
Submitted:
07 August 2024
Posted:
08 August 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Long COVID comprises persistent symptoms which extend beyond four weeks post-SARS-CoV-2 infection. The potential association between long COVID and the endorsement of COVID-19 conspiracy theories has not been explored, particularly in Arab countries where high endorsement of these theories has been reported. This study aimed to explore the association between endorsing COVID-19 conspiracy theories and the prevalence of self-reported long COVID symptoms among adults in Jordan and Kuwait in addition to other Arab countries. The study employed a cross-sectional design using an electronic self-administered survey in Arabic language. Recruitment utilized snowball sampling via social media and the survey was distributed in July 2024. The survey instrument included sections on demographic information, the history of COVID-19 infection, and vaccination status. Long COVID manifestations were assessed using a score reflecting the frequency and intensity of ten recognized long COVID symptoms with subsequent categorization into three categories: low, middle, and high. The beliefs in COVID-19 conspiracy theories were measured via a 5-point Likert scale across five items. The final study sample comprised 756 respondents, the majority of whom self-reported a history of confirmed COVID-19 diagnosis at least once (n = 493, 65.2%). The results indicated a neutral average attitude towards COVID-19 conspiracy theories (mean score = 15.18±4.64 out of 30.00). Participants with high conspiracy theories scores were significantly more likely to report high (aOR = 6.85, 95% CI: 2.90–16.13, p < 0.001) and middle long COVID symptoms (aOR = 2.82, 95% CI: 1.32–6.06, p = 0.008) compared to those with lower scores. Additional predictors of higher long COVID reporting included female sex and lower self-reported household income. Frequent COVID-19 infections and hospitalizations were also associated with higher long COVID symptom reporting. The study results revealed a significant correlation between the endorsement of COVID-19 conspiracy theories and the higher frequency and magnitude of long COVID symptom reporting. The findings also highlighted the influence of sociodemographic factors and COVID-19 infection history on long COVID reporting, which suggests that public health strategies should address these factors to mitigate long COVID challenges effectively.
Keywords:
SARS-CoV-2
; Long COVID
; Post-COVID Condition
; Long Haul COVID
; PASC Post Acute Sequelae of COVID-19
; COVID-19 Post-Acute Sequelae
; COVID-19 Conspiracy Theories
; Health Communication
1. Introduction
The COVID-19 pandemic continues to impact daily life despite effective containment strategies [1]. COVID-19 consequences remain substantial due to the emergence of variants of concern, waning immunity over time, and the existence of unvaccinated demographic groups [2]. Additionally, COVID-19 has profoundly affected economic stability and psychosocial dynamics worldwide [3,4].
A significant consequence of the COVID-19 pandemic is the emergence of “long COVID”, which is a condition characterized by persistent symptoms that linger beyond the acute phase of SARS-CoV-2 infection [5,6,7,8]. This phenomenon presents a complex challenge for ongoing public health initiatives and healthcare management, complicated by its broadly defined symptoms and variable duration [7,9,10,11,12,13,14].
Long COVID, also known as Post-Acute Sequelae of SARS-CoV-2 infection (PASC), refers to a range of symptoms that persist for more than four weeks following the initial SARS-CoV-2 infection [15,16,17,18]. These symptoms can affect various organ systems and include fatigue, dyspnea, chest pain, cognitive dysfunction, muscle pain, joint pain, headaches, among other manifestations [19,20,21,22,23,24,25]. The World Health Organization (WHO) defines “long COVID” as the continuation or development of new symptoms three months post-infection, lasting for at least two months, and not explained by alternative diagnoses [26,27].
Studies estimated that the prevalence of long COVID in general practice has been variable depending on the measure used [28,29,30,31]. Common occurrence of long COVID was reported in different studies with rates that can reach up to 78% [32,33,34,35,36,37,38,39]. The risk factors for developing long COVID include female sex, older age, higher body mass index (BMI), smoking, pre-existing comorbidities, and previous hospitalization or intensive care unit (ICU) admission [30,40,41,42,43].
On a separate note, the COVID-19 pandemic witnessed a surge in conspiracy theories related to the virus origin, its vaccination, and the public health control measures [44,45,46,47,48,49,50]. These COVID-19 conspiracies negatively impacted public perceptions and behaviors towards the preventive measures including vaccination hesitancy and lower compliance to non-pharmaceutical intervention (NPI) measures [47,51,52,53,54].
COVID-19 conspiracy theories are unsubstantiated beliefs that propose alternative explanations for the origin, spread, and impact of COVID-19 [47,55,56,57]. These theories reject scientific consensus regarding natural SARS-CoV-2 origin and suggest that powerful groups manipulated or fabricated information on the pandemic for nefarious purposes [58,59,60]. Common conspiracy theories include beliefs that the virus was deliberately constructed as a bioweapon, that the pandemic is a hoax, or that COVID-19 vaccines are harmful and part of a global control agenda [53,61,62,63].
Conspiracy theories can undermine public health efforts by promoting vaccine hesitancy, reducing adherence to NPI measures (e.g., mask-wearing, social distancing), and causing mistrust in health authorities [64,65,66]. In the Middle East, several studies showed that individuals who believe in conspiracy theories were less likely to engage in positive health behaviors that mitigate the spread of different viruses [67,68,69,70,71].
Cognitive biases can play a significant role in the formation and maintenance of conspiracy beliefs [72,73,74]. Confirmation bias entails that individuals seek out information that confirms their pre-existing views and dismiss evidence that contradicts them [75,76]. The uncertainty and anxiety generated by the COVID-19 pandemic can heighten susceptibility to these cognitive biases, as people look for explanations that provide a sense of control and understanding [77,78]. This phenomenon is supported by recent research which reported that individuals who endorsed COVID-19 conspiracy theories reported experiencing more side effects following COVID-19 vaccine uptake [79,80].
Psychological issues including anxiety and depression were widely prevalent during the COVID-19 pandemic and can influence the reporting and perception of physical symptoms [81,82,83,84]. Thereby, psychological issues can lead to psychosomatic phenomena where mental and emotional factors manifest as physical symptoms which was evident during the COVID-19 pandemic [85,86]. Recent evidence suggests that individuals experiencing high levels of stress and anxiety are more likely to report somatic symptoms, which can overlap with those of long COVID [87,88,89,90]. Therefore, exploring the hypothesis that belief in conspiracy theories —which are frequently linked to elevated psychological distress— may correlate with increased reporting of long COVID manifestations appears as a promising area for research investigation.
Several studies investigated the correlation between conspiracy beliefs and health behaviors during the COVID-19 pandemic [64,91,92,93]. The results of various studies indicated that individuals who endorse COVID-19 conspiracy theories are more likely to report negative health outcomes and display mistrust in medical interventions including vaccination [94,95,96,97,98,99,100,101]. However, there is a general lack of studies that assess the potential association between conspiracy beliefs and self-reported long COVID symptoms.
Thus, the current study hypothesis posited that individuals endorsing conspiracy theories may exhibit psychological distress, cognitive biases, or health anxiety, potentially leading to an increased reporting of long COVID symptoms. Consequently, this study aimed to explore the association between self-reported long COVID manifestations and the belief in COVID-19 conspiracy theories in Jordan and Kuwait, where specific conspiratorial ideas regarding infectious diseases were notably prevalent [70,71].
2. Materials and Methods
2.1. Study Design and Ethical Approval
This study was based on a cross-sectional electronic survey. This survey aimed to gather data on the beliefs in COVID-19 conspiracy theories and the prevalence of self-reported long COVID symptoms among a cohort of individuals previously diagnosed with COVID-19 residing in Arab countries with a focus on two Arab countries, namely Jordan and Kuwait based on the nationality of the authors (M.S., R.J.O., and M.B. are Jordanians while K.A.-M., M.A.A., M.A., F.A., N.A., and S.A. are Kuwaiti).
The inclusion criteria were: (1) being an adult aged 18 years or older; (2) had a self-reported, confirmed history of COVID-19 infection; (3) very good reading and writing in Arabic; and (4) providing an electronic consent to participate in the study.
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (IRB) at the School of Pharmacy – Applied Science Private University (Approval number: 2024-PHA-27).
2.2. Recruitment and Data Collection
Recruitment of potential participants was done through a snowball convenience sampling technique, initiated in Jordan and Kuwait by the authors (three Jordanians and six Kuwaiti authors, including eight females and a single male).
Initial participants were contacted directly through social media platforms (WhatsApp, Instagram, Facebook, Snapchat, and Messenger), and were encouraged to share the survey link within their respective networks to ensure a broad community engagement.
The survey was administered electronically via Google Forms, without collecting participant identifiers to ensure anonymity and confidentiality of all participant responses. Prior to participation, electronic informed consent was obtained from all participants, adhering to the ethical permission standards. The survey distribution took place in July 2024 and the participants were not offered any incentives for participation. The survey language was Arabic.
2.3. Sample Size Calculation
The required sample size was determined using G*Power software [102,103], predicated on an anticipated small to medium effect size of 0.3, with an alpha set at 0.050 and aiming for a power of 95.0% as follows. Based on these parameters, the recruitment of 147 participants was required to achieve a sufficient statistical power to detect significant associations between conspiracy beliefs and long COVID symptoms.
2.4. Survey Instrument
Following the introductory section highlighting the aims of the study indicating the assessment of long COVID symptoms that persisted for at least 2 months following recovery from COVID-19, and the informed consent item, the first survey section assessed participant demographics as follows. (1) Age as a scale variable later trichotomized into 3 groups (18 – 39 years vs. 40 – 59 years vs. 60 years or older); (2) Sex (male vs. female); (3) Educational level (high school or less vs. undergraduate vs. postgraduate); (4) Self-reported financial status of household (low-income vs. middle-income vs. high-income); (5) History of chronic disease (yes vs. no); (6) Self-reported wight and height (to measure BMI which was categorized into four categories: <18.5 vs. 18.5–24.9 vs. 25.0–29.9 vs. ≥30); and (7) History of tobacco consumption including cigarettes, narghile, vaping, or any other form of smoking (current vs. ex-smoker vs. never smoked).
The second section inquired about the history of COVID-19, and its vaccination as follows. (1) How many times did you get a confirmed diagnosis of COVID-19? (zero vs. one vs. two vs. three or more); (2) If infected, did you get hospitalized for COVID-19? (yes vs. no); and (3) How many COVID-19 vaccine doses did you receive? (zero vs. 1 dose vs. 2 doses vs. three or more doses).
The third section assessed self-reported long COVID symptoms as follows based on the WHO definition of long COVID [26], with selection of the most commonly prevalent list of long COVID manifestations based on extensive literature review and assessment of content validity by the first and senior authors [19,20,21,22,23,24,25,37,42,104,105,106,107,108,109]. The long COVID symptoms was assessed by asking the participants: On a scale from 0 (not at all), to 1 (rarely), to 2 (often), to 3 (always), how often did you experience these symptoms following your COVID-19 diagnosis compared to the period before your diagnosis? (1) Unusually tired or fatigued; (2) Shortness of breath or difficulty in breathing; (3) Chest pain or discomfort; (4) Difficulty concentrating or memory problems; (5) Muscle or joint pain; (6) Trouble in sleeping or poor sleep quality; (7) Loss or change in your sense of taste or smell; (8) Headaches; (9) Feeling of rapid or irregular heartbeat; and (10) Feeling anxious or depressed. Then, the “long COVID score” was calculated by summing the scores for each individual item.
The final section assessed the endorsement of COVID-19 conspiracy theories using the following five items (assessed on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree) which were constructed based on [67,71,80,110]. (1) Coronavirus was created purposefully by hidden powerful groups to control the global population; (2) COVID-19 dangers were exaggerated by the media and governments to cause fear among the public; (3) The COVID-19 pandemic was a hoax and the virus does not exist; (4) COVID-19 vaccines were a scheme by big pharma companies to make money and control public; and (5) Governments used the COVID-19 pandemic as an excuse to impose restrictions and monitor people closely.
2.5. Statistical and Data Analysis
We implemented a categorization approach to analyze long COVID scores (low=0–9, middle=10–19, and high=20–30) and conspiracy scores (low=5–11, middle=12–18, and high=19–25). The internal consistency of the long COVID score and the COVID-19 conspiracy theories scale was assessed using Cronbach α, a measure to verify that the scale items reliably assessed the same underlying concept, confirming the internal consistency of this novel construct.
