
Submitted:
12 August 2024
Posted:
13 August 2024
You are already at the latest version
Abstract
Non-union is one of the severe complications of traumatic fracture and still no standard therapeutic recommendations currently. A total of eleven patients were treated on the lesions for non-union, after the failure of open reduction internal fixation (ORIF) or total hip replacement, by autologous conditioned serum (ACS) for one to three times monthly and followed up. Seven patients received ACS three times, three patients received it two times, and the only one who underwent total hip replacement received it once. Ten patients achieved union at the last follow-up visit, indicating the effectiveness of ACS on patients who suffered from non-union after ORIF. ACS has the potential as an alternative or adjective treatment for non-union and is worthy to be investigated further for the benefits of patients.
Keywords:
autologous conditioned serum
; fracture
; non-union
1. Introduction
Non-union is one of the severe complications of traumatic fracture, leads to functional impairment, morbidity and loss of quality of life [1]. The incidence of non-union among studies are various, from 2 to 15% has been reported, depends on the types of fracture and injured bone [2,3]. There are still no standard therapeutic recommendations for non-union. Local infection control, debridement, deformity correction, fixation, bone graft, and biological agents are all considered and utilized based on clinical experience and positive results were gained [4]. Among these strategies, transplanting autologous cancellous graft on the non-union site might have the highest level of consensus as a more effective treatment. Autologous cancellous graft acts as a scaffold and source of bone cells for new bone growth. However, the limited source indicates the need of developing new strategy. Platelet-rich plasma (PRP) is another biological agent that gains elevated attention on the potential role of orthopedic management, including non-union. Results of numerous basic, preclinical, and clinical researches have been published, the efficacy of PRP alone or combination with other treatments on non-union has been proven [5,6,7]. Despite majority of literature supports the positive effectiveness of PRP on non-union, conflicting results exist [8,9,10]. In addition, studies have shown that other biological agents may be more effective than PRP. Within bone morphogenetic proteins (BMPs) family that are released from mesenchymal stem cells, triggers chondroblastic and osteoblastic differentiation, BMP-7 shows superior efficacy during revision surgery compared to PRP [11,12]. BMP-2 is the first and only bioagent approved by the U.S. Food and Drug Administration for non-union treatment [13,14]. Furthermore, no standardized preparation and administration protocols also hinders the establishment of consensus to include PRP in the recommendation of non-union treatment. Thus, alternative and adjective treatments are still evaluating for non-union in orthopedic field.
Autologous conditioned serum (ACS) is another autologous blood-derived product, which is composed of enriched cytokines and growth factors that are secreted by blood cells including platelets after being stimulated by glass beads. The first device developed for processing ACS was originally branded as “Orthokine” in the late 1990s [15,16,17]. Previous studies have shown the efficacy of ACS on osteoarthritis [15,16,18,19,20]. Since PRP is the first autologous biological agent used for osteoarthritis therapy, we have conducted a study to directly compare the contents and the clinical efficacy of PRP and ACS for osteoarthritis treatment. ACS has higher capability of pain relief than PRP, which might be due to the higher levels of PDGF-BB and IL-1Ra of ACS [21].
In this study, we attempted to evaluate the clinical efficacy of ACS injection for patients with non-union fracture after open reduction internal fixation (ORIF) based on the knowledge from PRP on bone healing, aims to explore the clinical utility of ACS to garner more experiences of using autologous biological agents on orthopedical disorders.
2. Materials and Methods
2.1. Patients
Patients who were diagnosed by certified physicians as non-union radiologically at least 9 months [22] and have been treated by ORIF were asked for consent to receive the ACS treatment. In addition, one patient with non-union who underwent total hip replacement for bone defect was also included. Patients aged <18 years, having open wounds, major neurological diseases such as dementia, active thrombovascular diseases, or infections, and who were uncooperative were excluded. Patients were injected with 3.5 mL of ACS on the lesion, and ACS was fresh prepared for each treatment appointment every month. The clinical efficacy on non-union was evaluated by X-ray at the next monthly visit. The ACS treatment times between one and three times depended on the bone union status at the next monthly visit evaluated by the physicians. All the patients provided signed informed consent.
2.2. ACS Preparation
ACS was prepared from 10 mL blood of each patient. Non-fasting blood samples were collected and transferred into the PRPII sterile glass beads containing tube (Pen-Ling Biotechnology Co., Ltd. Taiwan) with one air pore on the top and medical grade glass beads inside and incubated at 37°C for 3 h to active described previously [21], followed by centrifugation at 4000 rpm for 5 minutes. ACS was harvested using a spinal needle through the air pore.
3. Results
3.1. Patients and Outcomes of ACS Injection
From 2022 to 2024, a total of eleven patients were treated by ACS injection(s) on the lesions of non-union one to three times monthly and followed up. Eight are males and three are females, aged between 21 to 66 years and the median and mean are 45 and 43 years, respectively. Nine patients were intervened surgically due to long bone fractures, the others underwent surgery because of osteoarthritis of hip and clavicle fracture. Ten patients were treated by ORIF and one (Case 7) underwent a total hip replacement, all cannot achieve bone union at least 9 months after initial surgical intervention. One patient (Case 1) performed revision intramedullary nail fixation after plate implant failure, however still no improvement. For ACS treatment, seven patients received three times, three patients received two times, and the only one who underwent total hip replacement received one time of ACS injection. Ten patients achieved union at the last follow-up visit. The only one (Case 5) who cannot become bone union after ACS treatment was presumably due to implant failure caused by unstable fixation.

Table 1.
