
Submitted:
30 July 2024
Posted:
31 July 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction: The COVID-19 pandemic challenged people with spinal cord injury (SCI) regarding a variety of mental and physical issues. New challenges may arise as the effects of the pandemic continue. The objective of the present study was to explore the social participation of Canadians with SCI during the second wave of COVID-19. Methods: Participants with SCI from two Canadian provinces (Quebec and British Columbia) were interviewed. Results: Eighteen participants completed interviews. Facilitators of social participation remain similar since the first wave of COVID-19, such as the use of technology, help received by relatives and the use of delivery services to obtain groceries and other essentials. Obstacles to mobility due to winter conditions and lack of considerations related to COVID-19 public health measures specific to wheelchair users were also discussed by participants. Conclusions: People with SCI perceived participation restrictions, little changes in life habits, and uncertainty about the future during the second wave of COVID-19. The unique living conditions of people with SCI, ability to adapt life habits, and the lived experiences of people with SCI may have contributed to an overall resilience during the pandemic. Adaptive families, social contacts and technology made a difference during the pandemic.
Keywords:
COVID-19
; Spinal Cord Injury
; Manual Wheelchair
; Social Participation
; Rehabilitation
; Social Support
1. Introduction
The COVID-19 pandemic has had considerable impact on the daily life of people with disabilities (PWDs) [1,2]. Public health measures have been put in place in effort to mitigate the transmission of the virus [3]. PWDs might be at higher risk of COVID-19 infection due to their underlying health conditions and their contact with multiple care providers [1]. A rapid review conducted in the early days of the pandemic revealed that PWDs experienced negative pandemic-related impacts on physical and psychological well-being, and on access to various services, such as rehabilitation services [4]. The public health measures put in place during the pandemic also influenced changes in social habits, daily activities and reduced physical activity for people with preexisting chronic conditions [5,6,7]. In this regard, the pandemic has exacerbated the inequalities already present in society, resulting in increased vulnerability of PWDs [8].
Recent literature has highlighted changes that negatively impacted the daily life of people with spinal cord injury (SCI) since the beginning of the pandemic, such as changes in mental and physical well-being that are associated with reduced physical activity [9]. In addition, increased barriers to mobility and transportation have been reported, such as the inability to obtain transportation to health care appointments [10]. These additional obstacles combined with limited and modified access to health services (e.g., cancellation of health care consultations and the cessation of face-to-face rehabilitation activities) resulted in additional medical complications [11]. Moreover, some people with SCI recognized improvements in the accessibility of medical appointments or rehabilitation services despite the reduced access to services overall. For example, telemedicine respected social distancing while reducing travel time and costs [12].
A recent exploration of social participation experiences of people with SCI during the first wave of the pandemic reported impacts on the accomplishment of and satisfaction with life habits among people with SCI [13]. Indeed, people with SCI faced additional difficulties in integrating public health measures in their daily habits and experienced negative impacts on psychological well-being [13]. These results are particularly concerning given the additional challenges that may have arisen as the pandemic continued to evolve. Facilitators that were available during wave one of the pandemic, such as increased social support and assistance from family and friends [13], may have decreased as people returned to work and pre-pandemic life activities during the second wave. Consequently, people with SCI may have experienced increased barriers to social participation as the pandemic continued. Therefore, the objective of this study was to explore the social participation of Canadians with SCI during the second wave of COVID-19 pandemic.
2. Materials and Methods
2.1. Design and Participants
In this cross-sectional study, a qualitative descriptive approach was used to conduct semi-structured interviews [14]. A convenience sample was recruited from a randomized controlled trial that was ongoing in Canada (i.e., Quebec City, Montreal and Vancouver) (ClinicalTrials.gov Identifier: NCT02826707) [15] to evaluate a peer-led physical activity program delivered using smartphones for people with SCI. As described by Best et al. [15] the inclusion and exclusion criteria were to: be 18 years or older, live in the community, have a SCI for ≥ 1 year, use a manual wheelchair for mobility and physical activity, be able to self-propel their wheelchair ≥ 100 m, not meet the SCI physical activity guidelines (90 min/week) [30], be able to communicate in English or French, and be cognitively able to engage in the ALLWheel intervention. Participants were excluded if they had a degenerative condition expected to progress quickly (e.g., amyotrophic lateral sclerosis) or if they had contraindication to physical activity. Participants of the randomized controlled trial who consented to be contacted for future studies were invited by telephone to take part in this study, which is independent from the larger trial. Among the present sample, thirteen people were also interviewed in a previous cross-sectional study aimed to explore social participation during the first wave of the pandemic [13]. This project was approved by Institutional Research Ethics Boards.
