
Submitted:
06 August 2024
Posted:
07 August 2024
You are already at the latest version
Abstract
Very few studies, often with very small cohortes, tended to prove chemotherapy efficiency against canine agressive mammary carcinomas, either on the metastasis or on the median survival of dogs after surgery and chemo, and this was not confirmed by other studies. As a result, we lack standardized efficient protocols that exist in human cases according to their grade and stage. In this case report of a relapsing grade III solid mammary carcinoma evolving into prominent lymphatic intravascular invasion with mutifocal nodal extension (stage 4), we applied an intensive treatment combining high dose surgery and intensive adjuvant chemotherapy. This adjuvant chemo combined a carboplatin maximal-tolerated-dose chemotherapy, with doses adjusted as necessary and a metronomic chemotherapy with firocoxib, toceranib and chloraminophen, progressively added together and carefully monitored. Adapting the doses allowed to avoid adverse events and to obtain 237 days of survival with good quality of life. To our knowledge, it is the first description of such a combination of treatment. That result should be confirmed by a prospective large-scale study.
Keywords:
solid canine mammary carcinoma
; grade III
; lymphatic intravascular invasion
; stage IV
; carboplatin chemotherapy
; metronomic chemotherapy
; toceranib
; firocoxib
; chloraminophene
; QoL
1. Introduction
Very few studies have proven chemotherapy efficacy against canine aggressive mammary carcinoma. When used separately, some drugs had interesting effects on the metastases of mammary carcinoma [1] or on the median survival of small cohorts after surgery [2,3], but other studies failed to prove any effect of chemotherapy on median survival after surgery [4,5,6,7]. This lack of results is likely due the heterogeneity of the cohorts (type of surgery, histologic type/grade, accurate extension assessment and type of treatment) and the small number of patients included in most publications. As a result, we still lack standardized efficient protocols, which do exist in human cases, according to the histologic classification, grade and stage of the tumor in dogs [8]. In this case report, we describe a relapsing grade III solid mammary carcinoma evolving into prominent lymphatic intravascular invasion with multifocal LN metastatic extension (stage IV); we applied an intensive treatment combining high-dose surgery and intensive adjuvant chemotherapy. The latter combined carboplatin maximal-tolerated-dose chemotherapy, with doses adjusted as necessary, and metronomic chemotherapy with firocoxib, toceranib and chloraminophene, progressively administered and carefully monitored. Adapting the dose of each molecule prevented adverse events and resulted in 237 days of survival with good quality of life. To our knowledge, it is the first description of such a treatment combination. This treatment should be tested in a large-scale prospective study.
2. Materials and Methods
The doses of each molecule and the precise protocol are detailed in Table 1. The dog was hospitalized for 24 h for each chemotherapy treatment, as required by French law, and treated with intravenous maropitant (1 mg/kg/d) before each intravenous chemotherapy treatment at the maximum tolerated dose. Maropitant (1 mg/kg/d PO) was also systematically prescribed for 4 days following each carboplatin chemotherapy treatment.
Blood counts were performed on an Idexx Procyte Dx and biochemical analyses on an Idexx Catalyst. The results at the nadir of chemotherapy at the maximum tolerated dose and on the day of the following chemotherapy treatment are shown in Table 1.
The adverse events were graded with VCOG CTCAE version 2 [9].
The scanner was a Philips Access (16-bar unit).
The fine-needle aspiration cytology was analyzed by Delphine Rivière, Inovievet laboratory.
The histological and immunohistochemical analyses were all performed at the Oniris laboratory by F. NGuyen, in the team led by J. Abadie, by using protocols already published elsewhere by their team. The immunohistochemical analyses were performed retrospectively.
Quality of life was systematically monitored in the form of an informal discussion with the owners at each visit, and any side-effect or change in behavior was noted.
3. Case Report
3.1. Clinical Presentation
A pinscher entire female dog, 8.5 years of age, weighing 4.0 kg, was referred for a relapse of a mammary tumor on 21 January 2021. She had had a unilateral right complete mastectomy 7 months prior at her general practitioner’s clinic, but the mammary tumor (size 3 cm) had not been submitted to histopathological study, and the dog had had no ovariohysterectomy with the mastectomy. She had her season in the meantime, but the exact date is unknown. A mammary tumor relapse was observed on the scar one month prior to consultation and had grown very quickly since then. On the day of the referral consultation, the relapsed mammary tumor had developed continuously from right M3 to M5 (previous location), presenting as a 3 cm diameter cord (13.5 cm long), and extended to the left mammary chain on M4-M5 (4.8 cm long; Figure 1). The right inguinal lymph node was 3 × 4 cm large, while the left one had a normal size. No other abnormal relevant points were noted on clinical examination.
3.2. Additional Medical Tests
A tomodensitometric examination (whole body) revealed the probable infiltration of the iliac, sacral, suprasternal and right inguinal lymph nodes (LNs). No metastases were identified in the lungs, abdominal organs or brain (Figure 2).
Fine-needle aspiration of the mammary tumor and the right inguinal LN was realized. The cells were free and round or, more rarely, in clusters, which confirmed the epithelial nature of the proliferation. The cells were medium to large in size with often vacuolated basophilic cytoplasm and had round nuclei, with a high nucleocytoplasmic ratio, and a coarse, reticulated chromatin pattern enriched with several nucleoli. Anisocytosis and anisokaryosis were very significant. Frequent mitosis and some plurinucleate cells were observed, and the right inguinal lymph node was completely infiltrated by the same cells (Figure 3).
An anaplastic carcinoma was suspected. The biochemistry analyses were within normal range (however, ALT: 157 UI/L (standard value <100 and Alb/Glob ratio of 0.7)). While waiting for the results of the FNA cytology, the dog was administered firocoxib (3.56 mg/kg/d). An informed consent form for surgery, stating the extremely unfavorable prognosis, was given to the owner, who still requested surgery. The blood cell count and clotting time were within normal range.
3.3. Surgery
Six days after the CT examination, the surgery firstly consisted of ovariectomy with the removal of the four iliac and two sacral LNs, the large removal of the right mammary cord with the right inguinal LN and M2-M5 left mammectomy (Figure 4).
The following day, a sternotomy was performed to remove the suprasternal LN. For this procedure, pain was managed with an epidural injection of morphine 2 h before the surgery and an IV bolus of fentanyl (5 mg/kg) and ketamine (0.6 mg/kg) before induction, which was induced with propofol (2 mg/kg) and diazepam (0.25 mg/kg). Surgery was realized on a continuous rate infusion (CRI) of ketamine (0.6 mg/kg/h) and fentanyl (5 mg/kg/h). The CRI was gradually reduced after surgery within the next 16 h. The dog was released on amoxicillin–clavulanic acid at 12.5 mg/kg BID for 5 days, firocoxib at 3.56 mg/kg once a day and furosemide at 1 mg/kg/d 5d (to reduce pelvic limb edema). A chloraminophene (2 mg every other day, 6.9 mg/m2 EOD) treatment was induced 10 days after the surgery. The wound dehisced in the right distal part, and a second surgery 11 days after the initial surgery was performed to close the wound.
