
Submitted:
13 August 2024
Posted:
16 August 2024
You are already at the latest version
Abstract
In the past thirty years, childhood obesity rates have risen significantly worldwide, affecting over 340 million children in affluent nations. This surge is intricately tied to metabolic disorders, notably insulin resistance, type 2 diabetes mellitus (T2DM), and the continually evolving spectrum of metabolic-associated (dysfunction) steatotic liver disease (MASLD). This review underscores the alarming escalation of childhood obesity and delves comprehensively into the evolving and dynamic changes of nomenclature surrounding diverse conditions of hepatic steatosis, from the initial recognition of non-alcoholic fatty liver disease (NAFLD) to the progressive evolution into MASLD. Moreover, it emphasizes the crucial role of pediatric endocrinologists in thoroughly and accurately investigating MASLD onset in children with T2DM where each condition influences and exacerbates the progression of the other. The review critically highlights the inadequacies of current screening strategies and diagnosis, stressing the need for a paradigm shift. A proposed solution involves the integration of hepatic magnetic resonance imaging assessment in the diagnostic arsenal for children showing insufficient glycaemic control and weight loss post-T2DM diagnosis, thereby complementing conventional liver enzyme testing. This holistic approach aims to significantly enhance diagnostic precision, fostering improved outcomes in this vulnerable high-risk pediatric population.
Keywords:
liver
; steatosis
; obesity
; non-alcoholic fatty liver disease
; metabolic-associated (dysfunction) steatotic liver disease
; magnetic resonance imaging
1. Introduction
Over the last three decades, there has been a twofold to threefold increase in childhood obesity rates in high-income countries. According to the 2017 data from the WHO Global Health Observatory, obesity impacts over 340 million children and adolescents aged 5–19 years [1]. The rise in obesity prevalence parallels the increase of other metabolic disorders such as expanded visceral adiposity, type 2 diabetes (T2DM), dyslipidemia, liver steatosis, hypertension, atherosclerosis [2,3], and cholesterol cholelithiasis [4]. Obesity is associated with ongoing sub-clinical chronic low-grade inflammation in various tissues, including adipose tissue, skeletal muscle, liver, pancreatic islets, intestine, and brain [5]. The inflammation involves both innate and adaptive immune cells and acts as a causal link between obesity and its metabolic dysfunction-associated complications such as insulin resistance and T2DM. The inflammatory background in obesity was first suspected after a report of elevated TNFα levels in adipose tissue [6]. The precise molecular mechanisms through which inflammation in adipose tissue contributes to insulin resistance are not thoroughly understood and may involve multiple factors. Various immune cells, particularly macrophages and T cells [7,8,9], likely contribute to insulin resistance associated with obesity. These cells release type 1 cytokines such as TNFα, interleukin (IL)-1β, and IFNγ which can negatively regulate metabolism and induce insulin resistance in various cell types, including adipocytes and skeletal muscle myocytes, through paracrine or endocrine effects. The cytokines exert their effects by interacting with receptors in the cells, triggering a cascade of intracellular signaling pathways. These pathways, in turn, compromise insulin signaling and lead to the development of insulin resistance in the affected cells[10]. Insulin resistance and chronic inflammation play pivotal roles in the development of T2DM, contributing to liver steatosis and vice versa via the accumulation of free fatty acids as triglyceride droplets in the liver cells, thus causing lipotoxicity, inflammation, and fibrosis [11].
In this context, liver steatosis can develop as the organ manifestation of metabolic dysfunctions. The first definition of non-alcoholic fatty liver disease (NAFLD) refers to the presence of steatosis by imaging or liver biopsy in individuals with no alcohol consumption or a daily alcohol consumption of ≤20 g in females and ≤30g in males and no other cause of chronic liver disease [12]. NAFLD is a prevalent chronic liver disease, affecting more than 30% of the global population worldwide [13,14], and has become the predominant cause of chronic liver disease in adults [15,16]. NAFLD is usually a silent condition but in a subgroup of patients, NAFLD can progress towards non-alcoholic steatohepatitis (NASH), advanced fibrosis, liver cirrhosis, and ultimately to hepatocellular carcinoma [16]. The term NAFLD, however, does not accurately reflect the current understanding of disease drivers, while there is a growing awareness about the close link between NAFLD and metabolic dysfunctions/metabolic syndrome [17,18]. This situation has recently promoted the shift of terminology from NAFLD to metabolic dysfunction-associated fatty liver disease (MAFLD) in 2020 [17,18] and metabolic dysfunction-associated steatotic liver disease (MASLD) in 2023 within the overarching term of steatotic liver disease (SLD), encompassing several types of liver steatosis [14,19].
This review will discuss the pediatric endocrinologist's point of view when screening pediatric patients with T2DM, to detect the potential onset of MASLD more thoroughly and accurately. We will continue using the acronyms NAFLD/NASH when discussing studies designed before the change of nomenclature to MASLD. Otherwise, MASLD/MASH will become the terms of reference.
2. Diagnostic Criteria of Liver Steatosis along with Shift of Terminology
The change in terminology i.e., NAFLD to MAFLD to MASLD will likely improve the classification of patients, disease awareness, the terminology comprehension concerning involved pathophysiological aspects (not only a diagnosis of exclusion such as for NAFLD), and hopefully pave the way for more personalized therapeutic approaches [20]. Stigmatization of terms such as "non-alcoholic" and “fatty” will be overcome as well [17,18,19]. Following the consensus document, comparative studies by registries, population studies, community cohorts, and primary care settings point to an almost complete overlap of populations when using the terminology MASLD with respect to NAFLD [21,22,23], with MASLD requiring the presence of at least one of five cardiometabolic risk factors in the context of hepatic steatosis [14]. MASLD does not impact the characterization of fibrotic severity or the definition of steatohepatitis (based on the presence of liver inflammation and hepatocellular injury, i.e., ballooning of hepatocytes, with or without fibrosis), and therefore MASH can replace NASH without altering the predicted sequence to cirrhosis [24].
