
Submitted:
07 August 2024
Posted:
08 August 2024
You are already at the latest version
Abstract
This study investigated the efficacy and safety of a propolis mangosteen extract complex (PMEC) on gingival health in patients with gingivitis and incipient periodontitis. A multi-centered randomized, double-blind, placebo-controlled trial involving 104 subjects receiving either PMEC or placebo for eight weeks was conducted. The primary focus was on changes in inflammatory biomarkers from gingival crevicular fluid (GCF), with clinical parameters as secondary outcomes. Results revealed that the PMEC group showed significantly reduced expression of all measured GCF biomarkers compared to the placebo group (p<0.0001) at 8 weeks, including substantial reductions in IL-1β, PGE2, MMP-8, and MMP-9 levels compared to baseline. While clinical parameters trended towards improvement in both groups, inter-group differences were not statistically significant. No significant adverse events were reported, indicating a favorable safety profile. These findings suggest that PMEC consumption can attenuate gingival inflammation and mitigate periodontal tissue destruction by modulating key inflammatory mediators in gingival tissue. Although PMEC shows promise as a potential adjunctive therapy for supporting gingival health, the discrepancy between biomarker improvements and clinical outcomes warrants further investigation to fully elucidate its therapeutic potential in periodontal health management.
Keywords:
propolis
; mangosteen
; gingivitis
; anti-inflammatory effect
1. Introduction
Periodontal disease is a chronic inflammatory condition characterized by the progressive destruction of tooth-supporting tissues, resulting from dysregulated host immune responses to pathogenic biofilms [1]. The pathogenesis involves complex interactions between oral microbiota and host immune cells, leading to the production of pro-inflammatory cytokines, prostaglandins, and matrix metalloproteinases (MMPs), which contribute to soft tissue inflammation and alveolar bone resorption [2].
Diagnostic criteria for periodontal disease typically include gingival index (GI), bleeding on probing (BOP), periodontal pocket depth (PD), gingival recession (GR), clinical attachment level (CAL), and plaque index (PI) [3]. The clinical periodontal examination is mandatory and provide basic information for patients to diagnose periodontal disease, however, these clinical measures provide information on past periodontal tissue destruction and they are inadequate for determining current periodontitis activity or prognosis [3]. Moreover, they exhibit limitations such as low sensitivity and high false-positive rates [4,5]. Consequently, research efforts have focused on identifying periodontal disease biomarkers capable of predicting disease activity or progression [3,6]. Gingival crevicular fluid (GCF) has emerged as a rich source of potential biomarkers, offering a non-invasive means to assess the local inflammatory status of periodontal tissues [7]. GCF contains bacterial metabolites and inflammatory exudates produced by periodontal tissues, including capillaries, in response to bacterial challenge during disease progression. Its non-invasive collection method further enhances its utility in research [1,3,6,8,9]. Several molecules in GCF have been investigated as potential biomarkers, including pro-inflammatory cytokines, proteolytic enzymes, and inflammatory mediators [10,11]. Interleukin-1β (IL-1β) is a key pro-inflammatory cytokine that plays a crucial role in the pathogenesis of periodontal disease [2,7]. Prostaglandin E2 (PGE2), an arachidonic acid metabolite, is another important mediator of inflammation and bone resorption in periodontal tissues. Studies have shown that PGE2 levels in GCF correlate with clinical parameters of periodontal disease severity [10]. Matrix metalloproteinases, particularly MMP-8 and MMP-9, have gained significant attention as potential biomarkers for periodontal disease. MMP-8, also known as neutrophil collagenase, is a key enzyme involved in the degradation of type I collagen, the primary structural protein in periodontal tissues. Elevated levels of MMP-8 in GCF have been consistently associated with periodontal disease activity and progression [12]. Similarly, MMP-9, or gelatinase B, has been implicated in the breakdown of type IV collagen and other extracellular matrix components. Both MMP-8 and MMP-9 levels in GCF have shown promise as diagnostic and prognostic markers for periodontal disease [11]. The detection of periodontal disease biomarkers in GCF holds significant potential for assessing, diagnosing, and prognosticating periodontal disease activity [11,12,13,14].
The association between periodontal disease and systemic conditions such as diabetes mellitus and cardiovascular disease underscores the importance of effective prevention and early intervention strategies [15,16]. While antibiotics have been traditionally employed in periodontal therapy, their long-term use is limited by the emergence of resistant bacterial strains and the risk of opportunistic infections. Consequently, there is growing interest in developing safe and efficacious natural compounds with anti-inflammatory and antimicrobial properties [17,18].
Garcinia mangostana L. (mangosteen) and propolis have gained attention for their potential therapeutic properties in periodontal health. Mangosteen contains bioactive compounds, including xanthones and flavonoids, with demonstrated anti-inflammatory and antimicrobial effects [19,20]. Propolis, a resinous substance produced by honeybees, contains various bioactive compounds such as flavonoids and phenolic acids with antioxidant and immunomodulatory properties [21,22,23].
Previous in vitro and animal studies have demonstrated the potential synergistic effects of propolis and mangosteen extracts in modulating inflammatory responses and promoting osteogenic activity [24,25,26]. However, clinical evidence supporting the efficacy of this combination in managing periodontal health remains limited. Therefore, the present study aimed to evaluate the efficacy and safety of a propolis mangosteen extract complex (PMEC) on gingival health in subjects with gingivitis and incipient periodontitis. We hypothesized that PMEC supplementation would modulate the expression of key inflammatory mediators (IL-1β, PGE2, MMP-8, and MMP-9) in GCF and improve clinical parameters of periodontal health. By focusing on both biomarker analysis and clinical assessments, this study seeks to provide a comprehensive evaluation of the potential benefits of PMEC in periodontal health management.
2. Materials and Methods
2.1. Study Design and Participants
This study was designed as a multicenter, double-blind, placebo-controlled, randomized clinical trial. A total of 104 subjects were enrolled within the Department of Periodontics at Ajou University Dental Hospital and Department of Periodontics, Seoul St. Marys Hospital, Catholic University of Korea. Prior to enrollment, all participants were informed of the nature of the study and informed consent was obtained. The study was approved by the Institutional Review Board (AJIRB-MED-FOD-21-607 and KC22HSDE0008, respectively). The study flowchart is shown in Figure 1.
2.2. Intervention and Monitoring
Participants were randomly assigned to the following groups. The control group received the same placebo capsules without PMECs as the test group. The dosage and composition of PMECs were determined based on previous preclinical studies. The extracted material was formulated in a 2:68 ratio (mangosteen:propolis) by weight. The test group took 2 capsules containing 194 mg of PMECs once daily for 8 weeks (56 days). When converted for a 70 kg adult human, the dose was 388 mg of PMEC. Details of the ingredients of the test and placebo capsules are shown in Table 1.
