
Submitted:
29 July 2024
Posted:
30 July 2024
You are already at the latest version
Abstract
Gastric cancer (GC) is a major cause of cancer-related mortality worldwide, often associated with a bad prognosis because of its asymptomatic phenotype until advanced stages, highlighting the need for its prevention and early detection. GC development is preceded by gastric preneoplasia lesions (GPNL), namely atrophic gastritis (AG), intestinal metaplasia (IM), and dysplasia (DYS). GC is currently diagnosed by endoscopy, which is invasive and costly and has limited effectiveness for the detection of GPNL. Therefore, the discovery of non-invasive biomarkers in liquid biopsies, such as blood samples, to identify the presence of gastric preneoplasia and/or cancer lesions at an asymptomatic stage, is of paramount interest. This comprehensive review provides an overview of plasma/serum proteins recently identified and their diagnostic performance for the prediction of GPNL and early cancer lesions. Autoantibodies appear as promising biomarkers for AG, IM and early gastric cancer detection, along with inflammation and immunity-related proteins and antibodies against H. pylori virulence factors. There is a lack of specific protein biomarkers to detect DYS. Despite the need for further investigation and validation, some emerging candidates could pave the way to develop reliable, non-invasive diagnostic tests for the detection and prevention of GC.
Keywords:
liquid biopsy
; proteins
; plasma/serum
; atrophic gastritis
; intestinal metaplasia
; dysplasia
; early gastric cancer
; diagnosis
; prevention
1. Introduction
Gastric cancer (GC) is the fifth most common cancer and the fourth leading cause of cancer-related death worldwide (H. Sung et al. 2021). GC remains a serious public health problem, with a high mortality/incidence ratio (>0.8) in more than 70% of countries (Morgan et al. 2022). The highest incidence of GC is among Asian countries with more than 50% of the cases, followed by Central and Eastern Europe and South America. Cardia and non-cardia GC are distinguished, divided in three histological sub-groups, diffuse, intestinal-type and mixed, according to Lauren’s classification (Lauren 1965). While the incidence of non-cardia GC is highest among older populations (>50 years old), affecting twice more men than women, the incidence has steadily declined in this population over the last forty years. However, an increase of cases in younger populations (<50 years-old) has been observed, as reported in the US among non-Hispanic Whites and Hispanics, particularly in women (Anderson et al. 2018; Z. Wang, El-Serag, and Thrift 2021). A recent population-based modelling study predicts 1.8M new GC cases and 1.3M deaths by 2040, compared with 1.1M cases and 770,000 deaths in 2020 (Morgan et al. 2022). In most Western countries, GC is associated with a poor prognosis, mainly due to its late diagnosis. Importantly, countries with government-supported endoscopy screening programs, such as Japan and South Korea, reported low mortality-to-incidence ratios (0.43 and 0.35, respectively), highlighting the benefit of prevention (L. Shen et al. 2013; Bray et al. 2018). Population-wide endoscopy screening approaches in countries with intermediate or low incidence risk of GC are not cost-effective (Dan, So, and Yeoh 2006). In these countries, targeted endoscopic screening of high-risk individuals is the best approach to improve GC prevention. High-risk individuals are mainly related to a familial history of GC and Helicobacter pylori positive subjects. Indeed, the bacterium H. pylori which infects 4.4 billion people worldwide (Hooi et al. 2017), is recognized as a main risk factor for GC (Plummer et al. 2015). Therefore, screening and eradication of H. pylori infection have been proposed as a means to prevent GC. However, to be efficient, they need to occur as early as possible during the development of gastric preneoplasia lesions (GPNL) (Liou et al. 2020).
The most common GC subtype, intestinal type adenocarcinoma, results from the evolution of chronic inflammatory lesions, corresponding to non-atrophic gastritis (NAG) that evolves to atrophic gastritis (AG), with the development of intestinal metaplasia (IM) and dysplasia (DYS), preceding cancer lesions (Correa 1992). The progression of IM to GC is more likely in patients who develop DYS, with a pooled incidence rate of cancer of more than 12 cases per 10,000 person-years (Gawron et al. 2020). Depending on their extent and severity, identification of GPNL (AG, IM and DYS) during endoscopy should lead to a personalized monitoring to prevent GC (den Hollander et al. 2019; den Hoed et al. 2013; Pimentel-Nunes et al. 2019a). GPNL are commonly found in clinical practice and the European Society for Gastrointestinal Endoscopy has published specific monitoring recommendations (Pimentel-Nunes et al. 2019a). However, this surveillance in clinical practice remains imperfect, mainly due to the lack of clinical evidence in terms of patient benefit, and the absence of standardization of biopsy sampling methods and different analytical histology practices. In line with this, recent studies reported the absence of endoscopic detection of gastric lesions for 10 to 20% of patients, in the 6 to 36 months preceding the diagnosis of GC (Beck et al. 2021). In this context, non-invasive approaches to detect GPNL are therefore of paramount interest, especially for the screening of asymptomatic patients at risk of GC.
Liquid biopsy-based biomarkers discovery is a large field of investigation, initially focused on the diagnosis of adenocarcinomas (Matsuoka and Yashiro 2018). Biomarkers such as tumor cells, RNA, DNA, proteins and exosomes isolated from blood, urine, saliva or gastric juice have been proposed to predict the presence of gastric lesions (Leja and Linē 2021; Z.-B. Huang et al. 2021; Matsuzaki, Tsugawa, and Suzuki 2021). However, up to now, no candidates have emerged and successfully transferred from the bench phase to routine clinical practice.
Quantitative variation of the blood proteome reflects the general physiological state of cells and tissues. Circulating proteins have been proposed as a powerful tool for cancer screening, as previously reported with the CancerSeek test (Cohen et al. 2018). In this review, we discuss the histological characteristics of GPNL and early gastric cancer (EGC) lesions within the limits of their endoscopic detection, and present an overview of plasma/serum protein candidates identified over the period 2017-2024, and their diagnostic performance as listed in Table 1. Most of the candidates are related to EGC, highlighting the problematic lack in GPNL identification, mainly due to the challenge of their detection.
2. Detection of Gastric Pre-Neoplastic Lesions by Endoscopy
Typically, White-Light endoscopy detects only 53% of IM (Pimentel-Nunes et al. 2016). The endoscopy approach has been considerably refined with the improvement of technology, in particular with the development of virtual staining: Narrow Band Imaging (NBI) (Olympus, Japan), the ELUXEO™ system which allows switching between White-Light, Blue-Light Imaging (BLI) and Linked-Color Imaging (LCI) (Fujifilm, Japan), i-SCAN (Pentax, Japan) and optical zooms. For instance, it has been shown that with an appropriately experienced operator and sufficient examination time, second-generation NBI may detect almost every cases of extensive atrophy/IM without the need of biopsies (Lage et al. 2016).
In clinical practice, most endoscopists perform random biopsies, according to the updated Sydney system which recommends at least five samplings: two from the antrum, one from the incisura and two from the gastric body (Dixon et al. 1994). In order to standardize the histologic evaluation of GPNL, a score-grading of gastritis, referred to Operative Link on Gastritis Assessment (OLGA) has been proposed, and reliably identifies a subpopulation of patients (OLGA stages III-IV) at high risk of GC (Capelle et al. 2010a). However, OLGA relies on histological parameters of gastric atrophy, which suffer from low inter-observer reliability (Isajevs et al. 2014). Thus, the use of IM instead of AG has been recommended through the Operative Link on Gastric Intestinal Metaplasia (OLGIM) (Saka, Yagi, and Nimura 2015). Unlike OLGA, OLGIM score is associated with a high inter-observer agreement and classifies fewer patients as high risk III and IV (X. Wang et al. 2017; Capelle et al. 2010b). A recent prospective longitudinal and multicenter study carried out in Singapore on 2,980 patients followed up from 2004 to 2010, confirmed IM as a significant risk factor for EGC. Patients with OLGIM stages III-IV were at greater risk of GC, leading to their proposal to undergo endoscopic surveillance every two years (J. W. J. Lee et al. 2022).
As cited above, in low GC incidence countries the main issue is the absence of preventive screening programs, with only high-risk patients that can benefit from an endoscopy follow-up (Romańczyk et al. 2024). Asymptomatic patients with undetected GPNL will therefore escape “the surveillance radar”. These patients, for whom there is no prior indication for endoscopy surveillance, may be diagnosed too late at a symptomatic and advanced GC stage. In line with this, in 2019 in the US where the incidence of GC is low, it was estimated that 27,510 adults were diagnosed with 11,140 deaths observed (Thrift and El-Serag 2020; Siegel et al. 2023).
3. Emerging Serum/Plasma Protein Biomarkers for the Detection of Gastric Pre-Neoplasia and Early Cancer Lesions
3.1. Atrophic Gastritis (AG)
Compared to normal gastric mucosa, AG also referred as glandular atrophy, is defined as the loss of gastric glands, with or without metaplasia, in the setting of chronic inflammation (Figure 1A-a) (Shah et al. 2021). In the context of H. pylori infection, AG typically starts in the antrum and progressively spreads in the corpus following lesser gastric curvature (R. M. Genta 1998). Typical endoscopic features of AG include pale appearance of gastric mucosa, increased visibility of vasculature due to thinning of the gastric mucosa and loss of gastric folds (Figure 1A-b). Because these mucosal changes are often subtle, techniques to optimize the evaluation of the gastric mucosa such as virtual staining, are recommended. Histopathological evaluation of gastric biopsies is the gold standard for AG diagnosis (Dixon et al. 1994). However, it remains challenging with a poor reproducibility between pathologists for both diagnosis and assessment of the severity of lesions. Consequently, AG biomarkers are complex to identify.
3.1.1. Gastric Physiology-Related Biomarkers
AG affects the gastric corpus causing a reduction of pepsinogen (PG) secreted by parietal cells. Low PGI serum levels and PGI/PGII ratio can identify patients with advanced-stage AG (Zagari et al. 2017; Storskrubb et al. 2008), that require endoscopy, especially if their H. pylori serology is negative (Grozinsky-Glasberg et al. 2018). Based on blood sampling, in 2000′s, the combination of the serum level of PGI, PGII, Gastrin-17 (G-17) and anti-H. pylori IgG antibodies, was proposed as reliable to diagnose AG (Dong et al. 2019; Antico et al. 2012; Storskrubb et al. 2008), as recently reviewed (Romańczyk et al. 2024). The measure of these blood biomarkers estimated the global prevalence of AG between 23.9% and 27.0%, while for the same patients histological analysis gave a prevalence for AG of 31.6%-33.4% (Lahner et al. 2019). The corresponding test referred as GastroPanel®, allows evaluation of the capacity of corpus and antrum to produce acid and gastrin respectively, to estimate the inflammation of the gastric mucosa as well as the severity and location of AG. More recently, the diagnostic performance of GastroPanel® to detect AG was evaluated on 519 Finnish patients with dyspepsia, consulting for a gastroscopy (Koivurova et al. 2021). AG was detected in 53 patients (10.2%), with a concordance between serological data and the biopsy diagnosis of 92.4% (95% CI=90.0-94.6), and a weighted kappa of 0.86. Receiver operating characteristic (ROC) curve analysis for the prediction of moderate/severe AG in the corpus (AGC2+) gave area under the curve (AUC) values of 0.954 with a sensitivity (Se) of 92% and a specificity (Sp) of 98.8% for PGI (cut-off value of 30 ng/ml) and an AUC of 0.993 with Se of 100% and Sp 98.6% for PGI/PGII ratio (cut-off value of 3) (Table 1). In a French multicenter study on 344 patients at high risk of GC having a gastroscopy, 50% were detected for AG. GastroPanel® diagnostic performance showed a Se of only 39.9% (95% CI=31.9-48.2), with Sp of 93.4% (95% CI=88.9-96.4), a positive predictive value (PPV) of 81.9% (95% CI=71.1-90.0) and a negative predictive value (NPV) of 67.3 % (95% CI=61.4-72.8). Se was significantly higher to detect severe atrophy 60.8% (95% CI=46.1-74.6) and corpus AG (AGC) 61.0% (95% CI=49.2-72.0) but insufficient to detect either antral or corpus mild-atrophy (Chapelle et al. 2020). In that case, the diagnostic performance of GastroPanel® was not statistically different from PGI alone (Chapelle et al. 2020), and lower compared to the Finnish study (Koivurova et al. 2021). More recently, a French prospective multicenter study, using ChemiLuminescent Enzyme ImmunoAssay (CLEIA) has been reported on 356 patients undergoing upper endoscopy including: 91 with non-atrophic gastritis (NAG), 152 with AG and 113 subjects with normal mucosa (H). Sera were tested for PGI and PGII, in parallel with interleukin-6 (IL-6), human epididymal protein 4 (HE-4), adiponectin, ferritin and Krebs von den Lungen 6 (KL-6). In comparison to controls (H and NAG), for the detection of moderate to severe corpus AG (AGC2+/AGAC2+), the best Sp are observed at cut-off values for both PGI (≤20.2 ng/ml) and PGI/PGII (≤0.96), 95.6% and 98%, respectively (Table 1). Moreover, for the detection of moderate to severe antrum AG (AGA2+), PG alone was not sufficient with a level not significantly different compared to controls (H and NAG). Interestingly, IL-6 detects AG in the antrum (AGA2+) with a Se of 72.2% (95% CI=46.5-90.3). While the combination of PGI/PGII ratio with HE-4 showed a better Sp of 96.1% (95% CI=92.4-98.3), Se was only 40.7% (95% CI=27.6-55.0) for detection of moderate to severe AG at any stomach location (AG2+) (Chapelle et al. 2022). Thus, the diagnostic performance of PG testing is better to detect severe atrophy and corpus AG, but less efficient for detection of antral and corpus mild-atrophy.
The measure of PGI/PGII ratio has already been proposed in the 2000′s for the management of patients with low or high grade IM or DYS (Dinis-Ribeiro et al. 2004). A Malaysian study conducted on 72 patients (48 controls without chronic atrophic gastritis (H), 12 patients with chronic atrophic gastritis (CAG), 9 with IM and 3 with GC) analyzed Se and Sp of serum PGI, PGI/PGII ratio and G-17 to diagnose AG and IM (Loong et al. 2017). Patients with corpus CAG or IM had a lower PGI/PGII ratio compared with the controls group (7.2 vs 15.7, p<0.001). The severity of corpus AG and IM was correlated with the PGI/PGII ratio (r = -0.42, p<0.001) with an optimal cut-off of 10.0 (AUC=0.902 ; Se: 83.3% ; Sp: 77.9%), thus giving better diagnostic performance than the French cohort (Chapelle et al. 2022). These data support PGI/PGII ratio as specifically predictive for corpus CAG and IM, correlated with the type and severity of lesions, at least in Asian populations. More recently a retrospective Chinese study on EGC patients with low- or high-grade gastric intraepithelial neoplasia (GIN), proposed PGI and G-17 to differentiate GIN according to their grade of severity (Yanan et al. 2023).
3.1.2. Immunity and Related Autoantibodies
Parietal cell autoantibodies (PCAs) are primarily directed against the gastric proton pump H+/K+ ATPase (ATP4A and ATP4B). Anti-ATP4B autoantibodies (aAbs) are produced during autoimmune gastritis (AIG), induced by H. pylori infection, through molecular mimicry mechanism due to cross-reactivity between bacterial peptides and gastric H+/K+ ATPase (Amedei et al. 2003; D’Elios et al. 2004). The decrease of ATP4B has been associated with malignant transformation of the gastric mucosa and GC aggressiveness (Y. Pan et al. 2021). PCAs are prevalent in AG patients, thus reflecting atrophic damage to the oxyntic mucosa (Lahner et al. 2017; 2009). They are diagnostic markers for AIG and Biermer’s disease, characterized by the presence of AG (Rusak et al. 2016).
