Submitted:
22 July 2024
Posted:
15 August 2024
You are already at the latest version
Abstract
Inflammation and insulin resistance are recognized as central features in the pathology of psoriasis, profoundly affecting the lives of those affected by this condition. The relationship between lifestyle choices and psoriasis is well-documented, highlighting the potential benefits of dietary modifications and physical activity in managing the condition during exacerbations. Furthermore, growing evidence emphasizes the significant impact of nutritional interventions on various skin disorders, particularly those characterized by inflammation and insulin dysregulation. Notably, the role of dietary fats is of particular interest, with their influence on inflammation and insulin resistance in psoriasis garnering increasing attention. Moreover, the association between excessive adiposity and heightened psoriatic severity underscores the importance of weight management strategies in disease management. This review explores the intricate relationship between specific dietary fats and inflammation in psoriasis, offering a comprehensive analysis of their implications for disease progression and management.
Keywords:
Dietary fatsInflammationdisease managementPsoriasisPsoriatic arthritisQoL (quality of Life)
- Psoriasis, extensively researched and prevalent as a recurrent chronic dermatological condition, presents formidable challenges in its management due to its profound impact on patients’ quality of life (QOL).
- Lifestyle factors play a crucial role in managing psoriasis effectively. For example, incorporating regular exercise and maintaining a balanced diet can help reduce the inflammatory symptoms associated with the condition.
- Dietary fats, particularly polyunsaturated fatty acids (PUFAs), play a crucial role in regulating epidermal homeostasis and inflammation.
- An adequate intake of PUFAs alongside conventional medical treatment contributes to the improvement of inflammatory symptoms associated with psoriasis.
- The abundance of saturated fatty acids is associated with obesity. Obesity worsens the psoriatic symptoms. Hence, it is suggested to restrict the intake of these fatty acids.
- This review encompasses the intricate disease mechanism of cutaneous inflammation in psoriasis along with clinical trials designed to assess the impact of dietary fats on psoriasis disease state.
1. Introduction
Psoriasis is an incurable, chronic, and immune-mediated inflammatory disorder [1,2,3]. Lesions, itching, and pain accompanying the red, inflamed skin are its common distinguishing features [1]. There is a wide range of clinical subtypes of psoriasis; among them, plaque psoriasis is the most prevalent [2,4]. It is characterized by rough, symmetrical, silvery patches and plaques [4], which are primarily inclined on the scalp, elbows, and knees [2,4]. Psoriasis is the most pervasive skin disease worldwide [2]. As per WHO data, the occurrence rate of psoriasis ranges between 0.99% and 11.4%. Regarding psoriasis epidemiology, 81% of the countries worldwide have not stated any data. It mostly prevails in adults than children, so it is more prevalent in countries with older populations [5]. Interestingly, psoriasis is unevenly distributed demographically [4,5] and is more prevalent in developed countries [5]. Psoriasis aggravating symptoms make life difficult for patients. Psoriasis has a huge influence on patient’s personal and social life. It also affects the emotional well-being of individuals. It has been observed that in some cases psoriatic patients are not able to perform their daily duties. This inability to carry out routine work leads to low self-esteem and depression [1,2,3].
Diet significantly influences skin disorders because an imbalanced diet disrupts skin equilibrium and causes cutaneous alterations [6]. Several experimental studies have established /identified the crucial function of nutrients in the progression and prevention of certain diseases [7]. Nutrients are chemical substances that we get from our food/diet and serve as means of energy, building and maintaining body structure [6]. Diet might contribute to significant biological effects on the skin as malnutrition and malabsorption are considered to lead to skin disease prevalence [7]. Therefore, dietary interventions are essential for people suffering from skin diseases [8]. A cohort study was conducted to ascertain the probable influence of dietary interventions on the skin in psoriatic patients [9]. This study demonstrated that psoriatic patients consumed less sugar while consuming more fruit and vegetables compared to the counter controls. The study also reported more consumption of whole grain fiber, dairy, and vitamins. These dietary interventions resulted in favorable skin responses in psoriasis [9].
Deficient intake of essential dietary fats and numerous vitamins is associated with cutaneous problems [10]. Supplementation with certain nutrients, including essential fatty acids resulted in the prevention of skin damage from ultraviolet rays. The nutrition intervention of fish oils to manage inflammatory skin disorders improved symptoms by regulating the lipid inflammatory mediators [11]. A cross-sectional study comprising 302 healthy individuals assessed the impact of certain nutrients (including fats) on the skin. The association of nutrient concentration in serum and diet with human skin was investigated. That study revealed a significant association between intake of dietary fats (saturated, mono-unsaturated, and total fats) with skin hydration. MUFAs (mono-unsaturated fatty acids) were found to specifically impact the skin pH. Hence, the study extrapolated the significant correlation of nutritional factors, including essential fats, with skin state [12].
In the current review, we have provided an overview of dietary fats and then summarized their significance and association with insulin resistance (IR) and inflammation in psoriasis. Followed by a comprehensive review of clinical trials conducted to investigate the impact of dietary fatty acids on psoriasis. The clinical trials were selected from PubMed (https://pubmed.ncbi.nlm.nih.gov/) against query words dietary fats and psoriasis, between the time frame of January 1990 to February 2023. The current review incorporates all clinical studies published during this time frame. A total of 15 studies (as given in Table 1 & Table 2) fulfilled the inclusion criteria for the current review.
2. Dietary Fats: Essential Components and Classification
Lipids comprise fatty or oily compounds that are crucial for modulating the homeostatic function of the body. They are recognized as organic soluble and polar solvents insoluble. Lipids encompass phospholipids, steroids, waxes, and triglycerides (fats & oils) [13]. Dietary fats are composed of three fatty acids and glycerol esters. These serve as a mode of energy and source of essential fatty acids to the body and, therefore, are indispensable for regulating normal functions of the living system. Fats are an important component of a healthy diet as they provide flavor and satiety. Moreover, some vitamins (A, D, E, K) require fats to be absorbed in the body. Dietary fats are mainly divided into saturated and unsaturated compounds (as shown in Figure 1) depending on the presence of double bonds. Unsaturated fats are distinguished by one or more double bonds, while saturated have none [14].
2.1. Classification of Saturated Fatty Acids
Saturated fatty acids (SFAs) are further classified as short and medium-chain SFAs and longer-chain SFAs. SFAs have relatively shorter chains of carbons (4 to 12) and are obtained from palm, coconut oils, and milk. Whereas, long-chain SFAs are composed of more than 14 carbons, and some vegetable oils, meat, and butterfat are their predominant sources [14].
2.2. Classification of Unsaturated Fatty Acids
Unsaturated fatty acids are grouped as MUFAs (monounsaturated fatty acids) and PUFAs (polyunsaturated fatty acids) based on the number of double bonds. MUFAs have one double bond per molecule (oleic acid), while PUFAs are characterized by more than one double bond per molecule (linoleic acid). Linoleic acid, having 18 carbons and 2 double bonds, is an essential nutrient, which means the body needs it for normal functioning but cannot synthesize it. Oils obtained from corn, safflower, and soybean seeds are the sources of linoleic acid [14]. In the omega classification system of fatty acids, the first occurrence of a double bond is noted while counting carbons from the methyl end of fatty acids. For instance, oleic acid is grouped under -9 fatty acids (1st double bond at carbon number 9 while counting from methyl end) [14]. Olive oil serves as the chief source of MUFAs as it is highly enriched (70-80%) in oleic acid [15]. Correspondingly PUFAs are also classified in -3 and -6 groups [14]. -linolenic acid (ALA), having 18 carbons and 3 double bonds, is a parent member of -3 group. Other key members of this group are EPA(eicosapentaenoic acid) and DHA (docosahexaenoic acid), having 20 & 22 carbons and 5 & 6 double bonds, respectively. Both of these are long-chain derivates of -linolenic acid [14,16]. Fish and fish oils are known for numerous health benefits and are common sources of -3 PUFAs, providing EPA and DHA [17]. Similarly, Linoleic acid (LA), having 18 carbons and 2 double bonds, is a parent member of -6 group [14,16]. Its long-chain derivatives are Arachidonic acid (AA) and -linolenic acid (GLA) having 20 & 18 carbons and 4 & 3 double bonds, respectively [16].
2.3. Fatty Acids and Their Significance in Dermatological Physiology
Skin is a multifaceted organ that performs various vital functions within the body. Primarily, it acts as a protective barrier against external factors, helps in regulating body temperature, and contributes to metabolic processes and fluid balance [18]. The anatomy of the skin comprises distinct layers, specialized appendages such as hair follicles and glands, as well as immunological components, all working together to maintain skin health and function [19]. Within the skin’s structure, the epidermis stands out as a crucial layer composed of different elements, including fatty acids, lipids, and ceramides, among others [20]. Lipids, including fatty acids, play a pivotal role in maintaining the health of the epidermis, the outermost layer of the skin. They contribute significantly to the formation of an effective barrier against water loss, protect against radiation and harmful chemicals, and inhibit microbial entry [21]. The unique composition of lipids within the epidermal barrier is crucial for its proper function [22]. Moreover, lipids possess inflammatory characteristics and can act as signaling molecules that influence various skin conditions [23]. They participate in immune regulation, antimicrobial activity, and the modulation of the skin’s response to environmental stress [24]. Recent studies have identified specific lipid molecules that regulate epidermal homeostasis, offering exciting opportunities for developing therapeutic interventions for various skin conditions, including topical treatments or nutritional supplementation [25]. Fatty acids are vital for maintaining the integrity of the epidermal barrier and play key roles in cellular development and communication within the skin [26]. The fatty acid content of the diet significantly impacts skin health and is implicated in various skin diseases such as atopic dermatitis, psoriasis, and acne [27]. Various skin cell types, including keratinocytes, melanocytes, Langerhans cells, dermal fibroblasts, leukocytes, and macrophages, are involved in the production of oxygenated metabolites of fatty acids [28]. These metabolites, such as eicosanoids, octadecanoids, and docosanoids, are crucial for skin physiology, including maintaining the integrity of the epidermal barrier, cellular development, and communication [29]. Polyunsaturated fatty acids (PUFAs) like linoleic acid (LA) and arachidonic acid (AA) undergo metabolism through enzymatic pathways like cyclooxygenase and lipoxygenase, leading to the production of various metabolites such as prostaglandins and hydroxyeicosatetraenoic acid (HETE) [30]. These metabolites play diverse roles in skin physiological processes, and inflammation regulation, and exert both anti-inflammatory and antiproliferative effects, highlighting the critical role of fatty acid metabolism in maintaining skin homeostasis and the function [31,32]. Understanding their roles in skin biology is essential for developing effective treatments for dermatological conditions and diseases.
