
Submitted:
29 July 2024
Posted:
30 July 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The term “Long COVID” is commonly used to describe persisting symptoms after acute COVID‑19. Until now, proposed mechanisms for the explanation of Long COVID have not related quantitative measurements to basic laws. In this work, a common framework for the Long COVID pathophysiological mechanism is presented, based on the blood supply deprivation and the flow diffusion equation. Methods: Case-control studies with statistically significant differences between cases (post-COVID patients) and controls, from multiple tissues and geographical areas, were gathered and tabulated. Microvascular loss (ML) was quantified by vessel density reduction (VDR), foveal avascular zone enlargement (FAZE), capillary density reduction (CDR), and percentage of perfused vessels reduction (PPVR). Both ML and hemodynamic decrease (HD), were incorporated in the tissue blood supply reduction (SR) estimation. Results: ML data were found from 763 post-COVID patients with an average VDR, FAZE, CDR, and PPVR of 16%, 31%, 14%, and 21%, respectively. The average HD from 72 post-COVID patients was 37%. The estimated SR for multiple tissues with data from 634 post-COVID patients reached a sizeable 47%. This large SR creates conditions of lower mass diffusion rates, hypoxia, and undernutrition, which at a multi-tissue level, for a long time, can explain the wide variety of the Long COVID symptoms. Conclusions: Disruption of peripheral tissue blood supply by the contribution of both ML and HD is proposed here to be the principal cause of the mechanism leading to Long COVID symptoms.

Keywords:
Long COVID
; pathophysiology
; microcirculation
; mechanism
; blood supply
; case-control studies
; microvascular loss
; microthrombosis
; hemodynamics
; diffusion.
1. Introduction
When the World Health Organization (WHO) declared on May 5, 2023, the end of the emergency for Covid-19, there was still an increase in confirmed COVID-19 deaths at several places in African, American, European, Southeastern Asia, and Western Pacific regions [1]. Currently, over 7 million deaths and over 775 million confirmed cases have been reported globally [2]. It should be noted that these numbers are underestimations since many countries have stopped or changed the frequency of reporting [2].
Some people cannot fully recover after the COVID-19 disease, presenting long-term symptoms which are usually named “Long-COVID-19”, “Long COVID syndrome”, “post-COVID-19 condition”, or “post-acute COVID-19 syndrome” [3,4]. In short, the term “Long COVID” is commonly used to describe signs and symptoms that persist after acute COVID-19 and this term is going to be used here.
COVID-19 disease affects a multitude of organs and systems, and Long COVID, as a post-infection condition, relates to various systems such as the respiratory, cardiovascular, and nervous systems, underpinning the need for elucidating the exact pathophysiological mechanism [5]. COVID-19 not only reduces significantly axial blood microvessel velocity but also has the devastating effect of causing extensive microthrombosis, as was shown by recent quantitative work on post-COVID patients [6].
Soon after, a normative velocity model in the exchange microvessels was proposed and tested successfully as a disease discriminator on post-COVID conjunctival data [7]. However, microvascular loss (ML), due to microthrombosis, was not taken into account in the normative velocity model because only functional microvessels (with blood flow) were included in the velocity measurements. In reality, the tissue blood supply was even lower due to micro-occlusion. In addition, data in those papers [6,7] were taken only from the conjunctival tissue and a limited geographical region.
In this work, Long COVID symptoms are described first, according to the available data. Then, since most of these symptoms can be attributed to microvascular deprivation of proper blood supply, the concept of microvascular blood supply (S) per flat tissue area is defined. With S, the contribution of both the microvascular hemodynamic decrease (HD) and the ML, is taken into account in post-COVID patients. Tissue blood supply reduction (SR) for a long time is the cause of persistent lower mass diffusion rates and therefore multiple tissue hypoxia and undernutrition which can explain most of the Long COVID symptoms. Evidence in support of this mechanism is presented from previously published case-control microcirculatory data from multiple tissues and geographical areas around the world.
2. Background on Long COVID and Symptoms
Paul Garner was the first to describe in a blog of the British Medical Journal (May 5, 2020) his severe post-COVID symptoms, ongoing 7 weeks after infection. The term “Long COVID” was first used two weeks later by Elisa Perego (May 20, 2020), to describe the cyclical, and multiphasic Long-term Covid illness [8]. Carfi et al. [9] were the first to report symptoms from a cohort of 143 patients that persisted 36 days (on average) after hospital discharge and 87% of the patients suffered persistence of at least one symptom, especially fatigue (53%), dyspnea (43%), joint pain (27%), and chest pain (22%). In a multistate survey of 270 COVID-19 adults with milder outpatient illness [10], only 65% had returned to their usual health state when interviewed 2-3 weeks after positive testing. In comparison, more than 90% of influenza outpatients recover within 2 weeks after positive testing [10]. Puntmann et al. [11] were the first to report a cardiovascular magnetic resonance imaging cohort study of 100 patients who recently recovered from COVID-19, and in their work, cardiac involvement and ongoing myocardial inflammation were demonstrated in 78% and 60% of the patients, respectively. In addition, they found a statistically significant discrimination between controls and post-COVIDs using C-reactive protein (CRP), a blood biomarker that positively correlates with the incidence of thrombosis.
According to a 6-month retrospective cohort study of 273,618 survivors of COVID-19 [12], 57% had one or more Long COVID features recorded during the whole 6-month period. The most commonly reported symptoms by order of percentage were anxiety/depression (23%), abnormal breathing (19%), abdominal symptoms (16%), fatigue/malaise (13%), chest/throat pain (13%), other pain (12%), headache (9%), cognitive symptoms (8%), and myalgia (3%). Huang et al. [13] reported that 76% of 1733 COVID-19 patients discharged from the hospital had at least one symptom 6 months after the acute infection. There were similar reports for milder cases of COVID-19 without hospitalization [3], where 61% of patients older than 46 years had persistent symptoms at a 6-month follow-up.
Rezel-Potts et al. [14] conducted a large case-control study with 428,650 COVID-19 patients with a maximum follow-up time of 52 weeks after diagnosis and found that cardiovascular disease was increased in the early COVID phase (first 4 weeks) with principal manifestations of pulmonary embolism, atrial arrhythmias, and venous thromboses (5-fold increase). The 5-fold increase in venous thromboses aligns closely with the 6-fold increase in conjunctival microthrombosis reported in COVID-19 survivors soon after hospital discharge [6]. Katsoularis et al. [15] conducted a nationwide matched cohort study and found that COVID-19 is an independent risk factor for deep vein thrombosis, pulmonary embolism, and bleeding and that the risk of these outcomes is increased for three, six, and two months after COVID-19, respectively.
Other researchers have reported fatigue as a major manifestation of Long COVID with a high prevalence (60-70%) [16-19]. Poor sleep quality is another common manifestation of Long COVID [16,19,20], and there were demonstrations of chronic pain either as a newly developed condition or a worsening of preexisting chronic pain [21]. The important neurological and psychiatric symptoms observed during Long COVID greatly puzzle scientists worldwide [22]. In addition, a recent retrospective study [16] of 287 patients with Long COVID symptoms found that fatigue, sleepiness, and sleep quality were SARS-CoV-2 variant independent. This supports the view of a common Long COVID pathophysiological mechanism for all virus variants, which is presented in the next section.
3. Materials and Methods
3.1. The Normative Range (NR) Diagram
The recently introduced velocity-diffusion (V-J) equation [23] is based on the well-known flow-diffusion (Q-J) equation [24], which is one of the fundamental equations of vascular physiology. The V-J equation describes the relation of the axial blood microvessel velocity (V) with the mass diffusion rate (J) of each blood solute through the walls of a microvessel (Figure 1).
