
Submitted:
03 August 2024
Posted:
05 August 2024
You are already at the latest version
Abstract
Children and adolescents (C&A) with congenital heart defects (CHD) have decreased functional capacity and executive functioning (EF) due to brain abnormalities and decreased oxygen saturation. Exercise may improve EF via increased cognitive demands and cerebral blood supply. The purpose of this review was to identify current evidence describing the impact of physical activity (PA) interventions on EF in C&A with CHD. The following databases were searched from 2014-present: MEDLINE, EMBASE, CINAHL, Scopus, CENTRAL, and PsycInfo. Article inclusion criteria consisted of participants from birth to 18 years with CHD, interventions related to PA, and EF as an outcome. Articles were excluded if: adults were included, translation to English was impossible, and full access was unavailable. As a result of the review, 431 studies were screened. Three articles underwent full analyzation and only one met all criteria and this study found that with exercise there were significant improvements on self-reported cognitive functioning and parent-reported social functioning. Despite theoretical benefits, only one published study has investigated the role that PA interventions have on EF in C&A with CHD. Further investigation of the effect PA interventions have on EF in C&A with CHD is needed.
Keywords:
Children
; adolescents
; cognition
; congenital heart disease
; physical activity
; exercise
; aerobic training
1. Introduction
Children and adolescents (C&A) with congenital heart defects (CHD) have decreased functional capacity and executive functioning (EF) compared to typical peers. These children often do not have the opportunity or education to participate in safe physical activity (PA) and exercise [1]. CHDs are the most common birth defect in the United States and impact normal blood flow through the heart and great vessels [2,3]. These defects can result in the need for multiple surgical interventions with diverse timing. Most born with CHD are now surviving into adulthood. However, despite increased survival rates due to medical advancements, there continues to be risks such as hypoxic events during cardiac surgery and impaired cardiorespiratory functioning [4,5,6,7]. Individuals with CHD face additional challenges due to brain structural abnormalities, chronically decreased oxygenation, and perceived physical limitations [8]. The combination of physical limitation coupled with structural abnormalities of the brain often result in additional impairments in EF.
Executive functioning encompasses skills for goal-directed behavior which includes self-regulation and three key types of brain function consisting of working memory, mental flexibility, and self-control. These purposeful skills organize behavior and emotional regulation [7]. Children and adolescents with CHD are at risk for EF impairments due to disease severity, premature birth, and brain insults with alterations seen in brain volume, cortical measurements, and white matter microstructure [8]. Full term children with cyanotic defects are born with smaller brains and decreased grey matter volumes in the frontal lobe compared to typical peers [7]. Children with single ventricle physiology, such as those with hypoplastic left heart syndrome (HLHS), face greater impairments in EF. Due to staged palliative procedures, such as the Fontan procedure, children with HLHS face prolonged periods of time with reduced oxygenation and perfusion to the brain [7]. This can lead to school related activity limitations and participation restrictions when engaging in play with peers [6,7,9]. The prefrontal cortex (PFC) is vital for EF and continues to develop into late adolescence [2]. Due the connection with the developing PFC, EF continues to develop into early adulthood. This progressive maturation has been proposed as the rationale for the favorable effects of dynamic aerobic exercise on EF in C&A with CHD.
Exercise may improve EF in two ways including increasing cognitive demands and increasing cerebral blood supply [2]. Cognitive demands during sport-like activities and bimanual coordination stimulates higher thinking processes and requires direct attention to the novel and dynamic activity. Additionally, exercise promotes increased cerebral perfusion. In animal studies, aerobic exercise leads to increased blood capillary supply to the PFC and stimulates growth of new neurons and synapses [10]. In young adults, acute exercise has a positive effect on EF and arousal related prefrontal activation [11]. Beneficial effects of exercise have been shown during both acute and chronic exercise in C&A [2,11,12,13]. Despite this likely connection, there appears to be a lack of research investigating PA and EF in C&A with CHD.
A preliminary search of PubMed and Open Science Framework was conducted and no current or underway systematic reviews or scoping reviews on the topic were identified. Due to the lack of published evidence, the authors chose to conduct a scoping review to gain a better understanding of the scope or coverage of the literature related to how participation in a PA impacts EF in C&A with CHD and to identify knowledge gaps related to PA and EF in C&A with CHD.
