
Submitted:
12 August 2024
Posted:
13 August 2024
You are already at the latest version
Abstract
Objective: To report time-loss match injuries in Portugal’s “Divisão de Honra” (Portuguese First Tier) 2022/23 season focusing on injury incidence, injury burden, anatomical region and type of injury. Methods: A cohort prospective observational study was conducted. Data was collected through an online form sent for every team medical department categorizing player position, injury type, location and severity. Injury incidence and burden were calculated per 1000-player-match-hours. Results: The overall injury incidence was 54.4 injuries per 1000 player-match-hours (CI95% 30.3-96.2). Forwards had a higher incidence comparing to backs. Lower limbs were the most affected location (52% of the injuries). Sprain/ligaments injuries were the most common type of injury followed by muscle injuries. Discussion: The injury incidence was higher than what is reported in amateur competitions and lower than professional ones. Injury severity was similar to other studies. Our study suggests a lower injury burden compared to other semi-professional and elite leagues. Further research with broader participation and training injury data is needed.
Keywords:
Sports medicine
; injury surveillance
; Rugby
; injury prevention
; incidence
1. Introduction
Rugby Union is an emerging sport with around 8.46 million players around the world – an increase of 11% in global participation in 2023 compared to 2022 and is played across 132 countries [1]. As it is characterized by high physical demand with frequent player-to-player impacts and bouts of high-intensity activity, it has one of the highest injury incidence rates of all sports at amateur and elite levels [2].
A meta-analysis analyzing injury surveillance in match injuries in elite rugby male players reported 91 match injuries per 1000h of exposure [Confidence interval (CI) 95% 77-106] [3]. Another meta-analysis studied injuries in amateur male rugby union reporting different numbers of injuries with 46,8 (CI95% 34,4-59,2) match injuries per 1000h of exposure [4].
Literature is scarce in semi-professional rugby. No meta-analysis or systematic reviews on injury surveillance at this level were found, but a prospective cohort observational study analyzing four seasons in the Welsh Premiership senior men’s rugby squad during 4 seasons reported 99.8 match injuries per 1000 match-hours (CI 95% 87.3-114.0) a similar, but higher, number to professional rugby [5].
In 2023 the Portuguese National Squad made its second appearance in the World Cup, getting the first win ever at this level, getting Rugby Union’s media and public attention.
“Divisão de Honra” is the Portuguese first tier, a semi-professional competition, where each team has professional players playing full-time, players playing part-time jobs, and amateur players completing the squad. It’s composed of 10 teams with 18 games per team, 80 minutes per game. After the end of the regular season, 6 teams qualify for the playoffs with one-leg games.
There is only a study about injury surveillance in Portugal in “Divisão de Honra” 2017/18 season, reporting 37.92 (95%CI: 30.71-46.33) injuries per 1000 player-match-hours [6].
The present research aimed to gather data on match injuries sustained by first-tier rugby union players during the 2022/23 season to help promote player’s welfare and performance. Injury epidemiology studies are important to all rugby community, including medical departments, coaches, and players. These data are essential for implementing injury prevention strategies.
2. Materials and Methods
A cohort prospective observational study of senior male rugby union players in Portugal's top tier during the 2022/23 season (from September 2022 to May 2023) was conducted. All 10 teams were invited to participate in the study and informed consent was obtained from the players. This study was ethically approved (Regional Health Administration of Centro).
Injuries were reported through an online form following “Strengthening the Reporting of Observational Studies in Epidemiology - Sports Injury and Illness Surveillance” [7]. The form sought information on player position, date, type, anatomical location, and if it was a contact or non-contact injury. Injury was defined as “any physical complaint sustained by a player during a match which prevented the player from taking a full part in training and/or match play for more than a day following the day of injury.”[8]. Time-loss severity was reported as the number of days lost to training and matches. All injuries were followed until the end of the season. If the player didn’t return to competition before such an end the severity was calculated according to medical department experience according to the injury. Injury severity ranged from slight (0–1 day’s absence), mild (4–7 days’ absence), moderate (8–28 days’ absence) and severe (over 28 days’ absence) [9,10]. Match exposure was calculated for player-match-hours [number of players (15) X number of games X game duration (80 minutes = 1,33 hours)]. No allowances were made on exposure time for players removed (yellow or red cards) as in other studies in the literature [5,10]. Injury incidence rate was calculated as the number of injuries per 1000 player-match-hours (number of injuries/match exposure) X 1000 with 95%CI. Injury burden was calculated as days lost per 1000 player-match-hours (total days lost/ exposure hours) X 1000 with 95%CI. The 95%CI were calculated using bootstrapping as suggested by Williams et. Al. to offer a solid estimate of uncertainty for incidence and burden rate values [11].
