
Submitted:
07 August 2024
Posted:
14 August 2024
You are already at the latest version
Abstract
This study evaluated the presence of Human Papillomavirus (HPV) and Bovine Leukemia Virus (BLV) DNA in breast cancer (BC) samples from women in Northeastern Brazil. We analyzed 186 formalin-fixed, paraffin-embedded tissue block samples using PCR and qPCR to detect HPV and BLV DNA. BLV DNA was not detected in any BC patients. However, HPV DNA was found in 46.2\% of the BC samples: 44.6\% were positive for HPV16, 3.5\% for HPV31, and 2\% were coinfected with HPV16 and HPV31. Additionally, we found an association between HPV-positive BC and Ki-67 expression (P=0.03, OR=1.85; CI=1.02-3.34), as well as between HPV31-positive BC and mitotic index (P=0.047). Although BLV was not detected in BC patients from Northeastern Brazil, the association between HPV and cell proliferation markers warrants further investigation, as HPV may contribute to the aggressiveness of BC in these patients.
Keywords:
Breast Cancer
; Human Papillomavirus (HPV)
; Bovine Leukemia Virus (BLV)
; Northeastern Brazil
1. Introduction
Breast cancer (BC) is a major global health issue. In 2020, the World Health Organization (WHO) reported 2.3 million new cases and 685,000 deaths from BC [1,2]. In Brazil alone, 66,000 women were diagnosed with the disease in the same year [3].
BC is a heterogeneous and multifactorial disease, influenced by both genetic and environmental factors [4,5,6,7,8,9]. Additionally, studies suggests that infections with Mouse Mammary Tumor Virus (MMTV), Epstein-Barr Virus (EBV), Bovine Leukemia Virus (BLV), and Human Papillomaviruses (HPV) may contribute to its development [6,7,10].
HPV is a well-known cervical cancer agent [11,12]. However, studies have shown the presence of HPV and its putative role in non-cervical cancers, such as head and neck, lung, and breast cancers [5,6,13,14,15,16,17,18,19]. Concerning the BC, these studies have shown the presence of HPV DNA 16, 18, 31, 58 and the oncogenes expression of the HPV16 E6, E7 [5,18,20,21,22,23,24,25,26,27,28,29,30]. In addition, the viral load, presence of oncoproteins, and their isoforms were also reported in BC [30,31,32,33].
BLV is a retrovirus that infects cattle causing bovine leukosis [34]. BLV is highly prevalent in cattle, and studies suggest that their transmission to humans occurs by ingesting rare meat and unpasteurized milk [34]. In addition, recent studies indicated that BLV could act as a carcinogenic agent in BC since in situ PCR and immunohistochemistry studies detected BLV in BC [34,35,36,37,38,39].
Despite the existing evidence, the role of HPV and BLV in BC remains controversial, as some studies have failed to detect HPV or BLV DNA in BC samples [35,36,37,38,39,40,41,42,43,44]. Given the high prevalence of these viruses in certain regions, such as Northeastern Brazil—where cervical cancer and bovine leukosis are common and where the population consumes rare meat and unpasteurized cow’s milk [45,46,47,48] it is crucial to conduct further research. Therefore, this study aimed to investigate the presence of HPV and BLV DNA in breast cancer cases from Paraíba State, Northeastern Brazil.
2. Materials and Methods
2.1. Patients
We selected 186 formalin-fixed paraffin-embedded (FFPE) breast cancer (BC) samples from the UNI-LAB Clinical Pathology archives in João Pessoa, Paraíba State, Northeastern Brazil. These samples, collected between 2012 and 2017, included various BC subtypes: 66 (35%) Luminal A, 37 (20%) Luminal B, 31 (17%) HER2-positive, 23 (12%) triple-negative breast cancer (TNBC), 19 (10%) unclassified tumors (NCT), 6 (3%) Super HER2, and 4 (2%) Luminal HER2.
We assessed the presence or absence of HPV DNA in relation to several parameters, including mitotic index, the proliferation marker Ki-67, inflammatory infiltrates, nuclear pleomorphism, tubular differentiation, histological score, vascular invasion, estrogen receptor (ER) status, and progesterone receptor (PR) status. Patient ages ranged from 25 to 91 years. This study was approved by the Ethics and Research Committee under CAAE 4.506.821.
2.2. HPV and BLV Detection
DNA from FFPE BC samples was extracted according to Shi et al., 2002 [49]. The quality of the extracted DNA was verified using polymerase chain reaction (PCR) by amplifying a fragment of the B-globin gene with the primers listed in Table 1.
We used conventional and quantitative real-time PCR (qPCR) to detect BLV and DNA. For HPV detection, we initially employed consensus and degenerate primers MY09/11, followed by nested PCR using oligonucleotides GP05/06 (Table 1) (Table 1) [48,50]. Additionally, we conducted qPCR using the GP05/06 and E6 HPV16-Forward/E6 HPV16-Reverse primers (Table 1) (Table 1) [48]. DNA extracted from CaSki cell lines served a positive control, and all tests were performed in triplicate.
The presence of BLV in BC cases was analyzed using conventional PCR, qPCR, nested PCR, and Auto-Nested qPCR. The primers used targeted the Tax and Gag genes, as de-scribed by Buehring et al. (2014) and Buehring et al. (2019) (Table 1) [51,52]. Proviral DNA extracted from cultured FLK cells containing BLV was used as a positive control.
