Submitted:
30 July 2024
Posted:
30 July 2024
You are already at the latest version
Abstract
Background/Objectives: Women with subclinical hypothyroidism (SCH) were reported to be at an increased perinatal risk. We aimed to investigate the relationship between SCH and perinatal outcomes in singleton pregnancies resulting from assisted reproduction technology (ART). Methods: We retrospectively examined the perinatal outcomes of ART singleton pregnancies in women who underwent thyroid function screening before conception and delivered at our hospital from January 2020 to July 2023. We defined SCH as thyroid-stimulating hormone (TSH) levels <2.5 mU/L and normal free T4 levels. The patients were divided into three groups: normal thyroid function (group A), SCH without levothyroxine therapy (group B), and SCH with levothyroxine therapy (group C). The risks of preterm birth, preeclampsia, fetal growth restriction, manual placental removal, and blood loss at delivery were compared among the three groups. Results: Out of the 650 ART singleton deliveries, 581 were placed in group A, 34 in group B, and 35 in group C. The preterm birth rate at <34 weeks was significantly higher in group B and significantly lower in group C than in group A. The rate of preterm delivery at <34 weeks increased in correlation with TSH levels. Levothyroxine therapy was the significant preventive factor for preterm birth at <34 weeks. Conclusions: The preterm birth rate before 34 weeks was significantly higher in the SCH group. Levothyroxine therapy is a significant protective factor against preterm birth before 34 weeks. Universal screening for thyroid function and appropriate hormone therapy in pregnant women may help reduce perinatal risks, including preterm birth.
Keywords:
ART
; preterm birth
; subclinical hypothyroidism
; thyroid stimulating hormone
; levothyroxine therapy
1. Introduction
Thyroid function studies using the Japanese adult general health examination system documented thyroid dysfunction in nearly 10% of cases, with subclinical hypothyroidism (SCH) accounting for half of the cases [1]. This finding suggests that many pregnant women may have undiagnosed SCH. SCH is defined as normal free T4 levels and elevated serum thyroid-stimulating hormone (TSH) levels. It is observed in 2.0–2.5% of screened pregnant women according to reports from iodine-sufficient areas of the United States [2,3].
Some [4,5,6,7], but not all [8,9], studies have shown that women with SCH have a higher perinatal risk of severe preeclampsia, preterm delivery, placental abruption, neonatal respiratory distress syndrome, and/or pregnancy loss than do euthyroid women. One meta-analysis from 19 cohort studies reported an odds ratio (OR) of 1.29 (95% confidence interval [CI], 1.01–1.64) for preterm birth [10], and another meta-analysis reported an OR of 1.53 (95% CI, 1.09–2.15) for preeclampsia [6]. Interestingly, preterm delivery rates increase with TSH levels as follows: 5.4% of pregnancies with TSH levels between 4 and 6 mU/L, 7.8% between 6 and 10 mU/L, and 11.4% with >10 mU/L [11]. Furthermore, limited data suggest that perinatal outcomes are worse in women undergoing in vitro fertilization (IVF) if their preconception TSH levels are >2.5 mU/L. In one study of pregnancies after IVF, 150 deliveries with a preconception TSH level <2.5 mU/L were associated with a higher gestational age and birth weight than 45 deliveries with a TSH level >2.5 mU/L [12].
Because overt or SCH is thought to be associated with pregnancy complications and thyroid testing is common and easy to perform, attention has been focused on the utility of screening for thyroid dysfunction in all pregnant women. To the best of our knowledge, no high-quality studies have used a universal screening for thyroid function in pregnant women. The advantages and disadvantages of screening thyroid function in all pregnant women in early pregnancy remain inconclusive. This is because there are insufficient data to show not only the effects of thyroid disease on pregnancy but also the benefits of hormone therapy [13,14]. In Japan, universal screening for thyroid dysfunction in asymptomatic pregnant women is rare; however, universal screening for thyroid dysfunction is common in women initiating fertility treatment. This study aimed to examine the association between the presence of SCH and perinatal outcomes in assisted reproduction technology (ART) pregnancies using preconception thyroid function screening and the effects of thyroid hormone replacement (levothyroxine sodium hydrate) during pregnancy.
2. Materials and Methods
2.1. Participants
This retrospective cohort study analyzed the perinatal outcomes of pregnancies delivered at the Japanese Red Cross Nagoya Daiichi Hospital, Nagoya, Japan, between January 2020 and July 2023. This study included ART singleton pregnancies in which thyroid function screening was performed before conception (n=687). Among them, we excluded 22 cases of overt thyroid disease (n=22) and 15 cases of placenta previa (n=15) (Figure 1).