To examine associations between categorical variables, we utilized the Chi-Square (χ2) test. To ensure that the scale variables were appropriately distributed for further parametric analysis, we conducted normality testing using the Kolmogorov-Smirnov test. Given the non-normal distribution of the two scale variables (long COVID score as a scale variable and COVID-19 conspiracy theories scale), the Mann-Whitney U test (M-W) and Kruskal-Wallis test (K-W) non-parametric tests were selected. Additionally, we utilized Analysis of Variance (ANOVA) to assess differences in long COVID scores across various sub-groups, employing Eta squared (η²) to quantify effect size and the proportion of variance explained by these differences. Eta squared values were interpreted as follows. η² values from 0 to 0.01 indicated negligible influence; 0.01 to 0.06 represented modest influence with limited but discernible effects; 0.06 to 0.14 suggested a moderate impact where group differences notably affected outcome variance; 0.14 to 0.26 indicated a strong impact with substantial variance accounted for by group differences; and values of 0.26 and above represented an extremely strong influence, where group differences were the primary determinants of outcomes based on Maher et al. [111].
Multinomial logistic regression was employed to assess the associations between multiple independent variables and a categorical dependent variable (long COVID score categories). This regression model was particularly selected due to its efficacy in handling categorical outcomes with more than two categories. We included variables in this model that demonstrated potential significance (p < 0.100) in univariate analyses, suggesting their predictive relevance. The regression model effectiveness was evaluated using Nagelkerke R2, which adjusts the Cox and Snell R2 to a range between 0 and 1, which measures the explained variance by the model comprehensively. Furthermore, to avoid the pitfalls of multicollinearity, which can skew regression analysis results, we tested for multicollinearity using the Variance Inflation Factor (VIF). Our criteria for statistical significance were set at a p value of < 0.050.
All statistical analyses were conducted using IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp.
3. Results
3.1. Study Sample Characteristics
A total of 756 responses were received. A majority of the study respondents were young adults aged 18 – 39 years (n = 460, 60.9%), females (n = 533, 70.6%), undergraduates (n = 464, 61.5%), reported middle household income (n = 512, 67.8%), and were either from Jordan (n = 438, 58.0%) or Kuwait (n = 245, 32.5%) as illustrated in (Table 1). Slightly more than a quarter of the study participants reported a history of chronic disease (n = 193, 25.6%), more than a third of the study participants had a BMI in the range of 25.0 – 29.9 indicating healthy weight (n = 272, 36.0%), and a majority of the participants were non-smokers (n = 496, 65.7%). The majority of participants self-reported a history of confirmed COVID-19 diagnosis either once (n = 297, 39.3%), twice (n = 125, 16.6%), or three times or more (n = 71, 9.4%). For the self-reported history of COVID-19 vaccine uptake, two-thirds of the study participants reported completing the primary vaccination series (n = 329, 66.7%), while 106 participants reported the uptake of booster vaccine doses (21.5%, Table 1).
3.2. The Prevalence of Long COVID among Respondents Who Had Confirmed COVID-19 Diagnosis
The distribution of self-reported long COVID symptoms by the participants with a history of confirmed COVID-19 diagnosis is illustrated in (Figure 1).
The long COVID-19 scale showed a high internal consistency as evidenced by a Cronbach’s α value of 0.907. For the ten long COVID signs/symptoms, the highest average score was reported for muscle or joint pain (mean = 1.86±0.977), followed by feeling unusually tired or fatigued (mean = 1.79±0.886), headaches (mean = 1.68±1.005), trouble in sleeping or poor sleep quality (mean = 1.62±1.018), feeling anxious or depressed (mean = 1.61±1.031), difficulty concentrating or memory problems (mean = 1.58±1.034), feeling of rapid or irregular heartbeat (mean = 1.38±1.008), loss or change in the sense of taste or smell (mean = 1.26±1.082), while the lowest average scores were observed for shortness of breath or difficulty in breathing (mean = 1.19±0.963) and chest pain or discomfort (mean = 1.19±0.964).
For the overall long COVID score in the study sample and on a range from zero to 30 the mean score was 15.2±7.365. The distribution of the long COVID score showed non-normality as evidenced by the Kolmogorov-Smirnov test (p < 0.001). The following variables were significantly associated with higher long COVID scores as shown in (Figure 2). Being a young adult aged 18 – 39 years as opposed to being middle-aged or elderly (mean long COVID scores of 15.61 vs. 14.78 vs. 10.50, p = 0.018, K-W; η2 = 0.017); being a female (mean long COVID scores of 16.37 vs. 12.02, p < 0.001, M-W; η2 = 0.075); having a self-reported low income of household compared to middle and high income (mean long COVID scores of 16.27 vs. 15.39 vs. 12.80, p = 0.011, K-W; η2 = 0.020); having a history of chronic disease (mean long COVID scores of 16.64 vs. 14.64, p = 0.007, M-W; η2 = 0.014); having a confirmed history of COVID-19 diagnosis for three time or more compared to having the diagnosis twice or once (mean long COVID scores of 18.89 vs. 17.43 vs. 13.31, p < 0.001, K-W; η2 = 0.110); a history of hospitalization due to COVID-19 (mean long COVID scores of 17.79 vs. 14.93, p = 0.021, M-W; η2 = 0.011); and high endorsement of COVID-19 conspiracy theories as opposed to middle and low embrace of these theories (mean long COVID scores of 17.89 vs. 14.92 vs. 12.42, p < 0.001, K-W; η2 = 0.066, Figure 2).
By categorizing the long COVID score into three categories, the following variables were associated with a higher probability of having long COVID symptoms: younger age of 18 – 39 years, female sex, low monthly income of household, higher frequency of previous diagnosis of COVID-19, and higher embrace of COVID-19 conspiracy theories (Table 2).
3.3. Reliability of the Conspiracy Belief Scale
The COVID-19 conspiracy theories scale showed a fairly high internal consistency as evidenced by a Cronbach’s α value of 0.844, which confirmed the scale reliability to measure the construct consistently across items. The inter-item correlation analysis showed that the COVID-19 conspiracy theories scale was appropriate for its intended purpose with inter-item correlations ranging from moderate to strong (r = 0.403 to r = 0.748, Figure 3). This result indicated a coherent relationship among the items confirming the scale suitability to form a unified construct for the assessment of COVID-19 conspiracy beliefs.
3.4. The Endorsement of COVID-19 Conspiracy Theories among Respondents Who Had Confirmed COVID-19 Diagnosis
The mean score of COVID-19 conspiracy theories scale was 15.18±4.64 which indicated an overall neutral attitude to these theories among the respondents who reported a confirmed diagnosis of COVID-19. The distribution of the COVID-19 conspiracy theories scale showed non-normality as evidenced by the Kolmogorov-Smirnov test (p < 0.001).
A statistically significant higher embrace of COVID-19 conspiracy theories was noticed among the participants who did not receive COVID-19 vaccination compared to those who received a single dose, two doses, and three or more doses (mean COVID-19 conspiracy theories scores: 15.93 vs. 14.82 vs. 15.51 vs. 14.03, p = 0.021, K-W, Figure 4). Additionally, a statistically significant higher embrace of COVID-19 conspiracy theories was observed among the participants with higher long COVID scores (mean COVID-19 conspiracy theories scores: 16.54 vs. 15.26 vs. 13.20, p < 0.001, K-W, Figure 4).
3.5. Higher Reporting of Long COVID Manifestations Was Associated with the Endorsement of COVID-19 Conspiracy Theories in Multivariate Analysis
In our regression model on possible factors influencing long COVID scores, collinearity diagnostics indicated that all predictor variables exhibited minimal multicollinearity, which ensured the reliability of our regression estimates. The VIF for each predictor remained close to 1, with values ranging from 1.007 for the COVID-19 conspiracy score to 1.022 for the age category, which indicates the absence of substantial collinearity which might affect the analysis.
In multinomial logistic regression analysis, which showed a Nagelkerke R2 value of 0.266, the following variables were independently associated with statistically significant higher reporting of long COVID manifestations among the study respondents. High endorsement of COVID-19 conspiracy theories significantly predicted higher self-reporting of long COVID symptoms. Specifically, individuals scoring high on conspiracy beliefs (19 – 25) were much more likely to report high long COVID symptoms (adjusted Odds Ratio (aOR) = 6.85, 95% CI: 2.90–16.13, p < 0.001) and middle long COVID symptoms (aOR = 2.82, 95% CI: 1.32–6.06, p = 0.008) compared to those with lower scores.
Other significant predictors included sex, with females more likely to report both high (aOR = 5.15, 95% CI: 2.66–10.00, p < 0.001) and middle long COVID symptoms (aOR = 2.11, 95% CI: 1.26–3.55, p = 0.005), and household income, where self-reported low income levels correlated with higher long COVID symptom reporting compared to higher income levels. Furthermore, individuals with frequent COVID-19 diagnoses (three times or more) reported high long COVID symptoms (aOR = 10.31, 95% CI: 3.73–28.57, p < 0.001) and middle long COVID symptoms (aOR = 4.76, 95% CI: 1.81–12.50, p = 0.002), and a history of hospitalization due to COVID-19 was also associated with an increase in high long COVID symptom reporting (aOR = 5.53, 95% CI: 1.66–18.46, p = 0.005, Table 3).
4. Discussion
The findings of this study elucidated the complex interplay of various factors in the reporting of long COVID symptoms among a cohort of adult individuals residing mainly in Jordan and Kuwait. These factors included demographics, health history in terms of frequency and severity of COVID-19, and psychological influences manifested in conspiratorial ideation.
The study findings indicated that myalgia or arthralgia, fatigue, and headaches were the most commonly reported symptoms in long COVID among the study participants in the two Arab countries. This is consistent with the results of various studies and reviews in different regions worldwide [37,112,113]. Specifically, in a systematic review and meta-analysis dating back to 2022, myalgia was reported at a frequency of 22% and fatigue was reported at a rate of 37% at >12-month follow-up [36].
Several hypotheses were cited in recent literature in the pursuit of explaining musculoskeletal symptoms in long COVID-19 as reviewed by Deniz Evcik in [114]. Chronic inflammation, possibly triggered by inflammatory cytokines can reduce muscle protein synthesis [115]. Additionally, the effects of SARS-CoV-2 on myocytes and persistent viral gene particles may promote immune hyperactivation, with ongoing low-grade inflammation associated with long COVID manifestations [109,116,117].
A key and novel finding from our analysis in this study was the substantial impact of endorsing COVID-19 conspiracy theories on the magnitude and frequency of long COVID symptom self-reporting by the participants. In this study, the participants with high conspiracy theories scores were found to be significantly more likely to report long COVID manifestations. The reliability of this result is supported by the validity of the survey instrument used to assess the embrace of COVID-19 conspiracy theories in this study. The strong association between the endorsement of COVID-19 conspiracy theories and the increased reporting of long COVID symptoms was highlighted by an adjusted odds ratio of approximately 7. This statistic indicated that the participants who strongly believe in COVID-19 conspiracies were seven times more likely to report higher long COVID manifestations compared to those who hold few or no such beliefs. This finding emphasizes the significant impact that psychological factors including conspiratorial ideas can have on the perception and reporting of health conditions [118,119].
In our attempt to explain this result, we suggest that the increased reporting of physical symptoms alongside certain psychological constructs may be influenced by attentional bias [120,121]. Attention bias in the context of higher conspiratorial beliefs can heighten awareness of bodily sensations, leading to the misattribution of ordinary physical symptoms to more serious conditions [72]. The results from our multinomial logistic regression analysis emphasized that the interaction between psychological factors and health perceptions is likely mediated by cognitive and emotional responses, which can significantly enhance symptom awareness and reporting [122]. The insight gained from this particular result can enhance the collective understanding of the variability observed in long COVID manifestations and highlights the interplay between psychological constructs and physical health outcomes such as long COVID manifestations.
Another plausible explanation for the observed correlation between endorsing COVID-19 conspiracy theories and more pronounced long COVID manifestations in this study may involve the psychological and social dimensions of conspiracy beliefs. These beliefs may not only reflect broader psychological discomfort and social alienation but also exacerbate the focus on physical sensations which was shown in a study in the context of COVID-19 among senior citizens in China by Chen et al. [123]. This heightened attentiveness can lead to more frequent and intense reporting of symptoms. Thus, the endorsement of conspiracy theories could serve as an indicator of underlying psychological stress, which is known to be associated with increased symptom reporting [122]. This relationship highlights the complex interplay between psychological factors and the perception of health, which highlights the importance of considering these elements when managing long COVID.