Training injuries and non-injury-related absences weren’t recorded.
Significant differences in values for incidence and severity were assessed by comparing non-overlapping 95% confidence intervals for the variables.
Injury data was collected using Microsoft® Excel® and statistical analysis IBM SPSS Statistics [Version 29.0.2.0 (20)]. Shapiro-Wilk tests were used to check if there was a normal distribution of the variables or not.
3. Results
Only 5 of the 10 teams (50%) agreed to participate in this study in 18 games per team during the regular season, 3 of them not reaching playoffs. Two teams reached the playoffs, one losing in the quarterfinals and the other in the semifinals. Total match exposure in all teams reporting injuries was 1855,35h (Forwards 989,52h; Backs 865,83h). A total of 101 injuries were reported during the season, there were more injuries in forwards than in backs (64 vs. 38). Total injury incidence was 54,4 (CI95% 30,3-96,2) per 1000 match hours. Forwards injury incidence was higher in forwards 64,4 injuries per 1000 match hours (CI95% 38,7-103,4) vs. backs 43,9 injuries per 1000 match hours (CI95% 15,9-86,8) (Table 1). Injury burden was 1390,4 days-lost/1000h (1605,9 in forwards and 1144,1 in backs). There was no statistically significant difference in injury incidence and burden according to player position (p=0,798).
Lower limb was the most affected anatomical location with 52% of the injuries and an incidence of 29,0 injuries per 1000 match-hours (CI95% 13,7-52,0), followed by upper limb injuries, representing 24% of total injuries (incidence of 11,6/1000h – CI95% 2,6-27,2), head/neck 17% (10.8 injuries/1000h – CI95% 7,45-14,1) and trunk 7% (3,9 Injuries/1000h – CI95% 2,6-27,2). Figure 1 reports injury frequency according to anatomical location.
Mean injury severity was 25,05 days (standard deviation 42,8), similar between positions (25,5 vs. 24,8; p=0,744). For the reported injuries severity, 1 (1%) was slight, 30 (29,8%) were mild, 49 (49%) were moderate and 21 (20,8%) were severe.
Sprain/ligament injuries were the type of injury with the highest incidence with 14.4 injuries per 1000h match-hours (CI 95% 3,7-30,0) followed by muscle injuries with 8,1 injuries per 1000h of match exposure (CI 95% 4,9-11,5). Sprain/ligament injuries had the highest burden with 590,4 (CI95% 112,4-1068,3) days lost per 1000h of match exposure.
There was no significant difference observed in injury incidence and burden between backs and forwards across different anatomical locations (Table 2) and type of injury (Table 3) as indicated by the overlapping 95% CI.
Contact injuries were more frequent [71,3% of the injuries (n=72)].
We found no statistically significant difference in injury burden between players who sustained contact injuries and those who did not (p = 0.191).
4. Discussion
The primary goal of this study was to evaluate time-loss injuries in the Portuguese Rugby Union First Tier. Despite only 50% of the teams agreeing to participate in the study, injury incidence was 54,4 injuries per 1000 player-match-hours. This incidence rate was higher than what was reported in the 2017/18 season in the same division (37,92 CI 95% 30,71-46,33).6 This number falls between the reported incidences in amateur competitions (46,8 CI 95%: 34,4-59,2) and elite ones (91 CI 95%: 77-106) [3,4].
The variance in injury incidence could potentially be attributed to amateur players and medical departments may be less likely to report minor injuries compared to those in a semi-professional league with more focus on injury management and faster needs of return to sport.
Furthermore, the semi-professional structure of the “Divisão de Honra”, comprising both professional and amateur players, may also contribute to these injury rates, bringing a variation in player experience and physical readiness possibly influencing risk exposure and injury susceptibility. However, further investigation is needed to draw definitive conclusions.
Injury severity was comparable to other studies, with the mean time-loss per injury being 25 days, aligning with previously reported averages in rugby union injury research [3,4,5,6].
Our study found a lower overall injury burden (1390.4 days lost/1000 hours) compared to other semi-professional (3148.8 days/1000 hours) and elite (2692 days/1000 hours) rugby studies, indicating potentially fewer severe injuries or quicker recovery times within our cohort [3,5].
