
Submitted:
31 July 2024
Posted:
31 July 2024
You are already at the latest version
Abstract
Patients with inflammatory bowel diseases (IBD), including both ulcerative colitis (UC) and Crohn's disease (CD), are at a higher risk of developing colorectal cancer (CRC). However, advancements in endoscopic imaging techniques, integrated surveillance programs, and improved medical therapies have led to a decrease in the incidence of CRC among IBD patients. Currently, the management of patients with IBD who have a history of or ongoing active malignancy is an unmet need. This involves balancing the risk of cancer recurrence/progression with the potential exacerbation of IBD if the medications are discontinued. The objective of this review is to provide an updated summary of the epidemiology, causes, risk factors, and surveillance approaches for CRC in individuals with IBD, and to offer practical guidance on managing IBD patients with history of previous or active cancer.
Keywords:
inflammatory bowel disease
; Crohn’s disease
; ulcerative colitis
; colorectal cancer
; surveillance
1. Introduction
Inflammatory bowel disease (IBD) refers to chronic, immune-mediated conditions marked by recurring and remitting inflammation of the gastrointestinal tract [1]. Ulcerative colitis (UC) and Crohn's disease (CD) primarily affect the luminal tract of the gastrointestinal system [2]. However, their exact causes remain unclear and result from a complex interaction of immune dysregulation, microbial imbalance, and environmental factors in individuals with a genetic predisposition [2]. Patients with IBD have a higher risk of developing gastrointestinal cancers, especially colorectal cancer (CRC) [3]. Individuals with long-standing UC and Crohn's colitis (excluding limited proctitis) face an approximately 2–3-fold increased risk of CRC. This risk varies based on the study, time period, and individual risk factors [2]. Disease duration significantly influences the development of CRC associated with IBD, typically becoming a concern approximately 8 years after the onset of colitis [4]. Although the precise mechanism underlying this association remains unclear, it is plausible that prolonged exposure to repeated cycles of inflammatory insults and epithelial regeneration may contribute to this phenomenon [5]. Other major risk factors include the early onset of IBD in younger individuals, colonic inflammation, the severity of inflammation, backwash ileitis, the presence of strictures, and post-inflammatory polyps [6]. It remains uncertain whether the increased risk is due to a higher incidence of dysplastic polyps, which can be challenging to differentiate from benign post-inflammatory polyps during surveillance colonoscopies, or because post-inflammatory polyps are indicative of more severe inflammation [6]. To reduce the risk of CRC, management strategies focus on accurately assessing each patient's risk and distinguishing between high-risk and low-risk individuals (Figure 1) [2]. Fortunately, there is a trend towards a decline in the rates of CRC over time, likely due to advancements in medical therapies and the implementation of endoscopic screening/surveillance [7].
The aim of this review is to offer an updated summary of IBD-associated colorectal cancer (IBD-CRC), encompassing epidemiology, causes, and risk factors, with a focus on the significance of personalized risk assessment to recommend suitable surveillance protocols. We will also evaluate the efficacy and safety of medical therapies in patients with IBD-CRC and the effect of chemo-radiotherapy on the course of IBD.
2. Materials and Methods
We searched Pubmed, Embase, and Scopus databases up to June 30 2024 in order to identify studies regarding CRC and IBD. To achieve this, we employed specific search terms such as “colorectal cancer”, “CRC”, “malignancy”, “neoplasia”, “inflammatory bowel disease”, “IBD”, “Crohn’s disease”, “CD”, “ulcerative colitis”, “UC”, “surveillance”, “screening”, “CRC risk factors”. We limited our search to articles published in English. Three authors (FJ, BS, and DF) reviewed the titles and abstracts to determine eligible studies. The full texts of the selected articles were examined for inclusion, and their reference lists were manually searched to identify any studies that the electronic search might have missed. Abstracts and articles were included based on their relevance.
3. Epidemiology
IBD patients can develop both sporadic CRC and IBD-CRC [8]. Sporadic CRC typically originates from a dysplastic precursor (usually an adenomatous polyp). It ranks as the third most common cancer in men and the second most common in women, with over 1.9 million new cases reported in 2020 [9]. In the development of IBD-CRC, extensive areas of persistently inflamed mucosa are susceptible to neoplastic transformation through a process known as "field cancerization"[2]. In this case, the global incidence rate in CD is estimated to range from 19.5 to 344.9 per 100,000 individuals annually, and from 54.5 to 543.5 per 100,000 individuals annually in patients with UC [10]. For individuals with CD, the risk of IBD-CRC is estimated to be 1.9 times higher [11], whereas for patients with UC, the elevated CRC risk is estimated at a standardized incidence ratio (SIR) of 2.4 [12]. For the entire IBD population, on the other hand, the SIR for IBD-CRC is 1.7 [13,14]. The risk of IBD-CRC is significantly elevated (by as much as two to three times) in patients with a history of UC and CD of at least 8 years long-standing, referred as ‘long-standing’ [3]. However, the precise risk can vary depending on different studies and time periods. For example, a meta-analysis from 2001, reported an overall prevalence of CRC in UC patients to be 3.2% [15]. The cumulative risk of CRC was 2% after 10 years, 8% after 20 years, and 18% after 30 years of disease [15]. Conversely, this risk was lower ( 1%, 3%, and 7% at 10, 20, and 30 years, respectively) in more recent studies [16]. The decrease in CRC risk over time can be credited to improved inflammation management through the use of newer medications and strategies, the introduction of colonoscopic surveillance programs, the optimised visualisation of the mucosa using high-definition instruments, the increased adoption of surgical interventions like colectomy and the potential chemopreventive properties of 5-aminosalicylates (5-ASAs) [8,17].
4. Risk Factors
To minimize the impact of IBD-CRC, it is crucial to accurately assess each patient's risk and identify key factors that necessitate frequent monitoring or intensive treatment.
4.1. Patient-Related Factors
A family history of CRC is linked to a higher risk of developing IBD-CRC [18]. In fact, patients with first-degree relatives who have CRC face a two-fold higher risk of developing CRC compared to those without first-degree CRC relatives [3,19]. Sex differences were also observed, with male patients having a higher risk of CRC than female patients [20], likely due to the protective role of estrogen in CRC development [21]. The most consistently reported risk factors for CRC include primary sclerosing cholangitis (PSC), which is associated with an increased absolute risk of up to 31% [22]. Patients with PSC have a reported four-fold increased risk of developing CRC compared to those without PSC [23]. Finally, being diagnosed with UC at a young age (less than 40 years old) has consistently been linked to a higher risk of developing CRC compared to being diagnosed at an older age [24].
4.2. Disease-Related Factors
The specific type of IBD (UC, CD, or IBD-unclassified) has not consistently shown a differential association with the risk of IBD-CRC [2]. Disease duration is one of the most significant risk factors for IBD-CRC. Although the exact mechanism behind this association is not fully understood, it is possible that the prolonged exposure to repeated cycles of inflammation and epithelial regeneration contributes to the increased risk [5,15]. Extensive disease, typically defined as more than 50% colonic involvement in CD or inflammation extending beyond the splenic flexure in UC at any point during the disease, is linked to a significantly higher risk 2 to 3 times greater of IBD-CRC compared to intermediate-extent CD and left-sided UC [20]. Patients with IBD proctitis have a CRC risk comparable to that of the general population [2]. Histologic inflammation is a more significant risk factor for IBD-CRC than gross endoscopic inflammation. Rutter et al. showed that higher endoscopic and/or histologic inflammation scores were linked to an elevated CRC risk in a multivariate analysis [25]. Other studies [26,27,28] have also confirmed the link between increased severity of endoscopic and histological inflammation and the risk of CRC. It is important to note that an increase in the mean Nancy histologic index was also associated with CRC development [29]. Additionally, patients with IBD who had been previously diagnosed with low-grade dysplasia [5], along with the presence of post-inflammatory polyps or colon stenosis, face a greater risk of CRC compared to those without IBD [20].
5. Endoscopic Surveillance
To reduce the risk of CRC, endoscopic surveillance is recommended for patients with UC that extends beyond the rectum and CD with colonic involvement of at least one-third of the colon, beginning 8 years after diagnosis [30]. The intervals for surveillance should be based on previously identified risk factors [30]. The main goal of this surveillance is to detect premalignant lesions that can be removed endoscopically or early-stage CRC, thereby improving prognosis and treatment outcomes [31]. Figure 1 illustrates the recommended surveillance intervals following the initial colonoscopy, tailored to the individual's CRC risk.
