
Submitted:
24 July 2024
Posted:
25 July 2024
You are already at the latest version
Abstract
This paper presents the rationale for using ultra low intensity transcranial light photodynamic treatment (LIT-PDT) for treating glioblastoma. Glioblastoma is currently treated with maximal safe resection, temozolomide and ionizing irradiation. Mortality in 2024 remains at over 80% within several years from diagnosis. 5-aminolevulinic acid (5-ALA) is a heme precursor that is selectively taken up preferentially by malignant cells, including glioblastoma. Photon energy can be transduced to molecular oxygen by a 5-ALA metabolite, PpIX, transforming oxygen to the singlet state, a reactive oxygen species (ROS) that destroys or damages vital glioblastoma cell structures. In PDT, light energy ~ 100 to 200 J / cm2, at 630 nm is delivered intraoperatively after resection and preoperative oral 5-ALA. This generates ROS cytotoxicity in residual glioblastoma cells within the resection cavity wall. 630 nm light poorly penetrates skin, skull, and brain tissue. That currently restricts PDT to a single intraoperative session using high flux light. LIT-PDT addresses some current shortcomings of 5-ALA PDT treatment. Part 1 analyzes published data indicating that continuous ultra low light flux, 17 μW / cm2, over 24 hours for a total delivery of 1.5 J / cm2, is effective for 5-ALA PDT treatment. That opens the way for repetitive, extracranial light to deliver enough energy for low flux, long duration PDT to any deep brain structure using less than 12 W total distributed over the entire scalp area. In Part 2, by analysis of 5-ALA and PpIX physiology, it became apparent that four non oncology drugs - ciprofloxacin, deferiprone, telmisartan and ziprasidone, will increase energy capture by GB cells, thereby increasing PDT treatment cytotoxicity. A phased pilot study of LIT-PDT treatment is being planned.
Keywords:
5-ALA
; glioblastoma
; noninvasive
; photodynamic treatment
; repurposing
1. Introduction
This paper analyzes prior studies to show that a new treatment for glioblastoma (GB) that uses ultra low intensity transcranial light photodynamic treatment with drug augmented photodynamic treatment (LIT-PDT) can be an effective treatment. In PDT treatment, oxygen is transformed to its reactive singlet state by light, catalyzed by a 5-aminolevulinic acid (5-ALA) metabolite, PpIX. This singlet state is a reactive oxygen species (ROS) that oxidizes, and thereby destroys or damages, vital GB cell structures leading to cell death [1,2,3]. After oral administration 5-ALA is preferentially taken up by GB cells and converted to PpIX to a greater degree than the surrounding brain tissue. This has two important consequences. 1) PpIX fluoresces red after illumination with 415 nm light, enabling more complete intraoperative identification of tumor margins and hence more complete resection. 2) PpIX will transfer 635 nm light energy to ground state oxygen to generate ROS, preferentially killing GB cells [1,2,3].
Survival at 2 years after a diagnosis of GB remains <20% despite multimodal treatment. This paper presents a data analysis and synthesis of two data sets that can be combined to make a new treatment for GB. The first data set, Section 2 below, analyzes peer-reviewed PDT treatment of GB using orally administered 5-ALA as the photosensitizer. Our analysis concludes that ultra low light fluences delivered noninvasively, transcranially, over 24 hours is both feasible, safe, and predicted to be more effective than short duration, intraoperative high fluence 5-ALA PDT as currently used in treating GB.
The second data set, presented in Section 3 below, analyzes peer-reviewed data on four drugs from general medical practice - the antibiotic ciprofloxacin (cipro), the iron chelator deferiprone, and either the hypertension treatment drug telmisartan or the antipsychotic drug ziprasidone to increase effect of 630 nm light PDT in treating GB. They all have good evidence of increasing 5-ALA PDT effectiveness.
However, although many variables will influence survival, in the summer of 2024, standard treatment of GB with maximal safe resection, followed by irradiation and temozolomide, in a general GB population, still results a median overall survival under 2 years due to tumor recurrence [4,5].
Dozens of clinical trials of new medicines, and different forms and schedules of ionizing irradiation tried over the last 20 years have failed to greatly prolong survival [6,7]. The addition of the wearable Optune® device (Novocure Ltd., Haifa, Israel) that delivers 200 KHz electromagnetic radiation (radio frequency, non-ionizing) to the brain and tumor area has demonstrated good tolerability, some GB mitotic slowing and other potentially advantageous metabolic changes but only slight prolongation of median overall survival [8]. Using intraoperative PpIX fluorescence leads to better tumor demarcation, resection and slightly longer time to progression [9]. Ten years ago it was said that GB's fatal recurrence rate is almost 100% [10]. Despite some improvements in the standard of care, the same can be said today.
The usual first GB recurrence is within the first 20 mm of the resection cavity wall, and most of these are within the original irradiation field [11]. Extending resection, so-called extra marginal resection may prolong time to recurrence but not prevent it. At the time of diagnosis GB has already spread throughout the entire brain.
Based on our analysis of the transcranial light brain penetration studies of Tedford et al and Mathews et al, vide infra, we determined that i) noninvasive transcranial 630 to 660 nm light can deliver an ultra low fluence rate (17 μW / cm2) to a GB, to the post-resection peritumoral area, and to the entire brain and, ii) prolonged and repetitive delivery of such fluence is effective in mediating 5-ALA PDT killing of GB cells [12,13].
Thus the LIT-PDT Regimen includes two components: 1) ultra low light levels delivered continuously noninvasively over 24 hours with 5-ALA PDT, and 2) three orally administered drugs from general, non oncology medicine - ciprofloxacin, deferiprone, and telmisartan or ziprasidone - will augment capture of 630 nm photon energy, increasing ROS generation after 5-ALA. Details follow.
2. Multiple array, Ultra Low Fluence, Transcranial, Repetitive, 5-ALA PDT
In PDT of GB as currently constituted, oral 5-ALA is preferentially taken up by GB cells and metabolized to PpIX. PpIX transfers 630 nm light energy to ground state O2 (3O2), thereby generating singlet O2 (1O2), one of several ROS [14,15,16,17]. See Table 1. for oxygen related ROS definitions.
Ferrochelatase mediates iron incorporation into PpIX, transforming PpIX to non-ROS generating heme. PpIX accumulates in large quantities in GB cells after 5-ALA administration due to increased uptake of 5-ALA compared to non-GB brain tissue, and reduced ferrochelatase activity and increased heme demand in GB cells [15,18,19,20,21].
Intraoperative 5-ALA PDT heretofore has been by using ~200 J / cm2 total, of 635 nm light delivered to the resection cavity wall in five fractions of 12 minutes with 2 minute pause between the four periods. The light exposure is performed with the direct placement of up to 4 diffusers or through an Intralipid ™ filled Foley catheter intracavitary diffuser, for a delivery total of 720,000 mW.s = 720 J / cm2 total, fractionated over 1 hr [22].
This, delivered intraoperatively as a single session before closure immediately after fluorescence guided resection [19,21,22,23]. Exploration began twenty years ago of low fluence, mW 5-ALA PDT, delivered over extended periods of time to increase selective tumor cell kill through apoptosis. [24,25,26]. See Table 2 for definitions of light measurement terms.
The limitations of 5-ALA PDT as currently practiced are restricted to a single intraoperative PDT session. This means that high fluence light is required. As a consequence necrosis predominates as mode of death, as opposed to the preferable apoptosis that would predominate if ultra low fluence could be used. Approximately 4 to 13 mm deep to the surface of the resection cavity receives enough photon energy to generate cytotoxic ROS during intraoperative PDT [23,27]. Also blood clots and surgical debris may interfere in the efficacy of the intracavitary light delivery. Also, in current practice intraoperative high light flux PDT quickly exhausts available O2 supply even when ventilating the patient with 100% oxygen during the treatment. PDT requires O2 to be effective.
Prolonged or repetitive PDT leaving the resection cavity open with the attendant risks and procedure complications [28], or fully implantable light and power sources, the Globus Lucidus [29], have been in development to allow long term, repeated PDT. However we know that PpIX positive GB cells reside within the first 20 mm of the resection cavity wall [30,31]. Those cells will not receive enough short term light to be killed by intraoperative PDT, even by high flux delivery of 200 J / cm2 [12,13].
In vitro work by Mathews et al however has opened up another avenue to overcome the current limitations of one shot intraoperative PDT. Mathews et al [13] and others [32,33] have shown that ultra low fluence (<50 μW / cm2] delivered continuously over 24 hours can be repeated with resulting deep blockage of GB growth. Cytotoxicity was primarily by apoptosis, not necrosis. Mathews et al even showed no growth using four 24 hr periods of 17 μW / cm2 flux, 1.5 J / cm2 total delivered, 635 nm light, separated by 3 day intervals [13]. Note that 1.5 J / cm2 per 24 illumination day is less than 1% of the fluence used in today’s clinical intraoperative 5-ALA PDT:
86,400 s / day x 17 μW / cm2 = 1.5 J / cm2 .
If given once at a single session, Mathews reported that 12 J / cm2 was the required light dose to achieve similar growth suppression, an 8 times higher total energy delivery compared to the repeated 24 hour low flux treatment [13].
This small fluence can be delivered non-invasively, transcranially, to GB tissue from the scalp surface by using fully external multi LED 630 nm light array, through intact human skin and skull. The calculation behind this statement:
Lapchak measured light attenuation across the human calvaria and found that 4.2% of the incident power was transmitted with minor corrections for variations in depth and hydration [34,35,36]. Tedford et al measured attenuation versus depth in human brain parenchyma to be 2.4 / cm2 depending slightly on wavelength and geometry [12]. Assuming the head is broadly illuminated so that scattering may be neglected, we can reasonably estimate light power at the tumor in terms of power incident on the scalp reduced by these factors.
where
p = P × 0.042 × exp(-d / 2.4 cm)
p = delivered power density at the tumor in W / cm2
P = incident power density at the scalp in W / cm2
d = depth of the tumor beneath the cortex in cm
Matthews found in vitro that a protocol of long-term exposure at low power was effective on glioma spheroids at 17 µW / cm2. Inverting the formula, we can solve for the incident power density P sufficient to deliver a desired power density p at the tumor as a function of the tumor depth d. See Table 3 for the resultant predicted external 630 nm flux requirement noninvasively applied to the head to achieve 17 µW / cm2 at a GB post-resection area at the listed depth from the external light source.
p = P × 0.042 × exp(-d / 2.4 cm) .
