
Submitted:
06 August 2024
Posted:
07 August 2024
You are already at the latest version
Abstract
Aim: To study the relationship between the location of chest pain (topography) and site of coronary artery involvement in patients of Acute coronary syndrome (ACS) undergoing percutaneous transluminal coronary angioplasty (PTCA). Materials and Method: This observational study analyzed 589 angina topographic sites in 411 consecutive patients hospitalized for Acute Coronary syndrome (ACS) who underwent PTCA at a tertiary care center between January 2017 and December 2019. All parameters including the characteristics and site of the anginal pain, Electrocardiogram (ECG), and Coronary angiography (CAG) findings were recorded and analyzed for their topographical correlation with site of culprit vessel involvement. Result: Out of 411 patients, 337 were Males (82.0%) and 74 (18.0%) were females with 589 topographic sites of angina. The mean age of the study subject was 57.03± 11.28 years. In both ST elevation Myocardial Infarction (STEMI) and Non-ST-elevation Myocardial Infarction (NSTEMI), the Left anterior descending (LAD) was the most affected vessel in 201(63.4%) and 49(53.3%) respectively. The correlation coefficient for LAD occlusion was 0.298 (p=0.001) for the Retrosternal site. The Left Circumflex (LCX) artery showed a positive correlation of 0.647 (p= 0.001) for Jaw with Neck pain and of 0.585 (p=0.001) for Backache with Shoulder pain. The Right Coronary Artery (RCA) showed a positive correlation of 0.713 (p=0.001) for Retrosternal plus Jaw and Neck pain and of 0.719 (p=0.001) for Retrosternal plus Backache. Conclusion: The study reveals a significant correlation between chest pain topography and site of coronary artery involvement. It provides a basis for future research to develop tools that help healthcare professionals quickly identify culprit artery in ACS.
Keywords:
Chest Pain
; Angina
; Acute Coronary Syndrome
; Angina Topography
; STEMI
; NSTEMI
1. Introduction
Chest pain is one of the common reasons for patients to seek urgent medical attention. By systematically evaluating the characteristics of the pain, the clinician can often determine the probable cause of the pain from the patient’s history. Angina pectoris is a pain syndrome with identifiable characteristics, and can determine if a patient’s pain is typical of angina pectoris by carefully analyzing all aspects of the patient’s history. Patients with angina-like pain are more likely to have obstructive coronary disease than those with atypical pain syndromes, as confirmed by coronary arteriography investigations.[1] Patients with angina often describe the discomfort as dull, heavy, or crushing, and they may feel a pressing sensation instead of pain. Sharp, stabbing or burning pain is less common with angina. Anginal pain is usually felt as substernal or anterior chest discomfort, and it often spreads to the left arm in patients with coronary artery disease. About half of patients who experience recurring chest discomfort without coronary artery disease may have reflux esophagitis or esophageal contraction anomalies.[2]
Myocardial infarction is one of the common causes of acute chest pain that requires rapid medical attention. The quality and location of myocardial infarction pain are comparable to angina pectoris, but it is often more severe and longer-lasting. Nitroglycerin may not relieve pain when the patient experiences it at rest. In acute myocardial infarction, identifying the occluded vessel is crucial for several reasons viz. determining the appropriate artery for dilation and stenting especially in multivessel disease, quantifying the lesion severity and its significance, comparing with echocardiographic findings of hypokinesia or akinesia, and distinguishing recent from old occlusions. The diagnosis, management, and prognosis of myocardial infarction rely heavily on ST-segment changes observed in the 12-lead electrocardiogram.[3] However, only 70% of patients show new Q waves or ST segment elevations on their initial Electrocardiogram (ECG). Therefore, the absence of these signs does not rule out infarction.[2] Chest discomfort is one of the most common sign of an acute Myocardial Infarction (MI), and pain radiation and site are also important, although few studies have investigated these factors. This study explored the relationship between the location of angina and the affected coronary vessel. Establishing a successful correlation could improve diagnostic accuracy, facilitate early intervention, help optimize treatment planning and resource utilization, and provide a basis for developing decision-support tools or algorithms to help healthcare providers rapidly assess and manage patients with chest pain.
