
Submitted:
02 August 2024
Posted:
05 August 2024
You are already at the latest version
Abstract
Choline and essential fatty acids (EFA) are vital for fetal brain development, supporting pregnancy, and maintaining hormonal balance. They also promote overall health. The childbearing years present a window of opportunity to increase the intake of these key nutrients and develop healthy dietary habits. Survey data were collected for the Estudio Latinoamericano de Nutrición y Salud (ELANS), including participants from Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Peru, and Venezuela (n=9,218; 15-65 years old). Women of childbearing age were extracted from the largest database (n=3,704). The aims of this study were to evaluate the intake of choline and essential fatty acids in women of childbearing age, identify their food sources, and determine if supplements containing choline and EFA were available across the ELANS countries. In general, choline intake was inadequate in all countries, while essential fatty acids intake was normal or above requirements. Chile had the lowest intake of choline and Colombia the highest. The results showed that some countries had more inadequate choline intake than others. Consuming a larger quantity of eggs helped reduce choline inadequacy, as did including eggs and fish in the diet. The intake of essential fatty acids, including ALA, EPA, and DHA, showed variability. The contributions of EPA and DHA were lower than that of ALA, and the results differed by age group. In conclusion, choline intake is inadequate and EFA intake is variable among women of childbearing age in the ELANS study. More awareness and education are needed to achieve better intake of these nutrients.
Keywords:
choline
; essential fatty acids
; women of childbearing age
; diet
; Latin America
; ELANS
; dietary intake
1. Introduction
Choline is an essential nutrient relatively unknown by the general population. Recently, it has gained attention due to its role as a precursor molecule for the synthesis of phospholipids and the methyl-donor betaine [1].
Choline is a precursor of several key biomolecules such as: acetylcholine, phosphatidylcholine, sphingomyelin and betaine. Each of those are involved respectively in 1-neurotransmission that regulates early brain development and the function of attention, 2-as a component of biological membranes, 3-as a myelin constituent and 4-as a methyl donor that can engage in epigenetic marks through the DNA methylation processes, synthesis and repair [1,2,3].
The roles of choline during fetal development are numerous and its requirements during pregnancy are high [2] and its relevance for health includes: supporting normal brain development, acting as a protective factor when alcohol damage and infections occur and ameliorating intellectual disabilities by improving neural -cognitive functioning and memory [3,4].
Lately, choline is being used to improve physical performance, however its effects over the muscles are unclear [5].
As much as the relevance of choline intake through the diet of pregnant and lactating women is the intake of essential fatty acids (EFA) in the same population groups, as EFA complement the neurodevelopmental processes and are components of important key derivatives that are needed by the body such as vitamin D. Despite numerous research on this topic on animals models, including intake, and its effects when deficient very few studies in humans have been conducted on choline and EFA and the impact of adequate/inadequate intake in brain, cognitive and neurodevelopment in the human’s offspring [6].A study on childbearing age and pregnant women consumption of EFA (DHA and EPA) in the United States, reported an inadequate intake of both nutrients, particular in women belonging to disadvantaged communities, highlighting the concerns of deficiencies in socioeconomically vulnerable women [6].
In addition, from those few studies the evidence shows that an amount of choline more than double the requirements is needed during the third trimester of pregnancy to improve attention and focus of children at age [7]. Data obtained by Viva Cohort study in Massachusetts show that maternal choline intake within the recommended range during pregnancy was also associated with better memory function in children at seven years old compared to those whose mothers had an intake of 50% of the requirements [8].
The synthesis of choline as well as the vitamin D and docosahexaenoic (DHA) can occur in the body, however the produced amounts are insufficient to support the needs, therefore it is important to have an adequate intake to support this process [2,6].
Much of the relevance of choline and other nutrients intake is usually highlighted for pregnant and lactating women, much less is said about the adequacy of the intake in women of childbearing age. However, while there is significant knowledge and education on the benefits of the folic acid or iron intake during the pre-conceptional period, very little is known about choline and EFA intake during this period, and consequently information that is given to women is scarce promoting a knowledge gap regarding these nutrients [9,10].
Assuming that eating habits are a routine and women’s adequate pre-conceptional eating’s way are part of the important behaviors that will direct pregnancy toward a successful ending, we need to understand what the consumption trends are in this period and therefore determine whether women are well prepared to embrace pregnancy or not [11,12]. In addition, parental and particularly maternal pre-conceptional overall lifestyle can influence long term risk of the future generations in term of later development of chronic diseases and other morbidities, as stated in the Developmental Origins of Health and Disease concept [13].
In Latin America, access to adequate nutrition can be challenging for an important proportion of the population including women of fertile age. FAO in its panorama of food security for Latin America and the Caribbean [14] state that women are more food insecure than men across the region therefore exposing them to deficiencies that potentially will continue if getting pregnant.
In addition, it is important to draw the attention of the general population, and of women of childbearing age, pregnant and lactating women, to identify the sources of choline and EFA in the diet and what average intake maybe in different populations around the world. Further research on choline and EFA in Latin America is a key aspect to address the next generation’s nutritional wellbeing which makes this research a key aspect of the evaluation of the ELANS data.
The aim of this investigation was to study the choline and essential fatty acids intake in childbearing age women, identify the food sources, if supplements that contained choline and EFA existed across the studied countries and identify what potential adequate policies would help if inadequacies were found.
Until the best of our knowledge, this is the first study that would address choline and EFA intake in eight countries within the region and particularly on women of fertile age, thus our.
2. Materials and Methods
2.1. Study Sample
The data for this study were sourced from the Latin American Study of Nutrition and Health (ELANS) by its acronym in Spanish (Estudio Latinoamericano de Nutrición y Salud), a multicenter cross-sectional research project carried out across eight Latin American countries, including Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Peru, and Venezuela. Conducted over a one-year period from September 2014 to August 2015, this study focused on assessing the dietary intake and physical activity levels of individuals living in households. The study used a representative sample of urban populations, where 80-90% of the population resides in these countries.
The sample was obtained using a multistage probability sample stratified by geographical location, sex, age, and socioeconomic status. A total of 10,134 participants were eligible for ELANS study; however, due to refusal, 9680 participants comprised in the sample. Only those with complete data, who answered the socioeconomic questionnaire, and two 24 h dietary recalls were included in the ELANS study (n = 9128 participants). In this research, we analyzed data from women of childbearing age, defined as those aged between 15 and 49 years, so men and women over 49 years of age were excluded from the analyses. The final sample was comprised of 3704 women from 15 to 49 years old (Figure 1).
2.2. Sociodemographic Variables
Women were grouped into three age categories (15–19 years, 20–34 years and 35–49 years) according to WHO definitions [15] of women of childbearing age. Socio-economic status (SES) was assessed using a country-dependent questionnaire format, in accordance with legislative requirements or established local standards. The SES classification included three categories (low, medium, and high) based on national indexes specific to each country. This methodology was utilized to determine the mean per-person income of households and compare it with established thresholds for Latin Americans, as outlined by Fisberg et al. [16]. The categories of none or basic education, High school, and bachelor’s degree were utilized to distinguish educational levels. Marital status was grouped into single, marriage or couple, and divorce or widowed.
2.3. Dietary Data
Dietary intake information was assessed using two non-consecutive 24-hour recalls with two face-to-face household visits, with an interval of up to eight days between visits, with a focus on capturing day-to-day variation in food consumption by including both weekdays and weekend days in the recalls. The Multiple-Pass Method was employed to ensure a detailed recording of all foods and beverages consumed on the previous day. Portion sizes were estimated using photographic albums of common foods and household utensils. Local and traditional foods were harmonized using the USDA composition table for nutritional equivalence. The food intake data obtained from the recalls were standardized and converted into grams and milliliters by qualified nutritionists in each country. The collected data were transformed into nutrients using Nutrition Data System for Research software (NDS-R, Minnesota University, Minneapolis, MN, USA v. 2013) [17].
All food items were classified into one of the eighteen specific food groups based on their nutritional content. The food groups were as follows: (1) cereals, (2) tubers, (3) legumes, (4) dairy, (5) eggs, (6) beef, (7) poultry, (8) fish, (9) pork, (10) other meats, (11) vegetables, (12) fruits, (13) nuts and seeds, (14) butter, (15) margarine, (16) oils, (17) other fats, and (18) miscellaneous. Only the top five food group contributors to each nutrient were displayed in the results.
2.3.1. Choline and Essential Fatty Acids Intake
The Multiple Source Method (MSM), a web-based statistical modeling approach recommended by the European Prospective Investigation into Cancer and Nutrition (EPIC), was implemented to transform 24-hour recall-derived individual intake into usual daily intake distributions [18].
The study specifically focused on two essential fatty acids: omega-3 (w-3) and omega-6 (w-6). Among the w-3 fatty acids, Alfa-Linolenic Acid (ALA), Eicosapentaenoic Acid (EPA), and Docosahexaenoic Acid (DHA) were examined. In contrast, w-6 contains Linoleic Acid (LA) and Arachidonic Acid (ARA).
Through the employment of the MSM, the study was capable of estimating the usual intake of choline and essential fatty acids at the population level while taking into account within-person variance. Moreover, the typical intake of choline and essential fatty acids was individually assessed for each country, taking into consideration the variations in dietary habits among Latin American populations.
2.3.2. Choline and Essential Fatty Acids Adequacy
The intake levels of choline and essential fatty acids were assessed and evaluated against the US Institute of Medicine (IOM) Dietary Reference Intakes (DRI) standards [19], which stipulate a daily intake of 425 mg for choline, 1.1 g for ALA, and 11 or 12 g for LA in women between the ages of 15 and 18, and 19 to 49, respectively. The adequacy of each individual’s nutrient intake was calculated using the following formula: The observed intake value was divided by the DRI and multiplied by 100. The subject was classified as normal if the resulting number fell between 90% and 110%. If the number was less than 90%, the individual’s nutrient intake was deemed inappropriate because of deficiency. Conversely, if the number was greater than 110%, the individual’s intake was deemed inappropriate because of excess.
It should be highlighted that ALA and LA are considered essential fatty acids because humans cannot synthesize them. On the other hand, ALA is metabolized to EPA and subsequently to DHA, while LA is the precursor of ARA. Thus, EPA, DHA and ARA are not considered essential fatty acids as they can be synthesized endogenously [20]. For this reason, the National Academy of Medicine, the former Institute of Medicine, have not been established a Dietary References Intakes (DRIs) for EPA, DHA and ARA. The IOM only recommended that EPA and DHA contribute 10 percent of the total omega 3-fatty acid intakewhich should be approximately 160 mg/day [19]. Therefore, a percentage of adequacy cannot be provided for EPA, DHA and ARA.
2.4. Choline and Essential Fatty Acids within Prenatal Multivitamins-Supplements
To identify if choline and essential fatty acids existed as part of the pre-natal multivitamins-minerals-nutrients supplements available in the eight ELANS countries, the research team agreed to find the three most used prenatal supplements through experts and health professionals. After gathering the names, carefully reading the labels, and identifying the components named in each supplement a categorization according to: “choline included” and “EFA included” was performed to determine whether choline and essential fatty acids were available in their composition.
2.5. Statistical Analysis
Descriptive statistics analysis was computed for continuous variables as means, standard error of the mean (SEM), and minimum and maximum values. Categorical measures are presented as counts and percentages. The intake values in adequacy were compared using the Mann–Whitney or Kruskal–Wallis test, after the normality had been tested by the Skewness and Kurtosis test. In addition, chi-square analysis was used to evaluate possible associations. These analyses were performed for choline as well as for EFA.