It is crucial to maintain endoscopic surveillance in patients who have undergone surgical treatment. For instance, those who have had a subtotal colectomy should continue to have their rectum monitored, regardless of whether it is in continuity or diverted [30]. Furthermore, patients who undergo a total proctocolectomy with ileal pouch anastomosis (IPAA) remain at risk for developing CRC due to the retention of a small portion of rectal mucosa at the anastomosis site [30], [32]. This risk is 4.4- and 15.0-fold increase in patients with prior colorectal dysplasia or CRC [33]. There is also a theoretical, albeit extremely rare, risk of developing small bowel cancer within the ileal pouch [30]. Therefore, for patients with high-risk characteristics, such as a history of CRC or dysplasia, PSC, or persistent moderate to severe pouchitis and/or pre-pouch ileitis, annual pouch surveillance is recommended [14,30,34].
To enhance the effectiveness of endoscopic surveillance, it is essential to optimize mucosal visualization and improve operator performance [35]. Nonetheless, various international societies offer guidelines on techniques for surveillance colonoscopy [23,34,36,37,38,39,40]. The SCENIC Consensus confirmed that standard definition (SD) white-light endoscopy (WLE) is inferior to high definition (HD) WLE in detecting dysplasia in patients with IBD [36]. SD endoscopes generate image signals with a resolution ranging from 100,000 to 400,000 pixels, whereas HD endoscopes produce image signals with resolutions of up to one million pixels, equivalent to viewing a surface with 30- to 35-fold magnification [41]. So dye-spray chromoendoscopy (DCE) using methylene blue or indigo carmine or virtual electronic chromoendoscopy (VCE; e.g., iSCAN, narrow band imaging or NBI, blue laser imaging or BLI) with targeted biopsies is suggested in the setting of HD endoscopy [36,42,43] to increase the yield of colonic dysplasia [40]. The use of biopsies during endoscopic surveillance remains a subject of debate. Prior to the adoption of CE, IBD surveillance colonoscopies typically involved taking random biopsies from four quadrants every 10 cm along the colon, in addition to targeted biopsies of any visible lesions [30]. The SCENIC guidelines recommend using either DCE with targeted biopsy sampling or random biopsy sampling with HD-WLE [36]. However, conflicting data has been published regarding the utility and yield of this strategy, primarily due to the wide range of reported dysplasia detected in the random biopsies [44,45]. The subsequent update of the SCENIC guidelines recommends random biopsies only for patients at higher risk, including those with PSC, previous dysplasia, or a scarred and atrophic colon [37]. However, extensive guidance on surveillance colonoscopy techniques is available from various international societies (Table 1).
6. IBD Therapy and Cancer
6.1. Management of IBD Therapy in Patients with a History of Previous Cancer
In patients with IBD who have a history of cancer, the risk of developing new or recurrent of previous cancer is doubled compared to those without a history of cancer [14], with an overall cancer incidence rate of 21.1 per 1,000 person-years [46]. Due to the relatively small number of IBD patients with a history of cancer, most data on site-specific cancer risks are derived from patients who have undergone organ transplantation or have other immune-mediated inflammatory diseases. Gastrointestinal, bladder, kidney, sarcoma, melanoma, non-melanoma skin cancer and myeloma are considered high risk for recurrence (>25%) [47,48]. In contrast, lymphoma, testicular cancer, and cervical cancer are associated with a lower risk of recurrence [47,48]. The CESAME study group published the results of a prospective assessment examining the risk of new or recurrent cancer in IBD patients with a history of cancer, whether or not they were receiving immunosuppressants such as thiopurines, methotrexate (MTX), or TNF inhibitors [46]. During follow-up, the incidence of cancer was 21.1 per 1,000 patient-years (PY) in patients with a history of cancer, compared to 6.1 per 1,000 PY in patients without a history of cancer [46]. Among cancer patients receiving immunosuppressants, 23% had significantly higher rates of new and recurrent neoplastic disease (23.1 per 1,000 PY and 3.9 per 1,000 PY, respectively) compared to the 77% without prior cancer diagnoses (13.2 per 1,000 PY and 6.0 per 1,000 PY, respectively) with no statistically significant difference [46]. Comparable findings were reported in a meta-analysis of pooled data on immune-mediated inflammatory diseases (IMIDs) [49] and in a recent multicenter cohort study of consecutive IBD patients with a history of non-digestive neoplasms [50]. Both studies found that using conventional immunosuppressants after an initial tumor does not raise the risk of recurrence or new cancer [51]. The decision to use TNF inhibitors may involve a multidisciplinary approach with oncologists, who will consider the current and recent activity of IBD along with alternative treatment options [14]. A meta-analysis revealed that the use of TNF inhibitors in IMID patients with a history of cancer was not linked to a higher risk of cancer recurrence or the development of new cancers [49]. Comparable results were found in a Spanish registry of IBD patients [52] and in a multicenter study conducted in the United States that examined IBD patients with a history of cancer [53]. In 2020, research was published on the risk of recurrent or new primary cancer among Danish patients with immune-mediated diseases (such as IBD, RA, or psoriasis) who had a history of cancer. This group accounted for 2.8% of CRC cases in these patients [54]. The study found no significant difference in the risk of recurrent or new primary cancer between exposed to TNF inhibitor and unexposed patients [54]. In addition, there are also long-term data on non-TNF inhibitors. The incidence of cancer among UC patients treated with vedolizumab (VDZ) was less than 1% [55]. The GEMINI long-term safety study similarly found no significant increase in the risk of cancer, suggesting that the gut-selective α4β7 integrin antibody, VDZ, demonstrated a favorable safety profile concerning cancer risk [56]. There are reassuring data also for ustekinumab (UST). In a retrospective study involving IBD patients with a prior history of cancer, UST did not lead to increased rates of new or recurring cancer [57]. Furthermore, safety data on UST at 5 years in CD and 4 years in UC have recently been published [58]. The final cumulative safety data for UST showed that the rates of key safety events, including malignancies, were comparable with placebo [58]. There is a lack of data regarding the risks associated with filgotinib and upadacitinib in patients with a history of cancer. Recently, safety data on long-term treatment with tofacitinib (up to 9.2 years of exposure to the drug) in UC patients did not show an increased risk of cancer [59]. The safety data for IL-23p19 inhibitors primarily come from the use of guselkumab and risankizumab in managing psoriasis. Both risankizumab [60] and guselkumab [61] have shown favorable safety profiles. On the other hand, no long-term safety data are currently available for mirikizumab. In summary, current evidence indicates that advanced therapies do not increase the risk of new or recurrent cancer in IBD patients [40,62].
6.2. Management of IBD Therapy in Patients with Current Cancer
Managing IBD patients with CRC or another active cancer is challenging. Similarly, the impact of cancer treatments on the progression of IBD must be considered, as active IBD can complicate treatment choices and influence potential outcomes [63]. In CRC, azathioprine and MTX have been shown to negatively affect both disease-free survival and overall survival [64]. For these reasons, immunosuppressants should be discontinued for IBD patients who are currently diagnosed with or experiencing active cancer until the cancer is controlled [40]. Conversely, there are no restrictions on stopping thiopurine therapy for patients with tumors or pre-neoplastic lesions assessed to have a low risk of recurrence and have been effectively removed either endoscopically or surgically. However, they should undergo vigilant monitoring for cancer surveillance [40]. Regarding TNF inhibitors, as per the most recent ECCO guidelines, they are deemed suitable for use in patients with IBD who also have concurrent cancer. However, there is a lack of specific data regarding different cancer types and the optimal timing of TNF inhibitors treatment [40]. Similarly, there is a lack of adequate data concerning the safety of VDZ, UST, or JAK inhibitors in patients with active malignancies [40,62].
