
Submitted:
24 July 2024
Posted:
25 July 2024
You are already at the latest version
Abstract
Community Acquired Urinary Tract Infections account for 15% of all outpatient use of antibiotics, women are primarily affected; major causative microorganisms are uro-pathogenic E. Coli. Treatment is indicated for cystitis and pyelonephritis and includes B-lactams (amoxicillin-clavulanic acid or third generation cephalosporins), fluoroquin-olones (ciprofloxacin or levofloxacin), nitrofurantoin, fosfomycin, and trime-thoprim-sulfamethoxazole. Resistance to antibiotic treatment is of concern, several mecha-nisms have been associated with the acquisition of genes that confer antimicrobial re-sistance to fluoroquinolones, which often are associated with other patterns of resistance, especially in extended spectrum beta lactases (ESBL) producers. Several studies have ad-dressed the prevalence of uropathogens producing ESBL, but only a few have focused on resistance against fluoroquinolones and to our knowledge, none has been addressing the prevalence of isolates mutations that confer antimicrobial resistance to fluoroquinolones. The focus of the present review was to analyze recent published papers that describe the E. coli phylotype causing community acquired UTIs in association to fluoroquinolones re-sistance.
Keywords:
fluoroquinolone resistance
; urinary tract infections
; systematic review
; Escherichia coli
; community acquired bacterial infection
1. Introduction
Urinary tract infections (UTIs) account for approximately 3 million visits to health services annually and are responsible for up to 15% of all outpatient use of antibiotics in the United States [1]. They are considered the most prevalent community acquired (CA) bacterial infection [2]. Women are primarily affected, and majorly prevalent causative microorganisms are Escherichia coli (E. coli), Enterococcus, Staphylococcus, Proteus, Klebsiella, and Pseudomonas in order of frequency, with uropathogenic E. coli (UPEC) being the causative agent more than three-quarters of yearly UTIs [3,4]. Community-acquired UTI is defined as one presenting in outpatient clinics or primary care or at presentation to the emergency department, without prior hospitalization for the index episode, excluding patients in residential/long-term-care facilities.
Treatment is indicated for cystitis and pyelonephritis and includes B-lactams (amoxicillin-clavulanic acid or third generation cephalosporins), fluoroquinolones (ciprofloxacin or levofloxacin), nitrofurantoin, fosfomycin, and trimethoprim-sulfamethoxazole [5]. UTIs are the main cause of antibiotic consumption which is a concern since the widespread use of antibiotics has led to the growth of antimicrobial resistance in UPEC and other uropathogens, which has led to complications in treatment, prevention, and management of recurrent UTIs. Fluoroquinolones have the advantage of availability in both oral and parenteral forms, good absorption, and high urinary excretion rate [6] Figure 1. However, due to resistance, available guidelines, published in 2010, recommend the use of nitrofurantoin, fosfomycin, and trimethoprim-sulfamethoxazole for empirical therapy of acute uncomplicated cystitis [7].
Resistance against fluoroquinolones can occur as a result of either of the following 3 mechanisms: 1) chromosomal mutations that change the targets of the drug, such as the genes that codify for GyrA (a subunit from DNA gyrase), or ParC (subunit from topoisomerase IV); 2) mutations related to reduce the drug concentration in the bacterial cytoplasm through overexpression of efflux pumps and downregulation of porins; and 3) expression of genes that codify from plasmid mediated quinolone resistance proteins (PMQR), such as qnr, aac(6’)-lb-cr, quepA and oqxAB [8] (Figure 2).
PMQR mechanisms usually confer low-level resistance, but either alone or with chromosomal target mutations, they widen the selection window, and increase the minimum inhibitor concentration (MIC) of the strains and facilitate selection of higher level of resistance. Furthermore, the presence of plasmids carries genes encoding for resistance to other antimicrobials such as beta-lactams and aminoglycosides [9].
Antimicrobial resistance genes (ARGs) can be shared among E. coli strains via mobile genetic elements, which includes transposons, plasmids, the insertion of sequences and genomic islands [10]. Irrespective of the mechanism, the transmission of these elements will lead to a recombination among different E. coli strains. The current classification for identifying the phylogenetic order of E. coli strains is based on the presence or absence of four genetic sequences named chuA, yjaA, TspE4 and arpA; into phylotypes A, B1, B2, D, C, E, F, G, and Escherichia cryptic clade I [11]. Strains of UPEC pathotype usually belong to phylotypes B2 and D, but intestinal pathogenic and commensal E. coli strains belong to A and B1 [12].
Another factor related to the development of resistance in E. coli, is the use of antibiotics in veterinary medicine for food-producing animals, as a member of the gut microbiota E. coli that is resistant to antibiotics can be transmitted through the food chain or directly to humans. Or the animal product itself could contain the antibiotic residues promoting contact with humans and promoting the development of resistant bacteria [13]. Although this last factor has been more frequently associated with the production of extended spectrum beta lactamases (ESBL).
Several studies have addressed the presence of resistance against B-lactamases or the prevalence of uropathogens producing ESBL, but only a few have focused on resistance against fluoroquinolones and to our knowledge, none has been addressing the prevalence of isolates mutations that confer antimicrobial resistance to fluoroquinolones. The focus of the present review was to analyze recent published papers that describe the E. coli phylotype causing community acquired UTIs in association to fluoroquinolones resistance.
2. Materials and Methods
This systematic review was developed according to PRISMA guidelines [14]. We used PubMed to conduct searches and identify candidate studies to be included in the review. Keywords were obtained from Mesh terminology, and we used a combination of several terms to conduct searches. The terms included “community acquired infection” AND “urinary tract infection” AND “fluoroquinolones” AND “antimicrobial drug resistance” AND “antimicrobial resistance genes”. Papers were selected using filters to include recent (last 5 years), English or Spanish language, studies in adults. Which yielded 18 results, papers were downloaded and analyzed to meet additional inclusion criteria such as having an observational design, and performed with validated methods for urine culture, susceptibility testing and gene expression.