The listed external flux can be easily delivered by many of the current commercially available photobiomodulation helmets for home use, for which no prescription is needed. If we take an average scalp area to be 700 cm2 then total light energy delivered to the entire scalp area would be ~12 W to reach the deepest GB.
So Part 1 of the LIT-PDT program is to deliver post resection 17 μW / cm2 630 nm illumination to the resection area / 24 hrs after oral preoperative 5-ALA. Light will be delivered by an external multi LED array cap, giving broad head illumination such that light scattering may be neglected.
Prolonged transcranial 630 nm light delivery from 10 to 20 W light sources has a well established safety history of use in humans, a procedure called photobiomodulation [37,38,39,40,41]. Photobiomodulation refers to use of external low level (<20 mW / cm2) LED arrays to deliver transcranial light at ~630 nm (red) light to the brain with the aim of improving brain function deficits.
Dozens of clinical studies in humans have explored 630 nm photobiomodulation treatment to reduce impairments of Alzheimer’s disease [42,43], cognitive or executive function [44,45], Parkinson’s disease [46], traumatic brain injury [47,48], autism [49], and others [50,51,52]. While the results on brain function have not shown to have unequivocal benefit, all the studies have shown good safety with minimal or no side effects from this light delivery.
A wide variety of these photobiomodulation helmets delivering broad head illumination at 630 nm are currently commercially available for home use without prescription. Most of these can easily deliver 17 µW / cm2 to any part of the brain. Figure 1 shows a schematic of LIT-PDT illumination of a GB tumor area
3. The LIT-PDT Drugs
Drug repurposing refers to use of previously approved drugs that induce basic physiology changes that are beneficial in treating conditions other than their traditional or originally approved use.
The two of the four drugs discussed here, cipro, deferiprone, were discussed previously as potential adjuncts to PDT [53]. Table 4 lists the four augmentation drugs with their common use in general medical practice and their primary intended use in LIT-PDT. Figure 2 shows a schematic of the drugs’ locus of action in augmenting 5-ALA-PDT.
3.1. Ciprofloxacin
Cipro is a rather common broad-spectrum antibiotic in use in humans around the world. As an antibiotic, cipro works by inhibiting bacterial DNA gyrase while also stabilizing DNA strand damage created by DNA gyrase and topoisomerase IV. Repositioning cipro as a cancer cell cytotoxic drug has a research database empirically demonstrating such an effect but the mechanism by which it does so has not yet been firmly established [54,55,56,57].
Cipro exhibits an unexplained specificity in killing a variety of malignant cells at the 40 t0 80 μg/mL range while sparing non-transformed cells [58]. In vitro results indicated that cipro could be used as an adjuvant to treat GBM by increasing apoptosis and ROS production in these cells [59,60]. In glioma GL26 cells, cipro decreased cell viability and inhibited proliferation [61]. In the GB A-172 cell line, cipro induced an increased Bax/Bcl-2 ratio and tumor cell death. Also in the A-172 line cipro increased the cytotoxic effects of TMZ [59,60]. Other studies also showed the cytotoxic, anti-proliferative and pro-apoptotic effect of cipro towards the GB cell line U87MG GB cells [62].
In preclinical study, cipro augmented 5-ALA cytotoxicity to GB. Using Caesium-137 gamma irradiation, 0.66 MeV, 1 Gy / min, 8 Gy total, GB cytotoxicity and intracellular ROS increased in vitro with added 5-ALA alone. Adding cipro to 5-ALA further increased that irradiation’ s cytotoxicity. The effect was not large but it was clear and statistically significant [63].
Empirically cipro enhanced 5-ALA PDT cytotoxicity to chordoma cell lines in vitro when there was no effect of light alone, cipro alone, or 5-ALA alone [64]. Empirically cipro enhanced 5-ALA PDT cytotoxicity to meningioma cell lines in vitro when there was no effect of light alone, cipro alone, or 5-ALA alone [65].
Recognizing the preclinical database of inherent cytotoxicity to malignant cells, Gera et al gave 1000 mg/day cipro along with traditional chemotherapy with etoposide in acute myeloid leukemia in a phase 1b trial. That trial gave evidence of modest benefit from adding cipro [66].
3.2. Deferiprone
Deferiprone is an iron binding drug in human use to reduce iron overload. In preclinical study, a series of FDA/EMA approved, related iron binding drugs augmented 5-ALA cytotoxicity to GB by the same mechanism. By binding iron, iron becomes less available for incorporation into PpIX to create heme. That metabolic impediment results in a buildup of intracellular PpIX [67,68,69,70,71,72]. This process can be intuitively appreciated by Figure 2, as the left hand arrow going off from PpIX decreases, more PpIX is available to the right hand arrow process going off to singlet oxygen, 1O2.
Among the several FDA/EMA approved iron chelators for human use, deferiprone would be best for use in GB 5-ALA use because it achieves good brain tissue levels [73,74]. The other approved iron chelators do not. Deferiprone has been in use for 40 years and has a good history of tolerability, safety, and reduction of brain iron content [74,75].
3.3. ABCG2 and Telmisartan or Ziprasidone
ABCG2, also known as BCRP, is a 144 kDa homodimer drug efflux pump. It is the primary export pump for 5-ALA [80,81,82,83]. Many drugs that inhibit GB's ABCG2 efflux transporter will increase intracellular 5-ALA levels, increase PpIX accumulation, and increase 5-ALA PDT GB cell killing [84,85,86]. Accordingly, as part of the LIT-PDT Regimen, one of the currently marketed drugs that inhibits ABCG2 should be added to 5-ALA PDT GB treatment. Independently of potential benefits of use during 5-ALA PDT, ABCG2 inhibition increases brain tissue levels of temozolomide [87], the mainstay cytotoxic chemotherapy drug in GB.
A wide range of currently FDA/EMA marketed drugs, although marketed for other indications, have been shown to also inhibit transport function of ABCG2: aprepitant, dabigatran, meloxicam, ziprasidone [88], aripiprazole [89], telmisartan [90], febuxostat [91], lapatinib [81,84], rifapentine [92] among others. Of these we focus on two drugs, telmisartan and ziprasidone that coincidentally have documented growth inhibiting effects on GB of their own, alone, independently of light, PDT, or 5-ALA.
3.3.1. Telmisartan
Telmisartan is an angiotensin II receptor 1 blocking drug (an ARB) used to lower high blood pressure. It also exerts agonism at PPAR-gamma/alpha and exhibits neuroinflammation reducing effects [93,94]. Telmisartan inhibits ABCG2 drug transport [90,95,96]. IC IC50 was 17 μM at ABCG2 [90].
Unrelated to PDT, a review in 2016 outlined the potential advantages of adding telmisartan to standard GB treatment [97]. Since then further data on glioma growth inhibition by telmisartan alone has accrued [98,99,100]. Preclinical studies in a variety of other cancers have similarly shown growth suppression by telmisartan, independently from any effects on PDT [101,102,103,104,105,106,107]. These findings would favor using telmisartan to augment 5-ALA PDT as a drug with 5-ALA independent anti-GB effects as well as inhibition of ABCG2.
3.3.2. Ziprasidone
Almost all currently approved and marketed drugs to treat psychosis act to block dopaminergic signaling at dopamine receptor 2 (D2). Ziprasidone is one of the 20+ D2 blocking drugs currently approved and marketed to treat psychosis. Inhibitory IC50 of ziprasidone at ABCG2 was 2.8 µM [108].
See reviews from 2014 and 2020 on D2 drive in GB growth and the importance of inhibiting D2 signaling during GB treatment [109,110]. Since the original review in 2014, many papers have confirmed the GB growth drive from D2 agonism and the potential for D2 blocking drugs to inhibit GB growth [111,112,113,114,115,116,117,118,119]. These findings would favor using ziprasidone to augment 5-ALA PDT as a drug with 5-ALA independent anti-GB effects as well as inhibition of ABCG2.
The lower IC50 would favor ziprasidone as would the added benefit of D2 inhibition but risk of akathisia or unpleasant mental side effect potential would be votes against its use. In theory both telmisartan and ziprasidone could be used simultaneously - there is no predictable drug-drug interaction. It is unknown if the ABCG2 inhibiting effects would be additive to 5-ALA PDT. Nor do we know if the inherent anti-GB effects of telmisartan and ziprasidone, unrelated to 5-ALA or PDT, would be additive or not.
4. LIT-PDT and GB Ecosystems
As with most ecosystems in nature, different interacting communities exist within a GB. These cell communities are connected by pairwise interactions leading to a mutual interdependence of the different populations, each on each other.
In cancer generally and in GB specifically, current cancer research has identified multiple ecological roles played by each malignant cell subpopulation (community) and between malignant cell subpopulations and trophic non-malignant cell populations (monocyte lineage cells, neutrophils, lymphocytes, fibroblasts, endothelial cells, et al). These many dyads tend to be mutually supporting and have different spectra of vulnerabilities to growth inhibition, so we reason that the more mutually supporting ecosystems we can inhibit or kill, the more effective the treatment will be [120,121,122,123,124,125].
