
Submitted:
12 August 2024
Posted:
12 August 2024
You are already at the latest version
Abstract
Pneumococcal disease, caused by Streptococcus pneumoniae is the leading cause of high mortality in children worldwide. The tremendous direct cost of hospital admissions and significant indirect costs from productivity loss contributed considerably to the economic burden, with vaccination being the only efficient way against the illness. Our study aims to summarize the cost-effectiveness of the pneumococcal conjugate vaccine (PCV) implemented in the pediatric population. Employing online databases from Pubmed, Embase, and Medline, we looked for economic evaluation from 2018 until March 2024. The Incremental Cost-Effectiveness Ratios (ICER) and Quality-Adjusted-Life-Years (QALY) were the primary outcomes for measuring PCV's cost-effectiveness. A 28-item CHEERS 2022 checklist was applied to assess the quality of collected studies. Of the 16 papers found, 9/16 discussed the lower-valent vaccine (PCV13, PCV10) and 7/16 examined the higher-valent vaccine. (PCV20, PCV15). PCV13 and PCV10 required more cost and generated more QALY compared to no vaccination. Both PCV15 and PCV20 averted substantial healthcare costs and yielded greater quality of life than PCV13. Additionally, PCV20 was a dominant strategy compared to PCV15. Utilizing PCV13 is a very cost-effective option compared to not getting vaccinated. Transitioning from PCV13 to PCV20 would result in higher QALY gain and more cost-saving than switching to PCV15.
Keywords:
Cost-effectiveness analysis
; pneumococcal vaccine
; pediatric
; systematic review
1. Introduction
Streptococcus pneumoniae is the causative pathogen of pneumococcal disease (PD), which is currently the most widespread infectious illness worldwide [1,2,3,4]. The polysaccharide capsule, which characterizes its serotype, is the primary virulence component required for the organism to infect its host and induce illness [5,6]. Up until now, there are 101 distinct serotypes recognized [7]. A small number of serotypes mainly cause pneumococcal disease, whereas the majority produce serious illness [8]. There are 2 forms of PD: pneumococcal invasive disease (IPD) and non-invasive one [9]. Despite a relatively low occurrence, IPD is the most severe presentation, involving meningitis, bacteremia, and sepsis [10]. The mortality rate is substantial, with up to 10% for meningitis and 15% for bacteremia, and survivors may have serious aftereffects [3]. Conversely, non-invasive disease includes more prevalent but milder conditions such as otitis media, sinusitis, and pneumonia [11,12,13].
Pneumococcus infections can strike persons of any age. However, those with underlying medical conditions, young children under 2, and adults over 65 are probably the most susceptible [10]. The annual mortality rate from pneumococcal disease among children is approximately one million, with the majority of these deaths occurring in developing nations [14,15]. Pneumonia significantly contributes to this burden, evidenced by its association with approximately 11–20 million severe hospitalized cases among children under 5 years of age [16]. Recent estimates from the World Health Organization (WHO) indicated that in 2019, pneumonia was responsible for the demise of 740,180 children under 5 years old, constituting 14% of all pediatric deaths within this age [17]. Notably, the most vulnerable region focused on South Asia (2,500 cases per 100,000 children) and West and Central Africa (1,620 cases per 100,000 children) [18]. In Ethiopia, acute respiratory infections are the leading cause of mortality among children under five, comprising 18% of deaths within this age group. Pneumonia contributes explicitly to 16.4% of all deaths in the country, making Ethiopia the highest pneumonia-related mortality rate among Sub-Saharan African nations [18].
The implementation of pneumococcal conjugate vaccines (PCVs) via infant immunization has demonstrated success in mitigating the prevalence of pneumococcal infections [19,20,21,22]. The first vaccine circulated was PCV7 in the USA in the year 2000, serving the pediatric population [23]. Before PCV introduction, IPD’s annual incidence rate was recorded as the highest in children under 2 years old in the USA, with 165 cases/100,000 children <12 months of age and 203 cases/100,000 children 12–23 months of age [23]. The number of cases due to PCV7 serotypes then fell considerably to less than 1 case per 100,000 by 2007, after the introduction of PCV7 [24]. The prevalence of S. pneumoniae infections has decreased significantly since the dissemination and implementation of PCV13, which provided protection against a broader range of serotypes than PCV7 [25]. In the USA, a review of the literature in 2021 regarding the cumulative 20-year effect of PCV among children under the age of five showed that PCVs helped to reduce 91% of IPD incidences between 1997 and 2019 [23]. Additionally, annual pneumonia hospitalizations decreased by 66%–79%, from 110,000 cases among children under 5 years old [23]. In England and Wales, the implementation of PCV13 has led to a reduction of over 50% in the overall incidence of IPDs [25].
Though vaccination is the most efficient approach to saving lives, the economic burden is huge: healthcare costs US$13.7 billion each year, while societal costs US$14.3 billion worldwide [26].The primary contributor to the considerable financial burden of the illness was the hospitalization cost [26,27,28]. A 19-year evaluation of Canadian healthcare expenses following the introduction of PCV13 in infants found that admission to the hospital accounted for 92% of overall costs, which amounted to $7.25 billion (2018 Canadian dollars) [28]. In a low-income country like Nigeria, the surveillance discovered that one-third of the households suffered from hospitalization charges that exceeded 25% of their monthly income, emphasizing the burden of significant treatment costs [26]. Not to mention considerable indirect costs from productivity losses, including premature disability and fatalities in children ($3.1 billion in 2004 [2007 US dollars]) and days of work loss for taking care of their child ($914 million in 2004) [19].
Given S.pneumoniae stands out as the most common cause of community-acquired-pneumonia (CAP) in children <5 years of age [29], the treatment expenses were tremendous. A retrospective study conducted from 2003 to 2019 found that, among children in England, CAP exhibited the highest annual inpatient admission rate per 1,000 patients, surpassing both IPD and pneumococcal pneumonia [30]. In Europe, the aggregate medical bills associated with CAP were approximated at €10.1 billion annually, with about one-third of these expenditures allocated to indirect costs [27]. In Germany, all-cause-pneumonia (ACP) accounted for the highest outpatient visit rate between 2014-2019 in children under 16 years old [16].
In terms of cost per episode, IPD had the most significant treatment costs but the fewest cases compared to AOM and pneumonia [16,29,30]. On the contrary, albeit AOM's treatment cost per case was relatively modest, it was the most significant contributor to the PD economic burden because of the high frequency and massive amount of antibiotic prescribing charges [21,27,29,30]. Following Amicizia et al.’s research, which took place in Italy from 2012 to 2018, AOM was deemed as the most recorded PD case, with 61.6% (17,040 episodes) [27]. The same pattern was documented in the United States, where AOM episodes were ten-fold higher than IPD alone (about 16 million vs 2500 cases) [29]. As a result, $4.3 billion was spent each year (in the period 2014-2018) [29]. In England, AOM treatment costs 13,484,959£ per year, twice that of IPD, with 5,907,285£ [30].
Nevertheless, the burden of PD persists due to the emergence of non-vaccine serotypes (NVT), a phenomenon known as serotype replacement [14,16,27,31,32]. The ongoing rise in the occurrence of NVT serotypes, explicitly 3 and 19A, may counteract the positive impact of the decreased prevalence of vaccine serotypes (VTs) subsequent to the implementation of PCV13 [25,33]. Currently, the development of higher-valent vaccines is underway to address this issue of NVT, including PVCV15, which has recently gained approval for use in infants and adults in Europe, the US, and Canada, and PCV20, which has been approved for adult use in Europe and the US [16,30]. Given that vaccine costs remain relatively high and accessibility remains a concern, it is imperative to assess the cost-effectiveness of these vaccines. Such data are essential for governments to allocate resources effectively based on informed decisions. Consequently, we aim to conduct a systematic review focusing on the cost-effectiveness of authorized vaccines currently available on the market to elucidate the prevailing trends in this regard.
2. Materials and Methods
2.1. Search Strategy
Our research was carried out using the PRISMA 2020 checklist [34]. We conducted a comprehensive search for economic analyses pertaining to pneumococcal vaccines from 2018 to 2024 using electronic sources, including Pubmed, Medline, and Embase. The last article was retrieved on March 2024. The key phrases included “pneumococcal disease,” “PCV,” “pediatric,” and “cost-effectiveness analysis” were used to search publications. The main code used in the search process proceeded as follows: ((pneumococcal) AND (cost-effectiveness)) AND ((PCV) OR (pneumococcal conjugate vaccine)) AND (pediatric).
2.2. Selection Process
The inclusion criteria for qualifying the economic evaluations are as follows: (1) the study falls within the scope of economic analysis, encompassing cost-effectiveness analysis (CEA), cost-utility analysis (CUA), or cost-benefit analysis (CBA); (2) the investigation centers on the pediatric population (under 18 years of age); (3) specific pneumococcal vaccines are compared; (4) pertinent information regarding health outcomes such as incremental cost-effectiveness ratio (ICER), quality-adjusted life years (QALY), or disability-adjusted life years (DALY) is provided; (5) a clear determination regarding the cost-effectiveness of the intervention is presented; (6) full-text accessibility is ensured; (7) articles are published in English.
