soc Pharm Sci Soc Can des Sci Pharm. 2015;18(4):339–43. [CrossRef]
- Szymaszkiewicz A, López-Gómez L, Zielińska M, Abalo R. Nutraceuticals and peripheral glial cells: a possible link? J Integr Neurosci. 2022 Jan;21(1):1.
- Yuan J, Tao Y, Wang M, Huang F, Wu X. Natural compounds as potential therapeutic candidates for multiple sclerosis: Emerging preclinical evidence. Phytomedicine. 2024 Jan;123:155248. [CrossRef]
- Rito Y, Torre-Villalvazo I, Flores J, Rivas V, Corona T. Epigenetics in Multiple Sclerosis: Molecular Mechanisms and Dietary Intervention. Cent Nerv Syst Agents Med Chem. 2018 Jan;18(1):8–15. [CrossRef]
- Menéndez SG, Manucha W. Vitamin D as a Modulator of Neuroinflammation: Implications for Brain Health. Curr Pharm Des. 2024;30(5):323–32. [CrossRef]
- Wergeland S, Torkildsen Ø, Myhr K-M, Aksnes L, Mørk SJ, Bø L. Dietary vitamin D3 supplements reduce demyelination in the cuprizone model. PLoS One. 2011;6(10):e26262. [CrossRef]
- Soleimani M, Jameie SB, Mehdizadeh M, Keradi M, Masoumipoor M, Mehrabi S. Vitamin D3 influence the Th1/Th2 ratio in C57BL/6 induced model of experimental autoimmune encephalomyelitis. Iran J Basic Med Sci. 2014 Oct;17(10):785–92.
- Dias da Silva W, Tambourgi D V. IgY: a promising antibody for use in immunodiagnostic and in immunotherapy. Vet Immunol Immunopathol. 2010 Jun;135(3–4):173–80.
- Lee L, Samardzic K, Wallach M, Frumkin LR, Mochly-Rosen D. Immunoglobulin Y for Potential Diagnostic and Therapeutic Applications in Infectious Diseases. Front Immunol. 2021;12:696003. [CrossRef]
- Paraschiv AC, Vacaras V, Nistor C, Vacaras C, Nistor DT, Vesa SC, et al. Dysbiosis in Multiple Sclerosis: Can Immunoglobulin Y Supplements Help? J Gastrointestin Liver Dis. 2024 Mar;33(1):115–22.
- Shinto L, Calabrese C, Morris C, Sinsheimer S, Bourdette D. Complementary and alternative medicine in multiple sclerosis: survey of licensed naturopaths. J Altern Complement Med. 2004 Oct;10(5):891–7.
- Shinto L, Calabrese C, Morris C, Yadav V, Griffith D, Frank R, et al. A randomized pilot study of naturopathic medicine in multiple sclerosis. J Altern Complement Med. 2008 Jun;14(5):489–96. [CrossRef]
- Teixeira MZ. Immunomodulatory drugs (natalizumab), worsening of multiple sclerosis, rebound effect and similitude. Homeopathy. 2013 Jul;102(3):215–24. [CrossRef]
- Paraschiv A-C, Vacaras V, Nistor C, Vacaras C, Strilciuc S, Muresanu DF. The effect of multiple sclerosis therapy on gut microbiota dysbiosis: a longitudinal prospective study. Microb cell (Graz, Austria). 2024;11:106–15. [CrossRef]
- Tran Nguyen; Talal Alzahrani. Ginkgo Biloba [Internet]. 2023 [cited 2024 Jul 11]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK541024/.
- Lovera JF, Kim E, Heriza E, Fitzpatrick M, Hunziker J, Turner AP, et al. Ginkgo biloba does not improve cognitive function in MS: a randomized placebo-controlled trial. Neurology. 2012 Sep;79(12):1278–84.
- Lovera J, Bagert B, Smoot K, Morris CD, Frank R, Bogardus K, et al. Ginkgo biloba for the improvement of cognitive performance in multiple sclerosis: a randomized, placebo-controlled trial. Mult Scler. 2007 Apr;13(3):376–85.
- Yin J-J, He Y, An J, Miao Q, Sui R-X, Wang Q, et al. Dynamic Balance of Microglia and Astrocytes Involved in the Remyelinating Effect of Ginkgolide B. Front Cell Neurosci. 2019;13:572. [CrossRef]
- Seifar F, Khalili M, Khaledyan H, Amiri Moghadam S, Izadi A, Azimi A, et al. α-Lipoic acid, functional fatty acid, as a novel therapeutic alternative for central nervous system diseases: A review. Nutr Neurosci. 2019 May;22(5):306–16. [CrossRef]
- Rocamonde B, Paradells S, Barcia JM, Barcia C, García Verdugo JM, Miranda M, et al. Neuroprotection of lipoic acid treatment promotes angiogenesis and reduces the glial scar formation after brain injury. Neuroscience. 2012 Nov;224:102–15. [CrossRef]
- Marracci GH, McKeon GP, Marquardt WE, Winter RW, Riscoe MK, Bourdette DN. Alpha lipoic acid inhibits human T-cell migration: implications for multiple sclerosis. J Neurosci Res. 2004 Nov;78(3):362–70.
- Espiritu AI, Remalante-Rayco PPM. High-dose biotin for multiple sclerosis: A systematic review and meta-analyses of randomized controlled trials. Mult Scler Relat Disord. 2021 Oct;55:103159.
- Levy MJF, Garcia-Diaz B, Sedel F, Baron-Van Evercooren A, Mozafari S. High Dose Pharmaceutical Grade Biotin (MD1003) Accelerates Differentiation of Murine and Grafted Human Oligodendrocyte Progenitor Cells In Vivo. Int J Mol Sci. 2022 Dec;23(24). [CrossRef]
- Sedel F, Bernard D, Mock DM, Tourbah A. Targeting demyelination and virtual hypoxia with high-dose biotin as a treatment for progressive multiple sclerosis. Neuropharmacology. 2016 Nov;110(Pt B):644–53. [CrossRef]
- Cree BAC, Cutter G, Wolinsky JS, Freedman MS, Comi G, Giovannoni G, et al. Safety and efficacy of MD1003 (high-dose biotin) in populations with progressive multiple sclerosis (SPI2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Neurol. 2020 Dec;19(12):988–97.
- Pietta PG. Flavonoids as antioxidants. J Nat Prod. 2000 Jul;63(7):1035–42.
