
Submitted:
01 August 2024
Posted:
02 August 2024
You are already at the latest version
Abstract
Background: Pediatric obesity treatment is based on high-intensity lifestyle counseling. However, high dropout rates and low effectiveness have been reported even in specialized centers. Mobile health technologies have been used in research settings to overcome these limits with contrasting results. This study aims to evaluate the effectiveness of a six-month intervention with a mobile app for the treatment of pediatric obesity at 6 and 12 months of follow-up. Methods: Patients were randomly assigned to standard care or standard care plus mobile app (2:1). The mobile app delivered high-intensity lifestyle counseling for diet and physical activity. Results: Seventy-five subjects were prospectively enrolled. At six months of follow-up, the m-app group showed significantly lower dropout rates compared to standard care(p=0.01). The risk of dropout was significantly higher in controls compared to the intervention group (OR 3.86,95%C.I. 1.39-10.42,p=0.01). After one year of follow-up, we observed lower albeit non statistically significant dropout rates in the m-app compared to the standard care group(p=0.24). No differences were observed in terms of z-score BMI and percentage of BMI reduction between the two groups. Conclusion: our findings suggest that mobile app might help in the clinical management of children and adolescents with obesity in terms of dropout reduction.
Keywords:
obesity 1
; treatment 2
; m-Health 3
1. Introduction
Obesity in children and adolescents is a major public health concern globally. The increasing prevalence of obesity in children has been observed in both developed and developing countries [1]. The prevalence of pediatric obesity has increased dramatically over the past five decades. According to the WHO, overweight/obese young children (0-5yr) increased from 32 million globally in 1990 to 37 million in 2022. For children aged 5-19 years, the number rose from 31 million in 1990 to 160 million in 2022 [2].
In 2019, the World Obesity Federation projected that by 2025, there would be approximately 70 million children aged 0-5 years and 206 million children and adolescents aged 5–19 years living with obesity [3].
Similar trends are observed worldwide, with the steepest increases occurring in low- and middle-income countries. The prevalence is similar among boys and girls, with slightly higher values for obesity in boys [4].
This trend poses a severe threat to future public health since children and adolescents with obesity are more likely to develop obesity-related comorbidities [5]. There are several diseases caused by obesity, in the short, medium, or longer term, depending upon age and obesity severity [1]. All body systems can be affected [6]: comorbidities including cardiovascular disease (hypertension, dyslipidemia, endothelial dysfunction, left ventricular hypertrophy) [7,8]; respiratory disease (asthma, obstructive sleep apnea-OSAS, sleep disorders, hypoventilation syndrome) [9,10,11]; endocrine disease (impaired glucose tolerance, polycystic ovary syndrome, metabolic syndrome, type 2 diabetes) [12,13]; gastrointestinal disease (fatty liver disease, gastroesophageal reflux, micronutrient deficiencies) [14], skin alteration (acanthosis nigricans, psoriasis), musculoskeletal and dental alteration (cavities and periodontal disease, pain, fractures, slipped capital femoral epiphysis) [15,16]; kidney damage [17], and psychiatric problems (anxiety and depression) [1,6].
Several factors contribute to determinate obesity, including a combination of genetic, socioeconomic, environmental, behavioral, and psychosocial factors [1].
Obesity can be influenced by an obesogenic environment, which includes dietary habits (high intake of energy-dense, micronutrient-poor foods, sugar-sweetened beverages, and fast food) [18,19], lower levels of physical activity (sedentary lifestyles, characterized by reduced physical activity and increased screen time) [20,21,22], and socioeconomic status (lower socioeconomic status is associated with higher obesity rates due to limited access to healthy foods and health education).
Behavioral factors include eating patterns (portion size, irregular meal timings, skipping breakfast, and high frequency of snacking) [19] and sleep (sleep deprivation, poor sleep quality, or late bedtime can disrupt hormonal regulation of appetite) [23].
Psychosocial factors, family dynamics, and mental health (such as stress, anxiety, or depression) can also exacerbate dysfunction of the energy regulatory system favoring weight gain. In addition, several factors in early life are associated with a high risk of developing obesity, like maternal obesity, gestational diabetes, and excessive gestational weight gain [24,25].
The complexity of obesity pathogenesis influences the complexity of treatment. Treatment first aims to prevent the development of chronic diseases, reduce adiposity, improving physical and psychosocial comorbidities. Therapy integrates multiple components including nutrition, exercise, psychological counseling, pharmacotherapy, and surgical procedures [26]. The first approach for pediatric obesity is the promotion of lifestyle modifications, including diet, physical activity, and eating behaviors [27]
Scientific societies [27,28] suggest the promotion of healthy dietary habits (avoiding the consumption of calorie-dense, nutrient-poor foods, encouraging the consumption of whole fruits) and physical activity education (20 minutes, optimally 60 minutes, of vigorous physical activity at least 5 days per week) at a multilevel involving children and adolescents, parents, and communities. Other strategies are anti-obesity medication and metabolic/bariatric surgery [27]. The current guidelines [29] highlight the relevance of counseling intensity to achieve lifestyle modifications in children and adolescents with obesity. They suggest at least 26 “contact” hours of counseling in a period of 3-12 months to guarantee this high-intensity approach [29]. However, this is not commonly applicable in clinical settings for health professionals and families. Moreover, even if lifestyle treatment is the first approach, it is not always successful. Several studies have reported high drop-out rates in lifestyle intervention for children and adolescents with obesity [30,31,32]. The major barriers to treatment compliance include low socioeconomic status, distance from the clinic, psychological comorbidities, and parents with obesity [30,31,32]. These data highlight the importance of personalizing the intervention according to the family and patient needs and of developing new strategies for treatment delivery. In this light, electronic health (e-Health) resources are a promising tool.
In a clinical trial, Hagman et all [33] demonstrated that a digital support system with a personalized weight-loss target curve and daily weight measurements shared by the family and the clinic was more effective in terms of weight loss and dropout rates than the standard care for the treatment of children with obesity.
Digital tools can help children with obesity to manage their weight and improve their overall health through different strategies. Advanced algorithms can analyze data to provide personalized feedback and recommendations. These devices might encourage teenagers and adults to increase their physical activity and change how they eat, track their weight, and food, and provide motivational messages [34]. Moreover, mobile health systems (m-Health) can monitor physical activity, dietary intake, and sleep patterns, thus providing real-time feedback and helping children understand their habits, making it easier to set and achieve health goals. In addition, m-Health devices can help caregivers to identify wrong patterns and make necessary adjustments.
The presence of goal setting, progress tracking, and rewards can incentivize the patient to stay motivated; in addition, m-Health apps can send reminders and notifications that help to create a daily healthy routine.
Some digital tools can facilitate remote coaching and telehealth consultations, allowing healthcare providers to offer personalized advice and support without the need for frequent in-person visits [33].