Luciferase ImmunoPrecipitation System (LIPS) is a technology that enables the detection of specific serum antibodies by immunoprecipitation of the corresponding luciferase reporter-tagged antigens. A prospective case-finding study on 218 patients who underwent gastric biopsies, reported the measurement of ATP4A and ATP4B aAbs by LIPS, concomitantly with the quantification of global PCAs and PGI serum levels by ELISA (Lahner et al. 2020). Histopathology classified 107 subjects in the group of AG in the corpus (AGC) (autoimmune 81.2%, and multifocal extensive 18.8%) and 111 in the control group (H). In AGC patients, ATP4A, ATP4B and PCAs titers were higher than in controls, whereas PGI serum level was reduced (p<0.0001). ROC-AUC analysis for ATP4A, ATP4B, PCAs and PGI to predict the presence of AGC, indicated Se of 75%, 77%, 69% and 73% with Sp of 88%, 88%, 91% and 80% respectively (Table 1). Thus, PCAs showed a higher Sp than PGI, highlighting their good performance to predict AGC. In combination with PGI, they should improve the AG diagnosis specially in the corpus.
AG precedes the development of IM (Figure 1B), a pivotal stage in the progression to GC. To assess the individual risk of evolution to cancer, it is mainly recommended to consider IM instead of atrophy (J. W. J. Lee et al. 2022; Pimentel-Nunes et al. 2019a), thus highlighting the need to further characterize IM specific biomarkers.
3.2. Intestinal Metaplasia (IM)
Gastric IM induces histological changes to the gastric glands, such that they acquire the characteristics of intestinal glands, with a brush border, and the presence of goblet and Paneth cells not usually present in the normal gastric mucosa (Figure 1A-c). Conventional White-Light endoscopy cannot accurately diagnose IM (Pimentel-Nunes et al. 2016). Virtual staining techniques are more sensitive, but may be limited due to significant inter-observer variability (R. J. Huang et al. 2019). Through NBI technology, IM are characterized by the presence of particular features, including tubulo-villous and irregular mucosal pattern, light blue crests, variable vascular density and white opaque fields as in Figure 1A-d (Kanemitsu et al. 2017). IM can be distinguished as complete (type I) and incomplete (type II-III). Incomplete IM are associated with a less differentiated phenotype and a higher grade of severity (Robert M. Genta et al. 2023). A large prospective longitudinal study indicated that, while the difference was not statistically significant, OLGIM stages II-IV patients with incomplete IM are at increased risk of EGC compared with complete IM (Hazard Ratio (HR) 5.96 ; 95% CI,=0.77-46.4 ; p=0.09) (J. W. J. Lee et al. 2022). Moreover, patients with IM (OLGIM III-IV) were at higher risk of GC within two years (adjusted-HR 20.7; 95% CI=5.04-85.6; p<0.01), compared to patients with OLGIM II also at significant risk of EGC (adjusted-HR 7.34; 95% CI=1.60-33.7; p=0.02). Importantly, the progression of IM to higher malignancy can take about 6 years, a period during which the diagnosis of IM and periodical surveillance are essential. A risk stratified approach has been proposed, recommending endoscopic surveillance for high- (OLGIM III-IV) and intermediate-risk (OLGIM II) patients within 2 and 5 years, respectively (J. W. J. Lee et al. 2022). These data further highlight the importance of liquid biopsy-based biomarker discovery to improve the detection/prevention of gastric cancer in these patients. In line with this, several serum protein candidates have emerged as listed in Table 1, including inflammation-related factors, autoantibodies and H. pylori antibodies.
3.2.1. Inflammation and Immunity-Related Proteins
Circulating serum levels of inflammatory mediators are a characteristic of tissue inflammation as associated with GPNL. They may reflect gastric tissue activity and are directly correlated with systemic regulation. Using Luminex® bead-based assays, the serum level of 28 immune- and inflammation-related markers was evaluated on 174 H. pylori-positive individuals, including 99 patients with IM or DYS and 75 controls with NAG (M. Song et al. 2019). Five biomarker candidates were identified: two C-C motif ligands (CCL) chemokines/macrophage inflammatory protein (MIP) (CCL3/MIP1A; CCL20/MIP3A) and interleukins IL-1ß, IL-4 and IL-5 (Figure 1B). As reported in Table 1, the association of the third tertile category with IM was similar for CCL3/MIP1A, IL-4 and IL-5, and lower for CCL20/MIP3A and IL-1β. The T-helper 2 (Th2) cytokines IL-4 and IL-5 showed a correlation of 0.5, allowing to distinguish NAG from IM. IL-1ß is one component of the Th17 immune response also involving IL-17A induced by H. pylori infection. Recently, higher serum IL-17 levels have been reported in H. pylori-infected patients with IM and DYS (n=45), compared to NAG patients (n=45) and healthy subjects (H) (n=45) (Della Bella et al. 2023). The ROC analysis for IL-17A showed AUC of 0.62 and 0.67 for IM/DYS vs NAG and H (Table 1) respectively, leading the authors to propose IL-17A as a potent biomarker to predict IM and/or DYS and to improve the prevention of GC.
C-reactive protein (CRP) plays an important role in inflammation. It is involved in the production of cytokines such as IL-6. Serum CRP level increases with the degree of inflammation in H. pylori-infected patients with chronic gastritis (Ishida et al. 2008). A study on patients with AG (GAG ; n=68), gastric IM (GIM ; n=98) and NAG (H ; n=70) as controls, investigated serum CRP levels (Kutluana et al. 2019). Both GIMG and GAG groups showed serum CRP levels 2.5-fold higher than controls. ROC analysis indicated an AUC of 0.77 with Se of 66.3% and Sp of 77.6%, to differentiate patients with IM and/or AG from those with chronic NAG (Table 1), with a CRP cut-off value ≥1.95 mg/l. In the same study, serum neopterin levels were also measured. Neopterin is a signaling pyrazino-pyrimidine compound defined as a biomarker of cellular immune response, with pre-diagnostic capacity in the development of CRC (Aleksandrova et al. 2015). As with CRP, neopterin serum levels are higher among H. pylori-positive patients. Pearson’s correlation analysis confirmed that high serum neopterin levels were positively correlated with the presence of AG and IM, with an AUC of 0.876 (Se: 93% ; Sp 76%), corresponding to neopterin cut-off value ≥10.15 nmole/l.
Also playing important roles in response to gastric mucosal injuries and inflammation are the Trefoil Factor Family (TFF) peptides, strongly expressed in mucus-producing cells. TFFs include three members involved in the defense and repair of the mucosa and in tumorigenesis (Aihara, Engevik, and Montrose 2017). The progressive loss of TFF1 and TFF2, along with the induction of TFF3, has long been thought to be involved at the early stages of gastric carcinogenesis (Leung et al. 2002). At the tissue level, TFF3 is normally absent from the pyloric mucosa, except in IM (Lavery et al. 2014). In a cross-sectional Latin American study on 288 patients diagnosed by gastric endoscopy (110 GIM ; 14 GC) and 164 H controls, slight but significantly higher median serum TFF3 levels were detected by ELISA in the GIM group (13.1 ng/ml) compared with controls (11.9 ng/ml) (p=0.024) (Latorre et al. 2022). Interestingly, increasing OLGIM stages are associated with higher levels of serum TFF3 (Rho coefficient = 0.124, p = 0.04). TFF3 diagnosis performance for GIM is characterized by AUC of only 0.58 (95% CI=0.51-0.65) with moderate Se and Sp of 55.5% and 58.5%, respectively. In order to identify serum biomarkers for high-risk OLGIM, a large prospective longitudinal multicenter cohort study of 2,980 patients was carried out in Singapore from 2004 to 2010 (J. W. J. Lee et al. 2022). GIM were diagnosed in 1,321 patients (44.3%) (OLGIM I n=906 ; OLGIM II-IV n=415). The serum level of TFF3, macrophage Migration Inhibitory Factor (MIF), a pleiotropic immunoregulatory cytokine, and PGI/PGII were measured. While MIF and PGI/PGII ratio decreased with increasing OLGIM, TFF3 increased and allowed the differentiation of OLGIM 0/II from OLGIM III/IV among H. pylori-negative patients (AUC=0.749 ; 95% CI=0.628-0.870; p<0.01), proving to be a more performant serum biomarker than PG, under these conditions. These data were confirmed by a Chinese cohort on nearly 4,000 patients, as was the association between TFF and the presence of GPNL (Zan et al. 2022). In this study, patients with IM (n=1,002) showed the highest concentration of serum TFF3 levels, with an odds ratio (OR) of 1.92 (Table 1). Not only TFF3, but also serum TFF1 and TFF2 levels increased progressively from CAG, IM, low grade dysplasia (LGD) to GC. Therefore, it seems that TFF3 performs better as a diagnostic marker in Latin American populations compared with Asian populations.
3.2.2. Immunity and Related Autoantibodies
Serum aAbs against tumor-associated antigens (TAAs) have been proposed as sensitive immunodiagnostic biomarkers, especially for the risk stratification of patients with premalignant lesions. A recombinant antigen microarray was developed to analyze the prevalence of aAbs directed against 102 TAAs, in large case-control cohorts from two independent Caucasian and Asian populations (Meistere et al. 2017). Thirteen and eight aAbs signatures were identified in the Caucasian and Asian cohorts respectively, allowing GC patients to be distinguished from H controls (Caucasian: Se 24% - Sp 91% ; Asian: Se 24% - Sp 93%). aAbs against cancer-testis antigen 2 (CTAG2), DEAD-box helicase 53 (DDX53) and an artificial peptide ID1625 were detected in both cohorts. These aAbs signatures were then investigated in the serum of 100 CAG and 775 IM Caucasian patients, according to the OLGIM score. Seroreactivity tends to increase with the increase of OLGIM score and was significantly higher in advanced/severe IM (OLGIM III/IV). GC-associated seroreactivity was detected in 13% of patients with advanced/severe IM (OLGIM III/IV) and increased in comparison with mild/moderate IM (5.3%) (OLGIM I/II), comparable with that seen in EGC patients (12%). Autoantibody reactivity against CTAG2 and DDX53 gave a similar response with stage I GC of intestinal type, indicating that both OLGIM III/IV and EGC patients have comparable aAbs responses. Interestingly, these data indicate that humoral immune response against TAAs is generated during the earliest stages of GPNLs, as a defense mechanism against cancer cell development.
3.2.3. Antimicrobial Defense
H. pylori infection is a major event at the origin of the development of IM (Correa 1992). Using Luminex®-based H. pylori multiplex serology (Michel et al. 2009), serum samples from 1,402 individuals of a Chinese high-risk GC population, including 412 patients with IM, 145 with DYS and 333 with undifferentiated DYS, were assayed for antibodies against 13 H. pylori recombinantly expressed fusion proteins (UreA, Catalase, GroEL, NapA, CagA, HP0231, VacA, HpaA, Cad, HyuA, Omp, HcpC and HP0305) (Epplein et al. 2018). Omp and HP0305 were found as the strongest markers of risk for the presence of GPNL with OR, 5.37 (95% CI=4.20-6.89) and OR, 3.85 (95% CI=3.04-4.88), respectively. Moreover, a classification model of GPNL that included age, smoking, and H. pylori seropositivity for Omp and HP0305 resulted in an AUC of 0.751 (95% CI=0.725-0.777) and OR, 7.43; (95% CI=5.59-9.88) (see Table 1), even better than the AUC value for the H. pylori oncoprotein CagA: 0.7184 (95% CI=0.68-0.74).
More recently, using H. pylori-nucleic acid programmable protein arrays (NAPPA), the humoral response to 1,528 H. pylori proteins was investigated comparing IM and NAG patients in discovery (n=50/group) and validation (n=100/group) cohorts. Among the 62 IgG and 11 IgA antibodies with more than 10% seropositivity in IM and/or NAG group, 12 IgG and 6 IgA showed relative higher seroprevalence in IM than in NAG cases, leading to the identification of a signature of 11 IgG with the best diagnostic performance to distinguish IM from NAG (AUC=0.81; 95% CI=0.75-0.87) (see Table 1). Anti-CagA, previously reported to positively correlate with the presence of IM (K.-F. Pan et al. 2014), gave AUC of 0.77 (95% CI=0.70-0.84), close to anti-Omp27 (AUC=0.73) (L. Song et al. 2023). As also previously reported (Epplein et al. 2018), this signature included H. pylori antibodies against outer membrane proteins (OMPs) and essential factors for bacterial survival and gastric colonization (Figure 1B).
3.3. Dysplasia (DYS)
Gastric DYS are associated with a high risk of synchronous carcinoma in other areas of the stomach (Carmack et al. 2009), found in up to 30% of patients with gastric DYS (Abraham et al. 2003). The World Health Organization (WHO) defines DYS as the presence of histologically unequivocal neoplastic epithelium without evidence of tissue invasion (Morson et al. 1980) and associated with gastric inflammation (Lewin 1998). Several DYS classification systems - including the Padova, Vienna, and WHO systems - have been developed to standardize the definition of gastric DYS and neoplasia between Western and Japanese pathologists. Two types of DYS have been described with gastric and intestinal immunophenotype associated with low- (Figures 1A-e and 1A-g) and high-grade (Figure 1A-f) of severity, respectively (Valente et al. 2015). Progression incidence from low- (LGD) and high-grade DYS (HGD) to carcinoma was reported as 2.8-11.5% and 10-68.8%, respectively. A nationwide cohort study in the Netherlands including patients previously detected for GPNLs identified in the Dutch nationwide histopathology registry (PALGA), indicated a 10 years GC risk in patients with mild-to-moderate DYS and severe DYS of 4% and 33%, respectively (de Vries et al. 2008). Due to higher risk of progression to carcinoma in HGD patients, endoscopic or surgical resection is recommended (Kim et al. 2020), while for LGD patients it is only recommended in the case of visible lesions (J. K. Sung 2016; Pimentel-Nunes et al. 2019b). Because of the rapid progression from HGD to gastric neoplasia, the detection of DYS is challenging. The sensitivity of White-Light endoscopy to detect DYS is 51-74% and can be further improved to 92% by magnifying endoscopy with NBI (Young, Philpott, and Singh 2021). Importantly, even after endoscopic resection (ER), long-term and periodical surveillance of gastric DYS is strongly recommended, highlighting the usefulness of non-invasive biomarkers for the follow-up of these patients.
Despite the fact that identification of liquid biopsy-based biomarkers is crucial to detect DYS, they have been investigated in only very few studies, likely due to their challenging diagnosis. As cited above, the serum level of IL-17A has been reported as an indicator of the presence of IM and DYS and a potential biomarker to predict GC development (Della Bella et al. 2023). IL-17A is induced by H. pylori, for which the presence of antibodies against its virulence factors OMP and HP0305 as serological biomarkers has been proposed, not only related to the presence of IM but also of DYS (Epplein et al. 2018). This short list, as illustrated in Figure 1B, highlights the special efforts required to improve the diagnosis and early detection of DYS, an essential requirement to reduce the global burden of GC.