- Ielpo MT, Basile A, Miranda R, Moscatiello V, Nappo C, Sorbo S, et al. Immunopharmacological properties of flavonoids. Fitoterapia. 2000 Aug;71 Suppl 1:S101-9. [CrossRef]
- Atucha NM, Romecín P, Vargas F, García-Estañ J. Effects of Flavonoids in Experimental Models of Arterial Hypertension. Curr Top Med Chem. 2022;22(9):735–45. [CrossRef]
- Jaeger BN, Parylak SL, Gage FH. Mechanisms of dietary flavonoid action in neuronal function and neuroinflammation. Mol Aspects Med. 2018 Jun;61:50–62. [CrossRef]
- Williamson G, Kay CD, Crozier A. The Bioavailability, Transport, and Bioactivity of Dietary Flavonoids: A Review from a Historical Perspective. Compr Rev food Sci food Saf. 2018 Sep;17(5):1054–112. [CrossRef]
- Cichon N, Saluk-Bijak J, Gorniak L, Przyslo L, Bijak M. Flavonoids as a Natural Enhancer of Neuroplasticity-An Overview of the Mechanism of Neurorestorative Action. Antioxidants (Basel, Switzerland). 2020 Oct;9(11). [CrossRef]
- Faysal M, Dehbia Z, Zehravi M, Sweilam SH, Haque MA, Kumar KP, et al. Flavonoids as Potential Therapeutics Against Neurodegenerative Disorders: Unlocking the Prospects. Neurochem Res. 2024 Aug;49(8):1926–44. [CrossRef]
- Vauzour D, Vafeiadou K, Rodriguez-Mateos A, Rendeiro C, Spencer JPE. The neuroprotective potential of flavonoids: a multiplicity of effects. Genes Nutr. 2008 Dec;3(3–4):115–26. [CrossRef]
- Bakoyiannis I, Daskalopoulou A, Pergialiotis V, Perrea D. Phytochemicals and cognitive health: Are flavonoids doing the trick? Biomed Pharmacother. 2019 Jan;109:1488–97.
- Hendriks JJA, Alblas J, van der Pol SMA, van Tol EAF, Dijkstra CD, de Vries HE. Flavonoids influence monocytic GTPase activity and are protective in experimental allergic encephalitis. J Exp Med. 2004 Dec;200(12):1667–72.
- Bayat P, Farshchi M, Yousefian M, Mahmoudi M, Yazdian-Robati R. Flavonoids, the compounds with anti-inflammatory and immunomodulatory properties, as promising tools in multiple sclerosis (MS) therapy: A systematic review of preclinical evidence. Int Immunopharmacol. 2021 Jun;95:107562. [CrossRef]
- Marventano S, Kolacz P, Castellano S, Galvano F, Buscemi S, Mistretta A, et al. A review of recent evidence in human studies of n-3 and n-6 PUFA intake on cardiovascular disease, cancer, and depressive disorders: does the ratio really matter? Int J Food Sci Nutr. 2015;66(6):611–22. [CrossRef]
- Chénais B, Blanckaert V. The janus face of lipids in human breast cancer: how polyunsaturated Fatty acids affect tumor cell hallmarks. Int J Breast Cancer. 2012;2012:712536. [CrossRef]
- Davinelli S, Intrieri M, Corbi G, Scapagnini G. Metabolic indices of polyunsaturated fatty acids: current evidence, research controversies, and clinical utility. Crit Rev Food Sci Nutr. 2021;61(2):259–74. [CrossRef]
- Colussi G, Catena C, Baroselli S, Nadalini E, Lapenna R, Chiuch A, et al. Omega-3 fatty acids: from biochemistry to their clinical use in the prevention of cardiovascular disease. Recent Pat Cardiovasc Drug Discov. 2007 Jan;2(1):13–21. [CrossRef]
- Khandelwal S, Kelly L, Malik R, Prabhakaran D, Reddy S. Impact of omega-6 fatty acids on cardiovascular outcomes: A review. J Prev Cardiol. 2013 Feb;2(3):325–36.
- D’Archivio M, Scazzocchio B, Vari R, Santangelo C, Giovannini C, Masella R. Recent Evidence on the Role of Dietary PUFAs in Cancer Development and Prevention. Curr Med Chem. 2018;25(16):1818–36. [CrossRef]
- Mbarik M, Biam RS, Robichaud P-P, Surette ME. The impact of PUFA on cell responses: Caution should be exercised when selecting PUFA concentrations in cell culture. Prostaglandins Leukot Essent Fatty Acids. 2020 Apr;155:102083. [CrossRef]
- Benatti P, Peluso G, Nicolai R, Calvani M. Polyunsaturated fatty acids: biochemical, nutritional and epigenetic properties. J Am Coll Nutr. 2004 Aug;23(4):281–302. [CrossRef]
- Siegert E, Paul F, Rothe M, Weylandt KH. The effect of omega-3 fatty acids on central nervous system remyelination in fat-1 mice. BMC Neurosci. 2017 Jan;18(1):19. [CrossRef]
- Chen S, Zhang H, Pu H, Wang G, Li W, Leak RK, et al. n-3 PUFA supplementation benefits microglial responses to myelin pathology. Sci Rep. 2014 Dec;4:7458. [CrossRef]
- van Meeteren ME, Baron W, Beermann C, Dijkstra CD, van Tol EAF. Polyunsaturated fatty acid supplementation stimulates differentiation of oligodendroglia cells. Dev Neurosci. 2006;28(3):196–208. [CrossRef]
- Talukdar T, Zamroziewicz MK, Zwilling CE, Barbey AK. Nutrient biomarkers shape individual differences in functional brain connectivity: Evidence from omega-3 PUFAs. Hum Brain Mapp. 2019 Apr;40(6):1887–97.