2.2. Data Collection
Sociodemographic data (i.e., age, sex, province of residence, employment status, length of time using a wheelchair) were extracted from the baseline measures collected in the ongoing randomized trial. Between December 2020 and April 2021, participants completed a semi-structured interview conducted by a research associate (CR). Figure 1 presents the key public health measures in place at the time of the interviews in Quebec and British Colombia according to Canadian Institute for Health Information [16]. A semi-structured interview guide developed by the research team comprised 19 open-ended questions and prompts that were guided by the Human Development Model – Disability Creation Process (HDM-DCP) [17]. The complete interview guide is available as a Supplemental Material. Data were collected remotely and recorded by telephone and videoconference (Teams/Zoom) in English or French. The duration of the interview ranged from 20 to 45 minutes. Interviews were audio recorded and transcribed verbatim (NJL) or using TranscribeMe services.
2.3. Data Analysis
Deductive line-by-line coding and thematic analysis [14] were conducted [18] by two research associates (NJL and DB) in the original language (English or French). The same codebook reported by Fortin-Bedard et al. was used to guide the deductive analysis [13]. The interviews were coded using NVivo (version 13) by a research associate (NJL) [19]. Two research associates (NJL and DB) met to discuss their common understanding of the codes at mid-point and at the end of the coding process to ensure consistency between coders [18]. Codes were verified by two researchers with experience in the HDM-DCP (FR and KLB) to ensure credibility [20]. French quotes were translated to English using translation software (DeepL).
3. Results
Among the 18 participants included, 12 (67%) were males, their mean (SD) age and years of wheelchair experience were 49 (15) years and 15 (13) years, respectively (Table 1).
Three interrelated themes emerged, including 1) “Perceived participation restrictions for people with SCI and their loved ones during COVID-19”, which suggested there were interruptions and changes in health service provision during COVID-19, barriers and inconveniences to maintain life habits and strategies developed during the pandemic to continue participating in meaningful activities; 2) “There was no change in life habits (but newfound ways to do some things)”, which highlights that life simply continued as usual and the participants developed new pastimes and interests; and 3) “What does the future hold?” which describes participants’ perceptions about the pandemic during the lockdown and for the months to come.
3.1. Perceived participation restrictions for people with SCI and their loved ones during COVID-19
3.1.1. Interruptions and changes in service provision.
Due to the different public health measures, some participants reported limitations or changes in home-based social and health services, such as home visits or medical appointments. Others mentioned experiencing irregular services, which may have resulted in increased burden on family members who assumed some tasks.
In terms of rehabilitation care, a participant expressed experiencing participation restrictions due to limited access to physiotherapy, which was associated with experiencing more muscle spasms and having to take more medications to manage health. In addition, another participant mentioned that not having access to gym equipment limited their ability to do lower limb exercises.
Several participants highlighted that health-care appointments were delayed due to the pandemic, with a participant describing being placed on a waiting. In this way the needs of many participants were not being met. However, when possible and for less urgent situations, participants used telephone or videoconference appointments to meet with healthcare professionals:
“I have a psychologist whom I continued to see on Skype and then my nutritionist on Zoom. So, in that sense, I was well served. I have had a telephone consultation with my doctor twice. […] At the pharmacy, they are absolutely great. It’s delivery, but it’s also the perception of what’s urgent? (participant 8).”
Participants seemed to appreciate telehealth services, as it reduced travel time, costs, limit contact and waiting time.
Impacts on home services were also described, such as house-cleaning and personal hygiene services:
“What is most difficult is help for maintaining the household. I do business with a cooperative that provides a weekly cleaning service to come and do the cleaning, but it becomes difficult because, every week, we ask ourselves: "1): who will come? And 2): are we going to have someone?” […] When we don’t have [the person comes to do the housework and the laundry], it’s my spouse who has to do it. […] It gets really challenging, because if there is no one coming, the burden falls on him (Participant 7).”
3.1.2. Barriers and inconveniences
Although participants expressed feeling confined during the pandemic, experiences of confinement were common before the pandemic. For example, mobility during winter was always a challenge due to cold and snow-covered sidewalks, and the pandemic did not change the situation much:
“I’m more confined, basically. I’ve been more confined in advance with the winter, because if I want to go outside, but in a wheelchair, it’s more difficult. I mean, […] sometimes when it’s snowed enough, there’s no snow edge for a few days, that it’s accessible. Then the cold too, I don’t move, so I can’t go out when it’s -10ºC, -15ºC. It’s too cold. You are more confined in the house (participant 12).”
However, some participants felt the pandemic decreased likelihood to leave the home in the winter, as people were afraid of getting stuck outside or getting sick and having to go to the hospital:
“[During] winter, I didn’t want to get sick to avoid going to the hospital sick because of COVID (participant 5).”
When participants did leave their homes, there were often additional environmental barriers to overcome. These barriers were due to public health measures installed during the pandemic, which limited access to locations for people using a wheelchair:
“They put concrete blocks so that people don’t go there, but it’s just the campers that aren’t allowed to go there with their tents. They went there as well because there were people who went over the block, but I with my wheelchair couldn’t go over the concrete block, because they closed that to the world (Participant 5).”