2. Materials and Methods
The protocol for this scoping review was published in the Open Science Framework (https://doi.org/10.17605/OSF.IO/YFNX3) and created in accordance with the PRISMA extension for scoping reviews (PRISMA-ScR) [14]. An initial search strategy was conducted by one physical therapist to refine search terms and determine most appropriate databases. The search was then revised by physical therapists with pediatric and cardiovascular and pulmonary board specialties and included a total of four physical therapists, two of whom had previous experience conducting scoping reviews. Revisions to the scoping review were made to further refine the search terms and focus on the possible influence of interventions on EF. Article inclusion criteria consisted of participants from birth to 18 years with CHD, interventions related to PA, and EF as an outcome. Articles were excluded if: adults were included, translation to English was impossible, and full access was not available. The following databases were searched from 2014-present: MEDLINE, EMBASE, CINAHL, Scopus, CENTRAL, and PsycInfo. An example of a search string for the MEDLINE database is as follows: (Child OR Adolescent OR Pediatric) AND (Neurorehabilitation OR exercise capacity OR physical activity OR resistance training) AND (Congenital heart disease OR congenital heart defects OR Heart Defects OR Congenital surgery) AND (Executive function OR cognitive function OR cognitive performance).
Following the search, all identified citations were collected and exported into Covidence 2022 (Melbourne, Australia) and duplicates were removed. The articles were then independently screened by two team members for eligibility and inclusion criteria. The text words of the titles were analyzed, and the abstracts were reviewed for eligibility based on the inclusion and exclusion criteria. All eligible articles were then retrieved and reviewed. Reasons for exclusion of sources of evidence at full text that did not meet inclusion criteria were recorded. A third reviewer was available to resolve any discrepancies in article eligibility and data extraction, however, this was not required. The reference lists of eligible articles were also reviewed for inclusion. Article search terms included children, pediatrics, exercise, PA, CHD, cognition, and EF. The results of the search and the study inclusion process is reported in flow diagram format according to PRISMA-ScR [14,15].
Data was extracted by two team members and placed into a data extraction form, which was adapted from the JBI Manual for Evidence Synthesis [16]. The data extracted included specific details about the participants, study methods, and key findings. Due to the nature of scoping reviews, a formal assessment of methodological quality was not included in this scoping review.
3. Results
As a result of the scoping review, 431 studies were identified, and the findings are reported in Figure 1.
Six studies were duplicates and one was marked ineligible. After removal, 424 studies remained available for screening. Articles were excluded with titles and abstracts that were not relevant to pediatrics, children with CHD, PA, or EF. Out of the articles screened only four abstracts were sought out for full analyzation [17,18,19,20]. After full analyzation, one of the four articles examined only included subjects who exceeded our age range inclusion criteria [20] resulting in a total of three articles for further review and possible inclusion [17,18,19]. The data from the three articles are reported in Table 1.
Out of the three articles assessed for eligibility, only the study by Dulfer et al met all inclusion criteria [17]. Although the study by Dulfer et al. did include adults, 46 C&A aged 10-15 years with post-surgical repair for tetralogy of Fallot (ToF) or Fontan circulation underwent a stratified randomization to a control or exercise group. The exercise group (n=25) performed 40 minutes of aerobic dynamic cardiovascular training preceded and followed by a 10-minute warm up and cooldown. Walking, jogging, running, bicycling, and dynamic play activities were performed three times/week for three months at 60-70% of heart rate reserve. Cognitive functioning was measured using the parent and adult form of the TNO/AZL Child Quality of Life Questionnaire. Significant findings were only found for the 10–15-year cohort of children and included improved self-reported cognitive functioning (p<.05, r=.30) and parent-reported social functioning (p<.05, r=.30) [17]. It was additionally found that children with lower baseline scores of motor and cognitive functioning had significant improvements after intervention (z= -2.54, p<.05, r=.57 and z= -2.11, p<.05, r=.50 respectively) [17].
