
Submitted:
13 August 2024
Posted:
14 August 2024
You are already at the latest version
Abstract
Reproductive disorders are a common event in modern reproductive medicine, occurring both in spontaneous and assisted pregnancies. Studies of the molecular mechanisms of implantation disorders in thin endometrium, including the study of gene transcriptional activity, have shed light on the identification of potential biological markers of endometrial receptivity. Background/Objectives: to reveal significantly dysregulated selected genes expression between RIF and RPL patients with thin endometrium. Methods: Endometrial samples were collected in the implantation window days (LH+7 – LH+10) of the natural menstrual cycle from RIF patients (n=20) and RPL patients (n=19). Ten genes were chosen as target genes regarding their possible relations with the implantation process. Total RNA was purified, reverse-transcribed; gene expression was quantified by RT-PCR. Results: The expression of the IL-15, INFG and HPRT1 genes were significantly decreased in RIF with thin endometrium patients compared to the RPL patients (log2 fold change=0.92, p=0.023 for IL-15, log2 fold change=1.24, p=0.046 for INFG, and log2 fold change=0.579, p=0.046 for HPRT1). There were not significant differences in expression of CXCL8, CXCL1, MMP10, C4BPA, TNC, VEGFB and HAND2 genes between groups. Conclusions: decreased expression of IL-15, INFG and HPRT1 genes was found in patients with RIF with thin endometrium compared to the endometrium of women with RPL. This has practical significance for clinicians for differentiated prescription of immunomodulatory therapy in patients undergoing ART programs.
Keywords:
endometrial receptivity
; recurrent implantation failure
; recurrent pregnancy loss
; thin endometrium
; transcriptomics
1. Introduction
Reproductive disorders are a common event in modern reproductive medicine, occurring both in spontaneous and assisted pregnancies [1]. The causes of adverse reproductive outcomes are multifactorial, in one third of cases it is due to the quality of the embryo and in two-thirds - to abnormal endometrial receptivity [2]. Receptive endometrium is not a binary state (all-or-nothing), rather the degree and type of abnormal receptivity leads to a range of reproductive problems: from complete recurrent implantation failure (RIF) or infertility to severe pregnancy loss (RPL) or miscarriage and mild implantation failure and invasion (preeclampsia) [3]. Despite the importance of endometrial receptivity for implantation, the precise mechanisms involved in regulation of endometrial receptivity remain poorly understood [4].
Abnormal receptivity is also associated with thin endometrium (endometrial thickness less than 7 mm during the “implantation window”), the exact etiology and physiopathology of this condition remain largely unclear [5,6]. And existing treatments are unable to achieve satisfactory clinical effects in many patients with thin endometrium [7]. Studies of the molecular mechanisms of implantation disorders in thin endometrium, including the study of gene transcriptional activity, have shed light on the identification of potential biological markers of endometrial receptivity [8,9,10].
In the receptive phase of the endometrium in healthy women, a large number of genes representing various signaling pathways and meta-signatures are differentially expressed [11,12]. However, many researchers propose to use the most frequently occurring genes for further analysis [13,14]. Gene ontology analysis revealed that widespread meta-signatures are represented by immune response genes, including pro-inflammatory signaling cascade - C-X-C motif chemokine ligand 8 (CXCL8) and C-X-C motif chemokine ligand 1 (CXCL1), complement cascade - Complement Component 4 Binding Protein Alpha (C4BPA), abnormal activation of the innate and adaptive immune system - interleukin 15 (IL-15), Heart- and neural crest derivatives-expressed transcript 2 (HAND2), interferon gamma (INFG), vascular proliferation - vascular endothelial growth factor B (VEGF-B), breakdown of extracellular matrix and tissue remodeling - Matrix metallopeptidase 10 (MMP10), generation of purine nucleotides - Hypoxanthine phosphoribosyltransferase 1 (HPRT1) and cell adhesion - Tenascin C (TNC) [15,16,17,18,19].
In this study, we took 10 of the above-mentioned genes (CXCL8, CXCL1, HPRT1, MMP10, INFG, C4BPA, TNC, VEGFB, HAND2 and IL15) that showed altered activity in the receptive phase in healthy women. The research question is whether the expression of the selected genes will differ in thin endometrium with clinical forms of implantation disorders (RIF, RPL), and if there are differences, then in what direction should therapeutic approaches be developed.
2. Materials and Methods
2.1. Subjects
The study was conducted among women who applied to the Scientific Center of Obstetrics, Gynecology and Perinatology (Kazakhstan, Almaty) for reproductive disorders from September to December 2023. The inclusion criteria on the group were the presence of a thin endometrium (less than 7 mm during the implantation window during ultrasound examination) and a history of reproductive losses in anamnesis – RPL or RIF.
RPL was defined based on ESHRE guidelines of 2 or more miscarriage confirmed by positive human chorionic gonadotropin [20]. RIF was at least 3 unsuccessful transfers of good-quality embryos after in vitro fertilization-embryo transfer [21]. In addition, the woman's age was < 40 years, without karyotype anomalies.
A total of 39 patients were recruited for transcriptional analysis (20 RIF and 19 RPL patients). Demographic and clinical characteristics of the study groups are presented in Table 1.
After clinical characteristics were compared between two groups, no statistical differences were found by age and BMI. All participants were under 40 years of age. Prothrombin time was significantly reduced in the RIF group (p<0.05), which indicates a patient's tendency to thrombotic vascular lesions. There were no significant differences between the groups in blood hormone levels.