Materials and Method:
This observational study analyzed consecutive patients of Acute Coronary Syndrome (ACS) between the age group of 18 years to 80 years who were admitted to a tertiary care Medical Institute between January 2017 and December 2019. The ethical clearance was obtained from the Institutional Ethical Committee. The cases were grouped in age intervals by decades.
Exclusion criteria: Patients with a known past history of coronary artery disease with or without previous Myocardial Infarction, non-obstructive heart disease or other established cardiac illnesses and those who had undergone angioplasty or coronary artery bypass grafting (CABG) surgery previously were excluded to avoid biases.
The following variables were evaluated : a) Age and gender demographic variables; b) the topography of angina and site of vessel involvement and c) The type of ACS.
Anginal Pain topography was recorded in a pictorial format for the sites where the patient reported pain, as illustrated in Illustration 1.
Each of the 411 patients was asked to mark all the areas he/she experienced chest pain prior to undergoing coronary angiography to avoid observer or reporting bias. E.g. If subject experienced pain in retrosternal, jaw and back area it was marked as area 1,2,8 (See Illustration 1). All the datasets were captured in tabular form in cumulative frequency and the final yield is plotted in Tables 2 and 3.
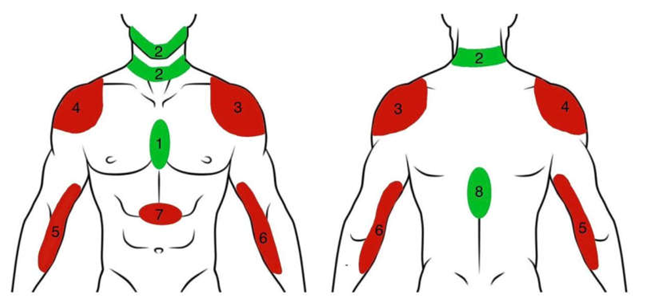
Illustration 1. Pictorial format for all the sites where patient experienced pain. Sites marked in green correspond to the example provided above. 1- Retrosternal, 2- Jaw Neck ,3- Left Shoulder ,4- Right Shoulder ,5- Right Arm ,6- Left Arm 7- Epigastrium 8- Back. Red color depicts the potential sites while green color highlights the site of pain experienced by the patient.
Statistical Analysis
Categorical variables were defined as percentages. The chi-square and ANOVA tests were used to analyze the categorical variables. A correlation analysis between the variables was determined using Pearson’s correlation test, and statistical significance was accepted at p<0.05. Multivariate analysis was done between site of pain and coronary artery occlusion. Coefficient of correlation for statistically significant values was then arrived using regression analysis using SPSS v 24.
Result:
Total of 411 eligible patients with 589 angina topographic sites with ACS were analyzed in this study.
Age, Sex Distribution, and Types of ACS
Out of the total 411 cases, 74(18%) were females while 337(82%) were males. The highest percentage of males were in the age group of 51-60 years (35.5% of total males), while the highest percentage of females were in the age group of 51-60 (30.1% of total females). (Table 1)
For types of ACS, a decade-wise grouping of patients was done. Our study showed that ST Elevated MI (STEMI) was more prevalent than Non-ST Elevated MI (NSTEMI) at this center, followed by Unstable angina (UA). STEMI was found to be maximum in the age group of 61- 70 years (82.4%), whereas NSTEMI and UA were more prevalent in the age group 71-80 years (16.5%) and age group 61- 70 years (8.6%), respectively. This difference was not statistically significant in our study. LAD (250 cases, 60.8%), was the most commonly involved vessel, followed by RCA (95 cases, 23.1%), and LCX (53 cases, 12.9%). Among patients with STEMI, LAD was affected in 201 (63.4%) patients, RCA in 80 (25.2%) patients, LCX in 33 (10.4%) patients, and LMCA in 2 (0.6%) patients. The affected vessels in NSTEMI were LAD, LCX, and RCA in the descending order of their involvement; LAD was most commonly occluded affecting 49 patients (53.3%), while RCA was least occluded affecting in 15 patients only (16.3%) (Table 3).
