
Submitted:
12 August 2024
Posted:
13 August 2024
You are already at the latest version
Abstract
Objectives: The tau protein is essential for stabilizing microtubules. Changes in its phosphorylation are identified in many neurodegenerative diseases, such as frontotemporal dementia and Alzheimer's disease. The hyperphosphorylation of the tau protein is linked to various factors, including stress, which has a substantial impact on depressive illness. The present study aimed to systematically review studies that describe the association between tau protein and depression.Design: The present study used the PRISMA statement 2020 as the inclusion criterion for articles describing tau protein in individuals with depression. The exclusion criterion was the lack of comparison of tau protein levels with individuals without depression.Results: A total of 138 papers were identified, of which 21 were ultimately included. One out of every three articles included demonstrated the statistical significance of the tau protein values between the depression group and controls. Only one had an adequate sample but demonstrated results without any major significance.Conclusions: The association between tau protein and depression remains unclear. Studies with adequate sampling are necessary to answer this question.
Keywords:
tau
; tau proteins
; tauopathies
; depression
; systematic review
1. Introduction
The tau protein was identified in 1975 in the laboratory of the Department of Biochemistry at Princeton University in New Jersey as a factor associated with tubulin in the microtubules of neurons [1]. They determined that tubulin cannot promote the elongation of microtubules without the tau protein [2].
Depression has been described as melancholia since Hippocrates’ time (370-460 B.C.) [3]. It was described as a nosological entity by the Scottish doctor William Cullen in 1780 [4]. From 1860 onwards, references to depression as a symptom of melancholia began to appear [5]. In 1899, Kraepelin used the term depression for the first time as a disease in the group of manic-depressive psychosis [6]. By the 1960s, depression was verified in two forms, one unipolar and the other bipolar [7]. Within unipolar depression, some classification subdivisions have been proposed, with Major Depressive Disorder (MDD) being the most important in the context of this review.
Tau is synthesized by the microtubule-associated protein tau gene (MAPT) and was kwon six isoforms expressed in the adult human brain ranging from 352 to amino acids in length. The proteins vary due to one or two inserts in the N-terminal and the C-terminal half. The insert in the C-terminal half codes for a repeat of 31 amino acids. As a result, there are three isoforms with four repeats (4R) and three isoforms with three repeats (3R). These repeats, along with adjacent sequences, are essential components of the microtubule-binding domains of tau.[8]
Tau protein plays a role in stabilizing microtubules and contributes to transporting nutrients and other substances along neurons. The binding of tau protein to microtubules is regulated by negative phosphorylation. Mutations in MAPT can alter the phosphorylation of tau protein, promote difficulty in binding to microtubules, and lead to the formation of neurofibrillary aggregates.[9] Tau protein hyperphosphorylation has been linked to numerous diseases such as diabetes, Parkinson's disease, Huntington's disease, Pick's disease, etc [10]. Alzheimer's disease is the best-documented disease in which tau protein plays a pathophysiological role [11].
The process of neuronal damage by the tau protein begins with its hyperphosphorylation. Numerous factors seem to collaborate in causing an imbalance between the elements that trigger tau hyperphosphorylation and those responsible for its dephosphorylation. Most hyperphosphorylation promoters hyperactivate glycogen synthase kinase-3β (GSK-3β) and inhibit PP2A phosphatase, promoting an imbalance between phosphorylation mechanisms [12]. Hyperphosphorylated tau protein accumulates in neurofilaments and destabilizes microtubules with consequent neuronal atrophy and death.
Depression is associated with the hypofunction of brain neurocircuits due to synaptic damage. The primary neurotransmitter linked to depression is serotonin [13]. Subsequently, many other neurotransmitters were associated with depression, such as norepinephrine, dopamine, glutamate, and GABA. Changes in neurotransmitters result from epigenetic, neuroendocrine, and inflammatory changes triggered by stress or other aggressive agents, such as SARS-CoV-2 [14,15].
The relationship between depression and inflammatory processes is complex, demonstrating a bidirectional relationship where depression activates inflammatory mechanisms and vice versa. Proinflammatory cytokines and acute phase proteins are increased in MDD, as are monocyte and macrophage activations, with substantial participation of microglia.[16]
The central genes associated with stress and depression are NR3C1, FKPB 5, SLC6A4, BDNF, SKA2, OXTR, LINGO3, POU3F1, and ITGB1 [17]. Stress can boost the activity of GSK-3β, resulting in epigenetic changes and pathogenic inflammation in Depression [18]. Chronic stress increases the functioning of neurocircuitry from the prefrontal cortex to the amygdala and hippocampus and increases the production and release of corticosteroids and insulin.[19] Another hormone implicated in the pathophysiology of depression is ghrelin, which appears to exert an antidepressant function.[20]
These hormonal changes will interfere with the functioning of GSK-3β and increase the hyperphosphorylation of tau protein.[21] The homeostatic objective of increasing tau protein hyperphosphorylation is to reduce neurotransmission and decrease the perception of persistent unpleasant stimuli.[22] (Figure 1)
GSK-3β could be a convergent point with tau hyperphosphorylation and depression. Understanding the physiopathology of stress is valuable for improving prevention strategies for neurodegenerative diseases in the elderly. This review aims to explore existing literature to identify studies addressing the potential correlation between tau and depression.
The physiological stress response can have profound implications for an individual's well-being. Elevated levels of stress hormones, such as glucocorticoids and insulin, can induce a state of hypervigilance, which in turn accelerates communication between specific brain regions, culminating in heightened psychological discomfort. Moreover, increased levels of insulin and glucocorticoids may induce hyperphosphorylation of tau protein, leading to the destabilization of microtubules. This instability can subsequently attenuate the speed of neurotransmission, potentially reducing psychological suffering to restore equilibrium.
2. Method
This study used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement, updated guideline 2020 [23]. (Figure 2)
On April 1, 2024, it was searched electronic websites (PubMed, Embase, and Scielo) using the MeSH Terms (Emtree – major focus exploded) [“tau” and “depression”] or [“tau protein” and “depression”] or [“tau proteins” and “depression”]. No time type of publication or language limitations were used. All articles were read in full by one of the authors and the other two read all abstracts.
The question (PECOS) under study was: Do individuals (P) exposed to high levels of Tau protein (E), compared to individuals with normal levels of Tau protein (C), exhibit a higher prevalence of depression (O)? Case-control studies and other kinds of study that discriminate between the control group and case of depression(S) were selected, with the inclusion criterion for articles describing tau protein in individuals with depression and the exclusion criterion being the lack of comparison of tau protein levels with individuals without depression.