3.4. Early Gastric Cancer (EGC)
EGC is defined as gastric carcinoma confined to the mucosa and/or submucosa (T1), irrespective of lymph node involvement (Figure 1A-h) (AJCC Cancer Staging Manual, n.d.; Zaanan et al. 2018; Espinel et al. 2015). When the tumor invades the muscularis propria (T2), it is classified as advanced GC (AGC†). The vessel plus surface (VS) endoscopic classification system has been described to differentiate cancerous and non-cancerous lesions using magnifying endoscopy (K. Yao, Anagnostopoulos, and Ragunath 2009). Its robustness to diagnose EGC is well validated (Ezoe et al. 2011; Kenshi Yao et al. 2014). VS classification evaluates the microvascular (MV) and micro surface (MS) patterns. The diagnostic criteria are 1) the presence of an irregular MV pattern with a demarcation line; 2) the presence of an irregular MS pattern with a demarcation line. Another criteria also to be considered is the absence of glands, with complete architectural loss of the mucosal and vascular pattern predicting neoplastic changes of the gastric mucosa (Figure 1A-i) (Pimentel-Nunes et al. 2019a). Lesions that meet at least one of these criteria are considered as cancerous, with Se of 97% (Miyaoka et al. 2020). This Japanese classification is not easily transposable to GC low-incidence countries, where endoscopic screening at population scale is not pertinent, virtual chromoendoscopy not systematically performed and magnification not always available.
In contrast to DYS, circulating plasma/serum proteins to diagnose EGC have been abundantly investigated, as indicated by the numerous biomarker candidates in the recent literature (Figure 1B). In the present review, only studies that clearly distinguish EGC from AGC† and that define diagnostic performance of the identified proteins have been considered.
3.4.1. Gastric Physiology-Related Proteins
Due to its role in gastric mucosal defense through the regulation of the NFkB signaling pathway and cytokine expression, Gastrokin 1 (GKN1) is a significant player in the GC process (Yoon et al. 2013). Serum GKN1 level measured by ELISA in 500 GC patients from South Korea, among which 140 had EGC and 360 had AGC†, was significantly lower compared to H controls (n=200). ROC analysis showed that a GKN1 cut-off value of 4.94 ng/ml clearly discriminated GC patients from controls with a high AUC of 0.995 (95% CI=0.9919-0.9988), Se of 91.2% and Sp of 96%. Moreover, serum GKN1 level was lower in AGC† than in EGC patients, allowing these patients to be distinguished from controls with the best AUC value of 1.0, Se of 79.3% and Sp of 96% for EGC and 95.8% and 96% respectively for AGC† (Table 1) (Yoon et al. 2019). Importantly, serum GKN1 concentrations measured in seven other types of cancer, including hepatocellular carcinoma (HCC), colorectal (CRC), breast (BRC), ovarian (OVC) and prostate (PRC) cancers, did not show significant differences compared with controls, supporting GKN1 as a potent, specific diagnostic biomarker for EGC and AGC†.
3.4.2. Inflammation and Immunity-Related Biomarkers
Interleukin-26 (IL-26) belonging to the IL-10 cytokine family is produced by Th17 cells. IL-26 regulates chronic inflammation processes and autoimmune disease (Gowhari Shabgah et al. 2022). The serum concentration of IL-26, CEA, CA19-9, CA125, CA72-4 and ferritin was measured by ELISA in 100 patients with benign gastric diseases and 302 GC patients, including stages I (n=75), II (n=73), III (n=125) and IV (n=29) (Xue et al. 2019). Serum IL-26, CEA, CA19-9, CA125, CA72-4 levels were positively correlated with the severity of gastric lesions, and were differentially significant among the 5 groups of patients (r=0.528, p<0.001 ; r=0.314, p<0.001 ; r=0.236, p=0.017 ; r=0.197, p=0.032 ; r=0.285, p<0.001, respectively). In contrast, ferritin is negatively correlated with the severity of GC lesions (r=-0.329 ; p=0.015).
Luminex bead-based assays were developed and used on a discovery cohort of 497 individuals (63 EGC, 113 AGC†, 117 atypical hyperplasia (AH) and 204 H controls), to measure serum CEA and CA72-4 levels in combination with serum IL-6, IL-8 and TNFa levels, leading to the proposal of a diagnostic model (J. Li et al. 2018). ROC analysis determined an AUC of 0.95 (95% CI=0.93-0.97) to discriminate between H and GC patients and 0.95 (95% CI=0.92-0.98) to discriminate between H and EGC or AGC† patients. Interestingly, the combination CA72-4, IL-6, IL-8 and TNFa gave better AUC values of 0.97 (95% CI=0.95-0.99), 0.98 (95% CI=0.96-0.99) and 0.96 (95% CI=0.94-0.98) to discriminate between AH and GC, EGC and AGC†, respectively (J. Li et al. 2018). A joint analysis performed on a validation cohort of 165 individuals (66 H, 41 AH, 19 EGC, 39 AGC†) confirmed that the proposed models discriminate EGC patients from H subjects, using the combination CEA+CA72-4+IL-6+IL-8+TNFa with Se: 84.21% and Sp: 90.91%, whilst the combination CA72-4+IL-6+IL-8+TNFa with Se: 78.95% and Sp: 85.37% discriminated EGC patients from patients with AH. Thus, the panel of these inflammatory mediators may provide a potent screening tool to detect EGC lesions (Figure 1B).
The Small Proline-Rich Protein 2A (SPRR2A) has been recently identified as a novel target for p73, a member of the p53 tumor suppressor family and may contribute to inflammation (Kong et al. 2021). The diagnostic performance of SPRR2A was investigated by ELISA in serum samples from 100 controls (H), 100 patients with chronic gastritis (CG ; 48 chronic superficial gastritis and 52 CAG), 200 with GC (I+II n=122 ; III+IV n=78), 40 with rectal cancer (RC) and 50 with colon cancer (CC) (Xu et al. 2020). The correlation between serum SPRR2A levels, GC clinical pathological parameters and ROC analysis was considered. The median serum SPRR2A concentration in GC patients was significantly higher than in controls and gastritis or CC patients (p<0.001). A cut-off value of 80.7 pg/ml yielded an AUC of 0.851 (95% CI=0.785-0.916 ; Se: 75.7% ; Sp: 74.5%) and 0.820 (95% CI=0.742-0.899 ; Se: 90.5% ; Sp: 61.7%), to discriminate GC patients from controls and from gastritis patients, respectively. However, for distinguishing GC patients at stage I and II from controls, the AUC for serum SPRR2A was a little bit lower: 0.78 (95% CI=0.669-0.891 ; Se: 69.6% ; Sp: 68.1%), indicating that SPRR2A is not among the best EGC biomarkers.
Most of the best-known serological cancer biomarkers are glycoproteins, such as CA19-9, CEA, CA15-3, CA79-9, also related to inflammation. Despite their current use in clinical oncology, their predictivity of EGC and/or GC lesions is low. Recent studies have further identified glycoprotein candidates to predict EGC, among which the glycoprotein inter-alpha-trypsin heavy chain 4 (ITIH4) belonging to the inter-alpha-trypsin inhibitor (ITI) family, shows significant high levels in cancer (Mir et al. 2015). ITIH4 is a type II acute phase protein involved in inflammatory host response to trauma, closely related to tumorigenesis and metastasis. Combining several methods (mass spectrometry, ELISA, western blot (WB), immunohistochemical staining), serum ITIH4 level was evaluated in a Chinese population cohort of 400 individuals. Patients presented lesions of chronic superficial gastritis (CSG) associated with H. pylori infection (Hpi ; n=37), low-grade intra-epithelial neoplasia (LGN) corresponding to the precancerous group (n=28), EGC (n=38), AGC† (n=70), and other system malignant tumors (OST) (n=49). H individuals (n=178) were also included as controls (Sun et al. 2021). For all cases, the diagnosis was confirmed via a combination of upper gastrointestinal endoscopy, magnifying endoscopy narrow-band imaging (ME-NBI), endoscopic ultrasonography and histopathology. Using mass spectrometry analysis, higher significant levels of ITIH4 were observed in serum samples from EGC patients compared to AGC† and H, with a high diagnostic performance corresponding to an AUC of 0.839 (95% CI=0.7393-0.9396) at a cut-off level of 171.2 ng/mL, with Se of 73.08% and Sp of 94.44% to discriminate EGC from controls.
Protein combinations allow higher diagnostic performance than single biomarkers. In a retrospective study based on the recruitment of 100 GC patients including 28 with EGC (TNM I-II stage), and 50 H individuals (Q. Shen et al. 2019), high-throughput protein detection technology, using multiplex proximity extension assays (PEA) identified over 300 proteins, and a signature of 19 serum proteins that together distinguish GC cases from controls. They included carcinoembryonic antigen-related cell adhesion molecule 5 (CEACAM5 or CEA), carbonic anhydrase 9 (CA9), mesothelin (MSLN), C-C motif chemokine 20 (CCL20), stem cell factor/KIT ligand (SCF), transforming growth factor alpha (TGF-a), matrix metalloproteinase-1 (MMP-1), matrix metalloproteinase-10 (MMP-10), insulin-like growth factor I (IGF-1), CUB domain-containing protein 1 (CDCP1), peptidyl-prolyl cis-trans isomerase A (PPIA), dimethylarginine dimethylaminohydrolase 1 (DDAH-1), heme oxygenase 1 (HMOX-1), friend leukemia integration 1 transcription factor (FLI1), IL-7, zinc finger and BTB domain-containing protein 17 (ZBTB-17), amyloid beta A4 precursor protein-binding family B member 1-interacting protein (APBB1IP), kazal-type serine protease inhibitor domain-containing protein (KAZALD-1) and a disintegrin and metalloproteinase with thrombospondin motifs 15 (ADAMTS-15). They are related to inflammation and/or immune response (IL-7, PPIA, HMOX-1, ZBTB-17, APBB11P, CCL20), metabolism and cellular physiology (CA9, IGF-1, DDAH-1, FLI1), cell cycle regulation (TGFa), cell adhesion (CEACAM5, MSLN, CDCP1), cell differentiation (SCF) and extracellular matrix (MMP-1, MMP-10, KAZALD, ADAMTS-15). Variation of each protein was analyzed by univariate analysis. Elastic-net logistic regression was performed to select serum proteins for the diagnostic model. Together, these proteins provided an increased diagnostic capacity to discriminate EGC patients at TNM I-II stage (AUC=0.99 ; Se: 89% ; Sp: 100%) from H controls, compared to each protein considered separately. The best diagnostic performance for a single protein of this panel is for MMP-1 with AUC of 0.75 and a Se of 68% and Sp of 78% (Shen et al. 2019).
As mentioned above, also related to the inflammatory process are TFFs, previously proposed to improve GC screening (Aikou et al. 2011). Using ELISA, Choi et al. measured the levels of TFF3 and cadherin 17 (CDH17) related to cell adhesion. As with TFF3, CDH17 is recognized as a tissue marker for IM (Matsusaka et al. 2016). The analysis was carried out on plasma samples from 111 GC patients and 44 H individuals. The GC group includes 42, 39, 27 and 3 cases related to TNM stages I, II, III and IV, respectively (Choi et al. 2017). Both plasma CDH17 and TFF3 levels were increased in GC patients compared to controls. TFF3 levels were significantly different between GC stage I (9.913±0.841 ng/ml) and H (6.195±0.702 ng/ml) (p=0.001) and CDH17 levels between GC stages II (0.578±0.091 ng/ml) and III (0.549±0.088 ng/ml) and H samples (0.329±0.060 ng/ml) (p=0.023 and 0.037, respectively). As reported in Table 1, ROC analysis to differentiate between GC stagesand controls, gave AUC for CDH17 (GC stages II-III) of 0.667 (p=0.003) with Se:77.3% and Sp: 61.4%, and for TFF3 (GC stage I) a higher AUC of 0.703 (p=0.001) with Se:83.3% and Sp: 54.5%, (Choi et al. 2017).
Haptoglobin (HPT) is one of the major acute phase glycoproteins, accounting for 0.4% to 2.6% of blood proteins. Aberrant glycosylation of HPT has been associated with chronic inflammation and cancer (Jeong et al. 2020). A targeted glycoproteomic platform using nanoliquid chromatography (LC)/quadrupole time-of flight (Q-TOF) mass spectrometry (MS) and MS/MS, combined with antibody-assisted purification, was set up to investigate specific glycan structures and the involvement of HPT glycosylation in GC (Lee et al., 2016, 2018). Sera from 15 H controls and 10 GC patients subdivided in two groups based on the TNM classification (stage I n=5 and stage III-IV n=5) were tested. After HPT pronase digestion, fingerprint glycopeptides (glycan moiety + small peptide tag) that represent each glycosite were quantitatively monitored for efficient tracking of site specific glycoform changes in HPT: HN dipeptide, NHSE tetrapeptide, NAT and HPN tripeptides that were selected as peptide tags for glycosites Asn-184, Asn-207, Asn-211, and Asn-241, respectively. The greatest magnitude of difference was observed at Asn-241, and the most significant difference was at Asn-211 where fucosylated complex-type glycans were found to be 9.6-fold and 4.2-fold more abundant in GC than in H (p=6.06×10-5 and p=2.2×10-7, respectively). Finally, based on ROC analyses (AUC=1 ; Se: 100% ; Sp: 100%), three fucosylated and/or sialylated complex-type glycans were identified as potential biomarkers: Hex6HexNAc5Fuc1NeuAc1 at Asn-211, Hex6HexNAc5Fuc1NeuAc1 at Asn-241 and Hex7HexNAc6Fuc1 at Asn-241. When testing only EGC, these three complex-type glycans still corresponded to AUC=1 (Lee et al. 2018). Although further investigations are required for these data to be confirmed, for example using larger cohorts and considering patients with GPNL, protein glycosylations constitute promising biomarkers to detect EGC.
Another example is thrombospondins (THBSs), belonging to Ca2+ binding glycoproteins, secreted from immune and mesenchymal cells, as well as endotheliocytes. Through interactions with a large range of proteins, THBSs are implicated in various biological procedures, including cell-to-cell and cell-to-matrix interaction, cell migration, blood vessels production, apoptosis, and cytoskeletal regulation. Serum THBS2 and CA19-9 levels were measured by ELISA on blood samples from 41 H individuals, 33 benign gastric tumor (BGT) and 46 EGC patients. The benign or EGC stages were confirmed according to the American Joint Committee on Cancer (AJCC) TNM (tumor–node–metastasis) classification (L. Li et al. 2021). The serum THBS2 level in EGC and BGT patients was upregulated dramatically compared to H individuals (p < 0.05), as was the level of CA19-9 (p<0.05). A significant correlation between THBS2 and CA19-9 serum levels was observed only in EGC patients (p=0.04), which showed a good capacity to distinguish EGC from H with AUC of 0.816 (95% CI=0.722–0.911) and 0.901 (95% CI=0.833–0.968), respectively. Furthermore, the combination of both enhanced their predictivity, with an individual index of AUC=0.951 (95% CI=0.912–0.989). Thus, THBS2 or CA19-9 are able to predict EGC as single biomarkers and their combination improved their diagnostic performance (Figure 1B).
In a Korean study including 60 GC patients (31 EGC and 29 AGC†) and 29 H controls, THBS1 with clusterin isoform 1, vitronectin and tyrosine-protein kinase SRMS were also identified as potent GC biomarkers by quantitative mass spectrometry (MS/MS) (Yoo et al. 2017). ROC analysis indicated AUC of 0.646, 0.878, 0.756, 0.887 for THBS1, clusterin isoform 1, vitronectin and tyrosine protein kinase SRMS respectively, for discrimination of EGC from controls. In the case of AGC†, the diagnostic accuracy is better for clusterin isoform 1 with AUC of 0.937 while AUC was 0.833, 0.856 and 0.656 for vitronectin, Tyrosine protein kinase SRMS and THBS1, respectively.