Patients’ characteristics.
| Case | Age (years) | Sex | Diagnosis | Previous treatment outcomes | Non-union duration before ACS (months) | ACS Injection times | Outcomes |
|---|---|---|---|---|---|---|---|
| 1 | 50 | Female | Tibial fracture | Plate implant failure, followed by intramedullary nail at 9 months but still non-union | 9 | 3 | Union |
| 2 | 47 | Male | Right femoral shaft fracture | Non-union after ORIF | 9 | 3 | Union |
| 3 | 45 | Male | Right tibia and fibula fracture | Dynamization of distal screws on tibia; ACS injection was given on fibula. | 9 | 3 | Union |
| 4 | 39 | Female | Right clavicle fracture | Non-union after ORIF | 9 | 2 | Union |
| 5 | 66 | Male | Right upper femoral fracture | Plate implant failure, followed by gamma nail fixation at 9 months but still non-union | 9 | 3 | Non-union; due to unstable fixation |
| 6 | 34 | Male | Left distal femur fracture | Non-union after ORIF | 9 | 3 | Union |
| 7 | 53 | Male | Acetabulum bone defect | Non-union after total hip replacement | 25 | 1 | Union |
| 8 | 50 | Male | Left distal femur lateral condyle fracture | Non-union after ORIF | 36 | 2 | Union |
| 9 | 39 | Male | Right ulnar fracture | Non-union after ORIF | 14 | 2 | Union |
| 10 | 21 | Female | Right upper tibia fracture | Non-union after ORIF | 12 | 3 | Union |
| 11 | 27 | Male | Left radial & ulnar fracture | Non-union after ORIF | 9 | 3 | Union |
ACS: autologous conditioned serum; ORIF: open reduction internal fixation.
The radiographic results of the representative cases including Case 1, 4, 6 and 11 are shown in Figure 1, Figure 2, Figure 3 and Figure 4, respectively. Case 1 was treated by plate implant (Figure 1a) and revisional intramedullary nail fixation (Figure 1b), but the fractural space still existed after revision rod for 9 months (Figure 1c). After the third injection, union was achieved at the last evaluation, which was three months after the third injection (Figure 1d).
Case 4 only received two ACS injections for non-union clavicle fracture, because the progress of bone healing is excellent, the physician decided no more treatment was required (Figure 2). In the present study, up to three ACS injections were designed as the standard therapeutic plan based on clinical experience, however, the physicians could alter the plan according to clinical response. Thus, regular monitoring is necessary to make decisions. Radiography is an effective method with good availability for evaluating bone healing. Thus, routinely radiographic evaluation should be performed before and during ACS treatment in this study for the evaluation of the effeteness of ACS.
Case 6 suffered from non-union femur fracture after ORIF for nine months then was treated by ACS injections three times, and complete bone healing was achieved (Figure 3).
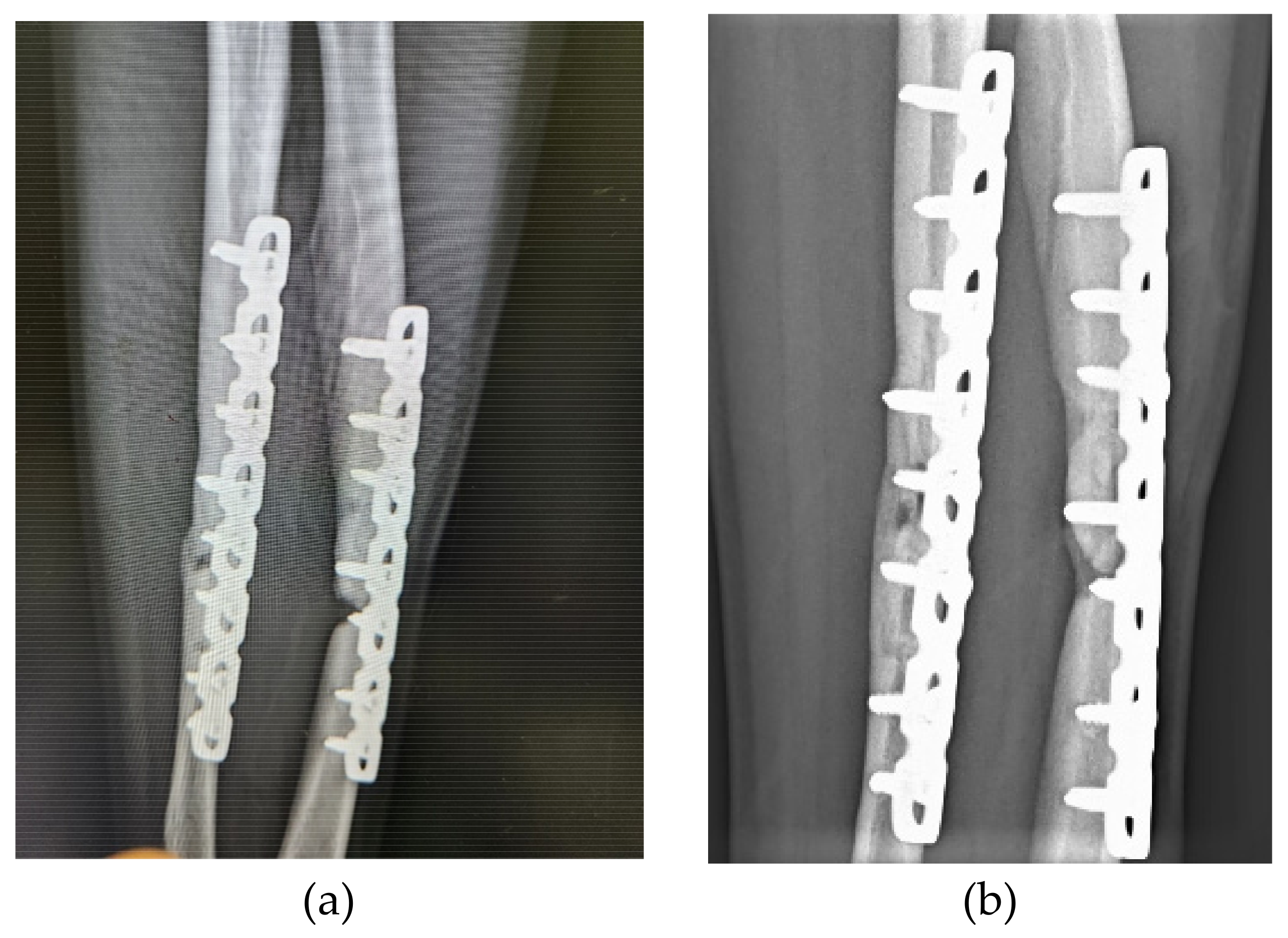
Case 11 had both radial and ulnar fractures on left arm, and received three ACS injections for non-union after ORIF for nine months. Evident healing efficacy of ACS was observed from the results of X-ray evaluation (Figure 4).