To evaluate the impact of different factors that could affect choline adequacy, a classification tree (CT) algorithm was applied to determine differences between countries and the food source that affect inadequacy of the choline intake. This technique selects predictors that produce differentiated groups in accordance with adequacy levels, which is important for the purpose of this study due to the relevance of choline and because in general there is less information on choline intake. In all cases, tests were performed with a statistical significance level of 0.05. Microsoft Excel®® 2016 software and the IBM SPSS®® version 25 statistical packages were used for data loading and analysis.
2.6. Ethics
The ELANS protocol, which was registered at Clinical Trials (#NCT02226627) and approved by the Western Institutional Review Board (#20140605), also received approval from the ethical review boards of the participating institutions. Participants provided informed consent for inclusion in the country-level study, and their confidentiality was maintained using identification codes instead of names. Data transfers were securely conducted through a file-sharing system.
3. Results
3.1. Sociodemographic Characteristics
An analysis of data was performed on women of childbearing age, which was defined as individuals aged between 15 and 49 years. The sociodemographic characteristics of the participants, including age, socioeconomic status (SES), educational level, and marital status, among countries were studied by applying a chi-square test to evaluate the heterogeneity of the variables whose profiles are presented in Table 1. The distribution of women according to the age varied across the countries included in this study (p=0,043). Costa Rica and Ecuador had a higher proportion of younger women (17.8% and 17.3%, respectively), while Argentina and Brazil had a relatively larger population of older women of childbearing age (41.5% and 40.6%, respectively). Venezuela had the highest proportion of women in the low socioeconomic level (76%), whereas Peru, Costa Rica, and Ecuador showed a prevalence >10% in the high socioeconomic level (p<0,001). The educational level of Venezuela was considerably higher than that of the other countries (p<0,001). A Bachelor’s degree was reported by 20.7% of Venezuelan women, nearly twice the mean proportion in the total ELANS group. On the other hand, Ecuador had the highest proportion of women with none or basic educational level (83.6 %). Most of women across all countries were married or in a couple relationship, with Ecuador having the highest percentage (57.7%), followed by Peru (57.5%). Argentina had the highest percentage of divorced or widowed women (12.3%), while Venezuela and Chile had a higher proportion of single women (48.2 % and 47.2 %, respectively) (p<0,001).
3.2. Choline Intake
Table 2 displays choline intake and adequacy of the sample with deficient, normal, or excessive consumption. The average daily choline intake of the study participants was 305 mg/day, which was 71.8% of the IOM-recommended intake of 425 mg/day (adequacy), consequently, women in this population are in deficit of this nutrient by 28mg/day. As a result, 79.8 % of the participants were deficient in choline consumption. All countries follow this trend, especially Chile, which had the lowest intake (238.6 mg/day) and highest proportion of deficient consumption (95.4%). Additionally, Colombia had the highest intake (373.1 mg/day) and the highest proportion of excessive intake (19 %). Despite this, more than half of the Colombian women (55.2%) had deficient intake. No significant differences in choline consumption parameters were observed between age groups (p=0.099), socioeconomic status (=0.608), educational level (p=0.072), and marital status (p=0.057).
Figure 2 provides a comparison of the choline intake (mg/day) of the five most contributing food groups in the ELANS. According to the data, eggs were found to be a significant source of choline in most countries, except Brazil, where beef was the main source (p<0.001). Colombia reported the highest per capita intake of choline from eggs, at 154,02 mg/day. In contrast, poultry consumption exhibited more consistent levels of choline intake across the countries studied. Notably, Peru had the greatest contribution to choline intake (77.92 mg/day) in the poultry group.
Fish and pork consumption exhibited variability, thus having an impact on choline intake levels among the Latin American countries. Certain countries, such as Peru (39.4 mg/day) and Brazil (31.82 mg/day), relied heavily on fish as a source of choline.
In contrast, countries like Argentina had a lower consumption level (6.63 mg/day) from fish group. Pork consumption also showed variations in choline intake, with some countries such as Costa Rica (37.2 mg/day) and Ecuador (32.2 mg/day), reporting higher contribution levels. However, countries like Peru had the lowest contribution (14.12 mg/day).
3.3. Classification Tree algorithm
To identify the principal sources of food that explain differences among countries related to adequacy of Choline’s intake, a classification tree (CT) is presented (Figure 3). In this context, the inadequate by deficit group was represented by “< 90 %”, while the normal and excessive groups were merged and represented by “> 90 %”.
The CT algorithm implemented revealed a primary division into two groups of countries: Group 1: comprising Argentina, Colombia, and Ecuador (66.7% deficient) and Group 2: comprising Brazil, Chile, Costa Rica, Peru, Venezuela (86.9% deficient). The second division in both groups was established by consumption of choline coming from the eggs (mg/day), suggesting that an increase in eggs intake helpsto reduce choline insufficiency. The third division considered egg and fish consumption, as well as, the country, as relevant variables. A significant increase in adequacy level of choline was observed in women who included a larger quantity of eggs or fish in their diets. Furthermore, Chile and Venezuela were classified as countries in which, despite having a good contribution of choline from eggs, they had a higher proportion of people with deficient intake of this nutrient.
3.4. Essential Fatty Acids Intake
Regarding omega 3, Table 3 provides information on the consumption parameters of alpha-linolenic acid (ALA) among women of childbearing age. Additionally, Table 4 highlights the intake of eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and the total amount of omega-3 fatty acids (as the sum of ALA+EPA+DHA). As expected, the contributions of EPA and DHA were lower than that of ALA, therefore, their values are presented in milligrams (mg). In all cases, the contribution of DHA was greater than that of EPA. The overall average consumption of ALA among the participants was recorded at 1.38 grams, with an adequacy percentage of 125.5%; therefore, 55.6% of the sample exhibited excessive ALA intake. A Table 4 show the mean contribution of EPA + DHA was less than 100 mg, so the total omega 3 consumed was 1.47 g.
Argentina and Chile exhibited a lower average ALA consumption of 0.98 g and 1.01 g, corresponding to an adequacy level of 89.1% and 92.2%, respectively. They also had the highest percentage of participants with deficient intake at 57.6% and 55,7%, respectively (p<0.001). In contrast, Venezuela exhibited the highest ALA average consumption at 1.72 g, with an adequacy level of 156.3% (p<0.001). Due to this, Venezuela had the lowest percentage of individuals with deficient intake at 11.9%, on par with the highest proportion of participants with excessive intake levels at 76% (p<0.001). This trend was similar that to of total w-3 values (Table 4). Regarding EPA and DHA, Ecuador had the highest intake of both fatty acids (37 mg and 113,5 mg, respectively), while for EPA, the lowest values were for Argentina, Brazil, and Chile (<18,5 mg). For DHA, the lowest value was found in Brazil (59,3 mg).
These findings indicate that the consumption of ALA, and consequently of total w-3, varies among different age groups, with statistically significant differences (p<0.001), but not for the EPA and DHA intake (Table 4). Specifically, the 35-49 years age group exhibited lower ALA intake than the younger group, with an average difference of approximately 200 mg between the two groups. Furthermore, the data reveal that more than half of the women in all three age groups had excessive ALA intake, with the highest percentages identified in the younger age categories (p<0.001). The analysis also indicated that there was no statistically significant difference in w-3 and constituent intake across the different socioeconomic status groups (p>0.050).
There was a slight increase in ALA, total w-3intake, and ALA adequacy as education level increased (p<0.001), but this was not observed for EPA and DHA (p>0.050). Individuals with a Bachelor’s degree had the highest ALA intake and adequacy percentage (1.48 g and 134.9 %, respectively). Women with a Bachelor’s degree had the lowest percentage of deficit in adequacy within the diet (21.1 %) and the highest proportion of excessive intake (55.6 %). In comparison, those with no education or basic education had the highest ALA percentage of deficiency (32.6 %) and a lower proportion of excessive diet (50.3 %).
The data suggests a contradictory difference in the omega 3 fatty acids by marital status (p<0,001). While single individuals have the highest average intake of ALA and total omega 3 (1.42 g and 1.51 g, respectively), the divorced or widowed individuals had the lowest (1.31 g and 1.41 g, respectively). However, for the EPA and DHA, was quite the opposite, with higher intake values in the divorced or widowed women (23 mg and 75.4 mg, respectively), in comparison with the singles women (20.6 g and 67.1 g, respectively).
The five food groups that made the greatest contribution to the consumption of total omega-3 fatty acids are illustrated in Figure 4. These groups were oils, fish, cereals, other fats, and margarine, with notable variations between countries (p<0.001). In most countries, vegetable oils were the primary source of w-3 fatty acids, with the exception of Ecuador, where fish was the primary dietary source (0.61g); and Argentina, where other types of fats (such as animal fat, fatty dressings, and condiments), and cereals were the primary sources (0.3 g and 0.28 g, respectively). Margarine made a greater contribution in Venezuela (0.37 g) than in the rest of the countries.
In relation to omega 6, Table 5 provides information on the consumption parameters of linoleic acid (LA) among women of childbearing age. Additionally, Table 6 highlights the intake of arachidonic acid (ARA), and the total amount of omega-6 fatty acids (as the sum of LA+ARA). As expected, the contributions of ARA were lower than that of LA; therefore, the ARA values are presented in mg. The overall average consumption of LA among the participants was 13.91 grams, with an adequacy percentage of 125.5 %. A little less than a half (49.7 %) of the sample exhibited excessive LA intake. The mean contribution of ARA was 141.9 mg, so the total omega 6 consumed was 14 g.
SEM: Standard error of the mean. Min: Minimum value. Max: Maximum value.Chile exhibited the lowest levels of LA, LA adequacy, ARA, and total w-6 intake, whereas Ecuador displayed the highest values (p<0.001). Therefore, Chile was the country with the highest percentage of Deficient intake (47.2%), while Ecuador had the highest percentage of excessive intake (73.5%). Similarly, to w-3, higher w-6 intake levels were observed in women between 15 and 19 years old than in those between 35 and 49 years old (p<0.001). These data show a trend of increasing percentage of Deficient weight as age increases from the younger (18.4 %) to older (36.6 %) age groups. The intake parameters of w-6 turned out to be independent of the SES and the education level of the women (p>0.050). The marital status was significantly different only in the LA adequacy percentage and in the ARA intake. The Divorced or Widowed women had a lower intake than the single women (p=0.004).
The five food groups that made the greatest contribution to the consumption of total omega-6 fatty acids are illustrated in Figure 5. These groups were oils, cereals, other fats, poultry and margarine, with some variations between countries (p<0.001). In all the countries, vegetable oils were the primary source of w-6 fatty acids.
In Argentina, the cereals and other fats had a higher contribution to the w-6 intake. Poultry was prominent in the w-6 contribution of the Peruvian women, while the margarine was the second more contributor of w-6 in Brazil.
3.5. Available Choline and Essential Fatty Acids in Supplements
Table 7 shows the three different brands most prescribed and available as pre-natal supplements in the eight countries that constitute ELANS. The analysis revealed that none of the products in Argentina, Brazil, Chile, Colombia, Costa Rica, Peru, or Venezuela contain Choline or Omega-6. However, at least one brand in each country declares the presence of Omega-3 in their supplements. Most brands across the countries declare the DHA/EPA content, except for Venezuela where only the total Omega-3 content is specified. Colombia stands out as the country with all three brands declaring the presence of Omega-3, followed by Chile, Brazil, and Venezuela with two brands each declaring Omega-3. Additionally, Argentina, Costa Rica, and Peru are noted as countries where the DHA content in pre-natal supplements is below 200 mg.