Previous studies have shown a strong link between heightened perception of physical symptoms and various psychological constructs, which supports the findings of our current study. For example, Lee et al. demonstrated that somatic symptom burden was closely associated with health anxiety, and both independently contribute to psychological distress, functional impairment, and increased healthcare utilization [124]. Similarly, Santoro et al. found that the severity of somatic symptoms could predict heightened levels of cyberchondria, a condition characterized by excessive and anxiety-driven online searches for health-related information, with health anxiety acting as a partial mediator in this relationship [125]. Pérez-Gay Juárez et al. highlighted the significant uncertainty during the COVID-19 pandemic regarding disease risks, public health measures, and novel vaccine safety [126]. This uncertainty exacerbates the tendency to over-interpret physical symptoms, particularly among individuals with a high intolerance of uncertainty, further supporting the interconnectedness of psychological responses and the perception of physical health during crises [126].
It is important at this point to acknowledge that the participants in our study might indeed experience physical long COVID symptoms at least to some extent. Additionally, it is essential to acknowledge that dismissing the physical nature of long COVID manifestations could have adverse consequences for the millions affected by this pervasive condition [32,33,34,35,36,37,38,39,127]. However, our findings also revealed a clear association between the endorsement of conspiracy theories and an increased perception and reporting of long COVID manifestations. This suggests that psychological factors influenced by misinformation and conspiratorial beliefs play a significant role in the manifestation of long COVID as reviewed by José Mora-Romo in [128]. Addressing these psychological aspects can be essential for effective management of long COVID, as interventions aimed at mitigating these influences could substantially alleviate symptoms of long COVID [89]. These psychological aspects of COVID-19 and long COVID burden have been demonstrated in recent studies from Germany and France [129,130,131]. Although changing deeply entrenched conspiracy beliefs presents a formidable challenge, incorporating psychological interventions into the treatment regimen could significantly improve outcomes for long COVID patients, complementing other medical treatments [128,132].
This study results also highlighted significant sex differences in the reporting of long COVID symptoms. In this study, female participants were more likely than males to report both high and moderate long COVID symptoms, with notable odds ratios indicating a strong sex disparity. This finding is consistent with existing literature suggesting that females may be more perceptive of bodily symptoms or more willing to report health issues [133,134]. Additionally, the social and psychological burdens which were disproportionately carried by females during the COVID-19 pandemic—such as increased caregiving roles and job insecurity—might contribute to higher symptom reporting rates [135,136].
The significantly higher reporting of long COVID manifestations among females in this study is consistent with the findings of previous research as follows. For example, the “Long-COVID in Scotland” study by Hastie et al. demonstrated a notably higher likelihood of no or partial recovery among females following COVID-19 [137]. Similarly, a study by Michael C. Sneller et al. in the U.S. highlighted an increased risk for PASC among females [138]. Additionally, Cohen and Yana van der Meulen Rodgers found that females were not only more prone to long COVID but also more likely to experience significant activity limitations due to the condition [139]. Moreover, a cross-sectional study in Denmark identified female sex as a significant factor, with an odds ratio of 1.7, associated with the development of de novo, multitype, post-COVID pain [140]. These consistent findings across diverse studies in various locations adds further support to our finding of the sex-related disparities in the impact and recovery patterns of long COVID.
Furthermore, our findings indicated that the frequency of COVID-19 diagnoses and prior hospitalizations due to COVID-19 were strong predictors of increased reporting of long COVID manifestations. This correlation likely reflects the direct physiological consequences of severe or recurrent SARS-CoV-2 infections, which tend to result in more pronounced residual health effects. The higher likelihood of long COVID occurrence following severe COVID-19 as indicated by a history of hospitalization or re-infection was highlighted in a recent review [141]. Therefore, the role of vaccination to prevent initial infection and to lessen its severity can be critical for effective mitigation of the risk of long COVID [142,143,144].
Finally, several limitations should be considered when interpreting the findings of our study. First, the cross-sectional design precluded any causal inferences between conspiracy beliefs and the reporting of long COVID symptoms in this study. Second, the reliance on self-reported data introduced the potential for subjective bias, which could lead to the overestimation or underestimation of the true associations between the study variables. Additionally, the study demographic composition, with a predominance of female participants potentially influenced by the majority of female authors, limits the generalizability of the results to broader populations due to the presence of selection bias. Finally, despite the validity of the scales used for assessment of conspiracy beliefs, the lack of a reliable tool for comprehensive assessment of long COVID may have resulted in an element of measurement bias.
5. Conclusions
The correlation between conspiracy beliefs and the reporting of long COVID symptoms in this study highlighted the complex role that cognitive and psychological factors play in health perceptions. This study findings point to the role of individual beliefs, coupled with demographic factors in influencing the reporting of long COVID symptoms. The strong association between conspiracy beliefs and symptom reporting emphasized the need for targeted public health interventions that address misinformation and its broader psychological and societal impacts. Understanding these dynamics is crucial for developing strategies that not only combat the spread of misinformation but also support the identification and treatment of long COVID.
Author Contributions
Conceptualization, M.S.; methodology, M.S., K.A.-M., M.A.A., M.A., F.A., N.A., S.A., R.J.O. and M.B.; software, M.S.; validation, M.S. and M.B.; formal analysis, M.S.; investigation, M.S., K.A.-M., M.A.A., M.A., F.A., N.A., S.A., R.J.O. and M.B.; resources, M.S.; data curation, M.S., K.A.-M., M.A.A., M.A., F.A., N.A., S.A., R.J.O. and M.B.; writing—original draft preparation, M.S.; writing—review and editing, M.S., K.A.-M., M.A.A., M.A., F.A., N.A., S.A., R.J.O. and M.B.; visualization, M.S.; supervision, M.S.; project administration, M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (IRB) at the School of Pharmacy – Applied Science Private University (Approval number: 2024-PHA-27).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ANOVA | Analysis of Variance |
| aOR | Adjusted Odds Ratio |
| BMI | Body mass index |
| CI | Confidence interval |
| COVID | Coronavirus disease |
| ICU | Intensive care unit |
| K-W | Kruskal-Wallis test |
| M-W | Mann-Whitney U test |
| NPI | Non-pharmaceutical intervention |
| PASC | Post-Acute Sequelae of SARS-CoV-2 infection |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| VIF | Variance Inflation Factor |
| WHO | The World Health Organization |
References
- World Health Organization (WHO). COVID-19 epidemiological update – 17 June 2024. Available online: https://www.who.int/publications/m/item/covid-19-epidemiological-update-edition-168 (accessed on 5 August 2024).
- Meyerowitz, E.A.; Scott, J.; Richterman, A.; Male, V.; Cevik, M. Clinical course and management of COVID-19 in the era of widespread population immunity. Nature Reviews Microbiology 2024, 22, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, H.; Sharifi, A.; Damanbagh, S.; Nazarnia, H.; Nazarnia, M. Impacts of the COVID-19 pandemic on the social sphere and lessons for crisis management: a literature review. Natural Hazards 2023, 117, 2139–2164. [Google Scholar] [CrossRef] [PubMed]
- Kunal, K.; Choudhary, P.; Kumar, J.; Prakash, R.; Singh, A.; Kanchan, K. Psychosocial Impact of COVID-19–A Global Scenario. 2022. [CrossRef]
- Jiao, T.; Huang, Y.; Sun, H.; Yang, L. Research progress of post-acute sequelae after SARS-CoV-2 infection. Cell Death & Disease 2024, 15, 257. [Google Scholar] [CrossRef]
- Koc, H.C.; Xiao, J.; Liu, W.; Li, Y.; Chen, G. Long COVID and its Management. Int J Biol Sci 2022, 18, 4768–4780. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Hansel, N. Conceptual and Methodological Barriers to Understanding Long COVID. COVID 2024, 4, 582–591. [Google Scholar] [CrossRef]
- Muthuka, J.K.; Nzioki, J.M.; Kelly, J.O.; Musangi, E.N.; Chebungei, L.C.; Nabaweesi, R.; Kiptoo, M.K. Prevalence and Predictors of Long COVID-19 and the Average Time to Diagnosis in the General Population: A Systematic Review, Meta-Analysis and Meta-Regression. COVID 2024, 4, 968–981. [Google Scholar] [CrossRef]
- Castanares-Zapatero, D.; Chalon, P.; Kohn, L.; Dauvrin, M.; Detollenaere, J.; Maertens de Noordhout, C.; Primus-de Jong, C.; Cleemput, I.; Van den Heede, K. Pathophysiology and mechanism of long COVID: a comprehensive review. Ann Med 2022, 54, 1473–1487. [Google Scholar] [CrossRef] [PubMed]
- Szabo, S.; Zayachkivska, O.; Hussain, A.; Muller, V. What is really 'Long COVID'? Inflammopharmacology 2023, 31, 551–557. [Google Scholar] [CrossRef]
- Krishna, B.; Wills, M.; Sithole, N. Long COVID: what is known and what gaps need to be addressed. Br Med Bull 2023, 147, 6–19. [Google Scholar] [CrossRef]
- Tziolos, N.R.; Ioannou, P.; Baliou, S.; Kofteridis, D.P. Long COVID-19 Pathophysiology: What Do We Know So Far? Microorganisms 2023, 11, 2458. [Google Scholar] [CrossRef]
- Au, L.; Capotescu, C.; Eyal, G.; Finestone, G. Long covid and medical gaslighting: Dismissal, delayed diagnosis, and deferred treatment. SSM Qual Res Health 2022, 2, 100167. [Google Scholar] [CrossRef] [PubMed]
- Henderson, A.D.; Butler-Cole, B.F.; Tazare, J.; Tomlinson, L.A.; Marks, M.; Jit, M.; Briggs, A.; Lin, L.Y.; Carlile, O.; Bates, C.; et al. Clinical coding of long COVID in primary care 2020-2023 in a cohort of 19 million adults: an OpenSAFELY analysis. EClinicalMedicine 2024, 72, 102638. [Google Scholar] [CrossRef] [PubMed]
- Thaweethai, T.; Jolley, S.E.; Karlson, E.W.; Levitan, E.B.; Levy, B.; McComsey, G.A.; McCorkell, L.; Nadkarni, G.N.; Parthasarathy, S.; Singh, U.; et al. Development of a Definition of Postacute Sequelae of SARS-CoV-2 Infection. Jama 2023, 329, 1934–1946. [Google Scholar] [CrossRef] [PubMed]
- Danesh, V.; Arroliga, A.C.; Bourgeois, J.A.; Boehm, L.M.; McNeal, M.J.; Widmer, A.J.; McNeal, T.M.; Kesler, S.R. Symptom Clusters Seen in Adult COVID-19 Recovery Clinic Care Seekers. J Gen Intern Med 2023, 38, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Davis, H.E.; Assaf, G.S.; McCorkell, L.; Wei, H.; Low, R.J.; Re'em, Y.; Redfield, S.; Austin, J.P.; Akrami, A. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine 2021, 38, 101019. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet 2023, 401, e21–e33. [Google Scholar] [CrossRef]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab Syndr 2021, 15, 869–875. [Google Scholar] [CrossRef]
- Aghajani Mir, M. Brain Fog: a Narrative Review of the Most Common Mysterious Cognitive Disorder in COVID-19. Mol Neurobiol 2023. [Google Scholar] [CrossRef]
- Serafini, A.; Tagliaferro, A.; Balbi, F.; Bordo, A.; Bernardi, S.; Berta, G.; Trucco, L.; Perretta, E.; Gualco, E.; Zoccali, P.; et al. Screening of a Small Number of Italian COVID-19 Syndrome Survivors by Means of the Fatigue Assessment Scale: Long COVID Prevalence and the Role of Gender. COVID 2021, 1, 518–527. [Google Scholar] [CrossRef]
- Kaur, A.; Michalopoulos, C.; Carpe, S.; Congrete, S.; Shahzad, H.; Reardon, J.; Wakefield, D.; Swart, C.; ZuWallack, R. Post-COVID-19 Condition and Health Status. COVID 2022, 2, 76–86. [Google Scholar] [CrossRef]
- Luchian, M.-L.; Demeure, F.; Higny, J.; Berners, Y.; Henry, J.; Guedes, A.; Laurence, G.; Saidane, L.; Höcher, A.; Roosens, B.; et al. Three Years of COVID-19 Pandemic—Is the Heart Skipping a Beat? COVID 2023, 3, 715–727. [Google Scholar] [CrossRef]
- Tana, C.; Bentivegna, E.; Cho, S.J.; Harriott, A.M.; García-Azorín, D.; Labastida-Ramirez, A.; Ornello, R.; Raffaelli, B.; Beltrán, E.R.; Ruscheweyh, R.; et al. Long COVID headache. J Headache Pain 2022, 23, 93. [Google Scholar] [CrossRef]
- Su, S.; Zhao, Y.; Zeng, N.; Liu, X.; Zheng, Y.; Sun, J.; Zhong, Y.; Wu, S.; Ni, S.; Gong, Y.; et al. Epidemiology, clinical presentation, pathophysiology, and management of long COVID: an update. Mol Psychiatry 2023, 28, 4056–4069. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Post COVID-19 condition (Long COVID). Available online: https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition (accessed on 7 July 2024).