3.4. Histological Description
The histopathological examination indicated a grade III solid mammary carcinoma evolving towards prominent lymphatic intravascular carcinomatosis with numerous neoplastic emboli and multifocal LN metastatic extension (all the lymph nodes removed were infiltrated, including the suprasternal LN) (Figure 5), corresponding to stage IV in the WHO classification (T3N2M0). The margins were free of tumoral tissue.
Immunohistochemistry was performed on the tumor and on the infiltrated lymph nodes. The tumor was triple-negative and non-basal-like (ER-negative tumor and 1/1000 positive cells in the LN; PR- and HER2-negative in all localizations, with negative cytokeratin CK5/6-positive cells <1%).
3.5. Adjuvant Treatment
Fourteen days after the initial surgery, the wound healing was good, and carboplatin chemotherapy (270 mg/m2) was initiated, with maropitant (1 mg/kg/d) being prescribed for 4 days after each chemotherapy treatment; the chloraminophene treatment was continued every other day, and firocoxib was administered every day, although a suspension of the latter was prescribed for 7 days after the carboplatin chemotherapy to avoid the risk of inducing renal failure (owner misunderstanding).
A second carboplatin chemotherapy treatment was performed 3 weeks later (202 mg/m2 due to neutropenia; Table 1) with short suspension of firocoxib.
When a vulvar edema appeared, firocoxib treatment was restored. Three weeks later, the prescapular lymph nodes were enlarged (L: 2 cm; R: 3.5 cm); fine-needle aspiration cytology showed infiltration of these LNs by the same mammary tumor cells. The dog was administered toceranib (2.03 mg/kg EOD), and 4 days later, the two LNs were removed. The histological examination confirmed their infiltration by tumor cells. The next carboplatin chemotherapy treatment was performed 1.5 month after the second one, to avoid wound dehiscence, and the next chemotherapy treatments (six in toto) were performed every 4 weeks (see Table 1). For each chemotherapy treatment, chloraminophene was stopped 2 days before and restored 3 days after the treatment, firocoxib was stopped the day before and restored 8 days later, and the toceranib was stopped the day before and restored 5 days later. Toceranib and chloraminophene were given alternately. Carboplatin doses were gradually reduced to 150 mg/m2 due to neutropenia on the day of chemotherapy. After the sixth carboplatin dose, only firocoxib, chloraminophene and toceranib were maintained.
3.6. Quality of Life and Follow-Up
The dog had very good quality of life during the whole treatment period, with no weight loss (rather, weight gain from 4 to 4.9 kg), stable appetite, normal activity and interaction with her owners, with normal habits, and usual play phases. After the prescapular LN invasion, she did not show other relapses, to the point that the owners took her on a walking holiday 10 days after the sixth chemotherapy treatment. After a walk, she suddenly developed a ventral hematoma with inguinal lymph node reaction. Firocoxib chloraminophene and toceranib treatments were stopped by the veterinary practitioner. Five days later, when they came back for a referral follow-up, the hematoma had shrunk. There was no sign of local recurrence of the mammary tumor, but an enlarged inguinal LN. The fine-needle aspiration of this LN contained only inflammatory cells and did not indicate tumoral infiltration. The clotting time was within normal values. The blood cell count showed thrombocytopenia, confirmed with a blood smear examination. An ultrasound abdominal examination did not show any abnormal LNs. The dog was administered amoxicillin–clavulanic acid for 10 days, and the hematoma resolved.
Five weeks after the last carboplatin chemotherapy treatment, firocoxib and toceranib were reinstated despite persistent thrombocytopenia. Flaccid tail, evolving into posterior paresis within 24 h presented very suddenly 7 days later. A CT examination (Figure 6) revealed several spinal metastases, but no other locations of metastases, and the dog died on the next day. In order to respect the owners’ wishes, necropsy was not performed, nor was vertebral histology. The time from initial surgery (carried out in our referral center) to death from the mammary tumor was 237 days (7 months and 25 days).
4. Discussion
In the new histologic classification proposed by Goldschmidt in 2011 [10], solid carcinomas are considered highly malignant canine mammary carcinomas. They share the poorest prognosis with anaplastic carcinomas, comedocarcinomas, and “carcinoma and malignant myoepitheliomas”, if inflammatory carcinomas are excluded [11,12,13]. In the reported case, the tumor was larger than 5 cm; grew very fast, with poor cellular differentiation; invaded lymphatic vessels, with severe carcinomatosis; and infiltrated sacral, iliac and suprasternal LNs. All of these elements were very-poor-prognosis parameters [11,14]. Histologic stage IIIb has the worst prognosis, with a median survival time of 163 days after surgery [15,16]. Moreover, with numerous infiltrated lymph nodes, without other tissue infiltration demonstrated by tomodensitometric examination, the stage of the reported tumor was at least IV, which further worsened the prognosis [12]. As mammary carcinoma cells tend to invade bone marrow [17,18,19,20], we cannot be certain that bone marrow metastases were not already present, but they were not visible upon the first tomodensitometric examination as bone lesions. We could have carried out a bone marrow puncture and used the cell block technique or a biopsy to look for the presence of epithelial cells in the marrow by immunohistochemistry examination [21], but the round cellular appearance of the tumor cells and their CK5/6 negativity would probably have produced a false-negative result in that case. A cell-free DNA test could have detected the mammary tumor cells, but the detection rate in blood is only about 61%, and that in bone marrow is unknown [22].
Very few published case series reported an effect of maximum-tolerated-dose chemotherapy alone on specific survival in dogs bearing canine mammary tumors [1,2,3,4,5,6,7,23,24]. Carboplatin alone [3], in addition to naltrexone [7] or with concurrent metronomic cyclophosphamide chemotherapy [24] seemed to have an interesting effect on survival in female dogs with mammary carcinomas. Cox2 overexpression promotes angiogenesis and invasion [25]; the use of anti-cox2 anti-inflammatory drugs has previously shown an effect on certain types of mammary carcinoma, namely, inflammatory mammary carcinomas [23,26,27,28,29]. It seems that firocoxib could also promote the apoptosis of mammary cancer cells, particularly in the case of triple-negative tumors, in vitro and in vivo [30]. In Lavalle’s study, carboplatin was first instated without anti-inflammatory drugs, which were given after the last chemotherapy treatment for 6 months [3]. Previously published studies indicated that toceranib had effects on inflammatory mammary carcinomas [28,31], which also invade lymphatic vessels, as did the solid carcinoma described in our case.
