
Submitted:
02 August 2024
Posted:
05 August 2024
You are already at the latest version
Abstract
Glioblastomas (GBMs) are the most malignant and intractable of all cancers, with an unfavourable clinical prognosis for affected patients. The objective was analysis the sensitivity of GBM cells to the antimicrobial peptides (AMPs) cathelicidin (LL-37) and protegrin-1 (PG-1), both alone and in combination with chemotherapy, to predict overall survival (OS) in the patients. The study was conducted on 27 GBM patients treated in the neurosurgical departments of the Almazov Medical Research Centre (Saint-Petersburg, Russia) from 2021 to 2024. The cytotoxic effects of chemo-therapy, AMPs and their combinations on brain tumor cells were assessed by MTT assay using 50%-inhibitory concentration (IC50). In GBM cells from the patients, LL-37 and PG-1 exhibited strong anticancer effects, surpassing those of chemotherapy drugs. These LL-37 and PG-1 anti-cancer effects were associated with a statistically significant increase in life expectancy and OS in GBM patients. These findings were confirmed by the experiments on rats with C6 glioma, where intranasal administration of LL-37 (300 μM) and PG-1 (600 μM) increased the life expectancy of the animals to 69 and 55 days, respectively, compared to 24 days in the control group (HR=4.139, p=0.0005; HR=2.542, p=0.0759). Additionally, the combination of LL-37 and PG-1 with chemo-therapy drugs showed that a high IC50 of LL-37 with cisplatin (cutoff >800 μM) in GBM cells was associated with increased life expectancy (19 vs 5 months, HR=4.708, p=0.0101) and OS in GBM patients. These combinations could be used in future GBM treatments.
Keywords:
glioblastoma
; LL-37
; PG-1
; cytotoxicity
; chemotherapy drugs
; combinations of LL-37
; PG-1 with chemotherapy
; overall survival of the GBM patients
1. Introduction
Oncological diseases currently present significant social and economic challenges [1]. According to estimates from the World Health Organization (WHO) and the International Agency for Research on Cancer (Globocan), in 2020, there were 19,292,789 new cases of cancer and 9,958,133 cancer-related deaths worldwide [2]. The prevalence of primary brain and central nervous system tumors was assessed at 308,102 cases in 2020 [3]. Glioblastoma multiforme (GBM) is the most frequent and aggressive brain tumor in adults, accounting for 85-90% of all human brain tumors [4]. The Clinical prognosis for the patients with these tumors is unfavorable with a life expectancy of only 14.6 months and a 100% relapse rate [5].
Current GBM treatment includes neurosurgery, radiotherapy, and chemotherapy with temozolomide (TMZ) [4,6]. The most effective chemotherapy drugs for GBM treatment are ТMZ, cisplatin (CSP), carboplatin (CARB), etoposide (ETO), and doxorubicin (DOX) [4,7,8,9]. Several factors contribute to the failure of GBM therapy, including the heterogeneity of GBMs, which encompasses GBM stem cells (GSCs) that are often resistant to radiochemotherapy [10]. This heterogeneity is also due to the expression of various surface and intracellular markers that contribute to the development of multidrug resistance, tumor metastases and relapses in treated patients [11].
A new approach to cancer therapy may involve the use of cationic antimicrobial peptides (AMPs) or their combinations with chemotherapy drugs. To date, more than 23,253 AMPs have been identified [12]. Most AMPs are composed of 12–50 amino acid molecules with a high content of arginine and/or lysine. AMPs exhibit different structures and possess antimicrobial, antiviral, immunomodulatory activities, with some demonstrating anticancer effects [13]. These effects depend on the structural characteristics and mechanisms of each peptide. In this study, we focused on two neutrophilic peptides with different structures: human cathelicidin (LL-37) with an α-helical structure, and pig protegrin-1 (PG-1) with a β-hairpin conformation. Cathelicidin LL-37 shows multidirectional tissue-specific actions: increased expression of the cathelicidin antimicrobial peptide (CAMP) gene and its secretion are associated with the progression of lung epithelial adenocarcinoma (A549), breast cancer (MCF-7, MDA-MB-435s, MDA-MB-231), pancreas, prostate, ovaries, A375, A875 skin melanoma and oral squamous cell carcinoma cells. Conversely, the expression of the CAMP gene and LL-37 secretion levels are significantly inhibited in stomach, HT-29, HCT116 colon cancers, HL-60, MG63 acute myeloid, K562 erythromyeloid leukemia, U937 lymphoma, and SH-SY5Y neuroblastoma cells [14,15].
Recently, we also demonstrated that LL-37 induces cell death in C6 and U251 glioma cells [16,17,18]. However, at high concentrations, these peptides are toxic to human cells, which poses a challenge for their use in medical practice [19]. One potential solution to this challenge is reducing the effective concentrations of AMPs. This reduction can be achieved through the synergistic anticancer effects of combining LL-37 and PG-1 with chemotherapy drugs. The sensitivity of GBM to LL-37, PG-1 antimicroblal peptides, as well as their combinations with chemotherapy, for predicting patient survival remains unexplored.
The aim of the study was to analyse the sensitivity of GBM cells to the antimicrobial peptides LL-37, PG-1, both alone and in combination with chemotherapy, to predict the OS of GBM patients.
2. Materials and Methods
2.1. Clinical Characteristics of Patients
The study involved 27 GBM patients treated in the neurosurgical departments of the Almazov Medical Research Centre (Saint-Petersburg, Russia) from 2021 to 2024. All patients provided informed consent and underwent surgical resections, MRI in the neurology departments, and histological verification in the pathomorphological departments. The investigation was approved by the local Ethics Committee of the Institute of Experimental Medicine (№ 6/20, from 10/21/2020).
2.2. Cell Culture
Biopsies of tumors were collected from the patients. Primary GBM samples were cut into small (2–4 mm) pieces under sterile conditions, and washed to remove blood and necrotic elements. Tumor cells were dissociated in a 0.25% trypsin solution in EDTA for 5–10 min at 37°C and cultured at a concentration of 1×104 cells per well in 96-well flat-bottomed plates (TPP, Trasadingen, Switzerland). The cells were maintained in Dulbecco’s Modified Eagle Medium (DMEM, Sigma-Aldrich, St.-Louis, MO, USA) containing 10% fetal bovine serum (Sigma-Aldrich, St. Louis, MO, USA) and gentamicin sulfate 10−4 g/mL (Shandong Weifang Pharmaceutical Factory Co., Weifang, China) in a CO2 incubator (Heracell, Waltham, MA, USA) at 37◦C with 95% humidity and 5% CO2 for 1–2 days [20,21].
2.3.МТТ. Assay
The cytotoxic effects of chemotherapy, AMPs and their combinations in GBM cells (1×104 cells/well) was assessed using the MTT assay in 96-well flat-bottomed plates [22]. Two-fold serial dilutions of LL-37, PG-1 and 2-10 fold dilutions of chemotherapy drugs, were added in 50 μl of DMEM to the wells of cell culture plates. For testing combinations of two substances, 25 μL of each reagent were added at the appropriate dose. Each dose of the reagents and their combinations were tested in triplicate. As a positive control, 50 μL of DMEM was added to the wells with tumor cells instead of the reagent. As a negative control (0% viable cells), 100 μL of DMEM was added to the empty wells of the plate. Plates with samples were incubated for 24 h at 37°C with 5% CO2. The next day, 25 μL of MTT solution (5 mg/mL) was added to the wells and incubated for 3 h under the same conditions. At the end of incubation, 50 μL of isopropanol with 0.04 N HCl was added to all samples and thoroughly mixed. The optical density of the solution was measured at a wavelength of 540 nm, with the optical density at 590 nm subtracted as background, using a SpectraMax 250 plate spectrophotometer with SoftMax Pro 5.2 software (Molecular Devices, USA). The cytotoxicity of the substances was calculated as the percentage of dead cells based on comparing the optical density of samples with positive (100% viable cells) and negative (0% viable cells) controls according to formula 1:
where DC (%) is the percentage of dead cells in the sample, OD (sample) is the optical density of the sample containing the substance at a given concentration; and OD (0% VC) is the average optical density of wells with a culture medium that does not contain cells.
