
Submitted:
29 July 2024
Posted:
29 July 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
This systematic examines research into patients diagnosed with retinal vascular occlusive diseases (RVODs) secondary to coronavirus disease 2019 (COVID-19) infection or vaccination. RVODs include central retinal vein occlusion, branch retinal vein occlusion, central retinal artery occlusion, and branch retinal artery occlusion. Previous studies have posited a possible link between RVODs and COVID-19. RVODs are of two types: retinal vein occlusion and retinal artery occlusion. These disorders develop when retinal blood vessels become clogged by thrombi or fat deposition. The retina is an important component of the visual apparatus. Its photoreceptors are stimulated by the light hitting the eye and record its pattern. The retina then relays this visual information to the brain. When retinal blood vessels become clogged, the damage can range from slightly reduced vision to complete blindness. COVID-19 causes endothelial dysfunction and increased levels of von Willebrand factor antigens in the blood. Elevation of von Willebrand factor activates the coagulation process and platelet aggregation. The treatment methods and visual prognosis in COVID-19-related RVODs do not differ from conventional RVODs. However, ophthalmologists need to be aware of the possible relationship and should consider RVODs when they encounter patients with vision loss following COVID-19 infection or vaccination.
Keywords:
branch retinal artery occlusion
; branch retinal vein occlusion
; central retinal artery occlusion
; central retinal vein occlusion
; COVID-19
; retinal vascular occlusive disease
1. Introduction
The coronavirus disease 2019 (COVID-19) has had huge global health implication and continues to ravage healthcare systems around the world [1]. COVID-19 infection can be followed by multi-organ pathology and vascular damage [2] that, in turn, increases the risk of fatal vascular occlusive diseases such as thrombosis, myocardial infarction, arrhythmia, and cerebral apoplexy [3,4,5,6]. Elevation of thrombotic tendencies and increased risk of thrombosis have been found to persist for several months after COVID-19 infection [7].
Fundus photography (which is fast and noninvasive) and fundoscopic examination of the ocular fundus give ophthalmologists direct access to the retina and its vasculature. The retinal arteries and veins are believed to be representative of the state of the body’s entire microvascular system [8]. Therefore, it is advisable for ophthalmologists to check for any vascular abnormalities caused by COVID-19 following infection. It has been posited that the increased risk of thrombosis caused by COVID-19 may be associated with the development of retinal vascular occlusive diseases (RVODs).
RVODs include retinal vein occlusion (RVO) and retinal artery occlusion (RAO). Both of these are subdivided into central and branch occlusions, i.e., central retinal vein occlusion (CRVO), central retinal artery occlusion (CRAO), branch retinal vein occlusion (BRVO), and branch retinal artery occlusion (BRAO). After diabetic retinopathy, RVO is the most common retinal vascular disease [9]. The prevalence of RVOs in the developed world is 5.2 per 1,000, while that of CRVOs is 0.8 per 1,000 [10].
In CRVO, sudden visual impairment is common; while in BRVO, visual field defects and shape distortion are typical symptoms. RVOs affect visual function and are characterized by retinal hemorrhage, soft exudate, and macula edema. CRVO can be classified as ischemic or nonischemic. The ischemic type of CRVO can cause neovascular glaucoma and blindness. The primary treatment methods are anti-vascular endothelial growth factor (VEGF) antibodies and retinal photocoagulation [11,12,13]. Since the introduction of anti-VEGF antibodies, there has been a significant improvement in the prognoses for these conditions [13].
RAO is an acute disease in which the occlusion usually causes sudden visual reduction. If retinal blood flow does not return promptly, at least some visual reduction and visual field defects will be permanent. Although many treatment methods are reported [14,15], there is not yet an established standardized treatment and RAO remain difficult to treat. Yet, RAO carries a risk of cardiovascular events [16], such as cerebral stroke and may also be a symptom of a systemic condition. The visual prognosis for CRAO is poor and decimal visual acuity (VA) usually falls below 0.05 [17].
RVODs are relatively common disorders that can cause severe visual impairment. Risk factors for RVODs include hypercoagulability and thrombotic disorders. In this review, we investigate the relationship between COVID-19 and RVODs.
2. Mechanism of Vascular Occlusion of COVID-19
Severe acute respiratory syndrome-related coronavirus 2 (SARS-CoV-2), the virus that causes COVID-19, invades cells by attaching to angiotensin-converting enzyme 2 (ACE2) proteins [18,19]. COVID-19-associated coagulopathy increases the generation of the coagulation factor, thrombin, in the veins and arteries. This phenomenon is strongly correlated with vascular endothelial damage [20,21]. Vascular endothelial cells infected with SARS-CoV-2 release through ACE 2 release von Willebrand factor and angiopoietin 2. Von Willebrand factor causes platelets to adhere to the connective tissue under vascular endothelial cells and this becomes a foothold for thrombin [22]. ACE2 increases inflammation and exacerbates apoptosis and the permeability of vascular endothelial cells [22]. Infection of these cells also decreases antithrombogenicity. Inflammatory macrophages secrete inflammatory cytokines as a defense against viral infection. Then, crosstalk between the inflammatory and coagulation factors further reinforces both processes. SARS-CoV-2 can also directly infect macrophages. Infected macrophage then expresses tissue factor, another coagulation factor, activating the exogenous blood coagulation system. Crosstalk between inflammatory and coagulation processes cause platelet and neutrophil activation. Neutrophil extracellular traps are released from the activated neutrophils and a coagulation cascade proceeds. This reduces the levels of ACE2 on cell surfaces, creating an ideal microenvironment for thrombin production.
3. CRVO after COVID-19 Infection
Reported cases of CRVO development after COVID-19 infection are summarized in Table 1A and 1B [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38]. The average age across the studies listed was 36.4 ± 11.0 years. This is significantly younger than the average age of 71.2 ± 12.0 years obtained from our unpublished data (p < 0.001, unpaired t-test), which was gathered before the COVID-19 pandemic. This difference seems to suggest that COVID-19 infection can lead to CRVO at an earlier age than it might usually occur. The total number of cases reported in the listed studies was 27, comprising 16 males and 11 females. Our unpublished data included 148 CRVO cases, comprising 74 males and 74 females. There were no significant differences in incidence between this study and our unpublished data (p = 0.38, unpaired t-test). In a study conducted before the pandemic, Li et al. reported that CRVO presents more frequently in men (50.3%) before COVID-19 pandemic [39]. The time between COVID-19 diagnosis and CRVO symptom onset ranged between 0–6 months. The authors point out the difficulties in defining the point at which symptoms should no longer be considered COVID-19-related, and judging when CRVO was not a complication of COVID-19 infection. There was no fixed period within which blood test results due to COVID-19 infection returned to normal. The average logarithmic VA at the initial visit as 0.73 ± 0.75 referring to previous report [40]. This was not significantly different from that found in our unpublished data (0.77 ± 0.57; p = 0.71, unpaired t-test). The most common treatment for CRVO was intravitreal injection of anti-VEGF antibodies; however, systemic corticosteroids were administered to those patients whose CRVO symptoms were within a few days of COVID-19 infection. Although photocoagulation is sometimes performed in the treatment of CRVO, none of the cases reported underwent this procedure. The final mean logarithmic VA was 0.22 ± 0.49, whereas that in our unpublished CRVO data, gathered before the COVID-19 pandemic, was 0.58 ± 0.75. Our unpublished final logarithmic VA was taken 12 ± 2 months after treatment. The final mean logarithmic VA in the present study is significantly better than that from our unpublished data (p < 0.01, unpaired t-test). Sen et al. have reported that younger age affected visual outcomes in CRVO treated with intravitreal injection of anti-VEGF antibodies [41]. Furthermore, in a sample comprised of 85 patients with CRVOs and 26 with BRVOs, Dărăbuș et al. found that the most important nonimaging predictors of best-corrected visual acuity (BCVA) after RVOs were age and baseline BCVA [42]. Thus, it should be borne in mind that the younger average age in this study is likely to have affected the visual outcomes.
4. CRVO after COVID-19 Vaccination
Reported cases of CRVO that developed after COVID-19 vaccination are shown in Table 2A–2D [43,44,45,46,47,48,49,50,51,52,53,54]. The average age in this subject was 39.4 ± 13.3 years a, which was not significantly different to the age of those who developed CRVO after COVID-19 infection (summarized in Table 1A and 1B) (p = 0.45, unpaired t-test). There were 13 cases of postvaccine CRVO, comprised of nine males and four females. The sex ratio of those with CRVO after vaccination did not differ significantly from that of the CRVO after infection subset (p = 0.79, unpaired t-test). The time between receipt of the COVID-19 vaccine and CRVO symptom onset ranged from was 0 to 25 days, with an average of 9.1 ± 7.3 days.
Table 2B shows which vaccine type each patient received. However, the relatively small number of reported cases prevent us from determining whether the risk of CRVO differs between the different vaccines. The number of COVID-19 vaccination that patients had received prior to CRVO onset ranged between 1–3 and averaged 1.8 ± 0.7.
There was no fixed tendency in blood correction. Logarithmic VA at the initial visit was 0.81 ± 0.73 referring to previous report [40] and there was not significant difference from CRVO after COVID-19 infection shown in Table 1B (p = 0.78, unpaired t-test).
Although intravitreal injection of anti-VEGF antibody was the main treatment, whole body administration of corticosteroid was performed in some instances. Only one case was treated with retinal photocoagulation. The mean final logarithmic VA was 0.18 ± 0.31 and there was no significant difference between this and the mean final logarithmic VA of those with CRVO after COVID-19 infection shown in Table 1B (p = 0.78, unpaired t-test).
5. BRVO after COVID-19 Infection
The subset who developed BRVO after COVID-19 infection are summarized in Table 3A and Table 8B [55,56,57,58,59,60]. Their average age was 56.8 ± 11.7 years. In a study conducted before the COVID-19 pandemic, Lee et al. reported an average age of 58.2 years in a sample of 354 BRVO patients [61]. This is very close to the average age found in this review. Li et al. and Lee et al. have both reported a slightly higher incidence of BRVO among women (54.5% and 58.8%, respectively) [39,61]. The ratio of males to females was 5: 3. The ocular laterality in those with BRVO after COVID-19 infection was one right eye and six left eyes. Li et al. reported a right eye onset preference in BRVO (51.0%) [39]. The mean time, in days, between COVID-19 diagnosis and initial BRVO symptoms was 50.6 ± 41.2 days. There were no patterns observed in the return to normal of blood test abnormalities
Logarithmic visual acuity at initial visit was 0.67 ± 0.66 referring to previous report [40]. For those with BRVO after COVID-19 infection, intravitreal injection of anti-VEGF antibodies was the main treatment. The final logarithmic VA of this subset was 0.38 ± 0.42.
6. BRVO after COVID-19 Vaccination
The cases who developed BRVO after COVID-19 vaccine are shown in Table 4A and 4B [62,63,64,65,66,67,68,69,70,71]. Their average age was 55.5 ± 13.2 years and there was no significant difference between this and the average age of those who developed BRVO after COVID-19 infection (p = 0.82, unpaired t-test). The ratio of males to females was 6: 7. The mean time between COVID-19 vaccination and BRVO symptom onset was 5.1 ± 5.8 days. This was not significantly different from the mean time of those with CRVO after COVID-19 vaccination (p = 0.10, unpaired t-test).
The vaccines used were by Pfizer, Moderna, and AstraZeneca. The average number of vaccines received was 1.4 ± 0.5. This was not significantly different from the average number received by those with CRVO after COVID-19 vaccination (p=0.14).
There are no specific findings in blood correction. Logarithmic visual acuity at the initial visit was 0.27±0.34 and there was no significant difference compared to logarithmic visual acuity at the initial visit BRVO after COVID-19 infection (P=0.14).
The main treatment was intravitreal anti-VEGF antibody injection. The final logarithmic VA was 0.0.35 ± 0.11 and there was no significant difference between this final VA and that reported in those with BRVO after COVID-19 infection (p = 0.14).