This study was approved by the Ethics Committee of the Japanese Red Cross Aichi Medical Center Nagoya Daiichi Hospital, Nagoya, Japan (approval number: 2023-070). Data were compiled and analyzed such that personal information could not be identified.
2.2. Data Collection and Definition
In this study, we defined SCH as preconception TSH levels >2.5 mU/L and normal free T4 levels. Patients with preconception TSH levels <2.5 mU/L were assigned to group A (normal group). Patients with SCH were divided into two groups—women who took levothyroxine sodium hydrate before and throughout pregnancy (group C) and those who did not (group B). The following maternal and perinatal data were obtained from medical records: age, parity, gestational weeks at delivery, body mass index before pregnancy, history of abortion, history of previous cesarean deliveries, preterm birth (at <37 weeks, <34 weeks, <32 weeks, and <28 weeks), preeclampsia, fetal growth restriction (FGR), blood loss at delivery, transfusion, manual placental removal, and the value of TSH before pregnancy. We also obtained the birth weight of the newborns. Preeclampsia was defined as the appearance of gestational hypertension, proteinuria, and/or signs of end-organ dysfunction during pregnancy [15]. FGR was defined as body weight at birth <–1.5 than the standard deviation for gestational age in Japan [16].
2.3. Statistical Analyses
Data were entered into a spreadsheet software (Excel, Microsoft Japan Co., Ltd., Tokyo, Japan). EZR (version 1.37; Saitama, Japan) was used for all the data analyses. The Shapiro–Wilk test was used to analyze the normality of the data. The Kruskal–Wallis test was used to compare continuous variables among the three groups. The Mann–Whitney U test was used for nonparametric comparisons during the post hoc analysis. Fisher’s exact test was used to compare categorical variables. In multivariate analysis, maternal age, body mass index, parity, preeclampsia, FGR, history of abortion, levothyroxine therapy, and TSH levels were selected as variables associated with preterm birth. P<0.05 was considered statistically significant.
3. Results
Among the 650 ART singleton deliveries in this study, 581 were assigned to group A, 34 to group B, and 35 to group C (Figure 1). The three groups did not significantly differ in terms of age, body mass index, history of previous cesarean deliveries, blood loss at delivery, manual placental removal, transfusion, preeclampsia, FGR, history of abortion, and neonatal body weight (Table 1).
Expectedly, the TSH levels were significantly lower in group A than in groups B and C (P<0.001). The rate of preterm birth at <34 weeks was significantly higher in group B (14.7%) and significantly lower in group C (0%) than in group A (P=0.046). Group C had no cases of preterm delivery under 34 weeks. The preterm birth rate at <37 weeks was lower in group C (5.7%) than in groups A and B; however, the difference was not significant (P=0.059) (Table 1).
When 69 patients diagnosed with SCH (groups B and C) were examined for the rate of preterm delivery at <34 weeks per TSH level, the rates were 1/30 (3.3%) at TSH levels of 2.5–3 mU/L, 2/22 (9.1%) at 3–4 mU/L, and 2/17 (11.8%) at >4 mU/L. The rate of preterm delivery at <34 weeks increased according to the TSH levels, but the difference was not statistically significant.
The results of multivariate analysis of the risk of preterm birth at <37 weeks are shown in Table 2.
When performing the multivariate analysis, we included maternal age, body mass index, parity, preeclampsia, FGR, history of abortion, levothyroxine therapy, and TSH levels as variables to calculate the OR. Preeclampsia (OR=4.98) and FGR (OR=3.31) were significant risk factors for preterm birth at <37 weeks; however, levothyroxine therapy and TSH levels did not affect the risk of preterm birth at <37 weeks.
The results of the multivariate analysis of the risk of preterm birth at <34 weeks are shown in Table 3.
In the multivariate analysis, we included maternal age, body mass index, parity, preeclampsia, FGR, history of abortion, levothyroxine therapy, and TSH level as variables to calculate the OR. The significant risk factor for preterm birth at <34 weeks was preeclampsia (OR=3.65; 95% CI, 1.65–8.09), and the significant preventive factor was levothyroxine therapy (OR=0.117; 95% CI, 0.015–0.948).