Diagnostic criteria related to the novel nomenclatures differ in the case of NAFLD, MAFLD, or MASLD. For both NAFLD and MAFLD the initial diagnosis of “liver steatosis” is achieved by blood biomarkers, imaging, or histology after liver biopsy. For MASLD, the starting point is the initial diagnosis of “steatotic liver” which requires either imaging or histology. The following diagnostic pathways also differ with the three nomenclatures. The presence of NAFLD is based on exclusion of major steatogenic causes [12]. The diagnosis of MAFLD is more focused on metabolic aspects, and is based on the presence of overweight/obesity or type 2 diabetes. In addition, in the case of lean/normal weight individuals, MAFLD is diagnosed in those accumulating at least 2 out of 7 cardiometabolic risk abnormalities [17,18]. The diagnosis of MASLD takes into account the adult and pediatric age, and requires at least 1 out of 5 cardiometabolic risk abnormalities. Other discernible causes must be absent. he criterion of weekly alcohol consumption becomes important to further classify the steatotic liver as MASLD (no or little alcohol consumption), metabolic dysfunction-associated alcoholic liver disease (MetALD) or pure alcoholic liver disease (ALD). Specific etiology of steatotic liver or cryptogenic liver disease need also to be considered according to specific cases, when finalizing the diagnosis of MASLD. In the absence of overt cardiometabolic criteria, the exploration of alternative causes is essential to reach the diagnosis of a specific etiology. If none is identified, the steatotic liver disease is termed cryptogenic. If additional factors contributing to steatosis are identified, a combined etiology is recognized [19,20,25].
2.1. Refining the Diagnosis of MASLD
2.1.1. Adults
According to the current nomenclature following the Delphi consensus [19], the overarching SLD diagnosed by imaging or histology encompasses subcategories that includes:
- -
-
MASLD (i.e., liver steatosis, at least one cardiometabolic risk factor, no other discernible cause, no alcohol consumption or a weekly consumption ≤140 g in females and ≤210 g in males). In adult populations, the initial diagnosis of SLD requires the exact analysis of cardiometabolic criteria to reach the final diagnosis of MASLD or MetALD. The abnormalities are the following:
- Body mass index (BMI) ≥25 kg/m2 (23 kg/m2 for Asians) or waist circumference >94 cm (males), >80 cm (females) or ethnicity adjusted;
- Fasting serum glucose ≥100 mg/dL or 2-hrs post-load glucose levels ≥140 mg/dL) or HbA1c ≥5.7% or T2DM or treatment for T2DM
- Blood pressure ≥130/85 mmHg or specific antihypertensive treatment
- Plasma triglycerides ≥150 mg/dL or lipid-lowering treatment
- Plasma HDL-cholesterol ≤40 mg/dL (males), ≤50 mg/dL (females), or lipid-lowering treatment.
- -
- MetALD, i.e., an overlap of MASLD and ALD, i.e., liver steatosis, no other discernible cause, and intermediate weekly alcohol consumption of 140-350 g in females and 210-420g in males with a continuum ranging from MASLD-predominant to ALD-predominant types.
- -
- ALD, i.e., liver steatosis with weekly alcohol consumption >350 g in females and ≥ 420g in males)
- -
- Specific etiology SLD (i.e., drug-induced liver injury DILI, monogenic diseases such as lysosomal acid lipase deficiency LALD, Wilson disease, hypobetalipoproteinemia, inborn error of metabolism, and miscellaneous such as Hepatitis C virus, malnutrition, celiac disease).
- -
- Cryptogenic SLD, a label prone to re-classification in the future, as long as further diagnostic entities are reached. Importantly, the diagnosis of SLD must be re-assessed periodically to rule out incoming findings suggesting novel diagnoses.
For MASLD, the concept of an affirmative diagnosis allows for the coexistence of mixed forms of liver disease, e.g. MASLD plus viral hepatitis or autoimmune hepatitis.
2.1.2. Children and Adolescents
MAFLD has become the most common cause of liver disease also in children. This phenotype will likely benefit from early interventions aimed at the treatment of liver steatosis, obesity, and metabolic abnormalities, therefore reducing the long-term consequences of metabolic, cardiovascular, and liver complications. Aspects related to a child’s and family’s quality of life need also to be considered [26]. In this respect, lifestyle changes consisting of dietary interventions, physical activity, and nutritional and psychological counseling have been shown to improve body mass index (BMI), aminotransferase levels, and hepatic steatosis in children with MAFLD [27]. Diagnostic criteria for the pediatric MASLD area are also detailed in the Delphi consensus paper and are very close to the adult ones [19]. Following the first diagnosis of steatotic liver on imaging or liver biopsy, at least one specific cardiometabolic risk factor out of five must be present, i.e.,
- Overweight/obesity – i.e., BMI ≥85th percentile for age/sex (BMI Z-score ≥+1) or waist circumference >95th percentile (values may vary by ethnicity or race);
- Prediabetes/diabetes testified by fasting serum glucose ≥100 mg/dL or random serum glucose ≥200 mg/dL or 2-hour oral glucose tolerance test ≥140 mg/dL or HbA1c ≥5.7% or established diagnosis of T2DM or specific treatment for T2DM.
- Hypertension testified by blood pressure (BP) ≥130/80 mmHg for age ≥13 years; for age <13 years, BP ≥95th percentile or ≥130/80 mmHg (whichever is lower) or use of antihypertensive treatment.
- Hypertriglyceridemia with triglyceride ≥100 mg/dL for age <10 years or triglyceride ≥150 mg/dL for age ≥10 years or lipid-lowering treatment
- Low cholesterol HDL, i.e., HDL ≤40 mg/dL or lipid-lowering treatment.