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis 2022, 22, e102–e107. [Google Scholar] [CrossRef] [PubMed]
- Jeffrey, K.; Woolford, L.; Maini, R.; Basetti, S.; Batchelor, A.; Weatherill, D.; White, C.; Hammersley, V.; Millington, T.; Macdonald, C.; et al. Prevalence and risk factors for long COVID among adults in Scotland using electronic health records: a national, retrospective, observational cohort study. EClinicalMedicine 2024, 71, 102590. [Google Scholar] [CrossRef]
- Hua, M.J.; Gonakoti, S.; Shariff, R.; Corpuz, C.; Acosta, R.A.H.; Chang, H.; Asemota, I.; Gobbi, E.; Rezai, K. Prevalence and Characteristics of Long COVID 7-12 Months After Hospitalization Among Patients From an Urban Safety-Net Hospital: A Pilot Study. AJPM Focus 2023, 2, 100091. [Google Scholar] [CrossRef]
- Huerne, K.; Filion, K.B.; Grad, R.; Ernst, P.; Gershon, A.S.; Eisenberg, M.J. Epidemiological and clinical perspectives of long COVID syndrome. Am J Med Open 2023, 9, 100033. [Google Scholar] [CrossRef] [PubMed]
- Perlis, R.H.; Santillana, M.; Ognyanova, K.; Safarpour, A.; Lunz Trujillo, K.; Simonson, M.D.; Green, J.; Quintana, A.; Druckman, J.; Baum, M.A.; et al. Prevalence and Correlates of Long COVID Symptoms Among US Adults. JAMA Netw Open 2022, 5, e2238804. [Google Scholar] [CrossRef]
- Jangnin, R.; Ritruangroj, W.; Kittisupkajorn, S.; Sukeiam, P.; Inchai, J.; Maneeton, B.; Maneetorn, N.; Chaiard, J.; Theerakittikul, T. Long-COVID Prevalence and Its Association with Health Outcomes in the Post-Vaccine and Antiviral-Availability Era. J Clin Med 2024, 13, 1208. [Google Scholar] [CrossRef]
- Hastie, C.E.; Lowe, D.J.; McAuley, A.; Mills, N.L.; Winter, A.J.; Black, C.; Scott, J.T.; O’Donnell, C.A.; Blane, D.N.; Browne, S.; et al. True prevalence of long-COVID in a nationwide, population cohort study. Nature Communications 2023, 14, 7892. [Google Scholar] [CrossRef]
- Ford, N.D.; Agedew, A.; Dalton, A.F.; Singleton, J.; Perrine, C.G.; Saydah, S. Notes from the Field: Long COVID Prevalence Among Adults - United States, 2022. MMWR Morb Mortal Wkly Rep 2024, 73, 135–136. [Google Scholar] [CrossRef] [PubMed]
- Harris, E. US Survey: About 7% of Adults, 1% of Children Have Had Long COVID. Jama 2023, 330, 1516. [Google Scholar] [CrossRef] [PubMed]
- Alkodaymi, M.S.; Omrani, O.A.; Fawzy, N.A.; Shaar, B.A.; Almamlouk, R.; Riaz, M.; Obeidat, M.; Obeidat, Y.; Gerberi, D.; Taha, R.M.; et al. Prevalence of post-acute COVID-19 syndrome symptoms at different follow-up periods: a systematic review and meta-analysis. Clin Microbiol Infect 2022, 28, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-de-Las-Peñas, C.; Notarte, K.I.; Macasaet, R.; Velasco, J.V.; Catahay, J.A.; Ver, A.T.; Chung, W.; Valera-Calero, J.A.; Navarro-Santana, M. Persistence of post-COVID symptoms in the general population two years after SARS-CoV-2 infection: A systematic review and meta-analysis. J Infect 2024, 88, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Torres-Macho, J.; Macasaet, R.; Velasco, J.V.; Ver, A.T.; Culasino Carandang, T.H.D.; Guerrero, J.J.; Franco-Moreno, A.; Chung, W.; Notarte, K.I. Presence of SARS-CoV-2 RNA in COVID-19 survivors with post-COVID symptoms: a systematic review of the literature. Clin Chem Lab Med 2024, 62, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.H.; Bao, Y.; Chen, S.; Bednarczyk, R.A.; Vasudevan, L.; Corlin, L. Prior COVID-19 Diagnosis, Severe Outcomes, and Long COVID among U.S. Adults, 2022. Vaccines (Basel) 2024, 12, 669. [Google Scholar] [CrossRef] [PubMed]
- Tsampasian, V.; Elghazaly, H.; Chattopadhyay, R.; Debski, M.; Naing, T.K.P.; Garg, P.; Clark, A.; Ntatsaki, E.; Vassiliou, V.S. Risk Factors Associated With Post-COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA Intern Med 2023, 183, 566–580. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, V.; Zanelli, S.; Foppiani, A.; Verduci, E.; Benatti, B.; Bollina, R.; Bombaci, F.; Brucato, A.; Cammarata, S.; Calabrò, E.; et al. Long COVID in Children, Adults, and Vulnerable Populations: A Comprehensive Overview for an Integrated Approach. Diseases 2024, 12, 95. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Raveendran, A.V.; Giordano, R.; Arendt-Nielsen, L. Long COVID or Post-COVID-19 Condition: Past, Present and Future Research Directions. Microorganisms 2023, 11, 2959. [Google Scholar] [CrossRef]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat Med 2022, 28, 1706–1714. [Google Scholar] [CrossRef]
- Pertwee, E.; Simas, C.; Larson, H.J. An epidemic of uncertainty: rumors, conspiracy theories and vaccine hesitancy. Nature Medicine 2022, 28, 456–459. [Google Scholar] [CrossRef] [PubMed]
- Romer, D.; Jamieson, K.H. Conspiracy theories as barriers to controlling the spread of COVID-19 in the U.S. Social Science & Medicine 2020, 263, 113356. [Google Scholar] [CrossRef]
- Jabkowski, P.; Domaradzki, J.; Baranowski, M. Exploring COVID-19 conspiracy theories: education, religiosity, trust in scientists, and political orientation in 26 European countries. Scientific Reports 2023, 13, 18116. [Google Scholar] [CrossRef] [PubMed]
- van Mulukom, V.; Pummerer, L.J.; Alper, S.; Bai, H.; Čavojová, V.; Farias, J.; Kay, C.S.; Lazarevic, L.B.; Lobato, E.J.C.; Marinthe, G.; et al. Antecedents and consequences of COVID-19 conspiracy beliefs: A systematic review. Soc Sci Med 2022, 301, 114912. [Google Scholar] [CrossRef]
- Fotakis, E.A.; Simou, E. Belief in COVID-19 related conspiracy theories around the globe: A systematic review. Health Policy 2023, 137, 104903. [Google Scholar] [CrossRef]
- Freeman, D.; Waite, F.; Rosebrock, L.; Petit, A.; Causier, C.; East, A.; Jenner, L.; Teale, A.-L.; Carr, L.; Mulhall, S.; et al. Coronavirus conspiracy beliefs, mistrust, and compliance with government guidelines in England. Psychological Medicine 2022, 52, 251–263. [Google Scholar] [CrossRef]
- Brown, P.; Waite, F.; Larkin, M.; Lambe, S.; McShane, H.; Pollard, A.J.; Freeman, D. “It seems impossible that it’s been made so quickly”: a qualitative investigation of concerns about the speed of COVID-19 vaccine development and how these may be overcome. Human Vaccines & Immunotherapeutics 2022, 18, 2004808. [Google Scholar] [CrossRef]
- Hughes, J.P.; Efstratiou, A.; Komer, S.R.; Baxter, L.A.; Vasiljevic, M.; Leite, A.C. The impact of risk perceptions and belief in conspiracy theories on COVID-19 pandemic-related behaviours. PLoS One 2022, 17, e0263716. [Google Scholar] [CrossRef]
- Pinazo-Calatayud, D.; Agut-Nieto, S.; Arahuete, L.; Peris, R.; Barros, A.; Vázquez-Rodríguez, C. The strength of conspiracy beliefs versus scientific information: the case of COVID 19 preventive behaviours. Frontiers in Psychology 2024, 15, 1325600. [Google Scholar] [CrossRef]
- De Coninck, D.; Frissen, T.; Matthijs, K.; d’Haenens, L.; Lits, G.; Champagne-Poirier, O.; Carignan, M.-E.; David, M.D.; Pignard-Cheynel, N.; Salerno, S.; et al. Beliefs in Conspiracy Theories and Misinformation About COVID-19: Comparative Perspectives on the Role of Anxiety, Depression and Exposure to and Trust in Information Sources. Frontiers in Psychology 2021, 12, 646394. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines (Basel) 2021, 9, 160. [Google Scholar] [CrossRef]
- Ferreira, S.; Campos, C.; Marinho, B.; Rocha, S.; Fonseca-Pedrero, E.; Barbosa Rocha, N. What drives beliefs in COVID-19 conspiracy theories? The role of psychotic-like experiences and confinement-related factors. Soc Sci Med 2022, 292, 114611. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Gay Juárez, F.; Khayyat, L.; Ronca, M.; Gold, I. Viral Belief: The Psychology of COVID Conspiracy Theories. 2024; pp. 53-79. [CrossRef]
- van Prooijen, J.W.; Douglas, K.M. Belief in conspiracy theories: Basic principles of an emerging research domain. Eur J Soc Psychol 2018, 48, 897–908. [Google Scholar] [CrossRef] [PubMed]
- Hartman, T.K.; Marshall, M.; Stocks, T.V.A.; McKay, R.; Bennett, K.; Butter, S.; Gibson Miller, J.; Hyland, P.; Levita, L.; Martinez, A.P.; et al. Different Conspiracy Theories Have Different Psychological and Social Determinants: Comparison of Three Theories About the Origins of the COVID-19 Virus in a Representative Sample of the UK Population. Frontiers in Political Science 2021, 3, 642510. [Google Scholar] [CrossRef]
- Hakim, M.S. SARS-CoV-2, Covid-19, and the debunking of conspiracy theories. Rev Med Virol 2021, 31, e2222. [Google Scholar] [CrossRef] [PubMed]
- Douglas, K.M. COVID-19 conspiracy theories. Group Processes & Intergroup Relations 2021, 24, 270–275. [Google Scholar] [CrossRef]
- Tsamakis, K.; Tsiptsios, D.; Stubbs, B.; Ma, R.; Romano, E.; Mueller, C.; Ahmad, A.; Triantafyllis, A.S.; Tsitsas, G.; Dragioti, E. Summarising data and factors associated with COVID-19 related conspiracy theories in the first year of the pandemic: a systematic review and narrative synthesis. BMC Psychol 2022, 10, 244. [Google Scholar] [CrossRef]
- Imhoff, R.; Lamberty, P. A Bioweapon or a Hoax? The Link Between Distinct Conspiracy Beliefs About the Coronavirus Disease (COVID-19) Outbreak and Pandemic Behavior. Social Psychological and Personality Science 2020, 11, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.S.; Kamal, A.M.; Kabir, A.; Southern, D.L.; Khan, S.H.; Hasan, S.M.M.; Sarkar, T.; Sharmin, S.; Das, S.; Roy, T.; et al. COVID-19 vaccine rumors and conspiracy theories: The need for cognitive inoculation against misinformation to improve vaccine adherence. PLoS One 2021, 16, e0251605. [Google Scholar] [CrossRef]