4. Discussion
We investigated the effects of SCH and its preconception treatment on the perinatal outcomes of ART singleton pregnancies, all of which were screened for thyroid function prior to conception. The preterm birth rate at <34 weeks was significantly higher in patients with SCH; however, it was significantly lower in patients with SCH treated with levothyroxine therapy before pregnancy. The rate of preterm delivery at <34 weeks increased according to TSH levels. The multivariate analysis revealed that levothyroxine therapy was a significant protective factor against preterm birth at <34 weeks.
Women with SCH have a higher risk of preeclampsia and preterm delivery than do euthyroid women [5,6,10]. However, in this study, we found that the rate of preterm birth at <34 weeks was significantly higher in patients with SCH and was not significantly different for preterm birth (<37, <32, and <28 weeks) and preeclampsia. The results may be because of the fact that our study was limited to cases of singleton ART pregnancies. In general, women undergoing infertility treatment appear to have a small but statistically significant increase risk for preterm birth, low birth weight, and severe maternal morbidity (such as preeclampsia, antepartum hemorrhage, transfusion, thrombotic embolism, and disseminated intravascular coagulation) [17,18,19]. Therefore, the background factors of ART pregnancy may have influenced these results. Limited data also suggest that in women undergoing IVF, cases with preconception TSH levels >2.5 mU/L may result in a lower gestational age at delivery and lower birth weight [12], but other pregnancy outcomes, such as the rate of preterm birth, the rate of FGR, preeclampsia, blood loss during delivery, and transfusion, may not have been examined. To the best of our knowledge, there are no other studies on the association between SCH and adverse outcomes in ART pregnancies, and we believe that this study provides new insights. In addition, the rate of preterm delivery at <34 weeks increased according to the TSH level, but was not significant in this study. The results are significantly interesting, but the limited number of cases did not allow for significant differences. Previous studies have reported that TSH levels correlate with preterm birth rates [11], but there are no high-quality data stratified by cutoff of the TSH level, presence of antithyroid antibodies, or treatment for SCH. Thus, future studies are required.
Screening for hypothyroidism in asymptomatic pregnant women during early pregnancy remains controversial. In prospective trials, even with universal screening for thyroid function, there was no improvement in pregnancy outcomes compared with a targeted or no screening group [20]. In a randomized trial, >4500 women in their first trimester of pregnancy participated. They were randomly assigned to either a universal screening group or a case-finding group [21]. Overall, the total number of adverse outcomes was similar between the case-finding and universal screening groups. However, secondary analysis revealed that low-risk women diagnosed with SCH and treated with thyroid hormone therapy in the universal screening group had 57% fewer adverse outcomes (preterm birth, preeclampsia, gestational diabetes, miscarriage) than did low-risk women diagnosed with SCH but not treated in the case finding group [21]. In addition, it has been suggested that universal screening may show higher cost-effectiveness [22,23]. As mentioned above, universal screening of thyroid function in pregnant women has its advantages and disadvantages, but the results of our study suggest that although limited to ART pregnancies, preconception screening and treatment for SCH may contribute to improved perinatal outcomes. In the future, universal screening for thyroid function and proper hormone therapy in pregnant women may contribute to reducing perinatal risks, including preterm birth.
There are no established criteria for the indications for SCH treatment in pregnant women. In a multicenter trial, 677 pregnant women with SCH (median TSH, 4.4 mU/L; free T4, normal) were randomized to levothyroxine therapy or placebo [24]. Levothyroxine treatment had no significant effect on maternal or fetal outcomes, such as preterm delivery, preeclampsia, gestational hypertension, and miscarriage, and there was no interaction effect with thyroid peroxidase (TPO) antibody positivity. In a meta-analysis of nine randomized controlled trials and 13 cohort studies, there was no benefit of SCH treatment on pregnancy outcomes [9]. However, evaluation of antithyroid antibody is also important in women diagnosed with SCH [4]. In a systematic review by the American Thyroid Association, regarding pregnancy-specific complications, although there is clearly a higher risk in TPO-positive women with TSH >2.5 mU/L, the risk was not constant in TPO-negative women, even at significantly higher TSH levels (>5–10 mU/L) [25]. In a trial of 131 TPO antibody-positive women diagnosed with SCH, levothyroxine replacement significantly reduced the rate of preterm delivery, especially in women with TSH ≥4 mU/L [26]. At present, it is uncertain whether thyroid hormone replacement therapy reduces perinatal risk in women with SCH. A recent meta-analysis suggested that high levels of TPO antibodies, even in euthyroid pregnant women, could adversely influence pregnancy outcomes after ART [27]. In contrast, euthyroid patients with TPO and/or antithyroglobulin antibodies showed no significant differences in pregnancy outcomes following fresh or frozen embryo transfer [28]. Therefore, the perinatal risk of antithyroid antibodies alone in euthyroid patients remains inconclusive. In the present study, we revealed that levothyroxine therapy could reduce the risk of preterm birth at <34 weeks among patients with SCH with TSH ≥2.5 mU/L. However, complete data on anti-TPO antibodies were not available; therefore, further studies are required in the future.