After measuring axial velocities at many microvessels with the same diameter, from the same tissue of many healthy subjects (control group), an average axial velocity (AV) can be estimated statistically corresponding to an average mass diffusion rate (AJ). Since the AV is determined statistically, a normative range (NR) of the AV can be defined for microvessels of this diameter, corresponding to normal resting conditions, in a normative range (NR) diagram (Figure 1). The UR (Underemic Range) is a range of average axial velocities corresponding to underemic conditions on the left of the NR, and the HR (Hyperemic Range) is the range of average axial velocities corresponding to hyperemic conditions on the right of the NR. Underemic conditions are indicative of hypoxia, malnutrition, and disease. The NR diagram is the backbone of the normative microvascular velocity model and can be extended to many diameters [7].
3.2. Hemodynamic Decrease (HD)
In case-control hemodynamic studies, when a statistically significant reduction in the average blood velocity is detected in the case (post-COVID) group, it is direct proof that the average axial velocity (AV) of the case group is shifted to the left, in the underemic range (Figure 1). To quantify this shift, “Hemodynamic Decrease” (HD) is defined here as:
Where AVCONTROL and AVCOVID are
the average axial blood velocities in the control group and the post-COVID
group, respectively. HD ranges between 0% and 100% (for AVCONTROL >
AVCOVID). HD can be quantified with various techniques such as
Conjunctival Video Capillaroscopy (CVC) [25,26],
Laser Doppler Flowmetry (LDF) [27], and
special Magnetic Resonance Imaging (MRI) [28].
3.3. Microvascular Loss (ML)
“Microvascular loss” (ML) is defined generally as a deprivation of microvessels in a given tissue. ML can be detected in various tissues with various techniques such as Optical Coherence Tomography Angiography (OCTA), CVC, sublingual video capillaroscopy (SVC), and Nailfold Video Capillaroscopy (NVC).
In the following subsections, the well-known indices of vessel density (VD), foveal avascular zone (FAZ), capillary density (CD), and percentage of perfused vessels (PPV) are utilized to make quantitative estimates of ML from case-control studies.
3.3.1. Vessel Density Reduction (VDR)
Vessel density (VD) is defined as the total functional microvessel area per unit area in the region of measurement and is measured in percent (%). Functional microvessels are considered those with blood flow since most techniques require blood flow to detect a microvessel [29]. VD reduction (VDR) is defined as:
Where VDCONTROL and VDCOVID
are the averages in the control and the post-COVID group, respectively. For VDCONTROL
> VDCOVID, VDR ranges between 0% and 100%.
3.3.2. Foveal Avascular zone Enlargement (FAZE)
The foveal avascular zone (FAZ) is an approximately circular area without any blood vessels with a diameter of about 0.5 mm, located at the center of the fovea in the eye fundus. FAZ however, gets proper supply due to the special tissue architecture of that retinal section (foveal pit or foveola about 0.35 mm in diameter). FAZ enlargement (FAZE) is defined as:
Where FAZCONTROL and FAZCOVID are the averages in the control and the post-COVID group, respectively. FAZE can be considered a kind of microvascular loss in the most critical area of vision.
3.3.3. Capillary Density Reduction (CDR)
Capillary density (CD) is defined as the total capillary number per linear millimeter and is measured by nailfold video capillaroscopy (NVC). Capillary density reduction (CDR) is defined as:
Where CDCONTROL and CDCOVID are the averages in the control and the post-COVID group, respectively. CDR ranges between 0% and 100 (for CDCONTROL > CDCOVID).
3.3.4. Percentage of Perfused Vessels Reduction (PPVR)
The percentage of perfused vessels (PPV) is defined as the percentage of the number of perfused (functional) vessels over the total number of vessels, at a given microvascular area (field of view). The PPV is an index inversely related to the microvascular damage (thrombotic microoclusion) sustained by a tissue. The percentage of perfused vessels reduction (PPVR) is defined as:
Where PPVCONTROL and PPVCOVID are the averages in the control and the post-COVID group, respectively. PPVR ranges between 0% and 100% (for PPVCONTROL > PPVCOVID).
3.4. Blood Supply Reduction (SR)
In case-control microvascular studies, when a statistically significant ML is detected in the tissue of the case group, it is evident that there is an oxygen and nutrient undersupply in that tissue area. The current difficulty with the normative velocity model of Figure 1 is that ML is not taken into account. It is as if Figure 1 has many “zero points” (V = 0, J = 0) which are not measured. However, the higher the average zero points, the higher the tissue undersupply.
To overcome this difficulty, the blood supply (S) per flat tissue area is defined. For a given flat tissue surface area (field of view) of a subject, the blood supply S is the sum of all the blood volume flows (Q1 + Q2 + … + Qn) of the n functional exchange microvessels. This can be written as S = n Q, where Q is the average blood volume flow of the n microvessels. This can be written as S = n b V, where b is a parameter for the average cross-sectional area (m2) of the n microvessels and V is the average axial blood velocity (m/s) of the n microvessels. In this way, changes in the average number of functional microvessels can be incorporated into the S calculations.
In a case-control study with post-COVID patients, the average blood supply per flat tissue area for the control group can be expressed as SCONTROL = nCONTROL•bCONTROL•VCONTROL, where SCONTROL, nCONTROL, bCONTROL, and VCONTROL are the control group averages for the S, n, b, and V, respectively. In the same manner, for the post-COVID group: SCOVID = nCOVID•bCOVID• VCOVID.
In a situation where an average reduction of alpha (α) percent was observed in the number of microvessels in the post-COVID group, then nCOVID could be expressed as [(100-α)/100]nCONTROL. If on surplus an average hemodynamic reduction of HD percent was observed in the remaining functional microvessels, then VCOVID could be expressed as [(100-HD)/100]VCONTROL. Therefore, the average post-COVID group blood supply is written as:
With the condition that the average cross-sectional area of the remaining functional microvessels in the post-COVID group is the same as that in the control group (bCONTROL = bCOVID), equation 6 is written:
Finally, the blood supply reduction (SR) in percent is defined as:
After inserting equation 7 into equation 8:
Using equation 9, the total supply reduction SR from both the microvascular hemodynamic decrease (HD) and the microvascular loss (α) is taken into account. Of the four microvascular loss quantitative measures (VDR, FAZE, CDR, and PPVR), only two were defined on a flat tissue area: VDR and PPVR. Here it is considered that α can be approximated by VDR or PPVR depending on the available data.
3.5. The Proposed Pathophysiological Microcirculatory Mechanism for Long COVID
The steps and possible outcomes of the COVID-19 disease progress are shown in numbered rectangular boxes (Figure 2, boxes 1-9). The common framework for the proposed Long COVID mechanism is represented schematically by boxes 6, 7, 8, and 9, which are included in a dashed black line (Figure 2). Box 6 represents the subgroup of COVID-19 survivors with microvascular loss (ML) and hemodynamical decrease (HD) for several months after testing negative. Box 7 shows that both ML and HD, lead to tissue blood supply reduction (SR). The significant SR has consequently much lower diffusion rates (J) hence, multiple tissue hypoxia and undernutrition (box 8), which can be considered the cause of the Long COVID symptoms (box 9).
3.6. Statistical Analysis
Data were gathered from case-control microcirculatory studies with patients in the recovery phase of the COVID-19 disease (0 to 6 months after hospitalization or after having tested negative). These studies have reported statistically significant HD and ML metrics (VDR, FAZE, CDR, and PPVR). The Microsoft Office EXCEL 2016 software (professional edition) was used for the estimation of median, mean, and standard error of the mean (SEM). The statistical estimations were performed on different tissues since HD and ML metrics were all defined in relative units (percentages) to the control group reference.
4. Results
4.1. Hemodynamic Decrease (HD) case-control studies [Table 1]
In Table 1, case-control data are shown from 72 post-COVID patients, where a statistically significant HD was measured in 3 different tissue types (conjunctiva, skin, and brain), from 3 distant countries: Greece, Russia, and China. The reported HD ranged between 29% (p < 0.05) and 45% (p < 0.001) with a mean value of 37% and a standard error of the mean (SEM) of 8%.