2.3. Statistical Analysis
We performed chi-square and Fisher’s exact tests to compare the clinical aspects of BC patients across the following groups: (i) BC HPV DNA-positive and BC HPV DNA-negative; (ii) BC HPV16 DNA-positive and BC HPV16 DNA-negative; (iii) BC HPV31 DNA-positive and BC HPV31 DNA-negative; (iv) BC BLV DNA-positive and BC BLV DNA-negative. All P-values were two-sided, with a significance level set at 0.05. Data analysis was conducted using SPSS version 26 (SPSS Inc., Illinois, USA).
3. Results
3.1. BLV and HPV DNA Detection in BC
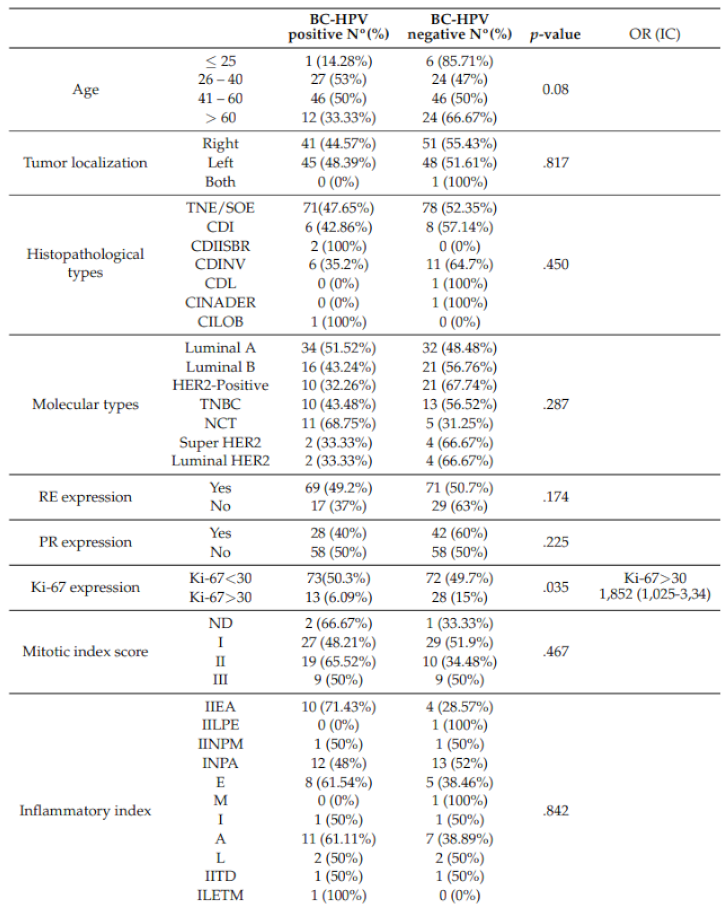
We screened HPV and BLV DNAs in 186 BC cases and did not detect BLV in any of them. On the other hand, we detected HPV DNA in 46.2% (86/186) of the total cases. Among these, we observed 39% (34/86) of HPV DNA in Luminal A, 18% (16/86) in Luminal B, 11% (10/86) in HER-2, 12% (10/86) in TNBC, 13% (11/86) in NCT, 2% (2/86), in Super HER2 and 2% (2/86) in Luminal HER2. Although we detected HPV DNA in all molecular types of BC, no significant differences were observed between BC HPV DNA-positive cases and molecular types (Table 2). In addition, we did not find significant differences between BC HPV DNA-positive and mitotic index, inflammatory infiltrate nuclear pleomorphism, tubular differentiation, histological score, vascular invasion, ER, and PR (Table 2). However, BC HPV DNA-positive cases are associated with the Ki-67 expression (Table 2). Finally, we did not observe statistical differences between Luminal vs. Non-Luminal (p= 0.338) and 86 Luminal A vs. Luminal B (p= 0.281) in BC HPV DNA-positive cases.
3.2. HPV16 and 31 DNA Detection in BC
The most frequent HPV type in the BC cases was HPV16 (44.6%, 83/186). It was also the most common type in Luminal A, Luminal B, HER2, TNBC, and Super HER2. However, despite its high prevalence, we did not observe significant differences between BC HPV16 DNA-positive cases and molecular types, mitotic index, inflammatory infiltrate, nuclear pleomorphism, tubular differentiation, histological grade, vascular invasion, ER, PR, and Ki-67 (Table 1 of the supplementary data). Furthermore, we did not find significant differences between Luminal vs. Non-Luminal groups and BC HPV16 DNA-positive cases (p=0.636).
We found 3.8% (7/186) of HPV31 in all BC patients, specifically in Luminal A and TNBC cases. When comparing Luminal vs. Non-Luminal types, no significant differences were observed with BC HPV31 DNA-positive cases (p=0.269). Additionally, there were no significant differences between BC HPV31 DNA-positive cases and molecular types, inflammatory infiltrate, nuclear pleomorphism, tubular differentiation, histological grade, vascular invasion, ER, PR, and Ki-67 expression (Table 2 of the supplementary data). However, a significant association was found between the mitotic index and BC HPV31 DNA-positive cases (p=0.047). Coinfections with HPV16 and HPV31 genotypes were observed in 2% (4/186) of the total BC samples.
4. Discussion
This study investigated the presence of BLV, HPV16, HPV31, and their coinfections in BC samples from women in Northeast Brazil. We did not detect BLV in any BC samples. However, HPV DNA was found in 46% of the samples, with HPV16 present in 44% of the tumors. Despite the high prevalence of HPV, there was no association between HPV, HPV16, or HPV31 DNA and molecular types, inflammatory infiltrate, nuclear pleomorphism, tubular differentiation, histological grade, vascular invasion, ER, or PR. We did observe an association between HPV and cell proliferation markers.