Sprain/Ligament injuries had the highest incident and highest burden as according to other studies, amateur, semi-professional and elite [4,5,10].
As according to the literature, most of the injuries (71%) surged after contact, nonetheless the injury burden wasn’t significantly different from contact and non-contact injuries.
5. Conclusions
Our findings highlight injury epidemiology in Portuguese top-tier rugby. This study follows what’s has been reported in the sport. It emphasizes the need for targeted injury prevention strategies focusing on improving player availability and safety, nonetheless, further research with broader participation is needed for a more comprehensive picture.
In our study training injuries weren’t accounted for as teams have limitations in injury reporting and accountability of training exposure (at a semi-professional level, amateur players may miss training sessions because of work, school, family, or other issues). However, training injuries are reported in the literature to represent a small percentage of all injuries.
Author Contributions
Conceptualization: Nuno Lopes, António Miguel Cruz-Ferreira; Methodology: Nuno Lopes, António Cruz-Ferreira, Software: Diana Torres Lima, Data collection: Nuno Lopes António Cruz-Ferreira, Data analysis Diana Torres Lima, Nuno Lopes, António Miguel Cruz-Ferreira; Original Draft Preparation: Nuno Lopes; Writing, review and editing: Diana Torres Lima, Marta Amaral Silva, Luíz Miguel Santiago; Supervision: António Miguel Cruz-Ferreira, Marta Amaral Silva, Luíz Miguel Santiago. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. Publication funded by CEISUC/CiBB. CEISUC/CiBB is funded by national funds through FCT – Foundation for Science and Technology, I.P., under the Multiannual Financing of R&D Units 2020-2023.
Institutional Review Board Statement
The study was approved by the Ethics Committee of “Administração Regional de Saúde do Centro”.
Informed Consent Statement
Informed consent was obtained from all athletes involved in the study The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
To all medical staff of every team from “Divisão de Honra“ who accept to participate.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WORLD RUGBY, ‘Global rugby participation increasing ahead of Rugby World Cup 2023’. Available online: https://www.rugbyworldcup.com/2023/news/836825/global-rugby-participation-increasing-ahead-of-rugby-world-cup-2023.
- J. H. M. Brooks and S. P. T. Kemp, ‘Recent Trends in Rugby Union Injuries’, Jan. 2008. [CrossRef]
- S. Williams et al., ‘Injuries in Elite Men’s Rugby Union: An Updated (2012–2020) Meta-Analysis of 11,620 Match and Training Injuries’, Sports Medicine, vol. 52, no. 5, pp. 1127–1140, May 2022. [CrossRef]
- C. Yeomans et al., ‘The Incidence of Injury in Amateur Male Rugby Union: A Systematic Review and Meta-Analysis’, Sports Medicine, vol. 48, no. 4, pp. 837–848, Apr. 2018. [CrossRef]
- S. L. Evans, O. E. Davis, E. S. Jones, J. Hardy, and J. A. Owen, ‘Match and training injury risk in semi-professional rugby union: A four-year study’, J Sci Med Sport, vol. 25, no. 5, pp. 379–384, May 2022. [CrossRef]
- M. Cruz-Ferreira, J. C. Rodrigues, Vital Paulo, E. M. Cruz-Ferreira, and F. Moreira, ‘The burden of match injuries in Portuguese senior male club rugby union: A cohort prospective study’, Sports & Exercise Medicine Switzerland, 2023. [CrossRef]
- R. Bahr et al., ‘International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sport 2020 (including STROBE Extension for Sport Injury and Illness Surveillance (STROBE-SIIS))’, Br J Sports Med, vol. 54, no. 7, pp. 372–389, Apr. 2020. [CrossRef]
- W. Fuller et al., ‘Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries’, Br J Sports Med, vol. 40, no. 3, pp. 193–201, Mar. 2006. [CrossRef]
- W. Fuller et al., ‘Consensus statement on injury definitions and data collection procedures for studies of injuries in rugby union’, Br J Sports Med, vol. 41, no. 5, pp. 328–331, May 2007. [CrossRef]
- J. H. M. Brooks, C. W. Fuller, S. P. T. Kemp, and D. B. Reddin, ‘Epidemiology of injuries in English professional rugby union: Part 1 match injuries’, Br J Sports Med, vol. 39, no. 10, pp. 757–766, Oct. 2005. [CrossRef]
- S. Williams, J. W. Shaw, C. Emery, and K. A. Stokes, ‘Adding confidence to our injury burden estimates: Is bootstrapping the solution?’, Br J Sports Med, vol. 58, no. 2, pp. 57–58, Jan. 2024. [CrossRef]
Figure 1.