DC(%)=(OD(control)-OD(sample))/(OD(control)-OD(0% VC))×100
2.4. Determination of IC50 Dose, Combination Index and Combination Effects
To study the anticancer effects of LL-37, PG-1, chemotherapy and their combinations on GBM cells, the dose of 50% inhibition of cell viability (IC50) was calculated. Tumor cells were incubated with LL-37, PG-1, CIS, CARB, DOX, TMZ, and ETO at various concentrations (Table 1).
The IC50 of LL-37, PG-1, chemotherapy and their combinations were calculated by nonlinear regression analysis using Origin Pro 8.5 software. The IC50 of the chemotherapy in each combination was determined based on fixed proportions for each pair, depending on the IC50 values of the chemotherapy according to formula 2:
where W is the proportion of the chemotherapy drug within the combination.
IC50 (substance) = IC (combination) × W
2.5. C6/Wistar Rat Intracerebral Glioma Model
Experiments were performed on 15 Wistar rats weighing 200–300 g, maintained on a standard diet in the vivarium of the Institute of Experimental Medicine (Saint Petersburg, Russia). Each rat was anesthetized by intraperitoneal injection of 10% chloral hydrate (4 ml/kg) and fixed in a prone position using a rat stereotactic device. All rats underwent neurosurgical operations with the inoculation of 1 ×106 C6 glioma cells in 10 µl of saline. The rats were then randomly divided into two groups: control (n = 5) and experimental (n = 10). Control animals received intranasal injections of 20 µl of saline twice a week. In the experimental groups, 20 µl of LL-37 (n = 5) and PG-1 (n = 5) was intranasal were administered intranasally at a dose of 300 µM/ml and 600 µM/ml, respectively, twice a week. The weight, tumor size, and survival of the animals were assessed. The study was approved by the local ethics committee at the Institute of Experimental Medicine (No. 6/20 dated October 21, 2020) [23].
2.6. Reagents
The following reagents were used in the study: human cathelicidin LL-37 (Cat No AS-61302, 1 mg, Anaspec, USA); protegrin-1 (Cat No AS-64819-05, 0.5 mg, Anaspec, USA), gentamicin sulfate (solution of 40 mg/mL, Shandong Weifang Pharmaceutical Factory Co., Liaocheng, China); Doxorubicin-LANS® (solution of 2 mg/mL, Veropharm, Moscow, Russia); Carboplatin-LANS® (solution of 10 mg/mL, Veropharm, Moscow, Russia); temozolomide (Temodal capsules, 100 mg, Orion Pharma, Espoo, Finland); Cisplatin-LANS® (solution of 0.5 mg/mL, Veropharm, Moscow, Russia); etoposide (solution of 20 mg/mL, Ebewe Pharma, Unterach am Attersee, Austria); and a streptavidin–biotin–peroxidase kit (LSAB2, Dako, Glostrup, Denmark).
2.7. Statistical Analysis
All experiments were performed at least in triplicate. The statistical significance of differences between the means of different treatments and their respective control groups was determined using Student’s t-test. Multiple differences between several groups were calculated using a one-way ANOVA test. Data were presented with the standard deviation and considered significant at p < 0.05. To compare the differences between two independent groups with a small number of samples (n < 30), the nonparametric Mann–Whitney U-test was used [24]. Descriptive statistics, ANOVA test, and OS analysis were performed using GraphPad Prism software (version 8.01, 09.21.2020, company, San Diego, CA, USA).
3. Results
3.1. Personalized In Vitro Cytotoxic Effects of Chemotherapy Drugs, LL-37, PG-1 and Their Combinations on Patients' GBM Cells Using the MTT Assay
Initially, we evaluated the anticancer effects of LL-37, PG-1, comparing them to the effects of the chemotherapy drugs on GBMs cells (Table 3).
Table 3 shows that GBM cells from patients exhibited multidrug resistance to chemotherapy drugs. Specifically, GBM cells from patients No. 11961, 6770, 18871, and 114495 were resistant to all five tested drugs. GBM samples from patients No. 11081 and 62642 showed resistance to four drugs: carboplatin, TMZ, CIS, and ETO. GBM cells from patients No. 55068, 25873, and 49142 displayed resistance to doxorubicin, carboplatin, TMZ, and CIS. Additionally, the GBM cells demonstrated personalized sensitivity to the chemotherapy drugs. For instance, the GBM sample from patient No. 57595 was the most sensitive to DOX and TMZ. GBM samples from patients No. 15159, 7934, and 25873 were most sensitive to carboplatin and CIS, respectively. The highest sensitivity to ETO was observed in GBM cells from patient No. 60886.
Notably, GBM cells from patients No. 7934 and 60886 were also most sensitive to LL-37 and PG-1. Both LL-37 and PG-1 exhibited potent anticancer activities (IC50 values ranging from 1.0 to 35.6 μM), surpassing the efficacy of the chemotherapy drugs.
Subsequently, we assessed the effects of combinations of LL-37 and PG-1 with chemotherapy drugs on GBM cells by calculating the IC50 values for these combinations (Table 4 and Table 5).
Data presented in Table 4 and Table 5 reveal that GBM samples No 11961, 6770, 25873, 55068, and 114495 showed increased sensitivity to the combination of LL-37 with DOX compared to DOX alone. Similarly, GBM cells from patients No 6770, 25873, 55068, and 60886 exhibited greater sensitivity to the combination of PG-1 with DOX. Combinations of LL-37 with carboplatin or TMZ were more effective than the individual chemotherapy drug alone for GBM samples No 11081, 7934, and 60886. Additionally, GBM cells from patients No 57595 and 55068 demonstrated enhanced sensitivity to the LL-37 and CARB combination compared to CARB alone. GBM cells from patients No 6770, 49142, and 114495 were more sensitive to the combination of LL-37 with TMZ than to TMZ alone. GBM samples No 11081, 25873, and 60886 also showed increased sensitivity to the combinations of PG-1 with DOX, TMZ, or CIS compared to the individual chemotherapy drugs. Notably, eight out of ten GBM samples were more responsive to the combination of PG-1 with TMZ than to TMZ alone. Furthermore, GBM samples No 11081, 6770, 57595, and 15159 exhibited greater sensitivity to the combinations of LL-37 with CIS or ETO compared to the chemotherapy drugs alone. GBM cells from patients No 25873 and 60886 responded more favourably to the LL-37 and CIS combination, while the sample No 7934 was more sensitive to LL-37 combined with ETO than to ETO alone.
Six from ten GBM samples were more sensitive to the combination of PG-1 with CIS compared to CIS alone. To the combination PG-1 with ETO was more sensitive GBM cells No 6770, 7934, 25873 and 15159. In contrast, GBM cells of the patients also showed resistance to the combinations chemotherapy with LL-37, PG-1, tables 4,5. However, resistance was also observed. GBM samples from patients No 11081, 49142, 57595, and 62642 were more resistant to the combinations of LL-37 or PG-1 with doxorubicin. Additionally, patients No 7934, 49142, 15159, and 60886 showed increased resistance to the LL-37 and doxorubicin combination compared to doxorubicin alone. GBM cells from patients No 11961, 25873, and 15159 exhibited higher resistance to the combinations of LL-37 with carboplatin or TMZ compared to the chemotherapy drugs alone.
Moreover, GBM samples No 6770 and 114495 exhibited greater resistance to the combination of LL-37 with carboplatin compared to carboplatin alone. In contrast, GBM samples No 7934, 49142, 57595, and 62642 demonstrated resistance to the PG-1 + CARB and PG-1 + CIS combinations. GBM cells from patients No 57595 and 55068 were more resistant to the combination of LL-37 with TMZ than to TMZ alone. Interestingly, only two GBM samples, No 15159 and 62642, showed resistance to the combination of PG-1 with TMZ compared to TMZ alone. Furthermore, GBM cells from patients No 49142, 57595, and 62642 were more resistant to the combinations of LL-37 with CIS or ETO than to these drugs alone. The same patients, along with No 57595, also exhibited increased resistance to the combinations of PG-1 with CIS or ETO compared to the individual chemotherapy drugs. GBM samples No 55068, 60886, and 7934 showed higher resistance to the combinations of PG-1 with ETO and CIS than to the drugs alone.
