
Submitted:
25 July 2024
Posted:
26 July 2024
You are already at the latest version
Abstract
Quality of life (QoL) focuses on a person’s ability to live a fulfilling life. In the elderly population, it helps in determining successful aging. Because of a scarcity of information regarding predictors of QoL in the elderly population in developing countries, this study was undertaken to assess the overall QoL and its predictors in the elderly population in an urban setting of Bangladesh. In this cross-sectional study, 275 participants were enrolled by systematic sampling at the outpatient department of a tertiary care hospital in Dhaka, Bangladesh. Data were collected by using a pretested semi-structured standard questionnaire for QoL (OPQOL-35). Pearson’s correlation was used to assess the association between QoL and sociodemographic factors. The Chi-square test was done for assessing the statistical significance between categorical variables. Multivariate linear regression was conducted to identify predictors of QoL, after controlling for potential confounders. The median age of the participants (n = 275) was 65 years (range, 60 to 85; 25th and 75th percentile, 60 and 68, respectively). The majority (78%) of them were married and 20% were widowed or divorced. The median score of QoL was 113 (25th and 75th percentile, 101 and 124, respectively). Most of the participants had a very poor (bad as can be) or poor (bad) QoL. Only 7.3% were observed to have “good” QoL (scores 140 or more). Females had significantly poorer QoL scores compared to males (p = 0.01). Educational status, marital status, body mass index and sleep duration significantly predicted QoL in a multiple regression analysis. In conclusion, the QoL of the elderly individuals in Bangladesh was very poor or poor. Future research should focus on service-oriented interventions, especially targeting women. Counseling of elderly people for enhancing their quality of life may include improving sleep patterns, healthy diets, regular exercise, and caring for their mental health.
Keywords:
elderly patient
; quality of life
; OPQOL-35
; BMI
; QoL
; sleep pattern
; Bangladesh
1. Introduction
Population aging is now a daunting challenge across the globe. The number of people aged 60 and older is projected to reach nearly 2.1 billion in 2050 from 382 million in 1980 [1]. Compared to the developed world, the demographic transition is more challenging in Asian countries like Bangladesh, China, and India because of the growing population and inadequate social support system for elderly citizens in those countries [2]. According to the United Nations projection, Asia will be the largest resident of elderly people, with 38% (one billion) elderly living in China and India alone [2]. In Bangladesh, approximately 8% of the total population is 60 years or older, which is projected to rise to 11.5% by 2030 [3], and to 20.2% by 2051 [4].
Quality of Life (QoL) underscores the importance of the wellbeing of a community. According to the World Health Organization, QoL refers to how a person views their place in society, taking into account their cultural and societal norms, as well as their personal goals, aspirations, values, and apprehensions [5]. Therefore, QoL is affected by a wide range of factors – starting from individual health status to socioeconomic factors. Each of the factors does not affect QoL in isolation, rather they interplay together. However, data are scarce in identifying the determinants of the elderly’s QoL, particularly in developing countries. In a study of elderly people in China and India, the determinants of perceived QoL of elderly people included gender, household income, education, co-morbidity, and social cohesion [2]. In a previous study in Bangladesh, factors associated with low health-related QoL among older citizens included increasing age, being widowed, having a lower level of education, and lower socioeconomic status. In another cross-sectional study [6], health-related factors such as sleep problems, depression, and health service availability, and social factors such as religiosity and social support were correlated with the QoL of elderly people.
Despite a few reports of cross-sectional studies, there are several gaps in the literature. For example, studies [2,7,8] attempted to measure elderly people’s perceived QoL but didn’t quantitatively measure QoL and its impact. Only a few earlier studies [6,7] showed correlations between QoL and individual and social factors. However, no robust analytical methods (such as multivariate analyses) were used to determine the predictive models of QoL scores among this population. To fill out the gap in the literature, we aimed to quantitatively measure the QoL scores of elderly people and determine the predictors of QoL scores in this population.
2. Methods and Materials
2.1. Study Design and Selection of Samples
This is a cross-sectional study, conducted from March 2023 to February 2024, among the elderly patients who visited the Outpatient Department of National Institute of Traumatology & Orthopaedic Rehabilitation (NITOR), Dhaka, Bangladesh. The eligible patients included people of either gender, aged 60 to 85 years. The required patients were enrolled (see sample size estimation below) using a systematic random sample procedure, and every alternate patient was selected from among about the 476 patients who visited the Outpatient Department of the Hospital daily.
2.1. Ethical Procedures
The study was conducted following the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of NITOR (Memo No. NITOR-PT-93-2023-03). The study objectives and the procedures were explained before the informed consent was obtained. Participation in the study was completely voluntary, and the participants had the right to withdraw from the study at any time during the study. They were assured about the anonymity, confidentiality of the data, and risks and benefits. No body samples were obtained. The study data were collected by using a standard questionnaire, which is described below.
2.2. Questionnaire
Participants were interviewed using a structured and standard questionnaire (OPQOL-35) to collect information on sociodemographic characteristics and physical health status. A copy of the questionnaire is added in the supplementary materials at the end. Health-related quality of life (HRQoL) was measured by using the Likert scale data collected through the questionnaire. The questionnaire had a 5-point score for each of the 35 questions, with a range of “strongly agree” to “strongly disagree” (1-5 scores). The questionnaire was originally developed by Ann Bowling in 2009 [9]. The total score ranges from a minimum of 35 to a maximum of 175. The total scores were categorized as follows: Less than 99 of QoL as bad as can be, 100-119 as bad, 120-139 as optimum, 140-159 as good, and 160-175 of QoL as good as can be [9]. In our study, the survey instrument was translated into Bengali by forward and backward translation and the validity of the questionnaire was field tested among 30 elderly participants from the same cohort. Any inconsistencies in data were identified and corrected at the field level. Cronbach’s alpha for reliability was calculated for the 35 items of the QoL questionnaire. The overall Cronbach’s alpha score was 0.88, meaning that the QoL questionnaire was reliable.