- Lopresti AL. Potential Role of Curcumin for the Treatment of Major Depressive Disorder. CNS Drugs. 2022 Feb;36(2):123–41. [CrossRef]
- Xu X-Y, Meng X, Li S, Gan R-Y, Li Y, Li H-B. Bioactivity, Health Benefits, and Related Molecular Mechanisms of Curcumin: Current Progress, Challenges, and Perspectives. Nutrients. 2018 Oct;10(10). [CrossRef]
- Tossetta G, Fantone S, Giannubilo SR, Marzioni D. The Multifaced Actions of Curcumin in Pregnancy Outcome. Antioxidants (Basel, Switzerland). 2021 Jan;10(1). [CrossRef]
- Ghafouri-Fard S, Shoorei H, Bahroudi Z, Hussen BM, Talebi SF, Taheri M, et al. Nrf2-Related Therapeutic Effects of Curcumin in Different Disorders. Biomolecules. 2022 Jan;12(1). [CrossRef]
- Liu S, Liu J, He L, Liu L, Cheng B, Zhou F, et al. A Comprehensive Review on the Benefits and Problems of Curcumin with Respect to Human Health. Molecules. 2022 Jul;27(14). [CrossRef]
- Abdollahi E, Momtazi AA, Johnston TP, Sahebkar A. Therapeutic effects of curcumin in inflammatory and immune-mediated diseases: A nature-made jack-of-all-trades? J Cell Physiol. 2018 Feb;233(2):830–48.
- Sadek MA, Rabie MA, El Sayed NS, Sayed HM, Kandil EA. Neuroprotective effect of curcumin against experimental autoimmune encephalomyelitis-induced cognitive and physical impairments in mice: an insight into the role of the AMPK/SIRT1 pathway. Inflammopharmacology. 2024 Apr;32(2):1499–518. [CrossRef]
- ELBini-Dhouib I, Manai M, Neili N-E, Marzouki S, Sahraoui G, Ben Achour W, et al. Dual Mechanism of Action of Curcumin in Experimental Models of Multiple Sclerosis. Int J Mol Sci. 2022 Aug;23(15). [CrossRef]
- Salehi B, Calina D, Docea AO, Koirala N, Aryal S, Lombardo D, et al. Curcumin’s Nanomedicine Formulations for Therapeutic Application in Neurological Diseases. J Clin Med. 2020 Feb;9(2). [CrossRef]
- Kulashekar M, Stom SM, Peuler JD. Resveratrol’s Potential in the Adjunctive Management of Cardiovascular Disease, Obesity, Diabetes, Alzheimer Disease, and Cancer. J Am Osteopath Assoc. 2018 Sep;118(9):596–605.
- Malhotra A, Bath S, Elbarbry F. An Organ System Approach to Explore the Antioxidative, Anti-Inflammatory, and Cytoprotective Actions of Resveratrol. Oxid Med Cell Longev. 2015;2015:803971. [CrossRef]
- Jasiński M, Jasińska L, Ogrodowczyk M. Resveratrol in prostate diseases - a short review. Cent Eur J Urol. 2013;66(2):144–9. [CrossRef]
- Rocha-González HI, Ambriz-Tututi M, Granados-Soto V. Resveratrol: a natural compound with pharmacological potential in neurodegenerative diseases. CNS Neurosci Ther. 2008;14(3):234–47. [CrossRef]
- Springer M, Moco S. Resveratrol and Its Human Metabolites-Effects on Metabolic Health and Obesity. Nutrients. 2019 Jan;11(1). [CrossRef]
- Berman AY, Motechin RA, Wiesenfeld MY, Holz MK. The therapeutic potential of resveratrol: a review of clinical trials. NPJ Precis Oncol. 2017;1. [CrossRef]
- Vang O, Ahmad N, Baile CA, Baur JA, Brown K, Csiszar A, et al. What is new for an old molecule? Systematic review and recommendations on the use of resveratrol. PLoS One. 2011;6(6):e19881. [CrossRef]
- Tomé-Carneiro J, Larrosa M, González-Sarrías A, Tomás-Barberán FA, García-Conesa MT, Espín JC. Resveratrol and clinical trials: the crossroad from in vitro studies to human evidence. Curr Pharm Des. 2013;19(34):6064–93. [CrossRef]
- Shamsher E, Khan RS, Davis BM, Dine K, Luong V, Somavarapu S, et al. Nanoparticles Enhance Solubility and Neuroprotective Effects of Resveratrol in Demyelinating Disease. Neurother J Am Soc Exp Neurother. 2023 Jul;20(4):1138–53. [CrossRef]
- Ghaiad HR, Nooh MM, El-Sawalhi MM, Shaheen AA. Resveratrol Promotes Remyelination in Cuprizone Model of Multiple Sclerosis: Biochemical and Histological Study. Mol Neurobiol. 2017 Jul;54(5):3219–29. [CrossRef]
- Yao P, Liu Y. Terpenoids: Natural Compounds for Non-Alcoholic Fatty Liver Disease (NAFLD) Therapy. Molecules. 2022 Dec;28(1). [CrossRef]
- Ahmad A, Tiwari RK, Ansari IA. Revisiting the Antiviral Efficacy of Terpenoids: Plausible Adjunct Therapeutics for Novel SARS-CoV-2? Endocr Metab Immune Disord Drug Targets. 2021;21(12):2119–30.
- Paduch R, Kandefer-Szerszeń M, Trytek M, Fiedurek J. Terpenes: substances useful in human healthcare. Arch Immunol Ther Exp (Warsz). 2007;55(5):315–27. [CrossRef]
- Shin M, Liu QF, Choi B, Shin C, Lee B, Yuan C, et al. Neuroprotective Effects of Limonene (+) against Aβ42-Induced Neurotoxicity in a Drosophila Model of Alzheimer’s Disease. Biol Pharm Bull. 2020 Mar;43(3):409–17. [CrossRef]
- Mony TJ, Elahi F, Choi JW, Park SJ. Neuropharmacological Effects of Terpenoids on Preclinical Animal Models of Psychiatric Disorders: A Review. Antioxidants (Basel, Switzerland). 2022 Sep;11(9). [CrossRef]
- Yang H, Dou QP. Targeting apoptosis pathway with natural terpenoids: implications for treatment of breast and prostate cancer. Curr Drug Targets. 2010 Jun;11(6):733–44. [CrossRef]
- de las Heras B, Hortelano S. Molecular basis of the anti-inflammatory effects of terpenoids. Inflamm Allergy Drug Targets. 2009 Mar;8(1):28–39. [CrossRef]
- Carsanba E, Pintado M, Oliveira C. Fermentation Strategies for Production of Pharmaceutical Terpenoids in Engineered Yeast. Pharmaceuticals (Basel). 2021 Mar;14(4). [CrossRef]
- Tomassini V, d’Ambrosio A, Petsas N, Wise RG, Sbardella E, Allen M, et al. The effect of inflammation and its reduction on brain plasticity in multiple sclerosis: MRI evidence. Hum Brain Mapp. 2016 Jul;37(7):2431–45. [CrossRef]
- Cicero AFG, Colletti A. Polyphenols Effect on Circulating Lipids and Lipoproteins: From Biochemistry to Clinical Evidence. Curr Pharm Des. 2018;24(2):178–90. [CrossRef]
- Giglio RV, Patti AM, Cicero AFG, Lippi G, Rizzo M, Toth PP, et al. Polyphenols: Potential Use in the Prevention and Treatment of Cardiovascular Diseases. Curr Pharm Des. 2018;24(2):239–58. [CrossRef]
- Gorzynik-Debicka M, Przychodzen P, Cappello F, Kuban-Jankowska A, Marino Gammazza A, Knap N, et al. Potential Health Benefits of Olive Oil and Plant Polyphenols. Int J Mol Sci. 2018 Feb;19(3). [CrossRef]
- Focaccetti C, Izzi V, Benvenuto M, Fazi S, Ciuffa S, Giganti MG, et al. Polyphenols as Immunomodulatory Compounds in the Tumor Microenvironment: Friends or Foes? Int J Mol Sci. 2019 Apr;20(7).