4. Discussion
Data regarding using ACS for fracture in addition to non-union treatments is limited; to date, the present study might be the first one that aims to evaluate the therapeutic efficacy of ACS on non-union. Before accumulating sufficient evidence of ACS by in vitro, in vivo and clinical studies in the future, most of the perspectives of ACS in the study are expended from the previous experiences and studies of PRP on bone healing.
The mechanism of PRP for treating non-union is providing concentrated platelet and specific growth factors, including platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), transforming growth factor (TGF) and insulin-like growth factor-1 (IGF-1) at the region of bone defect to establish required microenvironment for bone regeneration. These effectors induce the process of bone healing, including cellular proliferation, matrix formation, osteoid production and collagen synthesis that are through activating and regulating osteoblasts, osteoclasts and mesenchymal stem cells (MSCs), and are represented by soft callus formation, hard callus formation and bone remodeling [23,24,25]. That means both new skeletal tissue and surrounding soft tissue are reconstructed under the effects provided by PRP [25,26]. The plurality of involved growth factors, cells and physical functions reflect the complexity of bone healing process is extraordinarily high, while autologous blood-derived products such as PRP or ACS which are composed by many cytokines and growth factors may have better and more comprehensive effects than one specific component since multiple pathways should be activated for initiating bone healing, and interaction between components may have synergy.
The efficacy of PRP on non-union has been proven by previous studies. A randomized, double-blinded, placebo-controlled study evaluated the efficacy of PRP in patients with non-union fracture together with autologous bone graft and internal fixation, and saline served as the placebo. PRP showed therapeutic effect on non-union, indicated by significant higher bone healing rate compared to that in the placebo group as 81.1% vs. 55.3% (P = 0.025) [27]. A meta-analysis including above mentioned clinical trial and additional two randomized controlled studies, one prospective study and nine retrospective studies showed similar results; compared to the control group, patients suffering from long-bone delayed union and non-union treated by PRP had higher bone healing rate (85.8% vs. 60.27% and OR = 3.07; 95% CI, 1.37-6.87; P = 0.006) [28]. Using PRP alone or combined with other conventional treatments i.e., autografts transplant, compression plates and/or fixation devices have been reported and compared by many investigators with various study designs [5]. Clinical trials were conducted for the comparison of PRP along and combined with internal fixation. Combination of PRP and surgery provided greater bone healing rate (94% vs. 78%, P < 0.05) and shorter bone healing time (91.6 ± 6.9 vs. 115.2 ± 8.4 days, P < 0.05) compared to those of PRP along, indicated the benefit of incorporating autologous biologic agents into established clinical practice [29]. In addition, surgery combined with other biological agents such as MSCs for non-union is also evaluated [30,31], indicating the unmet need is critical, more studies about newly developed biological agents should be performed to evaluate the effect(s) on new bone regeneration.
Even ORIF is the standard treatment for fractures of numerous sites, however, internal fixation is sometimes challenging due to the complex anatomy, leading to the relatively high non-union rate despite the continuing advances in surgical technique [32]. Treatment of non-union after success ORIF is also a challenge. For distal humerus fractures, up to 25% of non-union occurred after ORIF [33], and additional surgery including revision ORIF is the current recommendation [34,35]. However, the complication rate is very high with unsatisfactory outcomes, bone healing may be not achieved after this secondary operation [34]. Thus, alternative treatment such as applying biological agents to promote bone healing is still necessary to be investigated for treating non-union after ORIF.
Many risk factors have been known that associated with non-union, including the location and type of bones. For example, as the weight-bearing bones, the fracture of femur and tibia usually need more time to reach union [36]. Increasing age, alcohol consumption, smoking and deficiency of nutrition such as Vitamin D, calcium, or protein that is essential for bone healing are associated with delay union or non-union [37]. Particularly, the success rate of ORIF can be significantly impacted by the age of the patients. In elderly patients, because of the relatively high prevalence of osteoporosis and poor condition of surrounding soft tissue, the non-union rate may increase [38]. Three injections of ASC still cannot achieve union in Case 5 and the possible reason is unstable fixation, which may be associated to the elder age. Furthermore, from the experiences of PRP, the type of bone may also affect the healing outcomes and lead to controversial results in the literature; positive effects were often found in well-vascularized cancellous bone where cells for new bone regeneration are abundant, and cases of no effects were usually had defects on maxillary bone or mandibular bone [39,40]. One patient (Case 7) who underwent total hip replacement was also included in this study. Only one injection was needed to achieve union, this may also indicate the impact of bone type on the efficacy of biological agents such as ACS.
Since the healing process and impact factor are both complicated, optimalization of treatment plan that combine surgical intervention and autologous biological agents for individual needs should be considered based on the evidence. For example, the optimal timing of treating non-union fracture using autologous biological agents is still evaluating. The experience from PRP shows varied intervals after injury among studies, from six to 12 months have been reported [41,42]. The present study defined non-union as at least nine months after initial invention for treating injury, and the results indicated that ACS injection has therapeutic effect on non-union fracture at least nine months after ORIF. Consider the non-union rate in patients who underwent the standard ORIF treatment is still high, ACS might be used earlier in the early phase of fracture. Furthermore, the conventional treatments for fracture including surgery, immobilization and rehabilitation are all time-consuming and significantly impact patients’ quality of life. If ACS is used as an alternative or adjective treatment not only improve the bone healing rate and enhance the healed bone’s structural integrity but also shorten the time for bone healing, possibly can greatly enhance the outcomes and provide benefit on quality of life for patients suffering from fracture. The optimal number of injections is also unclear. In the case of using PRP for osteoarthritis, Subramanyam et al. [43] reported that three injections were suggested since superior outcomes to single and double injections were observed, and Andersen et al. [29] indicated that for non-union, usually a single dose was given, but in some studies, multiple injections were applied depending on the status of the fractural site [44,45]. In our previous study, PRP or ACS was given every 2 weeks five times for osteoarthritis [21]. In the present study, up to three injections were applied because postpone additional surgery until 12 months after injury may obtain unsatisfied patients’ outcomes. The injection interval can be shortened in patients with slow healing rate to increase the total dose of ACS, but the treatment protocol needs more studies to be established.