We included papers that reported on fluoroquinolones resistance for uropathogens causing community acquired urinary tract infections. A library was created in EndNote and duplicates were removed (2 duplicates found). Data extracted from selected studies included country of the study, study setting, time frame, patient demographics, uropathogens isolated, antimicrobial susceptibility, and mutations prevalence related to antimicrobial resistance. Some studies were eliminated or excluded because it was not possible to distinguish patterns of resistance between community acquired and hospital acquired UTIs, or because the resistance pattern included mixed pathogens.
3. Results
The number of papers selected at each stage is described in PRISMA flow diagram (Figure 3). A total of 19 studies were included in this systematic review.
The total amount of papers was selected from a wide distribution of studies around the world, obtaining 5 papers from North America, 3 from South America, 5 from Europe and 6 from the Asian Region.
Of the studies analyzed, they were performed during a minimum period of 1 month as the case of Brazil, where it was performed in November 2015 [15] and Romania during June, 2018 [16], the longest period was 5 years and was performed in Canada from 2015 to 2019 [17] and Saudi Arabia during the same period [3].
Of the 19 studies, only 5 mentioned phylotype. The most common phylotype was B2.
10 studies refer to antimicrobial resistance genes (ARGs), the most common AR genes were blaCTX-M and blaTEM. Only 11 studies mentioned ESBL producing strains. 2 studies from Asia (Turkey, Egypt) mentioned genes that codify from plasmid mediated quinolone resistance proteins (PMQR), such as qnr, aac (6’)-lb-cr, quepA and oqxAB. The most common PMQR were qnrS and qnrB. The countries with highest resistance rates were Bangladesh (69%) follow by Iran (55.6%).
4. Discussion
Fluoroquinolone resistance emerged in the mid-1990s due to their extensive use, for the following couple of decades its resistance continued to increase [18]. Up-to-date information points toward a decreased rate in the United States (7%), a higher incidence in Europe and Asia (28%), and the highest rates are found in developing countries [6]. Others results revealed a high rate of fluoroquinolone resistance in UPEC in India (>60%). For 2014 Europe, resistance to fluoroquinolone was reported in 22% of strains, In Poland, resistance to fluoroquinolone was observed in about 30% of UPEC and in Germany 2013–2014, the percentage of ciprofloxacin-resistant UPEC strains was 17.3%. In America for 2013–2014 in Brazil 18.8% outpatients were resistant to ciprofloxacin [19].Our review is consistent with these previous findings, although percentages have changed over the las five years. Nevertheless, the global burden of drug-resistant infections is enormous, both in terms of mortality and financial costs. Globally, it has been estimated that 700,000 people die each year, due to drug resistance, and approximately 23,000 of them happen in the United States. The Centers for Disease Control and Prevention estimate the cost of antimicrobial resistance in the United States to be of 55 billion dollars each year [20].
The presence of a drug-resistant strain in an individual may arise by direct infection with a drug resistant strain, or alternatively the sensitive strain may mutate during a single infection and become resistant during transient treatment with fluoroquinolones [21].
The phenotypic antibiotic resistance of uropathogens causing UTIs is of importance to make informed based decisions and to determine the causes of such changes in incidences according to the region. Table 1 depicts a summary of the studies found addressing this issue.
4.1. Reported Resistance Rates and in Community Acquired Uncomplicated Urinary Tract Infections
A recent systematic review, related to E. coli resistance to fluoroquinolones in uCA-UTIs in women, found that ciprofloxacin resistance in isolates varies by countries but nevertheless tends are rising across the time, specifically in the United Kingdom, where it raised from 0.5% in 2008 to 15.3% in 2016; in Spain from 22.9 to 30.8%, and Germany 8.5 to 15.1%. Furthermore, in Asia a substantial increase was reported to ciprofloxacin from 25% in 2008 to 40% in 2014; with the highest percentage of resistance reported in Bangladesh (69%) [33]. A retrospective study conducted in China found a resistance rate to ciprofloxacin in UPEC to be from 55-70% in a study period from 2012-2019 [35].
While in North America resistance increased from 4% in 2008 to 12% in 2017 [36]. Our review found a decrease resistance from 18% to 14.2% in recurrent UTIs and 8.6% in non-recurrent UTIs in the United States [24], while in Canada resistance rates seem to be higher and related to regions [17]. Fluoroquinolone resistance rates in patients with uCA-UTIs in Turkey reported an increase from 20-30% in 1996 to 52% in adults with CA-UTIs in 2020 [2].
In our country, a previous study performed in 2020 reported less than 40% of isolated strains to be resistant to ciprofloxacin, although this resistance was in ESBL producers [25].
Additional studies performed in Latin America, specifically in Uruguay found that up to 13.6% of E. coli isolates causing CA-UTI in adults were resistant to Ciprofloxacin in 2014 [37]. However, in our review we found trends of fluoroquinolones resistance from 15-29% for the treatment of community acquired uUTIs [26,27].
4.2. Plasmidic Fluoroquinolone Resistance Genes and Phylotypes Prevalence
A study performed in samples from 168 Iranian women with community acquired uncomplicated UTIs demonstrated a high prevalence of resistance against cefotaxime and aztreonam and the lowest rates of resistance were associated to ciprofloxacin. In this same study phylotypes of E. coli isolated were B2>D>E>F>B1>C>A [13].
In 2013, a study performed in Algeria reported the presence of mutations in E. coli associated with resistance to fluoroquinolones, they found up to 56.66% of isolates carrying mutations in gyrA and parC [38].
More recently, a study performed in Egypt (2016-2017) found higher frequencies of the gene qnrB (100%); QnrS gene was detected in 74.4%, and qepA gene in 10% in samples form community and hospital acquired UTIs [34].
A study performed in Turkey aimed at investigating the frequency of plasmid mediated fluoroquinolone resistance (PMFR) genes in ESBL producing E. coli strains isolated from pediatric and adult patients with UTI, they found that up to one third (92/258) of all isolates carried at least one PMFR gene, the most prevalent was qnrS in 67.4% of isolates [2]. A second study from Turkey, performed in 2019, found that the most prevalent clone responsible for UTI was E. coli clone O25b-ST131 (22%), which bared in up to 73%, the gene CTX-M-1 and in 37% the gene CTX-M-15 [32].
