
Submitted:
05 August 2024
Posted:
06 August 2024
You are already at the latest version
Abstract
There is currently no effective treatment strategy for the recurrent/metastatic adenoid cystic carcinoma (R/M ACC). Furthermore, recent single-agent and combination immunotherapy trials have failed in unselected ACC cohorts unlike non-ACC salivary gland cancers. Genomic profiling revealed no actionable targets but NOTCH1 and KDM6A frameshift and CTCF splice site mutations (no MYB/L fusion) with a low TMB, MSS and negative PD-L1. We recommended anti-PD-1 plus anti-CTLA-4 combination based on TMB 2-fold greater than median TMB in ACC, tumor harboring multiple immunogenic frameshift or splice site mutations, and PD-L1 negativity. Accordingly, we achieved a complete response in a radiotherapy and chemotherapy-refractory patient with locally recurrent lacrimal gland ACC and lung metastasis following personalized immunotherapy in combination with integrative therapeutics. Therefore, it is crucial to assess not only conventional immune biomarkers but also patient-specific parameters.
Keywords:
Personalized immunotherapy
; Precision oncology
; Immune checkpoint inhibitor (ICI)
; Integrative therapies
; Adenoid cystic carcinoma (ACC)
; Frameshift mutation
; Splice site mutation
Introduction
Adenoid cystic carcinoma (ACC) is a rare type of cancer that typically originates from secretory glands, constituting 1.5-2% of all head and neck cancers [1]. The major salivary glands account for the majority of the cases, followed by minor salivary glands [1,2]. Lacrimal glands (LG) are structurally similar to the salivary glands but LG ACCs are much rarer in frequency and much poorer in prognosis [3,4]. Still, ACC at both anatomical regions share many common properties, including high rates of perineural invasion and convergent genomic profiles [4]. ACC is a biphasic tumor composed of myoepithelial and epithelial cellular components, and is divided into 3 histological patterns: cribriform and tubular (mostly low grade 1/2), and solid (generally grade 3), where the loss of myoepithelial cells is often associated with aggressive solid histology [5]. ACC usually exhibits high rates of locoregional recurrence or distant metastasis, warranting long-term surveillance. Initial treatment plan usually includes surgery and/or adjuvant radiotherapy (RT - based on surgical margin), with no effective chemotherapy (CT) regimen existing. Recurrent/metastatic (R/M) ACC patients are usually incurable, and the systemic therapies are palliative in nature. Therefore, molecularly-guided therapies are urgently needed.
Response to immune checkpoint inhibitors (ICIs) has been initially described and approved in unresectable or metastatic tumors (tissue/site agnostic) with TMB higher than 10 muts/Mb [6], and microsatellite instability-high (MSI-H) solid tumors [7]. Although previous studies reported a low TMB in the ACC [5,8], diverse single or dual immunotherapy approaches have been investigated in these patients. The objective response rates (ORR - with or without radiotherapy), however, have been scarce in unselected ACC cohorts [9]. As of recently, TMB is open to debate due to cancer type-dependent variations. Accordingly, multiple new parameters potentially affecting and/or predicting the benefit from immuno-oncology drugs have emerged, including but not limited to cancer type-dependent neoantigenic repertoire [10], clonality/subclonality of the alterations [11], mutational signatures [12,13], type of alterations [14], and functions of the mutated genes and their involvement in immune processes [15]. The efficacy of ICIs may also be improved when combined with chemotherapy, targeted therapies or agents that modify tumor microenvironment (TME). Combined inhibition of non-redundant PD-1 and CTLA-4 immune checkpoints, especially in tumors with baseline negative PD-L1 status, increases infiltration and expansion of the activated (not exhausted) effector T cells in the tumor periphery and triggers unique cellular responses compared with monotherapy [16,17]. Likewise, high-dose intravenous vitamin C (IVC) is able to facilitate immune cell infiltration in the TME, thereby augmenting the activity of the ICIs in a T cell-dependent manner with high tolerability and minimal toxicity [18,19,20,21]. Curcumin could suppress immune-related oncogenic pathways such as nuclear factor kappa B (NF-κB), and function as an adjuvant to boost immune response and immunotherapy efficacy [22]. Consequently, the response rates could be improved by a holistic approach encompassing the consideration of not only TMB, MSI or PD-L1 but also these emerging markers as well as by rational drug combinations.
In short, it is critical to perform in-depth characterization of each tumor to offer new treatment modalities thus improve patient outcomes and/or quality of life. Here we achieved a durable and complete tumor regression in an R/M ACC patient through dual immunotherapy and IVC/bioavailable oral curcumin (BOC) combination despite negative immunotherapy biomarkers. This highlights the importance of considering not only conventional markers but also patient-specific factors. Altogether, personalized immunotherapy could maximize the likelihood of treatment success.
Case Presentation
Diagnosis and Pathology: In 2012, a 39-year-old Caucasian female with no family history of cancer or inherited diseases was admitted to the hospital with swelling in the left eye and was diagnosed with left lacrimal gland ACC (solid variant/type). The patient underwent a lateral orbitotomy with a positive surgical margin. The pathological staging of the tumor was T3N0M0 (stage III – 4x3x1.5 cm). Macroscopically, the solid area was found to continue at the margins of the specimen. Microscopically, the cysts showed an invasive malignant tumor in a stroma with fibrosis and occasional myxoid changes. The tumor was composed of solid and focal cribriform nests of basaloid cells, and showed infiltration into partially preserved normal acinar structures and perineural areas (Figure 1). Immunohistochemical (IHC) staining revealed that p63 and calponin were negative in tumor cells, while ESA (EPCAM) and c-Kit (CD117) are diffusely but patchy positive. Tumor cells were stained diffusely positive for phospho-NF-κB p65 (S536), and weak-to-moderate positive for c-Kit in a separate analysis (Figure 1).