4.2. Microvascular Loss (ML) Case-Control Studies [Table 2, Table 3, Table 4 and Table 5]
Post-COVID case-control data [30-46] of statistically significant microvascular loss (ML), are available zero to six months after hospital exit or after testing negative. These data come from A] the retina (measured by OCTA, Table 2 and Table 3), B] the choroid (measured by OCTA, Table 2), C] the sublingual tissue (measured by SVC, Table 2), D] the nailfold (measured by NVC, Table 4), and E] the conjunctiva (measured by CVC, Table 5).
According to these data, there was a statistically significant microvascular loss (ML) observed in 763 post-COVID patients. Results from these data are presented in the following subsections with quantitative estimates of the defined ML measures (Tables 2–5).
4.2.1. Vessel Density Reduction (VDR) Case-Control Studies [Table 2]
In Table 2, case-control data are shown from 562 post-COVID patients, where a statistically significant VDR was measured in 3 different tissues: the retina, the choroid, and the sublingual tissue [30-37, 40-44]. The reported VDRs ranged between 2 and 51% with a mean value of 16% and a standard error of the mean (SEM) of 5%.
4.2.2. FAZ Enlargement (FAZE) Case-Control Studies [Table 3]
In Table 3, case-control data are shown from 275 post-COVID patients [31-33, 37-39, 41], where a statistically significant FAZE was measured in the most critical area for proper vision. The reported FAZE ranged between 11 and 65% with a mean (± SEM) value of 31 ± 7%.
4.2.3. Capillary Density Reduction (CDR) Case-Control Studies [Table 4]
In Table 4, case-control data are shown from 86 post-COVID patients [45, 46], in whom a statistically significant CDR was measured. The reported CDR ranged between 11 and 17% with a mean (± SEM) equal to 14 ± 4%. In the study of Sulli et al. [46] no drug reversed significantly the CDR in COVID-19 survivors.
4.2.4. Percentage of Perfused Vessels Reduction (PPVR) case-control studies [Table 5]
Regarding the conjunctival microvascular bed, an average PPVR of 21% was reported (Table 5).
4.3. Blood SUPPLY REDUCTion (SR) [Table 6]
From HD and PPVR measurements on the same tissue (conjunctiva, Table 1 and Table 5, [6]) the estimated SR is 57% (Table 6). After combining the HD data of Table 1 [conjunctiva, skin, and brain], from 72 patients, with the VDR data of Table 2 [retinal, choroidal, and sublingual tissue], from 562 patients, an SR estimation of 47% is shown in Table 6.

Table 2.
Post-COVID case-control studies with statistically significant Vessel Density Reduction (VDR).
Table 2.
Post-COVID case-control studies with statistically significant Vessel Density Reduction (VDR).
| TISSUE | STUDY | VASCULAR BED | VDR (%) | N | |
|---|---|---|---|---|---|
| Retina | Savastano et al. [30] | RPCP | 3 | 80 | |
| Gonzalez-Zamora et al. [31] | foveal SCP | 48 | 25 | ||
| foveal DCP | 33 | ||||
| Bilbao-Malavé et al. [32] | foveal SCP | 51 | 17 | ||
| Abrishami et al. [33] | foveal DCP | 13 | 31 | ||
| Guemes-Villahoz et al. [34] | SCP & DCP | 7 | 66 | ||
| Hazar et al. [35] | superior sector DCP | 2 | 50 | ||
| Cennamo et al. [36] | whole image RPCP | 8 | 40 | ||
| Erogul et al. [37] | whole image SCP | 3 | 32 | ||
| Kalaw et al. [40] | 3 inner retinal layers | 8 | 7 | ||
| Urfalioğlu et al. [41] | DCP | 3 | 72 | ||
| El-Hadad et al. [42] | Deep macular plexus | 11 | 50 | ||
| RPCP | 6 | ||||
| Choroid | Üçer & Cevher [43] | choroidal microvessels | 6 | 65 | |
| Sublingual | Osiaevi et al. [44] | sublingual microvessels | 41 | 27 | |
| MEDIAN | 8 | - | |||
| MEAN ± SEM | 16 ± 5 | - | |||
| RANGE | 49 | - | |||
| TOTAL | 562 | ||||
Data refer to a post-COVID period of 0 to 6 months except for the study of Osiaevi et al. [44] that measured up to 18 months after infection. N: number of post-COVID patients, RPCP: Radial Peripapillary Capillary Plexus, SCP: Superficial Capillary Plexus, DCP: Deep Capillary Plexus, SEM: Standard Error of the Mean.
4.4. Results Supporting the Proposed Mechanism
According to available clinical information (Table 1), the axial blood microvessel flow of 72 post-COVID patients, was lower than normal with an average hemodynamic decrease (HD) of 37% (Figure 2, box 6). In addition, there was a statistically significant microvascular loss (ML) in 763 post-COVID patients (Table 2, Table 3, Table 4 and Table 5) and specifically, an average vessel density reduction (VDR) of 16% (Table 2, 562 patients), an average foveal avascular zone enlargement (FAZE) of 31% (Table 3, 275 patients), an average capillary density reduction (CDR) of 14% (Table 4, 86 patients), and a Percentage of Perfused Vessels Reduction (PPVR) of 21% (Table 5, 17 patients].
Table 3.
Post-COVID case-control studies with statistically significant Foveal Avascular Zone Enlargement (FAZE) in the human retina.
Table 3.
Post-COVID case-control studies with statistically significant Foveal Avascular Zone Enlargement (FAZE) in the human retina.
| STUDY | VASCULAR BED | FAZE (%) | N |
|---|---|---|---|
| Gonzalez-Zamora et al. [31] | SCP | 55 | 25 |
| Bilbao-Malave et al. [32] | SCP | 65 | 17 |
| Abrishami et al. [33] | whole image (SCP and DCP) | 12 | 31 |
| Erogul et al. [37] | whole image (SCP and DCP) | 11 | 32 |
| Dipu et al. [38] | SCP | 19 | 35 |
| DCP | 15 | ||
| Kal et al. [39] | SCP | 30 | 63 |
| DCP | 51 | ||
| Urfalioğlu et al. [41] | DCP FAZ | 20 | 72 |
| MEDIAN | 20 | - | |
| MEAN ± SEM | 31 ± 7 | - | |
| RANGE | 54 | - | |
| TOTAL | 275 | ||
Data refer to a post-COVID period of 0 to 6 months. N: number of post-COVID patients, SCP: Superficial Capillary Plexus, DCP: Deep Capillary Plexus. SEM: Standard Error of the Mean.
Table 4.
Post-COVID case-control studies with statistically significant Capillary Density Reduction (CDR) in the human nailfold.
Table 4.
Post-COVID case-control studies with statistically significant Capillary Density Reduction (CDR) in the human nailfold.
| STUDY | VASCULAR BED | CDR (%) | N |
|---|---|---|---|
| Çakmak et al. [45] | finger nailfold capillaries | 17 | 25 |
| Sulli et al. [46] | finger nailfold capillaries | 11* | 61 |
| MEDIAN | 14 | - | |
| MEAN ± SEM | 14 ± 3 | - | |
| RANGE | 6 | - | |
| TOTAL | 86 | ||
Data refer to a post-COVID period of 0 to 10 months except for the study of Sulli et al. [46] that measured patients up to 10 months after hospital discharge. N: number of post-COVID patients. * The average CDR between mild/moderate (34 subjects) and severe (27 subjects) cases.
Table 5.
Post-COVID case-control studies with statistically significant Percentage of Perfused Vessels Reduction (PPVR) in the human conjunctiva.
Table 5.
Post-COVID case-control studies with statistically significant Percentage of Perfused Vessels Reduction (PPVR) in the human conjunctiva.
| STUDY | VASCULAR BED | PPVR (%) | N |
|---|---|---|---|
| Koutsiaris et al. [6] | eye conjunctiva | 21 | 17 |
Data refer to a post-COVID period of 0 to 1 month. N: number of post-COVID patients.
The contribution of both hemodynamic decrease (HD) (Table 1) and vessel density reduction VDR (Table 2), is translated to an estimated blood supply reduction SR of 47% in multiple tissues (Table 6), (Figure 2, box 7). This estimation is very close to the 57% of the human conjunctiva (Table 6), where HD and PPVR measurements were performed on the same tissue.