3. The Interplay of Obesity, Insulin Resistance, and Inflammation in Psoriasis Pathogenesis
Obesity is defined as the amassing of unusual and surplus fat in the living body to the extent that it becomes harmful to the health [33]. In the state of obesity, the fat is stored in the body’s subcutaneous and abdominal adipose tissue [34]. Obesity is significantly associated with an elevated risk of developing psoriasis and may exacerbate the disease’s symptoms [35,36,37]. The extremity of psoriasis symptoms is proportional to the severity of the obesity [37]. Obesity might act as a promoting factor in the advancement of psoriasis through pro-inflammatory pathways [37]. Moreover, the excess body fat might contribute to hampering medical treatment [35], as poor response to the therapy is observed in obese patients [37]. Hence, weight loss in obese psoriasis patients is presumed to ameliorate the characteristic disease symptoms [35].
Obesity is linked with an elevated risk of insulin resistance (IR) in the body. Raised amounts of non-esterified fatty acids, glycerol, certain hormones, and pro-inflammatory cytokines are noticed in obesity [38]. The augmented amount of these observed features is involved in the progression of IR [38]. The term IR is defined as the resistance exhibited by the body towards insulin on glucose intake, metabolism, and storage [39]. IR is also regarded as a significant contributing mechanism in the manifestation of psoriasis [36]. [40] experimentally demonstrated that IR is responsible for the characteristic epidermal symptoms in psoriasis.
Obesity is also associated with inflammation in the body [33,34]. The term inflammation refers to well-organized sequential events engendered to sustain homeostasis in tissue or organs of the body [33]. It is caused as a protective response by the injured or destructive body tissue/organ to deal with the injurious agent and injured tissue. Further, inflammation is considered a substantial risk factor in the progression of both cardiovascular and non-cardiovascular diseases in humans. Psoriasis is one of the non-cardiovascular diseases [33]. In consistent with the discussion, we can propose that weight loss in obese psoriasis patients improves disease symptoms. Obesity is suggestively associated with IR and inflammation, both of which contribute to the development of psoriasis. Dietary interventions play a significant role in obesity. Therefore, a healthy diet is presumed to have a positive impact on obesity [34].
4. How Dietary Fats Might Impact Inflammation in Psoriasis
4.1. Immunological Mechanisms Underlying Psoriasis Pathogenesis
Psoriasis is one of the known immune-mediated inflammatory diseases [41]. The role of innate and adaptive immune systems in psoriasis pathogenesis is unquestionable. The chiefly involved immune system components are T-cell signaling and dendritic cells (DCs) [27]. DCs, the proficient antigen-presenting cells (APCs), play a crucial part in the early development of psoriasis. The stimulation of these cells is not well understood. It is suggested that they might be activated in response to the production of antimicrobial peptides (AMPs). AMPs are observed to be upregulated in psoriatic lesions, and they are generated by keratinocytes in response to injury [42]. S100 proteins, cathelicidin, and defensins are some of the known AMPs that are crucially involved in the progression of psoriasis. AMPs are produced as an initial response to invading pathogens. In psoriasis, they are involved in the dysregulation of the immune system, which ultimately causes the increased generation of pro-inflammatory mediators [43].
Psoriasis-specific inflammation is triggered by the activation of cytokines. The overexpression of cytokines is observed in psoriasis lesions. The triggering of cytokines elevates epidermal keratinocyte proliferation resulting in the typical scales/lesions in psoriasis [41]. These cytokines chiefly include tumor necrosis factor (TNF), type I Interferons (IFNs) and Interleukin (IL)-17. They function to hyperactive the immune system. TNF is primarily generated from epithelial and immune cells. TNF triggers both vascular endothelial and immune cells to cause inflammation. Further, by regulating apoptosis TNF also contributes to lymphoid tissue progression. Overexpression of TNFs are observed in various autoimmune diseases, including psoriasis, in areas of inflammation. Particularly in psoriatic scales/lesions, upregulation of TNF, (tumor necrosis factor receptor 1) TNFR1, and (tumor necrosis factor receptor 2) TNFR2 is observed. The presence of TNFR1 on keratinocytes makes them sensitive to TNF. Inflammatory and immune responses by keratinocytes are observed upon activation with TNF(as TNF binds to its receptor present on keratinocytes). Chemokines that induct skin-specific memory T cells, neutrophils, and macrophages, are also produced by stimulated keratinocytes [44]. IFNs are responsible for antiviral activity to combat viral infections in the body. Fascinatingly, they are also associated with the progression of autoimmune and inflammatory diseases, including psoriasis. Type 1 INFs (IFN- and IFN-) mainly function by facilitating the initial/early-stage lesions, however, the absence of these is reported in chronic psoriasis lesions [41,44]. Skin injuries might initiate psoriasis lesions. Type 1 IFNs are proposed to be critically involved in the instigation of psoriasis lesions in case of injury [45]. Furthermore, the increased level of INF- is observed in psoriasis lesions and is conclusively associated with the disease worsening [41]. Cytokines belonging to the IL-1 family are regarded as pro-inflammatory, and differential expressions of these are observed in lesional and non-lesional psoriasis skin concerning counter controls [41]. T-helper 17 (Th17) cells that play a pivotal role in the development of psoriasis are characterized by IL-23/IL-17 axis [44].
The pathogenic role of Th17 cells is evident in inflammatory and autoimmune disorders. In psoriasis, these cells produce cytokines (IL-17A, IL-17F, IL-21, IL-22, and IL-26) that are important in disease development. During skin trauma (injury, certain infections, or medications), self-nucleotides and AMPs are secreted from keratinocytes. These AMPs and self-nucleotides form complexes that are recognized by plasmacytoid dendritic cells (pDCs). The stimulated pDCs then expedite the activation of CD8+ T cells. These activated cells travel to the epidermis and generate cytokines that eventually result in increased skin proliferation and inflammation. Fascinatingly, pDC might also produce IFNs, which are responsible for the production of additional cytokines (TNF, IL-12, and IL-23) by instigating myeloid dendritic cells (mDCs). These cytokines possibly stimulate TH1 and TH17 cells. The activated Th17 cells produce IL-17, potentially elevating epidermal proliferation and IL-23 secretion by keratinocytes, thus sustaining chronic inflammation in psoriasis [46].
4.2. Omega-3 and Omega-6 Polyunsaturated Fatty Acids in Inflammation
Under normal circumstances, inflammation is an important attribute of the host defense mechanism and is also involved in tissue healing. Still, dysregulation in inflammation might lead to uncurbed tissue damage and certain diseases [47]. AA acts as a precursor of numerous significant pro-inflammatory regulators like prostaglandins, leukotrienes and associated complexes [47,48]. Higher intake of -3 PUFAs is related to the fractional replacement of AA with EPA and DHA in cell membranes. These -3 fatty acids induced reduced amount of AA leads to an anti-inflammatory effect [48]. Generally, the increased dietary intake of -6 PUFAs is associated with elevated inflammation. Nevertheless, the experimental studies designed to elucidate the impact of increased intake of -6 fatty acids (AA or its long-chain derivative LA) on healthy human beings revealed that levels of numerous inflammatory markers do not expedite with -6 fatty acid intake. Additionally, epidemiological studies advocated that AA or LA might aid in decreased inflammation. Meanwhile, there exists conflicting evidence supporting the potential inhibition of -3 PUFA-induced anti-inflammatory activities by -6 PUFAs. Hence, in inflammation, the interplay between -3 and -6 PUFAs is intricate and remains elusive [47].
4.3. Impact of Fatty Acid Levels on Psoriasis Severity and Comorbidities
In an interesting cohort study [49] investigated the correlation of obesity with psoriasis and reported free fatty acid serum level as the substantial parameter that exacerbates the severity of the disease. Further, they evaluated the impact of a high-fat diet (rich in SFAs with low levels of PUFAs) in a psoriasis mouse model and reported that elevated levels of FFAs in both lean and obese mice profoundly contribute to the aggravation of early inflammation associated with psoriasis. High-fat diet results in increased levels of SFAs. SFAs are responsible for the escalated inflammatory responses to pro-inflammatory stimuli, which eventually amplifies keratinocyte activation. Thus, restricting the intake of saturated fatty acids is suggested as it will ameliorate the symptoms of psoriasis.
Metabolic disturbances, type-2 diabetes, obesity, cardio-metabolic disorders, and hypertension are common extracutaneous disease manifestations associated with psoriasis. Fatty acids could be regarded as a link between psoriasis and these comorbidities. To unravel this potential link, [50] investigated fatty acids serum concentrations obtained from 85 plaque psoriasis patients against 32 controls. The patients were analyzed for characteristics like lipid profile, inflammatory markers, PASI, BMI, and reported disease-related comorbidity. As anticipated, an aberrant fatty acids profile was observed in psoriasis patients compared to healthy individuals. Interestingly, this abnormal fatty acid profile was reported in both obese and non-obese patients. The psoriasis patients with hypertension comorbidity exhibited higher levels of SFAs. Moreover, the psoriasis patients having obesity and hypertension showed an increased SFA/UFA ratio. This ratio could be regarded as a cardio-metabolic threat marker in psoriasis patients. Furthermore, the saturated and unsaturated fatty acids ratio was observed to expand with disease time span in both the non-obese and obese patients. The study extrapolated that an aberrant fatty acids profile might contribute to psoriatic-associated comorbidities by exhibiting metabolic disturbances.
4.4. The Therapeutic Role of Polyunsaturated Fatty Acids in Psoriasis
These fats are considered beneficial, as they help manage IR, and ease inflammation [17]. A cohort study suggested dietary interventions by replacing saturated fats with unsaturated fats, particularly PUFAs, to reduce the risk of heart diseases [51]. In literature, a comparatively lower incidence rate of inflammatory skin diseases, including psoriasis, is reported in fish-eating individuals than in meat-eating populations [52]. The PUFAs belonging to -3 and -9 groups are significant in treating various cutaneous disorders, including psoriasis, as these PUFAs are suggested as adjunctive treatments based on their potential therapeutic effects [16]. Stratum corneum is regarded as a safeguarding barrier of the skin as it protects against the external environment. This outermost layer of the epidermis helps in modulating hydration and water retention, thus protecting against skin cracking. This layer is composed of anucleated cells called as corneocytes. These cells are keratinocytes that have achieved the last level of differentiation. Corneocytes appear to be flat in a lipid-rich extracellular matrix. Atypical parakeratosis, characterized by insufficient keratinocyte maturation and withholding of nuclei in the stratum corneum, has been observed in patients suffering from numerous skin diseases, including psoriasis. Additionally, scaling or flaking of skin caused by unusual parakeratosis is a characteristic of diseases related to depletion in stratum corneum [53]. The -3 and -6 fatty acids play a role in the differentiation and maturation of stratum corneum cells, thus also aiding in the regulation of the stratum corneum permeability barrier. Moreover, these PUFAs are also crucial in restricting pro-inflammatory eicosanoids, pro-inflammatory cytokines, and lipoxygenase. These fatty acids also aid in building sunburn tolerance and wound healing. Further, these PUFAs also assist in the eradication of malignant cells by stimulating apoptosis [16].
