
Submitted:
26 July 2024
Posted:
29 July 2024
You are already at the latest version
Abstract
Fortified human milk is the first choice for preterm infants. Although individualized fortification is recommended, the optimal method for this population remains uncertain. We conducted a comparative study assessing the growth effects of adjusted (AF) and targeted fortification (TF) in extremely low birth weight (ELBW) infants. This single-center, randomized, controlled clinical trial was conducted at a tertiary neonatal unit in Spain. Eligible participants were premature infants with a birthweight <1000g exclusively fed with human milk. A total of 38 patients were enrolled, 15 of them randomised to AF group and 23 to TF group. AF was based on BUN concentration and TF on human milk analysis. The primary outcome was weight gain velocity (g/kg/day).No significant differences were found in weight gain velocity at 28 days, at 36 weeks of postmenstrual age, at discharge nor during intervention. Protein intake was significantly higher in AF group (5.02 g/kg/day vs 4.48 g/kg/day, p= 0.001). No differences were found in lipids, carbohydrates and energy intake; neither in weight z score change between the different time points; nor in length and head circumference growth. Both AF and TF are comparable methods of fortification and provide appropriate growth rate in ELBW infants.
Keywords:
preterm infants
; neonatal nutrition
; growth
; human milk
; human milk fortification
; blood urea nitrogen
; individualized fortification
1. Introduction
Human milk is the first choice for preterm infants and it is associated with multiple short and long-term benefits [1,2,3,4,5,6,7]. When mother's own milk (MOM) is not available, donor human milk (DHM) is the best alternative [8,9].
Despite its advantages, MOM or DHM do not meet the nutritional requirements of preterm infants, especially in terms of protein, calcium and phosphorus. This is particularly true for extremely low birth weight (ELBW) infants due to their accelerated growth [1,10,11,12,13]. The goal of fortification is to increase the nutrient concentration of human milk (HM) to the level required to optimize growth [8,14,15,16,17,18,19].
There are three approaches for fortifying HM for ELBW infants. Standard fortification (SF), the most widely used strategy, consists of adding a fixed amount of multicomponent fortifier per 100 ml of HM during the entire fortification period [1,16]. This method assumes a fixed estimated HM composition with a protein content of 1.5 g/dL, without considering temporal or inter-individual variations [13]. However, this assumption may not be accurate [20] and this strategy has been shown to lead to suboptimal growth in ELBW infants [15,21,22,23,24].
Individualized fortification is emerging as a potential solution to mitigate the inherent variability in HM composition. However, the optimal fortification strategy remains uncertain [24]. It involves two different methods: adjusted fortification (AF) based on blood urea nitrogen (BUN) concentration as a marker of protein nutrition [26,27,28,29] and targeted fortification (TF) based on regular analysis of HM and fortification adjustment according to the actual macronutrient composition [30,31]. It allows tailor-made fortification to meet the required nutritional recommendations. Despite the theoretical advantages of this nutritional strategy, its implementation involves significant challenges [32,33,34,35,36,37,38].
The aim of this study is to compare the effects of AF and TF on growth and neonatal morbidity in ELBW preterm infants.
2. Materials and Methods
2.1. Study Design
Prospective, single center, randomized, controlled, interventional study performed in a tertiary referral neonatal unit at La Paz University Hospital (Madrid, Spain). The study protocol was approved by the local ethics committee. Written informed parenteral consent was obtained. The trial was registered at ClinicalTrials.gov with identification number NCT04982133.
A Priori Research Hypothesis
Targeted fortification will improve postnatal weight gain and growth over adjusted fortification.
2.2. Participants
Preterm infants with birthweight < 1000 g fed with MOM or DHM were eligible for the study when they reached an enteral feeding volume ≥ 100 mL/kg/day. Exclusion criteria: major congenital malformation, chromosomopathies, metabolic disease or gastrointestinal surgery.
Randomization
Patients whose parents signed the informed consent were randomized to a fortification method. A stratified randomization method based on intrauterine growth restriction (IUGR) defined as birth percentile <3 or <10 with altered prenatal doppler was initially proposed. However, given the low incidence of IUGR in our population, it was changed to a simple randomization method. A list of unique randomization codes was followed and assigned consecutively to each study participant. Siblings of multiple births were randomized individually. It was not possible to blind the medical team to the group allocation but the investigators only did fortification changes. The results of the HM analysis in AF group were blinded until the end of the study.
2.3. Nutritional Intervention
Infants were randomly assigned to one of the two parallel treatment groups on top of standard fortification with a multicomponent fortifier (PreNAN Human milk fortifier™, Nestlé, Vevey, Switzerland) powder with a recommended dosage of 1 g per 25 mL providing an additional 0.7 g of fat, 1.42 g of protein, and 1.3 g of carbohydrates per 100 mL of HM. Study arms were the following: (1) AF modified fortification based on BUN concentration; (2) TF based on HM macronutrient content.
Nutritional intake was assessed twice a week. The intervention was continued until 36 weeks of postmenstrual age (PMA) or until discharge, whichever came first. The study was also discontinued when DHM was replaced by formula due to hospital criteria (weight > 1500 g or age > 6 weeks). Parenteral and enteral feeding regimens were standardized by internal feeding guidelines, which remained unchanged during the study period. The target volume of enteral nutrition was 150-180 ml/kg/day. MOM feeding was supplemented with DHM when necessary to achieve adequate enteral intake.
2.3.1. Adjusted “Modified” Fortification
- BUN < 10 mg/dl: protein fortification was increased one level by adding a protein fortification module [oligopeptides (Clinical Nutrition, SA, Barcelona, Spain) 0.5 g/100 ml, 1 g/100 ml or 1.5 g/100 ml].
- BUN > 16 mg/dl: fortification was decreased one level if growth was adequate. If BUN > 10 mg/dl but growth was inadequate defined as decrease in weight z-score on Fenton curves, an insufficient intake of other macronutrients was inferred, and non-protein kilocalories were supplemented with lipids in the form of medium-chain triglycerides [MCT 1-2 ml/kg (Nutricion Medica, Madrid, Spain)] and glucose polymer powder [0.97 g carbohydrates/g (Fantomalt, Nutricia, Netherlands) 2 g/100 ml].
Multicomponent fortification was never withdrawn regardless of BUN value. The adjusted “modified” fortification scheme is illustrated in Figure 1.
2.3.2. Targeted Fortification
Adjustments were made according to the twice-weekly macronutrient analysis of HM. Monocomponent modules (oligopeptides, MCT or glucose polymer powder) were added to reach the nutritional targets recommended by the European Society of Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) in relation to enteral intake in preterm infants [41]: protein 3.5-4.5 g/kg/day, carbohydrate 11.6-13.2 g/kg/day, lipids 4.8-6.6 g/kg/day and energy 110-135 kcal/kg/day. Initial fortification with the multicomponent fortifier was never withdrawn even though some macronutrients exceeded the nutritional recommendations.