- Rodrigo R, Libuy M, Feliu F, Hasson D. Polyphenols in disease: from diet to supplements. Curr Pharm Biotechnol. 2014;15(4):304–17. [CrossRef]
- Vacca RA, Valenti D, Caccamese S, Daglia M, Braidy N, Nabavi SM. Plant polyphenols as natural drugs for the management of Down syndrome and related disorders. Neurosci Biobehav Rev. 2016 Dec;71:865–77. [CrossRef]
- Mabrouk M, El Ayed M, Démosthènes A, Aissouni Y, Aouani E, Daulhac-Terrail L, et al. Antioxidant effect of grape seed extract corrects experimental autoimmune encephalomyelitis behavioral dysfunctions, demyelination, and glial activation. Front Immunol. 2022;13:960355. [CrossRef]
- Colovic MB, Vasic VM, Djuric DM, Krstic DZ. Sulphur-containing Amino Acids: Protective Role Against Free Radicals and Heavy Metals. Curr Med Chem. 2018 Jan;25(3):324–35. [CrossRef]
- Partti-Pellinen K, Marttila O, Vilkka V, Jaakkola JJ, Jäppinen P, Haahtela T. The South Karelia Air Pollution Study: effects of low-level exposure to malodorous sulfur compounds on symptoms. Arch Environ Health. 1996;51(4):315–20. [CrossRef]
- Jaakkola JJ, Partti-Pellinen K, Marttila O, Miettinen P, Vilkka V, Haahtela T. The South Karelia Air Pollution Study: changes in respiratory health in relation to emission reduction of malodorous sulfur compounds from pulp mills. Arch Environ Health. 1999;54(4):254–63. [CrossRef]
- Gurvitz M, Lui GK, Marelli A. Adult Congenital Heart Disease-Preparing for the Changing Work Force Demand. Cardiol Clin. 2020 Aug;38(3):283–94. [CrossRef]
- Caylak E, Aytekin M, Halifeoglu I. Antioxidant effects of methionine, alpha-lipoic acid, N-acetylcysteine and homocysteine on lead-induced oxidative stress to erythrocytes in rats. Exp Toxicol Pathol Off J Gesellschaft fur Toxikologische Pathol. 2008 Aug;60(4–5):289–94. [CrossRef]
- Ghaiad HR, A Abd-Elmawla M, Gad ES, A Ahmed K, Abdelmonem M. Modulating miR-146a Expression by Hydrogen Sulfide Ameliorates Motor Dysfunction and Axonal Demyelination in Cuprizone-Induced Multiple Sclerosis. ACS Chem Neurosci. 2023 Sep;14(17):3047–58.
- Yao G, Yun Y, Sang N. Differential effects between one week and four weeks exposure to same mass of SO2 on synaptic plasticity in rat hippocampus. Environ Toxicol. 2016 Jul;31(7):820–9. [CrossRef]
- Munger KL, Chitnis T, Ascherio A. Body size and risk of MS in two cohorts of US women. Neurology. 2009 Nov;73(19):1543–50. [CrossRef]
- Neto A, Fernandes A, Barateiro A. The complex relationship between obesity and neurodegenerative diseases: an updated review. Front Cell Neurosci. 2023;17:1294420. [CrossRef]
- Seidell JC. Obesity, insulin resistance and diabetes--a worldwide epidemic. Br J Nutr. 2000 Mar;83 Suppl 1:S5-8.
- Mokry LE, Ross S, Timpson NJ, Sawcer S, Davey Smith G, Richards JB. Obesity and Multiple Sclerosis: A Mendelian Randomization Study. PLoS Med. 2016 Jun;13(6):e1002053.