4.4.1. Essential Fatty Acids: Implications for Skin Health
Essential fatty acids (EFA) are not produced by the body, yet they are essential for biological processes going out in the body to maintain health. Therefore, EFAs must be provided with food. EFAs include polyunsaturated fatty acids (PUFA) [54]. There are only two essential fatty acids for humans, alpha-linolenic acid and linoleic acid, and these fatty acids act as parent fats to the -3 and -6 families of EFA, respectively [16]. Hence, there exist two families of EFA, which are -3 and -6 [54]. Lack of EFA might cause cutaneous disorders. Anomalies in EFA metabolism might play a critical role in skin diseases like psoriasis, acne, and eczema [55]. EFAs (linoleic acid, -6 fatty acid) play a vital role in the maintenance of epidermis by preventing trans-epidermal water loss. Moreover, EFAs (arachidonic acid metabolites) act as chief inflammatory agents of the skin. Their role in inflammatory responses indicates their potential involvement in progression of the skin diseases like atopic dermatitis and psoriasis. Thus, dietetic and pharmacological regulation of arachidonic acid metabolism is crucial in the management of inflammatory skin diseases [56].
[50] unraveled the serum fatty acid patterns in psoriasis patients to reveal the possible relation of fatty acids with disease severity and associated comorbidities. The study revealed disturbances in fatty acid profiles in all psoriasis patients. In addition, in non-obese patients, a significant link between lower concentrations of DHA, -3 PUFA (p-values 0.044 and 0.048, respectively) and high levels of MUFAs (p-value = 0.024) with PASI was revealed. Overall, these outcomes suggest that lower observed levels of PUFAs could stimulate a pro-inflammatory state and cause systemic inflammation in psoriasis.
5. Clinical Trials That Assessed the Impact of Fatty Acids in Psoriasis and Psoriatic Arthritis
5.1. Psoriasis
Researchers are conducting experimental studies to evaluate the probable association of fatty acids with psoriasis and its associated symptoms. Clinical trials that assessed the impact of fatty acids in psoriasis are given in Table 1 and are described below.
Fish oil has been opted in various studies to evaluate its cosmetic, anti-inflammatory, and therapeutic actions on the skin. Eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA), which are the -3 polyunsaturated fatty acids (PUFAs), are the main active ingredients in fish oil that are associated with regulating skin homeostasis [57]. Moreover, its intake resulted in favorable outcomes in treating various skin disorders, including psoriasis and cancer [57]. Because of these reasons, fish oil is mainly selected in clinical trials to evaluate its potential positive effect on psoriasis. [58] explored the impact of oily fish and white fish consumption in 18 patients suffering from plaque psoriasis. Patients were recommended to take 170 g of white fish daily for 4 weeks. Afterward, the patients were randomly selected to go with the same diet or to replace with fish oil for 6 weeks. After that, the white and oily fish diets were swapped for 6 weeks. This study reported that oily fish intake resulted in better clinical outcomes with increased plasma eicosapentaenoic acid levels, therefore, it recommended fish oil intake as a supplement in psoriasis. The suggested fish types are herring, kipper, mackerel, pilchard, salmon, and sardine. In another interesting experimental design, the comparative analysis of the prospective beneficial impacts of fish and corn oils on the clinical indications associated with psoriasis was studied. [59] examined the influence of long-chain -3 fatty acids in 145 psoriatic patients in a 4-month double-blind trial. The experiment was designed to give 6 g of fish oil (very long-chain -3 fatty acids) daily or an isoenergetic quantity of corn oil, and patients were counseled to restrict their saturated fatty acid diet. Afterward, the 48-hour dietary recall was performed, followed by a serum phospholipid examination of patients. Interestingly, the study revealed no significant alteration in the Psoriasis Area and Severity Index (PASI) score in both groups. However, in the corn oil group, the amelioration of clinical symptoms was observed by lessened desquamation, scaling, and redness of the skin. In the fish oil group, a significantly reduced scaling and cellular infiltration was reported. The study extrapolated that no notable transformation was detected in clinical symptoms of psoriasis among fish and corn oil groups. Moreover, the improvement in clinical symptoms in the fish oil group is not associated with an elevated serum level of very long-chain -3 fatty acids. However, in the corn oil group, improved clinical symptoms are correlated with raised eicosapentaenoic acid and total -3 fatty acids. [60] investigated the effectiveness of intravenously given fish oil (-3 fatty acid based lipid) emulsion on plaque psoriasis patients based on a randomized and double-blinded study design. Eighty-three plaque psoriasis hospitalized patients from 8 European centers exhibiting a PASI score of 15 (at least), were involved in this study for a period of 2 weeks. Fourty-three patients were randomly selected to intravenously get the dose of lipid emulsion based on -3 fatty acid (Omegavenous; 200 ml with 4.2 gm of both EPA and docosahexaenoic acid (DHA)) per day. Per day, a typical lipid emulsion based on -6 fatty acid (Lipovenous; EPA+DHA < 0.1 gm/100 ml) was administered to forty randomly selected patients. The therapy impact was then inspected and followed up based on PASI scores and self-assessments reported by the patients. In -3 and -6 groups, the PASI scores were significantly (p = 0.048) reduced by 11.2 +/- 9.8 and 7.5 +/- 8.8, respectively. Further, comparatively improved symptoms were observed in -3 group based on reduced skin scaling, erythema, and infiltration. No critical side-effects were seen in both groups. This study extrapolated that -3 intravenous injection is efficacious for alleviating chronic plaque psoriasis symptoms, and this positive effect of the therapy might correlate with alterations in inflammatory eicosanoid production.
PUFAs possess conclusive therapeutic outcomes in several autoimmune and chronic inflammatory diseases as these fatty acids notably function in the alterations of the lipid composition of the cell membrane, cell metabolism & signaling, and gene expression. Hence, the probable beneficial effect of PUFAs has been investigated in various inflammatory disorders, including psoriasis [61]. [62] examined the influence of polyunsaturated ethyl ester lipids (Angiosan) in psoriasis and psoriasis arthritis. A total of 80 psoriasis patients were enrolled in this trial, and 34 of these were also suffering from psoriasis arthritis. The patients were given eicosapentaenoic acid ethyl ester 1122 mg and docosahexaenoic acid ethyl ester 756 mg per day. PASI score was taken before, after 6 and 8 months of treatment. Remarkably, the before-treatment PASI score of 3.56 reduced to 1.98 after 4 months and further significantly scaled down to 1.24 when calculated after 6 months of treatment (P < 0.001). Overall, favorable clinical outcomes were achieved from the trial. Participants reported reduced skin pruritus (itchy skin), scaling, and plaques. Seven patients were cured completely; 14 exhibited more than 75% recovery, while 14 showed unsatisfactory outcomes. Most of the psoriasis arthritis patients reported alleviated symptoms with reduced joint pain. Hence, the study deduced that polyunsaturated ethyl ester lipids might be taken as potent adjuvant in both psoriasis and psoriasis arthritis treatment. In another study, [63] explored the influence of -3 PUFAs in patients suffering from psoriasis. In a randomized, double-blind, and placebo-controlled study design, 20 patients were enrolled who were hospitalized for acute guttate psoriasis. These patients were grouped to receive infusions with -3 lipid or the conventional -6 lipid emulsions for 10 days. Subjective scoring of clinical indicators provided by the patients and the scoring of disease symptoms like erythema, desquamation, and infiltration were utilized to measure the disease severity. These scores were recorded at baseline and within 10 days. Ordinary mitigations in disease symptoms were observed in patients who received the -6 lipid regimen, as indicated by the differences in scores (16-25%). Yet, all patients in the -3 lipid emulsion group exhibited notable amelioration in clinical manifestations by showing significant (p < 0.05) differences in all scores (45-76%). Response to both these regimens was different. In the case -3 regimen, more than a 10-fold upsurge of neutrophil EPA-derived 5-1ipoxygenase product formation was reported, while this trend was not observed in the -6 group. On the other hand, the production of neutrophil platelet-activating factor (PAF) was elevated in the case of the -6 regimen and declined in the -3 regimen. The study concluded that -3 lipids infusions resulted in favorable clinical outcomes on inflammatory cutaneous scales in guttate psoriasis by regulating the eicosanoid metabolism.
Long-chain -3 fatty acids are observed to facilitate favorable clinical outcomes in some chronic inflammatory diseases, like inflammatory bowel disease (IBS), rheumatoid arthritis, and asthma by expediting anti-inflammatory actions [64]. In a clinical trial, [65] examined the influence of food supplementation of long-chain -3 PUFAs on the propagation of T-cells, secretion of ILs (IL-2 & IL-6) and TNF from T-cells, and expression of interleukin-2 receptor alpha-chain (CD25 ) in psoriasis and atopic dermatitis. In this study, 19 psoriasis $ 21 atopic dermatitis patients, and 20 healthy individuals were enrolled. The severity of the diseases in patients was classified as moderate to severe based on PASI in psoriasis, and Hanifin and Rajka score in atopic dermatitis. Twenty-one patients were administered 6 g of EPA and DHA in the form of gelatin capsules per day with their routine diet for 4 months. Whereas 19 patients in the control group were given 6 g of corn oil per day in gelatin capsules for 4 months. Psoriasis patients exhibited a relatively higher IL-6 generation for atopic dermatitis patients. However, a similar trend was observed in IL-2 and TNF secretion, T-cell propagation, and CD25 expression in both disease sub-groups. After the trial, patients in -3 fatty acids group displayed a significant (p < 0.05) decline in CD25-positive lymphocytes. In the corn oil group, elevated measures of TNF were detected in patients. Hence, the study deduced that the supplementation of -3 PUFAs might be associated with anti-inflammatory actions by impeding the expression of CD25-positive lymphocytes in psoriasis and atopic dermatitis.
Psoriasis is associated with metabolic syndrome [66,67] based on symptoms like IR, abdominal obesity, nonalcoholic fatty liver disease (NAFLD), type 2 diabetes, and high blood pressure [66]. [68] examined the influence of food supplements along with etanercept therapy (anti-TNF treatment), on 40 psoriasis patients who also exhibited the symptoms of metabolic syndrome. The study was specifically designed to analyze the anticipated improvement in metabolic syndrome symptoms after food supplementation (containing Q10 coenzyme, Krill oil, lipoic acid, resveratrol, Vitis vinifera seed oil, vitamin E and selenium) during etanercept therapy. The patients were split into two groups. The first group was treated with etanercept therapy only, while the second received food supplementation along with the therapy. The study concluded that anti-TNF treatment along with food supplementation might aid in regulating normal lipid profile in psoriasis patients who also suffered from metabolic syndrome.