Diverse studies have demonstrated the presence of HPV DNA in BC, showing detection in both fresh and FFPE tissues using various methodologies such as IHC, conventional PCR, qPCR, and in situ PCR. [18,20,21,22,23,24,27,28,29,30,40,53,54,55,56,57,58]. In addition, these studies detected HPV DNA using different methodologies, such as IHC, conventional PCR, qPCR, and in situ PCR [18,20,21,22,23,24,27,28,29,30,40,52,53,54,55,56,57]. These studies reported HPV DNA prevalence in BC ranging from 0% to 71%, influenced by detection methods and sample processing techniques [18,20,21,22,23,24,27,28,29,30,40,52,53,54,55,56,57]. The methodology used to detect HPV DNA and the sample processing with fixation may reflect the prevalence variation in BC. Our study found a prevalence of HPV DNA in 46% of BC patients from Northeastern Brazil, where cervical cancer is a major public health concern [45,46,47,48,59,60]. Among these samples, 44% were infected by HPV16 and 3.8% by HPV31. Coinfection with HPV16 and 31 was found in 1.6% of total samples. Some studies found similar results in a different population, where HPV16 is most prevalent and HPV31 is less common [23,29,60]. HPV 16 and HPV 31 are the most frequent genotypes found in cervical cancer in women from Northeastern Brazil. However, this coinfection was less frequent in BC patients. We used conventional PCR and qPCR to detect HPV DNA in BC samples. Although PCR and qPCR did no to detect multiple HPV types simultaneously, this methodology suits HPV DNA detection.
Among BC patients, HPV DNA was found most frequently in Luminal patients, which contrasts with other studies showing a higher frequency in TNBC and HER-2 patients [24,61,62]. Although HPV DNA was most prevalent in Luminal patients, specifically Luminal A, these frequencies were not statistically significant. Similarly, HPV DNA was most frequent in PR and ER expression, but these differences were not statistically significant. However, we found a significant association between Ki-67 expression and HPV DNA in BC, as well as between the mitotic index and BC HPV31 positivity. Studies by de Carolis et al. (2019) also showed a similar association between BC HPV DNA-positive status and Ki-67 in Luminal B patients [24]. Both the Ki-67 marker and the mitotic index measure cell proliferation, suggesting that BC HPV DNA-positive cases may be more aggressive than BC HPV DNA-negative cases. Future studies with larger case-control samples are needed to clarify the role of cell proliferation markers in BC patients infected by HPV.
This study did not detect BLV in BC patients from Northeastern Brazil. Previous investigations using various methodologies, including in situ PCR, qPCR, and sequencing to amplify LTR, gag, pol, env, or tax genes, also observed the absence of BLV in BC [62,63]. However, some studies have reported the presence of BLV in BC patients from different regions worldwide, including Brazil [51,52,64,65,66,67,68,69]. The discrepancy between our findings and those of other studies may be attributed to different environmental factors and methodologies used to detect BLV. Environmental factors such as lower meat consumption and coinfections with different viruses could explain these differences. In this study, we used conventional PCR, qPCR, Nested PCR, and AutoNested PCR to amplify gag and tax gene fragments. Interestingly, we found a high prevalence of HPV and an absence of BLV, whereas a study by Baltzell et al. (2017) found BLV but no coinfection with HPV [65]. Future studies should aim to clarify the relationship between BC and coinfections with common local viral agents, such as HPV and BLV.
5. Conclusions
This study identified HPV16 and HPV31, but not BLV, in BC patients. Additionally, we found a significant association between BC HPV-positive cases and cell proliferation markers. Future research should aim to elucidate the relationship between cell proliferation markers and BC HPV DNA-positive cases in the context of carcinogenesis.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Clinical and histological characteristics of patients according to HPV16 status in the BC. Table S2: Clinical and histological characteristics of patients according to HPV31 status in the BC.
Author Contributions
Conceptualization, Z.d.M.N., M.T.C.M., E.M.L.M A.P.A.D.G..; methodology, Z.d.M.N., D.dL.S., I.C.F., K.C.G.d.N., A.L.d.S.J., N.I.P.O., A.F.d.S., S.S.T.H., J.R.G.d.O., I.R.d.C.F., A.C.d.F..; writing—original draft preparation, Z.d.M.N and A.P.A.D.G.; writing—review and editing, Z.d.M.N, A.V and A.P.A.D.G..; supervision, A.P.A.D.G..; project administration, A.P.A.D.G..; funding acquisition, A.P.A.D.G.. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Federal University of Paraíba (UFPB) call 03/2020. AV ’s work was supported in part by the Italian Ministry of Foreign Affairs and International Cooperation, grant number PGRBR22GR03.
Informed Consent Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by Federal Institute of Paraíba, Ethics Committee Ethics and Research Committee under CAAE: CAAE 4.506.821.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Soerjomataram, I.; Bray, F. Planning for tomorrow: global cancer incidence and the role of prevention 2020–2070. Nature Reviews Clinical Oncology 2021, 18, 663–672. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer Journal for Clinicians 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- INCA, 2020.
