Submitted:
31 July 2024
Posted:
01 August 2024
You are already at the latest version
Abstract
Abstract: Coal production in mining areas frequently results in a host of negative effects that spread to the neighboring populations, affecting their general well-being and health. This qualitative investigation, which sought to understand how communities living close to coal mines evaluated the effects of mining on their health and well-being, was motivated by the dearth of literature in the province of Limpopo. Eighty-one people in three villages close to the mine provided us with data. Results show that locals' opinions of the social, psychological, and bodily effects of coal mining are worrisome. There were themes that showed how several factors, such as noise pollution, land degradation, and pollution of the air and water, negatively affect physical well-being. Stress, anxiety, and terror were common as a result of safety worries and uncertain livelihoods that harmed mental health. Social wellbeing suffered as a result of the mining industry's negative effects on social cohesiveness, economic inequality, and stigma. Participants also noted that important environmental issues impacting community health and well-being include socioeconomic disparities, air and water pollution, occupational health and safety concerns, and social and cultural disturbances. This study emphasizes how urgently extensive research is needed to validate and
Keywords:
Coal mining
; Community voice
; Health impacts
; Perceived
; Well-being
1. Introduction
Coal, also called fossil fuel [1], which has been used for heating and cooking since cavemen, is derived from open-cast mines (53%), ground bord-and-pillar operations (40%), stopping (4%), and longwall mining (3%) [2], and it remains South Africa’s (SA) primary energy source at 70%. Commercial coal mining activities in SA started in 1870 and increased between 1879 and 1889 to support the gold and diamond mining endeavors [3]. With other countries such as India getting coal from SA, exploration of new coal fields is currently active, involving Black Economic Empowerment (BEE), leading to the establishment of over 20 junior coal mining and exploration companies in South Africa. The concern is that coal mining activities produce huge tons of mineral waste, causing ambient (outdoor) air pollution and poor air quality.
According to the World Health Organization (WHO) [4], in 2019, approximately 99% of the world's population resided in areas that did not meet the WHO's air quality guidelines. Thus, breathing air contains high levels of pollutants. According to the WHO [5], low- and middle-income countries (LMIC) are suffering from the highest exposures to ambient air pollution, with nitrogen dioxide (NO2) being one of the main pollutants. NO2 is known to cause health issues such as asthma, lung inflammation, and reduced lung function. Thus, particles with a diameter of 10 microns or less (<PM 10) can penetrate and lodge deep inside the lungs, causing irritation and inflammation and damaging the lining of the respiratory tract [6; 7]. Particles with a diameter of 2.5 microns or less have more health-damaging effects. These particles penetrate the lung barrier and enter the blood system, affecting all major organs of the body and increasing the risk of heart and respiratory diseases, as well as lung cancer and strokes [8]. The WHO [4] established an association between prenatal exposure to high NO2 levels of air pollution and developmental delay at age three, as well as psychological and behavioral problems later on, including symptoms of attention deficit hyperactivity disorder (ADHD), anxiety, and depression. Ambient (outdoor) air pollution resulted in 4.2 million premature deaths worldwide in 2019, with 89% of such premature deaths occurring in low- and middle-income countries [5], which is equivalent to 1·1 million deaths across Africa, with the majority of deaths due to non-communicable diseases. Thus, Khan & Ghouri [9] assert that polluted air can cause a shorter lifespan.
Burning coal in power plants leaves behind a gray powder-like substance known as coal ash, which is an additional concern. Coal-fired power plants produce more than 100 million tons of coal ash and other waste products. Coal-fired power plants reuse about a third of this waste, often in concrete, while they store the remainder in landfills, abandoned mines, and hazardous, highly toxic ponds. Unlined ponds or pits store the majority of coal ash. All coal ash contains concentrated amounts of toxic elements, including arsenic, lead, and mercury. Over time, heavy metals in the ash can escape into nearby waterways and contaminate drinking water. Coal ash exposure increases the risk of cancer, heart damage, reproductive issues, neurological disorders, and other serious health conditions.
Another coal mining concern is water pollution through acid mine drainage, which occurs when certain substances (typically iron sulfide, FeS2, or fool's gold) oxidize after exposure to air and water. Runoff can change the pH of nearby streams to the same level as vinegar or battery acid. Highly acidic water contains heavy toxic metals such as arsenic, lead, and mercury, which contaminate nearby rivers, lakes, and aquifers. Skin irritation, kidney damage, and neurological diseases are some of the effects of acid mine drainage on human health. Acid rain, on the other hand, causes respiratory problems such as bronchitis, pneumonia, and permanent lung damage.
In response to the notion that policy actions in energy, transport and waste management, etc., significantly reduces health risks among populations, the National Environmental Management: Air Quality Act 39 [10] prescribes that MECs of Health in Provinces through a gazette, and municipalities in terms of a by-law, should identify substances or mixtures of substances in ambient air which, through ambient concentrations, bioaccumulation, deposition, or in any other way, present a threat to health, well-being or the environment in the municipality or which the municipality reasonably believes present such a threat; and establish local standards for emissions from point, non-point or mobile sources; and require persons falling within specified categories to prepare and submit related pollution prevention plans. The above should be based on the national ambient air quality standards [11]. According to Schedule 2 of the National Environmental Management Act 39 [11], the national ambient air quality standards for NO2 in one hour are 200 micrograms/m3 and 40 micrograms/m3 annually, whereas for particulate matter (PM10), they are 75 micrograms/m3 in 24 hours and 40 micrograms/m3 annually.
Problem Statement
AQMesh, which is the organization monitoring air quality around mining facilities in South Africa, highlights that the South African average air quality (real-time PM2.5 and PM10 air pollution) level of 49 micrograms/m3 on July 26, 2024, 12:12 [12], is above the national air quality annual standard of 40 micrograms/m3 [13]. A CREA (14) study in Limpopo also looked at how air pollution (PM2.5, NO2, SO2) from the Lephalale Coal Mine (LCM) and nearby sources (Medupi and Matimba power stations and the Grootgeluk coal mine) will affect people's health over the 35-year project lifecycle and how this extra health burden will affect the South African economy. The CREA [14] study detected exceedances in all air quality standards, i.e., PM10 (daily and annual), NO2 (hourly), SO2 (hourly and daily), and PM2.5 (daily and annual), which are not only restricted to nearby communities. For instance, when considering emissions from the LCM mine and existing sources, over 20 million residents exceed the standard value for daily average PM2.5 concentrations. Emissions from the LCM mine and existing major sources exceed the daily standard average PM10 concentrations for over 500,000 inhabitants. The standard value for When considering emissions from the LCM IPP and existing sources, over 2 million residents exceed the standard value for hourly average. According to CREA [14], such excesses increase the risk of a wide range of health outcomes for local residents, including preterm birth (3%) and premature mortality (2%) as well as health risks such as chronic bronchitis in both adults (17%) and children (12%).
Statistics SA [15] highlights that in 2017, Limpopo was the province of usual residence for 10.2% (n = 40685) of the deceased, with tuberculosis (TB) ranking as the No. 1 cause of death at 6.4%, followed by diabetes mellitus (5.7%), cerebrovascular disease (5%), other forms of heart disease (4.9%), HIV (4.8%), hypertension diseases (4.5%), influenza and pneumonia (4.2%), and chronic lower respiratory diseases (2.9%). According to Statsa [15], Capricorn district had the highest number (n = 12, 206) of deaths in 2017, followed by Mopani (8,961), Greater Sekhukhune (8,632), Vhembe (7931), and Waterberg (5,977). The proportion of deaths in Limpopo province attributed to environmental risks associated with mining activities remains unclear. This lack of certainty regarding the predisposing factors underlying causes of deaths misdirects program preventive interventions in the province. Prüss-Ustün et al. [16] looked at scientific evidence from around the world and found that 8.2 million deaths were caused by noncommunicable diseases in 2017. This was followed by 2.5 million deaths caused by infectious, parasitic, neonatal, and nutritional diseases. In addition, the WHO [13] estimates that in 2019, some 37% of outdoor air pollution-related premature deaths were due to ischaemic heart disease and stroke, 18% and 23% of deaths were due to chronic obstructive pulmonary disease and acute lower respiratory infections, respectively, and 11% of deaths were due to cancer within the respiratory tract.
Rationale
Studies investigating the perceived health impacts of coal mining activities in Limpopo Province are necessary, given the current development of four projects that cumulatively add 426 Mt to the existing reserve base, accounting for more than 100% of South Africa's current coal reserves. This suggests that coal mining in Limpopo could potentially continue well beyond the current average mining period [17]. Previous studies on this phenomenon include Nephalama and Muzerengi [18], who focused on the influence of coal mining on groundwater quality at Masisi village, whereas Momoh et al. [19] covered the potential implications of mine dust on human health at Mukula Mine in Limpopo Province. Additional studies looked at miners' health and safety [20]; Chipa [21] focused on mining corporate social responsibility and sustainable communities' livelihoods post mine closure. These studies did not give community voice to the environmental health impacts perceived by residents in close proximity to mines. It is important to understand the impact of coal mining activities on the health and well-being of residents in close proximity to coal mines to inform intervention programs that mitigate the effects of mining pollution. This study adds the voice of communities in close proximity to coal mines in Limpopo Province.
Significance of the Study
The purpose of this study is to assess the physical health of individuals and community members living near a coal mine. This may help government policymakers amend the regulations (MPRDA, NEMA, and NEM: AQA) and requirements for mining activities. This study may also compel the Department of Health to conduct additional studies on the cumulative health problems of residents around coal mines. We hope the department will then construct more health facilities for communities surrounding mining areas.