Obesity is indicated by the raised levels of pro-inflammatory cytokines, which mainly include TNF-, IL-6, and acute-phase proteins such as C-reactive protein (CRP). Additionally, a lower level of anti-inflammatory cytokines (adiponectin) is reported in obese individuals. Obesity aggravates psoriasis symptoms and contributes to the worsened response to systemic treatments [37]. In a randomized control clinical trial, [69] evaluated the impact of an energy-restricted (rich in -3 PUFA and reduced in -6 PUFA) diet in 44 obese plaque psoriasis patients who were receiving immune-modulating drugs all through the study. Low-level systemic inflammation in obese psoriasis patients is attributed to poor response to immuno-modulating drugs. Enrolled patients either continued their habitual diet or were administrated with an energy-restricted diet (constituting an average of 2.6g -3 PUFA per day) for 6 months. The effect of diets on metabolic markers and clinical response to immune-modulating treatment was evaluated. A significant reduction (p < 0.05) in PASI, itch score, and Dermatological Life Quality Index were observed compared to baseline in the energy-restricted group. Additionally, a notable decline in weight, serum total cholesterol, and waist circumference was observed in the control group. Hence, the study concluded that the energy-restricted diet (rich in -3 PUFA and reduced in -6 PUFA) considerably improved the metabolic profile and treatment response to immunotherapy in obese plaque psoriasis patients.
Topical therapy plays a critical role in managing all types and severity of psoriasis. Mostly it is sufficient to treat mild, and acts as an adjuvant in moderate to severe state [70]. Topical corticosteroids show anti-inflammatory, immunosuppressive, and antiproliferative characteristics. Consequently, they are widely used for treating various skin diseases, including psoriasis [71]. However, unfavorable effects like striae and atrophy are observed after long-term usage of these agents. For that reason, corticosteroids are mixed with other topical agents to enhance their effect and safety profile for long-term use[70]. In a placebo-control and double-blind study, [72] examined the impact of -3 PUFAs as a topical therapy in psoriasis for 8 weeks. 53 moderate to severe psoriasis patients were enrolled. In each patient, two stable and comparable psoriasis lesions were assigned as indicator lesions. 2 topical preparations were made by using purified -3 PUFAs (at 1 and 10% concentrations). One indicator lesion was then randomly treated with any of the 2 prepared topical preparations, while the second indicator lesion was applied with a placebo. The changes in the indicators like erythema, pruritus, desquamation, local psoriasis severity index, and area involved were considered to measure efficacy. Interestingly, all indicator lesions, including both the -3 PUFAs and placebo-treated, improved remarkably after 8 months. Moreover, the therapy was well taken as no clinically associated adverse effects were reported. The study conveyed no clinical and statistically related variance between -3 PUFAs and placebo-treated topical medications for treating psoriasis lesions in a randomized and double-blind study design. In another fascinating study, [72] investigated the impact of topical administration of olive oil, honey, and beeswax mixture alone and in combination with corticosteroids, on patients suffering from psoriasis vulgaris and atopic dermatitis in a single-blinded study. A total of 18 psoriasis patients were enrolled in this study. Out of these, 10 were given clobetasol propionate medication (corticosteroid). A total of 21 atopic dermatitis patients enrolled, and out of these 11 were treated with betamethasone medication (corticosteroid). A blend of honey, which contained olive oil, beeswax, and honey in equal ratios (1:1:1) was prepared. Afterward, this blend was mixed in a ratio of 1:1, 2:1, and 3:1 with corticosteroids to produce mixture A, B and C, respectively. Dermatitis patients were put through bilateral half-body comparability to investigate the impact of honey blend versus vaseline, or mixture A versus Vaseline and betamethasone blend (1:1) in patients taking betamethasone medication. In psoriasis patients, the outcome of the honey blend was compared against paraffin, or mixture A versus paraffin-clobetasol propionate blend (1:1) in patients who were taking clobetasol propionate medication. The participants were then assessed for symptoms like scaling, redness, and itching. In the honey blend group, 8/10 dermatitis and 5/8 psoriasis patients exhibited remarkable improvement after treatment. 5/11 dermatitis and 5/10 psoriasis participants showed no worsening symptoms upon decreasing 75% corticosteroid dosage by applying mixture C. Hence, the study recommended honey blend topical usage for mitigating symptoms in dermatitis and psoriasis vulgaris.
5.2. Psoriatic Arthritis
Psoriatic arthritis is chronic inflammatory arthritis having an intricate etiology. It is indicated by immune-mediated inflammation of joints, skin, and/or other organs. About 20 to 30% psoriasis patients also suffer from psoriatic arthritis. Both genetic and environmental aspects contribute to defining its sophisticated pathogenesis. Certain infections or mechanical stress are factors that might elicit inflammatory activities, like the production of IL-23, in joints and skin. IL-23 is regarded as the significant cytokine involved in the development of both psoriasis and psoriatic arthritis [73]. The clinical trials that evaluated the impact of consumption of fatty acids on psoriasis arthritis are given in Table 2 and are described below.
In an interesting double-blinded pilot study, [74] evaluated the effect of oral treatment with seal oil in psoriasis arthritis patients. A total of 43 patients entered the study and orally received either seal oil or soy oil (as control) for 2 weeks. Clinical and biochemical variables were observed at baseline, on completion of the trial (2 weeks), and 4 weeks after the trial. During the treatment, patients continued their daily dosage of NSAID and disease-modifying antirheumatic drugs (DMARD). Twenty enrolled patients in each group completed the trial, thus making a total of 40 patients. Remarkable progress in the global assessment of the disease was observed (p < 0.01) in the seal oil group after 4 weeks of treatment. Both groups exhibited amelioration in the tender joint count, with insignificant differences between them. Moreover, in the seal oil group, declines in the ratios of -6 to -3 PUFAs, and in AA to EPA were significantly (p < 0.01) observed. Additionally, 20% of enrolled patients in the trial showed increased calprotectin (S100A8-A9) levels in feces. It might depict asymptomatic colitis in these patients. The study concluded that patients treated with seal oil showed moderate progress in the global evaluation of the disease, along with alleviation in tender joints. Further, the change in the fatty acid serum composition might indicate an anti-inflammatory impact. Consequently, seal oil treatment might provoke therapeutic outcomes similar to NSAID in psoriasis arthritis.
Marine -3 PUFAs and -linolenic acid are known for anti-inflammatory activities. In a randomized and placebo-controlled (olive oil) human intervention trial, [75] evaluated the effect of anti-inflammatory activities of these fatty acids alone or combined, on blood lipids, in patients who had psoriatic arthritis or rheumatoid arthritis. 60 patients, including 6 with psoriatic arthritis and 54 with rheumatoid arthritis, were randomly divided into 4 groups in a double-blinded study design. 47 participants completed the study. The patients in groups 1 & 2 received 3 grams/day of long-chain -3 PUFAs and 3.2 grams/day of -linolenic acid, respectively. Group 3 received the combination of both (1.6 grams of -3 PUFAs and 1.8 grams of -linolenic acid per day), and group 4 received 3 grams/day of olive oil as control, in the form of capsules, for 12 weeks. The clinical status of the patients was noted, and blood samples were collected for evaluation before and after these interventions. Group 1 exhibited significant (p ≤ 0.001) declines in the ratio of AA to EPA, from 6.5 ± 3.7 to 2.7 ± 2.1 present in plasma lipids, and 25.1 ± 10.1 to 7.2 ± 4.7 found in the membrane of erythrocytes. However, no significant impact of these interventions on the AA to EPA ratio was observed in groups 2, 3, and 4. A remarkable upsurge in the concentrations of -linolenic acid and dihomo--linolenic acid found in cholesteryl esters, the membrane of erythrocytes, and plasma lipids, were observed in group 2 due to the consumption of -linolenic acid. In group 3, the consumption of both -3 PUFAs and -linolenic resulted in an upsurge in the concentrations of -linolenic acid and dihomo--linolenic acid found in cholesteryl esters, the membrane of erythrocytes, and plasma lipids. Yet this rise was merely half compared to group 2.
In a randomized, double-blind, and placebo-controlled study, [76] evaluated the effect of marine -3 PUFAs on cardiac autonomic and hemodynamic function in psoriasis arthritis patients. 145 patients were enrolled for 24 weeks and were given 3 grams of either -3 PUFAs (I the form of fish intake) or olive oil. Clinical parameters like Heart rate & heart rate variability (HRV), blood pressure & central blood pressure, pulse wave velocity (PWV), and granulocyte fatty acids composition were noted at baseline and end of the trial. This study reported significant (p = 0.03) differences in the average of all normal RR intervals (time interval noted between two successive R waves in the electrocardiogram) noted at baseline when compared to patients having maximum vs minimum -3 PUFAs intake. In -3 PUFAs group a rise in RR (p= 0.13) and a decline in heart rate (p= 0.12) were observed compared to the control (olive oil group) after the supplementation. Whereas, a significant (p= 0.01) rise and decline in RR intervals and heart rate, respectively, were observed in the -3 PUFAs group compared to the control. The clinical parameters of blood pressure & central blood pressure, and PWV remained the same after the supplementation in -3 PUFAs group. The study extrapolated the prospective protective outcomes of -3 PUFAs consumption against cardiovascular diseases in psoriasis arthritis patients based on the observed increased RR intervals.
Psoriasis patients, particularly those with concomitant psoriatic arthritis, showed a higher intake of analgesics (for alleviating joint pain) in comparison to the general population [77]. In a compelling study, [78] assessed the marine -3 PUFA impact on inflammatory biomarkers and consumption of analgesics (non-steroidal anti-inflammatory drug (NSAID) and paracetamol) in psoriatic arthritis patients. In a randomized and double-blind study design, 145 psoriatic arthritis patients were enrolled. They were either given 3 g of -3 PUFA or olive oil (as control) supplementation per day, for 24 weeks. 133 patients finished the study. Both -3 PUFA and control groups exhibited a significant decline in Disease Activity Score (DAS28-CRP) and PASI compared to baseline. However, a significant decrease in consumption of analgesics (p = 0.04) and leukotriene B4 generation were observed in -3 PUFA group concerning the control group.
Changes in the expression of extracellular matrix (ECM) are associated with the characteristic inflammatory nature of psoriasis [79]. [80] conducted a study to analyze the impact of -3 PUFA on ECM metabolites in psoriasis arthritis patients compared to controls based on a randomized and double-blind design. A total of 142 psoriasis arthritis patients were given dietary fish oil (-3 PUFA) for 24 weeks. 57 normal individuals were also included as a reference. Serum ECM metabolite levels were compared between controls and patients (taken at baseline and after 24 weeks of treatment). As anticipated, the study concluded elevated tissue turnover based on increased ECM metabolite proteins in psoriasis arthritis compared to controls. However, consumption of -3 PUFA resulted in no impact on tissue turnover in psoriasis arthritis.

Table 1.