Treatment: In 2012, after lateral orbitotomy with positive surgical margin, the patient was treated with adjuvant RT (60 Gray = Gy) without CT. In 2015, a palpable growth at lower outer quadrant of the eye was observed and considered local recurrence by radiologic evaluation. She later underwent another operation that removed orbital contents, bones and adjacent contents with negative surgical margins. No adjuvant RT/CT was planned considering previous RT and complete resection. In October 2018, partial maxillectomy was performed due to maxillary recurrence detected during routine check-up. Due to the positive surgical margin, adjuvant concurrent chemoradiotherapy (CRT - 60 Gy plus cisplatin) followed by cisplatin/doxorubicin was planned. Although there was a suspected lung metastasis around this time, a mass on zygomatic bone and ocular cavity as well as multiple metastases in the lung were confirmed in February 2019. She was later admitted to our clinic for a second opinion, and we recommended a CGP test to design a personalized treatment plan. Due to post-surgery complications, the patient received adjuvant CRT starting from March 2019 through May 2019. She experienced grade 2 nausea and asthenia. The patient was later offered carboplatin plus paclitaxel considering the lung metastases, which she refused after receiving two cycles (July – August 2019). Moreover, response evaluation in August 2019 did not show a significant response at primary or metastatic sites.
CGP-guided Treatment: According to the FoundationOne® CDx (F1 CDx) CGP results (March 2019), the specimen harbors NOTCH1 D2442fs*35 (VAF: 45.6%), CTCF splice site 223+1G>A (48.8%), and KDM6A P1107fs*13 (48.2%) alterations with a TMB of 4 muts/Mb, MSS and negative PD-L1 (TPS: 0% - Dako 22C3 pharmDx™). Variants of unknown significance (VUS) include KDM5A G1116E (47.2%), MSH2 A2T (53.9%), MSH6 A36V (52.1%), MYC V280del (29.1%), and PIK3C2G Y676H (46.9%). The specimen was negative for any MYB/MYBL fusions by the CGP. Consequently, dual immunotherapy (ipilimumab 50 mg in total, nivolumab 400 mg – approved by health authorities) in combination with high-dose intravenous vitamin C (IVC - 1.5 g/kg biw on consecutive days, frequency was later reduced) and BOC (NovoCurmin by Dyna Sci – 2x2 capsules) were started in October 2019. The BOC was utilized to impair NF-κB signaling pathway, which we have successfully used in our previous ACC case based on the same rationale [23]. The IVC, on the other hand, was included to augment immunotherapy response and induce tumor-selective DNA damage. The control PET/CT scan in February 2020 showed noticeable regression of lung metastases, but the mass on zygomatic bone was still present. We interpreted this as pseudoprogression but the patient did not consent to a new biopsy, and stereotactic body radiation therapy (SBRT) was planned by an external clinic. Subsequently, she was treated with SBRT (CyberKnife® - 30 Gy). We decided to continue the immunotherapy for 3 more months by also considering the potential abscopal effect and synergy between the immunotherapy and RT. The patient complained of grade 2 asthenia and TSH levels were found to be elevated during this period. She was diagnosed with thyroiditis and later developed hypothyroidism, probably due to the immunotherapy [24]. Accordingly, thyroid hormone replacement therapy was started. Apart from this, the treatment was well-tolerated with only mild adverse events (AEs). After 3 months, a complete regression was observed in both lung parenchyma and zygoma. No tumor was observed at 1-year follow-up (Figure 2 and Figure 3). The last immunotherapy was given in December 2020, and there was no disease progression or serious AEs. The patient was tested positive for COVID-19 in March 2021. Overall, we had achieved a radiologic complete response and long-term progression-free survival (PFS) before the patient died due to COVID-19 pneumonitis at the end of April 2021.
Discussion
ACC is a rare and enigmatic cancer characterized by biological diversity and lack of biomarkers to guide targeted treatment approaches. The current standard-of-care (SOC) is surgery followed by adjuvant RT, sometimes together with CT. Of patients receiving radiotherapy, more than half will eventually develop local or distant recurrence. Single agent or combinatorial CT, on the other hand, provided minimal clinical benefit. Therefore, alternative approaches such as targeted agents and immunotherapy should be explored.
Receptor tyrosine kinase (RTK) inhibitors yielded no-to-low objective responses although a considerable proportion (~40%) of ACC tumors do harbor alterations in tyrosine kinase genes [8,25]. Therefore, targeted approaches are currently far from being solid treatment options. The frequency of somatic mutations was associated with solid histology [26]. There were frequent alterations in NOTCH genes with the majority seen in NOTCH1 [8,26]. Unlike MYB-NFIB fusions and TERT promoter alterations, NOTCH1 mutations are linked to decreased survival [8], and more common among tumors with solid histology and liver/bone metastases [8,27]. A separate study reported an ACC subtype characterized by NOTCH activating mutations (unlike LOF mutations in HNSCC) and enrichment of solid histology [5]. Furthermore, those with NOTCH1 activating mutations had even shorter overall survival (OS) compared with NOTCH1 inactivating mutations. Some NOTCH alterations could confer sensitivity to gamma secretase inhibitors (GSIs). However, our patient was not expected to benefit from GSI treatment as nonsense or frameshift mutations removing C-terminal PEST degron domain stabilize the NICD and require ligand-dependent activation or extracellular negative regulatory region (NRR) mutation for complete activation. The mutations in chromatin remodeling genes are also commonly observed in the ACC tumors [8,26]. Our patient has alterations in 3 such genes: KDM6A, KDM5A and CTCF. NOTCH1 mutations are mutually exclusive with TERT alterations, but exhibit co-occurrence pattern with KDM6A, suggesting a cooperation between them. Accordingly, KDM6A alterations lead to poor survival among ACC patients. CTCF is a transcriptional repressor of c-Myc and could result in MYC upregulation or increased activity when it has a LOF mutation, driving a more aggressive phenotype and disease course [5]. Alterations in PI3K signaling genes (a VUS in PIK3C2G) were also typically observed in tumors with a solid histology, an aggressive subset of the ACC tumors [26]. In brief, tumor mutational profile and burden of the patient was compatible with solid variant ACC, thus associated with worse prognosis.