3. Results
One hundred and thirty-eight articles were found, eighteen of which were repeated. One was written in Spanish, one in German, four in Mandarin, and the others in English. All were read in full by one of the authors, and two read all abstracts. The two co-authors who read all the abstracts agreed to exclude 42 articles for not meeting the inclusion criteria. Reading the four articles written in Chinese with the help of AI Chat. The author, who read all the articles in full, agreed with excluding 42 articles and noted the inappropriateness of another 57, including 21 for data extraction. (Table 1 and Table 2)
This study included data for 2.300 individuals (707 with MDD and 1,593 without MDD). Seven studies were found showing significant statistical differences in tau levels between depression and controls. Andreasen et al observed that CSF-tau was increased in probable (690 ± 341 pg/mL; p < 0.0001) and possible (661 ± 447 pg/mL; p < 0.0001) AD, but not in depression (231 ± 110 pg/mL) compared with control subjects (227 ± 101 pg/mL); however, the patients with depression showed a significant correlation (r = 0.96, p < 0.0001) between baseline and follow-up of 6 to 9 months, without intervention, CSF-tau levels, with a coefficient of variance (CV) of 9.4%, with mean percentage change in CSF-tau between baseline and follow-up was 96.9 pg/mL ±16.8% in depression [24]. Buerger et al described P-tau231 levels were higher in Major Depression patients than in healthy comparison subjects (Mann-Whitney U=226, df=1, p<0.05) [25]. Kumar et al detected the global [18F]FDDNP binding value significantly higher in the depression group (n = 20) when compared with that of controls (n = 19) with significant group differences in global [18F]FDDNP binding levels (Cohen d effect size of 1.12, p =.03), as well as in PC binding (Cohen d effect size of 1.07, p =.04) [30]. Pomara et al observed a significant correlation compared baseline and follow-up of depressive patients versus health controls between CSF Aβ40 and T-tau levels (r=.586, p=.011), between CSF Aβ42 and T-tau levels (r=.557, p=.016) and did not observe a significant correlation between CSF Aβ40 or Aβ42 and P-tau levels (p>.700) in the same groups [34]. Gonzales et al found higher P-tau and T-tau levels comparing chronic subsyndromal symptoms of depression with health controls, however, in the fully adjusted models for age, there were no significant group differences for P-tau (β = 2.584, p =.392) or T-tau (β = 4.676, p =.497) [35]. Babulal et al demonstrated an odds ratio (OR) of 2.42 (CI=1.14 - 5.14; p = .021) for the presence of tau elevated in Positron Emission Tomography to be depression.[37] Moriguchi et al showed mean cortical SUVRs for [11C]PBB3, which followed a normal distribution with a Kolmogorov–Smirnov test (p > 0.05), and there was no violation of the equal variance assumption with a Levene’s test (p > 0.05), in patients were higher than those in healthy controls [t(38)=2.46, p= 0.02] [40].
4. Discussion
According to the prevalence of depression, studies should contain 160 participants [45]. Most studies were carried out with a small sample size. Only five studies had an adequate sample. Among these, the study by Gonzales et al (depression with an n = 80 and controls with an n = 158) demonstrated a statistically significant difference between P-tau (p = .004). The study by Bubalat et al had an inadequate distribution between the numbers of depression (n = 38) and controls (n = 263), yet it demonstrated an association between tau and depression. The study by Liu et al had a reasonable sample size (n = 139) and demonstrated no statistical difference. The study by Chan et al had an inadequate distribution between the numbers of depression (n = 30) and controls (n = 169) and demonstrated no statistical difference. The study by Schuurmans et al had an inadequate distribution between the numbers of depression (n = 51) and controls (n = 439) and demonstrated no statistical difference.
Thus, Gonzales' study seems to be the only one capable of producing reliable results. However, their findings seem conflicting since adjusting for age did not maintain the statistical difference found.
Brown et al.'s 2016 review found 11 articles comparing tau and depression directly [46]. Of these, three were not seen by our search tools [47,48,49]. Reading them in full, we did not find an adequate comparison between depression and tau, considering that they were explicitly designed for other purposes. This way, even if found in our search tools, they would be excluded, and we would have no difference in our results. The other eight articles from that review are among the 21 included in this study.
The best approach to determine if there is a connection between tau protein and depression is through follow-up studies. Cross-sectional measurements are unlikely to reveal significant differences between groups with depression and healthy controls. The buildup of tau protein may be only evident in cases of chronic depression, necessitating longitudinal studies to compare with healthy controls. If depression is indeed linked to tau protein accumulation, patients may experience cognitive decline, which could complicate the analysis. Therefore, patients with depression who develop tau protein accumulation may be diagnosed with MCI or AD, making it impractical to measure this in a cross-sectional study.
Depression is linked to long-term stress. The capacity to be resilient to stress varies from person to person and can be influenced by genetics, diet, exercise, and other health conditions [50]. To understand the potential connection between protein and depression, it's essential to identify which groups are most vulnerable.
5. Conclusion
The current body of research concerning the association between depression and tau protein is limited to a single comprehensive study. Consequently, our understanding of the central focus of our research remains uncertain. It is imperative to conduct studies with enough participants, ensuring even distribution between case and control groups, aiming to facilitate the generation of precise conclusions. Moreover, prioritizing follow-up studies is crucial in delineating the relationship between depression and tau protein.
Author Contributions
Juliano Flávio Rubatino Rodrigues helped define the research criteria, searched online platforms, read all the articles, extracted the data, and wrote the text. Lívia Peregrino Rodrigues read all the abstracts and selected the articles to be included in this review, proofreading the English after all the written text and drawing Figure 1. Franciany Cunha Peregrino Rodrigues read all the abstracts and selected the articles to be included and excluded from this review. Fernando Victor Martins Rubatino helped extract data from selected articles and contributed to writing the introduction and discussion of this article. Kelly Cristina Atalaia da Silva contributed to writing the introduction and discussion of this article. María Fernanda Serna Rodriguez supervised the scientific nature of this review. Hannes Fischer contributed with arguments and translation of excerpts from German. Pedro Marco Karan Barbosa monitored the methodology. Spencer Luiz Marques Payão contributed to the theoretical argument. Moacir Fernandes de Godoy defined the terms of this review and supervised the methodology. Gerardo Maria de Araújo Filho guided the entire review.
Funding
The authors' resources were used.
Acknowledgments
We thank CAPES for providing access to article search platforms.
Conflicts of interest
The authors declare no conflicts of interest with the present study.