Clinical studies that assessed the impact of fatty acids in psoriasis
| Sr. no. | Fatty acid | No. of patients | Patient info | Year | Region | Combined with |
Intake type | PMID & Reference |
|---|---|---|---|---|---|---|---|---|
| 1 | polyunsaturated ethyl ester lipids (Angiosan) |
80 | psoriasis and psoriatic arthritis |
1990 | Finland | - | food supplementation |
PMID: 2139859 [62] |
| 2 | oily fish consumption | 18 | plaque psoriasis | 1993 | UK | - | food supplementation |
PMID: 8491161 [58] |
| 3 | fish and corn oils | 145 | moderate to severe psoriasis |
1993 | Norway | - | food supplementation |
PMID: 8502270 [59] |
| 4 | lipid infusion (-3 PUFAs) | 20 | guttate psoriasis | 1993 | Germany | - | infusions | PMID: 8219661 [63] |
| 5 | Highly purified -3 PUFAs | 52 | moderate plaque psoriasis |
1993 | Germany | - | topical | PMID: 8286257 ZEPELIN et al. |
| 6 | -3 PUFAs (long-chain) | 19 psoriasis and 21 atopic dermatitis |
moderate to severe psoriasis and atopic dermatitis |
1994 | Norway | - | food supplementation |
PMID: 8050452 [65] |
| 7 | lipid emulsion (fish oil based) | 83 | plaque psoriasis | 1998 | Europe | - | intravenously administrated |
PMID: 9555791 [60] |
| 8 | natural honey, beeswax and olive oil mixture |
18 psoriasis, 21 dermatitis |
psoriasis and dermatitis |
2003 | UAE | - | topical | PMID: 15022655 [72] |
| 9 | nutraceutical comprising Q10 coenzyme, Krill-oil, lipoic acid, resveratrol, Vitis vinifera seed oil, vitamin E and selenium |
40 | moderate to severe psoriasis |
2013 | Italy | anti-TNF treatment |
food supplementation |
PMID: 24442048 [68] |
| 10 | -3 PUFAs rich diet | 44 | obese patients with plaque psoriasis |
2013 | Italy | mmuno-suppressive drugs |
food supplementation |
PMID: 24120032 [69] |
Table 2.
Clinical studies that assessed the impact of fatty acids in psoriasis arthritis
| Sr. no. | Fatty acid | No. of patients | Patient info | Year | Region | Combined with |
Intake type | PMID & Reference |
|---|---|---|---|---|---|---|---|---|
| 1 | seal oil | 43 | Psoriatic arthritis | 2006 | Norway | - | oral treatment | PMID: 16465662 [74] |
| 2 |
-3 PUFA and -linolenic acid |
60 | 6 Psoriatic arthritis and 54 rheumatoid arthritis |
2011 | Germany | - | food supplementation |
PMID: 21816071 [75] |
| 3 | marine -3 PUFA | 145 | Psoriatic arthritis | 2016 | Denmark | - | food supplementation |
PMID: 27955663 [76] |
| 4 | marine -3 PUFA | 145 | Psoriatic arthritis | 2018 | Denmark | - | food supplementation |
PMID: 28303758 [78] |
| 5 | Dietary fish oils (-3 PUFA) |
142 | Psoriatic arthritis | 2021 | Denmark | - | food supplementation |
PMID: 33885930 [80] |
6. Discussion
The significant role of fatty acids, particularly PUFAs, is unquestionable in human health. The deficiency of -6 PUFA (linoleic acid) is correlated with the formation of scales and water loss from the epidermis. Moreover, PUFAs might stimulate antiproliferative and anti-inflammatory cutaneous metabolites. Hence, it is suggested that PUFAs enriched dietary supplementations, like vegetable and fish oils, might be beneficial in managing inflammatory skin disorders or could be taken as an adjunct along with standard medical treatments [82]. A diet, that contains higher levels of -6 to -3 PUFAs (western diet), facilitates the progression of many autoimmune and inflammatory diseases, including cardiovascular diseases and cancers. While the declining level of -6 to -3 PUFAs, which indicates an increased -3 PUFA consumption, is linked with preventing the pathogenesis of these diseases. This is because -3 PUFAs are attributed to generating anti-inflammatory effects, as these fatty acids might suppress the activity of cytokines (like TNF-, IL-1, and IL-6) [83]. Inflammation, which is the hallmark of psoriasis, is instigated by the overexpression of cytokines during the disease state of psoriasis [41].
EFAs (-3 and -6) also play a significant role in the inhibition of pro-inflammatory cytokines, progression of wound healing, and augmentation of apoptosis in malignant cells. On that account, EFAs are also considered an adjunctive treatment in diverse skin diseases like acne vulgaris, atopic dermatitis, and psoriasis [16]. -3 EFA -linolenic acid, and its long-chain derivatives DHA & EPA are essentially involved in functioning and maintaining structures of membranes of the retina and CNS (central nervous system) [14]. PUFAs are significant in regulating inflammation and immunity. Dietary intake of -6 PUFAs is relatively higher than -3 PUFAs. AA, an -6 PUFA, is involved in the generation of inflammatory mediators belonging to the eicosanoid family. In this way, AA impacts inflammatory cells by modulating cytokine production and regulates the immune system’s equilibriums. The intake of -3 PUFAs, mainly provided from fish and fish oil, declines the concentration of AA in the cell membrane. This decline of AA lessens the eicosanoid production. Therefore, -3 PUFAs are regarded as AA antagonists. These -3 fatty acids could also potentially influence the activities of innate and adaptive immune systems by either acting as AA antagonist or through eicosanoid-independent mechanisms [84].
Because of the discussed significant characteristics of PUFAs in modulating inflammatory cellular responses, several experimental studies have been conducted intending to evaluate the anticipated therapeutic outcomes in various inflammatory diseases, including psoriasis. The current review covers the clinical trials conducted to investigate the impact of fatty acids in psoriasis (and psoriatic arthritis) based on the inclusion criteria stated in the introduction section. The observed favorable outcomes of clinical trials in psoriasis that are covered in the current review are shown in Figure 2.
Fish oils are enriched with -3 PUFAs; therefore, they are widely selected in clinical trials of inflammatory diseases (including psoriasis) to evaluate the likely anti-inflammatory responses. For instance, a study [58] suggested the supplementation with fish oils of herring, kipper, mackerel, pilchard, salmon, and sardine for improved clinical symptoms in plaque psoriasis. As these fish oil supplementations caused elevated EPA levels in patients. Likewise, another clinical trial [59] reported favorable clinical outcomes in psoriasis patients who took fish oil supplements. The improvements were indicated as diminishing scaling. Additionally, no considerable difference was observed between the outcomes of supplementation with corn and fish oil groups in psoriasis. In another clinical trial [60], intravenously administration of fish oil resulted in relief in classical clinical manifestations of chronic plaque psoriasis, as indicated by reduced scaling, erythema, and infiltration. This study also reported improved symptoms in both -3 (fish oil) and -6 PUFAs groups with no adverse effects; however, comparatively better clinical outcomes were observed in the fish oil group.
Angiosan (polyunsaturated ethyl ester lipids) food supplementation in psoriasis patients who were also suffering from psoriatic arthritis resulted in a significantly scaled-down PASI score along with overall relief from the symptoms and joint pain. Therefore, angiosan could be taken as an adjuvant during the course of psoriasis and psoriasis arthritis treatment [62]. Nutritional supplementation with -3 PUFAs in guttate psoriasis resulted in therapeutic outcomes as depicted by reduced scaling [63]. Long-chain -3 PUFAs food supplementation resulted in amelioration of symptoms, which is associated with anti-inflammatory activity caused by decreased expression of CD25 positive lymphocytes [65]. In psoriasis patients, who showed metabolic syndrome, the effect of food supplementation (containing Q10 coenzyme, Krill-oil, lipoic acid, resveratrol, Vitis vinifera seed oil, vitamin E, and selenium) combined with anti-TNF treatment resulted in maintaining normal lipid profile [68]. In obese psoriasis patients, administration of energy-restricted (rich in -3 PUFA and reduced in -6 PUFA) diet reduces weight, waist circumference, and total serum control. It also resulted in a better response to an immune-modulating therapy along with an improved metabolic profile.
As topical therapy, -3 PUFAs produced no significant improvement in clinical symptoms with no adverse effects while treating moderate to severe psoriasis compared to placebo ZEPELIN et al. . However, another study reported mitigating psoriasis vulgaris symptoms after topical treatment with olive oil, honey, and beeswax mixture [72]. In psoriatic arthritis, food supplementation with seal oil resulted in beneficial therapeutic results like amelioration in tender joints similar to NSAIDs [74]. In addition, food supplementation with marine -3 PUFAs in psoriasis arthritis patients generated protective effects against cardiovascular diseases [76]. Fascinatingly, another study reported that analgesic intake significantly reduced in psoriatic arthritis after food supplementation with -3 PUFAs [78]. Nevertheless, the consumption of -3 PUFAs produced no considerable impact on elevated levels of ECM metabolites (linked with inflammation) in psoriasis arthritis [80].
Long-chain saturated fatty acids are more prone to stimulate IR, inflammation and fat storage in the body compared to the medium-chain SFAs and MUFAs [85]. Long-chain SFAs, include stearic and palmitic acids found in butter and palm oil, respectively. Hence, these fats should be avoided in psoriasis. Whereas, medium chain saturated fats and MUFAs include lauric acid and oleic acid, respectively. Lauric acid is present in coconut oil and olive oil is chiefly enriched with oleic acid. Accordingly, olive and coconut oils are favorable options to include in the diet for psoriasis patients [85]. In grownups, a diet rich in SFAs underlines the risk of obesity based on the fat mass and obesity-associated gene [86]. Although obesity is a significant risk factor in psoriasis [35,36,37,49] reported that diet containing high amounts of fats, particularly saturated fatty acids, might elevate early cutaneous inflammation in psoriasis patients irrespective of obesity.
7. Conclusion
Obesity, a risk factor in psoriasis, and a high-fat diet (rich in saturated fats) might exacerbate psoriasis symptoms and result in poor response to medical treatment. However, based on the discussion of clinical trials, the current review suggests that a balanced, hypocaloric diet, which is rich in -3 PUFAs, might aid in managing both psoriasis and psoriatic arthritis along with conventional medical treatments.
Author Contributions
Sidra Adil contributed to writing, formatting, and reviewing the manuscript. Salma Tariq authored the section on "Fatty Acids and Their Significance in Dermatological Physiology. Hasan Sohaib Alavi, Zartasha Mustansar, and Sumair Naseem Qureshi provided a thorough review and valuable suggestions for the improvement of the article."
