Submitted:
07 August 2024
Posted:
11 August 2024
You are already at the latest version
Abstract
Background: Menopause signifies the end of a woman's reproductive phase, characterized by the cessation of ovarian hormone production and the termination of menstrual cycles, typically occurring between the ages of 45 and 55. The transition involves a range of physical and psychological symptoms manifesting before, during, and after menopause. Method: This cross-sectional analytical study assessed the level of awareness regarding menopausal symptoms among women in Bharatpur-9, Chitwan. A non-probability sampling technique was used to select 257 respondents. Data were collected using a semi-structured interview schedule and analyzed with SPSS version 20.0. Results: Among the respondents, 53.3% were aged 40-49 years (Mean ± S.D.; 48.84 ± 6.27), and 69.3% experienced menarche between ages 13- 15. A majority (59.9%) had not yet reached menopause. Knowledge of menopausal symptoms was as follows: joint pain (90.7%), sleep problems (90.7%), irritability (90.7%), hot flushes (22.2%), anxiety (22.2%), sadness (22.2%), vaginal dryness (22.6%), loss of interest in sex (25.7%), palpitations (18.7%), and decreased visual acuity (9.3%). Statistical significance was found between awareness levels and factors such as religion (p=0.00), ethnicity (p=0.00), educational status (p=0.006), family type (p=0.043), cessation of menstruation (p=0.013), and cause of menopause (p=0.00). Overall, 53.7% of respondents had average knowledge about menopausal symptoms. Conclusion: The study concluded that over half of the respondents possessed average awareness of menopausal symptoms. Hence, there is a need for women to receive correct and comprehensive information regarding menopausal symptoms and their management.
Keywords:
menopausal symptoms
; menopause awareness
; women's health
; menopausal transition
; symptom management
1. Introduction
1.1. Background of the Study
Menopause is a biological process marking the end of a woman's reproductive capacity, characterized by the permanent cessation of ovarian follicular activity and the subsequent decline in circulating estrogen and progesterone levels. This transition typically occurs between the ages of 45 and 55 and is associated with various physiological and psychological changes, including vasomotor symptoms, genitourinary syndrome, and increased risk for osteoporosis and cardiovascular disease (Dutta, 2016).
Menopause, while not classified as an illness, is associated with several health conditions that can increase mortality in menopausal women. The physiological changes during menopause include vaginal atrophy, bone demineralization, behavioral alterations, urinary issues, increased adiposity, and diminished sexual desire (Kalhan, et al., 2020). Knowledge of menopausal symptoms and their complications enables women to manage these changes more effectively and prevent serious, irreversible consequences through appropriate treatments (Shrestha, 2016). The prevalence of menopausal symptoms varies by region, with reported incidences of 74% in Europe, 36-50% in North America, 45-69% in Latin America, and 22-63% in Asia. In the United States, 85% of postmenopausal women experience symptoms at some point in their lives (Menopause Epidemiology and Demographics, 2021). The average age of menopause in Western countries is 51 years, compared to 46 years in India and 48.7 years in Nepal (Bhandari, Amatya & Giri, 2020). A cross-sectional study in Kathmandu found that menopausal symptoms affected daily activities in 59.3% of postmenopausal women, with severe impacts reported by 1.9%, reduced work efficiency by 58.8%, and hindered social activities in 43.2% (Prajapati, 2020).
Menopausal issues are a significant health concern in Nepal, where many women are unaware of the condition and its associated symptoms. The onset of menopause can be particularly traumatic for women unfamiliar with these changes, highlighting the importance of awareness and education about menopause and its symptoms to empower women to make informed health decisions (Gyawali, Subedi, Yasmin & Pandey, 2016), (Lee & Suh, 2010).
1.2. Literature Review
Nishant et al. (2008) examined the severity of menopausal symptoms and quality of life in Pakistani women, finding that 78.79% had inadequate knowledge and 15.8% were aware of menopausal symptoms. Commonly reported symptoms included backache (75.66%), insomnia (63.44%), vasomotor symptoms (59.4%), night sweats (45.19%), and memory loss (62.10%). Similarly, Mujahid, Siddiqui, and Hussain (2013) investigated the awareness of menopausal symptoms among 205 young Pakistani women of different educational backgrounds at Dr. Ziauddin Hospital, Karachi. The mean age of respondents was 34.34 ± 3.8 years. The study found that 65.9% had completed intermediate or higher education, and 57.6% had sought information about menopause, with doctors being the source for 53.4%. Only 43.4% knew what menopause was, and 58% were aware of the average age of menopause in Pakistan.
Anjum et al. (2013) conducted a study on the awareness and perception of menopause among 93 Pakistani women over 42 years old at Civil Hospital, Karachi. The study found that 59.14% had knowledge of menopause, 33.33% were aware of its symptoms, and 10.75% knew about its treatment. Additionally, 44.09% were satisfied with its cessation, while 40.86% wanted it to continue. Furthermore, 69.89% desired education on menopause, and 47.31% felt the need for medical treatment. In the same year, Vijayalakshmi, Ramesh, and Eileen (2013) found prevalent symptoms among Northern Indian women included tiredness (92.90%), headache (88.80%), joint discomfort (76.20%), and sleeplessness (54.40%). Paudyal and Nepal (2014) conducted a study at Lumbini Medical College (LMC) involving 142 women aged 40-60 years, revealing that half of the respondents were between 40-44 years old, 99.3% were married, and 57.7% were literate. The study found that 74.6% of respondents were menstruating women, with friends and relatives being the main source of information on perimenopausal symptoms for 81.2% of the participants. Knowledge levels on perimenopausal symptoms were poor for 63.4%, fair for 33.8%, and good for only 2.8% of respondents.
Swaraj et al. (2017) studied menopausal health status among Nepalese women, revealing that 59.2% were unaware of menopausal health problems. The most commonly known symptoms were abnormal bleeding (17.65%), sweating (15.75%), hot flushes (14.95%), and joint pain (14.25%). The most experienced symptoms were joint pain (36.8%), hot flushes (29.2%), and irregular bleeding (29.1%), with 29.3% consulting health workers and 46.3% accepting menopause as a part of life. Moreover, Leena, Joseph, and Ackee (2017) found among 100 postmenopausal women in India that only 19.5% of symptomatic women sought treatment, and 77.9% had positive perceptions of menopause. Prajapati (2020) examined the awareness of menopausal symptoms and their effect on daily life among 160 postmenopausal women attending the female outpatient department of Patan Hospital, Nepal. The study showed that 81.2% of the women had inadequate awareness of menopausal symptoms, which affected daily activities in 59.3% of the cases, work efficiency in 58.8%, and social activities in 43.2%. Educational, marital, and occupational status were significantly associated with awareness levels, and the symptoms had a notable impact on daily life. Similarly, Sharma et al. (2021) surveyed 203 postmenopausal women aged 45-60 years in selected wards of Tokha Municipality, Kathmandu. The study revealed that over half (50.2%) were unaware of menopausal symptoms, and 59.6% reported that menopause-related symptoms affected their daily work activities.