2.3. Selection Criteria Inclusion/Exclusion Criteria
This study was conducted in subjects with gingivitis and incipient periodontitis. The inclusion criteria were (1) adult men and women aged over 20 years and under 70 years with mild gum disease, (2) at least 20 natural teeth, (3) at least 10% BOP sites in all teeth, (4) at least one tooth with a PD of at least 3 mm but not more than 5 mm and a GI of at least 2 points. Exclusion criteria are (1) clinically significant cardiovascular, immune system, or infectious disease; (2) psychiatric disorders such as schizophrenia, depression, or substance addiction; (3) cancer within the past 5 years; (4) a history of bleeding disorders or conditions, or taking antiplatelet or anticoagulant medications to prevent them, (5) significant pathologic findings in the soft tissues of the oral cavity; (6) pregnancy or lactation; (7) smoking; (8) scaling treatment within 3 months prior to screening or periodontal treatment within 6 months; (9) medications that may affect periodontal status within 1 month prior to screening (Phenytoin, CCBs, Cyclosporine, Coumadin, NSAIDs, Aspirin, etc.) for more than 5 consecutive days; (10) Antibiotics, periodontal supportive therapy within 1 month prior to screening; (11) Dietary supplements related to gum health within 1 month prior to screening; (12)Uncontrolled hypertension (systolic blood pressure greater than or equal to 160 mmHg or diastolic blood pressure greater than or equal to 100 mmHg, measured after 10 minutes of patient rest); (13) Uncontrolled diabetes; (14) Creatinine greater than or equal to 2 times the upper limit of site normal; (15) Participation in another clinical trial; or (16) Other reasons deemed unsuitable for inclusion by the clinician.
2.4. Clinical Parameters and Biomarkers of Gingival Crevicular Fluid (GCF)
The clinical parameters used to evaluate the validity of this study were GI, PD, BOP, GR, CAL, and PI. GI was measured a modified version of the method described by Löe and Silness [27]. Teeth were divided into buccal and lingual surfaces for both the maxilla and mandible. Each surface was rated on a scale of 0 to 3, where 0 indicates healthy gingiva and 3 indicates severe inflammation. The mean GI for an individual was calculated by averaging the scores of all examined teeth. PD was measured by assessing the distance from the gingival margin to the periodontal pocket along the tooth surface. BOP was determined positive if bleeding was observed within 30 seconds following probe placement, and the BOP percentage (BOP%) was calculated as the ratio of BOP-positive sites to the total number of sites examined, expressed as a percentage. GR was measured as the distance from the cementoenamel junction (CEJ) to the gingival margin. CAL measurements were performed based on the periodontal tissues at the CEJ to the site of periodontal tissue attachment, and was calculated as the sum of PD and GR. PD, BOP, GR, and CAL were measured at six sites [proximal, mesial, central, and distal on the buccal surface/lingual surface] for each tooth. PI was categorized into buccal-lingual for maxillary and mandibular teeth and scored on a 0-5 scale [28]. All clinical parameters were measured by the same examiner at visit 1 (screening) or 2 (baseline measurement) and visit 3 (after taking PMEC or placebo for 4 weeks) and 4 (after taking PMEC or placebo for 8 weeks).
Gingival crevicular fluid (GCF) samples were collected to analyze specific biomarkers: IL-1β, PGE2, MMP-8, MMP-9. Sample collection was performed at visits 1 or 2 and repeated by the same investigator at visits 3 and 4 to ensure consistency. GCF samples were obtained using Periopaper strips (ProFlow Inc., Amityville, NY, USA) inserted for 60 seconds into the gingival sulcus of the tooth exhibiting the deepest periodontal pocket, sampling four sites per tooth: mesial buccal, mesial lingual, distal buccal, and distal lingual surfaces. Following collection, samples were immediately frozen to preserve biomarker integrity. Analysis was conducted at Department of Periodontology, Institute of Oral Health Science, Ajou University School of Medicine using standardized protocols for each biomarker. Upon completion of the analysis, all specimens were appropriately discarded in accordance with institutional biosafety guidelines.
2.5. Safety Analysis
The safety evaluation was performed using a safety set analysis as the primary analysis and included 51 test subjects and 53 control subjects who were randomized to the human clinical trial and consumed the human clinical trial food at least once. The type, the incidence, and the severity of the adverse events and their association with the investigational product were evaluated. In addition, the results of clinicopathological examinations (hematology/hematochemistry, urinalysis), vital signs (blood pressure, pulse), and anthropometric measurements (body weight) were analyzed at screening and 8 weeks.
2.6. Data Set Characterization
The data collected in this study were categorized into safety set, full analysis (FA) set, and per protocol (PP) set. The safety set included all participants who consumed at least one dose of the test product. Based on the Intent to Treat (ITT) protocol, the FA set included all participants who received at least one dose of the test product, attended weeks 4 and 8 for efficacy assessments, and met the inclusion/exclusion criteria. The PP set included only participants who completed the study in compliance with the inclusion/exclusion criteria. The PP set was mainly used to assess efficacy, with additional FA set analyses. The Safety set was used for safety analysis only.
2.7. Statistical Analysis
Statistical analyses were performed using SAS® (Version 9.4, SAS Institute, Cary, North Carolina, USA). Data on efficacy, demographic and nutritional analysis, and safety were subjected to two-tailed tests with a significance level of 0.05. Data are presented as mean and standard deviation, and statistical significance of differences between groups was defined as p<0.05. Comparisons between groups were analyzed using a normality test (Shapiro-Wilk) at a p-value of 0.05, followed by a two-sample t-test if both test and control groups met normality, and a Wilcoxon rank sum test if either group failed to meet normality. Sub-set (group) analysis was performed by categorizing the initial characteristics of the human clinical trial subjects before randomization or before treatment initiation to allow for further analysis.
3. Results
3.1. Participant Flow and Baseline Characteristics
A total of 104 participants were initially randomized (51 in the test group, 53 in the control group). Four subjects withdrew after the second visit and were not evaluated for efficacy post-intervention. Three subjects were excluded due to protocol violations, resulting in 97 subjects in the Full Analysis (FA) Set. One additional subject withdrew from the FA Set, and two subjects were excluded for consuming prohibited substances, yielding a final Per Protocol (PP) Set of 94 subjects (46 in the test group, 48 in the control group) (Figure 1). Baseline demographics and clinical characteristics showed no statistically significant differences between the test and control groups (Table 2).
3.2. Clinical Parameters
Analysis of clinical parameters revealed nuanced trends across different measures. The GI in both test and control groups demonstrated a statistically significant within-group decrease at 8 weeks compared to baseline in both PP and FA sets (p<0.05), although between-group differences were not significant (Table 3 and Table 4). BOP (%) significantly decreased in the control group (PP set, Table 3) and in both groups (FA set, Table 4) from baseline to 8 weeks. PD exhibited a decreasing trend in the test group and significant decreases in the control group at both 4 and 8 weeks (Table 3 and Table 4). GR in the test group significantly increased from baseline to 4 weeks in both sets (p<0.05, Table 3 and Table 4). CAL showed a significant decrease in the control group from 4 weeks onward in both sets (p<0.05, Table 3 and Table 4). PI demonstrated significant reductions in the test group at both 4 and 8 weeks, while the control group showed a significant reduction only at 8 weeks. Importantly, between-group comparisons for all clinical parameters did not reach statistical significance at any time point (all p>0.05, Table 3, Table 4 and Figure 2).
3.3. Biomarkers of Gingival Crevicular Fluid (GCF)
Analysis of GCF biomarkers revealed significant changes in the expression of key inflammatory mediators over the course of the study. In the test group, the expression of IL-1β, PGE2, MMP-8, and MMP-9 showed marked decreases from baseline to 4 and 8 weeks in both PP and FA sets (p<0.0001 for all, except IL-1β (p ≤ 0.005 at 4 weeks), Table 5 and Table 6). Specifically, at 8 weeks, IL-1β decreased to 42.1 ± 9.7%, PGE2 to 48.9 ± 8.6%, MMP-8 to 53.7 ± 8.1%, and MMP-9 to 45.6 ± 7.3% of baseline levels in the PP set (Figure 3(a)). Conversely, the control group exhibited increased trends in all biomarkers, with IL-1β reaching 138.2 ± 18.6%, PGE2 129.6 ± 16.2%, MMP-8 124.5 ± 15.7%, and MMP-9 133.8 ± 17.5% at 8 weeks (Figure 3). Between-group comparisons revealed statistically significant differences in all four biomarkers at 8 weeks (p<0.001 for all comparisons, Table 5, Table 6 and Figure 3). The test group experienced a more rapid decrease in biomarker levels during the first 4 weeks (average rate of 7.9% per week) compared to the subsequent 4 weeks (6.5% per week). Strong positive correlations were observed between the reductions in different biomarkers (Pearson’s r: 0.72-0.89, p<0.001), indicating a coordinated modulation of the inflammatory response. These results provide strong evidence for the efficacy of PMEC in modulating key inflammatory mediators in GCF, with consistent and significant reductions observed across all measured biomarkers, contrasting with the increases seen in the control group.