2.2. Ethics Approval
This study was approved by the Ethical Committee of Al Farabi Kazakh National University, Kazakhstan (Code: IRBA400/IRB 00010790). All patients have been asked to sign a written informed consent.
2.3. Sample Processing
Endometrial samples were obtained by Pipelle biopsy using Goldstein catheter (SonoBiopsyTM J-GSBX-072026 size (Fr) 7.2 Cook Incorporated, USA), in LH+7 – LH+10 days (the implantation window) of the natural menstrual cycle. Samples from RPL (n=19) and RIF patients (n=20) with thin endometrium were transferred into Cryotubes with 1 ml of RNA-later stabilization solution (Thermo Fisher Scientific) in a refrigerator 4°C for 12 h, and the next day to store in freezer −20°C. After sample collection was completed, they were transferred to M. Aitkhozhin Institute of Molecular Biology and Biochemistry (Almaty, Kazakhstan).
2.4. RNA Isolation from Endometrial Samples
Isolation of total RNA from endometrial samples was performed using Dynabeads™ mRNA DIRECT™ Purification Kit (Thermo Fisher Scientific) according to the manufacturer’s protocol. The isolated RNA was immediately subjected to further analysis.
2.5. cDNA Synthesis and Quantitative Polymerase Chain Reaction (PCR)
Reverse-transcription and quantitative PCR was performed using primers and probes from TaqMan™ Gene Expression Assay (Applied Biosystems, USA). cDNA was obtained using High-capacity cDNA Reverse Transcription Kit (Applied Biosystems) according to the manufacturer’s protocol. Quantitative PCR was performed in duplicates using TaqMan Fast Advanced Master Mix (Applied Biosystems) under the conditions recommended by the manufacturer on the StepOnePlus Real-Time PCR System (Applied Biosystems). Primary processing was performed using StepOnePlus 2.2.2 and ExpressionSuite v1.3 programs. Relative quantification of gene expression is carried out using the comparative Ct (ΔΔCt) method with modifications as described by Königshoff M. et al. (2009) [22]. Relative transcript abundance is expressed in ΔCt values (ΔCt = Ctreference − Cttarget). Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and tyrosine 3-monooxygenase/tryptophan 5-monooxygenase activation protein zeta (YWHAZ) housekeeping genes was used as a reference, in accordance with previous study [11]. ΔΔCt value (ΔΔCt = ΔCtcase − ΔCtcontrol) was considered as log2 fold change.
2.6. Statistical Analysis
Most of the statistics were performed in the Jamovi program (https://www.jamovi.org). Statistical significance of the differences in ΔCt between the groups was calculated using the two-tailed Mann–Whitney U test. Spearman's rank correlation method was used to examine the relationship between quantitative variables. P<0.05 was considered statistically significant. Due to the explorative nature of the study no adjustment for multiple testing was performed. For a comparative visualization of gene expression levels, box plots were constructed using a web tool BoxPlotR (http://shiny.chemgrid.org/boxplotr). The characteristics of the markers were evaluated by ROC analysis using the web-tool easy ROC [23], and Jamovi. Youden’s index method was used to calculate optimal cut-off points. Evaluation of classifiers by interpretation of the area under the ROC curve (AUC) was performed as described by [24].
3. Results
3.1. The Level of mRNA in Endometrial Samples of RIF Patients in Comparison with RPL Patients
Comparative gene expression statistics between RPL and RIF patients are presented in Table 2.
The study showed that the expression of 3 out of 10 genes differs significantly between the studied groups. It was found, that the expression of the IL-15, INFG and HPRT1 genes were significantly decreased in RIF with thin endometrium patients compared to the RPL patients (log2 fold change=0.92, p=0.023 for IL-15, log2 fold change=1.24, p=0.046 for INFG, and log2 fold change=0.579, p=0.046 for HPRT1) (Figure 1). There were not significant differences in expression of CXCL8, CXCL1, MMP10, C4BPA, TNC, VEGFB and HAND2 genes between groups.
3.2. Associations with Clinical and Laboratory Characteristics
Spearman's rank correlation method was used to examine the relationship between expression of studied genes and quantitative laboratory characteristics in two groups. The correlations are presented in Table 3. In patients with RIF, significant inverse moderate correlations were observed between HAND2 and TSH (rho = -0.671, p = 0.001), HAND2 and fibrinogen (rho = -0.465, p = 0.038), VEGFB and prolactin (rho = -0.446, p = 0.049), VEGFB and TSH (rho = -0.526, p = 0.017). In patients with RPL significant inverse moderate correlations have been established between CXCL1 and prothrombin time (rho = -0.456, p = 0.04959), MMP10 and Activated Partial Thromboplastin Time (rho = -0.494, p = 0.0317); direct moderate correlation between CXCL1 and Activated Partial Thromboplastin Time (rho = 0.587, p = 0.0083). It should be noted, that after adjustment for multiple comparisons none correlations remained significant.
3.3. ROC Analysis
We performed ROC analysis to evaluate the potential of using mRNA of genes differentially expressed in the endometrium of RIF patients as markers for predicting RIF. The results are presented in Table 4. The areas under the ROC curve (AUC) were obtained for IL-15 (0.713), INFG (0.701) and HPRT1 (0,692) (Figure 2). The best combination was the combination of IL-15 and HPRT1 resulted in an increase in AUC to 0.800 (with a specificity of 68.4% and a sensitivity of 85.0%).