The multiple tissue undersupply observed for so long (post-COVID period of 0 - 6 months, Table 1, Table 2, Table 3, Table 4, Table 5 and Table 6) leads to lower mass diffusion rates (J) according to the normative range diagram (Figure 1). The consequence of the persistent lower J is under-supply of oxygen (tissue hypoxia), undernutrition, and under-dispense of waste (Figure 2, box 8).
Hypoxic and undernutrition conditions at a multi-tissue level for a long time can explain the wide variety of the reported Long COVID symptoms (Figure 2, box 9): anxiety, depression, headache, cognitive decline, abnormal breathing, abdominal symptoms, fatigue, sleep disorders, and myalgia (see Section 2). This is especially true for the principal symptoms that derive from the brain, which is the most sensitive organ to oxygen supply: anxiety, depression, headache, cognitive decline, abnormal breathing, and sleep disorders.
Data refer to a post-COVID period of 0 to 6 months. α(alpha): average reduction in the number of functional exchange microvessels in the post-COVID group, PPVR: Percentage of Perfused Vessels Reduction, VDR: Vessel Density Reduction, HD: Hemodynamic Decrease, N: number of post-COVID patients.
Table 6.
Blood supply reduction (SR).
| TISSUE (DATA SOURCE) |
α (%) | HD (%) | SR (%) | N | |
|---|---|---|---|---|---|
| PPVR (%) | VDR (%) | ||||
| Conjunctiva (Table 1 & Table 5) |
21 | - | 45 | 57 | 17 |
| Conjunctiva/Skin/Brain (Table 1) |
- | - | 37 | - | 72 |
| Retina/Choroid/Sublingual (Table 2) |
- | 16 | - | - | 562 |
| Multiple Tissues (Table 1 & Table 2) |
- | 16 | 37 | 47 | 634 |
Data refer to a post-COVID period of 0 to 6 months. α(alpha): average reduction in the number of functional exchange microvessels in the post-COVID group, PPVR: Percentage of Perfused Vessels Reduction, VDR: Vessel Density Reduction, HD: Hemodynamic Decrease, N: number of post-COVID patients.
5. Discussion
Life is sustained by the diffusion of oxygen and nutrients towards the intracellular space. In animals with a circulatory system, this diffusive process takes mainly place in the exchange microvessels where the adequate supply of blood is of uttermost importance. When the normal tissue blood supply is disrupted at the microvascular level, there are serious side effects.
Early in the COVID-19 pandemic, Polak et al. [47] reported the importance of microvascular histological patterns and their persistence throughout the clinical course in their systematic review including 131 lung samples from either antemortem or postmortem COVID-19 patients (Figure 2, boxes 3-5). They identified 76 cases (59%) with microvascular damage (microthrombi) and proposed directed anti-inflammatory, anticoagulant, and/or anticomplement agents. Pretorius et al. [48] detected amyloid microclots in twenty COVID-19-positive blood samples before patient treatment, and Jung et al. [49] reported abdominal microcirculatory disorders (Figure 2, box 3). At the beginning of 2022, coagulopathy in patients hospitalized with COVID-19 was well-documented [50] and there were reports of enhanced hypercoagulability [51] and impaired fibrinolysis [52]. Endothelial dysfunction [53] is another characteristic of COVID-19 related to microvascular disease and vascular aging [54].
In this work, a common framework (Figure 2, boxes 6-9) was presented for the pathophysiological mechanism of the Long COVID symptoms reported by COVID-19 patients after hospital exit or after testing negative. After the acute phase (Figure 2, box 3), a multisystemic microvasculopathy persists for several months (Figure 2, box 6), as was presented in the results, for about 800 post-COVID patients (Table 1, Table 2, Table 3, Table 4 and Table 5). This can explain the Long COVID symptoms through the quantitative pathophysiological mechanism of the tissue blood supply reduction (SR) (Figure 2, boxes 7-9).
Regarding post-COVID patients, Patterson et al. [55] in the middle of 2020, reported that SARS-CoV-2 infection is associated with a wide spectrum of neurological syndromes, and D-dimers were markedly elevated in all patient subgroups. In a cohort study of 100 patients who recovered from COVID-19 [11], statistically significant discrimination between controls and post-COVIDs was reported using C-reactive protein (CRP), a blood biomarker that positively correlates with the incidence of thrombosis. Pretorius et al. [56] found microclots that were resistant to fibrinolysis, and a substantial increase in α2-antiplasmin, in blood samples from 11 post-COVID patients at least 2 months after recovery. The presence of amyloid microclots was also reported in blood samples from 80 post-COVID patients [57] (but without controls). Scheim et al. [58] proposed a mechanism of microclot formation with a central role of sialylated glycan attachments between SARS-CoV-2 spike protein and red blood cells. Kell and Pretorius [59] proposed ischemic injury from fibrin amyloid microclots as the primary factor for the Long COVID condition, and in line with this, Astin et al. [60] proposed lower tissue oxygen availability (chronic hypoxia) as a pathophysiological mechanism of Long COVID. The microclot blocking of capillaries in post-COVID patients was confirmed in vivo by Koutsiaris et al. [6] who also proposed microthrombosis as a possible explanation for Long COVID syndrome and speculated the existence of a possibly unknown coagulation factor.
The propositions mentioned above are well-fitted into the pathophysiological context of the present work, with the difference that here, case-control in vivo quantitative data were gathered, from multiple human tissues and multiple geographical places, with statistically significant differences between post-COVID cases and controls (Tables 1 to 5, Figure 2, box 6).
The major finding of a case-control study [61] with 120 Long COVID individuals 3-4 months after the acute infectious phase was the association of Long COVID with decreased antioxidant defenses as indicated by the lowered total antioxidant capacity of plasma. In addition, a high percentage of the variance in the severity of the Long COVID neuropsychiatric symptoms was explained by the increased C-reactive protein and the oxidative stress toxicity to antioxidant ratio. These findings are in support of the pathophysiological model resulting in tissue hypoxia in this work (Figure 2, box 8).
In a study with 87 COVID-19 survivors after hospitalization [62], exercise intolerance was reported, and a hypothesis of lung microvascular injury was made, as a pathophysiological mechanism leading to increased dead space as a fraction of tidal volume during exercise in post-COVID-19 patients. This hypothesis fits very well in the context of this work.
Gareau and Barrett [63] proposed a role of the impaired microbiota-gut-brain axis signaling in the development of Long COVID but this does not explain the extensive microthrombosis. However, a potential link to microthrombosis may exist in the gut-lung axis through the degradation of the intestinal epithelial cell junctional proteins and hence of the biochemical barrier to the microvessels.
Reiss et al. [64] explored possible mechanistic pathways between Long COVID and nervous system inflammation. In their review, it was noted that impaired blood flow in the brain due to viral invasion of the microvascular endothelium may be a neuropathological mechanism of Long COVID which agrees with this work.
In three recent Long COVID reviews [5,65,66] the need for understanding the pathophysiological mechanism of Long COVID was underscored, and various possible cellular and molecular mechanisms were described. Among them, the general concept of endothelial dysfunction-damage, microclot formation, persistent microvascular injury, and impairment of oxygen transfer, is in good agreement with this work, which supports it as the most prevalent mechanism.
For an indication of when the microvascular status returns to normal, a recent work [67] with retinal evaluations at an average of 15.2 ± 6.9 months post SARS-CoV-2 infection, reported no significant differences from controls.
Assuming conservatively that only 10% of the COVID-19-infected people developed Long COVID [68], at least 77.5 million subjects worldwide have shown Long COVID symptoms [2]. With insufficient current Long COVID diagnostic and treatment options [68] more basic and clinical research is needed for understanding Long COVID pathophysiological mechanisms.
6. Conclusions
In conclusion, a pathophysiological framework for the explanation of Long COVID was presented, based on published quantitative case-control data of reduced peripheral microvascular blood supply from about 800 post-COVID patients. More research data are essential to elucidate the Long COVID mechanism.