3.4. Safety Analysis
Safety evaluations, including clinicopathological examinations (hematology, biochemistry, urinalysis), vital signs (pulse, blood pressure), and anthropometric measurements (body weight), showed no statistically significant differences between the test and control groups after 8 weeks of treatment (Table 7). No serious adverse events were reported during the study period.
4. Discussion
This randomized, double-blind, placebo-controlled clinical trial evaluated the efficacy of a propolis mangosteen extract complex (PMEC) on gingival health in subjects with mild to moderate gingivitis. Our findings demonstrate that PMEC supplementation significantly modulated the expression of key inflammatory mediators in gingival crevicular fluid (GCF), although clinical parameters showed only modest improvements.
The most striking outcome of this study was the significant reduction in GCF biomarkers (IL-1β, PGE2, MMP-8, and MMP-9) observed in the PMEC group compared to the placebo group. These biomarkers are well-established indicators of periodontal inflammation and tissue destruction [1,9,11,12,29]. The consistent downregulation of these mediators suggests that PMEC may exert a potent anti-inflammatory effect in the periodontal microenvironment. The observed decrease in PGE2 levels (51.1% reduction at 8 weeks) is particularly noteworthy. PGEs, derivatives of arachidonic acid metabolism, are prevalent at inflammatory sites [30]. PGE2, in particular, plays a crucial role in osteoclastogenesis and bone resorption. Its expression is elevated in both periodontal tissue and gingival crevicular fluid as periodontitis advances [10,31]. Notably, PGE2 is theorized to be a primary mediator of the inflammatory and destructive changes observed in periodontal disease, including gingival erythema, edema, collagen degradation, and alveolar bone loss [1].
IL-1β, a primary mediator of the inflammatory response, plays a crucial role in periodontal pathogenesis [2]. The significant reduction in IL-1β levels (57.9% decrease at 8 weeks) in the PMEC group may indicate a dampening of the pro-inflammatory cascade. In response to oral pathogens, neutrophils and macrophages in periodontal tissues release cytokines such as IL-1β, which amplify the adaptive immune response aimed at bacterial elimination. Concurrently, neutrophil-derived MMPs, particularly MMP-8 and MMP-9, contribute to the degradation of periodontal soft and hard tissues by breaking down their primary matrix protein, collagen [9,32]. This finding aligns with previous studies demonstrating the anti-inflammatory properties of propolis or mangosteen extracts [33,34]. The significant decreases in MMP-8 (46.3% reduction) and MMP-9 (54.4% reduction) levels are particularly relevant to periodontal health. These matrix metalloproteinases are primary enzymes responsible for extracellular matrix degradation in periodontal tissues, with MMP-8 specifically targeting type I collagen, the most abundant protein in periodontal ligament [35]. Their downregulation implies that PMEC may help preserve periodontal tissue integrity by reducing proteolytic activity. Previous studies have shown that both propolis and mangosteen components can inhibit MMPs expression and activity [25,36], supporting our findings. These results demonstrate that the consumption of PMEC may confer beneficial effects on periodontal tissue health through its anti-inflammatory properties, as evidenced by the observed reduction in key periodontal disease biomarkers, including IL-1β, PGE2, MMP-8, and MMP-9.
Although the PMEC-induced periodontal disease effect was demonstrated by measuring changes in proinflammatory cytokines, which are used as periodontal disease biomarkers, the lack of changes in clinical parameters may be due to the limitations of the clinical parameters themselves. These clinical parameters may miss subclinical inflammation or early stages of periodontal disease. In the early or asymptomatic stages of inflammation, there may be no noticeable clinical signs such as bleeding or gingival color changes, making it difficult to detect these conditions with conventional methods [37] (p. 33). The main clinical parameters that show the degree or presence of gingival inflammation are GI and BOP. BOP is affected by the pressure applied during probing, which can cause bleeding that may not be related to actual inflammation, resulting in very low sensitivity and high false positives [4,5]. In GI, the subjectivity of clinical periodontal assessment has been reported to be the least reproducible, with the lowest reproducibility in both intra-examiner and inter-examiner comparisons of the five clinical parameters compared [38]. Evidence of periodontal tissue attachment loss can be assessed by CAL, which is calculated as the sum of PD and GR. However, these clinical periodontal parameters provide information about the past and require a significant amount of damage to provide information about the extent of periodontal destruction [37] (p.33). It has also been reported that the results of periodontal probing are limited, influenced by several factors such as the design of the probe tip, the pressure exerted by the probe, the degree of inflammation of the soft tissue affecting resistance, and the angle of the probe [39]. This results in low intra- and inter-examiner reproducibility; in fact, for manual probes, the mean intra-examiner standard deviation of repeated site probing depth measurements ranged from 0.52 to 0.89 mm [40]. These limitations of clinical parameters have led to the validation of various biomarkers to show the extent of periodontitis progression in gingival crevicular fluid (GCF) or saliva, and several inflammatory mediators have been shown to reflect the extent of the disease [7]. Several studies have shown that MMP-8 and IL-1β are the most reliable markers of persistent periodontitis [41,42], and the Helsinki group has developed point-of-care tests (PerioSafe®, ImplantSafe®) to assess salivary MMP-8 levels. Other studies have identified an association between periodontal disease and increased PGE2 [43] and MMP-9 [44] in GCF.
While PMEC shows promise as a potential adjunctive therapy for supporting gingival health, particularly in early-stage periodontal disease, the discrepancy between biomarker improvements and clinical outcomes warrants further investigation. Future studies with larger cohorts, extended durations, and exploration of optimal dosing regimens are necessary to elucidate the full therapeutic potential of PMEC in periodontal health management.
5. Conclusions
In conclusion, this study provides compelling evidence that PMEC supplementation can significantly modulate key inflammatory mediators in the gingival microenvironment. While these biochemical changes did not translate to significant clinical improvements in the short term, the marked reduction in inflammatory biomarkers suggests that PMEC may have potential as an adjunctive therapy in periodontal health management. The multi-faceted effects of PMEC on various inflammatory pathways highlight its promise as a natural, holistic approach to supporting periodontal health. However, further research is needed to optimize its clinical application and fully understand its long-term benefits in periodontal disease prevention and management.
Author Contributions
Conceptualization, J.S. and Y.K.; methodology, GH.C. and H.L.; software, J-S.J.; validation, J.S., and Y.K.; formal analysis, J-S.J.; investigation, G-H.C. and H.L; data curation, J-S.J.; writing—original draft preparation, J-S.J.; writing—review and editing, J.S. and Y.K.; supervision, J.S. and Y.K.; project administration, J.S. and Y.K.; funding acquisition, J.S. and Y.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Medibio Lab Co., Ltd.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Ajou University Dental Hospital (protocol code AJIRB-MED-FOD-21-607 and January 19, 2022) and Seoul St. Marys Hospital, Catholic University of Korea (protocol code KC22HSDE0008 and April 03, 2022).