Studies from Venezuela and Brazil detected the same genes, blaTEM and blaSHV in E. coli isolates, while the blaCTX-M gene was only found in ESBL-producing isolates mainly in community acquired UTIs [15,26].
A metanalysis performed in 2022, reported an increase in the trend for phylotype B2 incidence, during the years 2014-2020 around the world. The authors’ discussion was around the presence of additional risk factors such as host species, nutrition, type of infection, geographical regions to explain the variation in phylotype frequency of E. coli [39]. With respect to this phylotype a study in Bucharest, Romania, performed in 2019, showed that up to 35% of the causative agent for CA-UTI was phylotype B2, 27% B1, and 22% phylotype A. They also investigated ESBL genes and found: blaCTM-M in 42.25%, blaTEM in 38.02% and finally blaSHV in 19.71% [16]. In Iran, during the spring of 2021, the prevalence of E. coli resistance genes was determined with the following percentages of the resistance genes blaTEM in 89.6%; blaCTX-M in 44.3%; blaSHV in 6.6% and blaCMY in 0.9%. The most frequent phylotypes was B2 in 29.2% and D in 17.9% [13].
4.3. Risk Factors Identified for Resistance
Fluoroquinolone resistant infections are often associated with known risk factors such as recent use of fluoroquinolones, subjects living in long-term care facilities or hospitalized patients, pregnancy, male patients, immunocompromised or those who have current or pre-existing functional or anatomical urinary tract abnormalities, advanced age, large prostate size, and high post-void residual volumes, hypertension and diabetes [25,37,40].
A systematic review found that in women with uCA-UTIs caused by isolates resistant to fluoroquinolones a risk factor could be post-menopausal or women with UTI recurrence [36]. Being a female could be a risk factor due to the anatomy of the female tract. The female urethra, which is shorter and closer to the anus, is the main reason why UTIs are more common in adolescents, adults and older women [3].
After the conduction of this present review, we found higher percentage of resistance to fluoroquinolones in Asian countries, these countries might have risk factors that they share and make them more vulnerable to develop an increase in resistance rates, such as a frequent non-prescription antimicrobial use [2].
Additional studies, performed in Europe have suggested regional difference with respect to ESBL positive isolates, with the identification of variables related to subjects (age), the environment, and antibiotic use in the last 3 months to determine the presence of this variants [41].
With respect to environmental factors, others have explored the possibility of regions with circulation of already resistant genotypes, which might be present in contaminated food, and promote person to person, propagation of the resistant pathogen [15]. Supporting the last variable, related to antibiotic use in the previous months, Dobbyn et al., found that in Canada, regions with better fluoroquinolone susceptibility were areas with more strict antibiotic prescribing regulations [17].
For older males, being susceptible to recurrent UTIs another mentioned risk factor that relates to bladder outlet obstruction is prostate enlargement, the recurrency of UTIs as well as antibiotic use have both been associated with antibiotic resistance [33]. In addition to this, travel and swimming have also been identified as risk factors for acquiring ESBL producing E. coli strains [13].
5. Conclusions
Fluoroquinolone resistance rates highlight the significance of local resistance monitoring and the investigation of underlying mechanism, including local prescription regulations, use in the setting of complicated infections, restrict their use in veterinary medicine and highlight the importance of a rational use of antimicrobials. This review offers some information related to resistant genes and bacterial phylotypes that can be useful to compare trends in the coming years.
Author Contributions
Conceptualization, M.G.Z; methodology, M.G.Z; software, A.R, F.C, A.N, P.C, L-V, and M.G.Z; validation, A.R, F.C, and M.G.Z; formal analysis, A.R, F.C, A.N, P.C, L-V, and M.G.Z; data curation, A.R, F.C, and M.G.Z; writing—original draft preparation, A.R, F.C, A.N, P.C, L-V, and M.G.Z; writing—review and editing, A.R, F.C, and M.G.Z; supervision, M.G.Z.
All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Takhar, S.S.; Moran, G.J. Diagnosis and management of urinary tract infection in the emergency department and outpatient settings. Infect Dis Clin North Am 2014, 28, 33–48. [Google Scholar] [CrossRef]
- Akgoz, M.; Akman, I.; Ates, A.B.; Celik, C.; Keskin, B.; Ozmen Capin, B.B.; Karahan, Z.C. Plasmidic Fluoroquinolone Resistance Genes in Fluoroquinolone-Resistant and/or Extended Spectrum Beta-Lactamase-Producing Escherichia coli Strains Isolated from Pediatric and Adult Patients Diagnosed with Urinary Tract Infection. Microb Drug Resist 2020, 26, 1334–1341. [Google Scholar] [CrossRef]
- Bazaid, A.S.; Saeed, A.; Alrashidi, A.; Alrashidi, A.; Alshaghdali, K.; S, A.H.; Alreshidi, T.; Alshammary, M.; Alarfaj, A.; Thallab, R.; et al. Antimicrobial Surveillance for Bacterial Uropathogens in Ha’il, Saudi Arabia: A Five-Year Multicenter Retrospective Study. Infect Drug Resist 2021, 14, 1455–1465. [Google Scholar] [CrossRef]