The article by Cooney et al was excluded because no intervention was conducted [18]. However, maximal cardiopulmonary exercise tests (CPET) were performed, and EF was assessed by the Wechsler Adult Intelligence Scale (WAIS-IV), the Wechsler Intelligence Scale for Children, 5th edition (WISC-V), and the Tower of London-Drexel (TOL). The study methodology consisted of CPET and neuropsychological testing (NPT) on children with single ventricle heart disease (SVHD) post Fontan palliation. Exercise testing was completed with a Medgraphics (Saint Paul, MN) metabolic cart. Breath-by-breath data were collected and averaged over 20 second intervals. The subjects performed a symptom-limited test using a ramp protocol on a cycle ergometer. Oxygen saturation, electrocardiogram, and blood pressure were also monitored and measured. A neuropsychologist completed the NPT in a single session on a different day than the CPET. Results from this study found that the percent predicted values for maximal oxygen consumption (VO2 max) and peak heart rate of the SVHD group were substantially lower than values for healthy, age-matched children (44% predicted VO2max, 76% peak heart). On EF and adaptive functioning, the SVHD cohort scored 1-1.5 standard deviations below normative values. Linear regression analyses found that both VO2max and anaerobic threshold were associated with parent-rated overall adaptive function. In fact, for one unit increase in VO2max, the global adaptive composite (GAC) increased by 1.13 units (95% CI 0.29, 1.96 p = 0.01). An increase in one unit of anaerobic threshold was related to an increase in GAC of 1.61 (95% CI 0.27,2.94; p = 0.02). Finally, peak heart rate was found to be related to sustained visual attention and an increase by one heartbeat was related to a decrease of 0.4 in the errors of omission T-score (95% CI (− 0.71, − 0.09); p = 0.01). It was further noted that none of the CPET variables were significantly related to working memory, processing speed, EF, or internalizing symptoms and ventilatory efficiency was not significantly related to any of the NPT variables.
Finally, the article by Verrall et al was excluded as it was a narrative review without a methodology fitting the inclusion criteria [19]. However, this article provided an important overview of the role exercise may have on EF in children with Fontan physiology. Proposed mechanisms include increasing grey and white matter volumes, enhancing white matter microstructure, and improving functional connectivity. Additionally, Verrall et al highlighted the effect exercise has on promoting neurogenesis and angiogenesis. The above improvements from PA may improve EF in C&A with CHD and reduce the risk of neurodegenerative decline and dementia in adults with CHD which is a growing concern in this patient population. The Verrall et al article along with others noted during the screening process provide substantial insight into a variety of potential interventions for individuals with CHD with exercise being a key method to improve EF in C&A and adults with CHD [19,21].
4. Discussion
During this scoping review process, it was noted that (1) EF was consistently impaired in children with CHD even as they age, (2) interventions for C&A with CHD need to be comprehensive to meet their unique needs, and (3) research remains limited.
EF is impaired in C&A with CHD. Infants with CHD are surviving into adulthood resulting in a focus on improving long term morbidity and quality of life [21,22]. Known secondary impairments are impaired cognition, behavioral problems, delayed gross and fine motor skills, reduced exercise capacity and impaired EF [17,18,19,20,21,22,23]. These impairments have been found to be associated with severity of CHD and were found to begin in infancy and persist throughout adulthood [19,21]. In the Boston Circulatory Arrest Trial, a cohort of patients with dextrotransposition of the great arteries (d-TGA) who underwent the arterial switch operation were followed longitudinally [24,25,26,27]. As infants, these patients had lower than normal scores on the Bayley Scales of Infant Development [24]. As children, abnormal neurodevelopment persisted and a third had received special services in school [25,26]. At 16 years of age, neurodevelopmental scores continued to be lower than age matched healthy peers and abnormal magnetic resonance imaging (MRI) was found [27]. In a cohort of children with Fontan physiology, similar neurodevelopmental outcomes were found including lower intelligence scores, EF, and 11% higher frequency of abnormalities on MRI [28]. In the Single Ventricle Reconstruction (SVR) trial, 6-year outcomes found similar results to the aforementioned studies including deficits of mild and severe motor disabilities occurring at 6 and 11 times the normal incidence rate. [29] Parent-reported EF impairment was also reported to have an odds ratio of 4.37 when compared to typical age and gender matched peers [30]. As young adults with CHD, Fox et al found that one in 10 individuals reported clinically significant difficulties with global EF. These impairments in EF were further associated with health risk behaviors such as increased tobacco use and greater saturated fat intake [20].