3.2. Prediction of GBM Patients’ Overall Survival Based on IC50 Values of Chemotherapy Drugs, LL-37, PG-1 and Their Combinations
We calculated the OS of GBM patients based on the IC50 values of chemotherapy drugs, LL-37, PG-1, and their combinations, as illustrated in Figure 1, Figure 2 and Figure 3.
Data in Figure 1 demonstrate that the median OS of GBM patients varies with different IC50 levels of chemotherapy drugs. For CIS, patients with a low IC50 (cutoff value less than 1.5 mM) had a median OS of 12.0 months, whereas those with a high IC50 (cutoff value greater than 1.5 mM) had a median OS of only 5.5 months (HR = 0.2933, χ² = 4.849, p = 0.0277). For TMZ, patients with a low IC50 (cutoff value less than 10 mM) had a median OS of 10.0 months, compared to 11.0 months for those with a high IC50 (cutoff value greater than 10 mM) (HR = 0.7631, χ² = 0.2057, p = 0.6502). Patients with a low IC50 of ETO (cutoff value less than 12 μM) had a median OS of 12.0 months, whereas those with a high IC50 (cutoff value greater than 12 μM) had a median OS of 10.5 months (HR = 0.4921, χ² = 1.667, p = 0.1966). For DOX, patients with a low IC50 (cutoff value less than 600 μM) had a median OS of 12.0 months, compared to 10.5 months for those with a high IC50 (cutoff value greater than 600 μM) (HR = 0.5863, χ² = 0.5306, p = 0.4664). Finally, for CARB, the median OS was 11.0 months regardless of the IC50 level (cutoff value less than or greater than 3 mM) (HR = 1.108, χ² = 0.02838, p = 0.8662).
Data presented in Figure 2 show that the median OS of GBM patients with a low IC50 of LL-37 (cutoff < 7 μM) was 18.0 months, compared to 9 months for those with a high IC50 of LL-37 (cutoff > 7 μM, HR=0.2881, χ2=6.160, p=0.0131), Fig. 2A. For GBM patients with a low IC50 of the LL-37 and DOX combination (cutoff < 500 μM), the median OS was 12.0 months, whereas it was 8 months for those with a high IC50 (cutoff > 500 μM, HR=0.5958, χ2=0.5819, p=0.4456), Fig. 2B. The median OS for patients with a low IC50 of the LL-37 and CARB combination (cutoff < 1400 μM) was 19.0 months, while for those with a high IC50 (cutoff > 1400 μM), it was 8 months (HR=0.7115, χ2=0.2156, p=0.6424), Fig. 2C. In patients with a low IC50 of the LL-37 and CIS combination (cutoff < 800 μM), the median OS was only 5.0 months, whereas it was 19 months for those with a high IC50 (cutoff > 800 μM, HR=4.708, χ2=6.624, p=0.0101), Fig. 2D. For the LL-37 and ETO combination, patients with a low IC50 (cutoff < 19 μM) had a median OS of 8 months, while those with a high IC50 (cutoff > 19 μM) had a median OS of 12 months (HR=1.678, χ2=0.5819, p=0.4456), Fig. 2E. Lastly, the median OS for patients with a low IC50 of the LL-37 and TMZ combination (cutoff < 1550 μM) was 10 months, compared to 12 months for those with a high IC50 (cutoff > 1550 μM, HR=1.443, χ2=0.2524, p=0.6154), Fig. 2F.
Data in Figure 3 show that the median OS for GBM patients with a low IC50 of PG-1 (cutoff < 7 μM) was 24.0 months, whereas it was only 10 months for those with a high IC50 (cutoff > 7 μM, HR=0.3185, χ2=4.923, p=0.0265), Fig. 3A. For patients with a low IC50 of the PG-1 and doxorubicin combination (cutoff < 215 μM), the median OS was 10.0 months, compared to 24 months for those with a high IC50 (cutoff > 215 μM, HR=1.955, χ2=1.298, p=0.2547), Fig. 3B. The median OS for patients with a low IC50 of the PG-1 and CARB combination (cutoff < 2300 μM) was 8.5 months, while it was 12 months for those with a high IC50 (cutoff > 2300 μM, HR=1.723, χ2=0.5545, p=0.4565), Fig. 3C. For the PG-1 and CIS combination, patients with a low IC50 (cutoff < 850 μM) had a median OS of 12.0 months, compared to 10 months for those with a high IC50 (cutoff > 850 μM, HR=0.6213, χ2=0.5208, p=0.4705), Fig. 3D. The median OS for patients with a low IC50 of the PG-1 and ETO combination (cutoff < 12.5 μM) was 18 months, while it was 8 months for those with a high IC50 (cutoff > 12.5 μM, HR=0.4151, χ2=1.871, p=0.1714), Fig. 3E. Finally, the median OS for patients with a low IC50 of the PG-1 and TMZ combination (cutoff < 2520 μM) was 12 months, compared to 8.5 months for those with a high IC50 (cutoff > 2520 μM, HR=0.5532, χ2=0.8026, p=0.3703), Fig. 3F.
3.3. Study of Survival Rate in Wistar Rats with C6 Glioma Following Intranasal Administration of LL-37 and PG-1
The observed high sensitivity of GBM cells to LL-37 and PG-1, as indicated by low IC50 levels, is statistically significantly associated with increased patient survival. Additionally, low IC50 values for the combination of PG-1 with ETO in GBM cells may correlate with enhanced patient longevity. Conversely, high IC50 levels for the combination of LL-37 with CIS in GBM cells also appear to be associated with extended survival in patients. These findings regarding the in vitro sensitivity of GBM cells to LL-37 and PG-1, and their correlation with patient survival, are supported by our experimental results on Wistar rats with C6 glioma. As illustrated in Fig. 4, the survival rate of these rats was evaluated following intranasal administration of LL-37 and PG-1.
Data in Fig. 4 reveal that the median survival of rats with C6 glioma treated with LL-37 (at a dose of 300 μM) was 69 days, compared to 24 days in the control group (HR=4.139, χ²=11.94, p=0.0005), Fig. 4A. Similarly, the median survival of rats with C6 glioma treated with PG-1 (at a dose of 600 μM) was 55 days, while the control group median survival was 24 days (HR=2.542, χ²=3.151, p=0.0759), Fig. 4B. Additionally, LL-37 treatment significantly reduced the volume of C6 glioma in the rats.
4. Discussion
In this study, we demonstrated that the cationic antimicrobial peptides LL-37 and PG-1 exhibit potent anticancer effects against GBM cells, Table 3. Previous research has shown that LL-37 secretion levels and CAMP gene expression are significantly reduced in colorectal cancer, glioma, and SH-SY5Y neuroblastoma [25,26]. Low expression of the CAMP gene could serve as an important biomarker for these cancers. LL-37's mechanisms of action involve interactions with various receptors, including formyl-peptide receptor-2 (FPR2), C-X-C Motif Chemokine Receptor 2 (CXCR2), purinergic receptors P2Y11 and P2X7, MAS-related GPR family member X2 (MrgX2), EGFR/ErbB1, erb-b2 receptor tyrosine kinase 2 (ERBB2), ligand-gated ion channels (LGIC), insulin-like growth factor 1 receptor (IGF1R), and toll-like receptors (TLRs), which are often overexpressed in tumors compared to normal cells. LL-37 typically binds to the transmembrane regions of these receptors, leading to conformational changes and modulation of receptor activity [27]. Binding of LL-37 to one of the G-protein-coupled receptors, though not yet fully characterized, results in decreased Bcl-2 levels and induces a cascade of apoptotic proteins, including Bax, Bak, Puma, and p53, as well as endonuclease G (EndoG) in HCT116 colorectal cancer cells [28].
Additionally, the expression of the CAMP gene in various cancer cells is inducible, for instance, by vitamin D3 [27]. This underscores the importance of further research to explore the relationship between CAMP expression and tumor development. The potential for LL-37 and its derivatives as therapeutic agents against malignant neoplasms has been extensively discussed in the literature. Several analogues of LL-37 with demonstrated antitumor activity have been developed and patented, highlighting the peptide's promising role in cancer treatment.