In the described case, the owner still requested treatment in spite of the extremely unfavorable prognosis. Given such an aggressive mammary carcinoma, growing very quickly, the treatment had to be intensive to hopefully have an effect. In multi-drug chemotherapy, “the combined agents should possess a demonstrable individual activity against the tumor type being treated, with the potential for synergistic and/or additive activity, as well as disparate mechanisms of action, and as a result distinct adverse event (AE) profiles. Moreover, the agents should ideally be able to be administered concurrently at an optimized therapeutic dose and interval” [32]. The proposed treatment consisted in high-dose surgery and combined maximum-tolerated-dose and metronomic chemotherapy treatments with carboplatin, firocoxib, chloraminophene and toceranib. To the best of our knowledge, metronomic chemotherapy and toceranib were previously used together after completing carboplatin sessions, and not at the same time, to treat osteosarcoma [33], and metronomic chemotherapy and piroxicam or firocoxib were administered after completing carboplatin sessions [3]. In a study by London, which included toceranib (2.75 mg/kg EOD), piroxicam (0.3 mg/kg) and cyclophosphamide (10 mg/m2 EOD), greater toxicity was described than with piroxicam (0.3 mg/kg) and cyclophosphamide (10 mg/m2 EOD) alone [33]. The combination of cyclophosphamide, cox2 inhibitors and toceranib at lower doses has been proven to be well tolerated in dogs bearing inflammatory carcinomas [31]. Toceranib phosphate was administered in the latter study at doses from 2.4 to 2.7 mg/kg PO on a Monday–Wednesday–Friday schedule, and cyclophosphamide was given at a dose of 12.5 mg/m2/d PO. In another study, which included piroxicam at 0,3 mg/kg and toceranib at 3.25 mg/kg EOD, 12% of tumor-bearing dogs developed azotemia (where one case was grade IV), and few developed gastrointestinal adverse effects [34]. In our study, the protocol was progressively implemented with the introduction of the different molecules in stages. The dose of carboplatin was adapted and progressively reduced according to the neutropenia at nadir and on the day of each chemotherapy. We selected a lower dose of toceranib compared with the doses described above in the other studies for three reasons: its frequent side-effects at the marketing authorization doses [33] or slightly lowered doses [34]; the risk of cumulative effects on liver or kidney function with firocoxib and carboplatin; lastly, the fact that using a 15 mg tablet would have led to a large overdose (3.75 mg/kg). As described in a previous study, where female dogs bearing mammary carcinoma were treated with carprofen for 3 months without any effect on renal function [35], no azotemia nor proteinuria occurred with firocoxib, in spite of its association with toceranib and carboplatin. No hepatitis, anemia, diarrhea nor vomiting occurred in our case either, in spite of the concomitant use of carboplatin, toceranib and firocoxib. No thrombocytopenia was noted during treatment, except at the end. Such thrombocytopenia has been previously described [24], but as having occurred cumulatively during the carboplatin and metronomic cyclophosphamide regimen. In Machado’s study [24], the dose of carboplatin used was 300 mg/m2 and was not changed in spite of progressive thrombocytopenia during the treatment. In published trials with ITK and concomitant maximal-tolerated-dose chemotherapy, it has been shown that chemotherapy doses had to be reduced. For instance, in a study combining toceranib and carboplatin in tumor-bearing dogs, carboplatin was used at the dose of 200 mg/m2 and toceranib at 2.75 mg/kg EOD. No unique or novel adverse events were observed. A dose of carboplatin of 200 mg/m2 induced neutropenia (grade I), anemia (grade I) and thrombocytopenia (grade I–III), as well as other events of low grade (gastrointestinal events, hypertension, etc.). Escalating carboplatin doses to 250 or 225 mg/m2 increased myelosuppressive effects [36]. The thrombocytopenia we noted occurred around the sixth dose of carboplatin and its subsequent discontinuation; it could have occurred due to the bone metastatic process, the cumulative/amplifying effect of the myelosuppression-associated drugs carboplatin, chloraminophene and toceranib or the dysimmune paraneoplastic mechanism. It did not resolve with chloraminophene and toceranib discontinuation and shortly preceded the discovery of spinal metastases. Paraneoplastic thrombocytopenia is more likely, either due to a dysimmune mechanism or the invasion of bone marrow by metastatic carcinoma cells (as shown by the tomodensitometric examination) or both; as we did not carry out a bone marrow examination at the time, we cannot conclude as to the cause of the thrombocytopenia.
The initial tumor was further tested after the dog’s death with immunohistochemistry and was subsequently found to be negative for C-kit and Cox2 (the histological and immunohistological examinations were carried out by Dr NGuyen at Abadie’s laboratory). We could not test for PDGF-R receptors due to a lack of antibodies against PDGR-R; firocoxib and toceranib may have had indirect effects on the tumor microenvironment or through PDGF-R.
Even if we have no proof that the chemotherapy attempted really prolonged this dog’s life, at the very least, we were able to observe that this protocol gave her very good quality of life and did not result in any serious side-effects, apart from grade 3 non-clinical neutropenia. Her quality of life was closely monitored based on a sustained and constant dialogue with the owner [37] in order to protect the dog from over-treatment, with the owner having been actively alerted with regard to this point at the start of the treatment.
5. Conclusions
A female dog suffering from a severely aggressive mammary carcinoma associated with a very poor prognosis was treated with radical surgery and multimodal therapy combining chemotherapy at the maximum tolerated dose and metronomic therapy, firocoxib and toceranib. To the best of our knowledge, such a treatment has never been published. Adapting the doses of carboplatin, toceranib, firocoxib and chloraminophene prevented the adverse events of the adjuvant treatments and the associated poor quality of life. The dog had a normal life, with no loss of activity, and did continue to interact with her owners, even more than before. The treatment, including the surgeries and the chemotherapy sessions, resulted in 237 days of survival. However, this is only one case; only a prospective study in a cohort of similar cases could determine whether this treatment could prolong the median specific survival time compared with a control population, whether it is safe and whether it could be applied in highly aggressive canine mammary carcinomas.