Another participant mentioned that it was difficult to wash their hands in some stores due to difficultly to use foot pedals on the floor. Consequently, the participant mentioned the importance to add handwashing stations with an accessible hand pump:
“When you walk into a grocery store, maybe you’ve noticed, or another store, it’s handwashing but it’s on a stand and then a rack. But instead of going with your hands, it’s your foot. You have to weigh with your foot. So that, good luck, with a chair (participant 11).”
3.1.3. It’s better than nothing.
Participants mentioned being more concerned about what is urgent and what is less urgent. In fact, they mentioned not going out anymore unless it is necessary, such as medical appointments. Most participants indicated that they have fewer opportunities to see their loved ones due to public health measures, resulting in a lack of social engagement. These public health measures were particularly difficult for one participant when contact with their family was limited during the holidays:
“The holidays are usually about family reunions […].. Then from that point on, yes, it was more difficult. I thought it was going to go over easily, that there wouldn’t be too many difficulties. Then finally, I found it a little difficult (Participant 16).”
The psychological impacts of the pandemic were varied among participants, as few participants experienced little or no change in mental health while other described how the pandemic was mentally challenging (e.g., increased depression, lack of motivation and stress):
“I think the biggest difficulty is the psychological impact of looking forward to a ray of hope, what with getting the vaccine and thinking that it was going to open up for everyone. Things were starting to open up again, and then to have these restrictions come down was, I think, a big psychological impact for everybody, me included. But it’s pretty depressing. (Participant 4)”
Nevertheless, participants reported being reassured to be able to see their loved ones outside (as mandated by the public health measures), even in winter:
“It was fun because we could see each other outside. What makes that, it was really reassuring and then that’s it, we really benefited more (Participant 6).”
Although participants were looking forward to the end of the pandemic, the second COVID wave which occurred mainly in winter, was perceived by some as an opportunity to take a break:
“You have to see it as [...] well, it’s a break. Then you have to take a break, take that break. You have to figure out what’s fun. Just take the opportunity to do things that people don’t have time to do because they’re working or because they always have too much to do. It’s a good time to take advantage of it to do things that you’ve been meaning to try to do, or that you like to do. This is the time. It’s time to think about yourself, pull out a good book, read. That’s it. It’s winter too (Participant 6).”
In addition, technology (e.g., Messenger and other videoconferencing systems) has been a good tool to stay in touch with their loved ones, despite the technological difficulties sometimes encountered (e.g., difficulty with the microphone, the sound does not work, etc.). Technologies was indeed helping people continue to meaningfully participate in their communities in the pandemic context.
3.2. There was no change in life habits (but we found new ways to do some things)
3.2.1. Life simply continued as usual.
Some participants reported no change in the attainment of some life habits as the pandemic evolved, despite the public health measures put in place. For example, participants mentioned having already experienced social distancing associated with using their wheelchair:
“I always have social distance with my mask and otherwise, you are with the wheelchair, the people will stay far from me. I have already my feet in front of me. (Participant 9)”
Specifically, one participant felt they were already physically limited due to their wheelchair before the pandemic:
“I don’t really see where I would need more services. I have the care I need. My activities are not too restricted because what I said, the confinement, there are quite a few people who have a hard time with that, but when you’re confined to a wheelchair, the confinement, in the winter, you know what I said: “Everyone is forced to do what I'm forced to do all the time.” It’s limiting everyone, but on that side, it’s limiting me a little bit, but a lot less than most people, I think. (Participant 15).”
Participants described being able to continue to carry out daily habits as usual, due to the help received by family members who took care of daily tasks such as grocery shopping:
“It’s the same as always. Personally, I’m lucky I have my girlfriend because she’s the one who does everything (participant 13).”
Participants also expressed that winter and summer during the pandemic were similar to previous years (e.g., fewer outdoor outings in winter) thus being minimally or not impacted by the pandemic context. While another participant conveyed, they maintained normal activities, such as work. Participants described how they continued to use home delivery services to receive medical equipment and groceries, services already used before the pandemic, which allowed them to maintain their usual life habits:
“For me, there hasn’t been much of a change because I don’t go out [much], so I was just going to do my little errands during the day, everything was open, so that’s okay. [...] I work at home a lot, so for me there hasn’t been much change. [...] [As far as medical accessories], they deliver here, once every two months, and it’s a good material ... as before, it hasn’t changed anything (Participant 17)”
Pertaining to interpersonal relationships, few participants reported minimal change regarding the frequency of contact with others. For instance, participants explained that even before the pandemic they did not go out much and described how physical barriers in their loved ones' homes limited accessibility:
“Let’s say that in the family, [...], I don’t want to visit them, because it’s not accessible. If I visited them, it was in summer (Participant 10)”.