Conversely, articles will be disqualified if they meet any of the following exclusion criteria: (1) the research does not fall within the scope of economic analysis; (2) participants are adults; (3) the comparison of pneumococcal vaccines is not clearly specified; (4) data regarding health outcomes are ambiguous; (5) no definitive conclusion regarding cost-effectiveness is drawn; (6) full-text accessibility is unavailable; (7) reports are not written in English.
2.3. Data Extraction
The chosen reports will then be summarized by extracting the following details: the first author, publication year, country, type of economic evaluation, target clinical outcomes, comparison, study, model approach, time horizon, discount rate, currency, perspective, vaccine coverage, vaccine schedule, herd effect inclusion in base-case analysis, funding source, health outcomes, and sensitivity analysis. Our primary outcome is ICER (incremental cost-effectiveness ratio), which can be defined as the ratio of the incremental costs to the incremental effectiveness achieved between two interventions [35]:
The effectiveness of health benefits can be measured in terms of QALYs (Quality-Adjusted Life Years) or DALYs (Disability-adjusted Life Years). All of the ICERs were retrieved within the base-case analysis of each cost-effectiveness evaluation.
The study includes two types of costs: direct and indirect. Direct costs include vaccination costs and healthcare costs (such as hospitalization expenses or treatment costs), while indirect costs encompass non-medical costs, such as caregivers' productivity loss when caring for their sick children.
If feasible, cost-effectiveness thresholds (CE threshold) were also derived from economic evaluation to compare the ICERs. It is the utmost monetary value that a healthcare decision-maker or society is willing to expend in exchange for one unit of health benefit [36]. In general, a cost-effectiveness threshold is established to identify interventions that exhibit comparatively or exceptionally favorable value for money [37]. GDP-based thresholds or WTP-based thresholds may be applied. Following the World Health Organization’s Choosing Interventions that are Cost–Effective project (WHO-CHOICE) suggestion, if the cost per disability-adjusted life-year (DALY) avoided was less than the national annual x1 GDP per capita of the country, the intervention is deemed “very cost-effective”, whereas the range within 2-3 times GDP per capita is considered as “cost-effective”, and then if the cost exceeds x3 GDP per capita it is called “not cost-effective” [37]. Willingness-to-pay (WTP) is the highest possible level of money the government is willing to pay in exchange for a health benefit. This threshold will determine whether or not a specific intervention is financially worthwhile to invest in. An intervention is thought to be "cost-effective" if the ICERs lie within the WTP range; conversely, if they go above the WTP, it is deemed "not cost-effective." [38].
The secondary outcome is sensitivity analysis (SA), which encompasses both deterministic sensitivity analysis (DSA) and probabilistic sensitivity analysis (PSA). Its aim is to assess uncertainty or examine the robustness of specific model outcomes under plausible ranges of key parameters. DSA employs a tornado diagram to visually represent the impact of the most significant parameter inputs, dynamically adjusting the value of a single economic model parameter at a time (e.g., case fatality rate, costs, or indirect effects). In contrast, PSA involves selecting each parameter from 1000 iterations of Monte Carlo simulation. This PSA enables the estimation of the disparity of the ICER when multiple inputs are varied simultaneously.
2.4. Articles Quality Assessment
To verify our selected economic analysis technique, we used the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) 2022 tool checklist [39]. The checklist, which consists of 28 elements, evaluates the essential data that must be provided for a typical economic analysis. Each item can be given one of three values: "1" for a fully completed response, "0.5" for a partially completed response, and "0" for information that was not relevant or was not applicable. Then we ranked the quality of reports based on the total score; those above 21 were deemed as high quality, reports scoring between 14-24 were classified as moderate quality, and the ones less than 14 were considered poor quality [40]. All of the articles were reviewed separately by two independent researchers.
3. Results
3.1. Studies Selection Process
Our selection process is summarized in Figure 1. A total of 434 articles were identified from different electronic databases, of which Pubmed accounted for 188 papers, Cochrane covered 3 articles, and the rest were from Embase. Following the removal of duplicates, we decomposed 409 papers by applying inclusion and exclusion criteria to the title and abstract screening. Consequently, we were left with 18 reports, from which we extracted data by accessing the full text. Two studies were eliminated during the process: one from Wang et al. [41] compared immunization schedules, and the other from Eythorsson et al. [42] could not articulate health outcomes but instead broke down clinical outcomes into distinct categories to evaluate cost-effectiveness. In the end, sixteen papers met the requirements for data analysis.
3.2. Characteristics of Included Studies
The overall information of the chosen evaluation is demonstrated in Table 1. The majority of collected articles were CEA with 13/16; there were 3/16 articles conducted CUA [43,44,45] with 1/16 used CBA [43]. Markov model was the most wildly used approach, which took account of 50% of the studies [43,44,46,47,48,49,50,51]. Time horizon varied from 1 year to 100 years (lifetime), with the length of 10 years being the most applied period in 8/16 articles [45,46,49,50,51,52,53,54].The discount rate also fluctuated from 1.50% to 7%, with the level of 3% being the most popular rate in 9/16 publications [43,44,47,48,50,51,52,55,56]. Each of the articles can apply more than one perspective, in which payer [43,45,46,49,54,55,57,58] and societal perspective [43,46,47,48,49,51,53] were both recorded in 8/16 papers. Additionally, vaccine uptake levels could be different depending on how long one country introduced PCV, ranging from 70% to 100%. Most of the studies were sponsored by pharmaceutical companies such as Pfizer (68.7%, 11/16 studied) [43,45,46,47,50,51,53,54,55,58], Merck (12.5%, 2/16 papers) [48,49], the other was from international organizations such as WHO, GAVI, and Melinda Gates Foundation (6.2%, 1/16 paper) [56].
3.3. Quality Assessment
16/16 articles were considered good quality, with the lowest score from 21.5/28 [45]. Details about quality grading following CHEER's 2022 statement are presented in Table 2. Most of the articles didn’t meet the information for item 21, “Approach to engagement with patients and others affected by the study,” and item 25, “Effect of engagement with patients and others affected by the study.”
3.4. Cost-Effectiveness Related Data
3.4.1. Lower-Valent Pneumococcal Vaccine
The incremental effect of lower-valent pneumococcal vaccine was summarized in Table 3, including PCV13, PCV10. The majority of countries that conducted PCV13 analysis focused on Asia [43,47,52,55,57]. Compared to no vaccination, implementing PCV13 would increase total cost (mainly driven by direct cost) and provide greater QALY [43,47,52,55,56,57]. All of the ICER was below x1 GDP per capita, indicating PCV13 is a cost-effective strategy [43,44,47,55,57]. In China, including herd effect would reduce the total cost and extend QALY, thus leading to much lower ICER per QALY gained (79,304 CNY vs. 3,777 CNY; cost inflated to year 2015) demonstrating a very cost-effective choice, compared to excluding herd-effect scenario [55]. In addition, PCV10 was reported to be cost-effective in Egypt and Bhutan, compared to no vaccination, with the ICERs lower than x1 GDP per capita [43,44]. In contrast, PCV10 was not cost-effective due to ICER exceeding the WTP 160,000 TBH/QALY in Thailand (cost inflated to the year 2018) when excluding the herd effect [47].
3.4.2. Higher-Valent Pneumococcal Vaccine
The results of ICER and cost reduction of the newest vaccines are illustrated in Table 4. Compared to PCV13, all of the higher valency PCVs were reported to be a dominant strategy [46,48,49,50,51,58]. These CEAs about the newest licensed vaccines took place in developed countries such as the USA, UK, Japan, Canada, and Germany. Implementing PCV15 resulted in higher vaccine costs, but the averted pneumococcal treatment costs offset it [48,49,58]. Consequently, using PCV15 led to higher QALY, higher LYs, and more cost-saving in terms of a 3+1 schedule. In the UK, with the willingness-to-pay threshold (WTP) of 20,000 GBP/QALY, choosing PCV15 in the 1+1 schedule was more cost-effective than PCV13 in the 1+1 schedule but not in PCV15 2+1 schedule, as the ICER was greater than WTP (313,229 GBP/ QALY vs. 20,000 GBP/ QALY) [58].
Similarly, PCV20 was dominant compared to PCV13 in 4/4 analysis [46,50,51,58]. Though it required investment to introduce the vaccine, the productivity loss reduction and the prevented medical cost outweighed it significantly. Considering the 1+1 schedule, PCV20 provided higher QALY gain (28,096 vs. 361), LYs gain (23,165 vs. 262), and more cost reduction (459 million GBP vs. -1 million GBP) than PCV15 when comparing with PCV13 [58] (cost was inflated to the year 2021).
3.5. Sensitivity Analysis
The result of sensitivity analysis in vaccines with lower valency was demonstrated in Table 5. When comparing PCV13 and PCV10 vaccines to no vaccination, the most driven parameters that affect ICERs are discount rate [43,44,57] and incidence rate [43,55,56,57]. The result from PSA indicated that 100% of iterations focused on the Northeast. It appeared that utilizing PCV13 would be more expensive but would also lead to a greater improvement in quality of life compared to not using any immunization [47,52,56].