Several studies have demonstrated improvements in self-reported diet, physical activity, and short-term weight loss [35,36,37,38,39]. However, scientific evidence for the effectiveness of these devices as an adjunct tool for the treatment of pediatric obesity is poor. To date, few studies have been conducted on children and adolescents with obesity. Moreover, the available trials are highly heterogeneous in terms of type of intervention (education, behavioral therapy, self-monitoring, and others), sample size, and study population.
In a recent meta-analysis, Metzendorf et al. [34] reported that in 13 studies on adults with obesity, smartphone apps probably may reduce BMI in the medium term, but the evidence is very uncertain. Moreover, the intervention failed to induce significant changes in physical activity, BMI reduction at 12 months, and quality of life. For adolescents, the available evidence base is even more restricted [34].
Based on this knowledge, this prospective study aims to investigate the effectiveness of a mobile app for smartphones (m-App) in the treatment of pediatric obesity compared to standard care. In detail, the main objectives of the study were: 1) verify the differences in dropout rates between control and intervention groups; 2) assess the differences in weight loss between m-app and standard care groups at 6 and 12 months of follow-up.
2. Materials and Methods
2.1. Study Design and Participants
The study is a prospective monocentric two-arm open-label randomized controlled trial. The intervention group received standard care provided by a trained pediatrician and a dietitian plus a smartphone app for the treatment of pediatric obesity. The control group received only standard care. Children and adolescents aged 6 years and above attending the pediatric obesity outpatient clinic of the University Hospital “Luigi Vanvitelli” were prospectively enrolled. According to international guidelines [29], obesity was defined based on body mass index (BMI) calculated as the ratio between the weight expressed in kilograms and the height squared expressed in meters (kg/m2). Patients were eligible if 1) they had a BMI ≥95th percentile for age and sex according to the WHO growth charts [40,41]; 2) they were not taking medications affecting body weight; 3) their parents owned and were able to use a smartphone; and 4) they gave the consent to participate. Children affected by secondary forms of obesity (i.e. endocrinopathies, syndromic obesity, monogenic forms) were excluded. Written informed consent from parents and children assent to participate was collected before the randomization procedure. The study was conducted according to the Declaration of Helsinki. The Ethical Institutional Review Board of the University of Campania “Luigi Vanvitelli” approved the study (protocol n. 14258/2023). All participants underwent a complete clinical examination as reported elsewhere [42]. Briefly, the child was examined wearing undergarments. Height was measured by a Harpenden stadiometer at the nearest 0.1 cm. Weight was assessed by a balance beam scale at the nearest 0.1 kg. Z-score BMI was calculated with the lambda-mu-sigma method [43]. Waist circumference was measured at the midpoint between the lowest rib and the iliac crest with an anelastic tape, and the average of two values was obtained. The ratio between waist and height (WHR) in centimeters was calculated as an indirect measure of truncal adiposity. Blood pressure was measured three times, and the average of the three measurements was reported. After baseline assessment, participants were randomly allocated to standard care or intervention with a 2:1 ratio using an online randomizer system (http://www.graphpad.com/quickcalcs/index.cfm). The complete auxological and clinical examinations were performed at 6 months and 12 months of follow-up.
2.2. Study Intervention
The control group received standard lifestyle care, consisting of nutritional and behavioral counseling provided by dieticians and pediatricians. During the first visit, patients and their families received a treatment plan based on a personalized physical activity plan (according to patient age, ability, and fitness level) and a balanced Mediterranean diet. Moreover, psychological counseling for the patient and the family was provided to identify potential comorbidities and provide behavioral therapy.
Follow-up visits were scheduled every three months according to standard care and outpatient clinic waiting lists and included clinical, nutritional, physical activity, and psychological assessment.
The intervention group received the standard care plus the smartphone app (Nutrilio) [Nutrilio FREE, Version 1.17.4, 2023] for six months. After the allocation to the intervention group, participants were invited to download the app through AppStore (iOS) or Google Play (Android) and received information on how to use the app.
The free Nutrilio app consists of a daily diary of diet and physical activity that is recorded and can be exported as a .csv file. The participants were invited to send this file once a week to the medical staff. After receiving the diary, the medical staff gave feedback to the family about the lifestyle behavior and potential improvements to be applied at home.
In-person visits were scheduled every three months as for the control group. The follow-up was completed after 12 months (6 months with smartphone app and 6 months with standard care alone).
2.3. Study Outcomes
The primary outcome of the study was the difference in dropout rates at 6 and 12 months of follow-up between the two groups. Dropout was defined as the presence of less than 1 visit in 6 months. Secondary outcomes were changes in body weight including 1) changes in z-score BMI: delta changes in z-score BMI were calculated at 6 and 12 months of follow-up compared to baseline evaluation; 2) clinically significant reduction of baseline BMI defined as a reduction of at least 5% of BMI after 6 and 12 months [44,45] clinically significant reduction of z-score BMI defined as a reduction of at least 0.25 units of z-score BMI at 6 and 12 months compared to baseline [46].
2.4. Statistical Analysis
Continuous variables were checked for normality by Kolmogorov-Smirnov test. Difference between groups for continuous variables were investigated by Mann Whitney U test. Chi-square or Fisher exact tests were used to test differences for categorical variables as appropriate. Data are expressed as median (interquartile range, IQR) or percentages. Univariate logistic regression analysis was performed to calculate the odds ratio (OR) for drop-out according to the allocation group. Moreover, a multivariate logistic regression analysis including age, gender, BMI, and Z-score BMI was performed to correct the effect of the allocation group for potential confounding factors. A p-value <0.05 was considered statistically significant. All the analyses have been performed using SAS® on Demand for Academics (SAS Institute Inc., Cary, NC, USA).
Study power was calculated based on a post-hoc analysis considering the main outcome of differences in dropout rates between the two groups. On the basis of the differences in dropout rates at 6 months between standard care (72%) and m-App intervention (40%), with a sample size of 75 participants, our study has a power of 80% to detect a difference in dropout between groups with an alpha level of 0.05.
3. Results
Seventy-five children and adolescents were enrolled (36 males, mean age 9.4 ± 1.5 years). The characteristics of the entire cohort are displayed in Table 1.
Fifty patients were allocated in the control group and 25 in the intervention group. The two groups did not differ in age, sex, BMI, and BMI z-score distribution (Table 2).
3.1. Drop out Assessment
After six months, 14 patients in the control group (28%) and 15 patients in the intervention group (60%) completed the follow-up. The dropout rate was significantly higher in the control group (72%) compared to the intervention group (40%, p=0.02) (Figure 1).
Children who completed the follow-up at 6 months did not significantly differ at baseline for age, gender, BMI, Z-score BMI, and blood pressure compared to those who did not show up at follow-up (Table 3).