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Globe, D.; Bayliss, M.S.; Harrison, D.J. The impact of itch symptoms in psoriasis: results from physician interviews and patient focus groups. Health and quality of life outcomes 2009, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Parrish, L. Psoriasis: symptoms, treatments and its impact on quality of life. British journal of community nursing 2012, 17, 524–528. [Google Scholar] [CrossRef]
- Böhm, D.; Stock Gissendanner, S.; Bangemann, K.; Snitjer, I.; Werfel, T.; Weyergraf, A.; Schulz, W.; Jäger, B.; Schmid-Ott, G. Perceived relationships between severity of psoriasis symptoms, gender, stigmatization and quality of life. Journal of the European Academy of Dermatology and Venereology 2013, 27, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Ainali, C.; Valeyev, N.; Perera, G.; Williams, A.; Gudjonsson, J.E.; Ouzounis, C.A.; Nestle, F.O.; Tsoka, S. Transcriptome classification reveals molecular subtypes in psoriasis. BMC genomics 2012, 13, 1–15. [Google Scholar] [CrossRef]
- Parisi, R.; Iskandar, I.Y.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.; Ashcroft, D.M. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. bmj 2020, 369. [Google Scholar] [CrossRef] [PubMed]
- Basavaraj, K.; Seemanthini, C.; Rashmi, R. Diet in dermatology: present perspectives. Indian journal of dermatology 2010, 55, 205. [Google Scholar] [CrossRef] [PubMed]
- Ada, L.S.; Anna, A.; Vincenzo, G. Foods, diet, and skin diseases. SKINmed: Dermatology for the Clinician 2004, 3, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Katta, R.; Desai, S.P. Diet and dermatology: the role of dietary intervention in skin disease. The Journal of clinical and aesthetic dermatology 2014, 7, 46. [Google Scholar]
- Afifi, L.; Danesh, M.J.; Lee, K.M.; Beroukhim, K.; Farahnik, B.; Ahn, R.S.; Yan, D.; Singh, R.K.; Nakamura, M.; Koo, J.; et al. Dietary behaviors in psoriasis: patient-reported outcomes from a US national survey. Dermatology and therapy 2017, 7, 227–242. [Google Scholar] [CrossRef]
- Roe, D.A. Nutrition and the skin; Liss, 1986.
- Boelsma, E.; Hendriks, H.F.; Roza, L. Nutritional skin care: health effects of micronutrients and fatty acids. The American journal of clinical nutrition 2001, 73, 853–864. [Google Scholar] [CrossRef]
- Boelsma, E.; Van de Vijver, L.P.; Goldbohm, R.A.; Klöpping-Ketelaars, I.A.; Hendriks, H.F.; Roza, L. Human skin condition and its associations with nutrient concentrations in serum and diet. The American journal of clinical nutrition 2003, 77, 348–355. [Google Scholar] [CrossRef]
- Ahmed, S.; Shah, P.; Ahmed, O. Biochemistry, lipids. StatPearls [Internet] 2021.
- Council, N.R.; others. Diet and health: implications for reducing chronic disease risk. - 1989.
- Nogoy, K.M.C.; Kim, H.J.; Lee, Y.; Zhang, Y.; Yu, J.; Lee, D.H.; Li, X.Z.; Smith, S.B.; Seong, H.A.; Choi, S.H. High dietary oleic acid in olive oil-supplemented diet enhanced omega-3 fatty acid in blood plasma of rats. Food Science & Nutrition 2020, 8, 3617–3625. [Google Scholar]
- McCusker, M.M.; Grant-Kels, J.M. Healing fats of the skin: the structural and immunologic roles of the ω-6 and ω-3 fatty acids. Clinics in Dermatology 2010, 28, 440–451. [Google Scholar] [CrossRef]
- Siriwardhana, N.; Kalupahana, N.S.; Moustaid-Moussa, N. Health benefits of n-3 polyunsaturated fatty acids: eicosapentaenoic acid and docosahexaenoic acid. Advances in food and nutrition research 2012, 65, 211–222. [Google Scholar] [PubMed]
- Linder, K.E. Structure and Function of the Skin. Feline Dermatology 2020, pp. 3–21.
- Monteiro-Riviere, N.A. Structure and function of skin. In Toxicology of the Skin; CRC Press, 2010; pp. 15–32.
- Wang, Z.; Man, M.Q.; Li, T.; Elias, P.M.; Mauro, T.M. Aging-associated alterations in epidermal function and their clinical significance. Aging (Albany NY) 2020, 12, 5551. [Google Scholar] [CrossRef] [PubMed]
- Nicolaou, A.; Kendall, A.C. Current insights into skin lipids and their roles in cutaneous health and disease. Current Opinion in Clinical Nutrition & Metabolic Care 2023, 26, 83–90. [Google Scholar]
- Nicolaou, A.; Harwood, J.L. Skin lipids in health and disease. Lipid Technology 2016, 28, 36–39. [Google Scholar] [CrossRef]
- Vietri Rudan, M.; Watt, F.M. Mammalian epidermis: a compendium of lipid functionality. Frontiers in physiology 2022, 12, 804824. [Google Scholar] [CrossRef]
- Pappas, A.; others. Lipids and skin health. Technical report, Springer, 2015.
- Feng, F.; Ma, L.; Qu, Z.; Dong, Y.; Yi, F.; Feng, F.; Ma, L.; Qu, Z.; Dong, Y.; Yi, F. Effects of skin surface lipids on skin health. Asian Journal of Beauty and Cosmetology 2019, 17, 149–155. [Google Scholar] [CrossRef]
- Nicolaou, A. Polyunsaturated Fatty Acid Oxygenated Metabolites in Skin. In Lipids and Skin Health; Springer, 2014; pp. 43–63.
- Greb, J.; Goldminz, A.; Elder, J.; Lebwohl, M.; Gladman, D.; Wu, J.; Mehta, N.; Finlay, A.; Gottlieb, A. Psoriasis. Nature Reviews Disease Primers 2016, 2. [Google Scholar] [CrossRef]
- Ziboh, V.A. Arachidonic acid metabolism in the skin. In Arachidonic Acid Metabolism and Tumor Promotion; Springer, 1985; pp. 5–20.
- Ziboh, V.A. The significance of polyunsaturated fatty acids in cutaneous biology. Lipids 1996, 31, S249–S253. [Google Scholar] [CrossRef] [PubMed]
- Sampath, H.; Ntambi, J.M. The role of fatty acid desaturases in epidermal metabolism. Dermato-endocrinology 2011, 3, 62–64. [Google Scholar] [CrossRef]
- Ricciotti, E.; FitzGerald, G.A. Prostaglandins and inflammation. Arteriosclerosis, thrombosis, and vascular biology 2011, 31, 986–1000. [Google Scholar] [CrossRef]
- Gross, E.; Ruzicka, T.; Restorff, B.v.; Stolz, W.; Klotz, K.N. High-affinity binding and lack of growth-promoting activity of 12 (S)-hydroxyeicosatetraenoic acid (12 (S)-HETE) in a human epidermal cell line. Journal of investigative dermatology 1990, 94, 446–451. [Google Scholar] [CrossRef]
- Ellulu, M.S.; Patimah, I.; Khazaâai, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: the linking mechanism and the complications. Archives of medical science: AMS 2017, 13, 851. [Google Scholar] [CrossRef]
- Lee, H.; Lee, I.S.; Choue, R. Obesity, inflammation and diet. Pediatric gastroenterology, hepatology & nutrition 2013, 16, 143. [Google Scholar]
- Jensen, P.; Skov, L. Psoriasis and obesity. Dermatology 2016, 232, 633–639. [Google Scholar] [CrossRef]
- Napolitano, M.; Megna, M.; Monfrecola, G. Insulin resistance and skin diseases. The Scientific World Journal 2015, 2015. [Google Scholar] [CrossRef]
- Rodríguez-Cerdeira, C.; Cordeiro-Rodríguez, M.; Carnero-Gregorio, M.; López-Barcenas, A.; Martínez-Herrera, E.; Fabbrocini, G.; Sinani, A.; Arenas-Guzmán, R.; González-Cespón, J.L. Biomarkers of inflammation in obesity-psoriatic patients. Mediators of inflammation 2019, 2019. [Google Scholar] [CrossRef]
- Kahn, S.E.; Hull, R.L.; Utzschneider, K.M. Mechanisms linking obesity to insulin resistance and type 2 diabetes. Nature 2006, 444, 840–846. [Google Scholar] [CrossRef] [PubMed]
- Kahn, B.B.; Flier, J.S.; et al. Obesity and insulin resistance. The Journal of clinical investigation 2000, 106, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Buerger, C.; Richter, B.; Woth, K.; Salgo, R.; Malisiewicz, B.; Diehl, S.; Hardt, K.; Boehncke, S.; Boehncke, W.H. Interleukin-1β interferes with epidermal homeostasis through induction of insulin resistance: implications for psoriasis pathogenesis. Journal of Investigative Dermatology 2012, 132, 2206–2214. [Google Scholar] [CrossRef]
- Baliwag, J.; Barnes, D.H.; Johnston, A. Cytokines in psoriasis. Cytokine 2015, 73, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Rendon, A.; Schäkel, K. Psoriasis pathogenesis and treatment. International journal of molecular sciences 2019, 20, 1475. [Google Scholar] [CrossRef] [PubMed]
- Batycka-Baran, A.; Maj, J.; Wolf, R.; Szepietowski, J. The new insight into the role of antimicrobial proteins-alarmins in the immunopathogenesis of psoriasis. Journal of immunology research 2014, 2014. [Google Scholar] [CrossRef]
- Grine, L.; Dejager, L.; Libert, C.; Vandenbroucke, R.E. An inflammatory triangle in psoriasis: TNF, type I IFNs and IL-17. Cytokine & growth factor reviews 2015, 26, 25–33. [Google Scholar]
- Zhang, L.j. Type1 interferons potential initiating factors linking skin wounds with psoriasis pathogenesis. Frontiers in Immunology 2019, 10, 1440. [Google Scholar] [CrossRef]
- Li, B.; Huang, L.; Lv, P.; Li, X.; Liu, G.; Chen, Y.; Wang, Z.; Qian, X.; Shen, Y.; Li, Y.; et al. The role of Th17 cells in psoriasis. Immunologic Research 2020, 68, 296–309. [Google Scholar] [CrossRef] [PubMed]
- Innes, J.K.; Calder, P.C. Omega-6 fatty acids and inflammation. Prostaglandins, Leukotrienes and Essential Fatty Acids 2018, 132, 41–48. [Google Scholar] [CrossRef]
- Calder, P.C. Polyunsaturated fatty acids and inflammation. Prostaglandins, leukotrienes and essential fatty acids 2006, 75, 197–202. [Google Scholar] [CrossRef]
- Herbert, D.; Franz, S.; Popkova, Y.; Anderegg, U.; Schiller, J.; Schwede, K.; Lorz, A.; Simon, J.C.; Saalbach, A. High-fat diet exacerbates early psoriatic skin inflammation independent of obesity: saturated fatty acids as key players. Journal of Investigative Dermatology 2018, 138, 1999–2009. [Google Scholar] [CrossRef] [PubMed]
- Myśliwiec, H.; Baran, A.; Harasim-Symbor, E.; Myśliwiec, P.; Milewska, A.J.; Chabowski, A.; Flisiak, I. Serum fatty acid profile in psoriasis and its comorbidity. Archives of Dermatological Research 2017, 309, 371–380. [Google Scholar] [CrossRef]
- Li, Y.; Hruby, A.; Bernstein, A.M.; Ley, S.H.; Wang, D.D.; Chiuve, S.E.; Sampson, L.; Rexrode, K.M.; Rimm, E.B.; Willett, W.C.; et al. Saturated fats compared with unsaturated fats and sources of carbohydrates in relation to risk of coronary heart disease: a prospective cohort study. Journal of the American College of Cardiology 2015, 66, 1538–1548. [Google Scholar] [CrossRef]
- Ring, J.; Kunz, B. Unsaturated fatty acids in the treatment of atopic eczema. In Handbook of atopic eczema; Springer, 1991; pp. 429–434.
