
Submitted:
06 August 2024
Posted:
07 August 2024
You are already at the latest version
Abstract
A Tamoxifen (TAM) response varies significantly among individuals due to genetic variations in cytochrome P450 2D6 (CYP2D6), as well as other TAM pharmacokinetic and/or pharmacodynamic proteins. In this study, 40 ER+ breast cancer patients who received at least 6 months of TAM treatment were prospectively recruited. The study aimed to evaluate, using HPLC-MS/MS, plasma concentrations of TAM and its metabolites, and to study the association with genetic polymorphisms (CYP2D6*4, CYP3A4*1B, CYP3A5*3, UGT2B7*2, UGT2B15*2, SULT1A1*2, and ESR1V364E) and adverse reactions. Bivariable linear regression analyses showed that CYP3A4*1/*1B is significantly associated with an increase of 4-hydroxyTAM plasmatic concentration, a decrease of endoxifen/4-hydroxyTAM ratio and the elimination of 17β estradiol. It was found that the CYP3A4*1/1B genotype alone could explain part of the variability in [4OHTAM], [endoxifen]/[4OHTAM], and 17β-estradiol plasma levels. Similarly, SULT1A1*1/*2 genotype affects the [endoxifen]/[4OHTAM] plasma ratio. Multivariable predictive models, incorporating both polymorphisms and non-genetic variables, are proposed to explain [NdesMeTAM]/[TAM], [4OHTAM]/[TAM], [endoxifen]/[NdesMeTAM], [endoxifen]/[4OHTAM], and 17β-estradiol plasma levels, as well as for predicting hot flashes and cramps. This preliminary study suggests that the genetic variants studied may influence the bioactivation and elimination of TAM, the clinically observed adverse reactions, and potentially the treatment efficacy.
Keywords:
breast cancer
; pharmacokinetics
; pharmacodynamics
; polymorphism
; RAM
; recurrence
; tamoxifen
1. Introduction
Breast cancer (BC) is the second leading cause of cancer death in women, driven by multiple factors [1,2]. Approximately 75% of breast tumor cells express the estrogen receptor (ER), and estrogen promotes cell growth by inducing factors like TGF-α, IGF, and EGF, while inhibiting the antiproliferative factor TGF-β [1,2]. This leads to cell proliferation and reduced apoptosis, facilitating tumor growth. ER-positive patients are treated with hormone therapy in addition to surgery, chemotherapy, and/or radiation therapy [4,5]. Hormone therapy involves blocking estrogen's effects using selective estrogen receptor modulators (SERMs) like tamoxifen (TAM, Nolvadex®). TAM acts as an estrogen antagonist in breast tissue but as an agonist in the endometrium [6,7]. It remains the preferred adjuvant endocrine therapy, increasing disease-free survival in pre- and post-menopausal women and reducing BC mortality by 34%. However, patient response to tamoxifen varies, and it can cause side effects [8,9].
ER has two subtypes, ERα and Erβ, and are made up of six regions (A-F). The constitutively active transcriptional function (AF-1) is contained in the A/B region. The DNA-binding domain (DBD) is contained in the C/D region. Finally, both, the estrogen-induced transcriptional activation function (AF-2) and the ligand-binding domain (LBD) are contained in the E/F region. Thus, the ER has two different transcriptional activation functions, the domain AF-1 independent of the presence of estrogen and the domain AF-2 dependent on estrogen [10].
In the absence of estrogen, the ER is associated with a large complex of heat shock protein in the nucleus or cytoplasm. In the presence of estrogen, it diffuses into the cell and binds to ER, this binding causes a conformational change in the receptor. ER binds to estrogen and a cascade of events begins in which it binds to regulatory regions of target genes and activates the transcription of specific genes. Through its DBD, ER can interact with certain estrogen response elements (EREs) of target genes or interact with DNA indirectly, through proteins such as AP1 or Runx1. Therefore, it can modify the chromatin structure and/or the general activity of the transcriptional apparatus because is a nucleation point for transcriptional co-regulators. Several proteins (>300) interact with members of the nuclear receptor superfamily, and also with ER. Therefore, after three decades it is difficult to determine the real effect of TAM [10,11].
TAM inhibits the function of the AF-2 domain of the estrogen receptor (ER). Consequently, it acts as an antagonist of estrogens in various cellular contexts, particularly affecting genes that rely solely on AF-2. This mechanism leads to decreased levels of insulin-like growth factor 1 (IGF-1), a factor that promotes tumor cell proliferation and triggers the release of transforming growth factor beta (TGF-β) [12,13,14].
CYP2D6, CYP3A4, and CYP3A5 are cytochrome P450 enzymes primarily expressed in the liver, essential for metabolizing tamoxifen (TAM) into its active form, endoxifen (4-hydroxy-N-desmethyltamoxifen), and less active metabolites like N-desmethyltamoxifen (N-desmethyl-TAM) and 4-hydroxy tamoxifen (4-hydroxyTAM). SULT (families 1, 2, 4) and UGT (families 1 and 2) are phase II detoxification enzymes that process TAM metabolites for elimination. SULT1A1, a sulfotransferase mainly in the liver, aids in sulfating TAM metabolites to facilitate excretion. UGT2B7 and UGT2B15, both UDP-glucuronosyltransferases, glucuronidate hydroxylated TAM metabolites, enhancing solubility and excretion. ESR1, the estrogen receptor in breast tissue, is TAM’s primary target, acting as a modulator to exert therapeutic effects. These proteins are crucial to TAM's metabolic pathway and its efficacy as a breast cancer treatment (Figure 1). In the liver, TAM biotransformation occurs in two phases. Phase I generates N-desmethyl-TAM, 4-hydroxyTAM, and endoxifen through different pathways. While N-desmethylTAM and endoxifen are the most abundant plasma metabolites, endoxifen and 4-hydroxyTAM are the most active, with a higher affinity for estrogen receptors and 30 to 100 times greater activity than TAM or N-desmethyl-TAM (15-17). In vitro studies show these metabolites effectively reduce cell proliferation. Due to its extended half-life, TAM reaches steady-state concentrations after four weeks, while N-desmethyl-TAM does so after eight weeks [18,19,20,21,22].
Patient response to TAM varies depending on factors such as age, histological type of the breast tumor, cellular differentiation, and menopausal status. In advanced disease, TAM demonstrates an overall response rate of approximately 30% in unselected patients, rising to 75% in patients with estrogen receptor-positive (ER+) and progesterone receptor-positive (PR+) tumors. As adjuvant therapy, TAM reduces the risk of recurrence by 25% and mortality by 17%. The greatest benefits are observed in patients aged over 50 with positive hormone receptors. Furthermore, the incidence of ipsilateral BC decreases by 50% in patients undergoing a five-year treatment course [8,21,22].
On the other hand, the long-term safety of TAM is well elucidated. Incidence of endometrial cancer and thromboembolic events have been observed [22,23,24].
Despite the various studies carried out in TAM, after 3 decades, there are still differences in the treatment response presented by patients that have not been explained. Although it is known that drug’s response is multifactorial, associated to the interaction of genetic, physiological, and environmental factors it is also known that the presence of genetic variations in the biotransformation enzymes could explain their efficacy and safety [25,26,27]. Certain genetic variations can influence the metabolism and effects of tamoxifen. The CYP2D6*4 allele (rs3892097) is a non-functional variant that, when homozygous, leads to a poor metabolizer phenotype, linked to reduced tamoxifen side effects and lower serum levels of its metabolites. The CYP3A4*1B allele (rs2740574) is associated with increased gene expression and a higher risk of endometrial cancer in BC patients treated with tamoxifen. The CYP3A5*3 allele (rs776746) results in a less active enzyme and correlates with tumor characteristics in postmenopausal BC patients on tamoxifen. Variants in CYP2C9*2 and *3 (rs17999853 and rs1057910) cause a slight reduction in tamoxifen metabolites. The SULT1A1*2 allele, a non-synonymous single-nucleotide polymorphism (SNP) (rs9282861; G638A; Arg213His), is linked to lower enzymatic activity, thermal stability, and an increased risk of recurrence in tamoxifen-treated BC patients, though its effect on tamoxifen metabolite levels is unclear. The UGT2B7*2 (rs7439366), a non-synonymous exonic genetic variant, leads to the substitution of histidine to tyrosine in codon 268 and is the most common functional genetic variant on UGT2B7 gene with reported influence on drug response, although it encodes for an enzyme with higher activity, has not been associated with BC patients under treatment with TAM and/or disease recurrence. The UGT2B15*2 allele (rs1902023), which results in a single G>T substitution, causing an amino acid change at position 85 from aspartic acid to tyrosine, is associated with decreased enzyme activity and a reduced risk of BC recurrence. BC patients with these enzyme mutations have a lower recurrence risk and a significantly reduced survival time [27,28,29,30,31,32,33,34,35,36].
On the other hand, several mutations in the ESR1 gene have been reported [37], though their impact on the efficacy and safety of tamoxifen (TAM) treatment remains unclear. Using SIFT and PolyPhen it was predicted that the SNP ESR1 V364E (rs121913044, 1461T>A) causes a deleterious change affecting the receptor [38]. This mutation is located at the N-terminus of the hormone-binding domain, expressed at lower levels, and has 40 times lower affinity for estrogen. Despite this, it shows higher transcriptional activity and acts as a potent negative dominant at 10-8 M estrogen. The ESR1 V364E mutation maintains its negative dominant activity, relying on estrogen for ERE binding, and when co-present with wild-type ER, it represses ER-mediated transcription even without DNA binding [39,40,41].
In recent years, differences in the responses to TAM-treatment in BC-patients have been associated with genetic variants in the biotransformation enzymes. However, there are still controversies to determine which enzymes and/or which genetic variants could explain the response to treatment with TAM [42,43,44,45]. In order to contribute to solving these controversies, we aim to associate TAM treatment with BC results, in survival terms and adverse reactions (ADRs-thickening of the endometrium, vaginal hemorrhage, headache, hot flush and cramps), with genetic variants in TAM-biotransformation genes (CYP2D6*4, CYP3A4*1B, CYP3A5*3, SULT1A1*2, UGT2B7*2, UGT2B15*2) and, ESR1 V364E, in patients with hormone-dependent BC, by generating predictive models for TAM response, according to their genetic-metabolic characteristics.
2. Materials and Methods
2.1. Patients
Forty (40) patients with BC histologically confirmed, >18 years old, without chronic unbalanced or systemic pathology or other active cancers with 6 months of TAM treatment, were enrolled prospectively for a Pharmacokinetic-Pharmacogenetic association study. The enrollment was carried out from August 2014 to January 2015 at the Polyclinic of Oncology of the National Cancer Institute. All the patients signed a written consent and an agreement to be included in this study.
The appropriate treatment of patients was scheduled according to Breast Cancer Clinical Guideline, 2nd Ed (2015), Santiago, Chile. The selection criteria were as follows:
Inclusion criteria:
- a)
- Patients with histologically confirmed breast cancer (BC) from the oncology department of the INC,
- b)
- Age >18 years,
- c)
- ER+, PR+, and HER2- status,
- d)
- Cancer stages I-III,
- e)
- No treatment with aromatase inhibitors, LHRH agonists, or concomitant treatments such as antivitamin K drugs, antidepressants, mitomycin, ritonavir, primidone, fluorouracil, methotrexate, and cyclophosphamide to avoid their influence on recurrence and ADRs profile of TAM.
- f)
- At least 24 months of TAM treatment to assess response (recurrence and ADRs).
Exclusion criteria:
- a)
- Patients who declined to donate samples for TAM metabolite HPLC assays,
- b)
- Patients without complete clinical records,
- c)
- Patients with chronic unbalanced systemic pathology or other active cancers,
Events (recurrence and ADRs) were evaluated after 6 months of TAM treatment. The treatment regimen consisted of surgery followed by radiotherapy and/or chemotherapy.
2.2. Genotyping Analysis
Using the NCBI dbSNP database (https://www.ncbi.nlm.nih.gov/snp/), the SNPinfo Web Server (https://snpinfo.niehs.nih.gov), and Ensembl genome database project (https://www.ensembl.org/index.html), the functional relevant SNPs were obtained. The selection was based on the level of evidence for each SNP and allele frequency.