4. Discussion
In this study, a prevalence of 80 % of women between 15-49 years old, with inadequate intake of choline was found, (below the 90% of the recommended intake established). That is an astonishing majority of women with inadequate consumption of this nutrient across the eight studied countries. As it is reported in other studies, choline intake is largely deficient in pregnant women, which has deleterious effects over fetal brain development, the ability to concentrate and visual memory during school age [3,8]. Also, because of this poor choline intake pattern, during pre-conceptional years one can easily understand that if becoming eventually pregnant, these women would continue with their eating habits, unless an intervention is strategically planned [20].
However, the intake of EFA can be disaggregated in twofold: one regarding ALA and LA and the other regarding DHA, EPA and ARA. While the ALA and LA showed adequacies of 125%, the intake of DHA + EPA was below 100 mg per day, below the suggested 160 mg per day. And again, DHA and EPA are two long chain EFA that are associated with cardiovascular health, joint and eye health and brain fetal development. For this study the researchers agree on using the former IOM recommendations, for choline and EFA, because there are no recommended values in Latin America. However, some other authorities recommend higher intakes of EFA. The Dietary Guidelines for the Americans recommends 250 mg per day [21] and The European Safety Authority states that an additional 100-200 mg per day of DHA and beyond 250 mg per day of EPA + DHA [22].
Few studies have addressed the choline intake in women of childbearing age. Mygind et al. [23] in a sample of 125 New Zealand women of reproductive age (18-40) a mean intake of 316mg/day with only 16% of the sample meeting or exceeding the requirements. The mean intake of the overall childbearing age women of ELANS was 305.0 mg/day with minimum and maximum values of 48.8mg and 913.7mg respectively, with only 20% of women meeting or exceeding the established requirements.
Derbyshire et al. [20] and Vennemann et al. [22] found that choline intake in childbearing age women in the USA, Europe and Australia had a mean intake within a range of 244 to 443 mg/day, below the 425 mg recommended by the IOM considered for this study as the reference. Among all the studies included in the literature revision by Derbyshire et al. only five percent of the non-pregnant women had choline intake above 631 mg/day in Sweden, above 578 mg/day in Finland and above 543 mg/day in the Netherlands [20]. Zhang et al. [24] found mean usual intakes of EPA, DHA combined from foods and dietary supplements of 88.1+ 3.0 mg per day, and 95% of their NHANES sample did not meet the intake of 250mg per day.
Nordgren et al. [6], in a sample of childbearing age women and pregnant women found no statistically different intakes of EPA and DHA and the mean was 89.0 mg per day. Also, the Nordgren et al. [6], reported that omega 3 fatty acid intake was significantly associated with poverty to income ratio, race, and educational attainment6.
In our study, a difference in the intake of ALA, total omega 3 intake showed a slight increase as the educational level increased, but this was not observed for EPA and DHA, and women with basic or no education had the highest percentage of ALA deficiency and a lower proportion of excess in the diet. A contradictory difference was observed by marital status, while single women had the highest average intake of ALA and total omega 3, divorced or widowed had the lowest, and the opposite was found for EPA and DHA, divorced and widowed showed higher intakes and lower intakes were reported for single women.
With the consistently reported “below of the requirements intake of choline and EPA and DHA” in women of fertile age, one could argue the following: first, women might not be aware of the existence and relevance of choline, and EFA, second, gynecologists and obstetricians are making emphasis in educating women about other nutrients such as calcium, iron, folic acid, but not choline, or EFA, third, a trend toward continuing the own existing eating habits could be expected, therefore, a childbearing age woman with a low intake of choline, and/or inadequate, deficient or excessive, EFA is potentially at risk of inadequate intake of those nutrients if becoming pregnant, moreover when no intervention is implemented, and fourth, the lack of dietary diversity showed by women, which might not be enough for covering the choline and/or EFA requirements. Another concern at this point is the lack of choline supplements, for the case of our study in the eight countries that constitute ELANS study. Among the most used pre-natal supplements utilized in these countries, not even one contained choline in its composition, however omega 3 fatty acids were present.
Keeping a diverse and quality diet is key to achieve a good nutrition status, in ELANS childbearing age women, diet diversity and adequacy of micronutrient was studied previously without considering for choline and essential fatty acids [25]. Nevertheless, results show an important proportion of women (42.3%) consuming from 1-4 groups of foods (eg: non diverse diet), and women consuming 5 food groups (30.4%; acceptable diet). The most consumed foods, as per the 50% or more of the sample were starchy staples (99.4%), and meat (84.2%) whereas eggs which are an important source of choline, accounted only for 35.6% of women. The lowest foods consumed were green leafy vegetables (6.8%) and nuts and seeds (2.8%) [26]. This gives an idea of what is like the food consumption in ELANSwomen of fertile age, which also has shown to be deficient in some key micronutrients such as Calcium, vitamin D and E [25,26].
Usually, nutrition education has made emphasis in the relevance of iron and folic acid intake during pre-conception and pregnancy, and with all reason: they are important. In addition, other vitamins and minerals are being recommended to be adequate for pregnant women, therefore, calcium, vitamin A, vitamin C among others is included into the available OTC supplements. Also, an emphasis has been made in adequate weight gain during pregnancy and the importance of eating proteins, the right fats, and carbohydrates, with subsequent recommendations to eat enough vegetables, fruits, lean proteins, and whole cereals. However, from the search among the available and most relevant health web pages one can infer that little information is given about choline intake and its sources. Important resources including the John Hopkins Medicine online [27], Medline plus [28] and even WHO [30] online platforms, do not mention choline and its importance during pregnancy, in an explicit and friendly accessible way or at other periods of life; nor the neuroprotective effects of EFA such as AA or DHA in the developing brain and later in life [30]. The previous, are resources with a high traffic of visits and these tools might be a good way to promote at least to start catching the attention of women. The only web page that included choline in a friendlier way was the My Health Finder from the U.S. Department of Health and Human Services [31], but these online platforms are not popular within the Latin American population. Regretfully, web page resources in Spanish are scarce and because people in general, do not know that choline and EFA are key factors to the fetal brain development they go unnoticed.
With the above being said, and the fact that only recently the pre-conceptional health and nutrition status has been gaining attention as part of the wellbeing that should be promoted to guarantee the future generations health, the need for going beyond iron and folate has arrived. The pre-conceptional period has been neglected for some time, however, as part of the concepts and theories that support the developmental origins of health and disease and the early programing of diseases by the exposure to environmental factors, being adequate nutrition a key fundamental one, starting in good health before pregnancy and all the determinants that influence good health will have a role in making an eventual pregnancy successful , particularly when we know that 50% of pregnancies are non-planned [32].
Finally, an effort should be made to make awareness about this important nutrient, as this study found no differences in the intake of choline of women by level of education, therefore an interpretation is that ELANS women of reproductive age might not have knowledge about the importance of choline intake nor their health care personal is making any mention or prescriptions so they consume an adequate amount either by their diet or taking a supplement, such as choline chloride, choline bitartrate or phosphatidylcholine, considering the choline’s role during the fetal period in the development of later cognitive abilities. Also, the fact that EFA do have differences according to educational and even marital status for women should be considered [33]. Both findings give a window of opportunities for intervention and education in such important nutrients for the future generations in this region.
This study has several strengths, among those the fact that every country has a national representative sample, there were 2 non-consecutives 24 hours recall and the use of the multiple pass method to minimize errors. However, it also has limitations, as the cross-sectional type of study does not allow to establish any causalities and only urban settings were considered, so rural population was not included.
Finally, we wish to emphasize the importance of the pre-conceptional period for establishing new healthy routines and health care in young women, as it is a period for learning and promoting health and introducing the new positive changes into the lifestyle of Latin American women of childbearing age. We also want to suggest the inclusion of this period of life as an important period to be targeted with policies and programs that strengthen nutritional and health education as part of the interventions designed to ensure the wellbeing of the future regional generations, as well as planning aid programs when needed that introduce the foods that make a difference in choline intake through diet such as eggs and fish. This combination of food aid with education will have the sustainability component of education in parallel with the aid provided to those in need. Programs such as “One egg per day” for young children in Burkina Faso, where significant improvements were reported when this program was implemented have sense if pre-conceptional and during pregnancy deficiencies of these nutrients are found. Mothers reported more resilience and better psychomotor functioning in their young children after the consumption of one egg per day during the time of this project implementation [34]. Empowering women, promoting education and resilience through the policies and programs to be implemented at the regional level, bring hope to better guarantee the wellbeing of future generations in Latin America.
5. Conclusions
Choline intake is inadequate for most ELANS women. Achieving the recommended amount of intake through diet along is challenging, especially when diets are not as diverse as they should be or do meet the required quantities. Regarding EFA, the results show adequate and even excessive intakes for the studied population, however the sources are different from those shown over other regions of the world. Regional efforts should be made to enhance adequacy of choline and EFA by improving education of women and health care personnel, through policies and programs aimed at guaranteeing the next generation’s health.
Author Contributions
Conceptualization, M.H.-C., M.C.Y.G. and L.Y.C.S.; methodology, M.F., I.K., M.H.-C., M.C.Y.G., L.Y.C.S. and M.L.-J.; software, G.R. and M.V.; validation, P.H. and Y.S.; formal analysis, G.R. and M.V.; investigation, P.H. and Y.S.; data curation, G.R., M.V., P.H. and Y.S.; writing—original draft preparation, M.H.-C., M.C.Y.G., L.Y.C.S. and M.L.-J.; writing—review and editing, G.G., M.R.L.-D., A.R., M.F. and I.K.; supervision, M.H.-C. and M.L.-J.; project administration, M.H.-C. All authors have read and agreed to the published version of the manuscript.
