
Submitted:
09 August 2024
Posted:
12 August 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Unheralded cardiac arrest among previously healthy young people without antecedent illness, months or years after COVID-19 vaccination, highlights the urgent need for risk stratification. The most likely underlying pathophysiology is subclinical myopericarditis and reentrant ventricular tachycardia or spontaneous ventricular fibrillation that is commonly precipitated after a surge in catecholamines during exercise or the waking hours of terminal sleep. Small patches of inflammation and/or edema can be missed on cardiac imaging and autopsy, and the heart can appear grossly normal. This paper reviews evidence linking COVID-19 vaccines to cardiac arrest where unfortunately the majority of victims have had no antecedent clinical evaluation. We propose a comprehensive strategy for evaluating cardiovascular risk post-vaccination, incorporating detailed patient history, antibody testing, and cardiac diagnostics in the best attempt to detect abnormalities before sudden cardiac death. This approach aims to identify individuals at higher risk of cardiac events after COVID-19 vaccination and guide appropriate clinical management. It is prudent for each primary care physician to have a pre-established plan when addressing this issue in their practice.
Keywords:
COVID-19
; mRNA vaccines
; myocarditis
; cardiac arrest
; risk stratification
; cardiovascular safety
Rationale for Risk Stratification
We continue to observe COVID-19 vaccinated persons suffer cardiac arrests since the inception of the mass vaccination campaign in late 2020 [1,2,3,4,5]. Figure 1 illustrates the likely mechanisms. Both Pfizer-BioNTech (BNT162b2) and Moderna (mRNA-1273) mRNA have been found in human heart muscle at autopsy [6]. Spike protein has been stained in endomyocardial biopsy samples of young men suffering from COVID-19 vaccine-induced myocarditis [7]. Victims have been found to have circulating Spike protein but ineffective antibodies, likely IgG4 subclass, that fail to neutralize Spike protein and allow its assault on the heart [8]. Positron emission tomography data have revealed a shift from free fatty acid metabolism to glucose metabolism in the hearts of the majority of individuals who have received a COVID-19 vaccine. [9]. The PET pattern resembles global ischemia. This could be due to vaccine Spike protein hemagglutination in myocardial capillaries or cellular changes in mitochondrial respiration and substrate metabolism [10]. Small patches of dysfunctional, inflamed, or scarred myocardium are sufficient to serve as a nidus for re-entrant ventricular tachycardia that can degrade to ventricular fibrillation and lead to cardiac arrest [11]. A surge in catecholamines (epinephrine, norepinephrine, and dopamine) that can occur during sports or the waking hours of sleep (3 AM to 6 AM) may trigger reentrant ventricular tachycardia or spontaneous ventricular fibrillation leading to a cardiac arrest in patients with COVID-19 vaccine subclinical myocarditis [12].
Elevated numbers of sudden deaths among athletes after COVID-19 vaccination have raised concerns [13]. Alessandria et al amplified these concerns, demonstrating higher all-cause death risks in COVID-19 vaccinated individuals compared to the unvaccinated. Participants that received 2 doses lost 37% of life expectancy compared to the unvaccinated population during follow-up [14]. The largest COVID-19 vaccine safety study to date with approximately 99 million vaccinated individuals found that the risk of myocarditis was significantly elevated after mRNA COVID-19 vaccinations, with the risk being 510% higher following the second dose of the mRNA-1273 vaccine and 186% higher following the second dose of the BNT162b2 vaccine, compared to baseline rates [15]. Hulscher et al have demonstrated that cardiac arrest within a few weeks of COVID-19 vaccination is likely caused by vaccine myocarditis with no prior premonitory phase that allows for detection [16]. Rose et al. found that among individuals with clinical myocarditis shortly after COVID-19 vaccination reported to the Vaccine Adverse Event Reporting System (VAERS), the mortality rate was 2.9% [17].
The U.S. Food and Drug Administration's Center for Biologics Evaluation and Research (CBER) has established a follow-up period of 5 to 15 years for novel genetic products to monitor for any long-term adverse effects that may emerge in the exposed population [18]. With the passage of time, we have learned much from the evaluation of many vaccine-injured victims who have symptoms months to years after injection [19,20,21]. Brogna et al found vaccine-generated stabilized prefusion Spike protein in subjects up to 6 months after COVID-19 mRNA vaccination [22]. Cardiac abnormalities have been observed for at least a year following the initial diagnosis of COVID-19 vaccine-induced myocarditis, suggesting the potential for long-term effects [23]. As of August 5th, 2024, we are unaware of any published risk stratification approach for the prevention of COVID-19 vaccine-induced cardiac arrest. Thus, we propose a comprehensive strategy to address this concerning gap in knowledge.