This study included cases of ART singleton pregnancies in which thyroid function screening was performed before fertility treatment. The SCH rate was higher in the infertile women than in the control women (healthy women with confirmed fertility) (13.9% vs. 3.9%) [29]. A recent study showed that pregnant women with singleton ART with a history of abortion or spontaneous abortion were more likely to have thyroid-related diseases [30]. In Japan, universal screening of thyroid function is commonly performed before fertility treatment. In addition, all patients in group C were already receiving appropriate levothyroxine therapy by an endocrinologist at the time of conception and were appropriately managed for SCH throughout their pregnancy. The strength of this study is that the patients’ backgrounds were well established. Second, because it is a single facility, pregnancy management and treatment policies are homogeneous, and a certain quality of care is maintained. Our institution follows the Guidelines for Obstetrical Practice in Japan and provides standardized care. The limitations of this study include the following: inclusion of only singleton data from ART pregnancies; the absence of data on placental abruption, neonatal respiratory distress syndrome, and/or pregnancy loss among adverse pregnancy outcomes; the absence of data on the prognosis of the child, such as respiratory disorders and cognitive function; and the absence of data on anti-TPO antibodies. Another limitation is that the criteria for levothyroxine therapy (groups B and C) in patients with SCH are unknown. Finally, the number of cases examined in this study was limited; therefore, it is possible that statistical differences could not be detected. This study has the following inherent limitations: limitations inherent to the study design, potential for selection bias, and the inability to generalize the findings to different populations. Therefore, large-scale studies are required in the future.
In conclusion, the rate of preterm birth at <34 weeks is significantly higher in patients with SCH; however, it is significantly lower in patients with SCH treated with levothyroxine therapy before and during pregnancy. Moreover, levothyroxine therapy is a significant protective factor against preterm birth at <34 weeks. These data provide valuable information for future clinical practice. Universal screening of thyroid function and proper hormone therapy in all pregnant women may reduce perinatal risks, including preterm birth. Further large-scale studies are warranted to estimate the perinatal risk of SCH, including data on antithyroid antibodies and the effects of levothyroxine therapy on perinatal risk, and to set cutoff values for appropriate therapeutic interventions.
Author Contributions
All authors contributed to the conception and design of this study. Material preparation, data collection, and analysis, Y.Narita, E.T., Y.Nakamura, M.S., Y.I., A.T., and T.A.; writing of the first draft of the manuscript, H.T.; and all authors commented on the previous versions of the manuscript. All the authors have read and approved the final version of the manuscript
Funding
This research was funded by the Japanese Red Cross Aichi Medical Center Nagoya Daiichi Hospital (Research Grant NFRCH 24-0008). The funding body had no role in the study design, data collection, analysis, interpretation, or the writing of the manuscript.
Institutional Review Board Statement
This study was conducted in accordance with the principles outlined in the 1964 Declaration of Helsinki. This study was approved by the Ethics Committee of the Japanese Red Cross Aichi Medical Center Nagoya Daiichi Hospital, Nagoya, Japan (approval number: 2023-070). Data were compiled and analyzed so that personal information could not be identified.
Informed Consent Statement
Patient informed consent was waived as this study used anonymous clinical data.
Data Availability Statement
The data in the manuscript will not be deposited. However, upon your request, we will submit data (deidentified participant data) that support the findings of this study.
Acknowledgments
We thank Editage (https://www.editage.com/) for the English language editing. We thank Atsushi Kubo for collecting data from the medical records.
Conflicts of Interest
The authors declare no conflict of interest. The authors alone are responsible for the content and writing of this manuscript.