Author Contributions
Conceptualization, C.B.-L., methodology, C.B.-L.; software, C.B.-L.; validation, C.B.-L. and E.L.; formal analysis, C.B.-L.; investigation, C.B.-L. and E.L.; resources, C.B.-L.; data curation, C.B.-L.; writing—original draft preparation, C.B.-L.; writing—review and editing, C.B.-L. and E.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research study received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study, because the ethical concern was discussed directly with the owner from the first consultation. We knew the prognosis was poor in the very short term, and the owner was determined to try treatment, despite of this poor prognosis. The discussion with him focused on the risk of relentless treatment, and we agreed together from the beginning that the veterinary team would stop treatment and urge him and his family to euthanize the dog if she showed any obvious decline in quality of life.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to warmly thank the Oniris laboratory team and particularly NGuyen Frederique for carrying out the immunohistochemistry analysis free of charge, which made it possible to better characterize the tumor and its nodal metastases.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Suryawanshi, R.V. Assessment of Efficacy and Toxicity of Cyclophosphamide Chemotherapy in Canines with Malignant Mammary Tumor: A Retrospective Study. Vet. Med. Int. 2021, 2021, 5520603. [Google Scholar] [CrossRef] [PubMed]
- Karayannopoulou, M.; Kaldrymidou, E.; Constantinidis, T.C.; Dessiris, A. Adjuvant Post-operative Chemotherapy in Bitches with Mammary Cancer. J. Vet. Med. A 2001, 48, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Lavalle, G.E.; De Campos, C.B.; Bertagnolli, C.; Cassali, G.D. Canine Malignant Mammary Gland Neoplasms with Advanced Clinical Staging Treated with Carboplatin and Cyclooxygenase Inhibitors. In Vivo 2012, 26, 375–380. [Google Scholar] [PubMed]
- Tran, C.M.; Moore, A.S.; Frimberger, A.E. Surgical treatment of mammary carcinomas in dogs with or without postoperative chemotherapy. Vet. Comp. Oncol. 2014, 14, 252–262. [Google Scholar] [CrossRef] [PubMed]
- Marconato, L.; Lorenzo, R.M.; Abramo, F.; Ratto, A.; Zini, E. Adjuvant gemcitabine after surgical removal of aggressive malignant mammary tumours in dogs. Vet. Comp. Oncol. 2008, 6, 90–101. [Google Scholar] [CrossRef] [PubMed]
- Simon, D.; Schoenrock, D.; Baumgartner, W.; Nolte, I. Postoperative Adjuvant Treatment of Invasive Malignant Mammary Gland Tumors in Dogs with Doxorubicin and Docetaxel. J. Vet. Intern. Med. 2006, 20, 1184–1190. [Google Scholar] [CrossRef] [PubMed]
- Machado, M.C.; da Costa-Neto, J.M.; Portela, R.D.; D’Assis, M.J.M.H.; Martins-Filho, O.A.; Barrouin-Mello, S.; Ferreira Borges, N.; Silva, F.L.; Estrela-Lima, A. The effect of naltrexone as a carboplatin chemotherapy-associated drug on the immune response, quality of life and survival of dogs with mammary carcinoma. PLoS ONE 2018, 13, e0204830. [Google Scholar] [CrossRef] [PubMed]
- Valdivia, G.; Alonso-Diez, Á.; Pérez-Alenza, D.; Peña, L. From Conventional to Precision Therapy in Canine Mammary Cancer: A Comprehensive Review. Front. Vet. Sci. 2021, 8, 623800. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, A.K.; Atherton, M.; Bentley, R.T.; Boudreau, C.E.; Burton, J.H.; Curran, K.M.; Dow, S.; Giuffrida, M.A.; Kellihan, H.B.; Mason, N.J.; et al. Veterinary Cooperative Oncology Group-Common Terminology Criteria for Adverse Events (VCOG-CTCAE v2) following investigational therapy in dogs and cats. Vet. Comp. Oncol. 2021, 19, 311–352. [Google Scholar] [CrossRef]
- Goldschmidt, M.; Peña, L.; Rasotto, R.; Zappulli, V. Classification and grading of canine mammary tumors. Vet. Pathol. 2011, 48, 117–131. [Google Scholar] [CrossRef]
- Abadie, J.; Nguyen, F.; Loussouarn, D.; Peña, L.; Gama, A.; Rieder, N.; Belousov, A.; Bemelmans, I.; Jaillardon, L.; Ibisch, C.; et al. Canine invasive mammary carcinomas as models of human breastcancer. Part 2: Immunophenotypes and prognostic significance. Breast Cancer Res. Treat 2018, 167, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Peña, L.; De Andrés, P.J.; Clemente, M.; Cuesta, P.; Pérez-Alenza, M.D. Prognostic Value of Histological Grading in Noninflammatory Canine Mammary Carcinomas in a Prospective Study with Two-Year Follow-Up: Relationship with Clinical and Histological Characteristics. Vet. Pathol. 2013, 50, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Canadas, A.; França, M.; Pereira, C.; Vilaça, R.; Vilhena, H.; Tinoco, F.; Silva, M.J.; Ribeiro, J.; Medeiros, R.; Oliveira, P.; et al. Canine Mammary Tumors: Comparison of Classification and Grading Methods in a Survival Study. Vet. Pathol. 2019, 56, 208–219. [Google Scholar] [CrossRef] [PubMed]
- de Araújo, M.R.; Campos, L.C.; Ferreira, E.; Cassali, G.D. Quantitation of the Regional Lymph Node Metastatic Burden and Prognosis in Malignant Mammary Tumors of Dogs. J. Vet. Intern. Med. 2015, 29, 1360–1367. [Google Scholar] [CrossRef] [PubMed]
- Chocteau, F.; Abadie, J.; Loussouarn, D.; Nguyen, F. Proposal for a Histological Staging System of Mammary Carcinomas in Dogs and Cats. Part 1: Canine Mammary Carcinomas. Front. Vet. Sci. 2019, 6, 388. [Google Scholar] [CrossRef]
- Nguyen, F.; Peña, L.; Ibisch, C.; Loussouarn, D.; Gama, A.; Rieder, N.; Belousov, A.; Campone, M.; Abadie, J. Canine invasive mammary carcinomas as models of human breast cancer. Part 1: Natural history and prognostic factors. Breast Cancer Res. Treat. 2018, 167, 635–648. [Google Scholar] [CrossRef] [PubMed]
- Marconato, L.; Facchinetti, A.; Zanardello, C.; Rossi, E.; Vidotto, R.; Capello, K.; Melchiotti, E.; Laganga, P.; Zamarchi, R.; Vascellari, M. Detection and Prognostic Relevance of Circulating and Disseminated Tumour Cell in Dogs with Metastatic Mammary Carcinoma: A Pilot Study. Cancers 2019, 11, 163. [Google Scholar] [CrossRef] [PubMed]