Research Purpose
To investigate community members’ perceptions about the health and well-being impacts of coal mining.
Research objectives
- To explore perceived impact of exposure to mining activities on the physical, mental and social well-being of community members in close proximity to a mine.
- To describe perceived factors associated with the health and well-being of community members exposed to mine activities.
Definition of terms
Perception: The view or prospect of anything such as biological, psychodynamic, behavioural, cognitive, and humanistic [22] In this study, perception refers to the view and perceptions of the community about their physical, mental, and social health and well-being.
Health impacts: Health impacts have been defined by WHO as a combination of procedures, methods, and tools by which a policy, programme or project may be judged as to its potential effects on the health of a population [23]. In this study, health impacts refer to negative and positive changes in community’s physical, mental, and social health resulting from exposure to mining activities around the study area.
Well-being: Well-being is the experience of health, happiness, and prosperity. In this study, well-being means physical, mental and social wellness.
Village: A small community or group of houses and associated buildings, larger than a hamlet and smaller than a town, with a population ranging from a few hundreds to few thousands, often located in rural areas, villages are normally permanent, with fixed dwellings [24]. In this study, a village refers to the Mutele area in Masisi.
2. Materials and Methods
We described the methodology below using the consolidated criteria for reporting qualitative research [COREQ] [25].
Research approach
The qualitative exploratory design was adopted to uncover the perceptions of health and well-being among community members living near a mine in the Limpopo Province.
Research design
The study was exploratory research, and perspectives and experiences of community members concerning the effects of a nearby coal mine on their health and well-being were probed through direct observations and interactions during one-on-one interviews.
Study setting.
This study was conducted at Mutele Village, a community situated near a coal mine called Tshikondeni. The village is within the magisterial district of Mutale in the Limpopo Province. Mutele Village comprises sub-villages called Mukomawabane, Tshivaloni, Sanari, Thondoni, Tshifunguduwe and Bileni. These sub-villages are approximately 15- 20 km away from the mine. All the sub-villages depend on one community health care clinic called Sanari Community Health Clinic.
Mutele Village is in Musina Local Municipality, which forms part of Vhembe District Municipality in the Limpopo Province. It is approximately 123 km from Thohoyandou and 70km from Musina and is characterised by scattered households. The road links are of poor quality except the roads to Tshikondeni Mine. The total area is 3.886 km2 while the total population is 91, 870 [26] with a population density of 24/km2. The dominant language is Tshivenda at about 96.8 % and others at 3.2 %.
Tshikondeni is a coal mine with both open-cast and underground mine and is owned by Exxaro Coal which is managed by Exxaro. It started operations in 1984 with only an underground mine and later added the open cast seam in 2003. Most general workers are from the surrounding communities. There is high rate of male employees at the mine compared to females. Some females work as domestic workers for the staff of Tshikondeni who resides at Tshikondeni Eco-village.
Study population and sampling
The study population comprised communities near the Tshikondeni Coal Mine. The communities around Tshikondeni Coal Mine include Tshivaloni, Mukomawabane, Bileni, Sanari, and Thondoni. However, the study specifically targeted community members residing in Mukomawabane, Bileni, and Mutele B. These three sub-villages were selected for their proximity to the coal mine (5km radius). The total area encompassing these communities is 3.886 km², with a combined population of 91,870 (26). The inclusion criteria for participants were individuals aged between 18 and 80 years. Participants were interviewed at their preferred location be it their home or workplace to ensure their comfort.
A non-probability purposive sampling was utilized to select the population. The study employed multistage sampling, encompassing the sub-villages, households, and the study participants. The selection of participants was based on the total population counts for sub-villages as reported by STATSSA [26]. Sub-villages near the mine were purposefully selected. The area of interest includes eight (8) sub-villages, out of which only three (3) were purposefully sampled prioritizing those in close proximity to the coal mine. The sub-villages selected include Bileni, Mukomawamabe, and Mutele B. Furthermore, a random sampling was also employed to select households within the three chosen sub-villages for inclusion in the study. To accomplish this, the number of all households were written on small pieces of paper and placed in a bowl. The researcher then randomly drew a piece of paper from the bowl to determine which household would be included in the study.
Data collection method
In this study, data was collected using two primary methods: audio-recorded semi-structured interviews and direct observation. A carefully designed semi-structured interview guide, served as the cornerstone for data collection. This tool was instrumental in facilitating discussions, enabling the researcher to delve into the lived experiences, perceptions, and conditions of life in the villages adjacent to the mine. One-on-one interviews were conducted to capture rich, in-depth information about the participants' health, well-being, and life circumstances. Recognizing the linguistic preferences and needs of the study population, most of the interview questions were translated into Tshivenda, the primary language spoken in the target area. This consideration ensured that participants could express themselves fully and comfortably, enhancing the quality and authenticity of the data collected. The process of data collection was iterative, with the researcher continuing to conduct interviews until reaching a point of data saturation. Data saturation, a key concept in qualitative research, indicated that no new information or themes were emerging from the interviews, thereby suggesting that the collected data sufficiently represented the phenomena under investigation.
Data management and analysis
Data management and analysis procedures were followed to analyse the collected data. Thematic analysis was conducted, involving categorizing, manipulating, ordering, and summarizing the data to derive meaningful insights. The data were transcribed from audiotapes with a focus on accuracy and quality. Then, underlying concepts were identified to develop category themes. These themes were used to code the data consistently.
Trustworthiness measures
In carrying out a study, it was important to ensure that data and findings represented the truth about the community’s perceptions on their health and well-being due to exposure to the selected coal mine activities. Thus, the four criteria widely used to appraise the trustworthiness of qualitative research, namely credibility, dependability, confirmability, and transferability were used to ensure rigour of inquiry. Prolonged engagements, persistent observations, member debrieifing and peer debriefing were used as strategies to ensure credibility of the study findings. To ensure transferability, this detailed report of the methodology guides future researchers to reproduce the study in similar settings, ensuring transferability. To ensure dependability, an enquiry audit twas performed by an external examiner appointed by the university for examination purposes. In addition, stepwise replication was done by an independent coder and the findings were compared to inform adjustments in coding. Reflxivity in terms of the researcher own feeling, actions and conflicts during data collection and analysis ensured confirmability.
3. Results
3.1 Demographic Information
This study collected data from eighty-one (81) participants from three villages in close proximity to Tshikondeni mine. Most participants (40.7% n=33) were from Ha-Mukomawabane; 32.1%, n=26; and 27.2%, n=22 of participants was from Ha-Mutele B and Bileni villages, respectively. Regarding age, the majority of participants (51.9%) were adults, i.e., aged between 36 and 60 years old. Youths only constituted a third of the study sample, with the elderly (over 61 years) comprising almost 15%. Most participants were women, who constituted almost 60% of the sample; 53.1% were single, 6.2% were cohabiting, 3.3% were married, and 7.4% were widowed. Concerning the level of education, more than half, i.e., 66.7% of the participants, had attained a secondary level education, with only 7.4 without a known education level and less than 5% with tertiary education. Only a fifth of the sample had primary education. Finally, the majority (51.9%) of the participants were unemployed, with only 35.8% reporting being employed. More than 10% of the sampled participants were unemployed (refer Appendix A: Table 2 for details).
3.2. Themes and Sub-Themes
Two themes emerged from thematic analysis of the data (see table 3), encapsulating the community's perceptions of the impacts of coal mining and the factors associated with the health and well-being of individuals exposed to such activities. Theme 1 is about the community's perceived impacts, covering aspects of physical, mental, and social well-being. Theme 2 explores the various factors perceived by the community as influential, including environmental, occupational health and safety, socio-economic, and social and cultural factors.
This section describes the community perceptions regarding the impact of coal mining activities on physical, mental, social well-being.
Physical Well-being
Results revealed that local communities think coal mining around their settlements exposes them to air pollution. As indicated in Figure 1, some participants believe that "coal mining operations often generate dust and release pollutants into the air”. Dust and several air pollutants associated with coal mining are detrimental to human physical well-being. According to one respondent coal mining leads
"…to respiratory problems such as asthma, bronchitis, and other respiratory diseases among community members" Participant #61.
Besides air pollution that is detrimental to their health, it was further revealed that coal mining may contaminate water sources. For instance, one participant said:
"Mining activities can contaminate water sources by releasing pollutants and chemicals used in the mining process, affecting drinking water quality and causing health issues" Participant # 2.
In addition to water contamination, some participants indicated that coal mining activities cause noise and vibrations. One participant said:
"Mining operations produce significant noise and vibrations, which can disrupt sleep patterns, cause stress, and potentially lead to hearing loss…" Participant #70.
As such, coal mining is disturbing the local communities` sleep patterns and potentially exposing them to shock due to blasting and tremors. On the same note, the land degradation associated with coal mining affects the local communities' physical well-being. For instance, one of the research participants lamented:
"Coal mining involves the excavation and removal of large amounts of soil and rock, leading to land degradation, soil erosion, and loss of agricultural productivity, which can impact food security and physical well-being" Participant #24.
Thus, in short, they revealed that local communities` physical well-being is perceived to be affected by coal mining in four unique ways, i.e., land degradation, noise and vibrations, air and water pollution, water contamination and outbreak of diseases.
Mental Well-being
Coal mining, according to study participants causes stress and anxiety among them. One participant lamented:
"Living near coal mines can cause stress and anxiety … due to concerns about the health impacts of mining activities, environmental degradation, and the uncertainty of the future" Participant #38.
Moreover, coal mining is perceived to be associated with fear and safety concerns among the local communities. For example, one participant said:
"Mining operations can bring safety risks, such as accidents, explosions, or collapses, creating fear and anxiety within the community" Participant #25.