The imperative to redefine the term NAFLD in the pediatric population is even more significant than in adults, as alcohol consumption is not a typical factor, considering the widespread prohibition for individuals under the age of 18 in most countries. In children with steatosis and without typical cardiometabolic risk factors, causes such as parenteral nutrition, hepatitis C, lipodystrophy, steatogenic medication such as valproate, or inborn errors of metabolism must be considered as well. Depending on the presence of cardiometabolic risk factors alone or additional factors, the possibility of MetALD or other combination etiologies is a possibility [19]. Of note, the ultimate diagnosis of MASH in children lacks reliable noninvasive biomarkers and requires liver biopsy. According to histology, a further classification includes definite and borderline zone 1 and zone 3 patterns.
3. MASLD Epidemiology and Natural History
Data on the prevalence of pediatric steatotic liver disease are scanty and depend largely on a difficult diagnosis. The nomenclature aspect, and as mentioned earlier, an almost complete overlap of populations exists between MASLD and NAFLD in adults [21,22,23], but this aspect is still poorly investigated in pediatric age [14]. These considerations highlight the difficulty in identifying children with hepatic steatosis, a preliminary requirement for making a diagnosis of MASLD. The prevalence of fatty liver disease in children is strongly influenced by the diagnostic methodology. According to the NAFLD terminology, indirect methods included imaging (mainly ultrasonography) or elevations in serum aminotransferase levels in at-risk subjects. For MASLD, diagnostic includes radiologic or biopsy evidence of steatosis in children with precise metabolic risk factors, although prospective studies in pediatric MASLD are lacking, so far. Results can be also influenced by the age of screening, i.e., generally after 9 years of age, although steatosis can also develop in utero [28] and cirrhosis earlier than 9 years of age [29,30]. A further aspect is the environmental context where studies are performed, i.e., different ethnic groups, community populations, or hospital setting, etc.
The estimates NAFLD prevalence for European populations range from 1.3% to 22.5% in children aged 3–18 years, or 11% in children aged 12.4 ± 2.6 years if defined by elevated AST or ALT concentrations more than 50 IU/L [31]. In the United States NAFLD prevalence ranges from 9.6% of all children aged between 2 and 19 years to 38.0% of obese children when fatty liver is defined by the presence of overweight (BMI ≥95th percentile) and elevated ALT concentrations: more than 25.8 IU/L for boys and more than 22.1 IU/L for girls [32,33]. According to the recent US National Health and Nutrition Examination Survey (2011 to 2018), elevated ALT (>22 units/L for females and >26 units/L for males) occurred in 16% of (likely NAFLD) adolescents, and in 39% of obese adolescents [34]. Another large population-based study in adolescents (range 1988-1994 to 2007-2010), examined increased ALT and reported that the prevalence of suspected NAFLD has more than doubled over the past 20 years affecting about 11% of adolescents and one-half of obese males [33]. A meta-analysis based on abnormal ALT at various thresholds and comparison with imaging reported that the estimated NAFLD prevalence was 7% and 14% in the general population (by 9 studies) and in children with obesity (by 14 studies), respectively[35]. Ultrasonography has been reported to have poor sensitivity and specificity for detecting and grading hepatic steatosis in children. Although the study is not recent, based on PubMed search of a limited number of papers, the authors found that US had positive predictive values of 47% to 62% [36]. Data on the prevalence of liver steatosis in children and adolescents examined by ultrasonography must be interpreted with caution, since further evidences are required [35]. By transient elastography and controlled attenuation parameter, utilizing the Health and Nutrition Examination Survey 2017–18 database, the prevalence of steatosis in US adolescents (12–18 years) was 24.2% [37]. Irrespective of the diagnostic methods employed, recent studies (which consider the differences between NAFLD and MAFLD) estimate that in the general population the MAFLD prevalence stood at 33.78%, while in a specific subgroup attending child obesity clinics, it was 44.94%. When examining subgroups, the prevalence of MAFLD was notably elevated in boys as opposed to girls, registering at 36.05% versus 26.84% in the general population and 50.20% versus 35.34% in the child obesity clinic-based population [38].
Histological studies have been performed during autopsy studies. The prevalence of fatty liver was 9.6% overall (steatohepatitis 3%) and 38% in obese children (steatohepatitis 23%) among 742 children and adolescents in a fairly representative study of unselected population in San Diego County [32]. Race/ethnicity played a role independently of obesity since Hispanic youth had a fivefold increase in risk for steatotic liver as compared with Black youth. White youth had intermediate risk. Another autopsy study conducted in New York City reported a lower prevalence and severity of NAFLD in black children compared with the general obese pediatric population. Hispanic children did not have a significantly increased rate of NAFLD compared with white children. This finding is most likely related to the large proportion of Caribbean Hispanic children in New York City and the lower proportion of Mexican/Central American Hispanic ethnicity compared with the San Diego County region [39]. The finding that Caribbean Hispanic ancestry is associated with a higher percentage of African genetic admixture, appears to be protective against hepatic steatosis [40]. Studies about the natural history of children with liver steatosis diagnosed by recent MASLD criteria are still required.
