
Submitted:
13 August 2024
Posted:
14 August 2024
You are already at the latest version
Abstract
Background/Objectives: Vitamin D’s effect on risk health outcomes is often evaluated using prospective cohort studies. Risk ratios (RRs; e.g., hazard ratios or odds ratios) are determined for incidence for participants with baseline serum 25-hydroxyvitamin D [25(OH)D] concentrations below or above specified values. Serum 25(OH)D concentrations vary over time, thereby diluting the effect of 25(OH)D for long follow-up periods. Inverse relationships between RR and follow-up period have been reported for all-cause mortality rate and cancer incidence rates. Here I evaluate the effect for neurological outcomes. Methods: I analyzed how follow-up period affected results from 10 cohort studies of all-cause dementia, 6 studies of Alzheimer’s disease, and 9 for cognitive impairment with respect to vitamin D deficiency. Results: For all-cause dementia, Alzheimer’s disease, and cognitive impairment, respectively, the linear regression fits are RR = 2.9 – 0.14 × years, r = 0.73, p = 0.02; RR = 2.9 – 0.14 × years, r = 0.69, p = 0.13; and RR = 1.8 – 0.066 × years, r = 0.72, p = 0.03. The regression fit to RR for the shortest follow-up period for each outcome is considered the best estimate of vitamin D deficiency’s effect on risk. Those values are approximately twice that found by averaging all RRs without considering the effect of follow-up period. Conclusions: Vitamin D’s effect on risk of neurological conditions should be determined with relatively short follow-up periods after repeated 25(OH)D measurements as warranted during follow-up.
Keywords:
Alzheimer’s disease
; cognitive impairment
; dementia
; follow-up period
; neurological conditions
; risk
; vitamin D deficiency
1. Introduction
Prospective cohort studies are often used to ascertain how lifestyle, diet, nutrient, and biomarkers affect health outcomes. The standard procedure is to enroll participants, obtain values for factors to be studied and those that might affect the outcome, monitor participants for several years, and note changes in the health condition of interest. In general, no additional measurements are made of the values of the factors. Because serum 25-hydroxyvitamin D [25(OH)D] concentrations change for various reasons, relying only on the baseline 25(OH)D concentration is a problem.
Since at least 1999, researchers have known that long-term follow up in prospective studies results in ”regression dilution” [1]. (Of the articles consulted in preparing this article, only Kuzma and colleagues (2016) [2] cited that article.) Since 2011, that same effect has been found in prospective cohort studies regarding serum 25(OH)D and cancer [3] and, since 2012, all-cause mortality rate [4]. Regarding cancer, the figures in my 2011 article [3] showed that the regression fit to the risk ratio (RR) for breast cancer incidence changed from 0.93 at 7 years of mean follow-up to 0.62 at no follow-up (zero). For colorectal cancer, the RR changed from 0.70 at 14 years of follow-up to 0.42 at zero. For prostate cancer, the RR changed from 0.93 at 28 years of follow-up to 1.08 at 4 years. That perhaps counterintuitive effect was supported in a later meta-analysis that related 15%‒20% increases in risk of prostate cancer to higher 25(OH)D concentrations. Vitamin D probably increased absorption of calcium and phosphorus from the gastrointestinal tract, and one or both are risk factors for prostate cancer [5]. For all-cause mortality rate, the RR decreased from 0.95 at 14 years of follow-up to 0.82 at 6 years [4]. An observational study in Norway reported that “depending on the method of adjusting for season, the correlation coefficient between serum 25(OH)D measurements from 1994 and 2008 ranged from 0.42 to 0.52” [6]. As shown in Figure 1 in Ref. [4], the correlation coefficients between repeated 25(OH)D measurements in cohort populations ranged from 0.5 to 0.8 for intervals from 1 to 5 years, indicating large uncertainty in using such measurements. A more recent report showed that the analysis of the risk of colorectal cancer with respect to serum 25(OH)D concentration on the basis of prospective cohort studies [7] was incorrect because the researchers had not realized that men had nearly four times the rate of change in RR with respect to follow-up time as women (Figure 1 [8]).
I read with interest the article by Zhang and colleagues [9] regarding the association between vitamin D levels and risk of dementia. The authors used the standard random effects model regarding 17 prospective cohort studies with 486,921 individuals. For dementia with respect to vitamin D deficiency, RR = 1.42 (95% confidence interval [CI], 1.21‒1.65). However, that analysis, which forms the basis for my article, did not consider each study’s median follow-up period.
2. Materials and Methods
To evaluate how follow-up period affects risk of dementia with respect to vitamin D deficiency, I used the data in Figure 2 from Zhang and colleagues [9] plus the results of a 2024 study [10] along with each study’s mean follow-up period. Data for Alzheimer’s disease (AD) were obtained from Figure 3a in Zhang and colleagues [9]. Data for cognitive impairment (CogImp) are from Figure 3b in Zhang and colleagues [9]. Table 1 and Table 2 show the relevant information regarding the data in the cohort studies. Unless otherwise noted, the hazard ratio (HR) or odds ratio (OR) values are those given in Figure 2 in Zhang and colleagues [9]. Those values are not included in Table 1 and Table 2 because of copyright issues. For dementia, mean ages of participants at baseline ranged from 53 (SD 17) to 85 (SD 7) years. The mean 25(OH)D concentrations for studies that gave values ranged from 32 (standard deviation [SD] 25) to 69 ± 19 nmol/L. The 25(OH)D comparisons included <25 versus >50 mol/L, <50 versus >50 mol/L, <50 versus ≥75 nmol/L, and so on. The mean follow-up period ranged from 5.6 to 30 years. For CogImp, mean ages participants at baseline ranged from 67 ± 5 to 74 (SD 7) years. Mean 25(OH)D concentrations for studies that gave values ranged from 50 (SD 21) to 84 (SD 54) nmol/L. The 25(OH)D comparisons included <25 versus ≥50 mol/L, <50 versus ≥75 nmol/L, and so on. The mean follow-up period ranged from 4.0 to 13 years.
In my analysis, I assume that the only important factor is the mean follow-up period. Though values for various factors could affect the HR, in the analysis it appears that they are smaller than the effect of follow-up period. Studies with mean follow-up period greater than 15 years were omitted because I considered those periods too long to yield meaningful data. One study with a very large 95% CI was omitted from the analysis.
Table 2a and Table 2b give the data associated with the CI studies. The numbers of cognitively normal participants at baseline and the number who developed CI are for those in the 25(OH)D categories used in the HR or OR analyses.