An important conclusion from this scoping review is that interventions for C&A with CHD need to be comprehensive and tailored to the individual needs of each child or adolescent. In a screened article by Rogers and Dixon, it was found that most pediatric cardiac rehabilitation programs follow the same standards for adult programs, but only a few addressed the unique needs of pediatric patients with CHD including concerns for developmental delays, motor skills, and cognitive disruptions [31]. In a study of factors influencing PA in adolescents with complex CHD, total PA was higher in males, adolescents in formal physical education classes, and those with higher self-efficacy [32]. Additionally, quality of life impairments are common and one in three adults with CHD have mood or anxiety disorders [33]. In view of the above, there is a need for the development and examination of comprehensive rehabilitation programs for C&A with CHD to improve factors responsible for greater EF.
Research examining the effects of PA on EF is currently limited. Only one published study was found investigating the role that PA interventions may have on EF in children with CHD [17]. In adults, PA has many well-known benefits on cognition. Research in older adults has found relationships between PA and hippocampal volume preservation as well as increased brain volume [34,35]. In the narrative review by Verrall et al., exercise was proposed as a therapeutic intervention for neurodevelopmental and cognitive dysfunction in people with Fontan circulation [19]. This is a special population of C&A with CHD as these children face prolonged periods of cyanosis. Proposed mechanisms for potential benefits from PA include improved brain structure and function, neuroprotective and reparative cellular and molecular processes, cognitive reserve, and resilience [19].
It is important to note that cardiorespiratory fitness is associated with grey matter volumes in areas that are typically most sensitive to aging such as the frontal parietal and temporal cortices as well as the hippocampus [35,36]. These areas also have known functions in EF. Although the focus of this study is on C&A with CHD, preliminary research suggests that there is an accelerated age associated brain volume loss in adults with Fontan circulation [19]. In healthy children, associations between hippocampal volume, fitness, and memory performance have been found [37]. In a study by Riggs et al., aerobic exercises promoted hippocampal growth and white matter recovery in children post radiation therapy for brain tumors [38]. These same findings may be true in C&A with CHD for which investigation of the relationship and effects of PA on EF in C&A with CHD are warranted. In the study by Dulfer et al, changes in EF were measured via quality-of-life questionnaires [17]. Future research could include measuring changes via formal cerebral imaging. Additionally previous research on EF in children with CHD have included performance-based tests of EF such as the Stroop Test and Trail Making Test [6] as well as reported measures such as the Behavior Rating Inventory of Executive Function [39]. Including the above outcomes in a comprehensive cardiac rehabilitation program for C&A with CHD is likely to improve the management of C&A with CHD.
This scoping review was limited due to the lack of research meeting search criteria. Future research is needed to examine if PA interventions impact EF in children with CHD.