4. MASLD Pathogenesis and Molecular Aspects
The pathogenesis and etiology of MASLD are not yet fully understood, however, they are known to be closely associated with metabolic dysfunction. The pathogenesis of MASLD appears to be multifactorial, arising from interaction among various factors such as genetic, epigenetic, environmental, and lifestyle factors [20]. MASLD is strongly associated with metabolic dysfunction, which very often develops due to unhealthy lifestyles and dietary habits. Low physical activity, a sedentary lifestyle, a Western diet, and high caloric intake contribute to the development of overweight and obesity[16], which are primary risk factors associated with MASLD [41]. Adipose tissue expansion, accompanying obesity, leads to its dysfunction. Dysfunctional adipose tissue releases molecules such as free fatty acids (FFA), reactive oxygen spices (ROS), and pro-inflammatory cytokines (leptin, IL-6, TNF-Alpha, etc) leading to impairment in insulin-signalling pathways and subsequent insulin resistance [42]. Insulin resistance disturbs the body homeostatic control of several gluco-lipid parameters, because of a status of sustained hyperinsulinemia. This imbalance contributes to the development of T2DM and de novo lipogenesis, promoting dyslipidemia [43]. Moreover, the release of pro-inflammatory molecules from visceral adipose tissue contributes to the development of a state of chronic low-grade systemic inflammation, which further impairs the insulin signalling pathway [42]. Factors such as alcohol, smoking, air pollutants, gut dysbiosis, and food contaminants may contribute to MASLD development and progression [16]. This increased uptake of FFA by the liver leads to hepatic lipid overload and their subsequent excessive accumulation within hepatocytes[44]. Hepatic intracellular lipids exert a lipotoxic effect on hepatocytes, known as “lipotoxicity”, which arises from their toxic metabolites such as lipophosphatidylcholine, ceramides, and diacylglycerol, resulting in increased oxidative stress and development of inflammation within hepatocytes, resulting in hepatocyte dysfunction and disruption of numerous physiological processes within the liver [16]. The liver plays a central role in lipid metabolism [45]. When hepatocytes become dysfunctional, they become unable to perform their normal functions, including lipid metabolism [46]. Consequently, hepatic dysfunction further leads to impaired lipid metabolism, ultimately resulting in the development of dyslipidemia, which has systemic effects [47]. Moreover, excessive lipids in the liver will further impair the insulin signing pathway, aggravating insulin resistance, and exacerbating dysregulation in lipid metabolism, notably marked by elevated triglycerides and LDL-cholesterol levels, and lowered HDL-cholesterol levels in circulation. This progression contributes significantly to the exacerbation of MASLD [48]. Hence, MASLD becomes a significant risk contributor for hepatic complications directly affecting the liver or as extra-hepatic complications [49,50].
5. Challenging Diagnosis of MASLD in Children and Adolescents
5.1. Clinical Aspects
As for adults, children with MASLD are largely asymptomatic [51], although a minority of children can describe right upper quadrant pain or vague abdominal discomfort and fatigue [52,53]. Other symptoms are even more vague and might depend on obesity-associated comorbidities, i.e., constipation, gastroesophageal reflux disease, and functional abdominal pain [54]. Other signs related to end-stage liver disease include spider angiomata, palmar erythema, muscle wasting, jaundice, or encephalopathy but they are rarely observed as MASLD in childhood has a rare progression to decompensated cirrhosis. As a consequence of the close association with insulin resistance/T2DM, the physical exam may reveal acanthosis nigricans and abdominal adiposity. This latter finding can hide the presence of hepatomegaly and/or splenomegaly. For pediatric MASLD, epidemiological data, risk factors, natural history, and therapy are based on studies investigating children with chronically elevated liver enzymes. While fatty liver disease with normal ALT levels is acknowledged in both adults and pediatric populations [55], increased ALT level alone may indicate liver injury but may not necessarily indicate NAFLD/MASLD. Laboratory abnormalities, if present, include elevated serum liver transaminases (alanine aminotransferase [ALT] and aspartate aminotransferase [AST]), alkaline phosphatase, and gamma-glutamyl transpeptidase (GGTP)[30,51,56,57,58].
5.2. Screening
In historical studies, the screening for NAFLD was based on the measurement of serum ALT [59]. Aminotransferase elevations act as a surrogate biomarker of NAFLD still yielding poor sensitivity and specificity for detecting steatosis and depending also on the ALT cut-off used in the studies [60]. For the detection of steatosis Jebeile et al. [1] recommend evaluation of ALT concentrations (< 25.8 IU/L for boys and < than 22.1 IU/L for girls), liver ultrasound or transient elastography indifferently. The North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPHGAN) recommends as screening test the measurement of serum ALT, as an inexpensive, minimally invasive, and universally available test [59]. However, the normal ALT cut-off varies across populations [61,62], and the sensibility of ALT measure in overweight and obese children age ≥ 10 years, (considering ALT ≥50 IU/L for boys and ≥44 IU/L for girls as abnormal) is less than 90% [60].
Conventional ultrasonography, although used in clinical practice, yields poor outcome for the diagnosis or grading of fatty liver in children [36]. The increased echogenicity can be detected by ultrasonography but sensitivity and specificity for detecting clinically significant liver disease are poor [59,63,64]. Ultrasonography and ALT exhibit comparable yet modest diagnostic precision (ROC of ALT and US were not significantly different: 0.74 and 0.70, respectively) for detecting hepatic steatosis in obese children. The diagnostic accuracy of ALT (optimal threshold ≥40 IU/L) and ultrasonography (optimal steatosis score ≥2) is comparable with moderate specificity (89% for ALT, 80% for ultrasonography), and their combination did not enhance overall accuracy, suggesting limitations in current screening strategies for hepatic steatosis in children[65]. Computed tomography, while reasonably effective in sensitivity and specificity for detecting steatosis, is not advisable for diagnostic purposes due to the associated risk of radiation.
More validation studies are necessary for the assessment of liver fibrosis by transient elastography (FibroScan®), ultrasound shear wave elastography or enhanced liver fibrosis test [65]. The same applies to other imaging tests such as magnetic resonance elastography for assessment of liver stiffness and magnetic resonance imaging proton density fat fraction for estimation of liver fat content [65,66]. These techniques, due to their high cost and time-consuming nature, are primarily applicable in research settings [67]. The first guideline was issued in 2012 by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition and recommended screening with ALT and imaging due to the possibility that some children with hepatic steatosis still have normal liver enzymes [68,69].
As outlined later in 2017 by the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition NASPHGAN guidelines, the initiation of screening for hepatic steatosis is recommended with ALT alone [59]. Screening starts between ages 9–11 years for obese children (BMI ≥95th percentile) and overweight children (BMI ≥85th and <94th percentile) who exhibit additional risk factors such as central adiposity, insulin resistance, pre-diabetes or diabetes, dyslipidemia, sleep apnea, or a family history of NAFLD/NASH. Consideration for earlier screening is warranted for younger patients with factors like severe obesity, family history of NAFLD/NASH, or hypopituitarism. Furthermore, it is advisable to screen siblings and parents of children with NAFLD if they present known risk factors, including obesity, Hispanic ethnicity, insulin resistance, pre-diabetes, diabetes, and dyslipidemia [59].