Most participants said they used digital technology (e.g., videoconferencing platform) before and during the pandemic to maintain contact with loved ones:
“Well, it’s easy. It’s easy to keep up with family and friend’s birthdays with a Zoom call or whatever. So, yeah, and I guess Facetime is the same thing really, but yeah (Participant 3).”
Some participants reported that public health measures had little influence on their participation in physical activities. Specifically, some participants reported continuing to engage in physical activity online, or at home, or to continue training in the gym, even though the gyms were closed for the general population. A participant reported:
“The gym, the big gym, it closed, but they made like a room for people like me, in wheelchairs, for people [with health issues] who need to train in the gym. [...] We are very happy. I am happy. (Participant 18)”
According to participants, to maintain the same level of autonomy to carry out some of their life habits (e.g., going shopping and groceries) they required more help from loved ones compared to before the pandemic.
3.2.1. New pastimes and interests.
Participants expressed feeling more freedom when the public health measures were less stringent but maintained vigilance to protect against the virus. It seems that protocols put in place by local service providers such as restaurants were an important consideration:
“It turned out that they [the restaurant] were already following COVID protocol before there was even COVID. So, we felt really safe there, so we went only there. (participant 2)”
In addition, the deprivation experienced during periods of heightened restrictions influenced how participants appreciated the ability to accomplish regular daily activities. In addition, participants highlighted how summer offers more participation opportunities, such as the possibly to visit their loved ones outside. During the pandemic context, some participants also described how they developed new ways to be physically active:
“I think strangely enough I’m more active now than I have been in the past two and a half years. […] Because I just started-- because a non-profit organization is doing all these exercise activities online and I just started boxing with this guy who used to be a boxer before he became disabled. And he’s doing online courses so I’m boxing three times a week now (Participant 1).”
Participants described how the pandemic period provided an opportunity for self-reflection and to enjoy new activities. Indeed, the pandemic context such as lockdown was an opportunity to do things that were not usually possible due to lack of time. In addition, reducing, or even stopping some social activities such as holiday gatherings that require a lot of preparation allowed a participant to be more relaxed and relieved.
3.3. What does the future hold?
3.3.1. Concerns
There was some feeling that the needs of PWDs were not considered during the pandemic:
“We have the impression that we are not on the map in times of COVID, in such a pandemic (participant 8).”
People with SCI reported experiencing numerous participation restrictions before the pandemic, which may have been heighten due to pandemic-related measures. Furthermore, despite vaccination, some people will continue to follow public health measures in their daily life, thus may continue to experience heighten restrictions. Despite confidence in the vaccine, a participant felt that several vaccines would be needed and that it would not be back to normal until 2022 or perhaps even 2023.
3.3.2. Hopes
A few participants believed that awareness of viral contamination will be enhanced. For example, people will have learned to wash their hands and cough into their elbow:
“I think people are going to be more careful now when people are going to sneeze or-- maybe even people are going to be less cuddly than before, are going to be more careful (Participant 14).”
Overall, participants were optimistic that the situation will improve with the arrival of the vaccine. Despite the challenging context, especially with masks and social distancing, some participants believed that people will be more comfortable reuniting with their loved ones in the spring. Another participant hopes that people will learn to take care of others.
Despite some return to normal, a participant felt that the availability of online programs (and technology) for people with disabilities will remain valuable after the pandemic:
“Online programs for people’s disabilities, I think, is a little bit of a gold mine. Because I’m watching the people on the Zoom calls and stuff like that [...] And I feel like people with disabilities are just so much more likely to show up if all they have to do is get up and get on Zoom at their home. Because it just eliminates so many of those barriers (Participant 2).”
Technology may continue to facilitate PWDs to participate in programs via videoconferencing, while removing many barriers to social participation such as transportation and accessible community spaces. Nevertheless, participants had other suggestions to facilitate participation. For example, efforts to prioritize access to stores for people in wheelchairs, instead of enforcing rules to line up outside. In addition, having personal shoppers available, or assistance offered for people with disabilities may facilitate in person activities:
I would think maybe in shopping or something like that. Because say you go to a store often […], things are too high, and I have to ask people for help but now with COVID, I can’t imagine like if somebody goes shopping and they have a disability and there are items that are too high—I’d ask strangers to help me and stuff. That might not be so appropriate anymore in this context so maybe having, I don’t know, personal shoppers or something being offered to people with disabilities (Participant 2).”
4. Discussion
This study showed that Canadians with SCI perceived participation restrictions, little changes in life habits, and uncertainty about the future during the second wave of COVID-19. Compared to the findings during the first wave of COVID-19 [13], there were very few changes. The status quo in social participation may be partly explained by the resilience of this population and the quick response of community members and organizations to help during wave one. The unique living conditions of people with SCI, ability to adapt life habits, and the lived experiences of people with SCI may have contributed to an overall resiliency during the pandemic.