High-throughput proteomic technologies such as magnetic-bead-based purification and matrix-assisted laser desorption/ionization time-of-flight mass spectrometry have been applied to serum samples from 32 GC patients (both pre- and post-operatively) and 30 H volunteers, leading to the identification of 12 peptide candidates. Ten of the peptides corresponded to 6 proteins: isoform I of fibrinogen alpha chain precursor (FGA), alpha-2-HS-glycoprotein precursor (AHSG), apolipoprotein A-I precursor (APOA-I), hemoglobin subunit beta (HBB), cytoskeleton-associated protein 5 (CKAP5) and eukaryotic peptide chain release factor GTP-binding subunit ERF3B (GSPT2) (Shi et al. 2018). Based on these data, a validation cohort including 42 paired GC patients (pre- and post-operative samples) among which 16 and 26 were at stages I/II and III/IV respectively, 30 CRC and 30 HCC patients and 28 H volunteers, was used to evaluate the serum level of these candidates by ELISA. This study further confirmed the diagnostic accuracy of FGA, AHSG and APOA-1, with significant higher amounts detected specifically in GC patients versus H controls, with AUCs of 0.98 (95% CI=0.95-1.00), 0.93 (95% CI=0.87-0.99) and 0.83 (95% CI=0.73-0.93), respectively. Importantly, EGC and AGC stages could be distinguished, with significantly higher levels of FGA, AHSG and APOA-1 in GC stage I/II compared with H controls (Figure 1B), with AUCs of 0.98 (95% CI=0.96-1.01), 0.82 (95% CI= 0.69-0.95) and 0.96 (95% CI=0.91-1.01), respectively.
3.4.3. Immunity and Related Autoantibodies
Serum aAbs against tumor-associated antigens (TAAs), reported above as IM biomarkers, are also able to distinguish EGC patients (Meistere et al. 2017). In a case control study on 407 GC patients in the gastric adenocarcinoma group (GAC) (I n=67 ; II n=87 ; III n=142 ; IV n=40 ; unknown n=71) and 407 H controls, aAbs against 14 TAAs were measured by ELISA (Qin et al. 2019). A panel of 9 aAbs against TAAs including c-Myc, p16, HSPD1 (Heat Shock Protein Family D (Hsp60) Member 1), PTEN (Phosphatase and tensin homolog), p53, NPM1 (Nucleophosmin 1), ENO1 (Enolase 1), p62 and HCC1.4 was identified, and could distinguish GC cases from H controls with AUC of 0.857 (Se: 71.5% ; Sp: 71.3%). Interestingly, this panel also identified EGC cases (stages I/II) from H with AUC of 0.737 (Se: 64.9% ; Sp: 70.5%). The production of these aAbs could promote the risk of GC and GC aggressiveness, as their presence is associated with a worse prognosis.
Anti-p53 has also been reported as a potent EGC biomarker with 4 other aAbs against TAAs (Panel I: anti-COPB1, anti-GNAS, anti PBRM1, anti-ACVR1B or Panel II: anti-SMARCB1, anti-COPB1, anti-SRSF2, anti-GNAS), in a study on independent training (205 GAC and 205 H) and validation (126 GAC and 126 H) cohorts, according to an immunodiagnostic prediction model using logistic regression (LR) and Fisher linear discriminant analysis (LDA), respectively (Yang et al. 2020). For the training cohort, the diagnostic accuracy of these panels to distinguish EGC (stages I+II) led to AUC of 0.885 (Se: 66.7% ; Sp:94.6%) and 0.869 (Se: 74.7% ; Sp: 90.3%) for panels I and II, respectively. The analysis of the validation cohort showed higher Se of 76.7% but lower Sp of 83.3 to 80.9% for panels I and II, respectively.
Using serological proteome analysis (SERPA) associated with nanoliter-liquid chromatography combined with quadrupole time of flight tandem mass spectrometry (Nano-LC-Q-TOF-MS/MS), 7 aAbs corresponding to RAE1 (mRNA export factor 1), PGK1 (phosphoglycerate kinase 1), NPM1 (nucleophosmin 1), PRDX3 (thioredoxin-dependent peroxide reductase), UBE2N (ubiquitin-conjugating enzyme E2), ARF4 (ADP-ribosylation factor 4) and ANXA2 (annexin A2), have also been reported to identify patients with precancerous lesions (PL) and EGC (Zhu et al. 2023). The aAbs were tested on 364 serum samples from 242 patients (51 PL, 78 EGC, 113 AGC†) and 122 controls (H) for their ability to detect precancerous lesions and GC by ELISA. All of the aAbs were present at higher levels in patients with PL, EGC and AGC than H. Anti-RAE1 best discriminated GC patients at different stages, with AUC of 0.710 (95% CI=0.628-0.793), 0.745 (95% CI=0.678-0.811), and 0.804 (95% CI=0.750-0.858) for PL, EGC, and AGC†, respectively. AUC was also calculated for panels incorporating multiple aAbs, for PL, EGC, and AGC†, showing that a combination of 3 aAbs (RAE1, NPM1, and PGK1; Model 1) has a slightly increased AUC compared to RAE1 aAb alone. Two predictive models considering gender, RAE1, PGK1, NPM1, and ARF4 aAbs (Model 2 for PL) and age, gender, RAE1, PGK1, and NPM1 aAbs (Model 3 for EGC) improved diagnostic efficiency, with AUC of 0.803 (95% CI=0.736-0.860) and 0.857 (95% CI=0.800-0.902), Se of 66.7% and 75.6%, and Sp of 78.7% and 87.7%, respectively, which is higher than the diagnostic accuracy based on a single index.
3.4.4. Cellular Physiology and Metabolism Related Proteins
In a prospective multicenter study, the diagnostic performances of the secreted glycoprotein anosmin 1 (ANOS1), a component of the extracellular matrix, of the dihydropyrimidinase-like 3 (DPYSL3), a cell-adhesion molecule involved in metastasis and of MAGED2, related to the melanoma-associated antigen (MAGE) family involved in cancer development were evaluated. Sera from 66 H volunteers and 301 GC patients classified in four groups according to the criteria of the 7th edition of the Union for International Cancer Control (UICC): I n=225 (74%) ; II n=47 (16%) ; III n=26 (9%); and IV n=3 (1%), were collected (Kanda et al. 2020). The serum levels of ANOS1, DPYSL3 and MAGED2 were quantified by ELISA. ANOS1 showed the highest AUC value (0.7058) for discrimination of patients with GC from H. However, Se and Sp for ANOS1 were of 36% and 85%, respectively compared to 48% and 82% for DPYSL3, and to 28% and 92% for MAGED2. Among the 301 GC patients, the correlation coefficients of serum levels for ANOS1/DPYSL3, DPYSL3/MAGED2, and MAGED2/ANOS1 were 0.4698, 0.2318, and 0.5095 (p<0.0001), respectively, indicating modest correlation between each pair. When evaluating their capability to discriminate patients with GC stage I (n = 225) from H, the AUC values for ANOS1, DPYSL3, and MAGED2 were 0.7131, 0.5948, and 0.5113, respectively. The levels of ANOS1 were significantly elevated in patients with stage I GC compared with H controls (median 1,179 ng/ml and 461 ng/ml, respectively, p<0.0001), whereas they were equivalent in patients with GC stages I and II–IV.
Mammalian thioredoxin reductase (TrxR) is a selenium-containing oxidoreductase that catalyzes the NADPH-dependent reduction of thioredoxin (Trx) disulfide and participates in several redox-sensitive signaling cascades that mediate numerous physiological processes. Trx was highly expressed in various malignancies and cancers. In a Chinese study, the diagnostic efficacy of TrxR activity, measured, in vitro by 5, 5′-dithiobis (2-nitrobenzoic) acid (DTNB) reduction assay, was compared with the concentrations of well-known GC biomarkers analyzed by ElectroChemiLuminescence ImmunoAssay (ECLIA) (Peng et al. 2019). A total of 923 patients, including 131 with GC before clinical intervention (I n=25 ; II n=39 ; III n=46 ; IV n=21), 662 with GC after chemical drug treatment (I n=40 ; II n=148 ; III n=179 ; IV n=295) (staged according to the 8th IASLC/AJCC staging system) and 130 H controls were enrolled. The plasma TrxR activity [median (IQR)] in GC patients before clinical interventions [9.09 (7.96, 10.45) U/mL] were significantly higher (p<0.0001, Mann-Whitney U test) than in H controls [3.69 (2.38, 5.32) U/mL]. The critical value of TrxR activity for GC diagnosis was set at 7.34 U/mL with an AUC of 0.963 (95% CI=0.943-0.983 ; Se of 85.50% ; Sp of 97.69%). The combination of CEA, CA19-9 and CA72-4 exhibited an improved diagnosis efficacy for GC cases (AUC 0.834 ; 95% CI=0.778-0.891 ; Se: 78.41% ; Sp: 96.92%) relative to any individual biomarker (p<0.05). Notably, when adding TrxR activity to this panel, diagnostic performance for GC was further improved with an AUC of 0.982 (95% CI=0.970–0.993), Se 91.6% and Sp 94.62%. Consistent with previous studies, serum CEA, CA72-4 and CA19-9 levels remained slightly altered in phase I/II GC patients compared with H controls. Importantly, plasma TrxR activity in phase I/II GC patients were significantly higher than in H controls (p<0.0001), highlighting its high sensitivity and diagnostic performance (AUC>0.900) for EGC diagnosis.
Thus, a wide panel of biomarkers has been identified to distinguish EGC from H controls and from AGC (Figure 1B). Importantly, a panel of biomarkers is associated with a better diagnostic accuracy than any single biomarker, as supported by various studies (Shen et al. 2019) (Yang et al. 2020) (Zhu et al. 2023), reflecting the complexity of the mechanisms associated to the early steps of gastric carcinogenesis.
4. Discussion and Future Perspectives
GC is mostly associated with a bad prognosis due to its asymptomatic phenotype until reaching an advanced stage, thus highlighting the need for its primary prevention and early detection. The identification of blood biomarkers appears the most suited strategy to improve the screening of patients at risk of GC. This is crucial in the perspective of large-scale preventive strategies. Due to their accessibility, stability and easy quantification, blood proteins are a valuable source of biomarkers for diagnosis, prognosis, and monitoring of cancer. More than 100 United States Food and Drug Administration-cleared or – approved biomarkers are plasma proteins (Dayon, Cominetti, and Affolter 2022). Recent technical advances in protein analysis and omics technologies have been adapted, combining immunodetection-based assays such as ELISA, together with Luminex-based multiplex assays and antibody arrays coupled to mass spectrometry-based high-throughput methods, and have largely improved protein biomarker discovery. Importantly, most studies show that protein biomarker panels are more representative of the cellular physiology status and associated with a better diagnostic accuracy than a single candidate. The current challenge is to identify the most robust and promising combination, easily translatable for clinical use (Hartl et al. 2023). This requires a standardization of preanalytical handling of blood-based samples (Geyer et al. 2019) and statistical methods.
An important highlight of the present review is the lack of blood protein biomarkers to predict the presence of DYS. Apart from a few inflammation-related proteins (M. Song et al. 2019; Della Bella et al. 2023) and anti-H. pylori factors (Epplein et al. 2018), no specific candidates for low or high grade DYS have been reported. Due to the high GC risk associated to DYS, further studies and clinical trials should be developed to overcome this drastic shortcoming. As described previously, the fleeting nature of DYS makes their endoscopic detection and the identification of related biomarkers challenging. Future improvement of endoscopy technologies and omics global approaches coupled to multiplex technologies should overcome this gap.
Autoimmune gastritis has been proposed as a preneoplastic step associated with an annual incidence of GC of 0.3% (Toh 2014). Presence of PCAs in 20 to 30% of H. pylori-positive patients and of anti-H. pylori antibodies in AIG patients further support the link between H. pylori infection and AIG. An important highlight of this review is the identification of aAbs as promising biomarker candidates for AG, IM and EGC detection. Compared to PGI for detection of AG, aAbs showed better diagnostic performance (Lahner et al. 2020). Cancer cell-induced immunological responses can result in the production of aAbs against TAAs and are emerging as candidates to predict EGC lesions, for example as panels including aAbs against tumor suppressors such as p53, p16 or the oncogene cMyc (Qin et al. 2019) (Yang et al. 2020). Moreover, aAbs have been reported to distinguish late-stage IM in both Caucasian and Asian populations, for example the aAbs anti-CTAG2 and anti-DDX3 for GC stage I (Meistere et al. 2017). These variations in serum aAbs support the increasing evidence that immune dysregulation and autoimmunity impact the development of gastric neoplasia, as does H. pylori-induced autoimmune gastritis (Bizzaro, Antico, and Villalta 2018). Importantly, some recent epidemiological data suggest increasing incidence in some young patient groups possibly due to autoimmunity, and if this tendency is confirmed, it may change the epidemiology of GC in the future. In these cases, the main event inducing the gastric carcinogenesis process would not be H. pylori-induced chronic inflammation (Petryszyn, Chapelle, and Matysiak-Budnik 2020). In this hypothesis, aAbs could be more robust biomarkers, less impacted by the physiopathological primum movens.
Our review further confirms the robustness of long-known GPNL biomarkers. Loss of gastric glands that characterizes AG is associated with variation of serum PGI level and PGI/PGII ratio, which also correlates with the severity of AG and IM (Koivurova et al. 2021; Chapelle et al. 2022). Also related to inflammation, the measure of serum TFF3 in combination with PG has been proposed as an alternative to endoscopy for the early detection of gastric lesions. Data from studies in Singaporean (Lee et al. 2022), Chinese (Zan et al. 2022) and Chilean (Latorre et al. 2022) populations, confirmed TFF3 as a potent serum biomarker to identify patients with gastric IM, as well as to distinguish low (OLGIM 0-II) from high-grade (OLGIM III-IV) IM (Lee et al. 2022). However, the best diagnostic performance to detect IM is related to antimicrobial defense, as observed with a panel of 11 antibodies directed against H. pylori bacterial factors that discriminate IM vs NAG patients (L. Song et al. 2023). Although this panel is promising, it cannot be generalized to all populations as it does not take into account the difference in the immunogenic profile among race/ethnicity, and it also excludes patients previously eradicated for H. pylori or that never met the infection.
EGC biomarkers are the most investigated. In addition to serum aAbs, inflammation and immunity-related proteins are potent biomarkers to predict EGC lesions. High-throughput technologies led to the identification of promising panels with better diagnosis accuracy than as single protein, as illustrated by a signature of 19 proteins showing 100% Sp to distinguish GC (stages I and II) from H subjects, despite its characterization on a small size cohort (Shen et al. 2019). Related to inflammation, the combination of IL-6, IL-8, TNFa and CA72-4 led to the discrimination of EGC with one of the best diagnostic performances (J. Li et al. 2018), as also observed with THBS2 combined with CA19-9 (L. Li et al. 2021). CA19-9, CEA and CA72-4 are all serum tumor markers for diagnosis of GC (H. Wang et al. 2022). Their combination with the measure of Trx activity increases the diagnosis accuracy of each component of this panel to predict GC. It should be noted that the measure of Trx activity alone is associated with a Sp of 97% for discrimination of EGC stage I and II lesions from H subjects (Peng et al. 2019). Further validation on a larger scale, and multicentric cohorts issued from various populations, would be worthwhile to further validate this signature. Post-translational modifications (PTMs) such as protein glycosylation are also promising biomarkers (Lee et al., 2018), with the identification of three HPT fucosylated and/or sialylated complex-type glycans associated with 100% Se and Sp to predict EGC lesions. However, as for other studies, these PTMs were identified in a small size cohort and need further validation.
Together, these results show that subtle alterations in the gastric mucosa result in sufficient changes to be detected in blood. This can be explained by a) the sensitivity of detection techniques b) the specificity of the normal gastric mucosa cell types and derived compounds, since their modifications are easily detectable. An important parameter to take into account in future investigations is related to the distinct epidemiological, clinical and pathological characteristics between Asian and non-Asian populations. As the results of data obtained in Asian populations are not systematically transposable to non-Asian populations, these data must be interpreted with caution. Further analysis and validation studies with a special focus on patients from restricted geographical areas, such as our recent PREGASIGN prospective and multicentric study that aims to identify specific plasma protein biomarkers of GPNL and EGC in the French population (ClinicalTrials.gov Identifier: NCT05854368), are required, together with cohorts from populations of various geographic origins, before translation for clinical use. These studies could pave the way to the development of reliable non-invasive diagnostic tests that could be useful in the context of large-scale population screening.