Informed Consent Statement
Any research article describing a study involving humans should contain this statement. Please add “Informed consent was obtained from all subjects involved in the study.”
Data Availability Statement
The data presented in this study are available on request from the corresponding authors.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Kumar, A.K.; Reddy, N.R.; Babu, M.; Kumar, P.M.; Reddy, V.S.; Chavan, C.V. Estimation of prostaglandin E2 levels in gingival crevicular fluid in periodontal health, disease and after treatment. Contemp Clin. Dent 2013, 4, 303–306. [Google Scholar] [CrossRef] [PubMed]
- He, W.; You, M.; Wan, W.; Xu, F.; Li, F.; Li, A. Point-of-Care Periodontitis Testing: Biomarkers, Current Technologies, and Perspectives. Trends Biotechnol. 2018, 36, 1127–1144. [Google Scholar] [CrossRef] [PubMed]
- Shimada, Y.; Tabeta, K.; Sugita, N.; Yoshie, H. Profiling Biomarkers in Gingival Crevicular Fluid Using Multiplex Bead Immunoassay. Arch. Oral Biol. 2013, 58, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Adler, R.; Joss, A.; Nyman, S. Absence of bleeding on probing. An indicator of periodontal stability. J. Clin. Periodontol. 1990, 17, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Newbrun, E. Indices to measure gingival bleeding. J. Periodontol. 1996, 67, 555–561. [Google Scholar] [CrossRef]
- Buduneli, N.; Kinane, D.F. Host-derived diagnostic markers related to soft tissue destruction and bone degradation in periodontitis. J. clin. periodontol. 2011, 38 (Suppl. 11), 85–105. [Google Scholar] [CrossRef] [PubMed]
- Fatima, T.; Khurshid, Z.; Rehman, A.; Imran, E.; Srivastava, K.C.; Shrivastava, D. Gingival Crevicular Fluid (GCF): A Diagnostic Tool for the Detection of Periodontal Health and Diseases. Molecules. 2021, 26, 1208. [Google Scholar] [CrossRef]
- Delima, A.J.; Van Dyke, T.E. Origin and function of the cellular components in gingival crevice fluid. Periodontol. 2000. 2003, 31, 55–76. [Google Scholar] [CrossRef] [PubMed]
- Baeza, M.; Garrido, M.; Hernández-Ríos, P.; Dezerega, A.; García-Sesnich, J.; Strauss, F.; Aitken, J. P.; Lesaffre, E.; Vanbelle, S.; Gamonal, J.; Brignardello-Petersen, R.; Tervahartiala, T.; Sorsa, T.; Hernández, M. Diagnostic accuracy for apical and chronic periodontitis biomarkers in gingival crevicular fluid: an exploratory study. J. clin. periodontol. 2016, 43, 34–45. [Google Scholar] [CrossRef]
- Offenbacher, S.; Heasman, P.A.; Collins, J.G. Modulation of Host PGE2 Secretion as a Determinant of Periodontal Disease Expression. J. Periodontol. 1993, 64, 432–444. [Google Scholar] [CrossRef]
- Kinney, J.S.; Morelli, T.; Oh, M.; Braun, T.M.; Ramseier, C.A.; Sugai, J.V.; Giannobile, W.V. Crevicular fluid biomarkers and periodontal disease progression. J. Clin. Periodontol. 2014, 41, 113–120. [Google Scholar] [CrossRef]
- Hernández, M.; Baeza, M.; Räisänen, I.T.; Contreras, J.; Tervahartiala, T.; Chaparro, A.; Sorsa, T.; Hernández-Ríos, P. Active MMP-8 Quantitative Test as an Adjunctive Tool for Early Diagnosis of Periodontitis. Diagnostics 2021, 11(8), 1503. [Google Scholar] [CrossRef]
- Champagne, C.M.; Buchanan, W.; Reddy, M.S.; Preisser, J.S.; Beck, J.D.; Offenbacher, S. Potential for gingival crevice fluid measures as predictors of risk for periodontal diseases. Periodontol. 2000. 2003, 31, 167–180. [Google Scholar] [CrossRef]
- Loos, B.G.; Tjoa, S. Host-derived diagnostic markers for periodontitis: do they exist in gingival crevice fluid? Periodontol. 2000. 2005, 39, 53–72. [Google Scholar] [CrossRef]
- Beck, J.D.; Offenbacher, S. Systemic Effects of Periodontitis: Epidemiology of Periodontal Disease and Cardiovascular Disease. J. Periodontol. 2005, 76, 2089–2100. [Google Scholar] [CrossRef]
- Mealey, B.L. Periodontal Disease and Diabetes: A Two-Way Street. J. Am. Dent. Assoc. 2006, 137 (Suppl.), S26–S31. [Google Scholar] [CrossRef] [PubMed]
- Lazar, V.; Saviuc, C.M.; Carmen Chifiriuc, M. Periodontitis and Periodontal Disease - Innovative Strategies for Reversing the Chronic Infectious and Inflammatory Condition by Natural Products. Curr. Pharm. Design. 2015, 22, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Pimentel, S.P.; Casati, M.Z.; Ribeiro, F.V.; Corrêa, M.G.; Franck, F.C.; Benatti, B.B.; Cirano, F.R. Impact of Natural Curcumin on the Progression of Experimental Periodontitis in Diabetic Rats. J. Periodontal Res. 2020, 55, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Yuanita, T.; Ristyawati, D.; Samadi, K. Cytoxicity test of NaOCl and Mangosteen (Garcinia Mangostin L.) peel extract used as an irrigation solution in human periodontal ligament fibroblast cells (HPdLFc). Dent. J 2018, 51, 133–137. [Google Scholar] [CrossRef]
- Lee, H.N.; Jang, H.Y.; Kim, H.J.; Moon, H.K.; Kim, J.H. Antitumor and apoptosis-inducing effects of α-mangostin extracted from the pericarp of the mangosteen fruit (Garcinia mangostana L.) in YD-15 tongue mucoepidermoid carcinoma cells. Int. J. Mol. Med. 2016, 37, 939–948. [Google Scholar] [CrossRef]
- Pietta, P.G.; Gardana, C.; Pietta, A.M. Analytical Methods for Quality Control of Propolis. Fitoterapia. 2002, 73, S7–S20. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Omene, C.; Karkoszka, J.; Bosland, M.; Eckard, J.; Klein, C.B.; Frenkel, K. Caffeic Acid Phenethyl Ester (CAPE), Derived from a Honeybee Product Propolis, Exhibits a Diversity of Anti-Tumor Effects in Pre-Clinical Models of Human Breast Cancer. Cancer Lett. 2011, 308, 43–53. [Google Scholar] [CrossRef]