References
- Kasagi, K.; Takahashi, N.; Inoue, G.; Honda, T.; Kawachi, Y.; Izumi, Y. Thyroid function in Japanese adults as assessed by a general health checkup system in relation with thyroid-related antibodies and other clinical parameters. Thyroid 2009, 19, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Allan, W.C.; Haddow, J.E.; Palomaki, G.E.; Williams, J.R.; Mitchell, M.L.; Hermos, R.J.; Faix, J.D.; Klein, R.Z. Maternal thyroid deficiency and pregnancy complications: implications for population screening. J. Med. Screen. 2000, 7, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Klein, R.Z.; Haddow, J.E.; Faix, J.D.; Brown, R.S.; Hermos, R.J.; Pulkkinen, A.; Mitchell, M.L. Prevalence of thyroid deficiency in pregnant women. Clin. Endocrinol. 1991, 35, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Shan, Z.; Li, C.; Mao, J.; Xie, X.; Wang, W.; Fan, C.; Wang, H.; Zhang, H.; Han, C.; et al. Maternal subclinical hypothyroidism, thyroid autoimmunity, and the risk of miscarriage: a prospective cohort study. Thyroid 2014, 24, 1642–1649. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Cabral, H.J.; Aschengrau, A.; Pearce, E.N. Associations between maternal thyroid function in pregnancy and obstetric and perinatal outcomes. J. Clin. Endocrinol. Metab. 2020, 105, e2015–e2023. [Google Scholar] [CrossRef] [PubMed]
- Toloza, F.J.K.; Derakhshan, A.; Männistö, T.; Bliddal, S.; Popova, P.V.; Carty, D.M.; Chen, L.; Taylor, P.; Mosso, L.; Oken, E.; et al. Association between maternal thyroid function and risk of gestational hypertension and pre-eclampsia: a systematic review and individual-participant data meta-analysis. Lancet Diabetes Endocrinol. 2022, 10, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Breathnach, F.M.; Donnelly, J.; Cooley, S.M.; Geary, M.; Malone, F.D. Subclinical hypothyroidism as a risk factor for placental abruption: evidence from a low-risk primigravid population. Aust. N.Z.J. Obstet. Gynaecol. 2013, 53, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Cleary-Goldman, J.; Malone, F.D.; Lambert-Messerlian, G.; Sullivan, L.; Canick, J.; Porter, T.F.; Luthy, D.; Gross, S.; Bianchi, D.W.; D’Alton, M.E. Maternal thyroid hypofunction and pregnancy outcome. Obstet. Gynecol. 2008, 112, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Jiao, X.F.; Zhang, M.; Chen, J.; Wei, Q.; Zeng, L.; Liu, D.; Zhang, C.; Li, H.; Zou, K.; Zhang, L.; et al. The impact of levothyroxine therapy on the pregnancy, neonatal and childhood outcomes of subclinical hypothyroidism during pregnancy: an updated systematic review, meta-analysis and trial sequential analysis. Front. Endocrinol. 2022, 13, 964084. [Google Scholar] [CrossRef]
- Consortium on Thyroid and Pregnancy—Study Group on Preterm Birth; Korevaar, T.I.M.; Derakhshan, A.; Taylor, P.N.; Meima, M.; Chen, L.; Bliddal, S.; Carty, D.M.; Meems, M.; Vaidya, B.; et al. Association of thyroid function test abnormalities and thyroid autoimmunity with preterm birth: A systematic review and meta-analysis. JAMA 2019, 322, 632–641. [Google Scholar] [CrossRef]
- Knøsgaard, L.; Andersen, S.; Hansen, A.B.; Vestergaard, P.; Andersen, S.L. Maternal hypothyroidism and adverse outcomes of pregnancy. Clin. Endocrinol. 2023, 98, 719–729. [Google Scholar] [CrossRef] [PubMed]
- Baker, V.L.; Rone, H.M.; Pasta, D.J.; Nelson, H.P.; Gvakharia, M.; Adamson, G.D. Correlation of thyroid stimulating hormone (TSH) level with pregnancy outcome in women undergoing in vitro fertilization. Am. J. Obstet. Gynecol. 2006, 194, 1668–1674. [Google Scholar] [CrossRef] [PubMed]
- Blatt, A.J.; Nakamoto, J.M.; Kaufman, H.W. National status of testing for hypothyroidism during pregnancy and postpartum. J. Clin. Endocrinol. Metab. 2012, 97, 777–784. [Google Scholar] [CrossRef]
- Vaidya, B.; Hubalewska-Dydejczyk, A.; Laurberg, P.; Negro, R.; Vermiglio, F.; Poppe, K. Treatment and screening of hypothyroidism in pregnancy: results of a European survey. Eur. J. Endocrinol. 2012, 166, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Matsubara, K.; Nakamoto, O.; Ushijima, J.; Ohkuchi, A.; Koide, K.; Makino, S.; Mimura, K.; Morikawa, M.; Naruse, K.; et al. Outline of the new definition and classification of “hypertensive disorders of pregnancy (HDP)”; a revised JSSHP statement of 2005. Hypertens. Res. Pregnancy 2018, 6, 33–37. [Google Scholar] [CrossRef]