7. CRAO after COVID-19 Infection
Cases of CRAO after COVID-19 infection are shown in Table 5A and 5B [72,73,74,75,76,77,78,79,80,81,82]. The average age was 50.0±17.3 years and the ratio of males to females was 9: 3. Four of the cases were in the right eye, six in the left, and one in both eyes. Lee found that, in 91 patients with acute nonarteritic CRAO, 62.6% were male and the average age was 66.4 years [83]. In this instance, the average age was reduced considerably by the inclusion of a 6-year-old boy [74]. Consistent with the findings of Li et al. [39], Lee reported a higher incidence of CRAO after COVID-19 infection in men. The mean time from COVID-19 diagnosis to symptom onset was 12.6 ± 9.5 days.
The logarithmic visual acuity at the initial visit was 2.29 ± 0.95 referring to previous report [40]. Treatment was irregular and the final logarithmic visual acuity was 2.44±0.90. Some cases had no light perception (NLP) at the initial visit, while others had NLP by the final visit. The visual outcomes among this subset were very severe. Shah et al. reported that 447 of the 484 patients who presented within 30 days and had comprehensive documentation showed VA ≤20/200 [84]. They further reported that, of the 441 patients with documented follow-up, 380 (86.2%) remained at that VA level long-term. It has previously been inferred that the shorter the duration between CRAO symptom onset and treatment, the better the prognosis. However, Shah et al. found this to have no effect on final VA outcomes [84]. St Peter et al. found that hyperbaric oxygen may be an effective treatment for nonarteritic CRAO, especially with early treatment and salvageable vision [85]. They emphasize the importance of the earliest treatment possible in patients with CRAO [85]. Currently, patients may receive one of various treatments for CRAO because no individual treatment has been established as particularly effective. Visual outcomes are very poor among those who suffer CRAO.
8. CRAO after Vaccination
CRAO cases after COVID-19 vaccination are shown in Table 6A-6D [86,87,88,89,90,91]. The average age was 55.5 ± 18.5 years and the male to female ratio was 3: 3. Of the 91 patients with acute nonarteritic CRAO reported by Lee, 62.6% were male and the average age was 66.4 years [83]. Thus, the average age among the cases shown in Table 6A to 6D is younger than that previously reported in CRAO unassociated with COVID-19 [83]. Also among patients with CRAO unrelated to COVID-19, Kido et al. have reported an incidence rate 1.4 times higher in males than females [92]. The time from COVID-19 vaccination to CRAO symptom onset ranged from 1 to 21 days, with a mean of 7.3 ± 7.4 days. The time between receipt of the COVID-19 vaccine and CRVO symptom onset was 9.1±7.3 days. There was no significant difference between these times for CRVO and CRAO after vaccination (p = 0.63, unpaired t-test).
The COVID-19 vaccines used were by Pfizer, Moderna, AstraZeneca, and Bharat Biotech.
Although there were some slightly abnormal blood test results, they were not a characteristic feature of the patients in this subset. VA at the initial visit was poor in most cases, but 20/40 in one case.
Some cases had NLP by their final visit and only one case recovered some of their visual function, which increased to 1.2 in decimal VA.
9. BRAO after COVID-19 Infection
Published cases of BRAO after COVID-19 infection are summarized in Table 7A and 7B [93,94,95,96]. The average age of this subset was 41.3 ± 17.8 years and all patients were male. The average time between COVID-19 diagnosis and BRAO symptom onset was 48.3 ± 39.6 days. There were no identifiable patterns in the return of blood test results to normal levels.
VA at the initial visit was 0.092±0.071 and this value is significantly better than VA at the initial visit of CRAO after COVID-19 infection (p < 0.001). Because excellent treatment is not established today, many treatments methods were irregular. The final VA value was not reported in all cases, which prevented a detailed examination of treatment effects on visual outcomes.
10. BRAO after COVID-19 Vaccination
Reported cases of BRAO after COVID-19 vaccination are summarized in Table 8A–8D [97,98,99]. The average age of this subset was 62.3 ± 21.2 years and the average number of days between vaccination and BRAO symptom onset was 21.0 ± 24.9. As stated above, the average age of patients with CRAO after COVID-19 vaccination was 55.5 ± 18.5 years, which was not significantly different from that of the patients with BRAO after COVID-19 vaccination (p = 0.57). The time between vaccination and symptom onset was 21.0 ± 24.9 days. This was not significantly different from the time between vaccination and CRAO symptom onset (p = 0.25).
Although all of the vaccines were made by the multinational corporation, Pfizer-BioNTech, there have been few reports on their relationship with RVODs.
VA at the initial visit averaged −0.025 ± 0.16, which was significantly better than that found among patients with CRAO after COVID-19 vaccination (p < 0.001). No significant difference was observed between BRAO after COVID-19 infection and BRAO after COVID-19 vaccination (p = 0.19).
Because treatment methods and final VA values were not provided in most reports, it was difficult to conduct a comprehensive investigation.
We will now consider the mechanisms involved in the pathogenesis of RVODs. Retinal veins can be occluded by arteriosclerosis. This causes components of the plasma to leak out of the vessel, which results in retinal hemorrhage and retinal edema. If the lesion does not reach the arcade area, no symptoms occur. However, once this region is reached, VA begins to decline rapidly. Risk factors for RVODs are older age, hypertension, diabetes, hyperlipidemia, smoking, and glaucoma [13]. RAO is frequently a symptom of an underlying disease, such as atrial fibrillation; heart valve diseases; stenosis or plaque formation in the internal carotid artery; or arteriosclerosis in older adults due to hypertension, diabetes, or hyperlipidemia [17]. However, RAO can also occur in youth among those with antiphospholipid syndrome and, exceptionally, those who take oral contraceptives. RVODs require medical scans and imaging and systemic treatments with internal medicine.
When the COVID-19 pandemic began, the resultant abnormalities of the blood coagulation system were greatly remarked upon. Tang et al. proposed that elevated d-dimer levels were predictive of a poor prognosis in infected patients. In fatal cases, the rate of disseminated intravascular coagulation (DIC) was 71.4% [100]. Tang et al. indicated that the patient was very unlikely to survive if DIC occurred [100]. COVID-19-associated coagulopathy is strongly correlated with vascular endothelial cell damage [20,21] and increased thrombin production in the veins and arteries. Several previous studies have verified that d-dimer elevation is an independent risk factor for thrombosis and death in COVID-19 patients [101,102,103]. However, the present study found that coagulative abnormalities are an infrequent occurrence in COVID-19 patients. Wang et al. posited that mild or focal coagulation activation could cause retinal vessel occlusions without a significant change in the patient’s d-dimer level [104].
The COVID-19 vaccine approved for clinical use at the end of 2020, is the primary infection control strategy. The vaccine is a combination of an adenovirus vector vaccine and a messenger RNA vaccine. While adenovirus vector vaccines rarely cause thrombosis or thrombocytopenia syndrome [105], messenger RNA vaccine can cause venous thrombosis and thrombocytopenia and is likely to be the element of the COVID-19 vaccine responsible for vaccine-related thrombi [106]. It is apparent that ophthalmologists need to monitor patients closely for thrombosis after COVID-19 infection and COVID-19 vaccination.
The regions vulnerable to arterial thrombosis are arteries of the extremities (39%), cerebral vessels (24%), large vessels (19%), coronary arteries (9%), and the superior mesenteric artery (8%) (the remaining 1% of cases occur in other vessels) [108]. Malas et al. has reported an overall incidence of COVID-19-induced venous thromboembolism (VTE) of 21% [108]. Furthermore, the VTE rate was 5% Among general ward patients, the rate of VTE is 5%, while the rate among ICU patients is 31% [108]. When such thrombosis occurs in the retina, it is classed as an RVOD. It has been shown in this review that the increased risk of RVODs following COVID-19 is unsurprising given their reinforcing effects on each other, particularly in relation to coagulation processes. However, it is very difficult to clarify the connection between COVID-19 infection or vaccine and RVODs. Epidemiological investigations make an important contribution to investigations into comorbid conditions and the triggering of one condition by another.
Modjtahedi et al. have reported an RVO incidence rate of 65 in 43,2515 patients (a crude incidence rate of 12.2 per million) in the 6 months after a COVID-19 diagnosis [109]. This is a clear increase in the rate of RVO compared to that seen in those not recently infected with COVID-19 [109]. A study in Spain by Napal et al. also showed an increased RVO incidence during COVID-19 pandemic [110]. Conversely, Parks et al. reported no increase in RVO after COVID-19 infection [111, 112.] Al-Moujahed reported a diagnosis of CRVO in 7,261 (2.5%) of the 285,759 new patients seen in the pre–COVID-19 period and in 4,098 (2.7%) of the 156,427 new patients seen during the COVID-19 pandemic [113]. The percentage of new diagnoses in retina clinics that were CRVO remained stable during the pandemic [113]. Although the rate of patients with newly-diagnosed CRVO during the COVID-19 pandemic is interesting, these rates have not remained clear. According to our unpublished data, the rate of patients with CRVO remained unchanged after the COVID-19 pandemic compared to before. However, retinal photocoagulation was performed significantly more frequently after the pandemic began (p < 0.001). This may say something about the possible pathogenesis of CRVO. Hashimoto et al. found low causality between RVO and COVID-19 vaccination [114]. Rachman et al. could not ascertain differences in the RVO risks of different types of COVID-19 vaccines due to a lack of detailed data on dosages and patient medical histories [115].
The RAO rate before and after COVID-19 pandemic is fascinating. Park et al. reported the RAO incidence rates per 100,000 people/year for 2018–2019 and 2020–2021 as 11.7 and 12.0, respectively [111]. Despite the increased incidence of RAO during the COVID-19 pandemic, SARS-CoV-2 infection did not significantly increase RAO incidence [111]. Al-Moujahed et al. reported an increase in CRAO cases during the first few months of the pandemic [113]. However, RAO diagnosis rates as percentages of all new diagnoses in retina clinics remained stable for the majority of the pandemic [113]. We are now investigating this issue and will release our data when the investigation is complete.
We found an increase in Vogt-Koyanagi-Harada disease associated with COVID-19 [116]. Seventy-three cases per 60 months of Vogt-Koyanagi-Harada disease occurred before pandemic and 53 cases per 33 months occurred after COVID-19 pandemic [116]. Liang et al. observed an overall reduction in eye injuries and substantial differences in the spectrum of ocular trauma during the COVID-19 pandemic [117]. There was also an increase in dry eye-related complaints among students during the pandemic. This may have resulted from increased screen time [118]. Alternatively, Krolo et al. reported that mask-associated dry eye increased during the COVID-19 pandemic [119]. While the incidence of endophthalmitis after intravitreal injections remained unchanged [120], the rate of endophthalmitis after vitrectomy increased, especially the variant caused by oral bacteria [121]. Shi et al. found that the incidence of optic neuritis increased during the COVID-19 pandemic as too did acute primary angle closure, although the reason for the latter was unknown [123].
At this point, we would like to briefly describe three interesting cases that we have encountered [124,125,126]. The first of these was a male in his early 50s who suffered a recurrence of macular edema (ME) due to BRVO 3 days after administration of the messenger RNA COVID-19 vaccine (Pfizer-BioNTech). He was treated for this with an additional intravitreal aflibercept injection [124]. However, the patient believed the COVID-19 vaccine could have been the cause of his ME recurrence, so refused any further vaccinations after that [124]. In the 29 months since his initial visit, no recurrence has been reported. The second case was a 59-year-old female patient who suffered a recurrence of Vogt-Koyanagi-Harada disease following her third dose of the messenger RNA COVID-19 vaccine (Pfizer-BioNTech). This recurrence was 46 years after initial treatment [125]. The patient’s inflammation was reduced by eye drops and oral corticosteroids. However, it seems that the vaccine may have triggered the recurrence [125]. The third case was a 21-year-old female who had been using oral contraceptives for 2 years [126]. Despite having received two doses of an mRNA-based COVID-19 vaccine, she contracted COVID-19 [126]. She then suffered BRVO with ME 40 days after COVID-19 diagnosis. She was treated with an intravitreal aflibercept injection [126]. In the 29 months since the patient’s initial visit, there has been no ME recurrence. BRVO with ME does not usually occur in young women but oral contraceptive use, COVID-19 vaccination, and COVID-19 infection are all risk factors for venous thromboembolism. In combination, they could have induced the patients of BRVO with ME [126]. These cases illustrate some of the ways COVID-19 infection and vaccine can lead to various ocular disease.