Funding
This research received no external funding.
Conflicts of Interest
The author declares no conflicts of interest.
References
- WHO (World Health Organization). COVID-19 Weekly Epidemiological Update. Edition 144, published 25 May 2023.
- WHO (World Health Organization). COVID-19 Weekly Epidemiological Update. Edition 168, published 17 June 2024.
- Blomberg, B.; Mohn, K.G.; Brokstad, K.A.; Zhou, F.; Linchausen, D.W.; Hansen, B.A.; et al. Long COVID in a prospective cohort of home-isolated patients. Nat. Med. 2021, 27, 1607–1613. [Google Scholar] [CrossRef]
- Venkatesan, P. NICE guideline on long COVID. Lancet Respir. Med. 2021, 9, 129. [Google Scholar] [CrossRef] [PubMed]
- Sideratou, C.M.; Papaneophytou, C. Persisting Shadows: Unraveling the Impact of Long COVID-19 on Respiratory, Cardiovascular, and Nervous Systems. Infectious Disease Reports 2023, 15, 806–830. [Google Scholar] [CrossRef]
- Koutsiaris, A.G.; Riri, K.; Boutlas, S.; Panagiotou, T.N.; Kotoula, M.; Daniil, Z.; Tsironi, E.E. COVID-19 hemodynamic and thrombotic effect on the eye microcirculation after hospitalization: A quantitative case-control study. Clin. Hemorheol. Microcirc. 2022, 82, 379–390. [Google Scholar] [CrossRef] [PubMed]
- Koutsiaris, A.G.; Riri, K.; Boutlas, S.; Daniil, Z.; Tsironi, E.E. A normative blood velocity model in the exchange microvessels for discriminating health from disease: Healthy controls versus COVID-19 cases. Clin. Hemorheol. Microcirc. 2023, 84, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Callard, F.; Perego, E. How and why patients made Long Covid. Soc. Sci. Med. 2021, 268, 113426. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F.; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Kim, S.S.; Lindsell, C.J.; et al. Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network — United States, March–June 2020. Morb. Mortal. Wkly Rep. 2020, 69, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Puntmann, V.O.; Carerj, M.L.; Wieters, I.; Fahim, M.; Arendt, C.; Hoffmann, J.; Shchendrygina, A.; Escher, F.; Vasa-Nicotera, M.; Zeiher, A.M.; Vehreschild, M.; Nagel, E. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. Erratum in: JAMA Cardiol. 2020, 5, 1308. 2020, 5, 1265–1273. [Google Scholar] [CrossRef]
- Taquet, M.; Dercon, Q.; Luciano, S.; Geddes, J.R.; Husain, M.; Harrison, P.J. Incidence, co-occurrence, and evolution of long-COVID features: A 6-month retrospective cohort study of 273,618 survivors of COVID-19. PLoS Med. 2021, 18, e1003773. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Rezel-Potts, E.; Douiri, A.; Sun, X.; Chowienczyk, P.J.; Shah, A.M.; Gulliford, M.C. Cardiometabolic outcomes up to 12 months after COVID-19 infection. A matched cohort study in the UK. PLoS Med. 2022, 19, e1004052. [Google Scholar] [CrossRef] [PubMed]
- Katsoularis, I.; Fonseca-Rodríguez, O.; Farrington, P.; Jerndal, H.; Lundevaller, E.H.; Sund, M.; Lindmark, K.; Fors Connolly, A.M. Risks of deep vein thrombosis, pulmonary embolism, and bleeding after covid-19: nationwide self-controlled cases series and matched cohort study. BMJ 2022, 377, e069590. [Google Scholar] [CrossRef]
- Percze, A.R.; Nagy, A.; Polivka, L.; Barczi, E.; Czaller, I.; Kovats, Z.; Varga, J.T.; Ballai, J.H.; Muller, V.; Horvath, G. Fatigue, sleepiness and sleep quality are SARS-CoV-2 variant independent in patients with long COVID symptoms. Inflammopharmacology 2023, 31, 2819–2825. [Google Scholar] [CrossRef]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long covid-mechanisms, risk factors, and management. BMJ Erratum in: BMJ 2021, 374, n1944. 2021, 374, n1648. [Google Scholar] [CrossRef]
- Baum, P.; Do, L.; Deterding, L.; Lier, J.; Kunis, I.; Saur, D.; Classen, J.; Wirtz, H.; Laufs, U. Cardiac function in relation to functional status and fatigue in patients with post-COVID syndrome. Sci. Rep. 2022, 12, 19575. [Google Scholar] [CrossRef]
- Merikanto, I.; Dauvilliers, Y.; Chung, F.; Wing, Y.K.; De Gennaro, L.; et al. Sleep symptoms are essential features of long-COVID - Comparing healthy controls with COVID-19 cases of different severity in the international COVID sleep study (ICOSS-II). J. Sleep. Res. 2023, 32, e13754. [Google Scholar] [CrossRef] [PubMed]
- Kalamara, E.; Pataka, A.; Boutou, A.; Panagiotidou, E.; Georgopoulou, A.; Ballas, E.; Chloros, D.; Metallidis, S.; Kioumis, I.; Pitsiou, G. Persistent Sleep Quality Deterioration among Post-COVID-19 Patients: Results from a 6-Month Follow-Up Study. J. Pers. Med. 2022, 12, 1909. [Google Scholar] [CrossRef] [PubMed]
- El-Tallawy, S.N.; Perglozzi, J.V.; Ahmed, R.S.; Kaki, A.M.; Nagiub, M.S.; LeQuang, J.K.; Hadarah, M.M. Pain Management in the Post-COVID Era-An Update: A Narrative Review. Pain Ther. 2023, 12, 423–448. [Google Scholar] [CrossRef]
- Peron, J.P.S. Direct and indirect impact of SARS-CoV-2 on the brain. Hum. Genet. 2023, 142, 1317–1326. [Google Scholar] [CrossRef]
- Koutsiaris, A.G. The velocity-diffusion equation in the exchange microvessels. Clin. Hemorheol. Microcirc. 2023, 84, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Renkin, E.M. B.W. Zweifach award lecture: regulation of the microcirculation. Microvasc. Res. 1985, 30, 251–63. [Google Scholar] [CrossRef] [PubMed]
- Jung, F.; Körber, N.; Kiesewetter, H.; Prünte, C.; Wolf, S.; Reim, M. Measuring the microcirculation in the human conjunctiva bulbi under normal and hyperperfusion conditions. Graefes Arch. Clin. Exp. Ophthalmol. 1983, 220, 294–7. [Google Scholar] [CrossRef] [PubMed]
- Koutsiaris, A.G. Meta-analysis of conjunctival microvascular hemorheology metrics. Microvasc. Res. 2022, 142, 104369. [Google Scholar] [CrossRef] [PubMed]
- Zharkikh, E.V.; Loktionova, Y.I.; Fedorovich, A.A.; Gorshkov, A.Y.; Dunaev, A.V. Assessment of Blood Microcirculation Changes after COVID-19 Using Wearable Laser Doppler Flowmetry. Diagnostics(Basel) 2023, 13, 920. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.; Wu, J.; Chen, T.; Li, J.; Zhang, G.; Wu, D.; Zhou, Y.; Zheng, N.; Cai, A.; Ning, Q.; Manyande, A.; Xu, F.; Wang, J.; Zhu, W. Long-term microstructure and cerebral blood flow changes in patients recovered from COVID-19 without neurological manifestations. J. Clin. Invest. 2021, 131, e147329. [Google Scholar] [CrossRef] [PubMed]