The mechanisms underlying PG-1's actions against tumor cells remain underexplored. Experimental data indicate that PG-1 disrupts cellular membranes. It has been shown to exhibit cytotoxic effects against various human cancer cell lines, including K562 erythromyeloid leukaemia, U-937 lymphoma, A-549 and A-431 epithelioid lung carcinoma, MG-63 osteosarcoma, and SH-SY5Y neuroblastoma cells [29,30,31]. Specifically, in MCF-7 cells, PG-1's cytotoxicity is linked to its oligomerization within cell membranes. This oligomerization leads to the formation of transmembrane pores, resulting in intracellular Ca²⁺ influx and inhibition of cyclin-dependent kinase 1A (CDKN1A) and proliferating cell nuclear antigen (PCNA). This cascade of events ultimately triggers apoptosis via p53 protein activation and caspase-3 [32,33]. CDKN1A and PCNA inhibit the transition from the G1 to S phase of the cell cycle, thus blocking cancer cell division and tumor growth [34]. PG-1 interacts with the transmembrane domains of MrgX2, IGF1, and EGF receptors [35,36], leading to the upregulation of p53 and apoptotic genes such as CDKN1A and p21 [34].
The cytotoxic effect of recombinant PG-1 on SH-SY5Y neuroblastoma cells is correlated with the presence of anionic sulfated proteoglycans in the tumor cell membranes. Notably, the membranes of malignant SH-SY5Y neuroblastoma cells exhibit a higher negative charge compared to low-grade tumour cells, which may facilitate the transport of K⁺ and Ca²⁺ ions into the cells. This alteration in transmembrane potential enhances PG-1 binding to these membranes [31]. These findings partially elucidate PG-1’s selective anticancer activity against neuroblastoma cells as opposed to non-neuronal cells like NIH-3T3 and HEK293T fibroblasts. Recent MTT assays and trypan blue staining have demonstrated that both PG-1 and LL-37 exhibit potent anticancer effects at concentrations below 10⁻⁵ M, showing greater efficacy compared to conventional chemotherapy drugs in C6 and U251 glioma cells [16,17].
We assessed the effects of combining LL-37 and PG-1 with various chemotherapy drugs on GBM cells from patients, Tables 4, 5. The combinations of LL-37 and PG-1 with CIS, ETO, and PG-1 with TMZ showed lower IC50 values compared to the IC50 levels of the chemotherapy drugs used alone. These findings align with the observation that these specific combinations of LL-37 with cisplatin and PG-1 with etoposide are associated with improved survival and OS in GBM patients, as shown in Figs. 2 and 3. Furthermore, these combinations also resulted in increased lifespan for rats with C6 glioma following intranasal administration of LL-37 and PG-1, as illustrated in Fig. 4.
Our recent studies have demonstrated that combinations of PG-1 and LL-37 with DOX and CARB exhibit synergistic effects in GBM cells [23]. Using the MTT assay, we identified synergistic effects for the combinations of PG-1 with CARB and LL-37 with ETO, and an additive effect for the combination of PG-1 with TMZ in C6 glioma cells. Additionally, trypan blue staining revealed that combinations of PG-1 with doxorubicin and cisplatin showed synergistic cytotoxic effects on C6 glioma cells [16]. LL-37 also synergistically enhanced the effects of doxorubicin and gentamicin in human K562 erythromyeloid leukaemia cells by increasing the ratio of necrotic and apoptotic cells. For PG-1, synergy was observed in combination with doxorubicin, actinomycin D, or polymyxin B in K562 cells, inducing both necrosis and apoptosis [29].
Both PG-1 and LL-37 enhance the anticancer effects of chemotherapy by damaging cell membranes and/or penetrating intracellularly, demonstrating a more pronounced effect on tumor cells compared to healthy cells. Consequently, PG-1 may be considered a more promising candidate for combination therapy compared to LL-37. To further improve the selectivity of PG-1 towards tumor cells, various strategies could be employed, such as designing new structural analogues of the peptide with optimized properties or creating chimeric molecules that incorporate the protegrin sequence along with specific binding sites for tumor cell markers. The molecular mechanisms by which PG-1 and LL-37 exert their effects on brain tumor cells remain inadequately explored, highlighting the need for continued research in this area.
5. Conclusions
LL-37 and PG-1 exhibit strong in vitro anticancer effects that surpass those of traditional chemotherapy drugs against GBM cells. The anticancer efficacy of LL-37 and PG-1 is significantly correlated with increased life expectancy and OS in GBM patients. This correlation is further supported by experiments showing that intranasal administration of LL-37 and PG-1 significantly extends the lifespan of rats with C6 glioma. Our study also evaluated the effects of combining LL-37 and PG-1 with chemotherapy drugs on GBM cells from patients. We found that both low and high IC50 values of the combinations of PG-1 with etoposide and LL-37 with cisplatin were associated with increased life expectancy and OS in GBM patients. These promising results suggest that such combinations could be developed for future GBM treatments. Overall, these findings underscore the importance of further research into the mechanisms of LL-37, PG-1, and their combinations as potential therapies for brain tumors.
Author Contributions
A.Ch., T.F, S.P. performed the investigations; A.Ch. wrote, reviewed, and edited the manuscript; A. Ts. conducted the statistical analysis, the English translation; A. K., E. F., S. S. performed neurosurgical operations on patients; S.P. performed neurosurgical operations with glioma C6 on the rats; M.M. S.I., O. Sh. A.S. edited the manuscript, performed the supervision and project administration. All authors have read and agreed to the published version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Ministry of Science and Higher Education of the Russian Federation, grant number №075-15-2022-302 (20.04.2022).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the local Ethics Committee of Institute of Experimental Medicine (№ 6/20, from 10/21/2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are openly available on Figshare at 10.6084/m9.figshare.16879432.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors declare no conflict of interest.
References
- Holecki, T.; Węgrzyn, M.; Frączkiewicz-Wronka, A.; Sobczyk, K. Oncological Diseases and Social Costs Considerations on Undertaken Health Policy Interventions. Int J Environ Res Public Health. 2020, 17(8), 2837. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021, 71(3), 209–249. [Google Scholar] [CrossRef] [PubMed]
- The International Agency for Research on Cancer (GLOBOCAN). https://gco.iarc.fr/today/fact-sheets-cancers.