The upper limit of normal (ULN) is different for adolescents 12 to 17 years (girls – 22 units/L; boys – 26 units/L referred to the 97th percentiles for a healthy lean population [70,71] and children 1 to <12 years (30 units/L, referred to the CALIPER study [72]). After the screening, the subsequent follow-up will depend on the degree and duration of ALT elevation, ranging from 1-3 years to a few months, to specialist referral with normal ALT, moderate ALT elevations (ALT >ULN but <80 units/L), ALT persistently >2 × ULN (ie, >44 units/L for adolescent girls and 52 units/L for boys) for three or more months, respectively. Attention must be given to the onset of other viral infections, acute increase of ALT, symptoms of more advanced liver disease [73], degree of obesity, ethnicity (Hispanic children [74]), or comorbid conditions contributing to the onset or progression of MASLD, namely obstructive sleep apnea (OSA), hypothyroidism, depression or anxiety, use of alcohol and drugs of family history for metabolic, autoimmune liver diseases, other chronic liver diseases, or insulin resistance, T2DM (see below).
Thus, each method described above has some limitations. The ultimate diagnosis of all stages of liver steatosis relies on liver biopsy as the gold standard, but the technique is invasive, has the potential for sampling errors, and is not easily accepted by patients and their families [66]. Until new evidence accumulate about the best screening methodology in pediatric MASLD, screening with ALT in most settings will remain the main approach to select the subgroup of subjects at increased risk of progression, although the subset of children with hepatic steatosis who have normal liver enzymes will be missed. Further limitations in this context are ULN which can govern sensitivity and specificity[60], and the possibility of progression to fibrosis despite normal ALT (12%) or moderately elevated ALT (54%)[55].
6. T2DM and MASLD
6.1. Interconnections
Diabetic children and adolescents are a particularly monitored population, given the high association between NAFLD/MAFLD and T2DM[75,76]. Indeed, MASLD is particularly common in children living with T2DM and/or obesity. The progression of NAFLD to NASH is influenced by insulin resistance and T2DM. In adults, Younossi et al. [75]demonstrated an increased prevalence of cirrhosis in 132 adult subjects with histologically confirmed NAFLD and T2DM compared to those without diabetes (25% vs. 10% respectively). The development of hepatocellular carcinoma in adults with NAFLD is influenced by T2DM, acting as an independent risk factor[77]. Whether such an effect will become apparent in young populations (pediatric patients, adolescents) deserves much attention. A mild increase in serum ALT is common in T2DM adolescents [78]. In addition, obese children often suffer from insulin resistance and T2DM [79] and develop an increased accumulation of intrahepatic fat with progression to liver steatosis [76]. According to the TODAY study, 6.5 % of youth exhibited a mild ALT elevation (1.5 to 2.5 times the upper limits of normal) shortly after being diagnosed with T2DM. Over the course of the study (2 to 6.5 years of follow-up), 16 % of participants experienced ALT elevations[80].
As for screening, the International Society for Pediatric and Adolescent Diabetes (ISPAD) has developed specific recommendations for prompt NAFLD detection in children with T2DM [81]. In T2DM children and adolescents, liver enzymes ALT and AST should be measured at diagnosis and annually thereafter, and sooner if abnormal. In addition, if liver enzymes remain >3 times the upper limit of normal after 6 months, patients must be seen by a pediatric gastroenterologist for consultation to exclude other causes of elevated liver enzymes, and to consider imaging and/or liver biopsy. Vice-versa, NAFLD is often associated with metabolic disturbances.
In general, children with biopsy-proven NAFLD suffer from a higher prevalence of impaired fasting glucose, impaired glucose tolerance, and T2DM compared to children without NAFLD of similar age, gender, and adiposity [82]. The prevalence of prediabetes or diabetes in children with biopsy-proven NAFLD is 20%–30% in Italy and in the United States [82,83]. Normoglycemic children with biopsy- or imaging-proven NAFLD in Israel, had a 3-fold increased risk for T2DM compared to youth without NAFLD. This difference was evident after adjustment for BMI [84]. In a meta-analysis, adults with T2DM had an increased prevalence of NAFLD (55.5%), NASH (37%), and advanced fibrosis (17%)[85]. The prevalence of T2DM and prediabetes in children with NAFLD is 23.4% and 6.5%, respectively. The prevalence of NASH is higher in children with T2DM (43.2%) compared to children with prediabetes (34.2%) or normal glucose tolerance (22%). Girls with NAFLD have a higher risk of having prediabetes and T2DM than boys with NAFLD [83]. Children with NAFLD exhibit notably higher rates of impaired fasting glucose when compared to matched controls who are overweight or obese [86]. Increased intrahepatic fat content is linked to more pronounced insulin resistance and impaired glucose regulation before the development of clinically overt diabetes [86,87]. D’Adamo et al. [86]demonstrated a central role of hepatic fat content in the pathogenesis of insulin resistance in obese adolescents independently of visceral fat and intrabdominal intramyocellular lipid content. However, whether hepatic steatosis is a consequence or a cause of the metabolic derangements in insulin sensitivity is still debatable[60]. The combined impact of MASLD and T2DM heightens the risks of morbidity and mortality in childhood[88]. In particular, T2DM in MASLD becomes a strong independent predictor of progression to inflammation and fibrosis, namely MASH [89].