- Buys, S.S.; Sandbach, J.F.; Gammon, A.; Patel, G.; Kidd, J.; Brown, K.L.; Sharma, L.; Saam, J.; Lancaster, J.; Daly, M.B. A study of over 35,000 women with breast cancer tested with a 25-gene panel of hereditary cancer genes. Cancer 2017, 123, 1721–1730. [Google Scholar] [CrossRef] [PubMed]
- Gupta, I.; Jabeen, A.; Al-Sarraf, R.; Farghaly, H.; Vranic, S.; Sultan, A.A.; Al Moustafa, A.E.; Al-Thawadi, H. The co-presence of high-risk human papillomaviruses and Epstein-Barr virus is linked with tumor grade and stage in Qatari women with breast cancer. Human Vaccines & Immunotherapeutics 2021, 17, 982–989. [Google Scholar] [CrossRef]
- Hsu, C.R.; Lu, T.M.; Chin, L.W.; Yang, C.C. Possible DNA viral factors of human breast cancer. Cancers 2010, 2, 498–512. [Google Scholar] [CrossRef] [PubMed]
- Kudela, E.; Kudelova, E.; Kozubík, E.; Rokos, T.; Pribulova, T.; Holubekova, V.; Biringer, K. HPV-Associated Breast Cancer: Myth or Fact? Pathogens (Basel, Switzerland) 2022, 11, 1510. [Google Scholar] [CrossRef] [PubMed]
- Malhone, C.; Longatto-Filho, A.; Filassi, J.R. Is Human Papilloma Virus Associated with Breast Cancer? A Review of the Molecular Evidence. Acta Cytologica 2018, 62, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Usman, M.; Hameed, Y.; Ahmad, M.; Jalil Ur Rehman, n.; Ahmed, H.; Hussain, M.S.; Asif, R.; Murtaza, M.G.; Jawad, M.T.; Iqbal, M.J. Breast Cancer Risk and Human Papillomavirus Infection: A Bradford Hill Criteria Based Evaluation. Infectious Disorders Drug Targets 2022, 22, e200122200389. [Google Scholar] [CrossRef]
- Mareti, E.; Chatzakis, C.; Pratilas, G.C.; Liberis, A.; Vavoulidis, E.; Papanastasiou, A.; Dampali, R.; Daniilidis, A.; Zepiridis, L.; Dinas, K. Human papillomavirus in breast cancer of patients with cervical intraepithelial neoplasia or cervical cancer history. A systematic review and meta-analysis. Journal of B.U.ON.: official journal of the Balkan Union of Oncology 2021, 26, 707–713. [Google Scholar] [PubMed]
- zur Hausen, H. Papillomaviruses in the causation of human cancers - a brief historical account. Virology 2009, 384, 260–265. [Google Scholar] [CrossRef]
- zur Hausen, H. Papillomaviruses in human cancers. Proc Assoc Am Physicians 1999, 111, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Badaracco, G.; Venuti, A.; Morello, R.; Muller, A.; Marcante, M.L. Human papillomavirus in head and neck carcinomas: prevalence, physical status and relationship with clinical/pathological parameters. Anticancer Res. 2000, 20, 1301–1305. [Google Scholar] [PubMed]
- Benson, E.; Li, R.; Eisele, D.; Fakhry, C. The clinical impact of HPV tumor status upon head and neck squamous cell carcinomas. Oral Oncol. 2014, 50, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, N.; Frederick, M.J.; Pickering, C.R.; Bettegowda, C.; Chang, K.; Li, R.J.; Fakhry, C.; Xie, T.X.; Zhang, J.; Wang, J.; et al. Exome sequencing of head and neck squamous cell carcinoma reveals inactivating mutations in NOTCH1. Science 2011, 333, 1154–1157. [Google Scholar] [CrossRef] [PubMed]
- Aguayo, F.; Castillo, A.; Koriyama, C.; Higashi, M.; Itoh, T.; Capetillo, M.; Shuyama, K.; Corvalan, A.; Eizuru, Y.; Akiba, S. Human papillomavirus-16 is integrated in lung carcinomas: a study in Chile. Br. J. Cancer 2007, 97, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Ilahi, N.E.; Anwar, S.; Noreen, M.; Hashmi, S.N.; Murad, S. Detection of human papillomavirus-16 DNA in archived clinical samples of breast and lung cancer patients from North Pakistan. J. Cancer Res. Clin. Oncol. 2016, 142, 2497–2502. [Google Scholar] [CrossRef] [PubMed]
- Di Lonardo, A.; Venuti, A.; Marcante, M.L. Human papillomavirus in breast cancer. Breast Cancer Research and Treatment 1992, 21, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Antonsson, A.; Spurr, T.P.; Chen, A.C.; Francis, G.D.; McMillan, N.A.J.; Saunders, N.A.; Law, M.; Bennett, I.C. High prevalence of human papillomaviruses in fresh frozen breast cancer samples. Journal of Medical Virology 2011, 83, 2157–2163. [Google Scholar] [CrossRef] [PubMed]
- Aguayo, F.; Khan, N.; Koriyama, C.; González, C.; Ampuero, S.; Padilla, O.; Solís, L.; Eizuru, Y.; Corvalán, A.; Akiba, S. Human papillomavirus and Epstein-Barr virus infections in breast cancer from chile. Infectious Agents and Cancer 2011, 6, 7. [Google Scholar] [CrossRef] [PubMed]
- Balci, F.L.; Uras, C.; Feldman, S.M. Is human papillomavirus associated with breast cancer or papilloma presenting with pathologic nipple discharge? Cancer Treatment and Research Communications 2019, 19, 100122. [Google Scholar] [CrossRef] [PubMed]