In addition to QoL-related data, we collected demographic data (including age, sex, marital status, occupation, monthly income, and any special allowances), food habits (especially the daily intakes of fruits and vegetables), amount of water intake, personal habits (such as smoking, exercise), sleep pattern (hours of sleep and any sleep disturbances), and we measured weight and height of the individual, and calculated body mass index (BMI).
2.4. Sample Size Estimation
The major variable of interest in QoL is the overall life satisfaction of the individual. We used data on patient satisfaction from Khan and colleagues [10] for the sample size estimation. Using the data, we calculated the sample size as follows:
Here, proportion of the people who had satisfaction, p = 20.4% or 0.204
q = 1 – p = 0.796
Z = 1.96 for α = 0.05 (95% confidence)
The required sample size was 275, after adjusting for an additional 10% attrition rate.
2.5. Statistical Analysis
The data analysis was conducted using IBM SPSS version 29. First, a descriptive statistical analysis was performed to assess the data distribution. To examine the association between sociodemographic factors and QoL, Pearson’s chi-square test or Fisher’s exact test was used. Bivariate correlations were assessed between QoL and sociodemographic factors. For the multivariate analysis, a linear regression model was constructed with the QoL score as the dependent variable. Only the covariates that were significantly associated with QoL in the bivariate analyses were included in the multivariate model. Statistical significance was determined using a P-value ≤ 0.05.
3. Results
3.1. Sociodemographic Characteristics
In this study, 275 adults were enrolled, and none dropped out. The age of the participants ranged from 60 to 85 years, with mean ± SD of age being 65 ± 5.5 years (95% confidence intervals = 0.69 to 3.17). Only 9% of them (n = 25) were aged 75 years or older. The majority (62.9%) of the participants were male (n = 173), married (n = 215, 78.2%), and had no formal education (n = 115, 41.8%) or primary education (n = 53, 19.3%) (Table 1). Based on the monthly family income, 75.3% (n = 207) were considered low-income families. About 75% had no additional income in terms of government-supported allowances, such as freedom fighter allowance, old-age allowance, or disability allowance.
The mean age of males was somewhat higher than that of females. There were also gender differences in marital status, educational categories, occupation, and residence type (Table 1).
3.2. Difference in Characteristics of Physical Health and Diet
Table 2 presents characteristics related to physical health, diet, smoking, sleep pattern, and QoL of the population. The BMI was normal in the study participants, with a mean ± SD of 24.36 ± 3.32. The obesity rate was higher in females (10.8%) than in males (4.0%). More than 75% of the people ate vegetables either daily or often. Similarly, about 70% of them ate some form of protein-rich foods, such as fish, meat, eggs, or lentils daily or often. However, fruit consumption was less common, comprising only 12% daily and about 15% often having fruits. As smoking is not socially acceptable in females in Bangladesh, none of the female participants reported ever smoking. Whereas 50% of the men were current or former smokers. The majority of individuals (51.6%) reported having 6 to 7 hours of sleep per day, which was quite adequate.
3.3. Quality of Life Scores
The study subjects (n = 275) had an overall poor QoL score as indicated by the mean ± SD scores of 113.79 ± 16.50. Of them, females had a significantly poorer score of QoL compared to their male counterparts (109.33 ± 16.06 vs. 116.41 ± 16.23, P < 0.001). When the categories of QoL were compared, most of the participants (65%) had very poor to poor QoL scores (bad as can be or bad), whereas, over a quarter of them had optimum level of scores, and only about 7% had good scores of QoL.
3.4. Distribution of Elderly People by Quality of Life (QoL) Categories
Among the 275 participants, the highest score observed was 159, while the lowest score was 70 out of a total possible score of 175. The median score of QoL was 113, while the 25th and the 75th percentile of the scores were 101 and 124, respectively. A significant proportion of the participants (65%) were identified as having a very poor (bad as can be) or poor (or bad) QoL. Only 7.3% were observed having “good” QoL. None of the participants had the highest score of having “QoL good as can be” (Figure 1).
3.5. Correlation between Sociodemographic Factors and Quality of Life (QoL) Scores
A bivariate correlation test (Table 3) showed that QoL directly correlated with educational status (r = 0.417, P <0.001), BMI (r = 0.159, P = 0.008), and hours of sleep (r = 0.195, P = 0.001). QoL was inversely correlated with age (r = -0.128, P = 0.034), meaning poorer QoL with increasing age even within the elderly population. The correlation coefficient (r) value of the association between QoL and gender was negative, meaning that the QoL scores were higher in male compared to females (gender: male = 0, and female = 1).