Help received from others, including help from family, friends, and community organizations, played a large role in the realization and satisfaction of life habits. Previous studies conducted before the pandemic [21,22] similarly reported that assistance from informal caregivers (i.e., family members) was an important facilitator of social participation among individuals with SCI. While this assistance was a facilitator, there were important considerations. First, assistance from informal caregivers who are family members may induce a greater exposition to the virus for people with SCI [23]. Second, informal caregivers must be adequately supported (e.g., financially) to allow them in turn, to support people with SCI [24]. A prospective study conducted with caregivers of people with amyotrophic lateral sclerosis indicated a significantly increased burden after the first lockdown in comparison with the early pandemic period in Italy [25]. In this regard, Jeyathevan et al., reported that the lack of access to community resources and fragmented continuity of care may represent barriers to caregiving of people with SCI [26]. Future studies should examine whether family members will be able to maintain their level of caregiver involvement over time. In addition, the longer-term impacts of the pandemic on social participation for people with SCI who have less social support [27] remains to be determined.
The use of digital technology was also facilitator to social participation reported in the early pandemic period [13], which was maintained as the pandemic continued. Indeed, in the present study, digital technology remained helpful to maintain contact with loved ones, to have virtual appointments with health professionals and to maintain physical activities. This result was consistent with a previous study conducted by Ammar et al., indicating that digital technologies can be a tool to promote social participation during the COVID-19 confinement, and in turn, can increase life satisfaction [28]. In this regard, the continuation of virtual healthcare services for people with SCI beyond the pandemic could be considered to reduce risk of infection and enhance convenience and flexibility [12]. Similarly, these benefits were perceived by participants the present study. Considering the consistency to which telehealth were reported as facilitators since the beginning of the pandemic, the continuous provision of virtual services could be relevant for individuals with SCI under certain conditions. Indeed, despite the potential benefits as highlighted in the present study, some challenges in using the technology remain. There are considerations for the provision of virtual healthcare services for people with disabilities, such as professionals being aware of the inequality of access to digital devices, in addition to variable internet connection, comfort and skills to use technology [29,30].
Similar to findings by Fortin-Bedard et al conducted at the beginning of the pandemic [13], participants reported facing increased environmental barriers during winter. However, reduced participation in winter has been previously reported among people with disabilities; therefore, may not be solely due to the pandemic. Indeed, weather conditions make wheelchair mobility difficult (e.g., sidewalks that are not cleared of snow), which mitigate the impact on life habits. For instance, previous findings reported that wheelchair users reduced their outing frequency during winter due to cold hands while pushing rims and slipping on the ice [31], and the general barrier of cold temperatures and snow [ref]. Moreover, there is limited research on winter-specific needs and supportive technologies for people who use mobility devices [31]. The winter exacerbates participation restrictions, which is particularly worrisome for people with SCI who experienced greater barriers to social participation throughout the pandemic. This lack of consideration for people with physical disabilities is a concerning result and further highlights the importance of advocacy for enhanced community accessibility and inclusivity for people with physical disabilities during and after the pandemic [2,32].
Resilience among people with SCI may mitigate the future impact as the pandemic continues [33]. Given that few changes regarding social participation were reported since the early pandemic period [13], the state of status quo suggests that people with SCI have self-adapted. In fact, PWDs had already integrated daily public health measures (e.g., avoiding sick people, maintaining social distancing, wearing a mask), which may have facilitated the integration of public health measures during the pandemic [34]. In addition, the regular use of delivery services for groceries and medical needs may facilitative community integration for people with SCI and may justify the minimal changes experienced during the pandemic [35]. Finally, a previous study reported that must people living with a SCI show resilience, which may have been a strength during the onset and continuation of the pandemic [36].
Limitations of this study must be addressed. First, the small heterogeneous convenience sample in two provinces in Canada with slightly different public health measures across the country which limits the transferability of the results. However, the interviews make it possible to explore in-depth the perceived experience of the participants [37]. Second, the same initial themes from a previous study were used for the analysis to focus on the evolution of the experience of people with SCI during the pandemic, which may have resulted in missing additional themes. Nevertheless, the data identified from the interviews were consistent with the a priori themes and subthemes. In addition, the interviews were conducted over a period of four months and in two provinces in Canada with different public health measures at the time on the interview, which may have influenced the reported experiences of the participants. For example, public health measures were stringent at the beginning of the interview period (i.e., December 2020 and January 2021), but were somewhat relaxed near the end of the interviews (i.e., February 2021) [3]. In this regard, it would have been interesting to compare changes in the perception of social participation from a longitudinal perspective. Finally, the results represent our perception of the participants’ reported experience during the interviews since the results were not returned to the participants for validation.
5. Conclusions
Findings suggest that people with SCI perceived participation restrictions, little changes in life habits compared to experience during the first wave of COVID-19, and uncertainty about the future during the second wave of COVID-19. The unique living conditions of people with SCI, ability to adapt life habits, and the lived experiences of people with SCI may have contributed to an overall resilience during the pandemic. Adaptive families and social contacts using technology made a difference during the pandemic, although the day to day lives of people with SCI did not change much.