Author Contributions
Conceptualization, A.C., J.M., and L.C.; methodology, A.C., J.M., G.C., and L.C; software, A.C. and L.C.; investigation, A.C., J.M., and L.C.; resources, A.C., J.M., and L.C.; data curation, A.C. and L.C.; writing—original draft preparation, A.C.; writing—review and editing, A.C., J.M, L.C., G.C., N.K-S.; and supervision, N.K-S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gauthier N, Curran T, O'Neill JA, Alexander ME, Rhodes J. Establishing a comprehensive pediatric cardiac fitness and rehabilitation program for congenital heart disease. Pediatr Cardiol. 2020;41(8):1569-1579. [CrossRef]
- Best, J.R. Effects of physical activity on children's executive function: Contributions of experimental research on aerobic exercise. Developmental Review. 2010;30(4):331-351. [CrossRef]
- Vassar R, Peyvandi S, Gano D, et al. Critical congenital heart disease beyond HLHS and TGA: neonatal brain injury and early neurodevelopment. Pediatr Res. Published online 2023. [CrossRef]
- Wong R, Al-Omary M, Baker D, et al. Cognitive dysfunction is associated with abnormal responses in cerebral blood flow in patients with single ventricular physiology: Novel insights from transcranial Doppler ultrasound. Congenit Heart Dis. 2019;14(4):638-644. [CrossRef]
- Spillmann R, Polentarutti S, Ehrler M, Kretschmar O, Wehrle FM, Latal B. Congenital heart disease in school-aged children: Cognition, education, and participation in leisure activities. Pediatr Res. Published online 2021. [CrossRef]
- Calderon J, Bellinger DC. Executive function deficits in congenital heart disease: Why is intervention important? Cardiol Young. 2014;25(7):1238-1246. [CrossRef]
- Cassidy AR, White MT, DeMaso DR, Newburger JW, Bellinger DC. Executive function in children and adolescents with critical cyanotic congenital heart disease. Journal of the International Neuropsychological Society. 2015;21(1):34-49. [CrossRef]
- Bolduc ME, Lambert H, Ganeshamoorthy S, Brossard-Racine M. Structural brain abnormalities in adolescents and young adults with congenital heart defect: a systematic review. Dev Med Child Neurol. 2018;60(12):1209-1224. [CrossRef]
- Sanz JH, Wang J, Berl MM, Armour AC, Cheng YI, Donofrio MT. Executive function and psychosocial quality of life in school age children with congenital heart disease. J Pediatr. 2018;202:63-69. [CrossRef]
- Dishman RK, Berthoud HR, Booth FW, et al. Neurobiology of exercise. Obesity. 2006;14(3):345-356. [CrossRef]
- Byun K, Hyodo K, Suwabe K, et al. Positive effect of acute mild exercise on executive function via arousal-related prefrontal activations: An fNIRS study. Neuroimage. 2014;98:336-345. [CrossRef]
- Lambrick D, Stoner L, Grigg R, Faulkner J. Effects of continuous and intermittent exercise on executive function in children aged 8-10 years. Psychophysiology. 2016;53(9):1335-1342. [CrossRef]
- Hsieh SS, Chueh TY, Huang CJ, et al. Systematic review of the acute and chronic effects of high-intensity interval training on executive function across the lifespan. J Sports Sci. 2021;39(1):10-22. [CrossRef]
- Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med. 2018;169(7):467-473. [CrossRef]
- Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8(5):336-341. [CrossRef]
- Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z, eds. JBI manual for evidence synthesis. Published online 202. [CrossRef]
- Dulfer K, Duppen N, Kuipers IM, et al. Aerobic exercise influences quality of life of children and youngsters with congenital heart disease: a randomized controlled trial. J Adolesc Health. 2014;55(1):65-72. [CrossRef]
- Cooney SJ, Campbell K, Wolfe K, DiMaria MV, Rausch CM. Is neurodevelopment related to exercise capacity in single ventricle patients who have undergone Fontan palliation? Pediatr Cardiol. 2021;42(2):408-416. [CrossRef]
- Verrall CE, Tran DL, Yang JYM, et al. Exercise as therapy for neurodevelopmental and cognitive dysfunction in people with a Fontan circulation: A narrative review. Front Pediatr. 2023;11:1111785. [CrossRef]
- Fox KR, Vannatta K, Jackson JL. Difficulties with Executive Function are associated with risky health behaviors among young adult congenital heart defect survivors. J Cardiovasc Nurs. 2023;38(1):60-69. [CrossRef]