A special case of mutually supporting ecosystems in cancer - the stem/non stem cells’ relationship - requires specific addressing. Throughout the common deadly cancers, including in GB, tumors tend to relapse after an initial tumor reduction with initial chemo or radiotherapy. Recurrence tends to arise from small numbers of the relatively treatment resistant GB stem cell subpopulation. Stem cells in the recurrent tumor are even more resistant to treatment than were the primary tumors’ stem cells. GB stem cells are at the apex of an entropic hierarchy and impart therapy resistance [20,126,127].
We have indications that GB stem cell subpopulations are more resistant to 5-ALA PDT [128,129]. However GB stem cells can respond to PDT [130,131,132,133,134], highlighting the importance of defeating resistance pathways as the augmentation drugs - telmisartan and ziprasidone advocated in this paper - are designed to do.
5. Discussion and Conclusions
Cipro, deferiprone, and febuxostat are well tolerated drugs, usually without side effects. Although surprises cannot be excluded, there is no a priori reason to suspect drug-drug interaction that would change that low side effect risk when these three are used together.
Low fluence light delivery in 5-ALA PDT has several advantages over the current use of high fluence intraoperative PDT. Lower fluence over a longer time results predominantly in apoptosis and less inflammation. Higher fluence 5-ALA PDT over a shorter time results in predominantly necrosis with relatively more inflammation and edema [25,135]. A second advantage of low fluence light is that we can repeatedly and noninvasively deliver it.
The safety of the human brain’s exposure to low wattage extracranial 630 nm has been well established by the large body of research on photobiomodulation [136,137,138,139,140,141].
Preclinical study of Mathews et al explored 17 μW / cm2 flux over considerably longer exposure times (24 hours, 1.5 J / cm2 total) but repeating this every fourth day [13]. A further advantage of low flux delivery is reduced immunosuppression elements [142].
A pilot study is planned. 36 hours prior to primary surgery, one newly diagnosed GB will receive 5-ALA by mouth, then 32 hours of continuous noninvasive 630 nm transcranial illumination of fluence calculated to deliver 17 μW / cm2 / 24 hours. Calculated as follows:
24h x 60 min x 60 sec = 86,400 sec in 1 day.
17 μW / cm2 x 86,400 sec =
1,468,800 μW.sec / cm2 / day = 1.5 J / cm2 / d, the in vitro dose that Mathews et al showed stopped all GB cell growth [13].
Thus the predicted total 630 nm light energy received by the tumor resection area will be 2.3 J / cm2 delivered over a continuous illumination time of 32 hours. Depending on results the next step would be the same illumination schedule, 32 hours on, off for 88 hours (1⅓ day on, 3⅔ days off) , for 4 cycles prior to surgery. Further schedules would be determined by these initial histology results. Evaluation of effect by necrosis, apoptosis, and K67 markers, and standard H&E pathology report.
As a consequence of this paper’s analysis of the data, a phased pilot study of LIT-PDT warranted and planned.
References
- Cramer SW, Chen CC. Photodynamic Therapy for the Treatment of Glioblastoma. Front Surg. 2020;6:81. [CrossRef]
- Harada Y, Murayama Y, Takamatsu T, Otsuji E, Tanaka H. 5-Aminolevulinic Acid-Induced Protoporphyrin IX Fluorescence Imaging for Tumor Detection: Recent Advances and Challenges. Int J Mol Sci. 2022;23(12):6478. [CrossRef]
- Huis In 't Veld RV, Heuts J, Ma S, Cruz LJ, Ossendorp FA, Jager MJ. Current Challenges and Opportunities of Photodynamic Therapy against Cancer. Pharmaceutics. 2023;15(2):330. [CrossRef]
- Vivas-Buitrago T, Domingo RA, Tripathi S, De Biase G, Brown D, Akinduro OO, Ramos-Fresnedo A, Sabsevitz DS, Bendok BR, Sherman W, Parney IF, Jentoft ME, Middlebrooks EH, Meyer FB, Chaichana KL, Quinones-Hinojosa A. Influence of supramarginal resection on survival outcomes after gross-total resection of IDH-wild-type glioblastoma. J Neurosurg. 2021;136(1):1-8. [CrossRef]
- Poon MTC, Sudlow CLM, Figueroa JD, Brennan PM. Longer-term (≥ 2 years) survival in patients with glioblastoma in population-based studies pre- and post-2005: a systematic review and meta-analysis. Sci Rep. 2020;10(1):11622. [CrossRef]
- Seyve A, Lozano-Sanchez F, Thomas A, Mathon B, Tran S, Mokhtari K, Giry M, Marie Y, Capelle L, Peyre M, Carpentier A, Feuvret L, Sanson M, Hoang-Xuan K, Honnorat J, Delattre JY, Ducray F, Idbaih A. Initial surgical resection and long time to occurrence from initial diagnosis are independent prognostic factors in resected recurrent IDH wild-type glioblastoma. Clin Neurol Neurosurg. 2020;196:106006. [CrossRef]
- Birzu C, French P, Caccese M, Cerretti G, Idbaih A, Zagonel V, Lombardi G. Recurrent Glioblastoma: From Molecular Landscape to New Treatment Perspectives. Cancers (Basel). 2020;13(1):47. [CrossRef]
- Szklener K, Bilski M, Nieoczym K, Mańdziuk D, Mańdziuk S. Enhancing glioblastoma treatment through the integration of tumor-treating fields. Front Oncol. 2023;13:1274587. [CrossRef]
- Eatz TA, Eichberg DG, Lu VM, Di L, Komotar RJ, Ivan ME. Intraoperative 5-ALA fluorescence-guided resection of high-grade glioma leads to greater extent of resection with better outcomes: a systematic review. J Neurooncol. 2022;156(2):233-256. [CrossRef]
- Olar A, Aldape KD. Using the molecular classification of glioblastoma to inform personalized treatment. J Pathol. 2014;232(2):165-77. [CrossRef]
- Gebhardt BJ, Dobelbower MC, Ennis WH, Bag AK, Markert JM, Fiveash JB. Patterns of failure for glioblastoma multiforme following limited-margin radiation and concurrent temozolomide. Radiat Oncol. 2014;9:130. [CrossRef]
- Tedford CE, DeLapp S, Jacques S, Anders J. Quantitative analysis of transcranial and intraparenchymal light penetration in human cadaver brain tissue. Lasers Surg Med. 2015;47(4):312-22. [CrossRef]
- Mathews MS, Angell-Petersen E, Sanchez R, Sun CH, Vo V, Hirschberg H, Madsen SJ. The effects of ultra low fluence rate single and repetitive photodynamic therapy on glioma spheroids. Lasers Surg Med. 2009;41(8):578-84. [CrossRef]
- Pignatelli P, Umme S, D'Antonio DL, Piattelli A, Curia MC. Reactive Oxygen Species Produced by 5-Aminolevulinic Acid Photodynamic Therapy in the Treatment of Cancer. Int J Mol Sci. 2023;24(10):8964. [CrossRef]
- Cramer SW, Chen CC. Photodynamic Therapy for the Treatment of Glioblastoma. Front Surg. 2020;6:81. [CrossRef]
- Marcus SL, de Souza MP. Theranostic Uses of the Heme Pathway in Neuro-Oncology: Protoporphyrin IX (PpIX) and Its Journey from Photodynamic Therapy (PDT) through Photodynamic Diagnosis (PDD) to Sonodynamic Therapy (SDT). Cancers (Basel). 2024;16(4):740. [CrossRef]
- Li B, Shen Y, Lin H, Wilson BC. Correlation of in vitro cell viability and cumulative singlet oxygen luminescence from protoporphyrin IX in mitochondria and plasma membrane. Photodiagnosis Photodyn Ther. 2024;46:104080. [CrossRef]
- Stummer W, Müther M, Spille D. Beyond fluorescence-guided resection: 5-ALA-based glioblastoma therapies. Acta Neurochir (Wien). 2024;166(1):163. [CrossRef]
- Peciu-Florianu I, Vannod-Michel Q, Vauleon E, Bonneterre ME, Reyns N. Long term follow-up of patients with newly diagnosed glioblastoma treated by intraoperative photodynamic therapy: an update from the INDYGO trial (NCT03048240). J Neurooncol. 2024;168(3):495-505. [CrossRef]
- Ibarra LE, Vilchez ML, Caverzán MD, Milla Sanabria LN. Understanding the glioblastoma tumor biology to optimize photodynamic therapy: From molecular to cellular events. J Neurosci Res. 2021;99(4):1024-1047. [CrossRef]
- Vermandel M, Dupont C, Lecomte F, Leroy HA, Tuleasca C, Mordon S, Hadjipanayis CG, Reyns N. Standardized intraoperative 5-ALA photodynamic therapy for newly diagnosed glioblastoma patients: a preliminary analysis of the INDYGO clinical trial. J Neurooncol. 2021;152(3):501-514. [CrossRef]
- da Silva EB Jr, Vasquez MWM, de Almeida Teixeira BC, Neto MC, Sprenger F, Filho JLN, Almeida-Lopes L, Ramina R. Association of 5-aminolevulinic acid fluorescence guided resection with photodynamic therapy in recurrent glioblastoma: a matched cohort study. Acta Neurochir (Wien). 2024;166(1):212. [CrossRef]
- Schipmann S, Müther M, Stögbauer L, Zimmer S, Brokinkel B, Holling M, Grauer O, Suero Molina E, Warneke N, Stummer W. Combination of ALA-induced fluorescence-guided resection and intraoperative open photodynamic therapy for recurrent glioblastoma: case series on a promising dual strategy for local tumor control. J Neurosurg. 2020;134(2):426-436. [CrossRef]