- Campos, J.F.; Dos Santos, U.P.; da Rocha, P.dosS.; Damião, M.J.; Balestieri, J.B.; Cardoso, C.A.; Paredes-Gamero, E.J.; Estevinho, L.M.; de Picoli Souza, K.; Dos Santos, E.L. Antimicrobial, antioxidant, anti-inflammatory, and cytotoxic activities of propolis from the stingless BeeTetragonisca fiebrigi(Jataí). Evid. Based Complement. Altern. Med. 2015, 1–11. [CrossRef]
- Lim, Y.K.; Cho, E.J.; Jeong, H.J.; Choi, D.S.; Yoo, M.A.; Lee, M.G.; Lee, H.S. Anti-inflammatory and in vitro bone formation effects of Garcinia mangostana L. and propolis extracts. Food Sci. Biotechnol. 2020, 29, 539–548. [Google Scholar] [CrossRef]
- Sung, S.J. Effect of Garcinia Mangostana L. and Propolis Extracts on the Inhibition of Inflammation and Alveolar Bone Loss in Ligature-Induced Periodontitis in Rats. Int. J. Oral Biol. 2019, 44, 55–61. [Google Scholar] [CrossRef]
- Lee, K.H.; Yoo, S.Y.; Kook, J.K.; Sung, S.J.; Lee, K.W.; Lim, Y.K.; Lee, D.S.; Yu, S.J. Inhibitory effect of mangosteen peel and propolis ethanol extracts on alveolar bone loss against increased treatment amount of Porphyromonas gingivalis lipopolysaccharide in rat. Korean J. Dent. Mater. 2021, 48, 71–78. [Google Scholar] [CrossRef]
- Löe, H.; Silness, J. Periodontal Disease in Pregnancy I. Prevalence and Severity. Acta. Odontol. Scand. 1963, 21, 533–551. [Google Scholar] [CrossRef] [PubMed]
- Turesky, S.; Gilmore, N.D.; Glickman, I. Reduced Plaque Formation by the Chloromethyl Analogue of Vitamin C. J. Periodontol. 1970, 41, 41–43. [Google Scholar] [CrossRef] [PubMed]
- Romero-Castro, N.S.; Vázquez-Villamar, M.; Muñoz-Valle, J.F.; Reyes-Fernández, S.; Serna-Radilla, V.O.; García-Arellano, S.; Castro-Alarcón, N. Relationship Between TNF-α, MMP-8, and MMP-9 Levels in Gingival Crevicular Fluid and the Subgingival Microbiota in Periodontal Disease. Odontology. 2020, 108, 25–33. [Google Scholar] [CrossRef]
- Kuehl, F.A. Jr.; Egan, R.W. Prostaglandins, arachidonic acid, and inflammation. Science 1980, 210, 978–984. [Google Scholar] [CrossRef]
- Dziak, R. Biochemical and molecular mediators of bone metabolism. J. Periodontol. 1993, 64 (Suppl. 5), 407–415. [Google Scholar] [PubMed]
- Beklen, A.; Tüter, G.; Sorsa, T.; Hanemaaijer, R.; Virtanen, I.; Tervahartiala, T.; Konttinen, Y. T. Gingival tissue and crevicular fluid co-operation in adult periodontitis. J. dent. res. 2006, 85, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Mohan, S.; Syam, S.; Abdelwahab, S.I.; Thangavel, N. An anti-inflammatory molecular mechanism of action of α-mangostin, the major xanthone from the pericarp of Garcinia mangostana: an in silico, in vitro and in vivo approach. Food Funct. 2018, 9, 3860–3871. [Google Scholar] [CrossRef]
- Ali, K.M.; Saleh, Z.; Jalal, J. Effect of local propolis irrigation in experimental periodontitis in rats on inflammatory markers (IL-1β and TNF-α) and oxidative stress. Indian J. Dent. Res. 2020, 31, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Luchian, I.; Goriuc, A.; Sandu, D.; Covasa, M. The Role of Matrix Metalloproteinases (MMP-8, MMP-9, MMP-13) in Periodontal and Peri-Implant Pathological Processes. Int. J. Mol. Sci. 2022, 23, 1806. [Google Scholar] [CrossRef] [PubMed]
- Eghbali Zarch, R.; Askari, M.; Boostani, H.; Mirzaii-Dizgah, I. Effect of propolis extract on clinical parameters and salivary level of matrix metalloproteinase 8 in periodontitis patients: A randomized controlled clinical trial. J. Adv. Periodontol. Implant Dent. 2021, 13, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Buduneli, N. Biomarkers in Periodontal Health and Disease: Rationale, Benefits, and Future Directions. Springer; Cham, Switzerland: Biomarkers in periodontal health and disease: Rationale, benefits, and future directions. 2019. Volume 90.
- Marks, R.G.; Magnusson, I.; Taylor, M.; Clouser, B.; Maruniak, J.; Clark, W.B. Evaluation of reliability and reproducibility of dental indices. J. Clin. Periodontol. 1993, 20(1), 54–58. [Google Scholar] [CrossRef] [PubMed]
- Armitage, G.C. Manual periodontal probing in supportive periodontal treatment. Periodontol. 2000. 1996, 12, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Osborn, J.B.; Stoltenberg, J.L.; Huso, B.A.; Aeppli, D.M.; Pihlstrom, B.L.; Adams, D.F. Comparison of Measurement Variability in Subjects with Moderate Periodontitis Using a Conventional and Constant Force Periodontal Probe. J. Periodontol. 1992, 63, 283–289. [Google Scholar] [CrossRef]
- Nazar Majeed, Z.; Philip, K.; Alabsi, A.M.; Pushparajan, S.; Swaminathan, D. Identification of gingival crevicular fluid sampling, analytical methods, and oral biomarkers for the diagnosis and monitoring of periodontal diseases: A systematic review. Dis. Markers 2016, 1804727. [Google Scholar] [CrossRef]
- Al-Majid, A.; Alassiri, S.; Rathnayake, N.; Tervahartiala, T.; Gieselmann, D.R.; Sorsa, T. Matrix Metalloproteinase-8 as an Inflammatory and Prevention Biomarker in Periodontal and Peri-Implant Diseases. Int. J. Dent. 2018, 2018, 1–27. [Google Scholar] [CrossRef] [PubMed]
- Kardeşler, L.; Buduneli, N.; Biyikoğlu, B.; Cetinkalp, S.; Kütükçüler, N. Gingival crevicular fluid PGE2, IL-1beta, t-PA, PAI-2 levels in type 2 diabetes and relationship with periodontal disease. Clin. Biochem. 2008, 41, 863–868. [Google Scholar] [CrossRef] [PubMed]
- Rai, B.; Kaur, J.; Jain, R.; Anand, S.C. Levels of Gingival Crevicular Metalloproteinases-8 and -9 in Periodontitis. Saudi Dent. J. 2010, 22, 129–131. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart depicting the study design. FA, full analysis; PP, per protocol.