- Jaillardon, L.; Barthélemy, A.; Goy-Thollot, I.; Pouzot-Nevoret, C.; Fournel-Fleury, C. Mammary gland carcinoma in a dog with peripheral blood and bone marrow involvement associated with disseminated intravascular coagulation. Vet. Clin. Pathol. 2012, 41, 261–265. [Google Scholar] [CrossRef]
- Clemente, M.; Pérez-Alenza, M.D.; Peña, L. Metastasis of canine inflammatory versus non-inflammatory mammary tumours. J. Comp. Pathol. 2010, 143, 157–163. [Google Scholar] [CrossRef]
- Cooley, D.M.; Waters, D.J. Skeletal metastasis as the initial clinical manifestation of metastatic carcinoma in 19 dogs. J. Vet. Intern. Med. 1998, 12, 288–293. [Google Scholar] [CrossRef]
- Taylor, B.E.; Leibman, N.F.; Luong, R.; Loar, A.S.; Craft, D.M. Detection of carcinoma micrometastases in bone marrow of dogs and cats using conventional and cell block cytology. Vet. Clin. Pathol. 2013, 42, 85–91. [Google Scholar] [CrossRef]
- Flory, A.; Kruglyak, K.M.; Tynan, J.A.; McLennan, L.M.; Rafalko, J.M.; Fiaux, P.C.; Hernandez, G.E.; Marass, F.; Nakashe, P.; Ruiz-Perez, C.A.; et al. Clinical validation of a next-generation sequencing-based multi-cancer early detection “liquid biopsy” blood test in over 1000 dogs using an independent testing set: The CANcer Detection in Dogs (CANDiD) study. PLoS ONE 2022, 17, e0266623. [Google Scholar] [CrossRef] [PubMed]
- Arenas, C.; Peña, L.; Granados-Soler, J.L.; Pérez-Alenza, M.D. Adjuvant therapy for highly malignant canine mammary tumours: Cox-2 inhibitor versus chemotherapy: A case–control prospective study. Vet. Rec. 2016, 179, 125. [Google Scholar] [CrossRef]
- Machado, M.C.; Yamamoto, P.A.; Pippa, L.F.; de Moraes, N.V.; Neves, F.M.F.; Portela, R.D.; Barrouin-Melo, S.M.; Hielm-Björkman, A.; Godoy, A.L.P.C.; Estrela-Lima, A. Pharmacokinetics of Carboplatin in Combination with Low-Dose Cyclophosphamide in Female Dogs with Mammary Carcinoma. Animals 2022, 12, 3109. [Google Scholar] [CrossRef] [PubMed]
- Queiroga, F.L.; Pires, I.; Lobo, L.; Lopes, C.S. The role of Cox-2 expression in the prognosis of dogs with malignant mammary tumours. Res. Vet. Sci. 2010, 88, 441–445. [Google Scholar] [CrossRef]
- Campos, C.B.D.E.; Lavalle, G.E.; Monteiro, L.N.; Pêgas, G.R.A.; Fialho, S.L.; Balabram, D. Adjuvant thalidomide and metronomic chemotherapy for the treatment of canine malignant mammary gland neoplasms. In Vivo 2018, 32, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- De Souza, C.H.; Toledo-Piza, E.; Amorin, R.; Barboza, A.; Tobias, K.M. Inflammatory mammary carcinoma in 12 dogs: Clinical features, cyclooxygenase-2 expression, and response to piroxicam treatment. Can. Vet. J. 2009, 50, 506–510. [Google Scholar]
- Rossi, F.; Sabattini, S.; Vascellari, M.; Marconato, L. The impact of toceranib, piroxicam and thalidomide with or without hypofractionated radi ation therapy on clinical outcome in dogs with inflammatory mammary carcinoma. Vet. Comp. Oncol. 2018, 16, 497–504. [Google Scholar] [CrossRef]
- Vieira, T.C.; Oliveira, E.A.; Dos Santos, B.J.; Souza, F.R.; Veloso, E.S.; Nunes, C.B.; Del Puerto, H.L.; Cassali, G.D. COX-2 expression in mammary invasive micropapillary carcinoma is associated with prognostic factors and acts as a potential therapeutic target in comparative oncology. Front. Vet. Sci. 2022, 12, 983110. [Google Scholar] [CrossRef]
- Brandi, A.; de Faria Lainetti, P.; Elias, F.; Rodrigues, M.M.P.; Fagundes Moraes, L.; Laufer-Amorim, R.; de Camargo, L.S.; Salles Gomes, C.O.M.; Fonseca-Alves, C.E. Firocoxib as a Potential Neoadjuvant Treatment in Canine Patients with Triple-Negative Mammary Gland Tumors. Animals 2022, 13, 60. [Google Scholar] [CrossRef]
- Alonso-Miguel, D.; Valdivia, G.; García-San José, P.; Alonso-Diez, Á.; Clares, I.; Portero, M.; Peña, L.; Pérez-Alenza, M.D. Clinical outcome of dogs diagnosed with canine inflammatory mammary cancer treated with metronomic cyclophosphamide, a cyclooxygenase-2 inhibitor and toceranib phosphate. Vet. Comp. Oncol. 2022, 20, 179–188. [Google Scholar] [CrossRef] [PubMed]
- DeVita, V.T.; Chu, E. Principles of Medical Oncology. In Cancer: Principles and Practice of Oncology, 8th ed.; DeVita, V.T., Rosenberg, S.A., Eds.; Lippincott-Raven Publishers: Philadelphia, PA, USA, 2008; pp. 340–342. [Google Scholar]
- London, C.A.; Gardner, H.L.; Mathie, T.; Stingle, N.; Portela, R.; Pennell, M.L.; Clifford, C.A.; Rosenberg, M.P.; Vail, D.M.; Williams, L.E.; et al. Impact of Toceranib/Piroxicam/Cyclophosphamide Maintenance Therapy on Outcome of Dogs with Appendicular Osteosarcoma following Amputation and Carboplatin Chemotherapy: A Multi-Institutional Study. PLoS ONE 2015, 10, e0124889. [Google Scholar] [CrossRef] [PubMed]
- Chon, E.; McCartan, L.; Kubicek, L.N.; Vail, D.M. Safety evaluation of combination toceranib phosphate (Palladia®) and piroxicam in tumour-bearing dogs (excluding mast cell tumours): A phase I dose-finding study. Vet. Comp. Oncol. 2012, 10, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Vargas Estrada, C.R.; Firmo, B.F.; Belchior Vela, D.; Maronezi, M.C.; Ramirez Uscategui, R.A.; Gasser, B.; Rossi Feliciano, M.A.; Pavan, L.; Nogueira Aires, L.P.; Piovan Lima, G.; De Nardi, A.B. Ultrasonographic assessment of renal perfusion in bitches with mammary carcinoma treated with long-term carprofen. Sci. Rep. 2021, 11, 23277. [Google Scholar] [CrossRef] [PubMed]
- Wouda, R.M.; Hocker, S.E.; Higginbotham, M.L. Safety evaluation of combination carboplatin and toceranib phosphate (Palladia) in tumour-bearing dogs: A phase I dose finding study. Vet. Comp. Oncol. 2018, 16, E52–E60. [Google Scholar] [CrossRef]
- Beata, C.; Beaudu-Lange, C.; Muller, C. Jusqu’où va-t-on dans les soins donnés à nos animaux de compagnie? Revue Vétérinaire Clinique 2021, 56, 157–169. [Google Scholar] [CrossRef]
Figure 1.
Aspect of right mammary scar on day of referral consultation.

Figure 2.