- Baltzell, K.; Buehring, G.C.; Krishnamurthy, S.; Kuerer, H.; Shen, H.M.; Sison, J.D. Limited evidence of human papillomavirus in [corrected] breast tissue using molecular in situ methods. Cancer 2012, 118, 1212–1220. [Google Scholar] [CrossRef] [PubMed]
- Cavalcante, J.R.; Pinheiro, L.G.P.; Almeida, P.R.C.d.; Ferreira, M.V.P.; Cruz, G.A.; Campelo, T.A.; Silva, C.S.; Lima, L.N.G.C.; Oliveira, B.M.K.d.; Lima, L.M.; et al. Association of breast cancer with human papillomavirus (HPV) infection in Northeast Brazil: molecular evidence. Clinics (Sao Paulo, Brazil) 2018, 73, e465. [Google Scholar] [CrossRef] [PubMed]
- De Carolis, S.; Storci, G.; Ceccarelli, C.; Savini, C.; Gallucci, L.; Sansone, P.; Santini, D.; Seracchioli, R.; Taffurelli, M.; Fabbri, F.; et al. HPV DNA Associates With Breast Cancer Malignancy and It Is Transferred to Breast Cancer Stromal Cells by Extracellular Vesicles. Frontiers in Oncology 2019, 9, 860. [Google Scholar] [CrossRef] [PubMed]
- Delgado-García, S.; Martínez-Escoriza, J.C.; Alba, A.; Martín-Bayón, T.A.; Ballester-Galiana, H.; Peiró, G.; Caballero, P.; PonceLorenzo, J. Presence of human papillomavirus DNA in breast cancer: a Spanish case-control study. BMC Cancer 2017, 17, 320. [Google Scholar] [CrossRef] [PubMed]
- Doosti, M.; Bakhshesh, M.; Zahir, S.T.; Shayestehpour, M.; Karimi-Zarchi, M. Lack of Evidence for a Relationship between High Risk Human Papillomaviruses and Breast Cancer in Iranian Patients. Asian Pacific journal of cancer prevention: APJCP 2016, 17, 4357–4361. [Google Scholar]
- Frega, A.; Lorenzon, L.; Bononi, M.; De Cesare, A.; Ciardi, A.; Lombardi, D.; Assorgi, C.; Gentile, M.; Moscarini, M.; Torrisi, M.R.; et al. Evaluation of E6 and E7 mRNA expression in HPV DNA positive breast cancer. European Journal of Gynaecological Oncology 2012, 33, 164–167. [Google Scholar]
- Gupta, I.; Ulamec, M.; Peric-Balja, M.; Ramic, S.; Al Moustafa, A.E.; Vranic, S.; Al-Farsi, H.F. Presence of high-risk HPVs, EBV, and MMTV in human triple-negative breast cancer. Human Vaccines & Immunotherapeutics 2021, 17, 4457–4466. [Google Scholar] [CrossRef]
- Habyarimana, T.; Attaleb, M.; Mazarati, J.B.; Bakri, Y.; El Mzibri, M. Detection of human papillomavirus DNA in tumors from Rwandese breast cancer patients. Breast Cancer (Tokyo, Japan) 2018, 25, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.; Dasgupta, H.; Roychowdhury, A.; Bhattacharya, R.; Mukherjee, N.; Roy, A.; Mandal, G.K.; Alam, N.; Biswas, J.; Mandal, S.; et al. Study of association and molecular analysis of human papillomavirus in breast cancer of Indian patients: Clinical and prognostic implication. PloS One 2017, 12, e0172760. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kim, C.; Lee, H.S.; Choi, Y.J.; Kim, H.Y.; Lee, J.; Chang, H.; Kim, A. Detection of Human Papillomavirus in Korean Breast Cancer Patients by Real-Time Polymerase Chain Reaction and Meta-Analysis of Human Papillomavirus and Breast Cancer. Journal of Pathology and Translational Medicine 2016, 50, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.A.; Castillo, A.; Koriyama, C.; Kijima, Y.; Umekita, Y.; Ohi, Y.; Higashi, M.; Sagara, Y.; Yoshinaka, H.; Tsuji, T.; et al. Human papillomavirus detected in female breast carcinomas in Japan. British Journal of Cancer 2008, 99, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Chang, P.; Wang, L.; Yao, Q.; Guo, W.; Chen, J.; Yan, T.; Cao, C. The role of human papillomavirus infection in breast cancer. Medical Oncology (Northwood, London, England) 2012, 29, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Marawan, M.A.; Alouffi, A.; El Tokhy, S.; Badawy, S.; Shirani, I.; Dawood, A.; Guo, A.; Almutairi, M.M.; Alshammari, F.A.; Selim, A. Bovine Leukaemia Virus: Current Epidemiological Circumstance and Future Prospective. Viruses 2021, 13, 2167. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Jiang, J.; Sun, W.; Zhang, J.; Huang, K.; Gu, X.; Yang, Y.; Xu, X.; Shi, Y.; Wang, C. Lack of association between bovine leukemia virus and breast cancer in Chinese patients. Breast cancer research: BCR 2016, 18, 101. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, M.P.; Saito, S.; Hara, Y.; Matsuura, R.; Takeshima, S.n.; Hosomichi, K.; Matsumoto, Y.; Furuta, R.A.; Takei, M.; Aida, Y. evidence of bovine leukemia virus proviral DNA and antibodies in human specimens from Japan. Retrovirology 2022, 19, 7. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Romano, L.; Fernández-Tamayo, N.; Gómez-Conde, E.; Reyes-Cardoso, J.M.; Ortiz-Gutierrez, F.; Ceballos, G.; Valdivia,; Piña, P. ; Salcedo, M. Absence of human papillomavirus sequences in epithelial breast cancer in a Mexican female population. Medical Oncology (Northwood, London, England) 2012, 29, 1515–1517. [Google Scholar] [CrossRef] [PubMed]