- Juanchich, M.; Sirota, M.; Jolles, D.; Whiley, L.A. Are COVID-19 conspiracies a threat to public health? Psychological characteristics and health protective behaviours of believers. Eur J Soc Psychol 2021, 51, 969–989. [Google Scholar] [CrossRef]
- Bierwiaczonek, K.; Gundersen, A.B.; Kunst, J.R. The role of conspiracy beliefs for COVID-19 health responses: A meta-analysis. Curr Opin Psychol 2022, 46, 101346. [Google Scholar] [CrossRef] [PubMed]
- Camargo, E.L.; Ribeiro, C.J.; Santos, G.R.; Almeida, V.S.; Carvalho, H.E.; Schneider, G.; Vieira, L.G.; Alvim, A.L.; Pimenta, F.G.; Carneiro, L.M.; et al. Belief in Conspiracy Theories about COVID-19 Vaccines among Brazilians: A National Cross-Sectional Study. COVID 2024, 4, 518–530. [Google Scholar] [CrossRef]
- Sallam, M.; Kareem, N.; Alkurtas, M. The negative impact of misinformation and vaccine conspiracy on COVID-19 vaccine uptake and attitudes among the general public in Iraq. Prev Med Rep 2024, 43, 102791. [Google Scholar] [CrossRef] [PubMed]
- Alsanafi, M.; Salim, N.A.; Sallam, M. Willingness to get HPV vaccination among female university students in Kuwait and its relation to vaccine conspiracy beliefs. Hum Vaccin Immunother 2023, 19, 2194772. [Google Scholar] [CrossRef]
- Sallam, M.; Ghazy, R.M.; Al-Salahat, K.; Al-Mahzoum, K.; AlHadidi, N.M.; Eid, H.; Kareem, N.; Al-Ajlouni, E.; Batarseh, R.; Ababneh, N.A.; et al. The Role of Psychological Factors and Vaccine Conspiracy Beliefs in Influenza Vaccine Hesitancy and Uptake among Jordanian Healthcare Workers during the COVID-19 Pandemic. Vaccines (Basel) 2022, 10, 1355. [Google Scholar] [CrossRef]
- Alsanafi, M.; Al-Mahzoum, K.; Sallam, M. Monkeypox Knowledge and Confidence in Diagnosis and Management with Evaluation of Emerging Virus Infection Conspiracies among Health Professionals in Kuwait. Pathogens 2022, 11, 994. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines (Basel) 2021, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Gagliardi, L. The role of cognitive biases in conspiracy beliefs: A literature review. Journal of Economic Surveys 2023, n/a. [Google Scholar] [CrossRef]
- Douglas, K.M.; Sutton, R.M.; Callan, M.J.; Dawtry, R.J.; Harvey, A.J. Someone is pulling the strings: hypersensitive agency detection and belief in conspiracy theories. Thinking & Reasoning 2016, 22, 57–77. [Google Scholar] [CrossRef]
- Douglas, K.M.; Sutton, R.M.; Cichocka, A. The Psychology of Conspiracy Theories. Current Directions in Psychological Science 2017, 26, 538–542. [Google Scholar] [CrossRef]
- Hart, W.; Albarracín, D.; Eagly, A.H.; Brechan, I.; Lindberg, M.J.; Merrill, L. Feeling validated versus being correct: a meta-analysis of selective exposure to information. Psychol Bull 2009, 135, 555–588. [Google Scholar] [CrossRef]
- Kaanders, P.; Sepulveda, P.; Folke, T.; Ortoleva, P.; De Martino, B. Humans actively sample evidence to support prior beliefs. Elife 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Kindred, R.; Bates, G.W. The Influence of the COVID-19 Pandemic on Social Anxiety: A Systematic Review. Int J Environ Res Public Health 2023, 20, 2362. [Google Scholar] [CrossRef] [PubMed]
- Carnahan, N.D.; Carter, M.M.; Sbrocco, T. Intolerance of Uncertainty, Looming Cognitive Style, and Avoidant Coping as Predictors of Anxiety and Depression During COVID-19: a Longitudinal Study. International Journal of Cognitive Therapy 2022, 15, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Alshehri, S.; Sallam, M. Vaccine conspiracy association with higher COVID-19 vaccination side effects and negative attitude towards booster COVID-19, influenza and monkeypox vaccines: A pilot study in Saudi Universities. Hum Vaccin Immunother 2023, 19, 2275962. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Abbasi, H.; Obeidat, R.J.; Badayneh, R.; Alkhashman, F.; Obeidat, A.; Oudeh, D.; Uqba, Z.; Mahafzah, A. Unraveling the association between vaccine attitude, vaccine conspiracies and self-reported side effects following COVID-19 vaccination among nurses and physicians in Jordan. Vaccine X 2023, 15, 100405. [Google Scholar] [CrossRef]
- Aljaberi, M.A.; Al-Sharafi, M.A.; Uzir, M.U.H.; Sabah, A.; Ali, A.M.; Lee, K.H.; Alsalahi, A.; Noman, S.; Lin, C.Y. Psychological Toll of the COVID-19 Pandemic: An In-Depth Exploration of Anxiety, Depression, and Insomnia and the Influence of Quarantine Measures on Daily Life. Healthcare (Basel) 2023, 11, 2418. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The psychological impact of COVID-19 on the mental health in the general population. Qjm 2020, 113, 531–537. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Aikebaier, S. COVID-19, new challenges to human safety: a global review. Front Public Health 2024, 12, 1371238. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int J Environ Res Public Health 2020, 17, 1729. [Google Scholar] [CrossRef]
- Zidkova, R.; Malinakova, K.; van Dijk, J.P.; Tavel, P. The Coronavirus Pandemic and the Occurrence of Psychosomatic Symptoms: Are They Related? Int J Environ Res Public Health 2021, 18, 3570. [Google Scholar] [CrossRef]
- Aaseth, K.; Grande, R.B.; Leiknes, K.A.; Benth, J.; Lundqvist, C.; Russell, M.B. Personality traits and psychological distress in persons with chronic tension-type headache. The Akershus study of chronic headache. Acta Neurol Scand 2011, 124, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Yap, E.C. Myofascial pain--an overview. Ann Acad Med Singap 2007, 36, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Lemogne, C.; Gouraud, C.; Pitron, V.; Ranque, B. Why the hypothesis of psychological mechanisms in long COVID is worth considering. J Psychosom Res 2023, 165, 111135. [Google Scholar] [CrossRef] [PubMed]
- Leibovitz, T.; Shamblaw, A.L.; Rumas, R.; Best, M.W. COVID-19 conspiracy beliefs: Relations with anxiety, quality of life, and schemas. Pers Individ Dif 2021, 175, 110704. [Google Scholar] [CrossRef] [PubMed]
- Earnshaw, V.A.; Eaton, L.A.; Kalichman, S.C.; Brousseau, N.M.; Hill, E.C.; Fox, A.B. COVID-19 conspiracy beliefs, health behaviors, and policy support. Transl Behav Med 2020, 10, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Simione, L.; Vagni, M.; Gnagnarella, C.; Bersani, G.; Pajardi, D. Mistrust and Beliefs in Conspiracy Theories Differently Mediate the Effects of Psychological Factors on Propensity for COVID-19 Vaccine. Front Psychol 2021, 12, 683684. [Google Scholar] [CrossRef] [PubMed]
- Jolley, D.; Marques, M.D.; Cookson, D. Shining a spotlight on the dangerous consequences of conspiracy theories. Curr Opin Psychol 2022, 47, 101363. [Google Scholar] [CrossRef]
- van Prooijen, J.W.; Etienne, T.W.; Kutiyski, Y.; Krouwel, A.P.M. Conspiracy beliefs prospectively predict health behavior and well-being during a pandemic. Psychol Med 2023, 53, 2514–2521. [Google Scholar] [CrossRef]
- Tselebis, A.; Sikaras, C.; Milionis, C.; Sideri, E.P.; Fytsilis, K.; Papageorgiou, S.M.; Ilias, I.; Pachi, A. A Moderated Mediation Model of the Influence of Cynical Distrust, Medical Mistrust, and Anger on Vaccination Hesitancy in Nursing Staff. Eur J Investig Health Psychol Educ 2023, 13, 2373–2387. [Google Scholar] [CrossRef]
- Bogart, L.M.; Ojikutu, B.O.; Tyagi, K.; Klein, D.J.; Mutchler, M.G.; Dong, L.; Lawrence, S.J.; Thomas, D.R.; Kellman, S. COVID-19 Related Medical Mistrust, Health Impacts, and Potential Vaccine Hesitancy Among Black Americans Living With HIV. J Acquir Immune Defic Syndr 2021, 86, 200–207. [Google Scholar] [CrossRef]
- Pivetti, M.; Paleari, F.-G.; Ertan, I.; Di Battista, S.; Ulukök, E. COVID-19 conspiracy beliefs and vaccinations: A conceptual replication study in Turkey. Journal of Pacific Rim Psychology 2023, 17, 18344909231170097. [Google Scholar] [CrossRef]
- Allen, J.D.; Fu, Q.; Shrestha, S.; Nguyen, K.H.; Stopka, T.J.; Cuevas, A.; Corlin, L. Medical mistrust, discrimination, and COVID-19 vaccine behaviors among a national sample U.S. adults. SSM Popul Health 2022, 20, 101278. [Google Scholar] [CrossRef]
- Carrieri, V.; Guthmuller, S.; Wübker, A. Trust and COVID-19 vaccine hesitancy. Scientific Reports 2023, 13, 9245. [Google Scholar] [CrossRef]
- Regazzi, L.; Lontano, A.; Cadeddu, C.; Di Padova, P.; Rosano, A. Conspiracy beliefs, COVID-19 vaccine uptake and adherence to public health interventions during the pandemic in Europe. European Journal of Public Health 2023, 33, 717–724. [Google Scholar] [CrossRef]
- Georgiou, N.; Delfabbro, P.; Balzan, R. COVID-19-related conspiracy beliefs and their relationship with perceived stress and pre-existing conspiracy beliefs. Pers Individ Dif 2020, 166, 110201. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Moro-López-Menchero, P.; Martín-Sanz, M.B.; Fernandez-de-Las-Peñas, C.; Gómez-Sanchez, S.M.; Gil-Crujera, A.; Ceballos-García, L.; Escribano-Mediavilla, N.I.; Fuentes-Fuentes, M.V.; Palacios-Ceña, D. Living and Coping with Olfactory and Taste Disorders: A Qualitative Study of People with Long-COVID-19. Healthcare (Basel) 2024, 12, 754. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Guijarro, C.; Velasco-Arribas, M.; Torres-Macho, J.; Franco-Moreno, A.; Truini, A.; Pellicer-Valero, O.; Arendt-Nielsen, L. Neuropathic post-COVID pain symptomatology is not associated with serological biomarkers at hospital admission and hospitalization treatment in COVID-19 survivors. Front Med (Lausanne) 2023, 10, 1301970. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Ryan-Murua, P.; Rodríguez-Jiménez, J.; Palacios-Ceña, M.; Arendt-Nielsen, L.; Torres-Macho, J. Serological Biomarkers at Hospital Admission Are Not Related to Long-Term Post-COVID Fatigue and Dyspnea in COVID-19 Survivors. Respiration 2022, 101, 658–665. [Google Scholar] [CrossRef]