Tumors are not isolated entities but form dynamic interactions with the surrounding stroma, endothelial cells and multiple types of immune cells, enabling alternative therapeutic approaches such as ICIs [28]. To date, a couple of markers have been utilized to predict response to and benefit from the ICIs [29,30], such as high tissue TMB (tTMB ≥10 muts/Mb) [6], MSI-H or dMMR status [31], or high PD-L1 [32]. However, there are many patients without response to immunotherapy despite the presence of these markers and those with robust responses without these markers. In line, threshold for high TMB has recently been questioned as it is challenging to determine a single, fixed cut-off in a tumor-agnostic manner. TMB failed to estimate benefit from the ICIs in many cancer types [33], and is an inadequate predictor of response to immunotherapy [34]. Previous studies have revealed a low median TMB of 0.3-2 muts/Mb [5,8], and less than 5 and 2% of all ACC cases harbor more than 10 and 20 muts/Mb, respectively [35], excluding >95% of the ACC patients from receiving immunotherapy. Recent studies and meta-analyses also challenged the value of PD-L1 expression as a predictive or prognostic biomarker and revealed that it has limited utility in various cancer types [32,36]. Furthermore, PD-L1 expression is quite uncommon or non-existent in the ACC specimens [37,38]. There is also no consensus on whether high or low PD-L1 (by which scoring parameter) or which cut-off for positive or negative staining predicts better clinical outcome, even in different studies of the same cancer type [39].
Phase 1b KEYNOTE-028 study of pembrolizumab in advanced salivary gland carcinoma (SGC) reported no ORR or durable responses in the ACC [40]. Nivolumab had a low ORR of 8.7% and a non-progressive rate of 33.3% at 6 months in NISCAHN phase 2 trial in patients with SGC [41]. A phase 2 trial of nivolumab plus ipilimumab in advanced SGC found that the combination had limited efficacy in the ACC [41,42]. However, in-depth analysis of the responding patients (2 confirmed and 1 unconfirmed PR) revealed that our patient similarly harbors more immunogenic KDM6A and NOTCH1 frameshift/truncation mutations, a potentially higher TMB (4 muts/Mb by F1 CDx – at least 2-fold higher than the median TMB) than the responding patients (25-45 muts by WES) as 306 muts by WES correspond to 8 muts/Mb by F1 CDx [43], and negative PD-L1 status. We recommended dual immunotherapy based on the idea that remodeling the TME by facilitating T cell initiation and trafficking via anti-CTLA-4 could convert the tumor to an immunologically hot state that can be later targeted by anti-PD-1. In sum, the current biomarkers used to guide immunotherapy are not sufficient for distinguishing the patients that may or may not benefit from the treatment. Therefore, an elaborate examination of all possible contributing factors should be routinely performed during clinical decision-making.
It is critical to follow a patient-centric approach to identify case-specific immune biomarkers and practice precision immunotherapy. Clonality or subclonality of the alterations present in a tumor has recently been recognized as a potential biomarker. Considering the co-occurrence pattern between the mutations in our patient and their variant allele frequency (~50%), they are likely to be clonal. While clonal neoantigens trigger T cell immunoreactivity and sensitivity to ICI, those of subclonal nature do not [33,44]. Similarly, a meta-analysis concluded that it is not quantity but quality of the mutations that determines the efficacy of immunotherapy in a cancer-type dependent manner [45]. Recent studies have also identified several gene alterations and pathways that could predict response or resistance to immune checkpoint blockade (ICB) better than TMB alone [46,47]. For instance, deleterious NOTCH alterations causing downregulation of NOTCH signaling in NSCLC or NOTCH signaling mutations in colorectal cancer (CRC) were found to be a predictive biomarker of favorable response to ICI [48,49], whereas it was elevated NOTCH signaling in small cell lung cancer [50]. In melanoma, NOTCH1 expression was shown to cause immunosuppressive tumor microenvironment while its inhibition enhanced immunotherapy efficacy [51]. Briefly, conflicting results render NOTCH1 especially unique as its role in immunotherapy should be meticulously defined on a per patient basis or at least in a cancer type-dependent manner. Similar to NOTCH1, KDM6A may serve as a favorable or unfavorable marker in metastatic urothelial carcinoma patients with TMB-H or in the general population, respectively [52,53]. Based on our patient’s outcome, we concluded that these mutations might augment immunotherapy efficacy in the ACC. Even in mismatch repair (MMR)-proficient tumors, IVC may enhance ICI efficacy by functioning as an adjuvant [18,54], which is currently tested in CRC patients in a pilot study [55]. In multiple preclinical models, vitamin C together with anti–PD-1 and anti–CTLA-4 induced apparent tumor growth inhibition or regression [18]. The IVC also induces oxidative stress and epigenetic reprogramming to cause cancer-selective DNA damage and cell death [56,57]. Similarly, curcumin may act as an immunomodulatory agent [22], impair proteasome activity [58] and induce NF-κB inhibitory events to prevent tumor growth and progression in preclinical cancer models [59]. We have previously used it in combination with imatinib and achieved a complete metabolic response in a c-Kit and phospho-NF-κB positive metastatic ACC [23], as both proteins are highly expressed and associated with disease progression in the ACC [60,61]. Bortezomib, another proteasome and NF-κB inhibiting agent, with doxorubicin provided high disease control rates in R/M ACC patients in a phase 2 trial [62]. Another important factor has lately emerged as a predictive marker is the type of alteration. Frameshift (Fs) and indel mutations carry a greater immunogenic potential as they elevate neoantigen abundance and mutant-binding specificity [63,64,65], partly stemming from high number of base and thus amino acid changes that drive changes in protein structure to expand epitope repertoire [66], unlike SNVs. In a real-world pan-cancer study, tumors with low TMB but Fs alterations had better PFS compared to those with low TMB without Fs alterations [67]. This could pave the way for development of personalized and potent cancer vaccines [68,69]. In head and neck cancer, the Fs mutations, including those in NOTCH1, were found to be enriched in the responders to anti-PD-1/PD-L1 therapies [70]. Pan-cancer splice site mutations may also generate more immunogenic peptides than missense mutations, with a positive correlation to high PD-L1 and PD-1 expression as well as to high T cell immune activity [71]. These genomic parameters could be complemented by immunophenotypic data to better discriminate between immune cold and hot tumors, thus response to the ICIs [72].
Collectively, ACC is an unpredictable and heterogeneous cancer type that exhibits high recurrence risk. Furthermore, the current status in the clinic or population-based clinical trials is zero-to-low response rates, underlying the need for personalized treatment. This necessitates tailor-made medicine with a detailed examination of each alteration and/or potential biomarker in a patient sample unlike one-size-fits-all approaches. Thus, we could gain new fronts in our fight against cancer and transform the current treatment landscape in the ACC.