Injuries frequency according to anatomical location.
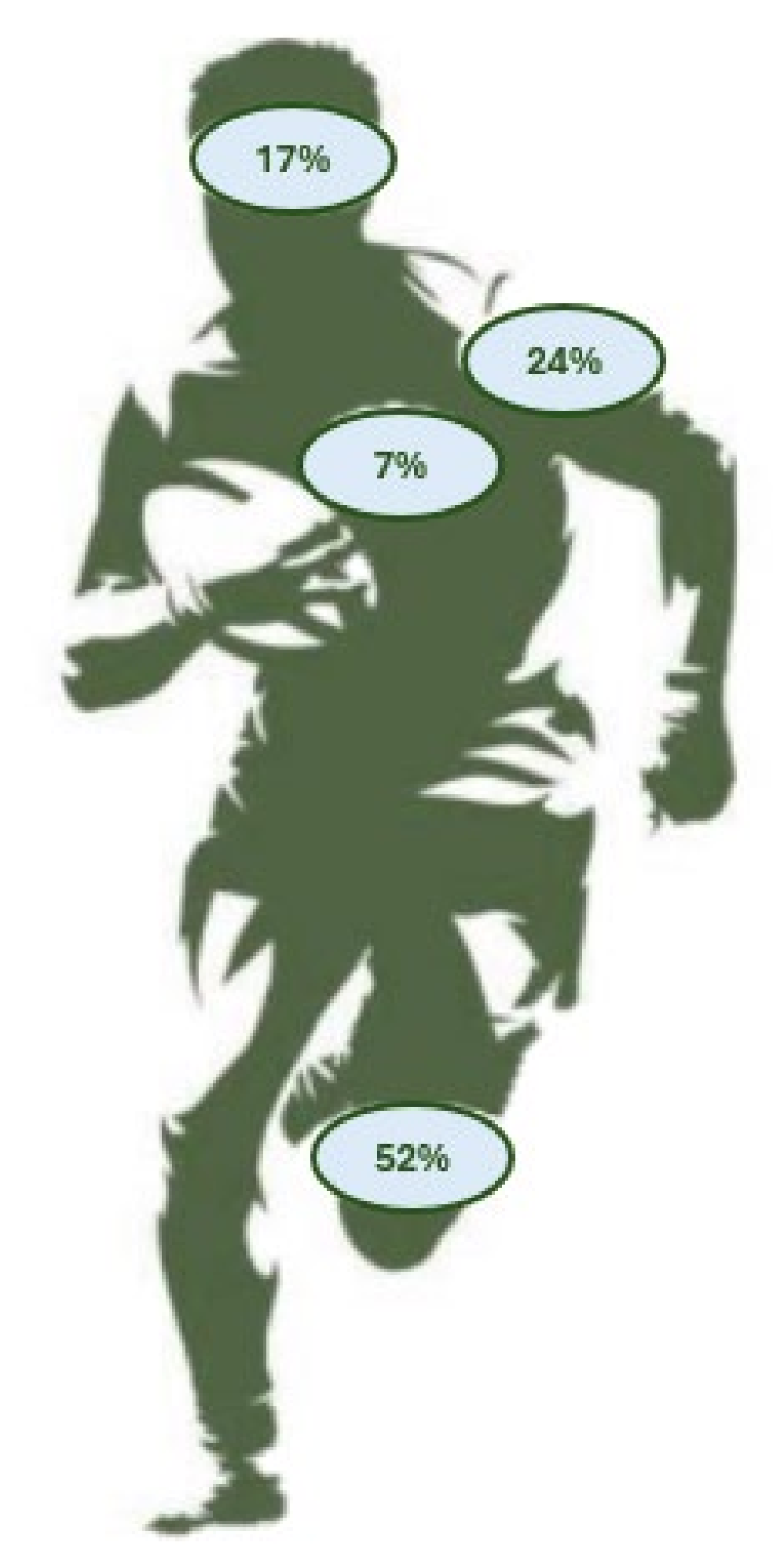

Table 1.
Total Match time-loss injury incidence, severity, and burden. CI: Confidence interval; d: days.
Table 1.