- Matias-Guiu, J.A.; Delgado-Alonso, C.; Díez-Cirarda, M.; Martínez-Petit, Á.; Oliver-Mas, S.; Delgado-Álvarez, A.; Cuevas, C.; Valles-Salgado, M.; Gil, M.J.; Yus, M.; et al. Neuropsychological Predictors of Fatigue in Post-COVID Syndrome. J Clin Med 2022, 11, 3886. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nature Medicine 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Donald, J.; Bilasy, S.E.; Yang, C.; El-Shamy, A. Exploring the Complexities of Long COVID. Viruses 2024, 16, 1060. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Taim, D.; Eid, H.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. COVID-19 misinformation: Mere harmless delusions or much more? A knowledge and attitude cross-sectional study among the general public residing in Jordan. PLoS One 2020, 15, e0243264. [Google Scholar] [CrossRef] [PubMed]
- Maher, J.M.; Markey, J.C.; Ebert-May, D. The Other Half of the Story: Effect Size Analysis in Quantitative Research. CBE—Life Sciences Education 2013, 12, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Torres-Macho, J.; Ruiz-Ruigómez, M.; Arrieta-Ortubay, E.; Rodríguez-Rebollo, C.; Akasbi-Moltalvo, M.; Pardo-Guimerá, V.; Ryan-Murua, P.; Lumbreras-Bermejo, C.; Pellicer-Valero, O.J.; et al. Presence of SARS-CoV-2 RNA in COVID-19 survivors with post-COVID symptoms 2 years after hospitalization: The VIPER study. J Med Virol 2024, 96, e29676. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Pellicer-Valero, O.J.; Martín-Guerrero, J.D.; Hernández-Barrera, V.; Arendt-Nielsen, L. Investigating the fluctuating nature of post-COVID pain symptoms in previously hospitalized COVID-19 survivors: the LONG-COVID-EXP multicenter study. PAIN Reports 2024, 9. [Google Scholar] [CrossRef]
- Evcik, D. Musculoskeletal involvement: COVID-19 and post COVID 19. Turk J Phys Med Rehabil 2023, 69, 1–7. [Google Scholar] [CrossRef]
- Peter, R.S.; Nieters, A.; Kräusslich, H.G.; Brockmann, S.O.; Göpel, S.; Kindle, G.; Merle, U.; Steinacker, J.M.; Rothenbacher, D.; Kern, W.V. Post-acute sequelae of covid-19 six to 12 months after infection: population based study. Bmj 2022, 379, e071050. [Google Scholar] [CrossRef] [PubMed]
- Diar Bakerly, N.; Smith, N.; Darbyshire, J.L.; Kwon, J.; Bullock, E.; Baley, S.; Sivan, M.; Delaney, B. Pathophysiological Mechanisms in Long COVID: A Mixed Method Systematic Review. Int J Environ Res Public Health 2024, 21. [Google Scholar] [CrossRef] [PubMed]
- Jiao, T.; Huang, Y.; Sun, H.; Yang, L. Research progress of post-acute sequelae after SARS-CoV-2 infection. Cell Death Dis 2024, 15, 257. [Google Scholar] [CrossRef] [PubMed]
- Douglas, K.M.; Sutton, R.M.; Cichocka, A. The Psychology of Conspiracy Theories. Curr Dir Psychol Sci 2017, 26, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.-y.; Chan, H.-W.; Douglas, K.M. Conspiracy Theories about Infectious Diseases: An Introduction. Journal of Pacific Rim Psychology 2021, 15, 18344909211057657. [Google Scholar] [CrossRef]
- Bar-Haim, Y.; Lamy, D.; Pergamin, L.; Bakermans-Kranenburg, M.J.; van, I.M.H. Threat-related attentional bias in anxious and nonanxious individuals: a meta-analytic study. Psychol Bull 2007, 133, 1–24. [Google Scholar] [CrossRef]
- Salkovskis, P.; Warwick, H.; Deale, A. Cognitive-Behavioral Treatment for Severe and Persistent Health Anxiety (Hypochondriasis). Brief Treatment and Crisis Intervention 2003, 3. [Google Scholar] [CrossRef]
- Schneiderman, N.; Ironson, G.; Siegel, S.D. Stress and health: psychological, behavioral, and biological determinants. Annu Rev Clin Psychol 2005, 1, 607–628. [Google Scholar] [CrossRef]
- Chen, W.C.; Chen, S.J.; Zhong, B.L. Sense of Alienation and Its Associations With Depressive Symptoms and Poor Sleep Quality in Older Adults Who Experienced the Lockdown in Wuhan, China, During the COVID-19 Pandemic. J Geriatr Psychiatry Neurol 2022, 35, 215–222. [Google Scholar] [CrossRef]
- Lee, S.; Creed, F.H.; Ma, Y.L.; Leung, C.M. Somatic symptom burden and health anxiety in the population and their correlates. J Psychosom Res 2015, 78, 71–76. [Google Scholar] [CrossRef]
- Santoro, G.; Starcevic, V.; Scalone, A.; Cavallo, J.; Musetti, A.; Schimmenti, A. The Doctor Is In(ternet): The Mediating Role of Health Anxiety in the Relationship between Somatic Symptoms and Cyberchondria. J Pers Med 2022, 12, 1490. [Google Scholar] [CrossRef]
- Pérez-Gay Juárez, F.; Solomonova, E.; Nephtali, E.; Gold, I. Conspiracies and contagion: Two patterns of COVID-19 related beliefs associated with distinct mental symptomatology. Psychiatry Research Communications 2024, 4, 100153. [Google Scholar] [CrossRef]
- Gorna, R.; MacDermott, N.; Rayner, C.; O'Hara, M.; Evans, S.; Agyen, L.; Nutland, W.; Rogers, N.; Hastie, C. Long COVID guidelines need to reflect lived experience. Lancet 2021, 397, 455–457. [Google Scholar] [CrossRef] [PubMed]
- Mora-Romo, J. Health psychology on long COVID: Strategies based on NICE and WHO guidelines recommendations. Salud mental 2022, 45, 199–208. [Google Scholar] [CrossRef]
- Bahmer, T.; Borzikowsky, C.; Lieb, W.; Horn, A.; Krist, L.; Fricke, J.; Scheibenbogen, C.; Rabe, K.F.; Maetzler, W.; Maetzler, C.; et al. Severity, predictors and clinical correlates of Post-COVID syndrome (PCS) in Germany: A prospective, multi-centre, population-based cohort study. EClinicalMedicine 2022, 51, 101549. [Google Scholar] [CrossRef] [PubMed]
- Engelmann, P.; Löwe, B.; Brehm, T.T.; Weigel, A.; Ullrich, F.; Addo, M.M.; Schulze Zur Wiesch, J.; Lohse, A.W.; Toussaint, A. Risk factors for worsening of somatic symptom burden in a prospective cohort during the COVID-19 pandemic. Front Psychol 2022, 13, 1022203. [Google Scholar] [CrossRef]
- Gouraud, C.; Bottemanne, H.; Lahlou-Laforêt, K.; Blanchard, A.; Günther, S.; Batti, S.E.; Auclin, E.; Limosin, F.; Hulot, J.S.; Lebeaux, D.; et al. Association Between Psychological Distress, Cognitive Complaints, and Neuropsychological Status After a Severe COVID-19 Episode: A Cross-Sectional Study. Front Psychiatry 2021, 12, 725861. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.N.; Ling, M.; Kerr, J.R.; Hill, S.R.; Marques, M.D.; Mawson, H.; Clarke, E.J.R. People do change their beliefs about conspiracy theories—but not often. Scientific Reports 2024, 14, 3836. [Google Scholar] [CrossRef]
- Barsky, A.J.; Peekna, H.M.; Borus, J.F. Somatic symptom reporting in women and men. J Gen Intern Med 2001, 16, 266–275. [Google Scholar] [CrossRef]
- Fillingim, R.B. Sex, gender, and pain: women and men really are different. Curr Rev Pain 2000, 4, 24–30. [Google Scholar] [CrossRef]
- Wade, M.; Prime, H.; Johnson, D.; May, S.S.; Jenkins, J.M.; Browne, D.T. The disparate impact of COVID-19 on the mental health of female and male caregivers. Soc Sci Med 2021, 275, 113801. [Google Scholar] [CrossRef]
- Purvis, R.S.; Ayers, B.L.; Rowland, B.; Moore, R.; Hallgren, E.; McElfish, P.A. "Life is hard": How the COVID-19 pandemic affected daily stressors of women. Dialogues Health 2022, 1, 100018. [Google Scholar] [CrossRef]
- Hastie, C.E.; Lowe, D.J.; McAuley, A.; Winter, A.J.; Mills, N.L.; Black, C.; Scott, J.T.; O'Donnell, C.A.; Blane, D.N.; Browne, S.; et al. Outcomes among confirmed cases and a matched comparison group in the Long-COVID in Scotland study. Nat Commun 2022, 13, 5663. [Google Scholar] [CrossRef]
- Sneller, M.C.; Liang, C.J.; Marques, A.R.; Chung, J.Y.; Shanbhag, S.M.; Fontana, J.R.; Raza, H.; Okeke, O.; Dewar, R.L.; Higgins, B.P.; et al. A Longitudinal Study of COVID-19 Sequelae and Immunity: Baseline Findings. Ann Intern Med 2022, 175, 969–979. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; van der Meulen Rodgers, Y. An intersectional analysis of long COVID prevalence. Int J Equity Health 2023, 22, 261. [Google Scholar] [CrossRef] [PubMed]
- Ebbesen, B.D.; Giordano, R.; Hedegaard, J.N.; Calero, J.A.V.; Fernández-de-las-Peñas, C.; Rasmussen, B.S.; Nielsen, H.; Schiøttz-Christensen, B.; Petersen, P.L.; Castaldo, M.; et al. Prevalence and Risk Factors of Multitype Post-COVID Pain in a Cohort of Previously Hospitalized COVID-19 Survivors: A Danish Cross-Sectional Survey. The Journal of Pain. [CrossRef]
- Boufidou, F.; Medić, S.; Lampropoulou, V.; Siafakas, N.; Tsakris, A.; Anastassopoulou, C. SARS-CoV-2 Reinfections and Long COVID in the Post-Omicron Phase of the Pandemic. Int J Mol Sci 2023, 24, 12962. [Google Scholar] [CrossRef] [PubMed]
- Català, M.; Mercadé-Besora, N.; Kolde, R.; Trinh, N.T.H.; Roel, E.; Burn, E.; Rathod-Mistry, T.; Kostka, K.; Man, W.Y.; Delmestri, A.; et al. The effectiveness of COVID-19 vaccines to prevent long COVID symptoms: staggered cohort study of data from the UK, Spain, and Estonia. Lancet Respir Med 2024, 12, 225–236. [Google Scholar] [CrossRef]
- Brannock, M.D.; Chew, R.F.; Preiss, A.J.; Hadley, E.C.; Redfield, S.; McMurry, J.A.; Leese, P.J.; Girvin, A.T.; Crosskey, M.; Zhou, A.G.; et al. Long COVID risk and pre-COVID vaccination in an EHR-based cohort study from the RECOVER program. Nature Communications 2023, 14, 2914. [Google Scholar] [CrossRef]
- Richard, S.A.; Pollett, S.D.; Fries, A.C.; Berjohn, C.M.; Maves, R.C.; Lalani, T.; Smith, A.G.; Mody, R.M.; Ganesan, A.; Colombo, R.E.; et al. Persistent COVID-19 Symptoms at 6 Months After Onset and the Role of Vaccination Before or After SARS-CoV-2 Infection. JAMA Netw Open 2023, 6, e2251360. [Google Scholar] [CrossRef]
Figure 1.
The frequency of long COVID symptoms as reported by the participants with a confirmed history of COVID-19 diagnosis (n = 493).
Figure 1.
The frequency of long COVID symptoms as reported by the participants with a confirmed history of COVID-19 diagnosis (n = 493).