Risk Stratification Approach
When patients are seen in clinical practice for the initial evaluation of cardiovascular symptoms following SARS-CoV-2 infection or vaccination, a proposed approach is outlined in Figure 2. COVID-19 vaccine-induced myocarditis is caused principally by the Spike protein [7,8,16,24]. Measures of cytokine activation and inflammation are secondary to Spike protein resident in the myocardium and circulating in blood [7,8].
A detailed SARS-CoV-2 infection and vaccine administration history is essential to the evaluation. Serious COVID-19 requiring hospitalization and mechanical ventilation should be noted. Each SARS-CoV-2 infection and COVID-19 vaccine dose can be considered an ‘exposure’. It can be reasonably assumed that the greater the number of exposures, the more likely it is to have large quantities of Spike protein in the body, where natural proteases and lysosomes seem unable to clear it [25].
An extended range total antibody against the Spike protein is a useful proxy for prior Spike exposure. For example, the Roche Diagnostics Elecsys Anti-SARS-CoV-2 Spike assay measures antibodies against the receptor binding domain (RBD) [26]. Roche Elecsys Anti-SARS-CoV-2 assay has a normal value of <0.8 U/ml, and in clinical practice, 0-1000 is low risk, and >1000 indicates higher risk with either multiple infections or COVID-19 vaccine administrations. We have observed that it is not uncommon to find patients with >25,000 U/ml, remaining unmeasurably high even years after vaccination. Antibody concentrations can take at least 12 months to taper off. Thus, a Spike antigen test measurable in whole blood, plasma, or serum is greatly needed to provide a real-time estimate of Spike toxicity.
If (1) the number of Spike protein exposures was low, (2) there were nonserious infections, (3) Spike antibody levels are below 1000 U/ml, (4) minimal or no injection site or initial systemic reaction to vaccination [27,28], and (5) if the vaccine was obtained from a low-risk batch [29,30] (with zero hospitalizations and deaths reported on 'How Bad is My Batch' [31]), then additional clinical investigation may not be warranted. If there are higher risk features as indicated in the Figure 2, then it is prudent to perform more formal cardiac testing and risk stratification.
It is reasonable to obtain an electrocardiogram and blood testing for high-sensitivity troponin, BNP/NT-ProBNP, galectin-3, and D-dimer. Elevated troponin may indicate ongoing myocarditis [32]. BNP/NT-proBNP are reliable indicators of cardiac pressure/volume overload and predict heart failure [33]. Galectin-3 is a chronic inflammation/fibrosis marker and when elevated predicts future heart failure [34]. D-dimer is a proxy for micro-blood clotting [35] and in our experience <0.2 is low risk, 0.2-0.5 is moderate, and >0.5 is high risk for thrombotic events. Patel et al demonstrated that 17% of participants exhibited an increase in d-dimer levels from their normal baseline following COVID-19 vaccination [36]. Genetic testing for pathogenic mutations in cardiac ion channels or major proteins is reasonable in patients with high-risk findings or resuscitated cardiac arrest. Mutations in the SCN5A sodium channel have been associated with an increased risk for COVID-19 vaccine cardiac arrest [37].
Point-of-care echocardiography or formal cardiac ultrasound and Doppler can be used to evaluate cardiac structure, function, and presence of pericardial fluid [38]. This package of diagnostics, when results are completely normal, suggests a low risk for future heart failure and cardiac death [39]. Conversely, multiple abnormalities found in ECG, blood tests, and echocardiography can prompt the use of cardiac MRI with contrast [40]. The MRI is confirmatory for LV function and importantly can detect areas of inflammation/scar with late gadolinium enhancement (LGE) [41]. In other types of cardiomyopathy, LGE ≥15% of the left ventricle indicates high risk for cardiac arrest [42].
Small patches of myocardial inflammation, edema, or fibrosis may not be detectable by axial slices on cardiac MRI or autopsy [43,44]. Thus, the heart may appear normal on post-mortem examination and the final report may indicate death due to “natural causes” in a healthy patient with no antecedent disease. We believe these cases likely represent previously silent subclinical myocarditis and cardiac fibrosis which serves as the substrate for re-entrant ventricular tachycardia that degenerates to ventricular fibrillation and asystole in patients that do not receive prompt defibrillation.