- Kobayashi K, Liu C, Jonas RA, Ishibashi N. The current status of neuroprotection in congenital heart disease. Children (Basel). 2021;8(12):1116. [CrossRef]
- van der Mheen M, Meentken MG, van Beynum IM, et al. CHIP-Family intervention to improve the psychosocial well-being of young children with congenital heart disease and their families: results of a randomised controlled trial. Cardiol Young. 2019;29(9):1172-1182. [CrossRef]
- Marino BS, Lipkin PH, Newburger JW, et al. Neurodevelopmental outcomes in children with congenital heart disease: evaluation and management: a scientific statement from the American Heart Association. Circulation. 2012;126(9):1143-1172. [CrossRef]
- Bellinger DC, Rappaport LA, Wypij D, Wernovsky G, Newburger JW. Patterns of developmental dysfunction after surgery during infancy to correct transposition of the great arteries. J Dev Behav Pediatr. 1997;18(2):75-83. [CrossRef]
- Bellinger DC, Wypij D, Kuban KC, et al. Developmental and neurological status of children at 4 years of age after heart surgery with hypothermic circulatory arrest or low-flow cardiopulmonary bypass. Circulation. 1999;100(5):526-532. [CrossRef]
- Bellinger DC, Wypij D, duPlessis AJ, et al. Neurodevelopmental status at eight years in children with dextro-transposition of the great arteries: the Boston Circulatory Arrest Trial. J Thorac Cardiovasc Surg. 2003;126(5):1385-1396. [CrossRef]
- Bellinger DC, Wypij D, Rivkin MJ, et al. Adolescents with d-transposition of the great arteries corrected with the arterial switch procedure: neuropsychological assessment and structural brain imaging. Circulation. 2011;124(12):1361-1369. [CrossRef]
- Bellinger DC, Watson CG, Rivkin MJ, et al. Neuropsychological status and structural brain imaging in adolescents with single ventricle who underwent the Fontan procedure. J Am Heart Assoc. 2015;4(12). [CrossRef]
- Sananes R, Goldberg CS, Newburger JW, et al. Six-year neurodevelopmental outcomes for children with single-ventricle physiology. Pediatrics. 2021;147(2):e2020014589. [CrossRef]
- Sanz JH, Berl MM, Armour AC, Wang J, Cheng YI, Donofrio MT. Prevalence and pattern of executive dysfunction in school age children with congenital heart disease. Congenit Heart Dis. 2017;12(2):202-209. [CrossRef]
- Rogers S, Dixon B. The new age of cardiac rehab: Do adult protocols meet the needs of children? Arch Phys Med Rehabil. 2021;102(10):e114.
- Kwon SJ, Choi EK, Lee KH, Im YM. Factors influencing physical activity in adolescents with complex congenital heart disease. Child Health Nurs Res. 2019;25(3):262-272. [CrossRef]
- Lui GK, Saidi A, Bhatt AB, et al. Diagnosis and management of noncardiac complications in adults with congenital heart disease: A scientific statement from the American heart association. Circulation. 2017;136(20):e348-e392.
- Soshi T, Andersson M, Kawagoe T, et al. Prefrontal plasticity after a 3-month exercise intervention in older adults relates to enhanced cognitive performance. Cereb Cortex. 2021;31(10):4501-4517. [CrossRef]
- Wilckens KA, Stillman CM, Waiwood AM, et al. Exercise interventions preserve hippocampal volume: A meta-analysis. Hippocampus. 2021;31(3):335-347. [CrossRef]
- Raichlen DA, Klimentidis YC, Bharadwaj PK, Alexander GE. Differential associations of engagement in physical activity and estimated cardiorespiratory fitness with brain volume in middle-aged to older adults. Brain Imaging Behav. 2020;14(5):1994-2003. [CrossRef]
- Chaddock L, Erickson KI, Prakash RS, et al. A neuroimaging investigation of the association between aerobic fitness, hippocampal volume, and memory performance in preadolescent children. Brain Res. 2010;1358:172-183. [CrossRef]
- Riggs L, Piscione J, Laughlin S, et al. Exercise training for neural recovery in a restricted sample of pediatric brain tumor survivors: a controlled clinical trial with crossover of training versus no training. Neuro Oncol. Published online 2016:now177. [CrossRef]
- Sanz JH, Berl MM, Armour AC, Wang J, Cheng YI, Donofrio MT. Prevalence and pattern of executive dysfunction in school age children with congenital heart disease. Congenit Heart Dis. Mar 2017;12(2):202-209. [CrossRef]
Figure 1.
Search strategy flowchart.