Our results show that the retrosternal area was the most commonly reported site of pain, seen in 353 (59.9%) patients. This was followed by retrosternum+jaw+neck pain seen in 77 (18.7%) patients and retrosternum+backache seen in 72 (17.5%) patients. The other reported sites of pain are highlighted in Table 2. The differences in STEMI and NSTEMI, mentioned in Table 2, are as follows: retrosternal site of pain is seen in 273 (85.8%) and 80 (87.5%) patients with STEMI and NSTEMI, respectively. In patients with STEMI, retrosternum+jaw+neck pain was seen in 65 (20.4%) patients, and retrosternum + backache was seen in 62 (19.5%) patients. While retrosternum + jaw + neck pain was seen in 12 (13%) patients and retrosternum +backache in 10 (10.9%) patients amongst those with NSTEMI. Table 4 describes the significance and strength of association between the involved vessel and the site of pain. LAD involvement was significantly associated with retrosternal pain with a coefficient of 0.298. Similarly, a statistically significant association was found between ’LCX and jaw + neck pain’ and ‘LCX and Backache + Shoulder pain’ with coefficients of 0.647 and 0.585, respectively. ’Retrosternal + Jaw + Neck’ and ’Retrosternal + Backache’ also had statistically significant correlations with the RCA involvement, with coefficients of 0.713 and 0.719, respectively.

Table 1.
Demographic Information.
| Variable | Mean ±SD/ N (%) | |
|---|---|---|
| 1 | Age(years) | 57.03±11.28 |
| 2 | Weight(Kilograms) | 63.28±13.66 |
| 3 | Male | 337 (82.0%) |
| 4 | Female | 74(18.0%) |
Table 2.
Sites of Pain in STEMI and NSTEMI patients.
| Pain Site | STEMI | NSTEMI | Total (%) | |
|---|---|---|---|---|
| 1 | Retrosternal | 273(60%) | 80(59.7%) | 353(59.9%) |
| 2 | Jaw and Neck | 13(2.8%) | 11(8.2%) | 24(4%) |
| 3 | Left Shoulder | 1(0.2%) | 1(0.7%) | 2(0.3%) |
| 4 | Right Shoulder | 0 | 0 | 0 |
| 5 | Right Arm | 0 | 0 | 0 |
| 6 | Left Arm | 0 | 0 | 0 |
| 7 | Epigastrium | 12(2.6%) | 4(2.9%) | 16(2.7%) |
| 8 | Backache | 0 | 0 | 0 |
| 9 | Retrosternal+ Jaw+ Neck | 65(14.3%) | 12(8.9%) | 77(13.07%) |
| 10 | Retrosternal + Jaw+ Neck +Backache | 2(0.4%) | 0 | 2(0.3%) |
| 11 | Retrosternal + Epigastrium | 2(0.4%) | 0 | 2(0.3%) |
| 12 | Retrosternal+ Epigastrium+ Backache | 1(0.2%) | 0 | 1(0.16%) |
| 13 | Retrosternal + Backache | 62(13.6%) | 10(7.5%) | 72(12.2%) |
| 14 | Retrosternal + Backache + Shoulder | 2(0.4%) | 1(0.7%) | 3(0.5%) |
| 15 | Retrosternal + Shoulder | 6(1.3%) | 2(1.5%) | 8(1.3%) |
| 16 | Jaw+ Neck + shoulder | 1(0.2%) | 0 | 1(0.16%) |
| 17 | Jaw+ Neck + Backache | 1(0.2%) | 0 | 1(0.16%) |
| 18 | Epigastrium + Backache | 1(0.2%) | 2(1.5%) | 3(0.5%) |
| 19 | Backache + Shoulder | 13(2.8%) | 11(8.2%) | 24(4%) |
Table 3.