The literature review highlights the varying levels of awareness regarding menopausal symptoms among women in different regions and settings. Multiple studies indicate that knowledge of menopausal symptoms is generally poor, with significant impacts on daily life, work efficiency, and social activities. There is a clear need for enhanced health education and awareness programs to improve the understanding of menopausal symptoms and appropriate health practices among women.
1.3. Rationale and Significance of the Study
The hormonal changes associated with menopause can significantly impact physical, emotional, mental, and social well-being. The severity and nature of symptoms experienced during menopause vary among individuals and can affect daily activities and quality of life (World Health Organization [WHO], 2021). Studies highlight the limited knowledge regarding menopausal symptoms among women. For instance, Paudyal and Nepal (2014) found that among 142 women aged 40-60 at Lumbini Medical College Teaching Hospital, 63.4% had poor knowledge, 33.8% had fair knowledge, and only 2.8% had a good level of knowledge about perimenopausal symptoms. Similarly, Prajapati (2020) revealed that 81.2% of 160 postmenopausal women in Kathmandu had inadequate awareness of menopausal symptoms. In Pakistan, Nishant et al. (2008) reported that 78.79% of women had inadequate knowledge of menopausal symptoms. Commonly reported symptoms included backache (75.66%), insomnia (63.44%), vasomotor symptoms (59.4%), night sweats (45.19%), and memory loss (62.10%).
These studies indicate that awareness of menopausal symptoms is generally low. Premenopausal women require access to quality health services and supportive communities and systems. However, menopause is often not discussed within families, communities, workplaces, or healthcare settings. Consequently, women may not recognize their symptoms as related to menopause or be aware of available counseling and treatment options. Therefore, assessing the level of awareness regarding menopausal symptoms among women in the community is crucial. The findings of this study will provide baseline data for further research on similar topics and help health academicians disseminate knowledge about menopausal symptoms, ultimately improving the quality of life for postmenopausal women. This study aims to assess the awareness of menopausal symptoms among the women of Bharatpur-9, Chitwan. Specifically, it seeks to determine the overall level of awareness and examine the association between this awareness and selected demographic variables. The research question guiding this investigation is: What is the level of awareness regarding menopausal symptoms among the women of Bharatpur-9, Chitwan?
The study employs a conceptual framework where the dependent variable is the awareness regarding menopausal symptoms. The independent variables include socio-demographic factors such as age, religion, ethnicity, education status, education level, occupation, economic status, and the status of menopause. By exploring these variables, the study aims to identify potential correlations and provide insights into the factors influencing awareness levels among this population.
2. Methodology
2.1. Research Design
This study employs a cross-sectional analytical design to evaluate the awareness of menopausal symptoms among women residing in Bharatpur-9, Chitwan. This design allows for the assessment of awareness levels at a specific point in time and facilitates the analysis of associated demographic factors. The research was conducted in Bharatpur-9, Chitwan, purposively selected for its diverse population and defined geographic boundaries. Bharatpur-9 is part of the Bharatpur metropolitan city in Bagmati Province, encompassing an area of 5.3 square kilometers with a population of 9,116 (4,240 males and 4,776 females). The area is characterized by a variety of ethnic groups living in a stable environment.
The target population comprised women aged 40-60 years residing in Bharatpur-9, Chitwan. This demographic was chosen due to its relevance to the study of menopausal symptoms.
2.2. Research Study Population and Selection Criteria
The study focused on women aged 40-60 years residing in Bharatpur-9, Chitwan, as this demographic is particularly relevant to the study of menopausal symptoms. This age range encompasses the typical onset and progression of menopause, making it an ideal group for assessing awareness and experiences related to menopausal changes.
The selection criteria for participants included specific inclusion and exclusion parameters to ensure the study's relevance and accuracy. Eligible participants were women aged 40-60 years living in Bharatpur-9. In contrast, those excluded from the study were women younger than 40 or older than 60 years, as well as those who were mentally ill, chronically ill, or disabled (e.g., visually impared). Additionally, women who did not provide informed consent were also excluded from the study. This selection process was designed to focus on a representative sample while ensuring that the participants could contribute valid and reliable data regarding menopausal symptoms.
2.3. Sampling Technique and Size
A non-probability purposive sampling method was employed. Houses within the selected ward were purposively chosen, starting from the first house to the left of the ward office. In cases where multiple eligible women resided in a single house, one woman was selected at random. Data collection continued until the required sample size was achieved.
The sample size was calculated using the formula:
Sample size (n) = Z²pq/E² [Where: Z = 1.96, Error (E) = 5% = 0.05, Prevalence (p) = 18.8% (Prajapati, 2020) = 0.188, q = 1 − p = 1 − 0.188 = 0.812]
Now, substituting the values:
n = (1.96)² ∗ 0.188 ∗ 0.812 / (0.05)² = 3.8416 ∗ 0.188 ∗ 0.812 / 0.0025 = 0.5868 / 0.0025 = 234.5 ≈ 234
Considering a 10% non-response rate:
10% of 234 = 10/100 ∗ 234 = 23.4 ≈ 23, Total Sample Size (n) = 234 + 23 = 257 Hence, the total sample size is 257.
2.4. Data Collection/ Analysis Procedure and Ethical Considerations
Data collection was conducted using a semi-structured interview schedule, which was meticulously developed in both English and Nepali to accommodate the linguistic needs of the participants and ensure comprehensibility. The instrument was organized into three distinct sections: Part I focused on gathering socio-demographic data, Part II addressed gynecological information, and Part III assessed awareness regarding menopausal symptoms. This structured approach allowed for a comprehensive collection of relevant information, facilitating a thorough analysis of the participants' awareness and experiences related to menopause.