Table 2.
a. Data for vitamin D deficiency and risk of cognitive impairment from Figure 3b in Zhang and colleagues (2024) [9].
| Country | Mean age (SD) (yrs) |
N | NCI | Test | Author, yr, Ref.* |
|---|---|---|---|---|---|
| USA | 74 ± 5) | 1812 F | MMSE, TMTB | (Slinin, 2012) [25] | |
| Italy | 74 ± 7) | 806 | 466 | MMSE | (Toffanello, 2014) [26] |
| USA | 74 ± 6) | 806 M | 126 | MMSE, TMTB | (Slinin, 2010) [27] |
| Italy | 74 ± 7) | 332 | MMSE | (Llewellyn, 2011) [28] | |
| USA | 72 ± 3 | 1564 | 324 | BVRT | (Kuzma, 2016 [CHS]) [2] |
| Chile | 67 ± 5 | 666 F, 289 M | MMSE | (Marquez, 2022) [29] | |
| Norway | 78 | 790 F, 644 M | MoCA | (Asante, 2023) [16] | |
| Sweden | 71 | 1182 M | 80 | MMSE | (Olsson, 2017) [18] |
| Netherlands | 74 ± 6) | 1044 | 346 | RAVLT | (Kuzma, 2016 [LASA]) [2] |
*See Figure 2 in Zhang and colleagues (2024) [9]; BVRT, Benton Visual Retention Test; CHS, Cardiovascular Health Study; F, female; LASA, Longitudinal Aging Study Amsterdam; M, male; MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; NCI, number with cognitive impairment; RAVLT, Rey’s Auditory Verbal Learning Test; SD, standard deviation; TMTB, Trail Making Test Part B.
Table 2.
b. Data for vitamin D deficiency and risk of cognitive impairment from Figure 3b in Zhang and colleagues (2024) [9].
| Assessment (yrs) | Mean BMI (SD) (kg/m2) |
Mean 25(OH)D (SD) (nmol/L) | 25(OH)D comparison (nmol/L) | Mean follow-up (yrs) | HR or OR (95% CI) |
Author, yr, Ref.* |
|---|---|---|---|---|---|---|
| 2 and 4 | 26 ± 5, F | <25 vs. ≥75 | 4.0 | * | (Slinin, 2012) [25] | |
| 4 | 27 ± 3 | 84 ± 54 | <50 vs. ≥75 | 4.4 | * | (Toffanello, 2014) [26] |
| 4.6 | 27 ± 3, M | <50 vs. ≥75 | 4.6 | * | (Slinin, 2010) [27] | |
| 3 and 6 | 52 ± 37 | <25 vs. ≥75 | 5.2 | * | (Llewellyn, 2011) [28] | |
| Annual | 26.6 ± 4.5 | <25 vs. ≥50 | 6.5 | * | (Kuzma, 2016 [CHS]) [2] | |
| ? | 29 ± 5, F 28 ± 4, M |
Cases: 58 ± 32 Noncases: 71 ± 38 |
30‒48 vs. >75 | 9.6 | * | (Marquez, 2022) [29] |
| 27 ± 3 | 50 ± 21 | <50 vs. >50 | 10 | * | (Asante, 2023) [16] | |
| 26 ± 3 | 69 ± 19 | <50 vs. ≥75 | 12 | * | (Olsson, 2017) [18] | |
| Every 3‒4 | 27 ± 4 | <25 vs. ≥50 | 13 | * | (Kuzma, 2016 [LASA]) [2] |
3. Results
In the analysis for dementia, I omitted one study with high uncertainty, accounting for only 0.7% of the weight, and three studies with follow-up periods of 17+ years. I conducted two studies, one with 11 studies and one with 10, omitting Féart and colleagues [17]. The linear fit to the data with 11 studies is RR = 2.8 – 0.12 × years, r = 0.59, p = 0.03. The linear fit to the data with 10 studies is RR = 2.9 – 0.14 × years, r = 0.73, p = 0.02 (Figure 1). (For 13.3 years, two studies reported RR = 1.22.) Zhang and colleagues (2024) calculated an estimated pooled RR of 1.42 (95% CI, 1.21‒1.65). For the shortest follow-up period, 5.6 years, the RR for the analysis with 10 studies is 2.1 (95% CI, 1.04‒3.9), 2.6 times higher than the value from Zhang and colleagues, though with much larger 95% CIs.
For the RR of AD versus 25(OH)D concentration as a function of follow-up period, I conducted two analyses. In the analysis with seven studies with less than 15 years of mean follow-up period in Zhang and colleagues (2024) [9] plus Chen and colleagues (2024) [10], the regression fit to the data was RR = 2.5 – 0.08 × years, r = 0.32, p = 0.48. With Féart and colleagues [17] omitted, the regression fit to the data was RR = 2.9 – 0.14 × years, r = 0.69, p = 0.13 (Figure 2). The estimated pooled RR in Zhang and colleagues [9] is 1.57 (95% CI, 1.15‒2.14). The value in this article for the six studies for the shortest follow-up period, 5.6 years, is 2.12 (95% CI, 1.01‒4.13). That estimate is 2.0 times higher than the estimate from Zhang and colleagues but again with higher 95% CI values.
The analysis for CI versus 25(OH)D concentration as a function of follow-up period used 6 of the 10 studies in Figure 3b from Zhang and colleagues (2024) [9], with one study omitted that had very large 95% CI values and three with follow-up times less than 5 years. The regression fit to the data is RR = 2.3 – 0.11 × years, r = 0.88, p = 0.02. (If three studies with mean follow-up period between 4.0 and 4.6 years are added, RR = 1.8 – 0.066 × years, r = 0.72, p = 0.03.) Figure 3 is a scatter plot of the data used in the analysis. The estimated pooled RR in Zhang and colleagues (2024) [9] is 1.34 (95% CI, 1.19‒1.52). The value in this article for the six studies for the shortest follow-up period, 4 years, is 1.73 (95% CI, 1.15‒2.04). That estimate is 2.1 times higher than the estimate from Zhang and colleagues but again with higher 95% CI values.
4. Discussion
As shown in the work of Clarke and colleagues [1], values for biological factors change over time. Therefore, apparent health effects related to those factors are reduced in long-term follow-up prospective studies. Serum 25(OH)D concentrations can change for several reasons.
Vitamin D production from solar UVB exposure decreases with age [30]. A recent experimental study reported that vitamin D production from sun exposure decreases by 13% per decade of life [31].
Serum 25(OH)D concentration is generally inversely correlated with body mass index (BMI; kilograms of mass per square meter of body surface area). For example, in the dementia study from Israel [13], mean BMI was 25 ± 4 kg/m2 for 25(OH)D concentrations >75 nmol/L, increasing to 29 ± 7 kg/m2 for 25(OH)D <2.5 nmol/L. Thus, if BMI changes, 25(OH)D concentration should also change.
Serum 25(OH)D concentration also is associated with dietary animal product content, especially for fish and meat [32]. If those components of diet change, 25(OH)D will change.
Fortifying food with vitamin D can change 25(OH)D, as it did in Finland, where that approach was approved at the end of 2002 [33]. Measurements of 25(OH)D and dietary assessments of 3650 participants in 1997 at 31 years of age and again in 2012‒2013 at 46 years of age determined that fortified foods accounted for most of 10.6-nmol/L increase in 25(OH)D from 54 ± 19 to 65 ± 19 nmol/L [34].
A 2017 letter to the editor reported changes in daily vitamin D supplementation with 1000 IU or more from data collected in the U.S. National Health and Nutrition Survey [35]. Prevalence for people ≥70 years increased from 1.5% (95% CI, 1.1%‒2.0%) in 2005‒2006 to 8.6% (95% CI, 5.6%‒13.1%) in 2007‒2008, and up to 38.5% (95% CI, 31.5%‒45.7%) in 2013‒2014. The Norwegian study noted that 33% of participants had changes in 25(OH)D concentrations over 10 years [16].