- Yoshida, S.; Unno, N.; Kagawa, H.; Shinozuka, N.; Kozuma, S.; Taketani, Y. Prenatal detection of a high-risk group for intrauterine growth restriction based on sonographic fetal biometry. Int. J. Gynecol. Obstet. 2000, 68, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Jaques, A.M.; Amor, D.J.; Baker, H.W.G.; Healy, D.L.; Ukoumunne, O.C.; Breheny, S.; Garrett, C.; Halliday, J.L. Adverse obstetric and perinatal outcomes in subfertile women conceiving without assisted reproductive technologies. Fertil. Steril. 2010, 94, 2674–2679. [Google Scholar] [CrossRef] [PubMed]
- Declercq, E.; Luke, B.; Belanoff, C.; Cabral, H.; Diop, H.; Gopal, D.; Hoang, L.; Kotelchuck, M.; Stern, J.E.; Hornstein, M.D. Perinatal outcomes associated with assisted reproductive technology: the Massachusetts Outcomes Study of Assisted Reproductive Technologies (MOSART). Fertil. Steril. 2015, 103, 888–895. [Google Scholar] [CrossRef]
- Murugappan, G.; Li, S.; Lathi, R.B.; Baker, V.L.; Luke, B.; Eisenberg, M.L. Increased risk of severe maternal morbidity among infertile women: analysis of US claims data. Am. J. Obstet. Gynecol. 2020, 223, 404.e1–404.e20. [Google Scholar] [CrossRef]
- Lazarus, J.H.; Bestwick, J.P.; Channon, S.; Paradice, R.; Maina, A.; Rees, R.; Chiusano, E.; John, R.; Guaraldo, V.; George, L.M.; et al. Antenatal thyroid screening and childhood cognitive function. N. Engl. J. Med. 2012, 366, 493–501. [Google Scholar] [CrossRef]
- Negro, R.; Schwartz, A.; Gismondi, R.; Tinelli, A.; Mangieri, T.; Stagnaro-Green, A. Universal screening versus case finding for detection and treatment of thyroid hormonal dysfunction during pregnancy. J. Clin. Endocrinol. Metab. 2010, 95, 1699–1707. [Google Scholar] [CrossRef]
- Thung, S.F.; Funai, E.F.; Grobman, W.A. The cost-effectiveness of universal screening in pregnancy for subclinical hypothyroidism. Am. J. Obstet. Gynecol. 2009, 200, 267.e1–267.e7. [Google Scholar] [CrossRef] [PubMed]
- Dosiou, C.; Barnes, J.; Schwartz, A.; Negro, R.; Crapo, L.; Stagnaro-Green, A. Cost-effectiveness of universal and risk-based screening for autoimmune thyroid disease in pregnant women. J. Clin. Endocrinol. Metab. 2012, 97, 1536–1546. [Google Scholar] [CrossRef] [PubMed]
- Casey, B.M.; Thom, E.A.; Peaceman, A.M.; Varner, M.W.; Sorokin, Y.; Hirtz, D.G.; Reddy, U.M.; Wapner, R.J.; Thorp, J.M., Jr.; Saade, G.; et al. Treatment of subclinical hypothyroidism or hypothyroxinemia in pregnancy. N. Engl. J. Med. 2017, 376, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Alexander, E.K.; Pearce, E.N.; Brent, G.A.; Brown, R.S.; Chen, H.; Dosiou, C.; Grobman, W.A.; Laurberg, P.; Lazarus, J.H.; Mandel, S.J.; et al. 2017 Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid 2017, 27, 315–389. [Google Scholar] [CrossRef] [PubMed]
- Nazarpour, S.; Ramezani Tehrani, F.; Simbar, M.; Tohidi, M.; Alavi Majd, H.; Azizi, F. Effects of levothyroxine treatment on pregnancy outcomes in pregnant women with autoimmune thyroid disease. Eur. J. Endocrinol. 2017, 176, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Yang, M.; Li, T.; Yang, M.; Wang, W.; Chen, Y.; Ding, Y.; Liu, J.; Xu, X.; Zhang, J.; et al. High level of thyroid peroxidase antibodies as a detrimental risk of pregnancy outcomes in euthyroid women undergoing ART: A meta-analysis. Mol. Reprod. Dev. 2023, 90, 218–226. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Qiu, S.; Jiang, W.; Huang, Z.; Shi, H.; Du, S.; Sun, Y.; Zheng, B. Impact of thyroid autoimmunity on pregnancy outcomes in euthyroid women following fresh/frozen-thawed embryo transfer. Clin. Endocrinol. 2023, 99, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Abalovich, M.; Mitelberg, L.; Allami, C.; Gutierrez, S.; Alcaraz, G.; Otero, P.; Levalle, O. Subclinical hypothyroidism and thyroid autoimmunity in women with infertility. Gynecol. Endocrinol. 2007, 23, 279–283. [Google Scholar] [CrossRef]
- Sun, H.; Su, X.; Liu, Y.; Li, G.; Liu, X.; Du, Q. Association between abortion history and perinatal and neonatal outcomes of singleton pregnancies after assisted reproductive technology. J. Clin. Med. 2022, 12, 1. [Google Scholar] [CrossRef]
Figure 1.