- Murphrey, M.B.; Miao, J.H.; Zito, P.M. Histology, stratum corneum. Europe PMC 2018.
- Kaur, N.; Chugh, V.; Gupta, A.K. Essential fatty acids as functional components of foods-a review. Journal of food science and technology 2014, 51, 2289–2303. [Google Scholar] [CrossRef]
- Horrobin, D.F. Essential fatty acids in clinical dermatology. Journal of the American Academy of Dermatology 1989, 20, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Berbis, P.; Hesse, S.; Privat, Y. Essential fatty acids and the skin. Allergie et immunologie 1990, 22, 225–231. [Google Scholar]
- Huang, T.H.; Wang, P.W.; Yang, S.C.; Chou, W.L.; Fang, J.Y. Cosmetic and therapeutic applications of fish oilâs fatty acids on the skin. Marine drugs 2018, 16, 256. [Google Scholar] [CrossRef] [PubMed]
- Collier, P.; Ursell, A.; Zaremba, K.; Payne, C.; Staughton, R.; Sanders, T. Effect of regular consumption of oily fish compared with white fish on chronic plaque psoriasis. European journal of clinical nutrition 1993, 47, 251–254. [Google Scholar]
- Soyland, E.; Funk, J.; Rajka, G.; Sandberg, M.; Thune, P.; Rustad, L.; Helland, S.; Middelfart, K.; Odu, S.; Falk, E.S.; et al. Effect of dietary supplementation with very-long-chain n-3 fatty acids in patients with psoriasis. New England Journal of Medicine 1993, 328, 1812–1816. [Google Scholar] [CrossRef]
- Mayser, P.; Mrowietz, U.; Arenberger, P.; Bartak, P.; Buchvald, J.; Christophers, E.; Jablonska, S.; Salmhofer, W.; Schill, W.B.; Krämer, H.J.; et al. ω-3 Fatty acid–based lipid infusion in patients with chronic plaque psoriasis: results of a double-blind, randomized, placebo-controlled, multicenter trial. Journal of the American Academy of Dermatology 1998, 38, 539–547. [Google Scholar] [CrossRef]
- Balić, A.; Vlašić, D.; Žužul, K.; Marinović, B.; Bukvić Mokos, Z. Omega-3 versus omega-6 polyunsaturated fatty acids in the prevention and treatment of inflammatory skin diseases. International journal of molecular sciences 2020, 21, 741. [Google Scholar] [CrossRef] [PubMed]
- Lassus, A.; Dahlgren, A.L.; Halpern, M.; Santalahti, J.; Happonen, H.P. Effects of dietary supplementation with polyunsaturated ethyl ester lipids (Angiosan®) in patients with psoriasis and psoriatic arthritis. Journal of international medical research 1990, 18, 68–73. [Google Scholar] [CrossRef]
- Grimminger, F.; Mayser, P.; Papavassilis, C.; Thomas, M.; Schlotzer, E.; Heuer, K.U.; Führer, D.; Hinsch, K.D.; Walmrath, D.; Schill, W.B.; et al. A double-blind, randomized, placebo-controlled trial of n-3 fatty acid based lipid infusion in acute, extended guttate psoriasis. The clinical investigator 1993, 71, 634–643. [Google Scholar] [CrossRef]
- Calder, P.C. n- 3 Polyunsaturated fatty acids, inflammation, and inflammatory diseases. The American journal of clinical nutrition 2006, 83, 1505S–1519S. [Google Scholar] [CrossRef] [PubMed]
- Søyland, E.; Lea, T.; Sandstad, B.; Drevon, A. Dietary supplementation with very long-chain n-3 fatty acids in man decreases expression of the interleukin-2 receptor (CD25) on mitogen-stimulated lymphocytes from patients with inflammatory skin diseases. European Journal of Clinical Investigation 1994, 24, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Fostini, A.C.; Fossà, I.; Girolomoni, G.; Targher, G. Psoriasis and the metabolic syndrome. Clinics in dermatology 2018, 36, 21–28. [Google Scholar] [CrossRef]
- Gelfand, J.M.; Yeung, H. Metabolic syndrome in patients with psoriatic disease. The Journal of Rheumatology Supplement 2012, 89, 24–28. [Google Scholar] [CrossRef]
- Skroza, N.; Proietti, I.; Bernardini, N.; La Viola, G.; Nicolucci, F.; Pampena, R.; Tolino, E.; Zuber, S.; Mancini, M.; Soccodato, V.; et al. Efficacy of food supplement to improve metabolic syndrome parameters in patients affected by moderate to severe psoriasis during anti-TNFα treatment. Giornale Italiano di Dermatologia e Venereologia: Organo Ufficiale, Societa Italiana di Dermatologia e Sifilografia 2013, 148, 661–665. [Google Scholar]
- Guida, B.; Napoleone, A.; Trio, R.; Nastasi, A.; Balato, N.; Laccetti, R.; Cataldi, M. Energy-restricted, n-3 polyunsaturated fatty acids-rich diet improves the clinical response to immuno-modulating drugs in obese patients with plaque-type psoriasis: a randomized control clinical trial. Clinical nutrition 2014, 33, 399–405. [Google Scholar] [CrossRef]
- Uva, L.; Miguel, D.; Pinheiro, C.; Antunes, J.; Cruz, D.; Ferreira, J.; Filipe, P. Mechanisms of action of topical corticosteroids in psoriasis. International journal of endocrinology 2012, 2012. [Google Scholar] [CrossRef]
- Castela, E.; Archier, E.; Devaux, S.; Gallini, A.; Aractingi, S.; Cribier, B.; Jullien, D.; Aubin, F.; Bachelez, H.; Joly, P.; et al. Topical corticosteroids in plaque psoriasis: a systematic review of efficacy and treatment modalities. Journal of the European Academy of Dermatology and Venereology 2012, 26, 36–46. [Google Scholar] [CrossRef] [PubMed]
- Al-Waili, N.S. Topical application of natural honey, beeswax and olive oil mixture for atopic dermatitis or psoriasis: partially controlled, single-blinded study. Complementary therapies in medicine 2003, 11, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, V.; Brent, L.H. Psoriatic arthritis. In StatPearls [Internet]; StatPearls Publishing, 2021.
- Madland, T.M.; Björkkjaer, T.; Brunborg, L.A.; Fröyland, L.; Berstad, A.; Brun, J.G. Subjective improvement in patients with psoriatic arthritis after short-term oral treatment with seal oil. A pilot study with double blind comparison to soy oil. The Journal of Rheumatology 2006, 33, 307–310. [Google Scholar]
- Dawczynski, C.; Hackermeier, U.; Viehweger, M.; Stange, R.; Springer, M.; Jahreis, G. Incorporation of n-3 PUFA and γ-linolenic acid in blood lipids and red blood cell lipids together with their influence on disease activity in patients with chronic inflammatory arthritis-a randomized controlled human intervention trial. Lipids in Health and Disease 2011, 10, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, S.; Schmidt, E.B.; Schlemmer, A.; Rasmussen, C.; Lindgreen, E.; Johansen, M.B.; Christensen, J.H. The effect of marine n-3 polyunsaturated fatty acids on cardiac autonomic and hemodynamic function in patients with psoriatic arthritis: a randomised, double-blind, placebo-controlled trial. Lipids in health and disease 2016, 15, 1–10. [Google Scholar] [CrossRef]
- Loft, N.; Nguyen, T.T.; Kristensen, L.E.; Thyssen, J.P.; Egeberg, A. Disease burden, symptoms, and use of analgesics in patients with psoriasis with or without psoriatic arthritis: A cross-sectional study. Journal of the American Academy of Dermatology 2022, 86, 590–597. [Google Scholar] [CrossRef]
- Kristensen, S.; Schmidt, E.; Schlemmer, A.; Rasmussen, C.; Johansen, M.B.; Christensen, J. Beneficial effect of n-3 polyunsaturated fatty acids on inflammation and analgesic use in psoriatic arthritis: a randomized, double blind, placebo-controlled trial. Scandinavian journal of rheumatology 2018, 47, 27–36. [Google Scholar] [CrossRef]
- Wagner, M.F.M.G.; Theodoro, T.R.; Oyafuso, L.K.M.; Pinhal, M.A.S.; et al. Extracellular matrix alterations in the skin of patients affected by psoriasis. BMC molecular and cell biology 2021, 22, 1–12. [Google Scholar] [CrossRef]
- Holm Nielsen, S.; Sardar, S.; Siebuhr, A.S.; Schlemmer, A.; Schmidt, E.B.; Bay-Jensen, A.C.; Karsdal, M.A.; Christensen, J.H.; Kristensen, S. Effect of n-3 PUFA on extracellular matrix protein turnover in patients with psoriatic arthritis: a randomized, double-blind, placebo-controlled trial. Rheumatology International 2021, 41, 1065–1077. [Google Scholar] [CrossRef]
- ZEPELIN, H.H.; Mrowietz, U.; Farber, L.; Bruck-Borchers, K.; Schober, C.; Huber, J.; LETZ, G.; KHNEN, R.; HRISTOPHERS, E.; Welzel, D. Highly purified omega-3-polyunsaturated fatty acids for topical treatment of psoriasis. Results of a double-blind, placebo-controlled multicentre study. British Journal of Dermatology 1993, 129, 713–717. [Google Scholar] [CrossRef]
- Ziboh, V.A.; Miller, C.C.; Cho, Y. Metabolism of polyunsaturated fatty acids by skin epidermal enzymes: generation of antiinflammatory and antiproliferative metabolites. The American journal of clinical nutrition 2000, 71, 361s–366s. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P. Evolutionary aspects of diet, the omega-6/omega-3 ratio and genetic variation: nutritional implications for chronic diseases. Biomedicine & pharmacotherapy 2006, 60, 502–507. [Google Scholar]
- Calder, P.; Grimble, R. Polyunsaturated fatty acids, inflammation and immunity. European journal of clinical nutrition 2002, 56, S14–S19. [Google Scholar] [CrossRef] [PubMed]
- DiNicolantonio, J.J.; OâKeefe, J.H. Good fats versus bad fats: a comparison of fatty acids in the promotion of insulin resistance, inflammation, and obesity. Missouri medicine 2017, 114, 303. [Google Scholar]
- Phillips, C.M.; Kesse-Guyot, E.; McManus, R.; Hercberg, S.; Lairon, D.; Planells, R.; Roche, H.M. High dietary saturated fat intake accentuates obesity risk associated with the fat mass and obesity–associated gene in adults. The Journal of nutrition 2012, 142, 824–831. [Google Scholar] [CrossRef]
Figure 1.