- Hanif, F.; Muzaffar, K.; Perveen, K.; Malhi, S.M.; Simjee, S.U. Glioblastoma Multiforme: A Review of its Epidemiology and Pathogenesis through Clinical Presentation and Treatment. Asian Pac J Cancer Prev. 2017, 18(1), 3–9. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, S.; Dinesan, M.; Ajayakumar, T. Survival and quality of life analysis in glioblastoma multiforme with adjuvant chemoradiotherapy: a retrospective study. Rep Pract Oncol Radiother. 2022, 27(6), 1026–1036. [Google Scholar] [CrossRef]
- Thomas, A.; Noël, G. Medulloblastoma: optimizing care with a multidisciplinary approach. J Multidiscip Healthc 2019, 12, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.; Lee, S.; Kim, H.; Kang, H.; Youn, H.; Jo, S.; et al. Revisiting Platinum-Based Anticancer Drugs to Overcome Gliomas. Int J Mol Sci. 2021, 22(10), 5111. [Google Scholar] [CrossRef] [PubMed]
- Leonard, A.; Wolff, J.E. Etoposide improves survival in high-grade glioma: a meta-analysis. Anticancer Res 2013, 33(8), 3307–15. [Google Scholar] [PubMed]
- Norouzi, M.; Yathindranath, V.; Thliveris, J.A.; Kopec, B.M.; Siahaan, T.J.; Miller, D.W. Doxorubicin-loaded iron oxide nanoparticles for glioblastoma therapy: a combinational approach for enhanced delivery of nanoparticles. Sci. Rep. 2020, 10, 11292. [Google Scholar] [CrossRef] [PubMed]
- Abou-Antoun, T.J., Hale, J.S., Lathia, J.D., Dombrowski, S.M. Brain Cancer Stem Cells in Adults and Children: Cell Biology and Therapeutic Implications. Neurotherapeutics. 2017, 14, 372–384. [CrossRef]
- Olivier, Ch.; Oliver, L.; Lalier, L.; Vallette, F.M. Drug Resistance in Glioblastoma: The Two Faces of Oxidative Stress. Front Mol Biosci. 2021, 7, 620677. [Google Scholar] [CrossRef]
- Ye, G.; Wu, H.; Huang, J.; Wang, W.; Ge, K.; Li, G.; Zhong, J.; Huang, Q. LAMP2: A major update of the database linking antimicrobial peptides. Database. 2020, 2020, baaa061. [Google Scholar] [CrossRef]
- Büyükkiraz, M.E.; Kesmen, Z. Antimicrobial peptides (AMPs): A promising class of antimicrobial compounds. J Appl Microbiol. 2022, 132(3), 1573–1596. [Google Scholar] [CrossRef] [PubMed]
- Wnorowska, U.; Fiedoruk, K.; Piktel, E.; Prasad, S.; Sulik, M.; Janion, M.; Daniluk, T.; Savage, P.B.; Bucki, R. Nanoantibiotics containing membrane-active human cathelicidin LL-37 or synthetic ceragenins attached to the surface of magnetic nanoparticles as novel and innovative therapeutic tools: Current status and potential future applications. J. Nanobiotechnol. 2020, 18, 3. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, K.; Okumura, K.; Isogai, H.; Isogai, E. The Human Cathelicidin Antimicrobial Peptide LL-37 and Mimics are Potential Anticancer Drugs. Front. Oncol. 2015, 5, 144. [Google Scholar] [CrossRef]
- Chernov, A.N.; Tsapieva, A.N.; Alaverdian, D.A.; Filatenkova, T.A.; Galimova, E.S.; Suvorova, M.; Shamova, O.V.; Suvorov, A.N. In vitro evaluation of cytotoxic effect of Streptococcus pyogenes strains, Protegrin PG-1, Cathelicidin LL-37, Nerve Growth Factor and chemotherapy on C6 glioma cell line. Molecules. 2022, 27(2), 569. [Google Scholar] [CrossRef]
- Chernov, A.; Filatenkova, T.; Alaverdian, D.; Tsapieva, A.; Kim, A.; Fedorov, E.; Scliar, S.S.; Matsko, M.V.; Galimova, E.S.; Shamova, O.V. Anticancer Effect of Cathelicidin LL-37, Protegrin PG-1, Nerve Growth Factor NGF, and Temozolomide: Impact on the Mitochondrial Metabolism, Clonogenic Potential, and Migration of Human U251 Glioma Cells. Molecules. 2022, 27, 4988. [Google Scholar] [CrossRef]
- Chernov, A.; Kudryavtsev, I.; Komlev, A.; Alaverdian, D.; Tsapieva, A.; Galimova, E.; Shamova, O. Nerve Growth Factor, Antimicrobial Peptides and Chemotherapy: Glioblastoma Combination Therapy to Improve Their Efficacy. Biomedicines. 2023, 11, 3009. [Google Scholar] [CrossRef]
- Lei, J.; Sun, L.; Huang, S.; Zhu, C.; Li, P.; He, J.; Mackey, V.; Coy, D.H.; He, Q. The antimicrobial peptides and their potential clinical applications. Am. J Transl Res. 2019, 11(7), 3919–3931. [Google Scholar] [PubMed]
- Freshney, R.I.; Griffiths, B.; Hay, R.J.; Reid, Y.A.; Carmiol, S.; Kunz-Schugart, L. Animal Cell Culture: A Practical Approach, 3rd ed.; Masters, J.R.W., Ed.; Oxford University Press: London, UK, 2000. [Google Scholar]
- Neuronal Cell Culture. Methods and Protocols. Eds: Amini, Sh.; White, M.K. Publisher: Humana Totowa, NJ, 2013. [Google Scholar] [CrossRef]
- Riss, T.L.; Moravec, R.A.; Niles, A.L.; Duellman, S.; Benink, H.A.; Worzella, T.J. et al. Assay Guidance Manual. Cell Viability Assays. Bethesda (MD): Eli Lilly & Company and the National Center for Advancing Translational Sciences. 2013. Last Update: July 1, 2016.
- Chernov, A.N.; Kim, A.V.; Skliar, S.S.; Fedorov, E.V.; Tsapieva, A.N.; Сhutko, A.L.; Matsko, M.V.; Galimova, E.S.; Shamova, O.V. Expression of molecular markers and synergistic anticancer effects of chemotherapy with antimicrobial peptides on glioblastoma cells. Cancer Chemother Pharmacol. 2024, 93(5), 455–469. [Google Scholar] [CrossRef]
- van Belle, G.; Fisher, L.D.; Heagerty, P.J.; Lumley, T. Biostatistics: A Methodology for the Health Sciences; Fisher, L.D., van Belle, G., Eds.; Jonh Wiley and Sons Inc.: Hoboken, NJ, USA, 2004. [Google Scholar]
- Piktel, E.; Niemirowicz, K.; Wnorowska, U.; Wątek, M.; Wollny, T.; Głuszek, K.; Góźdź, S.; Levental, I.; Bucki, R. The Role of Cathelicidin LL-37 in Cancer Development. Arch Immunol Ther Exp (Warsz). 2016, 64, 33–46. [Google Scholar] [CrossRef]
- Colle, J-H. ; Périchon, B.; Garcia, A. Antitumor and antibacterial properties of virally encoded cationic sequences. Biologics. 2019, 13, 117–126. [CrossRef]
- Chen, X.; Zou, X.; Qi, G.; Tang, Y.; Guo, Y.; Si, J.; Liang, L. Roles and Mechanisms of Human Cathelicidin LL-37 in Cancer. Cell Physiol. Biochem. 2018, 47(3), 1060–1073. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, K.; Fukuda, T.; Yoneyama, H.; Katayama, M.; Isogai, H.; Okumura, K.; Isogai, E. Anti-proliferative effect of an analogue of the LL-37 peptide in the colon cancer derived cell line HCT116 p53+/+ and p53-/-. Oncol Rep. 2012, 28, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Zharkova, M.S. , Artamonov, A.Yu., Grinchuk, T.M.; Butskina, E.A.; Pazina, T.Yu.; Orlov, D.S.; Shamova, O.V. Peptides of the innate immune system modulate the cytotoxic effect of antitumor antibiotics. Ross. Immunological J. 2016, 10(2), 548–550. [Google Scholar]
- Shamova, O.V.; Orlov, D.S.; Zharkova, M.S.; Balandin, S.V.; Yamschikova, E.V.; Knappe, D.; Hoffmann, R.; Kokryakov, V.N.; Ovchinnikova, T.V. Minibactenecins ChBac7.Nα and ChBac7. Nβ - Antimicrobial Peptides from Leukocytes of the Goat Capra hircus. Acta Naturae. 2016, 8(3), 136–146.
- Soundrarajan, N.; Park, S.; Quy Le Van Chanh, Cho, H-S.; Raghunathan, G.; Ahn, B.; Song, H.; Kim, J-H.; Park, C. Protegrin-1 cytotoxicity towards mammalian cells positively correlates with the magnitude of conformational changes of the unfolded form upon cell interaction. Sci Rep. 2019, 9, 11569. [CrossRef]
- Rothan, H.A.; Mohamed, Z.; Sasikumar, P.G.; Reddy, K.A.; Rahman, N.A.; Yusof, R. In Vitro Characterization of Novel Protegrin-1 Analogues Against Neoplastic Cells. Intern. J. Peptide Res. Ther. 2014, 20(3), 259–267. [Google Scholar] [CrossRef]
- Can, G.; Akpinar, B.; Baran, Y.; Zhivotovsky, B.; Olsson, M. 5-Fluorouracil signaling through a calcium–calmodulin-dependent pathway is required for p53 activation and apoptosis in colon carcinoma cells. Oncogene. 2013, 32, 4529–4538. [Google Scholar] [CrossRef]
- Yan, H.X.; Wu, H.P.; Zhang, H.L.; Ashton, C.; Tong, C.; Wu, J. DNA damage-induced sustained p53 activation contributes to inflammation-associated hepatocarcinogenesis in rats. Oncogene. 2013, 32, 4565–4571. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.; Kotian, A.; Subramanian, H.; Daniell, H.; Ali, H. Activation of human mast cells by retrocyclin and protegrin highlight their immunomodulatory and antimicrobial properties. Oncotarget. 2015, 6, 28573–28587. [Google Scholar] [CrossRef]
- Shamova, O.V.; Orlov, D.S.; Pazina, T.Y.; Yamshchikova, E.V.; Orlov, S.B.; Zharkova, M.S. Study of the molecular and cellular bases of the cytotoxic effect of antimicrobial peptides on tumor cells. Fundamental Res. 2012, 5, 207–212. [Google Scholar]
Figure 1.