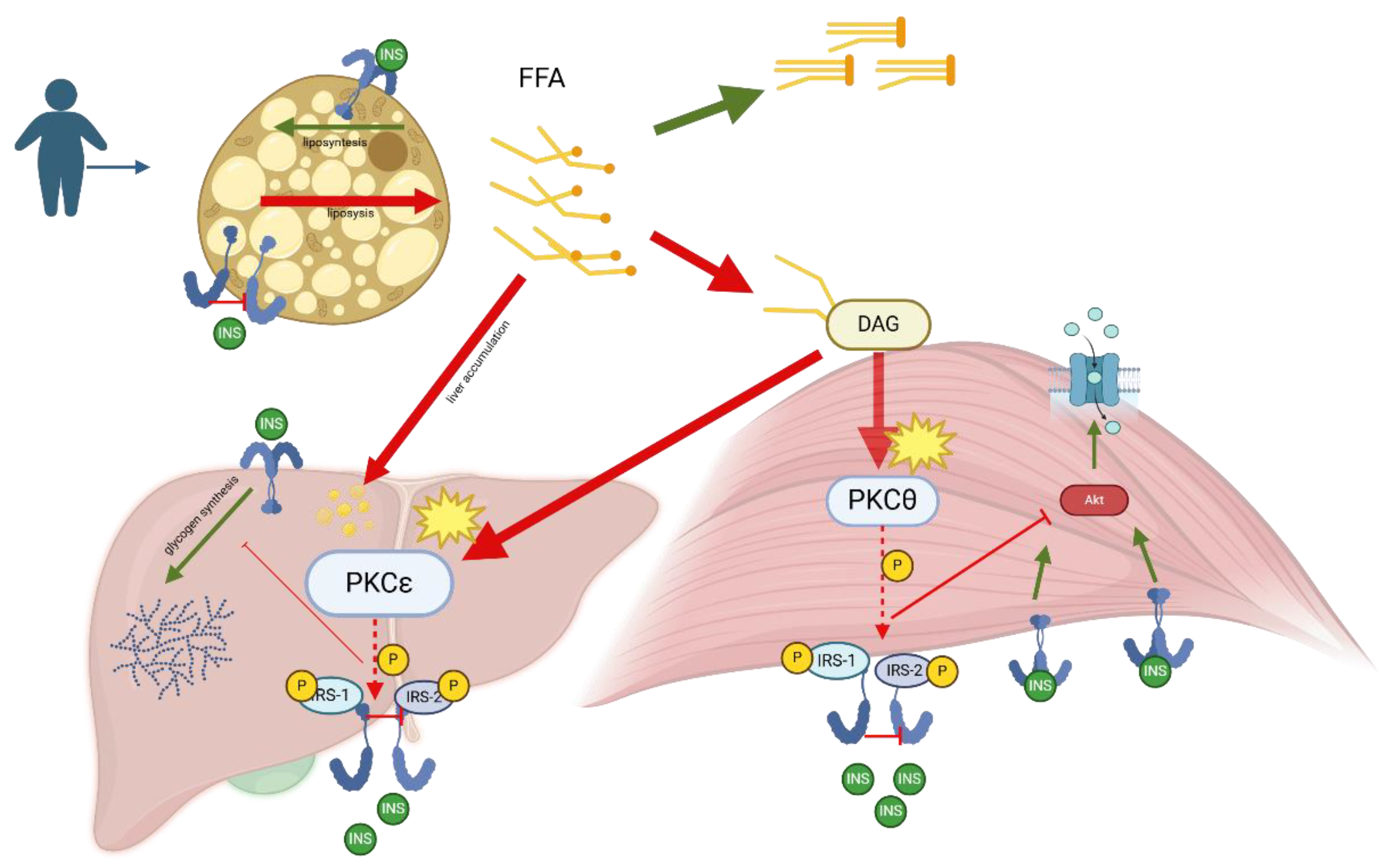
Figure 2.
Metabolic-associated fatty liver disease (MAFLD), previously known as NAFLD (Non-Alcoholic Fatty Liver Disease), is closely linked to insulin resistance. Elevated levels of free fatty acids (FFA) in the blood, commonly associated with obesity and metabolic diseases, are released through lipolysis from adipose tissue and taken up by the liver and muscles. In the liver, FFAs are esterified into triglycerides, leading to fat accumulation and hepatic steatosis, characteristic of MAFLD. When FFA supply exceeds the capacity for oxidation and storage as triglycerides, they are diverted into alternative pathways, including diacylglycerol (DAG) synthesis. Within cells, FFAs are esterified with glycerol-3-phosphate to form DAG. DAG acts as a second messenger, activating specific isoforms of protein kinase C (PKC), such as PKCθ in skeletal muscle and PKCε in the liver. Activated PKCθ and PKCε translocate to the cell membrane, where they phosphorylate serine/threonine residues on insulin receptor substrates (IRS-1 and IRS-2), impairing insulin signaling. This results in reduced Akt activation decreased translocation of GLUT4 glucose transporters to the cell membrane in muscles, and reduced glucose uptake. In the liver, impaired insulin signaling leads to reduced glycogen synthesis and increased gluconeogenesis, contributing to hyperglycemia and insulin resistance. Additionally, excess FFA in the liver enhances triglyceride synthesis and fatty acid oxidation, producing reactive oxygen species (ROS) that cause cellular damage and inflammation, progressing MAFLD from steatosis to steatohepatitis (NASH). The chronic inflammation and oxidative stress further stimulate the production of pro-inflammatory cytokines and chemokines, attracting inflammatory cells to the liver, and leading to fibrosis and potentially cirrhosis. Thus, the interplay between insulin resistance and MAFLD involves a complex network of metabolic disturbances, lipid accumulation, and inflammatory pathways.
Figure 2.