2.4. Analysis of Human Milk
Macronutrient composition analysis of MOM or DHM was performed in both groups twice a week. The analysis focused on the predominant type of human milk, defined as the HM type that represented more than 50% of the intake during the previous 3 days. The analysis was performed on an 8 ml aliquot obtained from a 24-hour pool of fresh HM. If fresh milk was not available, frozen milk was used, thawed 24 hours in a refrigerator at 4 °C, according to recommendations for thawing HM [42]. All samples were analyzed using a milk analyzer based on near infrared (NIR) spectroscopy (MilkoScanTM Mars, FOSS Analytical A/S, Hillerød, Denmark). HM composition of protein (true protein, g/100 ml), carbohydrate (lactose, g/100 ml), and fat (g/100 ml) were obtained, as well as a calculated value of Kcal/100 ml. Regarding energy calculation, we utilized the following standard equation to determine the energy content of human milk: we multiplied grams of protein by 4 kcal/g, grams of carbohydrates by 4 kcal/g, and grams of fats by 9 kcal/g, and summed these values to obtain the total kcal/dL.
Analysis of HM composition is integrated into routine laboratory analysis. Laboratory professionals perform equipment verification and control and they own a quality accreditation (UNE-EN-ISO-15189 standard).
2.5. Biochemical Analyses
In AF group serum urea, calcium, phosphorus and alkaline phosphatase in venous blood was performed weekly. In TF group the same serum measurements were performed, but only 28 days after the beginning of fortification, at 36 weeks PMA and at discharge. Serum urea was determined by the urease method. An automated clinical analyzer (Siemens Atellica Healthineers, Siemens Healthineers, Erlangen, Germany) was used.
2.6. Outcomes
The primary outcome was weight gain velocity (g/kg/day) in the following periods: birth to 28 days after the initiation of fortification, birth to 36 weeks PMA, birth to discharge and during the intervention. Weight was recorded daily to the nearest 5 g using an electronic scale (Kern MBC 15K2DM, Kern and Sohn, Balingen, Germany) or an incubator with adequate calibration (Babyleo TN500, Draeger, Lübeck, Germany).
Weight gain velocity was calculated according to Patel et al formula [43]: [1000 × ln(Wn/W1)]/(Dn − D1), where W1 is the weight at the start and Wn is the weight at the final day of the observation. D1 is the starting day and Dn is the final day of the observation period.
Secondary outcomes were:
- Length and head circumference (HC) growth. Cranial-heel length was measured on a length board in supine position (Añó sayol, Barcelona, Spain), and HC was measured with a non-stretching tape to the nearest 0.5 cm.
- Standard deviation score (SDS) differences, based on Fenton graphs [41], for weight, length and HC between the periods studied (SDS different time points − SDS birth). The research team performed all anthropometric measurements.
- Actual enteral macronutrient intake (g/kg/day and Kcal/kg/day).
- Nutritional achievements: initiation of enteral nutrition (hours), exclusive enteral nutrition (150 ml/kg/day) (days), parenteral nutrition cessation (days), start of HM fortification (days) and volume of enteral feeding at the beginning of fortification (ml/kg/day).
- Predominant HM type (>50% of intake during the study period): MOM or DHM.
- Perinatal characteristics and neonatal morbidities: early-onset sepsis [44], intraventricular hemorrhage ≥ grade II [45], white matter injury [46], significant ductus arteriosus [47,48], necrotizing enterocolitis defined as Bell’s stage > 2 [49], retinopathy [50], moderate-severe bronchopulmonary dysplasia [51,52], cholestasis [53], late-onset sepsis [44] and death.
- Neonatal intensive care unit (NICU) and hospital stay (days).
2.7. Sample Size and Statistical Analysis
Sample size was calculated based on the results of previous studies, where the reported weight gain for TF was 19.9 ± 2.7 g/kg/day [30], and for AF was 17.5 ± 3.2 g/kg/day [26]. The calculation was performed for a test power of 80%, resulting in a sample size of 38 participants. Losses of 15% were assumed.
Qualitative data is described in absolute frequencies and percentages and quantitative data by mean and standard deviation or median and interquartile range, based on its distribution. The normality of the continuous variables was studied using Kolmogorov-Smirnov test.
The association between variables were studied using chi-square test for categorical variable and Student's t-test, as a parametric test, or Mann-Whitney U test, as a non-parametric test, for continuous variables. To study the relationship between quantitative variables, Pearson's correlation, or its non-parametric equivalent Spearman's correlation, were used. Generalized linear repeated measures models were used to assess the relationship between protein intake and urea values.
All statistical tests were considered bilateral and p-values less than 0.05 were considered significant. Data was analyzed with SAS 9.4 statistical software (SAS Institute, Cary, NC).
3. Results
38 patients were included from April 2021 to April 2023 (104 preterm infants <1000g were admitted to the NICU in this period; Figure 2). 15 patients were randomized to AF group and 23 to TF group.
Mean (SD) gestational age was 27 weeks (2) and birth weight (interquartile range-IQR) was 835 g (710-894). Baseline general characteristics were comparable between both arms (Table 1). Other characteristics were as follows in the AF and TF group, respectively: complete lung maturation 87% vs 74%; incidence of chorioamnionitis 13% vs 35%; born by cesarean section 87% vs 74%.
The mean (SD) duration of the intervention was 50 (14) days in the AF group and 46 (16) days in the TF group (p = 0.40).

Table 1.
General characteristics of study population.
| General characteristics of study population | Adjusted fortification (n = 15) | Targeted fortification (n = 23) | p-value |
|---|---|---|---|
|
Gestational age (weeks) Mean (CI 95%) |
27 (26.27, 28.01) | 27 (25.88, 27.79) | 0.64 |
|
Birth weight (g) Mean (CI 95%) |
765 (669.79, 860.74) | 819 (767.77, 870.58) | 0.26 |
|
Birth weight z-score Mean (CI 95%) |
-0.8 (-1.42, -0.38) | -0.9 (-0.79, 0.18) | 0.09 |
|
Length birth (cm) Mean (CI 95%) |
32.5 (31.18, 33.82) | 33.5 (32.51, 34.51) | 0.19 |
|
Head circumference at birth (cm) Mean (CI 95%) |
23.3 (22.42, 24.17) | 23.6 (22.96, 24.16) | 0.58 |
| Male No (%) | 9/15 (60) | 11/23 (47.8) | 0.46 |
| Multiple gestation No (%) | 4/15 (26.7) | 11/23 (47.8) | 0.19 |
|
Umbilical cord pH Median (CI 95%) |
7.29 (7.17, 7.38) | 7.33 (7.23, 7.36) | 0.12 |
|
Initial weight loss (%) Mean (CI 95%) |
6.7 (4.30, 9.43) | 6.18 (4.23, 8.12) | 0.73 |
|
Birth weight regain (day) Median (CI 95%) |
6 (4.86, 7.81) | 7 (5.34, 7.96) | 0.47 |
|
Weight at hospital discharge (g) Mean (CI 95%) |
2691 (2364.26, 3017.07) | 2816 (2543.68, 3088.49) | 0.54 |
|
Length at hospital discharge (cm) Median (CI 95%) |
45 (43.57, 46.50) | 45 (43.96, 46.29) | 0.66 |
|
Head circumference at discharge (cm) Mean (CI 95%) |
33.7 (32.85, 34.45) | 33.2 (32.52, 33.96) | 0.43 |
CI: confidence interval.