With the global dissemination of COVID-19 vaccines, the pandemic has now (in 2024) been brought under some degree of control. Still, both COVID-19 and its vaccines have several unknown factors. Both could potentially have unknown complications or side effects. Because of the urgency, the usually lengthy process required for drug approval was hastened and this has led to social doubts about the safety of the vaccinations. Ophthalmologists are among the healthcare workers who may identify these complications and side effects in patients after their infection with or vaccination against COVID-19.
11. Conclusions
This review provides a comprehensive summary of RVOD cases secondary to either COVID-19 infection or COVID-19 vaccine reported to date. While RVOD following COVID-19 infection or vaccination is rare, those few cases reported are sufficient to have caused major concern. Although it would be prudent for clinicians to closely monitor any visual disturbances in patients recently infected with or vaccinated against COVID-19. However, we can neither support nor reject a possible association between RVOD and COVID-19 infection or vaccination based on the existing evidence. The patients reported in the reviewed studies constitute a heterogenous sample, among whom other underlying conditions and/or risk factors for RVODs cannot be ruled out. Therefore, further research with more data is warranted.
Author Contributions
Conceptualization, TM; data curation, TM; writing—original draft preparation, TM; writing—review and editing, SM, SI, KK; supervision, SM, SI, KK. All authors have read and agree to the final version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ullah, I.; Sohail, A; Shah, MUFA. ; Khurshid, M.; Diwan, MN.; Qadir, A.; Irfan, M. Central retinal vein occlusion in patients with COVID-19 infection: a systematic review. Ann Med Surg (Lond). 2021, 71, 102898. [Google Scholar] [CrossRef] [PubMed]
- Go, AS.; Reynolds, K.; Tabada, GH.; Prasad, PA.; Sung, SH.; Garcia, E.; Portugal, C.; Fan, D.; Pai, AP.; Fang, MC. COVID-19 and risk of VTE in ethnically diverse populations. Chest. 2021, 160, 1459–1470. [Google Scholar] [CrossRef] [PubMed]
- Sastry, S.; Cuomo, F.; Muthusamy, J. COVID-19 and thrombosis: The role of hemodynamics. Thromb Res. 2022, 212, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Capaccione, KM.; Leb, JS.; D'souza, B.; Utukuri, P.; Salvatore, MM. Acute myocardial infarction secondary to COVID-19 infection: A case report and review of the literature. Clin Imaging. 2021, 72, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Manolis, AS.; Manolis, AA.; Manolis, TA.; Apostolopoulos, EJ.; Papatheou, D.; Melita, H. COVID-19 infection and cardiac arrhythmias. Trends Cardiovasc Med. 2020, 30, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Hingorani, KS.; Bhadola, S.; Cervantes-Arslanian, AM. COVID-19 and the brain. Trends Cardiovasc Med. 2022, 32, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Katsoularis, I.; Fonseca-Rodríguez, O.; Farrington, P.; Jerndal, H.; Lundevaller, EH.; Sund, M.; Lindmark, K.; Fors Connolly, AM. Risks of deep vein thrombosis, pulmonary embolism, and bleeding after covid-19: nationwide self-controlled cases series and matched cohort study. BMJ. 2022, 377, e069590. [Google Scholar] [CrossRef]
- D'Alessandro, E.; Kawasaki, A.; Eandi, CM. Pathogenesis of vascular retinal manifestations in COVID-19 patients: a review. Biomedicines. 2022, 10, 2710. [Google Scholar] [CrossRef] [PubMed]
- Le, HG.; Shakoor, A. Diabetic and retinal vascular eye disease. Med Clin North Am. 2021, 105, 455–472. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.; Moss, SE.; Meuer, SM.; Klein, BE. The 15-year cumulative incidence of retinal vein occlusion: the Beaver Dam Eye Study. Arch Ophthalmol. 2008, 126, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, T.; Matsumoto, F.; Sakamoto, S.; Nakagawa, Y.; Suzuki, Y. Anti-VEGF therapy and retinal photocoagulation to prevent recurrence of central retinal vein occlusion: two case reports of young patients. Tokai J Exp Clin Med. 2020, 45, 249–253. [Google Scholar] [PubMed]
- Pielen, A.; Mirshahi, A.; Feltgen, N.; Lorenz, K.; Korb, C.; Junker, B.; Schaefer, C.; Zwiener, I.; Hattenbach, LO. ; RABAMES Study Group. Ranibizumab for branch retinal vein occlusion associated macular edema study (RABAMES): six-month results of a prospective randomized clinical trial. Acta Ophthalmol.
- Romano, F.; Lamanna, F.; Gabrielle, PH.; Teo, KYC. ; Battaglia, Parodi M.; Iacono P, Fraser-Bell S.; Cornish, EE.; Nassisi, M.; Viola, F.; Agarwal, A.; Samanta, A.; Chhablani, J.; Staurenghi, G.; Invernizzi, A. Update on retinal vein occlusion. Asia Pac J Ophthalmol (Phila). 2023, 12, 196–210. [Google Scholar] [CrossRef]
- Scott, IU.; Campochiaro, PA.; Newman, NJ.; Biousse, V. Retinal vascular occlusions. Lancet. 2020, 396(10266), 1927–1940. [Google Scholar] [CrossRef] [PubMed]
- Chronopoulos, A.; Schutz, JS. Central retinal artery occlusion-A new, provisional treatment approach. Surv Ophthalmol. 2019, 64, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Madike, R.; Cugati, S.; Chen, C. A review of the management of central retinal artery occlusion. Taiwan J Ophthalmol. 2022, 12, 273–281. [Google Scholar]
- Hayreh, SS.; Zimmerman, MB. Central artery occlusion: visual outcome. Am J Ophthalmol. 2005, 140, 376–391. [Google Scholar] [CrossRef] [PubMed]
- Park, A.; Iwasaki, A. Type I and Type III Interferons - Induction, Signaling, Evasion, and Application to Combat COVID-19. Cell Host Microbe. 2020, 27, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Onomoto, K.; Onoguchi, K.; Yoneyama, M. Regulation of RIG-I-like receptor-mediated signaling: interaction between host and viral factors. Cell Mol Immunol. 2021, 18, 539–555. [Google Scholar] [CrossRef]
- Goshua, G.; Pine, AB.; Meizlish, ML.; Chang, CH.; Zhang, H.; Bahel, P.; Baluha, A.; Bar, N.; Bona, RD.; Burns, AJ.; Dela Cruz, CS.; Dumont, A.; Halene, S.; Hwa, J.; Koff, J.; Menninger, H.; Neparidze, N.; Price, C.; Siner, JM.; Tormey, C.; Rinder, HM.; Chun, HJ.; Lee, AI. Endotheliopathy in COVID-19-associated coagulopathy: evidence from a single-centre, cross-sectional study. Lancet Haematol. 2020, 7, e575–e582. [Google Scholar] [CrossRef]
- Loo, J.; Spittle, DA.; Newnham, M. COVID-19, immunothrombosis and venous thromboembolism: biological mechanisms. Thorax. 2021, 76, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Chen, AT.; Wang, CY.; Zhu, WL.; Chen, W. Coagulation disorders and thrombosis in COVID-19 patients and a possible mechanism involving endothelial cells: a review. Aging Dis. 2022, 13, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Invernizzi, A.; Pellegrini, M.; Messenio, D.; Cereda, M.; Olivieri, P.; Brambilla, AM.; Staurenghi, G. Impending central retinal vein occlusion in a patient with Coronavirus disease 2019 (COVID-19). Ocul Immunol Inflamm. 2020, 28, 1290–1292. [Google Scholar] [CrossRef] [PubMed]
- Gaba, WH.; Ahmed, D.; Al Nuaimi, RK.; Dhanhani, AA.; Eatamadi, H. Bilateral central retinal vein occlusion in a 40-year-old man with severe Coronavirus disease 2019 (COVID-19) pneumonia. Am J Case Rep. 2020, 21, e927691. [Google Scholar] [CrossRef] [PubMed]
- Riazi-Esfahani H, Sadeghi, R. ; Soleymanzadeh, M.; Farrokhpour, H.; Bazvand, F.; Ebrahimiadib, N.; Khalili Pour E, Mirghorbani, M. Hemicentral retinal vein occlusion in a patient with a history of coronavirus disease 2019 infection: a case report and review of the literature. J Med Case Rep. 2024, 18, 50. [Google Scholar] [CrossRef]
- Sheth, JU.; Narayanan, R.; Goyal, J.; Goyal, V. Retinal vein occlusion in COVID-19: A novel entity. Indian J Ophthalmol. 2020, 68, 2291–2293. [Google Scholar] [CrossRef]
- Walinjkar, JA.; Makhija, SC.; Sharma, HR.; Morekar, SR.; Natarajan, S. Central retinal vein occlusion with COVID-19 infection as the presumptive etiology. Indian J Ophthalmol. 2020, 68, 2572–2574. [Google Scholar] [PubMed]
- Kılıçarslan, O.; Çebi, AY.; Uçar, D. Central retinal vein occlusion and occlusive vasculopathy at macula in a patient with recent COVID-19 infection. Taiwan J Ophthalmol 2022, 12, 477–481. [Google Scholar]
- Raval, N.; Djougarian, A.; Lin, J. Central retinal vein occlusion in the setting of COVID-19 infection. J Ophthalmic Inflamm Infect. 2021, 11, 10. [Google Scholar] [CrossRef] [PubMed]
- Finn, AP.; Khurana, RN.; Chang, LK. Hemi-retinal vein occlusion in a young patient with COVID-19. Am J Ophthalmol Case Rep. 2021, 22, 101046. [Google Scholar] [CrossRef]
- Lin, CH.; Sun, IT. Bilateral simultaneous central retinal vein occlusion secondary to COVID-19: a case report. Case Rep Ophthalmol. 2023, 14, 56–61. [Google Scholar] [CrossRef]
- Yahalomi, T.; Pikkel, J.; Arnon, R.; Pessach, Y. Central retinal vein occlusion in a young healthy COVID-19 patient: A case report. Am J Ophthalmol Case Rep. 2020, 20, 100992. [Google Scholar] [CrossRef]
- Venkatesh, R.; Reddy, NG.; Agrawal, S.; Pereira, A. COVID-19-associated central retinal vein occlusion treated with oral aspirin. BMJ Case Rep. 2021, 14, e242987. [Google Scholar] [CrossRef] [PubMed]
- Shroff, D.; Kumar, S.; Naidu, A.; Gupta, C.; Shroff, CM. Retinal vasoocclusive spectrum following COVID-19. Indian J Ophthalmol. 2022, 70, 1412–1415. [Google Scholar] [PubMed]
- Staropoli, PC.; Payson, A.; Negron, CI.; Prakhunhungsit, S.; Laufer, P.; Berrocal, AM. CRVO associated with COVID-19 and MTHFR mutation in a 15-year-old male. Am J Ophthalmol Case Rep. 2022, 26, 101522. [Google Scholar] [CrossRef] [PubMed]
- Ashkenazy, N.; Patel, NA.; Sridhar, J.; Yannuzzi, NA.; Belin, PJ.; Kaplan, R.; Kothari, N.; Benitez Bajandas GA, Kohly, RP. ; Roizenblatt, R.; Pinhas, A.; Mundae, R.; Rosen, RB.; Ryan EH Jr.; Chiang, A.; Chang, LK.; Khurana, RN.; Finn, AP. Hemi- and central retinal vein occlusion associated with COVID-19 infection in young patients without known risk factors. Ophthalmol Retina. 2022, 6, 520–530. [Google Scholar] [CrossRef] [PubMed]
- Płatkowska-Adamska, B.; Kal, M.; Krupińska, J.; Biskup, M.; Odrobina, D. Central retinal vein occlusion after discontinuation of rivaroxaban therapy in a young patient with COVID-19 pulmonary embolism: a case report. Am J Case Rep. 2022, 23, e937739. [Google Scholar] [CrossRef] [PubMed]
- Quigley, C.; Butler, T.; Byrne, L.; Moore, D.; Doyle, A. Post-Coronavirus disease 2019 (COVID-19) syndrome associated with central retinal vein occlusion: a case report. Ocul Immunol Inflamm. 2023, 31, 185–187. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Hall, NE.; Pershing, S.; Hyman, L.; Haller, JA.; Lee, AY.; Lee, CS.; Chiang, M.; Lum, F.; Miller, JW.; Lorch, A.; Elze, T. Age, gender, and laterality of retinal vascular occlusion: a retrospective study from the IRIS® registry. Ophthalmol Retina. 2022, 6, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.; Fishman, GA.; Anderson, RJ.; Tozatti, MS.; Heckenlively, JR.; Weleber, RG.; Edwards, AO.; Brown, J Jr. Visual acuity impairment in patients with retinitis pigmentosa at age 45 years or older. Ophthalmology. 1999, 106, 1780–1785. [Google Scholar] [CrossRef] [PubMed]
- Sen, P.; Gurudas, S.; Ramu, J.; Patrao, N.; Chandra, S.; Rasheed, R.; Nicholson, L.; Peto, T.; Sivaprasad, S.; Hykin, P. Predictors of visual acuity outcomes after anti-vascular endothelial growth factor treatment for macular edema secondary to central retinal vein occlusion. Ophthalmol Retina. 2021, 5, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Dărăbuș, DM.; Pac, CP.; Roşca, C.; Munteanu, M. Macular dynamics and visual acuity prognosis in retinal vein occlusions - ways to connect. Rom J Ophthalmol. 2023, 67, 312–324. [Google Scholar] [PubMed]
- Sonawane, NJ.; Yadav, D.; Kota, AR.; Singh, HV. Central retinal vein occlusion post-COVID-19 vaccination. Indian J Ophthalmol. 2022, 70, 308–309. [Google Scholar] [CrossRef] [PubMed]
- Ishiguro, K.; Hirano, Y.; Esaki, Y.; Yasukawa, T. Central retinal vein occlusion after mRNA COVID-19 vaccination. Case Rep Ophthalmol. 2023, 14, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Sankhala, KK.; Bose, S.; Gallemore, RP. Combined central retinal artery and vein occlusion with ischemic optic neuropathy after COVID-19 vaccination. Int Med Case Rep J. 2022, 15, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Wu, D. ; Lim, BXH.; Lim, DK.; Lingam, G.; Lim, CHL. Retinal vein occlusion following BNT162b2 (Pfizer-BioNTech) COVID-19 vaccination. Singapore Med J.