Informed Consent
Written informed consent was obtained from the patient for participation, treatment and publication of her anonymized data in this scientific publication.
Data Availability Statement
All the data generated for the study are available in this article or from the corresponding author upon request.
Acknowledgments
We are grateful to the Foundation Medicine, Inc. Molecular Tumor Board (Mehlika Hazar-Rethinam, PhD and Saad A. Khan, MD) for providing insight on molecular understanding of the tumor upon our request.
Conflicts of Interest Statement and Funding
The authors declare that they have no conflict of interest. The authors did not receive any funding for the publication.
References
- Steuer CE, Hanna GJ, Viswanathan K, et al. The evolving landscape of salivary gland tumors. CA Cancer J Clin 2023; 73: 597-619. 20230725. [CrossRef]
- Li N, Xu L, Zhao H, et al. A comparison of the demographics, clinical features, and survival of patients with adenoid cystic carcinoma of major and minor salivary glands versus less common sites within the Surveillance, Epidemiology, and End Results registry. Cancer 2012; 118: 3945-3953. 20111216. [CrossRef]
- Lesueur P, Rapeaud E, De Marzi L, et al. Adenoid Cystic Carcinoma of the Lacrimal Gland: High Dose Adjuvant Proton Therapy to Improve Patients Outcomes. Front Oncol 2020; 10: 135. 20200218. [CrossRef]
- Emerick C, Mariano FV, Vargas PA, et al. Adenoid Cystic Carcinoma from the salivary and lacrimal glands and the breast: Different clinical outcomes to the same tumor. Crit Rev Oncol Hematol 2022; 179: 103792. 20220813. [CrossRef]
- Ferrarotto R, Mitani Y, McGrail DJ, et al. Proteogenomic Analysis of Salivary Adenoid Cystic Carcinomas Defines Molecular Subtypes and Identifies Therapeutic Targets. Clin Cancer Res 2021; 27: 852-864. 20201110. [CrossRef]
- Marabelle A, Fakih M, Lopez J, et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol 2020; 21: 1353-1365. 20200910. [CrossRef]
- Marcus L, Lemery SJ, Keegan P, et al. FDA Approval Summary: Pembrolizumab for the Treatment of Microsatellite Instability-High Solid Tumors. Clin Cancer Res 2019; 25: 3753-3758. 20190220. [CrossRef]
- Ho AS, Ochoa A, Jayakumaran G, et al. Genetic hallmarks of recurrent/metastatic adenoid cystic carcinoma. J Clin Invest 2019; 129: 4276-4289. [CrossRef]
- Mahmood U, Bang A, Chen YH, et al. A Randomized Phase 2 Study of Pembrolizumab With or Without Radiation in Patients With Recurrent or Metastatic Adenoid Cystic Carcinoma. Int J Radiat Oncol Biol Phys 2021; 109: 134-144. 20200808. [CrossRef]
- Schumacher TN and Schreiber RD. Neoantigens in cancer immunotherapy. Science 2015; 348: 69-74. [CrossRef]
- McGranahan N, Furness AJ, Rosenthal R, et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 2016; 351: 1463-1469. 20160303. [CrossRef]
- Chen H, Chong W, Teng C, et al. The immune response-related mutational signatures and driver genes in non-small-cell lung cancer. Cancer Sci 2019; 110: 2348-2356. 20190723. [CrossRef]
- Long J, Wang D, Wang A, et al. A mutation-based gene set predicts survival benefit after immunotherapy across multiple cancers and reveals the immune response landscape. Genome Med 2022; 14: 20. 20220224. [CrossRef]
- Chae YK, Viveiros P, Lopes G, et al. Clinical and Immunological Implications of Frameshift Mutations in Lung Cancer. J Thorac Oncol 2019; 14: 1807-1817. 20190622. [CrossRef]
- Cormedi MCV, Van Allen EM and Colli LM. Predicting immunotherapy response through genomics. Curr Opin Genet Dev 2021; 66: 1-9. 20201208. [CrossRef]
- Wei SC, Anang NAS, Sharma R, et al. Combination anti-CTLA-4 plus anti-PD-1 checkpoint blockade utilizes cellular mechanisms partially distinct from monotherapies. Proc Natl Acad Sci U S A 2019; 116: 22699-22709. 20191021. [CrossRef]
- Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N Engl J Med 2015; 373: 23-34. 20150531. [CrossRef]
- Magri A, Germano G, Lorenzato A, et al. High-dose vitamin C enhances cancer immunotherapy. Sci Transl Med 2020; 12. [CrossRef]
- Hoffer LJ, Levine M, Assouline S, et al. Phase I clinical trial of i.v. ascorbic acid in advanced malignancy. Ann Oncol 2008; 19: 1969-1974. 20080609. [CrossRef]
- Peng D, He A, He S, et al. Ascorbic acid induced TET2 enzyme activation enhances cancer immunotherapy efficacy in renal cell carcinoma. Int J Biol Sci 2022; 18: 995-1007. 20220101. [CrossRef]
- Luchtel RA, Bhagat T, Pradhan K, et al. High-dose ascorbic acid synergizes with anti-PD1 in a lymphoma mouse model. Proc Natl Acad Sci U S A 2020; 117: 1666-1677. 20200107. [CrossRef]
- Paul S and Sa G. Curcumin as an Adjuvant to Cancer Immunotherapy. Front Oncol 2021; 11: 675923. 20210816. [CrossRef]
- Demiray M, Sahinbas H, Atahan S, et al. Successful treatment of c-kit-positive metastatic Adenoid Cystic Carcinoma (ACC) with a combination of curcumin plus imatinib: A case report. Complement Ther Med 2016; 27: 108-113. 20160701. [CrossRef]
- Barroso-Sousa R, Barry WT, Garrido-Castro AC, et al. Incidence of Endocrine Dysfunction Following the Use of Different Immune Checkpoint Inhibitor Regimens: A Systematic Review and Meta-analysis. JAMA Oncol 2018; 4: 173-182. [CrossRef]
- Laurie SA, Ho AL, Fury MG, et al. Systemic therapy in the management of metastatic or locally recurrent adenoid cystic carcinoma of the salivary glands: a systematic review. Lancet Oncol 2011; 12: 815-824. 20101210. [CrossRef]
- Ho AS, Kannan K, Roy DM, et al. The mutational landscape of adenoid cystic carcinoma. Nat Genet 2013; 45: 791-798. 20130519. [CrossRef]
- Sahara S, Herzog AE and Nor JE. Systemic therapies for salivary gland adenoid cystic carcinoma. Am J Cancer Res 2021; 11: 4092-4110. 20210915.