3.6. Linear Regression Analysis to Predict Quality of Life
The variables that were found statistically significant in bivariate analysis were entered into the model of the regression analysis. The dependent variable was QoL score which was a continuous variable. The selected independent variables were age, gender (0 = male, 1 = female), educational status (0 = no formal education, 1 = primary education, 2 = secondary education, 3 = higher secondary education, 4 = graduation, 5 = post-graduation), marital status (0 = married, 1 = unmarried, 2 = widow, 3 = divorced), BMI, and sleep duration (hours). There was no multicollinearity observed among the independent variables. Table 4 shows the results of a stepwise multiple linear regression analysis. The statistically significant predictors of QoL included educational status (95% CI, 2.81 to 5.11; P <0.001), sleep duration (95% CI, 1.77 to 6.89; P <0.001), marital status (95% CI, -4.0 to -0.49; P = 0.013), and BMI (95% CI, 0.05, 1.1; P = 0.031). Age (P = 0.076) and gender (P = 0.228) were excluded from the model.
The predicted model for the data was as follows:
Quality of life (scores) = 91.797 + 3.957 (educational status) + 4.332 (sleep duration) – 2.259 (marital status: 0 = married, 1 = unmarried, 2 = widow, 3 = divorced) + 0.578 (BMI).
4. Discussions
In this study, the elderly people showed poor QoL scores. Females had a worse score of QoL than men. QoL was significantly correlated with the sociodemographic parameters studied. Multivariate analysis also indicated higher educational status, sleep duration, and being married (compared to other categories of marital status), and a better nutritional status (in terms of BMI) significantly predicting a better quality of life score.
The demographic shift of the population due to increasing longevity, together with the epidemiologic transition from infectious and communicable diseases to chronic and non-communicable diseases, raises great concern for the quality of life of the increasing number of elderly people in any society. Consequently, there is a growing trend in appraising the quality of life among elderly populations using the survey instrument (OPQOL-35) similar to our study [11], and also by using modified survey tools [12]. However, studies showed acceptable levels of reliability and validity in using OPQOL-35 in a multidimensional population, and therefore, OPQOL-35 has a wider use [13]. In our study, the survey instrument was translated into Bengali and was field tested, and the reliability of the instrument was strong (having a Cronbach’s alpha of 0.88).
The relationship between age and HRQoL among the elderly varied, with poorer QoL with increasing age. However, in multivariate analysis, the effect of age in our study was nullified after controlling for others across different age groups. Additionally, in other studies [14], factors such as gender, education, employment status, and smoking also influence HRQoL in older adults. Increasing age is associated with a decline in health-related quality of life (HRQOL) in the elderly [15,16], like our study. Studies have shown that as individuals age, the prevalence of chronic diseases and disorders increases lead to a decrease in HRQOL [17]. In a study conducted in India, it was found that older age, male gender, lower education, absence of a spouse, lower economic status, and chronic disorders were associated with lower HRQoL [16].
Gender could be a strong factor in determining the quality of life. However, studies show conflicting results. In this study, the QoL of female participants was poorer than males in bivariate analysis. However, the effect of gender was removed when multiple other potential confounders were controlled for. In Iran, a study on the quality of life of elderly people showed that males lead a better quality of life than females from the perspective of functional capacity, perceived health, good housing conditions, an active lifestyle, economic status, and good social relationships [18]. On the contrary, another study suggested longstanding illnesses reducing the quality of life significantly in men but not in women [19]. The observed poorer QoL in Bangladeshi females is more likely due to societal neglect of them in general in the country, which leads to females living in more vulnerable health conditions and healthcare that affect adversely their QoL.
Marital status has been found to have a significant impact on the QoL of elderly individuals. Being married is associated with higher levels of life satisfaction and better QoL in terms of physical and psychological health, and social relationships [20,21]. Similarly, in this study, being married was a positive predictor of the overall QoL of elderly people. As socioeconomic problems are more common in older age, they have no scope to share their emotion and feelings when a partner is absent.
The educational qualifications of elderly individuals play a crucial role in shaping their quality of life. Research indicates a positive correlation between higher education levels and an improved quality of life in the elderly [22,23]. Education equips individuals with additional knowledge and information, fostering the adoption of healthier lifestyles and contributing to overall well-being and positive aging. Notably, engaging in educational programs for seniors has been linked to a higher quality of life, particularly among older women [24].
In a previous study, in elderly adults aged 70–90 years, obesity was linked to a decline in overall quality of life, particularly impacting independent living, social relationships, and the perception of pain [25]. Similar results were found in another study in Jiangsu, China that underweight is an explicit risk factor for low HRQoL in both the male and female elderly, while the effect of being overweight on low HRQoL varies slightly by gender [26]. In this study, the findings closely aligned with those of other studies. BMI demonstrated a significant correlation with QoL, with a lower BMI having a lower QoL.
A study in Australia showed that short and long sleep were significantly associated with poor self-rated health and lower quality of life in a large sample of middle-aged and older Australian adults [27]. Another study in China showed that appropriate sleep duration and good sleep quality are beneficial to quality of life. Meanwhile, maintaining good sleep status is also beneficial in reducing the prevalence of depression in the elderly [28]. Our study was consistent with previous studies in showing that sleep duration has a significant positive impact on QoL [27].
4.1. Limitations
As this was a cross-sectional study, we could only demonstrate a statistically significant relationship between QoL and other predictor variables. However, a causal association can’t be established from this type of study. A cross-sectional study may also suffer from reporting bias (underreporting or over-reporting). Furthermore, the study may not be representative of the entire population, as they rely on a single sample at one point in time.