Content validity was established through literature review and consultations with experts. The instrument was initially developed in English, translated to Nepali, and then back-translated to ensure accuracy. Reliability was tested by pretesting the instrument on 10% of the sample in a similar setting, Bharatpur-10. Formal authorization for the study was obtained from the relevant institutional authority following a request submitted by the college. Data collection was personally conducted by the researcher to ensure consistency and accuracy. The process involved administering a semi-structured interview schedule in Nepali, tailored for women over the age of 40, in alignment with the study's objectives. Each interview, lasting approximately 15-20 minutes, was conducted after obtaining informed consent from the participants. Data collection took place from 18th to 24th of 2079. To minimize potential biases, the researcher employed rigorous methods to maintain objectivity throughout the data collection phase.
Approval for the study was obtained from Shree Medical and Technical College and ethical clearance from the Shree Medical and Technical College Institutional Review Committee (SMTC-IRC). Administrative permission was secured from Bharatpur Municipality. Participants were informed about the study's nature and purpose, and written informed consent was obtained. Confidentiality was assured, and participants were free to withdraw at any time.
The collected data underwent a thorough process of coding, checking, reviewing, and organizing to ensure accuracy and completeness. The data were then entered into MS Excel before being imported into the Statistical Package for the Social Sciences (SPSS) version 20.0 for analysis. Descriptive statistical methods were utilized to present data in terms of frequency and percentages. Additionally, inferential statistical techniques, specifically the chi-square test, were employed to examine associations between awareness of menopausal symptoms and selected demographic variables.
3. Results and Data Analysis
The analysis was conducted using a descriptive cross-sectional analytical research design, aligned with the study's research questions and objectives. The findings are systematically presented across various tables to facilitate a clear understanding of the data. Specifically, Table 1 illustrates the socio-demographic characteristics of the respondents, while Table 2 presents their gynecological information. Table 3 and Table 4 focus on the respondents' awareness of menopausal symptoms, with Table 5 detailing their overall level of awareness. Finally, Table 6 explore the associations between the respondents' level of awareness and selected socio-demographic variables. This structured approach ensures a comprehensive examination of the data and highlights key patterns and relationships pertinent to the study.
Table 1 provides an overview of the socio-demographic characteristics of the respondents. It reveals that 53.3% of the participants were aged between 40 and 49 years. The majority, 87.5%, adhered to Hinduism, and 84% identified as Brahmin/Chhetri. As seen from the Figure 1, almost all respondents (96.9%) were literate, and 100% were housewives. A significant majority (93.8%) were married, and 67.7% lived in nuclear families.
Figure 1.
Analytical charts of respondents’ sociodemographic characteristics.
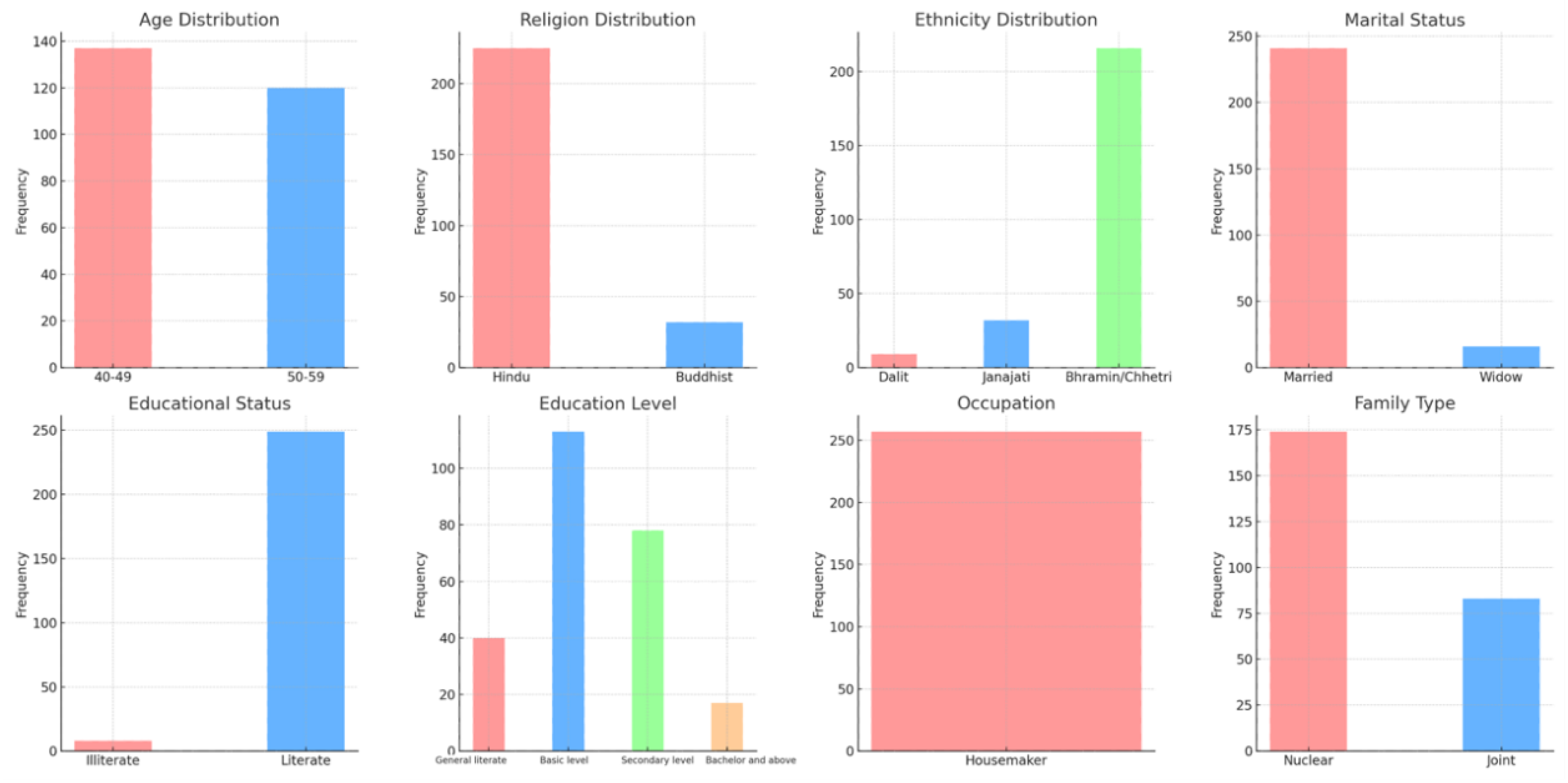

Table 2.
Respondents’ gynecological information (age at menarche, menstruation stop or not, cause of menopause, irregular menstruation), n = 257.
Table 2.
Respondents’ gynecological information (age at menarche, menstruation stop or not, cause of menopause, irregular menstruation), n = 257.