Vessels involved in STEMI and NSTEMI patients.
| Vessel Involved | STEMI | NSTEMI | Total (%) | |
|---|---|---|---|---|
| 1 | LAD | 201(63.4%) | 49(53.3%) | 250(60.8%) |
| 2 | LCX | 33(10.4%) | 20(21.7%) | 53(12.9%) |
| 3 | RCA | 80(25.2%) | 15(16.3%) | 95(23.1%) |
| 4 | LMCA | 2(0.6%) | 0 | 2(0.5%) |
LAD= Left Anterior Descending artery, LCX = Left Circumflex artery, RCA= Right Coronary Artery, LMCA= Left Main Coronary artery.
Table 4.
Significance of the results.
| LAD | LCX | RCA | LMCA | ||
|---|---|---|---|---|---|
| Retrosternal | Coefficient | 0.298 | -0.077 | -0.281 | 0.028 |
| Sig. | 0.001 | 0.121 | 0.001 | 0.571 | |
| Jaw + Neck | Coefficient | -0.310 | 0.647 | -0.137 | -0.017 |
| Sig. | 0.001 | 0.001 | 0.006 | 0.725 | |
| Retrosternal + Jaw + Neck | Coefficient | -0.496 | -0.129 | 0.713 | -0.034 |
| Sig. | 0.001 | 0.009 | 0.001 | 0.497 | |
| Retrosternal + Backache | Coefficient | -0.496 | -0.139 | 0.719 | -0.032 |
| Sig. | 0.001 | 0.005 | 0.001 | 0.518 | |
| Backache + Shoulder | Coefficient | -0.289 | 0.585 | -0.112 | -0.017 |
| Sig. | 0.001 | 0.001 | 0.023 | 0.725 |
Discussion:
Ischemic episodes in angina pectoris trigger chemosensitive and mechano- receptors in the heart.[4] This often occurs due to fissures or erosions of atherosclerotic plaques, which are common in ischemic syndromes like myocardial infarction and unstable angina. These events lead to the release of various chemical mediators into the coronary artery lumen, including serotonin, histamine, thromboxane A2, bradykinin, reactive oxygen species, lactic acid, and adenosine. These mediators, generated through the cyclooxygenase pathway, include prostaglandins (PGE2 and PGI2).[4]
These chemical mediators interact with specific receptors, predominantly on chemically sensitive terminals, which depolarize cardiac visceral spinal afferent fibers. The cell bodies of these fibers, originating from the heart and coronary arteries, are located in the dorsal root ganglia (DRG) of the T2-T6 spinal segments, potentially extending to the C8-T9 segments.[5] Chemo-sensitive nociceptors and mechanoreceptors innervate the epicardium, their excitation triggering pain, activating protective reflexes, and modulating cardiac function.
Sensitization of nociceptors occurs following injury or inflammation, with the release of prostaglandins, leukotrienes, substance P, and other mediators aggravating the condition. Unstable coronary atherosclerotic plaques can rupture or erode, activating platelets and releasing sensitizing chemicals that inflame the coronary arteries’ adventitia.[6,7,8,9] This activation of silent nociceptors and sensitization of chemosensitive receptors intensify the pain experience, particularly in patients infused with adenosine.[10]
Prostaglandins, lipid autacoids derived from arachidonic acid via the cyclooxygenase pathway, are found in elevated concentrations in the plasma of patients with unstable angina pectoris or acute myocardial infarction.[11]
Despite the pathophysiology of chest pain being understood, the localization of chest pain and pain pathways from the site of ischemia is not appropriately studied. The reasons are threefold. There is a paucity of sensory endings to the heart, a limited number of secondary sensory fibers in the spinothalamic tracts, and an absence of cortical area for localization of visceral pain in the post-central gyrus. The dermatomal distribution of pain fibers around the involved coronary and the corresponding segments of the spinal cord can, however, explain the relation and fill the existing lacunae.[12]
Our research has identified a strong link between the location of retrosternal pain and the blocked artery. The chest pain’s location is crucial for diagnosing ACS/AMI. Pain in the center of the chest is more likely to be ischemic compared to pain located peripherally, with retrosternal chest pain being the most prevalent. In our study, 353 patients (59.9%) experienced retrosternal chest pain. Lichstein et al.’s study, which examined the relationship between chest pain location and coronary artery occlusion, found that the majority of patients (68.11%) had left precordial pain, with a significantly high probability (0.69) of Left Anterior Descending (LAD) artery occlusion.[13]