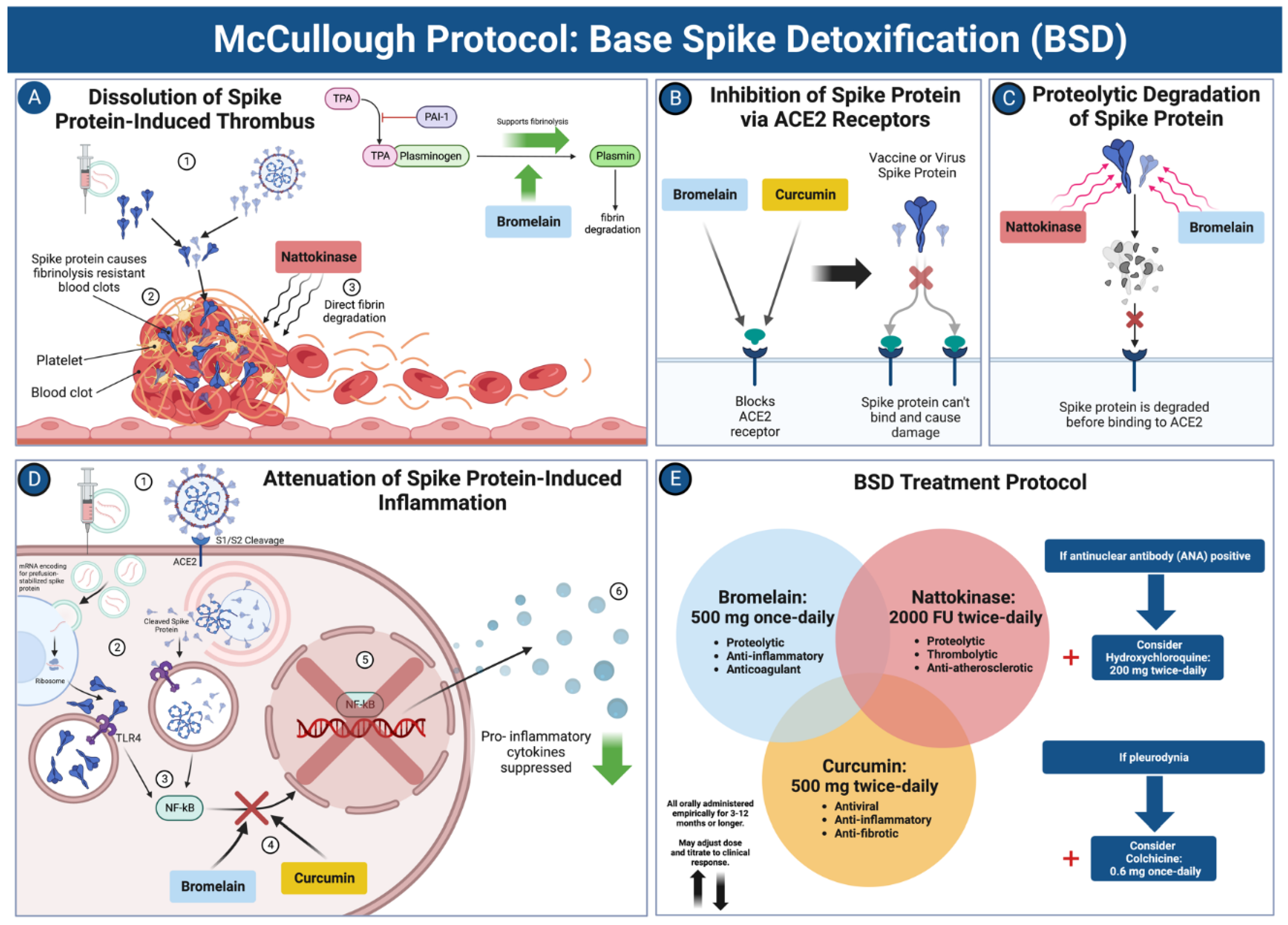
When risk stratification indicates low-risk, primary care office management is suggested with McCullough Protocol: Base Spike Detoxification and adjunctive medications depending on the syndrome (Figure 3) [25]. For subclinical myopericarditis, oral colchicine 0.6 mg BID (twice a day) or QD (once a day) is indicated for at least one year [45]. For COVID-19 vaccine-induced postural orthostatic tachycardia syndrome (POTS), use of colchicine and nadolol 20-40 mg BID can be helpful [46]. In patients who screen as high-risk, Base Spike Detoxification [25] is also indicated. For those at very high risk for cardiomyopathy and or ventricular arrhythmias, formal cardiology consultation is suggested with the main goals of preventing heart failure and sudden death. Additionally, some patients may require ICD implantation if there are symptomatic arrhythmias, LGE > 15%, or genetic predictors such as pathogenic SCN5A mutations [37,47].
Conclusions
In summary, we have proposed a risk stratification approach that addresses the clinical concern of future cardiac arrest following COVID-19 vaccination. The numerous studies highlighting serious cardiovascular safety concerns related to COVID-19 vaccines have raised public and physician awareness. It is prudent for each primary care physician to have a pre-established approach when addressing this issue in their practice.
Acknowledgments
None
Conflicts of Interest
The authors declare no conflict of interest.
Data Availability Statement
Data sharing is not applicable to this article as no new data were created in this study.
Ethics statement
Not applicable
Author Contributions
P.M and N.H: Conceptualization, Investigation, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
This research received no external funding.