References
- Weingarten, M.D.; Lockwood, A.H.; Hwo, S.-Y.; Kirschner, M.W. A Protein Factor Essential for Microtubule Assembly. Proc Nat Acad Sci USA 1975, 72, 1858–1862. [Google Scholar] [CrossRef] [PubMed]
- Witman, G.B.; Cleveland, D.W.; Weingarten, M.D.; Kirschner, M.W. Tubulin requires tau for growth onto microtubule initiating sites. Proc Natl Acad Sci USA 1976, 73, 4070–4074. [Google Scholar] [CrossRef]
- Sadeghfard, A.; Bozorgi, A.R.; Ahmadi, S.; Shojaei, M. The History of Melancholia Disease. Iran J M Sci 2016, 41, 75. [Google Scholar]
- Cullen, G. Synopsis Nosologiæ Methoticæ, 3rd ed.; Edinburg Press: London, UK, 1780; p. 349. [Google Scholar]
- Mayne, R.G. An Expository Lexion of the Terms, Ancient and Modern, in Medical and General Science; Churchill: London, 1860. [Google Scholar]
- Kendler, K.S. The genealogy of major depression: symptoms and signs of melancholia from 1880 to 1900. Mol Psychiatry 2017, 22, 1539–1555. [Google Scholar] [CrossRef] [PubMed]
- Perris, C. A study of a bipolar (manic-depressive) and unipolar recurrent depressive psychosis. Introduction. Acta Psychiatr Scand Suppl 1966, 9–14. [Google Scholar] [CrossRef]
- Qi, C.; Lövestam, S.; Murzin, A.; Peak-Chew, S.; Franco, C.; Bogdani, M.; Latimer, C.; Murrell, J.; Cullinane, P.; Jaunmuktane, Z.; et al. Tau filaments with the Alzheimer fold in cases with MAPT mutations V337M and R406W. bioRxiv. PrePrint 2024. [Google Scholar] [CrossRef]
- Zheng, H.; Sun, H.; Cai, Q.; Tai, H.C. The Enigma of Tau Protein Aggregation: Mechanistic Insights and Future Challenges. Int J Mol Sci 2024, 25, 4969. [Google Scholar] [CrossRef] [PubMed]
- Goedert, M.; Spillantini, M.G. Ordered Assembly of Tau Protein and Neurodegeneration. In Tau Biology, Takashima, A., Ed. Springer: Singapore, 2019; Volume 1184, pp. 3–21.
- Watanabe, H.; Bagarinao, E.; Yokoi, T.; Yamaguchi, H.; Ishigaki, S.; Mausuda, M.; Katsuno, M.; Soube, G. Tau Accumulation and Network Breakdown in Alzheimer's Disease. In Tau Biology, Takashima, A., Ed. Springer: Singapore, 2019; Volume 1184, pp. 231–240.
- Gratuze, M.; Joly-Amado, A.; Buee, L.; Vieau, D.; Blum, D. Tau, Diabetes and Insulin. In Tau Biology, Takashima, A., Ed.; Springer: Singapore, 2019; Volume 1184, pp. 259–287. [Google Scholar]
- Naumenko, V.S.; Popova, N.K.; Lacivita, E.; Leopoldo, M.; Ponimaskin, E.G. Interplay between Serotonin 5-HT1A and 5-HT7 Receptors in Depressive Disorders. CNS Neursci Therap 2014, 20, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Mei, B.; Wang, P.; Li, X.; Chen, X.; Wei, G.; Kuang, F.; Li, B.; Su, S. Prevalence and risk factors for persistent symptoms after COVID-19: a systematic review and meta-analysis. Clin Microbiol Infect 2024, 30, 328–335. [Google Scholar] [CrossRef]
- Bertollo, A.G.; Galvan, A.C.L.; Dallagnol, C.; Cortez, A.D.; Ignácio, Z.M. Early Life Stress and Major Depressive Disorder-An Update on Molecular Mechanisms and Synaptic Impairments. Mol Neurobiol 2024. [Google Scholar] [CrossRef]
- Beurel, E.; Toups, M.; Nemeroff, C.B. The Bidirectional Relationship of Depression and Inflammation: Double Trouble. Neuron 2020, 107, 234–256. [Google Scholar] [CrossRef]
- Bernad, B.-C.; Tomescu, M.-C.; Anghel, T.; Lungeanu, D.; Enătescu, V.; Bernard, E.S.; Nicoras, V.; Arnautu, D.-A.; Hogea, L. Epigenetic and Coping Mehcanisms of Stress in Affective Disorders: A Scoping Review. Medicina 2024, 60. [Google Scholar] [CrossRef] [PubMed]
- McCallum, R.T.; Perreault, M.L. Glycogen Synthase Kinase-3: A Focal Point for Advancing Pathogenic Inflammation in Depression. Cells 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Sheynin, J.; Liberzon, I. Circuit dysregulation and circuit-based treatments in posttraumatic stress disorder. Neurosci Lett 2017, 649, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Lis, M.; Miłuch, T.; Majdowski, M.; Zawodny, T. A link between ghrelin and major depressive disorder: a mini review. Front Psychiatry 2024, 15, 1367523. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Gong, W.G.; Wang, Y.J.; Sun, J.J.; Zhou, H.; Zhang, Z.J.; Ren, Q.G. Escitalopram alleviates stress-induced Alzheimer's disease-like tau pathologies and cognitive deficits by reducing hypothalamic-pituitary-adrenal axis reactivity and insulin/GSK-3β signal pathway activity. Neurobiol Aging 2018, 67, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Lozupone, M.; Bellomo, A.; Imbimbo, B.P. Do anti-amyloid- β drugs affect neuropsychiatric status in Alzheimer's disease patients? Ageing Research Reviews 2019, 55, 100948. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, N.; Minthon, L.; Clarberg, A.; Davidsson, P.; Gottfries, J.; Vanmechelen, E.; Vanderstichele, H.; Winblad, B.; Blennow, K. Sensitivity, specificity, and stability of CSF-tau in AD in a community-based patient sample. Neurology 1999, 53, 1488–1494. [Google Scholar] [CrossRef]
- Buerger, K.; Zinkowski, R.; Teipel, S.; Arai, H.; DeBernardis, J.; Kerkman, D.; McCulloch, C.; Padberg, F.; Faltraco, F.; Goernitz, A.; et al. Differentiation of Geriatric Major Depression From Alzheimer's Disease With CSF Tau Protein Phosphorylated at Threonine 231. Am J Psychiatry 2003, 160, 376–379. [Google Scholar] [CrossRef]
- Schönknecht, P.; Pantel, J.; Hartmann, T.; Werle, E.; Volkmann, M.; Essig, M.; Amann, M.; Zanabili, N.; Bardenheuer, H.; Hunt, A.; et al. Cerebrospinal fluid tau levels in Alzheimer's disease are elevated when compared with vascular dementia but do not correlate with measures of cerebral atrophy. Psychiatry Research 2003, 120, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Blasko, I.; Lederer, W.; Oberbauer, H.; Walch, T.; Kemmler, G.; Hinterhuber, H.; Marksteiner, J.; Humpel, C. Measurement of Thirteen Biological Markers in CSF of Patients with Alzheimer's Disease and Other Dementias. Dement Geriatr Cogn Disord 2006, 21, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Schönknecht, P.; Pantel, J.; Kaiser, E.; Thomann, P.; Schröder, J. Increased tau protein differentiates mild cognitive impairment from geriatric depression and predicts conversion to dementia. Neuroscience Letters 2007, 416, 39–42. [Google Scholar] [CrossRef]