- Ozturk, R.; Murt, A. Epidemiology of urological infections: a global burden. World J Urol 2020, 38, 2669–2679. [Google Scholar] [CrossRef]
- Chardavoyne, P.C.; Kasmire, K.E. Appropriateness of Antibiotic Prescriptions for Urinary Tract Infections. West J Emerg Med 2020, 21, 633–639. [Google Scholar] [CrossRef]
- Fasugba, O.; Gardner, A.; Mitchell, B.G.; Mnatzaganian, G. Ciprofloxacin resistance in community- and hospital-acquired Escherichia coli urinary tract infections: a systematic review and meta-analysis of observational studies. BMC Infect Dis 2015, 15, 545. [Google Scholar] [CrossRef]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis 2011, 52, e103–120. [Google Scholar] [CrossRef]
- Han, J.H.; Nachamkin, I.; Tolomeo, P.; Mao, X.; Bilker, W.B.; Lautenbach, E. Temporal changes in resistance mechanisms in colonizing Escherichia coli isolates with reduced susceptibility to fluoroquinolones. Diagn Microbiol Infect Dis 2013, 76, 491–496. [Google Scholar] [CrossRef]
- Jacoby, G.A.; Strahilevitz, J.; Hooper, D.C. Plasmid-mediated quinolone resistance. Microbiol Spectr 2014, 2. [Google Scholar] [CrossRef]
- Partridge, S.R.; Kwong, S.M.; Firth, N.; Jensen, S.O. Mobile Genetic Elements Associated with Antimicrobial Resistance. Clin Microbiol Rev 2018, 31. [Google Scholar] [CrossRef]
- Clermont, O.; Christenson, J.K.; Denamur, E.; Gordon, D.M. The Clermont Escherichia coli phylo-typing method revisited: improvement of specificity and detection of new phylo-groups. Environ Microbiol Rep 2013, 5, 58–65. [Google Scholar] [CrossRef]
- Touchon, M.; Perrin, A.; de Sousa, J.A.M.; Vangchhia, B.; Burn, S.; O’Brien, C.L.; Denamur, E.; Gordon, D.; Rocha, E.P. Phylogenetic background and habitat drive the genetic diversification of Escherichia coli. PLoS Genet 2020, 16, e1008866. [Google Scholar] [CrossRef]
- Afsharikhah, S.; Ghanbarpour, R.; Mohseni, P.; Adib, N.; Bagheri, M.; Jajarmi, M. High prevalence of β-lactam and fluoroquinolone resistance in various phylotypes of Escherichia coli isolates from urinary tract infections in Jiroft city, Iran. BMC Microbiol 2023, 23, 114. [Google Scholar] [CrossRef]
- Sohrabi, C.; Franchi, T.; Mathew, G.; Kerwan, A.; Nicola, M.; Griffin, M.; Agha, M.; Agha, R. PRISMA 2020 statement: What’s new and the importance of reporting guidelines. Int J Surg 2021, 88, 105918. [Google Scholar] [CrossRef]
- de Souza da-Silva, A.P.; de Sousa, V.S.; de Araújo Longo, L.G.; Caldera, S.; Baltazar, I.C.L.; Bonelli, R.R.; Santoro-Lopes, G.; Riley, L.W.; Moreira, B.M. Prevalence of fluoroquinolone-resistant and broad-spectrum cephalosporin-resistant community-acquired urinary tract infections in Rio de Janeiro: Impact of Escherichia coli genotypes ST69 and ST131. Infect Genet Evol 2020, 85, 104452. [Google Scholar] [CrossRef]
- Cristea, V.C.; Gheorghe, I.; Czobor Barbu, I.; Popa, L.I.; Ispas, B.; Grigore, G.A.; Bucatariu, I.; Popa, G.L.; Angelescu, M.C.; Velican, A.; et al. Snapshot of Phylogenetic Groups, Virulence, and Resistance Markers in Escherichia coli Uropathogenic Strains Isolated from Outpatients with Urinary Tract Infections in Bucharest, Romania. Biomed Res Int 2019, 2019, 5712371. [Google Scholar] [CrossRef]
- Dobbyn, D.; Zeggil, T.; Kudrowich, B.; Beahm, N.P. Ciprofloxacin resistances rates in Escherichia coli across Canada (CREAC): a longitudinal analysis 2015-2019. Int J Antimicrob Agents 2022, 59, 106532. [Google Scholar] [CrossRef]
- Jacoby, G.A. Mechanisms of resistance to quinolones. Clin Infect Dis 2005, 41 Suppl 2, S120–126. [Google Scholar] [CrossRef]
- KOT, B. Antibiotic Resistance Among Uropathogenic. Polish Journal of Microbiology 2019, 68, 403–415. [Google Scholar] [CrossRef]
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infect Drug Resist 2019, 12, 3903–3910. [Google Scholar] [CrossRef]
- Horcajada, J.P.; Vila, J.; Moreno-Martinez, A.; Ruiz, J.; Martinez, J.A.; Sanchez, M.; Soriano, E.; Mensa, J. Molecular epidemiology and evolution of resistance to quinolones in Escherichia coli after prolonged administration of ciprofloxacin in patients with prostatitis. J Antimicrob Chemother 2002, 49, 55–59. [Google Scholar] [CrossRef]
- Soucy, J.R.; Schmidt, A.M.; Quach, C.; Buckeridge, D.L. Fluoroquinolone Use and Seasonal Patterns of Ciprofloxacin Resistance in Community-Acquired Urinary Escherichia coli Infection in a Large Urban Center. Am J Epidemiol 2020, 189, 215–223. [Google Scholar] [CrossRef]
- Uppala, A.; King, E.A.; Patel, D. Cefazolin versus fluoroquinolones for the treatment of community-acquired urinary tract infections in hospitalized patients. Eur J Clin Microbiol Infect Dis 2019, 38, 1533–1538. [Google Scholar] [CrossRef]
- Fromer, D.L.; Cheng, W.Y.; Gao, C.; Mahendran, M.; Hilts, A.; Duh, M.S.; Joshi, A.V.; Mulgirigama, A.; Mitrani-Gold, F.S. Likelihood of Antimicrobial Resistance in Urinary E coli Isolates among US Female Patients with Recurrent vs Non-Recurrent Uncomplicated Urinary Tract Infection. Urology 2024. [Google Scholar] [CrossRef]
- Zavala-Cerna, M.G.; Segura-Cobos, M.; Gonzalez, R.; Zavala-Trujillo, I.G.; Navarro-Perez, S.F.; Rueda-Cruz, J.A.; Satoscoy-Tovar, F.A. The Clinical Significance of High Antimicrobial Resistance in Community-Acquired Urinary Tract Infections. Can J Infect Dis Med Microbiol 2020, 2020, 2967260. [Google Scholar] [CrossRef]