My results have implications for long-duration prospective cohort studies with respect to 25(OH)D concentration: they should measure the important factors at least every 4 years. That is the approach taken in Harvard University prospective studies of diet and risk of disease, for example, Bernstein and colleagues [36]. An added advantage of that approach is that the latency period between risk factor and health effect can be determined. In that study, the latency period between dietary meat intake and incidence of colorectal cancer was determined to be about 4–8 years.
The health benefits of vitamin D status may become apparent much more quickly than for diet in the incidence of adverse health outcomes. For example, in the VITAL study, in which half of more than 25,000 participants were supplemented with 2000 IU/day of vitamin D3 for a median time of 5.3 years, the incidence of overall cancer was not significantly affected for the entire group, but mortality rate was [37]. When the data for the first 1 or 2 years were omitted, the cancer mortality rate was significantly lower in the vitamin D treatment group than in the placebo group by about 20%‒25%. For cancer, different mechanisms are involved for incidence than for progression and metastasis [8]. A vitamin D randomized controlled trial (RCT) was conducted regarding progression from prediabetes to type 2 diabetes mellitus [38]. The vitamin D dose was 4000 IU/day and the median follow-up time was 2.5 years. When the results were reanalyzed, the HR for diabetes for an increase of 25 nmol/L in intratrial 25(OH)D level was 0.75 (95% CI, 0.68–0.82) in the vitamin D treatment arm and 0.90 (95% CI, 0.80–1.02) in the placebo arm.
The evidence that vitamin D reduces risk of AD was reviewed in 2023 in the Journal of Alzheimer’s Disease [39]. Some important mechanisms include reduced risk of insulin resistance (IR) and inflammation. The mechanisms linking brain insulin/insulin-like growth factor resistance include impaired function of glucose transporter 4, changes in insulin receptor function, energy deficit, increased oxidative stress, and hyperglycemia (see Table 1 in Nguyen and colleagues [40]). A 2019 review discussed vitamin D’s role in reducing IR [41]. The mechanisms include maintaining normal levels of reactive oxygen species and ionized calcium, thereby reducing epigenetic changes associated with insulin resistance such as oxidative stress and inflammation.
Therefore, I searched for the effect of vitamin D supplementation regarding health outcomes related to neurodegenerative diseases to ascertain whether supplementation is promising and what time scales are involved. A 3-month study involving elderly people with metabolic disorders showed that supplementation with 2000 IU/day of vitamin D significantly decreased the homeostatic model assessment for insulin and decreased oxidative DNA damage [42]. In addition, supplementation reduced metabolic parameters connected with IR and improved glucose and lipid metabolism.
A 2023 review by Lason and colleagues examined the vitamin D receptor as a potential target for age-related neurodegenerative diseases [43]. The review mentioned a study investigating the effect of vitamin D supplementation involving mild CogImp (MCI) patients [44]. That study included 16 MCI patients, 11 very early AD (VEAD) patients, and 25 healthy control subjects. Patients with 25(OH)D concentrations lower than 75 nmol/L were supplemented with 50,000 IU of vitamin D3 once a week for 6 weeks, followed by 1500‒2000 IU/day for 18 months. In MCI but not VEAD patients, lymphocyte susceptibility to death improved significantly after 6 months. After 18 months, Montreal Cognitive Assessment scores improved in MCI patients but not in VEAD patients. Because MCI is an important risk factor for AD [45,46], this finding supports the role of higher 25(OH)D concentrations in reducing risk of AD.
In addition, that review [43] included Table 1 with information for eight observational and vitamin D supplementation RCTs regarding late-life cognition, dementia, and AD. Three of those studies reported results of interest for this article. An 18-week RCT compared 4000 versus 400 IU/d vitamin D3 effects on visual memory [47]. Participants in the high-dose group increased mean serum 25(OH)D concentration from 67 ± 20 to 131 ± 26 nmol/L, whereas concentration in the low-dose group increased from 61 ± 22 to 86 ± 16 nmol/L. Those in the high-dose group with baseline 25(OH)D concentration <75 nmol/L increased performance in the Pattern Recognition Memory-Delayed task from 86 (SD 14) to 94 (SD 8) (p = 0.005). The change in the low-dose group had p = 0.61. No additional significant differences in cognitive function tests were apparent among the other 11 tests for people with 25(OH)D < 75 nmol/L.
A vitamin D supplementation RCT in AD patients conducted in China reported the best results regarding cognitive function [48]. A total of 105 AD patients who received 800 IU/d of vitamin D increased serum 25(OH)D concentrations from 47 ± 7 to 57 ± 4 nmol/L by the end of the year. The 105 participants in the control group decreased 25(OH)D from 49 ± 3 to 47 ± 3 nmol/L. The mean BMI in each group was 25 ± 3 kg/m2. People in the vitamin D treatment group had modest increases in full-scale IQ, information, digit span, vocabulary, block design, and picture arrangement, whereas participants in the control group had modest-to-large reductions in all those parameters. The p-values for the time and group effects for the vitamin D treatment group compared with the control group were significant to p < 0.001 for all but the vocabulary (p = 0.15 for time effect) and block design (p = 0.02). Thus, the RCT showed that vitamin D supplementation could significantly improve cognitive function in AD patients. Thus, that intervention study suggests that vitamin D supplementation can rapidly reduce AD risk factors.
As shown in Figure 1, Figure 2 and Figure 3, RR values increased linearly to the shorter mean follow-up time used for each analysis. However, three studies not included in the regression analysis for CogImp had lower RR than expected from the regression fit to the other six studies. Thus, vitamin D status can affect risk of overall dementia, AD, and CogImp in as little as 5 years. Therefore, any prospective studies of neurodegeneration should measure serum 25(OH)D concentrations at least every 5 years. Harvard has participants in its health studies complete food frequency questionnaires every 4 years [49].
Another measure that should be implemented is to seasonally adjust 25(OH)D concentrations. Many observational studies cited here measured 25(OH)D concentrations at different times of the year and then averaged the values. In the United States, mean adult wintertime serum 25(OH)D concentrations are about 75% of summertime values [50]. In addition, whenever results of meta-analyses of prospective studies are used scientifically or for health policy recommendations, the analyses should be reevaluated with respect to follow-up periods. Also, standardizing 25(OH)D concentration measurements would be helpful since 25(OH)D measured values vary with different assays and instruments. See, for example, Sempos and colleagues (2018) [51].
Low 25(OH)D concentrations are most probably causally linked to increased risk of AD. Thus, one way to reduce risk of AD is to supplement with vitamin D. A recent review outlined the evidence that supplementing with 2000 IU/day of vitamin D might be an appropriate way for many people to avoid vitamin D deficiency [52]. However, supplementation may not be effective for obese people and may not reduce risk of AD as a result of the higher systemic inflammation from visceral adipose tissue. A meta-analysis of 13 RCTs with 1955 overweight and obese subjects with low 25(OH)D concentrations found that vitamin D supplementation did not influence the inflammatory biomarkers C-reactive protein, tumor necrosis factor-α, and interleuken-6 concentrations [53].