- Valkenburg KC, de Groot AE and Pienta KJ. Targeting the tumour stroma to improve cancer therapy. Nat Rev Clin Oncol 2018; 15: 366-381. [CrossRef]
- Schlauch D, Fu X, Jones SF, et al. Tumor-Specific and Tumor-Agnostic Molecular Signatures Associated With Response to Immune Checkpoint Inhibitors. JCO Precis Oncol 2021; 5: 1625-1638. [CrossRef]
- Patel SP and Kurzrock R. PD-L1 Expression as a Predictive Biomarker in Cancer Immunotherapy. Mol Cancer Ther 2015; 14: 847-856. 20150218. [CrossRef]
- Boyiadzis MM, Kirkwood JM, Marshall JL, et al. Significance and implications of FDA approval of pembrolizumab for biomarker-defined disease. J Immunother Cancer 2018; 6: 35. 20180514. [CrossRef]
- Gandini S, Massi D and Mandala M. PD-L1 expression in cancer patients receiving anti PD-1/PD-L1 antibodies: A systematic review and meta-analysis. Crit Rev Oncol Hematol 2016; 100: 88-98. 20160210. [CrossRef]
- McGrail DJ, Pilie PG, Rashid NU, et al. High tumor mutation burden fails to predict immune checkpoint blockade response across all cancer types. Ann Oncol 2021; 32: 661-672. 20210315. [CrossRef]
- Samstein RM, Lee CH, Shoushtari AN, et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Nat Genet 2019; 51: 202-206. 20190114. [CrossRef]
- Ross JS, Gay LM, Wang K, et al. Comprehensive genomic profiles of metastatic and relapsed salivary gland carcinomas are associated with tumor type and reveal new routes to targeted therapies. Ann Oncol 2017; 28: 2539-2546. [CrossRef]
- Davis AA and Patel VG. The role of PD-L1 expression as a predictive biomarker: an analysis of all US Food and Drug Administration (FDA) approvals of immune checkpoint inhibitors. J Immunother Cancer 2019; 7: 278. 20191026. [CrossRef]
- Chen W, Fung AS, McIntyre JB, et al. Assessment Of Tumour Infiltrating Lymphocytes And Pd-l1 Expression In Adenoid Cystic Carcinoma Of The Salivary Gland. Clin Invest Med 2021; 44: E38-41. 20210321. [CrossRef]
- Sridharan V, Gjini E, Liao X, et al. Immune Profiling of Adenoid Cystic Carcinoma: PD-L2 Expression and Associations with Tumor-Infiltrating Lymphocytes. Cancer Immunol Res 2016; 4: 679-687. 20160616. [CrossRef]
- Oliva M, Spreafico A, Taberna M, et al. Immune biomarkers of response to immune-checkpoint inhibitors in head and neck squamous cell carcinoma. Ann Oncol 2019; 30: 57-67. [CrossRef]
- Cohen RB, Delord JP, Doi T, et al. Pembrolizumab for the Treatment of Advanced Salivary Gland Carcinoma: Findings of the Phase 1b KEYNOTE-028 Study. Am J Clin Oncol 2018; 41: 1083-1088. [CrossRef]
- Fayette J, Even C, Digue L, et al. NISCAHN: a phase II trial of nivolumab in patients with salivary gland carcinoma (Unicancer ORL-08). BMJ Oncol 2023; 2. [CrossRef]
- Vos JL, Burman B, Jain S, et al. Nivolumab plus ipilimumab in advanced salivary gland cancer: a phase 2 trial. Nat Med 2023; 29: 3077-3089. 20230824. [CrossRef]
- Fumet JD, Truntzer C, Yarchoan M, et al. Tumour mutational burden as a biomarker for immunotherapy: Current data and emerging concepts. Eur J Cancer 2020; 131: 40-50. 20200409. [CrossRef]
- Wolf Y, Bartok O, Patkar S, et al. UVB-Induced Tumor Heterogeneity Diminishes Immune Response in Melanoma. Cell 2019; 179: 219-235 e221. 20190912. [CrossRef]
- Litchfield K, Reading JL, Puttick C, et al. Meta-analysis of tumor- and T cell-intrinsic mechanisms of sensitization to checkpoint inhibition. Cell 2021; 184: 596-614 e514. 20210127. [CrossRef]
- Gajic ZZ, Deshpande A, Legut M, et al. Recurrent somatic mutations as predictors of immunotherapy response. Nat Commun 2022; 13: 3938. 20220708. [CrossRef]
- Martinez-Jimenez F, Priestley P, Shale C, et al. Genetic immune escape landscape in primary and metastatic cancer. Nat Genet 2023; 55: 820-831. 20230510. [CrossRef]
- Zhang K, Hong X, Song Z, et al. Identification of Deleterious NOTCH Mutation as Novel Predictor to Efficacious Immunotherapy in NSCLC. Clin Cancer Res 2020; 26: 3649-3661. 20200402. [CrossRef]
- Wang F, Long J, Li L, et al. Mutations in the notch signalling pathway are associated with enhanced anti-tumour immunity in colorectal cancer. J Cell Mol Med 2020; 24: 12176-12187. 20200914. [CrossRef]
- Roper N, Velez MJ, Chiappori A, et al. Notch signaling and efficacy of PD-1/PD-L1 blockade in relapsed small cell lung cancer. Nat Commun 2021; 12: 3880. 20210623. [CrossRef]
- Qiu H, Zmina PM, Huang AY, et al. Inhibiting Notch1 enhances immunotherapy efficacy in melanoma by preventing Notch1 dependent immune suppressive properties. Cancer Lett 2018; 434: 144-151. 20180721. [CrossRef]
- K. R. Reyes, L. Zhang, X. Zhu, et al. Association of biomarkers and outcomes in patients (pts) with metastatic urothelial carcinoma (mUC) treated with immune checkpoint inhibitors (ICIs). J Clin Oncol 2023. [CrossRef]
- T. Jindal, X. Zhu, L. Zhang, et al. Association of biomarkers and response to immune checkpoint inhibitors (ICIs) in patients with metastatic urothelial carcinoma (mUC) with high and low tumor mutation burden (TMB). J Clin Oncol 2023. [CrossRef]