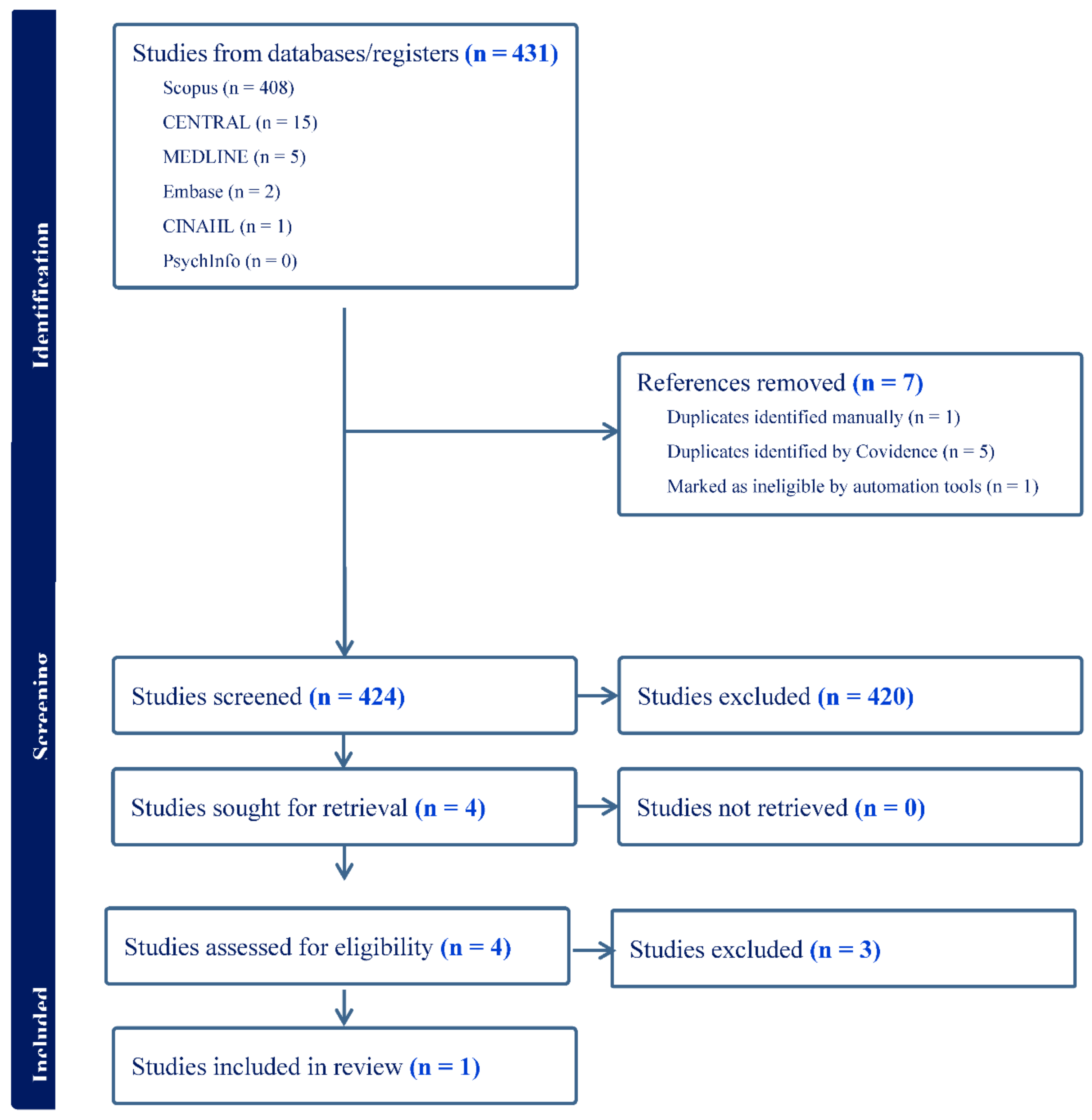

Table 1.
Data extraction form.