Overall survival of GBM patients based on high and low IC50 levels of chemotherapy drugs. The OS of GBM patients was assessed according to their IC50 levels for various chemotherapy drugs. The analysis was conducted using the Mantel-Cox test (χ²), with the following abbreviations: CARB (carboplatin), CIS (cisplatin), DOX (doxorubicin), ETO (etoposide), and TMZ (temozolomide).
Figure 1.
Overall survival of GBM patients based on high and low IC50 levels of chemotherapy drugs. The OS of GBM patients was assessed according to their IC50 levels for various chemotherapy drugs. The analysis was conducted using the Mantel-Cox test (χ²), with the following abbreviations: CARB (carboplatin), CIS (cisplatin), DOX (doxorubicin), ETO (etoposide), and TMZ (temozolomide).
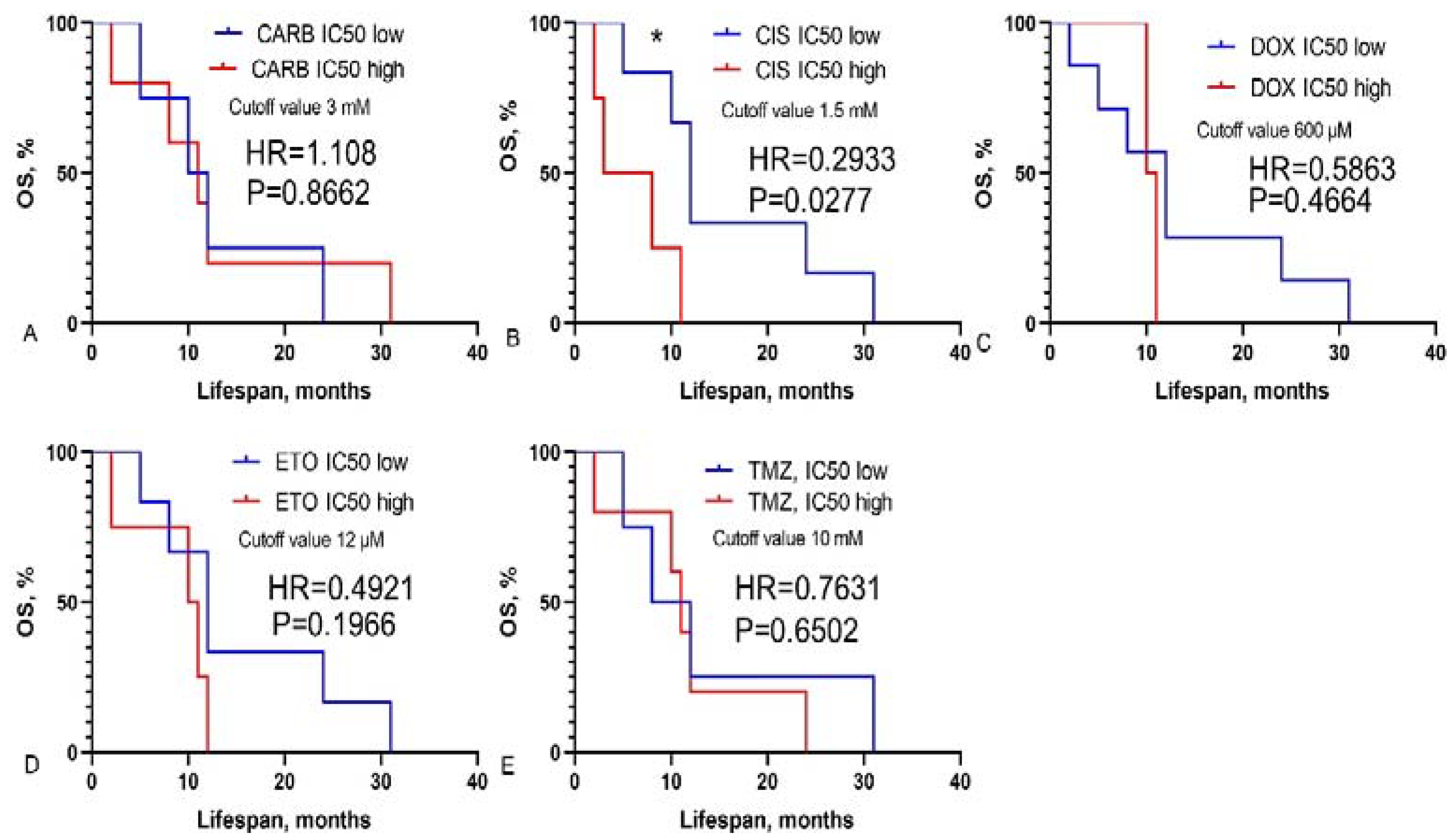
Figure 2.
Overall survival of GBM patients based on high and low IC50 levels of combinations of LL-37 with chemotherapy drugs. Mantel-Cox test, χ2.
Figure 2.
Overall survival of GBM patients based on high and low IC50 levels of combinations of LL-37 with chemotherapy drugs. Mantel-Cox test, χ2.
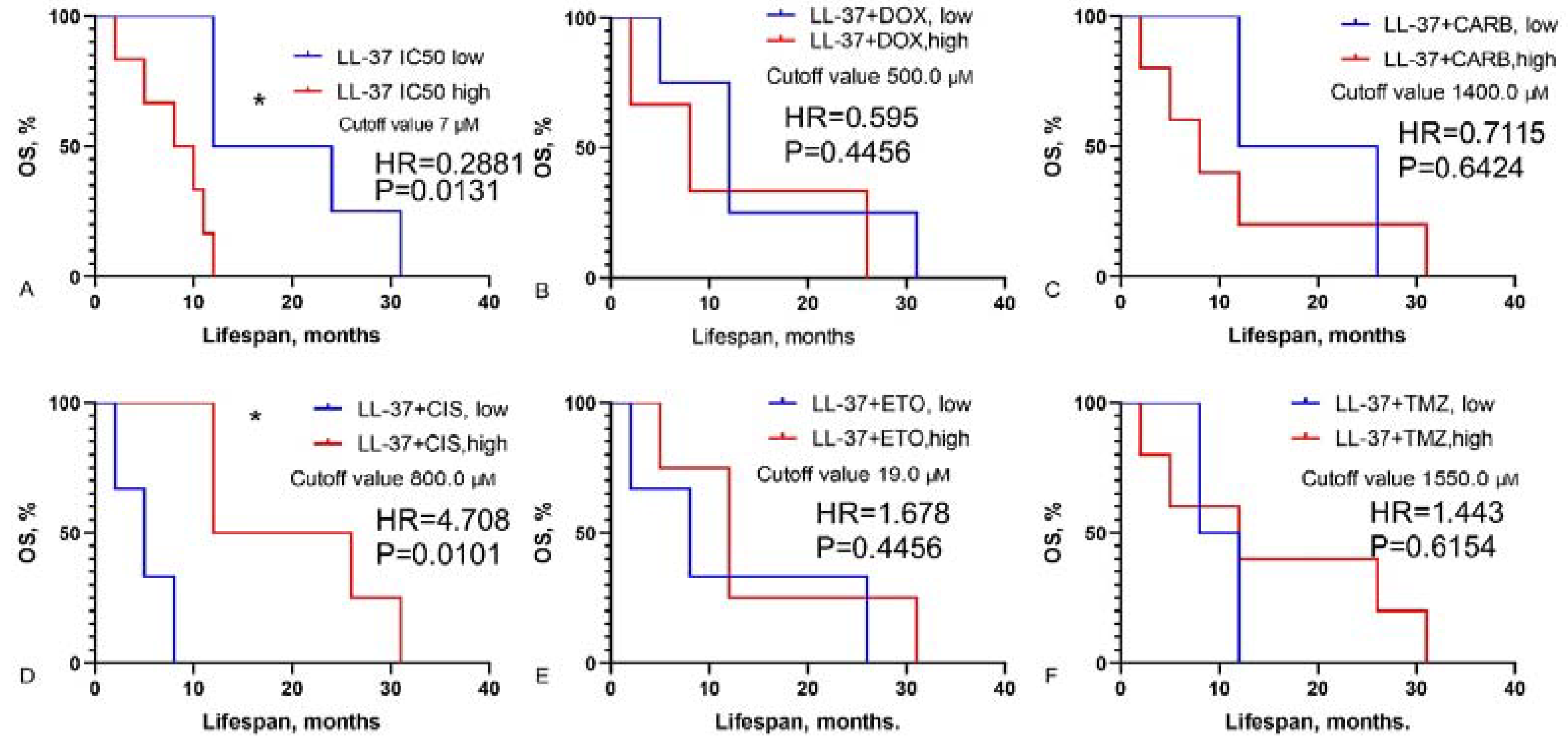
Figure 3.