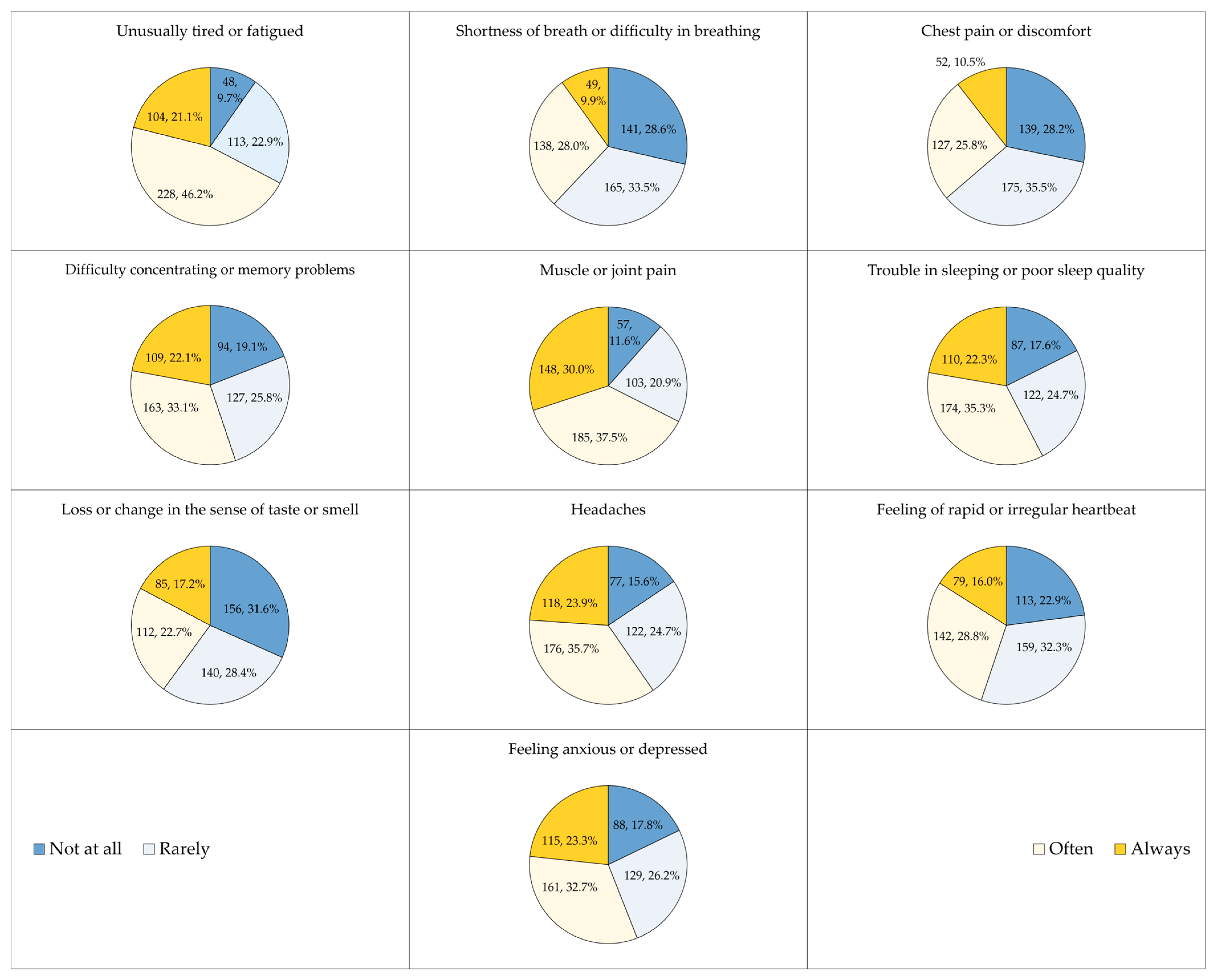
Figure 2.
The association between the long COVID scores and the study variables (n = 493) shown as error bars representing the 95% confidence intervals (CIs) of the mean. K-W: Kruskal Wallis H test; M-W: Mann Whiteny U test; BMI: Body Mass Index; COVID-19 conspiracy score: Calculated based on five items assessed using a 5-point Likert scale.
Figure 2.
The association between the long COVID scores and the study variables (n = 493) shown as error bars representing the 95% confidence intervals (CIs) of the mean. K-W: Kruskal Wallis H test; M-W: Mann Whiteny U test; BMI: Body Mass Index; COVID-19 conspiracy score: Calculated based on five items assessed using a 5-point Likert scale.
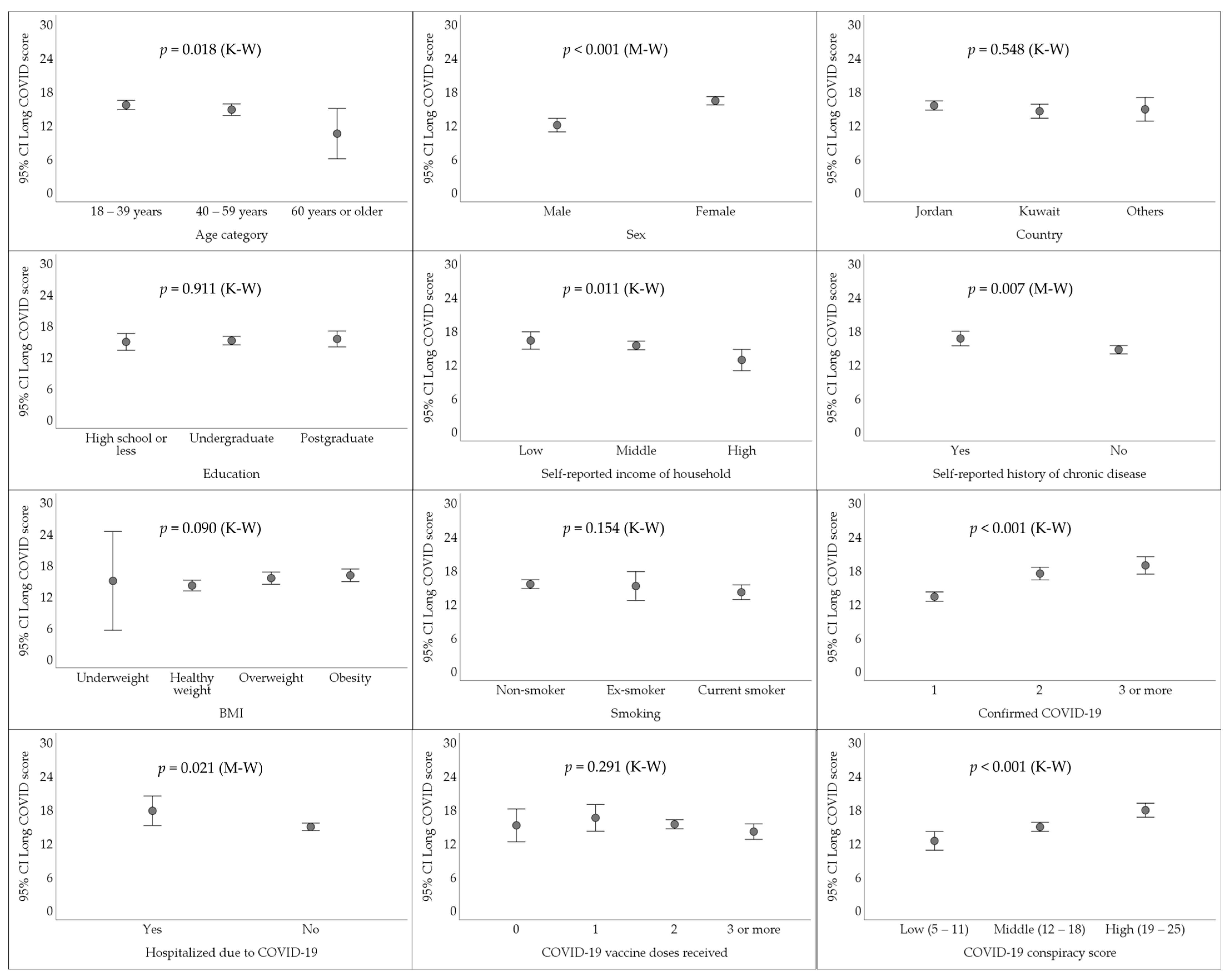
Figure 3.
The inter-item correlation matrix for the COVID-19 conspiracy theories scale. Higher correlations are indicated by deep shades of green.
Figure 3.
The inter-item correlation matrix for the COVID-19 conspiracy theories scale. Higher correlations are indicated by deep shades of green.
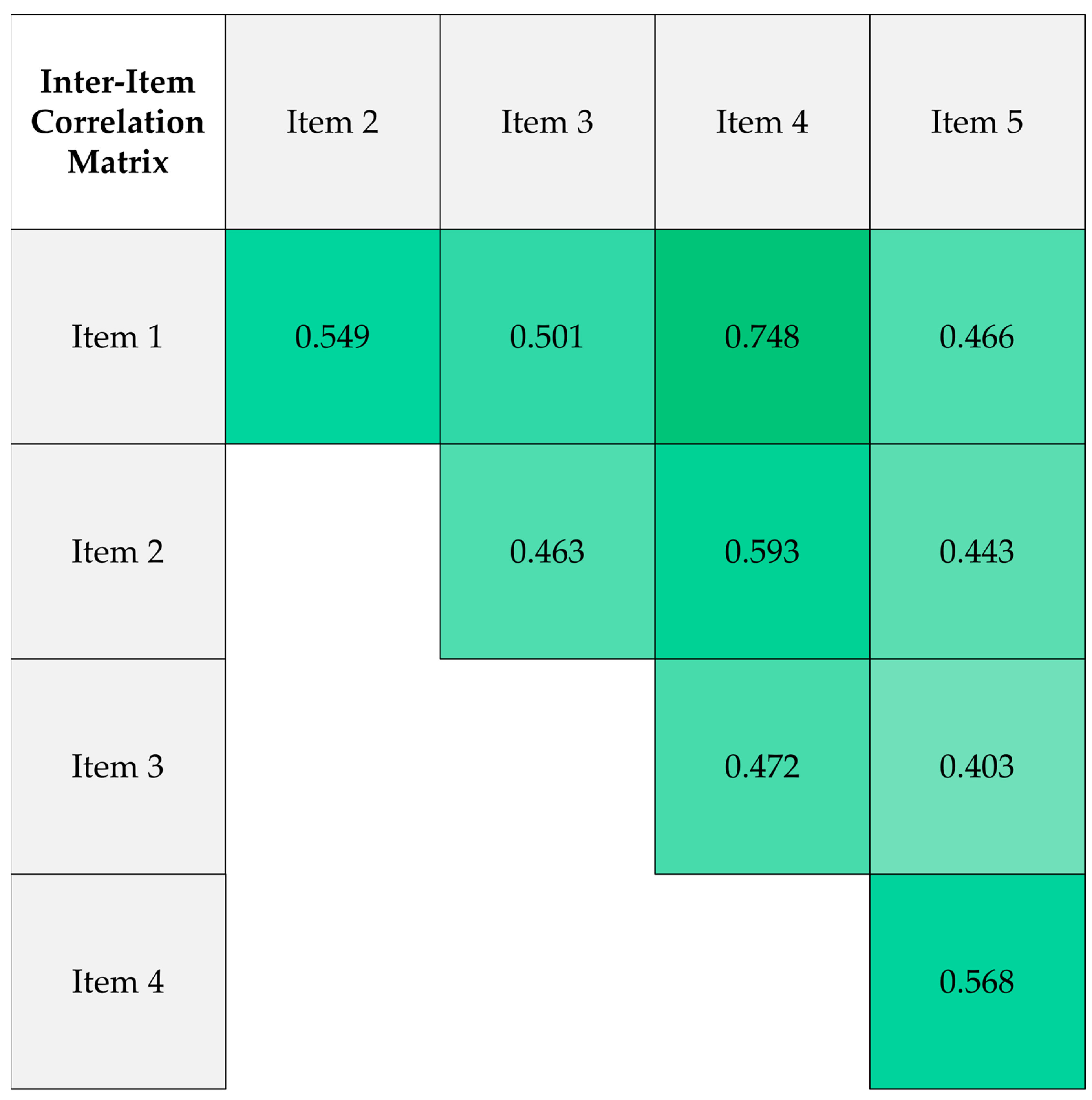
Figure 4.
The association between the embrace of COVID-19 conspiracy theories and the study variables (n = 493) shown as error bars representing the 95% confidence intervals (CIs) of the mean. K-W: Kruskal Wallis H test; M-W: Mann Whiteny U test.
Figure 4.
The association between the embrace of COVID-19 conspiracy theories and the study variables (n = 493) shown as error bars representing the 95% confidence intervals (CIs) of the mean. K-W: Kruskal Wallis H test; M-W: Mann Whiteny U test.