- Gudmundsson, P.; Skoog, I.; Waern, M.; Blennow, K.; Pálsoon, S.; Rosengren, L.; Gustafson, D. The Relationship Between Cerebrospinal Fluid Biomarkers and Depression in Elderely Women. Am J Geriatr Psychiatry 2007, 15, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Kepe, V.; Barrio, J.R.; Siddarth, P.; Manoukian, V.; Elderkin-Thompson, V.; Small, G.W. Protein Binding in Patients With Late-Life Depression. Arch Gen Psychiatry 2011, 68, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Reis, T.; Brandão, C.O.; Coutinho, E.S.F.; Engelhardt, E.; Laks, J. Cerebrospinal Fluid Biomarkers in Alzheimer's Disease and Geriatric Depression: Preliminary Finding from Brazil. CNS Neuroscience & Therapeutics 2012, 18, 524–529. [Google Scholar] [CrossRef]
- Pomara, N.; Bruno, D.; Sarreal, A.S.; Hernando, R.T.; Nierenberg, J.; Petkova, E.; Sidtis, J.J.; Wisniewski, T.M.; Mehta, P.D.; Pratico, D.; et al. Lower CSF Amyloid Beta Peptides and Higher F2-Isoprostanes in Cognitively Intact Elderly Individuals With Major Depressive Disorder. Am J Psychiatry 2012, 169, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Diniz, B.S.; Teixeira, A.L.; Machado-Vieira, R.; Talib, L.L.; Radanovic, M.; Gattaz, W.F.; Forlenza, O.V. Reduced Cerebrospinal Fluid Levels of Brain-Derived Neurotrophic Factor Is Associated With Cognitive Impairment in Late-Life Major Depression. Journals of Gerontology, Series B: Psychological Sciences and Social Sciences 2014, 69, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Pomara, N.; Bruno, D.; Osorio, R.S.; Reichert, C.; Nierenberg, J.; Sarreal, A.S.; Hernando, R.T.; Marmar, C.R.; Wisniewski, T.; Zetterberg, H.; et al. State-dependent alterations in CSF Abeta42 levels in cognitively intact elderly with late life major depression. Neuroreport 2016, 27, 1068–1071. [Google Scholar] [CrossRef]
- Gonzales, M.M.; Insel, P.S.; Nelson, C.; Touson, D.; Schöll, M.; Mattsson, N.; Sacuiu, S.; Bickford, D.; Weiner, M.W.; Mackin, R.S. Chronic depressive symptomatology and CSF amyloid beta and tau levels in mild cognitive impairment. Int J Geriatr Psychiatry 2017, gps.4926. [Google Scholar] [CrossRef]
- Liguori, C.; Pierantozzi, M.; Chiaravalloti, A.; Sancesario, G.M.; Mercuri, N.B.; Franchini, F.; Schillaci, O.; Sancesario, G. When Cognitive Decline and Depression Coexist in the Elderly: CSF Biomarkers Analysis Can Differentiate Alzheimer's Disease from Late-Life Depression. Frontiers in Aging Neuroscience 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Babulal, G.M.; Roe, C.M.; Stout, S.H.; Rajasekar, G.; Wisch, J.K.; Benzinger, T.L.S.; Morris, J.C.; Ances, B.M. Depression is Associated with Tau and Not Amyloid Poisitron Emission Tomography in Cognitively Normal Adults. J Alzheimer Dis 2020, 74, 1045–1055. [Google Scholar] [CrossRef]
- Liu, F.-r.; Yang, L.-y.; Zheng, H.-f.; Zhou, Y.; Chen, B.-b.; Xu, H.; Zhang, Y.-w.; Shen, D.-y. Plasma levels of Interleukin 18 but not amyloid-B or Tau are elevated in female depressive patients. Comprehensive Psychiatry 2020, 97, 1521159. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, J.C.; Stella, F.; Pais, M.V.; Radanovic, M.; Canineu, P.R.; Joaquim, H.P.G.; Talib, L.L.; Forlenza, O.V. Cognitive impairment in remitted late-life depression is not associated with Alzheimer's disease-related CSF biomarkers. Journal of Affective Disorders 2020, 272, 409–416. [Google Scholar] [CrossRef]
- Moriguchi, S.; Takahata, K.; Shimada, H.; Kubota, M.; Kitamura, S.; Kimura, Y.; Tagai, K.; Tarumi, R.; Tabuchi, H.; Meyer, J.H.; et al. Excess tau PET ligand retention in elderly patients with major depressive disorder. Mol Psychiatry 2020, 26, 5856–5863. [Google Scholar] [CrossRef]
- Chan, C.K.; Sieber, F.E.; Blennow, K.; Inouye, S.K.; Kahn, G.; Leoutsakos, J.-M.; Marcantonio, E.R.; Neufeld, K.J.; Rosenberg, P.B.; Wang, N.-Y.; et al. Association of Depression Symptoms With Postoperative Delirium and CSF Biomarkers for Alzheimer's Disease Among Hip Fracture Patients. Am J Geriatric Psychiatry 2021, 29, 1212–1221. [Google Scholar] [CrossRef] [PubMed]
- Golas, A.C.; Salwierz, P.; Rajji, T.K.; Bowie, C.R.; Butters, M.A.; Fischer, C.E.; Flint, A.J.; Herrmann, N.; Mah, L.; Mulsant, B.H.; et al. Assessing the Role of Past Depression in Patients with Mild Cognitive Impairment, with and without Biomarkers for Alzheimer's Disease. J Alzheimer's Disease 2023, 92, 1219–1227. [Google Scholar] [CrossRef]
- Salwierz, P.; Thapa, S.; Taghdiri, F.; Vasilevskaya, A.; Anastassiadis, C.; Tang-Wai, D.F.; Golas, A.C.; Tartaglia, M.C. Investigating the association between a history of depression and biomarkers of Alzheimer's disease, cerebrovascular disease, and neurodegeneration in patients with dementia. GeroScience 2024, 46, 783–793. [Google Scholar] [CrossRef]
- Schuurmans, I.K.; Ghanbari, M.; Cecil, C.; Ikram, M.A.; Luik, A.I. Plasma neurofilament light chain in association to late-life depression in the general population. Psychiatry and Clinical Nerurosciences 2024, 78, 97–103. [Google Scholar] [CrossRef]
- EL, N.; Levis, B.; Neyer, M.A.; Rice, D.B.; Booij, L.; Benedetti, A.; Thombs, B.D. Sample size and precision of estimates in studies of depression screening tool accuracy: A meta-research review of studies published in 2018-2021. Int J Methods Psychiatr Res 2022, 31, e1910. [Google Scholar] [CrossRef]
- Brown, E.E.; Iwata, Y.; Chung, J.K.; Gerretsen, P.; Graff-Guerrero, A. Tau in Late-Life Depression: A Systematic Review and Meta-Analysis. Journal of Alzheimer's Disease 2016, 54, 615–633. [Google Scholar] [CrossRef] [PubMed]
- Blennow, K.; Wallin, A.; Ågren, H.; Spenger, C.; Siegfried, J.; Vanmechelen, E. tau Protein in Cerebrospinal Fluid: A Biochemical Marker for Axonal Degeneration in Alzheimer Disease? Mol and Chemical Neuropathology 1995, 26, 231–245. [Google Scholar] [CrossRef] [PubMed]
- Hertze, J.; Minthon, L.; Zetterberg, H.; Vanmechelen, E.; Blennow, K.; Hansson, O. Evaluation of CSF Biomarkers as Predictors of Alzheimer's Disease: A Clinical Follow-Up Study of 4.7 Years. Journal of Alzheimer's Disease 2010, 21, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Madeira, C.; Lourenço, M.V.; Vargas-Lopes, C.; Suemoto, C.K.; Brandão, C.O.; Reis, T.; Leite, R.E.P.; Laks, J.; Jacob-Filho, W.; Pasqualucci, C.A.; et al. d-serine levels in Alzheimer's disease: implications for novel biomarker development. Transl Psychiatry 2015, 5, e561. [Google Scholar] [CrossRef]
- Kalisch, R.; Russo, S.J.; Müller, M.B. Neurobiology and Systems Biology of Stress Resilience. Physiol Rev 2024, 104, 1205–1263. [Google Scholar] [CrossRef]
Figure 1.