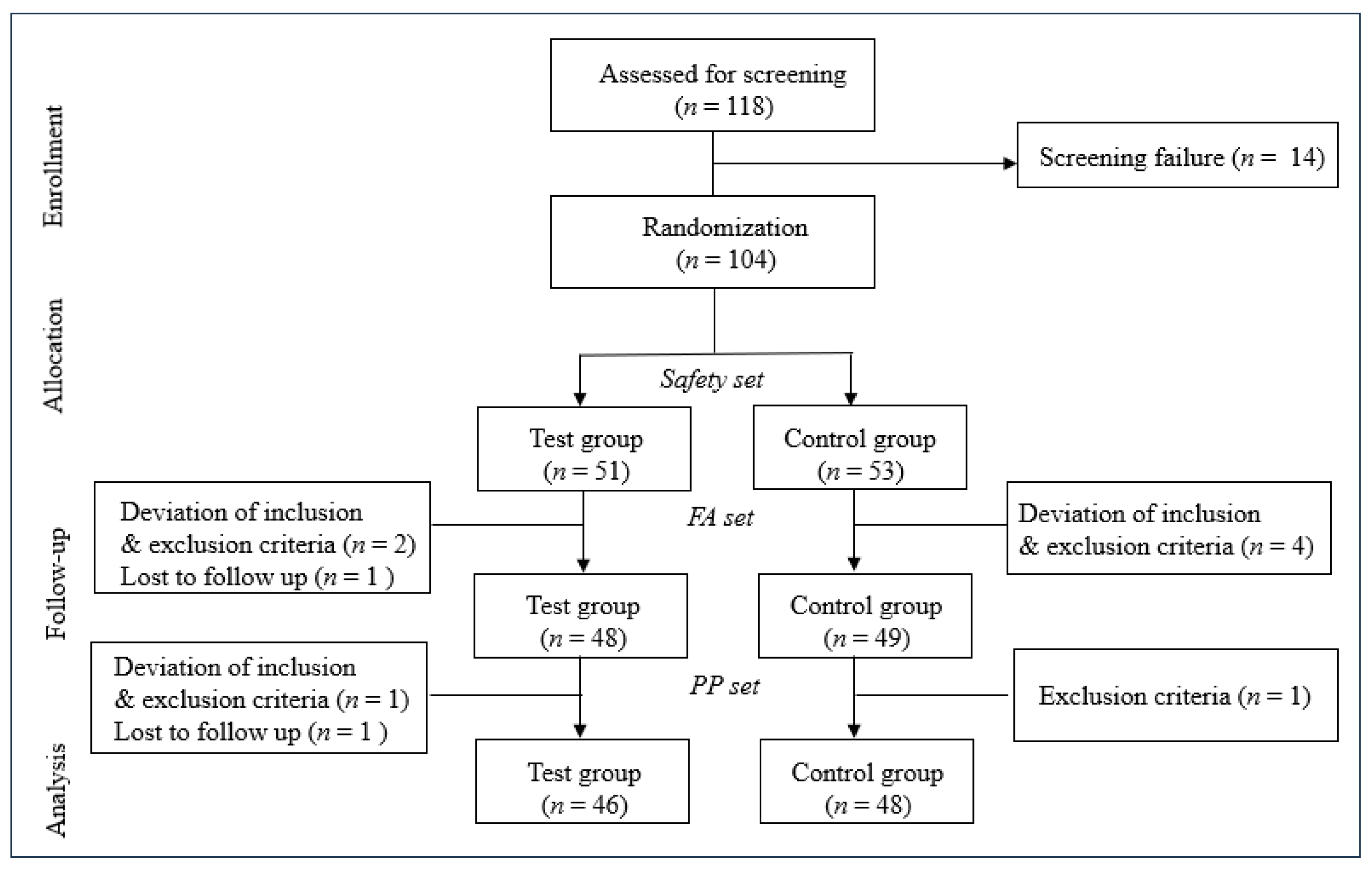
Figure 2.
Changes in clinical parameters over time in the PP Set (a) and the FA Set (b). Changes are presented as percentages relative to the baseline of the control group. Blue asterisks denote statistical significance (p<0.05) in the test group at weeks 4 and 8 compared to week 0 (baseline). Red asterisks indicate statistical significance (p<0.05) in the control group at weeks 4 and 8 compared to week 0. No significant differences in clinical parameters were observed between the PMEC and placebo groups at the evaluated time points; consequently, these data are not presented.
Figure 2.
Changes in clinical parameters over time in the PP Set (a) and the FA Set (b). Changes are presented as percentages relative to the baseline of the control group. Blue asterisks denote statistical significance (p<0.05) in the test group at weeks 4 and 8 compared to week 0 (baseline). Red asterisks indicate statistical significance (p<0.05) in the control group at weeks 4 and 8 compared to week 0. No significant differences in clinical parameters were observed between the PMEC and placebo groups at the evaluated time points; consequently, these data are not presented.
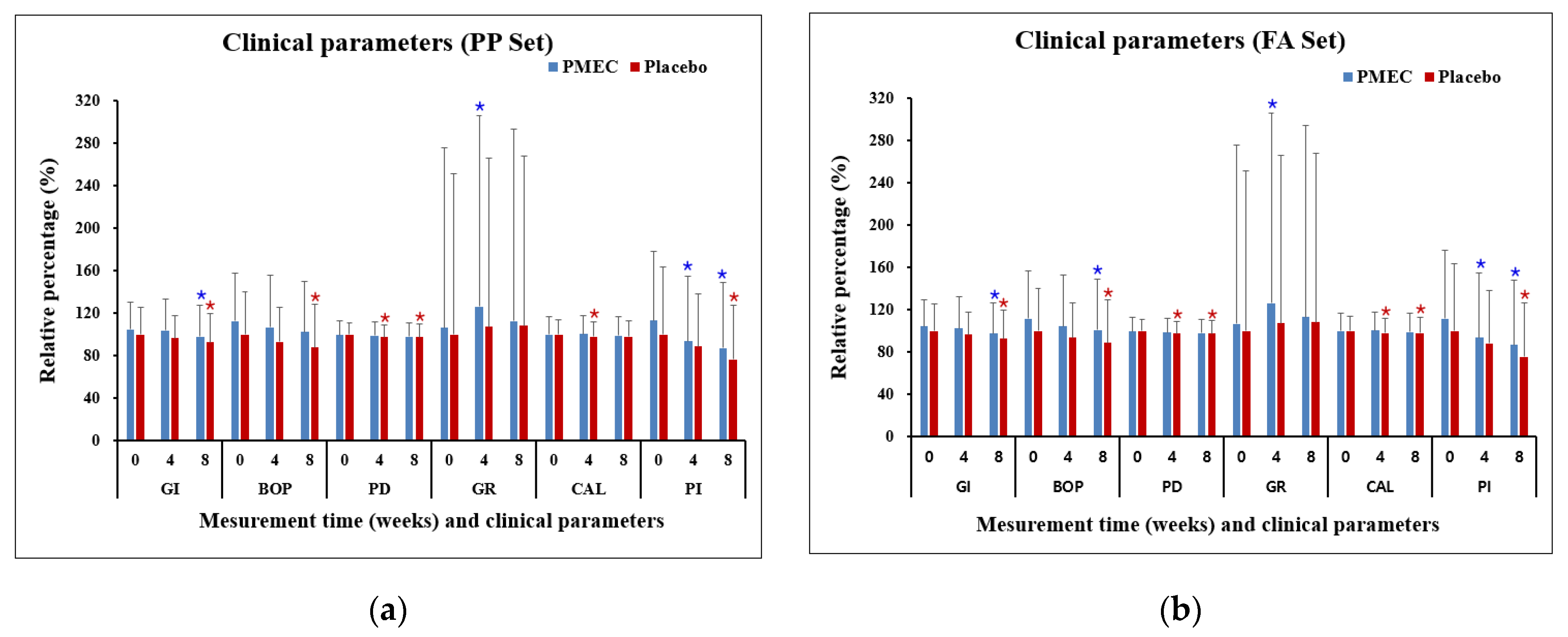
Figure 3.
Changes in inflammatory biomarkers in GCF over time in the PP Set (a) and the FA Set (b). Changes are presented as percentages relative to the baseline of the control group. Blue asterisks denote statistical significance (p<0.05) in the test group at weeks 4 and 8 compared to week 0 (baseline). Red asterisks indicate statistical significance (p<0.05) in the control group at weeks 4 and 8 compared to week 0 (baseline). Green asterisks denote statistically significant differences (p<0.05) between the PMEC and placebo groups at week 0, weeks 4 and 8.
Figure 3.
Changes in inflammatory biomarkers in GCF over time in the PP Set (a) and the FA Set (b). Changes are presented as percentages relative to the baseline of the control group. Blue asterisks denote statistical significance (p<0.05) in the test group at weeks 4 and 8 compared to week 0 (baseline). Red asterisks indicate statistical significance (p<0.05) in the control group at weeks 4 and 8 compared to week 0 (baseline). Green asterisks denote statistically significant differences (p<0.05) between the PMEC and placebo groups at week 0, weeks 4 and 8.