- Koutsiaris, A.G.; Batis, V.; Liakopoulou, G.; Tachmitzi, S.V.; Detorakis, E.T.; Tsironi, E.E. Optical Coherence Tomography Angiography (OCTA) of the eye: A review on basic principles, advantages, disadvantages and device specifications. Clin. Hemorheol. Microcirc. 2023, 83, 247–271. [Google Scholar] [CrossRef] [PubMed]
- Savastano, A.; Crincoli, E.; Savastano, M.C.; Younis, S.; Gambini, G.; De Vico, U.; Cozzupoli, G.M.; Culiersi, C.; Rizzo, S. Gemelli Against Covid-Post-Acute Care Study Group. Peripapillary Retinal Vascular Involvement in Early Post-COVID-19 Patients. J. Clin. Med. 2020, 9, 2895. [Google Scholar] [CrossRef]
- González-Zamora, J.; Bilbao-Malavé, V.; Gándara, E.; Casablanca-Piñera, A.; Boquera-Ventosa, C.; Landecho, M.F.; Zarranz-Ventura, J.; García-Layana, A. Retinal Microvascular Impairment in COVID-19 Bilateral Pneumonia Assessed by Optical Coherence Tomography Angiography. Biomedicines 2021, 9, 247. [Google Scholar] [CrossRef]
- Bilbao-Malavé, V.; González-Zamora, J.; Saenz de Viteri, M.; de la Puente, M.; Gándara, E.; Casablanca-Piñera, A.; Boquera-Ventosa, C.; Zarranz-Ventura, J.; Landecho, M.F.; García-Layana, A. Persistent Retinal Microvascular Impairment in COVID-19 Bilateral Pneumonia at 6-Months Follow-Up Assessed by Optical Coherence Tomography Angiography. Biomedicines 2021, 9, 502. [Google Scholar] [CrossRef]
- Abrishami, M.; Emamverdian, Z.; Shoeibi, N.; Omidtabrizi, A.; Daneshvar, R.; Saeidi Rezvani, T.; Saeedian, N.; Eslami, S.; Mazloumi, M.; Sadda, S.; Sarraf, D. Optical coherence tomography angiography analysis of the retina in patients recovered from COVID-19: a case-control study. Can. J. Ophthalmol. 2021, 56, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Guemes-Villahoz, N.; Burgos-Blasco, B.; Vidal-Villegas, B.; Donate-López, J.; de la Muela, M.H.; López-Guajardo, L.; Martín-Sánchez, F.J.; García-Feijoó, J. Reduced macular vessel density in COVID-19 patients with and without associated thrombotic events using optical coherence tomography angiography. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 2243–2249. [Google Scholar] [CrossRef] [PubMed]
- Hazar, L.; Karahan, M.; Vural, E.; Ava, S.; Erdem, S.; Dursun, M.E.; Keklikçi, U. Macular vessel density in patients recovered from COVID 19. Photodiagnosis Photodyn. Ther. 2021, 34, 102267. [Google Scholar] [CrossRef] [PubMed]
- Cennamo, G.; Reibaldi, M.; Montorio, D.; D'Andrea, L.; Fallico, M.; Triassi, M. Optical Coherence Tomography Angiography Features in Post-COVID-19 Pneumonia Patients: A Pilot Study. Am. J. Ophthalmol. 2021, 227, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Erogul, O.; Gobeka, H.H.; Dogan, M.; Akdogan, M.; Balci, A.; Kasikci, M. Retinal microvascular morphology versus COVID-19: What to anticipate? Photodiagnosis Photodyn. Ther. 2022, 39, 102920. [Google Scholar] [CrossRef]
- Dipu, T.; Goel, R.; Arora, R.; Thakar, M.; Gautam, A.; Shah, S.; Gupta, Y.; Chhabra, M.; Kumar, S.; Singh, K.; Kumar, S.; Garg, S.; Singh, H.; Pant, R. Ocular sequelae in severe COVID-19 recovered patients of second wave. Indian J. Ophthalmol. 2022, 70, 1780–1786. [Google Scholar] [CrossRef]
- Kal, M.; Winiarczyk, M.; Cieśla, E.; Płatkowska-Adamska, B.; Walczyk, A.; Biskup, M.; Pabjan, P.; Głuszek, S.; Odrobina, D.; Mackiewicz, J.; Zarębska-Michaluk, D. Retinal Microvascular Changes in COVID-19 Bilateral Pneumonia Based on Optical Coherence Tomography Angiography. J. Clin. Med. 2022, 11, 3621. [Google Scholar] [CrossRef]
- Kalaw, F.G.P.; Warter, A.; Cavichini, M.; et al. Retinal tissue and microvasculature loss in COVID-19 infection. Sci. Rep. 2023, 13, 5100. [Google Scholar] [CrossRef]
- Urfalioğlu, S.; Akkök, B.; Özdemir, G.; Daghan, B.; Guler, M. OCTA evaluation of posterior ocular blood flow in patients after COVID-19 infection without pneumonia. J Fr Ophtalmol. 2023, 46, 468–474. [Google Scholar] [CrossRef]
- El-Haddad, N.S.E.M.; Abd El-Wahed, E.; Abd El-Wahab, A.; Shalaby, S.; Farag, M.M.A.; Mohammed, N.S.; Shawky, S. The Effect of Post-Coronavirus Disease 2019 Infection on the Retinal Microvasculature. J. Curr. Ophthalmol. 2023, 35, 50–55. [Google Scholar] [CrossRef]
- Üçer, M.B.; Cevher, S. How does Covid-19 affect the choroidal structures at the early post-infectious period? J. Fr. Ophtalmol. 2023, 46, 106–113. [Google Scholar] [CrossRef]
- Osiaevi, I.; Schulze, A.; Evers, G.; Harmening, K.; Vink, H.; Kümpers, P.; Mohr, M.; Rovas, A. Persistent capillary rarefication in long COVID syndrome. Angiogenesis 2023, 26, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Çakmak, F.; Demirbuga, A.; Demirkol, D.; et al. Nailfold capillaroscopy: A sensitive method for evaluating microvascular involvement in children with SARS-CoV-2 infection. Microvasc. Res. 2021, 138, 104196. [Google Scholar] [CrossRef] [PubMed]
- Sulli, A.; Gotelli, E.; Bica, P.F.; Schiavetti, I.; Pizzorni, C.; Aloè, T.; Grosso, M.; Barisione, E.; Paolino, S.; Smith, V.; Cutolo, M. Detailed videocapillaroscopic microvascular changes detectable in adult COVID-19 survivors. Microvasc. Res. 2022, 142, 104361. [Google Scholar] [CrossRef] [PubMed]
- Polak, S.B.; Van Gool, I.C.; Cohen, D.; von der Thüsen, J.H.; van Paassen, J. A systematic review of pathological findings in COVID-19: a pathophysiological timeline and possible mechanisms of disease progression. Mod. Pathol. 2020, 33, 2128–2138. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, E.; Venter, C.; Laubscher, G.J.; Lourens, P.J.; Steenkamp, J.; Kell, D.B. Prevalence of readily detected amyloid blood clots in 'unclotted' Type 2 Diabetes Mellitus and COVID-19 plasma: a preliminary report. Cardiovasc. Diabetol. 2020, 19, 193. [Google Scholar] [CrossRef] [PubMed]