- Liu Z, Zhang T-T, Yu J, Liu Y-L, Qi S-F, Zhao J-J, et al. Excess Body Weight during Childhood and Adolescence Is Associated with the Risk of Multiple Sclerosis: A Meta-Analysis. Neuroepidemiology. 2016;47(2):103–8. [CrossRef]
- Hedström AK, Olsson T, Alfredsson L. Body mass index during adolescence, rather than childhood, is critical in determining MS risk. Mult Scler. 2016 Jun;22(7):878–83. [CrossRef]
- Hedström AK, Olsson T, Alfredsson L. High body mass index before age 20 is associated with increased risk for multiple sclerosis in both men and women. Mult Scler. 2012 Sep;18(9):1334–6. [CrossRef]
- Kavak KS, Teter BE, Hagemeier J, Zakalik K, Weinstock-Guttman B. Higher weight in adolescence and young adulthood is associated with an earlier age at multiple sclerosis onset. Mult Scler. 2015 Jun;21(7):858–65. [CrossRef]
- Kvistad SS, Myhr K-M, Holmøy T, Šaltytė Benth J, Wergeland S, Beiske AG, et al. Body mass index influence interferon-beta treatment response in multiple sclerosis. J Neuroimmunol. 2015 Nov;288:92–7. [CrossRef]
- Lutfullin I, Eveslage M, Bittner S, Antony G, Flaskamp M, Luessi F, et al. Association of obesity with disease outcome in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2023 Jan;94(1):57–61. [CrossRef]
- Harroud A, Manousaki D, Butler-Laporte G, Mitchell RE, Davey Smith G, Richards JB, et al. The relative contributions of obesity, vitamin D, leptin, and adiponectin to multiple sclerosis risk: A Mendelian randomization mediation analysis. Mult Scler. 2021 Nov;27(13):1994–2000. [CrossRef]
- Samara A, Cantoni C, Piccio L, Cross AH, Chahin S. Obesity, gut microbiota, and multiple sclerosis: Unraveling the connection. Mult Scler Relat Disord. 2023 Aug;76:104768. [CrossRef]
- Hedström AK, Lima Bomfim I, Barcellos L, Gianfrancesco M, Schaefer C, Kockum I, et al. Interaction between adolescent obesity and HLA risk genes in the etiology of multiple sclerosis. Neurology. 2014 Mar;82(10):865–72. [CrossRef]
- Pakpoor J, Schmierer K, Cuzick J, Giovannoni G, Dobson R. Estimated and projected burden of multiple sclerosis attributable to smoking and childhood and adolescent high body-mass index: a comparative risk assessment. Int J Epidemiol. 2021 Jan;49(6):2051–7. [CrossRef]
- Daniele G, Lunghi C, Dardano A, Binda P, Ceccarini G, Santini F, et al. Bariatric surgery restores visual cortical plasticity in nondiabetic subjects with obesity. Int J Obes (Lond). 2021 Aug;45(8):1821–9. [CrossRef]
- Lunghi C, Daniele G, Binda P, Dardano A, Ceccarini G, Santini F, et al. Altered Visual Plasticity in Morbidly Obese Subjects. iScience. 2019 Dec;22:206–13. [CrossRef]
- Sui SX, Ridding MC, Hordacre B. Obesity is Associated with Reduced Plasticity of the Human Motor Cortex. Brain Sci. 2020 Aug;10(9). [CrossRef]
- Hwang L-L, Wang C-H, Li T-L, Chang S-D, Lin L-C, Chen C-P, et al. Sex differences in high-fat diet-induced obesity, metabolic alterations and learning, and synaptic plasticity deficits in mice. Obesity (Silver Spring). 2010 Mar;18(3):463–9.
- Al-Dalaeen A, Al-Domi H. Does obesity put your brain at risk? Diabetes Metab Syndr. 2022 Mar;16(3):102444.
- Ji Z, Wu S, Xu Y, Qi J, Su X, Shen L. Obesity Promotes EAE Through IL-6 and CCL-2-Mediated T Cells Infiltration. Front Immunol. 2019;10:1881. [CrossRef]
- Stampanoni Bassi M, Iezzi E, Buttari F, Gilio L, Simonelli I, Carbone F, et al. Obesity worsens central inflammation and disability in multiple sclerosis. Mult Scler. 2020 Sep;26(10):1237–46. [CrossRef]
- Correale J, Marrodan M. Multiple sclerosis and obesity: The role of adipokines. Front Immunol. 2022;13:1038393. [CrossRef]
- Davanzo GG, Castro G, Monteiro L de B, Castelucci BG, Jaccomo VH, da Silva FC, et al. Obesity increases blood-brain barrier permeability and aggravates the mouse model of multiple sclerosis. Mult Scler Relat Disord. 2023 Apr;72:104605. [CrossRef]
- Shahi SK, Ghimire S, Lehman P, Mangalam AK. Obesity induced gut dysbiosis contributes to disease severity in an animal model of multiple sclerosis. Front Immunol. 2022;13:966417. [CrossRef]
- Spielman LJ, Little JP, Klegeris A. Inflammation and insulin/IGF-1 resistance as the possible link between obesity and neurodegeneration. J Neuroimmunol. 2014 Aug;273(1–2):8–21. [CrossRef]
- Mokhtarzade M, Agha-Alinejad H, Motl RW, Negaresh R, Baker JS, Zimmer P. Weight control and physical exercise in people with multiple sclerosis: Current knowledge and future perspectives. Complement Ther Med. 2019 Apr;43:240–6. [CrossRef]
- Bruce JM, Cozart JS, Shook RP, Ruppen S, Siengsukon C, Simon S, et al. Modifying Diet and Exercise in MS (MoDEMS): Study design and protocol for a telehealth weight loss intervention for adults with obesity & Multiple Sclerosis. Contemp Clin Trials. 2021 Aug;107:106495. [CrossRef]
- Bruce JM, Cozart JS, Shook RP, Befort C, Siengsukon CF, Simon S, et al. Modifying diet and exercise in multiple sclerosis (MoDEMS): A randomized controlled trial for behavioral weight loss in adults with multiple sclerosis and obesity. Mult Scler. 2023 Dec;29(14):1860–71. [CrossRef]
- Stenberg E, Forsberg L, Hedström A, Hillert J, Näslund E. Bariatric and metabolic surgery in populations with morbid obesity and multiple sclerosis - a nationwide, matched cohort study. Surg Obes Relat Dis Off J Am Soc Bariatr Surg. 2021 Jun;17(6):1108–14.
- Bencsath K, Jammoul A, Aminian A, Shimizu H, Fisher CJ, Schauer PR, et al. Outcomes of Bariatric Surgery in Morbidly Obese Populations with Multiple Sclerosis. J Obes. 2017;2017:1935204.
- Morales-Suarez-Varela M, Collado Sánchez E, Peraita-Costa I, Llopis-Morales A, Soriano JM. Intermittent Fasting and the Possible Benefits in Obesity, Diabetes, and Multiple Sclerosis: A Systematic Review of Randomized Clinical Trials. Nutrients. 2021 Sep;13(9). [CrossRef]
- Allogmanny S, Probst Y. Dietary Modification Combined with Nutrition Education and Counseling for Metabolic Comorbidities in Multiple Sclerosis: Implications for Clinical Practice and Research. Curr Nutr Rep. 2024 Jun;13(2):106–12. [CrossRef]
Figure 1.
Mechanisms involved in brain plasticity.