The effectiveness of PRP and ACS were not compared directly in the present study, however, from the study we conducted for osteoarthritis, ACS may be superior to PRP because of the higher levels of PDGF-BB and IL-1Ra of ACS. PDGF-BB and IL-1Ra levels were around 4.7 times (9512.7 vs. 2035.2 pg/mL) and 5.7 times (902.9 vs. 157.9 pg/mL) higher in ACS than in PRP [21]. PDGF-BB involves in cell proliferation, migration and angiogenesis. In the process of bone healing, PDGF-BB is responsible for inducing chemotaxis of osteoblasts which are essential cells to initiate the synthesis of new bone tissue [46]. IL-1Ra is the antagonist of IL-1β, and serves as the immunomodulator during bone healing because of the anti-inflammatory properties. In the early phase of bone injury, proinflammatory cytokine IL-1β recruits inflammatory cells to debride the lesion and stimulate the transient matrix hematoma for the recruitment of mesenchymal stromal cells to rebuild the new tissue [47]. However, prolonged inflammation hinders bone healing process because of the inhibition of MSCs differentiation and induction of apoptosis [48]. Thus, the anti-inflammation effect provided by IL-1Ra may be one of the central of the bone healing, but the detailed mechanism(s) should be explored by more in vitro and animal experiments. Other components within these autologous biological agents probably also play an important role in the bone healing process, such as exosomes are considered capable of promoting tissue regeneration [49], and the levels in ACS were 1.5 times higher than those in PRP (1.5 × 1013 ± 3.0 × 1012 vs. 6.0 × 1012 ± 4.9 × 1011 vesicles/mL, data not shown). Detailed analysis of the contents and their functions on bone healing should be conducted to explore the mechanism underlying the therapeutic effect.
5. Conclusions
ACS has effectiveness on bone healing in patients suffering from non-union treated by ORIF, however the optimal timing, injection numbers, and total dose, in addition to the molecular mechanism and comparison of other autologous biological agents should be clarified in the future.
Author Contributions
Conceptualization, P.-G.C., and C.-H.W.; methodology, M.-K.A.; software, C.-H.L.; validation, M.-J.H., and C.-S.H.; formal analysis, P.-G.C.; investigation, C.-H.W.; resources, M.-K.A.; data curation, C.-H.L.; writing—original draft preparation, K.-D.Y.; writing—review and editing, C.-H.W.; visualization, M.-K.A.; supervision K.-D.Y.; project administration, P.-G.C.; funding acquisition, P.-G.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all patients involved in the study.
Data Availability Statement
Data will be made available on request.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Turner, C.H. Biomechanics of bone: determinants of skeletal fragility and bone quality. Osteoporos Int 2002, 13, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Megas, P. Classification of non-union. Injury 2005, 36 Suppl 4, S30–S37. [Google Scholar] [CrossRef]
- Tzioupis, C.; Giannoudis, P.V. Prevalence of long-bone non-unions. Injury 2007, 38 Suppl 2, S3–S9. [Google Scholar] [CrossRef]
- Schlundt, C.; Bucher, C.H.; Tsitsilonis, S.; Schell, H.; Duda, G.N.; Schmidt-Bleek, K. Clinical and Research Approaches to Treat Non-union Fracture. Curr Osteoporos Rep 2018, 16, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.; Wragg, N.M.; Shariatzadeh, M.; Wilson, S.A.-O. The Use of Platelet-Rich Plasma (PRP) for the Management of Non-union Fractures.
- Xie, X.; Wang, Y.; Zhao, C.; Guo, S.; Liu, S.; Jia, W.; Tuan, R.S.; Zhang, C. Comparative evaluation of MSCs from bone marrow and adipose tissue seeded in PRP-derived scaffold for cartilage regeneration. Biomaterials 2012, 33, 7008–7018. [Google Scholar] [CrossRef] [PubMed]
- Alsousou, J.; Thompson, M.; Hulley, P.; Noble, A.; Willett, K. The biology of platelet-rich plasma and its application in trauma and orthopaedic surgery. The Journal of Bone & Joint Surgery British Volume 2009, 91-B, 987-996. [CrossRef]
- Sun, Y.; Feng Y Fau—Zhang, C.Q.; Zhang Cq Fau—Chen, S.B.; Chen Sb Fau—Cheng, X.G.; Cheng, X.G. The regenerative effect of platelet-rich plasma on healing in large osteochondral defects.