5. Conclusions
In Bangladesh, aging has become a significant social issue in the new millennium. To guarantee an overall healthy life for the elderly within the community, the results of this study should benefit policymakers and medical professionals by providing extra attention and enforcing policies for the health of the elderly, the majority of whom were found to have very poor QoL. Targeted interventions are urgently needed to address the poorer QoL of females in general, by formulating policies to ensure adequate treatment facilities, early institutional care, and other opportunities for the more vulnerable population of the society. Both the government and non-governmental organizations need to offer comprehensive services beyond medication. This may include nutrition care, social support, psychological support, and rehabilitation. Future research should focus on specific service-based interventions that enhance the quality of life in community settings as well as in elderly care facilities.
Author Contributions
Conceptualization, J.A.I. and P.K.S.; Methodology, J.A.I.; Software, J.A.I.; Validation, A.K.M., P.K.S. and J.A.I; Formal Analysis, M.A.R. and A.K.M; Investigation, T.M.; Resources, S.A.S.; Data Curation, J.F.K.; Writing—Original Draft Preparation, J.A.I.; Writing—Review & Editing, J.A.I., A.K.M; Visualization, P.K.S.; Supervision, A.K.M.; Project Administration, A.K.M.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of NITOR (Memo No. NITOR-PT-93-2023-03 and date of approval: March 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data collection questionnaires are provided in the Appendix A and Appendix B. The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A

Table S1.
Demographic Questionnaire.
| Participant ID No: /__/__/__/__/__/__/ | Date: | ||
| Name of the participant: | |||
| Address: | |||
| Section 1-Socio-demographic factor: | |||
| Serial No. | Question | Response | Code No. |
| 1 | What is your age? | /__/__/__/__/__/__/ Years | |
| 2 | Gender |
|
0 1 |
| 3 | What is your marital status? |
|
0 1 2 3 4 |
| 4 | What is your educational qualification? |
|
0 1 2 3 4 5 |
| 5 | What is your occupation? |
|
0 1 2 3 4 5 6 |
| 6 | If not retired or unemployed, monthly income from your occupation? |
 Ta taka Ta taka |
|
| 7 | What is your monthly family income? |
Ta taka |
|
| 8 | Where do you live? |
|
0 1 2 |
| Section 2-Physical health related factors: | |||
| Serial No. | Question | Response | Code No. |
| 9 | Height |
 I inch I inch |
|
| 10 | Weight |
kg |
|
| 11 | BMI |
kg/m2 |
|
| 12 | How many meals do you have a day? |
|
|
| 13 | Do you include vegetables in your diet? |
|
0 1 2 3 |
| 14 | Do you include fruits in your diet? |
|
0 1 2 3 |
| 15 | Do you include fish or meat or egg or lentil in your diet? |
|
0 1 2 3 |
| 16 | Do you include milk and milk products in your diet? |
|
0 1 2 3 |
| 17 | How many glasses of water do you drink every day? |
|
|
| 18 | Your smoking status? |
|
0 1 2 |
| 19 | How much do you sleep per day? |
H hour |
|
| Section 3-Institution and government related factors | |||
| Serial No. | Question | Response | Code No. |
| 21 | Do you receive any pension, old age allowance or NGO’s support? If yes, what kind of support do you get? |
|
0 1 2 3 4 5 |
| 22 | How much allowance do you get monthly? |
Ta taka |
|
Appendix B
Table S2.
Older People’s Quality of Life Questionnaire (OPQOL-35).
| Serial No. ________________ | ||||||
| We would like to ask you about your quality of life: | ||||||
| Please tick one box in each row. There are no right or wrong answers. Please select the response that best describes you/your views. | ||||||
| 1. Thinking about both the good and bad things that make up your quality of life, how would you rate the quality of your life as a whole? | ||||||
| Your quality of life as a whole is | Very good (1) | Good (2) |
Alright (3) |
Bad (4) | Very bad (5) | |
|
2. Please indicate the extent to which you agree or disagree with each of the following statements. (Tick one box in each row) | ||||||
| Life overall | ||||||
| 1 | I enjoy my life overall | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 2 | I am happy much of the time | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 3 | I look forward to things | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 4 | Life gets me down | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| Health | ||||||
| 5 | I have a lot of physical energy | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 6 | Pain affects my wellbeing | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 7 | My health restricts me looking after myself or my home | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 8 | I am healthy enough to get out and about | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| Social relationship | ||||||
| 9 | My family, friends or neighbors would help me if needed | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 10 | I would like more companionship or contact with other people | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 11 | I have someone who gives me love and affection | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 12 | I’d like more people to enjoy life with | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 13 | I have my children around which is important | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| Independence, control over life, freedom | ||||||
| 14 | I am healthy enough to have my independence | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 15 | I can please myself what I do | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 16 | The cost of things compared to my pension/income restricts my life | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 17 | I have a lot of control over the important things in my life | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| Home and neighborhood | ||||||
| 18 | I feel safe where I live | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 19 | The local shops, services and facilities are good overall | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 20 | I get pleasure from my home | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 21 | I find my neighborhood friendly | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| Psychological and emotional wellbeing | ||||||
| 22 | I take life as it comes and make the best of things | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 23 | I feel lucky compared to most people | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 24 | I tend to look on the bright side | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 25 | If my health limits social/ leisure activities, then I will compensate and find something else I can do | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| Financial circumstances | ||||||
| 26 | I have enough money to pay for household bills | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 27 | I have enough money to pay for household repairs or help needed in the house | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 28 | I can afford to buy what I want to | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 29 | I cannot afford to do things I would enjoy | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| Leisure and activities | ||||||
| 30 | I have social or leisure activities/hobbies that I enjoy doing | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 31 | I try to stay involved with things | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 32 | I do paid or unpaid work or activities that gives me a role in life | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 33 | I have responsibilities to others that restrict my social or leisure activities | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 34 | Religious, belief or philosophy is important to my quality of life | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
| 35 | Cultural/religious events/festivals are important to my quality of life | Strongly agree (1) | Agree (2) | Neither agree or disagree (3) | Disagree (4) | Strongly disagree (5) |
OPQOL: Copyright @ A. Bowling, St George’s, University of London & Kingston University [9].