References
- Hulscher, N.; Cook, M.; Stricker, R.; McCullough, P. A. Excess Cardiopulmonary Arrest and Mortality after COVID-19 Vaccination in King County, Washington. Preprints 2024, 2024051665. [CrossRef]
- Li YE, Wang S, Reiter RJ, Ren J. Clinical cardiovascular emergencies and the cellular basis of COVID-19 vaccination: from dream to reality?. Int J Infect Dis. 2022;124:1-10. [CrossRef]
- Sun CLF, Jaffe E, Levi R. Increased emergency cardiovascular events among under-40 population in Israel during vaccine rollout and third COVID-19 wave [published correction appears in Sci Rep. 2023 Aug 15;13(1):13276. doi: 10.1038/s41598-023-40234-1]. Sci Rep. 2022;12(1):6978. Published 2022 Apr 28. [CrossRef]
- Sadiq W, Waleed MS, Suen P, Chalhoub MN. Cardiopulmonary Arrest After COVID-19 Vaccination: A Case Report. Cureus. 2022;14(1):e21141. Published 2022 Jan 12. [CrossRef]
- Maruyama T, Uesako H. Lessons Learnt from Case Series of Out-of-hospital Cardiac Arrest and Unexpected Death after COVID-19 Vaccination. Intern Med. 2023;62(22):3267-3275. [CrossRef]
- Krauson AJ, Casimero FVC, Siddiquee Z, Stone JR. Duration of SARS-CoV-2 mRNA vaccine persistence and factors associated with cardiac involvement in recently vaccinated patients. NPJ Vaccines. 2023;8(1):141. Published 2023 Sep 27. [CrossRef]
- Baumeier C, Aleshcheva G, Harms D, et al. Intramyocardial Inflammation after COVID-19 Vaccination: An Endomyocardial Biopsy-Proven Case Series. Int J Mol Sci. 2022;23(13):6940. Published 2022 Jun 22. [CrossRef]
- Yonker LM, Swank Z, Bartsch YC, et al. Circulating Spike Protein Detected in Post-COVID-19 mRNA Vaccine Myocarditis. Circulation. 2023;147(11):867-876. [CrossRef]
- Nakahara T, Iwabuchi Y, Miyazawa R, et al. Assessment of Myocardial 18F-FDG Uptake at PET/CT in Asymptomatic SARS-CoV-2-vaccinated and Nonvaccinated Patients. Radiology. 2023;308(3):e230743. [CrossRef]
- Scheim DE, Vottero P, Santin AD, Hirsh AG. Sialylated Glycan Bindings from SARS-CoV-2 Spike Protein to Blood and Endothelial Cells Govern the Severe Morbidities of COVID-19. Int J Mol Sci. 2023;24(23):17039. Published 2023 Dec 1. [CrossRef]
- Vähätalo JH, Huikuri HV, Holmström LTA, et al. Association of Silent Myocardial Infarction and Sudden Cardiac Death. JAMA Cardiol. 2019;4(8):796-802. [CrossRef]
- Cadegiani FA. Catecholamines Are the Key Trigger of COVID-19 mRNA Vaccine-Induced Myocarditis: A Compelling Hypothesis Supported by Epidemiological, Anatomopathological, Molecular, and Physiological Findings. Cureus. 2022;14(8):e27883. Published 2022 Aug 11. [CrossRef]
- Polykretis P, McCullough PA. Rational harm-benefit assessments by age group are required for continued COVID-19 vaccination. Scand J Immunol. 2023;98(1):e13242. [CrossRef]
- Alessandria M, Malatesta GM, Berrino F, Donzelli A. A Critical Analysis of All-Cause Deaths during COVID-19 Vaccination in an Italian Province. Microorganisms. 2024; 12(7):1343. [CrossRef]
- Faksova K, Walsh D, Jiang Y, et al. COVID-19 vaccines and adverse events of special interest: A multinational Global Vaccine Data Network (GVDN) cohort study of 99 million vaccinated individuals. Vaccine. 2024;42(9):2200-2211. [CrossRef]
- Hulscher N, Hodkinson R, Makis W, McCullough PA. Autopsy findings in cases of fatal COVID-19 vaccine-induced myocarditis. ESC Heart Fail. Published online January 14, 2024. [CrossRef]
- Rose J, Hulscher N, McCullough PA. Determinants of COVID-19 vaccine-induced myocarditis. Ther Adv Drug Saf. 2024;15:20420986241226566. Published 2024 Jan 27. [CrossRef]
- Long Term Follow-Up After Administration of Human Gene Therapy Products [Internet]. FDA; 2020 [cited 2024 Aug 5]. Available from: https://www.fda.gov/media/113768/download.