4. Discussion
The use of Kyoto Encyclopedia of Genes and Genomes and Gene ontology databases for functional enrichment of genes has yielded significant results in reproductive medicine [17,25]. The endometrial receptivity in healthy women has been associated with up-regulation of a large number of genes in the receptive phase of the endometrium [26,27,28,29,30], including angiogenesis [15], metabolism, extracellular matrix and tissue remodeling [17], immune response [18,19], and cell adhesion [31].
Dysregulation at the endometrial level in patients suffering from implantation disorders (RIF, RPL) have functional similarities [25]. At the same time, patients with RIF have a defect in endometrial receptivity that alters the embryo-endometrium dialogue and prevents implantation, while RPL is characterized by optimal receptivity with a defect in embryo selectivity, allowing abnormal embryos to implant and increasing the risk of miscarriage [32]. The mechanisms leading to RIF may be either depletion of cytokines required for apposition-adhesion, or excess of cytokines leading to local cytotoxicity that may disrupt embryo implantation [18].
Our study is devoted to how significant the differences in gene expression in thin endometrium will be between RIF and RPL patients. In this study, gene expression of RIF patients with thin endometrium along with the matched endometrial tissues from RPL patients were explored, and we revealed the abnormal activation of the inflammatory environment in thin endometrium. We would like to highlight that immune response changes at the endometrial level were statistically significantly impaired in RIF group. It was found, that the expression of the IL-15, INFG and HPRT1 genes were significantly decreased in RIF with thin endometrium patients compared to the RPL patients (p=0.023, p=0.046 for INFG, and p=0.046, respectively).
IL-15 is key immune factor required for the activation and survival of uterine natural killer (uNK), activated uNK cells can promote spiral artery remodeling and secrete cytokines to induce immunotolerance [19]. The expression of IL-15 has been shown to be different in patients with RIF compared with fertile controls and correlates with local uNK (CD56+) recruitment and angiogenesis, also IL-15 mRNA levels in the mid-luteal endometrium were positively correlated with CD56+ uNK cells (r = .392, P = .008) [33].
In our study, the down-regulation of interferon gamma (INFG) gene in RIF patients with thin endometrium indicates to NK cell deficiency. NK cells are the main source of IFNG production [34]. Recent study [35] shown that the peripheral blood level of IFNG in the RPL group was significantly higher than the RIF group (P<0.05). A decrease in the production of INFG indicates the presence of acute and chronic viral diseases [36]. This indicates a significant pathogenetic mechanism of implantation failure associated with infection, which must be taken into account in the rehabilitation of patients with RIF.
This study demonstrated down-regulation of Hypoxanthine phosphoribosyltransferase 1 (HPRT1) gene in RIF patients. The protein encoded by this gene is a transferase that plays a central role in the formation of purine nucleotides via the purine salvage pathway by catalyzing the conversion of hypoxanthine. This gene was also selected for the ER Map®/ER Grade® panel as being involved in biological processes occurring in the preimplantation endometrium [11]. The purine hypoxanthine plays an important role in the regulation of oocyte maturation and early embryonic development; HPRT deficiency in rats disrupts early embryonic development and causes infertility in females [37]. This finding suggests the presence of metabolic disturbances in RIF associated with a thin endometrium. However, HPRT deficiency is a rare disorder, and therefore the decrease in the activity of this enzyme in receptivity disorders needs to be studied. Present study showed that patients with RIF and RPL had significant (p<0.05) inverse moderate correlations. Thus, a decrease in the level of the above-studied genes was associated with an increase in the level of pituitary hormones and activation of the hemostasis system.
The study confirms that the RIF and RPL populations are extremely heterogeneous, despite the similarity of risk factors, there are differences in the expression of genes. However, the prognostic potential of the IL-15, INFG genes and their combinations for the development of therapeutic approaches in women with RIF and thin endometrium was shown. The limitations of this study were the small sample size, which should be taken into account in the future, and stratification by clinical forms is recommended. Further studies are needed to confirm the observed changes in gene expression at the proteome and metabolome levels.
5. Conclusions
The study revealed a decrease in the expression of IL-15, INFG and HPRT1 genes in the thin endometrium of RIF patients compared to women with RPL. These data contribute to understanding the processes in the thin endometrium leading to implantation failures during IVF, and are also of practical significance for clinicians for differentiated prescription of immunomodulatory therapy in patients undergoing ART programs.
Author Contributions
Conceptualization, A.K., Y.A., G.K. and N.M.; Funding acquisition, G.A., G.M., and A.T.; Investigation, Y.A.; Methodology, A.K., Y.A., G.K., N.M., D.S.; Resources, A.K., G.A., G.M. and Zh.Zh.; Supervision, N.M.; Validation, Zh.Zh.; Visualization, G.M.; Writing – original draft, A.K., Y.A. and Zh.Zh.; Writing – review & editing, A.K., Y.A., G.K., N.M., G.A., G.M., D.S., A.T. and Zh.Zh. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Science Committee of the Ministry of Science and High Education of the Republic of Kazakhstan (Grant No. AP 14870089).
Institutional Review Board Statement
This study was approved by the Ethical Committee of Al Farabi Kazakh National University, Kazakhstan (Code: IRBA400/IRB 00010790).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Experimental and clinical-pathological data is available.