Tau and Stress Balancing.
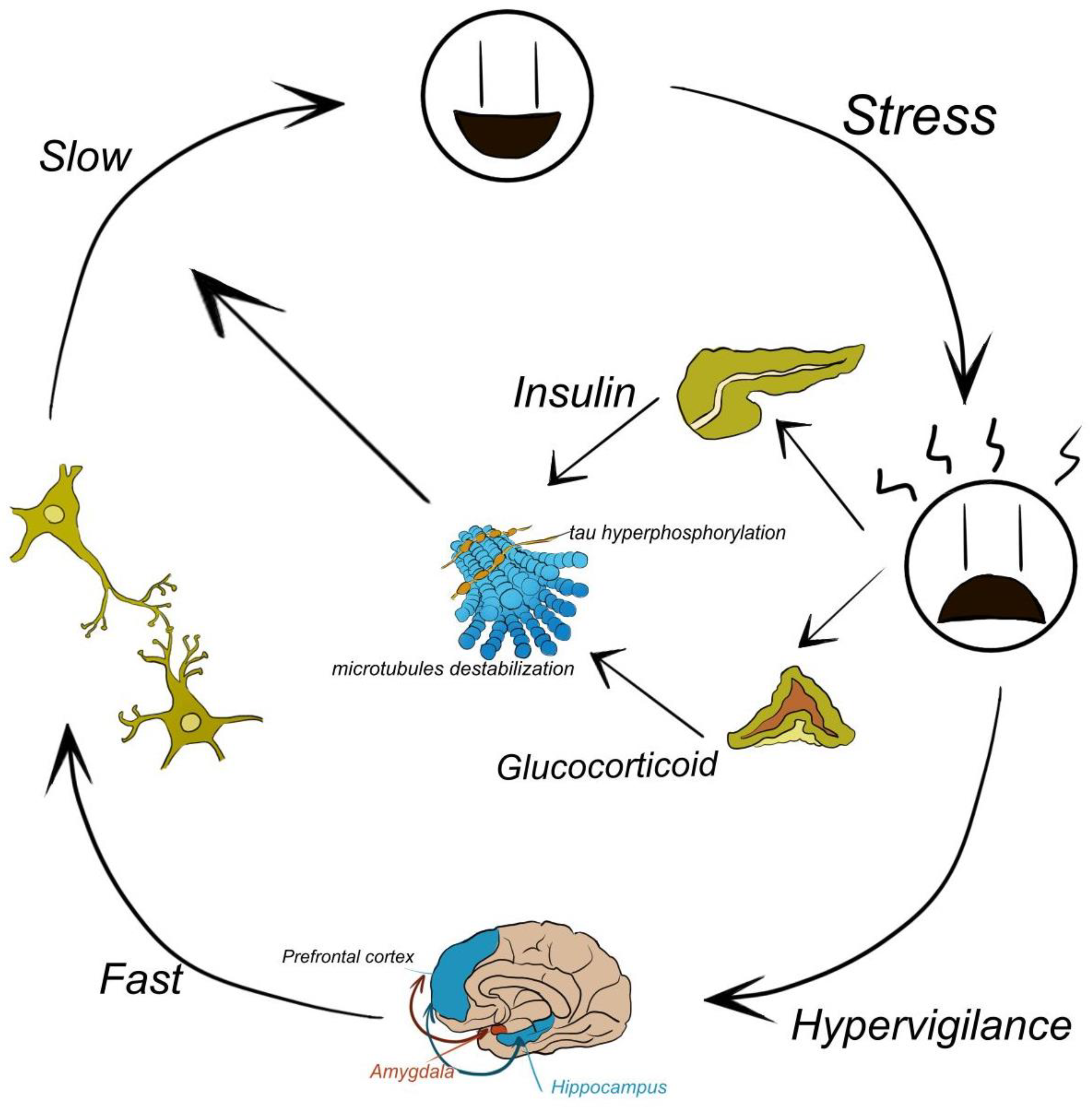
Figure 2.
– Flowchart.
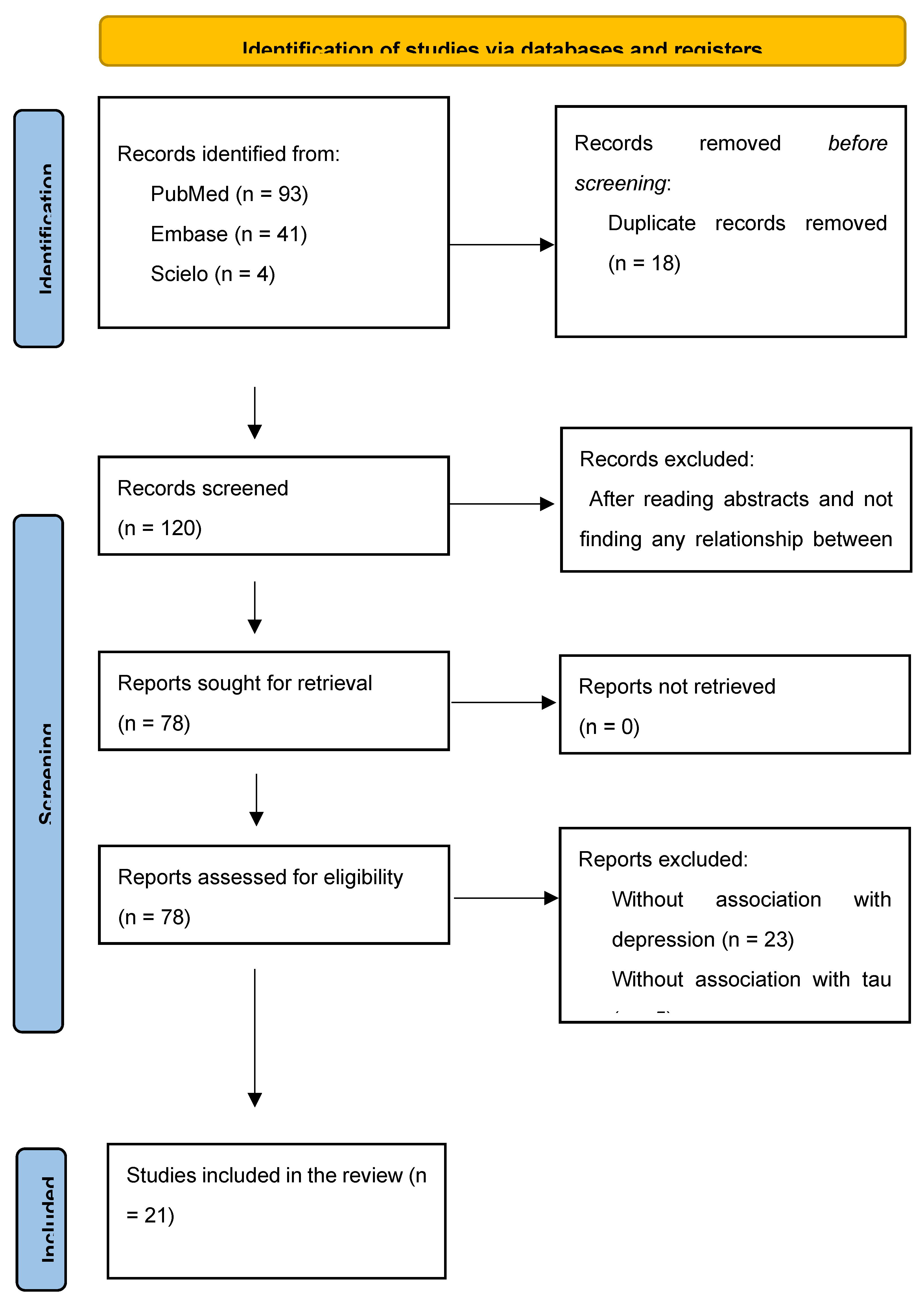

Table 1.