Supplementary Materials
The following supporting information can be downloaded at: www.mdpi.com/xxx/s1, interview guide.
Author Contributions
Conceptualization, N-J.L, F.R, K.L.B.; formal analysis, N.F-B, N-J.L, D.B.; investigation, C.R.; writing—original draft preparation, N.F-B, N-J.L.; writing—review and editing, N.F-B, N-J.L, D.B, C.R, J.B, S.N.S, K.P.A-N, F.R, K.L.B.; supervision, , F.R, K.L.B. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Craig H Neilsen Foundation Psychosocial Research program.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Research Ethics Boards.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
Identified data will be made available upon request.
Acknowledgments
Salary support for KLB and FR was provided by the Quebec Health Research Funds (FRQS). NFB was supported through an Accelerate Mitacs scholarship and holds a master training award from the Canadian Institutes of Health Research (CIHR) and from FRQS in partnership with the Unité de soutien au système de santé apprenant (SSA) Québec. SNS is supported through a Canada Research Chair in Participation, Well-Being, and Physical Disability (Tier 2) and JB is supported through a Canadian Research Chair in Rehabilitation Engineering Design.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Government of Canada. COVID-19 and people with disabilities in Canada 2021 [Accessed on 9 June 2021]. Available from: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/guidance-documents/people-with-disabilities.html#shr-pg0.
- Fortin-Bédard N, Lamontagne M-E, Ladry N-J, et al. Exploring the Experiences of People with Disabilities during the First Year of COVID-19 Restrictions in the Province of Quebec, Canada. Disabilities. 2023;3(1):12-27.
- Institut national de santé publique du Québec. Ligne du temps COVID-19 au Québec: Institut national de santé publique du Québec; 2021 [Accessed on 8 July 2021]. Available from: https://www.inspq.qc.ca/covid-19/donnees/ligne-du-temps.
- Lebrasseur A, Fortin-Bedard N, Lettre J, et al. Impact of COVID-19 on people with physical disabilities: A rapid review. Disability and Health Journal. 2021 Jan;14(1):101014.
- Di Stefano V, Battaglia G, Giustino V, et al. Significant reduction of physical activity in patients with neuromuscular disease during COVID-19 pandemic: the long-term consequences of quarantine. Journal of Neurology. 2021 Jan;268(1):20-26.
- Lopez-Sanchez GF, Lopez-Bueno R, Gil-Salmeron A, et al. Comparison of physical activity levels in Spanish adults with chronic conditions before and during COVID-19 quarantine. European Journal of Public Health. 2021 Feb 1;31(1):161-166.
- Capuano R, Altieri M, Bisecco A, et al. Psychological consequences of COVID-19 pandemic in Italian MS patients: signs of resilience? Journal of Neurology. 2021 Mar;268(3):743-750.
- Mesa Vieira C, Franco OH, Gómez Restrepo C, et al. COVID-19: The forgotten priorities of the pandemic. Maturitas. 2020 Jun;136:38-41.
- Marco-Ahulló A, Montesinos-Magraner L, González LM, et al. Impact of COVID-19 on the self-reported physical activity of people with complete thoracic spinal cord injury full-time manual wheelchair users. Journal of Spinal Cord Medicine. 2021 Jan 19:1-5.
- Stillman MD, Capron M, Alexander M, et al. COVID-19 and spinal cord injury and disease: results of an international survey. Spinal Cord Series and Cases. 2020 Apr 15;6(1):21.
- Gustafson K, Stillman M, Capron M, et al. COVID-19 and spinal cord injury and disease: results of an international survey as the pandemic progresses. Spinal Cord Series and Cases. 2021 2021/02/12;7(1):13.
- Buckingham SA, Anil K, Demain S, et al. Telerehabilitation for People With Physical Disabilities and Movement Impairment: A Survey of United Kingdom Practitioners. JMIRx Med. 2022 2022/1/3;3(1):e30516.
- Fortin-Bédard N, de Serres-Lafontaine A, Best KL, et al. Experiences of Social Participation for Canadian Wheelchair Users with Spinal Cord Injury during the First Wave of the COVID-19 Pandemic. Disabilities. 2022;2(3):398-414.
- Fereday J, Muir-Cochrane E. Demonstrating Rigor Using Thematic Analysis: A Hybrid Approach of Inductive and Deductive Coding and Theme Development. International Journal of Qualitative Methods. 2006;5(1):80-92.
- Best KL, Routhier F, Sweet SN, et al. The Smartphone Peer Physical Activity Counseling (SPPAC) Program for Manual Wheelchair Users: Protocol of a Pilot Randomized Controlled Trial. JMIR Res Protoc. 2017 Apr 26;6(4):e69.