Acknowledgments
The authors are appreciative to clinicians of the Scientific Center of Obstetrics, Gynecology and Perinatology, of the Institute of Reproductive Medicine (Almaty) and scientists of M. Aitkhozhin Institute of Molecular Biology and Biochemistry.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Wang, X.; Yu, Q. An update on the progress of transcriptomic profiles of human endometrial receptivity. Biol Reprod. 2018, 98, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Harrity, C.; Shkrobot, L.; Walsh, D.; Marron, K. ART implantation failure and miscarriage in patients with elevated intracellular cytokine ratios: response to immune support therapy. Fertil Res Pract. 2018, 4, 7. [Google Scholar] [CrossRef] [PubMed]
- Lessey, B.A.; Young, S.L. What exactly is endometrial receptivity? Fertil Steril. 2019, 111, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Zhou, W.; Sacco, M.; Downing, P.; Dimitriadis, E.; Zhao, F. Using organoids to investigate human endometrial receptivity. Front. Endocrinol. 2023, 14, 1158515. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, R.; Taketani, T.; Mihara, Y.; Sato, S.; Okada, M.; Tamura, I.; Jozaki, K.; Kajimura, T.; Asada, H.; Tamura, H.; Takasaki, A.; Sugino, N. Thin endometrium transcriptome analysis reveals a potential mechanism of implantation failure. Reprod Med Biol. 2017, 16, 206–227. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Lu, H.; Yu, X.; Dong, L.; Mi, L.; Wang, J.; Zheng, X.; Feng, K. The effect of icariin for infertile women with thin endometrium: A protocol for systematic review. Medicine (Baltimore). 2020, 99, e19111. [Google Scholar] [CrossRef] [PubMed]
- Azizi, R.; Aghebati-Maleki, L.; Nouri, M.; Marofi, F.; Negargar, S.; Yousefi, M. Stem cell therapy in Asherman syndrome and thin endometrium: stem cell-based therapy. Biomed. Pharmacother. 2018, 102, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Yao, G.; Wang, Y.; Xu, H.; Ji, X.; He, Y.; Zhu, Q.; Chen, Z.; Sun, Y. Transcriptomic changes during the pre-receptive to receptive transition in human endometrium detected by RNA-seq. J Clin Endocrinol Metab. 2014, 99, E2744–E2753. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.; Matthews, D. A.; Bessant, C. High Throughput Discovery of Protein Variants Using Proteomics Informed by Transcriptomics. Nucleic Acids Res. 2018, 46, 4893–4902. [Google Scholar] [CrossRef] [PubMed]
- Zong, L.; Zheng, S.; Meng, Y.; Tang, W.; Li, D.; Wang, Z.; Tong, X.; Xu, B. Integrated Transcriptomic Analysis of the miRNA-mRNA Interaction Network in Thin Endometrium. Front Genet. 2021, 16, 12–589408. [Google Scholar] [CrossRef] [PubMed]
- Enciso, M.; Carrascosa, J.P.; Sarasa, J.; Martínez-Ortiz, P.A.; Munné, S.; Horcajadas, JA.; Aizpurua, J. Development of a new comprehensive and reliable endometrial receptivity map (ER Map/ER Grade) based on RT-qPCR gene expression analysis. Hum Reprod. 2018, 33, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Messaoudi, S.; El Kasmi, I.; Bourdiec, A.; Crespo, K.; Bissonnette, L.; Le Saint, C.; Bissonnette, F.; Kadoch, I.-J. 15 years of transcriptomic analysis on endometrial receptivity: What have we learnt? Fertil. Res. Pract. 2019, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Altmäe, S.; Koel, M.; Võsa, U.; Adler, P.; Suhorutšenko, M.; Laisk-Podar, T.; Kukushkina, V.; Saare, M.; Velthut-Meikas, A.; Krjutškov, K.; Aghajanova, L.; Lalitkumar, P.G.; Gemzell-Danielsson, K.; Giudice, L.; Simón, C.; Salumets, A. Meta-signature of human endometrial receptivity: a meta-analysis and validation study of transcriptomic biomarkers. Sci Rep. 2017, 7, 10077. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Fan, Y.; Wang, J.; Shi, R. Dysfunctional intercellular communication and metabolic signaling pathways in thin endometrium. Front. Physiol. 2022, 13, 1050690. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Kumar, A.; Zhang, F.; Lee, C.; Tang, Z. Complicated life, complicated VEGF-B. Trends Mol Med. 2012, 18, 119–27. [Google Scholar] [CrossRef] [PubMed]