References
- United Nations. World Population Aging 2017 Highlights. Department of Economic and Social Affairs. United Nations, New York. Available online: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WPA2017_Highlights.pdf (accessed on 29 May 2024).
- Ghosh, D.; Dinda, S. Determinants of the quality of life among elderly: Comparison between China and India. International Journal of Community and Social Development 2020, 2, 71–98. [Google Scholar] [CrossRef]
- Sarker, A.R.; Zabeen, I.; Khanam, M.; Akter, R.; Ali, N. Healthcare-seeking experiences of older citizens in Bangladesh: A qualitative study. PLOS Glob Public Health. 2023, 3, e0001185. [Google Scholar] [CrossRef] [PubMed]
- Kabir, R.; Khan, H.T.; Kabir, M.; Rahman, M.T. Population aging in Bangladesh and its implication on health care. European Scientific Journal 2013, 9, 34–47. [Google Scholar]
- World Health Organization. WHOQOL: Measuring Quality of Life. World Health Organization, 2012. Available online: https://www.who.int/tools/whoqol (accessed on 26 March 2024).
- Uddin, M.A.; Soivong, P.; Lasuka, D.; Juntasopeepun, P. Factors related to quality of life among older adults in Bangladesh: A cross sectional survey. Nursing and Health Sciences. 2017, 19, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, J.; Rana, A.K.; Kabir, Z.N. Social capital and quality of life in old age: Results from a cross-sectional study in rural Bangladesh. Journal of Aging and Health 2006, 18, 419–434. [Google Scholar] [CrossRef] [PubMed]
- Sarker, A.R. Health-related quality of life among older citizens in Bangladesh. SSM - Mental Health 2021, 1. [Google Scholar] [CrossRef]
- Bowling, A. The psychometric properties of the older people′ s quality of life questionnaire, compared with the CASP-19 and the WHOQOL-OLD. Current Gerontology and Geriatrics Research 2009, 2009, 298950. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.N.; Mondal, M.N.I.; Hoque, N.; Islam, M.S.; Shahiduzzaman, M.D. A study on quality of life of elderly population in Bangladesh. American Journal of Health Research 2014, 2, 152–157. [Google Scholar] [CrossRef]
- McGee, H.; Morgan, K.; Hickey, A.; Burke, H.; Savva, G. Quality of life and beliefs about ageing. Available online: https://tilda.tcd.ie/publications/reports/pdf/w1-key-findings-report/Chapter10.pdf, (accessed on 24 July 2024).
- Carrard, S.; Mooser, C.; Hilfiker, R.; Mittaz Hager, A.G. Evaluation of the psychometric properties of the Swiss French version of the Older People’s Quality of Life questionnaire (OPQOL-35-SF). Health and Quality of Life Outcomes 2022, 20, 43. [Google Scholar] [CrossRef]
- Mares, J.; Cigler, H.; Vachkova, E. Czech version of OPQOL-35 questionnaire: The evaluation of the psychometric properties. Health and Quality of Life Outcomes 2016, 14, 93. [Google Scholar] [CrossRef]
- Krawczyk-Suszek, M.; Kleinrok, A. Health-related quality of life (HRQoL) of people over 65 years of age. Int J Environ Res Public Health 2022, 19, 625. [Google Scholar] [CrossRef]
- Lee, S.; Jung, M.; Kang, M. Age-varing association between physical activity and health-related quality of life among U.S. adults: 1928. Medicine & Science in Sports & Exercise 2022, 54, 573–573. [Google Scholar] [CrossRef]