Funding
I have no funding to report in preparing this review. However, I have received funding from Bio-Tech Pharmacal Inc. (Fayetteville, AR, USA), a supplier of vitamin D supplements.
References
- Clarke, R.; Shipley, M.; Lewington, S.; Youngman, L.; Collins, R.; Marmot, M.; Peto, R. Underestimation of risk associations due to regression dilution in long-term follow-up of prospective studies. Am J Epidemiol 1999, 150, 341–353. [Google Scholar] [CrossRef] [PubMed]
- Kuzma, E.; Soni, M.; Littlejohns, T.J.; Ranson, J.M.; van Schoor, N.M.; Deeg, D.J.; Comijs, H.; Chaves, P.H.; Kestenbaum, B.R.; Kuller, L.H. , et al. Vitamin D and Memory Decline: Two Population-Based Prospective Studies. J Alzheimers Dis 2016, 50, 1099–1108. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B. Effect of interval between serum draw and follow-up period on relative risk of cancer incidence with respect to 25-hydroxyvitamin D level: Implications for meta-analyses and setting vitamin D guidelines. Dermatoendocrinol 2011, 3, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B. Effect of follow-up time on the relation between prediagnostic serum 25-hydroxyvitamin D and all-cause mortality rate. Dermatoendocrinol 2012, 4, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Wilson, K.M.; Shui, I.M.; Mucci, L.A.; Giovannucci, E. Calcium and phosphorus intake and prostate cancer risk: a 24-y follow-up study. Am J Clin Nutr 2015, 101, 173–183. [Google Scholar] [CrossRef] [PubMed]
- Jorde, R.; Sneve, M.; Hutchinson, M.; Emaus, N.; Figenschau, Y.; Grimnes, G. Tracking of serum 25-hydroxyvitamin D levels during 14 years in a population-based study and during 12 months in an intervention study. Am J Epidemiol 2010, 171, 903–908. [Google Scholar] [CrossRef] [PubMed]
- McCullough, M.L.; Zoltick, E.S.; Weinstein, S.J.; Fedirko, V.; Wang, M.; Cook, N.R.; Eliassen, A.H.; Zeleniuch-Jacquotte, A.; Agnoli, C.; Albanes, D. , et al. Circulating Vitamin D and Colorectal Cancer Risk: An International Pooling Project of 17 Cohorts. J Natl Cancer Inst 2019, 111, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, A.; Grant, W.B. Vitamin D and Cancer: An Historical Overview of the Epidemiology and Mechanisms. Nutrients 2022, 14, 1448. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.X.; Wang, H.R.; Meng, W.; Hu, Y.Z.; Sun, H.M.; Feng, Y.X.; Jia, J.J. Association of Vitamin D Levels with Risk of Cognitive Impairment and Dementia: A Systematic Review and Meta-Analysis of Prospective Studies. J Alzheimers Dis 2024, 98, 373–385. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.J.; Sha, S.; Stocker, H.; Brenner, H.; Schottker, B. The associations of serum vitamin D status and vitamin D supplements use with all-cause dementia, Alzheimer's disease, and vascular dementia: a UK Biobank based prospective cohort study. Am J Clin Nutr 2024, 119, 1052–1064. [Google Scholar] [CrossRef] [PubMed]
- Littlejohns, T.J.; Henley, W.E.; Lang, I.A.; Annweiler, C.; Beauchet, O.; Chaves, P.H.; Fried, L.; Kestenbaum, B.R.; Kuller, L.H.; Langa, K.M. , et al. Vitamin D and the risk of dementia and Alzheimer disease. Neurology 2014, 83, 920–928. [Google Scholar] [CrossRef]
- Melo van Lent, D.; Egert, S.; Wolfsgruber, S.; Kleineidam, L.; Weinhold, L.; Wagner-Thelen, H.; Stoffel-Wagner, B.; Bickel, H.; Wiese, B.; Weyerer, S. , et al. Low Serum Vitamin D Status Is Associated with Incident Alzheimer's Dementia in the Oldest Old. Nutrients 2022, 15. [Google Scholar] [CrossRef]
- Kiderman, D.; Ben-Shabat, N.; Tsur, A.M.; Anis, S.; Watad, A.; Cohen, A.D.; Paz, Z.; Amital, H. Vitamin D Insufficiency is Associated with Higher Incidence of Dementia, a Large Community-Based Retrospective Cohort Study. J Geriatr Psychiatry Neurol 2023, 10.1177/08919887231163292, 8919887231163292. [CrossRef]
- Geng, T.; Lu, Q.; Wan, Z.; Guo, J.; Liu, L.; Pan, A.; Liu, G. Association of serum 25-hydroxyvitamin D concentrations with risk of dementia among individuals with type 2 diabetes: A cohort study in the UK Biobank. PLoS Med 2022, 19, e1003906. [Google Scholar] [CrossRef] [PubMed]
- Karakis, I.; Pase, M.P.; Beiser, A.; Booth, S.L.; Jacques, P.F.; Rogers, G.; DeCarli, C.; Vasan, R.S.; Wang, T.J.; Himali, J.J. , et al. Association of Serum Vitamin D with the Risk of Incident Dementia and Subclinical Indices of Brain Aging: The Framingham Heart Study. J Alzheimers Dis 2016, 51, 451–461. [Google Scholar] [CrossRef]
- Asante, E.O.; Mai, X.M.; Eldholm, R.S.; Skjellegrind, H.K.; Kolberg, M.; Brumpton, B.M.; Selbaek, G.; Chen, Y.; Sun, Y.Q. Vitamin D Status Over Time and Cognitive Function in Norwegian Older Adults: A Prospective Cohort of the HUNT Study. J Nutr Health Aging 2023, 27, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Féart, C.; Helmer, C.; Merle, B.; Herrmann, F.R.; Annweiler, C.; Dartigues, J.F.; Delcourt, C.; Samieri, C. Associations of lower vitamin D concentrations with cognitive decline and long-term risk of dementia and Alzheimer's disease in older adults. Alzheimers Dement 2017, 13, 1207–1216. [Google Scholar] [CrossRef] [PubMed]