3.1. Nutritional Strategy
Enteral nutrition was started at 24 hours in both groups (IQR AF 20-48 hours and TF 20-30 hours, p = 0.5), exclusive enteral nutrition was reached at 17 (IQR 13-26) days in AF group and at 15 (IQR 12-25) days in TF group (p = 0.48). No differences were found between groups in age (SD) at parenteral nutrition discontinuation [AF 17 (7) days vs TF 16 (9) days, p = 0.91].
Fortification was initiated in AF group at 15 (IQR 11-22) days and in TF group at 14 (IQR 10-21) days (p = 0.67). There was no significant difference in the volume of enteral nutrition at which fortification was initiated [AF 146 ml/kg/day (IQR 121-152) vs TF 145 ml/kg/day (IQR 123-155), p = 0.89]. Predominant type of feeding was MOM in both groups with a frequency of 73% in AF group and 52% in TF group (p = 0.192).
No differences were found in HM composition between groups in terms of protein, fat, lactose and energy. Protein intake was significantly higher in AF group [5.02 (0.51) g/kg/day vs 4.48 (0.17) g/kg/day, p = 0.001]. No significant differences were found in lipids, carbohydrates and energy intakes between the two arms (Table 2).
The same number of nutritional assessments were performed in both groups (mean 14, SD 4). Nutritional modifications (IQR) per patient were also similar (AF: 3 (2-4), TF: 4 (2-7); p = 0.165). In AF group non-protein kilocalories were added in 40% of the patients.
Table 2.
Macronutrient analysis of human milk (HM) and actual macronutrient intake in adjusted fortification group and targeted fortification group.
Table 2.
Macronutrient analysis of human milk (HM) and actual macronutrient intake in adjusted fortification group and targeted fortification group.
| HM analyses | Adjusted fortification (n = 15) | Targeted fortification (n = 23) | p-value | Intake | Adjusted fortification (n = 15) | Targeted fortification (n = 23) | p-value |
|---|---|---|---|---|---|---|---|
|
Protein HM (g/100 ml) Mean (CI 95%) |
1.34 (1.25, 1.45) | 1.27 (1.21, 1.35) | 0.20 |
Protein g/kg/day Mean (CI 95%) |
5.02 (4.73, 5.30) | 4.48 (4.41, 4.56) | 0.001 |
|
Lipid HM (g/100 ml) Median (CI 95%) |
7.32 (7.23, 7.77) | 7.61 (7.35, 7.79) | 0.10 |
Lipid g/kg/day Mean (CI 95%) |
7.15 (6.45, 7.85) | 6.56 (6.39, 6.74) | 0.10 |
|
Carbohydrates HM (g/100 ml) Median (CI 95%) |
3.30 (3.16, 3.90) | 3.20 (3.05, 3.34) | 0.80 |
Carbohydrates g/kg/day Mean (CI 95%) |
15.15 (14.09, 16.22) | 15.15 (14.54, 15.76) | 0.99 |
|
Energy HM (kcal/100 ml) Median (CI 95%) |
65.66 (63.67, 69.96) | 64.08 (62.78, 65.57) | 0.156 |
Energy kcal/kg/day Mean (CI 95%) |
144.72 (135.62, 153.83) | 137.63 (134.94, 140.32) | 0.13 |
CI: confidence interval.
3.2. Growth Outcomes
No significant differences were found in weight gain at 28 days after initiation of fortification, at 36 weeks of PMA, at discharge nor during the intervention (Table 3). No differences were observed in the difference in weight z score (SD) between the different studied time points: neither at 28 days after initiation of fortification [AF -0.82 (0.62) vs TF -1.18 (0.60), p = 0.09] nor at 36 weeks PMA [AF -1 (0.67) vs TF -1.23 (0.75), p = 0.36] nor at discharge [AF -0.9 (1.03) vs TF -1.13 (0.57), p = 0.38].
There was no effect of fortification type on length and HC growth, neither assessed in cm/week nor on changes in z score (Table 4).
3.3. Biochemical Parameters
Statistically significant differences were observed in urea at 36 weeks of PMA [AF 23 mg/dl (IQR 21-29 mg/dl) vs TF 15 mg/dl (IQR 11.7-23 mg/dl); p = 0.026] and at the end of the intervention [AF 24 mg/dl (IQR 21-32 mg/dl) vs TF 20 mg/dl (IQR 16-22 mg/dl); p = 0.018]. No differences were found in phosphorus, calcium or alkaline phosphatase values at any point.
A positive correlation was found between protein intake and serum urea concentration (p = 0.002, Figure 3).
3.4. Neonatal Morbidity and Hospital Stay
No differences were found in the main neonatal outcomes except for the presence of significant ductus arteriosus (AF group 47% vs TF group 78%, p = 0.045). Late onset sepsis was highly prevalent in both groups, with at least one episode of sepsis in 53% of patients in AF group and 65% in TF group (p = 0.46).
No differences were found in NICU stay (SD) [59 (34) days in AF group vs 58 (26) days in TF group, p = 0.915], hospital stay [84 (IQR 74-102) days in AF vs 81 (IQR 74-102) days in TF, p = 0.79] and PMA at discharge [39.1 (IQR 38.4-40.6) weeks vs 38.4 (IQR 37.9-40.3) weeks p = 0.40]. There was no difference in weight (SD) at the end of the intervention [2127 (481) g vs 2120 (437) g, p = 0.96] nor at hospital discharge [2690.7 (589.4) g vs 2816.1 (630) g, p = 0.542].
4. Discussion
The present study demonstrates no differences on postnatal weight gain and growth between AF and TF at different times of analysis. To our knowledge, this study is unique with respect to increased energy intakes and measurement of actual macronutrient intake in both groups. Our study took a rigorous approach to investigate the impact of individual fortification on growth of ELBW preterm infants. Previous studies have demonstrated the benefit in growth of TF vs SF [30,54,55,56]. A randomized clinical trial (RCT) comparing the three fortification methods found similar weight gain in AF and TF group but higher than SF. In this study protein intake was significantly higher in the individualized versus SF group (protein intake was 4.3 g/kg/day in AF group, 4.5 g/kg/day in TF group and 3.6 g/kg/day in SF group) [57].
Rochow et al [58] compared SF with TF. Similar to our study, fortification was initiated with a standard fortifier and fortification modules were added to adjust all HM macronutrients. The modules used for fat and protein fortification were different from ours. They found greater weight at 36 weeks and greater growth velocity in TF group.
However, few studies have compared AF method with TF. Bulut et al [59] compared the effect on growth of AF versus TF finding a positive effect on growth in TF group. Only protein was supplemented in both fortification groups and BUN limit used to increase protein intake was lower than in our study (5 mg/dl vs 10 mg/dl).
Different from Arslanoglu et al [26,27], that only increased protein intake, we increased caloric intake in the form of non-protein kilocalories for those patients with an inadequate growth response despite acceptable BUN concentration. This "modified" adjusted method, with a more complete adjustment, might justify the absence of differences in growth between the two groups.