- Romano, D.; Morescalchi, F.; Romano, V.; Semeraro, F. COVID-19 adenoviral vector vaccine and central retinal vein occlusion. Ocul Immunol Inflamm. 2022, 30, 1286–1288. [Google Scholar] [CrossRef] [PubMed]
- Endo, B.; Bahamon, S.; Martínez-Pulgarín, DF. Central retinal vein occlusion after mRNA SARS-CoV-2 vaccination: A case report. Indian J Ophthalmol. 2021, 69, 2865–2866. [Google Scholar] [CrossRef] [PubMed]
- Sung, SY.; Jenny, LA.; Chang, YC.; Wang, NK.; Liu, PK. Central retinal vein occlusion in a young woman with diabetes and hypertension after mRNA-based COVID-19 vaccination-a case report and brief review of the literature. Vaccines (Basel). 2023, 11, 365. [Google Scholar] [CrossRef] [PubMed]
- Dutta Majumder, P.; Prakash, VJ. Retinal venous occlusion following COVID-19 vaccination: report of a case after third dose and review of the literature. Indian J Ophthalmol. 2022, 70, 2191–2194. [Google Scholar] [CrossRef]
- Shah, PP.; Gelnick, S.; Jonisch, J.; Verma, R. Central retinal vein occlusion following BNT162b2 (Pfizer-BioNTech) COVID-19 messenger RNA vaccine. Retin Cases Brief Rep. 2023, 17, 441–444. [Google Scholar] [CrossRef] [PubMed]
- Takacs, A.; Ecsedy, M.; Nagy, ZZ. Possible COVID-19 mRNA vaccine-induced case of unilateral central retinal vein occlusion. Ocul Immunol Inflamm. 2023, 31, 1145–1150. [Google Scholar] [CrossRef] [PubMed]
- Nangia, P.; Prakash. , VJ.; Dutta Majumder P. Retinal venous occlusion in a child following Corbevax COVID-19 vaccination. Indian J Ophthalmol. 2022, 70, 3713–3715. [Google Scholar]
- Bialasiewicz, AA.; Farah-Diab, MS.; Mebarki, HT. Central retinal vein occlusion occurring immediately after 2nd dose of mRNA SARS-CoV-2 vaccine. Int Ophthalmol. 2021, 41, 3889–3892. [Google Scholar] [CrossRef]
- Nourinia, R.; Ghassempour, M.; Ahmadieh, H.; Abtahi, SH. Branch retinal vein occlusion after COVID-19. J Fr Ophtalmol. 2021, 44, e441–e443. [Google Scholar] [CrossRef] [PubMed]
- Duff, SM.; Wilde, M.; Khurshid, G. Branch retinal vein occlusion in a COVID-19 positive patient. Cureus. 2021, 13, e13586. [Google Scholar] [CrossRef] [PubMed]
- Karasu, B.; Kesim, E. Bilateral branch retinal vein occlusion following the diagnosis of mild coronavirus disease. Arq Bras Oftalmol. 2023, 86, 274–276. [Google Scholar] [CrossRef] [PubMed]
- Kapsis, P.; Agapitou, C.; Dimitriou, E.; Theodossiadis, P.; Chatziralli, I. Branch retinal vein occlusion after COVID-19 infection: a case report. Cureus. 2023, 15, e38172. [Google Scholar] [CrossRef] [PubMed]
- Shiroma, HF.; Lima, LH.; Shiroma, YB.; Kanadani, TC.; Nobrega, MJ.; Andrade, G.; de Moraes Filho, MN.; Penha, FM. Retinal vascular occlusion in patients with the Covid-19 virus. Int J Retina Vitreous. 2022, 8, 45. [Google Scholar] [CrossRef]
- Güven, YZ.; Akbalık, T.; Akay, F. Nasal vein occlusion after COVID-19: a case report. Indian J Ophthalmol. 2022, 70, 2195–2196. [Google Scholar] [CrossRef] [PubMed]
- Lee, JY.; Yoon, YH.; Kim, HK.; Yoon, HS.; Kang, SW.; Kim, JG.; Park, KH.; Jo, YJ.; Korean RVO Study. Baseline characteristics and risk factors of retinal vein occlusion: a study by the Korean RVO Study Group. J Korean Med Sci. 2013, 28, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Pur, DR.; Catherine Danielle Bursztyn LL, Iordanous, Y. Branch retinal vein occlusion in a healthy young man following mRNA COVID-19 vaccination. Am J Ophthalmol Case Rep. 2022, 26, 101445. [Google Scholar] [CrossRef]
- Sugihara, K.; Kono, M.; Tanito, M. Branch retinal vein occlusion after messenger RNA-based COVID-19 vaccine. Case Rep Ophthalmol. 2022, 13, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Gironi, M.; D’Aloisio, R.; Verdina, T.; Shkurko, B. Bilateral branch retinal vein occlusion after mRNA-SARS-CoV-2 booster dose vaccination. J Clin Med. 2023, 12, 1325. [Google Scholar] [CrossRef]
- Tanaka, H.; Nagasato, D.; Nakakura, S.; Nagasawa, T.; Wakuda, H.; Kurusu, A.; Mitamura, Y.; Tabuchi, H. Branch retinal vein occlusion post severe acute respiratory syndrome coronavirus 2 vaccination. Taiwan J Ophthalmol. 2022, 12, 202–205. [Google Scholar]
- Karageorgiou, G.; Chronopoulou, K.; Georgalas, I.; Kandarakis, S.; Tservakis, I.; Petrou, P. Branch retinal vein occlusion following ChAdOx1 nCoV-19 (Oxford-AstraZeneca) vaccine. Eur J Ophthalmol. 2023, 33, NP121–NP123. [Google Scholar] [CrossRef]
- Lee, J.; Ong, KW.; Wan Abdul Halim WH, Mohd Khialdin, S. ; Yong, MH. Case report: branch retinal vein occlusion post-mRNA SARS-CoV-2 (COVID-19) vaccination. Optom Vis Sci. 2023, 100, 799–803. [Google Scholar] [CrossRef] [PubMed]
- Silva, LSCD. ; Finamor, LPS.; Andrade, GC.; Lima, LH.; Zett, C.; Muccioli, C.; Sarraf, EP.; Marinho, PM.; Peruchi, J.; Oliveira, RDL.; Giralt, L.; Charcan, I.; Fonollosa, A.; Diaz, JD.; Davis, JL.; Nascimento, H.; Belfort R Jr. Vascular retinal findings after COVID-19 vaccination in 11 cases: a coincidence or consequence? Arq Bras Oftalmol. 2022, 85, 158–165. [Google Scholar]
- Peters, MC.; Cheng, SSH. ; Sharma, A.; Moloney, TP. Retinal vein occlusion following COVID-19 vaccination. Clin Exp Ophthalmol. 2022, 50, 459–461. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Seo, MH.; Choi, KE.; Lee, S.; Choi, B.; Yun, C.; Kim, SW.; Kim, YY. Vision-threatening ocular adverse events after vaccination against coronavirus disease 2019. J Clin Med. 2022, 11, 3318. [Google Scholar] [CrossRef] [PubMed]
- Bolletta, E.; Iannetta, D.; Mastrofilippo, V.; De Simone L, Gozzi, F. ; Croci, S.; Bonacini, M.; Belloni, L.; Zerbini, A.; Adani, C.; Fontana, L.; Salvarani, C.; Cimino, L. Uveitis and other ocular complications following COVID-19 vaccination. J Clin Med. 2021, 10, 5960. [Google Scholar] [CrossRef] [PubMed]
- Bapaye, MM.; Nair, AG.; Bapaye, CM.; Bapaye, MM.; Shukla, JJ. Simultaneous bilateral central retinal artery occlusion following COVID-19 infection. Ocul Immunol Inflamm. 2021, 29, 671–674. [Google Scholar] [CrossRef] [PubMed]
- Heidarzadeh, HR.; Abrishami, M.; Motamed Shariati, M.; Ghavami Shahri, SH.; Ansari Astaneh, MR. Atypical central retinal artery occlusion following COVID-19 infection: a case report. Case Rep Ophthalmol. 2023, 14, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Abbati, G.; Fazi, C.; Fortunato, P.; Trapani, S. Central retinal artery occlusion in a young child affected by COVID-19: a first case report. BMC Pediatr. 2023, 23, 462. [Google Scholar] [CrossRef]
- Montesel, A.; Bucolo, C.; Mouvet, V.; Moret, E.; Eandi, CM. Case report: central retinal artery occlusion in a COVID-19 patient. Front Pharmacol. 2020, 11, 588384. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, MR.; Lucena, ARV. ; Higino, TM.; Ventura, CV. Central retinal artery occlusion with cilioretinal artery sparing secondary to COVID-19: additional ocular complication. Indian J Ophthalmol. 2023, 71, 663–666. [Google Scholar] [CrossRef]
- Ucar, F.; Cetinkaya, S. Central retinal artery occlusion in a patient who contracted COVID-19 and review of similar cases. BMJ Case Rep. 2021, 14, e244181. [Google Scholar] [CrossRef] [PubMed]
- Yalçınbayır, Ö.; Uçan Gündüz, G.; Coşkun, F.; Hakyemez, B.; Doğanay, S. Different cases, different manifestations of post-COVID-19 retinal artery occlusion: a case series. Turk J Ophthalmol. 2023, 53, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Lekha, T.; Thomas, R.; Giridhar, A.; Gopalakrishnan, M. Retrospective diagnosis of COVID-19 following the detection of central retinal artery occlusion. Oman J Ophthalmol. 2022, 15, 234–236. [Google Scholar] [CrossRef] [PubMed]
- Acharya, S.; Diamond, M.; Anwar, S.; Glaser, A.; Tyagi, P. Unique case of central retinal artery occlusion secondary to COVID-19 disease. IDCases. 2020, 21, e00867. [Google Scholar] [CrossRef] [PubMed]
- Larochelle, RD.; Koduri, VA.; Chen, RC.; Subramanian, PS. Embolic abducens palsy and central retinal artery occlusion in a patient with COVID-19. J Neuroophthalmol. 2022, 42, e500–e501. [Google Scholar] [CrossRef] [PubMed]
- Been Sayeed SKJ. ; Chandra Das S.; Mahmud, R.; Moniruzzaman, M.; Rahman, MM. Acute ischemic stroke with central retinal artery occlusion as a rare presentation of COVID-19 disease. Cureus. 2021, 13, e17469. [Google Scholar]
- Lee, KE.; Tschoe, C.; Coffman, SA.; Kittel, C.; Brown, PA.; Vu, Q.; Fargen, KM.; Hayes, BH.; Wolfe, SQ. Management of acute central retinal artery occlusion, a "retinal stroke": an institutional series and literature review. J Stroke Cerebrovasc Dis. 2021, 30, 105531. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.; Zheng, X.; Patel, AP.; Bhatti, MT.; Gilbert, A.; Vora, RA. Central retinal artery occlusion: visual outcomes from a large northern California cohort. Ophthalmol Retina. 2024, 8, 566–570. [Google Scholar] [CrossRef] [PubMed]
- St Peter, D.; Na, D.; Sethuraman, K.; Mathews, MK.; Li, AS. Hyperbaric oxygen therapy for central retinal artery occlusion: visual acuity and time to treatment. Undersea Hyperb Med. 50.