| Author | Dulfer et al [17] | Cooney et al [18] | Verrall et al [19] |
|---|---|---|---|
| Aims/Purpose | To investigate the effect of an exercise program on HRQoL in children and adolescents with TOF or Fontan circulation. | To characterize the relationship between neurodevelopment and exercise capacity in SVHD post Fontan by evaluating associations between CPET and clinical NPT. |
To discuss current interventions and evidence supporting exercise as a potential intervention for improving cognitive functioning in people with Fontan circulation. |
| Population | 93 participants, ages 10-25 years with surgical repair for ToF or with Fontan circulation. |
23 participants, ages 7- 17 years old with Fontan circulation. |
Discusses impact from fetus to aging adult. |
| Methodology | Stratified, randomized controlled intervention conducted in five pediatric centers in The Netherlands. Random allocation with a ratio of 2:1 to a 12-week period with an exercise program for three times per week or a control group. | Retrospective, cross-sectional pilot study conducted in the United States. One time conduction of CPET with gas analysis and one time conduction of NPT. | Narrative summary and discussion with following categories : established neurodevelopmental and cognitive interventions; exercise, cognition, and Fontan physiology; neural mechanisms underpinning the exercise-cognition relationship; and psychosocial and behavioral mediators of the exercise-cognition relationship |
| Interventions | Exercise program consisted of three one-hour long training sessions a week. Patients already active were encouraged to continue to do activities two times a week. Hour session consisted of 10 minute warm up, 40 minutes aerobic training, and 10-minute cooldown. Participants trained within given heart rate ranges. | Exercise testing was performed with a Medgraphics (Saint Paul, MN) metabolic cart. Breath-by-breath data were collected and averaged over 20 s intervals. Patients performed a symptom-limited test using a ramp protocol on a cycle ergometer. Monitoring of oxygen saturation, electrocardiogram, and blood pressure was also measured. NPT was conducted in a single session on a day separate from the CPET. Standardized scores were assessed from tests of working memory, processing speed, sustained visual attention, executive function, parent ratings of adaptive function, and internalizing problems. Scores were standardized by age. |
Individuals with Fontan physiology have greater risk of neurodevelopmental and cognitive impairments. Exercise is low-risk and has benefits on physical and cognitive functioning. Future research is needed to provide exercise prescription and determine accessible interventions. |
| Outcomes | At baseline and follow up after 12 weeks, participants and parents as appropriate completed the HRQoL measures: for the 10-15 group, TACQOL CF and TACQOL PF; for the 16-25 group, SF-36 and CONHD-TAAQOL; and for the total group 10-25, LAS. |
CPET measures: VO2max indexed to body weight, anaerobic threshold, peak heart rate, ventilatory efficiency, pulmonary vasodilator use, and RER. Results were compared to percent predicted values for VO2max and peak heart rate based on gender, height, and weight. NPT measures: executive function (WAIS-IV or WISC-V and TOL), attention (CPT-2,3), adaptive function (ABAS-2,3), and emotional function (BASC-2,3) |
|
| Key Findings | Compared with the control-group, children, aged 10-15 years in the exercise-group improved significantly on self-reported cognitive functioning and parent-reported social functioning. Increase noted in this group with lower baseline HRQoL. Participants aged 16-25 years did not change their HRQoL. | Higher VO2max and anaerobic threshold were related to better adaptive functioning scores and higher peak heart rate was related to better scores on a measure of sustained visual attention. The relationship appeared strongest in relation to adaptive function, as both higher VO2 max and anaerobic threshold were significantly associated with a higher global adaptive composite score. CPET variables related to working memory, processing speed, executive functioning, or internalizing symptoms were not significant. Ventilatory efficiency was not significantly related to any of the NPT variables | Interventions for impaired neurodevelopment and cognitive dysfunction in people with Fontan circulation are lacking |
HRQoL= health-related quality of life; ToF= tetralogy of Fallot; TACQOL CF and PF= TNO/AZL Child Quality of Life Questionnaire Child Form and Parent Form; SF-36= Short Form-36 Health Survey; CONHD-TAAQOL= Congenital Heart Disease-TNO/AZL Adult Quality of Life Questionnaire; LAS= linear analogue scale; SVHD= single ventricle heart disease; CPET=cardiopulmonary exercise testing; NPT: neuropsychological testing; VO2max=maximal oxygen consumption; RER= respiratory exchange ratio; WAIS-IV= Wechsler Adult Intelligence Scale; WISC-V= Wechsler Intelligence Scale for Children, 5th edition; TOL= Tower of London-Drexel; CPT-2,3= Conners’ Continuous Performance Task, versions 2 and 3; ABAS-2,3= Adaptive Behavior Assessment System, Second and Third editions; and BASC-2,3= Behavior Assessment System for Children, versions 2 and 3.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