The results of DSA and PSA in higher-valent pneumococcal vaccines are presented in Table 6. It can be seen that the indirect effect was one of the parameters that affected the cost value [46,50,51] in DSA. In addition, the ICER of these PCVs was sensitive to vaccination cost [50]. However, in PSA results, PCV20 was shown to be a dominant intervention compared to both PCV13 and PCV15, as all of the stimulation focused on the Southeast quadrant, which indicated PCV20 was less costly and more effective than PCV13 [46,50,51,54]. The same pattern was observed in PCV15 vs. PCV13; the majority of the simulations demonstrated positive ICERs [48,49], indicated that PCV15 would be a more economical option to prevent pneumococcal disease compared to PCV13.
4. Discussion
Based on our research findings, employing PCV13 or PCV10 demonstrated enhanced cost-effectiveness and augmented quality-adjusted life years (QALY) in comparison to the absence of vaccination. The majority of ICERs were below half of the Gross Domestic Product (GDP) per capita[43,44,52], or falling within the WTP threshold [47,56], suggesting a very cost-effective option. Furthermore, despite the higher monetary investment necessary to manage the PCV13 vaccine, it has the potential to decrease the direct cost, particularly hospitalization costs significantly. According to the 10-year cohort in India, introducing the PCV13 vaccine program in India would cost 35 million USD (cost was inflated to the year 2017) [52]. However, the vaccine helped prevent 25,134,220 pneumococcal cases, which was equivalent to 51.6 million USD in healthcare cost reduction and averted 920,000 DALY compared to getting no immunization [52]. Similarly, the economic evaluation conducted in Egypt over a 100-year period by implementing PCV13 resulted in a saving of 0.88 USD in direct costs and a rise of 0.0462 QALY [43]. This resulted in an ICER of 926 USD per QALY gain (costs were inflated to 2016), which was equal to half of the country's GDP per capita of 3,479 USD [43]. This makes PCV13 a more cost-effective option, regardless of whether the herd effect is taken into account or the vaccine schedule is considered [43,45,53]. Employing PCV13 on a global scale would have the greatest impact in Africa and Asia, which averted annually 8.68 million DALY (95% Cl: 3.99 million to 16.8 million) and 3.88 million DALYs (95%Cl: 1.75 million 6.78 million), respectively [56]. The global cost of launching the vaccine was 15.5 billion INTL dollars. However, implementing PCV13 in countries that are not yet implementing the PCV program would require an investment of one-third of the global cost, which was 4.42 million INTL dollar [56].
Studies in Egypt, the Philippines, and South Africa demonstrated that PCV13 contributed higher cost reduction and extended QALY compared to PCV10 [43,45,53]. Bhutan and India are classified as low-middle income countries, whereas Egypt is considered a developing country with a per capita income that exceeds the threshold for qualifying for Gavi financial support. Among the various presentations of pneumococcal disease, acute otitis media (AOM) emerges as the foremost contributor to direct costs, primarily attributable to expenses incurred from antibiotic prescriptions, owing to its elevated incidence. As elucidated in the investigation conducted by Pichichero et al. (2023) on the burden of AOM, regions such as those within South and Southeast Asia, characterized by their status as low- and middle-income countries (LMICs), harbor the highest prevalence of the predominant strains responsible for AOM, largely due to the constrained distribution PCVs [59]. Consequently, the adoption of PCV13 emerges as the most prudent strategy for LMICs, facilitating optimal allocation of resources and fostering improvements in quality of life
On the other hand, our findings indicated that the most recent licensed vaccines, PCV15 and PCV20, demonstrated dominance when compared to the widely utilized PCV13 vaccine. The greatest benefit, again, was seen in AOM cost reductions. In the USA, using PCV20 contributed a $19.2 billion decline in direct costs, which largely came from averted AOM cases (5.4 million of the total 5.91 million PD cases) in the period of 10 years compared to PCV13 [50]. Also, the benefit was observed in reducing Invasive Pneumococcal IPD cases. In the United States, 21% of IPD cases were linked to PCV13, while PCV15 and PCV20 unique serotypes contributed to 17% and 22%, respectively, in children under five years of age [60]. It is worth mentioning that the percentage of IPD cases associated with serotypes covered by PCV15 and PCV20 was significantly higher than that of PCV13, by 1.8 and 2.9 times, respectively [60].
Furthermore, with 100% of studies showing dominant ICERs, it is pertinent to highlight that switching from PCV13 to PCV20 would be more beneficial in terms of direct cost reduction and yield a bigger gain in QALYs compared to switching from PCV13 to PCV15. From a societal standpoint, the utilization of PCV20 is associated with noteworthy savings in indirect costs attributed to productivity loss in contrast to the employment of PCV15. Notably, in Canada, the adoption of PCV20 has facilitated savings exceeding 300 million CAD in indirect costs from a societal perspective, an amount equating to one-third of the averted direct costs, which amounted to 1.5 billion CAD (inflated to 2022 costs [46]. Similarly, in the USA, PCV20 use saved 8 billion USD in direct costs, with work loss reductions of 1.9 billion USD, nearly a quarter of the total (adjusted to 2022 costs) [50].
The PCV20's superior impact on cost reduction compared to PCV15 was mostly caused by the more comprehensive serotype protection, specifically 10A, 11A, and 15B, which are expected to raise the incidence rate of IPD [54]. The economic burden of serotypes protected by licensed vaccines was investigated in a study conducted in thirteen countries that had established National Immunization Programs (NIPs) [61]. These countries included the United Kingdom, Australia, Austria, Canada, Finland, France, Germany, Italy, Netherlands, New Zealand, South Korea, Spain, and Sweden [61]. According to this investigation, PCV20 serotypes were responsible for an estimated 46% to 77% of the pneumococcal infection. The nations presently adopting PCV13 in their NIPs (Australia, Canada, France, Germany, Italy, South Korea, Spain, and the United Kingdom) exhibited a disease burden ranging from 2% to 33% for PCV15-unique serotypes, whereas PCV20-unique serotypes contributed from 16% to 69% [61]. These findings highlight the greater burden on PCV20 serotypes, suggesting that transitioning to PCV20 could result in more substantial cost reductions compared to PCV15.
The indirect effect played a crucial role in determining the cost-effectiveness of the pneumococcal vaccine. The indirect effect or herd effect refers to the protection provided to the unvaccinated population when a specific community achieves a high enough rate of vaccination uptake. Incorporating herd immunity into the economic analysis led to a reduction in disease transmission, contributing to a decrease in the number of cases of pneumococcal illness and, hence, lower treatment costs such as healthcare visits and hospitalization charges. Consequently, the ICER decreased, showing that the vaccination program becomes more cost-effective (less expensive, more sufficient). This may explain why, in the scenario without herd effect, the ICERs of utilizing PCV13 were nearly 20 times higher in China than in the scenario with herd effect (79,304 CNY / QALY vs. 3,777 CNY/QALY; the cost was inflated to 2015) as compared to no vaccination [57]. An analogous trend was noted in nations when comparing the cost-effectiveness of PCV15 vs. PCV13 [48,49,58]. PCV15 was shown to be a dominant strategy compared to PCV13 in Japan and USA [48,49], as PCV15 contributed to more cost reduction and generated higher QALY gains. However, in the analysis conducted by Wilson et al. in UK [58]The failure to consider the indirect effect resulted in an increase in vaccine and treatment costs, which caused a significant rise in the overall cost.
The PSA findings on PCV13 revealed that all of the stimulations were concentrated in the Northeast region. This suggests that implementing PCV13 is more money-consuming and more effective than not vaccinating. In contrast, both PCV15 and PCV20 were located in the Southeast quadrant, indicating that they were more cost-saving and enhanced greater effectiveness than PCV13. Therefore, both PCV15 and PCV20 are dominant compared to PCV13.
This is the first systematic review that incorporated a cost-effectiveness analysis of PCV20 and PCV15. Given that the Advisory Committee on Immunization Practices (ACIP) suggested the use of two vaccinations with higher valency, PCV15 in 2022 and PCV20 in 2023, our findings can offer a comprehensive assessment of the costs associated with these vaccines. This information is crucial for determining which PCV should be included in the National Immunization Program (NIP). The majority of our selected evaluation covered the herd effect in 12 out of 16 cases, ensuring that the complete benefits of introducing PCV may be adequately documented. Our study has multiple limitations. Each country exhibited varying levels of vaccine coverage, serotype distribution, and incidence rates of pneumococcal illness. Consequently, the ICER outcome may not accurately reflect the overall situation. Furthermore, the absence of clinical data about PCV15 and PCV20 necessitated the reliance on assumptions when considering the indirect impact on other serotypes covered by these vaccines.
5. Conclusions
Both PCV13 and PCV10 were more cost-effective than no vaccination. In terms of higher-valency vaccines, PCV15 and PCV20 exhibited a notable decrease in direct costs and a greater increase in (QALY) compared to PCV13. Also, PCV20 was reported to be a dominant strategy compared to PCV15, regardless of vaccine schedule.
6. Future Directions
As demonstrated above, PCV vaccines have transformed the childhood immunization landscape, providing robust protection against a wide range of serious pneumococcal infections and reducing the disease's costs. In the future, we can expect continued advances in PCV vaccine technology, leading to even greater efficacy and durability. As vaccination coverage expands, the global burden of pneumococcal disease is expected to decline further. Furthermore, further research into personalized vaccines or combination vaccines promises to transform immunization strategies to the needs of individual children.