- Singh, A.; Palaniyandi, S.; Palaniyandi, A.; Gupta, V. Health related quality of life among rural elderly using WHOQOL-BREF in the most backward district of India. Journal of Family Medicine and Primary Care 2022, 11, 1162. [Google Scholar] [CrossRef] [PubMed]
- Pal, A.K.; Govil, D.; Biswas, S. Relationship between falls/injuries and quality of life among the elderly in India. Research Square 2022. [Google Scholar] [CrossRef]
- Nejati, V.; Shirinbayan, P.; Akbari Kamrani, A.; Foroughan, M.; Taheri, P.; Sheikhvatan, M. Quality of life in elderly people in Kashan, Iran. Middle East Journal of Age and Ageing 2008, 5, 21–25. [Google Scholar]
- Netuveli, G.; Wiggins, R.D.; Hildon, Z.; Montgomery, S.M.; Blane, D. Quality of life at older ages: Evidence from the English longitudinal study of aging (wave 1). Journal of Epidemiology & Community Health 2006, 60, 357–363. [Google Scholar]
- Daely, S.; Nuraini, T.; Gayatri, D.; Pujasari, H. Impacts of age and marital status on the elderly’s quality of life in an elderly social institution. Journal of Public Health Research 2022, 11, jphr.2021.2731. [Google Scholar] [CrossRef] [PubMed]
- Nagargoje, V.P.; James, K.S.; Muhammad, T. Moderation of marital status and living arrangements in the relationship between social participation and life satisfaction among older Indian adults. Scientific Reports 2022, 12, 20604. [Google Scholar] [CrossRef] [PubMed]
- Damor, K.L.; Sonkaria, L.K.; Kewalramani, S.; Sidhu, J.; Lal, S. A study to assess quality of life of elderly residing in field practice area of urban health training center of SMS medical college Jaipur. Global Journal For Research Analysis (GJRA) 2019, 8. [Google Scholar] [CrossRef]
- Jurkiewicz, B.; Barnaś, E.; Kołpa, M. Senior education and the quality of life of women in different periods of old age. Journal of Education, Health and Sport 2022, 12, 217–230. [Google Scholar] [CrossRef]
- AlAbedi, G.; Naji, A. Quality of Life among Elderly at Primary Health Care Centers in Al-Amara City. Kufa Journal for Nursing Sciences 2020, 10, 62–69. [Google Scholar] [CrossRef]
- Wang, L.; Crawford, J.D.; Reppermund, S.; Trollor, J.; Campbell, L.; Baune, B.T.; Sachdev, P.; Brodaty, H.; Samaras, K.; Smith, E. Body mass index and waist circumference predict health-related quality of life, but not satisfaction with life, in the elderly. Quality of Life Research 2018, 27, 2653–2665. [Google Scholar] [CrossRef] [PubMed]
- You, H.; Li, X.; Jing, K.; Li, Z.; Cao, H.; Wang, J.; Bai, L.; Gu, J.; Fan, X.; Gu, H. Association between body mass index and health-related quality of life among Chinese elderly - Evidence from a community-based study. BMC Public Health 2018, 18, 1174. [Google Scholar] [CrossRef] [PubMed]
- Magee, C.A.; Caputi, P.; Iverson, D.C. Relationships between self-rated health, quality of life and sleep duration in middle aged and elderly Australians. Sleep Medicine 2011, 12, 346–350. [Google Scholar] [CrossRef]
- Zhi, T.F.; Sun, X.M.; Li, S.J.; Wang, Q.S.; Cai, J.; Li, L.Z.; Li, Y.X.; Xu, M.J.; Wang, Y.; Chu, X.F.; Wang, Z.D.; Jiang, X.Y. Associations of sleep duration and sleep quality with life satisfaction in elderly Chinese: The mediating role of depression. Archives of Gerontology and Geriatrics 2016, 65, 211–217. [Google Scholar] [CrossRef]
Figure 1.
Distribution of the participants by quality-of-life scores (n = 275).
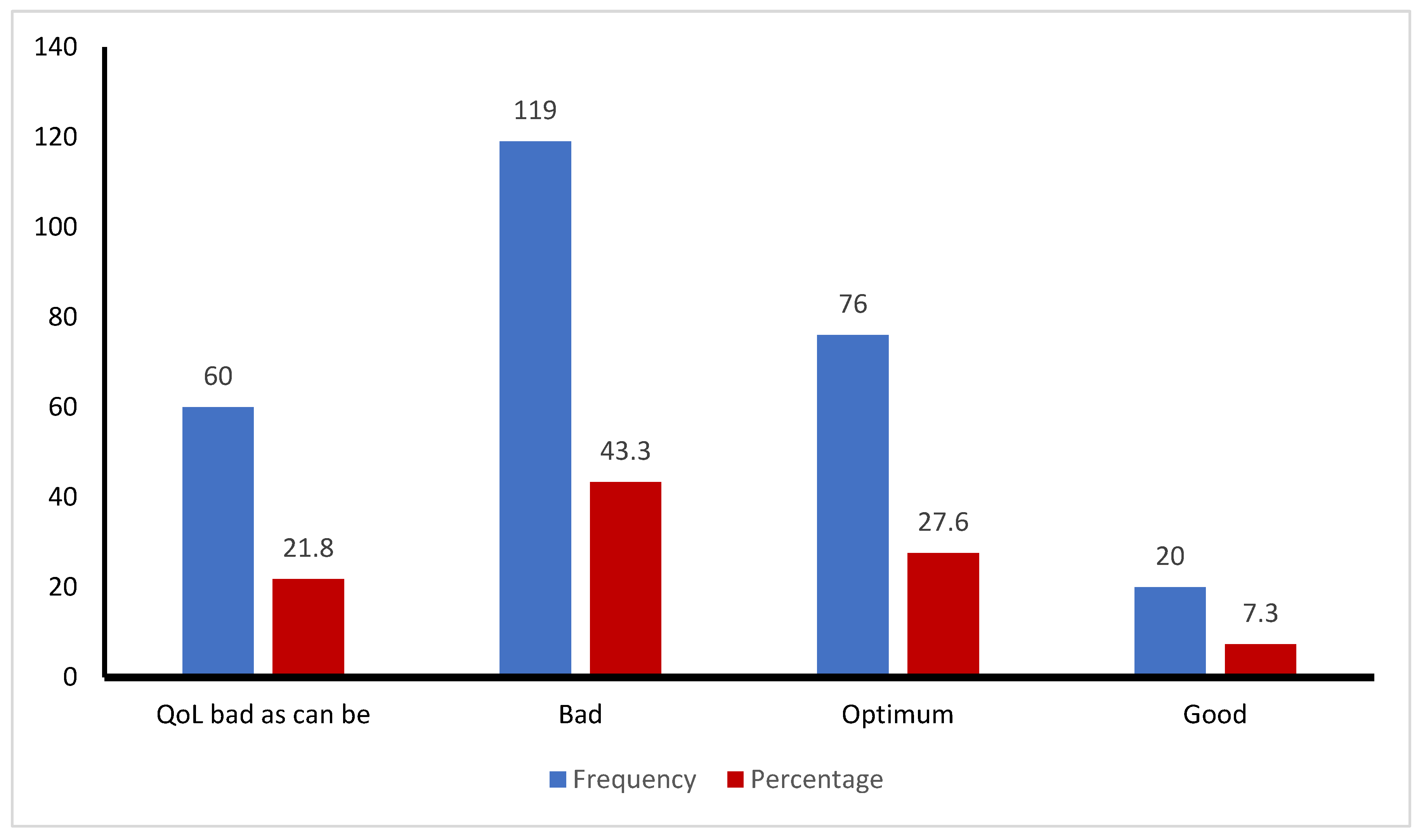
Table 1.