Funding
The ELANS was initially supported by a scientific grant from the Coca-Cola Company and support from the Ferrero, Instituto Pensi/Hospital Infantil Sabara, International Life Science Institute of Argentina, Universidad de Costa Rica, Pontificia Universidad Católica de Chile, Pontificia Universidad Javeriana, Universidad Central de Venezuela/Fundación Bengoa, Universidad San Francisco de Quito, and Instituto de Investigación Nutricional de Peru. The founding sponsors had no role in study design, data collection, analyses, or interpretation; writing of the manuscript; or the decision to publish the results. A grant from Abbott was received for the analysis of choline and EFA. The sponsor was not involved in any of the stages of this research.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The complete ELANS protocol was registered at Clinical Trials (#NCT02226627) and was approved by the Western Institutional Review Board (#20140605). Site-specific protocols were further approved by the ethical review boards of participating institutions.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data presented in this study are available upon request from the corresponding author. Data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
We would like to thank the following individuals at each of the participating sites who made substantial contributions to the ELANS: Luis A. Moreno, Brenda Lynch, Mariela Jauregui, Alejandra Guidi, Luis Costa, Regina Mara Fisberg, Viviana Guajardo, and Gerson Ferrari.The following are members of the ELANS Study Group: Chairs: Mauro Fisberg and Irina Kovalskys; Co-chair: Georgina Gómez Salas; core group members: Attilio Rigotti, Lilia Yadira Cortés Sanabria, Martha Cecilia Yépez García, Rossina Gabriella Pareja Torres, and Marianella Herrera-Cuenca; Steering Committee: Berthold Koletzko, Luis A. Moreno, and Michael Pratt; Project Managers: Viviana Guajardo and Ioná Zalcman Zimberg; International Life Sciences Institute-Argentina: Irina Kovalskys, Viviana Guajardo, María Paz Amigo, Ximena Janezic, and Fernando Cardini; Universidad I Salud: Myriam Echeverry and Martin Langsman; Instituto Pensi-Hospital Infantil Sabara-Brazil and Federal University of Sao Paulo: Mauro Fisberg, Ioná Zalcman Zimberg, and Natasha Aparecida Grande de França; Pontificia Universidad Católica de Chile: Attilio Rigotti, Guadalupe Echeverría, Leslie Landaeta, and Óscar Castillo; Pontificia Universidad JaverianaColombia: Lilia Yadira Cortés Sanabria, Luz Nayibe Vargas, Luisa Fernanda Tobar, and Yuri Milena Castillo; Universidad de Costa Rica: Georgina Gómez Salas, Rafael Monge Rojas, and Anne Chinnock; Universidad San Francisco de Quito-Ecuador: Martha Cecilia Yépez García, Mónica Villar Cáceres, and María Belén Ocampo; Instituto de Investigación Nutricional-Peru: Rossina Pareja Torres, María Reyna Liria, Krysty Meza, Mellisa Abad, and Mary Penny; Universidad Central de Venezuela: Marianella Herrera-Cuenca, Maritza Landaeta-Jiménez, Betty Méndez-Pérez, Maura Vásquez, Omaira Rivas, Carmen Meza, Guillermo Ramírez, and Pablo Hernández; accelerometry analysis: Priscila Bezerra.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Wallace TC, Blusztajn JK, Caudill MA, Klatt KC, Zeisel SH. Choline: The neurocognitive essential nutrient of interest to obstetricians and gynecologists. J Diet Suppl. 2020;17(6):733-752. [CrossRef]
- Derbyshire E, Obeid R. Choline, Neurological Development and Brain Function: A Systematic review focusing on the First 1000 Days: review. Nutrients. 2020;12 (6): 1731. [CrossRef]
- Korsmo HW, Jiang X, Caudill MA. Choline: Exploring the growing science on its benefits for moms and babies. Nutrients. 2019;11(8):1823. [CrossRef]
- Stephenson J, Heslehurst N, Hall J, Schoenaker DAJM, Hutchinson J, Cade JE, et al. Before the beginning: nutrition and lifestyle in the preconception period and its importance for future health. Lancet. 2018;391(10132):1830-1841. [CrossRef]
- Moretti A, Paoletta M, Liguori S, Bertone M, Toro G, Iolascon G. Choline: An essential nutrient for skeletal muscle. Nutrients. 2020;12(7):2144. [CrossRef]
- Nordgren TM, Lyden E, Anderson-Berry A, Hanson C. Omega-3 Fatty Acid Intake of Pregnant Women and Women of Childbearing Age in the United States: Potential for Deficiency?. Nutrients. 2017;9(3):197. [CrossRef]
- Bahnfleth CL, Strupp BJ, Caudill MA, Canfield RL. Prenatal choline supplementation improves child sustained attention: A 7-year follow-up of a randomized controlled feeding trial. FASEB J. 2022;36(1):e22054. [CrossRef]
- Boeke CE, Gillman MW, Hughes MD, Rifas-Shiman SL, Villamor E, Oken E. Choline intake during pregnancy and child cognition at age 7 years. Am J Epidemiol. 2013; 177(12):1338-47. [CrossRef]
- Jaiswal A, Dewani D, Reddy LS, Patel A. Choline Supplementation in Pregnancy: Current Evidence and Implications. Cureus. 2023;15(11):e48538. [CrossRef] [PubMed] [PubMed Central]
- Masih SP, Plumptre L, Ly A, Berger H, Lausman A, Croxford R, Kim Y, O’Connor DL. Pregnant Canadian Women Achieve Recommended Intakes of One-Carbon Nutrients through Prenatal Supplementation but the Supplement Composition, Including Choline, Requires Reconsideration. J Nutr. 2015;145(8):1824-1834. [CrossRef]
- Stephenson J, Heslehurst N, Hall J, Schoenaker DAJM, Hutchinson J, Cade JE, Poston L, Barrett G, Crozier SR, Barker M, Kumaran K, Yajnik CS, Baird J, Mishra GD. Before the beginning: nutrition and lifestyle in the preconception period and its importance for future health. Lancet. 2018;391(10132):1830-1841. Epub 2018 Apr 16. Erratum in: Lancet. 2018;391(10132):1774. [CrossRef] [PubMed] [PubMed Central]
- Fleming TP, Watkins AJ, Velázquez MA, Mathers JC, Prentice AM, Stephenson J, et al. Origins of lifetime health around the time of conception causes and consequences. Lancet. 2018;391(10132):1842-1852. [CrossRef]
- Gluckman PD, Hanson MA, Buklijas T. A conceptual framework for the developmental origins of health and disease. J Dev Orig Health Dis. 2010;1(1): 6-18. https://pzacad.pitzer.edu/~dmoore/2010_Gluckman%20et%20al_Concept’l%20framework%20for%20DOHaD_J%20of%20DOHaD.pdf. [CrossRef]
- FAO, IFAD, UNICEF, WFP, WHO. The State of Food Security and Nutrition in the World 2023. Urbanization, agrifood systems transformation and healthy diets across the rural–urban continuum [Internet]. Rome: FAO; 2023. [cited 27/2/2024] Available in: https://www.fao.org/3/cc3017en/online/cc3017en.html. [CrossRef]
- The Global Health Observatory [Internet]. Rome: WHO; 2023. [cited 27/2/2024]. Available in: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/women-of-reproductive-age-(15-49-years)-population-(thousands).
- Fisberg M, Kovalskys I, Gomez G, et al. Latin American Study of Nutrition and Health (ELANS): rationale and study design. BMC Public Health 2016; 16: 93.
- Kovalskys I, Fisberg M, Gómez G, Rigotti A, Cortés LY, Yépez MC, Pareja RG, Herrera-Cuenca M, Zimberg IZ, Tucker KL, Koletzko B, Pratt M. Standardization of the Food Composition Database Used in the Latin American Nutrition and Health Study (ELANS). Nutrients. 2015; 7(9):7914-7924. [CrossRef]
- Moshfegh A, Rhodes D, Baer D, Murayi T, Clemens J, Rumpler W, Paul D, Sebastian R, Kuczynski K, Ingwersen L, Staples R, Cleveland L. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am. J. Clin. Nutr 2008; 88: 324–332. [CrossRef]
- Institute of Medicine (IOM) Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients).Washington: The National Academies Press; 2005.
- Derbyshire E, Obeid R, Schön C. Habitual Choline intakes across the childbearing years: A Review. Nutrients. 2021;13(12):4390. [CrossRef]
- U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020-2025 [Internet]. 9th Edition.Washington: December 2020. [cited 27/2/2024]. Available in: https://www.dietaryguidelines.gov/sites/default/files/2020-12/Dietary_Guidelines_for_Americans_2020-2025.pdf.
- Vennemann FB, Ioannidou S, Valsta LM, Dumas C, Ocké MC, Mensink GB, et al. Dietary intake and food sources of choline in European populations. Br J Nutr. 2015;114(12):2046-55. [CrossRef]
- Mygind VL, Evans SE, Peddie MC, Miller JC, Houghton LA. Estimation of usual intake and food sources of choline and betaine in New Zealand reproductive age women. Asia Pac J Clin Nutr. 2013;22(2):319-24. [CrossRef]
- Zhang Z, Fulgoni VL, Kris-Etherton PM, Mitmesser SH. Dietary Intakes of EPA and DHA Omega-3 Fatty Acids among US Childbearing-Age and Pregnant Women: An Analysis of NHANES 2001-2014. Nutrients. 2018;10(4):416. [CrossRef]
- Herrera-Cuenca M, Previdelli AN, Koletzko B, Hernandez P, Landaeta-Jimenez M, Sifontes Y, et al. Childbearing age women characteristics in Latin America. Building Evidence Bases for Early Prevention. Results from the ELANS Study. Nutrients. 2020;13(1):45. [CrossRef]
- Gómez G, Nogueira Previdelli Á, Fisberg RM, Kovalskys I, Fisberg M, Herrera-Cuenca M, et al. Dietary diversity and micronutrients adequacy in women of childbearing age: results from ELANS study. Nutrients. 2020;12(7):1994. [CrossRef]
- Nutrition during pregnancy [Internet]. Maryland: Johns Hopkins University [cited 26/1/2024]. Available in:https://www.hopkinsmedicine.org/health/wellness-and-prevention/nutrition-during-pregnancy#:~:text=Dietary%20and%20Caloric%20Recommendations,be%20kept%20to%20a%20minimum.
- Nutrición durante el embarazo [Internet]. Maryland: NIH; 2021 [cited 26/1/2024]. Available in: https://medlineplus.gov/spanish/pregnancyandnutrition.html.
- WHO recommendations on antenatal care for a positive pregnancy experience. [Internet]. Geneva: WHO press; 2016 [cited 26/1/2024]. Available in: https://iris.who.int/bitstream/handle/10665/250796/9789241549912-eng.pdf?sequence=1.
- Sambra V, Echeverria F, Valenzuela A, Chouinard-Watkins R, Valenzuela R. Docosahexaenoic and Arachidonic Acids as Neuroprotective Nutrients throughout the Life Cycle. Nutrients. 2021; 13: 986. [CrossRef]
- Office of Disease Prevention and Health Promotion [Internet]. Maryland: OASH [last updated 31/1/2023 ; cited 26/1/2024]. Available in: https://health.gov/myhealthfinder/pregnancy/nutrition-and-physical-activity/eat-healthy-during-pregnancy-quick-tips.
- Nearly half of all pregnancies are unintended -a global crisis, says new UNFPA report [Internet]. New York: UNFPA; 2022 [cited 28/2/2024]. Available in: https://www.unfpa.org/press/nearly-half-all-pregnancies-are-unintended-global-crisis-says-new-unfpa-report.
- Heras-Sola J, Gallo-Vallejo JL. Importancia de la colina durante el embarazo y lactancia. Una revisión sistemática [Importance of choline during pregnancy and lactation: A systematic review]. Semergen. 2024; 50(1):102089. [CrossRef]
- University of Florida. Mothers see healthier children in the “One Egg Per Day” project in Burkina Faso. https://blogs.ifas.ufl.edu/lsil/2020/02/24/mothers-see-healthier-children-in-the-one-egg-per-day-project-in-burkina-faso/Access: June 6 2024.
Figure 1.
Flow chart of selection of ELANS childbearing age women participants.