- Canadian Institute for Health Information. Canadian COVID-19 Intervention Timeline 2022 [Accessed on 9 June 2021]. Available from: https://www.cihi.ca/en/canadian-covid-19-intervention-timeline.
- International Network on the Disability Creation Process. The Human Development Model – Disability Creation Process - Key Concepts 2021.[Accessed on 7 June 2021]. Available from: https://ripph.qc.ca/en/hdm-dcp-model/key-concepts/.
- Roberts K, Dowell A, Nie J-B. Attempting rigour and replicability in thematic analysis of qualitative research data; a case study of codebook development. BMC Medical Research Methodology. 2019 2019/03/28;19(1):66.
- QSR International Pty Ltd. NVivo (released in March 2020) 2020. Available from: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home.
- Nowell LS, Norris JM, White DE, et al. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. International Journal of Qualitative Methods. 2017 2017/12/01;16(1):1609406917733847.
- Barclay L, McDonald R, Lentin P, et al. Facilitators and barriers to social and community participation following spinal cord injury. Australian Occupational Therapy Journal. 2016 Feb;63(1):19-28.
- Munce SEP, Webster F, Fehlings MG, et al. Perceived facilitators and barriers to self-management in individuals with traumatic spinal cord injury: a qualitative descriptive study. BMC Neurology. 2014 2014/03/13;14(1):48.
- World Health Organization (WHO). Disability considerations during the COVID-19 outbreak 2020 [Accessed on 8 July 2021]. Available from: https://apps.who.int/iris/bitstream/handle/10665/332015/WHO-2019-nCov-Disability-2020.1-eng.pdf.
- Huang J, Pacheco Barzallo D, Rubinelli S, et al. What influences the use of professional home care for individuals with spinal cord injury? A cross-sectional study on family caregivers. Spinal Cord. 2019 2019/11/01;57(11):924-932.
- Giusiano S, Peotta L, Iazzolino B, et al. Amyotrophic lateral sclerosis caregiver burden and patients’ quality of life during COVID-19 pandemic. Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration. 2021:1-3.
- Jeyathevan G, Catharine Craven B, Cameron JI, et al. Facilitators and barriers to supporting individuals with spinal cord injury in the community: experiences of family caregivers and care recipients. Disability and Rehabilitation. 2020 Jun;42(13):1844-1854.
- Huang D, Siddiqui SA, Touchett HN, et al. Protecting the most vulnerable among us: Access to care and resources for persons with disability from spinal cord injury during the COVID-19 pandemic. PM & R : the journal of injury, function, and rehabilitation. 2021;13(6):632-636.
- Ammar A, Chtourou H, Boukhris O, et al. COVID-19 Home Confinement Negatively Impacts Social Participation and Life Satisfaction: A Worldwide Multicenter Study. International Journal of Environmental Research and Public Health. 2020;17(17).
- Annaswamy TM, Verduzco-Gutierrez M, Frieden L. Telemedicine barriers and challenges for persons with disabilities: COVID-19 and beyond. Disabil Health J. 2020 Oct;13(4):100973.
- Selick A, Durbin J, Hamdani Y, et al. Accessibility of Virtual Primary Care for Adults With Intellectual and Developmental Disabilities During the COVID-19 Pandemic: Qualitative Study. JMIR Form Res. 2022 2022/8/22;6(8):e38916.
- Ripat JD, Brown CL, Ethans KD. Barriers to wheelchair use in the winter. The Archives of Physical Medicine and Rehabilitation. 2015 Jun;96(6):1117-22.
- Andrews EE, Ayers KB, Brown KS, et al. No body is expendable: Medical rationing and disability justice during the COVID-19 pandemic. American Psychological Association; 2021. p. 451-461.
- Mikolajczyk B, Draganich C, Philippus A, et al. Resilience and mental health in individuals with spinal cord injury during the COVID-19 pandemic. Spinal Cord. 2021 2021/12/01;59(12):1261-1267.
- Desjeux, C. COVID-19 : handicaps, perte d’autonomie et aides humaines. Difficultés et tensions des gestes barrières et des équipements de protection individuelle à domicile. Alter. 2020 2020/09/01/;14(3):249-257.
- Cochran, AL. Impacts of COVID-19 on access to transportation for people with disabilities. Transportation Research Interdisciplinary Perspectives. 2020 2020/11/01/;8:100263.
- Kilic SA, Dorstyn DS, Guiver NG. Examining factors that contribute to the process of resilience following spinal cord injury. Spinal Cord. 2013 2013/07/01;51(7):553-557.
- Hammarberg K, Kirkman M, de Lacey S. Qualitative research methods: when to use them and how to judge them. Human Reproduction. 2016;31(3):498-501.
Figure 1.
Timeline of the COVID-19 public measure in Quebec and British Colombia.