Author Contributions
Conceptualization, T.B., K.N., D.L. and E.T.; methodology, K.N. and E.T.; formal analysis, all; writing-original draft preparation, T.B., K.N., and E.T.; writing-review and editing, T.B., K.N. and E.T.; providing histological images, C.J.; approved the submitted version: all. All authors have read and agreed to the published version of the manuscript.
Funding
The study was self-funded. No specific funding was obtained.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
We thank Richard Wheeler (Institut Pasteur, Paris, France) for reading the manuscript.
Conflicts of Interest
All the other authors: nothing to declare.
References
- Abraham, S.C.; Park, S.J.; Lee, J.-H.; Mugartegui, L.; Wu, T.-T. Genetic Alterations in Gastric Adenomas of Intestinal and Foveolar Phenotypes. Mod. Pathol. 2003, 16, 786–795. [Google Scholar] [CrossRef] [PubMed]
- Aihara, E.; Engevik, K.A.; Montrose, M.H. Trefoil Factor Peptides and Gastrointestinal Function. Annu. Rev. Physiol. 2017, 79, 357–380. [Google Scholar] [CrossRef]
- Aikou, S.; Ohmoto, Y.; Gunji, T.; Matsuhashi, N.; Ohtsu, H.; Miura, H.; Kubota, K.; Yamagata, Y.; Seto, Y.; Nakajima, A.; et al. Tests for Serum Levels of Trefoil Factor Family Proteins Can Improve Gastric Cancer Screening. Gastroenterology 2011, 141, 837–845. [Google Scholar] [CrossRef]
- AJCC Cancer Staging Manual. n.d. Accessed 15 March 2023. https://link.springer.com/book/9783319406176.
- Aleksandrova, K.; Chuang, S.-C.; Boeing, H.; Zuo, H.; Tell, G.S.; Pischon, T.; Jenab, M.; Bueno-De-Mesquita, B.; Vollset, S.E.; Midttun. ; et al. A Prospective Study of the Immune System Activation Biomarker Neopterin and Colorectal Cancer Risk. JNCI J. Natl. Cancer Inst. 2015, 107. [Google Scholar] [CrossRef]
- Amedei, A.; Bergman, M.P.; Appelmelk, B.J.; Azzurri, A.; Benagiano, M.; Tamburini, C.; van der Zee, R.; Telford, J.L.; Vandenbroucke-Grauls, C.M.; D'Elios, M.M.; et al. Molecular Mimicry between Helicobacter pylori Antigens and H+,K+–Adenosine Triphosphatase in Human Gastric Autoimmunity. J. Exp. Med. 2003, 198, 1147–1156. [Google Scholar] [CrossRef] [PubMed]
- Anderson, W.F.; Rabkin, C.S.; Turner, N.; Fraumeni, J.F.; Rosenberg, P.S.; Camargo, M.C. The Changing Face of Noncardia Gastric Cancer Incidence Among US Non-Hispanic Whites. JNCI J. Natl. Cancer Inst. 2018, 110, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Antico, A.; Tampoia, M.; Villalta, D.; Tonutti, E.; Tozzoli, R.; Bizzaro, N. Clinical Usefulness of the Serological Gastric Biopsy for the Diagnosis of Chronic Autoimmune Gastritis. J. Immunol. Res. 2012, 2012, 1–5. [Google Scholar] [CrossRef]
- Beck, M.; Bringeland, E.A.; Qvigstad, G.; Fossmark, R. Gastric Cancers Missed at Upper Endoscopy in Central Norway 2007 to 2016—A Population-Based Study. Cancers 2021, 13, 5628. [Google Scholar] [CrossRef] [PubMed]
- Bizzaro, N.; Antico, A.; Villalta, D. Autoimmunity and Gastric Cancer. Int. J. Mol. Sci. 2018, 19, 377. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Capelle, L.G.; de Vries, A.C.; Haringsma, J.; Ter Borg, F.; de Vries, R.A.; Bruno, M.J.; van Dekken, H.; Meijer, J.; van Grieken, N.C.; Kuipers, E.J. The staging of gastritis with the OLGA system by using intestinal metaplasia as an accurate alternative for atrophic gastritis. Gastrointest. Endosc. 2010, 71, 1150–1158. [Google Scholar] [CrossRef] [PubMed]
- Capelle, L.G.; de Vries, A.C.; Haringsma, J.; Ter Borg, F.; de Vries, R.A.; Bruno, M.J.; van Dekken, H.; Meijer, J.; van Grieken, N.C.; Kuipers, E.J. The staging of gastritis with the OLGA system by using intestinal metaplasia as an accurate alternative for atrophic gastritis. Gastrointest. Endosc. 2010, 71, 1150–1158. [Google Scholar] [CrossRef] [PubMed]
- Carmack, S.W.; Genta, R.M.; Graham, D.Y.; Lauwers, G.Y. Management of gastric polyps: a pathology-based guide for gastroenterologists. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Chapelle, N.; Osmola, M.; Martin, J.; Blin, J.; Leroy, M.; Jirka, I.; Moussata, D.; Lamarque, D.; Olivier, R.; Tougeron, D.; et al. Serum Pepsinogens Combined with New Biomarkers Testing Using Chemiluminescent Enzyme Immunoassay for Non-Invasive Diagnosis of Atrophic Gastritis: A Prospective, Multicenter Study. Diagnostics 2022, 12, 695. [Google Scholar] [CrossRef] [PubMed]
- Chapelle, N.; Petryszyn, P.; Blin, J.; Leroy, M.; Le Berre-Scoul, C.; Jirka, I.; Neunlist, M.; Moussata, D.; Lamarque, D.; Olivier, R.; et al. A panel of stomach-specific biomarkers (GastroPanel®) for the diagnosis of atrophic gastritis: A prospective, multicenter study in a low gastric cancer incidence area. Helicobacter 2020, 25, e12727. [Google Scholar] [CrossRef]
- Choi, B.; Lee, H.-J.; Min, J.; Choe, H.-N.; Choi, Y.-S.; Son, Y.-G.; Ahn, H.-S.; Suh, Y.-S.; Goldenring, J.R.; Yang, H.-K. Plasma expression of the intestinal metaplasia markers CDH17 and TFF3 in patients with gastric cancer. Cancer Biomarkers 2017, 19, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef] [PubMed]
- Correa, P. Human gastric carcinogenesis: a multistep and multifactorial process--First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention. . 1992, 52, 6735–40. [Google Scholar] [PubMed]
- Dan, Y.Y.; So, J.; Yeoh, K.G. Endoscopic Screening for Gastric Cancer. Clin. Gastroenterol. Hepatol. 2006, 4, 709–716. [Google Scholar] [CrossRef]
- Dayon, L.; Cominetti, O.; Affolter, M. Proteomics of human biological fluids for biomarker discoveries: technical advances and recent applications. Expert Rev. Proteom. 2022, 19, 131–151. [Google Scholar] [CrossRef]
- D'Elios, M.M.; Appelmelk, B.J.; Amedei, A.; Bergman, M.P.; Del Prete, G. Gastric autoimmunity: the role of Helicobacter pylori and molecular mimicry. Trends Mol. Med. 2004, 10, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Della Bella, C.; D’elios, S.; Coletta, S.; Benagiano, M.; Azzurri, A.; Cianchi, F.; de Bernard, M.; D’elios, M.M. Increased IL-17A Serum Levels and Gastric Th17 Cells in Helicobacter pylori-Infected Patients with Gastric Premalignant Lesions. Cancers 2023, 15, 1662. [Google Scholar] [CrossRef] [PubMed]
- Dinis-Ribeiro, M.; da Costa-Pereira, A.; Lopes, C.; Barbosa, J.; Guilherme, M.; Moreira-Dias, L.; Lomba-Viana, H.; Silva, R.; Abreu, N.; Lomba-Viana, R. Validity of Serum Pepsinogen I/II Ratio for the Diagnosis of Gastric Epithelial Dysplasia and Intestinal Metaplasia during the Follow-Up of Patients at Risk for Intestinal-Type Gastric Adenocarcinoma. Neoplasia 2004, 6, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Dixon, M.F., R. M. Genta, J.H. Yardley, and P. Correa. 1994. ‘Classification and Grading of Gastritis. The Updated Sydney System’. International Workshop on the Histopathology of Gastritis, Houston 20:1161–81.
- Dong, Z.; Zhang, X.; Chen, X.; Zhang, J. Significance of Serological Gastric Biopsy in Different Gastric Mucosal Lesions: an Observational Study. Clin. Lab. 2019, 65, 2141–2148. [Google Scholar] [CrossRef] [PubMed]
- Epplein, M.; Butt, J.; Zhang, Y.; Hendrix, L.H.; Abnet, C.C.; Murphy, G.; Zheng, W.; Shu, X.-O.; Tsugane, S.; Qiao, Y.-L.; et al. Validation of a Blood Biomarker for Identification of Individuals at High Risk for Gastric Cancer. Cancer Epidemiology Biomarkers Prev. 2018, 27, 1472–1479. [Google Scholar] [CrossRef] [PubMed]
- Espinel, J.; Uacute, J.; Espinel, E.P.S. Treatment modalities for early gastric cancer. World J. Gastrointest. Endosc. 2015, 7, 1062–1069. [Google Scholar] [CrossRef]
- Ezoe, Y.; Muto, M.; Uedo, N.; Doyama, H.; Yao, K.; Oda, I.; Kaneko, K.; Kawahara, Y.; Yokoi, C.; Sugiura, Y.; et al. Magnifying Narrowband Imaging Is More Accurate Than Conventional White-Light Imaging in Diagnosis of Gastric Mucosal Cancer. Gastroenterology 2011, 141, 2017–2025. [Google Scholar] [CrossRef] [PubMed]
- Gawron, A.J.; Shah, S.C.; Altayar, O.; Davitkov, P.; Morgan, D.; Turner, K.; Mustafa, R.A. AGA Technical Review on Gastric Intestinal Metaplasia—Natural History and Clinical Outcomes. Gastroenterology 2019, 158, 705–731. [Google Scholar] [CrossRef]
- Genta, R. M. 1998. ‘Review Article: Gastric Atrophy and Atrophic Gastritis--Nebulous Concepts in Search of a Definition’. Alimentary Pharmacology & Therapeutics 12 Suppl 1 (February):17–23.
- Genta, R.M.; Turner, K.O.; Robiou, C.; Singhal, A.; Rugge, M. Incomplete Intestinal Metaplasia Is Rare in Autoimmune Gastritis. Dig. Dis. 2023, 41, 369–376. [Google Scholar] [CrossRef]
- Shabgah, A.G.; Abdelbasset, W.K.; Rahman, H.S.; Bokov, D.O.; Suksatan, W.; Thangavelu, L.; Ahmadi, M.; Malekahmadi, M.; Gheibihayat, S.M.; Navashenaq, J.G. A comprehensive review of IL-26 to pave a new way for a profound understanding of the pathobiology of cancer, inflammatory diseases and infections. Immunology 2021, 165, 44–60. [Google Scholar] [CrossRef]
- Grozinsky-Glasberg, S.; Alexandraki, K.I.; Angelousi, A.; Chatzellis, E.; Sougioultzis, S.; Kaltsas, G. Gastric Carcinoids. Endocrinol. Metab. Clin. North Am. 2018, 47, 645–660. [Google Scholar] [CrossRef]
- Hartl, J.; Kurth, F.; Kappert, K.; Horst, D.; Mülleder, M.; Hartmann, G.; Ralser, M. Quantitative protein biomarker panels: a path to improved clinical practice through proteomics. EMBO Mol. Med. 2023, 15. [Google Scholar] [CrossRef]
- Hoed, C.M.D.; Holster, I.L.; Capelle, L.G.; de Vries, A.C.; Hartog, B.D.; ter Borg, F.; Biermann, K.; Kuipers, E.J. Follow-up of premalignant lesions in patients at risk for progression to gastric cancer. Endoscopy 2013, 45, 249–256. [Google Scholar] [CrossRef]
- Hollander, W.J.D.; Holster, I.L.; Hoed, C.M.D.; Capelle, L.G.; Tang, T.J.; Anten, M.-P.; Prytz-Berset, I.; Witteman, E.M.; ter Borg, F.; Hartog, G.D.; et al. Surveillance of premalignant gastric lesions: a multicentre prospective cohort study from low incidence regions. Gut 2018, 68, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Hooi, J.K.Y.; Lai, W.Y.; Ng, W.K.; Suen, M.M.Y.; Underwood, F.E.; Tanyingoh, D.; Malfertheiner, P.; Graham, D.Y.; Wong, V.W.S.; Wu, J.C.Y.; et al. Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 2017, 153, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.J.; Choi, A.Y.; Truong, C.D.; Yeh, M.M.; Hwang, J.H. Diagnosis and Management of Gastric Intestinal Metaplasia: Current Status and Future Directions. Gut Liver 2019, 13, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.-B.; Zhang, H.-T.; Yu, B.; Yu, D.-H. Cell-free DNA as a liquid biopsy for early detection of gastric cancer (Review). Oncol. Lett. 2020, 21, 1–1. [Google Scholar] [CrossRef]
- Isajevs, S.; Liepniece-Karele, I.; Janciauskas, D.; Moisejevs, G.; Putnins, V.; Funka, K.; Kikuste, I.; Vanags, A.; Tolmanis, I.; Leja, M. Gastritis staging: interobserver agreement by applying OLGA and OLGIM systems. Virchows Arch. 2014, 464, 403–407. [Google Scholar] [CrossRef]
- Ishida, Y.; Suzuki, K.; Taki, K.; Niwa, T.; Kurotsuchi, S.; Ando, H.; Iwase, A.; Nishio, K.; Wakai, K.; Ito, Y.; et al. Significant association between Helicobacter pylori infection and serum C-reactive protein. Int. J. Med Sci. 2008, 5, 224–229. [Google Scholar] [CrossRef]
- Jeong, S.; Oh, M.J.; Kim, U.; Lee, J.; Kim, J.-H.; An, H.J. Glycosylation of serum haptoglobin as a marker of gastric cancer: an overview for clinicians. Expert Rev. Proteom. 2020, 17, 109–117. [Google Scholar] [CrossRef]
- Kanda, M.; Suh, Y.-S.; Park, D.J.; Tanaka, C.; Ahn, S.-H.; Kong, S.-H.; Lee, H.-J.; Kobayashi, D.; Fujiwara, M.; Shimada, H.; et al. Serum levels of ANOS1 serve as a diagnostic biomarker of gastric cancer: a prospective multicenter observational study. Gastric Cancer 2019, 23, 203–211. [Google Scholar] [CrossRef]