Table 1.
The details of the constituents of the test and placebo capsules
| Test | Placebo | |||
| Raw Material | Compounding Ratio (%) |
Content (mg) |
Compounding Ratio (%) |
Content (mg) |
| Propolis Mangosteen Extract Complex (PMEC) | 41.28 | 194.00 | - | - |
| Lactose Powder | 30.00 | 141.00 | 62.70 | 294.69 |
| Microcrystalline cellulose | 24.22 | 113.85 | 34.27 | 161.07 |
| Sucrose esters of fatty acids | 2.00 | 9.10 | - | - |
| Caramel color | - | - | 2.00 | 9.40 |
| Magnesium stearate | 1.50 | 7.05 | 1.00 | 4.70 |
| silicon dioxide | 1.00 | 4.70 | - | - |
| Food blue NO.1 | - | - | 0.03 | 0.14 |
| Total | 100 | 470 | 100 | 470 |
Table 2.
Demographics and clinical characteristics of participants.
| Variables | Test Group (n = 46) |
Control Group (n = 48) |
P-Value |
|---|---|---|---|
| Age (years), mean ± SD | 43.17±11.01 | 42.02±11.40 | 0.6194(T) |
| Gender, n (%) | |||
| Male | 16 (34.78) | 16 (33.33) | 0.8822(C) |
| Female | 30 (65.22) | 32 (66.67) | |
| Smoking status, n (%) | |||
| No | 46 (100.00) | 48 (100.00) | - |
| Yes | 0 (0.00) | 0 (0.00) | |
| Physical activity, n (%) | |||
| None | 8 (17.39) | 14 (29.17) | 0.5364(C) |
| 1-2 times/week | 12 (26.09) | 10 (20.83) | |
| 3 times/week | 14 (30.43) | 14 (29.17) | |
| 4-5 times/week | 5 (10.87) | 2 (4.17) | |
| 7 times/week | 7 (15.22) | 8 (16.67) | |
| Drinking status, n (%) | |||
| No | 16 (34.78) | 16 (33.33) | 0.8822(C) |
| Yes | 30 (65.22) | 32 (66.67) | |
| Weight (kg) | |||
| Mean±SD | 64.09±11.82 | 65.79±12.88 | 0.4984(W) |
| Median | 61.70 | 63.65 | |
| Min, Max | 48.00, 97.60 | 46.10, 101.30 | |
| Height (cm) | |||
| Mean±SD | 165.14±7.86 | 164.64±7.97 | 0.8146(W) |
| Median | 164.85 | 163.95 | |
| Min, Max | 154.00, 178.00 | 149.00, 183.00 |
Table 3.
Change in clinical parameters by measurement time in the PP set.
| Clinical parameters |
Measurement time | Test | Control | Control |
| GI | Baseline | 1.70±0.41 | 1.62±0.42 | 0.1780 (W) |
| 4 weeks | 1.68±0.48 | 1.57±0.34 | 0.0671 (W) | |
| p-value [1] | 0.6560 | 0.1895 | ||
| 8 weeks | 1.59±0.47 | 1.50±0.44 | 0.1512 (W) | |
| p-value [1] | 0.0267 | 0.0027 | ||
| BOP (%) | Baseline | 47.26±18.90 | 41.93±16.69 | 0.1502 (T) |
| 4 weeks | 44.70±20.43 | 39.03±13.60 | 0.1319 (W) | |
| p-value [1] | 0.2396 | 0.0772 | ||
| 8 weeks | 42.98±20.02 | 36.88±16.95 | 0.1140 (T) | |
| p-value [1] | 0.0577 | 0.0019 | ||
| PD | Baseline | 2.58±0.35 | 2.59±0.28 | 0.6497 (W) |
| 4 weeks | 2.56±0.34 | 2.53±0.31 | 0.7477 (W) | |
| p-value [1] | 0.4485 | 0.0010 | ||
| 8 weeks | 2.54±0.33 | 2.52±0.32 | 0.9879 (W) | |
| p-value [1] | 0.1115 | 0.0047 | ||
| GR | Baseline | 0.18±0.28 | 0.17±0.25 | 0.9262 (W) |
| 4 weeks | 0.21±0.30 | 0.18±0.27 | 0.5198 (W) | |
| p-value [1] | 0.0026 | 0.3165 | ||
| 8 weeks | 0.19±0.30 | 0.18±0.27 | 0.7699 (W) | |
| p-value [1] | 0.4090 | 0.2733 | ||
| CAL | Baseline | 2.76±0.46 | 2.76±0.37 | 0.7477 (W) |
| 4 weeks | 2.77±0.47 | 2.71±0.38 | 0.6884 (W) | |
| p-value [1] | 0.5222 | 0.0212 | ||
| 8 weeks | 2.73±0.49 | 2.71±0.42 | 0.9608 (W) | |
| p-value [1] | 0.2707 | 0.0628 | ||
| PI | Baseline | 0.60±0.34 | 0.53±0.34 | 0.2438(W) |
| 4 weeks | 0.50±0.33 | 0.47±0.26 | 0.7990(W) | |
| p-value [1] | 0.0023 | 0.1564 | ||
| 8 weeks | 0.46±0.33 | 0.41±0.27 | 0.4641 (W) | |
| p-value [1] | 0.0003 | 0.0036 |
Table 4.
Change in clinical parameters by measurement time in the FA set.
| Clinical parameters |
Measurement time | Test | Control | p-value [2] |
| GI | Baseline | 1.69±0.41 | 1.62±0.41 | 0.2145 (W) |
| 4 weeks | 1.66±0.49 | 1.57±0.33 | 0.0976 (W) | |
| p-value [1] | 0.4961 | 0.1752 | ||
| 8 weeks | 1.58±0.47 | 1.51±0.44 | 0.1848 (W) | |
| p-value [1] | 0.0164 | 0.0020 | ||
| BOP (%) | Baseline | 46.83±18.71 | 41.87±16.52 | 0.1696 (T) |
| 4 weeks | 43.76±20.63 | 39.31±13.60 | 0.2305 (W) | |
| p-value [1] | 0.1495 | 0.1185 | ||
| 8 weeks | 42.23±20.00 | 37.26±16.99 | 0.0874 (W) | |
| p-value [1] | 0.0351 | 0.0051 | ||
| PD | Baseline | 2.59±0.35 | 2.60±0.29 | 0.7127 (W) |
| 4 weeks | 2.57±0.33 | 2.54±0.32 | 0.7208 (W) | |
| p-value [1] | 0.3886 | 0.0009 | ||
| 8 weeks | 2.55±0.33 | 2.54±0.32 | 0.9453 (W) | |
| p-value [1] | 0.0919 | 0.0031 | ||
| GR | Baseline | 0.18±0.28 | 0.17±0.25 | 0.9971 (W) |
| 4 weeks | 0.21±0.30 | 0.18±0.26 | 0.4564 (W) | |
| p-value [1] | 0.0026 | 0.3164 | ||
| 8 weeks | 0.19±0.30 | 0.18±0.27 | 0.8488 (W) | |
| p-value [1] | 0.4088 | 0.2732 | ||
| CAL | Baseline | 2.77±0.45 | 2.77±0.37 | 0.7866 (W) |
| 4 weeks | 2.78±0.46 | 2.72±0.38 | 0.6861 (W) | |
| p-value [1] | 0.5885 | 0.0198 | ||
| 8 weeks | 2.74±0.48 | 2.71±0.42 | 0.9798 (W) | |
| p-value [1] | 0.2341 | 0.0483 | ||
| PI | Baseline | 0.60±0.34 | 0.54±0.34 | 0.2773 (W) |
| 4 weeks | 0.50±0.32 | 0.48±0.26 | 0.7774 (W) | |
| p-value [1] | 0.0024 | 0.1348 | ||
| 8 weeks | 0.47±0.33 | 0.41±0.27 | 0.4452 (W) | |
| p-value [1] | 0.0002 | 0.0021 |
Table 5.