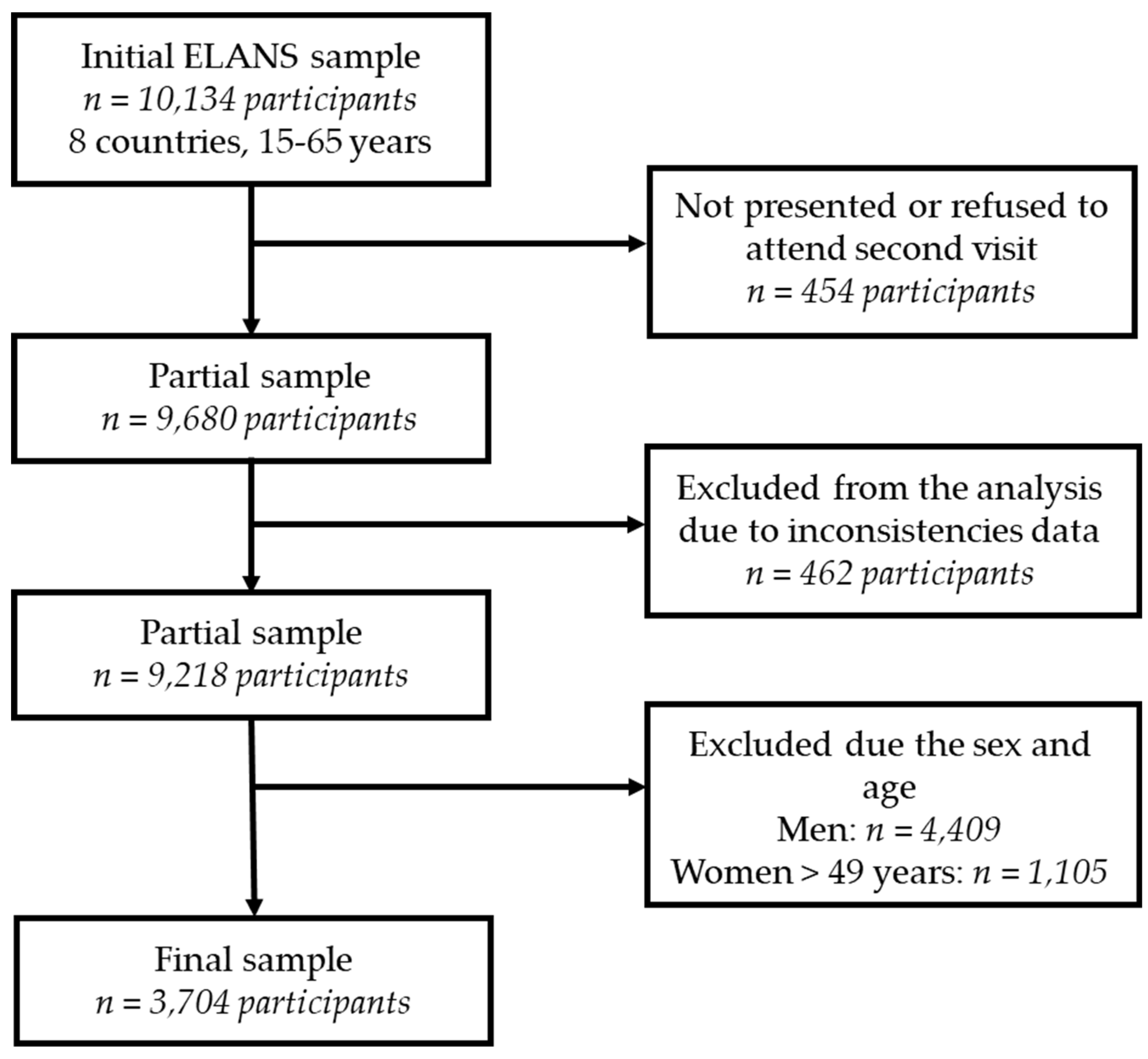
Figure 2.
Mean daily choline intake (mg/day) by the 5 most contributing food group and ELANS countries.
Figure 2.
Mean daily choline intake (mg/day) by the 5 most contributing food group and ELANS countries.
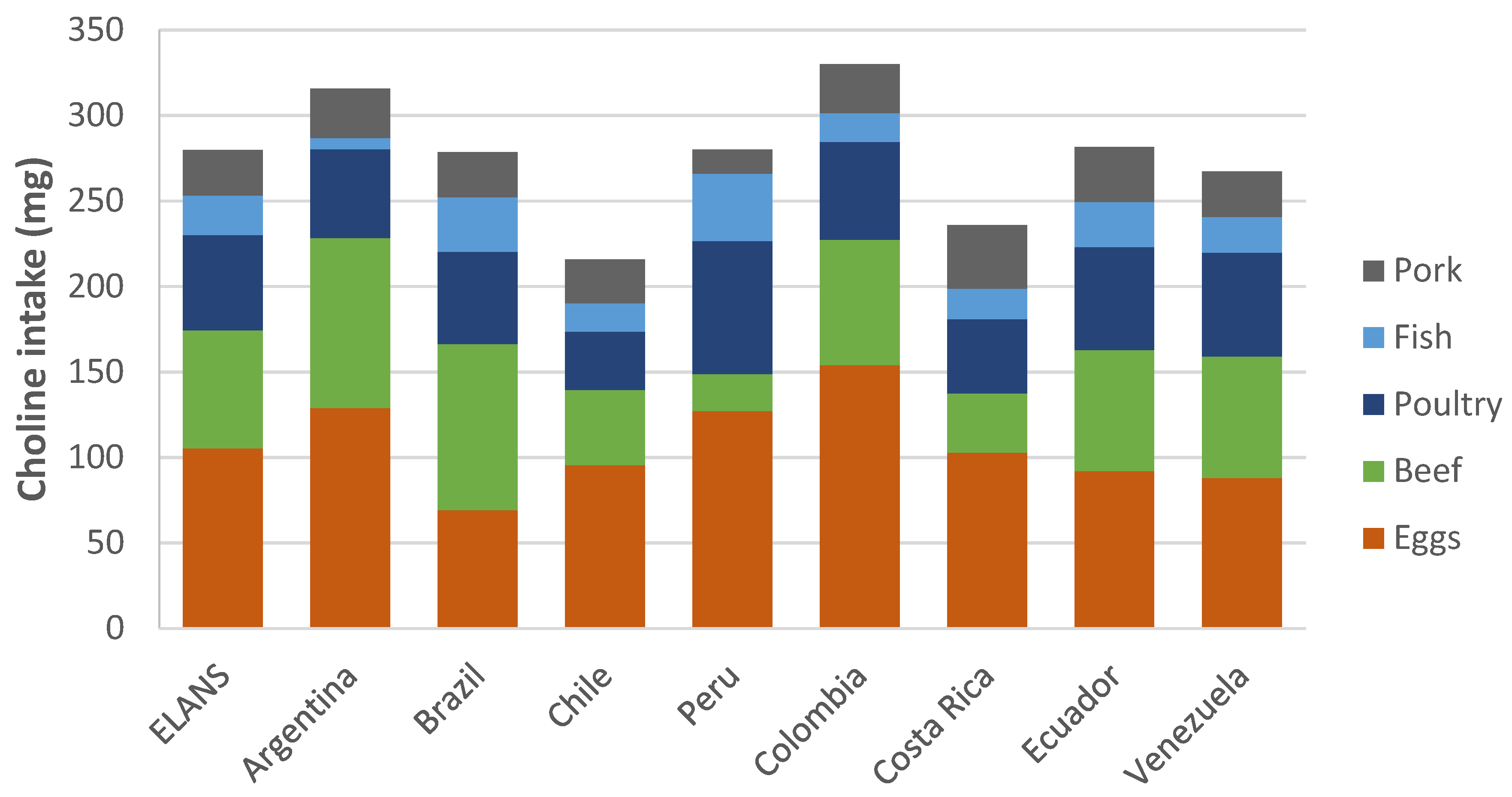
Figure 3.
CRT Tree for choline adequacy in three levels.
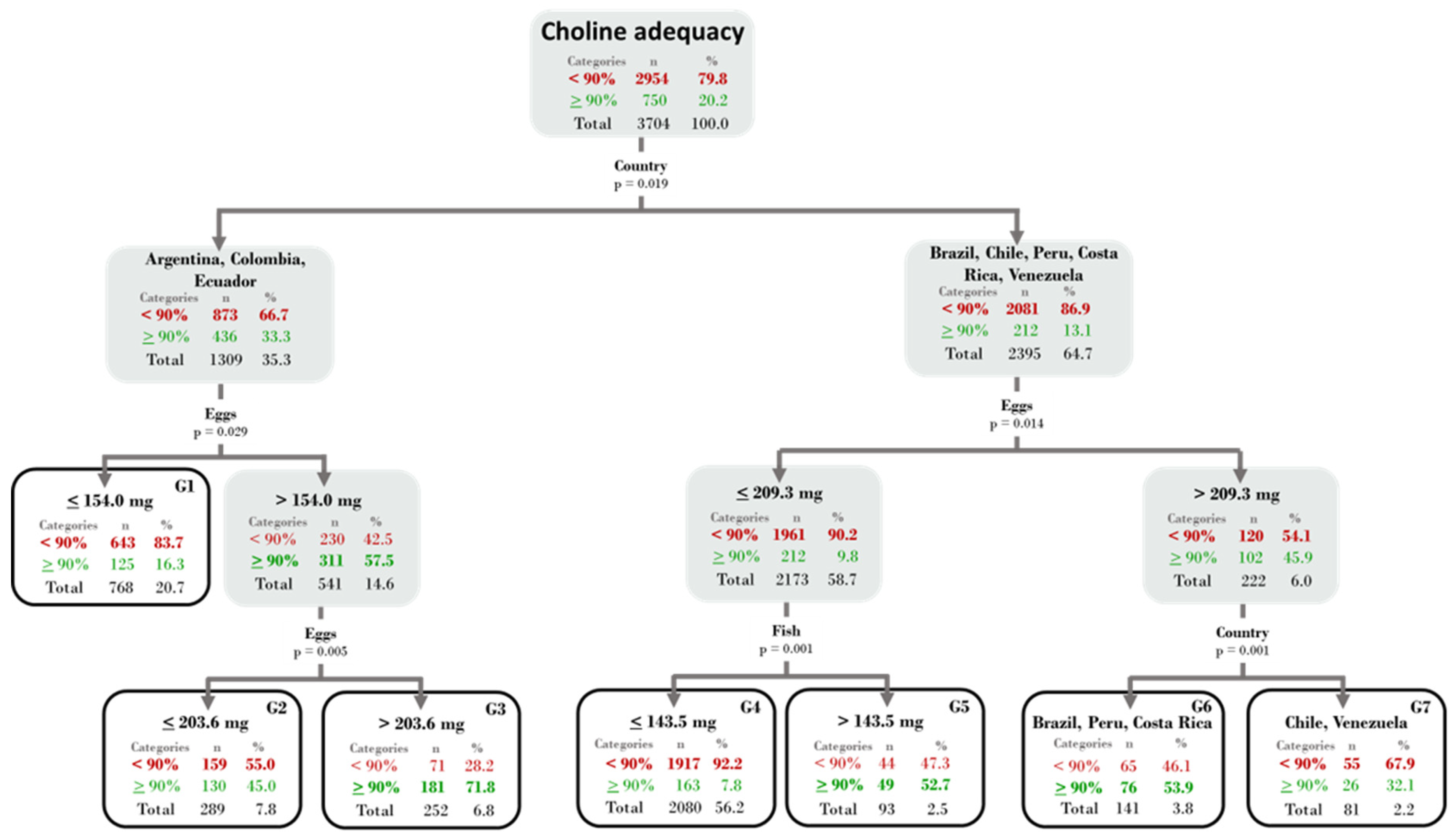
Figure 4.
Mean daily omega-3 intake (g/day) by the five most contributing food groups and ELANS countries.
Figure 4.
Mean daily omega-3 intake (g/day) by the five most contributing food groups and ELANS countries.