- Bisland SK, Lilge L, Lin A, Rusnov R, Wilson BC. Metronomic photodynamic therapy as a new paradigm for photodynamic therapy: rationale and preclinical evaluation of technical feasibility for treating malignant brain tumors. Photochem Photobiol. 2004;80:22-30. [CrossRef]
- Bogaards A, Varma A, Zhang K, Zach D, Bisland SK, Moriyama EH, Lilge L, Muller PJ, Wilson BC. Fluorescence image-guided brain tumour resection with adjuvant metronomic photodynamic therapy: pre-clinical model and technology development. Photochem Photobiol Sci. 2005;4(5):438-42. [CrossRef]
- Guo HW, Lin LT, Chen PH, Ho MH, Huang WT, Lee YJ, Chiou SH, Hsieh YS, Dong CY, Wang HW. Low-fluence rate, long duration photodynamic therapy in glioma mouse model using organic light emitting diode (OLED). Photodiagnosis Photodyn Ther. 2015;12(3):504-10. [CrossRef]
- Dupont C, Mordon S, Deleporte P, Reyns N, Vermandel M. A novel device for intraoperative photodynamic therapy dedicated to glioblastoma treatment. Future Oncol. 2017;13(27):2441-2454. [CrossRef]
- Eljamel MS, Goodman C, Moseley H. ALA and Photofrin fluorescence guided resection and repetitive PDT in glioblastoma multiforme: a single centre Phase III randomised controlled trial. Lasers Med Sci. 2008;23(4):361-7. [CrossRef]
- Bader N, Peschmann C, Kast RE, Heiland T, Merz T, McCook O, Alfieri A, Karpel-Massler G, Capanni F, Halatsch ME. Globus Lucidus: A porcine study of an intracranial implant designed to deliver closed, repetitive photodynamic and photochemical therapy in glioblastoma. Photodiagnosis Photodyn Ther. 2024;46:104059. [CrossRef]
- Andrieux G, Das T, Griffin M, Straehle J, Paine SML, Beck J, Boerries M, Heiland DH, Smith SJ, Rahman R, Chakraborty S. Spatially resolved transcriptomic profiles reveal unique defining molecular features of infiltrative 5-ALA metabolizing cells associated with glioblastoma recurrence. Genome Med. 2023;15(1):48. [CrossRef]
- Yano H, Nakayama N, Ohe N, Miwa K, Shinoda J, Iwama T. Pathological analysis of the surgical margins of resected glioblastomas excised using photodynamic visualization with both 5-aminolevulinic acid and fluorescein sodium. J Neurooncol. 2017;133(2):389-397. [CrossRef]
- Aguilar Cosme JR, Gagui DC, Green NH, Bryant HE, Claeyssens F. In Vitro Low-Fluence Photodynamic Therapy Parameter Screening Using 3D Tumor Spheroids Shows that Fractionated Light Treatments Enhance Phototoxicity. ACS Biomater Sci Eng. 2021;7(11):5078-5089. [CrossRef]
- Madsen SJ, Sun CH, Tromberg BJ, Wallace VP, Hirschberg H. Photodynamic therapy of human glioma spheroids using 5-aminolevulinic acid. Photochem Photobiol. 2000;72(1):128-34. [CrossRef]
- Lapchak PA, Boitano PD. Transcranial Near-Infrared Laser Therapy for Stroke: How to Recover from Futility in the NEST-3 Clinical Trial. Acta Neurochir Suppl. 2016;121:7-12. [CrossRef]
- Lapchak PA, Boitano PD, Butte PV, Fisher DJ, Hölscher T, Ley EJ, Nuño M, Voie AH, Rajput PS. Transcranial Near-Infrared Laser Transmission (NILT) Profiles (800 nm): Systematic Comparison in Four Common Research Species. PLoS One. 2015;10(6):e0127580. [CrossRef]
- Lapchak, PA. Taking a light approach to treating acute ischemic stroke patients: transcranial near-infrared laser therapy translational science. Ann Med. 2010;42(8):576-86. [CrossRef]
- Joshi H, Sinha P, Bowers D, John JP. Dose response of transcranial near infrared light stimulation on brain functional connectivity and cognition in older adults-A randomized comparison. J Biophotonics. 2024;17(2):e202300215. [CrossRef]
- Salehpour F, Cassano P, Rouhi N, Hamblin MR, De Taboada L, Farajdokht F, Mahmoudi J. Penetration Profiles of Visible and Near-Infrared Lasers and Light-Emitting Diode Light Through the Head Tissues in Animal and Human Species: A Review of Literature. Photobiomodul Photomed Laser Surg. 2019;37(10):581-595. [CrossRef]
- Fradkin Y, De Taboada L, Naeser M, Saltmarche A, Snyder W, Steingold E. Transcranial photobiomodulation in children aged 2-6 years: a randomized sham-controlled clinical trial assessing safety, efficacy, and impact on autism spectrum disorder symptoms and brain electrophysiology. Front Neurol. 2024;15:1221193. [CrossRef]
- Shahdadian S, Wang X, Liu H. Directed physiological networks in the human prefrontal cortex at rest and post transcranial photobiomodulation. Sci Rep. 2024;14(1):10242. [CrossRef]
- Huang N, Yao D, Jiang W, Wei C, Li M, Li W, Mu H, Gao M, Ma Z, Lyu J, Tong Z. Safety and Efficacy of 630-nm Red Light on Cognitive Function in Older Adults With Mild to Moderate Alzheimer's Disease: Protocol for a Randomized Controlled Study. Front Aging Neurosci. 2020;12:143. [CrossRef]
- Blivet G, Roman FJ, Lelouvier B, Ribière C, Touchon J. Photobiomodulation Therapy: A Novel Therapeutic Approach to Alzheimer's Disease Made Possible by the Evidence of a Brain-Gut Interconnection. J Integr Neurosci. 2024;23(5):92. [CrossRef]
- Su M, Nizamutdinov D, Liu H, Huang JH. Recent Mechanisms of Neurodegeneration and Photobiomodulation in the Context of Alzheimer's Disease. Int J Mol Sci. 2023;24(11):9272. [CrossRef]
- Gao Y, An R, Huang X, Liu W, Yang C, Wan Q. Effectiveness of photobiomodulation for people with age-related cognitive impairment: a systematic review and meta-analysis. Lasers Med Sci. 2023;38(1):237. [CrossRef]
- Nairuz T, Sangwoo-Cho, Lee JH. Photobiomodulation Therapy on Brain: Pioneering an Innovative Approach to Revolutionize Cognitive Dynamics. Cells. 2024;13(11):966. [CrossRef]
- Bicknell B, Liebert A, Herkes G. Parkinson's Disease and Photobiomodulation: Potential for Treatment. J Pers Med. 2024;14(1):112. [CrossRef]
- Stevens AR, Hadis M, Milward M, Ahmed Z, Belli A, Palin W, Davies DJ. Photobiomodulation in Acute Traumatic Brain Injury: A Systematic Review and Meta-Analysis. J Neurotrauma. 2023;40(3-4):210-227. [CrossRef]
- Lim, L. Traumatic Brain Injury Recovery with Photobiomodulation: Cellular Mechanisms, Clinical Evidence, and Future Potential. Cells. 2024;13(5):385. [CrossRef]
- Ceranoglu TA, Hutt Vater C. Dr. Joseph Biederman's Enduring Legacy: Illuminating the Path to Addressing Autistic Traits in Attention Deficit Hyperactivity Disorder With Transcranial Photobiomodulation. J Atten Disord. 2024;28(5):664-668. [CrossRef]
- Farazi N, Salehi-Pourmehr H, Farajdokht F, Mahmoudi J, Sadigh-Eteghad S. Photobiomodulation combination therapy as a new insight in neurological disorders: a comprehensive systematic review. BMC Neurol. 2024;24(1):101. [CrossRef]
- Ma H, Du Y, Xie D, Wei ZZ, Pan Y, Zhang Y. Recent advances in light energy biotherapeutic strategies with photobiomodulation on central nervous system disorders. Brain Res. 2024;1822:148615. [CrossRef]
- Chamkouri H, Liu Q, Zhang Y, Chen C, Chen L. Brain photobiomodulation therapy on neurological and psychological diseases. J Biophotonics. 2024;17(1):e202300145. [CrossRef]
- Kast RE, Skuli N, Sardi I, Capanni F, Hessling M, Frosina G, Kast AP, Karpel-Massler G, Halatsch ME. Augmentation of 5-Aminolevulinic Acid Treatment of Glioblastoma by Adding Ciprofloxacin, Deferiprone, 5-Fluorouracil and Febuxostat: The CAALA Regimen. Brain Sci. 2018;8(12):203. [CrossRef]
- Alomari S, Zhang I, Hernandez A, Kraft CY, Raj D, Kedda J, Tyler B. Drug Repurposing for Glioblastoma and Current Advances in Drug Delivery-A Comprehensive Review of the Literature. Biomolecules. 2021;11(12):1870. [CrossRef]
- Ferrario N, Marras E, Vivona V, Randisi F, Fallica AN, Marrazzo A, Perletti G, Gariboldi MB. Mechanisms of the Antineoplastic Effects of New Fluoroquinolones in 2D and 3D Human Breast and Bladder Cancer Cell Lines. Cancers (Basel). 2024;16(12):2227. [CrossRef]
- Kloskowski T, Fekner Z, Szeliski K, Paradowska M, Balcerczyk D, Rasmus M, Dąbrowski P, Kaźmierski Ł, Drewa T, Pokrywczyńska M. Effect of four fluoroquinolones on the viability of bladder cancer cells in 2D and 3D cultures. Front Oncol. 2023;13:1222411. [CrossRef]
- Huang CY, Yang JL, Chen JJ, Tai SB, Yeh YH, Liu PF, Lin MW, Chung CL, Chen CL. Fluoroquinolones Suppress TGF-β and PMA-Induced MMP-9 Production in Cancer Cells: Implications in Repurposing Quinolone Antibiotics for Cancer Treatment. Int J Mol Sci. 2021;22(21):11602. [CrossRef]
- Abdel-Aal MAA, Abdel-Aziz SA, Shaykoon MSA, Abuo-Rahma GEA. Towards anticancer fluoroquinolones: A review article. Arch Pharm (Weinheim). 2019;352(7):e1800376. [CrossRef]
- Zandi A, Zanjani TM, Ziai S, Poul YK, Hoseini M. Evaluation of the Cytotoxic Effects of Ciprofloxacin on Human Glioblastoma A-172 Cell Line. Middle East J Cancer. 2017;8(3):119-126.