- Krumholz HM, Wu Y, Sawano M, et al. Post-Vaccination Syndrome: A Descriptive Analysis of Reported Symptoms and Patient Experiences After Covid-19 Immunization. Preprint. medRxiv. 2023;2023.11.09.23298266. Published 2023 Nov 10. [CrossRef]
- Shrestha Y, Venkataraman R: The prevalence of post-COVID-19 vaccination syndrome and quality of life among COVID-19-vaccinated individuals [IN PRESS]. Vacunas. 2023. [CrossRef]
- Said KB, Al-Otaibi A, Aljaloud L, et al. The Frequency and Patterns of Post-COVID-19 Vaccination Syndrome Reveal Initially Mild and Potentially Immunocytopenic Signs in Primarily Young Saudi Women. Vaccines (Basel). 2022;10(7):1015. Published 2022 Jun 24. [CrossRef]
- Brogna C, Cristoni S, Marino G, et al. Detection of recombinant Spike protein in the blood of individuals vaccinated against SARS-CoV-2: Possible molecular mechanisms. Proteomics Clin Appl. 2023;17(6):e2300048. [CrossRef]
- Yu CK, Tsao S, Ng CW, et al. Cardiovascular Assessment up to One Year After COVID-19 Vaccine-Associated Myocarditis. Circulation. 2023;148(5):436-439. [CrossRef]
- Parry PI, Lefringhausen A, Turni C, et al. 'Spikeopathy': COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA. Biomedicines. 2023;11(8):2287. Published 2023 Aug 17. [CrossRef]
- Hulscher N, Procter BC, Wynn C, McCullough PA. Clinical Approach to Post-acute Sequelae After COVID-19 Infection and Vaccination. Cureus. 2023;15(11):e49204. Published 2023 Nov 21. [CrossRef]
- Elecsys® Anti-SARS-CoV-2 S. Roche Diagnostics. Accessed August 5, 2024. https://diagnostics.roche.com/us/en/products/lab/elecsys-anti-sars-cov-2-s-cps-000616.html.
- Komici K, Verderosa S, D'Amico F, Guerra G. Self-reported side effects following COVID-19 vaccination in athletes: A retrospective study. Hum Vaccin Immunother. 2023;19(2):2234788. [CrossRef]
- Schwab C, Domke LM, Hartmann L, Stenzinger A, Longerich T, Schirmacher P. Autopsy-based histopathological characterization of myocarditis after anti-SARS-CoV-2-vaccination. Clin Res Cardiol. 2023;112(3):431-440. [CrossRef]
- Schmeling M, Manniche V, Hansen PR. Batch-dependent safety of the BNT162b2 mRNA COVID-19 vaccine. Eur J Clin Invest. 2023;53(8):e13998. [CrossRef]
- Fürst T, Šourek P, Krátká Z, Janošek J. Batch-dependent safety of COVID-19 vaccines in the Czech Republic and comparison with data from Denmark. Eur J Clin Invest. Published online June 27, 2024. [CrossRef]
- Knoll F. How Bad is My Batch? [Online]. GitHub; 2024 [cited 2024 Aug 5]. Available at: https://knollfrank.github.io/HowBadIsMyBatch/HowBadIsMyBatch.html.
- Sen G, Scully P, Gordon P, Sado D. Advances in the diagnosis of myocarditis in idiopathic inflammatory myopathies: an overview of diagnostic tests. Rheumatology (Oxford). 2024;63(7):1825-1836. [CrossRef]
- Silver MA, Maisel A, Yancy CW, et al. BNP Consensus Panel 2004: A clinical approach for the diagnostic, prognostic, screening, treatment monitoring, and therapeutic roles of natriuretic peptides in cardiovascular diseases [published correction appears in Congest Heart Fail. 2005 Mar-Apr;11(2):102]. Congest Heart Fail. 2004;10(5 Suppl 3):1-30. [CrossRef]
- McCullough PA, Olobatoke A, Vanhecke TE. Galectin-3: a novel blood test for the evaluation and management of patients with heart failure [published correction appears in Rev Cardiovasc Med. 2012;13(1):e52]. Rev Cardiovasc Med. 2011;12(4):200-210. [CrossRef]
- Bounds EJ, Kok SJ. D Dimer. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 31, 2023.