- Albayrak, İ.G.; Azhari, F.; Çolak, E.N.; Balcı, B.K.; Ülgen, E.; Sezerman, U.; Baştu, E.; Günel, T. Endometrial gene expression profiling of recurrent implantation failure after in vitro fertilization. Mol Biol Rep. 2021, 48, 5075–5082. [Google Scholar] [CrossRef] [PubMed]
- Basatvat, S.; Russell, J.M.; Saare, M.; Thurston, L.M.; Salumets, A.; Fazeli, A. Potential innate immunity-related markers of endometrial receptivity and recurrent implantation failure (RIF). Reprod Biol. 2021, 21, 100569. [Google Scholar] [CrossRef] [PubMed]
- Lédée, N.; Petitbarat, M.; Rahmati, M.; Dubanchet, S.; Chaouat, G.; Sandra, O.; Perrier-d'Hauterive, S.; Munaut, C.; Foidart, J.M. New pre-conception immune biomarkers for clinical practice: interleukin-18, interleukin-15 and TWEAK on the endometrial side, G-CSF on the follicular side. J Reprod Immunol. 2011, 88, 118–23. [Google Scholar] [CrossRef] [PubMed]
- Murata, H.; Tanaka, S.; Tsuzuki-Nakao, T.; Kido, T.; Kakita-Kobayashi, M.; Kida, N.; Hisamatsu, Y.; Tsubokura, H.; Hashimoto, Y.; Kitada, M.; Okada, H. The transcription factor HAND2 up-regulates transcription of the IL15 gene in human endometrial stromal cells. J Biol Chem. 2020, 295, 9596–9605. [Google Scholar] [CrossRef] [PubMed]
- Bender Atik, R.; Christiansen, O.B.; Elson, J.; Kolte, A.M.; Lewis, S.; Middeldorp, S.; Nelen, W.; Peramo, B.; Quenby, S.; Vermeulen, N.; Goddijn, M.; ESHRE Guideline Group on RPL. ESHRE guideline: Recurrent pregnancy loss. Hum. Reprod. Open. 2018, 6, hoy004. [Google Scholar] [CrossRef]
- ESHRE Working Group on Recurrent Implantation Failure; Cimadomo D, de Los Santos MJ, Griesinger G, Lainas G, Le Clef N, McLernon DJ, Montjean D, Toth B, Vermeulen N, Macklon N. ESHRE good practice recommendations on recurrent implantation failure. Hum Reprod Open. 2023, 15, hoad023. [Google Scholar] [CrossRef]
- Königshoff, M.; Kramer, M.; Balsara, N.; Wilhelm, J.; Amarie, O.V.; Jahn, A.; Rose, F.; Fink, L.; Seeger, W.; Schaefer, L.; Günther, A.; Eickelberg, O. WNT1-inducible signaling protein-1 mediates pulmonary fibrosis in mice and is upregulated in humans with idiopathic pulmonary fibrosis. Journal of Clinical Investigation. 2009, 119, 772–787. [Google Scholar] [CrossRef] [PubMed]
- Goksuluk, D.; Korkmaz, S.; Zararsiz, G.; Karaagaoglu, A.E. Easy ROC: an interactive web-tool for ROC curve analysis using R language environment. The R Journal. 2016, 8, 213–230. [Google Scholar] [CrossRef]
- Muller, M.P.; Tomlinson, G.; Marrie, T.J.; Tang, P.; McGeer, A.; Low, D.E.; Detsky, A.S.; Gold, W.L. Can routine laboratory tests discriminate between severe acute respiratory syndrome and other causes of community-acquired pneumonia? Clin Infect Dis. 2005, 40, 1079–86. [Google Scholar] [CrossRef] [PubMed]
- Devesa-Peiro, A.; Sebastian-Leon, P.; Garcia-Garcia, F.; Arnau, V.; Aleman, A.; Pellicer, A.; Diaz-Gimeno, P. Uterine disorders affecting female fertility: what are the molecular functions altered in endometrium? Fertil Steril. 2020, 113, 1261–1274. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Yao, S.; Dong, Y.; Liu, D.; Wang, H.; Jiang, P.; Dai, C.; Lv, H.; Cao, C.; Zhou, Z.; Wang, L.; Gou, W.; Zhang, X.; Zhao, G.; Hu, Y. Down-regulation of PBK inhibits proliferation of human endometrial stromal cells in thin endometrium. Reprod Biol Endocrinol. 2022, 20, 25. [Google Scholar] [CrossRef] [PubMed]