- Zandi A, Zanjani TM, Ziai S, Poul YK, Hoseini M. The Synergistic Effects of the Combination of Ciprofloxacin and Temozolomide on Human Glioblastoma A-172 Cell Line. Middle East J Cancer. 2017;8(1): 31-38.
- Esmaeilzadeh A., Ebtekar M, Biglari A, Hassan Z. Influence of ciprofloxacin on glioma cell line GL26: A new application for an old antibiotic. African J Microbiol Res. 2012;6(23):4891-4896. [CrossRef]
- Beberok A, Rzepka Z, Respondek M, Rok J, Sierotowicz D, Wrześniok D. GSH depletion, mitochondrial membrane breakdown, caspase-3/7 activation and DNA fragmentation in U87MG glioblastoma cells: New insight into the mechanism of cytotoxicity induced by fluoroquinolones. Euro J Pharmacology. 2018;835:94-107. [CrossRef]
- Ueta K, Yamamoto J, Tanaka T, Nakano Y, Kitagawa T, Nishizawa S. 5-Aminolevulinic acid enhances mitochondrial stress upon ionizing irradiation exposure and increases delayed production of reactive oxygen species and cell death in glioma cells. Int J Mol Med. 2017;39(2):387-398. [CrossRef]
- Gull HH, Karadag C, Senger B, Sorg RV, Möller P, Mellert K, Steiger HJ, Hänggi D, Cornelius JF. Ciprofloxacin enhances phototoxicity of 5-aminolevulinic acid mediated photodynamic treatment for chordoma cell lines. Photodiagnosis Photodyn Ther. 2021;35:102346. [CrossRef]
- Cornelius JF, Slotty PJ, El Khatib M, Giannakis A, Senger B, Steiger HJ. Enhancing the effect of 5-aminolevulinic acid based photodynamic therapy in human meningioma cells. Photodiagnosis Photodyn Ther. 2014;11(1):1-6. [CrossRef]
- Gera K, Cline C, Al-Mansour Z, Medvec A, Lee JH, Galochkina Z, Hsu J, Hiemenz J, Farhadfar N, Dean EA, Wingard JR, Brown R. A phase ib clinical trial of oral ciprofloxacin and etoposide in subjects with resistant acute myeloid leukemia. Leuk Lymphoma. 2024:1-9. [CrossRef]
- Qin J, Zhou C, Zhu M, Shi S, Zhang L, Zhao Y, Li C, Wang Y, Wang Y. Iron chelation promotes 5-aminolaevulinic acid-based photodynamic therapy against oral tongue squamous cell carcinoma. Photodiagnosis Photodyn Ther. 2020;31:101907. [CrossRef]
- Magnussen A, Reburn C, Perry A, Wood M, Curnow A. Experimental investigation of a combinational iron chelating protoporphyrin IX prodrug for fluorescence detection and photodynamic therapy. Lasers Med Sci. 2022;37(2):1155-1166. [CrossRef]
- Howley R, Mansi M, Shinde J, Restrepo J, Chen B. Analysis of Renal Cell Carcinoma Cell Response to the Enhancement of 5-aminolevulinic Acid-mediated Protoporphyrin IX Fluorescence by Iron Chelator Deferoxamine. Photochem Photobiol. 2023;99(2):787-792. [CrossRef]
- Čunderlíková B, Kalafutová A, Babál P, Mlkvý P, Teplický T. Suppression of resistance to aminolevulinic acid-based photodynamic therapy in esophageal cell lines by administration of iron chelators in collagen type I matrices. Int J Radiat Biol. 2023;99(3):474-487. [CrossRef]
- Nomoto T, Komoto K, Nagano T, Ishii T, Guo H, Honda Y, Ogura SI, Ishizuka M, Nishiyama N. Polymeric iron chelators for enhancing 5-aminolevulinic acid-induced photodynamic therapy. Cancer Sci. 2023;114(3):1086-1094. [CrossRef]
- Chen Y, Deng H, Yang L, Guo L, Feng M. Desferrioxamine Enhances 5-Aminolaevulinic Acid- Induced Protoporphyrin IX Accumulation and Therapeutic Efficacy for Hypertrophic Scar. J Pharm Sci. 2023;112(6):1635-1643. [CrossRef]
- Uzungil V, Tran H, Aitken C, Wilson C, Opazo CM, Li S, Payet JM, Mawal CH, Bush AI, Hale MW, Hannan AJ, Renoir T. Novel Antidepressant-Like Properties of the Iron Chelator Deferiprone in a Mouse Model of Depression. Neurotherapeutics. 2022;19(5):1662-1685. [CrossRef]
- Romano N, Baiardi G, Pinto VM, Quintino S, Gianesin B, Sasso R, Diociasi A, Mattioli F, Marchese R, Abbruzzese G, Castaldi A, Forni GL. Long-Term Neuroradiological and Clinical Evaluation of NBIA Patients Treated with a Deferiprone Based Iron-Chelation Therapy. J Clin Med. 2022;11(15):4524. [CrossRef]
- Kontoghiorghes GJ. The Vital Role Played by Deferiprone in the Transition of Thalassaemia from a Fatal to a Chronic Disease and Challenges in Its Repurposing for Use in Non-Iron-Loaded Diseases. Pharmaceuticals (Basel). 2023;16(7):1016. [CrossRef]
- Piffaretti D, Burgio F, Thelen M, Kaelin-Lang A, Paganetti P, Reinert M, D'Angelo ML. Protoporphyrin IX tracer fluorescence modulation for improved brain tumor cell lines visualization. J Photochem Photobiol B. 2019;201:111640. [CrossRef]
- Reburn C, Gawthorpe G, Perry A, Wood M, Curnow A. Novel Iron-Chelating Prodrug Significantly Enhanced Fluorescence-Mediated Detection of Glioma Cells Experimentally In Vitro. Pharmaceutics. 2023;15(12):2668. [CrossRef]
- Teng L, Nakada M, Zhao SG, Endo Y, Furuyama N, Nambu E, Pyko IV, Hayashi Y, Hamada JI. Silencing of ferrochelatase enhances 5-aminolevulinic acid-based fluorescence and photodynamic therapy efficacy. Br J Cancer. 2011;104(5):798-807. [CrossRef]
- de Souza AL, Marra K, Gunn J, Samkoe KS, Kanick SC, Davis SC, Chapman MS, Maytin EV, Hasan T, Pogue BW. Comparing desferrioxamine and light fractionation enhancement of ALA-PpIX photodynamic therapy in skin cancer. Br J Cancer. 2016;115(7):805-13. [CrossRef]
- Kawai N, Hirohashi Y, Ebihara Y, Saito T, Murai A, Saito T, Shirosaki T, Kubo T, Nakatsugawa M, Kanaseki T, Tsukahara T, Shichinohe T, Li L, Hirano S, Torigoe T. ABCG2 expression is related to low 5-ALA photodynamic diagnosis (PDD) efficacy and cancer stem cell phenotype, and suppression of ABCG2 improves the efficacy of PDD. PLoS One. 2019;14(5):e0216503. [CrossRef]
- Howley R, Olsen J, Chen B. Effectiveness of lapatinib for enhancing 5-aminolevulinic acid mediated protoporphyrin IX fluorescence and photodynamic therapy in human cancer cell lines with varied ABCG2 activities. Photochem Photobiol. 2024 Mar 13. [CrossRef]
- Kobuchi H, Moriya K, Ogino T, Fujita H, Inoue K, Shuin T, Yasuda T, Utsumi K, Utsumi T. Mitochondrial localization of ABC transporter ABCG2 and its function in 5-aminolevulinic acid-mediated protoporphyrin IX accumulation. PLoS One. 2012;7(11):e50082. [CrossRef]
- Ishikawa T, Takahashi K, Ikeda N, Kajimoto Y, Hagiya Y, Ogura S, Miyatake S, Kuroiwa T. Transporter-Mediated Drug Interaction Strategy for 5-Aminolevulinic Acid (ALA)-Based Photodynamic Diagnosis of Malignant Brain Tumor: Molecular Design of ABCG2 Inhibitors. Pharmaceutics. 2011;3(3):615-35. [CrossRef]
- Mansi M, Howley R, Chandratre S, Chen B. Inhibition of ABCG2 transporter by lapatinib enhances 5-aminolevulinic acid-mediated protoporphyrin IX fluorescence and photodynamic therapy response in human glioma cell lines. Biochem Pharmacol. 2022;200:115031. [CrossRef]
- Müller P, Abdel Gaber SA, Zimmermann W, Wittig R, Stepp H. ABCG2 influence on the efficiency of photodynamic therapy in glioblastoma cells. J Photochem Photobiol B. 2020;210:111963. [CrossRef]
- Chandratre S, Olsen J, Howley R, Chen B. Targeting ABCG2 transporter to enhance 5-aminolevulinic acid for tumor visualization and photodynamic therapy. Biochem Pharmacol. 2023;217:115851. [CrossRef]