- Abdin, AD.; Gärtner, BC.; Seitz, B. Central retinal artery occlusion following COVID-19 vaccine administration. Am J Ophthalmol Case Rep. 2022, 26, 101430. [Google Scholar] [CrossRef] [PubMed]
- Chow, SY.; Hsu, YR.; Fong, VH. Central retinal artery occlusion after Moderna mRNA-1273 vaccination. J Formos Med Assoc. 2022, 121, 2369–2370. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Peltzer, C.; Buchowicz, B.; Dawson Slaney, E.; Maleki, A. Progressive central retinal artery occlusion, ophthalmic artery occlusion, and hemispheric intracranial thrombosis after COVID-19 mRNA vaccine application: case report. Case Rep Ophthalmol. 2023, 14, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Yamagishi, A.; Kitamura, Y.; Baba, T. Recovery from central retinal artery occlusion accompanying paracentral acute middle maculopathy after COVID-19 vaccination. Cureus. 2024, 16, e51501. [Google Scholar] [CrossRef] [PubMed]
- Thakar, M.; Bhattacharya, S. Central retinal artery occlusion after vaccination with whole virion inactivated SARSCoV- 2 vaccine Covaxin. Indian J Ophthalmol. 2022, 70, 3716–3718. [Google Scholar] [PubMed]
- Wang, LU.; Chen, FT.; Wang, JK.; Huang, TL.; Chang, PY.; Chen, YJ.; Hsu, YR. Ocular inflammatory manifestations following COVID-19 vaccinations in Taiwan: a case series. Taiwan J Ophthalmol. 2022, 12, 465–471. [Google Scholar] [PubMed]
- Kido, A.; Tamura, H.; Ikeda, HO.; Miyake, M.; Hiragi, S.; Tsujikawa, A. Nationwide incidence of central retinal artery occlusion in Japan: an exploratory descriptive study using the National Database of Health Insurance Claims (2011–2015). BMJ Open. 2020, 10, e041104. [Google Scholar] [CrossRef] [PubMed]
- Ateş, O.; Yıldırım, M.; Yıldırım, K. Branch retinal artery occlusion in patient with COVID-19: case report. Korean J Ophthalmol 2021, 35, 484–485. [Google Scholar] [CrossRef] [PubMed]
- Panigrahi, PK.; Navyasree, C.; Srija, YN. Combined central retinal vein occlusion with branch retinal artery occlusion in a leukaemic patient with COVID-19. Clin Exp Optom. 2023, 106, 933–934. [Google Scholar] [CrossRef]
- Hirosawa, K.; Inomata, T.; Sung, J.; Morooka, Y.; Huang, T.; Akasaki, Y.; Okumura, Y.; Nagino, K.; Omori, K.; Nakao, S. Unilateral branch retinal artery occlusion in association with COVID-19: a case report. Int J Ophthalmol. 2024, 17, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Uzun, A.; Keles Sahin, A.; Bektas, O. A unique case of branch retinal artery occlusion associated with a relatively mild Coronavirus disease 2019. Ocul Immunol Inflamm. 2021, 29, 715–718. [Google Scholar] [CrossRef] [PubMed]
- Ishibashi, K.; Yatsuka, H.; Haruta, M.; Kimoto, K.; Yoshida, S.; Kubota, T. Branch retinal artery occlusions, paracentral acute middle maculopathy and acute macular neuroretinopathy after COVID-19 vaccinations. Clin Ophthalmol. 2022, 16, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Girbardt, C.; Busch, C.; Al-Sheikh, M.; Gunzinger, JM.; Invernizzi, A.; Xhepa, A.; Unterlauft, JD.; Rehak, M. Retinal vascular events after mRNA and adenoviral-vectored COVID-19 vaccines—a case series. Vaccines (Basel). 2021, 9, 1349. [Google Scholar] [CrossRef] [PubMed]
- Murata, K.; Nagasato, D.; Tanaka, H.; Nakakura, S.; Nagasawa, T.; Mitamura, Y.; Tabuchi, H. Branch retinal artery occlusion with unruptured retinal arterial macroaneurysm post-SARS-CoV-2 vaccination: a case report. Eur J Ophthalmol. 2024, 34, NP53–NP56. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; Guan, L.; Wei, Y.; Li, H.; Wu, X.; Xu, J.; Tu, S.; Zhang, Y.; Chen, H.; Cao, B. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020, 395(10229), 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with Covid-19. J Thromb Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef] [PubMed]
- Choi, JJ.; Wehmeyer, GT.; Li, HA.; Alshak, MN.; Nahid, M.; Rajan, M.; Liu, B.; Schatoff, EM.; Elahjji, R.; Abdelghany, Y.; D'Angelo, D.; Crossman, D.; Evans, AT.; Steel, P.; Pinheiro, LC.; Goyal, P.; Safford, MM.; Mints, G.; DeSancho, MT. D-dimer cut-off points and risk of venous thromboembolism in adult hospitalized patients with COVID-19. Thromb Res. 2020, 196, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Wang, LU.; Chen, FT.; Wang, JK.; Huang, TL.; Chang, PY.; Chen, YJ.; Hsu, YR. Ocular inflammatory manifestations following COVID-19 vaccinations in Taiwan: a case series. Taiwan J Ophthalmol. 2022, 12, 465–471. [Google Scholar] [PubMed]
- Monagle, P.; Ng, AP.; Linden, M.; Ignjatovic, V.; Farley, A.; Taoudi, S.; Pasricha, SR.; Torresi, J. Vaccine-induced immune thrombosis and thrombocytopenia syndrome following adenovirus-vectored severe acute respiratory syndrome coronavirus 2 vaccination: a novel hypothesis regarding mechanisms and implications for future vaccine development. Immunol Cell Biol. 2021, 99, 1006–1010. [Google Scholar] [CrossRef] [PubMed]
- Hippisley-Cox, J.; Patone, M.; Mei, XW.; Saatci, D.; Dixon, S.; Khunti, K.; Zaccardi, F.; Watkinson, P.; Shankar-Hari, M.; Doidge, J.; Harrison, DA.; Griffin, SJ.; Sheikh, A.; Coupland, CAC. Risk of thrombocytopenia and thromboembolism after covid-19 vaccination and SARS-CoV-2 positive testing: self-controlled case series study. BMJ. 2021, 374, n1931. [Google Scholar] [CrossRef] [PubMed]
- Cheruiyot, I.; Kipkorir, V.; Ngure, B.; Misiani, M.; Munguti, J.; Ogeng'o, J. Arterial thrombosis in Coronavirus disease 2019 patients: a rapid systematic review. Ann Vasc Surg. 2021, 70, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Malas, MB.; Naazie, IN.; Elsayed, N.; Mathlouthi, A.; Marmor, R.; Clary, B. Thromboembolism risk of COVID-19 is high and associated with a higher risk of mortality: a systematic review and meta-analysis. EClinicalMedicine. 2020, 29, 100639. [Google Scholar] [CrossRef] [PubMed]
- Modjtahedi, BS.; Do, D.; Luong, TQ.; Shaw, J. Changes in the incidence of retinal vascular occlusions after COVID-19 diagnosis. JAMA Ophthalmol. 2022, 140, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Napal, B.; García-Palacios, JD.; González-Mesones, B.; Napal, JJ.; Hernández, JL. Retinal vein occlusion in the general population after COVID-19 vaccination and infection. Med Clin (Barc). 2023, 161, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Park, HS.; Kim, S.; Lee, CS.; Byeon, SH.; Kim, SS.; Lee, SW.; Kim, YJ. Retinal vascular occlusion risks during the COVID-19 pandemic and after SARS-CoV-2 infection. Sci Rep. 2023, 13, 16851. [Google Scholar] [CrossRef] [PubMed]
- Park, HS.; Lee, NK.; Lee, CS.; Byeon, SH.; Kim, SS.; Lee, SW.; Kim, YJ. Retinal artery and vein occlusion risks after coronavirus disease 2019 or coronavirus disease 2019 vaccination. Ophthalmology. 2024, 131, 322–332. [Google Scholar] [CrossRef]
- Al-Moujahed, A.; Boucher, N.; Fernando, R.; Saroj, N.; Vail, D.; Rosenblatt, TR.; Moshfeghi, DM. Incidence of retinal artery and vein occlusions during the COVID-19 pandemic. Ophthalmic Surg Lasers Imaging Retina. 2022, 53, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, Y.; Yamana, H.; Iwagami, M.; Ono, S.; Takeuchi, Y.; Michihata, N.; Uemura, K.; Yasunaga, H.; Aihara, M.; Kaburaki, T. Ocular adverse events after Coronavirus disease 2019 mRNA vaccination: matched cohort and self-controlled case series studies using a large database. Ophthalmology. 2023, 130, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Rachman, MJ.; Kalanjati, VP.; Rimbun, R.; Khadijah, F. Retinal vein occlusion amongst people vaccinated by mRNA- and viral vector- COVID-19 vaccines: a systematic review. Clin Ophthalmol. 2023, 28, 17–2825. [Google Scholar] [CrossRef] [PubMed]
- Muto, T.; Sakamoto, M.; Kusuda, S.; Haruyama, Y.; Machida, S.; Imaizumi, S.; Sekiryu, T. Effect of the COVID-19 pandemic on Vogt-Koyanagi-Harada disease. Sci Rep. 2024, 14, 13211. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Zhang, M.; Chen, M.; Lin, TPH. ; Lai, M.; Chen, H. Ocular trauma during COVID-19 pandemic: a systematic review and meta-analysis. Asia Pac J Ophthalmol (Phila). 2022, 11, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Sterczewska, A.; Wojtyniak, A.; Mrukwa-Kominek, E. Ocular complaints from students during COVID-19 pandemic. Adv Clin Exp Med. 2022, 31, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Krolo, I.; Blazeka, M.; Merdzo, I.; Vrtar, I.; Sabol, I.; Petric-Vickovic, I. Mask-associated dry eye during COVID-19 pandemic-how face masks contribute to dry eye disease symptoms. Med Arch. 2021, 75, 144–148. [Google Scholar] [CrossRef]
- H, Fortes.; D, Tailor P.; T Xu T.; A, Churchill R.; R Starr, M. Clinical characteristics and outcomes of endophthalmitis before and during the COVID-19 pandemic. J Ophthalmic Vis Res.