- Robertson, S.A.; Moldenhauer, L.M.; Green, E.S.; Care, A.S.; Hull, M.L. Immune determinants of endometrial receptivity: a biological perspective. Fertil Steril. 2022, 117, 1107–1120. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Gao, W.; Li, Y.; Wang, Y.; Liu, L.; Zhang, X. Potential Biomarkers and Endometrial Immune Microenvironment in Recurrent Implantation Failure. Biomolecules. 2023, 13, 406. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Eguren, A.; Bueno-Fernandez, C.; Gómez-Álvarez, M.; Francés-Herrero, E.; Pellicer, A.; Bellver, J.; Seli, E.; Cervelló, I. Evolution of biotechnological advances and regenerative therapies for endometrial disorders: a systematic review. Hum Reprod Update. 2024, dmae013. [Google Scholar] [CrossRef] [PubMed]
- Maziotis, E.; Kalampokas, T.; Giannelou, P.; Grigoriadis, S.; Rapani, A.; Anifantakis, M.; Kotsifaki, A.; Pantou, A.; Triantafyllidou, O.; Tzanakaki, D.; Neofytou, S.; Vogiatzi, P.; Bakas, P.; Simopoulou, M.; Vlahos, N. Commercially Available Molecular Approaches to Evaluate Endometrial Receptivity: A Systematic Review and Critical Analysis of the Literature. Diagnostics 2022, 12, 2611. [Google Scholar] [CrossRef]
- Bastu, E.; Demiral, I.; Gunel, T.; Ulgen, E.; Gumusoglu, E.; Hosseini, M.K.; Sezerman, U.; Buyru, F.; Yeh, J. Potential Marker Pathways in the Endometrium That May Cause Recurrent Implantation Failure. Reprod Sci. 2019, 26, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Macklon, N.S.; Brosens, J.J. The human endometrium as a sensor of embryo quality. Biol Reprod. 2014, 91, 98. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.X.; Wu, X.H. Decreased CD56+CD16-CD94+uNK cells in the mid-luteal phase in women with recurrent implantation failure are associated with IL-15 deficiency. Am J Reprod Immunol. 2023, 90, e13794. [Google Scholar] [CrossRef] [PubMed]
- Bashiri, A.; Halper, K.I.; Orvieto, R. Recurrent Implantation Failure-update overview on etiology, diagnosis, treatment and future directions. Reprod. Biol. Endocrinol. 2018, 16, 21. [Google Scholar] [CrossRef] [PubMed]
- Zargar, M.; Ghafourian, M.; Behrahi, F.; Nikbakht, R.; Salehi, A.M. Association of recurrent implantation failure and recurrent pregnancy loss with peripheral blood natural killer cells and interferon-gamma level. Obstet Gynecol Sci. 2024, 67, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, P.A.S.; Assone, T.; Prates, G.; Tedeschi, M.R.M.; Fonseca, L.A.M.; Casseb, J. The role of IFN-γ production during retroviral infections: an important cytokine involved in chronic inflammation and pathogenesis. Rev Inst Med Trop Sao Paulo. 2022, 30, 64–e64. [Google Scholar] [CrossRef] [PubMed]
- Meek, S.; Sutherland, L.; Wei, J.; Sturmey, R.; Binas, B.; Clinton, M.; Burdon, T. Hypoxanthine phosphoribosyltransferase (HPRT)-deficiency is associated with impaired fertility in the female rat. Mol Reprod Dev. 2020, 87, 930–933. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Differences in gene expression levels (ΔCt values) in endometrial tissue between RIF and RPL patients: (a) IL15 gene; (b) IFNG gene; (c) HPRT1 gene.
Figure 1.
Differences in gene expression levels (ΔCt values) in endometrial tissue between RIF and RPL patients: (a) IL15 gene; (b) IFNG gene; (c) HPRT1 gene.
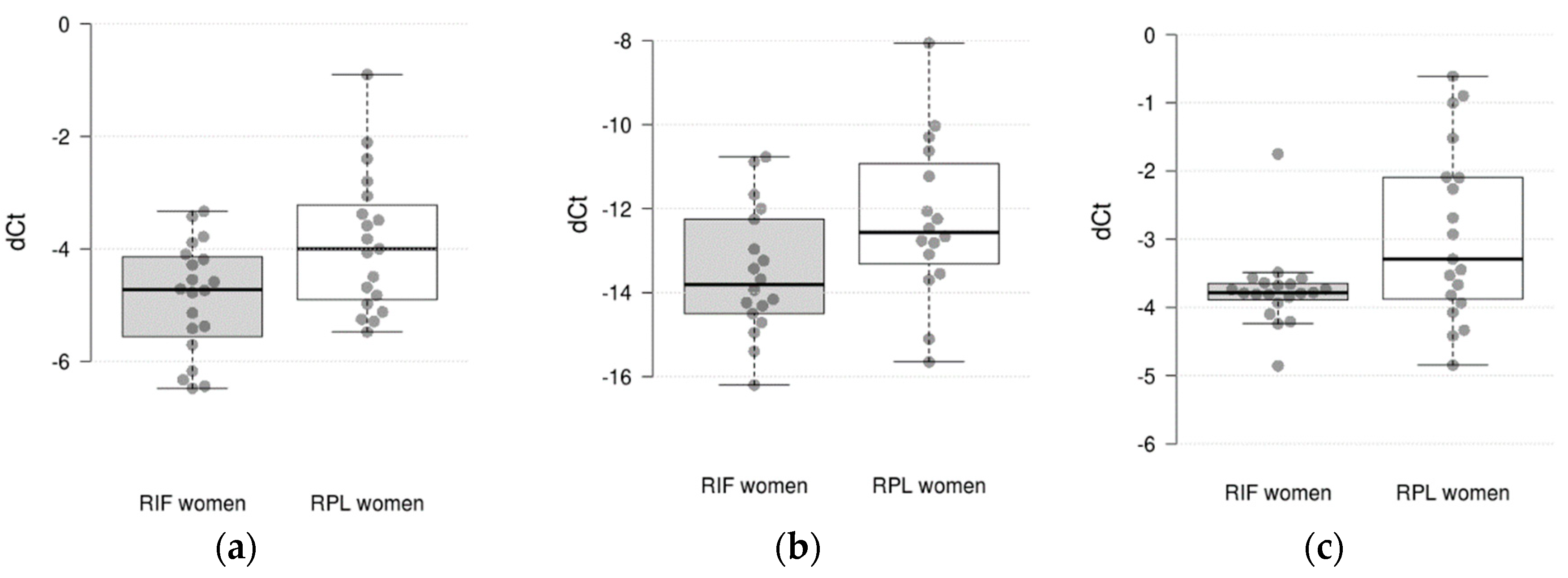
Figure 2.
ROC curves for potential markers and combinations of markers in discrimination RIF and RPL women: (a) IL15; (b) IFNG; (c) HPRT1 (d) combination of IL15 and IFNG; (e) combination of IL15 and HPRT1; (f) combination of IFNG and HPRT1; (g) combination of IL15, IFNG and HPRT1.
Figure 2.