Protein intake is the main growth factor when energy intake is appropriate [25,60]. In our study, protein intake in TF group was within the recommended range [25], meanwhile AF group exceeded the nutritional recommendations with a protein intake of 5.02 g/kg/day. This “superfortification” was not linked to a corresponding rise in non-protein kilocalories, as no differences were found in energy, carbohydrate, and lipid intake. Therefore, as energy intake becomes a limiting factor when protein intake is high, it is likely that protein intakes > 4.5 g/kg/day were not associated with a parallel increase in growth due to an inability to metabolize these proteins. Other explanation maybe a potential ceiling effect for enteral protein supply, at least for the population studied, indicating that an enteral protein intake exceeding 4.5 g/kg/d might not further improve weight gain in this population. Our results are in line with data recently reported by Miller et al [61], who also found no influence of increased enteral protein intake on weight gain in infants of similar gestational age at birth.
Plasma urea, the product of amino acid oxidation, is considered an estimator of protein intake. A target urea level of 21-34 mg/dl or BUN 10-16 mg/dl has been proposed with limited evidence [1]. We found significantly higher urea levels in the high protein intake group and a positive correlation between protein intake and plasma urea levels. This finding is consistent with other authors supporting the use of serum urea as an estimator of protein intake but appropriate levels should be defined [62].
Average growth rates during intervention were 16-17 g/kg/day, lower than previously reported with similar protein intakes but in recommended ranges [25,58]. In our study, late-onset sepsis was not an exclusion criterion, possibly explaining lower weight gain. As growth is similar between both groups, it is not surprising that no differences are found in the main neonatal morbidities nor hospital stay.
On the other hand, we used modular products for enteral feeding available in our NICU but evidence is scarce on their optimal composition for individual fortification.
Each method of fortification has several advantages and disadvantages. AF does not require a HM analyzer and urea determinations are part of routine blood tests in newborns. However, it requires frequent blood samples involving pain, discomfort and risk of anemia. AF may also involve a delay in nutritional adjustment as a metabolic response is needed [26,63].
TF has the advantage of adapting to changes in HM composition and adjusting different macronutrients to meet nutritional recommendations. The number of times per week that HM should be tested to achieve an accurate intake has not been defined. Several studies suggest that twice-weekly HM testing may provide adequate macronutrient intakes [33,64]. In addition, it requires the availability of trained staff in sample collection and maintenance and calibration of the HM analyzer. Therefore, it implies the need to consider material and human resources for its implementation. In any case, both fortification methods in our study required comparable nutritional modifications.
The strengths of the present study are the determination of actual macronutrient intakes with twice-weekly milk analyses in all infants and the length of intervention larger than previous studies. The macronutrients intake analysis in both groups make possible to evaluate the effect of both types of fortification on macronutrient intake. The study had limitations due to the inability to stratify by IUGR. However, a multivariate analysis was conducted to assess the impact of IUGR on the response variables, with no significant effect observed. In addition, a minor error in the estimation of macronutrient intake was accepted, as we based it on the composition of the predominant HM and on two days measurement per week of estimated intakes. These approaches allowed the study applicability in case results would be positive. Furthermore, the attending physician was not blinded having the possibility of visualizing serum urea in TF group. This did not cause any bias since the research team always established the nutritional strategy.
5. Conclusions
Both AF and TF provide adequate growth rate in ELBW infants. Therefore, the most plausible individualized fortification method should be chosen according to the resources available. To verify effects on neurocognitive outcome larger follow up is needed.
Author Contributions
Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data: M.S.H., M.S.P., M.C.J., G.C.S., M.M.L., M.T.M., C.S., I.L., M.J., E.E., M.C.L. Drafting the article or revising it critically for important intellectual content: M.S.H., M.S.P., M.C.L. Final approval of the version to be published: M.S.H., M.S.P., M.C.J., G.C.S., M.M.L., M.T.M., C.S., I.L., E.E., M.C.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of La Paz University Hospital (ethical approval code HULP: 5704, date 30 November 2020)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. Researchers submitting a methodologically sound proposal should contact miguel.saenz@salud.madrid.org. In order to access, requesters will need to sign a data access agreement.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Arslanoglu, S.; Boquien, C.Y.; King, C.; Lamireau, D.; Tonetto, P.; Barnett, D.; Bertino, E.; Gaya, A.; Gebauer, C.; Grovslien, A.; Moro, G.E.; Weaver, G.; Wesolowska, A.M.; Picaud, J.C. Fortification of Human Milk for Preterm Infants: Update and Recommendations of the European Milk Bank Association (EMBA) Working Group on Human Milk Fortification. Front. Pediatr. 2019, 7, 76. [Google Scholar] [CrossRef] [PubMed]
- Chetta, K.E.; Schulz, E.V.; Wagner, C.L. Outcomes improved with human milk intake in preterm and full-term infants. Semin. Perinatol. 2021, 45, 151384. [Google Scholar] [CrossRef] [PubMed]
- Sisk, P.M.; Lovelady, C.A.; Gruber, K.J.; Dillard, R.G.; O'Shea, T.M. Human milk consumption and full enteral feeding among infants who weigh ≤1250 grams. Pediatrics 2008, 121, 2007–2110. [Google Scholar] [CrossRef] [PubMed]
- Schanler, R.J. Evaluation of the evidence to support current recommendations to meet the needs of premature infants: the role of human milk. Am. J. Clin. Nutr. 2007, 85, 625S–628S. [Google Scholar] [CrossRef]
- Vohr, B.R.; Poindexter, B.B.; Dusick, A.M.; McKinley, L.T.; Higgins, R.D.; Langer, J.C.; Poole, W.K.; Wright, L.L.; Bauer, C.R.; Meinzen-Derr, J.; Parrott, R.H. Persistent beneficial effects of breast milk ingested in the neonatal intensive care unit on outcomes of extremely low birth weight infants at 30 months of age. Pediatrics 2007, 120, e953–e959. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.; Schanler, R.J.; Kim, J.H.; Patel, A.L.; Trawöger, R.; Kiechl-Kohlendorfer, U.; Chan, G.M.; Blanco, C.L.; Abrams, S.; Cotton, C.M.; Laroia, N.; Ehrenkranz, R.A.; Dudell, G.; Cristofalo, E.A.; Meier, P.P.; Lee, M.L.; Rechtman, D.J.; Lucas, A. An exclusively human milk-based diet is associated with a lower rate of necrotizing enterocolitis than a diet of human milk and bovine milk-based products. J. Pediatr. 2010, 156, 562–567.e1. [Google Scholar] [CrossRef] [PubMed]