We obtained either, peripheral blood or buccal mucosa cells, to extract genomic DNA using Genomic DNA Extraction Blood DNA Kit FavorPrep® (Catalog number FABGK 001-1, Favorgen®, Biotech Corp, Headquarters, Taiwan, China) and MasterAmp™ Buccal Swab Kit (Catalog number: MB71030 Epicentre®, an Illumina company, Madison, USA), respectively. SNPs for CYP450 genes (CYP2D6*4 (rs3892097), CYP3A4*1B (rs2740574), CYP3A5*3 (rs776746)), phase II genes (SULT1A1*2 (rs9282861), UGT2B7*2 (rs7439366), UGT2B15*2 (rs1902023)) and ESR1 V364E (rs121913044) were genotyped using polymerase chain reaction and restriction fragment length polymorphism analysis (PCR-RFLP). The presence of fragment products was observed in a 2% agarose gel (Catalog number: 161-3109, Bio-Rad Laboratories, Hercules, CA, USA) or 18% polyacrylamide gel depending on the fragment lengths and revealed with GelRed® 10000X DMSO (Catalog number: SCT122, Sigma-Aldrich Co, St. Luis, Missouri, USA) (Figure 2). Table A1 shows primer sequences and restriction enzymes used for genotyping. For Quality Assurance purposes we randomly choose 20% of the samples for a) repetition of the analysis and b) TaqMan® RT-PCR analysis for coincidence. When analyses were not coincident, we excluded the samples.
2.3. HPLC-MS/MS Analyses
After 3 months of treatment, steady-state plasma concentrations of TAM, N-desmethyl-TAM, 4-hydroxyTAM, and endoxifen were quantified by High-Performance Liquid Chromatography, coupled to mass-mass spectrometry (HPLC-MS/MS, AB SCIEX API 4000, USA) based on the method described by Binkhorst et al [46]. This method was validated and defined with respect to sensitivity, accuracy, precision, recovery, linearity, reproducibility following FDA guidelines. Tamoxifen-deuterated (Catalog number: TRC-T006007, Toronto Research Chemicals Inc., Canada) was used as internal standard. The linearity range was established using lower and upper limit values and limit of quantification described previously. A blank (matrix without internal standard) and a zero (matrix with internal standard) were included [47,48,49].
2.4. Statistical Analyses
GraphPad Prism 9.0 and STATA 11.1 were used for statistical analyses, considering p<0.05 as statistically significant. Mean ± standard deviation (SD), number, percentage, or frequency where appropriate were used. To determine quantitative variable distributions the Shapiro-Wilk test was used.
To compare mean values between groups the F-test in unpaired t-test with Welch's correction was used. The three groups were compared with Welch's ANOVA test in Brown-Forsythe (p>0.05 were parametric and p<0.05 were non-parametric distributions). To investigate differences in genotypic and allelic frequencies between the groups, unpaired t-test for parametric data, Mann-Whitney test for non-parametric data, Ordinary one-way ANOVA for parametric data, or Kruskal-Wallis´s test non-parametric data was used. For the associations between plasma concentrations of TAM, N-desmethyl-TAM, 4-hydroxy-TAM, and endoxifen, and ratios [NdesMeTAM]/[TAM], [4OHTAM]/[TAM], [Endoxifen]/[NdesMeTAM], and [Endoxifen]/[4OHTAM] and 17β estradiol, in relation to CYP2D6*4 (rs3892097), CYP3A4*1B (rs2740574), CYP3A5*3 (rs776746), SULT1A1*2 (rs9282861), UGT2B7*2 (rs7439366), UGT2B15*2 (rs1902023), and ESR1 V364E (rs121913044) polymorphisms of patients bivariable linear regression was used. Bivariable and multivariable logistic regression analyses were conducted to investigate the associations between genotypes, TAM metabolite concentrations and ratios, ADRs (endometrial cancer, endometrial hyperplasia, vaginal bleeding, phlebitis, headache, nausea, hot flash, cramps, bone pain and urticaria), demographic aspects, gynecological and pathological features. To achieve this, concentration ratios were transformed into discrete variables.
All association studies were conducted by selecting parameters with the best statistical association for each analysis. Inheritance models were used to determine associations between plasma levels and polymorphisms, including co-dominant (wild type vs. heterozygote vs. variant), dominant (wild type vs. heterozygote/variant), and recessive (wild type/heterozygote vs. variant) models. To evaluate associations, we calculate odds ratio (OR) and regression coefficients to logistic and linear regression models, respectively. In both cases, accuracy was evaluated through 95% confidence intervals. The multivariable models were adjusted step by step, using both forward and backward strategies, incorporating those variables that had a p value less than 0.1 in the bivariable analysis. Thus, multivariable models contain only the most relevant variables according to this procedure. To get values of variables which resulted as eliminated the dataset of this study is provided (https://github.com/Luisquinones56/BreastCaCQF.git).
3. Results
3.1. Genetics and Not Genetics Characteristics of Patients
3.2. The Therapeutic Response Characteristics of the Patients
Recurrence was found in 1 patient (2.5%). The most severely observed ADRs among patients were endometrial hyperplasia (7.5%) and vaginal bleeding (5%), and the most frequent were hot flashes (65%), bone pain (20%), and cramps (17.5%) (Table 3).
3.3. Association between Steady-State Plasma Concentration of Metabolites and Polymorphisms
After bivariable linear regression analyses between polymorphic variants and plasma concentration and/or ratios at steady state, we found that CYP3A4*1B variant allele was associated with [4OHTAM] (p=0.002), [endoxifen]/[4OHTAM] (p=0.041) and 17β estradiol plasma levels (p=0.003). No other statistically significant association between plasma concentration at steady state for either Tamoxifen, N-desmethyl-TAM, 4-hydroxy-TAM, endoxifen or 17β estradiol and CYP2D6*4, CYP3A5*3, SULT1A1*2, UGT2B7*2, UGT2B15*2 and ESR1 V364E were found (Figure 3 y Figure 4, Table 4 and Table A2).
Additionally, for bivariable logistic regression analyses, patients with [NdesMeTAM]/[TAM], [4OHTAM]/[TAM], [Endoxifen]/[NdesMeTAM], [Endoxifen]/[4OHTAM], and 17β-Estradiol we categorized plasma concentrations, levels greater than or equal to the average were classified as cases, while those with levels below the average were classified as controls (Table 5, and Tables A3-A5). In these analyses [endoxifen]/[4OHTAM] ratio was negatively associated with genotype *1/*2 of SULT1A1*2 in the codominant model of inheritance (ORc=0.14; p= 0.041; CI 95% 0.02-0.92) and ESR1 V364E in the dominant model of inheritance was near to significance (ORc= 0.25, p= 0.053, CI 95% 0.06-1.01). [4OHTAM]/[TAM] ratio was also negatively related to UGT2B7*2/*2, but this relationship was only near to significancy (ORc=0.09, p=0.068, CI 95% 0.007-1.18) like the relationship between 17β estradiol levels and UGT2B7*, in the recessive model of inheritance (ORc= 0.12, p=0.071; CI 95% 0.01-1.21).
As previously stated, following the bivariate analyses, the multivariable logistic regression models (encompassing both genetic and non-genetic variables) were incrementally refined using both forward and backward selection strategies. Consequently, we derived significant multivariable models for [NdesMeTAM]/[TAM] (p=0.03; Pseudo R2=0.3308), [4OHTAM]/[TAM] (p=0.03; Pseudo R2=0.4892), [endoxifen]/[NdesMeTAM] (p=0.0002; Pseudo R2=0.7603), [endoxifen]/[4OHTAM] (p=0.0190; Pseudo R2=0.4367), and 17βEstradiol (p=0.00209; Pseudo R2=0.5414) (Table 6, Table 7, Table 8, Table 9 and Table 10).
3.4. Association between Polymorphisms, Recurrence and Adverse Drug Reactions (ADRs) in Patients and Steady-State Plasma Concentration of Metabolites
No statistically significant associations were found in the bivariable logistic regression model analysis of recurrence and ADRs (endometrial cancer, endometrial hyperplasia, vaginal bleeding, phlebitis, headache, nausea, hot flash, cramps, bone pain, and urticaria), and concentration ratios of TAM, N-desmethyl-TAM, 4OHTAM and endoxifen, respectively, and 17β estradiol (Tables A4–A9). Conversely, after performed stepwise forward and backward procedure for multivariable logistic regression analyses, including ADRs, genetic, non-genetic variable and metabolite concentrations, we obtained significant models for hot flash (p = 0.0302; Pseudo R2 = 0.3323) (Table 11) and cramps (p = 0.0206; Pseudo R2 = 0.4168) (Table 12).
4. Discussion
Differences in response to tamoxifen in BC patients has been investigated by decades. The current response rate varies from 25% to 50% in patients and the adverse effects are also very variable [8,23,24,45]. This could be explained because TAM is a prodrug bioactivated in the liver by CYP to its metabolites, which are subsequently conjugated to facilitate their elimination by enzymes phase II (UGT and SULT), both processes being variables due to the presence of several genetic polymorphisms. The level of expression, in the liver, intestine, and other tissues that present these enzymes has great variability, leading to different levels of metabolites among patients [50,51].
CYP2D6 is recommended as a pharmacogenetic biomarker for this drug by the FDA (https://www.fda.gov/media/124784/download) and CPIC (https://cpicpgx.org/guidelines/cpic-guideline-for-tamoxifen-based-on-cyp2d6-genotype/), because 10 to 20% of the variability could be explained by genetic variations in this gene. However, studies have shown conflicting results, and there is still no consensus on the clinical utility of genetic variations as predictors of tamoxifen response in BC patients [42,43]. Consequently, to develop a potential predictive model that can estimate patient response based on their genetic and metabolic characteristics, researchers assessed the correlation between BC treatment outcomes with tamoxifen, specifically in terms of response (recurrence) and adverse drug reactions (ADRs), by investigating seven genetic variants in genes that encode proteins involved in the pharmacokinetics and pharmacodynamics of tamoxifen in women with hormone-sensitive BC undergoing adjuvant tamoxifen treatment.
In our study, average concentrations of TAM and its metabolites in steady-state were found similar to those found by other authors [47,48,49,50,51]. Using bivariable linear regression analyses t was found that the CYP3A4*1/*1B could explain the variability of [4OHTAM], [endoxifen]/[4OHTAM] and 17β estradiol plasma levels (Table 4). Therefore, because CYP3A4 is responsible for the metabolism of tamoxifen into its primary metabolites, including N-desmethyltamoxifen and 4-hydroxytamoxifen, the presence of a mutant allele modifies the biotransformation of 4-hydroxyTAM to endoxifen, The CYP3A4*1B allele causes variable expression of the gene, affecting the concentration of the enzyme without affecting the enzymatic activity [50]. These results correlate with Johänning et al., where CYP3A4 gene expression is upregulated in 4OHTAM treatment, and in normal conditions, CYP3A4 metabolizes the analyte efficiently [52]. Although these results contrast with those obtained by [33], where no association between CYP3A4 and these metabolites was found.
The SULT1A1*2 variant is associated with reduced enzyme activity, which can lead to decreased elimination and higher levels of active tamoxifen metabolites in the body. This accumulation can enhance the drug's efficacy but also heighten the risk of adverse effects, including hot flashes, endometrial hyperplasia, and other estrogenic side effects. In the bivariate logistic regression analyses, categorized plasma concentrations revealed that the SULT1A1*1/*2 genotype was significantly and negatively associated with the [Endoxifen]/[4OHTAM] ratio. This indicates that the presence of this genetic variant in one allele is sufficient to reduce the ratio, suggesting that the enzyme's low activity increases plasma levels of [4OHTAM], thereby decreasing the ratio (Figure 1). This correlates with the fact that this genetic variant is associated with lower enzymatic activity and the accumulation or elevation of 4-hydroxyTAM concentrations, as supported by the findings documented in our study, compared to the wild-type allele [34,53]. These results correlate with the study of Rebbeck et al. [54], who found that women with the SULT1A1*2 presented late menopause. However, these differ from those found by Gjerde et al [30], in a similar study, but they used the age-adjusted logistic regression model, thus they found that genetic variants of SULT1A1 gene modify the plasma concentration ratio NdesmethylTAM/TAM. In the present study, because of the low number of occurrences in some sub-groups, the analyses showed associations with no statistical significance with several metabolites. In this respect a potential association is observed among SULT1A1*1/*2 and 17β estradiol plasma levels, but it was not significant (Figure 4). The results may be clarified by increasing the sample size in future studies. Anyway, it is also possible that the variant explains a small part of the response, which can be also elucidated with a higher number of samples.