- Olsson, E.; Byberg, L.; Karlstrom, B.; Cederholm, T.; Melhus, H.; Sjogren, P.; Kilander, L. Vitamin D is not associated with incident dementia or cognitive impairment: an 18-y follow-up study in community-living old men. Am J Clin Nutr 2017, 105, 936–943. [Google Scholar] [CrossRef] [PubMed]
- Licher, S.; de Bruijn, R.; Wolters, F.J.; Zillikens, M.C.; Ikram, M.A.; Ikram, M.K. Vitamin D and the Risk of Dementia: The Rotterdam Study. J Alzheimers Dis 2017, 60, 989–997. [Google Scholar] [CrossRef]
- Graf, C.E.; Rossi, C.; Giannelli, S.V.; Nobari, B.H.; Gold, G.; Herrmann, F.R.; Zekry, D. Vitamin D is not associated with cognitive status in a cohort of very old hospitalized patients. J Alzheimers Dis 2014, 42 Suppl 3, S53–61. [Google Scholar] [CrossRef]
- Schneider, A.L.; Lutsey, P.L.; Alonso, A.; Gottesman, R.F.; Sharrett, A.R.; Carson, K.A.; Gross, M.; Post, W.S.; Knopman, D.S.; Mosley, T.H. , et al. Vitamin D and cognitive function and dementia risk in a biracial cohort: the ARIC Brain MRI Study. Eur J Neurol 2014, 21, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Knekt, P.; Saaksjarvi, K.; Jarvinen, R.; Marniemi, J.; Mannisto, S.; Kanerva, N.; Heliovaara, M. Serum 25-hydroxyvitamin d concentration and risk of dementia. Epidemiology 2014, 25, 799–804. [Google Scholar] [CrossRef] [PubMed]
- Fashanu, O.E.; Zhao, D.; Schneider, A.L.C.; Rawlings, A.M.; Sharrett, A.R.; Lutsey, P.L.; Gottesman, R.F.; Gross, A.L.; Guallar, E.; Alonso, A. , et al. Mid-life serum Vitamin D concentrations were associated with incident dementia but not late-life neuropsychological performance in the Atherosclerosis Risk in Communities (ARIC) Study. BMC Neurol 2019, 19, 244. [Google Scholar] [CrossRef] [PubMed]
- Afzal, S.; Bojesen, S.E.; Nordestgaard, B.G. Reduced 25-hydroxyvitamin D and risk of Alzheimer's disease and vascular dementia. Alzheimers Dement 2014, 10, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Slinin, Y.; Paudel, M.; Taylor, B.C.; Ishani, A.; Rossom, R.; Yaffe, K.; Blackwell, T.; Lui, L.Y.; Hochberg, M.; Ensrud, K.E. , et al. Association between serum 25(OH) vitamin D and the risk of cognitive decline in older women. J Gerontol A Biol Sci Med Sci 2012, 67, 1092–1098. [Google Scholar] [CrossRef] [PubMed]
- Toffanello, E.D.; Coin, A.; Perissinotto, E.; Zambon, S.; Sarti, S.; Veronese, N.; De Rui, M.; Bolzetta, F.; Corti, M.C.; Crepaldi, G. , et al. Vitamin D deficiency predicts cognitive decline in older men and women: The Pro.V.A. Study. Neurology 2014, 83, 2292–2298. [Google Scholar] [CrossRef]
- Slinin, Y.; Paudel, M.L.; Taylor, B.C.; Fink, H.A.; Ishani, A.; Canales, M.T.; Yaffe, K.; Barrett-Connor, E.; Orwoll, E.S.; Shikany, J.M. , et al. 25-Hydroxyvitamin D levels and cognitive performance and decline in elderly men. Neurology 2010, 74, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Llewellyn, D.J.; Lang, I.A.; Langa, K.M.; Melzer, D. Vitamin D and cognitive impairment in the elderly U.S. population. J Gerontol A Biol Sci Med Sci 2011, 66, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Marquez, C.; Angel, B.; Lera, L.; Bendayan, R.; Sanchez, H.; Albala, C. Exploring the Association between Vitamin D and Changes in Cognitive Function in Chilean Older Adults: Evidence from the ALEXANDROS Cohort Study. J Pers Med 2022, 12. [Google Scholar] [CrossRef] [PubMed]
- MacLaughlin, J.; Holick, M.F. Aging decreases the capacity of human skin to produce vitamin D3. J Clin Invest 1985, 76, 1536–1538. [Google Scholar] [CrossRef] [PubMed]
- Chalcraft, J.R.; Cardinal, L.M.; Wechsler, P.J.; Hollis, B.W.; Gerow, K.G.; Alexander, B.M.; Keith, J.F.; Larson-Meyer, D.E. Vitamin D Synthesis Following a Single Bout of Sun Exposure in Older and Younger Men and Women. Nutrients 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Crowe, F.L.; Steur, M.; Allen, N.E.; Appleby, P.N.; Travis, R.C.; Key, T.J. Plasma concentrations of 25-hydroxyvitamin D in meat eaters, fish eaters, vegetarians and vegans: results from the EPIC-Oxford study. Public Health Nutr 2011, 14, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Raulio, S.; Erlund, I.; Mannisto, S.; Sarlio-Lahteenkorva, S.; Sundvall, J.; Tapanainen, H.; Vartiainen, E.; Virtanen, S.M. Successful nutrition policy: improvement of vitamin D intake and status in Finnish adults over the last decade. Eur J Public Health 2017, 27, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Ikonen, H.; Lumme, J.; Seppala, J.; Pesonen, P.; Piltonen, T.; Jarvelin, M.R.; Herzig, K.H.; Miettunen, J.; Niinimaki, M.; Palaniswamy, S. , et al. The determinants and longitudinal changes in vitamin D status in middle-age: a Northern Finland Birth Cohort 1966 study. Eur J Nutr 2021, 60, 4541–4553. [Google Scholar] [CrossRef] [PubMed]
- Rooney, M.R.; Harnack, L.; Michos, E.D.; Ogilvie, R.P.; Sempos, C.T.; Lutsey, P.L. Trends in Use of High-Dose Vitamin D Supplements Exceeding 1000 or 4000 International Units Daily, 1999-2014. JAMA 2017, 317, 2448–2450. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.M.; Song, M.; Zhang, X.; Pan, A.; Wang, M.; Fuchs, C.S.; Le, N.; Chan, A.T.; Willett, W.C.; Ogino, S. , et al. Processed and Unprocessed Red Meat and Risk of Colorectal Cancer: Analysis by Tumor Location and Modification by Time. PLoS One 2015, 10, e0135959. [Google Scholar] [CrossRef] [PubMed]