- Guzmán, M.; Salazar, E.; Cordero, V.; Castro, A.; Villanueva, A.; Rodulfo, H.; De Donato, M. Multidrug resistance and risk factors associated with community-acquired urinary tract infections caused by Escherichia coli in Venezuela. Biomedica 2019, 39, 96–107. [Google Scholar] [CrossRef]
- Martos, I.; Colucci Camusso, G.; Albornoz, M.; Barros Nores, J.; Juaneda, R.; Belisle, D.F.; Furiasse, D. [Etiological profile and antimicrobial sensitivity in 1740 urinary infections of the community in the city of Córdoba, Argentina.]. Arch Esp Urol 2021, 74, 645–651. [Google Scholar]
- Findlay, J.; Gould, V.C.; North, P.; Bowker, K.E.; Williams, M.O.; MacGowan, A.P.; Avison, M.B. Characterization of cefotaxime-resistant urinary Escherichia coli from primary care in South-West England 2017-18. J Antimicrob Chemother 2020, 75, 65–71. [Google Scholar] [CrossRef]
- Leforestier, A.; Vibet, M.A.; Gentet, N.; Javaudin, F.; Le Bastard, Q.; Montassier, E.; Batard, E. Modeling the risk of fluoroquinolone resistance in non-severe community-onset pyelonephritis. Eur J Clin Microbiol Infect Dis 2020, 39, 1123–1127. [Google Scholar] [CrossRef]
- Naber, K.G.; Wagenlehner, F.; Kresken, M.; Cheng, W.Y.; Catillon, M.; Duh, M.S.; Yu, L.; Khanal, A.; Mulgirigama, A.; Joshi, A.V.; et al. Escherichia coli resistance, treatment patterns and clinical outcomes among females with uUTI in Germany: a retrospective physician-based chart review study. Sci Rep 2023, 13, 12077. [Google Scholar] [CrossRef]
- Jurałowicz, E.; Bartoszko-Tyczkowska, A.; Tyczkowska-Sieroń, E.; Kurnatowska, I. Etiology and bacterial susceptibility to antibiotics in patients with recurrent lower urinary tract infections. Pol Arch Intern Med 2020, 130, 373–381. [Google Scholar] [CrossRef]
- Demirci, M.; Ünlü, Ö.; İstanbullu Tosun, A. Detection of O25b-ST131 clone, CTX-M-1 and CTX-M-15 genes via real-time PCR in Escherichia coli strains in patients with UTIs obtained from a university hospital in Istanbul. J Infect Public Health 2019, 12, 640–644. [Google Scholar] [CrossRef]
- Islam, M.A.; Islam, M.R.; Khan, R.; Amin, M.B.; Rahman, M.; Hossain, M.I.; Ahmed, D.; Asaduzzaman, M.; Riley, L.W. Prevalence, etiology and antibiotic resistance patterns of community-acquired urinary tract infections in Dhaka, Bangladesh. PLoS One 2022, 17, e0274423. [Google Scholar] [CrossRef]
- Kotb, D.N.; Mahdy, W.K.; Mahmoud, M.S.; Khairy, R.M.M. Impact of co-existence of PMQR genes and QRDR mutations on fluoroquinolones resistance in Enterobacteriaceae strains isolated from community and hospital acquired UTIs. BMC Infect Dis 2019, 19, 979. [Google Scholar] [CrossRef]
- Sun, J.; Du, L.; Yan, L.; Dai, W.; Wang, Z.; Xu, X. Eight-Year Surveillance of Uropathogenic Escherichia coli in Southwest China. Infect Drug Resist 2020, 13, 1197–1202. [Google Scholar] [CrossRef]
- Stapleton, A.E.; Wagenlehner, F.M.E.; Mulgirigama, A.; Twynholm, M. Escherichia coli Resistance to Fluoroquinolones in Community-Acquired Uncomplicated Urinary Tract Infection in Women: a Systematic Review. Antimicrob Agents Chemother 2020, 64. [Google Scholar] [CrossRef]
- Seija, V.; Fratchez, V.; Ventura, V.; Pintos, M.; González, M. [Risk factors for community-acquired urinary tract infection caused by fluoroquinolone resistant E. coli]. Rev Chilena Infectol 2014, 31, 400–405. [Google Scholar] [CrossRef]
- Betitra, Y.; Teresa, V.; Miguel, V.; Abdelaziz, T. Determinants of quinolone resistance in Escherichia coli causing community-acquired urinary tract infection in Bejaia, Algeria. Asian Pac J Trop Med 2014, 7, 462–467. [Google Scholar] [CrossRef]
- Halaji, M.; Fayyazi, A.; Rajabnia, M.; Zare, D.; Pournajaf, A.; Ranjbar, R. Phylogenetic Group Distribution of Uropathogenic Escherichia coli and Related Antimicrobial Resistance Pattern: A Meta-Analysis and Systematic Review. Front Cell Infect Microbiol 2022, 12, 790184. [Google Scholar] [CrossRef]
- Thompson, D.; Xu, J.; Ischia, J.; Bolton, D. Fluoroquinolone resistance in urinary tract infections: Epidemiology, mechanisms of action and management strategies. BJUI Compass 2024, 5, 5–11. [Google Scholar] [CrossRef]
- van Driel, A.A.; Notermans, D.W.; Meima, A.; Mulder, M.; Donker, G.A.; Stobberingh, E.E.; Verbon, A. Antibiotic resistance of Escherichia coli isolated from uncomplicated UTI in general practice patients over a 10-year period. Eur J Clin Microbiol Infect Dis 2019, 38, 2151–2158. [Google Scholar] [CrossRef]
Figure 1.
Fluoroquinolones mechanism of action. E. coli DNA gyrase (which acts by unwinding the DNA double helix) is composed of two A subunits and two B subunits encoded by the GyrA and GyrB, respectively. The A subunits carrying the “codon trimming” functions of gyrase are the site of action of fluoroquinolones. The drug inhibits gyrase-mediated DNA supercoiling at concentrations that are clearly related to those required to inhibit bacterial proliferation.
Figure 1.
Fluoroquinolones mechanism of action. E. coli DNA gyrase (which acts by unwinding the DNA double helix) is composed of two A subunits and two B subunits encoded by the GyrA and GyrB, respectively. The A subunits carrying the “codon trimming” functions of gyrase are the site of action of fluoroquinolones. The drug inhibits gyrase-mediated DNA supercoiling at concentrations that are clearly related to those required to inhibit bacterial proliferation.