- Galasso, O.; Mariconda, M.; Romano, G.; Capuano, N.; Romano, L.; Iannò, B.; Milano, C. Expandable intramedullary nailing and platelet rich plasma to treat long bone non-unions. J Orthop Traumatol 2008, 9, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Kanthan, S.R.; Kavitha, G.; Addi, S.; Choon, D.S.; Kamarul, T. Platelet-rich plasma (PRP) enhances bone healing in non-united critical-sized defects: a preliminary study involving rabbit models. Injury 2011, 42, 782–789. [Google Scholar] [CrossRef] [PubMed]
- Calori, G.M.; Tagliabue, L.; Gala, L.; d’Imporzano, M.; Peretti, G.; Albisetti, W. Application of rhBMP-7 and platelet-rich plasma in the treatment of long bone non-unions: a prospective randomised clinical study on 120 patients. Injury 2008, 39, 1391–1402. [Google Scholar] [CrossRef] [PubMed]
- Roldán, J.C.; Jepsen, S.; Miller, J.; Freitag, S.; Rueger, D.C.; Açil, Y.; Terheyden, H. Bone formation in the presence of platelet-rich plasma vs. bone morphogenetic protein-7. Bone 2004, 34, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, L.; Priddy, L.B.; Esancy, C.; Klosterhoff, B.S.; Stevens, H.Y.; Tran, L.; Guldberg, R.E. Delivery vehicle effects on bone regeneration and heterotopic ossification induced by high dose BMP-2. Acta Biomater 2017, 49, 101–112. [Google Scholar] [CrossRef] [PubMed]
- James, A.W.; LaChaud, G.; Shen, J.; Asatrian, G.; Nguyen, V.; Zhang, X.; Ting, K.; Soo, C. A Review of the Clinical Side Effects of Bone Morphogenetic Protein-2. Tissue Eng Part B Rev 2016, 22, 284–297. [Google Scholar] [CrossRef] [PubMed]
- Baltzer, A.W.; Moser, C.; Jansen, S.A.; Krauspe, R. Autologous conditioned serum (Orthokine) is an effective treatment for knee osteoarthritis. Osteoarthritis Cartilage 2009, 17, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Meijer, H.; Reinecke, J.; Becker, C.; Tholen, G.; Wehling, P. The production of anti-inflammatory cytokines in whole blood by physico-chemical induction. Inflamm Res 2003, 52, 404–407. [Google Scholar] [CrossRef] [PubMed]
- Frizziero, A.; Giannotti, E.; Oliva, F.; Masiero, S.; Maffulli, N. Autologous conditioned serum for the treatment of osteoarthritis and other possible applications in musculoskeletal disorders. Br Med Bull 2013, 105, 169–184. [Google Scholar] [CrossRef] [PubMed]
- Darabos, N.; Haspl, M.; Moser, C.; Darabos, A.; Bartolek, D.; Groenemeyer, D. Intraarticular application of autologous conditioned serum (ACS) reduces bone tunnel widening after ACL reconstructive surgery in a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc 2011, 19 Suppl 1, S36–S46. [Google Scholar] [CrossRef] [PubMed]
- Goldring, M.B.; Berenbaum, F. Emerging targets in osteoarthritis therapy. Curr Opin Pharmacol 2015, 22, 51–63. [Google Scholar] [CrossRef] [PubMed]
- Vitali, M.; Ometti, M.; Drossinos, A.; Pironti, P.; Santoleri, L.; Salini, V. Autologous conditioned serum: clinical and functional results using a novel disease modifying agent for the management of knee osteoarthritis. J Drug Assess 2020, 25, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Cheng, P.-G.; Yang, K.D.; Huang, L.-G.; Wang, C.-H.; Ko, W.-S. Comparisons of Cytokines, Growth Factors and Clinical Efficacy between Platelet-Rich Plasma and Autologous Conditioned Serum for Knee Osteoarthritis Management. Biomolecules 2023, 13, 555. [Google Scholar] [CrossRef] [PubMed]
- Bishop, J.A.; Palanca, A.A.; Bellino, M.J.; Lowenberg, D.W. Assessment of compromised fracture healing. J Am Acad Orthop Surg 2012, 20, 273–282. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, B.; Wragg, N.M.; Wilson, S.L. The use of PRP injections in the management of knee osteoarthritis. Cell Tissue Res 2019, 376, 143–152. [Google Scholar] [CrossRef] [PubMed]
- Alsousou, J.; Thompson, M.; Hulley, P.; Noble, A.; Willett, K. The biology of platelet-rich plasma and its application in trauma and orthopaedic surgery: a review of the literature. J Bone Joint Surg Br 2009, 91, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Bleek, K.; Schell, H.; Schulz, N.; Hoff, P.; Perka, C.; Buttgereit, F.; Volk, H.D.; Lienau, J.; Duda, G.N. Inflammatory phase of bone healing initiates the regenerative healing cascade. Cell Tissue Res 2012, 347, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Ganji, E.; Killian, M.L. Tendon healing in the context of complex fractures. Clin Rev Bone Miner Metab 2018, 16, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Ghaffarpasand, F.; Shahrezaei, M.; Dehghankhalili, M. Effects of Platelet Rich Plasma on Healing Rate of Long Bone Non-union Fractures: A Randomized Double-Blind Placebo Controlled Clinical Trial. Bull Emerg Trauma 2016, 4, 134–140. [Google Scholar] [PubMed]
- Li, S.; Xing, F.; Luo, R.; Liu, M. Clinical Effectiveness of Platelet-Rich Plasma for Long-Bone Delayed Union and Nonunion: A Systematic Review and Meta-Analysis. Front Med (Lausanne) 2021, 8, 771252. [Google Scholar] [CrossRef] [PubMed]
- Andersen, C.; Wragg, N.M.; Shariatzadeh, M.; Wilson, S.L. The Use of Platelet-Rich Plasma (PRP) for the Management of Non-union Fractures. Curr Osteoporos Rep 2021, 19, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Labibzadeh, N.; Emadedin, M.; Fazeli, R.; Mohseni, F.; Hosseini, S.E.; Moghadasali, R.; Mardpour, S.; Azimian, V.; Ghorbani Liastani, M.; Mirazimi Bafghi, A.; et al. Mesenchymal Stromal Cells Implantation in Combination with Platelet Lysate Product Is Safe for Reconstruction of Human Long Bone Nonunion. Cell J 2016, 18, 302–309. [Google Scholar] [CrossRef]
- Centeno, C.; Schultz, J.; Cheever, M.; Freeman, M.; Robinson, B.; Faulkner, S. A case series of percutaneous treatment of non-union fractures with autologous, culture expanded, bone marrow derived, mesenchymal stem cells and platelet lysate. J Bioengineer & Biomedical Sci S 2011, 2, 2. [Google Scholar]
- Vauclair, F.; Goetti, P.; Nguyen, N.T.V.; Sanchez-Sotelo, J. Distal humerus nonunion: evaluation and management. EFORT Open Reviews 2020, 5, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Helfet, D.L.; Kloen, P.; Anand, N.; Rosen, H.S. Open reduction and internal fixation of delayed unions and nonunions of fractures of the distal part of the humerus. J Bone Joint Surg Am 2003, 85, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Vauclair, F.; Goetti, P.; Nguyen, N.T.V.; Sanchez-Sotelo, J. Distal humerus nonunion: evaluation and management. EFORT Open Rev 2020, 5, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Zaidenberg, E.E.; Juarez Cesca, F.; Pastrana, M.J.; Zaidenberg, C.R. Pedicled Vascularized Bone Graft of the Distal Radius for Recalcitrant Nonunion of the Distal Humerus.