Sociodemographic characteristics of the participants (n = 275).
| Characteristics | All participants (n = 275) | Male (n = 173) |
Female (n = 102) |
Chi-square | P - value |
| Age (mean ± SD) | 65.07 ± 5.5 | 65.78 ± 5.87 | 63.85 ± 4.49 | - | 0.002a |
| Marital status (%) | 22.72b | <0.001 | |||
| Married | 215 (78.2) | 156 (90.2) | 59 (78.2) | ||
| Unmarried | 2 (0.7) | 1 (0.6) | 1 (1.0) | ||
| Widow/divorced | 56 (20.3) | 16 (9.2) | 42 (41.2) | ||
| Education (%) | 29.48c | <0.001 | |||
| No formal education | 115 (41.8) | 54 (31.2) | 61 (59.8) | ||
| Primary education (grades 1-5) | 53 (19.3) | 35 (20.2) | 18 (17.6) | ||
| Secondary education (grades 6-12) | 52 (18.9) | 35 (20.2) | 17 (16.7) | ||
| Higher Secondary | 15 (5.5) | 13 (7.5) | 2 (2.0) | ||
| Graduation | 26 (9.5) | 23 (13.3) | 3 (2.9) | ||
| Post-graduation | 14 (5.1) | 13 (7.5) | 1 (1.0) | ||
| Occupation (%) | 221.67c | <0.001 | |||
| Retired | 39 (14.2) | 36 (20.8) | 3 (2.9) | ||
| Farmer | 22 (8.0) | 22 (12.7) | 0 | ||
| Businessman | 23 (8.4) | 21 (12.1) | 2 (2.0) | ||
| Service holder | 36 (13.1) | 34 (19.7) | 2 (2.0) | ||
| Unemployed | 55 (20.0) | 51 (29.5) | 4 (3.9) | ||
| Housewife | 88 (32.0) | 0 | 88 (86.3) | ||
| Others | 12 (4.4) | 9 (5.2) | 3 (2.9) | ||
| Family monthly income (Taka)d | 2.0c | 0.57 | |||
| Below 20,000 | 72 (26.2) | 42 (24.3) | 30 (28.4) | ||
| 20,000 – 39,999 | 135 (49.1) | 90 (52.0) | 45 (44.1) | ||
| 40,000 – 59,999 | 53 (19.3) | 31 (17.9) | 22 (21.6) | ||
| 60,000 and above | 15 (5.5) | 10 (5.8) | 5 (4.9) | ||
| Monthly allowances received (%) | 0.22b | 0.64 | |||
| None | 206 (74.9) | 124 (71.7) | 82 (80.4) | ||
| Pension | 33 (12.0) | 28 (16.2) | 5 (4.9) | ||
| Freedom fighter allowance | 9 (3.3) | 5 (2.9) | 4 (3.9) | ||
| Old age allowance | 25 (9.1) | 14 (8.1) | 11 (10.8) | ||
| Disability allowance | 2 (7.0) | 2 (1.2) | 0 | ||
| Residence type (%) | 5.94c | 0.05 | |||
| Urban | 131 (47.6) | 91 (52.8) | 40 (39.2) | ||
| Sub-urban | 32 (11.6) | 21 (12.1) | 11 (10.8) | ||
| Rural | 112 (40.7) | 61 (35.3) | 51 (50.0) | ||
a 95% confidence intervals (CI) for mean difference = 0.69 to 3.17; b Fisher’s exact correction test used for having 20% or more expected frequencies less than 5; c Pearson’s Chi-square; d 1 US dollar = 109.39 Taka (in June 2024).
Table 2.
Characteristics of physical health, dietary pattern, sleep hours, and quality of life of the participants (n = 275).
Table 2.
Characteristics of physical health, dietary pattern, sleep hours, and quality of life of the participants (n = 275).