- Bakhtiyrizadeh, S.; Hosseini, S.Y.; Yaghobi, R.; Safaei, A.; Sarvari, J. Almost Complete Lack of Human Cytomegalovirus and Human papillomaviruses Genome in Benign and Malignant Breast Lesions in Shiraz, Southwest of Iran. Asian Pacific journal of cancer prevention: APJCP 2017, 18, 3319–3324. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Goepfert, R.; Khan, N.A.; Koriyama, C.; Akiba, S.; Pérez-Sánchez, V.M. High-risk human papillomavirus in mammary gland carcinomas and non-neoplastic tissues of Mexican women: no evidence supporting a cause and effect relationship. Breast (Edinburgh, Scotland) 2011, 20, 184–189. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Goepfert, R.; Vela-Chávez, T.; Carrillo-García, A.; Lizano-Soberón, M.; Amador-Molina, A.; Oñate-Ocaña, L.F.; Hallmann, R.S.R. High-risk human papillomavirus (HPV) DNA sequences in metaplastic breast carcinomas of Mexican women. BMC Cancer 2013, 13, 445. [Google Scholar] [CrossRef] [PubMed]
- Eslamifar, A.; Ramezani, A.; Azadmanesh, K.; Bidari-Zerehpoosh, F.; Banifazl, M.; Aghakhani, A. Assessment of the Association between Human Papillomavirus Infection and Breast Carcinoma. Iranian Journal of Pathology 2015, 10, 41–46. [Google Scholar] [PubMed]
- Vernet-Tomas, M.; Mena, M.; Alemany, L.; Bravo, I.; De Sanjosé, S.; Nicolau, P.; Bergueiro, A.; Corominas, J.M.; Serrano, S.; Carreras, R.; et al. Human papillomavirus and breast cancer: no evidence of association in a Spanish set of cases. Anticancer Research 2015, 35, 851–856. [Google Scholar] [PubMed]
- Hedau, S.; Kumar, U.; Hussain, S.; Shukla, S.; Pande, S.; Jain, N.; Tyagi, A.; Deshpande, T.; Bhat, D.; Mir, M.M.; et al. Breast cancer and human papillomavirus infection: no evidence of HPV etiology of breast cancer in Indian women. BMC cancer 2011, 11, 27. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Li, J.; Ji, Y.; Ren, M.; Pang, B.; Chu, M.; Wei, L. Inconclusive role of human papillomavirus infection in breast cancer. Infectious Agents and Cancer 2015, 10, 36. [Google Scholar] [CrossRef]
- Gurgel, A.P.A.D.; Chagas, B.S.; do Amaral, C.M.M.; Albuquerque, E.M.B.; Serra, I.G.S.S.; Silva Neto, J.d.C.; Muniz, M.T.C.; de Freitas, A.C. Prevalence and genetic variability in capsid L1 gene of rare human papillomaviruses (HPV) found in cervical lesions of women from North-East Brazil. Biomed Res. Int. 2013, 2013, 546354. [Google Scholar] [CrossRef]
- Chagas, B.S.; Batista, M.V.d.A.; Crovella, S.; Gurgel, A.P.A.D.; Silva Neto, J.d.C.; Serra, I.G.S.S.; Amaral, C.M.M.; Balbino, V.Q.; Muniz, M.T.C.; Freitas, A.C. Novel E6 and E7 oncogenes variants of human papillomavirus type 31 in Brazilian women with abnormal cervical cytology. Infect. Genet. Evol. 2013, 16, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Gurgel, A.P.A.D.; Chagas, B.S.; do Amaral, C.M.; Nascimento, K.C.G.; Leal, L.R.S.; Silva Neto, J.d.C.; Cartaxo Muniz, M.T.; de Freitas, A.C. Prevalence of human papillomavirus variants and genetic diversity in the L1 gene and long control region of HPV16, HPV31, and HPV58 found in North-East Brazil. Biomed Res. Int. 2015, 2015, 130828. [Google Scholar] [CrossRef] [PubMed]
- Conceição Gomes Nascimento, K.; Gonçalves Lima,; Mota Nunes, Z. ; Rêgo Barros Júnior, M.; de Aragão Batista, M.V.; Lucena Araujo, A.R.; da Costa Silva Neto, J.; Simas Chagas, B.; Almeida Diniz Gurgel, A.P.; de Freitas, A.C. Detection of Human Papillomavirus DNA in Paired Peripheral Blood and Cervix Samples in Patients with Cervical Lesions and Healthy Individuals. Journal of Clinical Medicine 2021, 10, 5209. [Google Scholar] [CrossRef]
- Shi, S.R.; Cote, R.J.; Wu, L.; Liu, C.; Datar, R.; Shi, Y.; Liu, D.; Lim, H.; Taylor, C.R. DNA extraction from archival formalin-fixed, paraffin-embedded tissue sections based on the antigen retrieval principle: heating under the influence of pH. The Journal of Histochemistry and Cytochemistry: Official Journal of the Histochemistry Society 2002, 50, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Fuessel Haws, A.L.; He, Q.; Rady, P.L.; Zhang, L.; Grady, J.; Hughes, T.K.; Stisser, K.; Konig, R.; Tyring, S.K. Nested PCR with the PGMY09/11 and GP5(+)/6(+) primer sets improves detection of HPV DNA in cervical samples. J. Virol. Methods 2004, 122, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Buehring, G.C.; DeLaney, A.; Shen, H.; Chu, D.L.; Razavian, N.; Schwartz, D.A.; Demkovich, Z.R.; Bates, M.N. Bovine leukemia virus discovered in human blood. BMC Infectious Diseases 2019, 19, 297. [Google Scholar] [CrossRef] [PubMed]
- Buehring, G.C.; Shen, H.M.; Jensen, H.M.; Choi, K.Y.; Sun, D.; Nuovo, G. Bovine leukemia virus DNA in human breast tissue. Emerging Infectious Diseases 2014, 20, 772–782. [Google Scholar] [CrossRef] [PubMed]