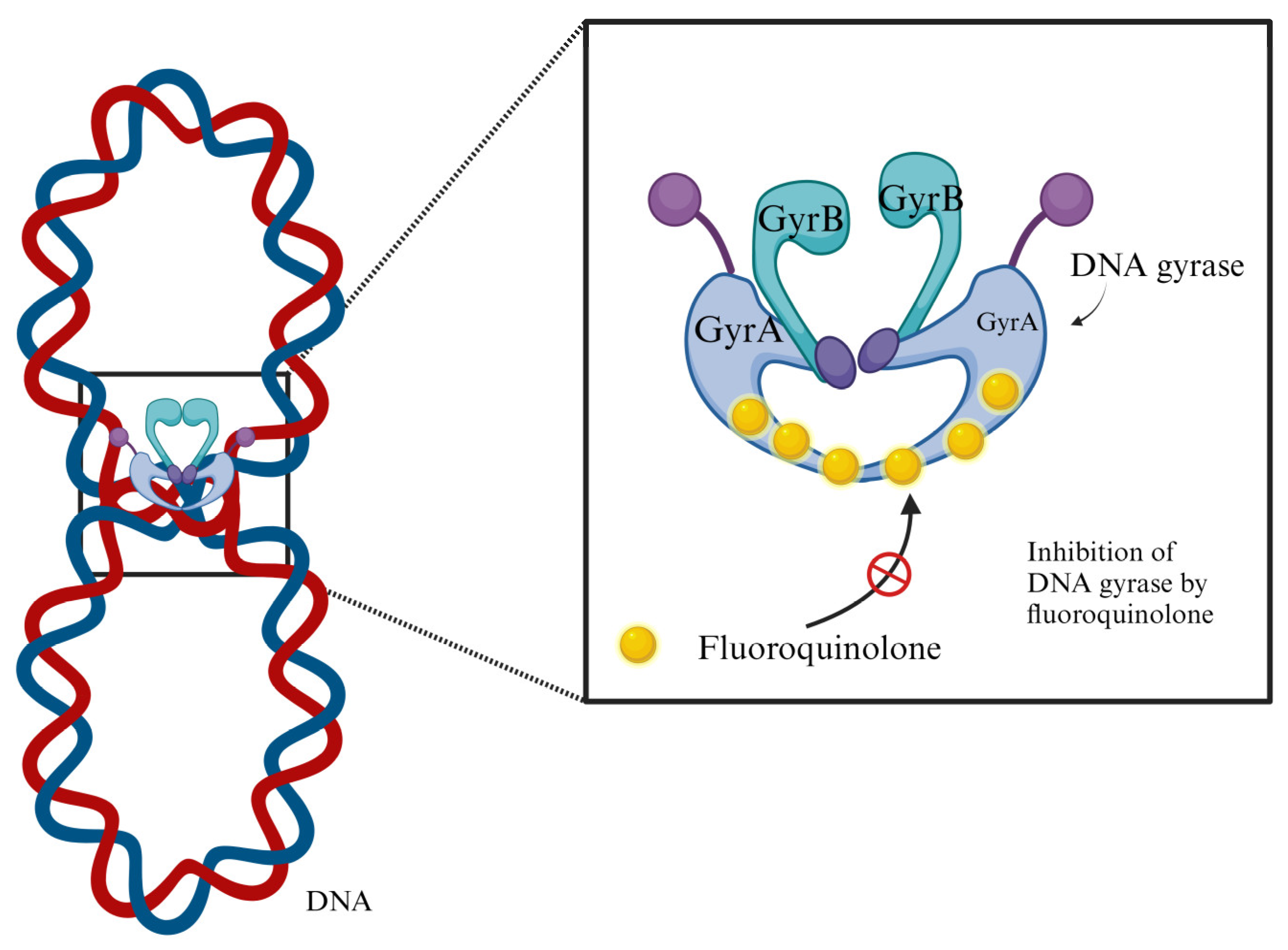
Figure 2.
Genes responsible for fluoroquinolones resistance in E. coli. 1) Chromosomal mutations inducing changes in the drug targets, such as the genes that codify for GyrA (Gram-negative); 2) Mutation related to reduce the drug concentration in the bacterial cytoplasm through overexpression of efflux pumps and downregulation of porins; and 3) expression of genes that codify from plasmid mediated quinolone resistance proteins (PMQR), such as qnr (protect DNA gyrase and topoisomerase IV), aac(6’)-ib-cr (acetylates the fluoroquinolone so that it is inactivated) , quepA and oqxAB (overexpression of multidrug efflux pumps or decreased permeability of outer membrane proteins).
Figure 2.
Genes responsible for fluoroquinolones resistance in E. coli. 1) Chromosomal mutations inducing changes in the drug targets, such as the genes that codify for GyrA (Gram-negative); 2) Mutation related to reduce the drug concentration in the bacterial cytoplasm through overexpression of efflux pumps and downregulation of porins; and 3) expression of genes that codify from plasmid mediated quinolone resistance proteins (PMQR), such as qnr (protect DNA gyrase and topoisomerase IV), aac(6’)-ib-cr (acetylates the fluoroquinolone so that it is inactivated) , quepA and oqxAB (overexpression of multidrug efflux pumps or decreased permeability of outer membrane proteins).