- de Gooijer MC, de Vries NA, Buckle T, Buil LCM, Beijnen JH, Boogerd W, van Tellingen O. Improved Brain Penetration and Antitumor Efficacy of Temozolomide by Inhibition of ABCB1 and ABCG2. Neoplasia. 2018;20(7):710-720. [CrossRef]
- Deng F, Sjöstedt N, Santo M, Neuvonen M, Niemi M, Kidron H. Novel inhibitors of breast cancer resistance protein (BCRP, ABCG2) among marketed drugs. Eur J Pharm Sci. 2023;181:106362. [CrossRef]
- Nagasaka Y, Oda K, Iwatsubo T, Kawamura A, Usui T. Effects of aripiprazole and its active metabolite dehydroaripiprazole on the activities of drug efflux transporters expressed both in the intestine and at the blood-brain barrier. Biopharm Drug Dispos. 2012;33(6):304-15. [CrossRef]
- Weiss J, Sauer A, Divac N, Herzog M, Schwedhelm E, Böger RH, Haefeli WE, Benndorf RA. Interaction of angiotensin receptor type 1 blockers with ATP-binding cassette transporters. Biopharm Drug Dispos. 2010;31(2-3):150-61. [CrossRef]
- Miyata H, Takada T, Toyoda Y, Matsuo H, Ichida K, Suzuki H. Identification of Febuxostat as a New Strong ABCG2 Inhibitor: Potential Applications and Risks in Clinical Situations. Front Pharmacol. 2016;7:518. [CrossRef]
- Assandri A, Ratti B, Cristina T. Pharmacokinetics of rifapentine, a new long lasting rifamycin, in the rat, the mouse and the rabbit. J Antibiot (Tokyo). 1984;37(9):1066-75. [CrossRef]
- Rodriguez-Perez AI, Sucunza D, Pedrosa MA, Garrido-Gil P, Kulisevsky J, Lanciego JL, Labandeira-Garcia JL. Angiotensin Type 1 Receptor Antagonists Protect Against Alpha-Synuclein-Induced Neuroinflammation and Dopaminergic Neuron Death. Neurotherapeutics. 2018;15(4):1063-1081. [CrossRef]
- Torika N, Asraf K, Danon A, Apte RN, Fleisher-Berkovich S. Telmisartan Modulates Glial Activation: In Vitro and In Vivo Studies. PLoS One. 2016;11(5):e0155823. [CrossRef]
- Ripperger A, Krischer A, Robaa D, Sippl W, Benndorf RA. Pharmacogenetic Aspects of the Interaction of AT1 Receptor Antagonists With ATP-Binding Cassette Transporter ABCG2. Front Pharmacol. 2018;9:463. [CrossRef]
- Hu M, Lee HK, To KK, Fok BS, Wo SK, Ho CS, Wong CK, Zuo Z, Chan TY, Chan JC, Tomlinson B. Telmisartan increases systemic exposure to rosuvastatin after single and multiple doses, and in vitro studies show telmisartan inhibits ABCG2-mediated transport of rosuvastatin. Eur J Clin Pharmacol. 2016;72(12):1471-1478. [CrossRef]
- Salacz ME, Kast RE, Saki N, Brüning A, Karpel-Massler G, Halatsch ME. Toward a noncytotoxic glioblastoma therapy: blocking MCP-1 with the MTZ Regimen. Onco Targets Ther. 2016;9:2535-45. [CrossRef]
- Quan W, Xu CS, Li XC, Yang C, Lan T, Wang MY, Yu DH, Tang F, Wang ZF, Li ZQ. Telmisartan inhibits microglia-induced neurotoxic A1 astrocyte conversion via PPARγ mediated NF-κB/p65 degradation. Int Immunopharmacol. 2023;123:110761.
- . [CrossRef]
- Chang YL, Chou CH, Li YF, Huang LC, Kao Y, Hueng DY, Tsai CK. Antiproliferative and apoptotic effects of telmisartan in human glioma cells. Cancer Cell Int. 2023;23(1):111. [CrossRef]
- Wang Y, Zhang T, Li C, Guo J, Xu B, Xue L. Telmisartan attenuates human glioblastoma cells proliferation and oncogenicity by inducing the lipid oxidation. Asia Pac J Clin Oncol. 2022;18(3):217-223. [CrossRef]
- Paul SK, Guendouzi A, Banerjee A, Guendouzi A, Haldar R. Identification of approved drugs with ALDH1A1 inhibitory potential aimed at enhancing chemotherapy sensitivity in cancer cells: an in-silico drug repurposing approach. J Biomol Struct Dyn. 2024:1-15. [CrossRef]
- Kumar U, Aich J, Devarajan S. Exploring the repurposing potential of telmisartan drug in breast cancer: an in-silico and in-vitro approach. Anticancer Drugs. 2023;34(10):1094-1103. [CrossRef]
- Yamana Y, Fujihara S, Kobara H, Oura K, Samukawa E, Chiyo T, Okamura M, Yamana H, Tadokoro T, Fujita K, Morishita A, Iwama H, Masaki T. MicroRNA profiles following telmisartan treatment in pancreatic ductal adenocarcinoma cells. J Cancer Res Ther. 2022;18(Supplement):S305-S312. [CrossRef]
- Khorsand M, Mostafavi-Pour Z, Razban V, Khajeh S, Zare R. Combinatorial effects of telmisartan and docetaxel on cell viability and metastatic gene expression in human prostate and breast cancer cells. Mol Biol Res Commun. 2022;11(1):11-20. [CrossRef]
- Khorsand M, Khajeh S, Eslami M, Nezafat N, Ghasemi Y, Razban V, Mostafavi-Pour Z. Telmisartan anti-cancer activities mechanism through targeting N-cadherin by mimicking ADH-1 function. J Cell Mol Med. 2022;26(8):2392-2403. [CrossRef]
- Tsujiya Y, Hasegawa A, Yamamori M, Okamura N. Telmisartan-Induced Cytotoxicity via G2/M Phase Arrest in Renal Cell Carcinoma Cell Lines. Biol Pharm Bull. 2021;44(12):1878-1885. [CrossRef]
- Tsujiya Y, Yamamori M, Hasegawa AI, Yamamoto Y, Yashiro M, Okamura N. Telmisartan Exerts Cytotoxicity in Scirrhous Gastric Cancer Cells by Inducing G0/G1 Cell Cycle Arrest. Anticancer Res. 2021;41(11):5461-5468. [CrossRef]
- Kast RE, Ellingson BM, Marosi C, Halatsch ME. Glioblastoma treatment using perphenazine to block the subventricular zone's tumor trophic functions. J Neurooncol. 2014;116(2):207-12. [CrossRef]
- Kast RE. Adding perphenazine to increase effectiveness of standard glioblastoma chemoirradiation. J BUON. 2020;25(4):1676-1686.
- Jeon HM, Oh YT, Shin YJ, Chang N, Kim D, Woo D, Yeup Y, Joo KM, Jo H, Yang H, Lee JK, Kang W, Sa J, Lee WJ, Hale J, Lathia JD, Purow B, Park MJ, Park JB, Nam DH, Lee J. Dopamine receptor D2 regulates glioblastoma survival and death through MET and death receptor 4/5. Neoplasia. 2023;39:100894. [CrossRef]
- Wang Y, Wang X, Wang K, Qi J, Zhang Y, Wang X, Zhang L, Zhou Y, Gu L, Yu R, Zhou X. Chronic stress accelerates glioblastoma progression via DRD2/ERK/β-catenin axis and Dopamine/ERK/TH positive feedback loop. J Exp Clin Cancer Res. 2023;42(1):161. [CrossRef]
- Weissenrieder JS, Reed JL, Green MV, Moldovan GL, Koubek EJ, Neighbors JD, Hohl RJ. The Dopamine D2 Receptor Contributes to the Spheroid Formation Behavior of U87 Glioblastoma Cells. Pharmacology. 2020;105(1-2):19-27. [CrossRef]
- He Y, Li J, Koga T, Ma J, Dhawan S, Suzuki Y, Furnari F, Prabhu VV, Allen JE, Chen CC. Epidermal growth factor receptor as a molecular determinant of glioblastoma response to dopamine receptor D2 inhibitors. Neuro Oncol. 2021;23(3):400-411. [CrossRef]
- Liu Z, Jiang X, Gao L, Liu X, Li J, Huang X, Zeng T. Synergistic Suppression of Glioblastoma Cell Growth by Combined Application of Temozolomide and Dopamine D2 Receptor Antagonists. World Neurosurg. 2019;128:e468-e477. [CrossRef]
- Shi L, Chen H, Chen K, Zhong C, Song C, Huang Y, Wang T, Chen L, Li C, Huang A, Qi S, Li H, Lu Y. The DRD2 Antagonist Haloperidol Mediates Autophagy-Induced Ferroptosis to Increase Temozolomide Sensitivity by Promoting Endoplasmic Reticulum Stress in Glioblastoma. Clin Cancer Res. 2023;29(16):3172-3188.