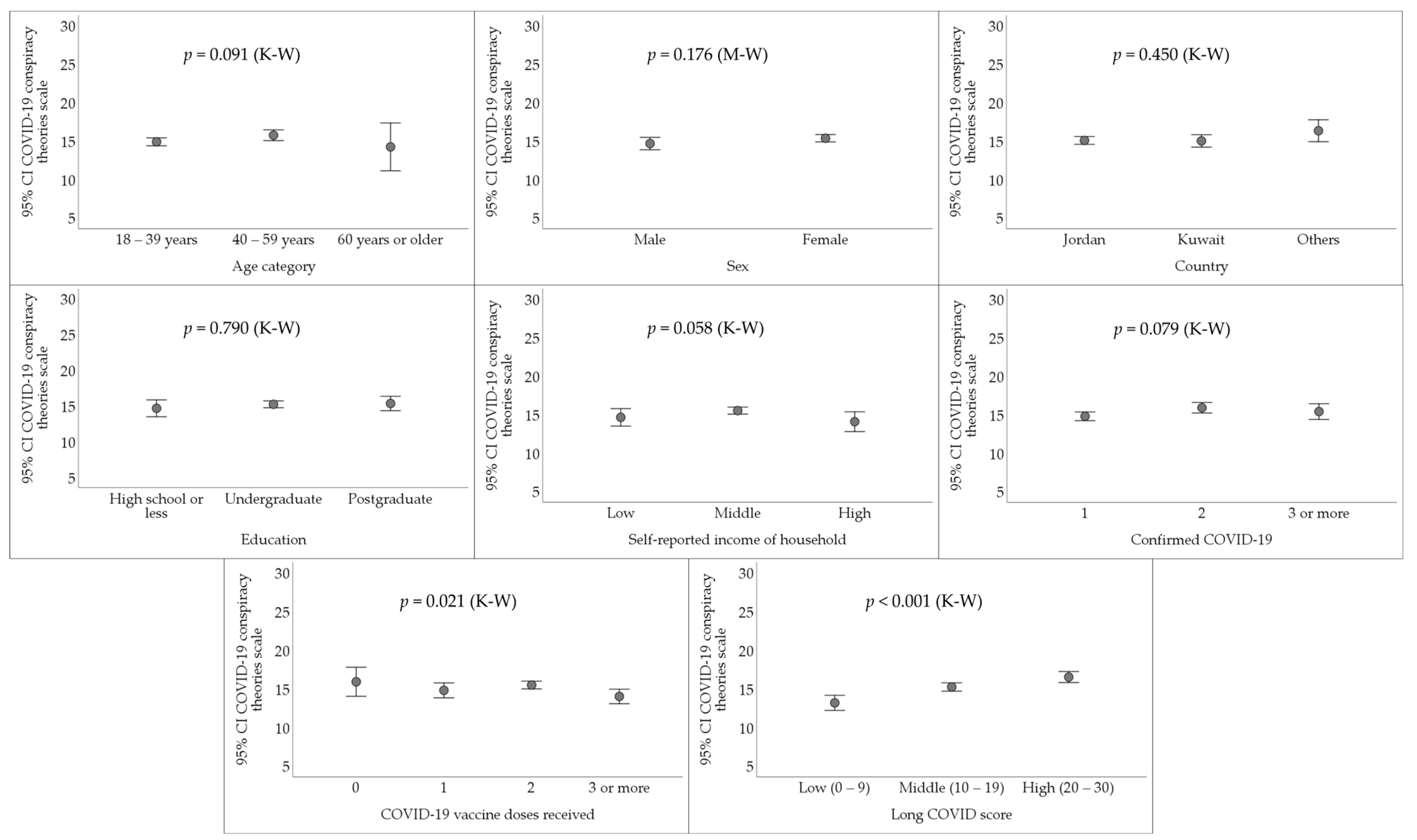

Table 1.
General characteristics of the study sample (N = 756).
| Variable | Category | Count (%) |
|---|---|---|
| Age category | 18 – 39 years | 460 (60.9) |
| 40 – 59 years | 263 (34.8) | |
| 60 years or older | 32 (4.2) | |
| Sex | Male | 222 (29.4) |
| Female | 533 (70.6) | |
| Country | Jordan | 438 (58.0) |
| Kuwait | 245 (32.5) | |
| Others 2 | 72 (9.5) | |
| Education | High school or less | 163 (21.6) |
| Undergraduate | 464 (61.5) | |
| Postgraduate | 128 (17.0) | |
| Self-reported income of household | Low | 139 (18.4) |
| Middle | 512 (67.8) | |
| High | 104 (13.8) | |
| Self-reported history of chronic disease | Yes | 193 (25.6) |
| No | 562 (74.4) | |
| Body Mass Index (BMI) | Underweight | 14 (1.9) |
| Healthy weight | 272 (36.0) | |
| Overweight | 255 (33.8) | |
| Obesity | 214 (28.3) | |
| Smoking | Non-smoker | 496 (65.7) |
| Ex-smoker | 58 (7.7) | |
| Current smoker | 201 (26.6) | |
| Confirmed COVID-19 1 | 0 | 262 (34.7) |
| 1 | 297 (39.3) | |
| 2 | 125 (16.6) | |
| 3 or more | 71 (9.4) | |
| Hospitalized due to COVID-19 | Yes | 39 (7.9) |
| No | 454 (92.1) | |
| COVID-19 vaccine doses received | 0 | 30 (6.1) |
| 1 | 28 (5.7) | |
| 2 | 329 (66.7) | |
| 3 or more | 106 (21.5) |
1 COVID-19: Coronavirus disease 2019; 2 Others: Comprised the following countries: Iraq (n = 15), Saudi Arabia (n = 11), Egypt (n = 11), Oman (n = 9), Qatar (n = 8), Bahrain (n = 7), other Arab countries (n = 6), United Arab Emirates (UAE) (n = 3), Syria (n = 1), and Palestine (n = 1).
Table 2.
The association between long COVID and different study variables in univariate analyses.
| Variable | Category | LongCOVID score | p value, χ2 | ||
| Low (0 – 9) | Middle (10 – 19) | High (20 – 30) | |||
| Count (%) | Count (%) | Count (%) | |||
| Age category | 18 – 39 years | 64 (20.8) | 143 (46.4) | 101 (32.8) | 0.026, 11.047 |
| 40 – 59 years | 38 (22.5) | 89 (52.7) | 42 (24.9) | ||
| 60 years or older | 8 (50.0) | 6 (37.5) | 2 (12.5) | ||
| Sex | Male | 49 (35.8) | 66 (48.2) | 22 (16.1) | <0.001, 26.894 |
| Female | 61 (17.1) | 172 (48.3) | 123 (34.6) | ||
| Country | Jordan | 62 (20.5) | 154 (50.8) | 87 (28.7) | 0.216, 5.786 |
| Kuwait | 38 (25.9) | 60 (40.8) | 49 (33.3) | ||
| Others 2 | 10 (23.3) | 24 (55.8) | 9 (20.9) | ||
| Education | High school or less | 21 (24.7) | 39 (45.9) | 25 (29.4) | 0.724, 2.064 |
| Undergraduate | 67 (21.4) | 158 (50.5) | 88 (28.1) | ||
| Postgraduate | 22 (23.2) | 41 (43.2) | 32 (33.7) | ||
| Self-reported income of household | Low | 12 (15.0) | 42 (52.5) | 26 (32.5) | <0.001, 23.387 |
| Middle | 67 (19.6) | 174 (50.9) | 101 (29.5) | ||
| High | 31 (43.7) | 22 (31.0) | 18 (25.4) | ||
| Self-reported history of chronic disease | Yes | 24 (18.6) | 58 (45.0) | 47 (36.4) | 0.111, 4.403 |
| No | 86 (23.6) | 180 (49.5) | 98 (26.9) | ||
| Body Mass Index (BMI) | Underweight | 3 (37.5) | 2 (25.0) | 3 (37.5) | 0.123, 10.033 |
| Healthy weight | 46 (25.7) | 92 (51.4) | 41 (22.9) | ||
| Overweight | 31 (19.6) | 80 (50.6) | 47 (29.7) | ||
| Obesity | 30 (20.3) | 64 (43.2) | 54 (36.5) | ||
| Smoking | Non-smoker | 72 (21.6) | 157 (47.0) | 105 (31.4) | 0.558, 3.000 |
| Ex-smoker | 7 (18.4) | 20 (52.6) | 11 (28.9) | ||
| Current smoker | 31 (25.6) | 61 (50.4) | 29 (24.0) | ||
| Confirmed COVID-19 | 1 | 91 (30.6) | 141 (47.5) | 65 (21.9) | <0.001, 38.147 |
| 2 | 13 (10.4) | 63 (50.4) | 49 (39.2) | ||
| 3 | 6 (8.5) | 34 (47.9) | 31 (43.7) | ||
| Hospitalized due to COVID-19 | Yes | 5 (12.8) | 17 (43.6) | 17 (43.6) | 0.091, 4.797 |
| No | 105 (23.1) | 221 (48.7) | 128 (28.2) | ||
| COVID-19 vaccine doses received | 0 | 9 (30.0) | 11 (36.7) | 10 (33.3) | 0.256, 7.758 |
| 1 | 4 (14.3) | 14 (50.0) | 10 (35.7) | ||
| 2 | 67 (20.4) | 160 (48.6) | 102 (31.0) | ||
| 3 | 30 (28.3) | 53 (50.0) | 23 (21.7) | ||
| COVID-19 conspiracy score 1 | Low (5 – 11) | 38 (38.8) | 40 (40.8) | 20 (20.4) | <0.001, 34.989 |
| Middle (12 – 18) | 55 (20.1) | 148 (54.2) | 70 (25.6) | ||
| High (19 – 25) | 17 (13.9) | 50 (41.0) | 55 (45.1) | ||
1 COVID-19 conspiracy score: Calculated based on five items assessed using a 5-point Likert scale; 2 Others: Comprised the following countries: Iraq (n = 15), Saudi Arabia (n = 11), Egypt (n = 11), Oman (n = 9), Qatar (n = 8), Bahrain (n = 7), other Arab countries (n = 6), United Arab Emirates (UAE) (n = 3), Syria (n = 1), and Palestine (n = 1).
Table 3.
Multivariate analyses for the factors associated with higher reporting of long COVID manifestations.
Table 3.
Multivariate analyses for the factors associated with higher reporting of long COVID manifestations.
| High long COVID score (20–30) vs. low long COVID score (0–9) | aOR1 (95% CI2) | p value |
|---|---|---|
| Factors | ||
| COVID-19 conspiracy theories | ||
| High COVID-19 conspiracies score (19–25) vs. low COVID-19 conspiracies score (5–11) | 6.85 (2.90–16.13) | <0.001 |
| High COVID-19 conspiracies score (19 – 25) vs. middle COVID-19 conspiracies score (12–18) | 3.21 (1.56–6.58) | 0.002 |
| Age | ||
| 18 – 39 years vs. 60 years or older | 3.62 (0.65–20.32) | 0.144 |
| 40 – 59 years vs. 60 years or older | 2.09 (0.36–12.16) | 0.413 |
| Sex | ||
| Female vs. male | 5.15 (2.66–10.00) | <0.001 |
| Self-reported income of household | ||
| Low vs. high | 4.70 (1.65–13.40) | 0.004 |
| Middle vs. high | 2.40 (1.10–5.22) | 0.027 |
| Frequency of COVID-19 confirmed diagnosis | ||
| Three times or more vs. once | 10.31 (3.73–28.57) | <0.001 |
| Three times or more vs. twice | 1.90 (0.60–6.06) | 0.276 |
| History of hospitalization due to COVID-19 | ||
| Yes vs. no | 5.53 (1.66–18.46) | 0.005 |
| Middle long COVID score (10–19) vs. low long COVID score (0–9) | ||
| Factors | ||
| COVID-19 conspiracy theories | ||
| High COVID-19 conspiracies score (19–25) vs. low COVID-19 conspiracies score (5–11) | 2.82 (1.32–6.06) | 0.008 |
| High COVID-19 conspiracies score (19–25) vs. middle COVID-19 conspiracies score (12–18) | 1.23 (0.63–2.42) | 0.538 |
| Age | ||
| 18 – 39 years vs. 60 years or older | 1.80 (0.54–6.04) | 0.340 |
| 40 – 59 years vs. 60 years or older | 1.66 (0.48–5.76) | 0.423 |
| Sex | ||
| Female vs. male | 2.11 (1.26–3.55) | 0.005 |
| Self-reported income of household | ||
| Low vs. high | 5.10 (2.03–12.84) | 0.001 |
| Middle vs. high | 3.12 (1.60–6.06) | 0.001 |
| Frequency of COVID-19 confirmed diagnosis | ||
| Three times or more vs. once | 4.76 (1.81–12.50) | 0.002 |
| Three times or more vs. twice | 1.52 (0.50–4.63) | 0.466 |
| History of hospitalization due to COVID-19 | ||
| Yes vs. no | 2.69 (0.86–8.43) | 0.089 |
1 aOR: Adjusted odds ratio; 2 CI: Confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