ROC curves for potential markers and combinations of markers in discrimination RIF and RPL women: (a) IL15; (b) IFNG; (c) HPRT1 (d) combination of IL15 and IFNG; (e) combination of IL15 and HPRT1; (f) combination of IFNG and HPRT1; (g) combination of IL15, IFNG and HPRT1.
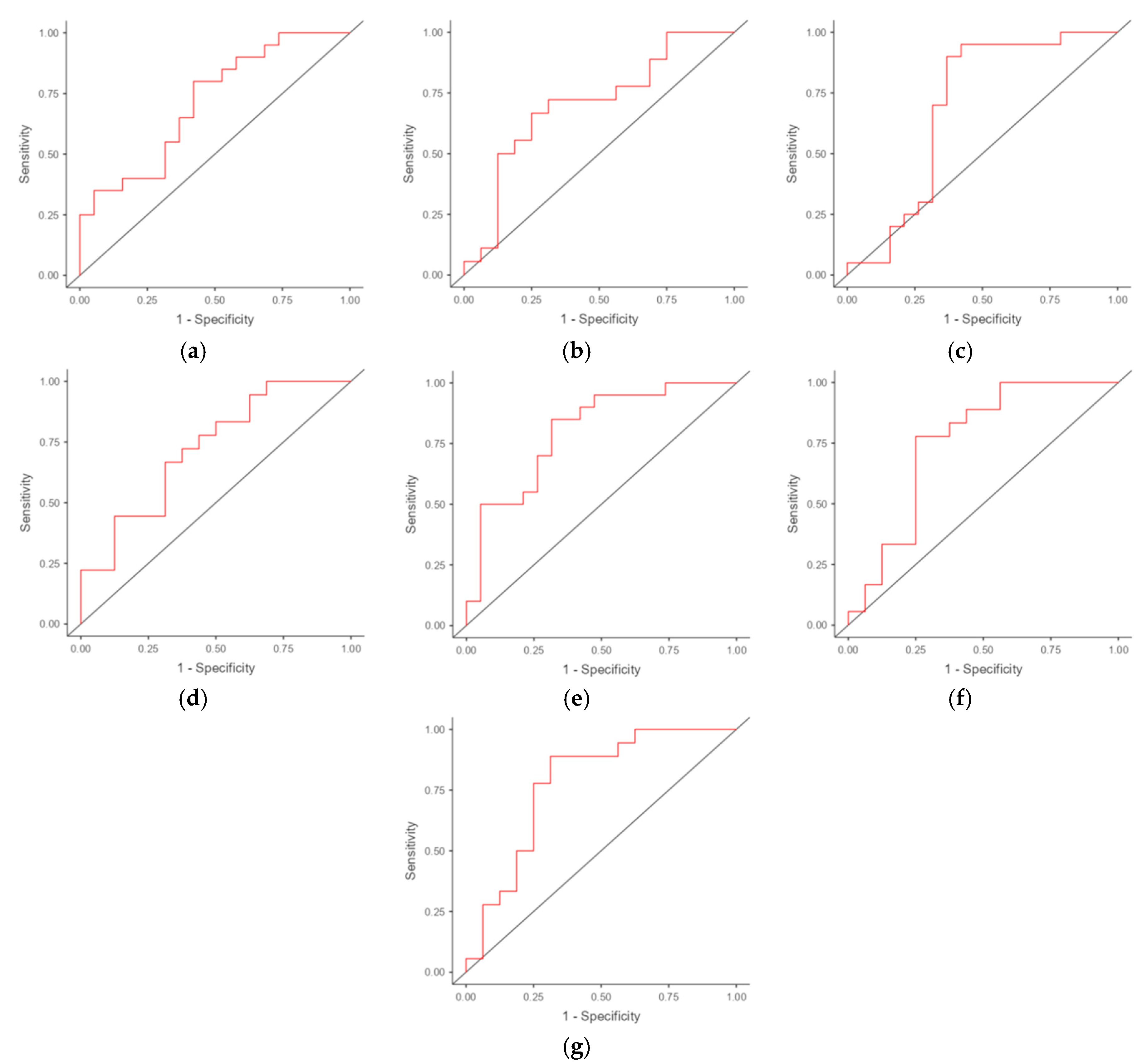

Table 1.
Demographic and clinical characteristics of the study groups.
| Characteristics | RIF patients (N = 20) |
RPL patients (N = 19) |
|---|---|---|
| Age (years): Mean±SD | 34.65 ± 5.29 | 33.37 ± 5.22 |
| BMI (kg/m2): Mean±SD | 23.36 ± 4.24 | 25.69 ± 4.79 |
| Endometrium thickness (mm): Mean±SD | 6.51 ± 1.27 | 6.13 ± 1.86 |
| Fibrinogen, g/L: Mean±SD | 3.05 ± 0.51 | 3.10 ± 0.23 |
| Protrombin index, %: Mean±SD | 99.16 ± 8.22 | 97.57 ± 6.49 |
| Protrombin time, sec: Mean±SD | 13.04 ± 2.35* | 14.69 ± 1.78 |
| Activated Partial Thromboplastin Time, sec: Mean±SD | 34.04 ± 3.61 | 32.10 ± 2.20 |
| International Normalized Ratio: Mean±SD | 1.04 ± 0.12 | 1.21 ± 0.14 |
| Anti-Mullerian Hormone, ng/mL: Mean±SD | 2.60 ± 1.03 | 2.64 ± 0.32 |
| Luteinizing hormone, mIU/mL: Mean±SD | 8.34 ± 2.13 | 11.24 ± 3.26 |
| Follicle stimulating hormone, mIU/mL: Mean±SD | 6.19 ± 1.43 | 6.00 ± 1.07 |
| Prolactin, mIU/L: Mean±SD | 325.0 ± 152.4 | 333.6 ± 61.6 |
| Thyroid stimulating hormone, mIU/mL: Mean±SD | 2.84 ± 0.74 | nd |
| Chronic endometritis, yes/no | 20/0 | 16/3 |
| Chronic salpingoophoritis, yes/no | 10/10 | 10/9 |
| Pelvic organs surgeries, yes/no | 10/10 | 6/13 |
| Endometriosis, yes/no | 5/15 | 4/15 |
| Uterine fibroids, yes/no | 1/19 | 3/16 |
| Polyps, yes/no | 1/19 | 4/15 |
*p<0.05, nd - no data.