Overall survival of GBM patients based on high and low IC50 levels of combinations of PG-1 with chemotherapy drugs. Mantel-Cox test, χ2.
Figure 3.
Overall survival of GBM patients based on high and low IC50 levels of combinations of PG-1 with chemotherapy drugs. Mantel-Cox test, χ2.
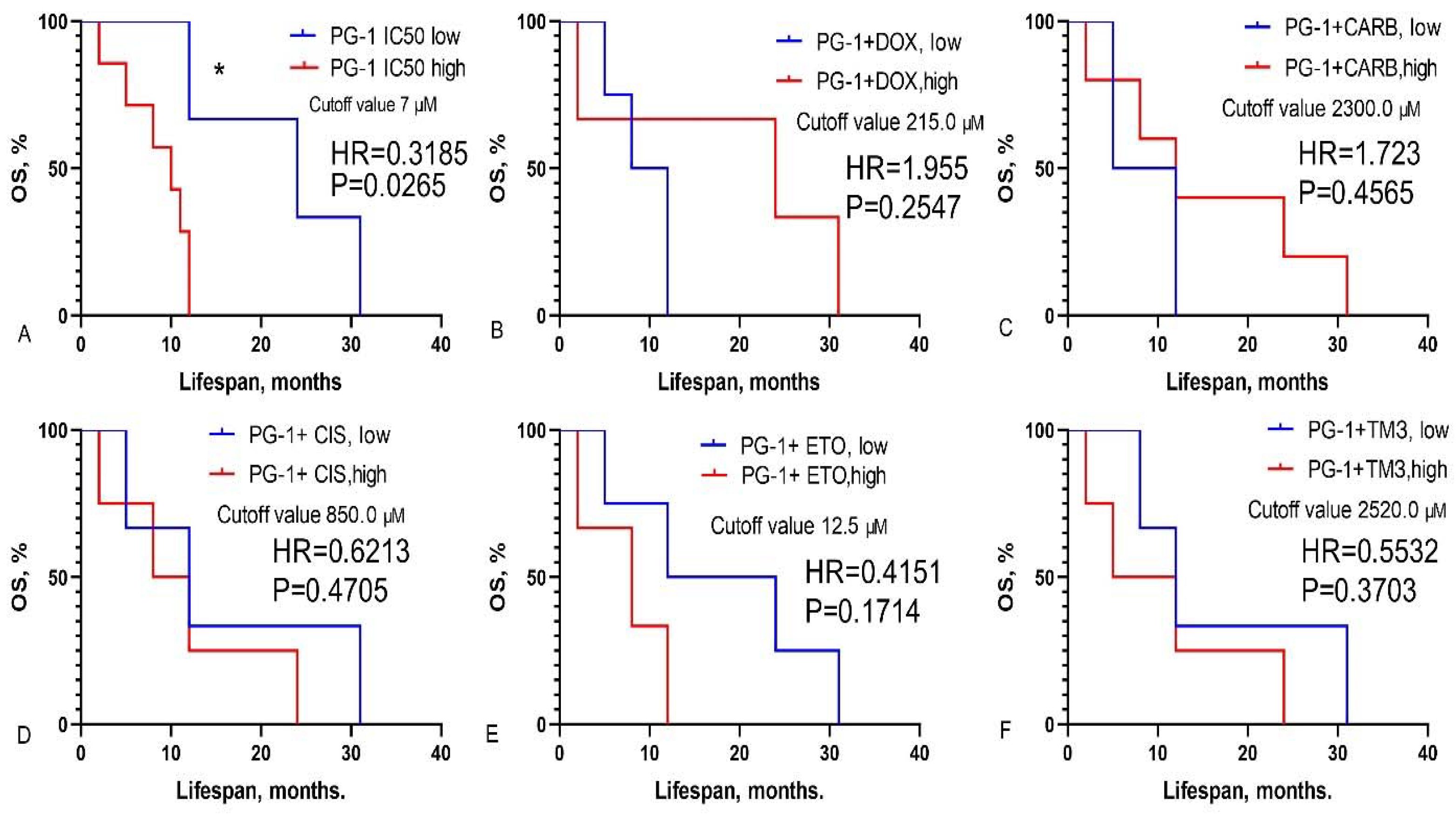
Figure 4.
Overall survival of Wistar rats with C6 glioma following administration of LL-37 and PG-1. The survival analysis was performed using the Mantel-Cox test, with χ² values indicated.
Figure 4.
Overall survival of Wistar rats with C6 glioma following administration of LL-37 and PG-1. The survival analysis was performed using the Mantel-Cox test, with χ² values indicated.
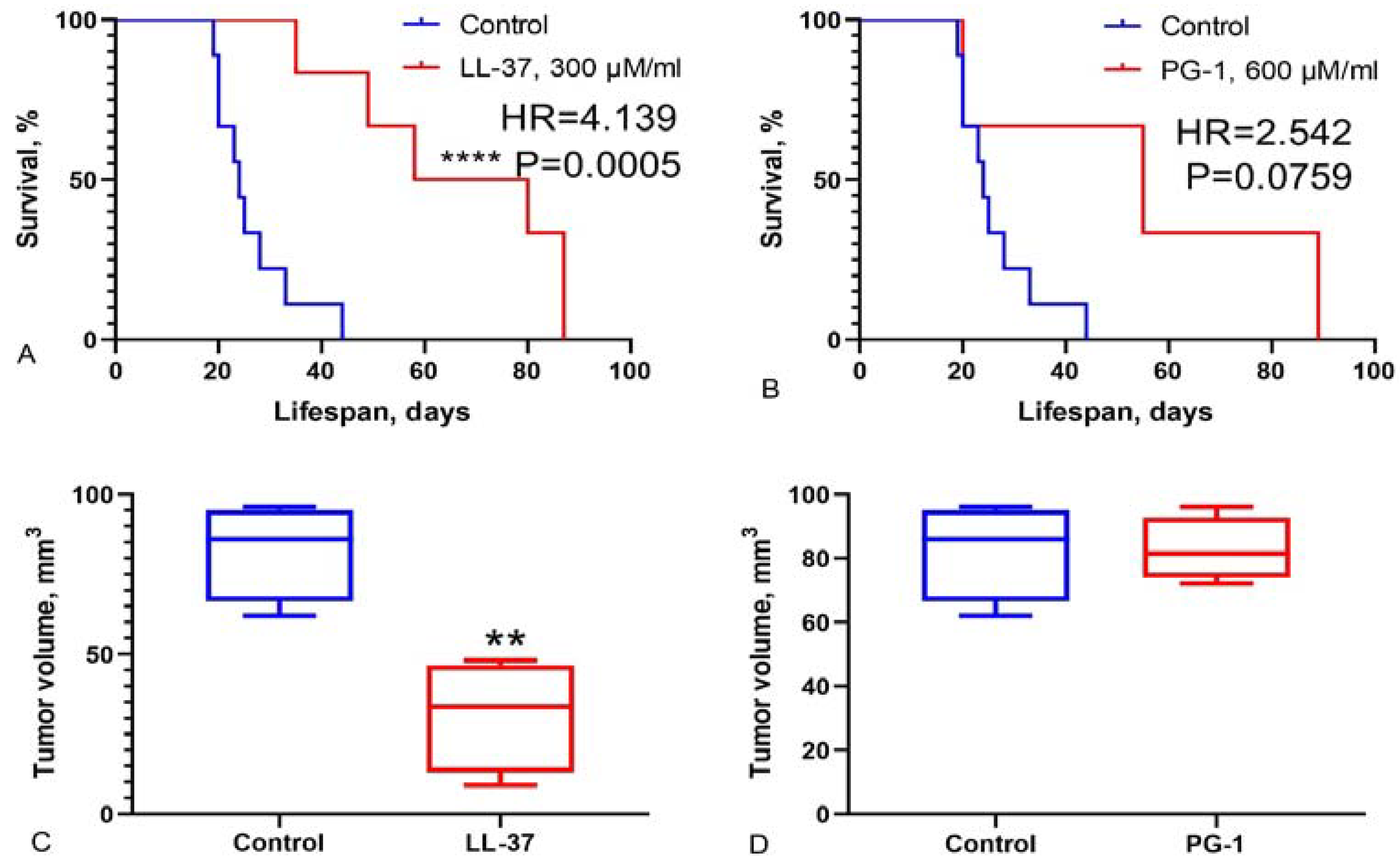

Table 1.