De Silva et al. noticed that precordial and retrosternal sites are the most common sites for chest pain in Coronary Artery Disease (CAD).[14] Bosner et al. analyzed 1212 patients (534 men and 678 women) for the etiology of their chest pain; of those, 180 patients (92 men and 88 women) were diagnosed with Coronary Heart Disease. The pain was present on the left side of the chest in 56 (63.6%) females and 63 (68.5%) males.[15] Lichstein et al. and Bosner et al. noticed that chest pain was localized on the right side of the chest in 11.5% and 17.2 % of patients respectively. Another study by Swap et al. showed positive likelihood ratio of 4.7 (1.9-12.0) of chest pain radiating to right arm or shoulder with the diagnosis of Acute Myocardial Infarction.[16] However, in our settings, none of the patients presented with right-sided chest pain. Leong et al also found that patients with chest pain were associated with LAD coronary artery occlusion in their study group. [17]
According to a study by From et al., 1,077 patients (72%) presented with STEMI and 423 (28%) presented with NSTEMI. In that study, only 127 patients (12%) with STEMI had a culprit lesion in the Left Circumflex (LCX) artery compared to 166 patients (39%) presenting with NSTEMI.[18] In our study, LCX was the culprit vessel in 33 (10.4%) patients with STEMI and 20 (21.7%) patients with NSTEMI. LCX was the second most commonly involved vessel after LAD in NSTEMI patients which is similar to the findings in the study by From et al. In contrast, in STEMI patients, LCX occlusion came third after LAD and Right Coronary Artery (RCA) occlusion in decreasing order of the involvement. Affected LCX occlusion was significantly associated with sites of chest pain at ’Jaw + Neck’ and ’Backache + Shoulder’ with positive correlations of 0.647 and 0.585, respectively.
In our study, RCA was the third most commonly affected vessel in patients with NSTEMI and second to LAD in patients with STEMI. RCA occlusion was significantly associated with sites ’Retrosternal + Jaw + Neck’ and ’Retrosternal + Backache’ with a positive correlation of 0.713 and 0.719, respectively. In the study by Karwoski et al., RCA and LCX were the most common infarct-related arteries in patients with STEMI and NSTEMI, respectively.[19] This is in contrast to our study. However, what can be found from their study is that STEMI Patients with total occlusion of LAD had higher mortality on follow-up at 36 months of follow-up compared to NSTEMI patients, which showed no differences in mortality between total occlusion and near total occlusion.
STEMI and NSTEMI present with similar complaints of chest pain. The management of these two entities differs, which makes it essential to differentiate them.[3,20] The initial management of left and right coronary circulation involvement is different, making it essential to identify the occlusion site correctly.[21] In cases of multi-vessel disease, particularly in NSTEMI where the identification of the culprit vessel based solely on ECG can be unclear, the use of angina topography can be instrumental in pinpointing the lesion that requires immediate attention. This method, in conjunction with ECG and imaging techniques like echocardiography, can enhance the accuracy of the diagnosis and the prioritization of treatment interventions which will help deliver timely intervention and improve outcomes.[22] Also, in the acute setting of ACS, utilizing angina topography alongside ECG and imaging can assist clinicians in selecting the appropriate guiding catheter with the intent to revascularize, rather than a diagnostic catheter upfront to save time. These strategic choices can significantly reduce door-to-balloon time, thereby improving the overall efficiency and effectiveness of the emergency cardiac care provided.[23]
The results of this study could contribute to improving patient communication and education in healthcare settings. Clinicians can utilize the understanding of chest pain patterns and their relationship with coronary artery pathology to inform patients about their condition prior to utilizing invasive diagnostic techniques. For instance, based on the study’s findings, a patient who presents with retrosternal pain spreading to the jaw and neck may be indicative of a right coronary artery (RCA) infarction, which is linked with the onset of symptoms such as nausea and vomiting,[24] and an elevated risk of developing complete heart block.[25] Also, nitrates should be avoided in patients with suspected right ventricular MI with RCA involvement.[26,27] Such likely adverse events can be explained to the patient beforehand leading to increased clarity about their own condition and improving doctor patient relationship.