- Kanemitsu, T.; Yao, K.; Nagahama, T.; Imamura, K.; Fujiwara, S.; Ueki, T.; Chuman, K.; Tanabe, H.; Atsuko, O.; Iwashita, A.; et al. Extending magnifying NBI diagnosis of intestinal metaplasia in the stomach: the white opaque substance marker. Endoscopy 2017, 49, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-I.; Park, J.Y.; Kim, B.J.; Hwang, H.W.; Hong, S.A.; Kim, J.G. Risk of metachronous gastric neoplasm occurrence during intermediate-term follow-up period after endoscopic submucosal dissection for gastric dysplasia. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Koivurova, O.-P.; Koskela, R.; Blomster, T.; Ala-Rämi, A.; Lumme, H.; Kettunen, O.; Hukkanen, J.; Karttunen, T.J.; Mäkinen, M.; Ronkainen, J.; et al. Serological Biomarker Panel in Diagnosis of Atrophic Gastritis andHelicobacter pyloriInfection in Gastroscopy Referral Patients: Clinical Validation of the New-Generation GastroPanel®Test. Anticancer. Res. 2021, 41, 5527–5537. [Google Scholar] [CrossRef] [PubMed]
- Kong, X.; Wang, D.; Sun, W.; Chen, M.; Chen, J.; Shi, J.; Zhang, J.; Chen, X. Small Proline-Rich Protein 2A and 2D Are Regulated by the RBM38-p73 Axis and Associated with p73-Dependent Suppression of Chronic Inflammation. Cancers 2021, 13, 2829. [Google Scholar] [CrossRef] [PubMed]
- Kutluana, U.; Kilciler, A.G.; Mizrak, S.; Dilli, U. Can neopterin be a useful immune biomarker for differentiating gastric intestinal metaplasia and gastric atrophy from non-atrophic non-metaplastic chronic gastritis? Gastroenterol. Y Hepatol. 2019, 42, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Lage, J.; Pimentel-Nunes, P.; Figueiredo, P.C.; Libanio, D.; Ribeiro, I.; Jacome, M.; Afonso, L.; Dinis-Ribeiro, M. Light-NBI to identify high-risk phenotypes for gastric adenocarcinoma: do we still need biopsies? Scand. J. Gastroenterol. 2015, 51, 501–506. [Google Scholar] [CrossRef]
- Lahner, E.; Brigatti, C.; Marzinotto, I.; Carabotti, M.; Scalese, G.; Davidson, H.W.; Wenzlau, J.M.; Bosi, E.; Piemonti, L.; Annibale, B.; et al. Luminescent Immunoprecipitation System (LIPS) for Detection of Autoantibodies Against ATP4A and ATP4B Subunits of Gastric Proton Pump H+,K+-ATPase in Atrophic Body Gastritis Patients. Clin. Transl. Gastroenterol. 2017, 8, e215. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Marzinotto, I.; Lampasona, V.; Dottori, L.; Bazzigaluppi, E.; Brigatti, C.; Secchi, M.; Piemonti, L.; Conti, L.; Pilozzi, E.; et al. Autoantibodies Toward ATP4A and ATP4B Subunits of Gastric Proton Pump H plus,K plus -ATPase Are Reliable Serological Pre-endoscopic Markers of Corpus Atrophic Gastritis. Clin. Transl. Gastroenterol. 2020, 11, e00240. [Google Scholar] [CrossRef]
- Lahner, E.; Norman, G.L.; Severi, C.; Encabo, S.; Shums, Z.; Vannella, L.; Fave, G.D.; Annibale, B. Reassessment of Intrinsic Factor and Parietal Cell Autoantibodies in Atrophic Gastritis With Respect to Cobalamin Deficiency. Am. J. Gastroenterol. 2009, 104, 2071–2079. [Google Scholar] [CrossRef]
- Lahner, E.; Zagari, R.M.; Zullo, A.; Di Sabatino, A.; Meggio, A.; Cesaro, P.; Lenti, M.V.; Annibale, B.; Corazza, G.R. Chronic atrophic gastritis: Natural history, diagnosis and therapeutic management. A position paper by the Italian Society of Hospital Gastroenterologists and Digestive Endoscopists [AIGO], the Italian Society of Digestive Endoscopy [SIED], the Italian Society of Gastroenterology [SIGE], and the Italian Society of Internal Medicine [SIMI]. Dig. Liver Dis. 2019, 51, 1621–1632. [Google Scholar] [CrossRef] [PubMed]
- Latorre, G.; Pizarro, M.; Ford, J.S.; Gándara, V.; Muñoz, G.; Araya, J.C.; Bellolio, E.; Villaseca, M.; Fuentes-López, E.; Cortés, P.; et al. Evaluation of trefoil factor 3 as a non-invasive biomarker of gastric intestinal metaplasia and gastric cancer in a high-risk population. Gastroenterol. Y Hepatol. 2023, 46, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Laurén, P. The Two Histological Main Types of Gastric Carcinoma: Diffuse and so-called Intestinal-Type Carcinoma. An Attempt at a Histo-Clinical Classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef] [PubMed]
- Lavery, D.L.; Nicholson, A.M.; Poulsom, R.; Jeffery, R.; Hussain, A.; Gay, L.J.; A Jankowski, J.; Zeki, S.S.; Barr, H.; Harrison, R.; et al. The stem cell organisation, and the proliferative and gene expression profile of Barrett's epithelium, replicates pyloric-type gastric glands. Gut 2014, 63, 1854–1863. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.J.; Zhu, F.; Srivastava, S.; Tsao, S.K.; Khor, C.; Ho, K.Y.; Fock, K.M.; Lim, W.C.; Ang, T.L.; Chow, W.C.; et al. Severity of gastric intestinal metaplasia predicts the risk of gastric cancer: a prospective multicentre cohort study (GCEP). Gut 2021, 71, 854–863. [Google Scholar] [CrossRef]
- Lee, J.; Hua, S.; Lee, S.H.; Oh, M.J.; Yun, J.; Kim, J.Y.; Kim, J.-H.; Kim, J.H.; An, H.J. Designation of fingerprint glycopeptides for targeted glycoproteomic analysis of serum haptoglobin: insights into gastric cancer biomarker discovery. Anal. Bioanal. Chem. 2018, 410, 1617–1629. [Google Scholar] [CrossRef] [PubMed]
- Leja, M.; Linē, A. Early detection of gastric cancer beyond endoscopy - new methods. Best Pr. Res. Clin. Gastroenterol. 2021, 50-51, 101731. [Google Scholar] [CrossRef] [PubMed]
- Leung, W.K.; Yu, J.; Chan, F.K.L.; To, K.F.; Chan, M.W.Y.; Ebert, M.P.A.; Ng, E.K.W.; Chung, S.C.S.; Malfertheiner, P.; Sung, J.J.Y. Expression of trefoil peptides (TFF1, TFF2, and TFF3) in gastric carcinomas, intestinal metaplasia, and non-neoplastic gastric tissues. J. Pathol. 2002, 197, 582–588. [Google Scholar] [CrossRef]
- Lewin, K.J. Nomenclature Problems of Gastrointestinal Epithelial Neoplasia. Am. J. Surg. Pathol. 1998, 22, 1043–1047. [Google Scholar] [CrossRef]
- Li, J.; Xu, L.; Run, Z.-C.; Feng, W.; Liu, W.; Zhang, P.-J.; Li, Z. Multiple cytokine profiling in serum for early detection of gastric cancer. World J. Gastroenterol. 2018, 24, 2269–2278. [Google Scholar] [CrossRef]
- Li, L.; Dong, J.; Fu, L.; Xia, X.; Pan, F.; Ning, Y. Clinical Value of Serum Thrombospondin-2 Combined with CA19-9 in Early Diagnosis of Gastric Cancer. J. Oncol. 2021, 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Liou, J.-M.; Malfertheiner, P.; Lee, Y.-C.; Sheu, B.-S.; Sugano, K.; Cheng, H.-C.; Yeoh, K.-G.; Hsu, P.-I.; Goh, K.-L.; Mahachai, V.; et al. Screening and eradication of Helicobacter pylori for gastric cancer prevention: the Taipei global consensus. Gut 2020, 69, 2093–2112. [Google Scholar] [CrossRef] [PubMed]
- Loong, T.H.; Soon, N.C.; Mahmud, N.R.K.N.; Naidu, J.; Rani, R.A.; Hamid, N.A.; Elias, M.H.; Rose, I.M.; Tamil, A.; Mokhtar, N.M.; et al. Serum pepsinogen and gastrin-17 as potential biomarkers for pre-malignant lesions in the gastric corpus. Biomed. Rep. 2017, 7, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, T.; Yashiro, M. Biomarkers of gastric cancer: Current topics and future perspective. World J. Gastroenterol. 2018, 24, 2818–2832. [Google Scholar] [CrossRef] [PubMed]
- Matsusaka, K.; Ushiku, T.; Urabe, M.; Fukuyo, M.; Abe, H.; Ishikawa, S.; Seto, Y.; Aburatani, H.; Hamakubo, T.; Kaneda, A.; et al. Coupling CDH17 and CLDN18 markers for comprehensive membrane-targeted detection of human gastric cancer. Oncotarget 2016, 7, 64168–64181. [Google Scholar] [CrossRef]
- Matsuzaki, J.; Tsugawa, H.; Suzuki, H. Precision Medicine Approaches to Prevent Gastric Cancer. Gut Liver 2021, 15, 3–12. [Google Scholar] [CrossRef]
- Meistere, I.; Werner, S.; Zayakin, P.; Siliņa, K.; Rulle, U.; Pismennaja, A.; Šantare, D.; Kikuste, I.; Isajevs, S.; Leja, M.; et al. The Prevalence of Cancer-Associated Autoantibodies in Patients with Gastric Cancer and Progressive Grades of Premalignant Lesions. Cancer Epidemiology Biomarkers Prev. 2017, 26, 1564–1574. [Google Scholar] [CrossRef] [PubMed]
- Michel, A.; Waterboer, T.; Kist, M.; Pawlita, M. Helicobacter pylori Multiplex Serology. Helicobacter 2009, 14, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Mir, S.A.; Rajagopalan, P.; Jain, A.P.; Khan, A.A.; Datta, K.; Mohan, S.V.; Lateef, S.S.; Sahasrabuddhe, N.; Somani, B.; Prasad, T.K.; et al. LC–MS-based serum metabolomic analysis reveals dysregulation of phosphatidylcholines in esophageal squamous cell carcinoma. J. Proteom. 2015, 127, 96–102. [Google Scholar] [CrossRef]
- Miyaoka, M.; Yao, K.; Tanabe, H.; Kanemitsu, T.; Otsu, K.; Imamura, K.; Ono, Y.; Ishikawa, S.; Yasaka, T.; Ueki, T.; et al. Diagnosis of early gastric cancer using image enhanced endoscopy: a systematic approach. Transl. Gastroenterol. Hepatol. 2020, 5, 50–50. [Google Scholar] [CrossRef]
- Morgan, E.; Arnold, M.; Camargo, M.C.; Gini, A.; Kunzmann, A.T.; Matsuda, T.; Meheus, F.; Verhoeven, R.H.; Vignat, J.; Laversanne, M.; et al. The current and future incidence and mortality of gastric cancer in 185 countries, 2020–40: A population-based modelling study. eClinicalMedicine 2022, 47, 101404. [Google Scholar] [CrossRef] [PubMed]
- Morson, B.C.; Sobin, L.H.; Grundmann, E.; Johansen, A.; Nagayo, T.; Serck-Hanssen, A. Precancerous conditions and epithelial dysplasia in the stomach. J. Clin. Pathol. 1980, 33, 711–721. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.; Formichella, L.; Zhang, L.; Zhang, Y.; Ma, J.; Li, Z.; Liu, C.; Wang, Y.; Goettner, G.; Ulm, K.; et al. Helicobacter pylori antibody responses and evolution of precancerous gastric lesions in a Chinese population. Int. J. Cancer 2013, 134, 2118–2125. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Wang, X.; He, Y.; Lin, S.; Zhu, M.; Li, Y.; Wang, J.; Wang, J.; Ma, X.; Xu, J.; et al. Tumor suppressor ATP4B serve as a promising biomarker for worsening of gastric atrophy and poor differentiation. Gastric Cancer 2021, 24, 314–326. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Zhou, Z.; Zhong, Y.; Sun, Y.; Wang, Y.; Zhu, Z.; Jiao, W.; Bai, M.; Sun, J.; Lu, J.; et al. Plasma activity of Thioredoxin Reductase as a Novel Biomarker in Gastric Cancer. Sci. Rep. 2019, 9, 1–11. [Google Scholar] [CrossRef]
- Petryszyn, P.; Chapelle, N.; Matysiak-Budnik, T. Gastric Cancer: Where Are We Heading? Dig. Dis. 2020, 38, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Pimentel-Nunes, P.; Libânio, D.; Lage, J.; Abrantes, D.; Coimbra, M.; Esposito, G.; Hormozdi, D.; Pepper, M.; Drasovean, S.; White, J.R.; et al. A multicenter prospective study of the real-time use of narrow-band imaging in the diagnosis of premalignant gastric conditions and lesions. Endoscopy 2016, 48, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Pimentel-Nunes, P.; Libânio, D.; Marcos-Pinto, R.; Areia, M.; Leja, M.; Esposito, G.; Garrido, M.; Kikuste, I.; Megraud, F.; Matysiak-Budnik, T.; et al. Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update 2019. Endoscopy 2019, 51, 365–388. [Google Scholar] [CrossRef]
- Pimentel-Nunes, P.; Libânio, D.; Marcos-Pinto, R.; Areia, M.; Leja, M.; Esposito, G.; Garrido, M.; Kikuste, I.; Megraud, F.; Matysiak-Budnik, T.; et al. Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update 2019. Endoscopy 2019, 51, 365–388. [Google Scholar] [CrossRef]
- Plummer, M.; Franceschi, S.; Vignat, J.; Forman, D.; de Martel, C. Global burden of gastric cancer attributable toHelicobacterpylori. Int. J. Cancer 2014, 136, 487–490. [Google Scholar] [CrossRef]
- Qin, J.; Wang, S.; Shi, J.; Ma, Y.; Wang, K.; Ye, H.; Zhang, X.; Wang, P.; Wang, X.; Song, C.; et al. Using recursive partitioning approach to select tumor-associated antigens in immunodiagnosis of gastric adenocarcinoma. Cancer Sci. 2019, 110, 1829–1841. [Google Scholar] [CrossRef] [PubMed]
- Romańczyk, M.; Osmola, M.; Link, A.; Druet, A.; Hémont, C.; Martin, J.; Chapelle, N.; Matysiak-Budnik, T. Non-Invasive Markers for the Detection of Gastric Precancerous Conditions. Cancers 2024, 16, 2254. [Google Scholar] [CrossRef]