- . [CrossRef]
- Awuah WA, Kalmanovich J, Mehta A, Huang H, Abdul-Rahman T, Cheng Ng J, Yarlagadda R, Kamanousa K, Kundu M, Nansubuga EP, Hasan MM, Lyndin M, Isik A, Sikora V, Alexiou A. Multilevel Pharmacological Effects of Antipsychotics in Potential Glioblastoma Treatment. Curr Top Med Chem. 2023;23(5):389-402. [CrossRef]
- Caragher SP, Shireman JM, Huang M, Miska J, Atashi F, Baisiwala S, Hong Park C, Saathoff MR, Warnke L, Xiao T, Lesniak MS, James CD, Meltzer H, Tryba AK, Ahmed AU. Activation of Dopamine Receptor 2 Prompts Transcriptomic and Metabolic Plasticity in Glioblastoma. J Neurosci. 2019;39(11):1982-1993. [CrossRef]
- Abbruzzese C, Matteoni S, Persico M, Villani V, Paggi MG. Repurposing chlorpromazine in the treatment of glioblastoma multiforme: analysis of literature and forthcoming steps. J Exp Clin Cancer Res. 2020;39(1):26. [CrossRef]
- Pinheiro T, Otrocka M, Seashore-Ludlow B, Rraklli V, Holmberg J, Forsberg-Nilsson K, Simon A, Kirkham M. A chemical screen identifies trifluoperazine as an inhibitor of glioblastoma growth. Biochem Biophys Res Commun. 2017;494(3-4):477-483. [CrossRef]
- Salvalaggio A, Pini L, Bertoldo A, Corbetta M. Glioblastoma and brain connectivity: the need for a paradigm shift. Lancet Neurol. 2024;23(7):740-748. [CrossRef]
- Broekman ML, Maas SLN, Abels ER, Mempel TR, Krichevsky AM, Breakefield XO. Multidimensional communication in the microenvirons of glioblastoma. Nat Rev Neurol. 2018;14(8):482-495. [CrossRef]
- White J, White MPJ, Wickremesekera A, Peng L, Gray C. The tumour microenvironment, treatment resistance and recurrence in glioblastoma. J Transl Med. 2024;22(1):540. [CrossRef]
- Kast RE, Alfieri A, Assi HI, Burns TC, Elyamany AM, Gonzalez-Cao M, Karpel-Massler G, Marosi C, Salacz ME, Sardi I, Van Vlierberghe P, Zaghloul MS, Halatsch ME. MDACT: A New Principle of Adjunctive Cancer Treatment Using Combinations of Multiple Repurposed Drugs, with an Example Regimen. Cancers (Basel). 2022;14(10):2563. [CrossRef]
- Rumie Vittar NB, Lamberti MJ, Pansa MF, Vera RE, Rodriguez ME, Cogno IS, Milla Sanabria LN, Rivarola VA. Ecological photodynamic therapy: new trend to disrupt the intricate networks within tumor ecosystem. Biochim Biophys Acta. 2013;1835(1):86-99. [CrossRef]
- Duenas-Gonzalez A, Gonzalez-Fierro A, Bornstein-Quevedo L, Gutierrez-Delgado F, Kast RE, Chavez-Blanco A, Dominguez-Gomez G, Candelaria M, Romo-Pérez A, Correa-Basurto J, Lizano M, Perez-de la Cruz V, Robles-Bañuelos B, Nuñez-Corona D, Martinez-Perez E, Verastegui E. Multitargeted polypharmacotherapy for cancer treatment. theoretical concepts and proposals. Expert Rev Anticancer Ther. 2024:1-13. [CrossRef]
- Prager BC, Bhargava S, Mahadev V, Hubert CG, Rich JN. Glioblastoma Stem Cells: Driving Resilience through Chaos. Trends Cancer. 2020;6(3):223-235. [CrossRef]
- Gimple RC, Bhargava S, Dixit D, Rich JN. Glioblastoma stem cells: lessons from the tumor hierarchy in a lethal cancer. Genes Dev. 2019;33(11-12):591-609. [CrossRef]
- Vilchez ML, Rodríguez LB, Palacios RE, Prucca CG, Caverzán MD, Caputto BL, Rivarola VA, Milla Sanabria LN. Isolation and initial characterization of human glioblastoma cells resistant to photodynamic therapy. Photodiagnosis Photodyn Ther. 2021;33:102097. [CrossRef]
- Rodríguez Aguilar L, Vilchez ML, Milla Sanabria LN. Targeting glioblastoma stem cells: The first step of photodynamic therapy. Photodiagnosis Photodyn Ther. 2021;36:102585. [CrossRef]
- Omura N, Nonoguchi N, Fujishiro T, Park Y, Ikeda N, Kajimoto Y, Hosomi R, Yagi R, Hiramatsu R, Furuse M, Kawabata S, Fukunaga K, Kuroiwa T, Nakano I, Wanibuchi M. Ablation efficacy of 5-aminolevulinic acid-mediated photodynamic therapy on human glioma stem cells. Photodiagnosis Photodyn Ther. 2023;41:103119. [CrossRef]
- Schimanski A, Ebbert L, Sabel MC, Finocchiaro G, Lamszus K, Ewelt C, Etminan N, Fischer JC, Sorg RV. Human glioblastoma stem-like cells accumulate protoporphyrin IX when subjected to exogenous 5-aminolaevulinic acid, rendering them sensitive to photodynamic treatment. J Photochem Photobiol B. 2016;163:203-10. [CrossRef]
- Kawai N, Hirohashi Y, Ebihara Y, Saito T, Murai A, Saito T, Shirosaki T, Kubo T, Nakatsugawa M, Kanaseki T, Tsukahara T, Shichinohe T, Li L, Hirano S, Torigoe T. ABCG2 expression is related to low 5-ALA photodynamic diagnosis (PDD) efficacy and cancer stem cell phenotype, and suppression of ABCG2 improves the efficacy of PDD. PLoS One. 2019;14(5):e0216503. [CrossRef]
- Fujishiro T, Nonoguchi N, Pavliukov M, Ohmura N, Kawabata S, Park Y, Kajimoto Y, Ishikawa T, Nakano I, Kuroiwa T. 5-Aminolevulinic acid-mediated photodynamic therapy can target human glioma stem-like cells refractory to antineoplastic agents. Photodiagnosis Photodyn Ther. 2018;24:58-68. [CrossRef]
- Spring BQ, Watanabe K, Ichikawa M, Mallidi S, Matsudaira T, Timerman D, Swain JWR, Mai Z, Wakimoto H, Hasan T. Red light-activated depletion of drug-refractory glioblastoma stem cells and chemosensitization of an acquired-resistant mesenchymal phenotype. Photochem Photobiol. 2024 Jun 23. [CrossRef]
- Rogers, GS. Continuous low-irradiance photodynamic therapy: a new therapeutic paradigm. J Natl Compr Canc Netw. 2012;10 Suppl 2:S14-7. [CrossRef]
- Nairuz T, Sangwoo-Cho, Lee JH. Photobiomodulation Therapy on Brain: Pioneering an Innovative Approach to Revolutionize Cognitive Dynamics. Cells. 2024;13(11):966. [CrossRef]
- Johnson PK, Fino PC, Wilde EA, Hovenden ES, Russell HA, Velez C, Pelo R, Morris AJ, Kreter N, Read EN, Keleher F, Esopenko C, Lindsey HM, Newsome MR, Thayn D, McCabe C, Mullen CM, Davidson LE, Liebel SW, Carr L, Tate DF. The Effect of Intranasal Plus Transcranial Photobiomodulation on Neuromuscular Control in Individuals with Repetitive Head Acceleration Events. Photobiomodul Photomed Laser Surg. 2024;42(6):404-413. [CrossRef]
- Chan ST, Mercaldo N, Figueiro Longo MG, Welt J, Avesta A, Lee J, Lev MH, Ratai EM, Wenke MR, Parry BA, Drake L, Anderson RR, Rauch T, Diaz-Arrastia R, Kwong KK, Hamblin M, Vakoc BJ, Gupta R. Effects of Low-Level Light Therapy on Resting-State Connectivity Following Moderate Traumatic Brain Injury: Secondary Analyses of a Double-blinded Placebo-controlled Study. Radiology. 2024;311(2):e230999. [CrossRef]
- Shahdadian S, Wang X, Liu H. Directed physiological networks in the human prefrontal cortex at rest and post transcranial photobiomodulation. Sci Rep. 2024;14(1):10242. [CrossRef]
- Kim JH, Son HS, Yu DA, Choe YB, Lee YW. Assessment of Effects of Low-Level Light Therapy on Scalp Condition and Hair Growth. Indian J Dermatol. 2023;68(4):487. [CrossRef]
- Estrada-Rojas K, Cedeño Ortiz NP. Increased Improvement in Speech-Language Skills After Transcranial Photobiomodulation Plus Speech-Language Therapy, Compared to Speech-Language Therapy Alone: Case Report with Aphasia. Photobiomodul Photomed Laser Surg. 2023;41(5):234-240. [CrossRef]
- Frost GA, Halliday GM, Damian DL. Photodynamic therapy-induced immunosuppression in humans is prevented by reducing the rate of light delivery. J Invest Dermatol. 2011;131(4):962-8. [CrossRef]
Figure 1.
Schematic drawing of transcranial 630 nm LED illumination of GB. The schematic indicates beams of light but the strong light diffusion by brain tissue results in light hitting the GB resection area from many angles.
Figure 1.
Schematic drawing of transcranial 630 nm LED illumination of GB. The schematic indicates beams of light but the strong light diffusion by brain tissue results in light hitting the GB resection area from many angles.