UGT2B7*2 and UGT2B15*2 variants encode enzymes with higher and lower activity, respectively, characterized by changes in Km and Vmax compared to the wild-type enzyme [36,55]. UGT2B7*2 variant can reduce the clearance of endoxifen leading to higher systemic levels, increasing the risk of adverse reactions such as thromboembolic events and endometrial changes. In the bivariate linear or logistic analyses, no significant associations with TAM metabolites were identified (Figure 4). However, it is noteworthy that the UGT2B7*2/*2 genotype showed near-significant associations with the [4OHTAM]/[TAM] ratio and 17β-estradiol concentrations in the codominant and recessive models, respectively (Table 5). These results could potentially reach significance with a larger sample size. These results correlate with Romero-Lorca et al (2015), who found significant differences in the activity of UGT2B7. In this study, the activity of the enzyme was reduced in individuals when they were analyzed in separated or grouped genotypes [56]. Analysis in cell cultures found similar results, where the expression of UGT2B7 and the levels of proteins decreased in patients carrying mutations [57].
On the other hand, bivariate logistic analysis indicated that the estrogen receptor ESR1 V364E variant might be inversely related to the endoxifen/4OHTAM ratio, although it did not reach statistical significance (OR=0.25, p=0.053). No studies have been reported about this relationship. This lack of previous studies on this relationship suggests the need for further investigation into the effect of this variant.
To further investigate the association between polymorphisms and metabolite levels, preliminary multivariable predictive models were developed. These models included the genotypes of the seven studied polymorphisms along with several relevant non-genomic factors. A significant preliminary predictive model was obtained for the [NdesMeTAM]/[TAM] ratio, incorporating the CYP2D6*4, CYP3A4*1B, and UGT2B7*2 genotypes, as well as non-genomic factors such as body mass index, family history of cancer, age at menarche, number of abortions, and postmenopausal status. This model explains (R2) 33.1% of the variability in the NdesMeTAM/TAM ratio (p=0.03) (Table 6). In this context, some authors have found that metabolite concentrations increase when the activity of CYP2D6 and CYP3A4 enzymes decreases, which is associated with the mutant genotype [30,50,58,59].
To explain the impact of UGT2B7*2 and UGT2B15*2 genotypes plus non-genomic factors (oral contraceptive treatment and postmenopausal status), we obtained a significant preliminary multivariable predictive model that explains about 48,9% of the variability in [4OHTAM/TAM] ratio (p=0.03) (Table 7).
A similar predictive model was generated between endoxifen/NdesMeTAM ratio (p=0.0002) with SULT1A1*2, UGT2B7*2, and UGT2B15*2 genotypes and relevant non-genomic factors (body mass index, age at menarche, number of deliveries, oral contraceptive treatment and cancer stage). We found that 76.0% of the endoxifen/NdesMeTAM ratio (p=0.0002) is associated with these variables (Table 8).
For [endoxifen/4OHTAM] ratio we obtained a significant multivariable logistic model including CYP2D6*4, SULT1A1*2, UGT2B7*2, UGT2B15*2, and ESR1 V364E genotypes and the non-genomic variables number of gestations, number of abortions and oral contraceptive treatment. The preliminary predictive model generated could explain 43.7% of the variability of [endoxifen/4OHTAM] ratio (p=0.01) (Table 9). These results were expected for SULT1A1 and UGT2B15 genotypes because these enzymes are specific for 4-hydroxyTAM and variant genotypes are associated with a decrease in catalytic activity, affecting the elimination of 4-hydroxyTAM. Similar correlations were described for CYP2D6, where the metabolites concentration increased in the presence of the mutant genotype [30,50].
Finally, a preliminary predictive multivariable model was obtained that explains 54.1% of the variability of 17β estradiol plasma levels (p=0.002) including the CYP3A5*3, SULT1A1*2, and UGT2B7*2 genotypes and relevant non-genomic factors (family history of breast or ovary cancers and menarche age) (Table 10).
Regarding adverse reactions, significant preliminary multivariable predictive models were obtained, but only for predicting hot flashes and cramps. The hot flash model, which included UGT2B7*2 and UGT2B15*2 genotypes, [4OHTAM]/[TAM] and [Endoxifen]/[NdesMeTAM] ratios, body mass index, and smoking habit, explained 33.2% of the variability (p=0.03) (Table 11). The cramps model, which included the UGT2B15*2 genotype, [Endoxifen]/[NdesMeTAM] ratio, height, and cancer stage, explained 41.6% of the probability of occurrence (p=0.02) (Table 12).
There are limitations in our study that must be considered for accurate interpretation of the results. Primarily, a significant constraint of this study is the relatively small sample size of patients, although we believe the inclusion of HPLC-MS/MS analyses on plasma samples makes it challenging to acquire a larger number of patients. In fact, from the original 162 potential participants [45] 122 rejected to give and extra sample for metabolite analyses. This limitation impacts the ability to establish associations, particularly concerning low-frequency polymorphisms, notably in the context of multivariable analyses. Additionally, not all patients had complete clinical data, introducing potential bias through differential misclassification, thereby affecting the robustness of the associations observed.
5. Conclusions
In this study, we assessed the potential association between the outcomes of TAM-treated breast cancer patients, TAM metabolite concentrations, and seven genetic polymorphisms. It was found that the CYP3A4*1/1B genotype alone could explain part of the variability in [4OHTAM], [endoxifen]/[4OHTAM], and 17β-estradiol plasma levels. Similarly, SULT1A1*1/*2 genotype affects the [endoxifen]/[4OHTAM] plasma ratio. Multivariable predictive models, incorporating both polymorphisms and non-genetic variables, are proposed to explain [NdesMeTAM]/[TAM], [4OHTAM]/[TAM], [endoxifen]/[NdesMeTAM], [endoxifen]/[4OHTAM], and 17β-estradiol plasma levels, as well as for predicting hot flashes and cramps. This preliminary study suggests that the genetic variants studied may influence the bioactivation and elimination of TAM, the clinically observed adverse reactions, and potentially the treatment efficacy.
Author Contributions
Conceptualization, CM) and LAQ; methodology, CM, MG, MT and KT; software CM and DC; validation, LAQ and GM; formal analysis, CM; investigation, CM, MG; data curation, CM, MG, DC, KL, NV, LC, MA, GM and LAQ; writing original draft preparation, CM, GM, MR, DC and LAQ; project administration, LAQ. All authors have read and agreed to the published version of the manuscript.
Funding
No funding was received.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of University of Chile (July 24, 2013), the Northern Metropolitan Health Service, National Cancer Institute (May 8, 2013), and Research Ethics Committee of the North Metropolitan Health Service (June 3, 2012, and according to Chilean Laws 20.120, 20.584, and 19.628, and the guidelines of the Good Clinical Practices”. .
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study. .
Data Availability Statement
The datasets used and/or analyzed during the current study are available from https://github.com/Luisquinones56/BreastCaCQF.git, any other requirement is available from the corresponding author on reasonable request.
Acknowledgments
The authors wish to thank the breast cancer patients from the “Instituto Nacional del Cáncer” for their altruistic collaboration in pursuit of the common welfare. We also thank the Latin American Society of Pharmacogenomics and Personalized Medicine (SOLFAGEM) for sponsoring this article and to de CYTED (Programa Iberoamericano de Ciencia y Tecnología para el Desarrollo) for supporting RELIVAF activities.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- American Cancer Society. Breast Cancer What is breast cancer? [Internet]. American Cancer Society. Cancer Facts and Figures Atlanta, Ga: American Cancer Society. 2021. p. 1–18. Available from: http://www.cancer.org/cancer/breast-cancer/about/what-is-breast-cancer.html (accessed on 18 June 2014).
- [Kumar, Vinay et al. Robbins & Cotran Pathologic Basis of Disease]. 11 ed. Barcelona: Elsevier, 2010. ISBN: 9780323790185.
- Band A, Laiho M. Crosstalk of TGF-β and estrogen receptor signaling in breast cancer. J Mammary Gland Biol Neoplasia. 2011 Jun;16(2):109–15. [CrossRef]
- MINSAL. Clinical Breast Cancer guideline for people over 15 years. [MINSAL. Guía clínica cáncer de mama en personas de 15 años y más. 1st Ed Santiago. 2005]. http://www.minsal.cl/portal/url/item/96721e0a5d1c5c1ee04001011e016513.pdf.
- MINSAL. Health Management of the Breast Cancer Program in Chile. [MINSAL. Guía clínica Cáncer de Mama. Santiago. 2015]. https://www.minsal.cl/wp-content/uploads/2015/09/GPC-CaMama.pdf.
- Hormone Therapy for Breast Cancer was originally published by the National Cancer Institute (NCI). https://www.cancer.gov/types/breast/breast-hormone-therapy-fact-sheet (accessed on 18 June 2014).