- Sakamoto, T.; Terasaki, H.; Yamashita, T.; Shiihara, H.; Funatsu, R.; Uemura, A; Japanese Retina and Vitreous Society. Increased incidence of endophthalmitis after vitrectomy relative to face mask wearing during COVID-19 pandemic. Br J Ophthalmol. 2023, 107, 1472–1477. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Danesh-Meyer, HV. A review of neuro-ophthalmic following COVID-19 infection and vaccination. Front Cell Infect Microbiol. 2024, 14, 1345683. [Google Scholar] [CrossRef] [PubMed]
- Liang, Z.; Yang, K.; Lv, K.; Ma, Y.; Hou, X.; Liang, Y.; Bao, Y.; Wu, H. Increased incidence of acute primary angle closure during the COVID-19 outbreak in China: A retrospective analysis. Medicine (Baltimore). 2024, 103, e38030. [Google Scholar] [CrossRef] [PubMed]
- Muto, T.; Machida, S.; Imaizumi, S.; Kamoi, K. Possible association between vaccination against SARS-CoV-2 and recurrence of macular edema due to branch retinal vein occlusion: a case report. J Int Med Res. 2023, 51, 3000605231213777. [Google Scholar] [CrossRef]
- Muto, T.; Sakamoto, M.; Imaizumi, S.; Kamoi, K. Reactivation of previously controlled Vogt-Koyanagi-Harada disease more than 46 years following COVID-19 vaccination: a case study. J Int Med Res. 2024, 52, 3000605231221081. [Google Scholar] [CrossRef]
- Muto, T.; Sakamoto, M.; Machida, S.; Imaizumi, S.; Hamada, Y.; Kamoi, K. Branch retinal vein occlusion following COVID-19 vaccination and SARS-CoV-2 infection while taking oral contraceptives. 2024. [Google Scholar] [CrossRef]
Figure 1.
Images from a 47-year-old female who developed branch retinal vein occlusion 3 weeks after receiving a COVID-19 diagnosis. (a) A retinal hemorrhage caused by the failure of the supratemporal vein in the patient’s right eye; (b) The retinal hemorrhage is visualized more clearly using autofluorescence mode; (c) Optical coherence tomography was used to focus in on the retinal foveola; (d) Retinal edema and an intraretinal cyst that have developed alongside the retinal hemorrhage.
Figure 1.
Images from a 47-year-old female who developed branch retinal vein occlusion 3 weeks after receiving a COVID-19 diagnosis. (a) A retinal hemorrhage caused by the failure of the supratemporal vein in the patient’s right eye; (b) The retinal hemorrhage is visualized more clearly using autofluorescence mode; (c) Optical coherence tomography was used to focus in on the retinal foveola; (d) Retinal edema and an intraretinal cyst that have developed alongside the retinal hemorrhage.
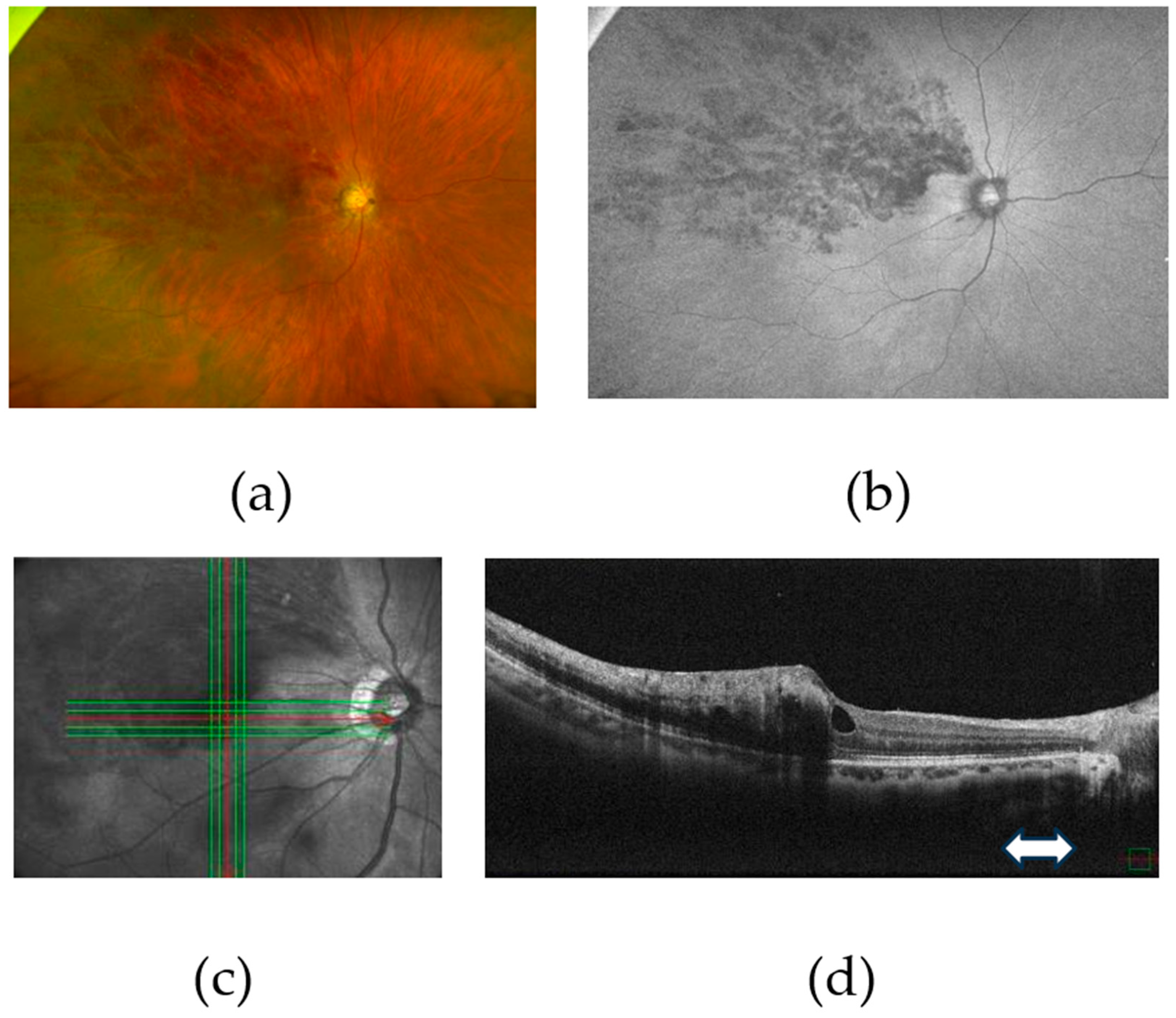

Table 1.
A.
| No. | Authors | Age | Sex | Laterality | Time between COVID-19 diagnosis and symptom onset (days) | Abnormal blood test findings |
|---|---|---|---|---|---|---|
| 1 | Invernizzi A et al. | 54 | F | R | 5 | CRP (31.1 mg/L) |
| Erythrocyte sedimentation rate (78) | ||||||
| lactate dehydrogenase (269 U/L) | ||||||
| PT 13.8 sec | ||||||
| aPTT 36.6 sec | ||||||
| fibrinogen (6.82 g/l) | ||||||
| d-dimer (426 μg/L) | ||||||
| 2 | Gaba WH et al. | 40 | M | R, L | 1 | ferritin (1518 μg/L) |
| lactate dehydrogenase (402 U/L) | ||||||
| d-dimer (>20 μg/L) | ||||||
| CRP (68 mg/L) | ||||||
| interlekin-6 (87.1 pg/mL) | ||||||
| 3 | Riazi-Esfahani H et al. | 35 | M | L | 120 | CRP borderline |
| homocysteine level borderline | ||||||
| 4 | Sheth JU, et al. | 52 | M | L | 10 | unremarkable |
| 5 | Walinjkar JA, et al. | 17 | F | R | 23 | not listed |
| 6 | Kılıçarslan O, et al. | 50 | M | R | 0 | PTT (20.3 s) |
| lactate dehydrogenase (222 U/L) | ||||||
| 7 | Raval et al. | 39 | M | R | 7 | unremarkable |
| 8 | Finn AP et al. | 32 | M | R | 30 | not listed |
| 9 | Lin CH et al. | 48 | M | R, L | 30 | d-dimer (1050 μg/L) |
| CRP (86.89 mg/L) | ||||||
| 10 | Yahalomi T et al. | 33 | M | L | 20 | unremarkable |
| 11 | Venkatesh R, et al. | 56 | F | L | 0 | d-dimer (707 μg/L) |
| ESR (52 mm) | ||||||
| 12 | Shroff D et al. | 41 | F | R | 21 | d-dimer (0.9 μg/L) |
| 13 | Staropoli PC et al. | 15 | M | L | 0 | no particular |
| 15 | Ashkenazy N et al. | 33 | M | 42 | not listed | |
| 29 | M | 84 | not listed | |||
| 24 | F | 28 | not listed | |||
| 36 | F | 98 | not listed | |||
| 22 | M | 63 | not listed | |||
| 18 | F | 21 | not listed | |||
| 50 | F | 126 | not listed | |||
| 41 | F | 105 | not listed | |||
| 34 | M | 98 | not listed | |||
| 30 | M | 42 | not listed | |||
| 31 | F | 7 | not listed | |||
| 38 | F | 28 | not listed | |||
| 16 | Płatkowska-Adamska B et al. | 38 | M | R | 180 | cholesterol (243 mg/dL) |
| d-dimer (543 ug/L) | ||||||
| 17 | Quigley C, et al. | 42 | M | R | 240 | WBC (3.5 x 109/L) |
| total cholesterol (5.4 mmol/L) | ||||||
| neutrophils (1.4 x 109/L) |
aPTT, activated partial thromboplastin time; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; F, female; L, left; M, male; PT, prothrombin time; PPT, partial prothrombin time; R, right; WBC, white blood cells.
Table 1.
B.
| No. | Authors | BCVA at initial visit | Treatment | Final BCVA |
|---|---|---|---|---|
| 1 | Invernizzi A et al. | 20/40 | oral prednisolone 60 mg/day | 20/20 (1 week) |
| 2 | Gaba WH et al. | 6/9 in the right eye | rivaroxaban 15 mg twice daily | |
| 6/18 in the left eye | ||||
| 3 | Riazi-Esfahani H et al. | CF | IV anti-VEGF (3 times) | not listed |
| 4 | Sheth JU, et al. | 6/60 | oral methylprednisolone (40 mg/day) | 6/9 (1 month) |
| IV Ranibizumab BS | ||||
| 5 | Walinjkar JA, et al. | 6/24 | IVR | 6/12 (2 month) |
| 6 | Kılıçarslan O, et al. | CF | IVA Systemic steroid therapy | CF (3 months) |
| 7 | Raval et al. | 20/150 | IVB | 20/30 |
| 8 | Finn AP et al. | 20/20 | not listed | not listed |
| 9 | Lin CH et al. | CF (both eyes) | IV anti-VEGF | not listed |
| 10 | Yahalomi T et al. | 20/25 | not listed | not listed |
| 11 | Venkatesh R, et al. | 6/18 | oral aspirin | 6/6 (1 month) |
| 12 | Shroff D et al. | 3/60 | IV anti-VEGF | not listed |
| 13 | Staropoli PC et al. | E” at 2 feet | Doxycycline 100mg twice daily | 20/200 |
| prednisolone eye drops | ||||
| IVB | ||||
| 15 | Ashkenazy N et al. | 20/20 | 20/15 | |
| 20/80 | IVB | 20/20 | ||
| 20/60 | 20/30 | |||
| 20/70 | IVB | 20/20 | ||
| 20/20 | 20/20 | |||
| 20/25 | 20/20 | |||
| 20/30 | plavix | 20/25 | ||
| 20/50 | 20/30 | |||
| 20/20 | 20/20 | |||
| CF | oral prednisolone | 20/20 | ||
| oral aspirin | ||||
| IVB | ||||
| 20/20 | 20/20 | |||
| 20/20 | IVB | 20/60 | ||
| 16 | Płatkowska-Adamska B et al. | 5/25 | IVR | 20/20 |
| 17 | Quigley C, et al. | 6/18 | IVB | not listed |
BCVA, best-corrected visual acuity; BS, biosimilar; CF, counting fingers; IV, intravitreal; IVA, intravitreal aflibercept; IVB, intravitreal bevacizumab; IVR, intravitreal ranibizumab; VEGF, vascular endothelial growth factor.