Metabolic-associated fatty liver disease (MAFLD), previously known as NAFLD (Non-Alcoholic Fatty Liver Disease), is closely linked to insulin resistance. Elevated levels of free fatty acids (FFA) in the blood, commonly associated with obesity and metabolic diseases, are released through lipolysis from adipose tissue and taken up by the liver and muscles. In the liver, FFAs are esterified into triglycerides, leading to fat accumulation and hepatic steatosis, characteristic of MAFLD. When FFA supply exceeds the capacity for oxidation and storage as triglycerides, they are diverted into alternative pathways, including diacylglycerol (DAG) synthesis. Within cells, FFAs are esterified with glycerol-3-phosphate to form DAG. DAG acts as a second messenger, activating specific isoforms of protein kinase C (PKC), such as PKCθ in skeletal muscle and PKCε in the liver. Activated PKCθ and PKCε translocate to the cell membrane, where they phosphorylate serine/threonine residues on insulin receptor substrates (IRS-1 and IRS-2), impairing insulin signaling. This results in reduced Akt activation decreased translocation of GLUT4 glucose transporters to the cell membrane in muscles, and reduced glucose uptake. In the liver, impaired insulin signaling leads to reduced glycogen synthesis and increased gluconeogenesis, contributing to hyperglycemia and insulin resistance. Additionally, excess FFA in the liver enhances triglyceride synthesis and fatty acid oxidation, producing reactive oxygen species (ROS) that cause cellular damage and inflammation, progressing MAFLD from steatosis to steatohepatitis (NASH). The chronic inflammation and oxidative stress further stimulate the production of pro-inflammatory cytokines and chemokines, attracting inflammatory cells to the liver, and leading to fibrosis and potentially cirrhosis. Thus, the interplay between insulin resistance and MAFLD involves a complex network of metabolic disturbances, lipid accumulation, and inflammatory pathways.
6.2. Follow-up Implications
The progression of pediatric fatty liver disease is not fully elucidated. Similarly, to adults, children with NAFLD and T2DM likely have an increased risk of progression to NASH and cirrhosis [83]. Data on the natural history of pediatric NAFLD emerge from a study of 122 children with biopsy-confirmed NAFLD, who enrolled in the placebo arm of clinical trials and received standard-of-care lifestyle counseling. One-third of participants experienced histological progression after a median of 1.6 years of follow-up, and this progression correlated with the severity of insulin resistance [90]. Repeat liver biopsy revealed that borderline/definite NASH at baseline ameliorated to no NASH (29%), fatty liver or borderline NASH at baseline showed progression to definite NASH (18%), NAFLD resolved in 2.4% percent (all children with steatosis but not NASH at baseline), fibrosis improved (34%) and progressed (23%). Clinical characteristics associated with disease progression/fibrosis worsening included baseline adolescent age, ALT, and total and low-density lipoprotein (LDL) cholesterol levels. Longitudinal predictors of disease progression were a rising ALT, gamma-glutamyl transpeptidase (GGTP), and hemoglobin A1c as well as the development of type 2 diabetes. These factors may help guide escalation to more intensive interventions and decisions regarding repeat liver biopsy. Overall, 7% of the cohort developed incident T2DM within two years, at a cumulative incidence rate nearly 300-fold the rate of the general pediatric population. Similarly, children with congenital generalized lipodystrophy, characterized by very high insulin resistance, exhibit advanced fatty liver disease and the complete spectrum of features associated with metabolic syndrome [91]. The strong association between T2DM and MAFLD, along with the rapid progression of the latter towards advanced liver diseases, especially in diabetic patients, underscores the imperative for pediatric endocrinologists to actively investigate the presence of MASLD in children with T2DM. We contend that ISPAD recommendations, advocating for steatosis screening through liver enzymes at the onset of the pathology and subsequently on an annual basis, may prove insufficient. The challenging determination of ALT normality cut-offs and their relative sensitivity and specificity could compromise the identification of children with MASLD in a significantly high-risk population. Likely, children who do not achieve adequate glycemic control and satisfactory weight loss in the year following the diagnosis of T2DM, and with normal liver enzyme testing, are candidates for hepatic MRI assessment.
6.3. Therapeutic Aspects
Most data on pediatric age derive from studies looking at therapeutic outcome in NAFLD or NASH (Table 1). Weight management by diet and exercise remains the only established treatment for NAFLD [29,59]. In selected adolescents with severe obesity, bariatric surgery may be appropriate [29]. A large meta-analysis based on 106 randomized controlled trials with 4 conducted in children, found limited evidence for therapy in NAFLD with no specific recommendations [92]. A systematic review in 2617 NAFLD individuals with and without T2DM reported that few antidiabetic medications improve liver enzymes but only glitazones and glucagon-like peptide 1 receptor (GLP-1) agonists, liraglutide and semaglutide appear to improve NAFLD histology. Longer trials are required in this field[93]. While the presence of NAFLD does not preclude the use of metformin, achieving optimal blood glucose levels and improving weight, do contribute to amelioration of NAFLD. Concerning specific NAFLD pharmacotherapy, to date, no medications are recommended for routine treatment of MASLD in children[59], including vitamin E, metformin, losartan, and cysteamine bitartrate. None of such treatments is superior to lifestyle intervention[94,95]. Such evidence underscores the key role of healthy lifestyle interventions promoting weight loss and optimizing blood glucose levels to improve NAFLD [96].
7. Conclusions
The continuous rise in childhood obesity and T2DM has increased the attention of researchers towards potential liver implications. The concern is mainly based on the rationale that metabolic dysfunction-associated conditions become chronic, long-lasting, and potentially harmful events in the lives of young populations. The close interactions between cardiometabolic risk abnormalities and MASLD will expose young individuals to a double risk, i.e., early cardiovascular and late liver related.
This is particularly true in both Westernized societies and emerging societies in developing countries where the effects of wrong lifestyles, including obesogenic diets and sedentary habits will affect the healthy status of several societies.
In this respect, pediatric populations and their families will require close surveillance now and, in the future, to prevent or to actively take care of T2DM, overweight, obesity, metabolic syndrome, and steatotic liver. Current screening methods for steatotic liver, such as ALT measurement and ultrasonography, exhibit limitations, emphasizing the need for precise diagnostic strategies, including hepatic MRI, to improve outcomes in this high-risk pediatric population.