Tau in depression versus controls.
| Citation | Depression | Controls | |
| Andreasen et al [24] | n = 28 - CSF T-tau, pg/mL = 231 ± 110 |
n = 65 - CSF T-tau, pg/mL = 227 ± 101 |
r = .96 p < .00001* |
| Buerger et al [25] | n = 34 - CSF P-tau231 not informed* |
n = 21 - CSF P-tau231 not informed |
U=226 p < .050 |
| Schönknecht et al [26] | n = 25 T-tau, pg/mL = 202.6 ± 96.2 |
n = 17 T-tau, pg/mL = 246.6 ± 111.4 |
p > .050 |
| Blasko et al [27] | n = 11 - CSF P-tau181 = 28.6 ± 5 |
n = 25 - CSF P-tau181 = 22.8 ± 2 |
p > .050 |
| Schönknecht et al [28] | n = 54 - CSF P-tau181 = 40.6 ± 14.8 |
n = 24 - CSF P-tau181 = 49.7 ± 9.4 |
p > .050 |
| Gudmunsdsson et al [29] | n = 11 - CSF T-tau, pg/mL = 287.5 ± 114.9 |
n = 70 - CSF tau, pg/mL = 331.7 ± 189.8 |
t = .445 p = .657 |
| Kumar et al [30] | n = 20 - PET FDDNP global = 1.10 ± 0.04 |
n = 19 - PET FDDNP global = 1.07 ± 0.03 |
t = 2.55 p < .010 |
| Reis et al [31] | n = 20 - CSF P-tau = 40.5 (15.5-60.4) T-tau = 169 (141-276) |
n = 8 P-tau = 40.3 (18.4-51.3) T-tau = 156 (108-219) |
p = .700 p = .200 |
| Pomara et al [32] | n = 28 - CSF P-tau = 48.9 ± 25.9 T-tau = 273.0 ± 114.3 |
n = 19 - CSF P-tau = 51.6 ± 20.9 T-tau = 328.7 ± 151.7 |
p = .710 p = .160 |
| Diniz et al [33] | n = 25 - CSF P-tau181 = 73.6 ± 49.2 |
n = 25 - CSF P-tau181 = 68.4 ± 54.1 |
p = .700 |
| Pomara et al [34] | n = 28 - CSF Baseline: P-tau = 48.68 ± 30.76 T-tau = 254.33 ± 122.39 Follow-up: P-tau = 49.63 ± 34.86 T-tau = 277.33 ± 111.98 |
n = 19 - CSF Baseline: P-tau = 48.93 ± 25.87 T-tau = 343.59 ± 152.59 Follow-up: P-tau = 51.12 ± 18.12 T-tau = 365.71 ± 136.17 |
P-tau x Aβ: p = .700 T-tau x Aβ40: p = .011 T-tau x Aβ42: p = .016 |
| Gonzales et al [35] | n = 80 - CSF P-tau = 47.34 ± 22.94 T-tau = 101.51 ± 58.44 |
n = 158 - CSF P-tau = 39.09 ± 22.44 T-tau = 83.92 ± 51.77 |
p = .004 p = .031 |
| Liguori et al [36] | n = 48 - CSF P-tau = 33.46 ± 8.56 T-tau = 205.42 ± 83.21 |
n = 58 - CSF P-tau = 32.75 ± 5.21 T-tau = 252.89 ± 43.26 |
p > .050 p > .050 |
| Bubalat et al [37] | n = 38 - PET tau- amyloid- = 15 (39.5%) tau- amyloid+ = 0 (0%) tau+ amyloid- = 16 (42.1%) tau+ amyloid+ = 7 (18.4%) |
n = 263 - PET tau- amyloid- = 142 (54%) tau- amyloid+ = 23 (8,7%) tau+ amyloid- = 57 (21.6%) tau+ amyloid+ = 41 (15.6%) |
OR = 2.42 (1.14-5.14) (p = .021) p = .301 p = .998 p = .060 p = .284 |
| Liu et al [38] | n = 64 - plasma tau = 4.322 ± 2.116 |
n = 75 - plasma tau = 4.488 ± 1.541 |
p = .247 |
| Loureiro et al [39] | LOD + cognitive impairment: n = 22 – CSF P-tau = 41.9 ± 5.2 T-tau = 93.8 ± 14.4 EOD + cognitive impairment: n = 31 – CSF P-tau = 38.4 ± 4.4 T-tau = 98.9 ± 11.8 |
n = 22 - CSF P-tau = 39.8 ± 5.4 T-tau = 83.7 ± 14.5 |
p > .050 p > .050 |
| Moriguchi et al [40] | n = 20 - PET [11C]PBB3 SUVRs = 0.96 ± 0.07 [11C]PiB SUVRs = 1.20 ± 0.20 |
n = 20 - PET [11C]PBB3 SUVRs=0.89 ± 0.08 [11C]PiB SUVRs = 1.24 ± 0.21 |
p = .020 p = .390 |
| Chan et al [41] | n = 30 - CSF P-tau = 63.11 ± 22.33 T-tau = 510.60 ± 215.17 |
n = 169 - CSF P-tau = 55.74 ± 25.80 T-tau = 492.41 ± 292.70 |
p = .170 p = .760 |
| Golas et al [42] | Depression only n = 7 - CSF P-tau = 40.6 ± 10.2 T-tau = 173.8 ± 80.7 Depression + MCI n = 12 - CSF P-tau = 53.3 ± 21.8 T-tau = 315.9 ± 282.8 |
MCI only n = 12 - CSF P-tau = 71.1 ± 28.3 T-tau = 473.0 ± 302.1 |
p = .066 p = .028*** |
| Salwierz et al [43] | Past depression+ n = 20 - CSF P-tau = 93.3 ± 48.0 T-tau = 699.1 ± 500.3 |
Past depression- n = 65 - CSF P-tau = 86.9 ± 40.1 T-tau = 656.0 ± 405.7 |
p = .554 p = .695 |
| Schuurmans et al [44] | MDD n = 51 T-tau (hr) = .92 (.75-1.12) |
Any depression symptoms n = 439 T-tau (hr) = .68 (.37-1.25) |
p > .050 |
CSF: cerebrospinal fluid; EOD: early-onset depression; hr; adjusted hazard ratio; LOD: late-onset depression; MCI: mild cognitive impairment; MDD: major depression disorders; P-tau: phosphorylated tau; PET: positron emission tomography; T-tau: total-tau. * This data refers to the correlation between baseline and follow-up data. There was no statistically significant difference between depression and control. ** The values measured by tau were presented in graphs without precise information about the real numbers. *** The data referred to the difference between cognitive loss and depression, where participants with MCI exhibited more significant levels of phosphorylated tau than participants with depression.