- Ngan, C.; Lawson, J.S.; Clay, R.; Delprado, W.; Whitaker, N.J.; Glenn, W.K. Early Human Papilloma Virus (HPV) Oncogenic Influences in Breast Cancer. Breast Cancer: Basic and Clinical Research 2015, 9, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, H.; Rassi, H.; Mansur, F.N. Investigation of Methylenetetrahydrofolate Reductase C677T Polymorphism and Human Papilloma Virus Genotypes in Iranian Breast Cancer. Monoclonal Antibodies in Immunodiagnosis and Immunotherapy 2017, 36, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Salman, N.A.; Davies, G.; Majidy, F.; Shakir, F.; Akinrinade, H.; Perumal, D.; Ashrafi, G.H. Association of High Risk Human Papillomavirus and Breast cancer: A UK based Study. Scientific Reports 2017, 7, 43591. [Google Scholar] [CrossRef] [PubMed]
- Khodabandehlou, N.; Mostafaei, S.; Etemadi, A.; Ghasemi, A.; Payandeh, M.; Hadifar, S.; Norooznezhad, A.H.; Kazemnejad, A.; Moghoofei, M. Human papilloma virus and breast cancer: the role of inflammation and viral expressed proteins. BMC cancer 2019, 19, 61. [Google Scholar] [CrossRef] [PubMed]
- Charostad, J.; Azaran, A.; Nakhaei, M.; Astani, A.; Kaydani, G.A.; Motamedfar, A.; Makvandi, M. Upregulation of Interleukin-6 in HPV-Positive Breast Cancer Patients. Iranian journal of immunology: IJI 2021, 18, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Metwally, S.A.; Abo-Shadi, M.A.; Abdel Fattah, N.F.; Barakat, A.B.; Rabee, O.A.; Osman, A.M.; Helal, A.M.; Hashem, T.; Moneer, M.M.; Chehadeh, W.; et al. Presence of HPV, EBV and HMTV Viruses Among Egyptian Breast Cancer Women: Molecular Detection and Clinical Relevance. Infection and Drug Resistance 2021, 14, 2327–2339. [Google Scholar] [CrossRef] [PubMed]
- Baldez da Silva, M.F.P.T.; Chagas, B.S.; Guimarães, V.; Katz, L.M.C.; Felix, P.M.; Miranda, P.M.; Lima, A.A.; Arraes, L.C.; Martins, D.B.G.; Lima Filho, J.L.; et al. HPV31 and HPV33 incidence in cervical samples from women in Recife, Brazil. Genet. Mol. Res. 2009, 8, 1437–1443. [Google Scholar] [CrossRef] [PubMed]
- Chagas, B.S.; Comar, M.; Gurgel, A.P.A.D.; Paiva, S.; Seraceni, S.; de Freitas, A.C.; Crovella, S. Association study between cervical lesions and single or multiple vaccine-target and non-vaccine target Human Papillomavirus (HPV) types in women from northeastern Brazil. PLoS One 2015, 10, e0132570. [Google Scholar] [CrossRef] [PubMed]
- de Villiers, E.M.; Sandstrom, R.E.; zur Hausen, H.; Buck, C.E. Presence of papillomavirus sequences in condylomatous lesions of the mamillae and in invasive carcinoma of the breast. Breast Cancer Res. 2005, 7, R1–11. [Google Scholar] [CrossRef] [PubMed]
- Piana, A.F.; Sotgiu, G.; Muroni, M.R.; Cossu-Rocca, P.; Castiglia, P.; De Miglio, M.R. HPV infection and triple-negative breast cancers: an Italian case-control study. Virology Journal 2014, 11, 190. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Jiang, J.; Sun, W.; Zhang, J.; Huang, K.; Gu, X.; Yang, Y.; Xu, X.; Shi, Y.; Wang, C. Lack of association between bovine leukemia virus and breast cancer in Chinese patients. Breast Cancer Research 2016, 18, 101. [Google Scholar] [CrossRef] [PubMed]
- Canova, R.; Weber, M.N.; Budaszewski, R.F.; da Silva, M.S.; Schwingel, D.; Canal, C.W.; Kreutz, L.C. Bovine leukemia viral DNA found on human breast tissue is genetically related to the cattle virus. One Health 2021, 13, 100252. [Google Scholar] [CrossRef] [PubMed]
- Schwingel, D.; Andreolla, A.P.; Erpen, L.M.S.; Frandoloso, R.; Kreutz, L.C. Bovine leukemia virus DNA associated with breast cancer in women from South Brazil. Scientific Reports 2019, 9, 2949. [Google Scholar] [CrossRef] [PubMed]
- Baltzell, K.A.; Shen, H.M.; Krishnamurthy, S.; Sison, J.D.; Nuovo, G.J.; Buehring, G.C. Bovine leukemia virus linked to breast cancer but not coinfection with human papillomavirus: Case-control study of women in Texas. Cancer 2018, 124, 1342–1349. [Google Scholar] [CrossRef] [PubMed]
- Buehring, G.C.; Shen, H.; Schwartz, D.A.; Lawson, J.S. Bovine leukemia virus linked to breast cancer in Australian women and identified before breast cancer development. PLoS ONE 2017, 12, e0179367. [Google Scholar] [CrossRef] [PubMed]
- Buehring, G.C.; Shen, H.M.; Jensen, H.M.; Jin, D.L.; Hudes, M.; Block, G. Exposure to Bovine Leukemia Virus Is Associated with Breast Cancer: A Case-Control Study. PloS One 2015, 10, e0134304. [Google Scholar] [CrossRef] [PubMed]
- Delarmelina, E.; Buzelin, M.A.; Souza, B.S.d.; Souto, F.M.; Bicalho, J.M.; Câmara, R.J.F.; Resende, C.F.; Bueno, B.L.; Victor, R.M.; Galinari, G.C.F.; et al. High positivity values for bovine leukemia virus in human breast cancer cases from Minas Gerais, Brazil. PloS One 2020, 15, e0239745. [Google Scholar] [CrossRef] [PubMed]

Table 1.