Table 2.
A.
| No. | Authors | Age | Sex | Laterality | Time between vaccination and刘symptom onset (days) |
|---|---|---|---|---|---|
| 1 | Sonawane NJ et al. | 50 | M | R | 4 |
| 43 | F | R | 3 | ||
| 2 | Ishiguro K et al. | 47 | M | R | 0 (8 hours) |
| 3 | Lee S et al. | 34 | M | L | 10-12 |
| 4 | Wu D et al. | 54 | M | L | 9 |
| 5 | Romano D et al. | 54 | F | R | 2 |
| 6 | Endo B et al. | 52 | M | L | 15 |
| 7 | Sung SY et al. | 25 | F | L | 10 |
| 8 | Dutta Majumder P et al. | 28 | M | R | 25 |
| 9 | Shah PP et al. | 27 | F | L | 10 |
| 10 | Takacs A et al. | 35 | M | R | 14 |
| 11 | Nangia P et al. | 13 | M | L | 15 |
| 12 | Bialasiewicz AA et al. | 50 | M | L | 0 |
F, female; L, left; M, male; R, right.
Table 2.
B.
| No. | Authors | Vaccine type | Vaccine number |
|---|---|---|---|
| 1 | Sonawane NJ et al. | Oxford-AstraZeneca (ChAdOx1 nCoV-19/ AZD1222) | second |
| Oxford-AstraZeneca (ChAdOx1 nCoV-19/ AZD1222) | second | ||
| 2 | Ishiguro K et al. | Pfizer/BioNTech (BNT162b2) | first |
| 3 | Lee S et al. | Pfizer/BioNTech (BNT162b2) | second |
| 4 | Wu D et al. | Pfizer/BioNTech (BNT162b2) | second |
| 5 | Romano D et al. | Oxford-AstraZeneca (ChAdOx1 nCoV-19/ AZD1222) | second |
| 6 | Endo B et al. | Pfizer/BioNTech (BNT162b2) | first |
| 7 | Sung SY et al. | Pfizer/BioNTech (BNT162b2) | third |
| 8 | Dutta Majumder P et al. | Oxford-AstraZeneca (ChAdOx1 nCoV-19/ AZD1222) | third |
| 9 | Shah PP et al. | Pfizer/BioNTech (BNT162b2) | first |
| 10 | Takacs A et al. | mRNA vaccine | first |
| 11 | Nangia P et al. | Corbevax COVID-19 vaccine | first |
| 12 | Bialasiewicz AA et al. | Pfizer/BioNTech (BNT162b2) | second |
Table 2.
C.
| No | Authors | Abnormal blood test findings | BCVA at initial visit |
|---|---|---|---|
| 1 | Sonawane NJ et al. | HbA1c 13.2% | 6/60 |
| Cre 1.9 mg/dL | |||
| ESR 49 | 5/60 | ||
| CRP 14.6 | |||
| RF 11 | |||
| d-dimer 6,077.4 ng/mL | |||
| 2 | Ishiguro K et al. | triglyceride 256 mg/dL | 20/200 |
| aPTT 30.6 s | |||
| CRP 177% | |||
| 3 | Lee S et al. | total cholesterol 227 | CF |
| LDL 159 | |||
| ESR 26 | |||
| 4 | Wu D et al. | not listed | 6/30 |
| 5 | Romano D et al. | normal | 20/400 |
| 6 | Endo B et al. | normal | 20/20 |
| 7 | Sung SY et al. | HbA1c 9.2% | 20/100 |
| 8 | Dutta Majumder P et al. | normal | 2/60 |
| 9 | Shah PP et al. | not listed | 20/20 |
| 10 | Takacs A et al. | serum prothrombin time 9.1 s | 0.5 |
| anti-prothrombin 123% | |||
| serum homocysteine 16.4 μmol/l | |||
| 11 | Nangia P et al. | normal | 6/7.5 |
| 12 | Bialasiewicz AA et al. | normal | 0.5 |
aPTT, activated partial thromboplastin time; BCVA, best-corrected visual acuity; CF, counting fingers; Cre, creatinine; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; HBA1c, hemoglobin A1c; LDL, low density lipoprotein; PT, prothrombin time; RF, rheumatoid factor.
Table 2.
D.
| No. | Authors | Treatment | Final BCVA |
|---|---|---|---|
| 1 | Sonawane NJ et al. | IV anti-VEGF | not listed |
| none | not listed | ||
| 2 | Ishiguro K et al. | IVA (5 treatments) | 20/20 (10 months) |
| 3 | Lee S et al. | oral methylprednisolone | 20/30 (3 weeks) |
| IV methylprednisolone | |||
| 4 | Wu D et al. | IVB | 6/12 |
| 5 | Romano D et al. | intravitreal dexamethasone implant | 20/200 |
| PRP | |||
| 6 | Endo B et al. | IV dexamethasone | 20/20 |
| IVB, oral apixaban | |||
| 7 | Sung SY et al. | IVR, IVA (3 treatments) | 20/30 |
| 8 | Dutta Majumder P et al. | pulse corticosteroid | 6/9 |
| oral corticosteroid | |||
| 9 | Shah PP et al. | IVR (3 treatments) | not listed |
| Acetazolamide | |||
| intravenous iron infusions | |||
| 10 | Takacs A et al. | IVA | 1.0 (2 months) |
| oral ASA protect | |||
| 11 | Nangia P et al. | pulse corticosteroid | 6/6 |
| 12 | Bialasiewicz AA et al. | aspirin | 1.0 (3 days) |
| IVA |
BCVA, best-corrected visual acuity; BS, biosimilar; CF, counting fingers; IVA, intravitreal aflibercept; IVB, intravitreal bevacizumab; IVR, intravitreal ranibizumab; PRP, pan-retinal photocoagulation; VEGF, vascular endothelial growth factor.
Table 3.
A.
| No. | Authors | Age | Sex | Laterality | Time between COVID-19 diagnosis and symptom onset (days) | Abnormal blood test findings |
|---|---|---|---|---|---|---|
| 1 | Nourinia R, et al. | 60 | F | L | 10 | slightly prolonged PT and PTT |
| high ESR level | ||||||
| high CRP level | ||||||
| high d-dimer level | ||||||
| high ferritin level | ||||||
| elevated WBC | ||||||
| 2 | Duff S, et al. | 74 | F | L | 90 | not listed |
| 3 | Karasu B, et al. | 48 | M | L | 60 | not listed |
| R | 90 | not listed | ||||
| 4 | Kapsis P, et al. | 65 | M | L | not listed | normal |
| 5 | Shiroma HF, et al. | 54 | F | not listed | 7 | not listed |
| 36 | M | not listed | 90 | not listed | ||
| 64 | M | not listed | 7 | not listed | ||
| 6 | Güven YZ, et al. | 53 | M | L | not listed | ESR 74 mm/h |
| CRP 29.8 mg/L | ||||||
| d-dimer 404 μg/L |
aPTT, activated partial thromboplastin time; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; F, female; L, left; M, male; PT, prothrombin time; PPT, partial prothrombin time; R, right; WBC, white blood cells.
Table 3.
B.
| No. | Authors | BCVA at Initial visit | Treatment | Final BCVA |
|---|---|---|---|---|
| 1 | Nourinia R, et al. | 20/200 | IVB | not listed |
| 2 | Duff S, et al. | 20/50 | intravitreal dexamethasone implant | not listed |
| 3 | Karasu B, et al. | 20/100 | heparin | 30/100 |
| 10/100 | pantoprazole | 40/100 | ||
| favipiravir | ||||
| 4 | Kapsis P, et al. | 6/36 | IVA | 6/9 |
| 5 | Shiroma HF, et al. | 20/25 | ketorolacid | 20/20 |
| 20/30 | IV anti VEGF | 20/20 | ||
| CF | IV anti VEGF | 20/200 | ||
| 6 | Güven YZ, et al. | 20/20 | not listed | not listed |
BCVA, best-corrected visual acuity; CF, counting fingers; IV, intravitreal; IVA, intravitreal aflibercept; IVB, intravitreal bevacizumab; VEGF, vascular endothelial growth factor.
Table 4.
A.
| No. | Authors | Age | Sex | Laterality | Time between vaccine and symptom onset (days) |
|---|---|---|---|---|---|
| 1 | Pur DR, et al. | 34 | M | R | 2 |
| 2 | Sugihara K, et al. | 38 | M | L | 2 |
| 3 | Gironi M, et al. | 50 | M | R | 1 |
| L | |||||
| 4 | Tanaka H, et al. | 50 | F | R | 3 |
| 56 | F | R | 3 | ||
| 5 | Karageorgiou G, et al. | 60 | M | R | 7 |
| 6 | Lee J, et al. | 41 | F | R | 2 |
| 7 | Silva LSCD, et al. | 66 | F | R | 16 |
| 8 | Peters MC, et al. | 71 | M | not listed | 2 |
| 73 | F | not listed | 3 | ||
| 47 | F | not listed | 5 | ||
| 9 | Choi M, et al. | 66 | M | L | 7 |
| 69 | F | L | 3 | ||
| 10 | Bolletta E, et al. | not listed | not listed | L | 23 |
| not listed | not listed | L | 2 | ||
| not listed | not listed | L | 2 | ||
| not listed | not listed | L | 3 |
F, female; L, left; M, male; R, right.
Table 4.
B.
| No. | Authors | type of vaccines | Numbers of times of vaccines |
|---|---|---|---|
| 1 | Pur DR, et al. | BNT162b2 (Pfizer-BioNTech) | first |
| 2 | Sugihara K, et al. | BNT162b2 (Pfizer-BioNTech) | second |
| 3 | Gironi M, et al. | mRNA-1237 vaccine (Moderna). | booster dose |
| 4 | Tanaka H, et al. | BNT162b2 (Pfizer-BioNTech) | first |
| BNT162b2 (Pfizer-BioNTech) | first | ||
| 5 | Karageorgiou G, et al. | ChAdOxl nCoV-19 (Oxford-AstraZeneca) | not listed |
| 6 | Lee J, et al. | not listed | second |
| 7 | Silva LSCD, et al. | ChAdOxl nCoV-19 (Oxford-AstraZeneca) | not listed |
| 8 | Peters MC, et al. | ChAdOxl nCoV-19 (Oxford-AstraZeneca) | first |
| ChAdOxl nCoV-19 (Oxford-AstraZeneca) | first | ||
| BNT162b2 (Pfizer-BioNTech) | first | ||
| 9 | Choi M, et al. | ChAdOxl nCoV-19 (Oxford-AstraZeneca) | second |
| ChAdOxl nCoV-19 (Oxford-AstraZeneca) | first | ||
| 10 | Bolletta E, et al. | not listed | second |
| not listed | first | ||
| not listed | second | ||
| not listed | second |
Table 4.
C.
| No. | Authors | Abnormal blood test findings | BCVA at initial visit |
|---|---|---|---|
| 1 | Pur DR, et al. | normal | 20/20 |
| 2 | Sugihara K, et al. | normal | 0.9 |
| 3 | Gironi M, et al. | mild alteration in liver function | 20/200 |
| 20/28 | |||
| 4 | Tanaka H, et al. | not listed | 20/25 |
| not listed | 13/20 | ||
| 5 | Karageorgiou G, et al. | normal | 20/20 |
| 6 | Lee J, et al. | ESR 46 mm/h | 6/18 |
| 7 | Silva LSCD, et al. | CRP 1.0 mg/dL | not listed |
| 8 | Peters MC, et al. | not listed | not listed |
| not listed | 6/60 | ||
| not listed | 6/19 | ||
| 9 | Choi M, et al. | not listed | 6/9.6 |
| not listed | 20/20 | ||
| 10 | Bolletta E, et al. | not listed | 20/20 |
| not listed | 20/20 | ||
| not listed | 20/100 | ||
| not listed | 20/32 | ||
| not listed | 20/22 |
BCVA, best-corrected visual acuity; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate.