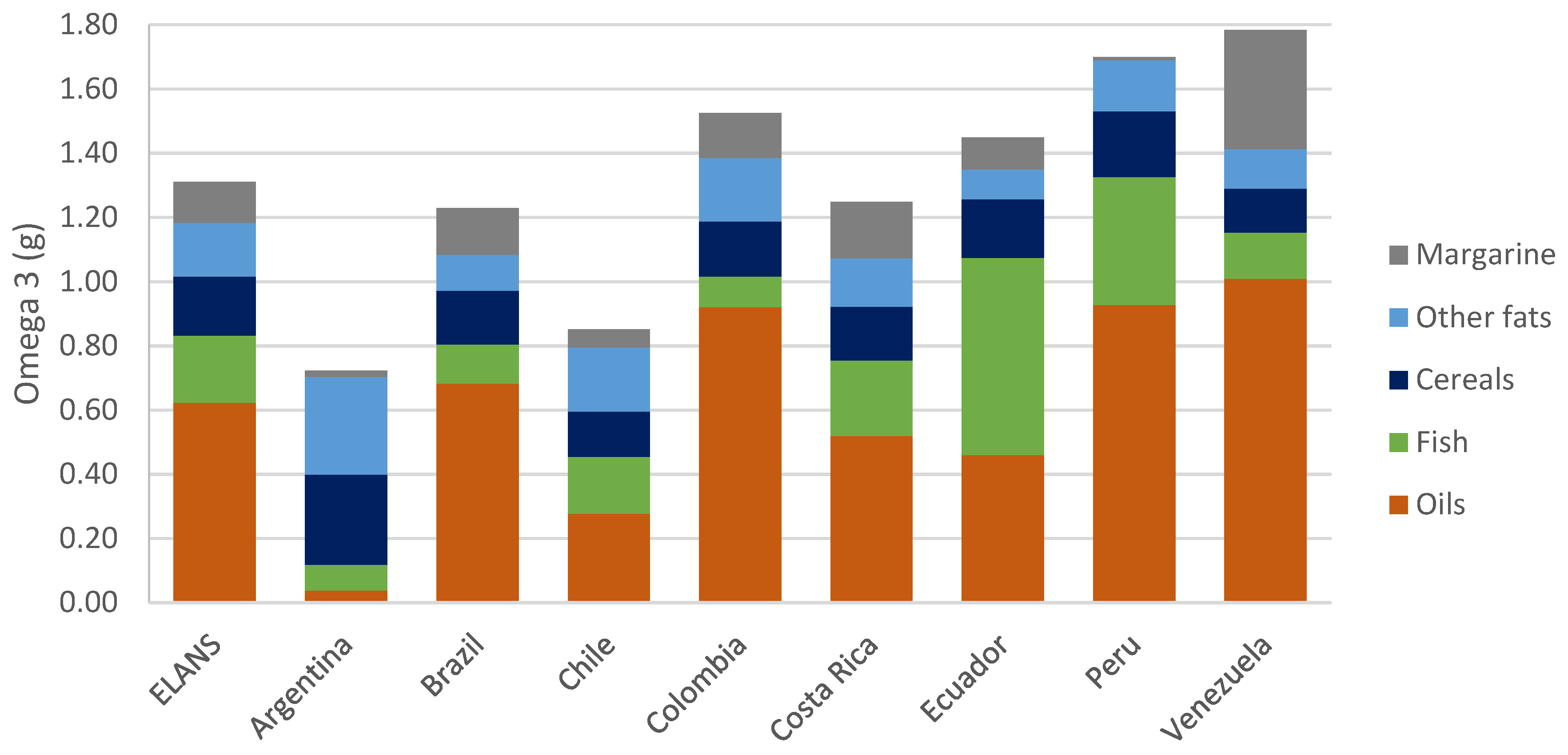
Figure 5.
Mean daily omega-6 intake (g/day) by the five most contributing food groups and ELANS countries.
Figure 5.
Mean daily omega-6 intake (g/day) by the five most contributing food groups and ELANS countries.


Table 1.
Sociodemographic characteristics of childbearing age women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
Table 1.
Sociodemographic characteristics of childbearing age women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
| Characteristics | ELANS | Argentina | Brazil | Chile | Colombia | Costa Rica | Ecuador | Peru | Venezuela | |||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | |
| Sample size | 3704 | 100.0 | 521 | 100.0 | 798 | 100.0 | 345 | 100.0 | 464 | 100.0 | 309 | 100.0 | 324 | 100.0 | 480 | 100.0 | 463 | 100.0 |
| Age group | ||||||||||||||||||
| 15–19 years | 539 | 14.6 | 61 | 11.7 | 95 | 11.9 | 56 | 16.2 | 67 | 14.4 | 55 | 17.8 | 56 | 17.3 | 75 | 15.6 | 74 | 16.0 |
| 20–34 years | 1771 | 47.8 | 244 | 46.8 | 379 | 47.5 | 152 | 44.1 | 224 | 48.3 | 143 | 46.3 | 152 | 46.9 | 246 | 51.3 | 231 | 49.9 |
| 35–49 years | 1394 | 37.6 | 216 | 41.5 | 324 | 40.6 | 137 | 39.7 | 173 | 37.3 | 111 | 35.9 | 116 | 35.8 | 159 | 33.1 | 158 | 34.1 |
| Socioeconomic status | ||||||||||||||||||
| Low | 1982 | 53.5 | 271 | 52.0 | 381 | 47.8 | 150 | 43.5 | 314 | 67.7 | 115 | 37.2 | 164 | 50.7 | 235 | 49.0 | 352 | 76.0 |
| Medium | 1385 | 37.4 | 228 | 43.8 | 352 | 44.1 | 165 | 47.8 | 132 | 28.4 | 155 | 50.2 | 120 | 37.0 | 154 | 32.0 | 79 | 17.1 |
| High | 337 | 9.1 | 22 | 4.2 | 65 | 8.1 | 30 | 8.7 | 18 | 3.9 | 39 | 12.6 | 40 | 12.3 | 91 | 19.0 | 32 | 6.9 |
| Education level | ||||||||||||||||||
| None and basic | 2139 | 57.7 | 359 | 68.9 | 344 | 43.1 | 217 | 62.9 | 280 | 60.4 | 248 | 80.3 | 271 | 83.6 | 111 | 23.1 | 309 | 66.8 |
| High school | 1196 | 32.3 | 134 | 25.7 | 386 | 48.4 | 91 | 26.4 | 132 | 28.4 | 40 | 12.9 | 35 | 10.8 | 320 | 66.7 | 58 | 12.5 |
| Bachelor’s degree | 369 | 10.0 | 28 | 5.4 | 68 | 8.5 | 37 | 10.7 | 52 | 11.2 | 21 | 6.8 | 18 | 5.6 | 49 | 10.2 | 96 | 20.7 |
| Marital Status | ||||||||||||||||||
| Single | 1527 | 41.2 | 186 | 35.7 | 342 | 42.9 | 163 | 47.2 | 206 | 44.4 | 128 | 41.4 | 111 | 34.3 | 168 | 35.0 | 223 | 48.2 |
| Married/Couple | 1863 | 50.3 | 271 | 52.0 | 388 | 48.6 | 162 | 47.0 | 226 | 48.7 | 154 | 49.8 | 187 | 57.7 | 276 | 57.5 | 199 | 43.0 |
| Divorced/Widowed | 314 | 8.5 | 64 | 12.3 | 68 | 8.5 | 20 | 5.8 | 32 | 6.9 | 27 | 8.7 | 26 | 8.0 | 36 | 7.5 | 41 | 8.9 |
Table 2.
Choline consumption parameters of childbearing age women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
Table 2.
Choline consumption parameters of childbearing age women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
| Choline consumption | Choline adequacy | Percentage of sample* | |||||||||||||||
| Characteristics | Milligrams (mg) | Percentage (%) | Deficient | Normal | Excessive | ||||||||||||
| n | Mean | SEM | Min | Max | Mean | SEM | Min | Max | n | % | n | % | n | % | |||
| Country | |||||||||||||||||
| ELANS | 3704 | 305.0 | 1.6 | 48.8 | 913.7 | 71.8 | 0.4 | 11.5 | 215.0 | 2954 | 79.8 | 520 | 14.0 | 230 | 6.2 | ||
| Argentina | 521 | 338.7 | 4.4 | 100.3 | 912.6 | 79.7 | 1.0 | 23.6 | 214.7 | 375 | 72.0 | 96 | 18.4 | 50 | 9.6 | ||
| Brazil | 798 | 294.7 | 3.5 | 48.8 | 913.7 | 69.3 | 0.8 | 11.5 | 215.0 | 666 | 83.5 | 92 | 11.5 | 40 | 5.0 | ||
| Chile | 345 | 238.6 | 3.8 | 62.1 | 503.7 | 56.1 | 0.9 | 14.6 | 118.5 | 329 | 95.4 | 14 | 4.1 | 2 | 0.6 | ||
| Colombia | 464 | 373.1 | 4.8 | 138.4 | 697.1 | 87.8 | 1.1 | 32.6 | 164.0 | 256 | 55.2 | 120 | 25.9 | 88 | 19.0 | ||
| Costa Rica | 309 | 262.5 | 4.9 | 69.0 | 662.9 | 61.8 | 1.1 | 16.2 | 156.0 | 280 | 90.6 | 21 | 6.8 | 8 | 2.6 | ||
| Ecuador | 324 | 327.6 | 5.0 | 138.4 | 614.8 | 77.1 | 1.2 | 32.6 | 144.7 | 242 | 74.7 | 63 | 19.4 | 19 | 5.9 | ||
| Peru | 480 | 313.8 | 3.7 | 99.8 | 663.9 | 73.8 | 0.9 | 23.0 | 156.2 | 382 | 79.6 | 80 | 16.7 | 18 | 3.8 | ||
| Venezuela | 463 | 269.8 | 3.6 | 69.2 | 542.0 | 63.5 | 0.8 | 16.3 | 127.5 | 424 | 91.6 | 34 | 7.3 | 5 | 1.1 | ||
| Age group | |||||||||||||||||
| 15–19 years | 539 | 301.3 | 4.1 | 69.0 | 662.9 | 70.9 | 1.0 | 16.2 | 156.0 | 441 | 81.8 | 66 | 12.2 | 32 | 5.9 | ||
| 20–34 years | 1771 | 310.3 | 2.3 | 87.0 | 912.6 | 73.0 | 0.6 | 20.5 | 214.7 | 1381 | 78.0 | 277 | 15.6 | 113 | 6.4 | ||
| 35–49 years | 1394 | 299.9 | 2.7 | 48.8 | 913.7 | 70.6 | 0.6 | 11.5 | 215.0 | 1132 | 81.2 | 177 | 12.7 | 85 | 6.1 | ||
| Socioeconomic status | |||||||||||||||||
| Low | 1982 | 306.5 | 2.3 | 48.8 | 913.7 | 72.1 | 0.5 | 11.5 | 215.0 | 1564 | 78.9 | 276 | 13.9 | 142 | 7.2 | ||
| Medium | 1385 | 303.1 | 2.6 | 69.2 | 912.6 | 71.3 | 0.6 | 16.3 | 214.7 | 1118 | 80.7 | 190 | 13.7 | 77 | 5.6 | ||
| High | 337 | 304.3 | 4.7 | 136.1 | 584.3 | 71.6 | 1.1 | 32.0 | 137.5 | 272 | 80.7 | 54 | 16.0 | 11 | 3.3 | ||
| Education level | |||||||||||||||||
| None and basic | 2139 | 301.4 | 2.2 | 48.8 | 913.7 | 70.9 | 0.5 | 11.5 | 215.0 | 1708 | 79.9 | 290 | 13.6 | 141 | 6.6 | ||
| High school | 1196 | 311.2 | 2.8 | 87.0 | 697.1 | 73.2 | 0.6 | 20.5 | 164.0 | 954 | 79.8 | 167 | 14.0 | 75 | 6.3 | ||
| Bachelor’s degree | 369 | 305.9 | 4.6 | 136.1 | 584.3 | 72.0 | 1.1 | 32.0 | 137.5 | 292 | 79.1 | 63 | 17.1 | 14 | 3.8 | ||
| Marital Status | |||||||||||||||||
| Single | 1527 | 301.5 | 2.5 | 69.0 | 913.7 | 70.9 | 0.6 | 16.2 | 215.0 | 1238 | 81.1 | 199 | 13.0 | 90 | 5.9 | ||
| Married/Couple | 1863 | 308.9 | 2.3 | 48.8 | 912.6 | 72.7 | 0.5 | 11.5 | 214.7 | 1459 | 78.3 | 283 | 15.2 | 121 | 6.5 | ||
| Divorced/Widowed | 314 | 299.5 | 5.5 | 62.1 | 637.1 | 70.5 | 1.3 | 14.6 | 149.9 | 257 | 81.8 | 38 | 12.1 | 19 | 6.1 | ||
Table 3.