- Frölke, J.P.; Patka, P. Definition and classification of fracture non-unions. Injury 2007, 38 Suppl 2, S19–S22. [Google Scholar] [CrossRef] [PubMed]
- Schmal, H.; Brix, M.; Bue, M.; Ekman, A.; Ferreira, N.; Gottlieb, H.; Kold, S.; Taylor, A.; Toft Tengberg, P.; Ban, I. Nonunion—consensus from the 4th annual meeting of the Danish Orthopaedic Trauma Society. EFORT Open Rev 2020, 5, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Ku, K.H.; Baek, J.H.; Kim, M.S. Risk Factors for Non-Union after Open Reduction and Internal Fixation in Patients with Distal Humerus Fractures. J Clin Med 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Froum, S.J.; Wallace, S.S.; Tarnow, D.P.; Cho, S.C. Effect of platelet-rich plasma on bone growth and osseointegration in human maxillary sinus grafts: three bilateral case reports. Int J Periodontics Restorative Dent 2002, 22, 45–53. [Google Scholar] [PubMed]
- Raghoebar, G.M.; Schortinghuis, J.; Liem, R.S.; Ruben, J.L.; van der Wal, J.E.; Vissink, A. Does platelet-rich plasma promote remodeling of autologous bone grafts used for augmentation of the maxillary sinus floor? Clin Oral Implants Res 2005, 16, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Bielecki, T.; Gazdzik, T.S.; Szczepanski, T. Benefit of percutaneous injection of autologous platelet-leukocyte-rich gel in patients with delayed union and nonunion. Eur Surg Res 2008, 40, 289–296. [Google Scholar] [CrossRef]
- Mariconda, M.; Cozzolino, F.; Cozzolino, A.; D’Agostino, E.; Bove, A.; Milano, C. Platelet gel supplementation in long bone nonunions treated by external fixation. J Orthop Trauma 2008, 22, 342–345. [Google Scholar] [CrossRef] [PubMed]
- Subramanyam, K.; Alguvelly, R.; Mundargi, A.; Khanchandani, P. Single versus multi-dose intra-articular injection of platelet rich plasma in early stages of osteoarthritis of the knee: A single-blind, randomized, superiority trial. Arch Rheumatol 2021, 36, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Say, F.; Türkeli, E.; Bülbül, M. Is platelet-rich plasma injection an effective choice in cases of non-union? Acta Chir Orthop Traumatol Cech 2014, 81, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.J.; Tan, X.X.; Ju, H.Y.; Su, J.P.; Yan, W.; Song, X.G.; Qin, L.W.; Ju, C.J.; Wang, L.S.; Zou, D.B. Autologous platelet lysates local injections for treatment of tibia non-union with breakage of the nickelclad: a case report. Springerplus 2016, 5, 2013. [Google Scholar] [CrossRef] [PubMed]
- Casati, L.; Celotti, F.; Negri-Cesi, P.; Sacchi, M.C.; Castano, P.; Colciago, A. Platelet derived growth factor (PDGF) contained in Platelet Rich Plasma (PRP) stimulates migration of osteoblasts by reorganizing actin cytoskeleton. Cell Adhesion & Migration 2014, 8, 595–602. [Google Scholar] [CrossRef]
- Schell, H.; Duda, G.N.; Peters, A.; Tsitsilonis, S.; Johnson, K.A.; Schmidt-Bleek, K. The haematoma and its role in bone healing. J Exp Orthop 2017, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Santolini, E.; West, R.; Giannoudis, P.V. Risk factors for long bone fracture non-union: a stratification approach based on the level of the existing scientific evidence. Injury 2015, 46 Suppl 8, S8–S19. [Google Scholar] [CrossRef]
- Ju, Y.; Hu, Y.; Yang, P.; Xie, X.; Fang, B. Extracellular vesicle-loaded hydrogels for tissue repair and regeneration. Mater Today Bio 2023, 18, 100522. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Case 1 is a 50-year-old female had non-union tibial fracture. (a) the failure of plate implant; (b) patient had received revisional intramedullary nail fixation; (c) the fracture had not healed 9 months after the revision intramedullary nailing; (d) three months after the 3rd injection of ACS with good union.
Figure 1.
Case 1 is a 50-year-old female had non-union tibial fracture. (a) the failure of plate implant; (b) patient had received revisional intramedullary nail fixation; (c) the fracture had not healed 9 months after the revision intramedullary nailing; (d) three months after the 3rd injection of ACS with good union.