- Shagufta, Ahmad I. Tamoxifen a pioneering drug: An update on the therapeutic potential of tamoxifen derivatives. Eur J Med Chem. 2018 Jan 1;143:515-531. [CrossRef] [PubMed]
- Kerr AJ, Dodwell D, McGale P, Holt F, Duane F, Mannu G, Darby SC, Taylor CW. Adjuvant and neoadjuvant breast cancer treatments: A systematic review of their effects on mortality. Cancer Treat Rev. 2022 Apr;105:102375. [CrossRef] [PubMed]
- Johnston SJ, Cheung KL. Endocrine Therapy for Breast Cancer: A Model of Hormonal Manipulation. Oncol Ther. 2018 Dec;6(2):141-156. [CrossRef] [PubMed]
- Kumar R, Zakharov MN, Khan SH, Miki R, Jang H, Toraldo G, Singh R, Bhasin S, Jasuja R. The dynamic structure of the estrogen receptor. J Amino Acids. 2011;2011:812540. [CrossRef] [PubMed]
- Stice JP, Knowlton AA. Estrogen, NFkappaB, and the heat shock response. Mol Med. 2008 Jul-Aug;14(7-8):517-27. [CrossRef]
- Singh M, Francis P, Michael M. Tamoxifen, cytochrome P450 genes and breast cancer clinical outcomes. Breast. 2011 Apr;20(2):111–8. [CrossRef]
- Irarrázaval, M. [Antagonism of tamoxifen and antidepressants among women with breast cancer]. Tamoxifeno y antidepresivos: ¿Antagonistas en la prevención del cáncer de mama? Rev Med Chil. 2011;139(1):89–99. [CrossRef]
- Early Breast Cancer Trialists' Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomized trials. Lancet. 2005 May 14-20;365(9472):1687-717. [CrossRef]
- Johnson MD, Zuo H, Lee KH, Trebley JP, Rae JM, Weatherman RV, Desta Z, Flockhart DA, Skaar TC. Pharmacological characterization of 4-hydroxy-N-desmethyl tamoxifen, a novel active metabolite of tamoxifen. Breast Cancer Res Treat. 2004 May;85(2):151-9. [CrossRef]
- Jordan V, Collins M, Rowsby L, Prestwich G. A monohydroxylated metabolite of tamoxifen with potent antioestrogenic activity. J Endocrinol. 1977 Nov;75(2):305–16. [CrossRef]
- Clarke R, Liu MC, Bouker KB, Gu Z, Lee RY, Zhu Y, Skaar TC, Gomez B, O'Brien K, Wang Y, Hilakivi-Clarke LA. Antiestrogen resistance in breast cancer and the role of estrogen receptor signaling. Oncogene. 2003 Oct 20;22(47):7316-39. [CrossRef]
- Borges S, Desta Z, Li L, Skaar TC, Ward BA, Nguyen A, Jin Y, Storniolo AM, Nikoloff DM, Wu L, Hillman G, Hayes DF, Stearns V, Flockhart DA. Quantitative effect of CYP2D6 genotype and inhibitors on tamoxifen metabolism: implication for optimization of breast cancer treatment. Clin Pharmacol Ther. 2006 Jul;80(1):61-74. [CrossRef]
- Nishiyama T, Ogura K, Nakano H, Ohnuma T, Kaku T, Hiratsuka A, Muro K, Watabe T. Reverse geometrical selectivity in glucuronidation and sulfation of cis- and trans-4-hydroxytamoxifens by human liver UDP-glucuronosyltransferases and sulfotransferases. Biochem Pharmacol. 2002 May 15;63(10):1817-30. [CrossRef]
- Novillo, A., Romero-Lorca, A., Gaibar, M. et al. Tamoxifen metabolism in breast cancer treatment: Taking the focus off the CYP2D6 gene. Pharmacogenomics J 17, 109–111 (2017). [CrossRef]
- Rondón-Lagos, M.; Villegas, V.E.; Rangel, N.; Sánchez, M.C.; Zaphiropoulos, P.G. Tamoxifen Resistance: Emerging Molecular Targets. Int. J. Mol. Sci. 2016, 17, 1357. [CrossRef]
- Kisanga ER, Gjerde J, Guerrieri-Gonzaga A, Pigatto F, Pesci-Feltri A, Robertson C, Serrano D, Pelosi G, Decensi A, Lien EA. Tamoxifen and metabolite concentrations in serum and breast cancer tissue during three dose regimens in a randomized preoperative trial. Clin Cancer Res. 2004 Apr 1;10(7):2336-43. [CrossRef]
- Fisher B, Costantino JP, Wickerham DL, Redmond CK, Kavanah M, Cronin WM, Vogel V, Robidoux A, Dimitrov N, Atkins J, Daly M, Wieand S, Tan-Chiu E, Ford L, Wolmark N. Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1 Study. J Natl Cancer Inst. 1998 Sep 16;90(18):1371-88. [CrossRef]
- Cuzick J, Forbes J, Edwards R, Baum M, Cawthorn S, Coates A, Hamed A, Howell A, Powles T; IBIS investigators. First results from the International Breast Cancer Intervention Study (IBIS-I): a randomized prevention trial. Lancet. 2002 Sep 14;360(9336):817-24. [CrossRef]
- Ma Q, Lu A. Pharmacogenetics, pharmacogenomics, and individualized medicine. Pharmacol Rev. 2011 Jun;63(2):437–59. [CrossRef]
- Higgins M, Stearns V. CYP2D6 polymorphisms and tamoxifen metabolism: clinical relevance. Curr Oncol Rep. 2010 Jan;12(1):7–15. [CrossRef]
- Goetz MP, Sangkuhl K, Guchelaar HJ, Schwab M, Province M, Whirl-Carrillo M, Symmans WF, McLeod HL, Ratain MJ, Zembutsu H, Gaedigk A, van Schaik RH, Ingle JN, Caudle KE, Klein TE. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and Tamoxifen Therapy. Clin Pharmacol Ther. 2018 May;103(5):770-777. [CrossRef] [PubMed]
- Rae JM, Drury S, Hayes DF, Stearns V, Thibert JN, Haynes BP, Salter J, Sestak I, Cuzick J, Dowsett M; ATAC trialists. CYP2D6 and UGT2B7 genotype and risk of recurrence in tamoxifen-treated breast cancer patients. J Natl Cancer Inst. 2012 Mar 21;104(6):452-60. [CrossRef]
- Lim JS, Chen XA, Singh O, Yap YS, Ng RC, Wong NS, Wong M, Lee EJ, Chowbay B. Impact of CYP2D6, CYP3A5, CYP2C9 and CYP2C19 polymorphisms on tamoxifen pharmacokinetics in Asian breast cancer patients. Br J Clin Pharmacol. 2011 May;71(5):737-50. [CrossRef]
- Gjerde J, Hauglid M, Breilid H, Lundgren S, Varhaug JE, Kisanga ER, Mellgren G, Steen VM, Lien EA. Effects of CYP2D6 and SULT1A1 genotypes including SULT1A1 gene copy number on tamoxifen metabolism. Ann Oncol. 2008 Jan;19(1):56-61. [CrossRef]
- Kiyotani K, Mushiroda T, Imamura CK, Hosono N, Tsunoda T, Kubo M, Tanigawara Y, Flockhart DA, Desta Z, Skaar TC, Aki F, Hirata K, Takatsuka Y, Okazaki M, Ohsumi S, Yamakawa T, Sasa M, Nakamura Y, Zembutsu H. Significant effect of polymorphisms in CYP2D6 and ABCC2 on clinical outcomes of adjuvant tamoxifen therapy for breast cancer patients. J Clin Oncol. 2010 Mar 10;28(8):1287-93. [CrossRef]
- Madlensky L, Natarajan L, Tchu S, Pu M, Mortimer J, Flatt SW, Nikoloff DM, Hillman G, Fontecha MR, Lawrence HJ, Parker BA, Wu AH, Pierce JP. Tamoxifen metabolite concentrations, CYP2D6 genotype, and breast cancer outcomes. Clin Pharmacol Ther. 2011 May;89(5):718-25. [CrossRef]
- Chu W, Fyles A, Sellers EM, McCready DR, Murphy J, Pal T, Narod SA. Association between CYP3A4 genotype and risk of endometrial cancer following tamoxifen use. Carcinogenesis. 2007 Oct;28(10):2139-42. [CrossRef]
- Arslan S, Silig Y, Pinarbasi H. Sulfotransferase 1A1 Arg(213)His polymorphism and prostate cancer risk. Exp Ther Med. 2011 Jan;2(6):1159–62. [CrossRef]
- Ahern TP, Christensen M, Cronin-Fenton DP, Lunetta KL, Søiland H, Gjerde J, Garne JP, Rosenberg CL, Silliman RA, Sørensen HT, Lash TL, Hamilton-Dutoit S. Functional polymorphisms in UDP-glucuronosyl transferases and recurrence in tamoxifen-treated breast cancer survivors. Cancer Epidemiol Biomarkers Prev. 2011 Sep;20(9):1937-43. [CrossRef]
- Lévesque E, Delage R, Benoit-Biancamano MO, Caron P, Bernard O, Couture F, Guillemette C. The impact of UGT1A8, UGT1A9, and UGT2B7 genetic polymorphisms on the pharmacokinetic profile of mycophenolic acid after a single oral dose in healthy volunteers. Clin Pharmacol Ther. 2007 Mar;81(3):392-400. [CrossRef]
- Herynk MH, Fuqua SAW. Estrogen receptor mutations in human disease. Endocr Rev. 2004 Dec 1;25(6):869–98. [CrossRef]
- Paul Flicek, M. Paul Flicek, M. Ridwan Amode, Daniel Barrell, Kathryn Beal, Simon Brent, Yuan Chen, Peter Clapham, Guy Coates, Susan Fairley, Stephen Fitzgerald, Leo Gordon, Maurice Hendrix, Thibaut Hourlier, Nathan Johnson, Andreas Kähäri, Damian Keefe, Stephen Keenan, Rhoda Kinsella, Felix Kokocinski, Eugene Kulesha, Pontus Larsson, Ian Longden, William McLaren, Bert Overduin, Bethan Pritchard, Harpreet Singh Riat, Daniel Rios, Graham R. S. Ritchie, Magali Ruffier, Michael Schuster, Daniel Sobral, Giulietta Spudich, Y. Amy Tang, Stephen Trevanion, Jana Vandrovcova, Albert J. Vilella, Simon White, Steven P. Wilder, Amonida Zadissa, Jorge Zamora, Bronwen L. Aken, Ewan Birney, Fiona Cunningham, Ian Dunham, Richard Durbin, Xosé M. Fernández-Suarez, Javier Herrero, Tim J. P. Hubbard, Anne Parker, Glenn Proctor, Jan Vogel, Stephen M. J. Searle, Ensembl 2011, Nucleic Acids Research, Volume 39, Issue suppl_1, 1 January 2011, Pages D800–D806. [CrossRef]