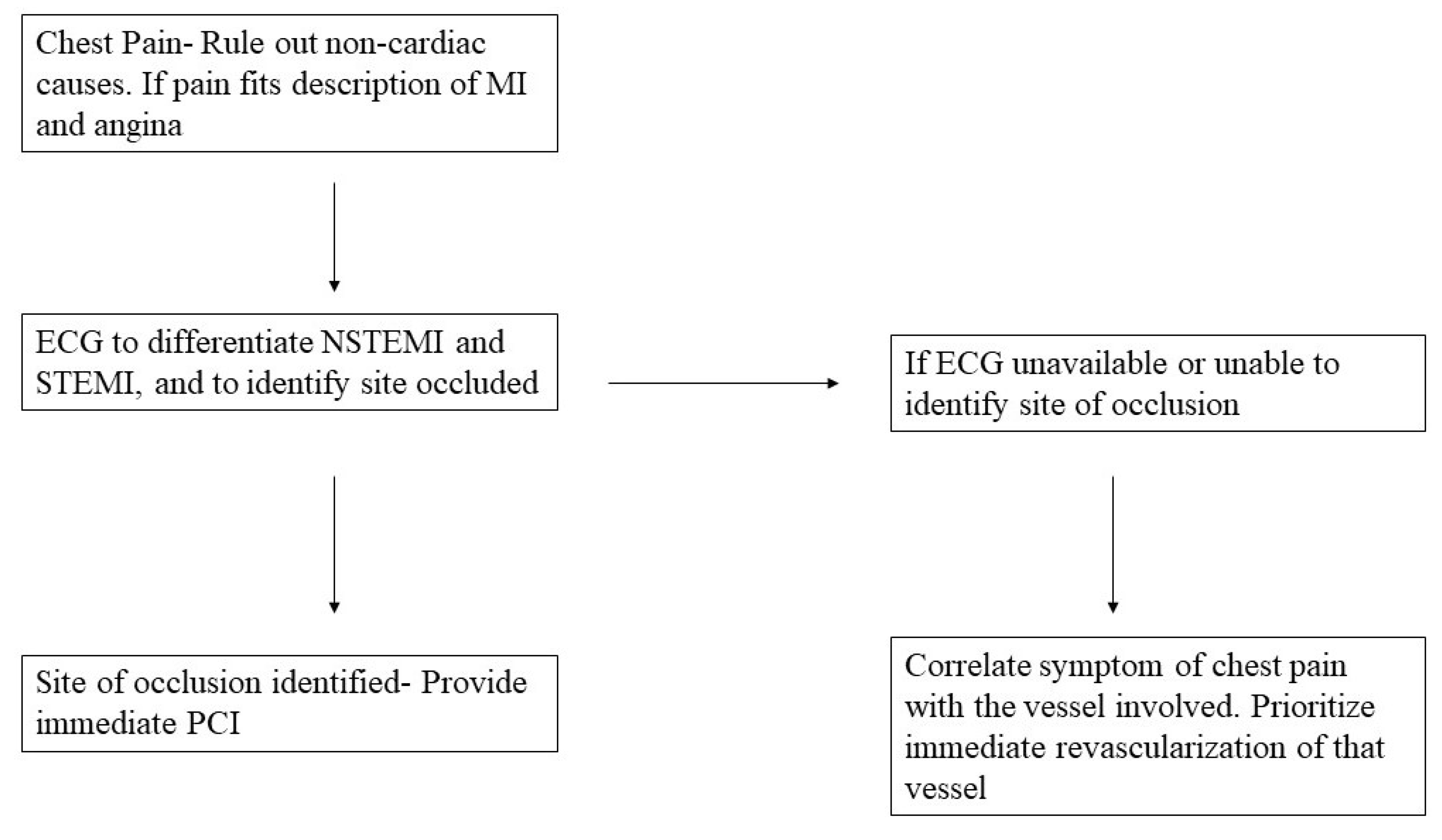
Figure 1.