Accidents, explosions, and collapse threaten the locals by living in perpetual fear. In addition, the results revealed that local communities in coal mining areas are mentally traumatised by the uncertainty associated with the loss of livelihoods. As indicated in Figure 2, some people were sceptical. A participant said:
"…coal mining activities may result in the displacement of local communities or the loss of traditional livelihoods, leading to helplessness, depression…" Participant # 15 and 77.
Social Well-being
Results revealed that coal mining affects the social well-being of the local communities. As indicated in Figure 3, coal mining is perceived to have the potential to disrupt the social fabric of communities by causing displacement, loss of traditional lands, and fragmentation of community cohesion leading to social tensions and conflicts. Besides its association with displacements, loss of traditional lands and fragmentation, coal mining has been perceived to increase inequality. For instance, one participant said:
"…. mining activities often create economic disparities within communities, as some individuals benefit from employment opportunities while others may be left without access to resources or opportunities, exacerbating social inequalities" Participants #15 and 44.
Some participants indicated that coal mining sometimes causes social stigma. As presented in Figure 3, communities living near coal mines may experience negative perceptions and social stigma associated with the mining industry, leading to isolation and marginalisation by society. As a result, this dents their social well-being and affects their overall health.
THEME 2: Factors perceived by the community as associated with the health and well-being of individuals exposed to coal mining
Environmental Factors
Results revealed that the local communities living near coal mining activities perceived that coal mining is associated with several health and wellness factors. Firstly, it emerged that coal mining compromises air quality. One participant said:
“Coal mining exposes us to dust, particulate matter and harmful emissions”. Participant # 16
This exposure can lead to respiratory and other health-related issues. Air pollution is detrimental to human health. Besides air pollution, coal mining is also associated with water pollution. As shown in Figure 4, one participant indicated that
"… mining activities can contaminate water sources leading to waterborne diseases and other health risks" Respondents #36.
Water quality is essential for safe and clean drinking water and maintaining good health but coal mining is reported to disturb this within local communities. Moreover, it was revealed that environmentally, coal mining is associated with severe noise and vibrations. As shown in Figure 4, mining operations generate noise and vibrations that can disrupt sleep patterns, cause stress, and harm mental health.
Occupational Health and Safety Factors
Coal mining is perceived to be associated with occupational hazards. For instance, one participant indicated that;
"… miners and workers directly involved in mining activities face specific occupational hazards, such as exposure to harmful substances, accidents, injuries, and occupational diseases, Participant #53.
These occupational hazard risks can also indirectly impact the wider community. Additionally, coal mining exposes workers to deplorable working conditions. As indicated in Figure 5, most mining working conditions within mines, including factors like poor ventilation, lack of proper safety equipment, and long working hours, can contribute to health issues and stress among workers. Thus, as far as coal mining is concerned, local communities perceived several occupational health and safety concerns that threaten their overall health.
Socio-economic Factors
Interviews conducted in the three selected villages revealed that although coal mining is associated with serious health concerns, it is also linked to several positive benefits to the local communities. For instance, some participants contend that coal mining can provide job opportunities and income for community members, contributing to improved economic well-being and social development. As shown in Figure 6, coal mining activities can also adversely affect local communities by creating economic disparities. One participant said:
"… mining can also lead to economic disparities within communities, where some individuals benefit from employment and business opportunities, while others may be left without access to resources or face negative economic consequences". Participant #25
In addition, some respondents indicated the association of coal mining with community infrastructure development. For instance, one participant said:
"The presence of mining activities can lead to the development of infrastructure, such as roads, schools, and healthcare facilities, which can positively impact the well-being of community members". Participant #26.
Social and Cultural Factors
Results also revealed that if correctly managed, coal mining may contribute to local economic development through enhanced community engagement. As indicated in Figure 7, some community members thought that the level of community participation and engagement in decision-making processes related to mining activities could influence the well-being of community members. Two participants said:
“…when communities are involved and their concerns are addressed, it can enhance their sense of empowerment and well-being and stimulate local economic development.” Participants #22 and 47.
Besides local economic development, coal mining has the potential to enhance social cohesion.
One participant said:
"… mining activities can affect social relationships and community cohesion. Positive social connections and support systems within the community contribute to better mental and social well-being". Participant #27.
On the same note, some participants contended that coal mining may disrupt or impact cultural heritage sites and practices, which can have psychological and social implications for community members. This has a direct bearing on the mental health of the local communities that are in areas where there is coal mining.
Figure 8 below summarizes the overall human health impact of coal mining activities as perceived by communities.
4. Discussion
The study findings revealed that participants' perceptions of living near coal mining activities vary widely. The participants shared certain perceptions about health and diseases that can lead to respiratory problems such as asthma and bronchitis, among others. One of the studies highlighted the issue of health and disease, which showed an increasing trend in disease prevalence with increasing exposure. The study reported that TB was positively and significantly associated with dust exposures (p < 0.01 and p < 0.05) [27].
The association and relationship of dust with TB have been well reported and documented in studies done on the gold mining industry and black coal miners, which have been reported to have an increased risk of TB due to mining activities. This could also be due to a variety of factors, including the types of jobs they have for historical reasons, their educational level, and their poor socio-economic background. Du Toit et al. [28] concluded that pulmonary tuberculosis was constant over the five-year period based on limited autopsy data. However, the SAMODD data base shows a decline for the year 2006, but overall, it indicates an increase in the number of tuberculosis cases in Mpumalanga coal mines.
The opening of a surface mine coincided with a substantial increase in medical visits for asthma, according to another study on coal surface mining. Du Toit et al. [28] also reported a significantly higher occurrence of respiratory symptoms among children exposed to coal dust. Contrary to the studies conducted in 1994, there was no relationship between surface coal mining and children’s respiratory health [29; 30]. In Turkey, Yapicci et al. [31] measured blood vessels for cadmium and lead in children living near coal mining activity and found levels substantially higher than in other urbanized areas of Turkey. Cadmium levels exceeded the World Health Organization risk limits [32].
Chronic inhalation of coal dust affects the lungs directly [33], and studies carried out on coal miners show devastating data on lung health. Percet et al. [34] concluded that studies carried out on coal miners showed devastating data on lung health. Silicosis, mixed dust pneumoconiosis, chronic obstructive airway disease, including emphysema, and chronic bronchitis are a spectrum of diseases triggered by coal inhalation.
Kurt et al. [35] note that individuals indirectly exposed to coal may develop chronic obstructive pulmonary disease (COPD), asthma, lung cancer, and respiratory infections. These may occur when a variety of environmental air pollutants are inhaled. Children and the elderly are particularly susceptible. Also, epidemiological studies conducted in urban centers and rural areas have provided evidence that environmental air pollution is strongly associated with increased risks of coronary artery disease, heart failure, stroke, and cardiovascular morbidity and mortality [36]. Cardiovascular diseases are associated with air and water contaminated with toxicants found in coal and coal processing.
Air pollution from coal mining has an impact on humans' reproductive functions. Environmental pollutants induce a deficiency in gametogenesis, resulting in reduced reproductive capacities in exposed populations [37]. Van der Zee et. al. [38] concluded that air contamination is an important environmental risk factor for lung diseases, and the smoking association may increase lung damage. Hendryx et. al. [36] said that left unchecked, climate change will have profound impacts on global population health. These impacts include an increase in infectious illness, heart-related morbidity and mortality, strains on health care and social services, and reduced labor capacity.
Mental Health and Well-Being
Living near coal mines is often associated with stress and anxiety, primarily due to concerns about the health impacts and the uncertainty of the future. Coal mining has also been linked to fear and safety concerns among local communities. Other studies demonstrated the impacts of coal seam gas (CSG) mining on mental factors that can affect an individual beyond their physical health. At the development stage, CSG mining has implications for the social determinants of health and well-being in a broader context (direct and indirect impacts) [39].
Environmental, Social and Cultural
This study also revealed that mining can lead to economic disparities within communities, with some individuals benefiting from employment and business opportunities, while others may lack access to resources or face negative economic consequences. Mactaggart et. al. [40] confirmed that mining activities can lead to major population growth, create job opportunities, and improve lifestyles.
There is a great interrelationship between the environmental and health impacts of coal mining on residents in close proximity to such mines. Such impacts include water pollution, air pollution, deforestation, and the loss of livelihoods. The results of the study showed that coal mine exposure can lead to respiratory and other health-related issues. Air pollution is detrimental to human health. Besides air pollution, coal mining is also associated with water pollution.
Muzerengi and Nephalama [41] sampled 22 boreholes around Tshikondeni Coal Mine, and the samples showed a high concentration of TDS. These concentrations were below the WHO [5] and South African [11] threshold concentrations. High TDS concentrations lead to saline water, making it unsuitable for drinking [42]. Munzerengi and Nephalama [41] concluded that the overall groundwater quality in the 6–10 km radius of Tshikondeni mine is not pristine, and they do not recommend it for domestic and agricultural direct use.
Chemicals used during coal processing or coal cleaning after extraction are primarily responsible for the detrimental impacts of coal mining on both surface and ground water. Local facilities carry out this process using proprietary formulas to eliminate impurities and non-combustible materials [32]. Contaminated water from mining sites or processing facilities has clearly impacted private drinking wells. The Environmental Protection Agency's Safe Drinking Water conducted an examination between 2001 and 2009 on areas with mining activities and non-mining areas, revealing an average of 73 Safe Drinking Water information system violations in mining areas, compared to 10 violations in non-mining areas [32].