Tomodensitometric examination before surgery. The right inguinal, iliac medial (a), lateral (b), sacral (c) and suprasternal (d) lymph nodes were increased in size and rounded in shape, with a strong homogeneous enhancement following the injection of the contrast medium, and were strongly suspected to be infiltrated. No metastases were identified in the lungs, abdominal organs or brain.
Figure 2.
Tomodensitometric examination before surgery. The right inguinal, iliac medial (a), lateral (b), sacral (c) and suprasternal (d) lymph nodes were increased in size and rounded in shape, with a strong homogeneous enhancement following the injection of the contrast medium, and were strongly suspected to be infiltrated. No metastases were identified in the lungs, abdominal organs or brain.
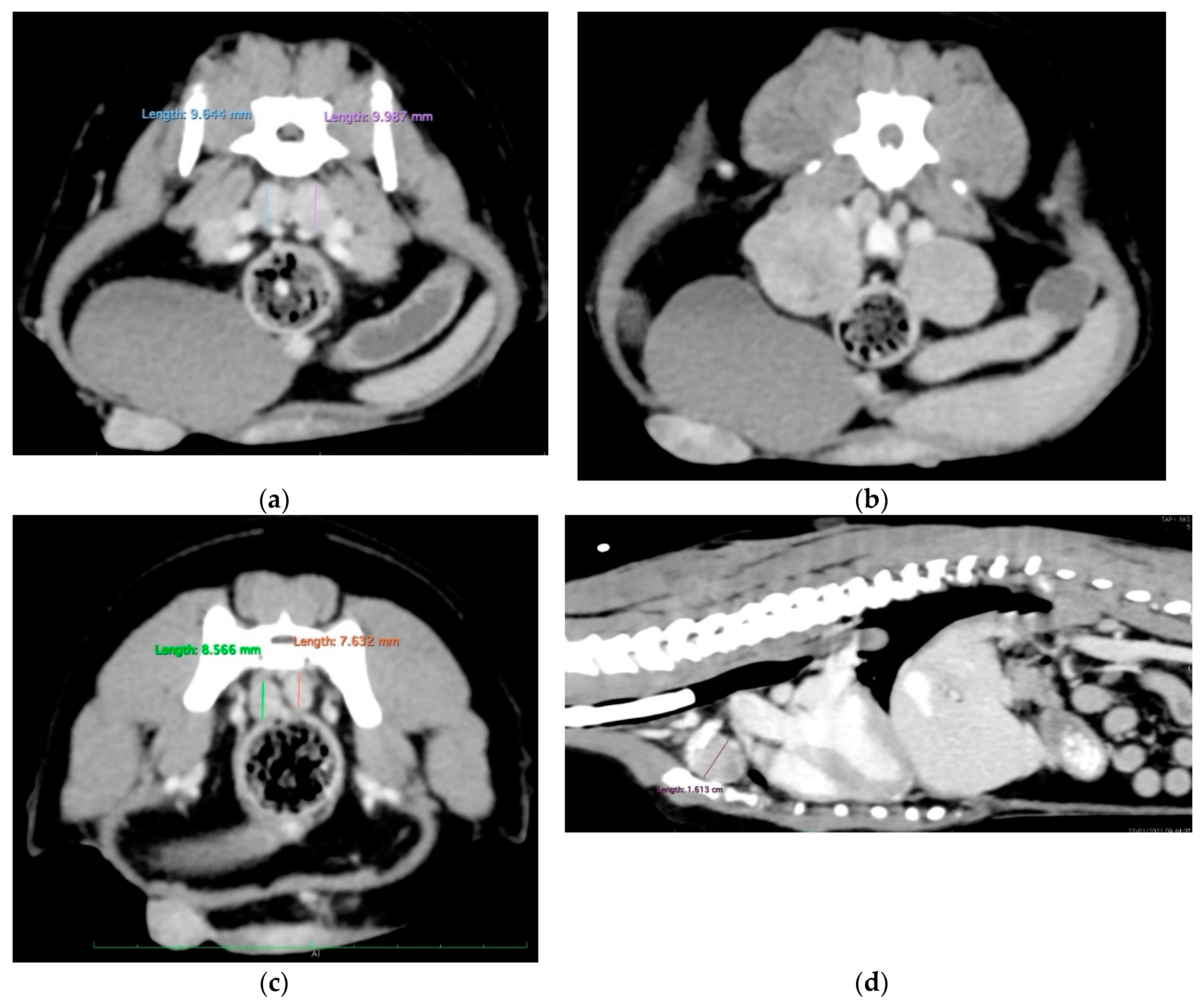
Figure 3.
Fine-needle aspiration of mammary tumor and right inguinal LN. (a) Magnification: ×10. The cells were free and round or, more rarely, in clusters, which confirmed the epithelial nature of the proliferation. (b) Magnification: ×100. The cells were medium to large in size with often vacuolated basophilic cytoplasm and had round nuclei, with a high nucleocytoplasmic ratio, and a coarse, reticulated chromatin pattern enriched with several nucleoli. Anisocytosis and anisokaryosis were very significant. Frequent mitosis and some plurinucleate cells were observed. (c) Magnification: ×100. The inguinal lymph node was completely infiltrated by the same cells. An anaplastic carcinoma was suspected. Photography: Delphine Rivière; @inovievet, Montpellier, France.
Figure 3.
Fine-needle aspiration of mammary tumor and right inguinal LN. (a) Magnification: ×10. The cells were free and round or, more rarely, in clusters, which confirmed the epithelial nature of the proliferation. (b) Magnification: ×100. The cells were medium to large in size with often vacuolated basophilic cytoplasm and had round nuclei, with a high nucleocytoplasmic ratio, and a coarse, reticulated chromatin pattern enriched with several nucleoli. Anisocytosis and anisokaryosis were very significant. Frequent mitosis and some plurinucleate cells were observed. (c) Magnification: ×100. The inguinal lymph node was completely infiltrated by the same cells. An anaplastic carcinoma was suspected. Photography: Delphine Rivière; @inovievet, Montpellier, France.

Figure 4.
(a) Aspect of mammary tumor relapse on day of surgery. The tumor had further grown within 6 days (see, for comparison, Figure 1). An ovariectomy was performed first, with the removal of iliac and sacral lymph nodes, followed by a complete radical excision of the right relapsing cord, which had grown fast in a week. The surgical plan was drawn with a red pencil. (b) The scar after the surgery. The following day, a sternotomy was performed to remove the suprasternal LN. (c) The removed sacral and iliac lymph nodes.
Figure 4.
(a) Aspect of mammary tumor relapse on day of surgery. The tumor had further grown within 6 days (see, for comparison, Figure 1). An ovariectomy was performed first, with the removal of iliac and sacral lymph nodes, followed by a complete radical excision of the right relapsing cord, which had grown fast in a week. The surgical plan was drawn with a red pencil. (b) The scar after the surgery. The following day, a sternotomy was performed to remove the suprasternal LN. (c) The removed sacral and iliac lymph nodes.