Univariate logistic regression analysis revealed that the standard care group showed a 3.86-fold higher risk for drop-out compared to the M-App group (OR 3.86, 95% C.I. 1.39-10.42, p=0.01). This risk was independent of the effect of age, gender, BMI, a,d Z-score BMI (p=0.008). At one year of follow-up, there were no differences in drop-out rate between the two groups (p=0.24); the standard care showed a 92% and the intervention group an 80% drop-out rate.
3.2. Weight-Loss Outcomes
Weight-loss achievement was evaluated as a reduction of Z-score BMI and as a reduction of baseline BMI in percentage. The two groups showed similar Z-score BMI reduction at 6 months of follow-up (p=0.51). The median reduction of Z-score BMI in the standard care group was -0.3 units (IQR -0.55; -0.18) and -0.29 (IQR -0.48; -0.11; see Figure 2). Moreover, the rates of clinically significant reduction (-0.25 units) of Z-score BMI did not differ between the two groups (standard care 66.7% versus M-App 53.3%; p=0.71). No differences were observed at 12 months in delta Z-score BMI reduction between the two groups (p=0.99).
The median reduction of BMI after 6 months was 3.75% (IQR 0.0%; 7.63%). There were no differences in BMI percentage change between the two groups (p=0.36). The median change of BMI in the standard care group was -2.3%(IQR -7.3%; 7.1%) versus -3.1% (IQR -6.8%; 0.0%; see Figure 3) in the M-App group. The rate of patients achieving at least 5% of BMI reduction compared to baseline did not differ between the two groups (53.3% of controls versus 33.3% of cases; p=0.46). Moreover, the two groups showed a similar BMI percentage change a t 12 months of follow-up (p=0.90).
4. Discussion
In this study, we investigated the effectiveness of a smartphone app (Nutrilio) in improving lifestyle intervention compliance in children and adolescents with obesity. The intervention lasted 6 months followed by 6 months of follow-up without the use of the smartphone app. We observed a significantly lower dropout rate in the m-App group compared to the standard care after the first six months of follow-up. However, this finding was not confirmed at 12 months of follow-up. Regression analysis confirmed that the use of the mobile app was protective against the risk of dropping during follow-up independently of other confounding factors.
Attrition represents a common concern in the treatment of obesity, both in childhood and adulthood [47,48]. Elevated attrition rates and poor compliance to treatment reduce the effectiveness of clinical interventions for lifestyle modifications and subsequently weight loss achievement. Moreover, dropout is associated with poor disease control and negative health outcomes in the medium and long term. Therefore, to improve the success of pediatric weight management programs, new strategies to counteract the dropout phenomenon should be promoted. Several studies have investigated the predictors of attrition during lifestyle intervention trials with heterogeneous results [49,50,51]. The rates of dropout are generally high and tend to vary according to the type of intervention (diet, physical activity, diet plus physical activity). In common clinical practice, the dropout rate in pediatric obesity is around 60% after one year of treatment [49,52]. Among predictors, low socioeconomic status, parental obesity, lower Z-score BMI at baseline, distance from the hospital, adolescence, and male gender have been associated with a higher risk of dropout [49,50]. Conversely, the presence of comorbidities, such as hyperglycemia, insulin resistance, and dyslipidemia have been associated with higher compliance to treatment. Probably this is due to more consciousness about obesity as a disease from both parents and patients [49].
In this context, mHealth can be a strategy to increase adherence. This theory is supported by the study by Roth et al. [53] who described a dropout rate of 19.7% after 12 months of intervention, lower than the dropout rate reported in other studies (ranging from 26.8-39%). However, it’s difficult to estimate the realistic effects of mHealth because of the high rate of dropouts. In fact, high rate of attrition was found in different studies about mHealth interventions reducing the positive outcomes of intervention [32673267; 29607800]. The study by Desmet et al. [54] focused on the attrition rate during a mHealth intervention in adolescents with obesity including also a psychological assessment. In this study, dropouts were associated with demographic factors (age, gender, and socio-economic status), health-related factors (baseline weight, initial motivation levels, and prior experience with technology), and feasibility of the app (features and support). No statistically significant difference in attrition was found across the different eating styles. The only significant negative predictor of attrition was adjusted BMI: a higher adjusted BMI may result in greater motivation to use mHealth apps [54]. In our study, we did not find predictors of dropout except for the m-app use. This finding might be related to the small sample size that has underpowered the ability to find other predictors.
Moreover, we evaluated the effect of the mobile app on weight loss outcomes. Weight loss was assessed as both Z-score BMI and BMI percentage reduction over time at 6 and 12 months. The two groups displayed a similar decrease in Z-score and BMI values over time. Therefore, in our study, the m-app intervention was not superior to standard care in inducing a more clinically significant weight loss. These findings might suggest that the m-app is useful in intensifying counseling and reducing the attrition rate, but not in increasing the subject’s adherence to lifestyle modifications. Scientific literature has reported that a 0.25 to 0.5 units reduction of Z-score BMI is associated with an improvement of cardiometabolic risk in children and adolescents with obesity [46]. Reinehr et al. reported in a cohort of about 1400 children with obesity that a reduction of at least 0.125 units of Z-score BMI was associated with an improvement of several cardiovascular risk factors (hypertension, dyslipidemia, insulin resistance). This effect was more pronounced for a Z-score reduction of 0.25 units after 1 year of lifestyle intervention in the Obeldicks trial [46]. Previous studies conducted in smaller groups have reported that a Z-score BMI lowering of 0.5 units might be beneficial for patients in terms of comorbidities resolution [55]. Conversely, another study reported a clinical benefit for a 0.01 unit decrease in systolic and diastolic blood pressure levels [56]. In our study, we did not perform blood tests to assess insulin levels, dyslipidemia, and glucose homeostasis. Therefore, we could not draw any conclusion about the cardiometabolic risk reduction and the best Z-score decrease cut-off for cardiometabolic profile improvement in our cohort.
In addition, during the last few years, the measures of clinically meaningful weight loss have been widely discussed. In clinical practice, current guidelines recommend using BMI for obesity diagnosis as a surrogate of body adiposity and the Z-score BMI represents an estimate of obesity severity [27,28,29]. However, when the Z-score BMI is measured in cohorts with many participants above the 97th percentile, the clinical utility for change over time is limited. The Z-score values for BMI above the 97th percentile are based on calculations and therefore might be less accurate [45]. Moreover, for severe obesity, the Z-score values are compressed with a narrow spectrum of variability even for significant changes in BMI values. This phenomenon reduces the impact of Z-score reduction after treatment leading to an underestimate of the treatment efficacy over time [45]. Therefore, other metrics for treatment outcomes estimates have been proposed, including the absolute and percentage change of BMI, the change in percent of median, the reduction of 5%-10%-15% of BMI, and others [46]. However, the application of these other metrics is scarce in pediatric research, limiting the possibility of comparing study outcomes and different intervention efficacies. In our study, we included the metric of percentage change of BMI and the reduction of at least 5% of baseline BMI after 6 months. As for the Z-score BMI decrease, we found no differences in terms of weight loss assessment between the two groups.