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Age at menarche (in complete years) | ||
| 13-15 | 178 | 69.3 |
| 16-18 | 79 | 30.7 |
| Mean ± SD (15.5 ± 0.683) | min.= 13 | max. = 18 |
| Menstruation stop or not | ||
| Yes | 103 | 40.1 |
| No | 154 | 59.9 |
| Cause of menopause (n = 103) | ||
| Natural | 87 | 84.4 |
| Surgical | 16 | 15.6 |
| Irregular menstruation (n = 154) | ||
| Yes | 0 | 0 |
| No | 154 | 100 |
The gynecological information of the respondents is presented in Table 2. It shows that more than half (69.3%) experienced menarche between the ages of 13 and 15 years. In terms of menstrual cessation, 59.9% had not yet stopped menstruating, while 84.4% experienced natural menopause as represented in Figure 2.
Figure 2.
Analytical charts of respondents’ gynecological information.
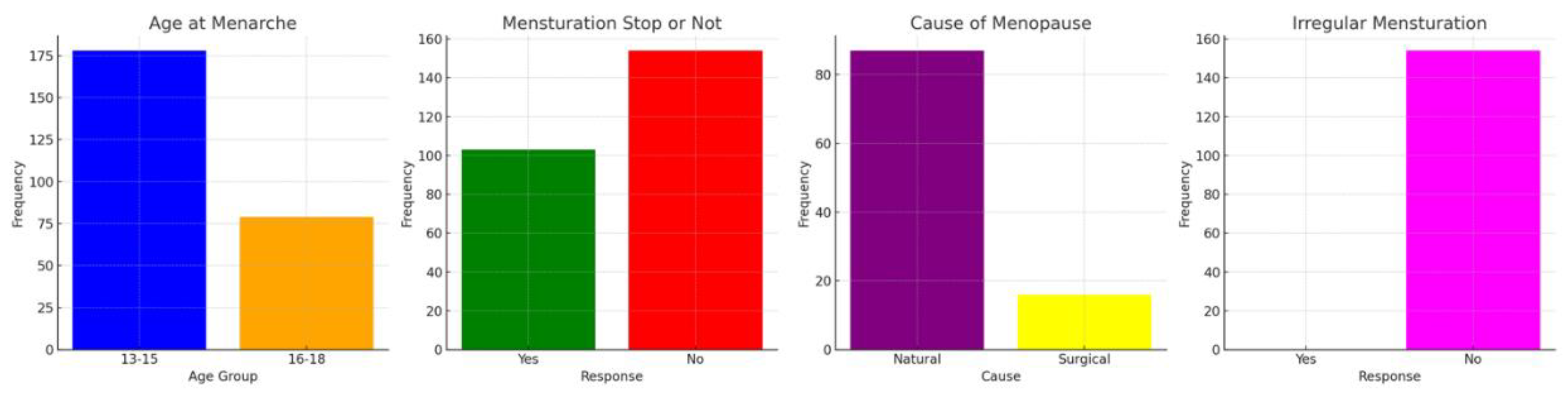
Table 3.
Respondents’ awareness regarding menopausal symptoms (meaning, age of menopause, cause, beginning sign, symptoms), n = 257.
Table 3.
Respondents’ awareness regarding menopausal symptoms (meaning, age of menopause, cause, beginning sign, symptoms), n = 257.
| Variable | Correct Answer | Frequency | Percentage (%) |
|---|---|---|---|
| Meaning of menopause | Cessation of menopause for 12 months | 257 | 100 |
| Age of menopause | 45-55 | 88 | 34.2 |
| Cause of menopause | Normal body process | 257 | 100 |
| Beginning sign of menopause | Irregular menstruation | 257 | 100 |
| Symptoms | |||
| Hot flushes/ night sweats | yes | 57 | 22.2 |
| Vaginal dryness | yes | 58 | 22.6 |
| Joint pain | yes | 233 | 90.7 |
| Loss of interest in sex | yes | 66 | 25.7 |
| Palpitation | yes | 48 | 18.7 |
| Decrease vision acuity | yes | 24 | 9.3 |
| Sleep problem | yes | 233 | 90.7 |
| Anxiety | yes | 57 | 22.2 |
| Sadness | yes | 57 | 22.2 |
| Irritability | yes | 233 | 90.7 |
Table 3 illustrates the respondents' awareness of menopausal symptoms. All participants (100%) were aware of the meaning of menopause, but only 34.2% knew the typical age of onset. Awareness was high regarding the causes of menopause (100%) and common symptoms like joint pain (90.7%), sleep problems (90.7%), and irritability (90.7%). However, the Figure 3 shows that only 22.2% were aware of hot flushes, anxiety, and sadness, while awareness of vaginal dryness was at 22.6%, loss of interest in sex at 25.7%, palpitations at 18.7%, and decreased vision acuity at 9.3%.
Figure 3.
Analytical charts of respondents’ awareness regarding menopausal symptoms.
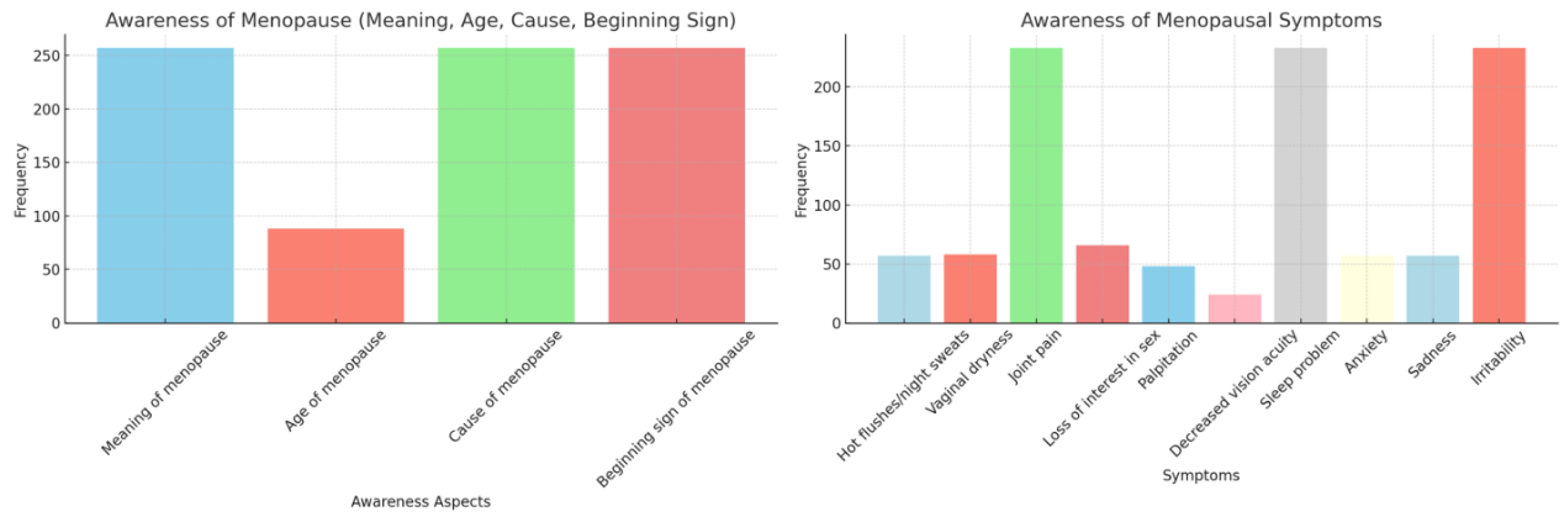
Table 4.