Alpha-Linolenic acid consumption parameters of childbearing age women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
Table 3.
Alpha-Linolenic acid consumption parameters of childbearing age women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
| Alpha Linolenic acid | Alpha Linolenic acid adequacy | Percentage of sample* | |||||||||||||||
| Characteristics | Grams (g) | Percentage (%) | Deficient | Normal | Excessive | ||||||||||||
| n | Mean | SEM | Min | Max | Mean | SEM | Min | Max | n | % | n | % | n | % | |||
| Country | |||||||||||||||||
| ELANS | 3704 | 1.38 | 0.01 | 0.23 | 7.71 | 125.5 | 0.9 | 20.7 | 701.2 | 1049 | 28.3 | 597 | 16.1 | 2058 | 55.6 | ||
| Argentina | 521 | 0.98 | 0.02 | 0.29 | 2.89 | 89.1 | 1.6 | 26.3 | 262.6 | 300 | 57.6 | 88 | 16.9 | 133 | 25.5 | ||
| Brazil | 798 | 1.44 | 0.02 | 0.38 | 4.79 | 130.9 | 1.8 | 34.5 | 435.3 | 159 | 19.9 | 131 | 16.4 | 508 | 63.7 | ||
| Chile | 345 | 1.01 | 0.02 | 0.23 | 3.10 | 92.2 | 2.2 | 20.7 | 282.0 | 192 | 55.7 | 59 | 17.1 | 94 | 27.2 | ||
| Colombia | 464 | 1.63 | 0.03 | 0.45 | 7.71 | 148.5 | 2.9 | 40.6 | 701.2 | 61 | 13.1 | 55 | 11.9 | 348 | 75.0 | ||
| Costa Rica | 309 | 1.30 | 0.03 | 0.41 | 3.93 | 118.0 | 2.8 | 37.3 | 357.3 | 98 | 31.7 | 56 | 18.1 | 155 | 50.2 | ||
| Ecuador | 324 | 1.23 | 0.03 | 0.39 | 4.05 | 111.4 | 2.7 | 35.0 | 368.6 | 123 | 38.0 | 76 | 23.5 | 125 | 38.6 | ||
| Peru | 480 | 1.56 | 0.03 | 0.50 | 4.35 | 142.2 | 2.4 | 45.1 | 395.5 | 61 | 12.7 | 76 | 15.8 | 343 | 71.5 | ||
| Venezuela | 463 | 1.72 | 0.03 | 0.30 | 5.01 | 156.3 | 2.9 | 26.9 | 455.6 | 55 | 11.9 | 56 | 12.1 | 352 | 76.0 | ||
| Age group | |||||||||||||||||
| 15–19 years | 539 | 1.49 | 0.03 | 0.34 | 5.01 | 135.6 | 2.7 | 31.0 | 455.6 | 132 | 24.5 | 78 | 14.5 | 329 | 61.0 | ||
| 20–34 years | 1771 | 1.42 | 0.02 | 0.29 | 7.71 | 129.1 | 1.4 | 26.3 | 701.2 | 465 | 26.3 | 284 | 16.0 | 1022 | 57.7 | ||
| 35–49 years | 1394 | 1.29 | 0.01 | 0.23 | 4.35 | 116.9 | 1.3 | 20.7 | 395.5 | 452 | 32.4 | 235 | 16.9 | 707 | 50.7 | ||
| Socioeconomic status | |||||||||||||||||
| Low | 1982 | 1.39 | 0.01 | 0.23 | 7.71 | 126.8 | 1.3 | 20.7 | 701.2 | 554 | 28.0 | 318 | 16.0 | 1110 | 56.0 | ||
| Medium | 1385 | 1.35 | 0.02 | 0.29 | 4.68 | 122.9 | 1.4 | 26.3 | 425.4 | 407 | 29.4 | 218 | 15.7 | 760 | 54.9 | ||
| High | 337 | 1.41 | 0.03 | 0.39 | 3.64 | 128.6 | 3.0 | 35.0 | 330.7 | 88 | 26.1 | 61 | 18.1 | 188 | 55.8 | ||
| Education level | |||||||||||||||||
| None and basic | 2139 | 1.32 | 0.01 | 0.23 | 7.71 | 120.2 | 1.2 | 20.7 | 701.2 | 698 | 32.6 | 365 | 17.1 | 1076 | 50.3 | ||
| High school | 1196 | 1.45 | 0.02 | 0.33 | 4.79 | 132.0 | 1.6 | 29.6 | 435.3 | 273 | 22.8 | 182 | 15.2 | 741 | 62.0 | ||
| Bachelor’s degree | 369 | 1.48 | 0.03 | 0.30 | 3.58 | 134.9 | 2.8 | 27.3 | 325.1 | 78 | 21.1 | 50 | 13.6 | 241 | 65.3 | ||
| Marital Status | |||||||||||||||||
| Single | 1527 | 1.42 | 0.02 | 0.34 | 4.79 | 129.3 | 1.5 | 31.0 | 435.3 | 406 | 26.6 | 242 | 15.8 | 879 | 57.6 | ||
| Married/Couple | 1863 | 1.36 | 0.01 | 0.23 | 7.71 | 123.5 | 1.3 | 20.9 | 701.2 | 549 | 29.5 | 295 | 15.8 | 1019 | 54.7 | ||
| Divorced/Widowed | 314 | 1.31 | 0.03 | 0.23 | 3.45 | 119.2 | 2.9 | 20.7 | 313.8 | 94 | 29.9 | 60 | 19.1 | 160 | 51.0 | ||
* This data refers to the number and row percentages (%) of women with deficient, normal, or excessive choline intake. SEM: Standard error of the mean. Min: Minimum value. Max: Maximum value.
Table 4.
Other omega-3 fatty acids intake of childbearing women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
Table 4.
Other omega-3 fatty acids intake of childbearing women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
| EicosapentaenoicAcid | DocosahexaenoicAcid | Omega 3 total | |||||||||||||
| Characteristics | Milligrams (mg) | Milligrams (mg) | Grams (g) | ||||||||||||
| n | Mean | SEM | Min | Max | Mean | SEM | Min | Max | Mean | SEM | Min | Max | |||
| Country | |||||||||||||||
| ELANS | 3704 | 21.9 | 0.3 | 1.2 | 275.3 | 71.2 | 0.9 | 6.1 | 814.5 | 1.47 | 0.01 | 0.25 | 7.80 | ||
| Argentina | 521 | 16.6 | 0.4 | 2.0 | 92.5 | 63.0 | 1.6 | 7.6 | 326.5 | 1.06 | 0.02 | 0.33 | 2.96 | ||
| Brazil | 798 | 16.9 | 0.4 | 1.2 | 138.8 | 59.3 | 1.5 | 6.1 | 491.7 | 1.52 | 0.02 | 0.45 | 4.97 | ||
| Chile | 345 | 18.5 | 1.1 | 1.9 | 171.7 | 64.3 | 3.2 | 6.6 | 479.5 | 1.10 | 0.02 | 0.25 | 3.15 | ||
| Colombia | 464 | 19.7 | 0.7 | 2.5 | 203.6 | 62.9 | 1.7 | 6.5 | 357.3 | 1.72 | 0.03 | 0.47 | 7.80 | ||
| Costa Rica | 309 | 21.4 | 0.9 | 3.4 | 97.7 | 70.8 | 2.6 | 14.7 | 332.1 | 1.39 | 0.03 | 0.46 | 3.99 | ||
| Ecuador | 324 | 37.0 | 2.0 | 7.3 | 275.3 | 113.5 | 5.8 | 7.1 | 814.5 | 1.38 | 0.03 | 0.46 | 4.39 | ||
| Peru | 480 | 31.1 | 1.1 | 4.7 | 151.1 | 89.6 | 2.7 | 16.3 | 346.5 | 1.68 | 0.03 | 0.54 | 4.44 | ||
| Venezuela | 463 | 21.1 | 0.5 | 6.6 | 99.9 | 66.4 | 1.6 | 17.0 | 248.4 | 1.81 | 0.03 | 0.40 | 5.12 | ||
| Age group | |||||||||||||||
| 15–19 years | 539 | 20.7 | 0.7 | 2.4 | 197.9 | 68.0 | 2.3 | 8.5 | 549.8 | 1.58 | 0.03 | 0.38 | 5.12 | ||
| 20–34 years | 1771 | 22.0 | 0.5 | 1.2 | 275.3 | 71.0 | 1.3 | 6.1 | 814.5 | 1.51 | 0.02 | 0.33 | 7.80 | ||
| 35–49 years | 1394 | 22.1 | 0.5 | 1.9 | 216.1 | 72.9 | 1.6 | 6.6 | 621.8 | 1.38 | 0.02 | 0.25 | 4.44 | ||
| Socioeconomic status | |||||||||||||||
| Low | 1982 | 21.9 | 0.4 | 2.0 | 275.3 | 71.3 | 1.3 | 6.1 | 814.5 | 1.49 | 0.01 | 0.25 | 7.80 | ||
| Medium | 1385 | 21.2 | 0.5 | 1.2 | 203.6 | 70.2 | 1.4 | 7.1 | 479.5 | 1.44 | 0.02 | 0.33 | 4.85 | ||
| High | 337 | 24.1 | 1.2 | 2.4 | 195.6 | 75.2 | 3.3 | 13.8 | 548.8 | 1.51 | 0.03 | 0.45 | 3.69 | ||
| Education level | |||||||||||||||
| None and basic | 2139 | 21.6 | 0.4 | 1.2 | 216.1 | 71.5 | 1.2 | 6.6 | 621.8 | 1.42 | 0.01 | 0.25 | 7.80 | ||
| High school | 1196 | 22.0 | 0.6 | 2.3 | 275.3 | 70.6 | 1.6 | 6.1 | 814.5 | 1.55 | 0.02 | 0.42 | 4.97 | ||
| Bachelor’s degree | 369 | 22.8 | 1.1 | 2.0 | 203.6 | 72.0 | 2.8 | 6.5 | 357.3 | 1.58 | 0.03 | 0.37 | 3.67 | ||
| Marital Status | |||||||||||||||
| Single | 1527 | 20.6 | 0.4 | 1.9 | 197.9 | 67.1 | 1.3 | 6.1 | 549.8 | 1.51 | 0.02 | 0.38 | 4.97 | ||
| Married/Couple | 1863 | 22.7 | 0.5 | 1.2 | 275.3 | 73.9 | 1.4 | 8.5 | 814.5 | 1.45 | 0.01 | 0.33 | 7.80 | ||
| Divorced/Widowed | 314 | 23.0 | 1.3 | 2.7 | 216.1 | 75.4 | 3.7 | 7.1 | 621.8 | 1.41 | 0.03 | 0.25 | 3.54 | ||
* This data refers to the number and row percentages (%) of women with deficient, normal, or excessive choline intake. SEM: Standard error of the mean. Min: Minimum value. Max: Maximum value.
Table 5.
Linoleic acid consumption parameters of childbearing age women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
Table 5.