- Jung, E.M.; Stroszczynski, C.; Jung, F. Contrast enhanced ultrasonography (CEUS) to detect abdominal microcirculatory disorders in severe cases of COVID-19 infection: First experience. Clin. Hemorheol. Microcirc. 2020, 74, 353–361. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Bonaca, M.P. Studying the coagulopathy of COVID-19. Lancet 2022, 399, 118–119. [Google Scholar] [CrossRef] [PubMed]
- Kelliher, S.; Weiss, L.; Cullivan, S.; O’Rourke, E.; Murphy, C.A.; Toolan, S.; et al. Non-severe COVID-19 is associated with endothelial damage and hypercoagulability despite pharmacological thromboprophylaxis. J. Thromb. Haemost. 2022, 20, 1008–1014. [Google Scholar] [CrossRef]
- Watson, O.; Pillai, S.; Howard, M.; Zaldua, J.C.; Whitley, J.; Burgess, B.; Lawrence, M.; Hawkins, K.; Morris, K.; Evans, P.A. Impaired fibrinolysis in severe Covid-19 infection is detectable in early stages of the disease. Clin. Hemorheol. Microcirc. 2022, 82, 183–191. [Google Scholar] [CrossRef]
- Xu, S.W.; Ilyas, I.; Weng, J.P. Endothelial dysfunction in COVID-19: an overview of evidence, biomarkers, mechanisms and potential therapies. Acta Pharmacol. Sin. 2023, 44, 695–709. [Google Scholar] [CrossRef] [PubMed]
- Badaras, I.; Laučytė-Cibulskienė, A. Vascular Aging and COVID-19. Angiology 2023, 74, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Paterson, R.W.; Brown, R.L.; Benjamin, L.; Nortley, R.; Wiethoff, S.; Bharucha, T.; et al. The emerging spectrum of COVID-19 neurology: clinical, radiological and laboratory findings. Brain 2020, 143, 3104–3120. [Google Scholar] [CrossRef]
- Pretorius, E.; Vlok, M.; Venter, C.; Bezuidenhout, J.A.; Laubscher, G.J.; Steenkamp, J.; Kell, D.B. Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc. Diabetol. 2021, 20, 172. [Google Scholar] [CrossRef]
- Pretorius, E.; Venter, C.; Laubscher, G.J.; Kotze, M.J.; Oladejo, S.O.; Watson, L.R.; Rajaratnam, K.; Watson, B.W.; Kell, D.B. Prevalence of symptoms, comorbidities, fibrin amyloid microclots and platelet pathology in individuals with Long COVID/Post-Acute Sequelae of COVID-19 (PASC). Cardiovasc. Diabetol. 2022, 21, 148. [Google Scholar] [CrossRef] [PubMed]
- Scheim, D.E.; Vottero, P.; Santin, A.D.; Hirsh, A.G. Sialylated Glycan Bindings from SARS-CoV-2 Spike Protein to Blood and Endothelial Cells Govern the Severe Morbidities of COVID-19. Int. J. Mol. Sci. 2023, 24, 17039. [Google Scholar] [CrossRef]
- Kell, D.B.; Pretorius, E. The potential role of ischaemia-reperfusion injury in chronic, relapsing diseases such as rheumatoid arthritis, Long COVID, and ME/CFS: evidence, mechanisms, and therapeutic implications. Biochem. J. 2022, 479, 1653–1708. [Google Scholar] [CrossRef]
- Astin, R.; Banerjee, A.; Baker, M.R.; Dani, M.; Ford, E.; Hull, J.H.; Lim, P.B.; McNarry, M.; Morten, K.; O'Sullivan, O.; Pretorius, E.; Raman, B.; Soteropoulos, D.S.; Taquet, M.; Hall, C.N. Long COVID: mechanisms, risk factors and recovery. Exp. Physiol. 2023, 108, 12–27. [Google Scholar] [CrossRef]
- Al-Hakeim, H.K.; Al-Rubaye, H.T.; Al-Hadrawi, D.S.; Almulla, A.F.; Maes, M. Long-COVID post-viral chronic fatigue and affective symptoms are associated with oxidative damage, lowered antioxidant defenses and inflammation: a proof of concept and mechanism study. Mol. Psychiatry. 2023, 28, 564–578. [Google Scholar] [CrossRef]
- Lafetá, M.L.; Souza, V.C.; Menezes, T.C.F.; Verrastro, C.G.Y.; Mancuso, F.J.; Albuquerque, A.L.P.; Tanni, S.E.; Izbicki, M.; Carlstron, J.P.; Nery, L.E.; Oliveira, R.K.F.; Sperandio, P.A.; Ferreira, E.V.M. Exercise intolerance in post-coronavirus disease 2019 survivors after hospitalization. ERJ Open Res. 2023, 9, 00538–2022. [Google Scholar] [CrossRef]
- Gareau, M.G.; Barrett, K.E. Role of the microbiota-gut-brain axis in postacute COVID syndrome. Am. J. Physiol. Gastrointest. Liver Physiol. 2023, 324, G322–G328. [Google Scholar] [CrossRef] [PubMed]
- Reiss, A.B.; Greene, C.; Dayaramani, C.; Rauchman, S.H.; Stecker, M.M.; De Leon, J.; Pinkhasov, A. Long COVID, the brain, nerves, and cognitive function. Neurol. Int. 2023, 15, 821–841. [Google Scholar] [CrossRef] [PubMed]
- Constantinescu-Bercu, A.; Lobiuc, A.; Căliman-Sturdza, O.A.; Oiţă, R.C.; Iavorschi, M.; Pavăl, N.E.; Șoldănescu, I.; Dimian, M.; Covasa, M. Long COVID: Molecular Mechanisms and Detection Techniques. Int. J. Mol. Sci. 2023, 25, 408. [Google Scholar] [CrossRef]
- Tziolos, N.R.; Ioannou, P.; Baliou, S.; Kofteridis, D.P. Long COVID-19 Pathophysiology: What Do We Know So Far? Microorganisms 2023, 11, 2458. [Google Scholar] [CrossRef] [PubMed]
- Noor, M.; McGrath, O.; Drira, I.; Aslam, T. Retinal Microvasculature Image Analysis Using Optical Coherence Tomography Angiography in Patients with Post-COVID-19 Syndrome. Journal of Imaging 2023, 9, 234. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: major findings, mechanisms and recommendations. Nat. Rev. Microbiol. Erratum in: Nat. Rev. Microbiol. 2023, 21, 408. 2023, 21, 133–146. [Google Scholar] [CrossRef]
Figure 1.
The velocity-diffusion (V-J) equation (black dot curve) and the normative range (NR) diagram [7]. After measuring axial blood velocities at many microvessels with the same diameter, from the same tissue of many healthy persons (control group), an average axial velocity (AV) and a normative range (NR) can be determined statistically. AJ is the average mass diffusion rate corresponding to AV. An “underemic range” (UR), and “hyperemic range” (HR) can be defined corresponding to average velocities (case group) on the left and the right of the NR, respectively.
Figure 1.
The velocity-diffusion (V-J) equation (black dot curve) and the normative range (NR) diagram [7]. After measuring axial blood velocities at many microvessels with the same diameter, from the same tissue of many healthy persons (control group), an average axial velocity (AV) and a normative range (NR) can be determined statistically. AJ is the average mass diffusion rate corresponding to AV. An “underemic range” (UR), and “hyperemic range” (HR) can be defined corresponding to average velocities (case group) on the left and the right of the NR, respectively.