Respondents’ awareness regarding menopausal symptoms (complications, management), n = 257.
| Variable | Correct Answer | Frequency | Percentage (%) |
|---|---|---|---|
| Complications of menopausal symptoms * | |||
| Urinary incontinence | yes | 59 | 23 |
| Obesity | yes | 41 | 16 |
| Osteoporosis | yes | 233 | 90.7 |
| Sleep disorders | yes | 241 | 93.8 |
| Decrease sexual desire | yes | 95 | 37 |
| Management of hot flushes * | |||
| Avoid eating hot and spicy meals | yes | 188 | 73.2 |
| Avid hot and crowded places | yes | 186 | 72.4 |
| Giving up smoking | yes | 257 | 100 |
| Deep breathing | yes | 52 | 20.2 |
| Drink coffee less | yes | 90 | 35 |
| Adequate sleep and activities effective to decreased irritability | yes | 132 | 51.4 |
| Effectiveness of calcium supplement in menopausal women | yes | 182 | 70.8 |
* Multiple Response.
The respondents' awareness of complications and management strategies for menopausal symptoms are represented in Table 4. Knowledge about sleep disorders was high (93.8%). Awareness of management techniques for hot flushes was notably high for smoking cessation (100%) and avoidance of hot and spicy meals (73.2%), though less so for deep breathing (20.2%). Awareness of adequate sleep and activities to reduce irritability was at 51.4%, and knowledge about the effectiveness of calcium supplements in managing menopausal symptoms was 70.8% as depicted in Figure 4.
Figure 4.
Analytical charts of respondents’ awareness regarding menopausal symptoms.
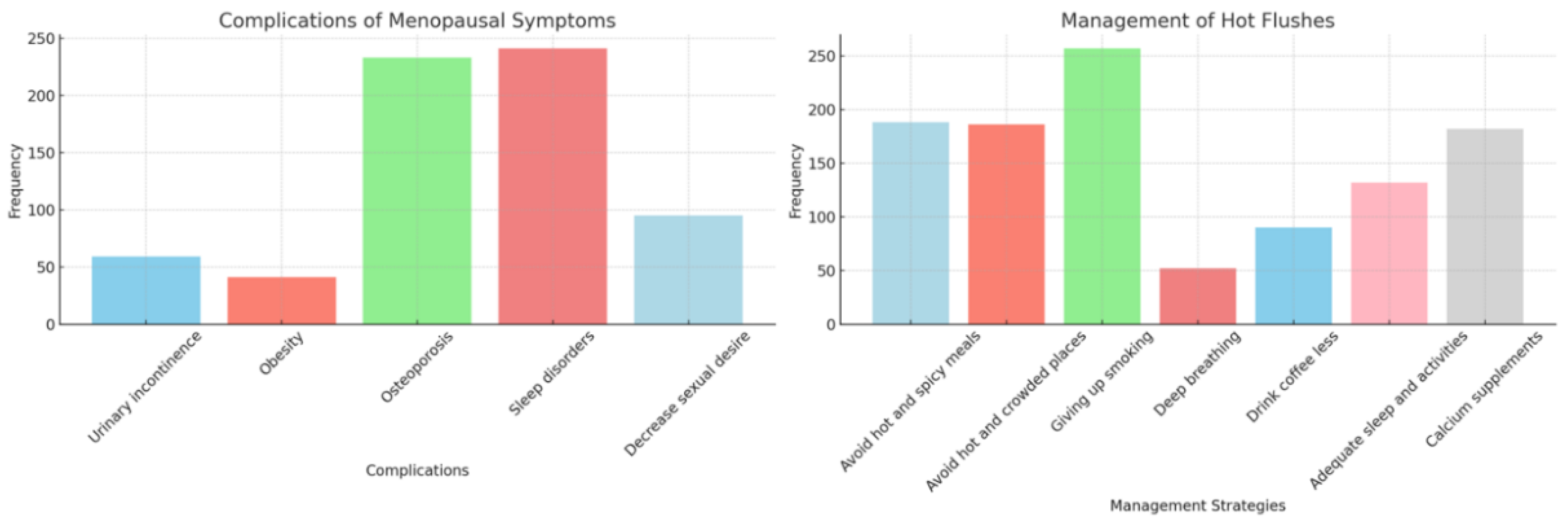
Table 5.
Respondents’ level of awareness on menopausal symptoms, n = 257.
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Poor (0-49%) | 103 | 40 |
| Average (50-75%) | 138 | 53.7 |
| Good (76-100%) | 16 | 6.2 |
| Total | 257 | 100 |
Mean ± SD (1.66 ± 0.591) min. = 1 max. = 3.
Table 5 summarizes the overall level of awareness regarding menopausal symptoms. A majority (53.7%) demonstrated average knowledge, 40% had poor knowledge, and only 6.2% had good knowledge.
Table 6.
Association between Respondents’ level of awareness and socio demographic variables, n = 257.
Table 6.