Apart from water contamination, air quality studies in mining environments outside of Appalachia have shown that surface mining creates localized air pollution. Researchers have also observed air pollution around coal mines in Germany [43], Australia [44], and Columbia [45]. We discussed in detail the physical health impacts of air pollution due to mining activities. Coal mining areas in China and Turkey have observed soil contamination secondary to air deposition [46]. Surface mines may experience air pollution due to various factors such as deforestation, the release of rock and soil to coal seams, the use of chemicals in explosives, wind erosion, dust from haul roads, the movement and processing of coal, and the heavy use of diesel-burning equipment such as draglines, trucks, and trains.
Mining areas in regional Queensland, Australia, experienced significant changes to the built environment and natural landscape, including the rapid growth of takeaway and fast-food outlets to meet population demands [40]. Coal seam gas mining utilizes a large amount of land due to the multitude of dispersed gas wells, difficult road access, pipelines, processing plants, and tailing dams. According to the Australian government, concentrated community centres have raised concerns about traffic, volume of activity, and destruction of the natural environment, which has impacted community well-being. The public health implications of the marked increase in these services are concerning, given the higher rates of overweight and obesity in rural areas compared to major cities. According to Smith et al. [47], the prevalence of obesity among young Australian adults increases with the availability of fast food and takeaway outlets.
5. Conclusions
This study has provided comprehensive insights into the perceived impacts of coal mining on the health and well-being of individuals residing near the Tshikondeni Coal Mine. These perceived physical, mental, and social dimensions of well-being, as well as the determining factors alluded to here, are, though not factual, supported by literature in other settings. We need to conduct a follow-up study to scientifically validate these perceptions, measuring the concentrations of mineral wastes in various sources like river water, boreholes, garden crops, etc., and describing the prevalence of disease conditions to guide health promotion intervention programs for communities near Limpopo coal mines. By adopting holistic approaches that prioritize community wellbeing and sustainability, we can work towards mitigating the health impacts of coal mining and fostering healthier, more resilient communities for generations to come.
Limitations
Most participants were reluctant to participate as they were not sure of the outcome of the study, and their perceptions could not be included in the study. Tshikondeni eco-village was excluded from the study because only mine workers live in that village. Their opinions and perceptions could have given a more significant insight about the impacts associated with coal mining. Since coal miners were excluded in this study, occupational health impacts were not thoroughly investigated. Due to the small villages around the mine; the educational level of participants and age group hindered the researcher from getting an in-depth perception about the impacts caused by Tshikondeni Coal Mine.
Author Contributions
Conceptualization, T. and TG.; methodology, T.; validation, TG; formal analysis T. investigation, T., resources, T.; data curation, T.; writing—original draft preparation, T and TG.; writing—review and editing, TG.; supervision, TG. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Human and Clinical Trials Research Ethics Committee (HCTREC) (protocol codeFHS/22/PH/11/0610; 10/09/2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
Heartfelt gratitude goes to the communities residing near Tshikondeni Coal Mine for their willingness to participate and share their invaluable insights. This study would not have been possible without their cooperation and contributions.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A

Table 2.
Demographic characteristics of participants.
| Participant 刘Identity | Name of the village | Age | Sex/Gender | Marital 刘Status | Level 刘Education | of | Employment 刘status |
|---|---|---|---|---|---|---|---|
| 1 | Ha-Mukomawabane | 52 | Male | Married | Grade 12 | Unemployed | |
| 2 | Ha-Mukomawabane | 40 | Male | Married | Grade 10 | Unemployed | |
| 3 | Ha-Mukomawabane | 62 | Female | Widowed | No education | Pension | |
| 4 | Ha-Mukomawabane | 39 | Female | Single | Grade 10 | Unemployed | |
| 5 | Ha-Mukomawabane | 68 | Male | Married | Standard 6 | Pension | |
| 6 | Ha-Mukomawabane | 83 | Female | Married | No education | Unemployed | |
| 7 | Ha-Mukomawabane | 25 | Female | Single | Grade 12 | Employed | |
| 8 | Ha-Mukomawabane | 43 | Male | Cohabitation | Grade 9 | Employed | |
| 9 | Ha-Mukomawabane | 24 | Female | Single | Grade 9 | Employed | |
| 10 | Ha-Mukomawabane | 56 | Female | Married | Grade 7 | Unemployed | |
| 11 | Ha-Mukomawabane | 30 | Female | Single | Grade 7 | Unemployed | |
| 12 | Ha-Mukomawabane | 67 | Male | Married | No education | Unemployed | |
| 13 | Ha-Mukomawabane | 57 | Female | Married | Grade 9 | Unemployed | |
| 14 | Ha-Mukomawabane | 28 | Female | Single | Tertiary | Unemployed | |
| 15 | Ha-Mukomawabane | 24 | Female | Single | Tertiary | Employed | |
| 16 | Ha-Mukomawabane | 36 | Male | Married | Grade 11 | Employed | |
| 17 | Ha-Mukomawabane | 50 | Male | Single | Grade 11 | Employed | |
| 18 | Ha-Mukomawabane | 40 | Female | Cohabitation | Grade 9 | Employed | |
| 19 | Ha-Mukomawabane | 36 | Male | Single | Grade 11 | Employed | |
| 20 | Ha-Mukomawabane | 31 | Female | Single | Grade 10 | Unemployed | |
| 21 | Ha-Mukomawabane | 59 | Female | Married | Grade 5 | Pension | |
| 22 | Ha-Mukomawabane | 47 | Female | Married | Grade 12 | Unemployed | |
| 23 | Ha-Mukomawabane | 66 | Female | Married | Grade 8 | Pension | |
| 24 | Ha-Mukomawabane | 25 | Female | Cohabitation | Grade 11 | Unemployed | |
| 25 | Ha-Mukomawabane | 29 | Female | Single | Grade 11 | Unemployed | |
| 26 | Ha-Mukomawabane | 19 | Male | Single | Grade 10 | Unemployed | |
| 27 | Bileni | 30 | Female | Single | Grade 10 | Employed |
28 Bileni 59 Female Single Standard 4 Unemployed
| 29 Bileni | 41 | Female | Single | Grade 11 | Employed |
| 30 Bileni | 76 | Male | Married | Standard 6 | Unemployed |
| 31 Bileni | 38 | Male | Single | Grade 8 | Employed |
| 32 Bileni | 25 | Male | Single | Grade 11 | Unemployed |
| 33 Bileni | 29 | Female | Married | Grade 9 | Employed |
| 34 Bileni | 48 | Male | Married | Standard 5 | Unemployed |
| 35 Bileni | 36 | Female | Single | Grade 10 | Employed |
| 36 Bileni | 23 | Female | Married | Grade 11 | Unemployed |
| 37 Bileni | 46 | Female | Single | Grade 8 | Unemployed |
| 38 Bileni | 36 | Female | Married | Grade 12 | Employed |
| 39 Bileni | 30 | Female | Single | Grade 12 | Employed |
| 40 Bileni | 72 | Male | Married | Standard 1 | Pension |
| 41 Bileni | 33 | Female | Married | Grade 10 | Employed |
| 42 Bileni | 31 | Female | Single | Grade 9 | Employed |
| 43 Bileni | 29 | Male | Cohabitation | Grade 11 | Employed |
| 44 Bileni | 56 | Male | Married | Standard 4 | Unemployed |
| 45 Bileni | 53 | Female | Single | Standard 4 | Employed |
| 46 Bileni | Uknown | Male | Widowed | No education | Pension |
| 47 Bileni | 18 | Female | Single | Grade 10 | Unemployed |
| 48 Bileni | 35 | Female | Cohabitation | Grade 10 | Employed |
| 49 Ha-Mutete B | 38 | Male | Single | Grade 12 | Unemployed |
| 50 Ha-Mutete B | 65 | Male | Single | Standard 3 | Pension |
| 51 Ha-Mutete B | 55 | Male | Single | Grade 11 | Unemployed |
| 52 Ha-Mutete B | 42 | Female | Married | Grade 11 | Unemployed |
| 53 Ha-Mutete B | 44 | Female | Married | Grade 12 | Employed |
| 54 Ha-Mutete B | 48 | Male | Widowed | Standard 7 | Employed |
| 55 Ha-Mutete B | 54 | Female | Single | Standard 4 | Employed |
| 56 Ha-Mutete B | 53 | Female | Married | Standard 10 | Unemployed |
| 57 Ha-Mutete B | 26 | Male | Single | Tertiary | Unemployed |
| 58 Ha-Mutete B | 38 | Male | Married | Standard 6 | Unemployed |
59 Ha-Mutete B 33 Male Single Grade 11 Employed
| 60 Ha-Mutete B | 41 | Female | Single | Grade 12 | Employed |
| 61 Ha-Mutete B | 61 | Female | Married | Standard 4 | Unemployed |
| 62 Ha-Mutete B | 35 | Female | Single | Grade 10 | Unemployed |
| 63 Ha-Mutete B | 45 | Male | Single | Grade 11 | Unemployed |
| 64 Ha-Mutete B | 23 | Male | Single | Grade 12 | Unemployed |
| 65 Ha-Mutete B | 47 | Male | Married | Grade 10 | Unemployed |
| 66 Ha-Mutete B | 60 | Female | Single | Standard 10 | Unemployed |
| 67 Ha-Mutete B | 99 | Female | Widowed | No education | Pension |
| 68 Ha-Mutete B | 23 | Female | Single | Grade 12 | Unemployed |
| 69 Ha-Mutete B | 44 | Female | Single | Grade 11 | Unemployed |
| 70 Ha-Mutete B | 54 | Male | Single | Grade 10 | Unemployed |
| 71 Ha-Mutete B | 53 | Female | Widowed | Grade 12 | Employed |
| 72 Ha-Mutete B | 60 | Female | Married | Grade 10 | Pension |
| 73 Ha-Mutete B | 79 | Female | Widowed | No education | Pension |
| 74 Ha-Mutete B | 21 | Male | Single | Grade 12 | Unemployed |
| 75 Ha-Mukomawabane | 40 | Female | Single | Grade 8 | Unemployed |
| 76 Ha-Mukomawabane | 53 | Female | Married | Grade 11 | Employed |
| 77 Ha-Mukomawabane | 28 | Male | Single | Tertiary | Unemployed |
| 78 Ha-Mukomawabane | 43 | Male | Single | Grade 10 | Unemployed |
| 79 Ha-Mukomawabane | 42 | Male | Single | Grade 10 | Employed |
| 80 Ha-Mukomawabane | 42 | Male | Single | Grade 10 | Employed |
81 Ha-Mukomawabane 29 Female Single Grade 11 Unemployed
Appendix B
All appendix sections must be cited in the main text. In the appendices, Figures, Tables, etc. should be labeled starting with “A”—e.g., Figure A1, Figure A2, etc.