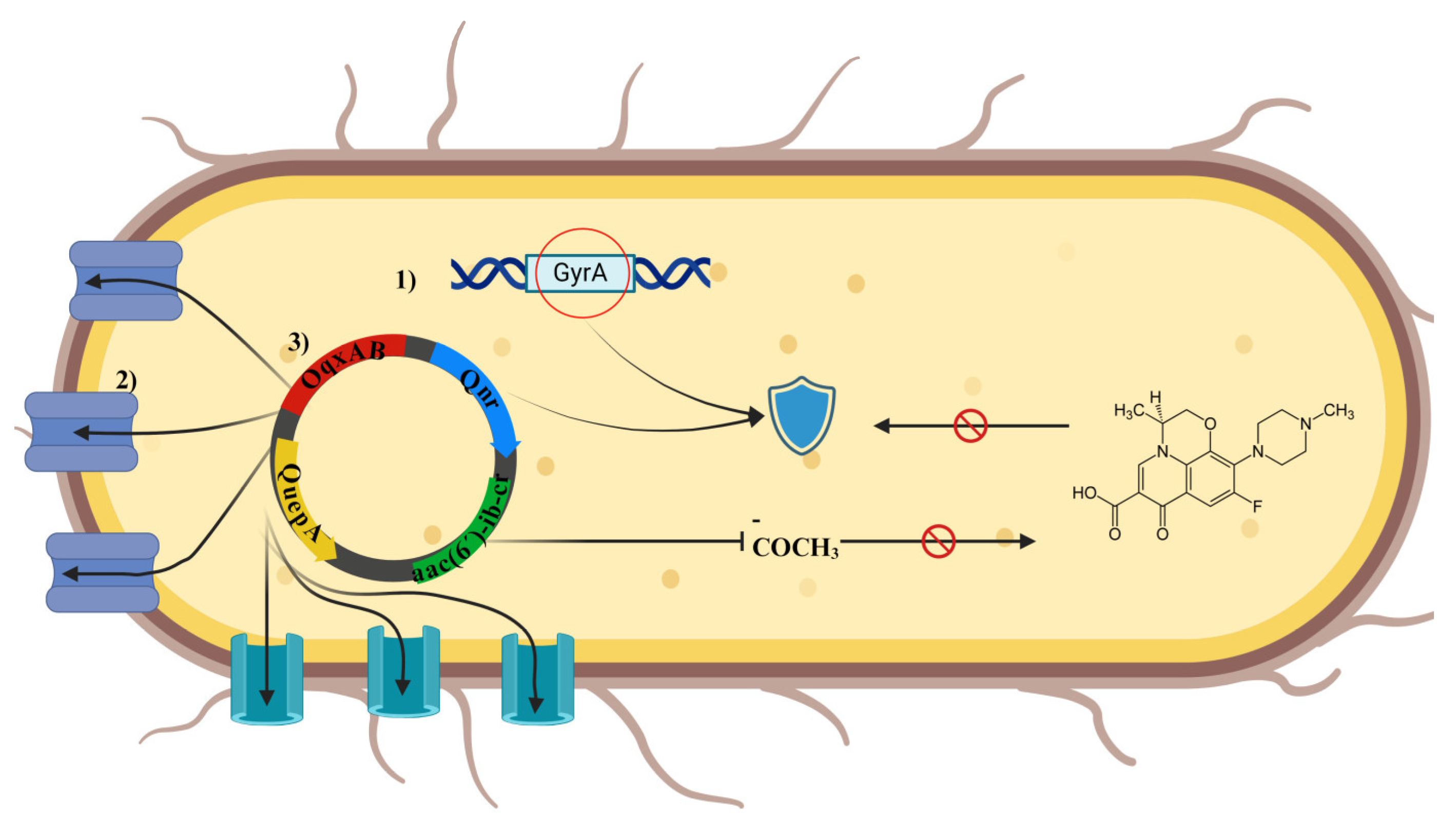
Figure 3.
PRISMA flow diagram for systematic reviews.
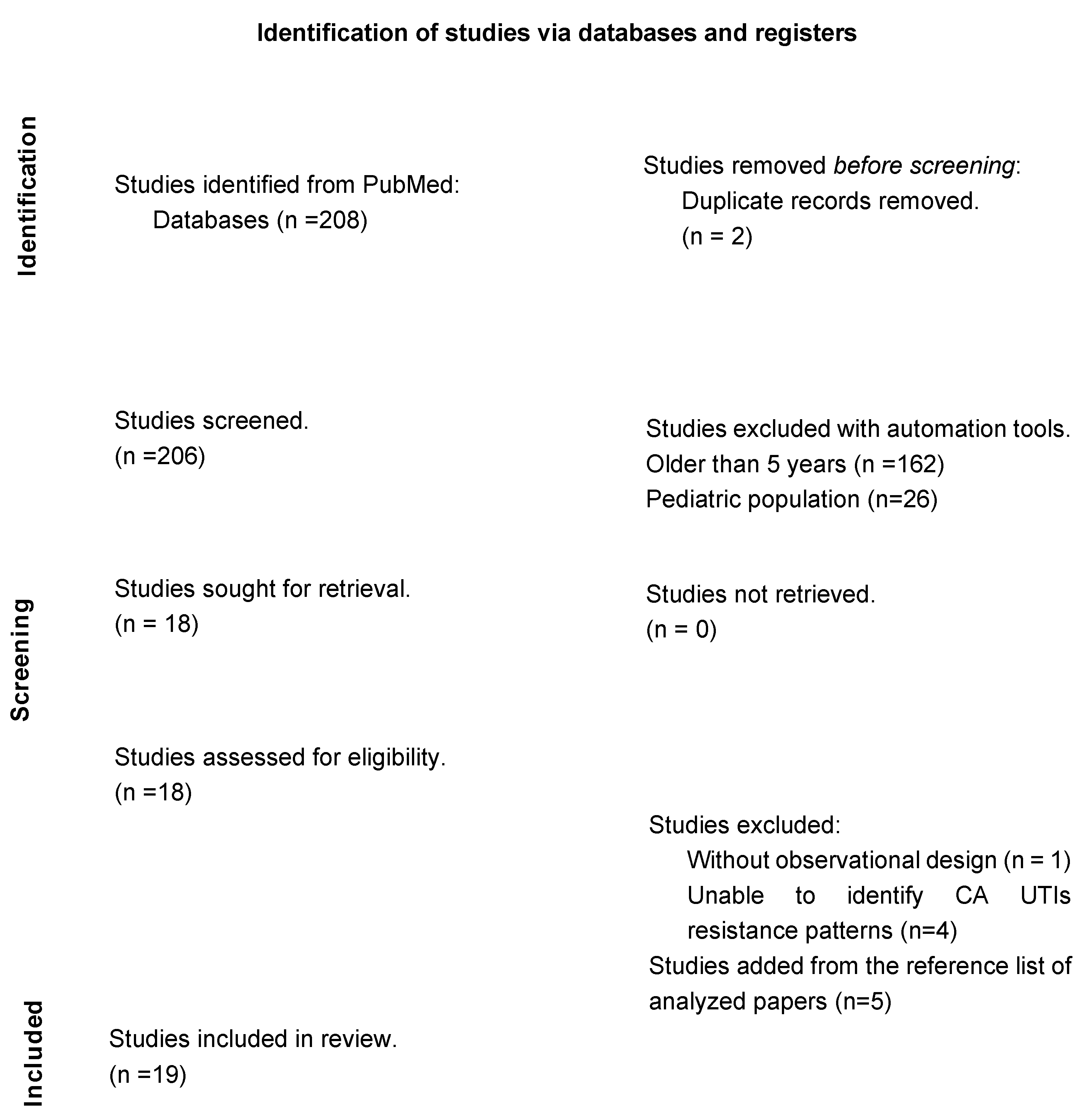

Table 1.