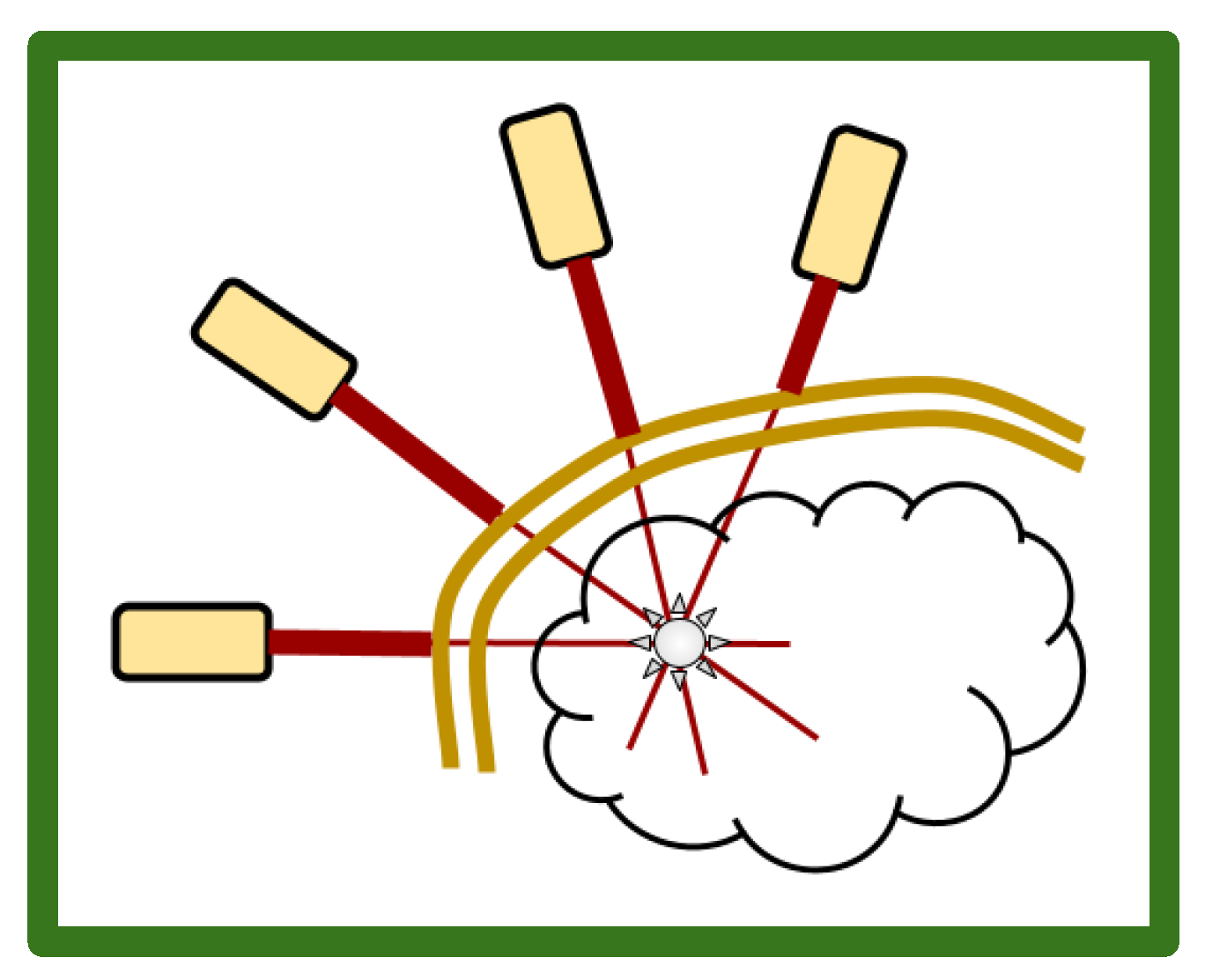
Figure 2.
A simplified schematic of 5-ALA entry into GB cells and its indirect action in creating cytotoxic ROS after cells’ exposure to EM irradiation. By inhibiting 5-ALA export, febuxostat increases intracellular 5-ALA. By inhibiting diversion of PpIX to heme synthesis, deferiprone increases intracellular PpIX.
Figure 2.
A simplified schematic of 5-ALA entry into GB cells and its indirect action in creating cytotoxic ROS after cells’ exposure to EM irradiation. By inhibiting 5-ALA export, febuxostat increases intracellular 5-ALA. By inhibiting diversion of PpIX to heme synthesis, deferiprone increases intracellular PpIX.
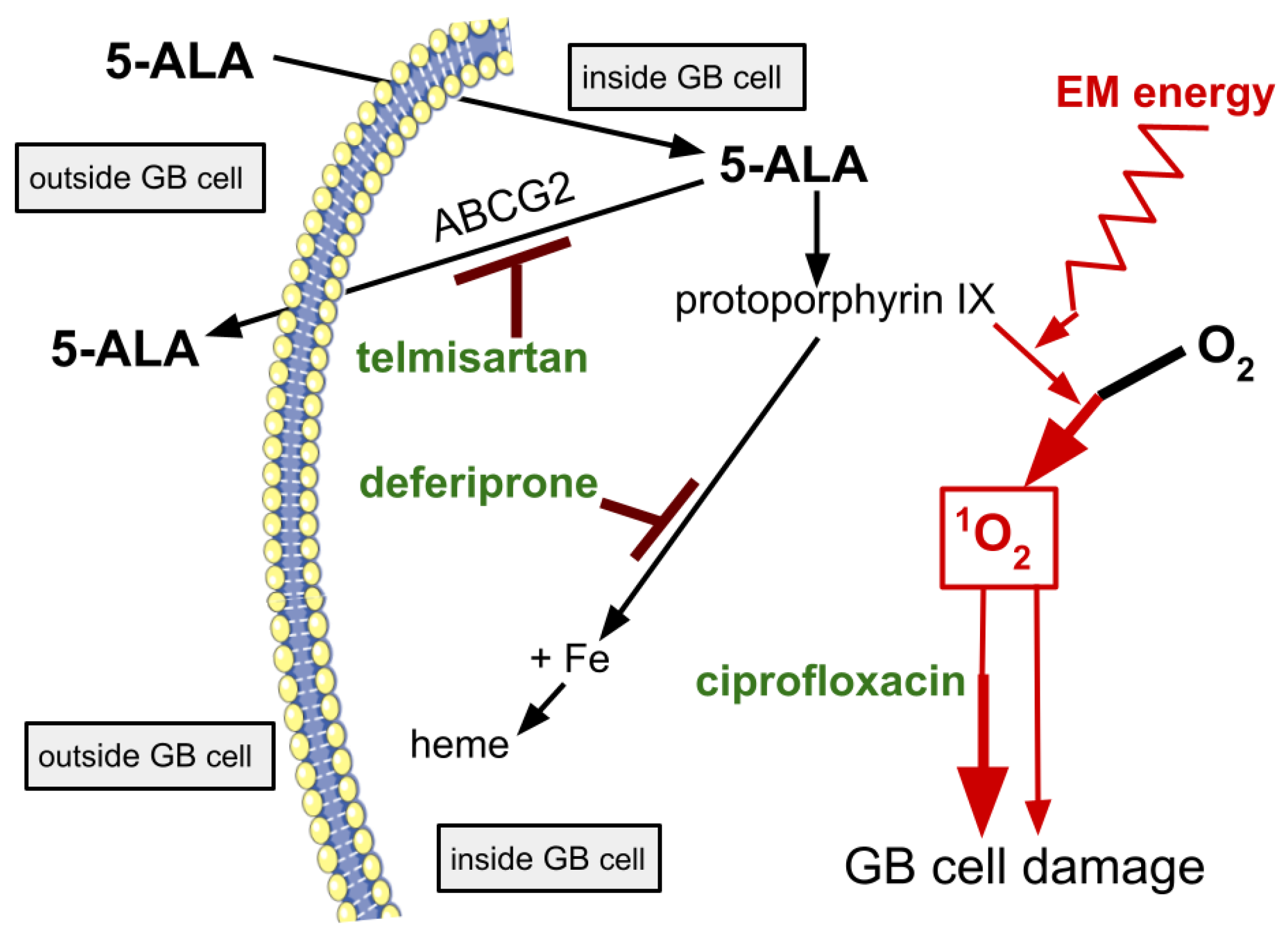

Table 1.
Glossary of some oxygen related terms.
| O2 | ground state triplet oxygen molecule, 3O2 stable, atmospheric oxygen |
| 3O2 | another designation of O2, the common form of atmospheric oxygen. |
| •OH | hydroxyl radical, a neutral, highly reactive ROS. |
| 1O2 | singlet oxygen molecule, half-life of microseconds, an ROS. |
| O2 •− | superoxide anion radical, an oxygen molecule with one unpaired outer shell electron, negative charge −1, an ROS. |
| O3 | ozone, trioxygen molecule, an ROS. |
| H2O2 | hydrogen peroxide, a non radical, non ionic, ROS. |
Table 2.
Light dosing terms defined. .
| term | definition | units |
| fluence | the energy delivered to a given area | J / cm2 |
| flux | the momentary power received by a given area | W / cm2 |
| irradiance | the momentary power received by a given area | W / cm2 |
| light dose | J/cm2 delivered over a specified time interval | J / cm2 |
Note: we speak of area and denote per cm2 but we are really referring to a volume of tissue, cm3 , with the understanding that tumor tissue proximal to light sources will receive slightly greater energy, the tumor tissue distal to the light source slightly less energy.
Table 3.
Incident power density (flux) of 630 nm light at the scalp skin surface required to deliver 17 µW / cm2 to GB tumor tissue at the listed brain depths deep to the scalp surface. Values calculated according to the attenuation formula.
Table 3.
Incident power density (flux) of 630 nm light at the scalp skin surface required to deliver 17 µW / cm2 to GB tumor tissue at the listed brain depths deep to the scalp surface. Values calculated according to the attenuation formula.
| GB tissue depth |
external flux required to achieve 17 µW / cm2 |
|---|---|
| at 3 cm ➞ | 1.4 mW / cm2 |
| at 5 cm ➞ | 3.3 mW / cm2 |
| at 7 cm ➞ | 7.5 mW / cm2 |
| at 9 cm ➞ | 17 mW / cm2 |
Table 4.
List of the three augmentation drugs with their general medical use and their use in LIT-PDT.
Table 4.
List of the three augmentation drugs with their general medical use and their use in LIT-PDT.
| drug | general medicine use | use in LIT-PDT |
|---|---|---|
| ciprofloxacin | antibiotic | increased protoporphyrin |
| deferiprone | iron chelation | iron chelation |
| telmisartan | hypertension | ABCG2 inhibition |
| ziprasidone | psychosis | D2 blocking |
Table 5.
An illustrative example of a possible schedule of events for the first GB case in a planned phased pilot study of LIT-PDT. This will be done without drug augmentation. Drug augmentation would start after safety of a transcranial illumination regimen has been established. PDT duration of this first use is predicted as 32 hours.
Table 5.
An illustrative example of a possible schedule of events for the first GB case in a planned phased pilot study of LIT-PDT. This will be done without drug augmentation. Drug augmentation would start after safety of a transcranial illumination regimen has been established. PDT duration of this first use is predicted as 32 hours.
| time | 5-ALA dose | illumination |
|---|---|---|
| - 36 hr | 1st 20 mg/kg p.o. | off |
| -33 hr | none | on |
| -28 hr | 2nd 20 mg/kg p.o | on |
| -9 hr | 3rd 20 mg/kg p.o. | on |
| -1 hr | none | off |
| 0 hr - surgery | none | off |
| + 4 hr, H&E, etc | none | off |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