Figure 5.
(a) Histopathological examination of the mammary tumor and lymph nodes. The mammary tumor was invasive ((a) ×10) with lymphatic intravascular invasion ((b) ×20). The examination indicated a grade III solid mammary carcinoma. Multifocal LN metastatic extension was noted ((c) ×10). Photography: @Oniris, Nantes, France.
Figure 5.
(a) Histopathological examination of the mammary tumor and lymph nodes. The mammary tumor was invasive ((a) ×10) with lymphatic intravascular invasion ((b) ×20). The examination indicated a grade III solid mammary carcinoma. Multifocal LN metastatic extension was noted ((c) ×10). Photography: @Oniris, Nantes, France.
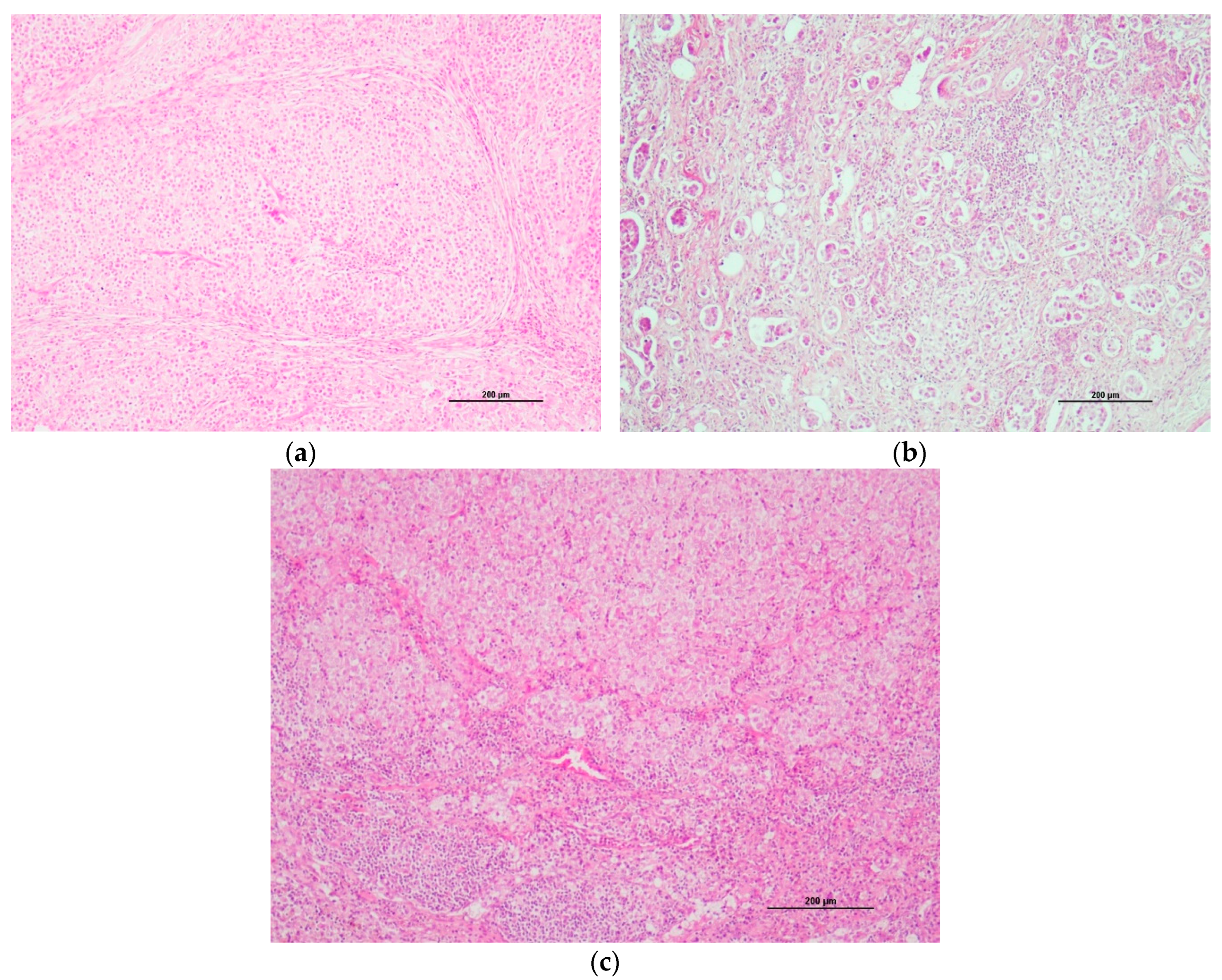
Figure 6.
The CT scan examination at the end. The C6, L3, L6, L7, S1 and S2 vertebral bodies showed cookie-cutter lesions. (The lesion at L6 severely invaded the medullary canal; not shown here.).
Figure 6.
The CT scan examination at the end. The C6, L3, L6, L7, S1 and S2 vertebral bodies showed cookie-cutter lesions. (The lesion at L6 severely invaded the medullary canal; not shown here.).
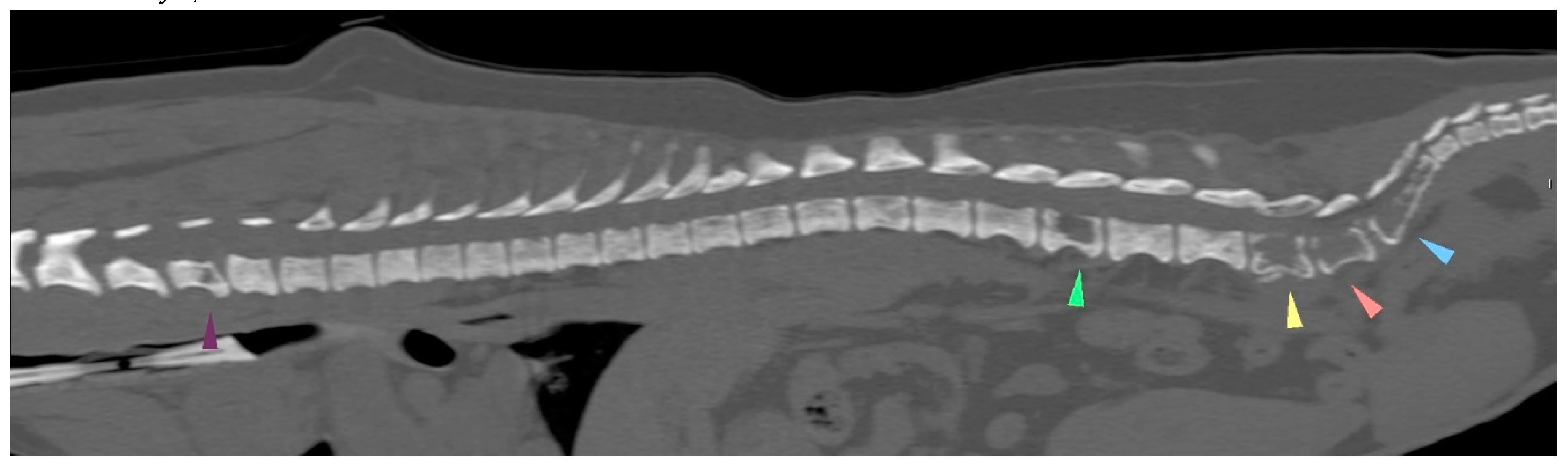

Table 1.