- Meinzen-Derr, J.; Poindexter, B.B.; Wrage, L.A.; Morrow, A.L.; Stoll, B.J.; Ehrenkranz, R.A. Role of human milk in extremely low birth weight infants' risk of necrotizing enterocolitis or death. J. Perinatol. 2009, 29, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Arslanoglu, S.; Ziegler, E.E.; Moro, G.E. Donor human milk for preterm infants: current evidence and research directions. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Quigley, M.; Embleton, N.D.; McGuire, W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst. Rev. 2019, 7, CD002971. [Google Scholar] [CrossRef]
- Bergner, E.M.; Taylor, S.N.; Gollins, L.A.; Hair, A.B. Human Milk Fortification: A Practical Analysis of Current Evidence. Clin. Perinatol. 2022, 49, 447–460. [Google Scholar] [CrossRef]
- Hair, A.B.; Scottoline, B.; Good, M. Dilemmas in human milk fortification. J. Perinatol. 2023, 43, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Wojcik, K.Y.; Rechtman, D.J.; Lee, M.L.; Montoya, A.; Medo, E.T. Macronutrient analysis of a nationwide sample of donor breast milk. J. Am. Diet. Assoc. 2009, 109, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.T.; Poindexter, B.B. Human Milk Fortification Strategies in the Neonatal Intensive Care Unit. Clin. Perinatol. 2023, 50, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Moro, G.E.; Benso, L.; Brovedani, P.; Cerbo, R.; Coscia, A.; Ferrero, I.; Finessi, M.; Migliore, S.; Nosetti, L.; Bertino, E. XII. Human Milk in Feeding Premature Infants: Consensus Statement. J. Pediatr. Gastroenterol. Nutr. 2015, 61 (Suppl 1), S16–S19. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Moro, G.E.; Ziegler, E.E.; The WAPM Working Group on Nutrition. Optimization of human milk fortification for preterm infants: new concepts and recommendations. J. Perinat. Med. 2010, 38, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Radmacher, P.G.; Adamkin, D.H. Fortification of human milk for preterm infants. Semin. Fetal Neonatal Med. 2017, 22, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, E.E. Human milk and human milk fortifiers. World Rev. Nutr. Diet. 2014, 110, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Hay, W.W.; Ziegler, E.E. Growth failure among preterm infants due to insufficient protein is not innocuous and must be prevented. J. Perinatol. 2016, 36, 500–502. [Google Scholar] [CrossRef] [PubMed]
- Beggs, M.R.; Bando, N.; Unger, S.; O'Connor, D.L. State of the evidence from clinical trials on human milk fortification for preterm infants. Acta Paediatr. 2022, 111, 1115–1120. [Google Scholar] [CrossRef]
- Cabrera Lafuente, M.; Manzanedo, R.; Estévez, M.; Segura, A. A prospective analysis of intake and composition of mother's own milk in preterm newborns less than 32 weeks' gestational age. J. Perinat. Med. 2018, 47, 106–113. [Google Scholar] [CrossRef]
- Ehrenkranz, R.A.; Younes, N.; Lemons, J.A.; Fanaroff, A.A.; Donovan, E.F.; Wright, L.L.; Katsikiotis, V.; Tyson, J.E.; Oh, W.; Shankaran, S.; et al. Growth in the neonatal intensive care unit influences neurodevelopmental and growth outcomes of extremely low birth weight infants. Pediatrics 2006, 117, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Fabrizio, V.; Turoli, D.; Da Frè, M.; Fanni, G.; Munno, A.; Stefanelli, A.; Zamprogna, S.; De Cunto, A. Individualized versus standard diet fortification for growth and development in preterm infants receiving human milk. Cochrane Database Syst. Rev. 2020, 11, CD013465. [Google Scholar] [CrossRef] [PubMed]
- Arslanoglu, S.; Moro, G.E.; Ziegler, E.E. Preterm infants fed fortified human milk receive less protein than they need. J. Perinatol. 2009, 29, 489–492. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.K.; Singhal, A.; Vaidya, U.; Banerjee, S.; Anwar, F.; Rao, S.; Modi, N.; Narang, A.; Sriram, K. Optimizing Nutrition in Preterm Low Birth Weight Infants-Consensus Summary. Front. Nutr. 2017, 4, 20. [Google Scholar] [CrossRef] [PubMed]
- Embleton, N.D.; Berrington, J.E.; McGuire, W.; Stewart, C.J.; Cummings, S.P. Enteral Nutrition in Preterm Infants (2022): A Position Paper From the ESPGHAN Committee on Nutrition and Invited Experts. J. Pediatr. Gastroenterol. Nutr. 2023, 76, 248–268. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Moro, G.E.; Ziegler, E.E. Adjustable fortification of human milk fed to preterm infants: does it make a difference? J. Perinatol. 2006, 26, 614–621. [Google Scholar] [CrossRef]
- Arslanoglu, S.; Corpeleijn, W.; Moro, G.E.; Braegger, C.; Campoy, C.; Colomb, V.; Decsi, T.; Domellöf, M.; Fewtrell, M.; Hojsak, I.; et al. Update of adjustable fortification regimen for preterm infants: a new protocol. J. Biol. Regul. Homeost. Agents 2012, 26 (Suppl. 3), 65–67. [Google Scholar]
- Arslanoglu, S. IV. Individualized Fortification of Human Milk: Adjustable Fortification. J. Pediatr. Gastroenterol. Nutr. 2015, 61 (Suppl 1), S4–S5. [Google Scholar] [CrossRef]
- Adamkin, D.H. Use of human milk and fortification in the NICU. J. Perinatol. 2023, 43, 551–559. [Google Scholar] [CrossRef]
- Rochow, N.; Fusch, G.; Choi, A.; Chessell, L.; Elliott, L.; McDonald, K.; Kuiper, E.; Purcha, M.; Turner, S.; Chan, E.; Fusch, C. Target fortification of breast milk with fat, protein, and carbohydrates for preterm infants. J. Pediatr. 2013, 163, 1001–1007. [Google Scholar] [CrossRef]
- Merlino Barr, S.; Groh-Wargo, S. Targeted fortification with human milk analysis: An opportunity for innovation. Semin. Fetal Neonatal Med. 2022, 27, 101392. [Google Scholar] [CrossRef]
- Gidrewicz, D.A.; Fenton, T.R. A systematic review and meta-analysis of the nutrient content of preterm and term breast milk. BMC Pediatr. 2014, 14, 216. [Google Scholar] [CrossRef] [PubMed]
- Rochow, N.; Fusch, G.; Choi, A.; Chessell, L.; Elliott, L.; McDonald, K.; Kuiper, E.; Purcha, M.; Turner, S.; Chan, E.; Fusch, C. Target fortification of breast milk: how often should milk analysis be done? Nutrients 2015, 7, 2297–2310. [Google Scholar] [CrossRef] [PubMed]
- Kwan, C.; Fusch, G.; Bahonjic, A.; Rochow, N.; Fusch, C. Infrared analyzers for breast milk analysis: fat levels can influence the accuracy of protein measurements. Clin. Chem. Lab. Med. 2017, 55, 1931–1935. [Google Scholar] [CrossRef] [PubMed]
- Parat, S.; Groh-Wargo, S.; Merlino, S.; Wijers, C.; Super, D.M. Validation of mid-infrared spectroscopy for macronutrient analysis of human milk. J. Perinatol. 2017, 37, 822–826. [Google Scholar] [CrossRef] [PubMed]
- Fusch, G.; Kwan, C.; Kotrri, G.; Fusch, C. "Bed Side" Human Milk Analysis in the Neonatal Intensive Care Unit: A Systematic Review. Clin. Perinatol. 2017, 44, 209–267. [Google Scholar] [CrossRef]