7. Management of Chemotherapy and Radiation Therapy in IBD
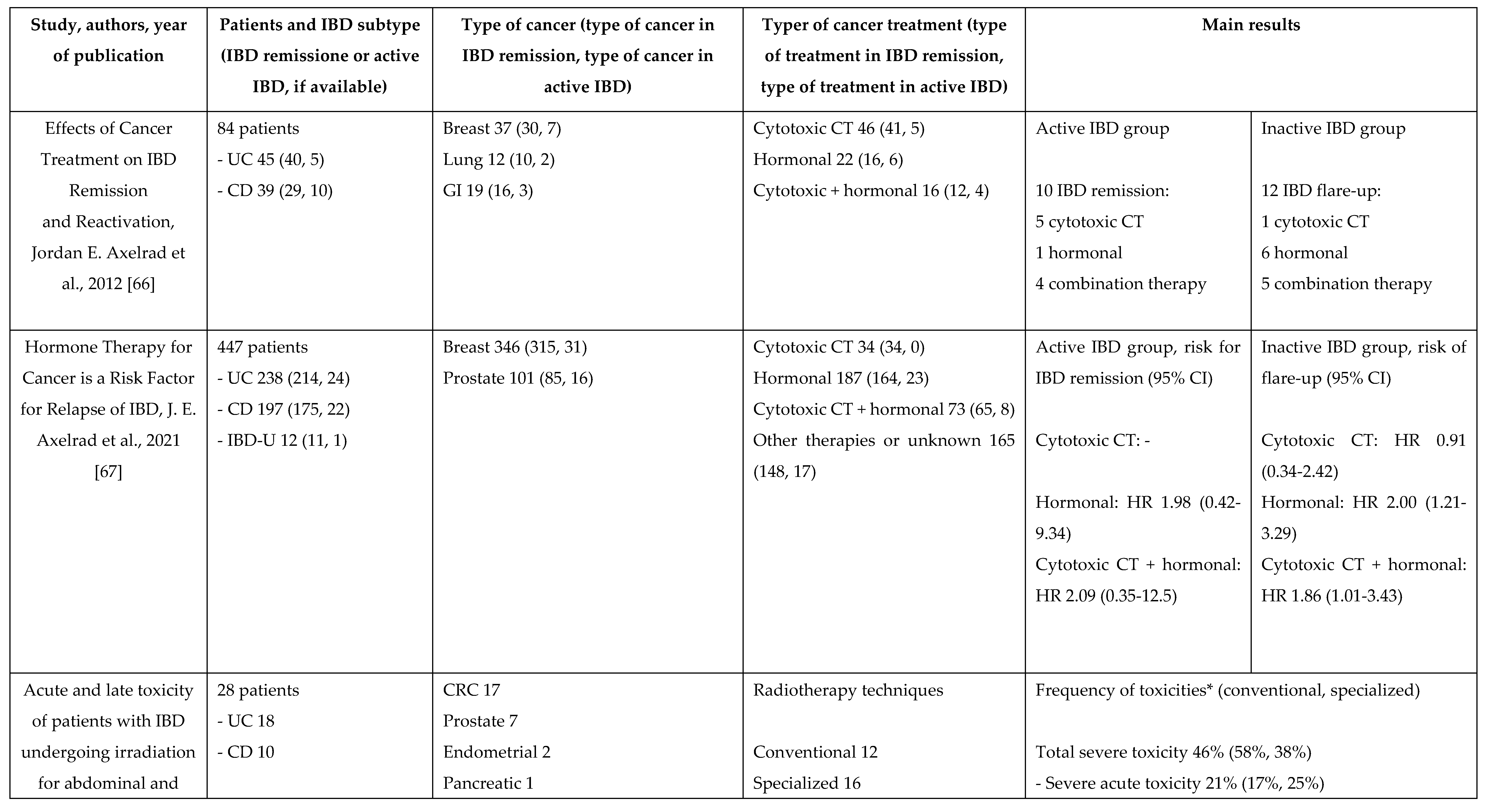
In clinical practice, it is crucial to prioritize cancer treatment in patients with IBD. Conversely, there is limited data available regarding the impact of cancer treatment on the progression of IBD [65,66] and not specific to CRC. In a retrospective study involving 84 patients with IBD who underwent cancer treatment for a solid malignant extraintestinal neoplasm, 66.7% of those with active IBD at the time of their cancer diagnosis achieved remission during their cancer treatment [66]. On the other hand, among IBD patients who were in clinical remission at the time of their cancer diagnosis, 17.4% experienced a flare of IBD following chemotherapy [66]. Cytotoxic chemotherapy may offer potential benefits for IBD patients in inducing or maintaining remission for solid tumors compared to those receiving only hormone therapy or a combination of cytotoxic chemotherapy and adjuvant hormone therapy [66]. In fact, cytotoxic drugs induce cell death or inhibit cell division in rapidly dividing cells, including T lymphocytes and malignant cells, resulting in antitumor and immunosuppressive effects [66]. Similar results were observed in another retrospective study involving 447 patients with IBD and concurrent breast cancer (78%) or prostate cancer (22%) [67]. Quiescent IBD was more likely to relapse in patients who received hormone therapies, either alone (HR 2.00, 95% CI 1.21-3.29) or combined (HR 1.86, 95% CI 1.01-3.43) with cytotoxic therapies [67]. Among the 34 patients who received only cytotoxic chemotherapy, 75% remained in IBD remission for up to 250 months [67]. Although few patients received cytotoxic therapies, there was a trend suggesting that those who underwent cancer treatment monotherapy with cytotoxic agents experienced some protection against IBD relapse [67]. A recent systematic review and meta-analysis, which included 33 studies with a total of 1,298 IBD patients undergoing cancer treatment, found that the overall incidence of IBD flares following cancer treatment was 30% [65]. These flares led to the use of systemic steroids in 25% of patients and biological therapies in 10%, while 14% of patients had to discontinue their cancer treatment [65]. (Table 2)
When administering chemotherapy to IBD patients, it is crucial to exercise caution when interpreting side effects like diarrhea [68]. It is important to determine whether the diarrhea is due to an IBD flare-up [69], a side effect of chemotherapy (such as with 5-fluorouracil and irinotecan) [70], an infectious cause (e.g., clostridium difficile and cytomegalovirus infection), or checkpoint-inhibitor induced colitis [71]. Immune checkpoint inhibitors (ICIs) target cytotoxic T-lymphocyte-associated protein-4 (CTLA-4) and programmed death-1/ligand (PD-1/PD-L1). ICIs often cause immune-related adverse events (irAEs), with gastrointestinal irAEs being among the most common and typically severe [71]. The risk of gastrointestinal toxicity that is 3 times higher in patients with IBD compared to those without IBD [62]. A modified Delphi process was established to reach a consensus on the management of ICI-induced colitis [72]. Oral corticosteroids are considered first-line treatment, with intravenous corticosteroids reserved for cases of severe toxicity [73]. For patients who do not respond to intravenous corticosteroids advanced therapy could be an off label option. In fact, in this context, infliximab (IFX) has been shown to be safe for use in patients with an active tumor and coexisting ICI-induced enterocolitis [74]. Some case series have also demonstrated the potential usefulness of VDZ [75] and tofacitinib [76] in this context.