Total Match time-loss injury incidence, severity, and burden. CI: Confidence interval; d: days.
| Total injuries | Injury incidence (95%CI) | Mean severity (d) | Injury burden (95%CI) | |
|---|---|---|---|---|
| Match injuries | 101 | 55,9 (30,3-96,2) | 25,0 | 1390,4 (610,3-2337,1) |
| Forwards | 63 | 64,4 (38,7-103,4) | 24,8 | 1605,9(768,2-3004,4) |
| Backs | 38 | 43,9 (15,9-86,8) | 25,5 | 1144,1(429,9-2019,3) |
Table 2.
Match time-loss injury incidence and burden by anatomical location and position. CI: Confidence interval.
Table 2.
Match time-loss injury incidence and burden by anatomical location and position. CI: Confidence interval.
| Injury Incidence (CI95%) | Injury Burden (95%CI) | |||||
|---|---|---|---|---|---|---|
| Match injury | All players | Forwards | Backs | All players | Forwards | Backs |
| Head/Neck | 10,8 (7,5-14,1) | 14,0 (6,7-19,2) | 13,0 (3,3-27,4) | 164,5(105,4-222.2) | 198,3(81,2-294,7) | 137,8(67,0-178,8) |
| Upper Limb | 11,6 (2,6-27,2) | 15,4 (7,0-26,1) | 9,5 (0-28,6) | 168,7(28,9-344-0) | 204,6(54,2-355,1) | 127,7(0,0-383,1) |
| Lower Limb | 29 (13,7-52,0) | 29,7 (14,3-54,8) | 28,3 (11,5-47,5) | 979,2(427,6-1685,3) | 1056,7(373,6-2322,0) | 890,7(342,9-1752,3) |
| Trunk | 3,9 (0,6-8,9) | 11,6 (2,6-27,2) | 0,0 (0,0-0,0) | 78,0(15,6-152,6) | 146,2(29,2-286,1) | 0,0(0,0-0,0) |
Table 3.
Match time-loss injury incidence and burden by type. CI: Confidence Interval.
| Injury Incidence (CI 95%) | Injury Burden (CI 95%) | |||||
|---|---|---|---|---|---|---|
| All players | Forwards | Backs | All players | Forwards | Backs | |
| Abrasion | 0,53(0,0-1,6) | 1,0(0,0-3,0) | 0,0(0,0-0,0) | 2,6(0,0-7,9) | 4,9(0,0-14,8) | 0,0(0,0-0,0) |
| Concussion | 4,9(2,6-8,3) | 5,1(0,9-10,4) | 4,8(1,2-8,4) | 83,2(30,6-141,1) | 68,4(8,5-156,0) | 87,7(16,7-175,4) |
| Fracture | 4,4(2,1-6,7) | 5,1(2,1-8,2) | 3,6(1,2-6,0) | 126,1(44,8-228,1) | 151,9(58,5;273,1) | 84,6(16,7-159,8) |
| Haematoma/ contusion/ bruise | 7,1(1,0-16,2) | 9,3(0,9-23,0) | 4,7(1,1-8,4) | 83,3(7,8-201,3) | 129,7(5,2;339,6) | 26,4(6,6-46,3) |
| Laceration | 4,2(1,1-7,3) | 6,9(2,0-11,8) | 1,1(0,0-3,2) | 27,0(6,1-49,9) | 44,0(11,5-76,6) | 6,6(0,0-19,7) |
|
Lesion of meniscus, cartilage or disc |
2,8(0,0-7,2) | 3,13(0,0-9,4) | 2,4(0,0-4,8) | 133,7 (0-369,8) | 220,3(0,0-661,0) | 30,3(0,0-88,8) |
| Muscle rupture/ tear/strain/cramps | 8,1(4,9-11,5) | 11,0(6,2-15,9) | 6,0(1,2-10,7) | 187,4(90,6-271,9) | 285,6(169,3-406,4) | 65,8(0,0-134,7) |
| Other | 1,7(0,0-3,9) | 2,1(0,0-4,2) | 2,1(0,0-4,2) | 23,9(0,0-58,5) | 39,1(0,0-103,8) | 7,3(0,0-21,9) |
| Sprain/ligament injury | 14,4(3,7-30,0) | 13,5(3,0-28,2) | 15,4(4,3-32,1) | 590,4(112,4-1068,3) | 564,1(98,2-1268,0) | 542,8(68,5-1282,4) |
| Tendon injury/rupture/ tendinopathy/bursitis | 5,0(0,6-10,0) | 7,3(0,0-15,7) | 6,0(0,0-15,5) | 85,2(8,4-199,4) | 99,2(0,0-239,1) | 60,6(0,0-150,4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