Author Contributions
Conceptualization, N.X.V. and T.T.B.; methodology, N.X.V.; software, U.M.B., H.T.H. and H.L.P.; validation, N.X.V. and T.T.B.; formal analysis, U.M.B, H.T.H. and H.L.P.; investigation, N.X.V.; resources, H.L.P., U.M.B., , H.T.H. and T.T.B.; data curation, H.L.P., U.M.B., T.T.B., and N.X.V.; writing—original draft preparation, H.L.P., U.M.B., H.T.H. and T.T.B.; writing—review and editing, N.X.V., H.L.P., U.M.B., and T.T.B.; visualization, N.X.V. and T.T.B.; supervision, N.X.V.; project administration, N.X.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data were collected from PubMed, Embase, and Cochrane databases.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ben-Shimol, S.; Regev-Yochay, G.; Givon-Lavi, N.; van der Beek, B.A.; Brosh-Nissimov, T.; Peretz, A.; Megged, O.; Dagan, R. Dynamics of Invasive Pneumococcal Disease in Israel in Children and Adults in the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) Era: A Nationwide Prospective Surveillance. Clin Infect Dis 2022, 74, 1639–1649. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, H.; Corcoran, M.; Mereckiene, J.; Cunney, R.; Cotter, S. Invasive pneumococcal surveillance to assess the potential benefits of extended spectrum conjugate vaccines (PCV15/PCV20) in older adults. Epidemiol Infect 2023, 151, e27. [Google Scholar] [CrossRef]
- Berical, A.C.; Harris, D.; Dela Cruz, C.S.; Possick, J.D. Pneumococcal Vaccination Strategies. An Update and Perspective. Ann Am Thorac Soc 2016, 13, 933–944. [Google Scholar] [CrossRef] [PubMed]
- Miellet, W.R.; Almeida, S.T.; Trzciński, K.; Sá-Leão, R. Streptococcus pneumoniae carriage studies in adults: Importance, challenges, and key issues to consider when using quantitative PCR-based approaches. Front Microbiol 2023, 14, 1122276. [Google Scholar] [CrossRef] [PubMed]
- Micoli, F.; Romano, M.R.; Carboni, F.; Adamo, R.; Berti, F. Strengths and weaknesses of pneumococcal conjugate vaccines. Glycoconj J 2023, 40, 135–148. [Google Scholar] [CrossRef]
- van Warmerdam, J.; Campigotto, A.; Bitnun, A.; MacDougall, G.; Kirby-Allen, M.; Papsin, B.; McGeer, A.; Allen, U.; Morris, S.K. Invasive Pneumococcal Disease in High-risk Children: A 10-Year Retrospective Study. Pediatr Infect Dis J 2023, 42, 74–81. [Google Scholar] [CrossRef]
- Ganaie, F.; Saad, J.S.; McGee, L.; van Tonder, A.J.; Bentley, S.D.; Lo, S.W.; Gladstone, R.A.; Turner, P.; Keenan, J.D.; Breiman, R.F.; et al. A New Pneumococcal Capsule Type, 10D, is the 100th Serotype and Has a Large cps Fragment from an Oral Streptococcus. mBio 2020, 11. [Google Scholar] [CrossRef]
- Pneumococcal Disease. Available online: https://www.cdc.gov/vaccines/pubs/pinkbook/pneumo.html (accessed on 30 March 2024).
- Pilishvili, T.; Bennett, N.M. Pneumococcal disease prevention among adults: Strategies for the use of pneumococcal vaccines. Vaccine 2015, 33 Suppl. S4, D60–D65. [Google Scholar] [CrossRef]
- Pneumococcal Conjugate Vaccine: What You Need to Know. Available online: https://www.cdc.gov/vaccines/hcp/vis/vis-statements/pcv.html (accessed on 30 March 2024).
- Pneumococcal conjugate vaccines in infants and children under 5 years of age: WHO position paper –February 2019. Available online: https://iris.who.int/handle/10665/310970 (accessed on 28 February 2024).
- Zarabi, N.; Aldvén, M.; Sjölander, S.; Fues Wahl, H.; Bencina, G.; Johnson, K.D.; Silfverdal, S.A. Clinical and economic burden of pneumococcal disease among adults in Sweden: A population-based register study. PLoS One 2023, 18, e0287581. [Google Scholar] [CrossRef]
- Asai, N.; Mikamo, H. Recent Topics of Pneumococcal Vaccination: Indication of Pneumococcal Vaccine for Individuals at a Risk of Pneumococcal Disease in Adults. Microorganisms 2021, 9. [Google Scholar] [CrossRef]
- Reslan, L.; Finianos, M.; Bitar, I.; Moumneh, M.B.; Araj, G.F.; Zaghlout, A.; Boutros, C.; Jisr, T.; Nabulsi, M.; Kara Yaccoub, G.; et al. The Emergence of Invasive Streptococcus pneumoniae Serotype 24F in Lebanon: Complete Genome Sequencing Reveals High Virulence and Antimicrobial Resistance Characteristics. Front Microbiol 2021, 12, 637813. [Google Scholar] [CrossRef] [PubMed]
- Pneumococcal Disease. Available online: https://www.who.int/teams/health-product-policy-and-standards/standards-and-specifications/vaccine-standardization/pneumococcal-disease (accessed on 4 April 2024).
- Hu, T.; Podmore, B.; Barnett, R.; Beier, D.; Galetzka, W.; Qizilbash, N.; Heckl, D.; Boellinger, T.; Weaver, J. Healthcare resource utilization and cost of pneumococcal disease in children in Germany, 2014-2019: a retrospective cohort study. Pneumonia (Nathan) 2023, 15, 7. [Google Scholar] [CrossRef] [PubMed]
- Pneumonia in children. Available online: https://www.who.int/news-room/fact-sheets/detail/pneumonia (accessed on 4 April 2024).
- Abebaw, T.A.; Aregay, W.K.; Ashami, M.T. Risk factors for childhood pneumonia at Adama Hospital Medical College, Adama, Ethiopia: a case-control study. Pneumonia (Nathan) 2022, 14, 9. [Google Scholar] [CrossRef]
- Hu, T.; Weiss, T.; Owusu-Edusei, K.; Petigara, T. Health and economic burden associated with 15-valent pneumococcal conjugate vaccine serotypes in children in the United States. J Med Econ 2020, 23, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Pecenka, C.; Usuf, E.; Hossain, I.; Sambou, S.; Vodicka, E.; Atherly, D.; Mackenzie, G. Pneumococcal conjugate vaccination in The Gambia: health impact, cost effectiveness and budget implications. BMJ Glob Health 2021, 6. [Google Scholar] [CrossRef] [PubMed]
- Edmondson-Jones, M.; Dibbern, T.; Hultberg, M.; Anell, B.; Medin, E.; Feng, Y.; Talarico, C. Impact of pneumococcal conjugate vaccines on healthcare utilization and direct costs for otitis media in children ≤2 years of age in two Swedish regions. Hum Vaccin Immunother 2022, 18, 1942712. [Google Scholar] [CrossRef] [PubMed]
- Ghia, C.J.; Horn, E.K.; Rambhad, G.; Perdrizet, J.; Chitale, R.; Wasserman, M.D. Estimating the Public Health and Economic Impact of Introducing the 13-Valent Pneumococcal Conjugate Vaccine or 10-Valent Pneumococcal Conjugate Vaccines into State Immunization Programs in India. Infect Dis Ther 2021, 10, 2271–2288. [Google Scholar] [CrossRef] [PubMed]
- Wasserman, M.; Chapman, R.; Lapidot, R.; Sutton, K.; Dillon-Murphy, D.; Patel, S.; Chilson, E.; Snow, V.; Farkouh, R.; Pelton, S. Twenty-Year Public Health Impact of 7- and 13-Valent Pneumococcal Conjugate Vaccines in US Children. Emerg Infect Dis 2021, 27, 1627–1636. [Google Scholar] [CrossRef]
- Manual for the Surveillance of Vaccine-Preventable Diseases. Available online: https://www.cdc.gov/vaccines/pubs/surv-manual/chpt11-pneumo.html#print (accessed on 25 February 2024).