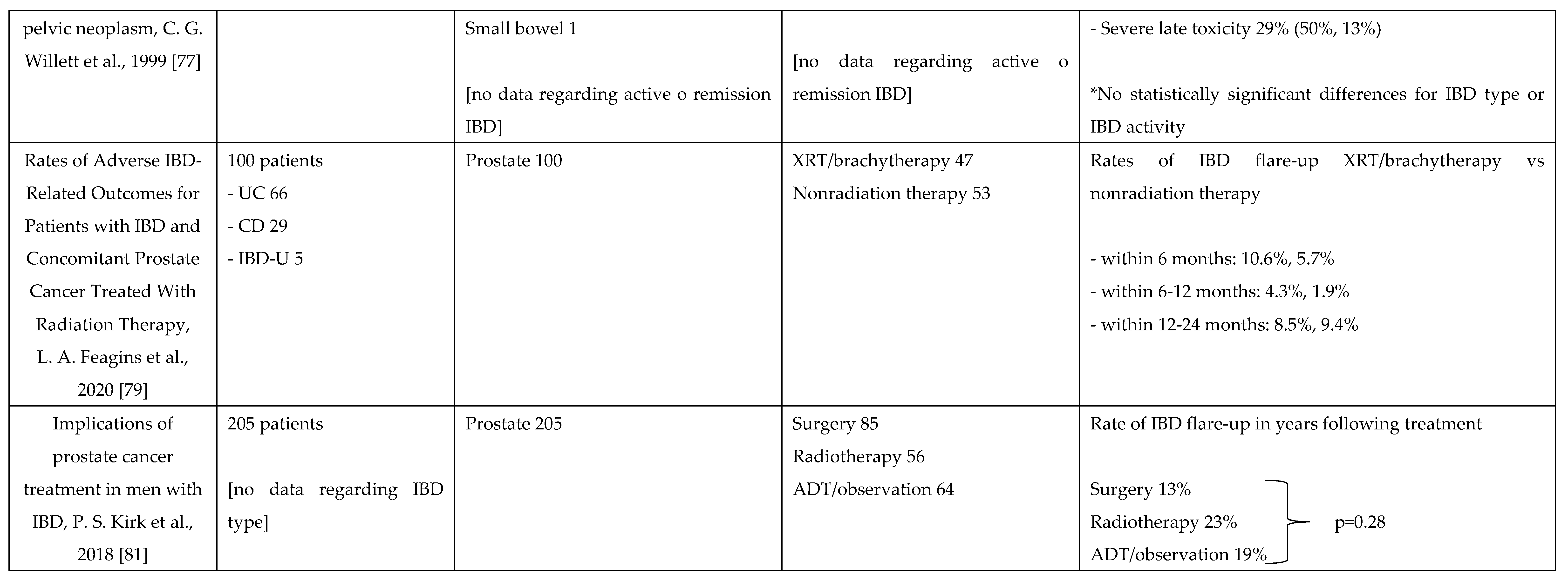
Data on the use of radiotherapy in patients with IBD is limited. Most oncologists avoid pelvic radiotherapy in IBD patients because of historically documented higher risks of toxicities and disease flares [77,78]. In a retrospective study of IBD patients with prostate cancer, 47% received radiotherapy. Among these patients, 10.6% experienced increased IBD flare-ups compared to 5.7% in those who did not receive radiotherapy, both within 6 months and 6–12 months after treatment (4.3% vs. 1.9%). [79]. Additionally, another study found that the 5-year survival rate for rectal cancers in patients with IBD who received pelvic radiation was similar to that of patients without prior IBD, with no increase in gastrointestinal toxicity observed [80]. Additionally, a systematic review showed that radiotherapy is generally safe for IBD patients, with acceptable toxicity profiles and a similar incidence of flares between those treated with radiotherapy and those who underwent surgery [81]. This indicates that radiotherapy is not an absolute contraindication for patients with IBD [78]. (Table 2)
8. Discussion
Patients with CD and UC have a higher risk of developing CRC compared to the general population [3]. Despite well-documented risk factors [5], the availability of guidelines for proper screening, surveillance, and management of pre-cancerous lesions [30,34,36], and advancements in endoscope fidelity and imaging techniques, its prognosis remains poorer than that of sporadic CRC [3]. Advancements in disease management, technology, and endoscopic quality have significantly altered our perception of precancerous lesions in IBD, bringing it closer to how we view dysplasia in the non-IBD population [34]. The practice of performing non-targeted biopsies and recommending colectomy for patients with low-grade or invisible dysplasia is increasingly being challenged. Instead, there is a growing preference for approaches that focus on meticulous inspection and targeted sampling of visible and subtle lesions using for example HD-WLE and DCE [34]. While endoscope fidelity and imaging techniques continue to advance, alternatives like the colon capsule are also developing. Capsule imaging is now employed to assess CD, although no publications currently address its use in detecting dysplasia in IBD [82]. Additionally, capsule imaging cannot perform biopsies, and it is well-documented that predicting IBD lesions histologically from visual images is suboptimal [30]. Artificial intelligence (AI)-based detection algorithms represent an exciting new frontier with the potential to assist endoscopists in identifying IBD dysplasia. AI capabilities have been tested for detecting colorectal neoplasia, but not specifically in patients with IBD [83]. In the future, AI could become an effective and safe tool for enhancing the quality of examinations in real time (e.g., sampling time, control of blind spots), potentially increasing the adenoma detection rate even in IBD patients [84]. Regarding patients with a previous or recent cancer diagnosis, there is limited data on the efficacy and safety of IBD therapies in patients with CRC. The recommendations in the latest ECCO guidelines for managing patients with IBD who have a history of or active oncological conditions are primarily based on data from other autoimmune diseases or various oncological situations [40,85,86]. For these reasons, the treatment of IBD patients following a cancer diagnosis necessitates a personalized approach. One of the most challenging and increasingly common areas of decision-making involves patients with a recent or active malignancy [40]. Therefore, if there is an active cancer, the primary focus should be on determining the appropriate cancer treatment under the guidance of a multidisciplinary team including oncologist, gastroenterologist, surgeon, radiologist [63]. Having a multidisciplinary team is crucial for effective therapy management, as it enhances the quality of care, patient satisfaction, and overall outcomes [87]. Additionally, the appropriate therapy must be tailored to the patient's characteristics, risk related to both IBD (such as disease severity, activity, choice of drug and risk of flare-up) and cancer (including risk of recurrence and time since cancer resolution) [62]. For these patients, it is also crucial to assess whether to start a new therapy or continue an existing IBD treatment in the event of a cancer diagnosis, especially if the IBD is active [40]. In the former scenario, selecting a treatment with the most favorable safety profile, including indirect data from non-IBD populations where relevant, is generally advisable. Regarding existing IBD treatments in the context of active cancer, it is recommended to withhold immunosuppressive therapies, particularly thiopurines [40]. For patients already receiving TNF inhibitors, treatment can be continued, if the IBD status risk assessment indicates a high risk of flare [40]. When patients experience flare-ups during active cancer treatment, other causes such as infections or diarrhea resulting from treatment with ICIs should first be ruled out [62]. After differential diagnosis, 5-ASA and corticosteroids are considered safe and can be used as first-line treatments for naive patients with clinically active IBD. If there is no response to corticosteroids or in patients already treated with advanced therapies, VDZ, UST or selective IL-23 inhibitors may be considered viable alternatives [62]. TNF inhibitors should be considered in patients with severe disease activity [62]. Therefore, prioritizing cancer survival, it is reasonable to continue cancer therapy with close monitoring for IBD using non-invasive tools such as intestinal ultrasound [88] and fecal calprotectin measurement [89].
9. Conclusions
Patients with IBD have a higher risk of developing CRC, making it crucial to identify risk factors and high-risk individuals to enhance their prognosis through targeted surveillance programs. The introduction of advanced imaging techniques has significantly enhanced the detection of precancerous lesions. In patients with IBD and concomitant active cancer or history of cancer is crucial to balance the benefit-risk ratio of IBD medications before making therapeutic decisions. Individualized approach involving multidisciplinary team and patient preferences is essential to achieve optimal disease control.
Author Contributions
SD conceived the study. JF, SB, and FD wrote the manuscript and created the tables. SD, MA, FF, TLP, LPB and AZ revised the manuscript. All the authors approved the final version of the manuscript.
Funding
No internal or external funding was received for this project.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Conflicts of Interest
J. Fanizza declares no conflict of interest. S. Bencardino declares no conflict of interest. F. D’Amico has served as a speaker for AbbVie, Sandoz, Janssen, Galapagos, Takeda, Ferring, Tillotts, and Omega Pharma; he has also served as advisory board member for Ferring, Galapagos, AbbVie, Janssen, and Nestlè. M. Allocca received consulting fees from Nikkiso Europe, Mundipharma, Janssen, Abbvie and Pfizer. F. Furfaro received consulting feesfrom Amgen and Abbvie and lecture fees from Janssen and Pfizer. A. Zilli declares no conflict of interest. T.L. Parigi declares no conflict of interest. L Peyrin-Biroulet declares consulting fees from AbbVie, Alimentiv, Alma Bio Therapeutics, Amgen, Applied Molecular Transport, Arena, Biogen, BMS, Celltrion, CONNECT Biopharm, Cytoki Pharma, Enthera, Ferring, Fresenius Kabi, Galapagos, Genentech, Gilead, Gossamer Bio, GSK, HAC-Pharma, IAG Image Analysis, Index Pharmaceuticals, Inotrem, Janssen, Lilly, Medac, Mopac, Morphic, MSD, Norgine, Novartis, OM Pharma, ONO Pharma, OSE Immunotherapeutics, Pandion Therapeutics, Pfizer, Prometheus, Protagonist, Roche, Sandoz, Takeda, Theravance, Thermo Fisher, Tigenix, Tillots, Viatris, Vifor, Ysopia, Abivax; he also declares grants from Takeda, Fresenius Kabi, Celltrion; he also has served as a speaker for Galapagos, AbbVie, Janssen, Genentech, Ferring, Tillots, Celltrion, Takeda, Pfizer, Sandoz, Biogen, MSD, Amgen, Vifor, Arena, Lilly, Gilead, Viatris, Medac. S. Danese has served as a speaker, consultant, and advisory board member for Schering-Plough, AbbVie, Actelion, Alphawasserman, AstraZeneca, Cellerix, Cosmo Pharmaceuticals, Ferring, Genentech, Grunenthal, Johnson and Johnson, Millenium Takeda, MSD, Nikkiso Europe, Novo Nordisk, Nycomed, Pfizer, Pharmacosmos, UCB Pharma, and Vifor.