Table 2.
Main findings.
| Citation | Design | Study aim | Relevance to tau and depression | Relevant Result |
| Andreasen et al [24] | Follow-up | To evaluate the sensitivity and specificity of CSF-tau in clinical practice as a diagnostic marker for AD compared with normal aging and depression, to study the stability of CSF-tau in longitudinal samples, and to determine whether CSF-tau levels are influenced by different covariates such as gender, age, duration or severity of disease, or possession of the APOE-ε4 allele. | To study factors that potentially may influence the variability (and thus the sensitivity and specificity) of CSF-tau. |
There were no significant correlations between age and CSF-tau either in the probable AD (r = -0.04), possible AD (r = 0.02), or control (r = 0.24) groups, whereas a significant correlation was found in the depression group (r = 0.74; p < 0.0001). |
| Buerger et al [25] | Case-control | Whether p-tau231 levels improve the differential diagnosis between geriatric major depression and Alzheimer’s disease. | P-tau231 levels could accurately discriminate between major depression and Alzheimer’s disease because they detect an early and specific feature of the pathophysiology of Alzheimer’s disease. | Significant difference in p-tau231 levels (χ2= 78, df=3, p<0.001) among all groups. P-tau231 levels were higher in major depression patients than in healthy comparison subjects (Mann-Whitney U=226, df=1, p<0.05). |
| Schönknecht et al [26] | Case-control | The potential value of tau levels in the differential diagnosis of AD, VD, and MDD. | The potential effects of psychotropic medication, such as antidepressants, on tau concentration. |
Tau protein concentrations in patients with AD were significantly (P-0.05) elevated compared with those in VD patients, depressed patients, and controls, but did not significantly differ between controls and patients with depression. |
| Blasko et al [27] | Case-control | To evaluate CSF levels of 13 potential biomarkers in patients with AD, frontotemporal lobe dementia, alcohol dementia, major depression, and control patients without any neuropsychiatric disease. | A variety of other possible markers have been examined in the CSF of AD patients to obtain an insight into the pathophysiology of AD and to establish them as disease markers and differentiate from other illnesses such as depression. |
By using the ratio P-tau181/Aβ42, AD patients were separated from healthy control subjects (area under the ROC curve, 0.901; p < 0.001), from subjects with FTLD (area under the ROC curve, 0.900; p = 0.006) and from subjects with alcohol dementia and major depression (area under the ROC curve, 0.909; p < 0.001 and 0.913; p < 0.001, respectively). |
| Schönknecht et al [28] | Case-control | Cross-sectionally, MCI patients would show higher t-tau and p-tau levels com- pared to patients with geriatric major depressive disorder and controls. | Though MCI often overlaps with depressive symptoms making early diagnosis difficult, to date no CSF marker has been probed to support the differential diagnosis of geriatric major depressive disorder and MCI eventually converting to AD. | CSF t-tau and p-tau levels were significantly increased in patients with mild cognitive impairment when contrasted to patients with geriatric major depressive disorder and control. |
| Gudmunsdsson et al [29] | Case-control | To better understand the biological basis and potential biomarkers for geriatric depression. |
Aβ42 and T-tau are sometimes used to discriminate geriatric depression from mild forms of AD in clinical studies. However, studies focusing on the relationship between these CSF biomarkers and geriatric depression are lacking. | T-tau levels increased with increasing age (linear- by-linear association, χ2 = 5.774, df=1, Monte Carlo p=0.015). No differences in T-tau were observed compare depression and controls. |
| Kumar et al [30] | Case-control | To examine and compare protein (amyloid and tau) binding in critical brain regions in patients diagnosed as having late-life MDD and healthy control. | Smaller brain volumes, identified using volumetric MRI estimates, are presumed to reflect neurodegeneration, although neuropathologic findings indicate only circumscribed neuronal loss in MDD. | The global [18F]FDDNP binding value was significantly higher in MDD group when compared with that of controls. Post hoc t tests demonstrated that the depressed group had significantly higher binding in the lateral temporal and PC regions when compared with controls (Cohen d effect sizes of 0.92 and 0.67, respectively). |
| Reis et al [31] | Case-control | Depression is a highly prevalent disorder in the elderly and one of the risk factors for developing dementia. The present study involves patients with AD, geriatric MDD and cognitively healthy controls aiming to compare baseline CSF biomarkers. | The assessment of changes in the concentrations of CSF Aβ42, T-tau, and P-tau in nondemented patients with depression with and without cognitive manifestations can provide important in- formation on the clinical course and outcome of these syndromes. | There was not any significant difference in measures of P-tau among the groups. Higher levels of P-tau were observed in four MDD patients compared with controls based on the previously established cut-off value of 61 pg/mL. |
| Pomara et al [32] | Case-control | Whether major depression was associated with CSF levels of amyloid beta, tau protein, and F2-isoprostanes in elderly individuals with major depressive disorder and age-matched nondepressed comparison subjects. | Increased brain amyloid beta and tau protein binding were observed in currently depressed individuals with MDD and no MCI. | No differences were observed in total and phosphorylated tau proteins. |
| Diniz et al [33] | Case-control | To determine the concentrations of brain-derived neurotrophic factor (BDNF), amyloid-β42, total Tau, and phosphorylated Tau in the cerebrospinal fluid (CSF) of patients with LLD and cognitive impairment compared to healthy older adults. | None of the previous studies specifically addressed whether cognitive impairment in older adults with LLD related to abnormalities in CSF biomarkers related to AD (i.e., Aβ42, total Tau, and phosphorylated Tau181) or other biomarkers. | No significant differences in T-Tau: LLD, 55.5 ± 36.6 pg/ml vs. controls, 49.0±33.9 pg/ml, t(48) = 0.64, p = .5; P-Tau181: LLD, 73.6±49.2 pg/ml vs. control, 68.4±54.1 pg/ml, t(48) = 0.35, p = .7). |