- Buffin, R.; Pinon, P.; Winer, N.; Lizee, S.; Guillet, R.; Bouderlique, C.; Laffont, I.; Jourdes, E.; Darmaun, D.; Rozé, J.C. Assessment of human milk composition using mid-infrared analyzers requires calibration adjustment. J. Perinatol. 2017, 37, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Ramey, S.R.; Merlino Barr, S.; Moore, K.A.; Groh-Wargo, S. Exploring Innovations in Human Milk Analysis in the Neonatal Intensive Care Unit: A Survey of the United States. Front. Nutr. 2021, 8, 692600. [Google Scholar] [CrossRef] [PubMed]
- Fenton, T.R. A new growth chart for preterm babies: Babson and Benda's chart updated with recent data and a new format. BMC Pediatr. 2003, 3, 13. [Google Scholar] [CrossRef]
- Fenton, T.R.; Anderson, D.; Groh-Wargo, S.; Hoyos, A.; Ehrenkranz, R.A. Accuracy of preterm infant weight gain velocity calculations vary depending on method used and infant age at time of measurement. Pediatr. Res. 2019, 85, 650–654. [Google Scholar] [CrossRef]
- Agostoni, C.; Buonocore, G.; Carnielli, V.P.; De Curtis, M.; Darmaun, D.; Decsi, T.; Domellöf, M.; Embleton, N.D.; Fusch, C.; Genzel-Boroviczeny, O.; et al. Enteral nutrient supply for preterm infants: commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Steele, C. Best Practices for Handling and Administration of Expressed Human Milk and Donor Human Milk for Hospitalized Preterm Infants. Front. Nutr. 2018, 5, 76. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.L.; Engstrom, J.L.; Meier, P.P.; Kimura, R.E. Accuracy of methods for calculating postnatal growth velocity for extremely low birth weight infants. Pediatrics 2005, 116, 1466–1473. [Google Scholar] [CrossRef]
- Celik, I.H.; Hanna, M.; Canpolat, F.E.; Mohan, P. Diagnosis of neonatal sepsis: the past, present and future. Pediatr. Res. 2022, 91, 337–350. [Google Scholar] [CrossRef]
- Parodi, A.; Govaert, P.; Horsch, S.; Bravo, M.C.; Ramenghi, L.A.; eurUS.brain group. Cranial ultrasound findings in preterm germinal matrix haemorrhage, sequelae and outcome. Pediatr. Res. 2020, 87 (Suppl 1), 13–24. [Google Scholar] [CrossRef] [PubMed]
- Agut, T.; Gosselin, J.; Dong, W.; Fortin-Pellerin, E.; Saint-Martin, C.; Brochu, M.E. Preterm white matter injury: ultrasound diagnosis and classification. Pediatr. Res. 2020, 87 (Suppl 1), 37–49. [Google Scholar] [CrossRef]
- van Laere, D.; van Overmeire, B.; Schepens, P.; Smits, M.; Devlieger, H. Application of NPE in the assessment of a patent ductus arteriosus. Pediatr. Res. 2018, 84 (Suppl 1), 46–56. [Google Scholar] [CrossRef] [PubMed]
- de Boode, W.P.; Kluckow, M.; McNamara, P.J.; Gupta, S. Role of neonatologist-performed echocardiography in the assessment and management of patent ductus arteriosus physiology in the newborn. Semin. Fetal Neonatal Med. 2018, 23, 292–297. [Google Scholar] [CrossRef]
- Bell, M.J.; Ternberg, J.L.; Feigin, R.D.; Keating, J.P.; Marshall, R.; Barton, L.; Brotherton, T. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann. Surg. 1978, 187, 1–7. [Google Scholar] [CrossRef]
- Chiang, M.F.; Quinn, G.E.; Fielder, A.R.; Ostmo, S.R.; Paul Chan, R.V.; Berrocal, A.; Flynn, J.T.; Hammersmith, J.A.; Hubbard, G.B.; Kushner, B.J.; et al. International Classification of Retinopathy of Prematurity, Third Edition. Ophthalmology 2021, 128, e51–e68. [Google Scholar] [CrossRef]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef] [PubMed]
- Bancalari, E.; Jain, D. Bronchopulmonary Dysplasia: Can We Agree on a Definition? Am. J. Perinatol. 2018, 35, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Davis, A.R.; Rosenthal, P.; Escobar, G.J.; Newman, T.B. Interpreting conjugated bilirubin levels in newborns. J. Pediatr. 2011, 158, 562–565. [Google Scholar] [CrossRef]
- De Halleux, V.; Close, A.; Stalport, S.; Studzinski, F.; Habibi, F.; Rigo, J. Intérêt de la supplémentation du lait maternel << à la carte>> [Advantages of individualized fortification of human milk for preterm infants]. Arch. Pediatr. 2007, 14 (Suppl 1), S5–S10. [Google Scholar] [PubMed]
- De Halleux, V.; Rigo, J. Variability in human milk composition: benefit of individualized fortification in very-low-birth-weight infants. Am. J. Clin. Nutr. 2013, 98, 529S–535S. [Google Scholar] [CrossRef]
- Morlacchi, L.; Mallardi, D.; Giannì, M.L.; Roggero, P.; Amato, O.; Piemontese, P.; Mosca, F. Is targeted fortification of human breast milk an optimal nutrition strategy for preterm infants? An interventional study. J. Transl. Med. 2016, 14, 195. [Google Scholar] [CrossRef]
- Kadıoğlu Şimşek, G.; Tayman, C.; Aydemir, O.; Altun, H.; Bağcı, O. Comparison of the Effect of Three Different Fortification Methods on Growth of Very Low Birth Weight Infants. Breastfeed. Med. 2019, 14, 63–68. [Google Scholar] [CrossRef]
- Rochow, N.; Fusch, G.; Ali, A.; Fusch, C. Individualized target fortification of breast milk with protein, carbohydrates, and fat for preterm infants: A double-blind randomized controlled trial. Clin. Nutr. 2021, 40, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Bulut, O.; Coban, A.; Uzunhan, O.; Ince, Z. Effects of Targeted Versus Adjustable Protein Fortification of Breast Milk on Early Growth in Very Low-Birth-Weight Preterm Infants: A Randomized Clinical Trial. Nutr. Clin. Pract. 2020, 35, 335–343. [Google Scholar] [CrossRef]
- Ziegler, E.E.; Thureen, P.J.; Carlson, S.J. Aggressive nutrition of the very low birthweight infant. Clin. Perinatol. 2002, 29, 225–244. [Google Scholar] [CrossRef]
- Miller, J.; Makrides, M.; Gibson, R.A.; McPhee, A.J.; Stanford, T.E.; Morris, S.; Huang, R.C.; Ryan, P.; Collins, C.T. Effect of increasing protein content of human milk fortifier on growth in preterm infants born at <31 wk gestation: a randomized controlled trial. Am. J. Clin. Nutr. 2012, 95, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Mathes, M.; Briana, D.D.; Bergmann, R.; Schuller, A.; Göpel, W.; Herting, E.; Kattner, E.; Windhorst, A.; Klerk, J.P.D.; Maier, R.F. Effect of increased enteral protein intake on plasma and urinary urea concentrations in preterm infants born at < 32 weeks gestation and < 1500 g birth weight enrolled in a randomized controlled trial—A secondary analysis. BMC Pediatr. 2018, 18, 154. [Google Scholar] [CrossRef]
- Rochow, N.; Landau-Crangle, E.; Fusch, C. Challenges in breast milk fortification for preterm infants. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 276–284. [Google Scholar] [CrossRef] [PubMed]
- Fusch, S.; Rochow, N.; Choi, A.; Fusch, C. Individualized Target Fortification of Breast Milk: Optimizing Macronutrient Content Using Different Fortifiers and Approaches. Front. Nutr. 2021, 8, 652641. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Adjusted “modified” fortification scheme. Adequate growth was defined as no decrease in weight z-score on Fenton curves compared to the weight measurement obtained during the previous weekly nutritional assessment.