Table 2.
Comparative gene expression statistics between RIF and RPL women.
| Gene | Ct mean ± SD | ΔCt mean ± SE | ΔΔCt (95% CI) log2 fold change |
P value | ||
|---|---|---|---|---|---|---|
| RIF | RLP | RIF | RLP | |||
| C4BPA | 30.51 ± 3.75 | 29.69 ± 3.29 | -8.20 ± 0.61 | -9.65 ± 0.38 | 0.99 (-0.06; 2.13) | 0.059 |
| CXCL1 | 28.19 ± 4.85 | 27.84 ± 4.27 | -5.53 ± 0.65 | -6.82 ± 0.29 | 0.83 (-0.33; 1.97) | 0.175 |
| HAND2 | 24.36 ± 4.29 | 22.90 ± 3.52 | -1.69 ± 0.44 | -1.88 ± 0.17 | 0.35 (-0.24; 1.00) | 0.235 |
| HPRT1 | 25.59 ± 3.81 | 24.77 ± 4.23 | -2.92 ± 0.29 | -3.75 ± 0.13 | 0.57 (0.01; 1.54) | 0.041 |
| IFNG | 33.68 ± 2.49 | 33.58 ± 2.85 | -12.27 ± 0.48 | -13.52 ± 0.36 | 1.24 (0.01; 2.43) | 0.046 |
| IL15 | 26.54 ± 3.63 | 25.89 ± 3.89 | -3.88 ± 0.28 | -4.87 ± 0.22 | 0.92 (0.10; 1.65) | 0.023 |
| IL8 | 28.93 ± 4.19 | 28.16 ± 4.00 | -6.26 ± 0.67 | -7.55 ± 0.54 | 1.09 (-0.04; 2.55) | 0.070 |
| MMP10 | 32.07 ± 3.89 | 29.76 ± 5.55 | -9.41 ± 0.86 | -8.74 ± 0.66 | -0.04 (-2.70; 1.81) | 0.945 |
| TNC | 27.24 ± 4.15 | 25.07 ± 4.49 | -4.57 ± 0.45 | -4.04 ± 0.40 | -0.58 (-1.45; 0.78) | 0.396 |
| VEGFB | 25.64 ± 3.46 | 24.20 ± 3.41 | -2.97 ± 0.19 | -3.18 ± 0.21 | 0.34 (-0.23; 0.77) | 0.214 |
| GAPDH | 22.90 ± 4.09 | 21.24 ± 4.45 | - | - | - | - |
| YWHAZ | 22.43 ± 3.47 | 20.81 ± 3.89 | - | - | - | - |
Table 3.
Detected correlations between gene expression levels and clinical and laboratory parameters.
Table 3.
Detected correlations between gene expression levels and clinical and laboratory parameters.
| Group | Parameter 1 | Parameter 2 | Spearman rho | P value |
|---|---|---|---|---|
| RPL group | CXCL1 | Protrombine time | -0.456 | 0.04959 |
| CXCL1 | Activated Partial Thromboplastin Time | 0.587 | 0.0083 | |
| MMP10 | Activated Partial Thromboplastin Time | -0.494 | 0.0317 | |
| RIF group | VEGFB | Prolactin | -0.446 | 0.049 |
| VEGFB | Thyroid stimulating hormone | -0.526 | 0.017 | |
| HAND2 | Thyroid stimulating hormone | -0.671 | 0.001 | |
| HAND2 | Fibrinogen | -0.465 | 0.038 |
Table 4.
ROC analysis results.
| Potential markers and combinations | AUC (95% CI) | Optimal cut-off point | Sensitivity (95% CI) | Specificity(95% CI) |
|---|---|---|---|---|
| IL15 | 0.713 (0.550-0.876) | -4.091 | 0.800 (0.563-0.943) | 0.579 (0.335-0.797) |
| IFNG | 0.701 (0.516-0.886) | -13.238 | 0.667 (0.410-0.867) | 0.750 (0.476-0.927) |
| HPRT1 | 0.692 (0.505-0.879) | -3.568 | 0.900 (0.683-0.988) | 0.632 (0.384-0.837) |
| IL15 + IFNG | 0.722 | - | 0.667 | 0.688 |
| IL15 + HPRT1 | 0.800 | - | 0.850 | 0.684 |
| IFNG + HPRT1 | 0.753 | - | 0.778 | 0.750 |
| IL15 + IFNG + HPRT1 | 0.778 | - | 0.889 | 0.688 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