- Manson, J.E.; Cook, N.R.; Lee, I.M.; Christen, W.; Bassuk, S.S.; Mora, S.; Gibson, H.; Gordon, D.; Copeland, T.; D'Agostino, D. , et al. Vitamin D Supplements and Prevention of Cancer and Cardiovascular Disease. N Engl J Med 2019, 380, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Dawson-Hughes, B.; Staten, M.A.; Knowler, W.C.; Nelson, J.; Vickery, E.M.; LeBlanc, E.S.; Neff, L.M.; Park, J.; Pittas, A.G.; Group, D.d.R. Intratrial Exposure to Vitamin D and New-Onset Diabetes Among Adults With Prediabetes: A Secondary Analysis From the Vitamin D and Type 2 Diabetes (D2d) Study. Diabetes Care 2020, 43, 2916–2922. [Google Scholar] [CrossRef] [PubMed]
- Gezen-Ak, D.; Dursun, E. Vitamin D, a Secosteroid Hormone and Its Multifunctional Receptor, Vitamin D Receptor, in Alzheimer’s Type Neurodegeneration. J. Alz. Disease 2023, 95, 1273–1299. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Ta, Q.T.H.; Nguyen, T.T.D.; Le, T.T.; Vo, V.G. Role of Insulin Resistance in the Alzheimer's Disease Progression. Neurochem Res 2020, 45, 1481–1491. [Google Scholar] [CrossRef] [PubMed]
- Szymczak-Pajor, I.; Sliwinska, A. Analysis of Association between Vitamin D Deficiency and Insulin Resistance. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Wenclewska, S.; Szymczak-Pajor, I.; Drzewoski, J.; Bunk, M.; Sliwinska, A. Vitamin D Supplementation Reduces Both Oxidative DNA Damage and Insulin Resistance in the Elderly with Metabolic Disorders. Int J Mol Sci 2019, 20. [Google Scholar] [CrossRef] [PubMed]
- Lason, W.; Jantas, D.; Leskiewicz, M.; Regulska, M.; Basta-Kaim, A. The Vitamin D Receptor as a Potential Target for the Treatment of Age-Related Neurodegenerative Diseases Such as Alzheimer's and Parkinson's Diseases: A Narrative Review. Cells 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- SanMartin, C.D.; Henriquez, M.; Chacon, C.; Ponce, D.P.; Salech, F.; Rogers, N.K.; Behrens, M.I. Vitamin D Increases Abeta140 Plasma Levels and Protects Lymphocytes from Oxidative Death in Mild Cognitive Impairment Patients. Curr Alzheimer Res 2018, 15, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Michaud, T.L.; Su, D.; Siahpush, M.; Murman, D.L. The Risk of Incident Mild Cognitive Impairment and Progression to Dementia Considering Mild Cognitive Impairment Subtypes. Dement Geriatr Cogn Dis Extra 2017, 7, 15–29. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.; T, O.C.; Johnson, S.; Cline, S.; Merikle, E.; Martenyi, F.; Simpson, K. Estimating Alzheimer's Disease Progression Rates from Normal Cognition Through Mild Cognitive Impairment and Stages of Dementia. Curr Alzheimer Res 2018, 15, 777–788. [Google Scholar] [CrossRef] [PubMed]
- Pettersen, J.A. Does high dose vitamin D supplementation enhance cognition?: A randomized trial in healthy adults. Exp Gerontol 2017, 90, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.; Hu, J.; Huo, X.; Miao, R.; Zhang, Y.; Ma, F. Effects of vitamin D supplementation on cognitive function and blood Abeta-related biomarkers in older adults with Alzheimer's disease: a randomised, double-blind, placebo-controlled trial. J Neurol Neurosurg Psychiatry 2019, 90, 1347–1352. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Song, M.; Eliassen, A.H.; Wang, M.; Fung, T.T.; Clinton, S.K.; Rimm, E.B.; Hu, F.B.; Willett, W.C.; Tabung, F.K. , et al. Optimal dietary patterns for prevention of chronic disease. Nat Med 2023, 29, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Kroll, M.H.; Bi, C.; Garber, C.C.; Kaufman, H.W.; Liu, D.; Caston-Balderrama, A.; Zhang, K.; Clarke, N.; Xie, M.; Reitz, R.E. , et al. Temporal relationship between vitamin D status and parathyroid hormone in the United States. PLoS One 2015, 10, e0118108. [Google Scholar] [CrossRef] [PubMed]
- Sempos, C.T.; Heijboer, A.C.; Bikle, D.D.; Bollerslev, J.; Bouillon, R.; Brannon, P.M.; DeLuca, H.F.; Jones, G.; Munns, C.F.; Bilezikian, J.P. , et al. Vitamin D assays and the definition of hypovitaminosis D: results from the First International Conference on Controversies in Vitamin D. Br J Clin Pharmacol 2018, 84, 2194–2207. [Google Scholar] [CrossRef] [PubMed]
- Pludowski, P.; Grant, W.B.; Karras, S.N.; Zittermann, A.; Pilz, S. Vitamin D Supplementation: A Review of the Evidence Arguing for a Daily Dose of 2000 International Units (50 microg) of Vitamin D for Adults in the General Population. Nutrients 2024, 16, 391. [Google Scholar] [CrossRef] [PubMed]
- Jamka, M.; Wozniewicz, M.; Walkowiak, J.; Bogdanski, P.; Jeszka, J.; Stelmach-Mardas, M. The effect of vitamin D supplementation on selected inflammatory biomarkers in obese and overweight subjects: a systematic review with meta-analysis. Eur J Nutr 2016, 55, 2163–2176. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Scatter plot of risk ratios (RRs) for dementia with respect to mean follow-up period less than 15 years from Figure 2 in Zhang and colleagues (2024) [9] plus Chen and colleagues (2024) [10] but omitting Féart and colleagues (2017) [17]. 95% CI, 95% confidence interval.
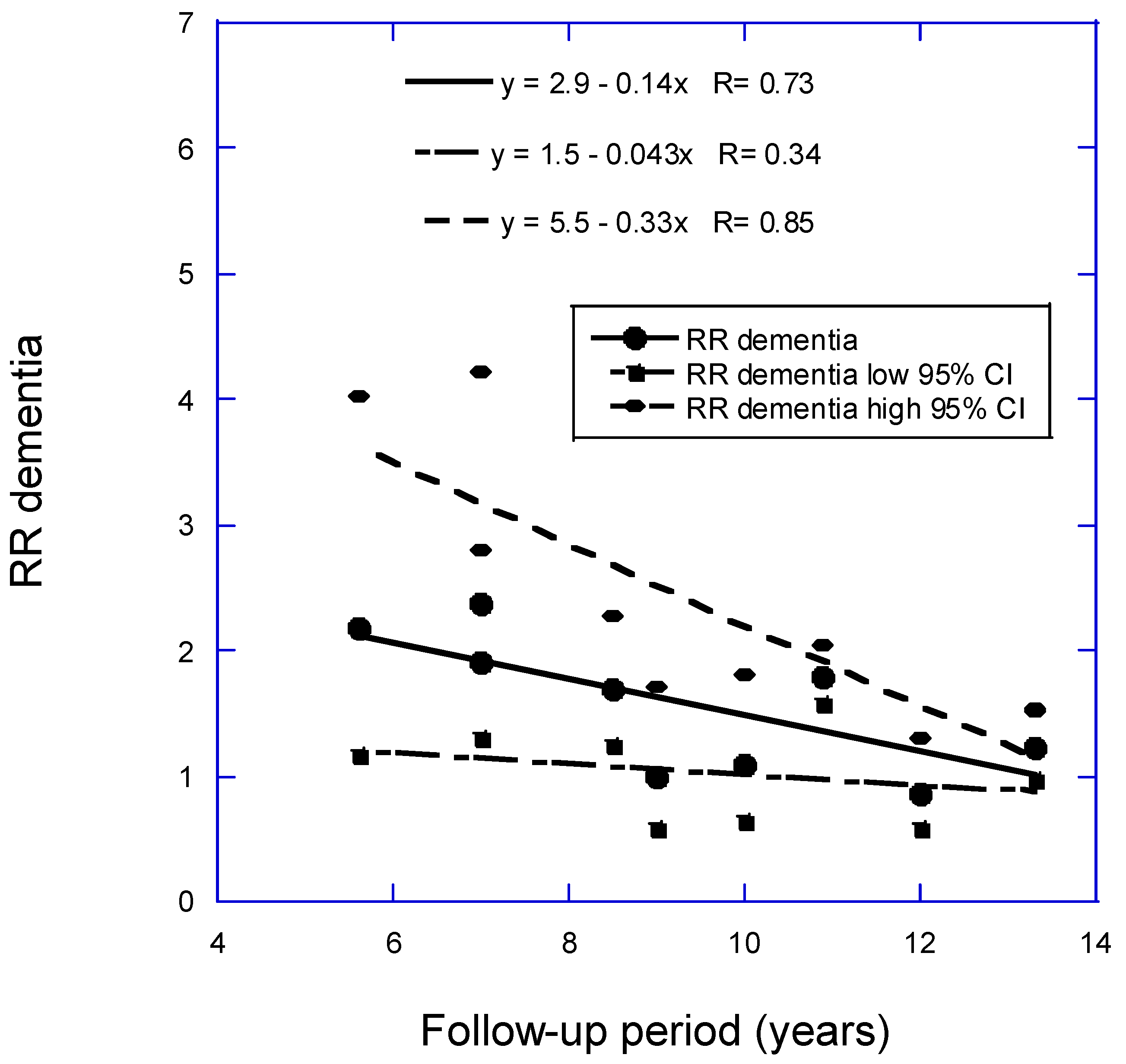
Figure 2.