The primers used for conventional PCR and quantitative PCR (qPCR) amplification of HPV and BLV DNA.
Table 1.
The primers used for conventional PCR and quantitative PCR (qPCR) amplification of HPV and BLV DNA.
| Sequence (5’3’) | Size (bp) | |
|---|---|---|
| β-globina | 110 bp | |
| PC04 | ACACAACTGTGTTCACTAGC | |
| GH20 | CAACTTCATCCACGTTCACC | |
| HPV DNA | ||
| *MY09 | CGTCCMARRGGAWACTGATC | 450 bp |
| *MY11 | GCMCAGGGWCATAAYAATGG | |
| HPV DNA | ||
| GP5 | TTTGTTACTGTGGTAGATAC | 110 bp |
| GP6 | GAAAAATAAACTGTAAATCA | |
| E6 HPV16 | GAGAAACTGCAATGTTTCAGGACC | 81 bp |
| TGTATAGTTGTTTGCAGCTCTGTGC | ||
| E6 HPV31 | CGTTTTCGGTTACAGTTTTACAAGC | 76 bp |
| AGCTGGACTGTCTATGACAT | ||
| TAX1 | CTTCGGGATCCATTACCTG | 373 bp |
| GCTCGAAGGGGGAAAGTGAA | ||
| TAX2 | ATGTCACCATCGATGCCTGG | 113 bp |
| AGCTGGACTGTCTATGACAT | ||
| GAG | ACCCTACTCCGGCTGACCTA | 272 bp |
| CTTGGACGATGGTGGACCAA |
* MY09/11 degenerated primers: M = A or C, W = A or T, Y = C or T, and R = A or G.
Table 2.
Clinical and histological characteristics of patients according to HPV status in the BC.
 |
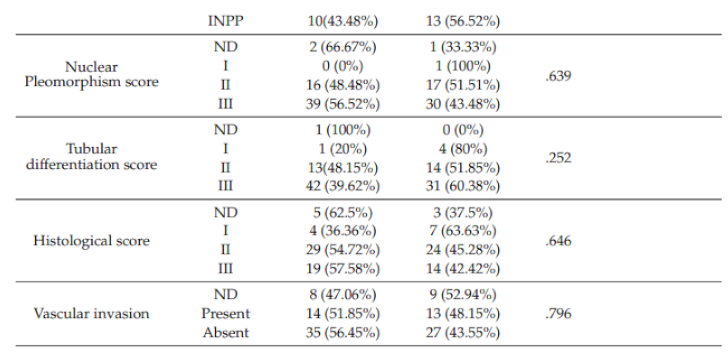 |
Data are presented as the number of patients and percentage. p-values were calculated by chi-square test or Fisher’s exact test. OR = Odds Ratio. *p<0.05-Statistical significantly. Inflammatory infiltrate IIEA: Absent tumor stromal inflammatory infiltrate; IILP E: Peritumoral lymphoplasmacytic inflammatory infiltrate scarce; INPM: Moderate peritoneal peritumoral neoplastic infiltrate; INPA: Absent peritoneal inflammation; E: Scarce; M: Moderate; I: Intense; A: Absent; L: Lightweight; IITD: Discrete tumor inflammatory infiltrate; ILETM: Lymphocytic infiltrates in the minimal tumor stroma; INPP: Present perineural inflammation. Mitotic index: I: measures the speed with which tumor cells expand and segment; II and III are related to the incidence of axillary metastasis. Degree of nuclear polymorphism; I: Small, regular, and uniform tumors; II: points with a moderate increase in size and variability; III: Significant variation; Degree of tubular differentiation: I: Most of the tumor (>75%); II: Moderate part of the tumor (10-75%); III: Little or no part of the tumor (<10%); Histological grade: I: cells similar to normal and slow growing; II: cells that look less like normal and have moderate growth; cells distinct from normal and fast-growing cells; Vascular invasion: Present: there is evidence of invasion of the vascular or lymphatic system and Absent: There was no evidence of lymphatic invasion.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