Association between Respondents’ level of awareness and socio demographic variables, n = 257.
| Variable | Level of Awareness | Chi-square | p-value | ||
|---|---|---|---|---|---|
| Poor | Average | Good | |||
| Age | 0.635 | 0.728 | |||
| 40-49 | 58 (42.31%) | 71 (51.8%) | 8 (5.8%) | ||
| 50-59 | 45 (37.5%) | 67 (55.8%) | 8 (6.7%) | ||
| Religion | 20.246 | <0.001 * | |||
| Hindu | 79 (35.1%) | 130 (57.8%) | 16 (7.1%) | ||
| Buddhist | 24(75%) | 8 (25%) | 0 | ||
| Ethnicity | 21.776 | <0.001* | |||
| Dalit | 4 (44.4%) | 5 (55.6%) | 0 | ||
| Janajati | 24 (75%) | 8 (25%) | 0 | ||
| Bramhin/Chhetri | 25 (34.7%) | 125 (57.9%) | 16 (7.4%) | ||
| Marital status | 2.492 | 0.288 * | |||
| Married | 95 (39.4%) | 130 (53.9%) | 16 (6.6%) | ||
| Widow | 8 (50%) | 8 (50%) | 0 | ||
| Educational status | 10.171 | 0.006* | |||
| Illiterate | 0 | 8 (100%) | 0 | ||
| Literate | 103 (41.4%) | 130 (52.2%) | 16 (6.4%) | ||
| Family type | 6.304 | 0.043* | |||
| Nuclear | 78 (44.8%) | 88 (50.6%) | 8 (4.6%) | ||
| Joint | 25 (30.1%) | 50 (60.2%) | 8 (9.6%) | ||
| Menstruation stop or not | 8.635 | 0.013 * | |||
| Yes | 30 (29.1%) | 65 (63.1%) | 8 (7.8%) | ||
| No | 73 (47.4%) | 73 (47.4%) | 8 (5.2%) | ||
| Cause of menopause(n = 103) | 16.414 | <0.001 * | |||
| Natural | 30 (34.5%) | 49 (56.3%) | 8 (9.2%) | ||
| Surgical | 0 | 16 (100%) | 0 | ||
Significance level at 0.05 ∗ likelihood ratio.
The association between the level of awareness and socio-demographic variables is examined in Table 6. Statistically significant associations were found between the level of awareness and variables such as religion (p-value = 0.00), ethnicity (p-value = 0.00), educational status (p-value = 0.006), family type (p-value = 0.043), cessation of menstruation (p-value = 0.013), and the cause of menopause (p-value = 0.00). According to Figure 5, these findings suggest that socio-demographic factors significantly influence awareness levels regarding menopausal symptoms.
4. Discussion and Recommendation
This section provides a comprehensive analysis of the study's findings, concluding with implications and recommendations. The discussion contextualizes the results in comparison to existing literature, while the conclusions are drawn from these findings.
The cross-sectional analytical study aimed to evaluate the level of awareness regarding menopausal symptoms among women in Bharatpur-9, Chitwan, involving 257 respondents. The primary objectives were to determine the level of awareness and its correlation with various socio-demographic variables. Data collection employed a non-probability sampling technique and was facilitated through a semi-structured interview schedule. The data was analyzed using SPSS software version 20.0.
4.1. Findings Related to Socio-Demographic Characteristics
The study revealed that 53.3% of respondents were aged between 40 and 49 years, with a mean age of 48.84 ± 6.27 years. This finding aligns with Bhandari et al. (2017), who reported a median menopause age of 48.3 years, and Nitin et al. (2014), whose study identified a mean menopausal age of 48.35 years.
Regarding religious affiliation, 87.5% of respondents identified as Hindu, and 12.5% were Buddhist. Ethnic composition showed that 84% of the respondents were Brahmin/Chhetri, while 16% belonged to other groups, such as Dalit or Janajati. In terms of education, 44% had only basic literacy, and 6.6% had attained a bachelor's degree or higher. All respondents (100%) were housewives. Marital status revealed that 93.3% were married, and 6.2% were widowed. Most respondents (67.7%) lived in nuclear families, while 32.3% were part of joint families.
These findings highlight the demographic profile of the study population and suggest that while some results align with existing literature, particularly concerning the age of menopause, other socio-demographic aspects such as religion, ethnicity, and family structure may not have been widely explored in previous research. This indicates a need for further studies to address these gaps and explore the implications of these demographic factors on menopausal awareness and health outcomes.
4.2. Findings Related to Gynecological Information
The study examined gynecological aspects relevant to menopause, revealing that 69.3% of respondents experienced menarche between ages 13 and 15, while 30.7% entered menarche between ages 16 and 18. The majority of respondents (59.9%) had not yet experienced cessation of menstruation, indicating that a significant proportion were premenopausal. Additionally, 84.4% of respondents reported undergoing natural menopause. The lack of comparable studies limits the ability to directly contrast these findings; however, these results provide foundational insights into the gynecological profiles of women in this study.
4.3. Findings Related to Respondents' Awareness of Menopausal Symptoms
Awareness of menopausal symptoms varied among respondents. Notably, only 22.2% of respondents were aware of hot flushes and sweating as symptoms of menopause. This finding is in contrast to Madhu Kumar et al. (2012), which reported a higher awareness level of 56.8%. However, it is somewhat consistent with Shanta, Shankar, Nawazia, and Susmita (2016), who found that 32.1% of their respondents were aware of these symptoms.
Conversely, the study demonstrated that 90.7% of respondents recognized sleep disturbances as a menopausal symptom. This result significantly contrasts with the 29.9% reported by Sameer, Mahesh, Neha, and Mather (2016), highlighting a discrepancy in awareness levels across different studies.
Awareness of palpitation as a symptom was reported by 48% of respondents, aligning with Shanta et al. (2016), who observed a 35.7% awareness level. Sadness was identified as a menopausal symptom by 22.2% of respondents, corroborating findings from Shanta et al. (2016) and Beth et al. (2014), which reported awareness levels of 30.7% and 30%, respectively.
The study found that 90.7% of respondents were aware of irritability as a symptom, a finding that supports Arifa (2015), who reported a similar awareness level of 96.1%. Conversely, only 22.2% of respondents recognized anxiety as a symptom, which is markedly lower than Shanta et al. (2016), who found a 67.9% awareness level. Sexual problems were identified by 25.7% of respondents, aligning with Nisher et al. (2011) and Shanta et al. (2016), who reported 34.2% and 31.4% awareness levels, respectively. Bladder problems were recognized by 23% of respondents, consistent with Rahman et al. (2011) and Syed, Siti, and Verna (2010), who reported awareness levels of 12.8% and 13.8%.
Finally, 22.6% of respondents were aware of vaginal dryness as a menopausal symptom, closely aligning with Shanta et al. (2016), who reported 25.5%. Additionally, 90.7% recognized joint and muscular discomfort, which is supported by Afria (2015), who found a 93.8% awareness level. These findings highlight significant variations in awareness of menopausal symptoms and underscore the need for targeted educational interventions to address gaps in knowledge and improve overall awareness among women.