- Du, Q.Q.; Shi, W.; Yu, D.; Yao, K.H. Epidemiology of non-vaccine serotypes of Streptococcus pneumoniae before and after universal administration of pneumococcal conjugate vaccines. Hum Vaccin Immunother 2021, 17, 5628–5637. [Google Scholar] [CrossRef]
- Adamu, A.L.; Karia, B.; Bello, M.M.; Jahun, M.G.; Gambo, S.; Ojal, J.; Scott, A.; Jemutai, J.; Adetifa, I.M. The cost of illness for childhood clinical pneumonia and invasive pneumococcal disease in Nigeria. BMJ Glob Health 2022, 7. [Google Scholar] [CrossRef] [PubMed]
- Amicizia, D.; Astengo, M.; Paganino, C.; Piazza, M.F.; Sticchi, C.; Orsi, A.; Varlese, F.; Hu, T.; Petigara, T.; Senese, F.; et al. Economic burden of pneumococcal disease in children in Liguria, Italy. Hum Vaccin Immunother 2022, 18, 2082205. [Google Scholar] [CrossRef] [PubMed]
- Vadlamudi, N.K.; Sadatsafavi, M.; Patrick, D.M.; Rose, C.; Hoang, L.; Marra, F. Healthcare Costs for Pneumococcal Disease in the Era of Infant Immunization With 13-Valent Pneumococcal Conjugate Vaccine: A Population-Based Study. Value Health 2022, 25, 1510–1519. [Google Scholar] [CrossRef]
- Hu, T.; Song, Y.; Done, N.; Mohanty, S.; Liu, Q.; Sarpong, E.M.; Lemus-Wirtz, E.; Signorovitch, J.; Weiss, T. Economic burden of acute otitis media, pneumonia, and invasive pneumococcal disease in children in the United States after the introduction of 13-valent pneumococcal conjugate vaccines during 2014-2018. BMC Health Serv Res 2023, 23, 398. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.; Podmore, B.; Cuñado Moral, A.; Matthews, I.; Sarpong, E.; Azpeitia, A.; Qizilbash, N. Healthcare resource utilisation and cost of pneumococcal disease from 2003 to 2019 in children ≤17 years in England. PLoS One 2023, 18, e0283084. [Google Scholar] [CrossRef] [PubMed]
- Nasreen, S.; Wang, J.; Sadarangani, M.; Kwong, J.C.; Quach, C.; Crowcroft, N.S.; Wilson, S.E.; McGeer, A.; Morris, S.K.; Kellner, J.D.; et al. Estimating population-based incidence of community-acquired pneumonia and acute otitis media in children and adults in Ontario and British Columbia using health administrative data, 2005-2018: a Canadian Immunisation Research Network (CIRN) study. BMJ Open Respir Res 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Ladhani, S.N.; Collins, S.; Djennad, A.; Sheppard, C.L.; Borrow, R.; Fry, N.K.; Andrews, N.J.; Miller, E.; Ramsay, M.E. Rapid increase in non-vaccine serotypes causing invasive pneumococcal disease in England and Wales, 2000-17: a prospective national observational cohort study. Lancet Infect Dis 2018, 18, 441–451. [Google Scholar] [CrossRef]
- Hu, T.; Weiss, T.; Bencina, G.; Owusu-Edusei, K.; Petigara, T. Health and economic burden of invasive pneumococcal disease associated with 15-valent pneumococcal conjugate vaccine serotypes in children across eight European countries. J Med Econ 2021, 24, 1098–1107. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Bang, H.; Zhao, H. Median-Based Incremental Cost-Effectiveness Ratio (ICER). J Stat Theory Pract 2012, 6, 428–442. [Google Scholar] [CrossRef]
- Cameron, D.; Ubels, J.; Norström, F. On what basis are medical cost-effectiveness thresholds set? Clashing opinions and an absence of data: a systematic review. Glob Health Action 2018, 11, 1447828. [Google Scholar] [CrossRef]
- Bertram, M.Y.; Lauer, J.A.; De Joncheere, K.; Edejer, T.; Hutubessy, R.; Kieny, M.P.; Hill, S.R. Cost-effectiveness thresholds: pros and cons. Bull World Health Organ 2016, 94, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Kazibwe, J.; Gheorghe, A.; Wilson, D.; Ruiz, F.; Chalkidou, K.; Chi, Y.L. The Use of Cost-Effectiveness Thresholds for Evaluating Health Interventions in Low- and Middle-Income Countries From 2015 to 2020: A Review. Value Health 2022, 25, 385–389. [Google Scholar] [CrossRef]
- Kunst, N.; Siu, A.; Drummond, M.; Grimm, S.E.; Grutters, J.; Husereau, D.; Koffijberg, H.; Rothery, C.; Wilson, E.C.F.; Heath, A. Consolidated Health Economic Evaluation Reporting Standards - Value of Information (CHEERS-VOI): Explanation and Elaboration. Value Health 2023, 26, 1461–1473. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Zhou, Y.; Li, Q.; Wang, G. Cost-Effectiveness of Newer Antidiabetic Drugs as Second-Line Treatment for Type 2 Diabetes: A Systematic Review. Adv Ther 2023, 40, 4216–4235. [Google Scholar] [CrossRef]
- Wang, C.; Su, L.; Mu, Q.; Gu, X.; Guo, X.; Wang, X. Cost-effectiveness analysis of domestic 13-valent pneumococcal conjugate vaccine for children under 5 years of age in mainland China. Hum Vaccin Immunother 2021, 17, 2241–2248. [Google Scholar] [CrossRef]
- Eythorsson, E.; Ásgeirsdóttir, T.L.; Erlendsdóttir, H.; Hrafnkelsson, B.; Kristinsson, K.G.; Haraldsson, Á. The impact and cost-effectiveness of introducing the 10-valent pneumococcal conjugate vaccine into the paediatric immunisation programme in Iceland-A population-based time series analysis. PLoS One 2021, 16, e0249497. [Google Scholar] [CrossRef] [PubMed]
- Sevilla, J.P.; Burnes, D.; El Saie, R.Z.; Haridy, H.; Wasserman, M.; Pugh, S.; Perdrizet, J.; Bloom, D. Cost-utility and cost-benefit analysis of pediatric PCV programs in Egypt. Hum Vaccin Immunother 2022, 18, 2114252. [Google Scholar] [CrossRef] [PubMed]
- Dorji, K.; Phuntsho, S.; Pempa; Kumluang, S.; Khuntha, S.; Kulpeng, W.; Rajbhandari, S.; Teerawattananon, Y. Towards the introduction of pneumococcal conjugate vaccines in Bhutan: A cost-utility analysis to determine the optimal policy option. Vaccine 2018, 36, 1757–1765. [Google Scholar] [CrossRef]
- Huang, L.; McDade, C.L.; Perdrizet, J.E.; Wilson, M.R.; Warren, S.A.; Nzenze, S.; Sewdas, R. Cost-Effectiveness Analysis of the South African Infant National Immunization Program for the Prevention of Pneumococcal Disease. Infect Dis Ther 2023, 12, 933–950. [Google Scholar] [CrossRef]
- Lytle, D.; Grajales Beltrán, A.G.; Perdrizet, J.; Ait Yahia, N.; Cane, A.; Yarnoff, B.; Chapman, R. Cost-effectiveness analysis of PCV20 to prevent pneumococcal disease in the Canadian pediatric population. Hum Vaccin Immunother 2023, 19, 2257426. [Google Scholar] [CrossRef]
- Dilokthornsakul, P.; Kengkla, K.; Saokaew, S.; Permsuwan, U.; Techasaensiri, C.; Chotpitayasunondh, T.; Chaiyakunapruk, N. An updated cost-effectiveness analysis of pneumococcal conjugate vaccine among children in Thailand. Vaccine 2019, 37, 4551–4560. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Hu, T.; Weaver, J.; Owusu-Edusei, K.; Elbasha, E. Cost-Effectiveness Analysis of Routine Use of 15-Valent Pneumococcal Conjugate Vaccine in the US Pediatric Population. Vaccines (Basel) 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Tajima, A.; Abe, M.; Weaver, J.; Huang, M. Cost-effectiveness analysis of pediatric immunization program with 15-valent pneumococcal conjugate vaccine in Japan. J Med Econ 2023, 26, 1034–1046. [Google Scholar] [CrossRef] [PubMed]
- Rozenbaum, M.H.; Huang, L.; Perdrizet, J.; Cane, A.; Arguedas, A.; Hayford, K.; Tort, M.J.; Chapman, R.; Dillon-Murphy, D.; Snow, V.; et al. Cost-effectiveness of 20-valent pneumococcal conjugate vaccine in US infants. Vaccine 2024, 42, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Ta, A.; Kühne, F.; Laurenz, M.; Eiff, C.v.; Warren, S.; Perdrizet, J. Cost-effectiveness of PCV20 to Prevent Pneumococcal Disease in the Pediatric Population - A German Societal Perspective Analysis. 2024. [CrossRef]
- Krishnamoorthy, Y.; Eliyas, S.K.; Nair, N.P.; Sakthivel, M.; Sarveswaran, G.; Chinnakali, P. Impact and cost effectiveness of pneumococcal conjugate vaccine in India. Vaccine 2019, 37, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Perdrizet, J.; Horn, E.K.; Nua, W.; Perez-Peralta, J.; Nailes, J.; Santos, J.; Ong-Lim, A. Cost-Effectiveness of the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) Versus Lower-Valent Alternatives in Filipino Infants. Infect Dis Ther 2021, 10, 2625–2642. [Google Scholar] [CrossRef]
- Warren, S.; Barmpouni, M.; Kossyvaki, V.; Gourzoulidis, G.; Perdrizet, J. Estimating the Clinical and Economic Impact of Switching from the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) to Higher-Valent Options in Greek Infants. Vaccines (Basel) 2023, 11. [Google Scholar] [CrossRef]
- Shen, K.; Wasserman, M.; Liu, D.; Yang, Y.H.; Yang, J.; Guzauskas, G.F.; Wang, B.C.M.; Hilton, B.; Farkouh, R. Estimating the cost-effectiveness of an infant 13-valent pneumococcal conjugate vaccine national immunization program in China. PLoS One 2018, 13, e0201245. [Google Scholar] [CrossRef]
- Chen, C.; Cervero Liceras, F.; Flasche, S.; Sidharta, S.; Yoong, J.; Sundaram, N.; Jit, M. Effect and cost-effectiveness of pneumococcal conjugate vaccination: a global modelling analysis. Lancet Glob Health 2019, 7, e58–e67. [Google Scholar] [CrossRef]
- Li, Y.; Wang, H.; Furnback, W.; Wang, B.C.M.; Zhu, S.; Dong, P. The Cost-Effectiveness of 13-Valent Pneumococcal Conjugate Vaccine in Seven Chinese Cities. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef]
- Wilson, M.; Lucas, A.; Mendes, D.; Vyse, A.; Mikudina, B.; Czudek, C.; Ellsbury, G.F.; Perdrizet, J. Estimating the Cost-Effectiveness of Switching to Higher-Valency Pediatric Pneumococcal Conjugate Vaccines in the United Kingdom. Vaccines (Basel) 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Pichichero, M.; Malley, R.; Kaur, R.; Zagursky, R.; Anderson, P. Acute otitis media pneumococcal disease burden and nasopharyngeal colonization in children due to serotypes included and not included in current and new pneumococcal conjugate vaccines. Expert Rev Vaccines 2023, 22, 118–138. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Wasserman, M.; Grant, L.; Farkouh, R.; Snow, V.; Arguedas, A.; Chilson, E.; Sato, R.; Perdrizet, J. Burden of pneumococcal disease due to serotypes covered by the 13-valent and new higher-valent pneumococcal conjugate vaccines in the United States. Vaccine 2022, 40, 4700–4708. [Google Scholar] [CrossRef]
- Wasserman, M.D.; Perdrizet, J.; Grant, L.; Hayford, K.; Singh, S.; Saharia, P.; Horn, E.K.; Farkouh, R.A. Clinical and Economic Burden of Pneumococcal Disease Due to Serotypes Contained in Current and Investigational Pneumococcal Conjugate Vaccines in Children Under Five Years of Age. Infect Dis Ther 2021, 10, 2701–2720. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of studies selection.