References
- Porter, R.J.; Arends, M.J.; Churchhouse, A.M.D. , e S. Din, «Inflammatory Bowel Disease-Associated Colorectal Cancer: Translational Risks from Mechanisms to Medicines», J. Crohns Colitis, vol. 15, fasc. 12, pp. 2131–2141, dic. 2021. [CrossRef]
- Shah, S.C. e S. H. Itzkowitz, «Colorectal Cancer in Inflammatory Bowel Disease: Mechanisms and Management», Gastroenterology, vol. 162, fasc. 3, pp. 715-730.e3, mar. 2022. [CrossRef]
- Sato, Y.; Tsujinaka, S.; Miura, T.; Kitamura, Y.; Suzuki, H. , e C. Shibata, «Inflammatory Bowel Disease and Colorectal Cancer: Epidemiology, Etiology, Surveillance, and Management», Cancers, vol. 15, fasc. 16, p. 4154, ago. 2023. [CrossRef]
- Westwood, M.; et al. , «Faecal immunochemical tests (FIT) can help to rule out colorectal cancer in patients presenting in primary care with lower abdominal symptoms: a systematic review conducted to inform new NICE DG30 diagnostic guidance», BMC Med., vol. 15, fasc. 1, p. 189, dic. 2017. [CrossRef]
- Yalchin, M.; Baker, A.-M.; Graham, T.A. , e A. Hart, «Predicting Colorectal Cancer Occurrence in IBD», Cancers, vol. 13, fasc. 12, p. 2908, giu. 2021. [CrossRef]
- Mattar, M.C.; Lough, D.; Pishvaian, M.J. , e A. Charabaty, «Current management of inflammatory bowel disease and colorectal cancer», Gastrointest. Cancer Res. GCR, vol. 4, fasc. 2, pp. 53–61, mar. 2011.
- Ananthakrishnan, A.N.; et al. , «Colonoscopy Is Associated With a Reduced Risk for Colon Cancer and Mortality in Patients With Inflammatory Bowel Diseases», Clin. Gastroenterol. Hepatol., vol. 13, fasc. 2, pp. 322-329.e1, feb. 2015. [CrossRef]
- Beaugerie, L. e S. H. Itzkowitz, «Cancers Complicating Inflammatory Bowel Disease», N. Engl. J. Med., vol. 372, fasc. 15, pp. 1441–1452, apr. 2015. [CrossRef]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A. , e F. Bray, «Global patterns and trends in colorectal cancer incidence and mortality», Gut, vol. 66, fasc. 4, pp. 683–691, apr. 2017. [CrossRef]
- Wheat, C.L.; Clark-Snustad, K.; Devine, B.; Grembowski, D.; Thornton, T.A. , e C. W. Ko, «Worldwide Incidence of Colorectal Cancer, Leukemia, and Lymphoma in Inflammatory Bowel Disease: An Updated Systematic Review and Meta-Analysis», Gastroenterol. Res. Pract., vol. 2016, pp. 1–18, 2016. [CrossRef]
- Jess, T.; Gamborg, M.; Matzen, P.; Munkholm, P. , e T. I. A. Sorensen, «Increased Risk of Intestinal Cancer in Crohn’s Disease: A Meta-Analysis of Population-Based Cohort Studies», Am. J. Gastroenterol., vol. 100, fasc. 12, pp. 2724–2729, dic. 2005. [CrossRef]
- Jess, T.; Rungoe, C. , e L. Peyrin–Biroulet, «Risk of Colorectal Cancer in Patients With Ulcerative Colitis: A Meta-analysis of Population-Based Cohort Studies», Clin. Gastroenterol. Hepatol., vol. 10, fasc. 6, pp. 639–645, giu. 2012. [CrossRef]
- Lutgens, M.W.M.D.; Van Oijen, M.G.H.; Van Der Heijden, G.J.M.G.; Vleggaar, F.P.; Siersema, P.D. , e B. Oldenburg, «Declining Risk of Colorectal Cancer in Inflammatory Bowel Disease: An Updated Meta-analysis of Population-based Cohort Studies», Inflamm. Bowel Dis., vol. 19, fasc. 4, pp. 789–799, mar. 2013. [CrossRef]
- Annese, V.; et al. , «European Evidence-based Consensus: Inflammatory Bowel Disease and Malignancies», J. Crohns Colitis, vol. 9, fasc. 11, pp. 945–965, nov. 2015. [CrossRef]
- Eaden, J.A. , «The risk of colorectal cancer in ulcerative colitis: a meta-analysis», Gut, vol. 48, fasc. 4, pp. 526–535, apr. 2001. [CrossRef]
- Selinger, C.P.; et al. , «Long-term Follow-up Reveals Low Incidence of Colorectal Cancer, but Frequent Need for Resection, Among Australian Patients With Inflammatory Bowel Disease», Clin. Gastroenterol. Hepatol., vol. 12, fasc. 4, pp. 644–650, apr. 2014. [CrossRef]
- Qiu, X.; Ma, J.; Wang, K. , e H. Zhang, «Chemopreventive effects of 5-aminosalicylic acid on inflammatory bowel disease-associated colorectal cancer and dysplasia: a systematic review with meta-analysis», Oncotarget, vol. 8, fasc. 1, pp. 1031–1045, gen. 2017. [CrossRef]
- Samadder, N.J.; et al. , «Family History Associates With Increased Risk of Colorectal Cancer in Patients With Inflammatory Bowel Diseases», Clin. Gastroenterol. Hepatol., vol. 17, fasc. 9, pp. 1807-1813.e1, ago. 2019. [CrossRef]
- Nuako, K.; Ahlquist, D.; Mahoney, D.; Schaid, D.; Siems, D. , e N. Lindor, «Familial predisposition for colorectal cancer in chronic ulcerative colitis: A case-control study», Gastroenterology, vol. 115, fasc. 5, pp. 1079–1083, nov. 1998. [CrossRef]
- Wijnands, A.M.; De Jong, M.E.; Lutgens, M.W.M.D.; Hoentjen, F.; Elias, S.G. , e B. Oldenburg, «Prognostic Factors for Advanced Colorectal Neoplasia in Inflammatory Bowel Disease: Systematic Review and Meta-analysis», Gastroenterology, vol. 160, fasc. 5, pp. 1584–1598, apr. 2021. [CrossRef]
- Söderlund, S.; et al. , «Inflammatory Bowel Disease Confers a Lower Risk of Colorectal Cancer to Females Than to Males», Gastroenterology, vol. 138, fasc. 5, pp. 1697-1703.e2, mag. 2010. [CrossRef]
- Soetikno, R.M.; Lin, O.S.; Heidenreich, P.A.; Young, H.S. , e M. O. Blackstone, «Increased risk of colorectal neoplasia in patients with primary sclerosing cholangitis and ulcerative colitis: A meta-analysis», Gastrointest. Endosc., vol. 56, fasc. 1, pp. 48–54, lug. 2002. [CrossRef]
- Magro, F.; et al. , «Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders», J. Crohns Colitis, vol. 11, fasc. 6, pp. 649–670, giu. 2017. [CrossRef]
- Ekbom, A.; Helmick, C.; Zack, M. , e H.-O. Adami, «Ulcerative Colitis and Colorectal Cancer: A Population-Based Study», N. Engl. J. Med., vol. 323, fasc. 18, pp. 1228–1233, nov. 1990. [CrossRef]
- Rutter, M.; et al. , «Severity of inflammation is a risk factor for colorectal neoplasia in ulcerative colitis», Gastroenterology, vol. 126, fasc. 2, pp. 451–459, feb. 2004. [CrossRef]
- Gupta, R.B.; et al. , «Histologic Inflammation Is a Risk Factor for Progression to Colorectal Neoplasia in Ulcerative Colitis: A Cohort Study», Gastroenterology, vol. 133, fasc. 4, pp. 1099–1105, ott. 2007. [CrossRef]
- Rubin, D.T.; et al. , «Inflammation Is an Independent Risk Factor for Colonic Neoplasia in Patients With Ulcerative Colitis: A Case–Control Study», Clin. Gastroenterol. Hepatol., vol. 11, fasc. 12, pp. 1601-1608.e4, dic. 2013. [CrossRef]
- Flores, B.M.; O’Connor, A. , e A. C. Moss, «Impact of mucosal inflammation on risk of colorectal neoplasia in patients with ulcerative colitis: a systematic review and meta-analysis», Gastrointest. Endosc., vol. 86, fasc. 6, pp. 1006-1011.e8, dic. 2017. [CrossRef]
- Kirchgesner, J.; et al. , «Nancy Index Scores of Chronic Inflammatory Bowel Disease Activity Associate With Development of Colorectal Neoplasia», Clin. Gastroenterol. Hepatol., vol. 18, fasc. 1, pp. 150-157.e1, gen. 2020. [CrossRef]
- Coelho-Prabhu, N. e J. D. Lewis, «Update on Endoscopic Dysplasia Surveillance in Inflammatory Bowel Disease», Am. J. Gastroenterol., vol. 118, fasc. 10, pp. 1748–1755, ott. 2023. [CrossRef]