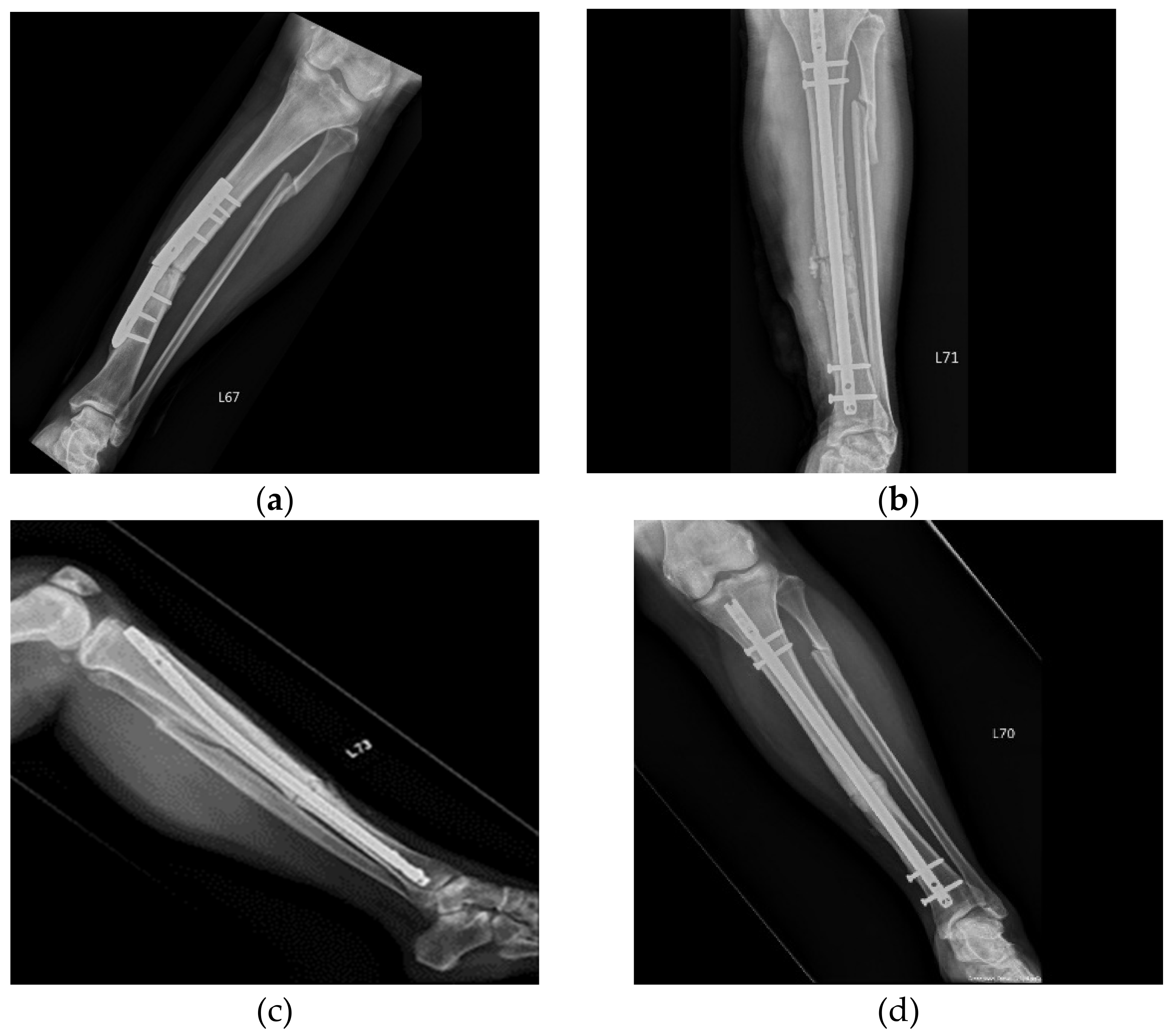
Figure 2.
Case 4 is a 39-year-old female treated by ACS due to a non-union clavicle fracture for 9 months after ORIF. (a) Before ACS treatment, the defect was visible; (b) one month after the 2nd injection. Complete bone healing indicated the excellent efficacy of ACS.
Figure 2.
Case 4 is a 39-year-old female treated by ACS due to a non-union clavicle fracture for 9 months after ORIF. (a) Before ACS treatment, the defect was visible; (b) one month after the 2nd injection. Complete bone healing indicated the excellent efficacy of ACS.
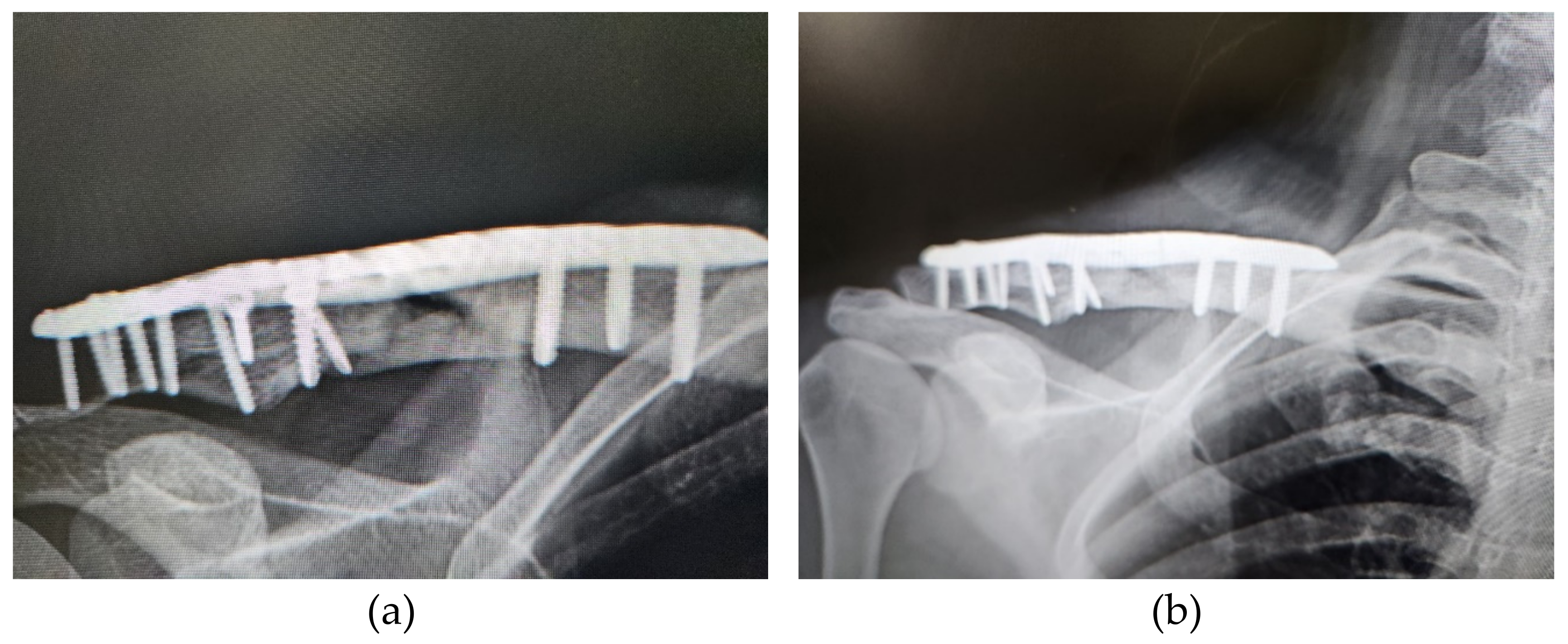
Figure 3.