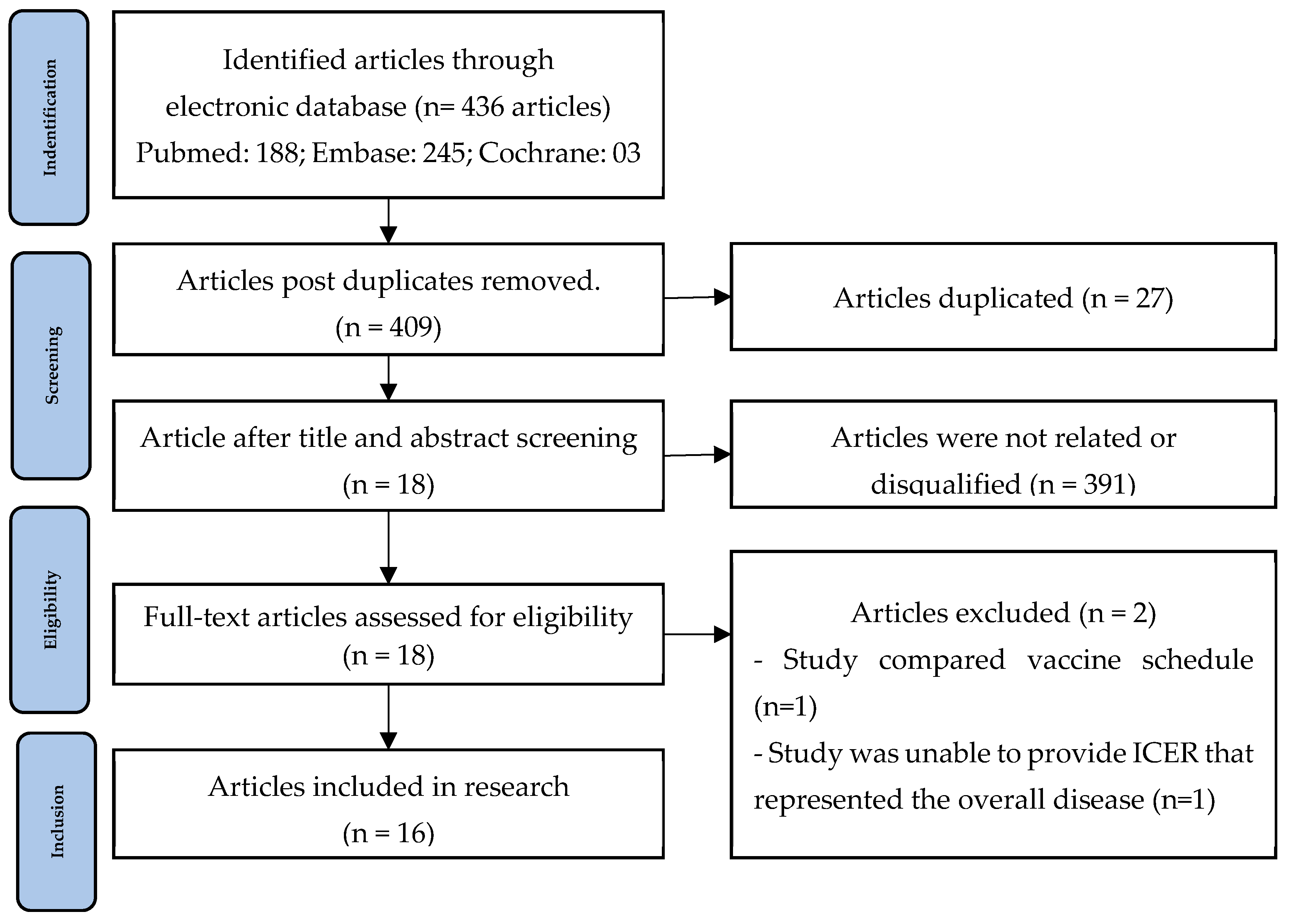

Table 1.
Characteristic of selected articles.
| No. | Author, Year, Country | Analysis type | Intervention | Clinical outcome | Model | Time horizon | Discount rate | Currency | Perspective | Vaccine coverage | Funding | Health outcome | SA |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Lytle et al., 2023, Canada [46] | CEA | PCV20 vs. PCV13 PCV20 vs. PCV15 |
IPD Pneumonia AOM |
Markov | 10 years | 1.50% | 2022 CAD | Payer Society |
84% | Pfizer | QALY | DSA, PSA |
| 2 | Sevilla et al., 2022, Egypt [43] | CBA CUA |
PCV13 vs. no vaccination PCV10 vs. no vaccination PCV13 vs. PCV13 |
IPD Pneumonia AOM |
Markov | 100 years | 3% | 2016 USD | Society Payer |
100% | Pfizer | RoR QALY, ICER |
DSA, PSA |
| 3 | Dilokthornsakul et al., 2019, Thailand [47] | CEA | PCV10 vs. no vaccination PCV10 vs. no vaccination |
IPD ACP All cause-AOM |
Markov | Lifetime | 3% | 2018 TBH | Society | - | Pfizer | QALY, ICER | PSA |
| 4 | Krishnamoorthy et al., 2019, India [52] | CEA | PCV13 vs. no vaccination | IPD Pneumonia AOM |
UNIVAC decision support | 10 years | 3% | 2017 USD | Government | 88% | - | DALY, ICER | PSA |
| 5 | Shen et al., 2018, China [55] | CEA | PCV13 vs. no vaccination | IPD Pneumonia AOM |
Decision analytic model | 1 year | 3% | 2015 CNY | Payer | 85% | Pfizer | QALY | DSA |
| 6 | Dorji et al., 2018, Bhutan [44] | CUA | PCV13 vs. no vaccination PCV10 vs. no vaccination PCV13 vs. PCV10 |
IPD Pneumonia AOM |
Markov | 100 years | 3% | 2017 USD | Government | 97% | WHO | QALY, ICER | DSA, PSA |
| 7 | Huang et al., 2023, USA [48] | CEA | PCV15 vs. PCV13 | IPD Pneumonia AOM |
Markov | Lifetime | 3% | 2021 USD | Society | 91.9% | Merck | QALY, LY, ICER | PSA, DSA |
| 8 | Tajima et al., 2023, Japan [49] | CEA | PCV15 vs. PCV13 | IPD NBPP, Pneumococcal AOM |
Markov | 10 years | 2% | 2015 USD | Payer Society |
100% | Merck | QALY, ICER | PSA, DSA |
| 9 | Li et al., 2021, China [57] | CEA | PCV13 vs. no vaccination | IPD Pneumonia AOM |
Decision analytic | 1 year | 5% | 2019 CNY | Payer | 70% | - | QALY, ICER | DSA |
| 10 | Wilson et al., 2022, UK [58] | CEA | PCV15 vs. PCV13 PCV20 vs. PCV13 PCV20 vs. PCV15 |
IPD Pneumonia AOM |
Economic model | 5 years | 3.5% | 2021 GBP | Payer | 91% | Pfizer | QALY, LY, ICER | DSA |
| 11 | Chen et al., 2019, 180 countries* [56] | CEA | PCV13 vs. no vaccination | IPD Pneumonia AOM |
Decision tree | 30 years | 3% | 2015 International dollars | Healthcare | - | WHO, Gavi, Bill & Melinda Gates Foundation | DALY, ICER | DSA, PSA |
| 12 | Perdrizet et al., 2021, Philipine [53] | CEA | PCV13 vs. PCV10-GSK | IPD Pneumonia AOM |
Decision analytic model | 10 years | 7% | 2020 PHP | Society | 90% | Pfizer | LY, QALY, ICER | - |
| 13 | Warren et al., 2023, Greece [54] | CEA | PCV20 vs. PCV15 | IPD Pneumonia AOM |
Decision-analytic mode | 10 years | 3.5% | 2023 EUR | Payer | 84.5% | Pfizer | LY, QALY, ICER | PSA |
| 14 | Huang et al., 2023, South Africa [45] | CUA | PCV13 vs. PCV10-GSK PCV13 vs. PCV10-SII |
IPD Pneumonia AOM |
Decision-analytic forecasting models | 10 years | 5% | 2022 R | Payer | 90.7% | Pfizer | LY, QALY, ICER | - |
| 15 | Rozenbaum et al., 2024, USA [50] | CEA | PCV20 vs. PCV13 PCV20 vs.PCV15 |
IPD ACP OM |
Markov | 10 years | 3% | 2022 USD | Healthcare Society |
83.5% | Pfizer | QALY, LYs | DSA, PSA |
| 16 | Ta et al., 2024, Germany [51] | CEA | PCV20 vs. PCV13 PCV20 vs.PCV15 |
IPD ACP All-cause AOM |
Markov | 10 years | 3% | 2020 EUR | Society | 76.8% | Pfizer | LY, QALY, ICER | PSA, DSA |
Abbreviation: CEA: Cost-Effectiveness Analysis; CUA: Cost-utility analysis; CBA: Cost Benefit Analysis; IPD: Invasive Pneumococcal Disease; AOM: Acute Otitis Media; NBPP: Non-Bacteremic Pneumococcal Pneumonia; ACP: All-Cause Pneumonia; OM: Otitis Media; WHO: World Health Organization, Gavi: The vaccine alliance, QALY: Quality-Adjusted-Life-Years; DALY: Disability-adjusted life years; LY: Life Years; ICERs: Incremental Cost-Effectiveness Ratios; RoR: Rate of Return; SA: sensitivity analysis DSA: Deterministic sensitivity analyses; PSA: Probabilistic sensitivity analysis. *: Africa, Asia, Europe, Latin America and the Caribbean, North America, and Oceania.