- Huguet, J.M.; et al. , «Colorectal cancer screening and surveillance in patients with inflammatory bowel disease in 2021», World J. Gastroenterol., vol. 28, fasc. 5, pp. 502–516, feb. 2022. [CrossRef]
- Vento, P.; Lepistö, A.; Kärkkäinen, P.; Ristimäki, A.; Haglund, C. , e H. J. Järvinen, «Risk of cancer in patients with chronic pouchitis after restorative proctocolectomy for ulcerative colitis», Colorectal Dis., vol. 13, fasc. 1, pp. 58–66, gen. 2011. [CrossRef]
- Derikx, L. A. A. P. . L. H. C. Nissen, L. J. T. Smits, B. Shen, e F. Hoentjen, «Risk of Neoplasia After Colectomy in Patients With Inflammatory Bowel Disease: A Systematic Review and Meta-analysis», Clin. Gastroenterol. Hepatol., vol. 14, fasc. 6, pp. 798-806.e20, giu. 2016. [CrossRef]
- Murthy, S.K.; Feuerstein, J.D.; Nguyen, G.C. , e F. S. Velayos, «AGA Clinical Practice Update on Endoscopic Surveillance and Management of Colorectal Dysplasia in Inflammatory Bowel Diseases: Expert Review», Gastroenterology, vol. 161, fasc. 3, pp. 1043-1051.e4, set. 2021. [CrossRef]
- Al Bakir, I.; Kabir, M.; Yalchin, M. , e A. Hart, «Optimising inflammatory bowel disease surveillance and dysplasia management—Where do we stand?», United Eur. Gastroenterol. J., vol. 10, fasc. 10, pp. 1054–1062, dic. 2022. [CrossRef]
- Laine, L.; et al. , «SCENIC International Consensus Statement on Surveillance and Management of Dysplasia in Inflammatory Bowel Disease», Gastroenterology, vol. 148, fasc. 3, pp. 639-651.e28, mar. 2015. [CrossRef]
- Rabinowitz, L.G.; Kumta, N.A. , e J. F. Marion, «Beyond the SCENIC route: updates in chromoendoscopy and dysplasia screening in patients with inflammatory bowel disease», Gastrointest. Endosc., vol. 95, fasc. 1, pp. 30–37, gen. 2022. [CrossRef]
- Lamb, C.A.; et al. , «British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults», Gut, vol. 68, fasc. Suppl 3, pp. s1–s106, dic. 2019. [CrossRef]
- Rubin, D.T.; Ananthakrishnan, A.N.; Siegel, C.A.; Sauer, B.G. , e M. D. Long, «ACG Clinical Guideline: Ulcerative Colitis in Adults», Am. J. Gastroenterol., vol. 114, fasc. 3, pp. 384–413, mar. 2019. [CrossRef]
- Gordon, H.; et al. , «ECCO Guidelines on Inflammatory Bowel Disease and Malignancies», J. Crohns Colitis, vol. 17, fasc. 6, pp. 827–854, giu. 2023. [CrossRef]
- Jang, J.-Y. , «The Past, Present, and Future of Image-Enhanced Endoscopy», Clin. Endosc., vol. 48, fasc. 6, pp. 466–475, nov. 2015. [CrossRef]
- Marion, J.F.; et al. , «Chromoendoscopy-Targeted Biopsies Are Superior to Standard Colonoscopic Surveillance for Detecting Dysplasia in Inflammatory Bowel Disease Patients: A Prospective Endoscopic Trial», Am. J. Gastroenterol., vol. 103, fasc. 9, pp. 2342–2349, set. 2008. [CrossRef]
- Bisschops, R.; et al. , «Chromoendoscopy versus narrow band imaging in UC: a prospective randomised controlled trial», Gut, vol. 67, fasc. 6, pp. 1087–1094, giu. 2018. [CrossRef]
- Moussata, D.; et al. , «Are random biopsies still useful for the detection of neoplasia in patients with IBD undergoing surveillance colonoscopy with chromoendoscopy?», Gut, p. gutjnl-2016-311892, gen. 2017. [CrossRef]
- Kandiah, K.; et al. , «Multicentre randomised controlled trial on virtual chromoendoscopy in the detection of neoplasia during colitis surveillance high-definition colonoscopy (the VIRTUOSO trial)», Gut, vol. 70, fasc. 9, pp. 1684–1690, set. 2021. [CrossRef]
- Beaugerie, L.; et al. , «Risk of new or recurrent cancer under immunosuppressive therapy in patients with IBD and previous cancer», Gut, vol. 63, fasc. 9, pp. 1416–1423, set. 2014. [CrossRef]
- Acuna, S.A.; Huang, J.W.; Dossa, F.; Shah, P.S.; Kim, S.J. , e N. N. Baxter, «Cancer recurrence after solid organ transplantation: A systematic review and meta-analysis», Transplant. Rev., vol. 31, fasc. 4, pp. 240–248, ott. 2017. [CrossRef]
- Bernheim, O.; Colombel, J.-F.; Ullman, T.A.; Laharie, D.; Beaugerie, L. , e S. H. Itzkowitz, «The management of immunosuppression in patients with inflammatory bowel disease and cancer», Gut, vol. 62, fasc. 11, pp. 1523–1528, nov. 2013. [CrossRef]
- Shelton, E.; et al. , «Cancer Recurrence Following Immune-Suppressive Therapies in Patients With Immune-Mediated Diseases: A Systematic Review and Meta-analysis», Gastroenterology, vol. 151, fasc. 1, pp. 97-109.e4, lug. 2016. [CrossRef]
- Poullenot, F.; et al. , «Comparative Risk of Incident Cancer in Patients with Inflammatory Bowel Disease with Prior Non-digestive Malignancy According to Immunomodulator: a Multicentre Cohort Study», J. Crohns Colitis, vol. 16, fasc. 10, pp. 1523–1530, nov. 2022. [CrossRef]
- Poullenot, F. e D. Laharie, «Management of Inflammatory Bowel Disease in Patients with Current or Past Malignancy», Cancers, vol. 15, fasc. 4, p. 1083, feb. 2023. [CrossRef]
- Mañosa, M.; et al. , «Immunomodulatory Therapy Does Not Increase the Risk of Cancer in Persons With Inflammatory Bowel Disease and a History of Extracolonic Cancers», Am. J. Gastroenterol., vol. 114, fasc. 5, pp. 771–776, mag. 2019. [CrossRef]
- Laredo, V.; García-Mateo, S.; Martínez-Domínguez, S.J.; De La Cruz, J.L.; Gargallo-Puyuelo, C.J. , e F. Gomollón, «Risk of Cancer in Patients with Inflammatory Bowel Diseases and Keys for Patient Management», Cancers, vol. 15, fasc. 3, p. 871, gen. 2023. [CrossRef]
- Waljee, A.K.; et al. , «Anti-tumour necrosis factor-α therapy and recurrent or new primary cancers in patients with inflammatory bowel disease, rheumatoid arthritis, or psoriasis and previous cancer in Denmark: a nationwide, population-based cohort study», Lancet Gastroenterol. Hepatol., vol. 5, fasc. 3, pp. 276–284, mar. 2020. [CrossRef]
- Cohen, R.D.; Bhayat, F.; Blake, A. , e S. Travis, «The Safety Profile of Vedolizumab in Ulcerative Colitis and Crohn’s Disease: 4 Years of Global Post-marketing Data», J. Crohns Colitis, vol. 14, fasc. 2, pp. 192–204, feb. 2020. [CrossRef]
- Card, T.; Ungaro, R.; Bhayat, F.; Blake, A.; Hantsbarger, G. , e S. Travis, «Vedolizumab use is not associated with increased malignancy incidence: GEMINI LTS study results and post-marketing data», Aliment. Pharmacol. Ther., vol. 51, fasc. 1, pp. 149–157, gen. 2020. [CrossRef]
- Hong, S.J.; et al. , «Ustekinumab and Vedolizumab Are Not Associated With Subsequent Cancer in IBD Patients with Prior Malignancy», Inflamm. Bowel Dis., vol. 28, fasc. 12, pp. 1826–1832, dic. 2022. [CrossRef]
- Ghosh, S.; et al. , «Safety of Ustekinumab in Inflammatory Bowel Disease: Pooled Safety Analysis Through 5 Years in Crohn’s Disease and 4 Years in Ulcerative Colitis», J. Crohns Colitis, p. jjae013, feb. 2024. [CrossRef]
- Panés, J.; et al. , «Analysis of tofacitinib safety in ulcerative colitis from the completed global clinical developmental program up to 9.2 years of drug exposure», United Eur. Gastroenterol. J., p. ueg2.12584, mag. 2024. [CrossRef]
- Ferrante, M.; et al. , «Long-Term Safety and Efficacy of Risankizumab Treatment in Patients with Crohn’s Disease: Results from the Phase 2 Open-Label Extension Study», J. Crohns Colitis, vol. 15, fasc. 12, pp. 2001–2010, dic. 2021. [CrossRef]