Dietary fats are classified as saturated and unsaturated based on the presence of double bonds. Saturated fats have none, while unsaturated have one or more double bonds. Saturated fats are further categorized as SFAs(short and medium-chain saturated fatty acids) and longer-chain SFAs. Milk fat, palm & coconut oils are the main sources of SFAs, while longer chain SFAs are chiefly found in some vegetable oils, meat, and butterfat. Unsaturated fats are grouped into MUFAs (mono-unsaturated fatty acids) and PUFAs (polyunsaturated fatty acids) based on the number of double bonds. MUFAs have one while PUFAs have two or more double bonds per molecule. In the omega classification system, oleic acid (OA), which is a MUFA, is placed in -9 group. Olive oil is highly enriched in oleic acid. Likewise, PUFAs are further categorized in -3 and -6 groups. -linolenic acid (ALA) and linoleic acid (LA) are the parent fatty acids of -3 and -6 groups, respectively. Other members of -3 are eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) derived from ALA. While Arachidonic acid (AA) and -linolenic acid (GLA) derivatives of LA belong to -6 group. Marine fish and fish oil are predominant sources of -3 PUFAs. In contrast, oils of corn, safflower, and soybeans are chief sources of -6 PUFAs.
Figure 1.
Dietary fats are classified as saturated and unsaturated based on the presence of double bonds. Saturated fats have none, while unsaturated have one or more double bonds. Saturated fats are further categorized as SFAs(short and medium-chain saturated fatty acids) and longer-chain SFAs. Milk fat, palm & coconut oils are the main sources of SFAs, while longer chain SFAs are chiefly found in some vegetable oils, meat, and butterfat. Unsaturated fats are grouped into MUFAs (mono-unsaturated fatty acids) and PUFAs (polyunsaturated fatty acids) based on the number of double bonds. MUFAs have one while PUFAs have two or more double bonds per molecule. In the omega classification system, oleic acid (OA), which is a MUFA, is placed in -9 group. Olive oil is highly enriched in oleic acid. Likewise, PUFAs are further categorized in -3 and -6 groups. -linolenic acid (ALA) and linoleic acid (LA) are the parent fatty acids of -3 and -6 groups, respectively. Other members of -3 are eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) derived from ALA. While Arachidonic acid (AA) and -linolenic acid (GLA) derivatives of LA belong to -6 group. Marine fish and fish oil are predominant sources of -3 PUFAs. In contrast, oils of corn, safflower, and soybeans are chief sources of -6 PUFAs.
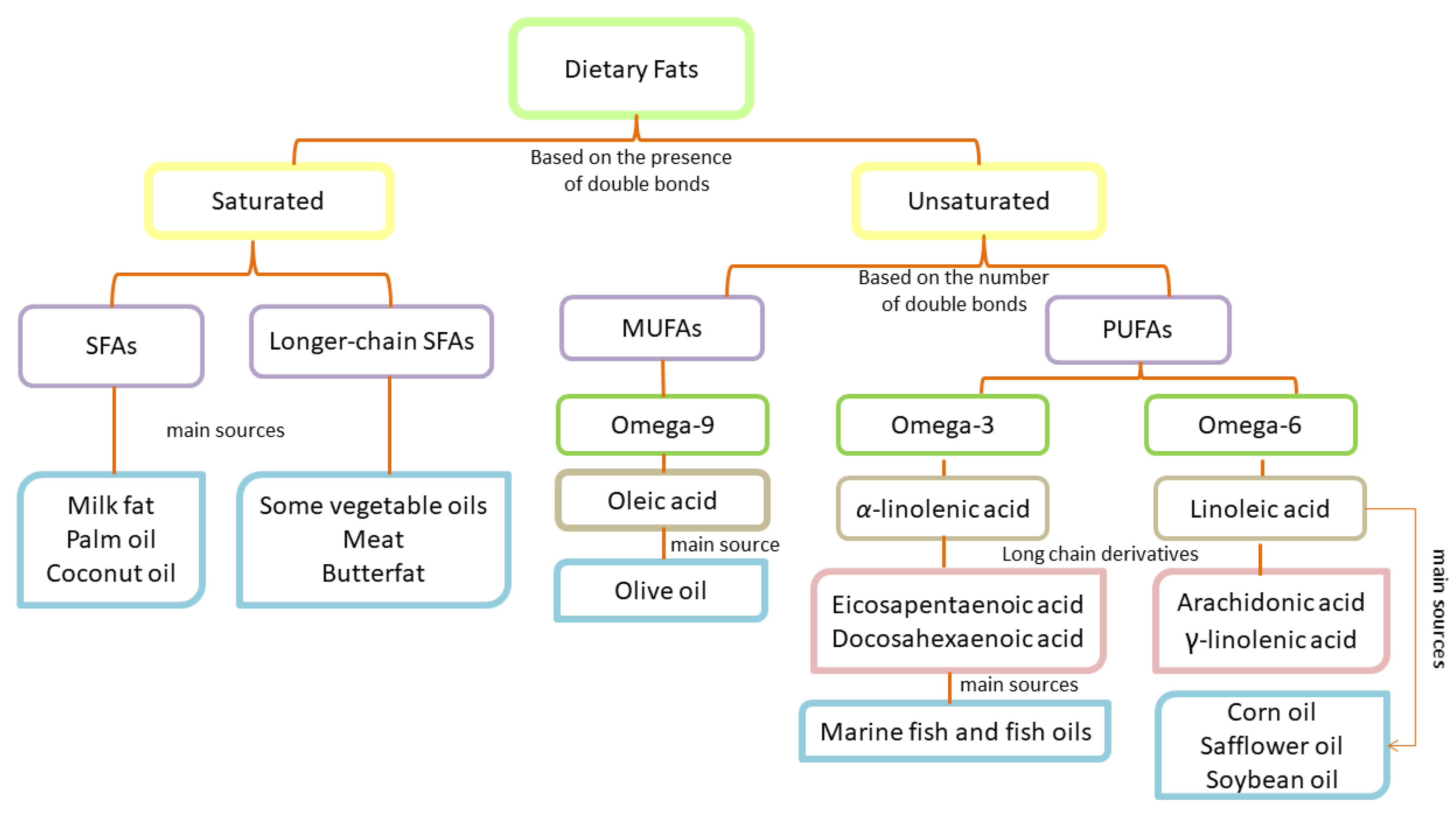
Figure 2.
Clinical favorable outcomes of dietary fats when consumed as food supplementation, intravenously administrated, and taken along with medical treatment.
Figure 2.
Clinical favorable outcomes of dietary fats when consumed as food supplementation, intravenously administrated, and taken along with medical treatment.
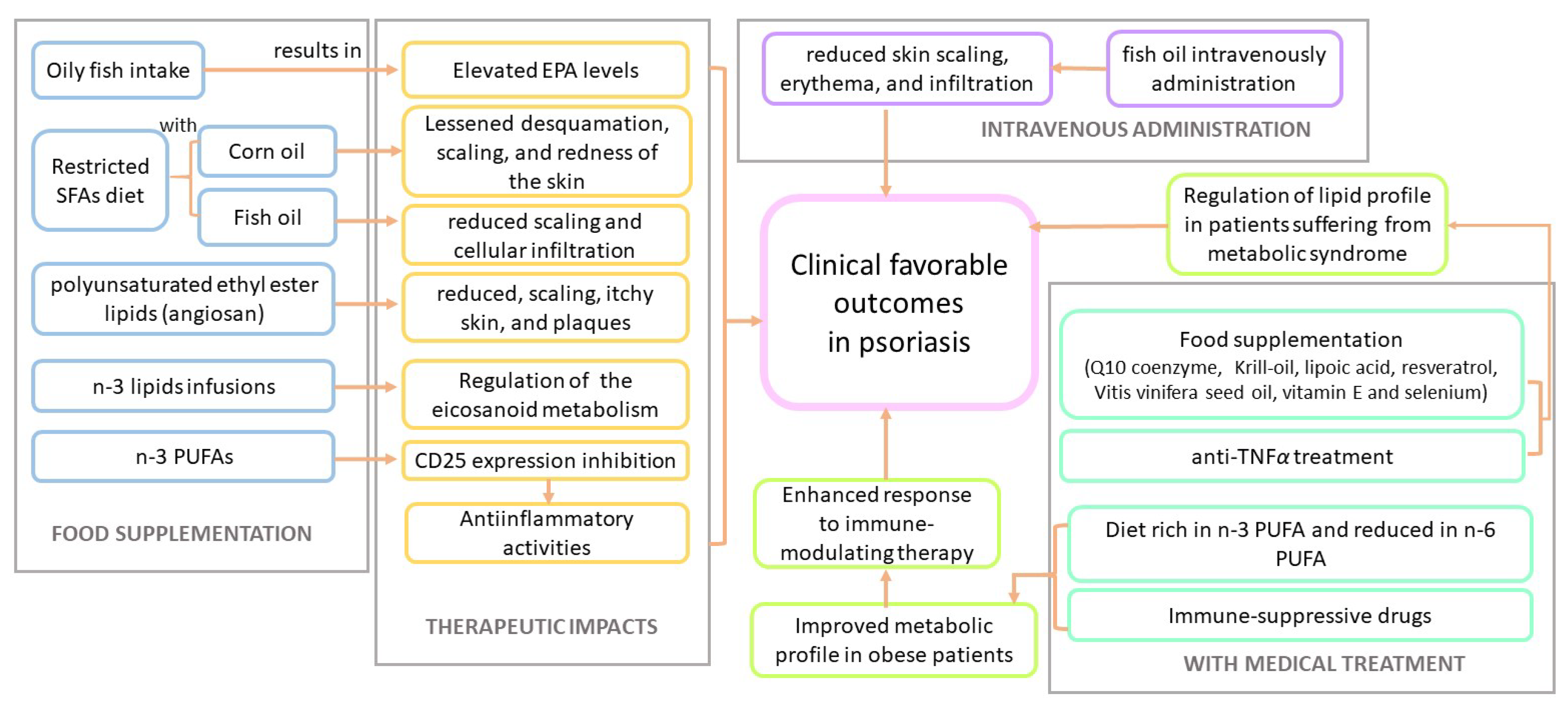
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