Table 2.
Quality assessment following CHEERS 2022 statement.
| No. | Item | Lytle et al., 2023 [46] | Sevilla et al., 2022 [43] | Dilokthornsaku et al., 2019 [47] | Krishnamoorthy et al., 2019 [52] | Shen et al., 2018 [55] | Dorji et al., 2018 [44] | Huang et al., 2023 [48] | Tajima et al., 2023 [49] | Li et al., 2021 [57] | Wilson et al., 2022 [58] | Chen et al., 2019 [56] | Perdrizet et al., 2021 [53] | Warren et al., 2023 [54] | Huang et al., 2023 [45] | Rozenbaum et al., 2024 [50] | Ta et al., 2024 [51] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Title | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 |
| 2 | Abstract | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 3 | Background and objective | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 4 | Health economic analysis plan | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 5 | Study population | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 6 | Setting and location | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 1 | 1 | 1 | 1 |
| 7 | Comparators | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 8 | Perspective | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 1 | 1 | 1 |
| 9 | Time horizon | 1 | 1 | 1 | 0.5 | 1 | 0.5 | 0.5 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 1 | 1 |
| 10 | Discount rate | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 1 | 0.5 | 0.5 | 1 | 1 |
| 11 | Selection of outcomes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 12 | Measurement of outcomes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 13 | Valuation of outcomes | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 14 | Measurement and valuation of resources and costs | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 15 | Currency, price date, and conversion | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 16 | Rationale and description of model | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 17 | Analytics and assumptions | 0.5 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 |
| 18 | Characterizing heterogeneity | 0.5 | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 0 | 1 | 1 | 1 |
| 19 | Characterizing distributional effect | 0.5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 | 0.5 |
| 20 | Characterizing uncertainty | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 |
| 21 | Approach to engagement with patients and others affected by the study | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 22 | Study parameters | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 23 | Summary of main results | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 24 | Effect of uncertainty | 1 | 1 | 1 | 1 | 0.5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 |
| 25 | Effect of engagement with patients and others affected by the study | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 26 | Study findings, limitations, generalizability, and current knowledge | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 27 | Source of funding | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 28 | Conflicts of interest | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Total score | 24.5 | 26 | 25.5 | 24.5 | 24.5 | 24 | 24 | 24.5 | 24.5 | 23.5 | 23.5 | 23.5 | 22.5 | 21.5 | 24 | 25 | |
| Conclusion | Good | Good | Good | Good | Good | Good | Good | Good | Good | Good | Good | Good | Good | Good | Good | Good | |
Table 3.
Incremental effect in lower-valent pneumococcal vaccine.
| Ref, country, currency | Schedule | Herd effect | Vaccination cost | Direct cost | Indirect cost | Total cost | LYs | Effectiveness | ICER | CE threshold | Cost-effective |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PCV13 vs. No vaccination | |||||||||||
| Sevilla et al., Egypt, 2016 USD [43] | 2+1 | Yes | 43.63 | -0.88 | - | 42.75 | - | 0.0462 QALY | 926 | GDP: 3,479 | Yes |
| Dorji et al., Bhutan, 2017 USD [44] | 2+1 | Yes | - | - | - | 0.03 | - | 0.0007 QALY | 40 | GDP: 2708 | Yes |
| Krishnamoorthy et al., India, 2017 USD [52] | 2+1 | No | 35,000,000 | -16,600,000 | - | -16,600,000 | - | 920,000 DALY | 467 | GDP: 1939.6 | Yes |
| Dilokthornsakul et al., Thailand, 2018 TBH [47] | 2+1 3+1 |
No | - - |
- - |
- - |
2571 3693 |
0.03 0.03 |
0.0349 QALY 0.0380 QALY |
73,674 97,269 |
WTP: 160,000 | Yes |
| Shen et al., China, 2015 CNY [55] | 3+1 | No Yes |
38,382,200,000 38,382,200,000 |
29,362,300,000 13,524,700,000 |
- - |
29,362,300,000 13,524,700,000 |
- - |
370,300 QALY 3,580,900 QALY |
79,304 3,777 |
GDP : 53,976 | Yes Yes |
| Li et al., China, 2019 CNY [57] | 3+1 | Yes | -323,757,862 | -28,646,835 | - | -28,646,835 | - | 14,880 QALY | Dominant | GDP: 157,300 | Yes |
| Chen et al., global, 2015 INTL dollar [56] | 2+1,3+1, 3+0 | Yes | 15,500,000,000 | 8,420,000,000 | -2,640,000,000 | 6,670,000,000 | - | 9,130,000 DALY | 724 | WTP: 1000 | Yes |
| PCV10 vs. No vaccination | |||||||||||
| Dilokthornsakul et al., Thailand, 2018 TBH [47] | 2+1 3+1 |
No | - - |
- - |
- - |
3881 5348 |
0.02 0.02 |
0.0228 QALY 0.0248 QALY |
170,437 215,948 |
WTP: 160,000 | No No |
| Sevilla et al., Egypt, 2016 USD [43] | 2+1 | Yes | 38.43 | 38.05 | - | 38.05 | - | 0.0192 QALY | 1,984.414 | GDP: 3,479 | Yes |
| Dorji et al.,Bhutan, 2017 USD [44] | 2+1 | Yes | - | - | - | 0.02 | - | 0.0006 QALY | 36 | GDP: 2708 | Yes |
| PCV13 vs. PCV10 | |||||||||||
| Sevilla et al., Egypt, 2016 USD [43] | 2+1 | Yes | 5.198 | 4.7 | - | 4.7 | - | 0.027 QALY | 173.98 | GDP: 3,479 | Yes |
| Perdrizet et al., Philipine , 2020 PHP [53] | 3+1 | No | 3,159,192,812 | -1,399,247,136 | -10,875,530,146 | - 12,274,777,282 | 156,061 | 153,349 QALY | Cost-saving | - | Yes |
| Huang et al., South Africa, 2022 R [45] | 2+1 | No | 587,690,427 | - 78,825,963 | - | - 78,825,963 | 4484 | 3191 QALY | Cost-saving | - | Yes |
* Abbreviation: INTL dollar: international dollar; WTP: Willingness-to-pay threshold; GDP: Gross Domestic Product; CE threshold: Cost-effectiveness threshold; LY: Life years; ICERs: Incremental Cost-Effectiveness Ratios; QALY: Quality-Adjusted-Life-Years; DALY: Disability-adjusted life years.
Table 4.