- Blauvelt, A.; et al. , «Malignancy rates through 5 years of follow-up in patients with moderate-to-severe psoriasis treated with guselkumab: Pooled results from the VOYAGE 1 and VOYAGE 2 trials», J. Am. Acad. Dermatol., vol. 89, fasc. 2, pp. 274–282, ago. 2023. [CrossRef]
- Wetwittayakhlang, P.; Tselekouni, P.; Al-Jabri, R.; Bessissow, T. , e P. L. Lakatos, «The Optimal Management of Inflammatory Bowel Disease in Patients with Cancer», J. Clin. Med., vol. 12, fasc. 6, p. 2432, mar. 2023. [CrossRef]
- Sebastian, S. e S. Neilaj, «Practical guidance for the management of inflammatory bowel disease in patients with cancer. Which treatment?», Ther. Adv. Gastroenterol., vol. 12, p. 175628481881729, gen. 2019. [CrossRef]
- Khoury, W.; Lavery, I.C. , e R. P. Kiran, «Effects of Chronic Immunosuppression on Long-term Oncologic Outcomes for Colorectal Cancer Patients Undergoing Surgery», Ann. Surg., vol. 253, fasc. 2, pp. 323–327, feb. 2011. [CrossRef]
- Grimsdottir, S.; Attauabi, M.; Dahl, E.K.; Burisch, J. , e J. B. Seidelin, «Systematic Review with Meta-analysis: The Impact of Cancer Treatments on the Disease Activity of Inflammatory Bowel Diseases», J. Crohns Colitis, vol. 17, fasc. 7, pp. 1139–1153, lug. 2023. [CrossRef]
- Axelrad, J.E.; Fowler, S.A.; Friedman, S.; Ananthakrishnan, A.N. , e V. Yajnik, «Effects of Cancer Treatment on Inflammatory Bowel Disease Remission and Reactivation», Clin. Gastroenterol. Hepatol., vol. 10, fasc. 9, pp. 1021-1027.e1, set. 2012. [CrossRef]
- Axelrad, J.E.; et al. , «Hormone Therapy for Cancer Is a Risk Factor for Relapse of Inflammatory Bowel Diseases», Clin. Gastroenterol. Hepatol., vol. 18, fasc. 4, pp. 872-880.e1, apr. 2020. [CrossRef]
- Conceição, D.; Saraiva, M.R.; Rosa, I. , e I. Claro, «Inflammatory Bowel Disease Treatment in Cancer Patients—A Comprehensive Review», Cancers, vol. 15, fasc. 12, p. 3130, giu. 2023. [CrossRef]
- O’Reilly, M.; Mellotte, G.; Ryan, B. , e A. O’Connor, «Gastrointestinal side effects of cancer treatments», Ther. Adv. Chronic Dis., vol. 11, p. 204062232097035, gen. 2020. [CrossRef]
- Stein, A. W. Voigt, e K. Jordan, «Review: Chemotherapy-induced diarrhea: pathophysiology, frequency and guideline-based management», Ther. Adv. Med. Oncol., vol. 2, fasc. 1, pp. 51–63, gen. 2010. [CrossRef]
- Soularue, E.; et al. , «Enterocolitis due to immune checkpoint inhibitors: a systematic review», Gut, vol. 67, fasc. 11, pp. 2056–2067, nov. 2018. [CrossRef]
- Desmedt, V.; et al. , «Position statement on the management of the immune checkpoint inhibitor-induced colitis via multidisciplinary modified Delphi consensus», Eur. J. Cancer, vol. 187, pp. 36–57, lug. 2023. [CrossRef]
- Haanen, J.; et al. , «Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up», Ann. Oncol., vol. 33, fasc. 12, pp. 1217–1238, dic. 2022. [CrossRef]
- Marthey, L.; et al. , «Cancer Immunotherapy with Anti-CTLA-4 Monoclonal Antibodies Induces an Inflammatory Bowel Disease», J. Crohns Colitis, vol. 10, fasc. 4, pp. 395–401, apr. 2016. [CrossRef]
- Bergqvist, V.; et al. , «Vedolizumab treatment for immune checkpoint inhibitor-induced enterocolitis», Cancer Immunol. Immunother., vol. 66, fasc. 5, pp. 581–592, mag. 2017. [CrossRef]
- Bishu, S.; Melia, J.; Sharfman, W.; Lao, C.D.; Fecher, L.A. , e P. D. R. Higgins, «Efficacy and Outcome of Tofacitinib in Immune checkpoint Inhibitor Colitis», Gastroenterology, vol. 160, fasc. 3, pp. 932-934.e3, feb. 2021. [CrossRef]
- Willett, C.G.; et al. , «Acute and late toxicity of patients with inflammatory bowel disease undergoing irradiation for abdominal and pelvic neoplasms», Int. J. Radiat. Oncol., vol. 46, fasc. 4, pp. 995–998, mar. 2000. [CrossRef]
- Bodofsky, S.; et al. , «Inflammatory bowel disease-associated malignancies and considerations for radiation impacting bowel: a scoping review», J. Gastrointest. Oncol., vol. 13, fasc. 5, pp. 2565–2582, ott. 2022. [CrossRef]
- Feagins, L.A.; et al. , «Rates of Adverse IBD-Related Outcomes for Patients With IBD and Concomitant Prostate Cancer Treated With Radiation Therapy», Inflamm. Bowel Dis., vol. 26, fasc. 5, pp. 728–733, apr. 2020. [CrossRef]
- Green, S.; Stock, R.G. , e A. J. Greenstein, «Rectal cancer and inflammatory bowel disease: natural history and implications for radiation therapy», Int. J. Radiat. Oncol., vol. 44, fasc. 4, pp. 835–840, lug. 1999. [CrossRef]
- Kirk, P.S.; et al. , «Implications of Prostate Cancer Treatment in Men With Inflammatory Bowel Disease», Urology, vol. 104, pp. 131–136, giu. 2017. [CrossRef]
- Brodersen, J.B.; Knudsen, T.; Kjeldsen, J.; Juel, M.A.; Rafaelsen, S.R. , e M. D. Jensen, «Diagnostic accuracy of pan-enteric capsule endoscopy and magnetic resonance enterocolonography in suspected Crohn’s disease», United Eur. Gastroenterol. J., vol. 10, fasc. 9, pp. 973–982, nov. 2022. [CrossRef]
- Solitano, V.; et al. , «Artificial Endoscopy and Inflammatory Bowel Disease: Welcome to the Future», J. Clin. Med., vol. 11, fasc. 3, p. 569, gen. 2022. [CrossRef]
- Da Rio, L.; et al. , «Artificial intelligence and inflammatory bowel disease: Where are we going?», World J. Gastroenterol., vol. 29, fasc. 3, pp. 508–520, gen. 2023. [CrossRef]
- Onuora, S. , «Cancer recurrence risk not increased by DMARDs», Nat. Rev. Rheumatol., vol. 17, fasc. 12, pp. 707–707, dic. 2021. [CrossRef]
- Sepriano, A.; et al. , «Safety of synthetic and biological DMARDs: a systematic literature review informing the 2019 update of the EULAR recommendations for the management of rheumatoid arthritis», Ann. Rheum. Dis., vol. 79, fasc. 6, pp. 760–770, giu. 2020. [CrossRef]
- Lee, C.K. e G. Y. Melmed, «Multidisciplinary Team-Based Approaches to IBD Management: How Might “One-Stop Shopping” Work for Complex IBD Care?», Am. J. Gastroenterol., vol. 112, fasc. 6, pp. 825–827, giu. 2017. [CrossRef]
- Helwig, U.; et al. , «Transmural Response and Transmural Healing Defined by Intestinal Ultrasound: New Potential Therapeutic Targets?», J. Crohns Colitis, vol. 16, fasc. 1, pp. 57–67, gen. 2022. [CrossRef]
- D’Amico, F.; et al. , «International consensus on methodological issues in standardization of fecal calprotectin measurement in inflammatory bowel diseases», United Eur. Gastroenterol. J., vol. 9, fasc. 4, pp. 451–460, mag. 2021. [CrossRef]
- DʼHaens, G.; et al. , «Fecal calprotectin is a surrogate marker for endoscopic lesions in inflammatory bowel disease»:, Inflamm. Bowel Dis., vol. 18, fasc. 12, pp. 2218–2224, dic. 2012. [CrossRef]
- Theede, K.; Holck, S.; Ibsen, P.; Ladelund, S.; Nordgaard-Lassen, I. , e A. M. Nielsen, «Level of Fecal Calprotectin Correlates With Endoscopic and Histologic Inflammation and Identifies Patients With Mucosal Healing in Ulcerative Colitis», Clin. Gastroenterol. Hepatol., vol. 13, fasc. 11, pp. 1929-1936.e1, nov. 2015. [CrossRef]
- D’Amico, F.; Nancey, S.; Danese, S. , e L. Peyrin-Biroulet, «A Practical Guide for Faecal Calprotectin Measurement: Myths and Realities», J. Crohns Colitis, vol. 15, fasc. 1, pp. 152–161, gen. 2021. [CrossRef]
Figure 1.