We acknowledge the presence of limitations that constrict the generalizability of our findings. The small sample size might have underpowered the study in identifying predictors of dropout in our cohort. Moreover, the subjects included in the study were homogeneous in terms of age, gender, and BMI distribution, therefore we did have not enough power to detect other risk factors for attrition to lifestyle intervention in pediatric obesity. However, at the same time, this represents also a strength of the study. In fact, we were able to assess the independent effect of the mobile application as an add-on therapy in the management of children and adolescents with obesity without other confounding factors.
To date, the available scientific evidence is highly heterogeneous, and for clinicians is hard to draw clear conclusions about the effectiveness of e-health technologies in clinical practice, especially in pediatric age.
5. Conclusions
This prospective monocentric randomized open-label trial showed that a mobile app with an educational and feedback activity was effective in reducing the attrition rate during a lifestyle intervention for pediatric obesity. This effect was limited to the use of the mobile app and was not confirmed after m-app use interruption. No effects were observed on weight loss achievement compared to standard care.
These findings suggest that m-health technologies represent a promising tool as support in clinical practice to empower lifestyle counseling intensity. Moreover, these tools allow healthcare professionals to perform a multilevel approach targeting both parents and children, as advocated by current guidelines. However, the dropout rate over time continues to be high and the strength of these findings should be further confirmed in larger studies.
Author Contributions
Conceptualization, G.R.U. and E.M.D.G.; methodology, P.M., GSRCDSS, and G.C.; software, A.D.S.; formal analysis, A.D.S.; investigation, F.M. and G.R.U.; data curation, M.M and G.R.; writing—original draft preparation, G.R.U. and M.M.; writing—review and editing, E.M.D.G., and P.B.; supervision, E.M.D.G.; funding acquisition, G.R.U. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the University of Campania Luigi Vanvitelli (Bando Giovani di Ateneo, D.R. n. 266 del 30/09/2022 to GRU).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of University of Campania Luigi Vanvitelli (protocol code 14258/2023 date 08/06/2023).”
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jebeile, H.; Kelly, A.S.; O’Malley, G.; Baur, L.A. Obesity in children and adolescents: epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol. 2022, 10(5):351-365. [CrossRef]
- World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 27 Jul 2024).
- Global Obesity Observatory. Available online: https://data.worldobesity.org/ (accessed on 27 Jul 2024).
- Nardone, P.; Ciardullo, S. Stato ponderale e stili di vita di bambine e bambini: i dati italiani della sorveglianza “OKkio alla SALUTE 2023” e il contributo dello studio “EPaS-ISS”, Roma (10 May 2024).
- Tiwari, A.; Balasundaram, P. Public Health Considerations Regarding Obesity. 2023 Jun 5. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 34283488.
- Marcus, C.; Danielsson, P.; Hagman, E. Pediatric obesity-Long-term consequences and effect of weight loss. J Intern Med. 2022; 292(6):870-891. [CrossRef]
- Friedemann, C.; Heneghan, C.; Mahtani, K.; Thompson, M.; Perera, R.; Ward, A.M. Cardiovascular disease risk in healthy children and its association with body mass index: systematic review and meta-analysis. BMJ. 2012; 345:e4759. [CrossRef]
- Chung, S.T.; Krenek, A.; Magge, S.N. Childhood Obesity and Cardiovascular Disease Risk. Curr Atheroscler Rep. 2023; 25(7):405-415. [CrossRef]
- Umano, G.R.; Galderisi, A.; Aiello, F.; Martino, M.; Camponesco, O.; Di Sessa, A.; Marzuillo, P.; Alfonso, P.; Miraglia Del Giudice, E. Obstructive sleep apnea (OSA) is associated with the impairment of beta-cell response to glucose in children and adolescents with obesity. Int J Obes (Lond). 2023 Apr;47(4):257-262. [CrossRef]
- Deng, X.; Ma, J.; Yuan, Y.; Zhang, Z.; Niu, W. Association between overweight or obesity and the risk for childhood asthma and wheeze: an updated meta-analysis on 18 articles and 73252 children. Pediatr Obes 2019; 14: e12532. [CrossRef]
- Umano, G.R.; Rondinelli, G.; Luciano, M.; Pennarella, A.; Aiello, F.; Mangoni di Santo Stefano, G.S.R.C.; Di Sessa, A.; Marzuillo, P.; Papparella, A.; Miraglia Del Giudice, E. Pediatric Sleep Questionnaire Predicts Moderate-to-Severe Obstructive Sleep Apnea in Children and Adolescents with Obesity. Children (Basel). 2022 Aug 27;9(9):1303. [CrossRef]
- Marzuillo, P.; Di Sessa, A.; Umano, G.R.; Nunziata, L.; Cirillo, G.; Perrone, L.; Miraglia Del Giudice, E.; Grandone, A. Novel association between the nonsynonymous A803G polymorphism of the N-acetyltransferase 2 gene and impaired glucose homeostasis in obese children and adolescents. Pediatr Diabetes. 2017 Sep;18(6):478-484. [CrossRef]
- Santoro, N.; Amato, A. Grandone, A.; Brienza, C.; Savarese, P.; Tartaglione, N.; Marzuillo, P.; Perrone, L.; Miraglia Del Giudice, E. Predicting metabolic syndrome in obese children and adolescents: look, measure and ask. Obes Facts. 2013; 6(1):48-56. [CrossRef]