Study flowchart of patient enrollment.
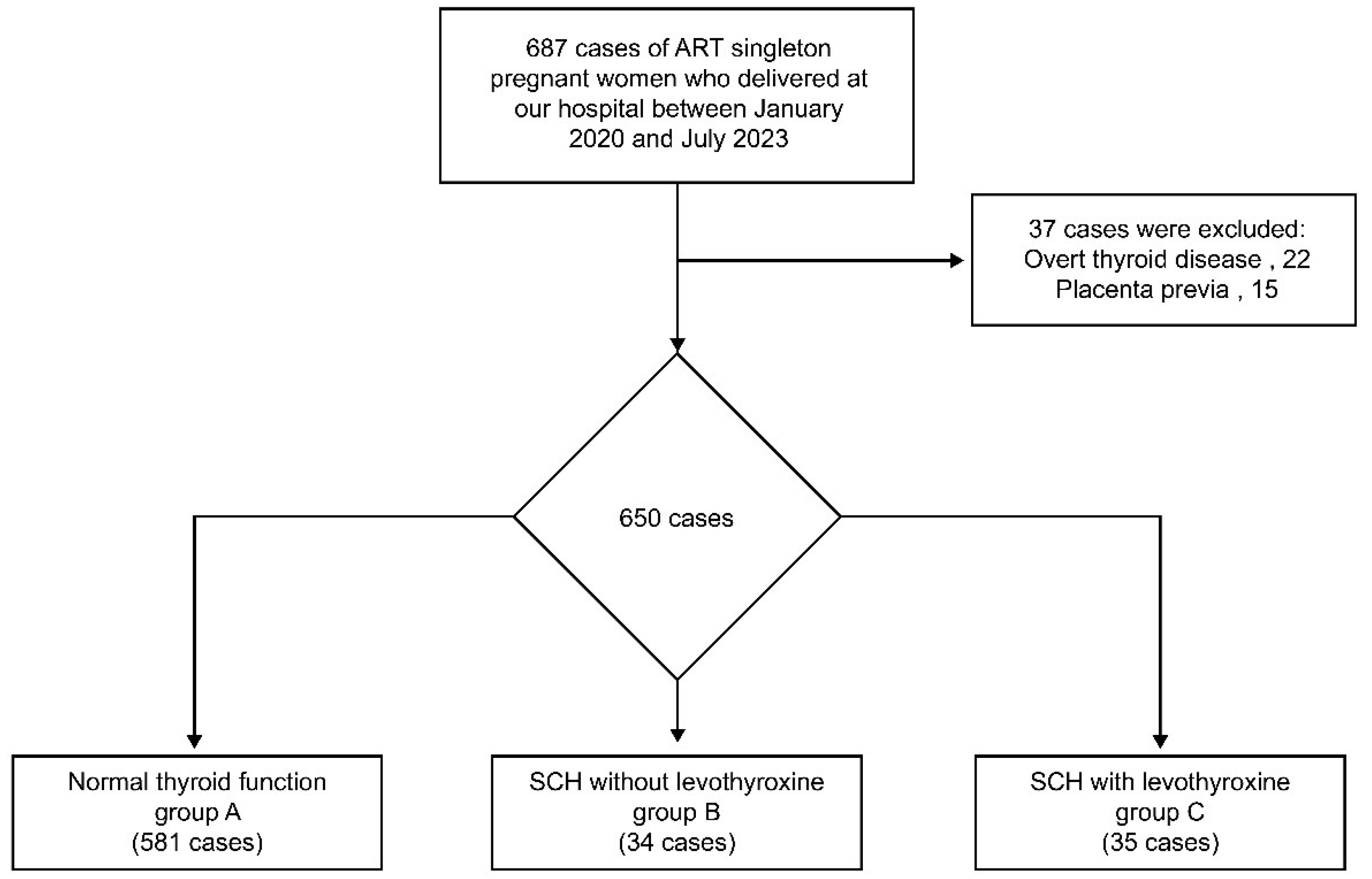

Table 1.