Summary of the studies addressing Fluoroquinolone resistance patterns in patients with urinary tract infections.
Table 1.
Summary of the studies addressing Fluoroquinolone resistance patterns in patients with urinary tract infections.
| Country / Year | Population | Period | Isolates | Resistance to FQ | Phylotype | AR gene | ESBL |
|---|---|---|---|---|---|---|---|
| Canada 2020 [22] | 11,333 isolates from community acquired UTIs (507 nosocomial) | April 2010 - Dec 2014 | E. Coli | CIP: 18.4% | NA | NA | NA |
| Canada 2022 [17] | 591 antibiograms from patients with CA UTIs | 2015 – 2019 | E. Coli | FQ: 11-63% | NA | NA | NA |
| USA 2019 [23] | 73 cases of CA-UTIs | April 2015 to May 2016 | E. Coli (59%) | CIP: 18% | NA | NA | NA |
| USA 2024 [24] |
68,033 cases of non-recurrent uUTI and 12,234 cases of recurrent UTIs |
October 2015 - February 2020 | E. Coli | Recurrent UTIs FQ: 14.2% Non-recurrent uUTIs FQ: 8.6% |
NA | NA | Recurrent UTIs 5.9% and non-recurrent UTIs 4.1% |
| Mexico 2020 [25] | 296 in patients with community acquired UTI. | 2018-2019 | E. Coli | CIP: 30% | NA | NA | 25.6% of which 89% were resistant to CIP |
| Venezuela 2019 [26] | 43 isolates from patients with uUTIs and 60 complicated UTIs | January - June 2014 | E. Coli | CIP: 29.7% | NA |
blaTEM ( 65.4%) blaCTX-M (34.6%) blaSHV (23.1%) |
20.4% |
| Brazil 2020 [15] | 499 isolates from patients with CA-UTIs | November 2015 | E. Coli | CIP: 20 % | B2 (30%) D (23%) A (13%) F (12%) B1 (9%) C (8%) E (3%) |
blaTEM (10%) blaSHV (3%) blaCTX-M (93%) |
8% |
| Argentina 2021 [27] | 1740 cases of CA-UTI’s | January 2016 to December 2017 | E. Coli (80%) | CIP: 15.2 % | B2 D |
blaCTX-M | 0.2% of which 56.9% were resistant to CIP |
| United Kingdom 2020 [28] | 836 E. coli isolates for resistance |
September 2017 – August 2018 | E. Coli | CIP: 50.7% | B2 D |
blaCTX-M pAmpC blaCMY blaDHA |
NA |
| France 2020 [29] | 190 Women with non-severe community-onset pyelonephritis. | Mar - Aug 2018, and Apr – Aug 2019 | E. Coli (84%) | FQ: 3-17% | NA | NA | NA |
| Germany 2023 [30] | 386 isolates from female patients with uUTIs | Jan 2017 -Dec 2019 | E. Coli | FQ: 5.2% CIP: 8.2% |
NA | NA | NA |
| Poland 2020 [31] | 796 Isolates from 332 patients with recurrent lower UTIs | 2016 - 2018 | E. coli (40%) | CIP: 39.9% | NA | NA | 9% |
| Romania 2019 [16] | 787 patients with CA-UTIs | June 2018 | E. coli (91%) | LEV: 14.86% CIP: 14.99% |
B2 (35%) B1 (27%) D (16%) A (22%). |
blaCTX-M (42.3%) blaTEM (38.0%) blaSHV (19.7%) fimH (93.9%) hlyD (44.3%) afaBC (38.2%) hlyA (12.4%) cnf-1 (7.7%). |
9% |
| Turkey 2019 [32] |
101 from CA UTIs and nosocomial UTIs | April - August 2018 |
E. Coli | CIP: 50.98% | NA |
blaCTX-M-1 (73%) blaCTX-M-15 (37%) O25b-ST131 (22%) |
50.49% |
| Turkey 2020 [2] | 141 adult outpatients with UTI | 01-06-2015 to 31-03-2016 | E. Coli | FQ: 35.92% | NA |
qnrS (67.4%) aac(6’)-1b-cr (42.4%) qnrB (7.6%) |
51.78%, of which 29.12% were resistant to FQ. |
| Bangladesh 2022 [33] | 4,500 patients with community-acquired UTIs | September 2016 – November 2018 | E. Coli (51.6%) | CIP: 69% |
NA | NA | NA |
| Egypt 2019 [34] | 440 Isolates from patients with UTIs | July 2016 -March 2017 | E. Coli (64%) | CIP: 19.2% NOR: 19.2% OFX: 19.2% |
NA |
qnrB (62.9%) qnrS (46.9%) qepA (6.3%) |
NA |
| Iran 2023 [13] | 168 CA uncomplicated UTI | Spring season of 2021 | E. Coli | CIP: 55.6% | B2 (29%) D 17.9% E 14.1% F 9.4% C 6.6 % |
blaTEM (89.6%) blaCTX-M (44.3%) blaSHV (6.6%) blaCMY (0.9%) |
52.8% |
| Saudi Arabia 2021 [3] | 428 patients with a positive urine culture (≥10^5 CFU/mL). |
Jan 2015 - Dec 2019 |
E. Coli (45%) |
CIP: 53.1% | NA | bla_CTX-M | 23.7%, of which 47.8% were resistant to CIP |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