- Eslam, M.; Alkhouri, N.; Vajro, P.; Baumann, U.; Weiss, R.; Socha, P.; Marcus, C.; Lee, W.S.; Kelly, D.; Porta, G.; El-Guindi, M.A.; Alisi, A.; Mann, J.P.; Mouane, N.; Baur, L.A.; Dhawan, A.; George, J. Defining paediatric metabolic (dysfunction)-associated fatty liver disease: an international expert consensus statement. Lancet Gastroenterol Hepatol 2021; 6: 864–73. [CrossRef]
- Maguolo, A.; Maffeis, C. Acanthosis nigricans in childhood: a cutaneous marker that should not be underestimated, especially in obese children. Acta Paediatr 2020; 109: 481–87. [CrossRef]
- Molina-Garcia, P.; Migueles, J.H., Cadenas-Sanc,0ez, C.; Esteban-Cornejo, I.; Mora-Gonzalez, J.; Rodriguez-Ayllon, M.; Plaza-Florido, A.; Vanrenterghem, J.; Ortega, F.B.; A systematic review on biomechanical characteristics of walking in children and adolescents with overweight/obesity: possible implications for the development of musculoskeletal disorders. Obes Rev 2019; 20: 1033–44. [CrossRef]
- Di Sessa, A.; Passaro, A.P. Colasante, A.M.; Cioffi, S.; Guarino, S.; Umano, G.R., Papparella, A.; Miraglia Del Giudice, E.; Marzuillo, P. Kidney damage predictors in children with metabolically healthy and metabolically unhealthy obesity phenotype. Int J Obes (Lond). 2023 Dec;47(12):1247-1255. [CrossRef]
- Mahumud, R.A.; Sahle, B.W.; Owusu-Addo, E.; Chen, W.; Morton, R.L.; Renzaho, A.M.N. Association of dietary intake, physical activity, and sedentary behaviours with overweight and obesity among 282,213 adolescents in 89 low and middle income to high-income countries. Int J Obes 2021; 45: 2404–18. [CrossRef]
- Liberali, R.; Kupek, E. Dietary patterns and childhood obesity risk: A systematic review. Child Obes 2020; 16: 70–85. [CrossRef]
- Fang, K.; Mu, M.; Liu, K.; He, Y. Screen time and childhood overweight/obesity: a systematic review and meta-analysis. Child Care Health Dev 2019; 45: 744–53. [CrossRef]
- Robinson, T.N.; Banda, J.A.; Hale, L.; Lu, A.S.; Fleming-Milici, F.; Calvert, S.L.; Wartella E. Screen media exposure and obesity in children and adolescents. Pediatrics 2017; 140 (suppl 2): S97–101. [CrossRef]
- Farooq, A.; Martin, A.; Janssen, X.; Wilson, M.G.; Gibson, A,M.; Hughes, A.; Reilly, J.J. Longitudinal changes in moderate-to-vigorous-intensity physical activity in children and adolescents: a systematic review and meta-analysis. Obes Rev 2020; 21: e12953. [CrossRef]
- Felső, R.; Lohner, Hollódy, K.; Erhardt, É.; Molnár, D. S. Relationship between sleep duration and childhood obesity: systematic review including the potential underlying mechanisms. Nutr Metab Cardiovasc Dis 2017; 27: 751–61. [CrossRef]
- Mihrshahi, S.; Baur, L.A. What exposures in early life are risk factors for childhood obesity? J Paediatr Child Health 2018; 54: 1294–98. [CrossRef]
- Woo Baidal, J.A.; Locks, L.M.; Cheng ER, Blake-Lamb TL, Perkins ME, Taveras EM. Risk factors for childhood obesity in the first 1,000 days: a systematic review. Am J Prev Med 2016; 50: 761–79. [CrossRef]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and Management of Childhood Obesity and Its Psychological and Health Comorbidities. Annu Rev Clin Psychol. 2020 May; 16:351-378. [CrossRef]
- Maffeis, C.; Olivieri, F.; Valerio, G.; Verduci, E.; Licenziati, M.R.; Calcaterra, V; Pelizzo, G.; Salerno, M.; Staiano, A.; Bernasconi, S.; Buganza R, Crinò, A.; Corciulo, N.; Corica, D.; Destro, F., Di Bonito, P.; Di Pietro, M.; Di Sessa, A.; deSanctis, L.; Faienza, M.F.; Filannino, G.; Fintini, D.; Fornari, E.; Franceschi, R.; Franco, F.; Franzese, A.; Giusti, L.F.; Grugni, G.; Iafusco, D.; Iughetti, L.; Lera, R.; Limauro, R.; Maguolo, A.; Mancioppi, V.; Manco, M.; Del Giudice, E.M, Morandi, A.; Moro, B.; Mozzillo, E.; Rabbone, I.; Peverelli, P.; Predieri, B.; Purromuto, S.; Stagi, S.; Street, M.E.; Tanas, R.; Tornese, G.; Umano, G.R.; Wasniewska, M. The treatment of obesity in children and adolescents: consensus position statement of the Italian society of pediatric endocrinology and diabetology, Italian Society of Pediatrics and Italian Society of Pediatric Surgery. Ital J Pediatr. 2023;49(1):69. [CrossRef]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity-Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2017; 102(3):709-757. [CrossRef]
- Hampl, S.E.; Hassink, S.G.; Skinner, A.C.; Armstrong, S.C.; Barlow, S.E.; Bolling, C.F.; Avila Edwards, K.C.; Eneli, I.; Hamre, R.; Joseph, M.M.; Lunsford, D.; Mendonca, E.; Michalsky, M.P.; Mirza, N.; Ochoa, E.R.; Sharifi, M.; Staiano, A.E.; Weedn, A.E.; Flinn, S.K.; Lindros, J.; Okechukwu, K. Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity. Pediatrics. 2023 Feb 1;151(2):e2022060640. Erratum in: Pediatrics. 2024 Jan 1;153(1):e2023064612. doi: 10.1542/peds.2023-064612. [CrossRef]
- Hassan, H.; Snoeck Henkemans, S.; van Teeffelen, J.; Kornelisse, K.; Bindels, P.J.E.; Koes, B.W.; van Middelkoop, M. Determinants of dropout and compliance of children participating in a multidisciplinary intervention programme for overweight and obesity in socially deprived areas. Fam. Pract. 2023, 40, 345–351. [CrossRef]
- Ligthart, K.A.M.; Buitendijk, L.; Koes, B.W.; van Middelkoop, M. The association between ethnicity, socioeconomic status and compliance to pediatric weight-management interventions—A systematic review. Obes. Res. Clin. Pract. 2017, 11 (Suppl. S1), 1–51. [CrossRef]
- Jensen, C.D.; Aylward, B.S.; Steele, R.G. Predictors of attendance in a practical clinical trial of two pediatric weight management interventions. Obesity 2012, 20, 2250–2256.