- Wrenn CK, Katzenellenbogen BS. Structure-function analysis of the hormone binding domain of the human estrogen receptor by region-specific mutagenesis and phenotypic screening in yeast. J Biol Chem. 1993 Nov 15;268(32):24089–98. [CrossRef]
- Ince BA, Schodin DJ, Shapiro DJ, Katzenellenbogen BS. Repression of endogenous estrogen receptor activity in MCF-7 human breast cancer cells by dominant negative estrogen receptors. Endocrinology. 1995 Aug;136(8):3194–9. [CrossRef]
- McInerney EM, Ince BA, Shapiro DJ, Katzenellenbogen BS. A transcriptionally active estrogen receptor mutant is a novel type of dominant negative inhibitor of estrogen action. Mol Endocrinol. 1996 Dec;10(12):1519-26. [CrossRef]
- Binkhorst L, Mathijssen RHJ, Jager A, van Gelder T. Individualization of tamoxifen therapy: much more than just CYP2D6 genotyping. Cancer Treat Rev. 2015 Mar;41(3):289–99. [CrossRef]
- Province MA, Goetz MP, Brauch H, Flockhart DA, Hebert JM, Whaley R, Suman VJ, Schroth W, Winter S, Zembutsu H, Mushiroda T, Newman WG, Lee MT, Ambrosone CB, Beckmann MW, Choi JY, Dieudonné AS, Fasching PA, Ferraldeschi R, Gong L, Haschke-Becher E, Howell A, Jordan LB, Hamann U, Kiyotani K, Krippl P, Lambrechts D, Latif A, Langsenlehner U, Lorizio W, Neven P, Nguyen AT, Park BW, Purdie CA, Quinlan P, Renner W, Schmidt M, Schwab M, Shin JG, Stingl JC, Wegman P, Wingren S, Wu AH, Ziv E, Zirpoli G, Thompson AM, Jordan VC, Nakamura Y, Altman RB, Ames MM, Weinshilboum RM, Eichelbaum M, Ingle JN, Klein TE; International Tamoxifen Pharmacogenomics Consortium. CYP2D6 genotype and adjuvant tamoxifen: meta-analysis of heterogeneous study populations. Clin Pharmacol Ther. 2014 Feb;95(2):216-27. [CrossRef]
- Reis SS, Carvalho AS, Fernandes R. Pharmacogenomics, CYP2D6, and Tamoxifen: A Survey of the Reasons Sustaining European Clinical Practice Paradigms. Medicina (Kaunas). 2019 Jul 5;55(7):344. [CrossRef] [PubMed]
- Miranda C, Galleguillos M, Torres R, Tardón K, Cáceres DD, Lee K, Redal MA, Varela NM, Quiñones LA. Preliminary Pharmacogenomic-Based Predictive Models of Tamoxifen Response in Hormone-dependent Chilean Breast Cancer Patients. Front Pharmacol. 2021 Nov 25;12:661443. [CrossRef] [PubMed]
- Binkhorst L, Mathijssen RH, Ghobadi Moghaddam-Helmantel IM, de Bruijn P, van Gelder T, Wiemer EA, Loos WJ. Quantification of tamoxifen and three of its phase-I metabolites in human plasma by liquid chromatography/triple-quadrupole mass spectrometry. J Pharm Biomed Anal. 2011 Dec 15;56(5):1016-23. [CrossRef]
- Lien EA, Søiland H, Lundgren S, Aas T, Steen VM, Mellgren G, Gjerde J. Serum concentrations of tamoxifen and its metabolites increase with age during steady-state treatment. Breast Cancer Res Treat. 2013 Sep;141(2):243-8. [CrossRef]
- Teunissen SF, Rosing H, Koornstra RH, Linn SC, Schellens JH, Schinkel AH, Beijnen JH. Development and validation of a quantitative assay for the analysis of tamoxifen with its four main metabolites and the flavonoids daidzein, genistein and glycitein in human serum using liquid chromatography coupled with tandem mass spectrometry. J Chromatogr B Analyt Technol Biomed Life Sci. 2009 Aug 15;877(24):2519-29. [CrossRef]
- Teunissen SF, Jager NGL, Rosing H, Schinkel AH, Schellens JHM, Beijnen JH. Development and validation of a quantitative assay for the determination of tamoxifen and its five main phase I metabolites in human serum using liquid chromatography coupled with tandem mass spectrometry. J Chromatogr B Analyt Technol Biomed Life Sci. 2011 Jun 1;879(19):1677–85. [CrossRef]
- Chen Y, Marcath LA, Eliassen FM, Lende TH, Soiland H, Mellgren G, Helland T, Hertz DL. Effect of Genetic Variability in 20 Pharmacogenes on Concentrations of Tamoxifen and Its Metabolites. J Pers Med. 2021 Jun 4;11(6):507. [CrossRef]
- Lee KH, Ward BA, Desta Z, Flockhart DA, Jones DR. Quantification of tamoxifen and three metabolites in plasma by high-performance liquid chromatography with fluorescence detection: application to a clinical trial. J Chromatogr B Analyt Technol Biomed Life Sci. 2003 Jul 5;791(1–2):245–53. [CrossRef]
- Johänning J, Kröner P, Thomas M, Zanger UM, Nörenberg A, Eichelbaum M, Schwab M, Brauch H, Schroth W, Mürdter TE. The formation of estrogen-like tamoxifen metabolites and their influence on enzyme activity and gene expression of ADME genes. Arch Toxicol. 2018 Mar;92(3):1099-1112. [CrossRef]
- Squirewell EJ, Duffel MW. The Effects of Endoxifen and Other Major Metabolites of Tamoxifen on the Sulfation of Estradiol Catalyzed by Human Cytosolic Sulfotransferases hSULT1E1 and hSULT1A1*1. Drug Metab Dispos. 2015 Jun;43(6):843–50. [CrossRef]
- Rebbeck TR, Su HI, Sammel MD, Lin H, Tran TV, Gracia CR, Freeman EW. Effect of hormone metabolism genotypes on steroid hormone levels and menopausal symptoms in a prospective population-based cohort of women experiencing the menopausal transition. Menopause. 2010 Sep-Oct;17(5):1026-34. [CrossRef]
- Lévesque E, Beaulieu M, Green M, Tephly T, Bélanger A, Hum D. Isolation and characterization of UGT2B15(Y85): a UDP-glucuronosyltransferase encoded by a polymorphic gene. Pharmacogenetics. 1997 Aug;7(4):317–25. [CrossRef]
- Romero-Lorca A, Novillo A, Gaibar M, Bandrés F, Fernández-Santander A. Impacts of the Glucuronidase Genotypes UGT1A4, UGT2B7, UGT2B15 and UGT2B17 on Tamoxifen Metabolism in Breast Cancer Patients. PLoS One. 2015 Jul 15;10(7):e0132269. [CrossRef]
- Hao Z, Xu J, Zhao H, Zhou W, Liu Z, He S, Yin X, Zhang B, Wang Z, Zhou X. The inhibition of tamoxifen on UGT2B gene expression and enzyme activity in rat liver contribute to the estrogen homeostasis dysregulation. BMC Pharmacol Toxicol. 2022 May 31;23(1):33. [CrossRef]
- Boucenna, A., Boudaoud, K., Hireche, A. et al. Influence of CYP2D6, CYP2C19 and CYP3A5 polymorphisms on plasma levels of tamoxifen metabolites in Algerian women with ER+ breast cancer. Egypt J Med Hum Genet 23, 122 (2022). [CrossRef]
- Saghafi F, Salehifar E, Janbabai G, Zaboli E, Hedayatizadeh-Omran A, Amjadi O, Moradi S. CYP2D6*3 (A2549del), *4 (G1846A), *10 (C100T) and *17 (C1023T) genetic polymorphisms in Iranian breast cancer patients treated with adjuvant tamoxifen. Biomed Rep. 2018; 9(5):446-452. [CrossRef]
Figure 1.
Biotransformation of tamoxifen in the cell.
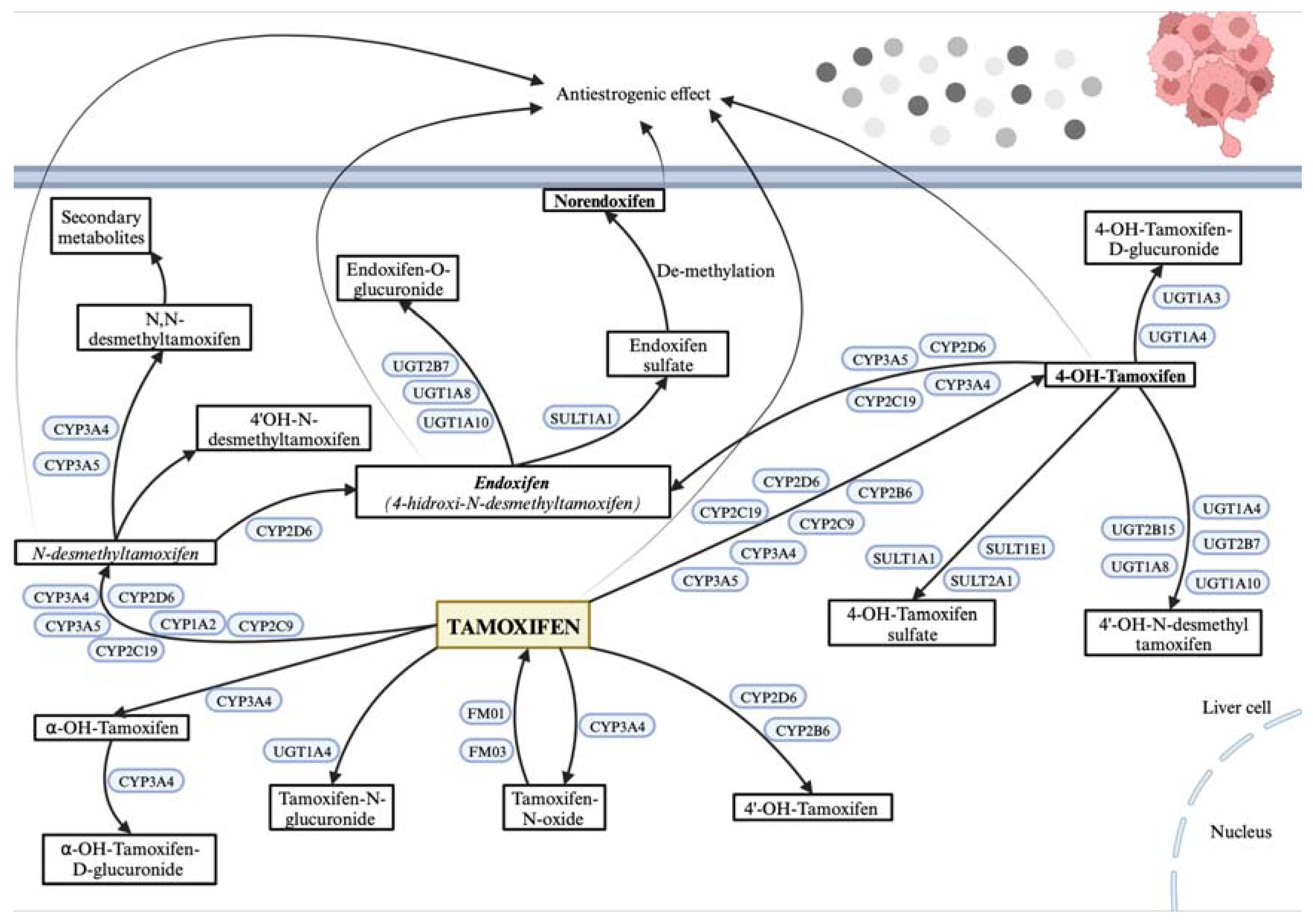
Figure 2.
Representative images of genotyping results for phase I variants (CYP2D6*4 (rs3892097), CYP3A4*1B (rs2740574), CYP3A5*3 (rs776746), phase II variants (SULT1A1*2 (rs9282861), UGT2B7*2 (rs7439366), UGT2B15*2 (rs1902023)) and ESR1 V364E (rs121913044). wt = wild type; MW Std = molecular weight standard. CYP3A4*1B and UGT2B15*2 were observed in 18% polyacrylamide gels, CYP2D6*4, CYP3A5*3, SULT1A1*2, UGT2B7*2 and ESR1 V364E 2% agarose gels.
Figure 2.
Representative images of genotyping results for phase I variants (CYP2D6*4 (rs3892097), CYP3A4*1B (rs2740574), CYP3A5*3 (rs776746), phase II variants (SULT1A1*2 (rs9282861), UGT2B7*2 (rs7439366), UGT2B15*2 (rs1902023)) and ESR1 V364E (rs121913044). wt = wild type; MW Std = molecular weight standard. CYP3A4*1B and UGT2B15*2 were observed in 18% polyacrylamide gels, CYP2D6*4, CYP3A5*3, SULT1A1*2, UGT2B7*2 and ESR1 V364E 2% agarose gels.
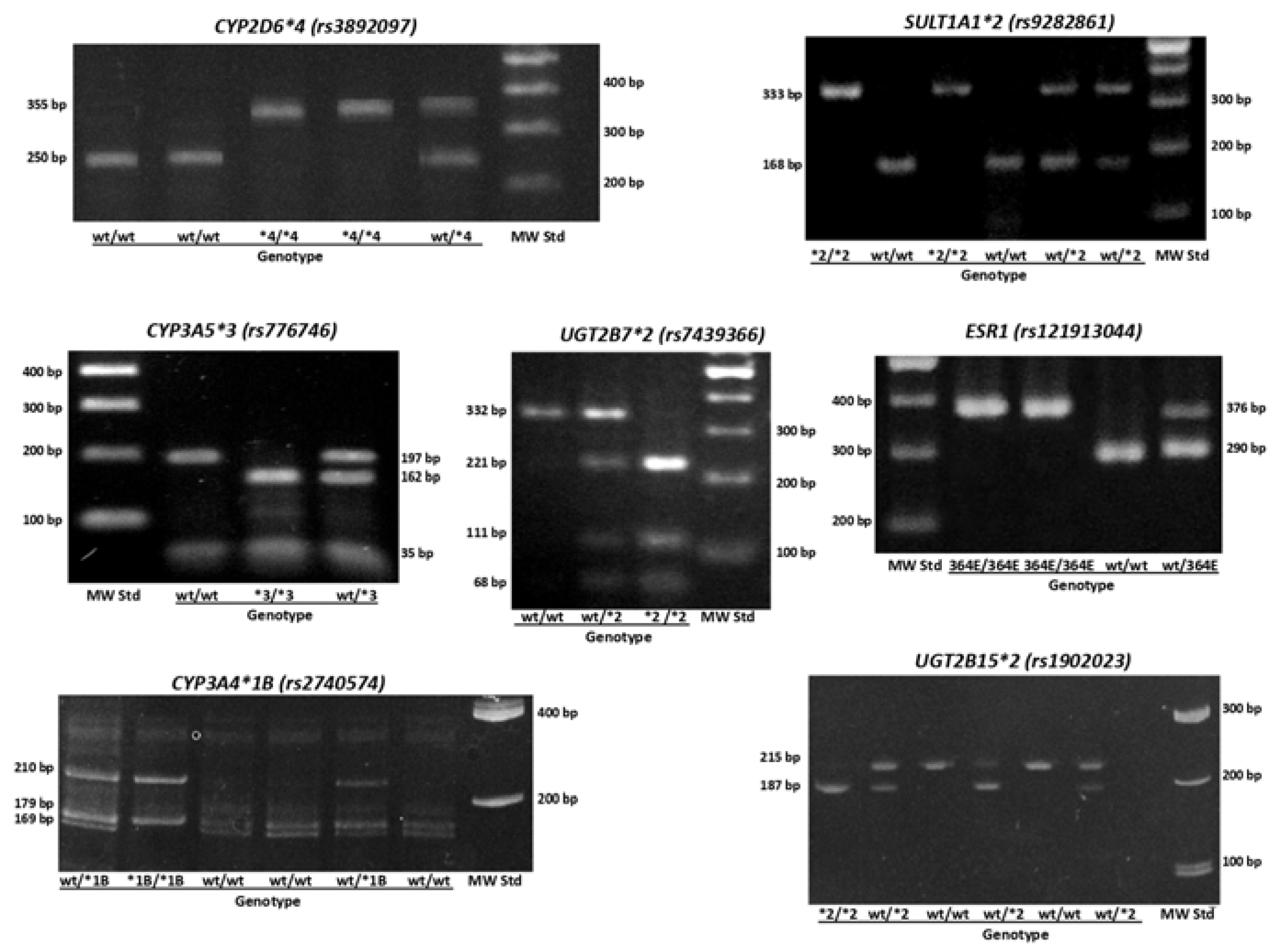
Figure 3.