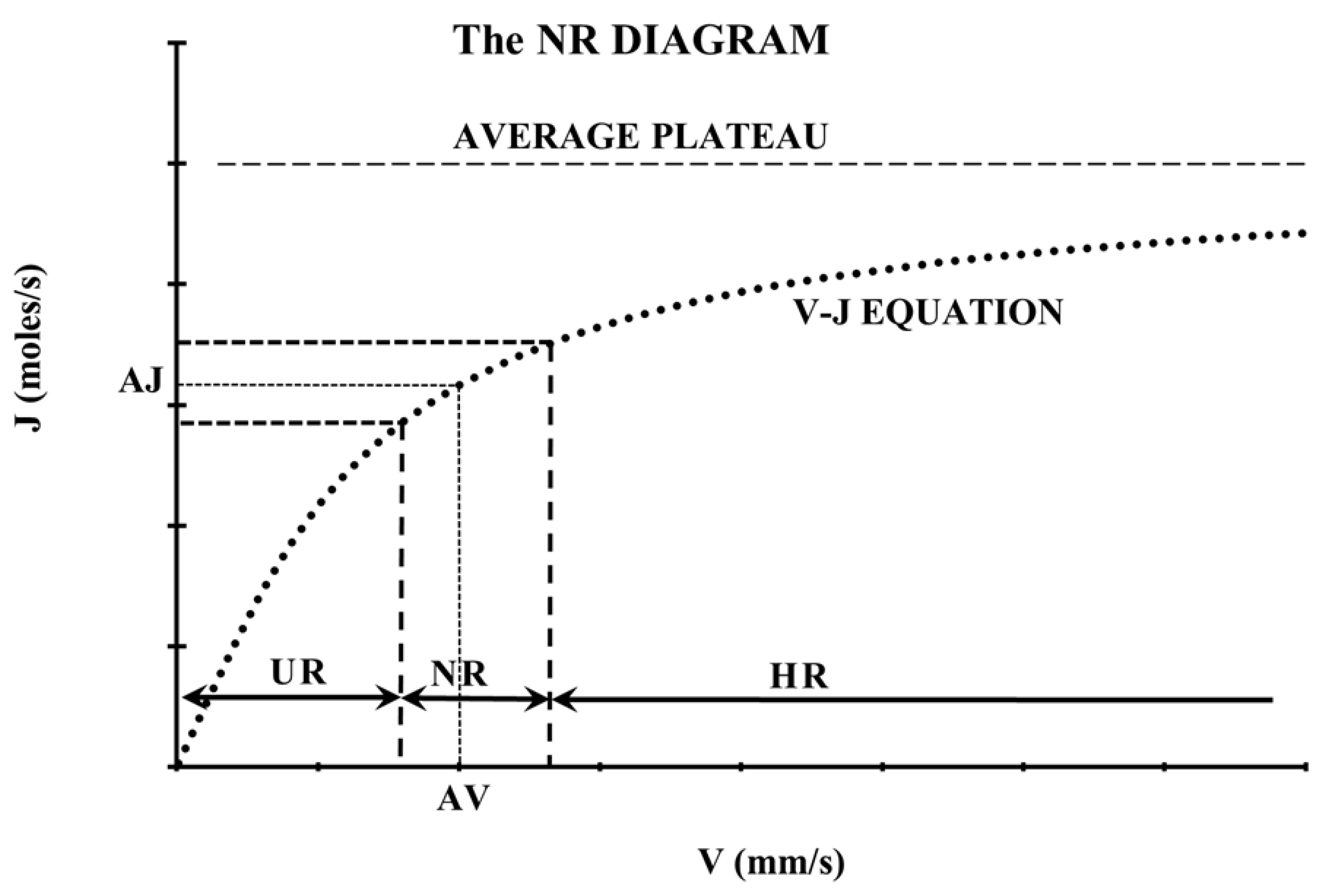
Figure 2.
The steps and possible outcomes of the COVID-19 disease progress are shown in numbered rectangular boxes. Boxes with end states are shown in solid bold black lines. The common framework for the proposed Long COVID mechanism is represented by boxes 6, 7, 8, and 9, which are inside the dashed black line. ICU: Intensive Care Unit, ML: Microvascular Loss, HD: Hemodynamic Decrease, NR: Normative Range, J: mass diffusion rate (moles/s).
Figure 2.
The steps and possible outcomes of the COVID-19 disease progress are shown in numbered rectangular boxes. Boxes with end states are shown in solid bold black lines. The common framework for the proposed Long COVID mechanism is represented by boxes 6, 7, 8, and 9, which are inside the dashed black line. ICU: Intensive Care Unit, ML: Microvascular Loss, HD: Hemodynamic Decrease, NR: Normative Range, J: mass diffusion rate (moles/s).
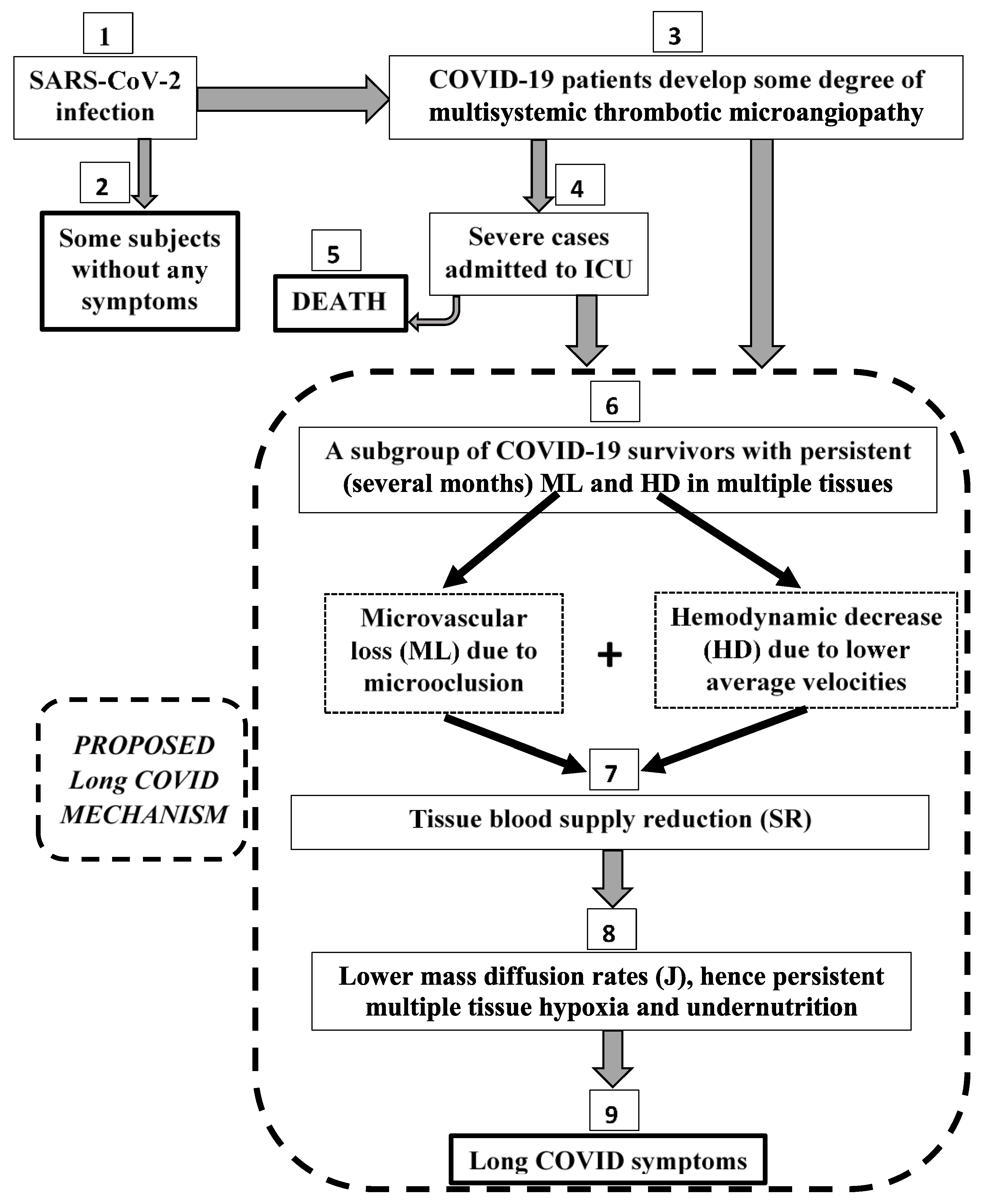
Table 1.
Post-COVID case-control studies with statistically significant hemodynamic decrease (HD).
| TISSUE | STUDY | VASCULAR BED / METHOD | HD (%) | N |
|---|---|---|---|---|
| Conjunctiva | Koutsiaris et al. [6] | exchange microvessels / CVC | 45 | 17 |
| Skin | Zharkikh et al. [27] | wrist and shin microvessels / LDF | 29 | 23 |
| Brain | Qin et al. [28] | gray matter cortex, subcortical nuclei / MRI | - | 32 |
| MEDIAN | 37 | - | ||
| MEAN ± SEM | 37 ± 8 | - | ||
| RANGE | 16 | - | ||
| TOTAL | 72 | |||
Data refer to a post-COVID period of 0 to 6 months. The HD of 45% [6] is the average among 3 different microvessel classes (capillaries, postcapillary venules of size 1 and 2). The HD of 29% [27] is the average between the wrists and shins. N: number of post-COVID patients, CVC: Conjunctival Video Capillaroscopy, LDF: Laser Doppler Flowmetry, MRI: Magnetic Resonance Imaging, SEM: Standard Error of the Mean.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