Table 4.
D.
| No. | Authors | Treatment | Final BCVA |
|---|---|---|---|
| 1 | Pur DR, et al. | observation | 20/20 |
| 2 | Sugihara K, et al. | second dose of IVA | 1.2 |
| 3 | Gironi M, et al. | IVR PC | not listed |
| IVR PC | not listed | ||
| 4 | Tanaka H, et al. | three doses of IVR | 20/20 |
| three doses of IVR | 20/20 | ||
| 5 | Karageorgiou G, et al. | not listed | not listed |
| 6 | Lee J, et al. | three doses of IVR | 6/6 |
| 7 | Silva LSCD, et al. | not listed | not listed |
| 8 | Peters MC, et al. | not listed | not listed |
| IVB | not listed | ||
| IVA | not listed | ||
| 9 | Choi M, et al. | IVB | not listed |
| observation | not listed | ||
| 10 | Bolletta E, et al. | oral aspirin | not listed |
| IV anti-VEGF | 20/20 | ||
| IV anti-VEGF | 20/40 | ||
| IV anti-VEGF | 20/25 | ||
| IV anti-VEGF | 20/20 |
BCVA, best-corrected visual acuity; IV, intravitreal; IVA, intravitreal aflibercept; IVB, intravitreal bevacizumab; IVR, intravitreal ranibizumab; PC, photocoagulation; VEGF, vascular endothelial growth factor.
Table 5.
A.
| No. | Authors | Age | Sex | Laterality | Time between COVID-19 diagnosis and symptom onset (days) | Abnormal blood test findings |
|---|---|---|---|---|---|---|
| 1 | Bapaye MM, et al. | 42 | M | B | 13 | normal |
| 2 | Heidarzadeh HR, et al. | 44 | M | L | 21 | normal |
| 3 | Abbati G, et al. | 6 | F | L | 0 | CRP 1.12 mg/L |
| R | 0 | |||||
| 4 | Montesel A, et al. | 59 | M | L | 10 | normal |
| 5 | de Oliveira MR, et al. | 68 | F | L | 23 | d-dimer 1,386 μg/L |
| CRP 22.9 mg/L | ||||||
| fibrinogen 587 mg/dL | ||||||
| 6 | Ucar F, et al. | 54 | M | L | not listed | fibrinogen 405.1 mg/dL |
| CRP 128.29 mg/L | ||||||
| d-dimer 1041 μg/L | ||||||
| ferritin 458.53 | ||||||
| platelets 486x109 | ||||||
| 7 | Yalçınbayır Ö, et al. | 48 | F | R | 14 | elevated d-dimer levels |
| elevated fibrinogen levels | ||||||
| elevated factor VIII levels | ||||||
| elevated von Willebrand factor levels | ||||||
| decreased antithrombin levels | ||||||
| 66 | M | L | 22 | elevated d-dimer levels | ||
| elevated fibrinogen levels | ||||||
| elevated factor VIII levels | ||||||
| elevated von Willebrand factor levels | ||||||
| 8 | Lekha T, et al. | 47 | M | R | unknown | not listed |
| 9 | Acharya S, et al. | 60 | M | R | 12 | not listed |
| 10 | Larochelle RD, et al. | 68 | M | R | 0 | not listed |
| 11 | Been Sayeed SKJ, et al. | 38 | M | L | unknown | not listed |
CRP, C-reactive protein; F, female; L, left; M, male; R, right.
Table 5.
B.
| No. | Authors | BCVA at initial visit | Treatment | Final BCVA |
|---|---|---|---|---|
| 1 | Bapaye MM, et al. | LP | not listed | LP |
| 2 | Heidarzadeh HR, et al. | LP | oral prednisolone, PRP | NLP |
| 3 | Abbati G,et al | HM | heparin | CF |
| NLP | intravenous steroid | NLP | ||
| oral prednisolone | ||||
| 4 | Montesel A, et al. | LP | not listed | CF |
| 5 | de Oliveira MR, et al. | 20/400 | ocular massage | CF |
| hypotensive eyedrops | ||||
| 6 | Ucar F, et al. | CF | 20% mannitol | not listed |
| anterior chamber paracentesis | ||||
| topical brimonidine | ||||
| dorzolamide/timolol | ||||
| moxifloxacin/dexamethasone combination drops | ||||
| oral acetazolamide | ||||
| oral aspirin | ||||
| 7 | Yalçınbayır Ö, et al. | HM | anterior chamber paracentesis | HM |
| LP | amoxicillin clavulanic acid | LP | ||
| prednisolone | ||||
| 8 | Lekha T, et al. | 6/36 | not listed | not listed |
| 9 | Acharya S, et al. | NLP | not listed | not listed |
| 10 | Larochelle RD, et al. | LP | not listed | not listed |
| 11 | Been Sayeed SKJ, et al. | CF | not listed | not listed |
| 11 | Been Sayeed SKJ, et al. | CF | not listed | not listed |
BCVA, best-corrected visual acuity; CF, counting fingers; HM, hand motion; LP, light perception; NLP, no light perception; PRP, pan-retinal photocoagulation.
Table 6.
A.
| No. | Authors | Age | Sex | Laterality | Time between vaccine and symptom onset (days) |
|---|---|---|---|---|---|
| 1 | Abdin AD, et al. | 76 | F | L | 2 |
| 2 | Chow SY, et al. | 70 | M | R | 5 |
| 3 | Chen J, et al. | 40 | F | L | 21 |
| 4 | Yamagishi A, et al. | 33 | F | L | 1 |
| 5 | Thakar M, et al. | 44 | M | L | 10 |
| 6 | Wang LU, et al. | 70 | M | R | 5 |
F, female; L, left; M, male; R, right.
Table 6.
B.
| No. | Authors | Vaccine type | Vaccine number |
|---|---|---|---|
| 1 | Abdin AD, et al. | ChAdOxl nCoV-19 (Oxford-AstraZeneca) | first |
| 2 | Chow SY, et al. | mRNA-1237 vaccine (Moderna). | first |
| 3 | Chen J, et al. | BNT162b2 (Pfizer-BioNTech) | first |
| 4 | Yamagishi A, et al. | BNT162b2 (Pfizer-BioNTech) | second |
| 5 | Thakar M, et al. | Covaxin (Bharat Biotech, BBV152) | second |
| 6 | Wang LU, et al. | mRNA-1237 vaccine (Moderna). | not listed |
Table 6.
C.
| No. | Authors | Abnormal blood test findings | BCVA at initial visit |
|---|---|---|---|
| 1 | Abdin AD, et al. | normal | HM |
| 2 | Chow SY, et al. | unremarkable | CF |
| 3 | Chen J, et al. | LDL 125 mg/dL | 20/40 |
| 4 | Yamagishi A, et al. | not listed | not listed |
| 5 | Thakar M, et al. | ESR 28 mm/h | LP |
| 6 | Wang LU, et al. | anti-PF 4 73.34 ng/mL | CF |
BCVA, best-corrected visual acuity; CF, counting fingers; ESR, erythrocyte sedimentation rate; HM, hand motion; LDL, low density lipoprotein; LP, light perception; PF, platelet factor.
Table 6.
D.
| No. | Authors | Treatment | Final BCVA |
|---|---|---|---|
| 1 | Abdin AD, et al. | ocular massage | not listed |
| 500 ml pentoxifylline IV | |||
| dorzolamide eye drop | |||
| aspirin 100 mg | |||
| 2 | Chow SY, et al. | clopidogrel and hyperbaric oxygen therapy | CF |
| 3 | Chen J, et al. | heparin | NLP |
| 4 | Yamagishi A, et al. | intravenous D-mannitol | 1.2 |
| acetazolamide | |||
| 10-minute ocular massage | |||
| 5 | Thakar M, et al. | not listed | not listed |
| 6 | Wang LU, et al. | hyperbaric oxygen therapy | CF |
| topical antiglaucoma drops |
BCVA, best-corrected visual acuity; CF, counting fingers; NLP, no light perception.
Table 7.
A.
| No. | Authors | Age | Sex | Laterality | Time between COVID-19 diagnosis and symptom onset (days) | Abnormal blood test findings |
|---|---|---|---|---|---|---|
| 1 | Ateş O, et al. | 34 | F | R | 107 | CRP levels slightly abnormal |
| lupus anticoagulant levels slightly abnormal | ||||||
| fibrinogen levels slightly abnormal | ||||||
| d-dimer levels slightly abnormal | ||||||
| ferritin levels slightly abnormal | ||||||
| 2 | Panigrahi PK, et al. | 23 | F | R | 21 | PT 16 s |
| d-dimer 732 ng/ml | ||||||
| serum ferritin 411 µg/L | ||||||
| 3 | Hirosawa K, et al. | 43 | F | R | 30 | WBC 11.7 x 109/L |
| 4 | Uzun A, et al. | 65 | F | L | 5 w | d-dimer 1.76 mg/L |
CRP, C-reactive protein; F, female; L, left; M, male; PT, prothrombin time; R, right; w, week; WBC, white blood cells.
Table 7.
B.
| No. | Authors | BCVA at initial visit | Treatment | Final BCVA |
|---|---|---|---|---|
| 1 | Ateş O, et al. | 10/10 | hyperbaric oxygen therapy | not listed |
| 2 | Panigrahi PK, et al. | 6/9 | systemic anticoagulants | not listed |
| 3 | Hirosawa K, et al. | 20/25 | alprostadil | not listed |
| 4 | Uzun A, et al. | 20/25 | aspirin | not listed |
BCVA, best-corrected visual acuity.
Table 8.
A.
| No. | Authors | Age | Sex | Laterality | Time between vaccine and symptom onset (days) |
|---|---|---|---|---|---|
| 1 | Ishibashi, et al. | 38 | F | R | 15 |
| 80 | M | R | 42 | ||
| 86 | M | L | 4 | ||
| 57 | F | R | 61 | ||
| 2 | Girbardt, et al. | 38 | M | R | 3 |
| 3 | Murata, et al. | 75 | M | R | 1 |
F, female; L, left; M, male; R, right.
Table 8.
B.
| No. | Authors | Vaccine type | Number of the vaccine received |
|---|---|---|---|
| 1 | Ishibashi, et al. | BNT162b2 (Pfizer-BioNTech) | first |
| BNT162b2 (Pfizer-BioNTech) | second | ||
| BNT162b2 (Pfizer-BioNTech) | second | ||
| BNT162b2 (Pfizer-BioNTech) | second | ||
| 2 | Girbardt, et al. | Comirnaty (Pfizer-BioNTech) | second |
| 3 | Murata, et al. | BNT162b2 (Pfizer-BioNTech) | fourth |
Table 8.
C.
| No. | Authors | Abnormal blood test findings | BCVA at initial visit |
|---|---|---|---|
| 1 | Ishibashi, et al. | not listed | 20/13 |
| not listed | 20/20 | ||
| not listed | 20/25 | ||
| not listed | 20/13 | ||
| 2 | Girbardt, et al. | normal | not listed |
| 3 | Murata, et al. | normal except those affected by diabetes | 0.7 |
BCVA, best-corrected visual acuity.
Table 8.
D.
| No. | Authors | Treatment | Final BCVA |
|---|---|---|---|
| 1 | Ishibashi, et al. | not listed | not listed |
| not listed | not listed | ||
| not listed | not listed | ||
| not listed | not listed | ||
| 2 | Girbardt, et al. | aspirin | not listed |
| simvastatin | |||
| 3 | Murata, et al. | no treatment | 0.7 |
BCVA, best-corrected visual acuity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