Risk ratios (RRs) for AD versus 25(OH)D versus mean follow-up period from Figure 3a in Zhang and colleagues (2024) [9] plus Chen and colleagues (2024) [10] but omitting Féart and colleagues (2017) [17]. 95% CI, 95% confidence interval.
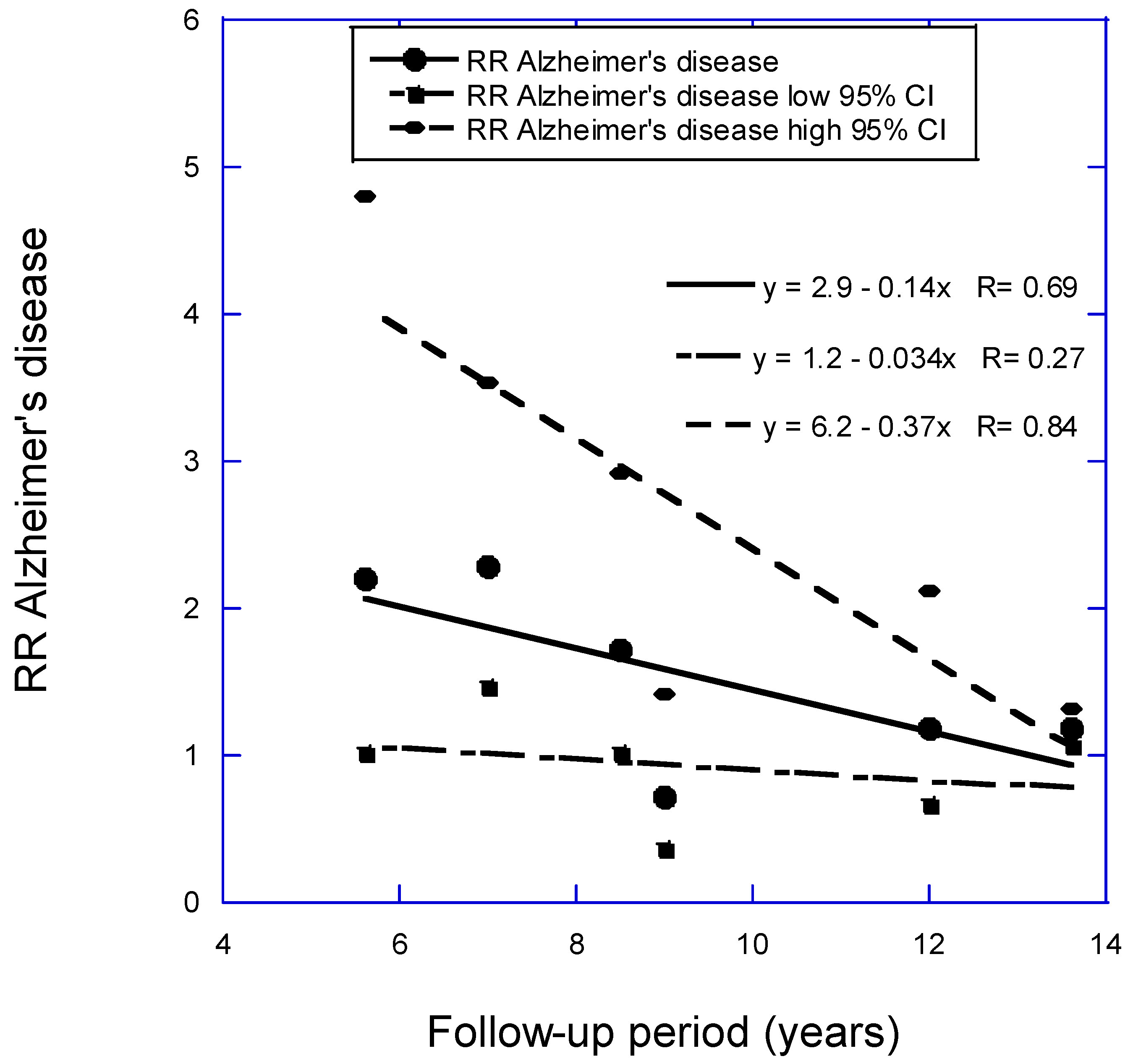
Figure 3.
Cognitive impairment versus 25(OH)D concentration with regression fit to follow-up period for six studies with mean follow-up periods from 5 to 13 years from Figure 3b in Zhang and colleagues (2024) [9]. 95% CI, 95% confidence interval; RR, risk ratio.