References
- Elem. Fossil energy study guide: Coal, 2024 https://www.energy.gov/sites/prod/files/Elem_Coal_Studyguide.pdf.
- CSIR. Introduction to South African coal mining and exploration, 2015. https://researchspace.csir.co.za/dspace/bitstream/handle/10204/8153/McGill_2015.pdf?sequence=1#:~:text=Coal%20was%20discovered%20in%20KwaZulu,the%20Eastern%20Cape%2C%20in%2018701.
- Environmental Monitoring Group, 2010. The Social and Environmental Consequences of Coal Mining in South Africa: a case study, 2010. https://www.bothends.org/uploaded_files/uploadlibraryitem/1case_study_South_Africa_updated.pdf.
- World Health Organization. How air pollution is affecting our health, 2022. https://www.who.int/news-room/spotlight/how-air-pollution-is-destroying-our-health.
- World Health Organisation. Ambient (outdoor) air pollution, 2023. https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health.
- Chiluba, B. C. ‘Critical review of Dust in the Mining Environment: A focus on Workers and Community Health’. University of Zambia, 2018. School of Health Sciences. [CrossRef]
- Michael, H. ‘The public health impacts of surface coal mining’. Department of Applied Health Science. Indiana University, 2015. Bloomington. IN 47405, USA.
- Ncube, V. ‘South Africa’s “Deadly Air” Case Highlights Health Risks from Coal’. Environmental and Human Rights, 2021. South Africa.
- Khan, M.A.; Ghouri, A.M. Environmental pollution: its effects on life and its remedies. Researcher World: Journal of Arts, Science & Commerce 2011, 2, 276–285. [Google Scholar]
- South Africa. National Environment Management: Air Quality Act (no. 39 of 2004). https://www.dffe.gov.za/sites/default/files/legislations/nema_amendment_act39.pdf.
- South Africa. National Environmental Management: Air Quality Act: National Ambient air quality standards, 2009. https://www.gov.za/sites/default/files/gcis_document/201409/328161210.pdf.
- AQI. South Africa air quality Index real-time PM2.5, PM10 air pollution level 26 July 2024, 12:00pm. https://www.aqi.in/dashboard/south-africa.
- AQMesh. AQMesh monitors air quality around mining facilities in South Africa, 2020. https://www.aqmesh.com/news/aqmesh-monitors-air-quality-around-mining-facilities-in-south-africa/.
- Centre for Research on Energy and Clean Air (CREA). Air quality, health, and economic impacts of a new coal mine and power plant in Lephalale, 2023. https://energyandcleanair.org/publication/air-quality-health-and-economic-impacts-of-a-new-coal-mine-and-power-plant-in-lephalale/.
- Statistics South Africa. Mortality and causes of death in South Africa: Findings from death notification, 2020. https://www.statssa.gov.za/publications/P03093/P030932017.pdf.
- Prüss-Ustün, A.; Wolf, J.; Corvalán, C.; Neville, T.; Bos, R.; Neira, M. Diseases due to unhealthy environments: an updated estimate of the global burden of disease attributable to environmental determinants of health. J. Public Heal. 2016, 39, 464–475. [Google Scholar] [CrossRef] [PubMed]
- Jacobs. South Africa has less than 50 years of mining left, Dialy investor, 2023. https://dailyinvestor.com/mining/34217/south-africa-has-less-than-50-years-of-mining-left/#:~:text=South%20Africa%20has%20approximately%20261,concentrated%20in%20a%20single%20mine.
- Nephalama, A and Muzerengi, C. ‘Assessment of the influence of Coal mining on groundwater quality. Case of Masisi village in the Limpopo Province of South Africa.’ University of Venda, 2023.
- Momoh, A.; Mhlongo, S.E.; Abiodun, O.; Muzerengi, C.; Mudanalwo, M. Potential implications of mine dusts on human health: A case study of Mukula Mine, Limpopo Province, South Africa. Pak. J. Med Sci. 2013, 29, 1444–1446. [Google Scholar] [CrossRef] [PubMed]
- Muthelo, L. Strategies to enhance compliance of health and safety standards at the selected mining industries in Limpopo Province, South Africa: occupational health nurse's perspective (Doctoral dissertation). Ulspace.ul.ac.za.
- Chipa, M. J. Mining, corporate social responsibility and communities in Limpopo Province: the case study of Mogalakwena Local Municipality, 2021. Scholar.ufs.ac.za.
- Martino, L. ‘Concepts of Health, wellbeing & Illness’. Health Knowledge Education, 2017. CPD & Revalidation from Phast.
- World Health Organization Ambient air pollution: a global assessment of exposure and burden of disease. Clean Air J. 2016, 26. [CrossRef]
- Adam, V.Y. and Awunor, N.S. ‘Perception and factors affecting utilization of health services in a rural community in Southern Nigeria’. Journal of Medicine and Biomedical Research, 2014, 13(2): 117-124.
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Statistics South Africa. ‘Mid-year population estimates 2017, 2011. Retrieved 11 June 2011. From http://www.statssa.gov.za/?p=2990.
- Mpofu, O. ‘Tuberculosis in coal mine workers in Mpumalanga, 2009. University of KwaZuluNatal, School of Medicine.
- du Toit, E.; Squire, S.B.; Dunbar, R.; Machekano, R.; Madan, J.; Beyers, N.; Naidoo, P. Comparing multidrug-resistant tuberculosis patient costs under molecular diagnostic algorithms in South Africa. Int. J. Tuberc. Lung Dis. 2015, 19, 960–968. [Google Scholar] [CrossRef] [PubMed]
- Pless-Mulloli, T.; Howel, D.; Prince, H. Prevalence of asthma and other respiratory symptoms in children living near and away from opencast coal mining sites. Leuk. Res. 2001, 30, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Howel, D. , Pless-Mulloli, T., & Darnell, R. Consultations of children living near opencast coal mines. Environmental Health Perspectives, 2001, 109(6), 567-571. [CrossRef]
- Yapicci, O. , Gozaydinoglu, S., & Doksoz, O. Assessment of heavy metal concentrations in the food web of lake Beysehir, Turkey. Environmental Monitoring and Assessment, 2006, 119(1– 3), 271–281. [CrossRef]
- Hendryx, M.; Entwhistle, J. Association between residence near surface coal mining and blood inflammation. Extr. Ind. Soc. 2015, 2, 246–251. [Google Scholar] [CrossRef]
- Martinello, N. Health effects of coal mining. In Encyclopedia of Environmental Health (Second Edition), 2021. Elsevier. [CrossRef]
- Percet, R. , Roig, J. , Monso, E., Brugada, J., & Cardús, J. Short-term association between air pollution and emergency room visits for chronic obstructive pulmonary disease: A time-series study in Barcelona. Revista Española de Salud Pública, 2017, 91, e1–e9. [Google Scholar] [CrossRef]
- Quittner, A.L.; Saez-Flores, E.; Barton, J.D. The psychological burden of cystic fibrosis. Curr. Opin. Pulm. Med. 2016, 22, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Hendryx, M. , Keith, J.Z. and Juhua, L. (2020). ‘Impacts of Coal use on Health’. Annual Review- Public Health, 2020, 41: 397- 415. [CrossRef]
- Carré, J.; Gatimel, N.; Moreau, J.; Parinaud, J.; Léandri, R. Does air pollution play a role in infertility?: a systematic review. Environ. Health 2017, 16, 82. [Google Scholar] [CrossRef] [PubMed]
- Van der Zee, S.C. , Broeke, R., Bast, A., & Zelissen, P.M.J. Diabetes mellitus type 2 and microvascular complications: the central role of neurogenic and endothelial disturbances. Current Vascular Pharmacology, 2016, 14(5), 442-454. [CrossRef]
- Mactaggart, F.; McDermott, L.; Tynan, A.; Gericke, C. Examining health and well-being outcomes associated with mining activity in rural communities of high-income countries: A systematic review. Aust. J. Rural. Heal. 2016, 24, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Mactaggart, F.; McDermott, L.; Tynan, A.; Gericke, C.A. Exploring the determinants of health and wellbeing in communities living in proximity to coal seam gas developments in regional Queensland. BMC Public Heal. 2017, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Munzerengi, C. and Nephalama, M. Assessment of the influence of Coal mining on groundwater quality’. Case of Masisi village in the Limpopo Province of South Africa, 2016, University of Venda.
- UNEP. ‘Environmental Impact Assessment Training Resource Manual, 2006. Second edition.
- Macctg, F. , Goodall, K., & Begum, N. Exploring the determinants of health and wellbeing in communities living proximity to coal seam gas developments in regional Queensland, 2018. Department of Health Care management: Berlin University of Technology, Germany.