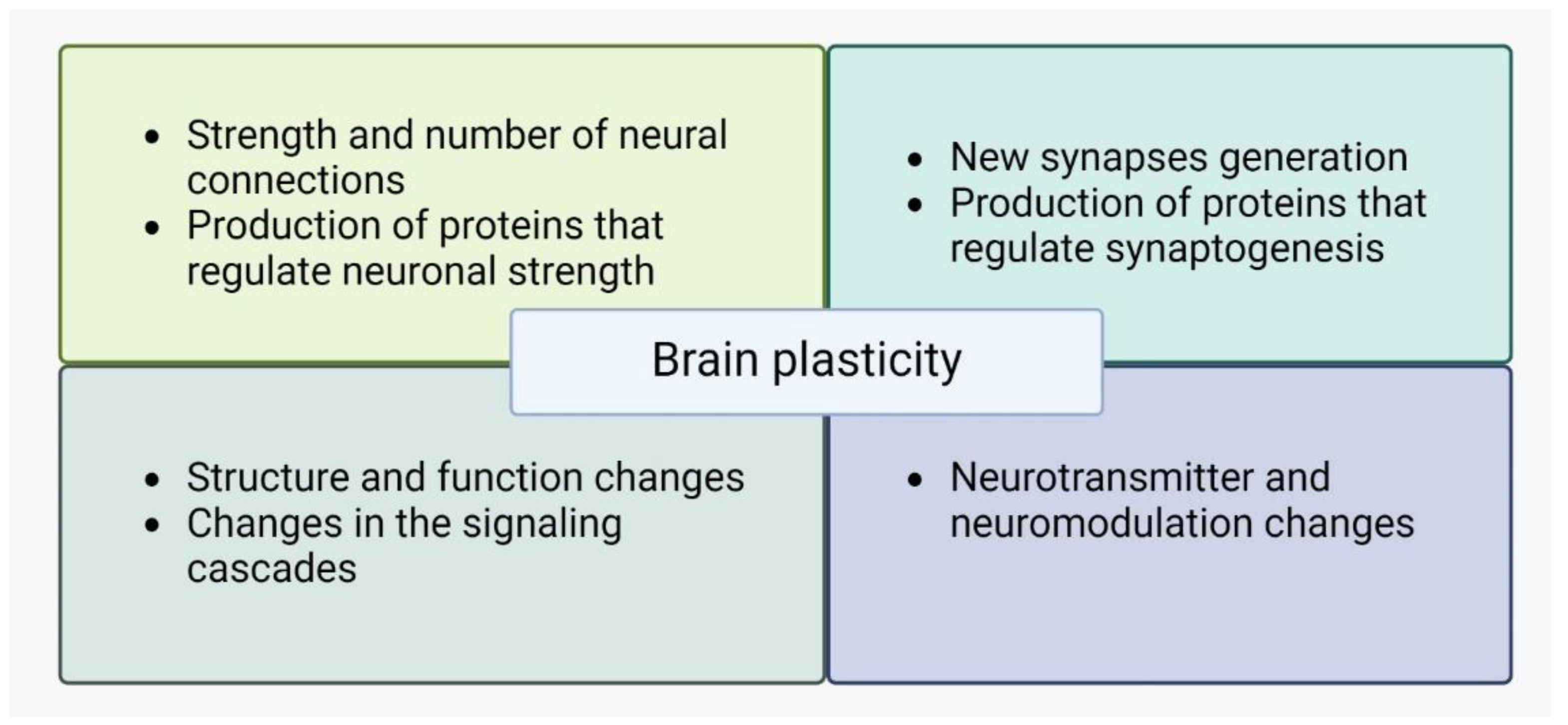
Figure 2.
Proposed mechanisms of neurodegeneration in MS.
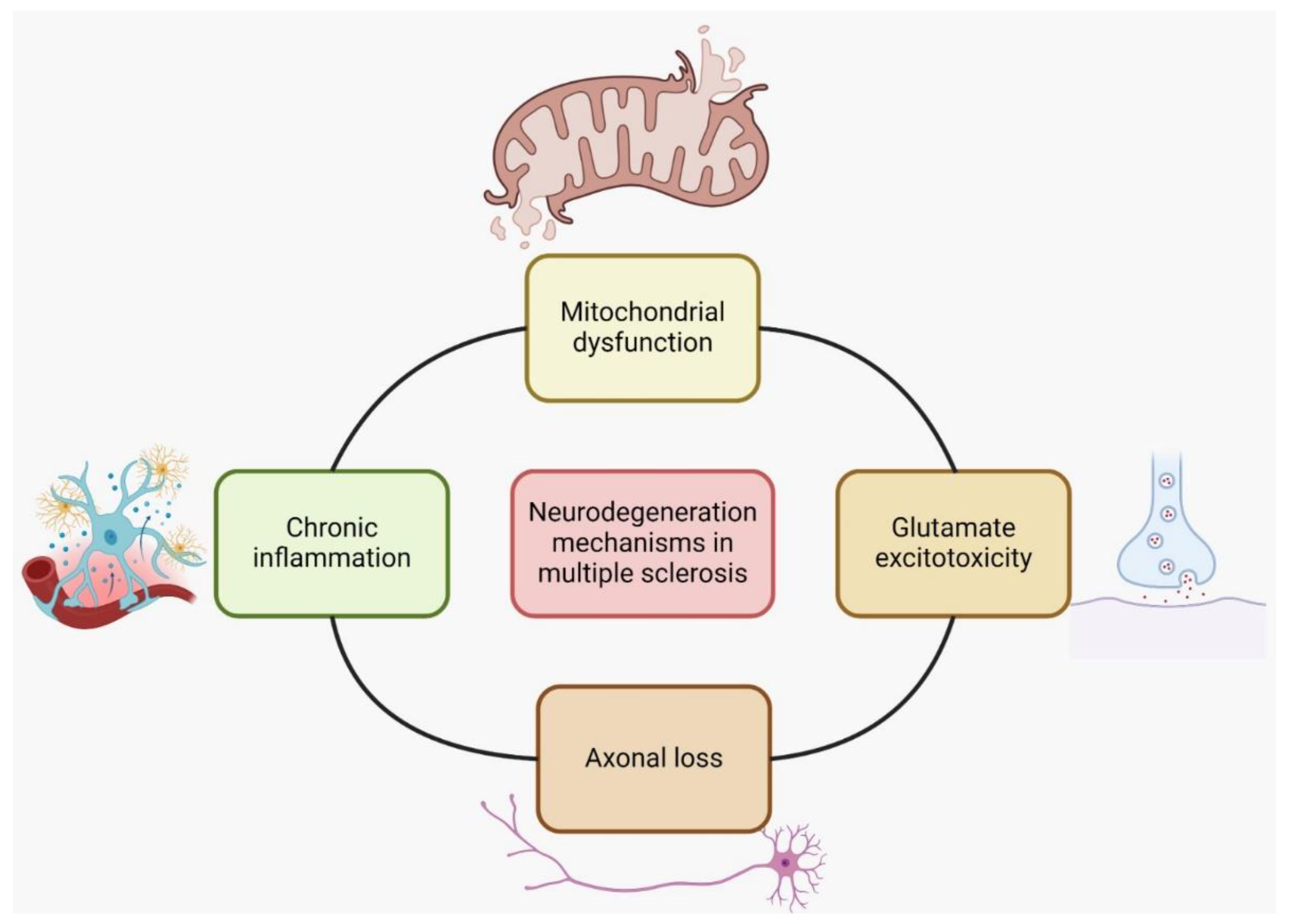
Figure 3.