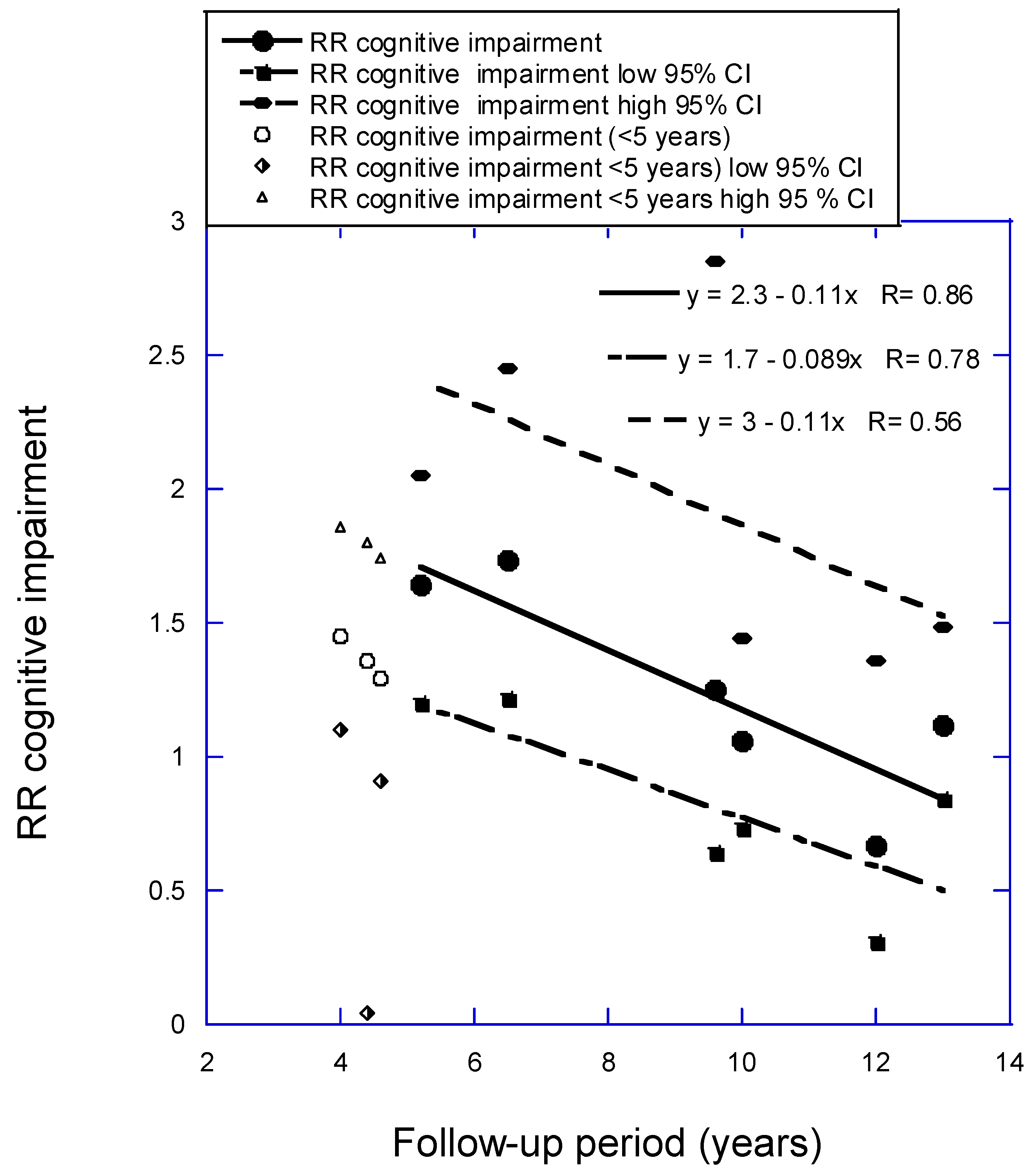
Table 1.
a. Data for vitamin D deficiency and risk of dementia or Alzheimer’s disease from Figure 2 and Figure 3a in Zhang and colleagues (2024) [9].
| Country | Mean age (SD) (yrs) |
NT | ND | NAD | Author, yr, Ref.* |
|---|---|---|---|---|---|
| USA | 74 ±5 | 1658 | 171 | 102 | (Littlejohns, 2014) [11] |
| Germany | 84 ± 3 | 861 F, 473 M | 250 | 209 | (van Lent, 2022) [12] |
| Israel | 53 ± 17 | 2454 F, 1824 M | 133 | Kiderman, 2023) [13] | |
| UK | 64.6 | 13,486 | 283 | 101 | (Geng, 2022) [14] |
| USA | 72 ± 7 | 1663 | 267 | 208 | (Karakis, 2016) [15] |
| Norway | 78 | 790 F, 644 M | (Asante, 2023) [16] | ||
| France | 73 (5 | 916 | 177 | 124 | (Féart, 2017) [17] |
| Sweden | 71 | 1182 M | 250 M | 116 M | (Olsson, 2017) [18] |
| Netherlands | 69 ± 8 | 3462 F, 2625 M | 795 | 641 | (Licher, 2017) [19] |
| UK | 62 ± 3 | 140,857 F, 128,372 M | 7087 | 3616 | (Chen, 2024) [10] |
| Omitted | |||||
| Switzerland | 85 ± 7 | 147 F, 53 M | 46 | (Graf, 2014) [20] | |
| USA | 62 | 793 B, 859 W | 145 | (Schneider, 2014) [21] | |
| Finland | Cases: 69 ± 7 Noncases: 56 ± 10 |
2724 F, 2286 M | 100 F, 51 M |
(Knekt, 2014) [22] | |
| USA | 57 ± 6 | 13,039 | 1323 | (Fashanu, 2019) [23] | |
| Denmark | 58 | 10,186 | 418 | 92 | (Afzal, 2014) [24] |
Table 1.
b. Data for vitamin D deficiency and risk of dementia or Alzheimer’s disease from Figure 2 and Figure 3a in Zhang and colleagues (2024) [9].
| Mean BMI (SD) (kg/m2) |
Mean 25(OH)D (SD) (nmol/L) | 25(OH)D comparison (nmol/L) |
Mean follow-up (yrs) |
HR or OR (95% CI) |
Author, yr, Ref.* |
|---|---|---|---|---|---|
| 27 ± 5 | <25 vs. >50 | 5.6 | * | (Littlejohns, 2014) [11] | |
| 26 ± 4 | 37.0 (IQR 24.8–58.3) |
<25 vs. >50 | 7 | * | (van Lent, 2022) [12] |
| 27 ± 6 | 54 ± 24 | <25 vs. >50 | 7 | * | Kiderman, 2023) [13] |
| 31 ± 5 | <25 vs. >50 | 8.5 | 1.69 (1.25‒2.27) | (Geng, 2022) [14] | |
| 27 ± 5 | 63 ± 28 | 9 | * | (Karakis, 2016) [15] | |
| 27 ± 3 | 50 ± 21 | <50 vs. >50 | 10 | 1.09 (0.64‒1.83) | (Asante, 2023) [16] |
| 26 ± 4 | <50 vs. >50 | 11.4 | * | (Féart, 2017) [17] | |
| 26 ± 3 | 69 ± 19 | <50 vs. ≥75 | 12 | * | (Olsson, 2017) [18] |
| 27 ± 4 | 49 (IQR 30‒69) | <25 vs. >50 | 13.3 | * | (Licher, 2017) [19] |
| 27 ± 4 | 50 ± 21 | <50 vs. >50 | 13.6 | * | (Chen, 2024) [10] |
| Omitted | |||||
| 23 ± 4 | 32 ± 25 | <25 vs. >75 | 2 | * | (Graf, 2014) [20] |
| 27 ± 5, W 30 ± 6, B |
64 ± 20 W; 43 ± 16 B |
High vs. low tertile | 16.6 | * | (Schneider, 2014) [21] |
| 26 ± 4 | Cases: 40 ± 20 Noncases: 43 ± 17 |
High vs. low quartile | 17 | * | (Knekt, 2014) [22] |
| 28 ± 5 | 61 ± 22 | <25 vs. >50 | 20 | * | (Fashanu, 2019) [23] |
| 25 ± 3 | 45 (M) 40 (F) |
<25th vs. >50th percentile | 30 | * | (Afzal, 2014) [24] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