| Characteristics | All participants (n = 275) | Male (n = 173) |
Female (n = 102) |
Chi-square | P - value |
| Body mass index, mean ± SD | 24.36 ± 3.32 | 24.24 ± 2.97 | 24.56 ± 3.85 | 0.47 | |
| Underweight | 4 (1.5) | 2 (1.2) | 2 (2.0) | 0.73a | 0.39 |
| Normal | 170 (61.8) | 108 (62.4) | 62 (60.8) | ||
| Overweight | 83 (30.2) | 56 (32.4) | 27 (26.5) | ||
| Obese | 18 (6.5) | 7 (4.0) | 11 (10.8) | ||
| Eat vegetables | 0.005a | 0.94 | |||
| Daily | 109 (39.6) | 70 (40.5) | 39 (38.2) | ||
| Often | 99 (36.0) | 61 (35.3) | 38 (37.3) | ||
| Sometimes | 64 (23.3) | 39 (22.5) | 25 (24.5) | ||
| None | 3 (1.1) | 3 (1.7) | 0 | ||
| Eat fruits | 0.86b | 0.84 | |||
| Daily | 33 (12.0) | 22 (12.7) | 11 (10.8) | ||
| Often | 42 (15.3) | 24 (13.9) | 18 (17.6) | ||
| Sometimes | 171 (62.2) | 109 (63.0) | 62 (60.8) | ||
| None | 29 (10.5) | 18 (10.4) | 11 (10.8) | ||
| Eat fish, meat, egg or lentil | 0.21a | 0.65 | |||
| Daily | 109 (39.6) | 67 (38.7) | 42 (41.2) | ||
| Often | 83 (30.2) | 51 (29.5) | 32 (31.4) | ||
| Sometimes | 81 (29.5) | 55 (31.8) | 26 (25.5) | ||
| None | 2 (0.7) | 0 | 2 (2.0) | ||
| Drink milk or milk product | 1.40b | 0.71 | |||
| Daily | 57 (20.7) | 39 (22.5) | 18 (17.6) | ||
| Often | 36 (13.1) | 21 (12.1) | 15 (14.7) | ||
| Sometimes | 123 (44.7) | 78 (45.1) | 45 (44.1) | ||
| None | 59 (21.5) | 35 (20.2) | 24 (23.5) | ||
| Smoking status | 73.78b | <0.001 | |||
| Current smoker | 30 (10.9) | 30 (17.3) | 0 | ||
| Former Smoker | 56 (20.4) | 56 (32.4) | 0 | ||
| Never smoked | 189 (68.7) | 87 (50.3) | 102 (100.0) | ||
| Sleep duration per day | 0.06b | 0.97 | |||
| 3-5 hours | 89 (32.4) | 56 (32.4) | 33 (32.4) | ||
| 6-7 hours | 142 (51.6) | 90 (52.0) | 52 (51.0) | ||
| 8-9 hours | 44 (16.0) | 27 (15.6) | 17 (16.7) | ||
| Quality of Life (QoL), mean ± SD | 113.79 ± 16.50 | 116.41 ± 16.23 | 109.33 ± 16.06 | <0.001 | |
| Quality of Life (QoL) score categoriesc | 11.45b | 0.01 | |||
| Bad as can be (less than 99) | 60 (21.8) | 28 (16.2) | 32 (31.4) | ||
| Bad (100 – 119) | 119 (43.3) | 75 (43.4) | 44 (43.1) | ||
| Optimum (120 – 139) | 76 (27.6) | 54 (31.2) | 22 (21.6) | ||
| Good (140 – 159) | 20 (7.3) | 16 (9.2) | 4 (3.9) |
a Fisher’s exact correction test used for having 20% or more expected frequencies less than 5; b Pearson’s Chi-Square; c None of the participants belonged to the highest category (160-175) of QoL scores.
Table 3.
Correlation between quality of life (QoL) scores with sociodemographic factors in elderly population (n = 275).
Table 3.
Correlation between quality of life (QoL) scores with sociodemographic factors in elderly population (n = 275).
| Age | Gender | Marital status | Education | Occupation | Body Mass Index | Sleep duration | OPQOL-35 Score | ||
| Age | r | 1 | -0.170** | 0.114 | -0.035 | -0.106 | -0.013 | -0.031 | -0.128* |
| P | 0.005 | 0.058 | 0.569 | 0.080 | 0.836 | 0.612 | 0.034 | ||
| Gender | r | 1 | 0.288** | -0.316** | 0.596** | 0.047 | 0.004 | -0.208** | |
| P | <0.001 | <0.001 | <0.001 | 0.434 | 0.953 | <0.001 | |||
| Marital status | r | 1 | -0.167** | 0.127* | 0.011 | -0.023 | -0.195** | ||
| P | 0.005 | 0.035 | 0.850 | 0.706 | 0.001 | ||||
| Education | r | 1 | -0.425** | 0.113 | 0.069 | 0.417** | |||
| P | <0.001 | 0.061 | 0.255 | <0.001 | |||||
| Occupation | r | 1 | -0.031 | 0.045 | -0.242** | ||||
| P | 0.614 | 0.462 | <0.001 | ||||||
| Body Mass Index | r | 1 | 0.033 | 0.159** | |||||
| P | 0.589 | 0.008 | |||||||
| Sleep duration | r | 1 | 0.195** | ||||||
| P | 0.001 | ||||||||
| OPQOL-35 Score | r | 1 | |||||||
| P | |||||||||
** Correlation is significant at the 0.01 level (2-tailed); * Correlation is significant at the 0.05 level (2-tailed).
Table 4.
Factors predicting quality of life in elderly people.
| Variablesa | β- coefficient | SE | P-value | 95% CI for β |
| Constant | 91.797 | 6.594 | ||
| Educational status | 3.957 | 0.585 | <0.001 | 2.81 to 5.11 |
| Sleep duration (h) | 4.332 | 1.30 | <0.001 | 1.77 to 6.89 |
| Marital status | -2.259 | 0.90 | 0.013 | -4.03 to -0.488 |
| Body mass index (BMI) | 0.578 | 0.267 | 0.031 | 0.054 to 1.103 |
Variables excluded from the model: age (P = 0.076) and gender (P = 0.228).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