Proposed mechanisms of neurodegeneration-nutraceuticals interference.
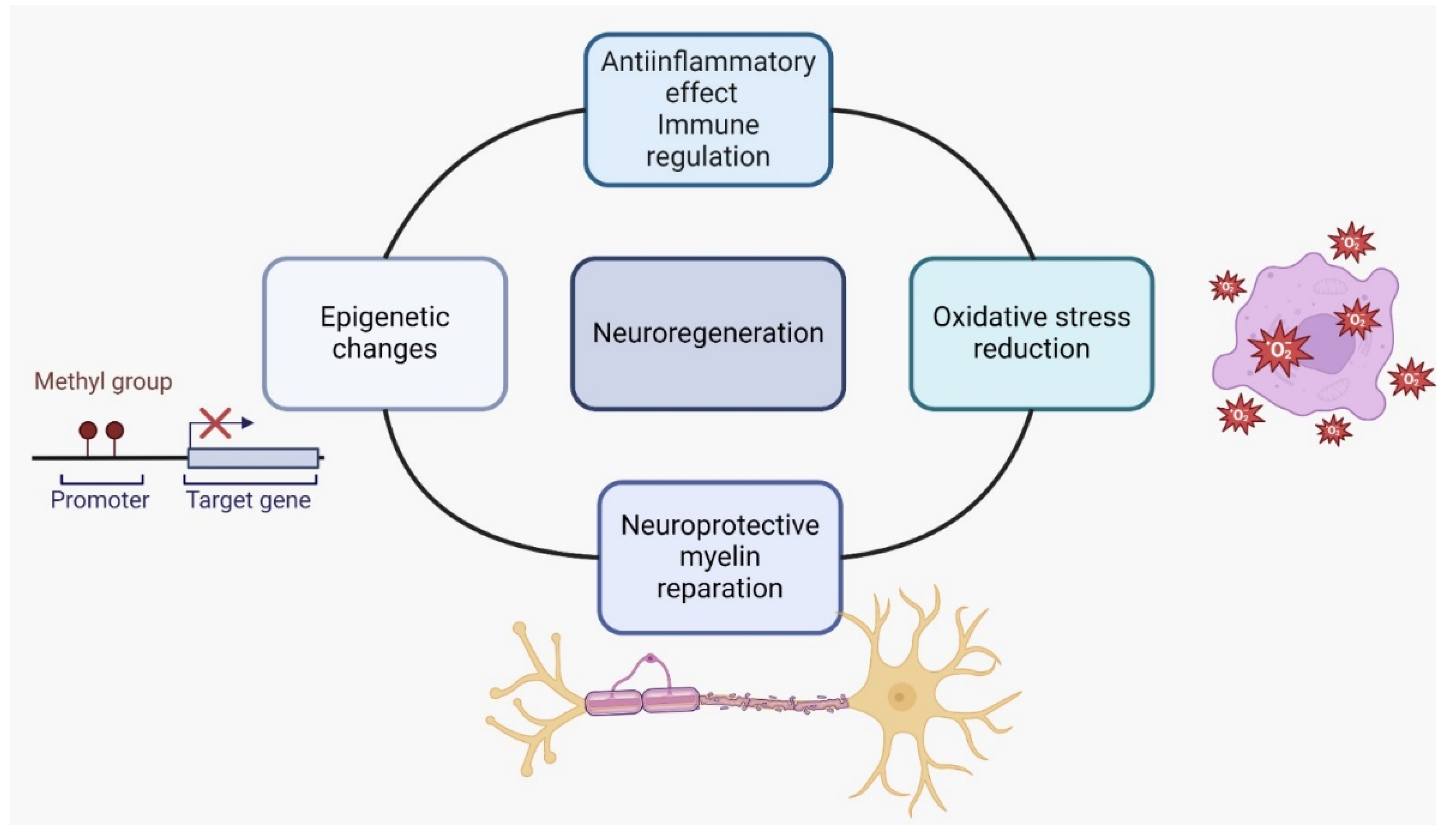
Figure 4.
The cascade of mechanisms in obesity-induced neurodegeneration.