Maternal characteristics and perinatal outcomes of this study.
| Group A (n=581) | Group B (n=34) | Group C (n=35) | P-value | |
|---|---|---|---|---|
| Maternal age (years)* | 36.5 (±4.3) | 36.6 (±4.7) | 36.5 (±3.8) | 0.988 |
| Pre-pregnant BMI (kg/m2)* | 21.5 (±3.4) | 22.0 (±2.6) | 21.8 (±2.8) | 0.634 |
| History of abortion | 218/581 (37.5%) | 11/34 (32.4%) | 8/35 (22.9%) | 0.194 |
| Preterm birth at <37 weeks | 106/581 (18.2%) | 9/34 (26.5%) | 2/35 (5.7%) | 0.059 |
| Preterm birth at <34 weeks | 36/581 (6.2%) | 5/34 (14.7%) | 0/35 (0%) | 0.046 |
| Preterm birth at <32 weeks | 32/581 (5.5%) | 1/34 (2.9%) | 0/35 (0%) | 0.411 |
| Preterm birth at <28 weeks | 16/581 (2.8%) | 0/34 (0%) | 0/35 (0%) | 1 |
| Preeclampsia | 56/581 (9.6%) | 3/34 (8.8%) | 4/35 (11.4%) | 0.945 |
| Fetal growth restriction | 23/581 (4.0%) | 1/34 (2.9%) | 0/35 (0%) | 0.768 |
| Cesarean delivery | 272/581 (46.8%) | 15/34 (44.1%) | 19/34 (54.3%) | 0.641 |
| Blood loss at delivery (ml)* | 812 (±676) | 970 (±716) | 788 (±406) | 0.393 |
| Manual placental removal | 53/581 (9.1%) | 3/34 (8.8%) | 5/35 (14.3%) | 0.591 |
| Transfusion | 33/581 (5.7%) | 1/34 (2.9%) | 0/35 (0%) | 0.374 |
| Neonatal birth weight (g)* | 2901 (±1339) | 2819 (±640) | 3064 (±475) | 0.705 |
| TSH value (uIU/ml)* | 1.36 (±0.57) | 4.02 (±2.47) | 3.55 (±1.07) | <0.001 |
BMI, body mass index; TSH, thyroid-stimulating hormone. *Median (range).
Table 2.
Multivariate logistic regression analysis for preterm birth at <37 weeks.
| Adjusted OR | 95% CI | P-value | |
|---|---|---|---|
| Maternal age | 1.00 | 0.956–1.05 | 0.880 |
| Pre-pregnant BMI | 1.00 | 0.939–1.07 | 0.991 |
| Nulliparous | 0.95 | 0.602–1.50 | 0.822 |
| History of abortion | 0.97 | 0.621–1.52 | 0.899 |
| Preeclampsia | 4.98 | 2.81–8.81 | <0.001 |
| Fetal growth restriction | 3.31 | 1.31–8.34 | 0.011 |
| Levothyroxine therapy | 1.36 | 0.378–1.36 | 0.230 |
| TSH value | 1.05 | 0.485–2.29 | 0.895 |
BMI, body mass index; TSH, thyroid-stimulating hormone; OR, odds ratio; CI, confidence interval.
Table 3.
Multivariate logistic regression analysis for preterm birth at <34 weeks.
| Adjusted OR | 95% CI | P-value | |
|---|---|---|---|
| Maternal age | 1.00 | 0.926–1.07 | 0.915 |
| Pre-pregnant BMI | 1.03 | 0.942–1.13 | 0.506 |
| Nulliparous | 1.20 | 0.567–2.53 | 0.638 |
| History of abortion | 1.20 | 0.606–2.40 | 0.595 |
| Preeclampsia | 3.65 | 1.65–8.09 | 0.001 |
| Fetal growth restriction | 2.92 | 0.877–9.74 | 0.081 |
| Levothyroxine therapy | 0.117 | 0.015–0.948 | 0.044 |
| TSH value | 2.18 | 0.750–6.36 | 0.152 |
BMI, body mass index; TSH, thyroid-stimulating hormone; OR, odds ratio; CI, confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