- Alpers, C.N.; Yee, J.L.; Ackerman, J.T.; Orlando, J.L.; Slotton, D.G.; Marvin-DiPasquale, M.C. Prediction of fish and sediment mercury in streams using landscape variables and historical mining. Sci. Total. Environ. 2016, 571, 364–379. [Google Scholar] [CrossRef] [PubMed]
- Huertas, J. I. , Tamayo, J. C., Llano, D., & Ramírez, J. Environmental impacts and legal control of coal mining in Colombia. Energy Policy, 2012, 46, 521–529. [Google Scholar] [CrossRef]
- Liping, J.; Bin, C. An Input-output Model to Analyze Sector Linkages and CO2 Emissions. Procedia Environ. Sci. 2010, 2, 1841–1845. [Google Scholar] [CrossRef]
- Smith, K. , & G. A. Overweight and obesity in Australia: The 1999-2000 Australian Diabetes, Obesity and Lifestyle Study (AusDiab). Medical Journal of Australia, 2009, 191(3), 202–210. [CrossRef]
Figure 1.
Community perceived impact of coal mining on local people's physical wellbeing.
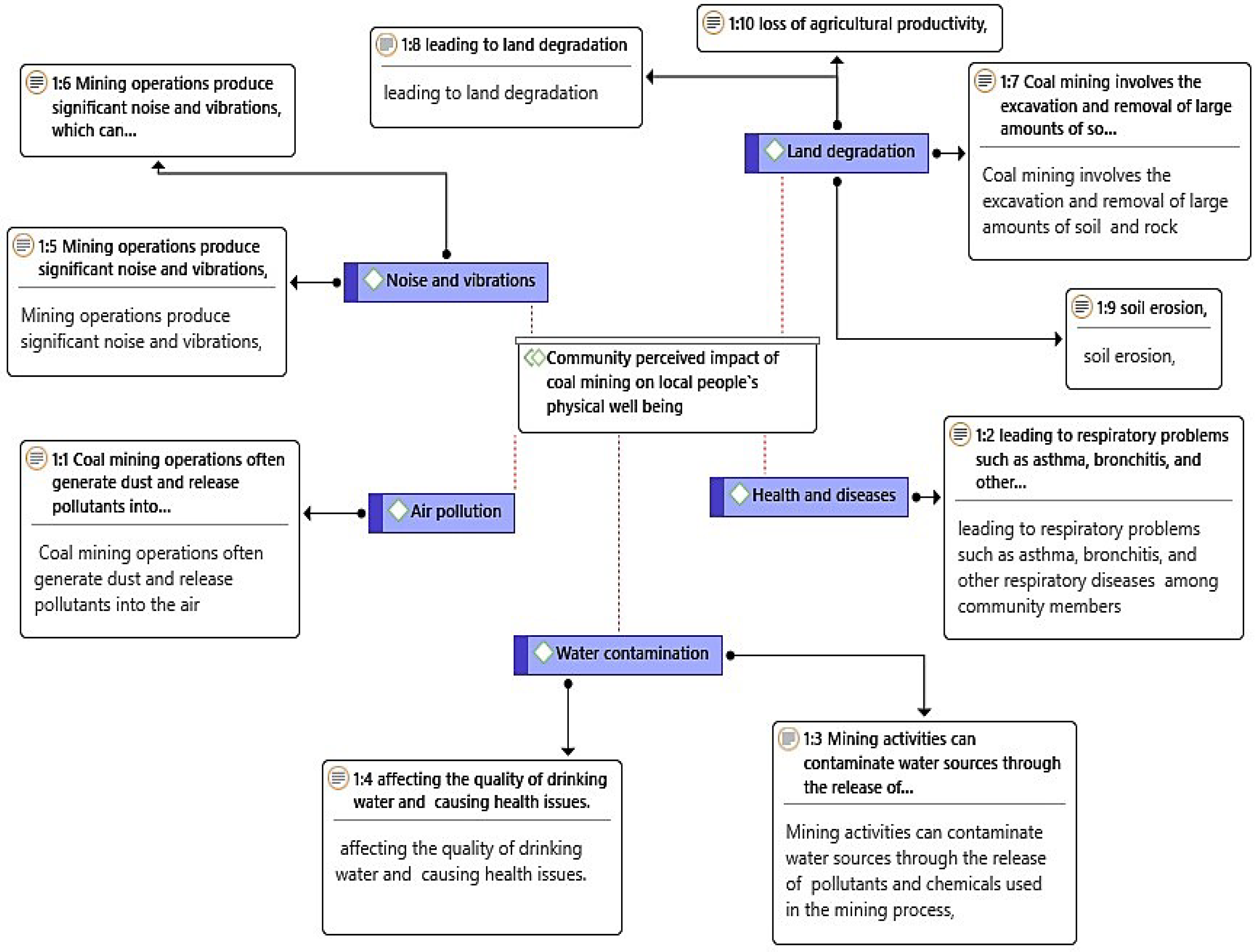
Figure 2.
Community perceived impact of coal mining on the mental health of local people.
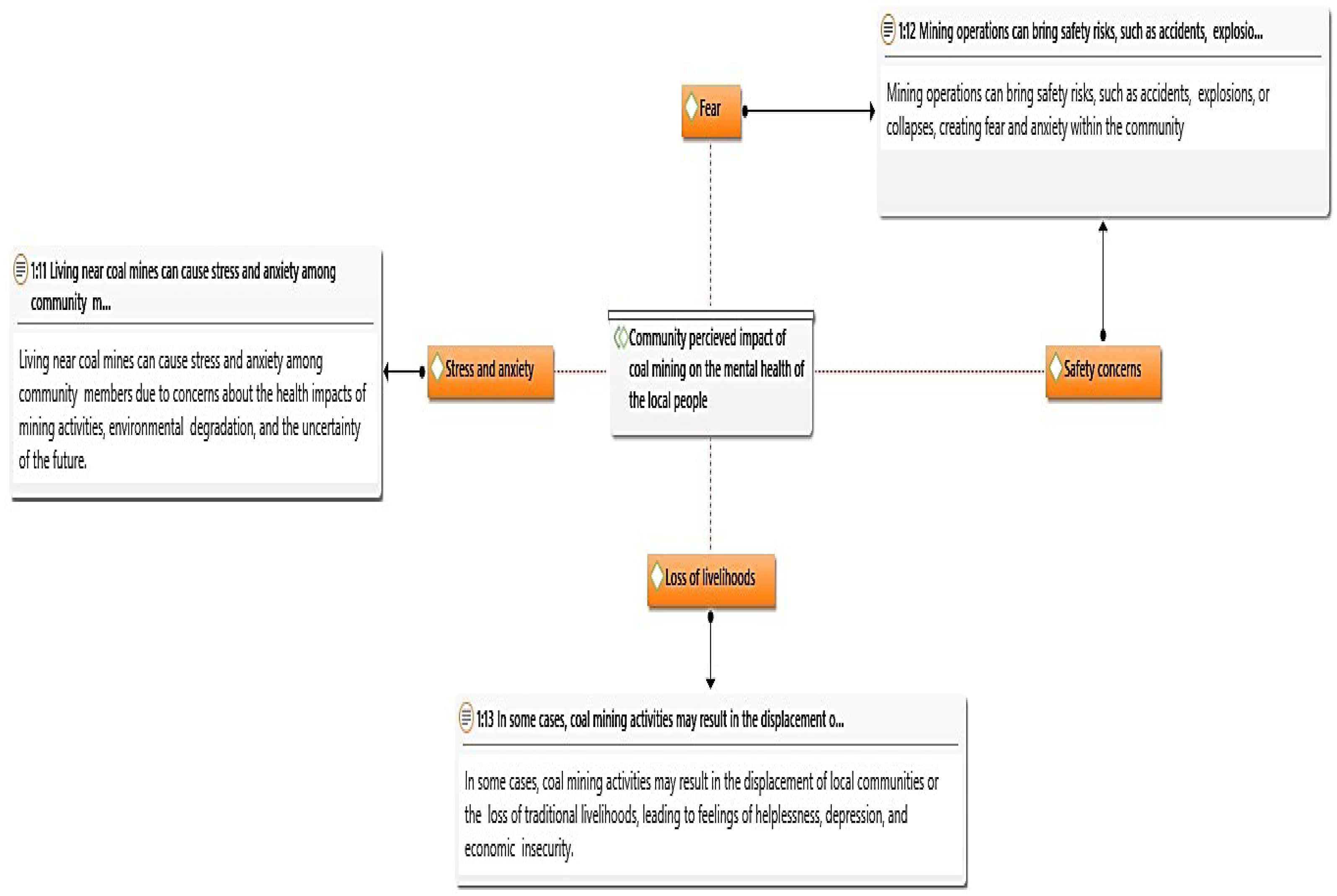
Figure 3.
Perceived impact of coal mining on the community's social well-being.