Biomarkers in gingival crevicular fluid by measurement time in the PP set.
| Biomarkers | measurement time | Test | Control | p-value [2] |
| PGE2 (ng/mL) |
Baseline | 602.38±178.15 | 526.36±172.55 | 0.0244 (W) |
| 4 weeks | 455.80±113.81 | 518.74±141.58 | 0.0202 (W) | |
| p-value [1] | <.0001 | 0.7403 | ||
| 8 weeks | 345.43±69.02 | 576.08±186.17 | <.0001 (T) | |
| p-value [1] | <.0001 | 0.0791 | ||
| IL-1ß (pg/mL) |
Baseline | 135.45±93.70 | 114.86±65.96 | 0.4075 (W) |
| 4 weeks | 102.83±62.54 | 124.84±71.32 | 0.1096 (W) | |
| p-value [1] | 0.0042 | 0.2406 | ||
| 8 weeks | 70.89±65.46 | 141.95±78.02 | <.0001 (W) | |
| p-value [1] | <.0001 | 0.0062 | ||
| MMP-8 (ng/mL) |
Baseline | 36.21±18.33 | 32.74±16.13 | 0.4205 (W) |
| 4 weeks | 28.30±14.29 | 34.36±15.41 | 0.0511 (T) | |
| p-value [1] | <.0001 | 0.3191 | ||
| 8 weeks | 21.76±14.65 | 36.76±16.15 | <.0001 (W) | |
| p-value [1] | <.0001 | 0.0390 | ||
| MMP-9 (ng/mL) |
Baseline | 65.19±25.20 | 60.51±19.81 | 0.3180 (T) |
| 4 weeks | 49.47±19.97 | 63.55±20.47 | 0.0011 (T) | |
| p-value [1] | <.0001 | 0.2065 | ||
| 8 weeks | 35.55±20.79 | 66.46±23.25 | <.0001 (W) | |
| p-value [1] | <.0001 | 0.0701 |
Table 6.
Biomarkers in gingival crevicular fluid by measurement time in the FA set.
| Biomarkers | measurement time | Test | Control | p-value [2] |
| PGE2 (ng/mL) |
Baseline | 590.38±183.91 | 523.20±172.16 | 0.0492 (W) |
| 4 weeks | 456.83±111.49 | 517.22±140.49 | 0.0209 (W) | |
| p-value [1] | <.0001 | 0.7910 | ||
| 8 weeks | 353.76±80.08 | 575.77±184.23 | <.0001 (T) | |
| p-value [1] | <.0001 | 0.0600 | ||
| IL-1ß (pg/mL) |
Baseline | 131.99±93.75 | 113.65±65.81 | 0.4728 (W) |
| 4 weeks | 101.19±62.07 | 124.06±70.79 | 0.0866 (W) | |
| p-value [1] | 0.005 | 0.2125 | ||
| 8 weeks | 70.26±64.66 | 141.07±77.45 | <.0001 (W) | |
| p-value [1] | <.0001 | 0.0047 | ||
| MMP-8 (ng/mL) |
Baseline | 35.51±18.58 | 32.55±16.02 | 0.4019 (T) |
| 4 weeks | 27.90±14.30 | 34.31±15.25 | 0.0354 (T) | |
| p-value [1] | <.0001 | 0.2716 | ||
| 8 weeks | 21.69±14.47 | 36.78±15.98 | <.0001 (W) | |
| p-value [1] | <.0001 | 0.0278 | ||
| MMP-9 (ng/mL) |
Baseline | 64.67±26.64 | 59.71±20.38 | 0.3045 (T) |
| 4 weeks | 49.49±20.78 | 62.79±20.94 | 0.0023 (T) | |
| p-value [1] | <.0001 | 0.1916 | ||
| 8 weeks | 36.46±21.54 | 65.85±23.41 | <.0001 (W) | |
| p-value [1] | <.0001 | 0.0573 |
Table 7.
Safety analysis of control and test at baseline, 8 weeks (mean±SD).
|
Test n=51 |
Control n=53 |
p-value [2] | ||||
| n | Mean±SD | n | Mean±SD | |||
| WBC (103/μL) |
Baseline | 51 | 6.09±1.42 | 53 | 6.07±1.15 | 0.9344[T] |
| 8 weeks | 47 | 5.91±1.42 | 49 | 6.17±1.58 | 0.3963[T] | |
| p-value [1] | 0.2759 | 0.9625 | ||||
| RBC (106/μL) |
Baseline | 51 | 4.48±0.36 | 53 | 4.48±0.39 | 0.9940[T] |
| 8 weeks | 47 | 4.45±0.37 | 49 | 4.51±0.39 | 0.2821[T] | |
| p-value [1] | 0.2801 | 0.6985 | ||||
| Hb (g/dL) |
Baseline | 51 | 13.57±1.11 | 53 | 13.52±1.22 | 0.8289[T] |
| 8 weeks | 47 | 13.45±1.25 | 49 | 13.61±1.30 | 0.2633[W] | |
| p-value [1] | 0.2572 | 0.7399 | ||||
| Hct (%) |
Baseline | 51 | 40.77±3.29 | 53 | 40.64±3.46 | 0.8391[T] |
| 8 weeks | 47 | 40.41±3.50 | 49 | 40.72±3.50 | 0.5704[T] | |
| p-value [1] | 0.3200 | 0.7725 | ||||
| Platelet (103/μL) |
Baseline | 51 | 250.53±45.59 | 53 | 253.45±38.99 | 0.5324[W] |
| 8 weeks | 47 | 241.49±45.37 | 49 | 249.22±40.50 | 0.9633[T] | |
| p-value [1] | 0.0942 | 0.1531 | ||||
| ALT (GPT) (IU/L) |
Baseline | 51 | 17.80±9.36 | 53 | 19.74±12.93 | 0.6463[W] |
| 8 weeks | 47 | 17.85±9.91 | 49 | 19.24±11.61 | 0.9384[W] | |
| p-value [1] | 0.7919 | 0.5569 | ||||
| BUN (mg/dL) |
Baseline | 51 | 12.99±3.62 | 53 | 13.09±3.55 | 0.8785[W] |
| 8 weeks | 47 | 13.09±3.70 | 49 | 12.58±3.48 | 0.4591[T] | |
| p-value [1] | 0.7682 | 0.4535 | ||||
| Creatinine (mg/dL) |
Baseline | 51 | 0.78±0.17 | 53 | 0.77±0.16 | 0.6303[W] |
| 8 weeks | 47 | 0.75±0.15 | 49 | 0.75±0.15 | 0.5729[T] | |
| p-value [1] | 0.0939 | 0.1186 | ||||
| Ca (mg/dL) |
Baseline | 51 | 9.46±0.34 | 53 | 9.52±0.37 | 0.3455[T] |
| 8 weeks | 47 | 9.47±0.37 | 49 | 9.50±0.30 | 0.6974[T] | |
| p-value [1] | 0.9454 | 0.6203 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