Figure 1.
Adjusted “modified” fortification scheme. Adequate growth was defined as no decrease in weight z-score on Fenton curves compared to the weight measurement obtained during the previous weekly nutritional assessment.
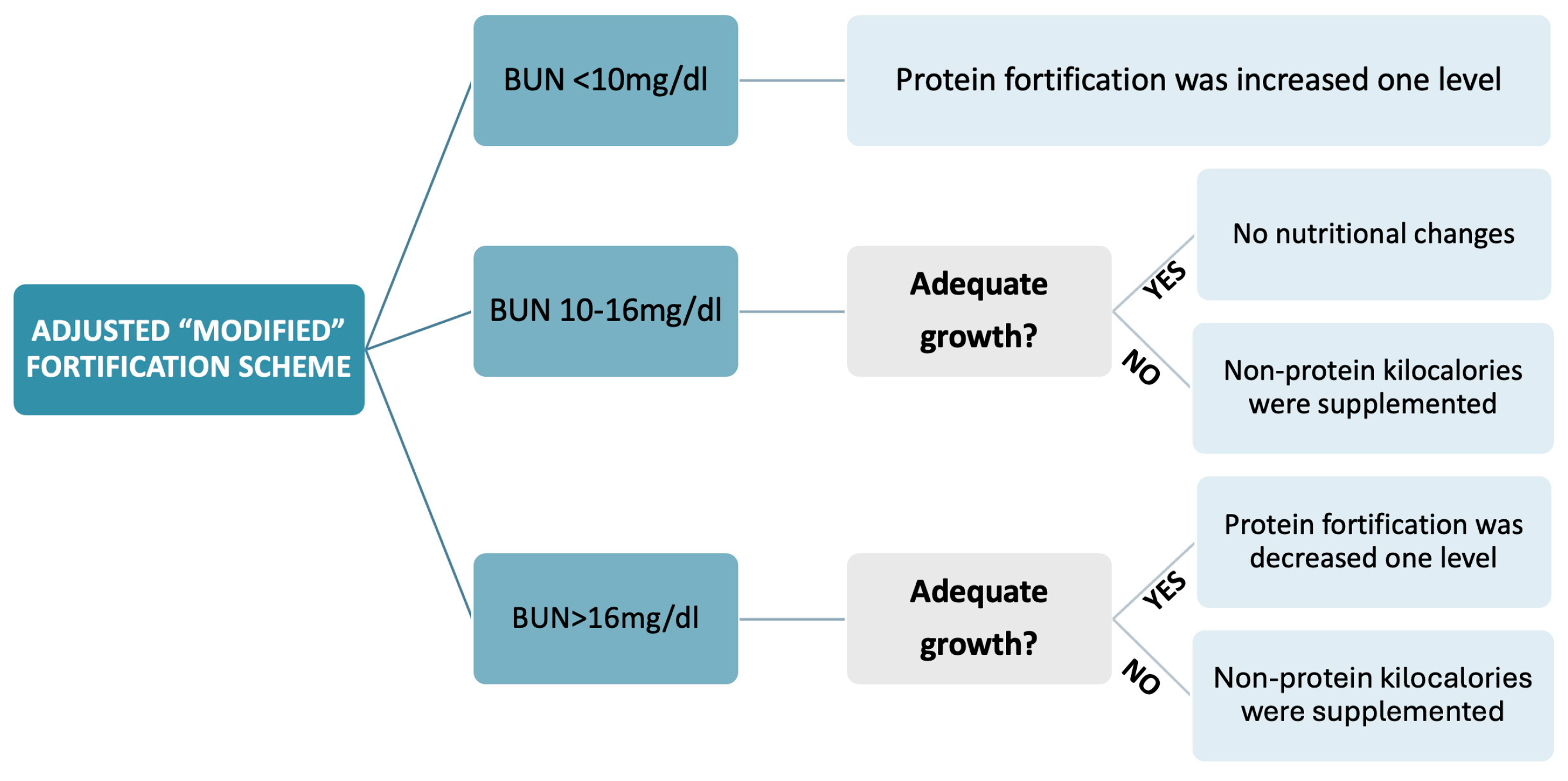
Figure 2.
CONSORT flow chart.
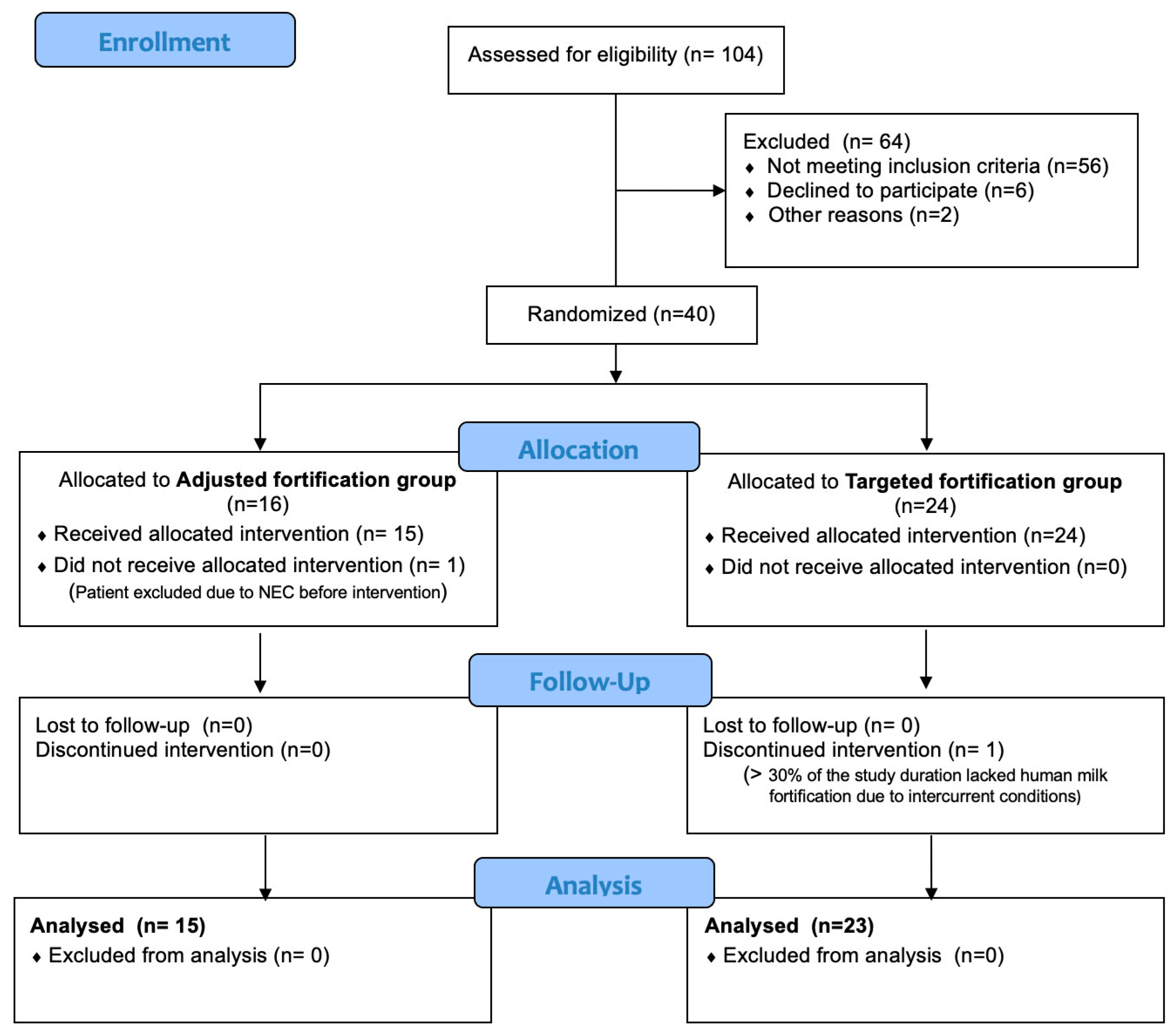
Figure 3.