- Bedhiafi T, Inchakalody VP, Fernandes Q, et al. The potential role of vitamin C in empowering cancer immunotherapy. Biomed Pharmacother 2022; 146: 112553. 20211220. [CrossRef]
- Sartore-Bianchi A, Amatu A, Nicolantonio FD, et al. High-dose vitamin C to enhance neoadjuvant immune checkpoint therapy in mismatch repair proficient colon cancer: The ALFEO pilot study. Journal of Clinical Oncology 2023. [CrossRef]
- Chen Q, Espey MG, Krishna MC, et al. Pharmacologic ascorbic acid concentrations selectively kill cancer cells: action as a pro-drug to deliver hydrogen peroxide to tissues. Proc Natl Acad Sci U S A 2005; 102: 13604-13609. 20050912. [CrossRef]
- Adibi A, Tokat UM, Ozgu E, et al. PARP inhibitor combinations with high-dose vitamin C in the treatment of Ewing sarcoma: two case reports and mechanistic overview. Ther Adv Med Oncol 2023; 15: 17588359231213841. 20231215. [CrossRef]
- Banerjee S, Ji C, Mayfield JE, et al. Ancient drug curcumin impedes 26S proteasome activity by direct inhibition of dual-specificity tyrosine-regulated kinase 2. Proc Natl Acad Sci U S A 2018; 115: 8155-8160. 20180709. [CrossRef]
- Sun ZJ, Chen G, Zhang W, et al. Curcumin dually inhibits both mammalian target of rapamycin and nuclear factor-kappaB pathways through a crossed phosphatidylinositol 3-kinase/Akt/IkappaB kinase complex signaling axis in adenoid cystic carcinoma. Mol Pharmacol 2011; 79: 106-118. 20101019. [CrossRef]
- Sun ZJ, Chen G, Hu X, et al. Activation of PI3K/Akt/IKK-alpha/NF-kappaB signaling pathway is required for the apoptosis-evasion in human salivary adenoid cystic carcinoma: its inhibition by quercetin. Apoptosis 2010; 15: 850-863. [CrossRef]
- Phuchareon J, van Zante A, Overdevest JB, et al. c-Kit Expression is Rate-Limiting for Stem Cell Factor-Mediated Disease Progression in Adenoid Cystic Carcinoma of the Salivary Glands. Transl Oncol 2014; 7: 537-545. 20141024. [CrossRef]
- Argiris A, Ghebremichael M, Burtness B, et al. A phase 2 trial of bortezomib followed by the addition of doxorubicin at progression in patients with recurrent or metastatic adenoid cystic carcinoma of the head and neck: a trial of the Eastern Cooperative Oncology Group (E1303). Cancer 2011; 117: 3374-3382. 20110118. [CrossRef]
- Turajlic S, Litchfield K, Xu H, et al. Insertion-and-deletion-derived tumour-specific neoantigens and the immunogenic phenotype: a pan-cancer analysis. Lancet Oncol 2017; 18: 1009-1021. 20170707. [CrossRef]
- Schwitalle Y, Kloor M, Eiermann S, et al. Immune response against frameshift-induced neopeptides in HNPCC patients and healthy HNPCC mutation carriers. Gastroenterology 2008; 134: 988-997. 20080111. [CrossRef]
- Ballhausen A, Przybilla MJ, Jendrusch M, et al. The shared frameshift mutation landscape of microsatellite-unstable cancers suggests immunoediting during tumor evolution. Nat Commun 2020; 11: 4740. 20200921. [CrossRef]
- Roudko V, Bozkus CC, Orfanelli T, et al. Shared Immunogenic Poly-Epitope Frameshift Mutations in Microsatellite Unstable Tumors. Cell 2020; 183: 1634-1649 e1617. 20201130. [CrossRef]
- Florou V, Floudas CS, Maoz A, et al. Real-world pan-cancer landscape of frameshift mutations and their role in predicting responses to immune checkpoint inhibitors in cancers with low tumor mutational burden. J Immunother Cancer 2023; 11. [CrossRef]
- Lou Y, Asmann Y, Thomas M, et al. Integrating INDEL Mutations into Neoantigen Prediction in Lung Cancer: Developing Personalized Cancer Vaccines. J Thorac Oncol 2017; 12: 1814-1815. [CrossRef]
- Gebert J, Gelincik O, Oezcan-Wahlbrink M, et al. Recurrent Frameshift Neoantigen Vaccine Elicits Protective Immunity With Reduced Tumor Burden and Improved Overall Survival in a Lynch Syndrome Mouse Model. Gastroenterology 2021; 161: 1288-1302 e1213. 20210702. [CrossRef]
- Hanna GJ, Lizotte P, Cavanaugh M, et al. Frameshift events predict anti-PD-1/L1 response in head and neck cancer. JCI Insight 2018; 3 20180222. [CrossRef]
- Jayasinghe RG, Cao S, Gao Q, et al. Systematic Analysis of Splice-Site-Creating Mutations in Cancer. Cell Rep 2018; 23: 270-281 e273. [CrossRef]
- Maleki Vareki S. High and low mutational burden tumors versus immunologically hot and cold tumors and response to immune checkpoint inhibitors. J Immunother Cancer 2018; 6: 157. 20181227. [CrossRef]
Figure 1.
The photomicrograph shows an adenoid cystic carcinoma specimen. There are solid and focal cribriform nests of basaloid cells (Hematoxylin-eosin staining, A - ×100, B - ×400). Immunohistochemistry showing a positive NF-κB p65 p-S536 staining (ab86299 at 1/200 - 1 g/ml, detected by DAB, C - ×40 and D - ×400). IHC showing weak-to-moderate focal positive c-Kit (CD117) staining (E - x200 and F - x400).
Figure 1.
The photomicrograph shows an adenoid cystic carcinoma specimen. There are solid and focal cribriform nests of basaloid cells (Hematoxylin-eosin staining, A - ×100, B - ×400). Immunohistochemistry showing a positive NF-κB p65 p-S536 staining (ab86299 at 1/200 - 1 g/ml, detected by DAB, C - ×40 and D - ×400). IHC showing weak-to-moderate focal positive c-Kit (CD117) staining (E - x200 and F - x400).