| Pomara et al [34] | Follow-up | To determine first whether late-life major depression (LLMD) and time (baseline to follow-up) influenced the Aβ levels; and second to determine whether any time-related change in Aβ was associated with changes in the severity of depressive symptoms | Several lines of evidence from epidemiological, case-control and longitudinal studies provide support for an association between depression (or depressive symptoms) and an increased risk for dementia and AD, or for depression as a prodromal state of AD. | Comparisons of the baseline to follow-up levels showed significant correlation between CSF Aβ42 levels and t-tau (r=0.557, P=0.016). A significant correlation was found between CSF Aβ40 and t-tau levels as well (r=0.586, P=0.011). Thus, increases in t-tau in the LLMD group, over time, were associated with increases in both CSF Aβ42 and CSF Aβ40. The same significant correlations were not found between p-tau and CSF Aβ42 or CSF Aβ40 (P’s >0.700). |
| Gonzales et al [35] | Case-control | To evaluate the association between SSD and CSF biomarkers in a subset of individuals with MCI and stable subsyndromal depressive symptomatology. | Emerging literature indicates that even subsyndromal symptoms of depression (SSD), depressive symptomology below the frequency and severity for clinical diagnosis, accelerates cognitive decline in MCI, and hastens the conversion to dementia. | No group differences were observed for CSF T-tau (p = .497) or P-tau (p = .392). Using Mann-Whitney U test was found a significative difference in CSF P-tau (p = 0.004). |
| Liguori et al [36] | Follow-up | To investigate the cross-sectional association between depressive symptoms and cerebral tau [18F T807 (also known as 18F-AV-1451) tau positron emission tomography (PET) imaging] in cognitively normal (CN) older adults. | Depressive symptoms, both major depression and subclinical depressive symptoms, are common in older adults, in whom they are disabling and can be associated with functional impairment, decreased quality of life, and cognitive impairment. | Higher GDS was significantly associated with greater IT tau (partial r = 0.188, p = 0.050) and marginally associated with greater EC tau (partial r = 0.183, p = 0.055). |
| Bubalat et al [37] | Cohort | To examined if tau and amyloid imaging were associated with a depression diagnosis among cognitively normal adults. | Higher PET amyloid levels and higher CSF ratio tau/Aβ42 at baseline developed more depressive symptoms as measured by a change score in the Geriatric Depression Scale (GDS) over one year, compared with participants with lower biomarker levels. | Participants with elevated tau were 1.42 times more chance to be depressed. Antidepressant use modified this relationship where participants with elevated tau who were taking antidepressants had greater odds of being depressed. |
| Liu et al [38] | Case-control | To determine whether plasma IL18, Aβ40, Aβ42, and the AD-associated tangle component Tau, as well as IL18 single nucleotide polymorphisms (SNPs) may be biomarkers for depression. | Peripheral Tau levels are altered in depressive patients and whether IL18, Aβ and Tau are as- sociated with each other in depression remain unclear. | None of the plasma levels of IL18, Aβ40, Aβ42, and Tau, the ratio of Aβ42/Aβ40, and the genotypes of IL18 SNPs were significantly different between combined depressive patients and combined healthy controls, or between male depressive patients and male controls. |
| Loureiro et al [39] | Case-control | To determine a panel of AD-related CSF biomarkers in a cross-section of elders with MCI with and without LLD. | Depression may alternatively be an incipient feature of a subjacent neurodegenerative disorder – e.g., AD at pre-dementia stages – in which case depressive symptoms could be, along with MCI. | Mean Aβ1-42/P-tau ratio: aMCI, 7.9 (p < 0.001); LOD 14.2 (p < 0.001); EOD, 15.3 (p < 0.001); controls, 17.1 (p < 0.001); p < 0.05. No differences were observed in total and phosphorylated tau proteins. |
| Moriguchi et al [40] | Case-control | To investigate tau and Aβ accumulations both simultaneously and separately in the same subjects with elderly MDD. | There is ample evidence that depression is a risk factor for AD. | Regional [11C]PBB3 SUVRs in MDD patients had a higher trend than those of healthy controls in the anterior cingulate cortex (t(38) = 2.13, p = 0.04). |
| Chan et al [41] | Cohort | To explore the association between depression and postoperative delirium in hip fracture patients, and to examine Alzheimer’s disease (AD) pathology as a potential underlying mechanism linking depressive symptoms and delirium. | In AD, a risk factor for postoperative delirium, depression and other neuropsychiatric symptoms have been the focus of growing interest as early manifestations or prodromal symptoms of an underlying neurodegenerative disease process. | Both CSF A 42/t-tau (β = −1.52, 95%CI = −2.1 to −0.05) and A 42/p-tau181 (β = −0.29, 95%CI = −0.48 to −0.09) were inversely associated with higher GDS-15 scores, where lower ratios indicate greater AD pathology. |
| Golas et al [42] | Cohort | To investigate the relationship between past depression and WMH burden in those with positive (AD+) and negative (AD-) CSF biomarker profiles for AD. | There is conflicting evidence to support a direct link between Aβ and tau, two of the pathological hallmarks of AD and LLD. | Participants with MCI exhibited greater levels of phosphorylated tau (P tau) than participants with MDD (p = 0.03). |
| Salwierz et al [43] | Cohort | To investigate the relationship between a history of depression and bio- markers of AD and CVD in patients with dementia in a clinical setting. | A growing body of research has explored the association between depression and dementia where individuals with a history of depression are not only at an increased risk of developing dementia. | Trends towards higher Fazekas scores in Past Depression− patients and a higher proportion of females with depression in Past Depression+ patients. No differences in T-tau were observed compare depression and controls. |
| Schuurmans et al [44] | Follow-up | Whether plasma biomarkers for neuropathology associate with late-life depression in middle-aged and elderly individuals. | Evidence shows that those who suffer from neurodegenerative disease are more likely to experience late-life depression. | With each log2 pg./mL increase in amyloid-β 40, participants had a 0.70 (95% CI [0.15, 1.25]) points higher depressive symptoms score at baseline. No other statistically significant cross-sectional or longitudinal associations were found. |
Aβ: amyloid-β; AD: Alzheimer’s disease; CSF: cerebrospinal fluid; CVD: cerebrovascular disease; EC: entorhinal cortex; FTLD: frontotemporal lobe dementia; GDS: Geriatric Depression Scale; IT: inferior temporal; LLD: late-life depression; MCI: mild cognitive impairment; MDD: major depression disorders; MRI: magnetic resonance imaging; P-tau: phosphorylated tau; T-tau: total-tau; VD: vascular disease.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