Doses of the LL-37, PG-1 and chemotherapy drugs.
| Drugs | Dose, μM |
|---|---|
| Doxorubicin | 920.0, 460.0, 230.0, 115.0, 73.6, 36.8, 18.4 |
| Carboplatin | 26,900.0, 2,690.0, 1,350.0, 673.0, 269.0, 134.0 |
| Cisplatin | 1,660.0, 830.0, 332.0, 166.0, 83.0, 33.2, 16.1 |
| Temozolomide | 15,500.0, 5,150.0, 1,550.0, 773.0, 386.0, 155.0 |
| Etoposide | 27.0, 13.5, 6.7, 3.3, 1.6, 0.8 |
| LL-37 | 32.0, 16.0, 8.0, 4.0, 2.0, 1.0 |
| PG-1 | 64.0, 32.0, 16.0, 8.0, 4.0, 2.0 |
Note: LL-37, PG-1 and chemotherapy drugs were dissolved in DMEM.
Table 3.
The IC50 of chemotherapy drugs, LL-37, PG-1 in human glioblastoma cells according to МТТ test.
Table 3.
The IC50 of chemotherapy drugs, LL-37, PG-1 in human glioblastoma cells according to МТТ test.
| ID patient | IC50, μM | ||||||
|---|---|---|---|---|---|---|---|
| DOX | CARB | TMZ | CIS | ETO | LL-37 | PG-1 | |
| 11081 | 290.4 | 29431.0 | 16179.5 | 2448.4 | 27.0 | 10.3 | 16.0 |
| 11961 | 3350.3 | 39792.9 | 43539.3 | 11919.7 | 86.5 | 32.2 | 123.6 |
| 6770 | 850.0 | 4000.0 | 14000.0 | 1090.0 | 26.3 | 9.5 | 8.7 |
| 7934 | 50.9 | 2000.0 | 7491.0 | 200.0 | 7.5 | 2.0 | 1.2 |
| 49142 | 548.3 | 2708.4 | 11056.0 | 776.0 | 11.4 | 6.6 | 7.4 |
| 25873 | 560.0 | 888.8 | 8619.2 | 300.0 | 8.9 | 24.1 | 30.1 |
| 57595 | 16.9 | 3093.6 | 194.5 | 1682.3 | 7.5 | 8.3 | 8.6 |
| 55068 | 546.5 | 27574.5 | 4789.5 | 1104.8 | 11.8 | 6.4 | 3.9 |
| 15159 | 179.2 | 116.4 | 436.8 | 698.1 | 11.4 | 32.1 | 15.8 |
| 62642 | 20.3 | 42495.1 | 24015.7 | 1158.5 | 32.3 | 28.1 | 34.3 |
| 60886 | 278.8 | 4498.0 | 2174.3 | >1660.0 | 6.3 | 1.1 | 1.2 |
| 18871 | 2682.8 | 24031.9 | 11976.9 | 1776.4 | 30.9 | 24.3 | 23.8 |
| 114495 | 3350.3 | 39792.9 | 43539.3 | 965.8 | 86.5 | 26.8 | 35.4 |
Note: DOX, doxorubicin; CARB, carboplatin; TMZ, temozolomide; CIS, cisplatin; ETO, etoposide; LL-37, human cathelicidin; PG-1, pig protegrin-1.
Table 4.
The IC50 of the combinations of LL-37 with chemotherapy drugs in human GBM according to МТТ assay.
Table 4.
The IC50 of the combinations of LL-37 with chemotherapy drugs in human GBM according to МТТ assay.
| ID patient | IC50 the combinations of LL-37 with chemotherapy, μM | ||||
|---|---|---|---|---|---|
| DOX | CARB | TMZ | CIS | ETO | |
| 11081 | 1832.7 | 1645.3 | 5150.0 | 485.3 | 13.8 |
| 11961 | 227.2 | 55122.9 | 54577.5 | 4825.5 | 12.7 |
| 6770 | 160.1 | 26481.5 | 1507.7 | 790.5 | 14.2 |
| 7934 | 160.0 | 1360.0 | 1550.0 | 800.0 | 19.5 |
| 49142 | 989.4 | 27187.6 | 10247.5 | 1594.8 | 11.8 |
| 25873 | 15.1 | 3307.9 | 9580.8 | 238.3 | 40.0 |
| 57595 | 4852.6 | 1424.0 | 689.6 | 388.2 | 6.6 |
| 55068 | 262.5 | 1234.5 | 5993.7 | 1201.9 | 37.4 |
| 15159 | 563.5 | 24100.4 | 5494.4 | 634.2 | 2.89 |
| 62642 | 91.9 | 48281.2 | 24523.8 | 984.5 | 37.7 |
| 60886 | 910.7 | 742.5 | 365.1 | 919.3 | 12.6 |
| 114495 | 178.9 | 35771.3 | 37621.4 | 351.9 | 0.96 |
Note: Green indicates that the IC50 of the combinations of LL-37 with chemotherapy drugs is lower than the IC50 values of chemotherapy drugs presented in Table 3. Red indicates that the IC50 of the combinations is higher than the IC50 values of chemotherapy drugs shown in Table 3. IC50 values for combinations that are not specifically highlighted in Table 4 or Table 5 are comparable to the IC50 values of chemotherapy drugs presented in Table 3.
Table 5.
The IC50 of the combinations of PG-1 with chemotherapy drugs in human GBM according to МТТ assay.
Table 5.
The IC50 of the combinations of PG-1 with chemotherapy drugs in human GBM according to МТТ assay.
| ID patient | IC50 the combinations of PG-1 with chemotherapy, μM | ||||
|---|---|---|---|---|---|
| DOX | CARB | TMZ | CIS | ETO | |
| 11081 | 1380.4 | 23637.9 | 15166.3 | 1118.6 | 37.1 |
| 6770 | 219.4 | 23963.5 | 4424.8 | 750.4 | 6.4 |
| 7934 | 50.0 | 2269.4 | 2518.5 | 700.0 | 0.9 |
| 49142 | 1230.3 | 32964.1 | 6117.6 | 1575.4 | 12.5 |
| 25873 | 74.9 | 362.2 | 4980.5 | 59.4 | 0.8 |
| 57595 | 41.2 | 14674.4 | 2.8 | 3851.7 | 16.6 |
| 55068 | 215.8 | 37804.8 | 1698.3 | 840.6 | 14.2 |
| 15159 | 179.1 | 1648.5 | 5297.4 | 315.3 | 4.7 |
| 62642 | 2299.2 | 44725.1 | 38364.4 | 3649.8 | 73.5 |
| 60886 | 30.6 | 3312.5 | 375.5 | 2295.3 | 25.8 |
Note: Green indicates that the IC50 of the combinations of PG-1 with chemotherapy drugs is lower than the IC50 values of chemotherapy drugs presented in Table 3. Red indicates that the IC50 of the combinations is higher than the IC50 values of chemotherapy drugs shown in Table 3. IC50 values for combinations that are not specifically highlighted in Table 4 or Table 5 are comparable to the IC50 values of chemotherapy drugs presented in Table 3.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