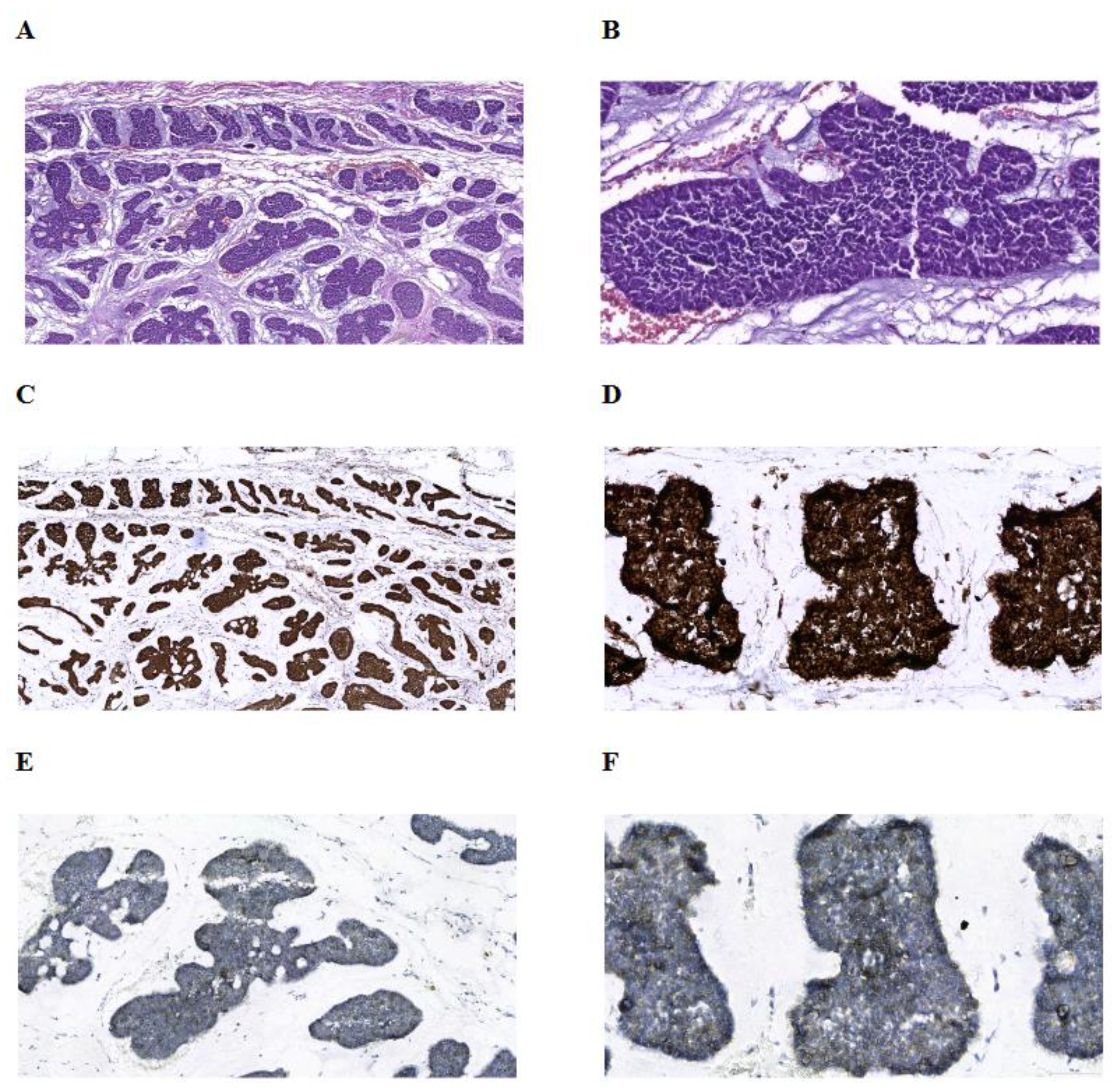
Figure 2.
Timeline of disease status and treatment (A). CT images showing the presence and absence of lung nodules before and after the treatment (August 2019: B, D, F, H – August 2020: C, E, G, I).
Figure 2.
Timeline of disease status and treatment (A). CT images showing the presence and absence of lung nodules before and after the treatment (August 2019: B, D, F, H – August 2020: C, E, G, I).