- Hagman, E.; Johansson, L.; Kollin, C.; Marcus, E.; Drangel, A.; Marcus, L.; Marcus, C.; Danielsson, P. Effect of an interactive mobile health support system and daily weight measurements for pediatric obesity treatment, a 1-year pragmatical clinical trial. Int J Obes (Lond). 2022 Aug;46(8):1527-1533. [CrossRef]
- Metzendorf, M.I.; Wieland, L.S.; Richter, B. Mobile health (m-health) smartphone interventions for adolescents and adults with overweight or obesity. Cochrane Database Syst Rev. 2024;2(2):CD013591. [CrossRef]
- Park, J.; Park, M.J.; Seo, Y.G. Effectiveness of Information and Communication Technology on Obesity in Childhood and Adolescence: Systematic Review and Meta-analysis. J Med Internet Res. 2021;23(11):e29003. [CrossRef]
- Azevedo, L.B.; Stephenson, J.; Ells, L. et al. The effectiveness of e-health interventions for the treatment of overweight or obesity in children and adolescents: A systematic review and meta-analysis. Obes Rev. 2022; 23(2):e13373. [CrossRef]
- DeSilva, S.; Vaidya, S.S. The Application of Telemedicine to Pediatric Obesity: Lessons from the Past Decade. Telemed J E Health. 2021; 27(2):159-166. [CrossRef]
- Alotaibi, M.; Alnajjar, F.; Cappuccio, M.; Khalid, S.; Alhmiedat, T.; Mubin, O. Efficacy of Emerging Technologies to Manage Childhood Obesity. Diabetes Metab Syndr Obes. 2022; 15:1227-1244. Erratum in: Diabetes Metab Syndr Obes. 2023; 16:2537-2538. doi: 10.2147/DMSO.S436332. [CrossRef]
- Quelly, S.B.; Norris, A.E.; DiPietro, J.L. Impact of mobile apps to combat obesity in children and adolescents: A systematic literature review. J Spec Pediatr Nurs. 2016; 21(1):5-17. [CrossRef]
- WHO Multicentre Growth Reference Study Group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr Suppl. 2006; 450:76-85. [CrossRef]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007; 85(9):660-7. [CrossRef]
- Umano, G.R.; Grandone, A.; Di Sessa, A.; Cozzolino, D.; Pedullà, M.; Marzuillo, P.; Del Giudice, E.M. Pediatric obesity-related non-alcoholic fatty liver disease: waist-to-height ratio best anthropometrical predictor. Pediatr Res. 2021; 90(1):166-170. [CrossRef]
- Cole, T.J. The LMS method for constructing normalized growth standards. Eur J Clin Nutr. 1990; 44(1):45-60.
- Wilding, J.P.H.; Batterham, R.L.; Calanna, S.; Davies, M.; Van Gaal, L.F.; Lingvay, I.; McGowan, B.M.; Rosenstock, J.; Tran, M.T.D.; Wadden, T.A.; Wharton, S.; Yokote, K.; Zeuthen, N.; Kushner, R.F.; STEP 1 Study Group. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021 18;384(11):989-1002. [CrossRef]
- Ryder, J.R.; Kelly, A.S.; Freedman, D.S. Metrics matter: Toward consensus reporting of BMI and weight-related outcomes in pediatric obesity clinical trials. Obesity (Silver Spring). 2022; 30(3):571-572. [CrossRef]
- Reinehr, T.; Lass, N.; Toschke, C.; Rothermel, J.; Lanzinger, S.; Holl, R.W. Which Amount of BMI-SDS Reduction Is Necessary to Improve Cardiovascular Risk Factors in Overweight Children? J Clin Endocrinol Metab. 2016; 101(8):3171-9. [CrossRef]
- Teixeira, P.J.; Going, S.B.; Houtkooper, L.B.; Cussler, E.C.; Metcalfe, L.L.; Blew, R.M.; Sardinha, L.B.; Lohman, T.G. Pretreatment predictors of attrition and successful weight management in women. Int J Obes Relat Metab Disord. 2004;28(9):1124-33. [CrossRef]
- Jelalian, E.; Hart, C.N.; Mehlenbeck, R.S.; Lloyd-Richardson, E.E.; Kaplan, J.D.; Flynn-O’Brien, K.T.; Wing, R.R. Predictors of attrition and weight loss in an adolescent weight control program. Obesity (Silver Spring). 2008; 16(6):1318-23. [CrossRef]
- Luppino, G.; Wasniewska, M.; Casto, C.; Ferraloro, C.; Li Pomi, A.; Pepe, G.; Morabito, L.A.; Alibrandi, A.; Corica, D.; Aversa T. Treating Children and Adolescents with Obesity: Predictors of Early Dropout in Pediatric Weight-Management Programs. Children (Basel). 2024; 11(2):205. [CrossRef]
- Jensen, C.D.; Aylward, B.S.; Steele, R.G. Predictors of attendance in a practical clinical trial of two pediatric weight management interventions. Obesity (Silver Spring). 2012; 20(11):2250-6. [CrossRef]
- Rojo, M.; Lacruz, T.; Solano, S.; Gutiérrez, A.; Beltrán-Garrayo, L.; Veiga, O.L.; Graell, M.; Sepúlveda, A.R. Family-reported barriers and predictors of short-term attendance in a multidisciplinary intervention for managing childhood obesity: A psycho-family-system based randomised controlled trial (ENTREN-F). Eur Eat Disord Rev. 2022;30(6):746-759. [CrossRef]
- Skelton, J.A.; Beech, B.M. Attrition in paediatric weight management: a review of the literature and new directions. Obes Rev. 2011; 12(5):e273-81. [CrossRef]
- Roth, L.; Ordnung, M.; Forkmann, K.; Mehl, N.; Horstmann, A. A randomized-controlled trial to evaluate the app-based multimodal weight loss program zanadio for patients with obesity. Obesity (Silver Spring). 2023; 31(5):1300-1310. [CrossRef]
- Desmet, M.; Fillon, A.; Thivel, D.; Tanghe, A.; Braet, C. Attrition rate and predictors of a monitoring mHealth application in adolescents with obesity. Pediatr Obes. 2023; 18(11):e13071. [CrossRef]
- Reinehr, T.; Andler, W. Changes in the atherogenic risk factor profile according to degree of weight loss. Arch Dis Child. 2004; 89(5):419-22. [CrossRef]
- Szczyrska, J.; Brzeziński, M.; Szlagatys-Sidorkiewicz, A. Long-term effects of 12-month integrated weight-loss programme for children with excess body weight- who benefits most? Front Endocrinol (Lausanne). 2023; 14:1221343. [CrossRef]
Figure 1.
Drop-out and 6-month follow-up rates according to allocation group.