- Patel, F., Roux, J.L., Sawry, S., Kieser, R., Dhar, M., Gill, K., Lazarus, E., Nana, A., Garrett, N., Moore, P.L., Sigal, A., Gray, G., Rees, H., Jacobson, B.F., & Fairlie, L. Clot Twist - D-dimer analysis of healthy adults receiving heterologous or homologous booster COVID-19 vaccine after a single prime dose of Ad26.COV2.S in a phase II randomised open-label trial, BaSiS. 2024. medRxiv. [CrossRef]
- Ittiwut C, Mahasirimongkol S, Srisont S, et al. Genetic basis of sudden death after COVID-19 vaccination in Thailand. Heart Rhythm. 2022;19(11):1874-1879. [CrossRef]
- Maheshwari S, Dagor H. Evolving the Scope of Cardiac Point-of-Care Ultrasound in the Current Era. Cureus. 2024;16(2):e53985. Published 2024 Feb 10. [CrossRef]
- Money DB, Mehio M, Scoma C, Gupta S. Cardiac Point-of-Care Ultrasound (P.O.C.U.S.) Utilization for Hospitalists in the Assessment of Patients with Cardiac Complaints: An Educational Overview. J Community Hosp Intern Med Perspect. 2023;13(4):1-8. Published 2023 Jun 29. [CrossRef]
- Rajiah PS, François CJ, Leiner T. Cardiac MRI: State of the Art. Radiology. 2023;307(3):e223008. [CrossRef]
- Sen G, Scully P, Gordon P, Sado D. Advances in the diagnosis of myocarditis in idiopathic inflammatory myopathies: an overview of diagnostic tests. Rheumatology (Oxford). 2024;63(7):1825-1836. [CrossRef]
- Chan RH, Maron BJ, Olivotto I, et al. Prognostic value of quantitative contrast-enhanced cardiovascular magnetic resonance for the evaluation of sudden death risk in patients with hypertrophic cardiomyopathy. Circulation. 2014;130(6):484-495. [CrossRef]
- Karur GR, Aneja A, Stojanovska J, et al. Imaging of Cardiac Fibrosis: An Update, From the AJR Special Series on Imaging of Fibrosis. AJR Am J Roentgenol. 2024;222(6):e2329870. [CrossRef]
- Zhu L, Wang Y, Zhao S, Lu M. Detection of myocardial fibrosis: Where we stand. Front Cardiovasc Med. 2022;9:926378. Published 2022 Sep 29. [CrossRef]
- Valore L, Junker T, Heilmann E, et al. Case report: mRNA-1273 COVID-19 vaccine-associated myopericarditis: Successful treatment and re-exposure with colchicine. Front Cardiovasc Med. 2023;10:1135848. Published 2023 Apr 17. [CrossRef]
- Sanada Y, Azuma J, Hirano Y, Hasegawa Y, Yamamoto T. Overlapping Myocarditis and Postural Orthostatic Tachycardia Syndrome After COVID-19 Messenger RNA Vaccination: A Case Report. Cureus. 2022;14(11):e31006. Published 2022 Nov 2. [CrossRef]