- Rusak, E.; Chobot, A.; Krzywicka, A.; Wenzlau, J. Anti-parietal cell antibodies – diagnostic significance. Adv. Med Sci. 2016, 61, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Saka, A.; Yagi, K.; Nimura, S. OLGA- and OLGIM-based staging of gastritis using narrow-band imaging magnifying endoscopy. Dig. Endosc. 2015, 27, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.C.; Piazuelo, M.B.; Kuipers, E.J.; Li, D. AGA Clinical Practice Update on the Diagnosis and Management of Atrophic Gastritis: Expert Review. Gastroenterology 2021, 161, 1325–1332. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Shan, Y.-S.; Hu, H.-M.; Price, T.J.; Sirohi, B.; Yeh, K.-H.; Yang, Y.-H.; Sano, T.; Yang, H.-K.; Zhang, X.; et al. Management of gastric cancer in Asia: resource-stratified guidelines. Lancet Oncol. 2013, 14, e535–e547. [Google Scholar] [CrossRef]
- Shen, Q.; Polom, K.; Williams, C.; de Oliveira, F.M.S.; Guergova-Kuras, M.; Lisacek, F.; Karlsson, N.G.; Roviello, F.; Kamali-Moghaddam, M. A targeted proteomics approach reveals a serum protein signature as diagnostic biomarker for resectable gastric cancer. EBioMedicine 2019, 44, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Shi, F.; Wu, H.; Qu, K.; Sun, Q.; Li, F.; Shi, C.; Li, Y.; Xiong, X.; Qin, Q.; Yu, T.; et al. Identification of serum proteins AHSG, FGA and APOA-I as diagnostic biomarkers for gastric cancer. Clin. Proteom. 2018, 15, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA: A Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Song, L.; Song, M.; Rabkin, C.S.; Chung, Y.; Williams, S.; Torres, J.; Corvalan, A.H.; Gonzalez, R.; Bellolio, E.; Shome, M.; et al. Identification of anti-Helicobacter pylori antibody signatures in gastric intestinal metaplasia. J. Gastroenterol. 2022, 58, 112–124. [Google Scholar] [CrossRef]
- Song, M.; Rabkin, C.S.; Torres, J.; Kemp, T.J.; Zabaleta, J.; A Pinto, L.; Hildesheim, A.; Sánchez-Figueroa, L.; Guarner, J.; Herrera-Goepfert, R.; et al. Circulating inflammation-related markers and advanced gastric premalignant lesions. J. Gastroenterol. Hepatol. 2018, 34, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Storskrubb, T.; Aro, P.; Ronkainen, J.; Sipponen, P.; Nyhlin, H.; Talley, N.J.; Engstrand, L.; Stolte, M.; Vieth, M.; Walker, M.; et al. Serum biomarkers provide an accurate method for diagnosis of atrophic gastritis in a general population: The Kalixanda study. Scand. J. Gastroenterol. 2008, 43, 1448–1455. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Jin, J.; Jing, H.; Lu, Y.; Zhu, Q.; Shu, C.; Zhang, Q.; Jing, D. ITIH4 is a novel serum biomarker for early gastric cancer diagnosis. Clin. Chim. Acta 2021, 523, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.K. Diagnosis and management of gastric dysplasia. Korean J. Intern. Med. 2016, 31, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Thrift, A.P.; El-Serag, H.B. Burden of Gastric Cancer. Clin. Gastroenterol. Hepatol. 2019, 18, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Toh, B.-H. Diagnosis and classification of autoimmune gastritis. Autoimmun. Rev. 2014, 13, 459–462. [Google Scholar] [CrossRef]
- Valente, P.; Garrido, M.; Gullo, I.; Baldaia, H.; Marques, M.; Baldaque-Silva, F.; Lopes, J.; Carneiro, F. Epithelial dysplasia of the stomach with gastric immunophenotype shows features of biological aggressiveness. Gastric Cancer 2014, 18, 720–728. [Google Scholar] [CrossRef]
- de Vries, A.C.; van Grieken, N.C.; Looman, C.W.; Casparie, M.K.; de Vries, E.; Meijer, G.A.; Kuipers, E.J. Gastric Cancer Risk in Patients With Premalignant Gastric Lesions: A Nationwide Cohort Study in the Netherlands. Gastroenterology 2008, 134, 945–952. [Google Scholar] [CrossRef]
- Wang, H.; Jin, W.; Wan, C.; Zhu, C. Diagnostic value of combined detection of CA72-4, CA19-9, and carcinoembryonic antigen comparing to CA72-4 alone in gastric cancer: a systematic review and meta-analysis. Transl. Cancer Res. 2022, 11, 848–856. [Google Scholar] [CrossRef]
- Wang, X.; Lu, B.; Meng, L.; Fan, Y.; Zhang, S.; Li, M. The correlation between histological gastritis staging- ‘OLGA/OLGIM’ and serum pepsinogen test in assessment of gastric atrophy/intestinal metaplasia in China. Scand. J. Gastroenterol. 2017, 52, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; El-Serag, H.B.; Thrift, A.P. Increasing Incidence of Advanced Non-cardia Gastric Cancers Among Younger Hispanics in the USA. Dig. Dis. Sci. 2020, 66, 1669–1672. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Wei, S.; Chen, Y.; Yu, D.; Wang, X.; Dong, X. Serum Small Proline-Rich Protein 2A (SPRR2A) Is a Noninvasive Biomarker in Gastric Cancer. Dis. Markers 2020, 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Xue, T.; Yang, J.; Song, P.; Zhou, G. Investigation on correlations of serum IL-26 with diagnosis and staging of gastric cancer. . 2019, 24, 215–220. [Google Scholar]
- Yanan, Z.; Juan, W.; Xin, M.; Kejian, W.; Fangyu, W. Application of serum gastric function markers and digestive tumor indices to the diagnosis of early gastric cancer and precancerous lesions. SciVee 2023, 44, 795–800. [Google Scholar] [CrossRef]
- Yang, Q.; Qin, J.; Sun, G.; Qiu, C.; Jiang, D.; Ye, H.; Wang, X.; Dai, L.; Zhu, J.; Wang, P.; et al. Discovery and Validation of Serum Autoantibodies Against Tumor-Associated Antigens as Biomarkers in Gastric Adenocarcinoma Based on the Focused Protein Arrays. Clin. Transl. Gastroenterol. 2020, 12, e00284. [Google Scholar] [CrossRef] [PubMed]
- Yao, K.; Anagnostopoulos, G.; Ragunath, K. Magnifying endoscopy for diagnosing and delineating early gastric cancer. Endoscopy 2009, 41, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Yao, K.; Doyama, H.; Gotoda, T.; Ishikawa, H.; Nagahama, T.; Yokoi, C.; Oda, I.; Machida, H.; Uchita, K.; Tabuchi, M. Diagnostic performance and limitations of magnifying narrow-band imaging in screening endoscopy of early gastric cancer: a prospective multicenter feasibility study. Gastric Cancer 2014, 17, 669–679. [Google Scholar] [CrossRef] [PubMed]
- Yoo, M.; Park, J.; Han, H.; Yun, Y.; Kang, J.W.; Choi, D.; Lee, J.W.; Jung, J.H.; Lee, K.; Kim, K.P. Discovery of gastric cancer specific biomarkers by the application of serum proteomics. Proteomics 2017, 17. [Google Scholar] [CrossRef]
- Yoon, J.H.; La Cho, M.; Choi, Y.J.; Back, J.Y.; Park, M.K.; Lee, S.W.; Choi, B.J.; Ashktorab, H.; Smoot, D.T.; Nam, S.W.; et al. Gastrokine 1 regulates NF-κB signaling pathway and cytokine expression in gastric cancers. J. Cell. Biochem. 2013, 114, 1800–1809. [Google Scholar] [CrossRef]
- Yoon, J.H.; Park, Y.G.; Nam, S.W.; Park, W.S. The diagnostic value of serum gastrokine 1 (GKN1) protein in gastric cancer. Cancer Med. 2019, 8, 5507–5514. [Google Scholar] [CrossRef] [PubMed]
- Young, E.; Philpott, H.; Singh, R. Endoscopic diagnosis and treatment of gastric dysplasia and early cancer: Current evidence and what the future may hold. World J. Gastroenterol. 2021, 27, 5126–5151. [Google Scholar] [CrossRef] [PubMed]
- Zaanan, A.; Bouché, O.; Benhaim, L.; Buecher, B.; Chapelle, N.; Dubreuil, O.; Fares, N.; Granger, V.; Lefort, C.; Gagniere, J.; et al. Gastric cancer: French intergroup clinical practice guidelines for diagnosis, treatments and follow-up (SNFGE, FFCD, GERCOR, UNICANCER, SFCD, SFED, SFRO). Dig. Liver Dis. 2018, 50, 768–779. [Google Scholar] [CrossRef] [PubMed]
- Zagari, R.M.; Rabitti, S.; Greenwood, D.C.; Eusebi, L.H.; Vestito, A.; Bazzoli, F. Systematic review with meta-analysis: diagnostic performance of the combination of pepsinogen, gastrin-17 and anti-Helicobacter pylori antibodies serum assays for the diagnosis of atrophic gastritis. Aliment. Pharmacol. Ther. 2017, 46, 657–667. [Google Scholar] [CrossRef]
- Zan, X.; Chen, Z.; Guo, Q.; Zhang, Z.; Ji, R.; Zheng, Y.; Zhang, J.; Wu, Z.; Wang, X.; Ye, Y.; et al. The Association of Trefoil Factors with Gastric Cancer and Premalignant Lesions: A Cross-Sectional Population-Based Cohort Study. Cancer Epidemiology Biomarkers Prev. 2022, 31, 625–632. [Google Scholar] [CrossRef]
- Zhu, Q.; He, P.; Zheng, C.; Chen, Z.; Qi, S.; Zhou, D.; Li, Y.; Ouyang, Q.; Zi, H.; Tang, H.; et al. Identification and evaluation of novel serum autoantibody biomarkers for early diagnosis of gastric cancer and precancerous lesion. J. Cancer Res. Clin. Oncol. 2023, 149, 8369–8378. [Google Scholar] [CrossRef]
Figure 1.
A) Histologic and Endoscopic characteristics of gastric lesions during gastric carcinogenesis. Gastric histologic lesions obtained from gastric biopsies, H&E staining (a, c, e, f, h) and examination in NBI (b, d, g) and White Light (i), Olympus endoscopy without optical zoom. Lesions of gastric atrophy (a, b). a (17.4x): chronic follicular atrophic non-metaplastic gastritis (complete atrophy). b: glandular atrophy shows pale appearance of gastric mucosa (green arrow), increased visibility of vasculature due to thinning of the gastric mucosa (red arrows), and loss of gastric folds. Lesions of intestinal metaplasia (c, d). c (9.4x): chronic atrophic and metaplastic gastritis (severe atrophy, severe intestinal metaplasia). d: intestinal metaplasia (red arrows) in gastric corpus. Rounded to branched pit pattern, with mucosa slightly darker than adjacent mucosa. Green arrows show normal gastric corpus mucosa, with round pit pattern. Lesions of dysplasia (e, f, g). e (31.5x): low-grade dysplasia. f (31.3x): high-grade dysplasia. g: endoscopically visible low-grade dysplasia with central ulcer. Vessel disorganization (red arrows) and glandular disorganization (green arrows) are observed. Glandular atrophy (yellow arrows) surrounds the lesion. Lesions of early gastric cancer (h, i). h (3.8x): early gastric cancer (intramucosal, red arrow). i: early gastric cancer centered by an ulcer. Absent glands with complete architectural loss of the mucosal and vascular pattern. B) Plasma biomarkers identified at each step of the gastric cancer cascade. *Detailed in Table 1.
Figure 1.
A) Histologic and Endoscopic characteristics of gastric lesions during gastric carcinogenesis. Gastric histologic lesions obtained from gastric biopsies, H&E staining (a, c, e, f, h) and examination in NBI (b, d, g) and White Light (i), Olympus endoscopy without optical zoom. Lesions of gastric atrophy (a, b). a (17.4x): chronic follicular atrophic non-metaplastic gastritis (complete atrophy). b: glandular atrophy shows pale appearance of gastric mucosa (green arrow), increased visibility of vasculature due to thinning of the gastric mucosa (red arrows), and loss of gastric folds. Lesions of intestinal metaplasia (c, d). c (9.4x): chronic atrophic and metaplastic gastritis (severe atrophy, severe intestinal metaplasia). d: intestinal metaplasia (red arrows) in gastric corpus. Rounded to branched pit pattern, with mucosa slightly darker than adjacent mucosa. Green arrows show normal gastric corpus mucosa, with round pit pattern. Lesions of dysplasia (e, f, g). e (31.5x): low-grade dysplasia. f (31.3x): high-grade dysplasia. g: endoscopically visible low-grade dysplasia with central ulcer. Vessel disorganization (red arrows) and glandular disorganization (green arrows) are observed. Glandular atrophy (yellow arrows) surrounds the lesion. Lesions of early gastric cancer (h, i). h (3.8x): early gastric cancer (intramucosal, red arrow). i: early gastric cancer centered by an ulcer. Absent glands with complete architectural loss of the mucosal and vascular pattern. B) Plasma biomarkers identified at each step of the gastric cancer cascade. *Detailed in Table 1.
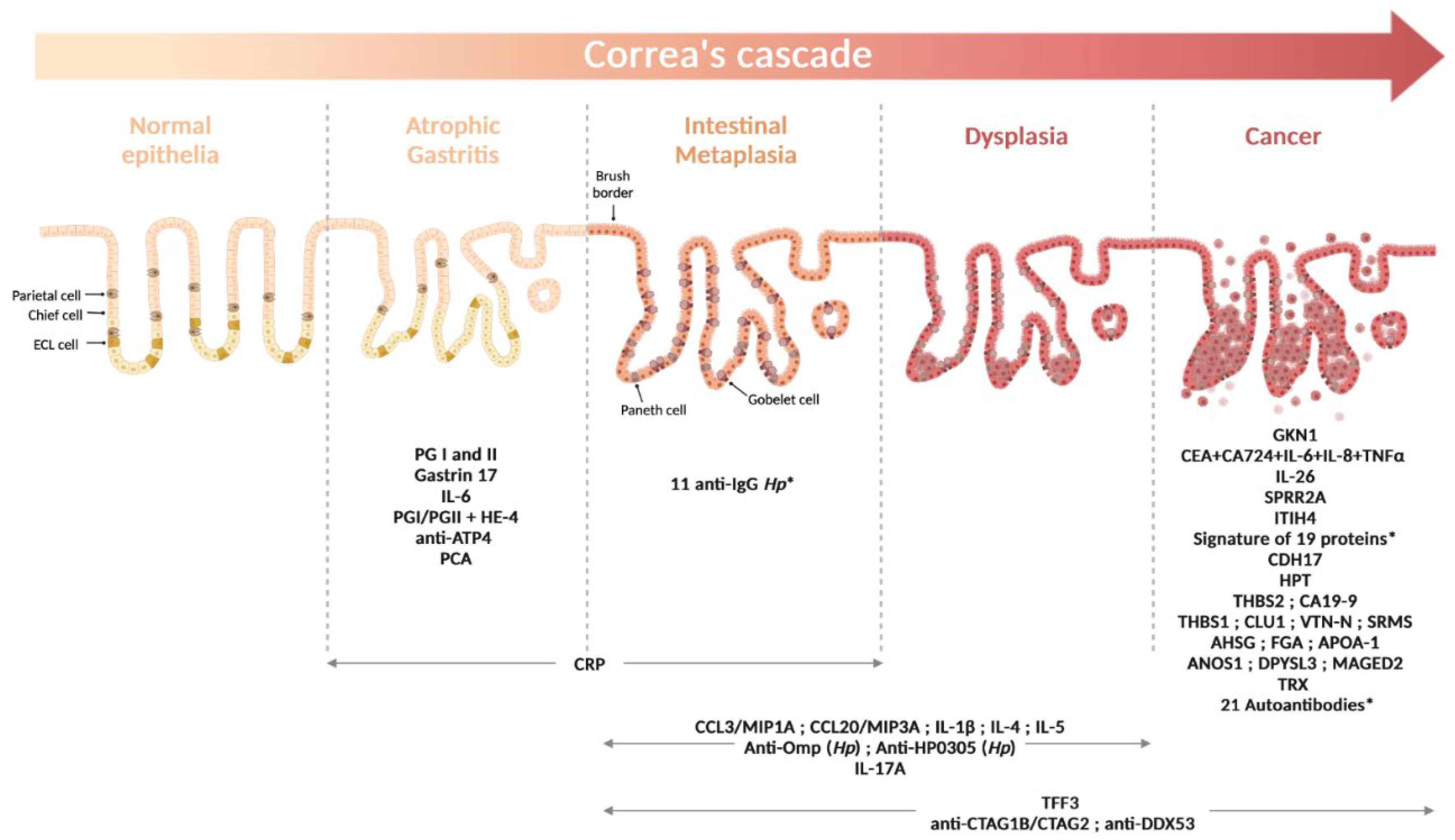

Table 1.
Diagnostic performance of the reported protein biomarkers, according to the type of gastric lesions.
Table 1.