Correlation between protein intake and serum urea concentration.
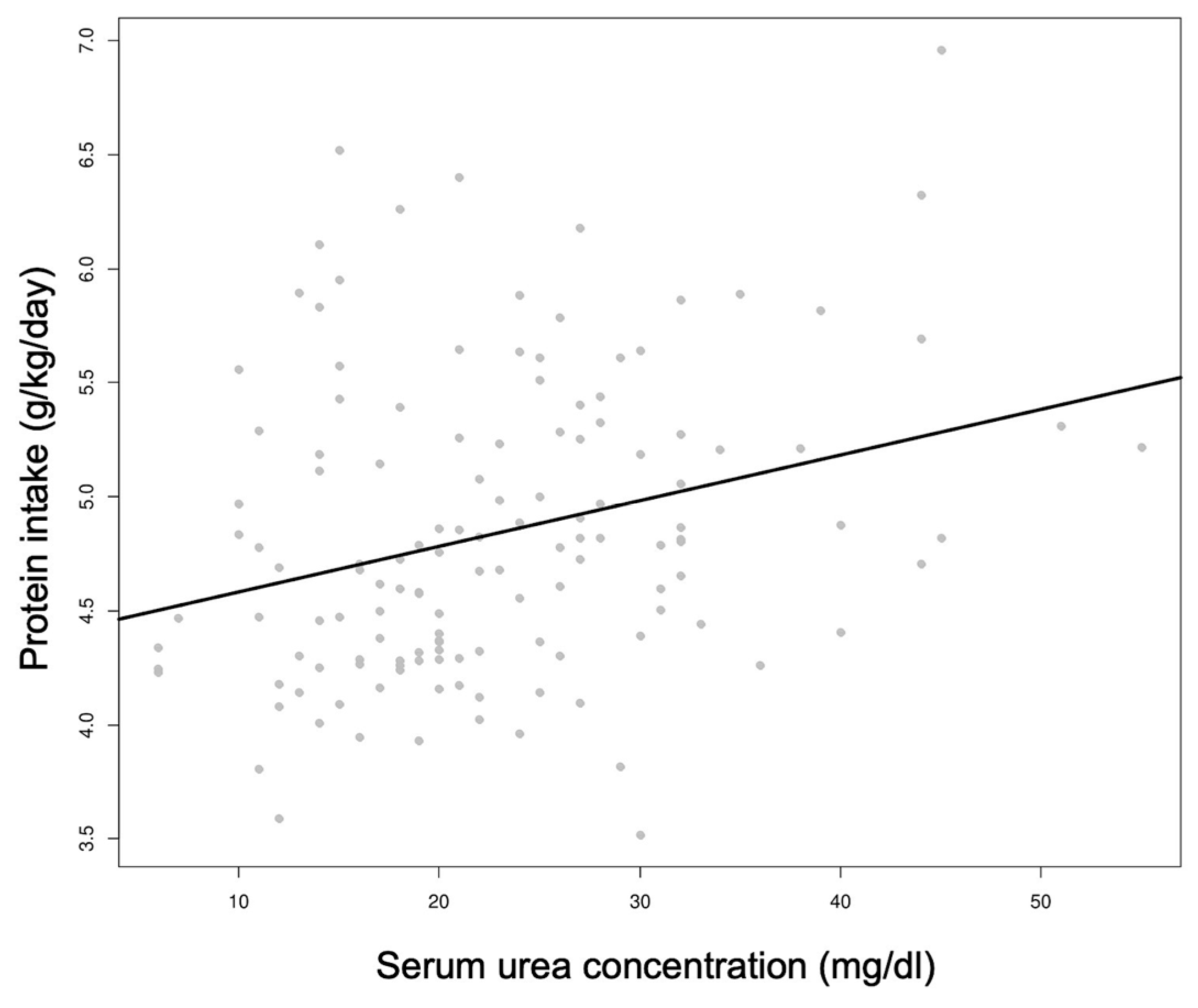
Table 3.
Weight gain (g/kg/day) in adjusted fortification group and targeted fortification group.
| Weight gain g/kg/day | Adjusted fortification (n = 15) | Targeted fortification (n = 23) | p-value |
|---|---|---|---|
|
From birth to 28 days from the start of HM fortification Mean (CI 95%) |
14.06 (12.31, 15.81) | 13.24 (12.13, 14.36) | 0.38 |
|
From birth to 36 weeks PMA Median (CI 95%) |
15.31 (13.37, 16.42) | 14.02 (13.16, 16.41) | 0.53 |
|
From birth to discharge Median (CI 95%) |
14.53 (13.01, 15.46) | 14.04 (13.35, 15.12) | 0.68 |
|
During the intervention Mean (CI 95%) |
16.33 (15.26, 17.40) | 16.89 (15.44, 18.34) | 0.56 |
PMA: Postmenstrual age. CI: confidence interval.
Table 4.
Length and head circumference growth in adjusted fortification group and targeted fortification group.
Table 4.
Length and head circumference growth in adjusted fortification group and targeted fortification group.
| Length growth cm/week | Adjusted fortification (n = 15) | Targeted fortification (n = 23) | p-value | Head circumference growth cm/week | Adjusted fortification (n = 15) | Targeted fortification (n = 23) | p-value |
|---|---|---|---|---|---|---|---|
|
From birth to 28 days from the start of HM fortification Mean (CI 95%) |
0.91 (0.78, 1.05) | 0.86 (0.74, 0.98) | 0.536 |
From birth to 28 days from the start of HM fortification Mean (CI 95%) |
0.78 (0.65, 0.93) | 0.73 (0.64, 0.83) | 0.44 |
|
From birth to 36 weeks PMA Median (CI 95%) |
0.95 (0.89, 1.08) | 0.88 (0.70, 1.49) | 0.38 |
From birth to 36 weeks PMA Median (CI 95%) |
0.85 (0.76, 0.94) | 0.86 (0.70, 1.18) | 0.86 |
|
From birth to discharge Median (CI 95%) |
0.91 (0.89, 1.07) | 0.94 (0.79, 1.33) | 0.47 |
From birth to discharge Median (CI 95%) |
0.83 (0.75, 0.91) | 0.79 (0.67, 1.09) | 0.41 |
PMA: Postmenstrual age. CI: confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