Case 6 is a 34-year-old male treated by ACS due to non-union femur fracture for 9 months after ORIF with plate fixation. (a) Before ACS treatment, the defect was visible; (b) one month after the 3rd injection; (c) radiographic results one year after the 3rd injection showed complete healing of the bone defect.
Figure 3.
Case 6 is a 34-year-old male treated by ACS due to non-union femur fracture for 9 months after ORIF with plate fixation. (a) Before ACS treatment, the defect was visible; (b) one month after the 3rd injection; (c) radiographic results one year after the 3rd injection showed complete healing of the bone defect.
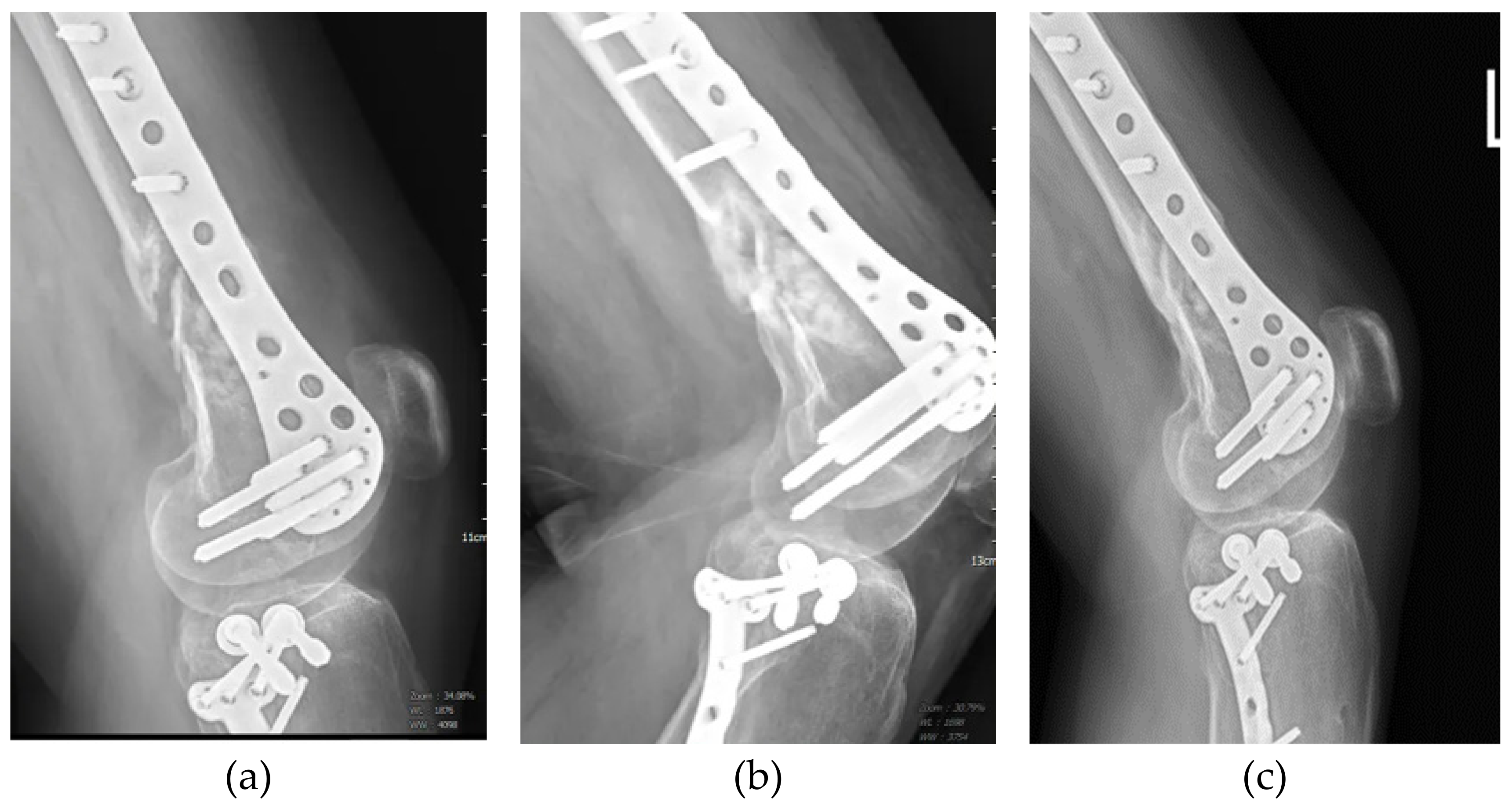
Figure 4.
Case 11 is a 27-year-old male who suffered by non-union left radial and ulnar shaft fracture after ORIF. (a) Before ACS treatment, obvious defects of both bones were found; (b) one-month after the 3rd injection by radiographic evaluation.
Figure 4.
Case 11 is a 27-year-old male who suffered by non-union left radial and ulnar shaft fracture after ORIF. (a) Before ACS treatment, obvious defects of both bones were found; (b) one-month after the 3rd injection by radiographic evaluation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