Flowchart demonstrating application of this study.
The Limitations of our study include the small sample size of 411 patients admitted to a single tertiary care center. Even though the association between the site of pain and the vessel involved was statistically significant, a larger sample size with collaboration from multiple centers can strengthen the findings and help provide readily available information in the form of charts in rural areas. Secondly, chest pain and its location are subjective, and it is difficult to correlate it objectively. This may create a bias. Future developments of tools or models to identify the pain location may help resolve this bias. Future studies and models to identify the dermatomal distribution of pain can help solve this subjective bias. Another limitation is the lack of clarity in interpretation of the data for the multivessel involvement and chest pain location. Multiple coronary vessels are often involved, which requires more extensive multicentric studies to justify the findings. To aptly justify the value of studies, we recommend participation from smaller centers to be involved in the study. Based on our limitations and findings, we recommend more extensive studies in the future with multicentric involvement, training of medical professionals to interpret symptoms and findings, availability of rapid kits at an affordable rate, models to predict the location of pain and vessel involved from collaboration at larger centers, and finding the dermatomal association between them.
Conclusion:
Our study describes the significant association between chest pain location and coronary artery involvement. Angina topography can help in identifying the culprit vessel in patients undergoing coronary angiography or intervention in ACS.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Sanjivani Hospital Ethics Committee (GUJIEC/17/2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hickam, DH. Chest Pain or Discomfort. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations [Internet]. 3rd ed. Boston: Butterworths; 1990 [cited 2024 Mar 15]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK416/.
- Hickam, DH. Chest Pain or Discomfort. In: Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations [Internet]. 3rd ed. Boston: Butterworths; 1990 [cited 2024 Mar 15]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK416/.
- Akbar H, Foth C, Kahloon RA, Mountfort S. Acute ST-Elevation Myocardial Infarction. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Mar 15]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK532281/.
- Fu LW, Longhurst JC. Regulation of Cardiac Afferent Excitability in Ischemia. In: Canning BJ, Spina D, editors. Sensory Nerves [Internet]. Berlin, Heidelberg: Springer Berlin Heidelberg; 2009 [cited 2024 Mar 15]. p. 185–225. (Handbook of Experimental Pharmacology; vol. 194). Available from: http://link.springer.com/10.1007/978-3-540-79090-7_6.
- Vance WH, Bowker RC. Spinal origins of cardiac afferents from the region of the left anterior descending artery. Brain Research. 1983 Jan;258(1):96–100.
- Crea F, Biasucci LM, Buffon A, Liuzzo G, Monaco C, Caligiuri G, et al. Role of Inflammation in the Pathogenesis of Unstable Coronary Artery Disease. The American Journal of Cardiology. 1997 Sep;80(5):10E-16E.
- Flores NA, Sheridan DJ. The pathophysiological role of platelets during myocardial ischaemia. Cardiovascular Research. 1994 Mar 1;28(3):295–302.
- Kohchi K, Takebayashi S, Hiroki T, Nobuyoshi M. Significance of adventitial inflammation of the coronary artery in patients with unstable angina: results at autopsy. Circulation. 1985 Apr;71(4):709–16.
- Van Der Wal AC, Becker AE, Van Der Loos CM, Das PK. Site of intimal rupture or erosion of thrombosed coronary atherosclerotic plaques is characterized by an inflammatory process irrespective of the dominant plaque morphology. Circulation. 1994 Jan;89(1):36–44.