4.4. Findings Related to Respondents' Level of Awareness
The analysis of the respondents' level of awareness regarding menopausal symptoms indicates varied results compared to existing literature. The study found that only 6.2% of respondents demonstrated a good level of awareness. This finding is notably lower than Shams (2018), which reported an 18.8% prevalence of good awareness. This discrepancy suggests that the respondents in this study had less comprehensive knowledge about menopausal symptoms compared to the sample studied by Shams. In terms of fair awareness, 53.7% of respondents in this study fell into this category. This proportion is significantly higher than the 11% reported by Shams (2018), indicating a greater degree of moderate understanding among the current study's participants. This difference may reflect variations in educational interventions or access to information between the populations studied.
Conversely, 40% of respondents were classified as having a poor level of awareness regarding menopausal symptoms. This finding is markedly lower than the 70.2% reported by Shams (2018). The lower proportion of poor awareness in this study could suggest improvements in general knowledge or differing demographic characteristics that influence awareness levels.
Overall, the disparities in awareness levels between this study and Shams (2018) highlight the need for further investigation into the factors contributing to these differences, such as variations in educational outreach or socio-cultural influences.
5. Conclusion
The study revealed that most respondents showed average knowledge of menopausal symptoms. The findings indicated that awareness of menopausal symptoms was significantly associated with various sociodemographic factors, including ethnicity, religion, educational status, occupation, family type, cessation of menstruation, and the perceived causes of menopause. These associations underscore the necessity for targeted educational interventions to enhance awareness and understanding of menopausal symptoms. Providing accurate information through diverse channels, including mass media, is crucial to improving awareness and managing symptoms effectively.
The primary limitation of this study is its focus on a single community within Bharatpur-9, Chitwan, which may not be representative of broader populations. Additionally, the relatively small sample size restricts the generalizability of the findings. These limitations suggest that caution should be exercised when extrapolating the results to other settings or populations.
The findings from this study offer valuable baseline data for future research on menopausal symptoms. They provide insights that could assist educators, healthcare professionals, and policymakers in designing and implementing effective awareness programs tailored to this age group. The data can guide the development of targeted educational strategies and interventions aimed at improving knowledge and management of menopausal symptoms. To enhance the generalizability of the findings, future research should expand to include a larger and more diverse sample across multiple communities. Conducting similar studies on a broader scale would provide a more comprehensive understanding of menopausal awareness and could inform more effective public health strategies.
References
- Anjum, F.; Ghayas, S.; Jahan, N.; Yasin, H. Awareness and perception of menopause in Pakistani women. World Journal of Pharmacy and Pharmaceutical Sciences 2013, 2, 429–436. [Google Scholar]
- Dasgupta, D.; Ray, S. Menopausal problems among rural and urban women from eastern India. Journal of social, behavioral, and health sciences 2009, 3, 2. [Google Scholar]
- Dutta, D.C. A Textbook of Gynecology, 7th ed.; The Health Sciences Publisher: New Delhi, 2016; pp. 46–48. [Google Scholar]
- Ghimire, N.; Dhakal, P.; Norrish, D.; Dangal, G.; Sharma, D.; Dhimal, M.; Aryal, K.K.; Jha, B.K.; Karki, K.B. Menopausal health status of women of Kapilvastu district of Nepal. 2015. [Google Scholar]
- Gyawali, S.; Subedi, S.N.; Yasmin, N.; Pandey, S. Health care seeking practice for menopausal problems among women in Syangja District, Nepal. International Journal of Health Sciences and Research 2016, 6, 247–253. [Google Scholar]
- Kalhan, M.; Singhania, K.; Choudhary, P.; Verma, S.; Kaushal, P.; Singh, T. Prevalence of menopausal symptoms and its effect on quality of life among rural middle aged women (40–60 years) of Haryana, India. International Journal of Applied and Basic Medical Research 2020, 10, 183. [Google Scholar] [PubMed]
- Lee, J.Y.; Suh, C.S. The attitude of postmenopausal women towards hormone replacement therapy (HRT) and the effects of HRT on lipid profile Geneva Foundation for Medical and Research First Census Meeting on Menopause in the East Asian Region. 2010. https://www.ijrcog.org/index.php/ijrcog/article/view/2222.
- Madhukumar, S.; Gaikwad, V.; Sudeepa, D. A community-based study on perceptions about menopausal symptoms and quality of life of post-menopausal women in Bangalore rural. Int J Health Sci Res 2012, 2, 49–56. [Google Scholar]
- Mahajan, N.; Aggarwal, M.; Bagger, A. Health issues of menopausal women in North India. Journal of Midlife Health 2012, 3, 84–97. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3555032. [CrossRef] [PubMed]
- Mujahid, S.; Siddiqui, A.A.; Hussain, R. Awareness of menopausal symptoms among young Pakistani women of different educational backgrounds. Journal of SAFOMS 2013, 1, 18. [Google Scholar] [CrossRef]
- Nisar, N.; SoHo, N.A. The severity of Menopausal symptoms and the quality of life at the different status of Menopause: a community-based survey from rural Sindh, Pakistan. International Journal Collab Res on Internal Med & Public Health 2010. https://www.ncbi.nlm.nih.gov/pubmed/19024187.
- Nitin, J.; Kondagunta, N.; Vittal, S.; Maria, N.; Jagadish, P. Assessment of menopausal symptoms among women attending various outreach clinics in South Canara District of India. 2014. [Google Scholar]
- Paudyal, P.N.; Nepal, M. Knowledge on Perimenopausal Symptoms among Women Attending Lumbini Medical College Teaching Hospital. Journal of Lumbini Medical College 2014, 2, 41–44. [Google Scholar] [CrossRef]
- Prajapati, M.M. Awareness regarding menopausal symptoms and effect on daily life of postmenopausal women. Journal of Patan Academy of Health Sciences 2020, 7, 130–136. [Google Scholar] [CrossRef]
- Raj Bhandari, S.; Amatya, A.; Giri, K. Relation of Ethnicity and Menopausal Symptoms in Nepal. Journal of the South Asian Federation of Menopause Societies. 2013. https://www.womenshealth.gov/files/documents/fact-sheet-menopause.pdf.