Association between plasma concentration at steady state of Tamoxifen, N-desmethylTAM, 4-hydroxyTAM and endoxifen, and concentration of 17β estradiol, and the presence of CYP2D6 *4, CYP3A4 *1B, and CYP3A5 *3 polymorphisms in patients.
Figure 3.
Association between plasma concentration at steady state of Tamoxifen, N-desmethylTAM, 4-hydroxyTAM and endoxifen, and concentration of 17β estradiol, and the presence of CYP2D6 *4, CYP3A4 *1B, and CYP3A5 *3 polymorphisms in patients.
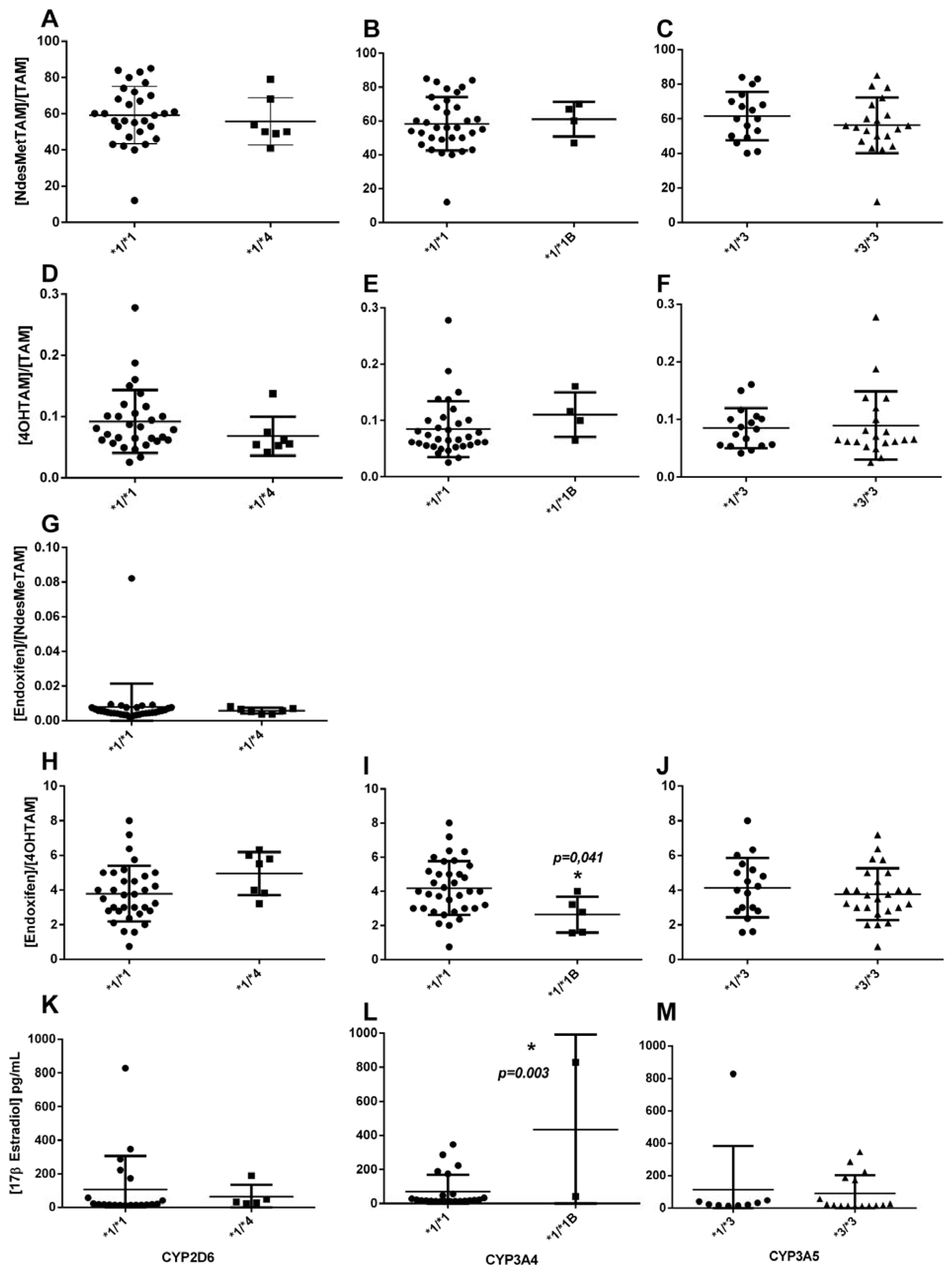
Figure 4.
Association between the steady-state plasma concentration of 4-hydroxyTAM and endoxifen, and the concentration of 17β estradiol, and SULT1A1 *2, UGT2B7 *2, and UGT2B15 *2 polymorphisms in patients.
Figure 4.
Association between the steady-state plasma concentration of 4-hydroxyTAM and endoxifen, and the concentration of 17β estradiol, and SULT1A1 *2, UGT2B7 *2, and UGT2B15 *2 polymorphisms in patients.
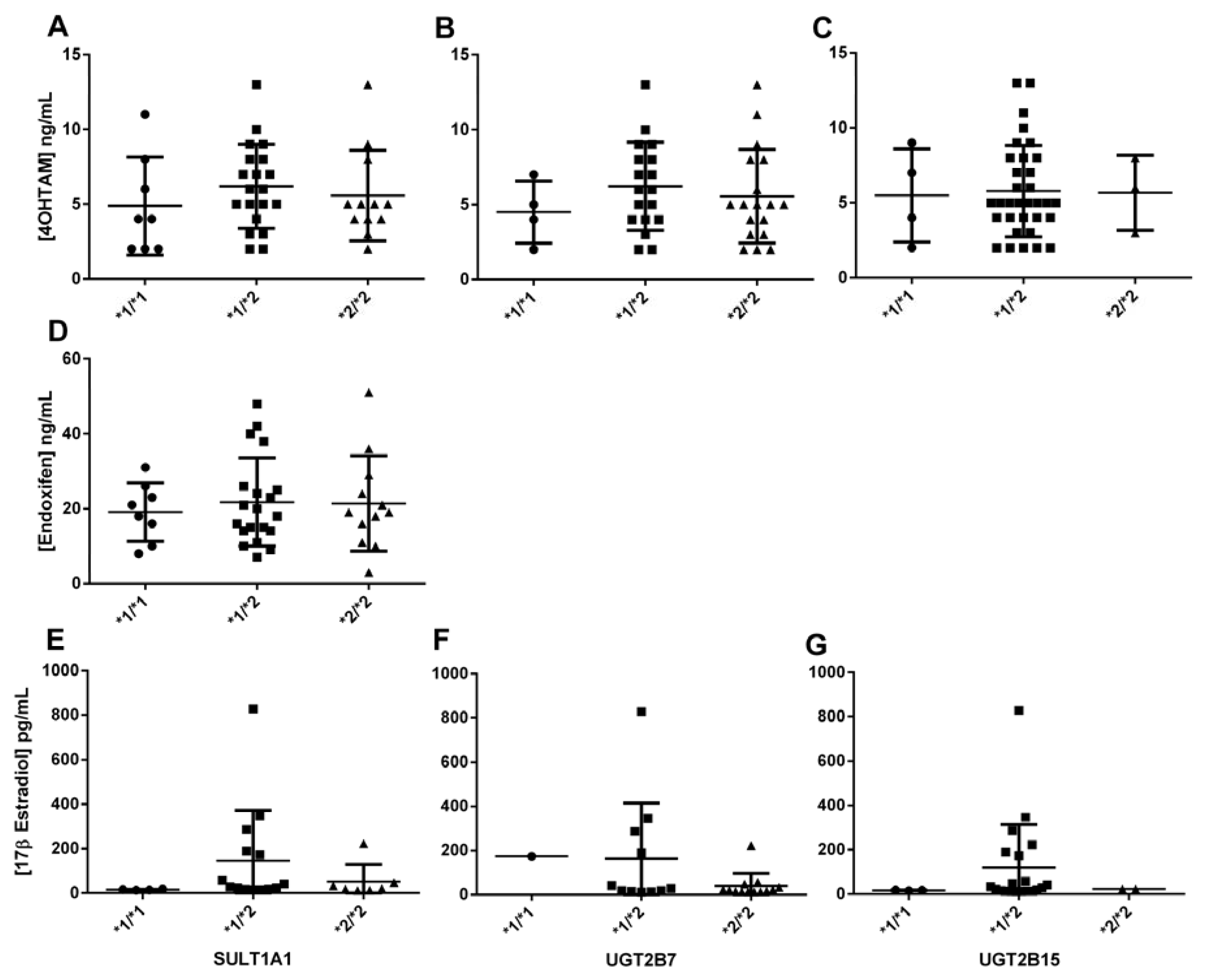

Table 1.
General characteristics of patients (n = 40).
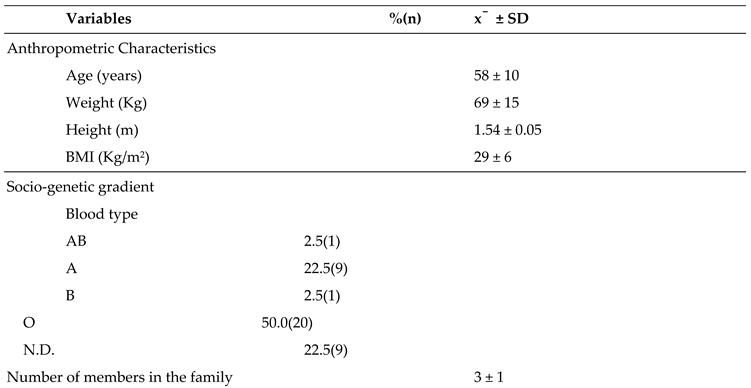
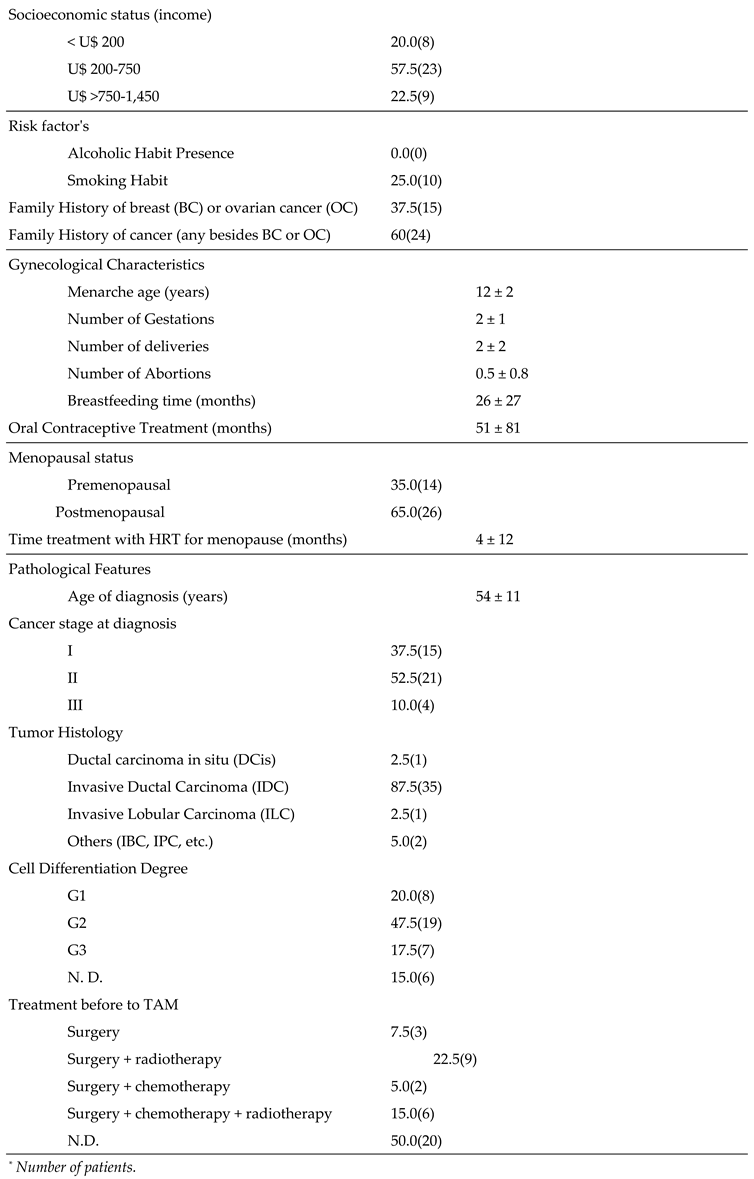

Table 2.