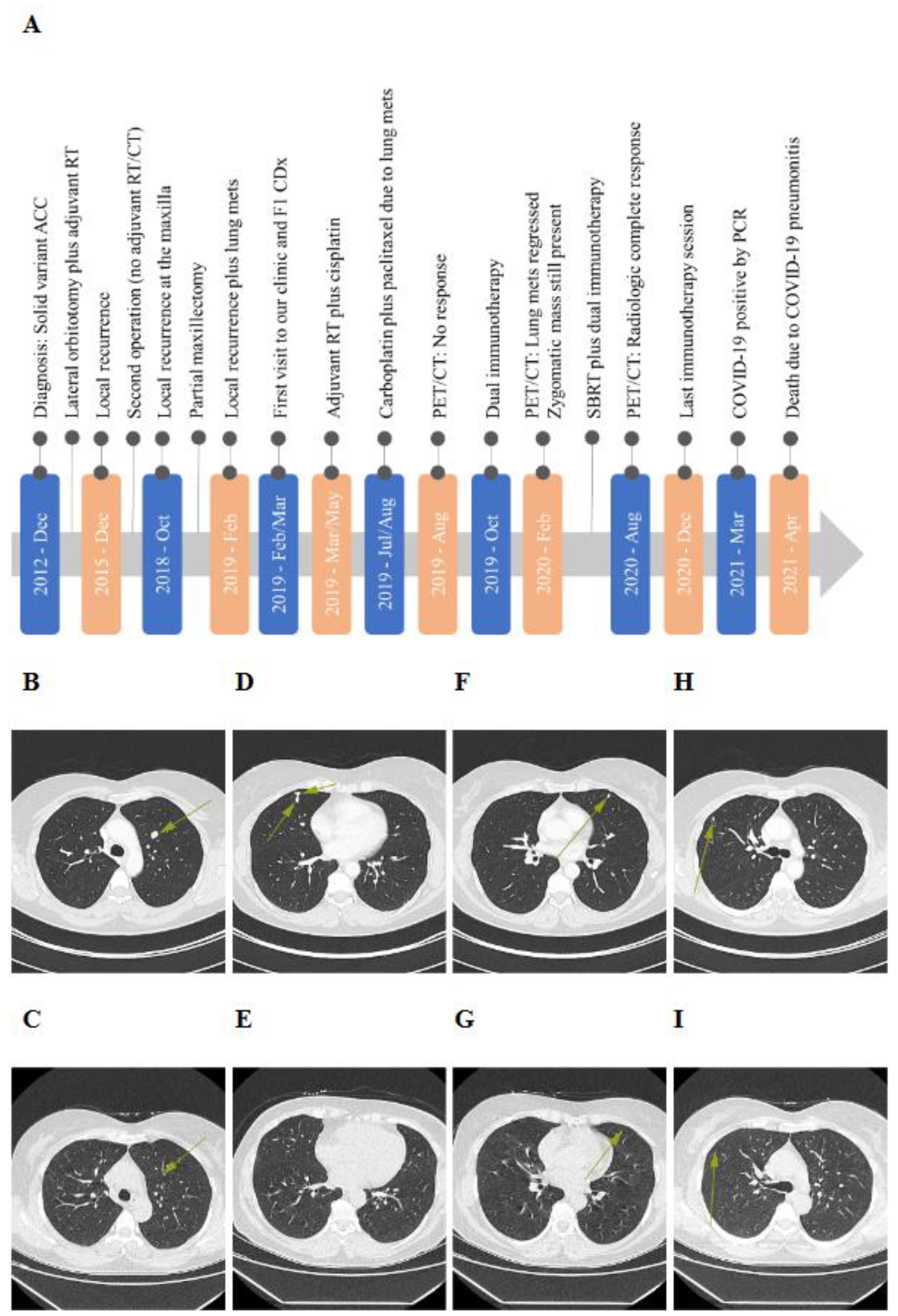
Figure 3.
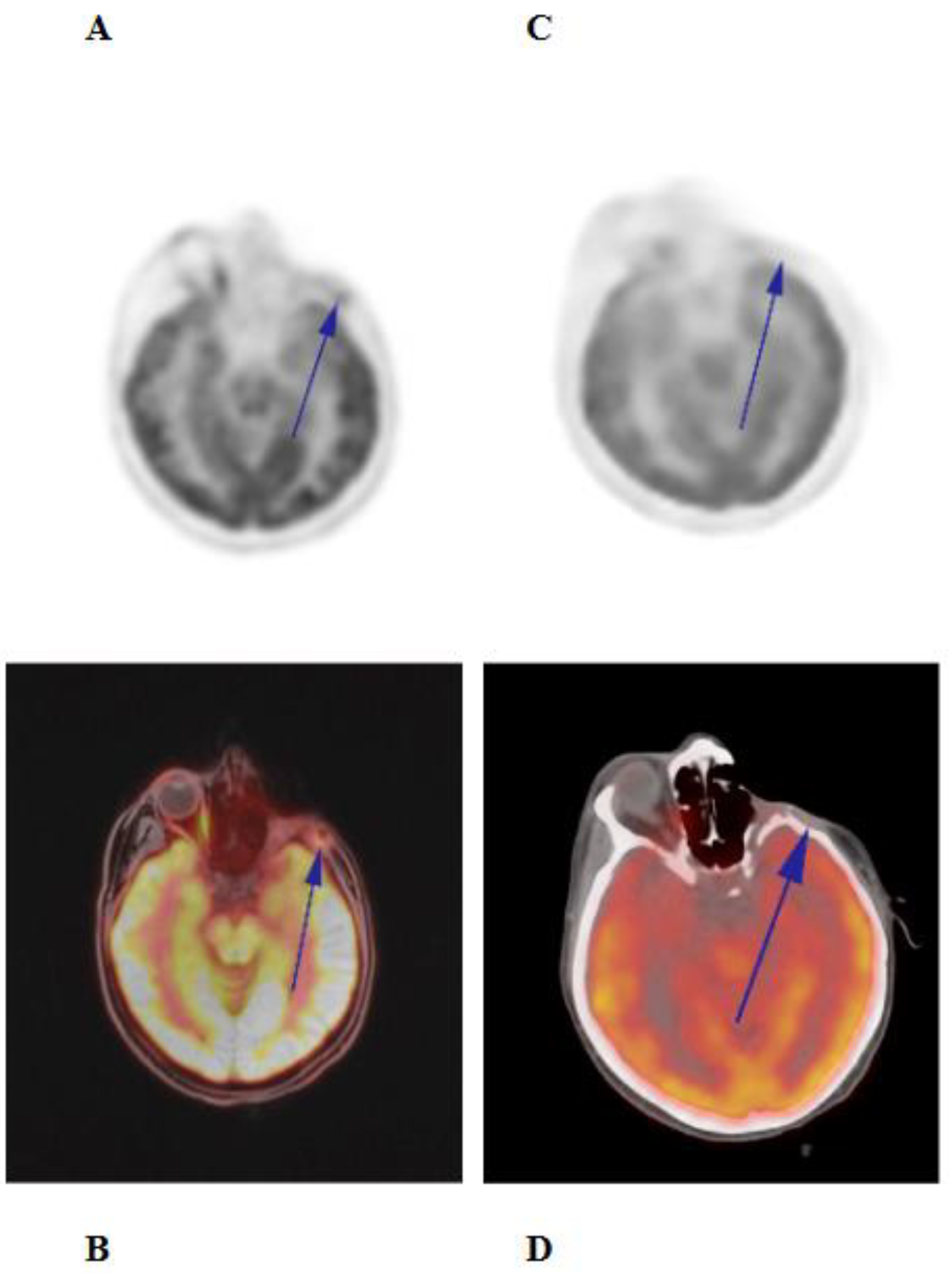
The PET/CT images showing marked tumor regression (A, C) and showing no pathologic FDG uptake (B, D) following the treatment.
Figure 3.
The PET/CT images showing marked tumor regression (A, C) and showing no pathologic FDG uptake (B, D) following the treatment.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