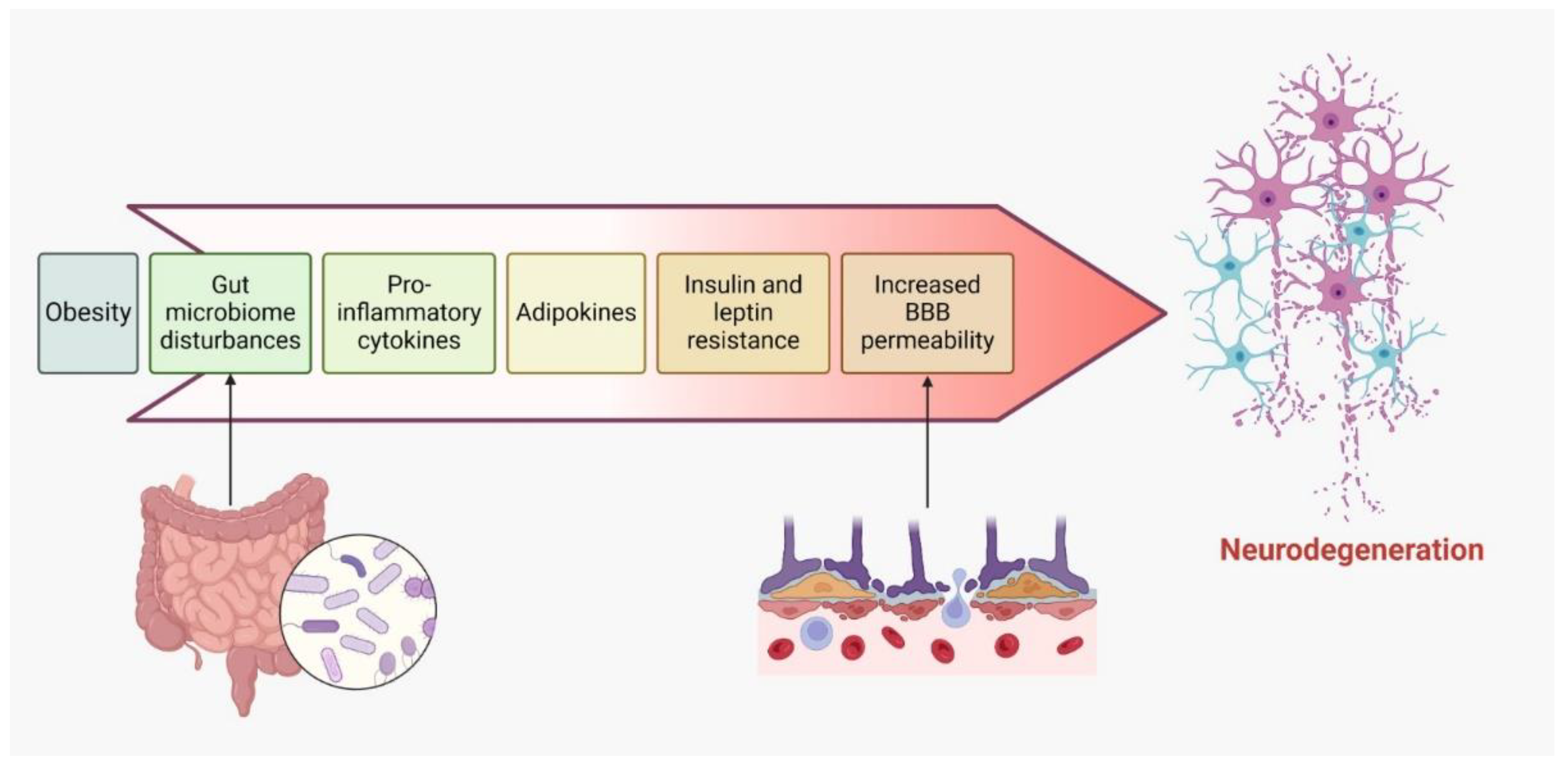

Table 1.
Modifiable risk and protective factors of neurodegeneration in MS.
| Risk factors | Protective factors |
| Smoking | Smoking cessation |
| Obesity | Calorie restriction Physical activity |
| Childhood low sun exposure | Higher sun exposure Vitamin D3 supplementation |
| Oxidative diet | Antioxidant supplementation Diet re-assessment |
Table 2.
Summary of nutraceuticals used in MS.
| Compound | Primary Function/Effect | Role in Brain Plasticity and MS | Key Findings and Studies |
|---|---|---|---|
| Vitamin D3 (Cholecalciferol) | Maintains calcium and phosphate balance for bone health, with emerging roles in brain health. | Immunomodulatory and neuroprotective effects; promotes neurogenesis and synaptic plasticity. | May reduce disease activity and demyelination in MS; early intervention in EAE mice controlled neuroinflammation [64,65,66]. |
| Immunoglobulin Y (IgY) | Avian antibody involved in immune defense; passive immunity to offspring via egg yolk. | Limited research in MS, but potential in modulating immune responses and gut microbiota. | Positive outcomes in clinical trials for MS, with reduced symptoms and altered immune responses; further research needed [67,68,69]. |
| Homeopathy | CAM approach using highly diluted substances for symptom relief based on individualized treatment. | Limited evidence; potential placebo effect. | Some individuals report symptom relief; more research is required to determine efficacy in MS [12,70,71,72,73]. |
| Ginkgo biloba extract (GBE) | Plant extract with neuroprotective and neuroregenerative properties; enhances cerebral blood flow. | Limited evidence in MS; potential effects on synaptic plasticity. | No significant cognitive improvement in MS; potential neuroprotective effects in neurological diseases [74,75,76,77]. |
| Alpha Lipoic Acid (ALA) | Antioxidant and anti-inflammatory compound with roles in mitochondrial energy production. | Promotes neuroprotection and repair after injury; potential therapy for MS. | Preclinical and clinical studies show promising effects; more research needed to establish efficacy in MS [78,79,80]. |
| Biotin (Vitamin B7) | Cofactor in metabolic processes, energy production, and fatty acid synthesis. | Potential in preventing brain neurodegeneration in MS. | High-dose biotin (MD1003) shows promise in slowing MS progression; mechanisms include enhanced energy production and myelin synthesis [4,60,81,82,83,84]. |
| Flavonoids | Plant polyphenols with antioxidant, anti-inflammatory, and immunomodulatory properties. | Neuroprotective and neuroplasticity-promoting effects; limited direct evidence in MS. | Positive therapeutic effects in EAE models; potential benefits for brain plasticity in MS, but more research needed [85,86,87,88,89,90,91,92,93,94,95]. |
| Polyunsaturated Fatty Acids (PUFA) | Essential fatty acids with anti-inflammatory properties and roles in brain function. | Modulate microglial responses; promote remyelination and oligodendrocyte differentiation. | Omega-3 PUFA supplementation reduces demyelination in MS models; associated with improved brain connectivity in humans [96,97,98,99,100,101,102,103,104,105,106,107]. |
| Curcumin | Natural compound with antioxidant, anti-inflammatory, and neuroprotective properties. | Potential benefits for brain health and plasticity in MS, though limited research specific to MS. | Demonstrated neuroprotective effects and reduced demyelination in MS animal models; more research needed [108,109,110,111,112,113,114,115,116]. |
| Resveratrol | Polyphenol with antioxidant, anti-inflammatory, and anti-cancer properties. | Limited research in MS; potential neuroprotective effects. | Improved outcomes in EAE mouse models; promotes remyelination and motor coordination in MS-like conditions in mice [117,118,119,120,121,122,123,124,125,126]. |
| Terpenoids | Natural compounds with diverse biological activities, including anti-inflammatory and antioxidant effects. | Studied for potential benefits in chronic illnesses, including neurological conditions. | Preclinical studies suggest neuropharmacological effects; further research needed to explore benefits in MS and brain plasticity [127,128,129,130,131,132,133,134]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