Genotype frequencies of CYP2D6*4, CYP3A4*1B, CYP3A5*3, SULT1A1, UGT2B7*2,.UGT2B15*2 and ESR1 V364E.
Table 2.
Genotype frequencies of CYP2D6*4, CYP3A4*1B, CYP3A5*3, SULT1A1, UGT2B7*2,.UGT2B15*2 and ESR1 V364E.
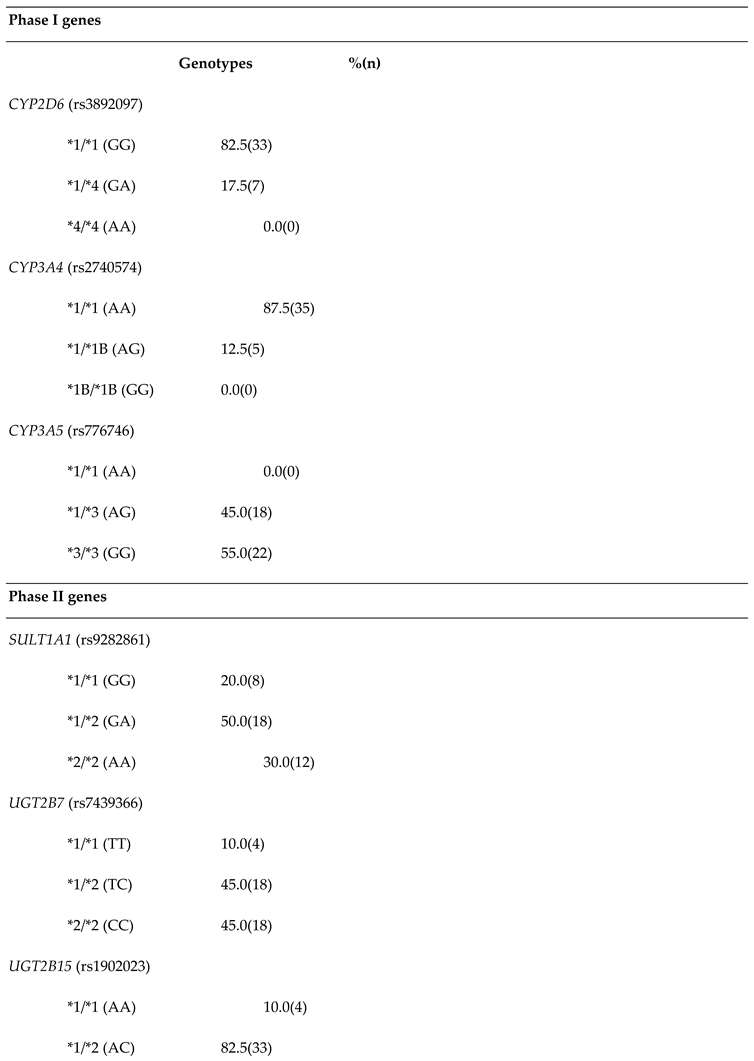
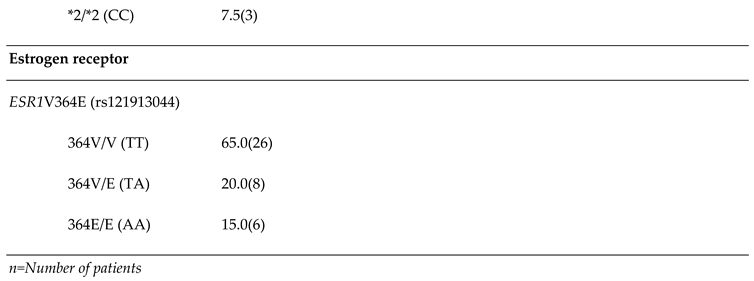
Table 3.
Recurrence and Adverse Drug Reactions (ADRs) in patients (n=40).
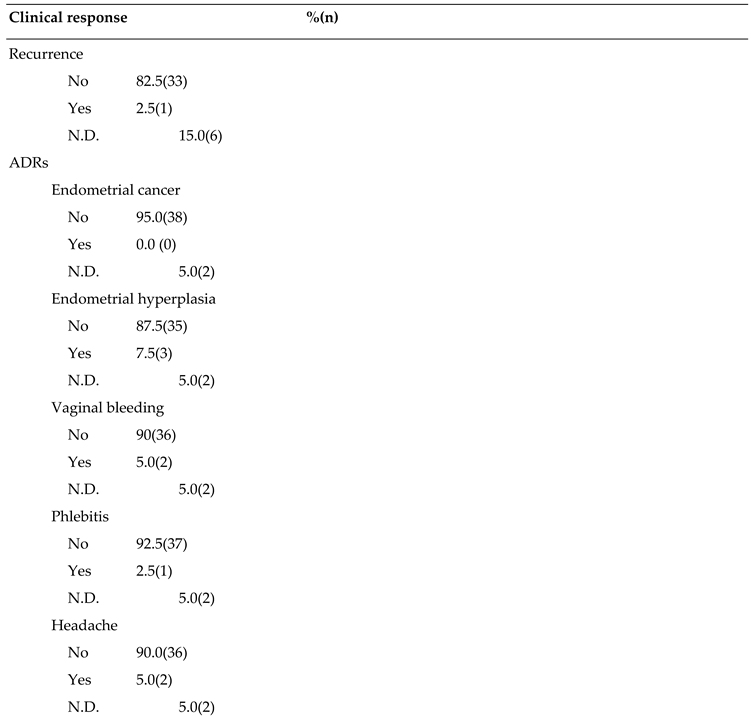
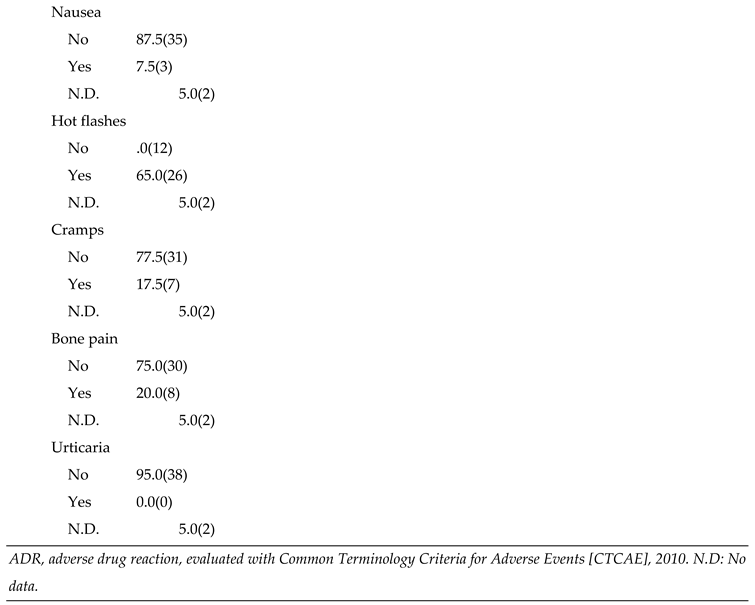
Table 4.
Bivariable linear regression analyses between steady-state plasma concentrations of TAM metabolites and 17β estradiol, in relation to genetic polymorphisms in patients.
Table 4.
Bivariable linear regression analyses between steady-state plasma concentrations of TAM metabolites and 17β estradiol, in relation to genetic polymorphisms in patients.
| n |
Frequency (%) |
mean (SD) | Bivariable model | |||||
| [4OHTAM] | Coef | (CI 95%) | p value | R2 | ||||
| CYP3A4*1/*1 (AA) | 35 | (87.5) | 5.22 (2.48) | |||||
| CYP3A4*1/*1B (AG) | 5 | (12.5) | 9.4 (3.58) | 4.17 | (1.63 ; 6.71) | 0.002 | 0.22 | |
| [Endoxifen]/[4OHTAM] | ||||||||
| CYP3A4*1/*1 (AA) | 35 | (87.50) | 4.18 (1.57) | |||||
| CYP3A4*1/*1B (AG) | 5 | (12.50) | 2.63 (1.04) | -1.54 | (-3.03 ; -0.06) | 0.0410 | 0.10 | |
| [17β estradiol] | ||||||||
| CYP3A4*1/*1 (AA) | 23 | (92.00) | 70.21 (99.18) | |||||
| CYP3A4*1/*1B (AG) | 2 | (8.00) | 434.50 (556.49) | 364.28 | (133.63 - 594.94) | 0.0030 | 0.31 | |
SD: Standard Deviation; CI: Confidence Interval; R2: Determination Coefficient; TAM: Tamoxifen. 4OHTAM: 4-.hydroxyTAM. n: number of subjects. SD: Standard deviation. Coef.: regression coefficient.
Table 5.
Bivariable logistic regression analyses of TAM metabolites and 17β Estradiol in relation to genetic polymorphism in patients.
Table 5.
Bivariable logistic regression analyses of TAM metabolites and 17β Estradiol in relation to genetic polymorphism in patients.
| Cases | Controls | |||||||||
| n | % | n | % | ORc | (CI 95%) | p-value* | pR2 | |||
| [4OHTAM]/[TAM] | ||||||||||
| UGT2B7 genoypes | ||||||||||
| *1/*1 (TT) | 3 | (18.75) | 1 | (4.17) | Ref. | - | 0.09 | |||
| *1/*2 (TC) | 9 | (56.25) | 9 | (37.50) | 0.33 | (0.028 - 3.84) | 0.378 | |||
| *2/*2 (CC) | 4 | (25.00) | 14 | (58.33) | 0.09 | (0.007 - 1.18) | 0.068 | |||
| [Endoxifen]/[4OHTAM] | ||||||||||
| SULT1A1 genoypes | ||||||||||
| *1/*1 (GG) | 6 | (30.00) | 2 | (10.00) | Ref. | - | 0.12 | |||
| *1/*2 (GA) | 6 | (30.00) | 14 | (70.00) | 0.14 | (0.02-0.92) | 0.041 | |||
| *2/*2 (AA) | 8 | (40.00) | 4 | (20.00) | 0.66 | (0.09-4.92) | 0.691 | |||
| ESR1 V364E genoypes | ||||||||||
| 364V/364V (TT) | 16 | (80.00) | 10 | (50.00) | Ref. | - | 0.07 | |||
| 364V/364E (TA) + 364E/364E (AA) | 4 | (20.00) | 10 | (50.00) | 0.25 | (0.06- 1.01) | 0.053 | |||
| 17βEstradiol | ||||||||||
| UGT2B7 genoypes | ||||||||||
| *1/*1 (TT)+*1/*2 (TC) | 5 | (83.33) | 7 | (36.84) | Ref. | - | 0.15 | |||
| *2/*2 (CC) | 1 | (16.67) | 12 | (63.16) | 0.12 | (0.01-1.21) | 0.071 | |||
TAM: Tamoxifen; 4OHTAM: 4-hydroxyTAM; n: number of subjects; ORc: Crude Odds Ratio; pR2:PseudoR2; CI95%: Confidence Interval.*Significant value in bold (p<0.05).