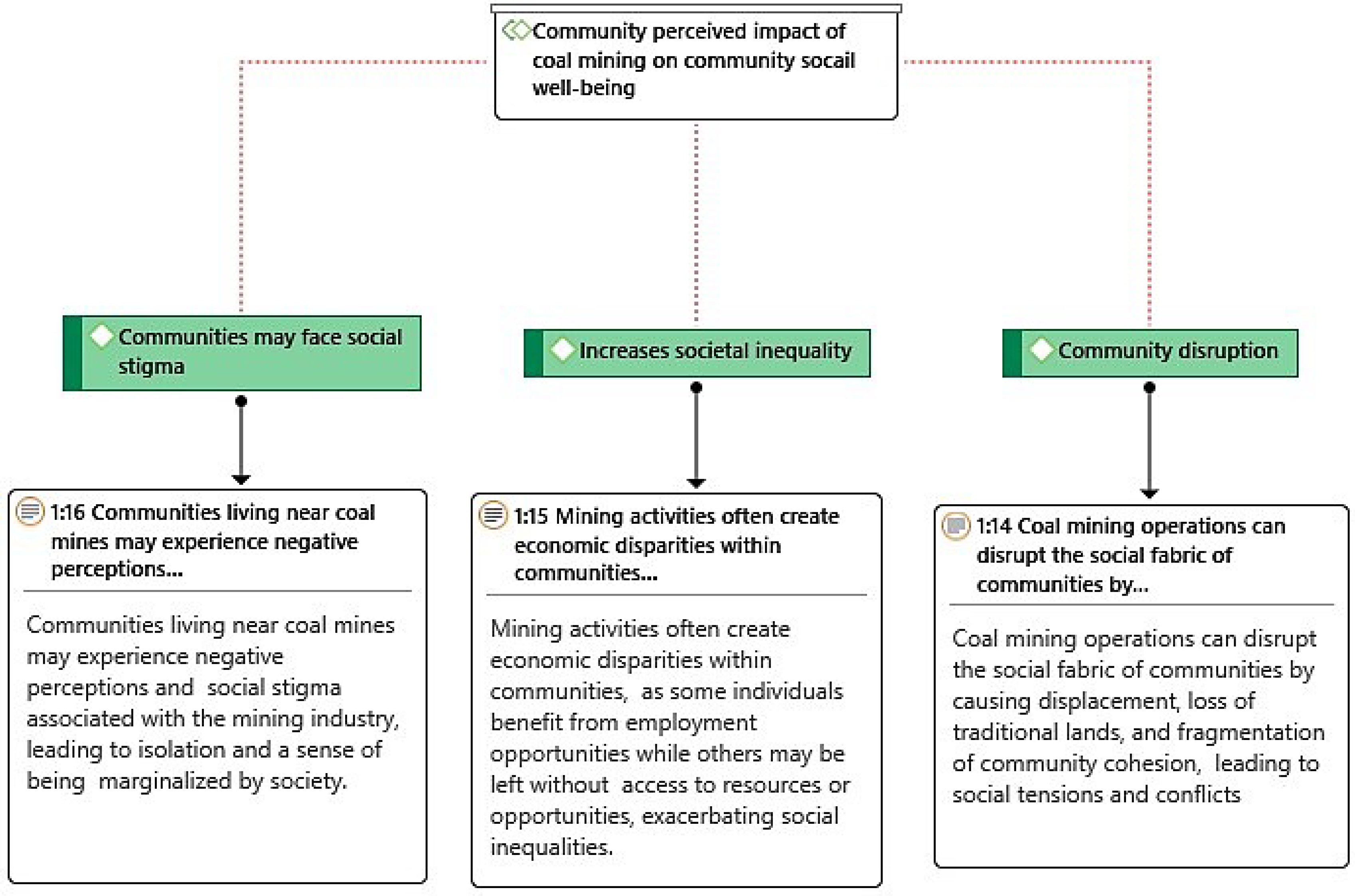
Figure 4.
Environmental Factors associated with coal mining.
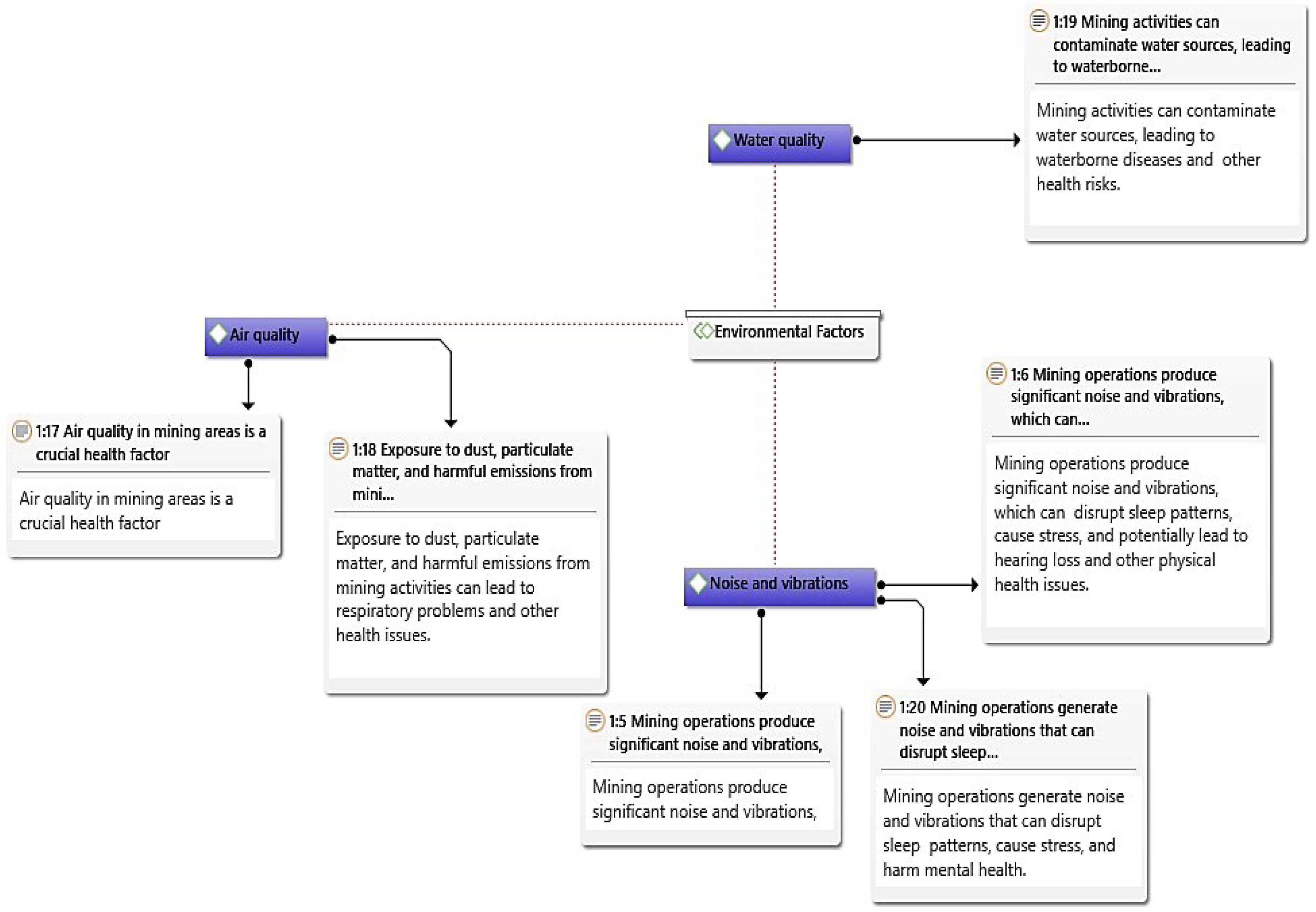
Figure 5.
Occupational Health and Safety Factors.
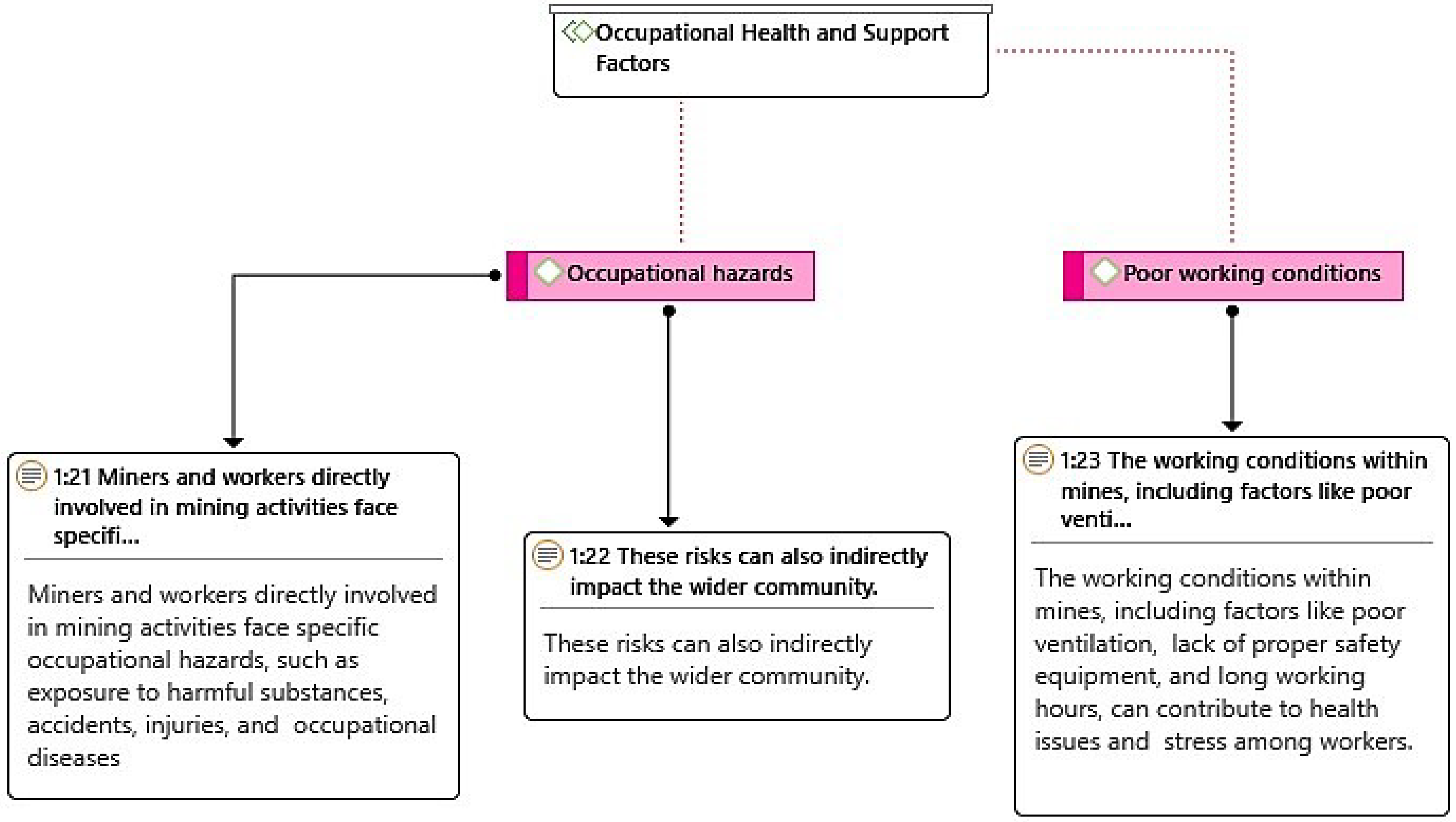
Figure 6.