Diagnostic performance of the reported protein biomarkers, according to the type of gastric lesions.
| Protein biomarker (cut-off values). | Studied cohort | Comparison conditions | AUC | Se % | Sp % | OR (95% CI) | Reference |
|---|---|---|---|---|---|---|---|
| Atrophic Gastritis (AG) | |||||||
| G-17 | 519 (446 H ; 35 Hp-gastritis ; 38 AG) | *AGA vs H | 0.402 | 10.7 | 69.5 | NA | Koivurova et al., 2021 |
| AGA2+ vs H | 0.429 | 15.4 | 70.4 | ||||
| PGI (15 ng/ml) | **AGC vs H | 0.777 | 55.6 | 99.8 | |||
| AGC2+ vs H | 0.878 | 76.0 | 99.6 | ||||
| PGI (30 ng/ml) | **AGC vs H | 0.858 | 72.2 | 99.4 | |||
| AGC2+ vs H | 0.954 | 92.0 | 98.8 | ||||
| PGI/PGII (3) | **AGC vs H | 0.885 | 77.8 | 99.2 | |||
| AGC2+ vs H | 0.993 | 100 | 98.6 | ||||
|
Gastropanel® : PGI/PGII ; G-17 ; Anti-Hp |
344 (196 H ; 148 AG) | AG vs H | NA | 39.9 | 93.4 | NA | Chapelle et al., 2020 |
| AGC vs H | 61.0 | 98.5 | |||||
| PGI (≤30 ng/ml) | 356 (113 H ; 91 NAG ; 152 AG) | AGC2+/AGAC2+ vs H/NAG | 0.856 | 77.8 | 83.8 | NA | Chapelle et al., 2022 |
| PGI (≤20.2 ng/ml) | AGC2+/AGAC2+ vs H/NAG | 0.856 | 77.8 | 95.6 | |||
| PGI/PGII (≤3) | AGC2+/AGAC2+ vs H/NAG | 0.859 | 75 | 92.6 | |||
| PGI/PGII (≤0.96) | AGC2+/AGAC2+ vs H/NAG | 0.859 | 72.2 | 98 | |||
| IL-6 | AGA2+ vs H/NAG | 0.588 | 72.2 | 41.2 | |||
| PGI/PGII + HE-4 | AG2+ vs H/NAG | 0.684 | 40.7 | 96.1 | |||
| PGI / PGII | 72 (48 H ; 12 CAG ; 9 IM ; 3 GC) | CAG/IM vs H | 0.902 | 83.3 | 77.9 | NA | Loong et al., 2017 |
| Anti-ATP4A | 218 (111 H ; 107 AGC) | AGC vs H | 0.826 | 75 | 88 | NA | Lahner et al., 2020 |
| Anti-ATP4B | 0.838 | 77 | 88 | ||||
| PCA | 0.805 | 69 | 91 | ||||
| PGI | 0.775 | 73 | 80 | ||||
| Intestinal Metaplasia (IM) | |||||||
| CCL3/MIP1A | 174 (75 NAG ; 95 IM ; 4 IM/DYS) | IM/DYS vs NAG | NA | NA | NA | 3.08 (1.23-7.68) p=0.027 |
Song et al., 2019 |
| CCL20/MIP3A | 2.69 (1.10-6.57) p=0.049 |
||||||
| IL-1ß | 2.39 (1.02-5.60) p=0.047 |
||||||
| IL-4 | 3.02 (1.29-7.12) p=0.009 |
||||||
| IL-5 | 3.07 (1.32-7.14) p=0.007 |
||||||
| IL-17A | 135 (45 H ; 45 NAG ; 45 IM/DYS) | IM/DYS vs NAG IM/DYS vs H NAG vs H |
0.62 | NA | NA | NA | Della Bella et al., 2023 |
| 0.67 | |||||||
| 0.64 | |||||||
| CRP (>1.95 mg/l) | 236 (70 H ; 68 GAG ; 98 GIMG) | GAG/GIMG vs H | 0.77 | 66.3 | 77.6 | NA | Kutluana et al., 2019 |
| TFF3 | 288 (164 H ; 110 GIM ; 14 GC) | GIM vs H | 0.58 | 55.5 | 58.5 | 1.2 (0.87-1.65) p=0.273 |
Latorre et al., 2022 |
| 2,980 (1,659 H ; 1,321 IM) | IM (OLGIM III-IV) vs IM (OLGIM 0-II) | 0.749 | NA | NA | NA | Lee et al., 2022 | |
| 3,986 (773 H ; 746 CAG ; 1,002 IM ; 1,334 LGD ; 131 GC) | IM vs H | NA | NA | NA | 1.92 (1.64-2.25) p<0.001 |
Zan et al., 2022 | |
| Anti-Omp | 1,402 (512 H ; 890 PGL) | PGL vs H | NA | NA | NA | 5.37 (4.20-6.89) p<0.0001 |
Epplein et al., 2018 |
| Anti-HP0305 | NA | 3.85 (3.04-4.88) p<0.0001 |
|||||
| Anti-Omp+Anti-HP0305 | 0.751 | 7.43 (5.59-9.88) p<0.001 |
|||||
| anti-HP1177/Omp27 |
Validation, 200 (100 NAG ; 100 IM) |
IM vs NAG | 0.73 | NA | NA | 8.08 ; p< 0.001 | Song et al., 2023 |
| anti-HP0547/CagA | 0.77 | 4.64 ; p< 0.001 | |||||
| anti-HP0596/Tipa | 0.66 | 3.97 ; p=0.002 | |||||
| anti-HP0103/TlpB | 0.68 | 3.83 ; p=0.001 | |||||
| anti-HP1125/PalA/Omp18 | 0.65 | 3.08 ; p=0.001 | |||||
| anti-HP0153/RecA | 0.55 | 0.48 ; p=0.030 | |||||
| anti-HP0385 | 0.57 | 0.41 ; p=0.006 | |||||
| anti-HP0243/NapA | 0.63 | 0.39 ; p=0.016 | |||||
| anti-HP0371/AccB /FabE | 0.65 | 0.37 ; p=0.017 | |||||
| anti-HP0900/HypB | 0.50 | 0.35 ; p= 0.048 | |||||
| anti-HP0709 | 0.61 | 0.30 ; p= 0.003 | |||||
| Panel of the 11 anti-HP | 0.81 | NA | |||||
| Early Gastric Cancer (EGC) | |||||||
| GKN1 (4.94 ng/ml) | 700 (200 H ; 140 EGC ; 360 AGC†) | GC vs H | 0.995 | 91.2 | 96 | NA | Yoon et al., 2019 |
| EGC vs H | 1.000 | 79.3 | 96 | ||||
| AGC† vs H | 1.000 | 95.8 | 96 | ||||
| CEA+CA724+IL-6+IL-8+TNFa | Discovery: 497 (204 H ; 117 AH ; 63 EGC ; 113 AGC†) | GC vs H | 0.95 | NA | NA | NA | Li et al., 2018 |
| EGC vs H | 0.95 | ||||||
| AGC† vs H | 0.95 | ||||||
| CA724+IL-6+IL-8+TNFa | GC vs AH | 0.97 | NA | NA | NA | ||
| EGC vs AH | 0.98 | ||||||
| AGC† vs AH | 0.96 | ||||||
| CEA+CA724+IL-6+IL-8+TNFa | Validation: 165 (66 H ; 41 AH ; 19 EGC ; 39 AGC†) | GC vs H | NA | 89.66 | 92.42 | NA | |
| EGC vs H | 84.21 | 90.91 | |||||
| AGC†vs H | 92.31 | 90.91 | |||||
| CA724+IL-6+IL-8+TNFa | GC vs AH | NA | 87.93 | 87.80 | NA | ||
| EGC vs AH | 78.95 | 85.37 | |||||
| AGC†vs AH | 92.31 | 90.24 | |||||
| SPRR2A (80.7 pg/ml) | 490 (100 H ; 100 CG ; 200 GC (I+II n=122, III+IV n=78) ; 40 RC ; 50 CC) | GC (I+II) vs H | 0.78 | 69.6 | 68.1 | NA | Xu et al., 2020 |
| ITIH4 (171.2 ng/ml) | 400 (178 H ; 37 Hpi ; 28 LGN ; 38 EGC ; 70 AGC† ; 49 OST) | EGC vs H | 0.8394 | 73.08 | 94.44 | NA | Sun et al., 2021 |
| Signature of 19 proteins: CEACAM5+CA9+MSLN+CCL20+SCF+TGFa+MMP-1+MMP-10 +IGF-1 +CDCP1+PPIA+DDAH-1 +HMOX-1 +FLI1+IL-7+ZBTB-17 +APBB1IP+KAZALD-1+ADAMTS-15 |
150 (50 H ; 100 GC (I n=8, II n=20, III n=57, IV n=14, missing n=1)) | GC (I+II) vs H | 0.99 | 89 | 100 | NA | Shen et al., 2019 |
| TFF3 | 155 (44 H ; 111 GC (I n=42, II n=39, III n=27, IV n=3)) | GC (I) vs H | 0.703 | 83.3 | 54.5 | NA | Choi et al., 2017 |
| CDH17 | GC (II+III) vs H | 0.667 | 77.3 | 61.4 | |||
|
HPT Asn-211: Hex6HexNAc5Fuc1NeuAc1 HPT Asn-241: Hex6HexNAc5Fuc1NeuAc1Hex7HexNAc6Fuc1 |
25 (15 H ; 10 GC (I n=5, III-IV n=5)) | GC (I) vs H | 1 | 100 | 100 | NA | Lee et al., 2018 |
| THBS2 | 120 (41 H ; 33 BGT ; 46 EGC) | EGC vs H | 0.816 | NA | NA | NA | Li et al., 2021 |
| EGC vs BGT | 0.840 | ||||||
| CA19-9 | EGC vs H | 0.901 | |||||
| EGC vs BGT | 0.847 | ||||||
| THBS2 / CA19-9 | EGC vs H | 0.951 | |||||
| EGC vs BGT | 0.928 | ||||||
| THBS1 | 89 (29 H ; 31 EGC ; 29 AGC†) | EGC vs H | 0.646 | NA | NA | NA | Yoo et al., 2017 |
| AGC† vs H | 0.656 | ||||||
| Clusterin isoform 1 | EGC vs H | 0.878 | |||||
| AGC† vs H | 0.937 | ||||||
| Vitronectin | EGC vs H | 0.756 | |||||
| AGC† vs H | 0.833 | ||||||
| Tyrosine protein kinase SRMS | EGC vs H | 0.887 | |||||
| AGC† vs H | 0.856 | ||||||
| AHSG | Validation: 130 (28 H ; 42 GC (I n=5, II n=11, III n=21, IV n=5) ; 30 CRC ; 30 HCC) | GC vs H | 0.93 | NA | NA | NA | Shi et al., 2018 |
| GC (I+II) vs H | 0.82 | ||||||
| FGA | GC vs H | 0.98 | |||||
| GC (I+II) vs H | 0.98 | ||||||
| APOA-1 | GC vs H | 0.83 | |||||
| GC (I+II) vs H | 0.96 | ||||||
| 9 TAA-panel: c-Myc+p16+HSPD1+PTEN+p53+NPM1+ ENO1+p62+HCC1.4 |
814 (407 H ; 407 GAC (I n=67, II n=87, III n=142, IV n=40, unknown n=71)) | GC vs H | 0.857 | 71.5 | 71.3 | NA | Qin et al., 2019 |
| GC (I+II) vs H | 0.737 | 64.9 | 70.5 | ||||
|
Training: 410 (205 H ; 205 GAC (I n=38, II n=42, III n=75, IV n=33 ; NA n=17)) Validation: 252 (126 H ; 126 GAC (I n=15, II n=15, III n=27, IV n=7 ; NA n=62)) |
GC (I+II) vs H | Yang et al., 2020 | |||||
| TAA-panel I: p53+COPB1+GNAS+PBRM1+ACVR1B |
|||||||
| Panel I, | |||||||
| Training | 0.885 | 66.7 | 94.6 | NA | |||
| Validation | 0.821 | 76.7 | 83.3 | ||||
| TAA-panel II: p53+SMARCB1+COPB1+SRSF2+GNAS |
|||||||
| Panel II, | |||||||
| Training | 0.869 | 74.7 | 90.3 | NA | |||
| Validation | 0.876 | 76.7 | 80.9 | ||||
| RAE1 aAbs | 364 (122 H ; 51 PL ; 78 EGC ; 113 AGC†) | EGC vs H | 0.745 | 94.9 | 47.1 | NA | Zhu et al., 2023 |
| PGK1 aAbs | 0.648 | 41 | 87.6 | ||||
| NPM1 aAbs | 0.611 | 20.5 | 100 | ||||
| PRDX3 aAbs | 0.613 | 88.5 | 65.2 | ||||
| UBE2N aAbs | 0.585 | 24.4 | 95 | ||||
| ARF4 aAbs | 0.488 | 11.5 | 98.3 | ||||
| ANXA2 aAbs | 0.563 | 19 | 86.9 | ||||
| ANOS1 | 367 (66 H ; 301 GC (I n=225, II n=47, III n=26, IV n=3)) | GC vs H | 0.7058 | 36 | 85 | NA | Kanda et al., 2020 |
| GC (I) vs H | 0.7131 | 36 | 85 | ||||
| DPYSL3 | GC vs H | 0.6188 | 48 | 82 | |||
| GC (I) vs H | 0.5948 | 45 | 82 | ||||
| MAGED2 | GC vs H | 0.5031 | 28 | 92 | |||
| GC (I) vs H | 0.5113 | 27 | 92 | ||||
| TrxR activity |
Before clinical intervention: 261 (130 H ; 131 GC (I n=25, II n=39, III n=46, IV n=21) |
GC (I) vs H | 0.948 | 80.00 | 97.69 | NA | Peng et al., 2019 |
| GC (II) vs H | 0.955 | 84.62 | 97.69 | ||||
| GC (III) vs H | 0.971 | 89.13 | 96.15 | ||||
| GC (IV) vs H | 0.974 | 90.48 | 97.69 | ||||
| GC vs H | 0.963 | 85.5 | 97.69 | ||||
| CEA+CA19-9+CA72-4 | GC vs H | 0.834 | 78.41 | 96.92 | |||
| CEA+CA19-9+CA72-4+TrxR | GC vs H | 0.982 | 91.60 | 94.62 | |||
**AGC, AGC of any grade ; *AGA, AGA of any grade ; AG, atrophic gastritis ; AG2+, moderate to severe AG ; AGA, AG in the antrum ; AGA2+, moderate to severe AGA ; AGAC, atrophic gastritis of the antrum and corpus ; AGAC2+, moderate to severe AGAC ; AGC, AG in the corpus ; AGC†, advanced gastric cancer ; AGC2+, moderate to severe AGC ; AH, atypic hyperplasia ; AUC, area under the curve ; BGT, benign gastric tumor ; CAG, chronic atrophic gastritis ; CC, colon cancer ; CG, chronic gastritis ; CI, confidence interval ; CRC, colorectal cancer ; DYS, dysplasia ; EGC, early gastric cancer ; GA, gastric atrophy ; GAC, gastric adenocarcinoma ; GAG, gastric atrophy group ; GC, gastric cancer ; GIM, gastric intestinal metaplasia ; GIMG, gastric intestinal metaplasia group ; H, healthy controls ; HCC, hepatocellular cancer ; Hpi, chronic superficial gastritis associated with Helicobacter pylori infection ; IM, intestinal metaplasia ; LGD, low-grade dysplasia ; LGN, low-grade intraepithelial neoplasia ; NA, not available ; NAG, non-atrophic gastritis ; OR, odds ratio ; OST, other system malignant tumors ; PGL, precancerous gastric lesions ; PL, precancerous lesions ; RC, rectal cancer ; Se, sensitivity ; Sp, specificity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