Clinical follow-up data, serial blood cell counts and biochemistry results. SV: interval of standard values; PCV, packed cell volume; RBCs, red blood cells; WBCs, white blood cells; ALT, alanine amino transferase. Toxicity grades specified according to VCOG CTCAE version 2.
Table 1.
Clinical follow-up data, serial blood cell counts and biochemistry results. SV: interval of standard values; PCV, packed cell volume; RBCs, red blood cells; WBCs, white blood cells; ALT, alanine amino transferase. Toxicity grades specified according to VCOG CTCAE version 2.
| Date And carboplatin chemotherapy |
Chloraminophene 2 mg EOD |
Firocoxib 14,2 mg/d |
toceranib 10 mg | clinical examination and treatment steps | weight (kg) | RBCs (10^12/L) SV [5,6-8,8] | PCV (%) SV [37,3-61,7] | Hb (g/dL) SV [13,1-20,5] | WBCs (10^9/L) SV [5,05-16,7] | Neutrophils (10^9/L) SV [2,9-11,6] | Monocytes (10^9/L) SV [0,16-1,12] | Lymphocytes (10^9/L) SV [1-5,1] | Platelets (10^3/µL) SV [148-484] | ALT (IU/L) SV [10-125] | Blood Creatinine (mg/L) SV [5-18] |
| 21/01/28 | from 21/02/07 | from 21/02/09 3,56 mg/kg |
21/01/27-28 surgery in two steps 21/02/06 wound dehiscence (surgery on 21/02/08) |
4,0 | 7,85 | 49,4 | 17,3 | 9,33 | 7,83 | 0.,61 | 0,68 | 195 | 157 | 5 | |
| 21/02/11 chemotherapy N°1, 270 mg/m² | stop 21/02/11 restart 21/02/18 to 21/03/05 |
to 21/03/05 3,56 mg/kg |
4 | ||||||||||||
| 21/03/05 chemotherapy N°2, 202 mg/m² | stop 21/03/05 restart 21/03/13 to 21/04/23 |
stop | 4,1 | 7,27 | 46,8 | 18,3 | 3,6 | 1,85 grade 1 |
0,14 | 1,62 | 198 | 160 | 5 | ||
| 21/03/18 | vulvar edema | 7,36 | 46,5 | 15,9 | 6,16 | 2,94 grade 1 |
0,36 | 2,85 | 65 grade 2 |
||||||
| 21/03/26 | restart | 2,43 mg/kg EOD | vulvar edema, granulation of mammary tissue in left previous M4-M5 location increased Left (2cm) and right (3,5 cm) prescapular LN. |
4,1 | 7,09 | 44,9 | 15,4 | 6,77 | 4,41 | 0,23 | 2,12 | 175 | 88 | 6,4 | |
| 21/03/30 | surgical removal of Left and Right prescapular LN | ||||||||||||||
| 21/04/16 | correct surgical scar | 4,0 | |||||||||||||
| 21/04/23 chemotherapy N°3 162 mg/m² | stop 21/04/21 restart 21/04/26 2 mg one in 3 days |
stop 21/04/22 restart 21/05/01 3,39 mg/kg |
stop 21/04/22 restart 21/04/28 2,38 mg/kg |
4,2 | 6,92 | 44 | 15,1 | 4,69 | 3,94 | 0,3 | 0,19 | 314 | 56 | 5,8 | |
| 21/05/10 | normal clinical examination | 6,97 | 45,1 | 18,8 | 3,06 | 1,93 Grade 1 |
0,08 | 1,05 | 220 | 41 | 10,5 | ||||
| 21/05/20 chemo carboplatin N°4 151 mg/m² |
stop 21/05/18 restart 21/06/29 2 mg one in 3 days |
stop 21/05/19 restart 21/07/03 2,91 mg/kg |
stop 21/05/19 restart 21/07/01 2,04 mg/kg |
normal clinical examination | 4,89 | 7,75 | 50,3 | 16,8 | 4,18 | 3,52 | 0,27 | 0,17 | 266 | ||
| 21/06/05 | stop 21/06/13 | 7,61 | 49 | 17,0 | 2,75 | 1,61 Grade 1 |
0,06 | 1,08 | 145 | 32 | 7,3 | ||||
| 21/06/16 | 8,05 | 52,5 | 15,4 | 4,18 | 2,61 Grade 1 |
0,06 | 1,51 | 158 | |||||||
| 21/06/25 chemotherapy N°5 carboplatin 151 mg/m² |
restart 21/06/29 | stop 21/06/24 | stop 21/06/23 | normal clinical examination | 4,850 | 7,06 | 45,9 | 15,4 | 3,55 | 2,67 Grade 1 |
0,32 | 0,13 | 176 | 41 | 5,4 |
| 21/07/10 | normal clinical examination | 6,88 | 45,5 | 15,7 | 2,88 | 2,2 Grade 1 |
0,07 | 0,61 | 147 | 32 | 10 | ||||
| 21/07/23 chemotherapy n°6 carboplatin 151 mg/m² |
stop 21/07/21 restart 210727 |
stop 21/07/22 restart 21/07/31 |
stop 21/07/22 restart 21/07/29 2,03 mg/kg |
normal clinical examination | 4,930 | ||||||||||
| 21/08/07 | stopped 21/08/02 | stopped 21/08/02 | stopped 21/08/02 | left himb limb edema and ventral hematoma inguinal LN 18mm (not infiltrated by cancer cells) normal clotting time |
5,83 | 37,5 | 12,9 | 1,31 |
0 ,88 Grade 3 |
0,11 | 0,09 | 39 Grade 3 |
|||
| 21/08/16 | the hematoma is shrinking and the limb edema has disappeared | 6,94 | 44,9 | 14,6 | 3,83 | 3,32 | 0,08 | 0,42 | 35 Grade 3 |
||||||
| 21/08/25 | restart firocoxib | restart toceranib | 7,24 | 47,7 | 16,0 | 4,66 | 3,63 | 0,15 | 0,88 | 42 Grade 3 |
|||||
| 21/09/01 | flaccid tail, evolving into posterior paresis within 24 hours spinal metastases (CT examination) and death on 21/09/22 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