- Gaspardone A, Crea F, Tomai F, Iamele M, Crossman DC, Pappagallo M, et al. Substance P potentiates the algogenic effects of intraarterial infusion of adenosine. Journal of the American College of Cardiology. 1994 Aug;24(2):477–82.
- Hirsh PD, Campbell WB, Willerson JT, Hillis LD. Prostaglandins and ischemic heart disease. The American Journal of Medicine. 1981 Dec;71(6):1009–26.
- White JC. Cardiac Pain: Anatomic Pathways and Physiologic Mechanisms. Circulation. 1957 Oct;16(4):644–55.
- Lichstein E, Breitbart S, Shani J, Hollander G, Greengart A. Relationship between location of chest pain and site of coronary artery occlusion. American Heart Journal. 1988 Mar;115(3):564–8.
- de Silva RA, Bachman WR. Cardiac consultation in patients with neuropsychiatric problems. Cardiol Clin. 1995 May;13(2):225–39.
- Bösner S, Haasenritter J, Hani MA, Keller H, Sönnichsen AC, Karatolios K, et al. Gender differences in presentation and diagnosis of chest pain in primary care. BMC Fam Pract. 2009 Dec;10(1):79.
- Swap CJ. Value and Limitations of Chest Pain History in the Evaluation of Patients With Suspected Acute Coronary Syndromes. JAMA. 2005 Nov 23;294(20):2623.
- Leong K, Jones RH. Influence of the location of left anterior descending coronary artery stenosis on left ventricular function during exercise. Circulation. 1982 Jan;65(1):109–14.
- From AM, Best PJM, Lennon RJ, Rihal CS, Prasad A. Acute Myocardial Infarction Due to Left Circumflex Artery Occlusion and Significance of ST-Segment Elevation. The American Journal of Cardiology. 2010 Oct;106(8):1081–5.
- Karwowski J, Gierlotka M, Gąsior M, Poloński L, Ciszewski J, Bęćkowski M, et al. Relationship between infarct artery location, acute total coronary occlusion, and mortality in STEMI and NSTEMI patients. Polish Archives of Internal Medicine [Internet]. 2017 May 5 [cited 2024 Mar 15]; Available from: http://pamw.pl/en/node/4018.
- Basit H, Malik A, Huecker MR. Non–ST-Segment Elevation Myocardial Infarction. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Mar 15]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK513228/.
- Femia G, French JK, Juergens C, Leung D, Lo S. Right ventricular myocardial infarction: pathophysiology, clinical implications and management. Reviews in Cardiovascular Medicine. 2021;22(4):1229.
- Stähli BE, Varbella F, Linke A, Schwarz B, Felix SB, Seiffert M, et al. Timing of Complete Revascularization with Multivessel PCI for Myocardial Infarction. N Engl J Med. 2023 Oct 12;389(15):1368–79.
- Menees DS, Peterson ED, Wang Y, Curtis JP, Messenger JC, Rumsfeld JS, et al. Door-to-Balloon Time and Mortality among Patients Undergoing Primary PCI. N Engl J Med. 2013 Sep 5;369(10):901–9.
- Ahmed SS, Gupta RC, Brancato RR. Significance of nausea and vomiting during acute myocardial infarction. Am Heart J. 1978 May;95(5):671–2.
- Aguiar Rosa S, Timóteo AT, Ferreira L, Carvalho R, Oliveira M, Cunha P, et al. Complete atrioventricular block in acute coronary syndrome: prevalence, characterisation and implication on outcome. Eur Heart J Acute Cardiovasc Care. 2018 Apr;7(3):218–23.
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. European Heart Journal. 2018 Jan 7;39(2):119–77.
- Neumar RW, Shuster M, Callaway CW, Gent LM, Atkins DL, Bhanji F, et al. Part 1: Executive Summary: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation [Internet]. 2015 Nov 3 [cited 2024 May 22];132(18_suppl_2). Available from: https://www.ahajournals.org/doi/10.1161/CIR.0000000000000252.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