Linoleic acid consumption parameters of childbearing age women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
| Linoleic acid | Linoleic acid adequacy | Percentage of sample* | |||||||||||||||
| Characteristics | Grams (g) | Percentage (%) | Deficient | Normal | Excessive | ||||||||||||
| n | Mean | SEM | Min | Max | Mean | SEM | Min | Max | n | % | n | % | n | % | |||
| Country | |||||||||||||||||
| ELANS | 3704 | 13.91 | 0.09 | 2.94 | 57.92 | 125.5 | 0.9 | 20.7 | 701.3 | 1131 | 30.5 | 732 | 19.8 | 1841 | 49.7 | ||
| Argentina | 521 | 15.11 | 0.26 | 3.63 | 41.28 | 89.1 | 1.6 | 26.3 | 262.7 | 132 | 25.3 | 94 | 18.0 | 295 | 56.6 | ||
| Brazil | 798 | 12.84 | 0.18 | 3.22 | 36.28 | 130.9 | 1.8 | 34.5 | 435.3 | 301 | 37.7 | 166 | 20.8 | 331 | 41.5 | ||
| Chile | 345 | 11.44 | 0.21 | 2.94 | 27.21 | 92.2 | 2.2 | 20.7 | 282.0 | 163 | 47.2 | 70 | 20.3 | 112 | 32.5 | ||
| Colombia | 464 | 13.94 | 0.26 | 3.58 | 57.92 | 148.5 | 2.9 | 40.6 | 701.3 | 134 | 28.9 | 98 | 21.1 | 232 | 50.0 | ||
| Costa Rica | 309 | 13.44 | 0.27 | 3.65 | 31.18 | 118.0 | 2.8 | 37.3 | 357.3 | 99 | 32.0 | 71 | 23.0 | 139 | 45.0 | ||
| Ecuador | 324 | 17.47 | 0.35 | 5.88 | 43.75 | 111.5 | 2.7 | 35.0 | 368.6 | 38 | 11.7 | 48 | 14.8 | 238 | 73.5 | ||
| Peru | 480 | 14.10 | 0.22 | 4.75 | 34.53 | 142.2 | 2.4 | 45.1 | 395.5 | 118 | 24.6 | 98 | 20.4 | 264 | 55.0 | ||
| Venezuela | 463 | 13.81 | 0.25 | 3.93 | 39.87 | 156.3 | 2.9 | 26.9 | 455.6 | 146 | 31.5 | 87 | 18.8 | 230 | 49.7 | ||
| Age group | |||||||||||||||||
| 15–19 years | 539 | 15.19 | 0.26 | 4.36 | 41.88 | 135.6 | 2.7 | 31.0 | 455.6 | 99 | 18.4 | 99 | 18.4 | 341 | 63.3 | ||
| 20–34 years | 1771 | 14.18 | 0.13 | 3.58 | 57.92 | 129.1 | 1.4 | 26.3 | 701.2 | 522 | 29.5 | 347 | 19.6 | 902 | 50.9 | ||
| 35–49 years | 1394 | 13.06 | 0.13 | 2.94 | 36.28 | 116.9 | 1.3 | 20.7 | 395.5 | 510 | 36.6 | 286 | 20.5 | 598 | 42.9 | ||
| Socioeconomic status | |||||||||||||||||
| Low | 1982 | 13.95 | 0.12 | 3.04 | 57.92 | 126.8 | 1.3 | 20.7 | 701.2 | 598 | 30.2 | 391 | 19.7 | 993 | 50.1 | ||
| Medium | 1385 | 13.89 | 0.14 | 2.94 | 41.28 | 122.9 | 1.4 | 26.3 | 425.4 | 423 | 30.5 | 271 | 19.6 | 691 | 49.9 | ||
| High | 337 | 13.74 | 0.30 | 4.45 | 43.75 | 128.6 | 3.0 | 35.0 | 330.7 | 110 | 32.6 | 70 | 20.8 | 157 | 46.6 | ||
| Education level | |||||||||||||||||
| None and basic | 2139 | 13.99 | 0.12 | 2.94 | 57.92 | 120.2 | 1.2 | 20.7 | 701.2 | 665 | 31.1 | 409 | 19.1 | 1065 | 49.8 | ||
| High school | 1196 | 13.90 | 0.15 | 4.03 | 47.77 | 132.0 | 1.6 | 29.6 | 435.3 | 351 | 29.3 | 249 | 20.8 | 596 | 49.8 | ||
| Bachelor’s degree | 369 | 13.44 | 0.24 | 3.58 | 31.37 | 134.9 | 2.8 | 27.3 | 325.1 | 115 | 31.2 | 74 | 20.1 | 180 | 48.8 | ||
| Marital Status | |||||||||||||||||
| Single | 1527 | 14.07 | 0.14 | 3.58 | 47.77 | 129.3 | 1.5 | 31.0 | 435.3 | 449 | 29.4 | 293 | 19.2 | 785 | 51.4 | ||
| Married/Couple | 1863 | 13.84 | 0.13 | 2.94 | 57.92 | 123.5 | 1.3 | 20.9 | 701.2 | 578 | 31.0 | 367 | 19.7 | 918 | 49.3 | ||
| Divorced/Widowed | 314 | 13.52 | 0.29 | 3.04 | 35.84 | 119.2 | 2.9 | 20.7 | 313.8 | 104 | 33.1 | 72 | 22.9 | 138 | 43.9 | ||
* This data refers to the number and row percentages (%) of women with deficient, normal, or excessive choline intake.
Table 6.
Other omega 6 fatty acids intake of childbearing age women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
Table 6.
Other omega 6 fatty acids intake of childbearing age women aged 15-49 years in the Latin American Study of Nutrition and Health (ELANS).
| Arachidonic Acid | Omega 6 total | |||||||||
| Characteristics | Milligrams (mg) | Grams (g) | ||||||||
| n | Mean | SEM | Min | Max | Mean | SEM | Min | Max | ||
| Country | ||||||||||
| ELANS | 3704 | 141.9 | 0.9 | 22.0 | 536.8 | 14.0 | 0.1 | 3.0 | 58.1 | |
| Argentina | 521 | 146.9 | 2.5 | 23.2 | 372.3 | 15.3 | 0.3 | 3.7 | 41.5 | |
| Brazil | 798 | 126.2 | 1.8 | 26.3 | 350.3 | 13.0 | 0.2 | 3.3 | 36.4 | |
| Chile | 345 | 116.3 | 2.7 | 29.4 | 482.8 | 11.6 | 0.2 | 3.0 | 27.3 | |
| Colombia | 464 | 149.8 | 2.5 | 22.0 | 335.7 | 14.1 | 0.3 | 3.6 | 58.1 | |
| Costa Rica | 309 | 133.2 | 3.0 | 25.3 | 415.2 | 13.6 | 0.3 | 3.7 | 31.3 | |
| Ecuador | 324 | 172.9 | 3.6 | 53.4 | 536.8 | 17.6 | 0.4 | 6.0 | 44.1 | |
| Peru | 480 | 157.7 | 2.4 | 23.2 | 321.0 | 14.3 | 0.2 | 4.8 | 34.8 | |
| Venezuela | 463 | 142.4 | 2.2 | 50.9 | 300.1 | 13.9 | 0.3 | 4.0 | 40.1 | |
| Age group | ||||||||||
| 15–19 years | 539 | 141.6 | 2.4 | 25.3 | 343.8 | 15.3 | 0.3 | 4.4 | 42.0 | |
| 20–34 years | 1771 | 144.7 | 1.3 | 26.3 | 536.8 | 14.3 | 0.1 | 3.6 | 58.1 | |
| 35–49 years | 1394 | 138.5 | 1.5 | 22.0 | 482.8 | 13.2 | 0.1 | 3.0 | 36.4 | |
| Socioeconomic status | ||||||||||
| Low | 1982 | 143.9 | 1.2 | 22.0 | 536.8 | 14.1 | 0.1 | 3.1 | 58.1 | |
| Medium | 1385 | 138.8 | 1.5 | 23.2 | 415.2 | 14.0 | 0.1 | 3.0 | 41.5 | |
| High | 337 | 143.3 | 3.1 | 23.2 | 348.6 | 13.9 | 0.3 | 4.5 | 44.1 | |
| Education level | ||||||||||
| None and basic | 2139 | 141.7 | 1.2 | 22.0 | 482.8 | 14.1 | 0.1 | 3.0 | 58.1 | |
| High school | 1196 | 143.6 | 1.6 | 24.3 | 536.8 | 14.0 | 0.2 | 4.1 | 48.0 | |
| Bachelor’s degree | 369 | 137.7 | 2.6 | 23.2 | 340.5 | 13.6 | 0.2 | 3.6 | 31.5 | |
| Marital Status | ||||||||||
| Single | 1527 | 139.3 | 1.4 | 23.2 | 415.2 | 14.2 | 0.1 | 3.6 | 48.0 | |
| Married/Couple | 1863 | 144.9 | 1.3 | 26.3 | 536.8 | 14.0 | 0.1 | 3.0 | 58.1 | |
| Divorced/Widowed | 314 | 137.0 | 3.3 | 22.0 | 368.3 | 13.7 | 0.3 | 3.1 | 36.0 | |
* This data refers to the number and row percentages (%) of women with deficient, normal, or excessive choline intake. SEM: Standard error of the mean. Min: Minimum value. Max: Maximum value.
Table 7.
Choline and essential fatty acids are the three most prominent pre-natal supplements by country.
Table 7.
Choline and essential fatty acids are the three most prominent pre-natal supplements by country.
| Pre-natal supplements | ||||
| Country | Option 1 | Option 2 | Option 3 | |
| Argentina | Comercial name | Maternil | Supradyn | --- |
| Choline (mg) | 0 | 0 | --- | |
| Omega-3 (mg) | 135 (105 DHA) | 0 | --- | |
| Omega-6 (mg) | 0 | 0 | 0 | |
| Brazil | Comercial name | Materna | Regenesis | OragestanGold |
| Choline (mg) | 0 | 0 | 0 | |
| Omega-3 (mg) | 0 | 300 (250 DHA) | 300 (200 DHA) | |
| Omega-6 (mg) | 0 | 0 | 0 | |
| Chile | Comercial name | Enfamom | Supradyn | One-a-day |
| Choline (mg) | 0 | 0 | 0 | |
| Omega-3 (mg) | 235 (200 DHA) | 0 | 235 (200 DHA) | |
| Omega-6 (mg) | 0 | 0 | 0 | |
| Colombia | Comercial name | Enfamom | Natele | One-a-day |
| Choline (mg) | 0 | 0 | 0 | |
| Omega-3 (mg) | 235 (200 DHA) | 125 (125 DHA) | 235 (200 DHA) | |
| Omega-6 (mg) | 0 | 0 | 0 | |
| Costa Rica | Comercial name | Gestavit | Natele | Medox |
| Choline (mg) | 0 | 0 | 0 | |
| Omega-3 (mg) | 150 (150 DHA) | |||
| Omega-6 (mg) | 0 | 0 | 0 | |
| Ecuador | Comercial name | Natalben | Natele | Panvit |
| Choline (mg) | 0 | 0 | 0 | |
| Omega-3 (mg) | 240 (200 DHA) | 0 | 0 | |
| Omega-6 (mg) | 0 | 0 | 0 | |
| Perú | Comercial name | Gestavit | Supradyn | Maddre |
| Choline (mg) | 0 | 0 | 0 | |
| Omega-3 (mg) | 150 (150 DHA) | 0 | 0 | |
| Omega-6 (mg) | 0 | 0 | 0 | |
| Venezuela | Comercial name | Maternavit | Miagest | Multivinol |
| Choline (mg) | 0 | 0 | 0 | |
| Omega-3 (mg) | 275 | 320 | 0 | |
| Omega-6 (mg) | 0 | 0 | 0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