Perceived socio-economic factors associated with health and well-being in coal mining communities.
Figure 6.
Perceived socio-economic factors associated with health and well-being in coal mining communities.

Figure 7.
Social and cultural factors of coal mining directly affect community members` health and wellbeing.
Figure 7.
Social and cultural factors of coal mining directly affect community members` health and wellbeing.
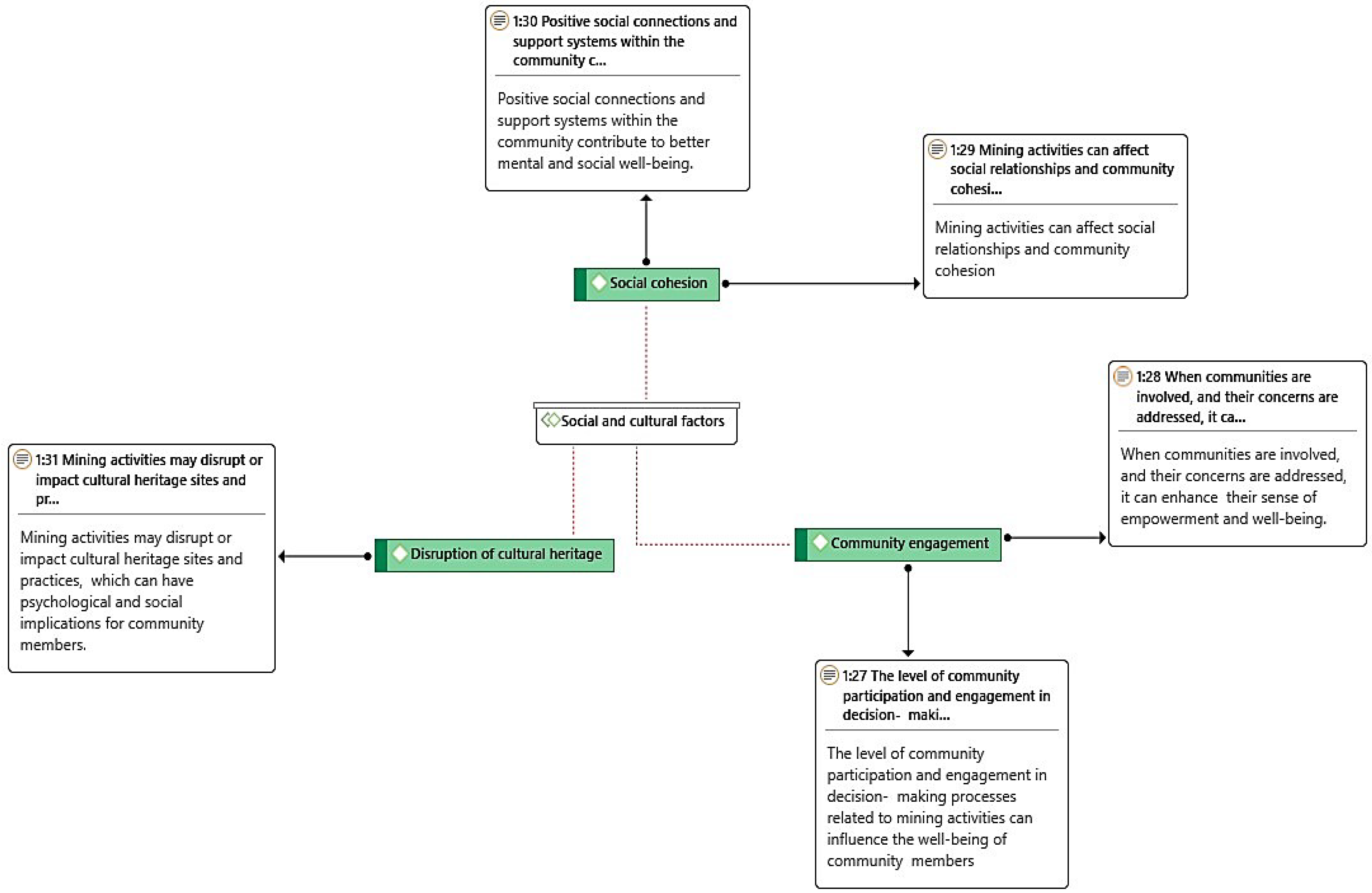
Figure 8.
Summary perceptions of the community members around Tshikondeni Coal mine.
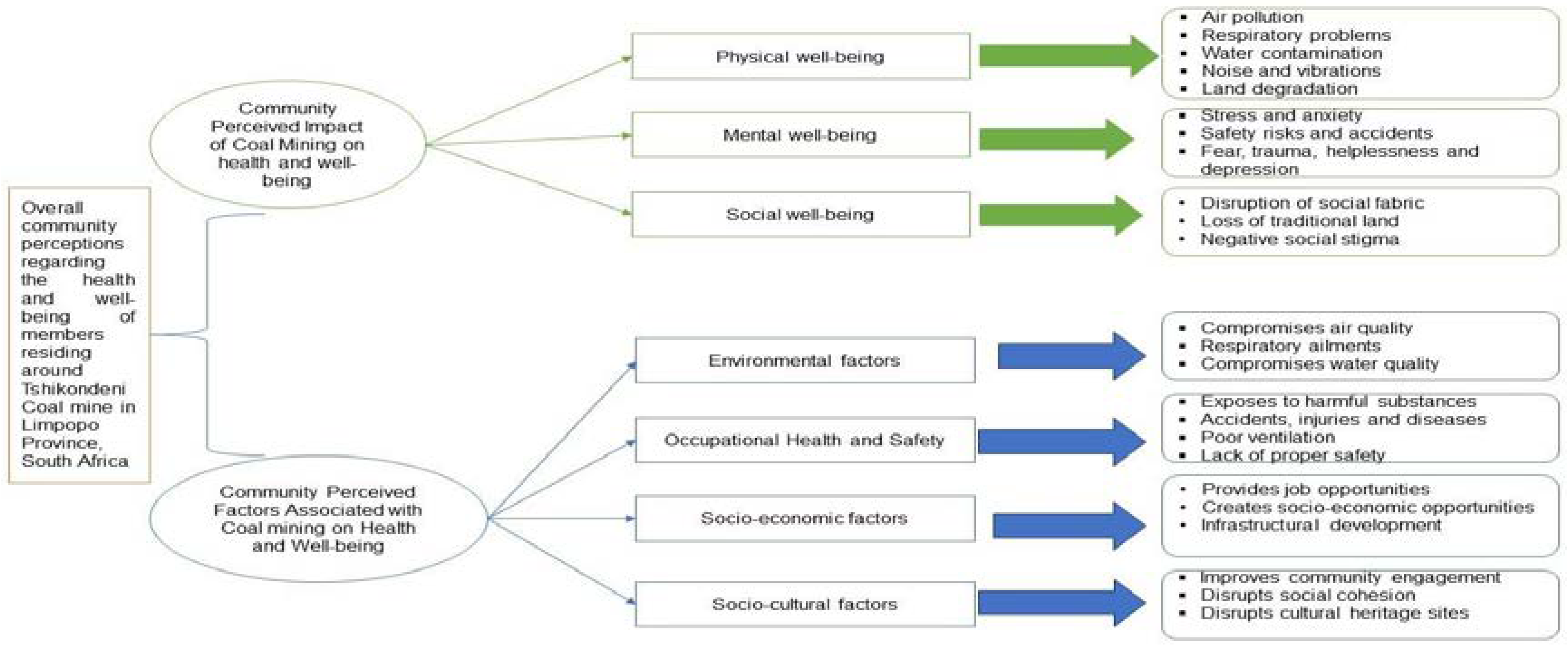
Table 1.
List and population count of sub-Villages.
| No. | Names of sub-villages | Population count | Sample size |
|---|---|---|---|
| 1 | Bileni | 117 | 22 |
| 2 | Mukomawabane | 388 | 33 |
| 3 | Thondoni (Mutele B) | 422 | 26 |
| TOTAL | 927 | 81 |
Source: (26).
Table 3.
Themes and sub-themes.
| Themes | Sub-themes |
|---|---|
| Community perceived impacts of coal mining | Physical impact 刘Mental impact 刘Social impact |
| Factors perceived by the community as associated with the health and well-being of individuals exposed to coal mining. | Environmental factors 刘Occupational factors 刘Socio-economic factors 刘Socio-cultural factors |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