Incremental effect in higher-valent pneumococcal vaccine.
| Ref, country, currency | Schedule | Herd effect | Vaccine cost | Direct cost | Indirect cost | Total cost | LYs | Effectiveness | ICER | CE threshold | Cost-effective |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PCV15 vs. PCV13 | |||||||||||
| Huang et al., USA, 2021 USD [48] | 3+1 | Yes | 25,200 | -6,800,033,529 | -4,017,519,577 | -10,817,553,106 | 90,026 | 96,056 QALY | Dominant | - | Yes |
| Tajima et al., Japan, 2022 JPY [49] | 3+1 | Yes | 3,091 | -235,135,797 | -130,475,159 | -365,610,955 | 7 | 24 QALY | Dominant | - | Yes |
| Wilson et al., UK, 2021 GBP [58] | 1+1 vs. 1+1 2+1 vs. 1+1 |
No | 7,900,205 212,402,154 |
1,124,922 200,554,981 |
- | 1,124,922 200,554,981 |
262 475 |
361 QALY 640 QALY |
3112 313,229 |
WTP: 20,000 | Yes No |
| PCV20 vs. PCV13 | |||||||||||
| Lytle et al., Canada, 2022 CAD [46] | 2+1 | Yes | 82,002,815 | −3,226,480,346 | -656,062,710 | −3,882,543,056 | - | 47,056 QALY | Dominant | - | Yes |
| Wilson et al., UK, 2021 GBP [58] | 1+1 vs. 1+1 2+1 vs. 1+1 |
No | 38,303,366 215,602,573 |
-459,192,688 -403,126,911 |
- | -459,192,688 -403,126,911 |
23,165 28,818 |
28,096 QALY 35,009 QALY |
Dominant Dominant |
WTP: 20,000 | Yes Yes |
| Rozenbaum et al., USA, 2022 USD [50] | 3+1 | Yes | 2,338,463,867 | -19,189,701,809 | -3,726,859,511 | − 20,578,097,453 | 515,203 | 271,414 QALY | Dominant | - | Yes |
| Ta et al., Germany, 2022 EUR [51] | 3+1 vs. 2+1 | Yes | 525,362,283 | -2,035,127,528 | -358,136,083 | -2,393,263,611 | 563,014 | 904,854 QALY | Dominant | - | Yes |
| PCV20 vs. PCV15 | |||||||||||
| Lytle et al., Canada, 2022 CAD [46] | 2+1 | Yes | 82,083,788 | −1,484,267,884 | --307,853,576 | -1,792,121,460 | - | 21,881 QALY | Dominant | - | Yes |
| Wilson et al., UK, 2021 GBP [58] | 1+1 vs. 1+1 1+1 vs. 2+1 2+1 vs. 2+1 2+1 vs. 1+1 |
No | 30,403,161 -174,098,788 3,200,419 207,702,386 |
-460,317,610 -659,747,669 -603,681,892 -404,251,833 |
- | -460,317,610 -659,747,669 -603,681,892 -404,251,833 |
22,903 22,690 28,343 28,556 |
27,735 QALY 27,456 QALY 34,369 QALY 34,648 QALY |
Dominant Dominant Dominant Dominant |
WTP: 20,000 | Yes Yes Yes Yes |
| Warren et al., Greece, 2023 EUR [54] | 3+1 | No | −4,566,825 | -58,138,419 | - | -58,138,419 | 551 | 486 QALY | 110,000 |
- | Yes |
| Rozenbaum et al., USA, 2022 USD [50] | 3+1 | Yes | 2,437,771,654 | -8,003,928,578 | −1,898,767,496 | − 9,902,696,074 | 279,655 | 146,168 QALY | Dominant | - | Yes |
| Ta et al., Germany, 2022 EUR [51] | 3+1 vs. 2+1 | Yes | 522,747,819 | -1,343,839,409 | -284,161,097 | -1,628,000,506 | 400,731 | 646,235 QALY | Dominant | - | Yes |
Abbreviation: INTL dollar: international dollar; WTP: willingness-to-pay threshold; GDP: Gross Domestic Product; CE threshold: cost-effectiveness threshold; LY: life years; ICERs: Incremental Cost-Effectiveness Ratios; QALY: Quality-Adjusted Life Years; DALY: Disability-adjusted Life Years.
Table 5.
Sensitivity analysis in lower-valent pneumococcal vaccines.
| Ref | DSA | PSA | |
|---|---|---|---|
| The most impactful parameter on ICERs | Probability | Quadrant | |
| PCV13 vs. no vaccination | |||
| Sevilla et al. [43] | - Base-year incidence rates - Discount rate - PCV direct and indirect effects on inpatient pneumonia - Modeling horizon length |
- | - |
| Dilokthornsakul et al. [47] | - | 100% | Northeast |
| Krishnamoorthy et al. [52] | - | 100% | Northeast |
| Shen et al. [55] | Incidence rates of inpatient pneumonia in ages 0–4 | - | - |
| Dorji et al. [44] | - The variation in serotype coverage - Duration of vaccine protection - Excluding indirect vaccine effects (herd protection) - Discount rate |
- | - |
| Li et al. [57] | - Incidence of inpatient pneumonia 0-2y, 2-4y, 18-34y - Total direct cost - Discount rate |
- | - |
| Chen et al. [56] | - Disease incidence - Case fatality rate - Vaccine price |
100% | Northeast |
| PCV10 vs. no vaccination | |||
| Sevilla et al. [43] | - Base-year incidence rates - Discount rate - PCV direct and indirect effects on inpatient pneumonia - Modeling horizon length |
- | - |
Abbreviation: ICERs: Incremental Cost-Effectiveness Ratios; DSA: Deterministic sensitivity analyses; PSA: Probabilistic sensitivity analysis; PCV: pneumococcal conjugate vaccine.
Table 6.
Sensitivity analysis in higher-valent pneumococcal vaccines.
| Ref | DSA | PSA | ||
|---|---|---|---|---|
| Interest value | Most impactful parameter | Probability | Quadrant | |
| PCV20 vs. PCV13 | ||||
| Lytle et al. [46] | Cost | - Percentage of the indirect effect of PCV20 accrued - The steady-state indirect effects against hospitalized pneumonia - Age-specific serotype distribution of hospitalized pneumonia - The direct medical cost per hospitalized pneumonia episode |
100% | Southeast |
| QALY | - Utility decrement of simple OM - Utility decrement of hospitalized pneumonia - Utility decrement of non-hospitalized pneumonia |
|||
| Wilson et al. [58] | NMB | -Percentage PP cases that (≥65 years), - The hospitalized pneumonia incidence ( ≥65 years) - The direct costs for hospitalized pneumonia (≥65 years) |
- | - |
| Rozenbaum et al. [50] | Cost | - Vaccine serotype coverage - Indirect effect accrual for PCV20 - PCV20 and PCV13 cost per dose |
100% | Southeast |
| QALY | - Indirect effect accrual for PCV20 - Vaccine serotype coverage - Maximum indirect effect for all-cause hospitalized NBP |
|||
| Ta et al. [51] | Cost | -Maximum indirect effect against hospitalized pneumonia (PCV20) - Serotype distribution by age - Incidence of hospitalized pneumonia - Cost per episode of hospitalized pneumonia |
100% | Southeast |
| QALY | - Maximum indirect effects on hospitalized pneumonia (PCV20) - Serotype distribution by age - Baseline utilities - Hospitalized pneumonia incidence - CFR for hospitalized pneumonia |
|||
| PCV15 vs. PCV13 | ||||
| Huang et al. [48] | ICERs | - VEs against all-cause inpatient pneumonia - Vaccine coverage rate - Indirect effects - Incidence and fatality rates of bacteremic pneumonia in the elderly |
100% | Southeast |
| Tajima et al. [49] | ICERs | - PCV15 and PCV13 serotype-specific VE in inpatient pneumonia (including serotype-specific VE for V114 and PCV13) - Direct and indirect cost per episode - Baseline incidence rate - Percentage attributable to S. pneumoniae - Serotype distribution - QALY decrement |
98.7% | Southeast |
| PCV20 vs. PCV15 | ||||
| Warren et al. [54] | - | - | 100% | Southeast |
| Rozenbaum et al. [50] | Cost | - Indirect effect accrual for PCV20 - Cost per dose of PCV20 and PCV15 - Maximum indirect effect in hospitalized pneumonia for PCV20 - Vaccine serotype coverage |
100% | Southeast |
| QALY | - Indirect effect accrual for PCV20 - Maximum indirect effect in hospitalized pneumonia for PCV20 - Indirect effect accrual for PCV15 - Vaccine serotype coverage |
|||
| Ta et al. [51] | Cost | - Maximum indirect effect against hospitalized pneumonia (PCV20) - Serotype distribution by age - Incidence of hospitalized pneumonia - Cost per episode of hospitalized pneumonia |
98.4% | Southeast |
| QALY | - Maximum indirect effects on hospitalized pneumonia (PCV20) - Serotype distribution by age - Baseline utilities - Hospitalized pneumonia incidence - Indirect effect accrual for PCV20 |
|||
Abbreviation: ICERs: Incremental Cost-Effectiveness Ratios; DSA: Deterministic sensitivity analyses; PSA: Probabilistic sensitivity analysis; PCV: pneumococcal conjugate vaccine; ICERs: Incremental Cost-Effectiveness Ratios; QALY: Quality-Adjusted-Life-Years; OM: otitis media; PP: pneumococcal pneumonia; VE: vaccine effectiveness; CFR: case fatality rate, NMB: net monetary benefit, NBP: all-cause non-bacteremic pneumonia.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