- Iqbal AM, Butt N, Jamal SF. Automatic Internal Cardiac Defibrillator. In: StatPearls. Treasure Island (FL): StatPearls Publishing; May 22, 2023.
Figure 1.
COVID-19 Vaccine-induced Cardiac Arrest. Abbreviations: NSR = normal sinus rhythm, VT = ventricular tachycardia, VF = ventricular fibrillation, BNP/NT-proBNP = brain natriuretic peptide and N-terminal proBNP. *All the studies referenced in this figure are listed in the reference section of this manuscript. Created with BioRender.com.
Figure 1.
COVID-19 Vaccine-induced Cardiac Arrest. Abbreviations: NSR = normal sinus rhythm, VT = ventricular tachycardia, VF = ventricular fibrillation, BNP/NT-proBNP = brain natriuretic peptide and N-terminal proBNP. *All the studies referenced in this figure are listed in the reference section of this manuscript. Created with BioRender.com.
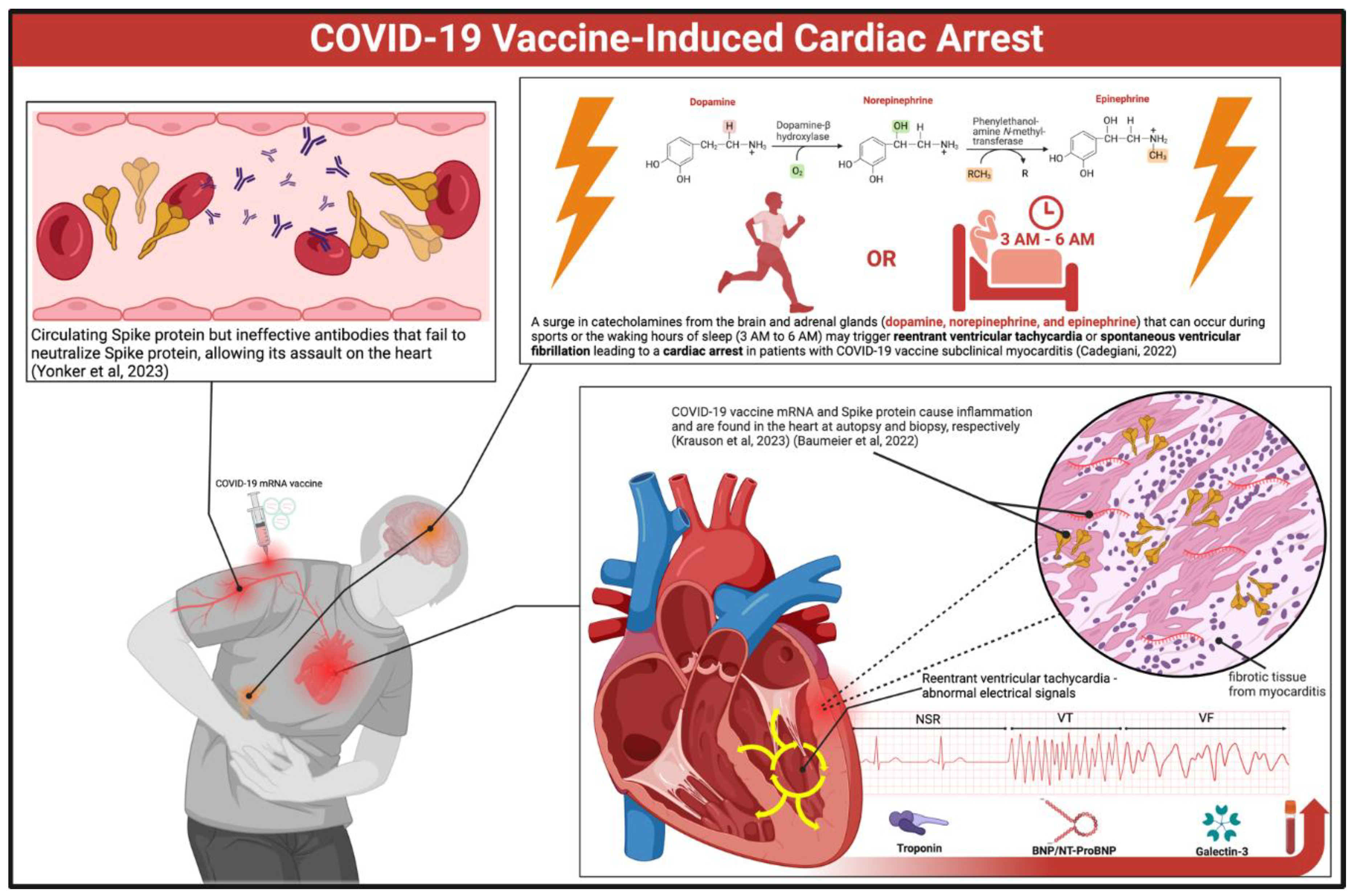
Figure 2.
Risk Stratification Approach for Future Cardiac Arrest after COVID-19 Vaccination. Green boxes indicate clinical features, test results, and patients at lower risk. Red and pink boxes show tests and results indicating higher risk. Abbreviations: Hx = history, AU/ml = antibody units per milliliter, HR = heart rate, BP = blood pressure, ECG = electrocardiogram, Hs-troponin = high-sensitivity troponin, BNP/NT-proBNP = brain natriuretic peptide and N-terminal proBNP, LVEF = left ventricular ejection fraction, POTS = Postural orthostatic tachycardia syndrome. *Created with BioRender.com.
Figure 2.
Risk Stratification Approach for Future Cardiac Arrest after COVID-19 Vaccination. Green boxes indicate clinical features, test results, and patients at lower risk. Red and pink boxes show tests and results indicating higher risk. Abbreviations: Hx = history, AU/ml = antibody units per milliliter, HR = heart rate, BP = blood pressure, ECG = electrocardiogram, Hs-troponin = high-sensitivity troponin, BNP/NT-proBNP = brain natriuretic peptide and N-terminal proBNP, LVEF = left ventricular ejection fraction, POTS = Postural orthostatic tachycardia syndrome. *Created with BioRender.com.
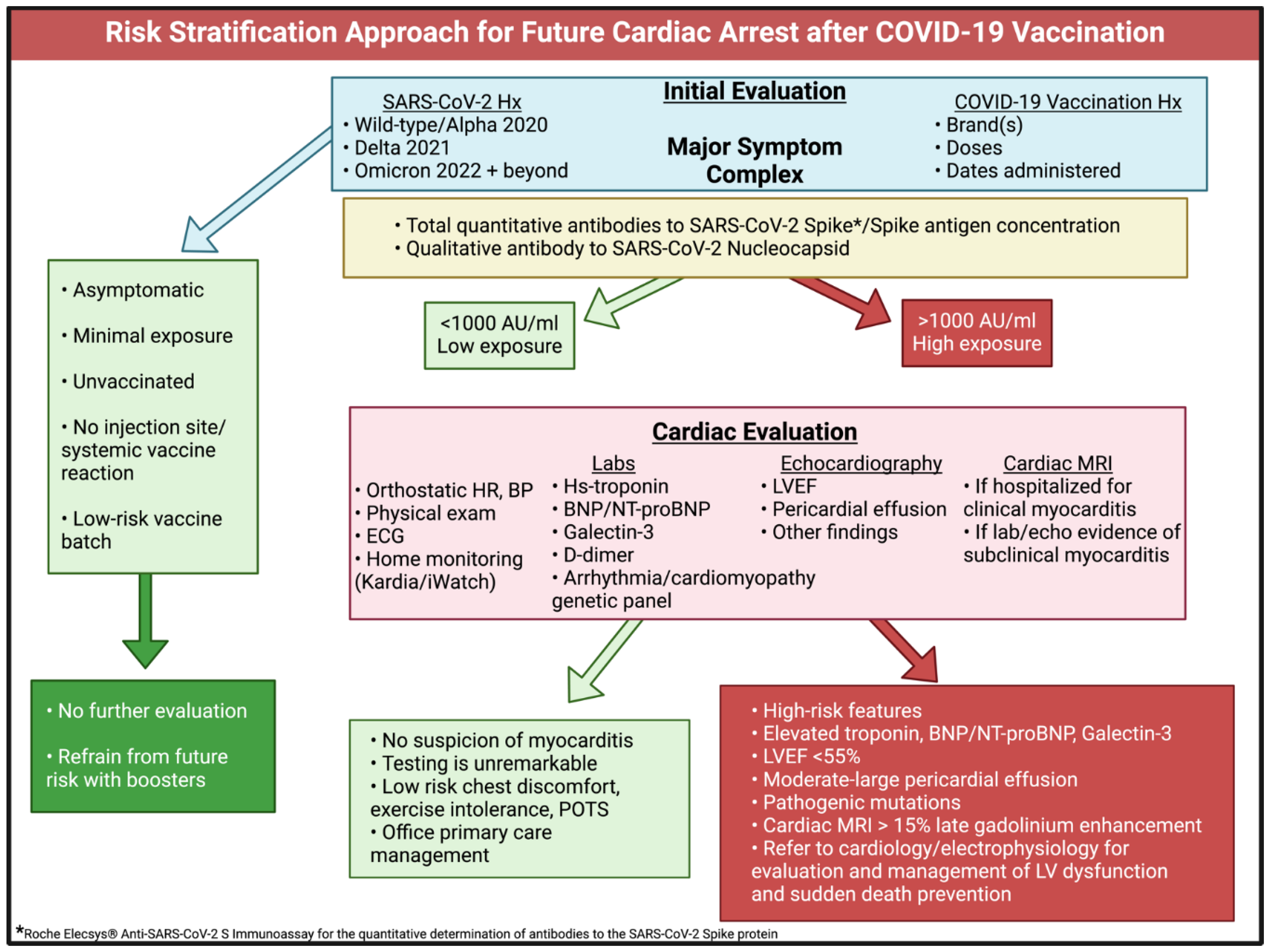
Figure 3.