Table 6.
Multivariable logistic regression analysis or logit model* for [NdesMeTAM]/[TAM], after stepwise.forward and backward procedure bivariable analysis.
Table 6.
Multivariable logistic regression analysis or logit model* for [NdesMeTAM]/[TAM], after stepwise.forward and backward procedure bivariable analysis.
| Coef.** | 95% CI | p-value | |
| Body mass index, (Kg/m2) | 0.212 | -0.0005 - 0.424 | 0.051 |
| Family history of cancer (any besides BC or OC) | -0.992 | -2.904 - 0.919 | 0.309 |
| Menarche age (years) | 0.741 | 0.067 - 1.415 | 0.031 |
| Number of Abortions | -0.949 | -2.450 - 0.552 | 0.215 |
| Menopausal status | |||
| Premenopausal | Ref. | ------- | ------ |
| Postmenopausal | -1.144 | -2.970 - 0.6823007 | 0.220 |
| CYP2D6 genotypes | |||
| *1/*1 (GG) | Ref. | ------- | ------- |
| *1/*4 (GA) | 0.400 | -2.172243 – 2.973472 | 0.760 |
| CYP3A4 genotypes | |||
| *1/*1 (AA) | Ref. | -------- | -------- |
| *1/*1B (AG) | 2.029 | -1.003382 – 5.062251 | 0.190 |
| UGT2B7 genotypes | |||
| *1/*1 (AA) | Ref. | -------- | -------- |
| *1/*2 (AC) | 1.713 | -1.586425 – 5.013695 | 0.309 |
| *2/*2 (CC) | 1.548 | -1.898279 – 4.995144 | 0.379 |
| Constant (β0) | -15.140 | -29.25346 – 1.027427 | 0.035 |
*Model p=0.03; Pseudo R2=0.3308;**Logit – Cumulative standard logistic distribution (F). P value< 0.05 is considered significant (in bold).
Table 7.
Multivariable logistic regression analysis or logit model* for [4OHTAM]/[TAM], after stepwise. forward and backward procedure bivariable analysis.
Table 7.
Multivariable logistic regression analysis or logit model* for [4OHTAM]/[TAM], after stepwise. forward and backward procedure bivariable analysis.
| Coef.** | 95% CI | p-value | |
| Oral Contraceptive Treatment (months) | -.1861939 | -0.806 - 0.434 | 0.557 |
| Menopausal status | |||
| Premenopausal | Ref. | -------- | -------- |
| Postmenopausal | -1.787.515 | -5.157 – 1.582 | 0.299 |
| UGT2B7 genotypes | |||
| *1/*1 (TT) | Ref. | -------- | -------- |
| *1/*2 (TC)+*2/*2 (CC) | -3.038.116 | -6.422 - 0.346 | 0.078 |
| UGT2B15 genotypes | |||
| *1/*1 (AA) | Ref. | -------- | -------- |
| *1/*2 (AC)+*2/*2 (CC) | -.3406396 | -4.690 – 4.009 | 0.878 |
| Constant (β0) | 1.811.823 | -2.709 – 6.333 | 0.432 |
*Model p=0.03; Pseudo R2=0.4892 **Logit – Cumulative standard logistic distribution (F).P value< 0.05 is considered significant.
Table 8.
Multivariable logistic regression analysis or logit model* for [Endoxifen]/[NdesMeTAM],. after stepwise forward and backward procedure bivariable analysis.
Table 8.
Multivariable logistic regression analysis or logit model* for [Endoxifen]/[NdesMeTAM],. after stepwise forward and backward procedure bivariable analysis.
| Coef.** | 95% CI | p-value | |
| Body mass index, (Kg/m2) | -1.717 | -4.595 – 1.161 | 0.242 |
| Smoking Habit | 2.858 | -8.536 – 65.715 | 0.131 |
| Menarche age (years) | 2.992 | -0.858 – 6.843 | 0.128 |
| Number of deliveries | -5.306 | -13.268 – 2.656 | 0.192 |
| Oral Contraceptive Treatment (months) | -0.883 | -2.247 - 0.479 | 0.204 |
| Cancer stage at diagnosis | |||
| I | Ref. | -------- | -------- |
| II | -38.106 | -89.189 – 12.975 | 0.144 |
| III | -13.250 | -29.259 – 2.757 | 0.105 |
| SULT1A1 genotypes | |||
| *1/*1 (GG) | Ref. | -------- | -------- |
| *1/*2 (GA)+*2/*2 (AA) | -32.463 | -78.521 – 13.594 | 0.167 |
| UGT2B7 genotypes | |||
| *1/*1 (TT) | Ref. | -------- | -------- |
| *1/*2 (TC)+*2/*2 (CC) | -46.126 | -112.404 – 20.152 | 0.173 |
| UGT2B15 genotypes | |||
| *1/*1 (AA) | Ref. | -------- | -------- |
| *1/*2 (AC)+*2/*2 (CC) | 36.600 | -19.086 – 92.287 | 0.198 |
| Constant (β0) | 59.908 | -42.134 – 161.951 | 0.250 |
*Model p=0.0002; Pseudo R2=0.7603**Logit – Cumulative standard logistic distribution (F). P value< 0.05 is considered significant.
Table 9.
Multivariable logistic regression analysis or logit model* for [Endoxifen]/[4OHTAM], after stepwise. forward and backward procedure bivariable analysis.
Table 9.
Multivariable logistic regression analysis or logit model* for [Endoxifen]/[4OHTAM], after stepwise. forward and backward procedure bivariable analysis.
| Coef.** | 95% CI | p-value | |
| Family history of cancer (any besides BC or OC) | -1.446 | -3.574 - 0.680 | 0.183 |
| Number of Gestations | 0.034 | -0.567 - 0.637 | 0.910 |
| Number of Abortions | 1.419 | -0.146 – 2.985 | 0.076 |
| Oral Contraceptive Treatment (months) | 0.011 | -0.001 - 0.025 | 0.076 |
| CYP2D6 genotypes | |||
| *1/*1 (GG) | Ref. | -------- | -------- |
| *1/*4 (GA) | 2.733 | -0.420 – 5.888 | 0.089 |
| SULT1A1 genotypes | |||
| *1/*1 (GG) | Ref. | -------- | -------- |
| *1/*2 (GA) | -2.394 | -5.426 - 0.636 | 0.122 |
| *2/*2 (AA) | 0.441 | -2.247 – 3.130 | 0.747 |
| UGT2B7 genotypes | |||
| *1/*1 (AA) | Ref. | -------- | -------- |
| *1/*2 (AC) | -0.494 | -3.454 – 2.466 | 0.744 |
| *2/*2 (CC) | -0.664 | -3.467 – 2.137 | 0.642 |
| UGT2B15 genotypes | |||
| *1/*1 (AA) | Ref. | -------- | -------- |
| *1/*2 (AC)+*2/*2 (CC) | -3.566 | -7.290 - 0.156 | 0.060 |
| ESR1 V364E genotypes | |||
| 364V/364V (TT) | Ref. | -------- | -------- |
| 364V/364E (TA) | 0.460 | -2.920 – 3.841 | 0.790 |
| 364E/364E (AA) | -1.353 | -5.322 – 2.615 | 0.504 |
| Constant (β0) | 3.761 | -0.279 – 7.802 | 0.068 |
*Model p=0.0190; Pseudo R2=0.4367 **Logit – Cumulative standard logistic distribution (F). P value< 0.05 is considered significant.
Table 10.
Multivariable logistic regression analysis or logit model* for 17βEstradiol, after stepwise forward and. backward procedure bivariable analysis.
Table 10.
Multivariable logistic regression analysis or logit model* for 17βEstradiol, after stepwise forward and. backward procedure bivariable analysis.
| Coef.** | 95% CI | p-value | |
| Family History of breast (BC) or ovary cancer (OC) | 3.747.633 | -0.714 – 8.209 | 0.100 |
| Menarche age (years) | 0.978 | 0.036 – 1.920 | 0.042 |
| CYP3A5 genotypes | |||
| *1/*3 (AG) | Ref. | -------- | -------- |
| *3/*3 (GG) | 3.434 | -1.953 – 8.821 | 0.212 |
| SULT1A1 genotypes | |||
| *1/*1 (GG) | Ref. | -------- | -------- |
| *1/*2 (GA) | 20.980 | -5068.281 – 5110.242 | 0.994 |
| *2/*2 (AA) | 20.234 | -5069.027 – 5109.496 | 0.994 |
| UGT2B7 genotypes | |||
| *1/*1 (TT)+*1/*2 (TC) | Ref. | -------- | -------- |
| *2/*2 (CC) | -1.911 | -4.998 – 1.175 | 0.225 |
| Constant (β0) | -38.556 | -5127.862 – 5050.748 | 0.988 |
*Model p=0.00209; Pseudo R2=0.5414**Logit – Cumulative standard logistic distribution (F) P value< 0.05 is considered significant (in bold).
Table 11.
Multivariable logistic regression analysis or logit model* for hot flash, after stepwise forward. and backward procedure bivariable analysis.
Table 11.
Multivariable logistic regression analysis or logit model* for hot flash, after stepwise forward. and backward procedure bivariable analysis.
| Coef.** | 95% CI | p-value | |
| Body mass index, (Kg/m2) | 0.209 | -0.0118 - 0.429 | 0.064 |
| Smoking Habit | 3.328 | -0.116 – 6.772 | 0.058 |
| UGT2B7 genotypes | |||
| *1/*1 (TT) | Ref. | -------- | -------- |
| *1/*2 (TC) | 1.431 | -1.910 – 4.773 | 0.401 |
| *2/*2 (CC) | -1.317 | -4.424 – 1.789 | 0.406 |
| UGT2B15 genotypes | |||
| *1/*1 (AA) | Ref. | -------- | -------- |
| *1/*2 (AC)+*2/*2 (CC) | 0.860 | -1.630 – 3.351 | 0.498 |
| [4OHTAM]/[TAM] | |||
| <0.087 | Ref. | -------- | -------- |
| ≥0.087 | -3.935 | -9.222 – 1.350 | 0.144 |
| [Endoxifen]/[NdesMeTAM] | |||
| <0.0075 | Ref. | -------- | -------- |
| ≥0.0075 | -0.603 | -3.074 – 1.866 | 0.632 |
| Constant (β0) | -5.792 | -12.757 – 1.172 | 0.103 |
*Model p=0.0302; Pseudo R2=0.3323 **Logit – Cumulative standard logistic distribution (F). P value < 0.05 is considered significant.
Table 12.
Multivariable logistic regression analysis or logit model* for Cramps, after stepwise forward. and backward procedure bivariable analysis.
Table 12.
Multivariable logistic regression analysis or logit model* for Cramps, after stepwise forward. and backward procedure bivariable analysis.
| Coef.** | 95% CI | p-value | |
| Height, (m) | 12.187 | -8.938 – 33.313 | 0.258 |
| Cancer stage at diagnosis | |||
| I | Ref. | -------- | -------- |
| II | -18.408 | -13849.15 - 13812.33 | 0.998 |
| III | 0.882 | -1.804 – 3.569 | 0.520 |
| UGT2B15 genotypes | |||
| *1/*1 (AA) | Ref. | -------- | -------- |
| *1/*2 (AC) | -1.598 | -4.657 – 1.460 | 0.306 |
| *2/*2 (CC) | 19.037 | -13811.71 - 13849.78 | 0.998 |
| [Endoxifen]/[NdesMeTAM] | |||
| <0.0075 | Ref. | -------- | -------- |
| ≥0.0075 | 1.069 | -1.228 – 3.367 | 0.362 |
| Constant (β0) | -18.787 | -51.506 – 13.931 | 0.260 |
*Model p=0.0206; Pseudo R2=0.4168 **Logit – Cumulative standard logistic distribution (F). P value < 0.05 is considered significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