Surveillance strategies recommended for patients with IBD based on risk stratification. CD: Crohn’s disease; CRC: colorectal cancer; FDR: first-degree relative; PSC: primary sclerosing cholangitis.
Figure 1.
Surveillance strategies recommended for patients with IBD based on risk stratification. CD: Crohn’s disease; CRC: colorectal cancer; FDR: first-degree relative; PSC: primary sclerosing cholangitis.
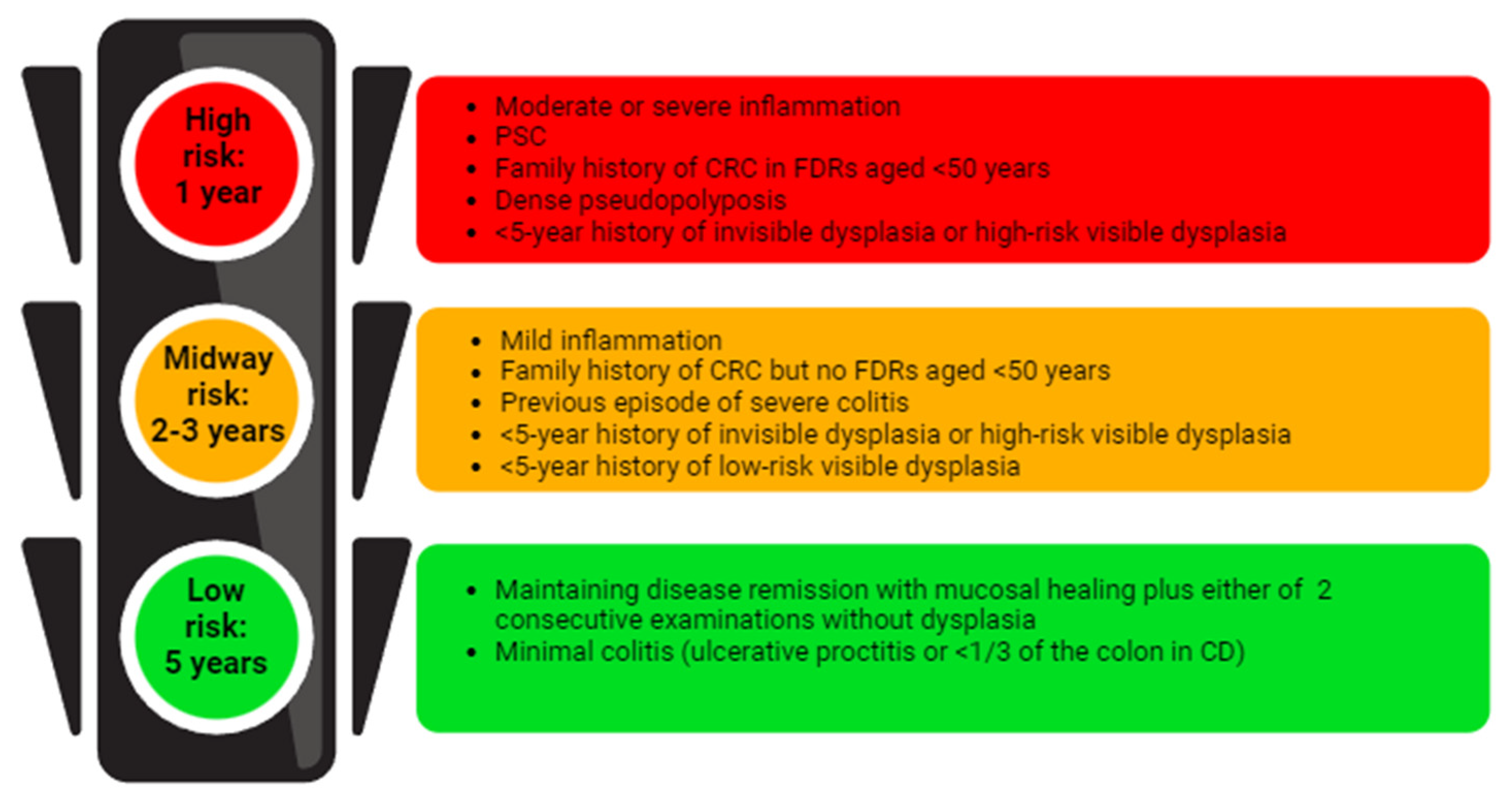

Table 1.
Overview of recommendations from international organizations for dysplasia surveillance in patients with IBD. ACG, American College of Gastroenterology; AGA, American Gastroenterological Association; BSG, British Society of Gastroenterology; CE, chromoendoscopy; ECCO, European Crohn’s and Colitis Organization; HD, high definition; SD, standard definition; WLE, white light endoscopy; NBI, narrow band imaging; PSC, primary sclerosing cholangitis; VCE, virtual chromoendoscopy.
Table 1.
Overview of recommendations from international organizations for dysplasia surveillance in patients with IBD. ACG, American College of Gastroenterology; AGA, American Gastroenterological Association; BSG, British Society of Gastroenterology; CE, chromoendoscopy; ECCO, European Crohn’s and Colitis Organization; HD, high definition; SD, standard definition; WLE, white light endoscopy; NBI, narrow band imaging; PSC, primary sclerosing cholangitis; VCE, virtual chromoendoscopy.
| Guideline (year of publication) | Type of endoscopic surveillance | Random or targeted biopsies |
| SCENIC Consensus (2015) [36] | HD recommended If SD, dye-CE recommended If HD, dye-CE suggested |
No consensus |
| SCENIC commentary (2022) [37] | HD-WLE, dye-CE, or VCE | Random limited to highest-risk groups only (PSC, prior dysplasia, atrophic scarred colon, ongoing active inflammation) |
| ECCO Guideline (2017) [23] | HD recommended | Random if WL Targeted only if dye-CE |
| ECCO Guideline (2023) [40] | HD-WLE, dye-CE, or VCE | Targeted biopsies Random in high-risk (PSC or history of dysplasia) |
| ACG Clinical Guideline (2019) [39] | If SD, dye-CE recommended If HD, dye-CE or VCE recommended |
No recommendation |
| AGA Clinical Practice update (2021) [34] |
HD recommended Dye-CE should be considered VCE acceptable alternative if HD |
Random if WL only and all patients with high risk (PSC or history of dysplasia) Targeted if dye-CE or VCE |
| BSG Guideline (2019) [38] | HD recommended If SD, dye-CE recommended If HD, dye-CE suggested NBI not suggested |
Targeted recommended |
Table 2.
Main results of some studies concerning the pharmacological and non-pharmacological treatment of active cancer in patients with IBD. IBD, inflammatory bowel disease; GI, gastrointestinal; UC, ulcerative colitis; CD, Crohn disease; IBD-U, IBD-unclassified; CT, chemotherapy; HR, hazard ratio; XRT, radiotherapy; ADT, androgen deprivation therapy.
Table 2.
Main results of some studies concerning the pharmacological and non-pharmacological treatment of active cancer in patients with IBD. IBD, inflammatory bowel disease; GI, gastrointestinal; UC, ulcerative colitis; CD, Crohn disease; IBD-U, IBD-unclassified; CT, chemotherapy; HR, hazard ratio; XRT, radiotherapy; ADT, androgen deprivation therapy.
 |
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