McCullough Protocol: Base Spike Detoxification (BSD). A: Dissolution of spike protein-induced thrombus. Nattokinase directly degrades fibrinolysis-resistant fibrin (from spike protein), and bromelain upregulates fibrinolysis. B: Inhibition of spike protein via ACE2 receptors. Bromelain and curcumin block the ACE2 receptor, preventing spike protein from binding. C: Proteolytic degradation of spike protein. Nattokinase and bromelain degrade spike proteins, rendering them inactive. D: Attenuation of spike protein-induced inflammation. Bromelain and curcumin downregulate the NF-kB signaling pathway induced by spike protein, leading to the suppression of inflammatory molecules. E: BSD treatment protocol. The full treatment regimen and the addition of other compounds based on clinical indication are illustrated. Abbreviations: TPA = tissue plasminogen activator, PAI-1 = plasminogen activator inhibitor-1, ACE2 = angiotensin converting enzyme-2, NF-kB = nuclear factor kappa B, S1/S2 = spike protein subunits S1/S2, TLR4 = toll-like receptor 4. *Figure and legend reprinted from Hulscher et al [25]. Permission to use this figure has been granted in accordance with the open access Creative Common CC BY 4.0 license. Created with BioRender.com.
Figure 3.
McCullough Protocol: Base Spike Detoxification (BSD). A: Dissolution of spike protein-induced thrombus. Nattokinase directly degrades fibrinolysis-resistant fibrin (from spike protein), and bromelain upregulates fibrinolysis. B: Inhibition of spike protein via ACE2 receptors. Bromelain and curcumin block the ACE2 receptor, preventing spike protein from binding. C: Proteolytic degradation of spike protein. Nattokinase and bromelain degrade spike proteins, rendering them inactive. D: Attenuation of spike protein-induced inflammation. Bromelain and curcumin downregulate the NF-kB signaling pathway induced by spike protein, leading to the suppression of inflammatory molecules. E: BSD treatment protocol. The full treatment regimen and the addition of other compounds based on clinical indication are illustrated. Abbreviations: TPA = tissue plasminogen activator, PAI-1 = plasminogen activator inhibitor-1, ACE2 = angiotensin converting enzyme-2, NF-kB = nuclear factor kappa B, S1/S2 = spike protein subunits S1/S2, TLR4 = toll-like receptor 4. *Figure and legend reprinted from Hulscher et al [25]. Permission to use this figure has been granted in accordance with the open access Creative Common CC BY 4.0 license. Created with BioRender.com.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