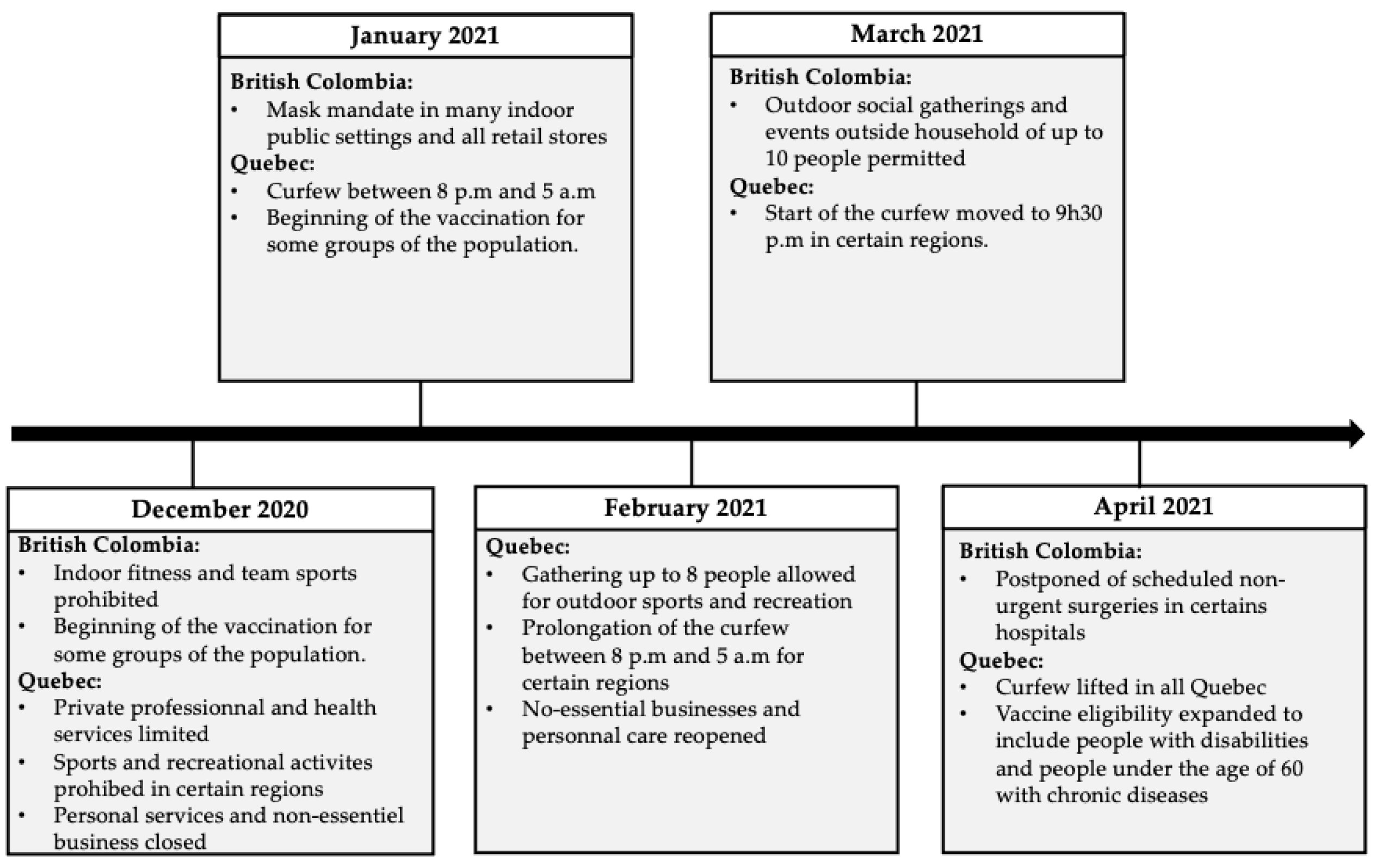

Table 1.
Characteristics of participants (n=18, unless stated) .
| Characteristics | |
|---|---|
| mean [SD] | |
| Age, years | 48.8 [15.1] |
| Time Using Any wheelchair, years | 15.1 [13.3] |
| n (%) | |
| Sex | |
| Women | 6 (33.3) |
| Men | 12 (66.7) |
| Province of Origin | |
| Quebec | 14 (77.8) |
| British Columbia | 4 (22.2) |
| Employment Status (n=17) | |
| Employed | 3 (17.6) |
| Unemployed | 9 (53.0) |
| Retired | 5 (29.4) |
| Highest Education Level | |
| High school (started) | 6 (33.3) |
| College/University (started) | 2 (11.1) |
| College/University (completed) | 7 (38.9) |
| Post-graduate studies | 2 (11.1) |
| Annual Household Income, $ (n=16) | |
| < 29’999 | 7 (43.7) |
| 30’000-44’999 | 3 (18.8) |
| 45’000-59’999 | 3 (18.8) |
| > 60’000 | 3 (18.8) |
| Diagnostic | |
| Paraplegic | 15 (83.3) |
| Tetraplegic | 3 (16.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