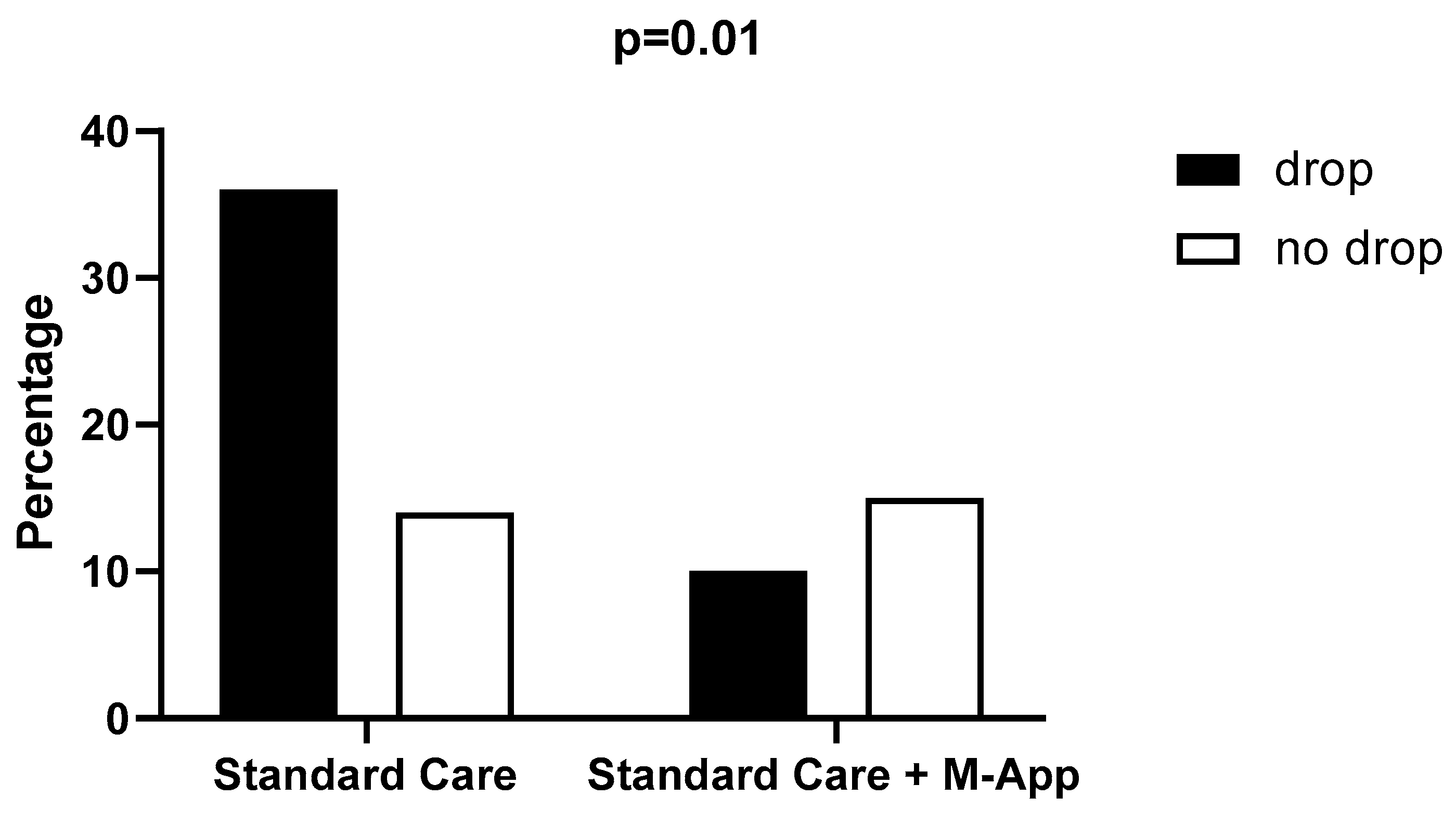
Figure 2.
Differences in delta Z-score BMI at 6-month follow-up between standard care and M-App groups.
Figure 2.
Differences in delta Z-score BMI at 6-month follow-up between standard care and M-App groups.
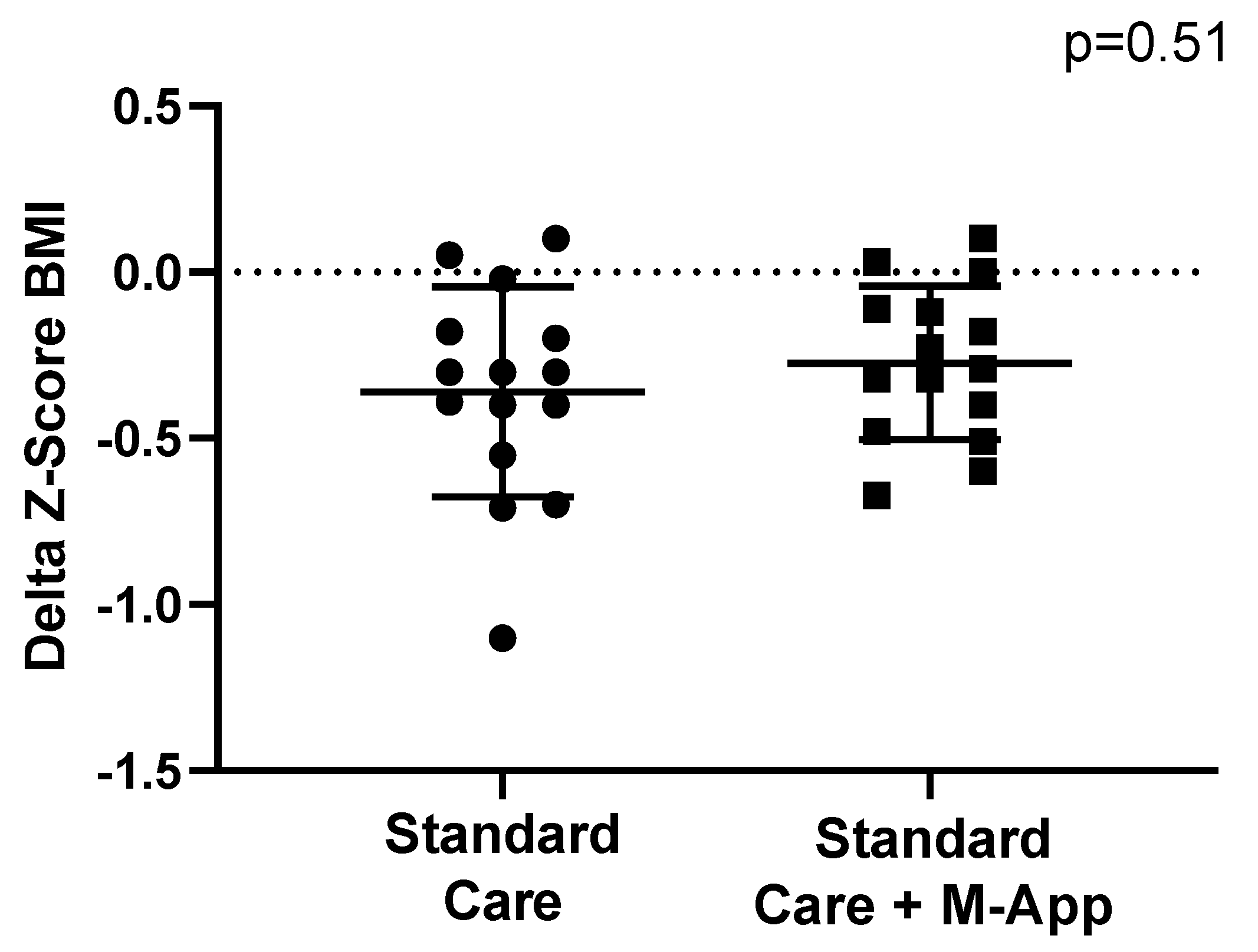
Figure 3.
Differences in BMI percentage reduction at 6-month follow-up between standard care and M-App groups.
Figure 3.