- Raj Bhandari, S.; Subedi, R.; Dangal, G.; Phuyal, A.; Vaidya, A.; Karki, A.; Tuladhar, H.; Gurung, B.; Joshi, L.; Shrestha, S. Menopausal Health Status of the Nepalese Women. Journal of Nepal Medical Association 2017, 56, 107–111. [Google Scholar] [CrossRef]
- Shams, A. Knowledge, Attitude and Severity of Menopausal Symptoms among Women Attending Primary Health Care Centers in Cairo, Egypt. Journal of Community Medicine & HealthCare 2018. [Google Scholar]
- Sharma, S.; Adhikari, L.; Karmacharya, I.; Kaphle, M. Menopausal Symptoms among Postmenopausal Women of a Selected Municipality: A Cross-sectional Survey. JNMA: Journal of the Nepal Medical Association 2021, 59, 1155. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, R.P.G.K. Awareness of Menopause among Women Attending at Gynae Outpatient Department in Kathmandu University Hospital, Nepal. 2016. [Google Scholar]
- Singh, A.; Pradhan, S.K. Menopausal symptoms of postmenopausal women in a rural community of Delhi, India: A cross-sectional study. J Midlife Health 2014, 5, 62–67. https://www.ncbi.nlm.nih.gov/pubmed/24970983. [CrossRef] [PubMed]
- Subedi, A.; Shrestha, J.; Chaudhary, J.K. Menopausal Symptoms among Postmenopausal Women Visiting Outpatient Department of a Tertiary Care Centre: A Descriptive Cross-sectional Study. JNMA: Journal of the Nepal Medical Association 2022, 60, 617. [Google Scholar] [CrossRef] [PubMed]
Figure 5.
Analytical charts of respondents’ level of awareness and socio demographic variables.
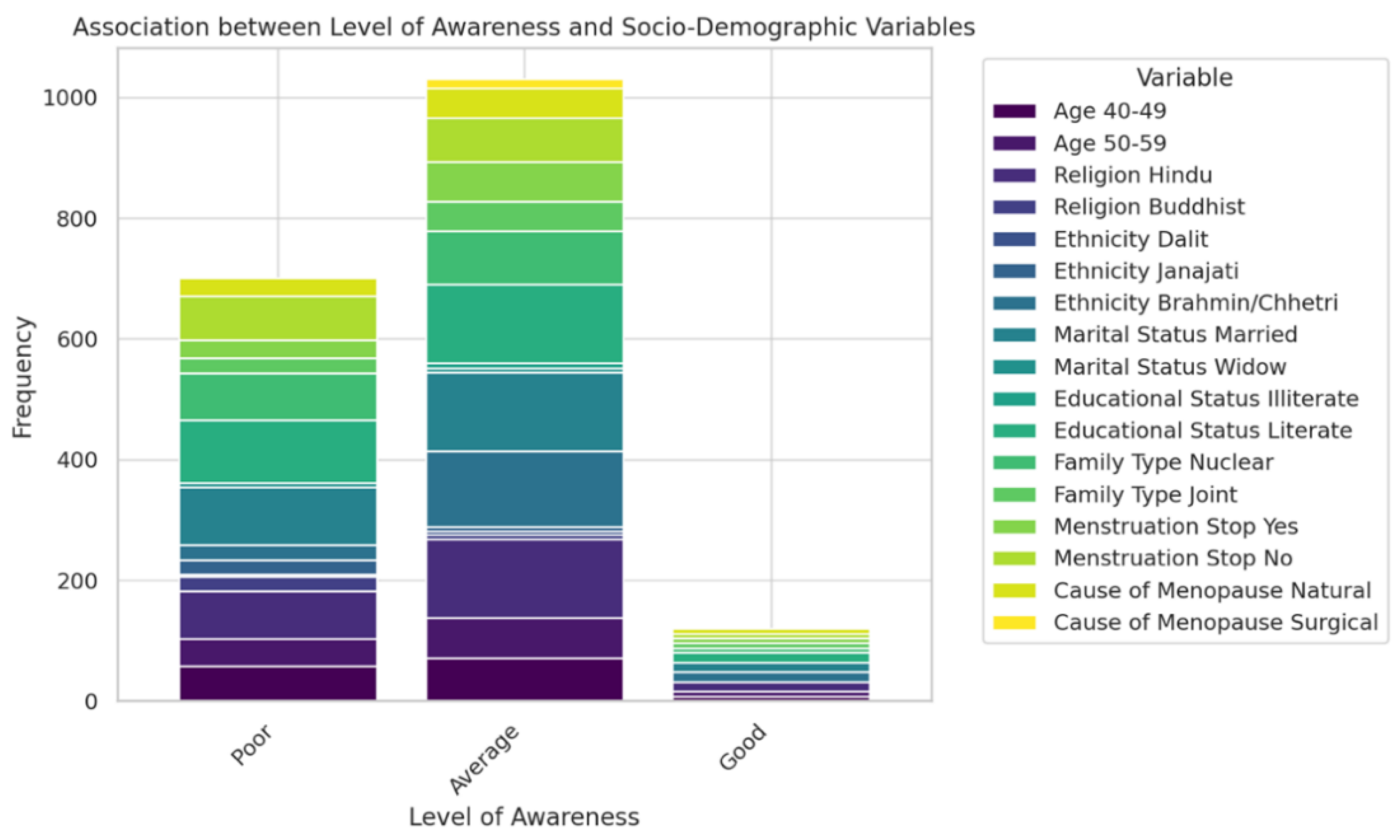
Table 1.
Respondents’ sociodemographic characteristics (age, religion, ethnicity, marital status, educational status, educational level, occupation, family type), n = 257.
Table 1.
Respondents’ sociodemographic characteristics (age, religion, ethnicity, marital status, educational status, educational level, occupation, family type), n = 257.
| Variable | Frequency | Percentage (%) |
|---|---|---|
| Age | ||
| 40-49 | 137 | 53.3 |
| 50-59 | 120 | 46.7 |
| min. = 40, max. = 59, Mean ± SD (48.84 ± 6.27) | ||
| Religion | ||
| Hindu | 225 | 87.5 |
| Buddhist | 32 | 12.5 |
| Ethnicity | ||
| Dalit | 9 | 3.5 |
| Janajati | 32 | 12.5 |
| Bhramin/Chhetri | 216 | 84 |
| Marital status | ||
| Married | 241 | 93.8 |
| widow | 16 | 6.2 |
| Educational status | ||
| Illiterate | 8 | 3.1 |
| Literate | 249 | 96.9 |
| Education level (n = 249) | ||
| General literate | 40 | 15.6 |
| Basic level | 113 | 44 |
| Secondary level | 78 | 30.7 |
| Bachelor and above | 17 | 6.6 |
| Occupation | ||
| Housemaker | 257 | 100 |
| Family type | ||
| Nuclear | 174 | 67.7 |
| Joint | 83 | 32.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