Differences in BMI percentage reduction at 6-month follow-up between standard care and M-App groups.
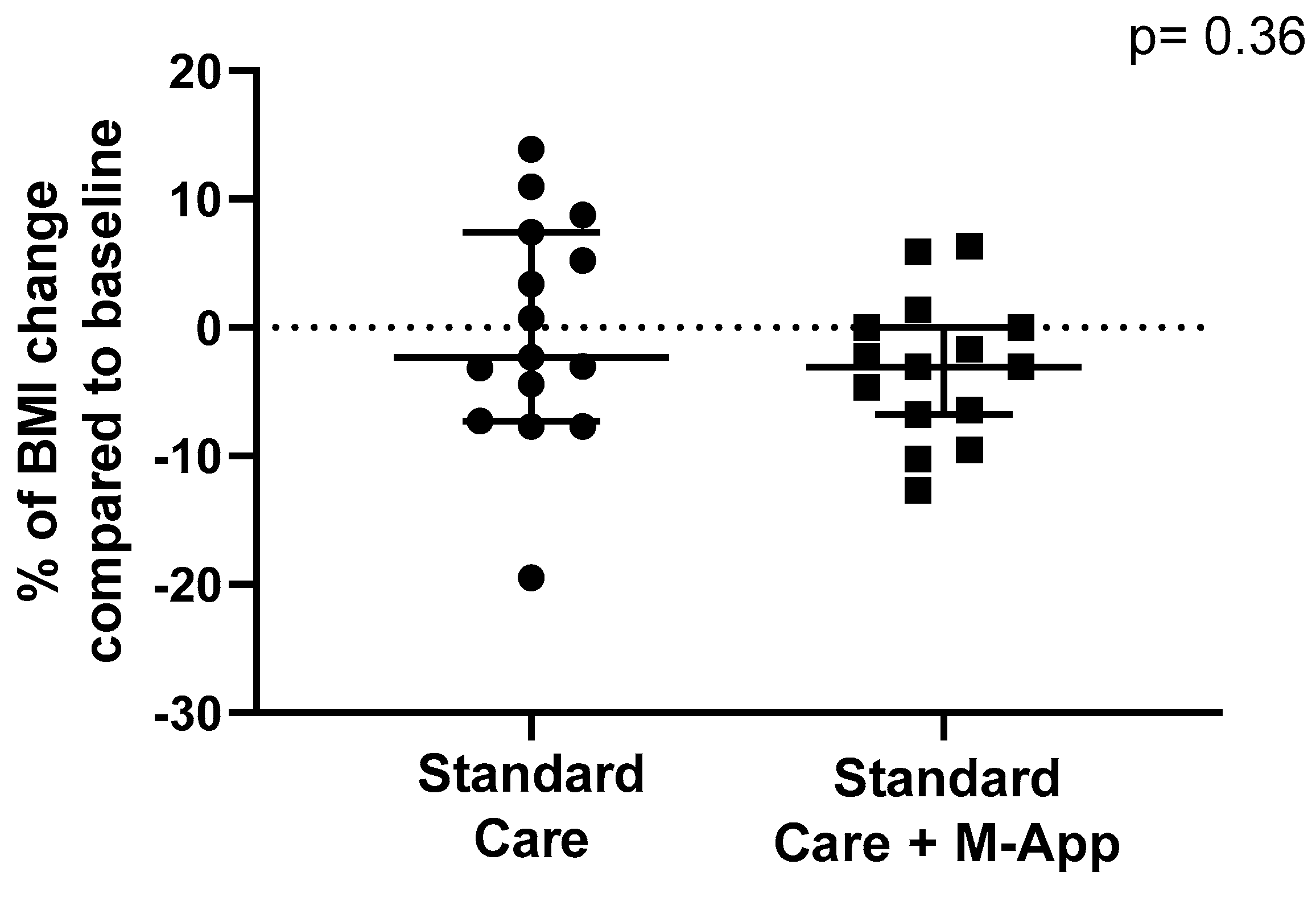

Table 1.
Characteristics of the entire cohort.
| Parameter | data |
|---|---|
| Subjects (n) | 75 |
| Male (%) | 48 |
| Age (IQR) [years] | 9.4 ± 1.5 |
| BMI (IQR) [kg/m2] | 27.6 ± 4.1 |
| Z-score BMI | 3.1 ± 0.7 |
| Systolic Blood Pressure [mmHg] | 113 ± 15 |
| Diastolic Blood Pressure [mmHg] | 69 ± 9 |
| Waist Circumference [cm] | 85 ± 10 |
| Waist-to-Height ratio | 0.59 ± 0.06 |
Table 2.
Characteristics of the groups according to intervention.
| Standard Care+M-App | Standard Care | p | |
|---|---|---|---|
| Subjects (n) | 25 | 50 | |
| Male (%) | 44 | 50 | 0.81 |
| Age (IQR) [years] | 10.6 (8.3-10.9) | 9.3 (8-10.3) | 0.20 |
| BMI (IQR) [kg/m2] | 28.1 (25.2-29.5) | 26.8 (24.3-29.9) | 0.99 |
| Z-score BMI (IQR) | 2.9 (2.8-3.3) | 3.3 (2.55-3.65) | 0.32 |
| Systolic Blood Pressure (IQR) [mmHg] | 111 (105-118) | 111 (100-125) | 0.45 |
| Diastolic Blood Pressure (IQR) [mmHg] | 67 (59-75) | 70 (65-80) | 0.14 |
| Waist Circumference (IQR) [cm] | 86 (79-90) | 84 (78-91) | 0.97 |
| Waist-to-Height ratio (IQR) | 0.58 (0.56-0.6) | 0.61 (0.55-0.65) | 0.14 |
Table 3.
Baseline characteristics according to drop-out and 6-months of follow-up.
| Dropped-out | Returned at follow-up | p | |
|---|---|---|---|
| Subjects (n) | 46 | 29 | |
| Male (%) | 58 | 41 | 0.48 |
| Age (IQR) [years] | 9.6 (8.4-10.7) | 9.1 (8.1-10.6) | 0.35 |
| BMI (IQR) [kg/m2] | 26.9 (24.8-31.1) | 28.3 (24.0-29.7) | 0.40 |
| Z-score BMI (IQR) | 3.0 (2.4-3.5) | 3.2 (2.9-3.7) | 0.27 |
| Systolic Blood Pressure (IQR) [mmHg] | 113 (104-125) | 111 (100-125) | 0.72 |
| Diastolic Blood Pressure (IQR) [mmHg] | 71 (60-75) | 70 (60-80) | 0.85 |
| Waist Circumference (IQR) [cm] | 84 (79-89) | 89 (77-94) | 0.27 |
| Waist-to-Height ratio (IQR) | 0.60 (0.57-0.63) | 0.59 (0.54-0.65) | 0.47 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