Taking together, the battle against obesity especially in early ages is becoming more and more challenging. Thus, high medical, social, and economic consequences and potentially serious long-term sequelae are anticipated. This truth also stands for the rising prevalence of steatotic liver disease in children with metabolic disorders. We need more confidence and new actions to reverse such unfavourable trends.
References
- Jebeile, H.; Kelly, A.S.; O'Malley, G.; Baur, L.A. Obesity in children and adolescents: epidemiology, causes, assessment, and management. Lancet Diabetes Endocrinol 2022, 10, 351–365. [Google Scholar] [CrossRef] [PubMed]
- Wasniewska, M.; Pepe, G.; Aversa, T.; Bellone, S.; de Sanctis, L.; Di Bonito, P.; Faienza, M.F.; Improda, N.; Licenziati, M.R.; Maffeis, C.; et al. Skeptical Look at the Clinical Implication of Metabolic Syndrome in Childhood Obesity. Children (Basel, Switzerland) 2023, 10. [Google Scholar] [CrossRef]
- Di Bonito, P.; Di Sessa, A.; Licenziati, M.R.; Corica, D.; Wasniewska, M.; Umano, G.R.; Morandi, A.; Maffeis, C.; Faienza, M.F.; Mozzillo, E.; et al. Is Metabolic Syndrome Useful for Identifying Youths with Obesity at Risk for NAFLD? Children (Basel, Switzerland) 2023, 10. [Google Scholar] [CrossRef]
- Portincasa, P.; Di Ciaula, A.; Bonfrate, L.; Stella, A.; Garruti, G.; Lamont, J.T. Metabolic dysfunction-associated gallstone disease: expecting more from critical care manifestations. Internal and emergency medicine 2023, 18, 1897–1918. [Google Scholar] [CrossRef]
- Ellulu, M.S.; Patimah, I.; Khaza'ai, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: the linking mechanism and the complications. Arch Med Sci 2017, 13, 851–863. [Google Scholar] [CrossRef] [PubMed]
- Hotamisligil, G.S.; Shargill, N.S.; Spiegelman, B.M. Adipose expression of tumor necrosis factor-alpha: direct role in obesity-linked insulin resistance. Science 1993, 259, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Parekh, V.V.; Gabriel, C.L.; Bracy, D.P.; Marks-Shulman, P.A.; Tamboli, R.A.; Kim, S.; Mendez-Fernandez, Y.V.; Besra, G.S.; Lomenick, J.P.; et al. Activation of invariant natural killer T cells by lipid excess promotes tissue inflammation, insulin resistance, and hepatic steatosis in obese mice. Proceedings of the National Academy of Sciences of the United States of America 2012, 109, E1143–1152. [Google Scholar] [CrossRef]
- DeFuria, J.; Belkina, A.C.; Jagannathan-Bogdan, M.; Snyder-Cappione, J.; Carr, J.D.; Nersesova, Y.R.; Markham, D.; Strissel, K.J.; Watkins, A.A.; Zhu, M.; et al. B cells promote inflammation in obesity and type 2 diabetes through regulation of T-cell function and an inflammatory cytokine profile. Proceedings of the National Academy of Sciences of the United States of America 2013, 110, 5133–5138. [Google Scholar] [CrossRef]
- Boulenouar, S.; Michelet, X.; Duquette, D.; Alvarez, D.; Hogan, A.E.; Dold, C.; O'Connor, D.; Stutte, S.; Tavakkoli, A.; Winters, D.; et al. Adipose Type One Innate Lymphoid Cells Regulate Macrophage Homeostasis through Targeted Cytotoxicity. Immunity 2017, 46, 273–286. [Google Scholar] [CrossRef]
- Wu, H.; Ballantyne, C.M. Metabolic Inflammation and Insulin Resistance in Obesity. Circ Res 2020, 126, 1549–1564. [Google Scholar] [CrossRef] [PubMed]
- Marusic, M.; Paic, M.; Knobloch, M.; Liberati Prso, A.M. NAFLD, Insulin Resistance, and Diabetes Mellitus Type 2. Can J Gastroenterol Hepatol 2021, 2021, 6613827. [Google Scholar] [CrossRef]
- Ludwig, J.; Viggiano, T.R.; McGill, D.B.; Oh, B.J. Nonalcoholic steatohepatitis: Mayo Clinic experiences with a hitherto unnamed disease. Mayo Clinic proceedings. Mayo Clinic 1980, 55, 434–438. [Google Scholar]
- Yip, T.C.; Vilar-Gomez, E.; Petta, S.; Yilmaz, Y.; Wong, G.L.; Adams, L.A.; de Ledinghen, V.; Sookoian, S.; Wong, V.W. Geographical similarity and differences in the burden and genetic predisposition of NAFLD. Hepatology 2023, 77, 1404–1427. [Google Scholar] [CrossRef]
- Rinella, M.E.; Neuschwander-Tetri, B.A.; Siddiqui, M.S.; Abdelmalek, M.F.; Caldwell, S.; Barb, D.; Kleiner, D.E.; Loomba, R. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 2023, 77, 1797–1835. [Google Scholar] [CrossRef]
- Paik, J.M.; Kabbara, K.; Eberly, K.E.; Younossi, Y.; Henry, L.; Younossi, Z.M. Global burden of NAFLD and chronic liver disease among adolescents and young adults. Hepatology 2022, 75, 1204–1217. [Google Scholar] [CrossRef]
- Portincasa, P. NAFLD, MAFLD, and beyond: one or several acronyms for better comprehension and patient care. Internal and emergency medicine 2023, 18, 993–1006. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J.; International Consensus, P. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014 e1991. [Google Scholar] [CrossRef]
- Mendez-Sanchez, N.; Bugianesi, E.; Gish, R.G.; Lammert, F.; Tilg, H.; Nguyen, M.H.; Sarin, S.K.; Fabrellas, N.; Zelber-Sagi, S.; Fan, J.G.; et al. Global multi-stakeholder endorsement of the MAFLD definition. The lancet. Gastroenterology & hepatology 2022, 7, 388–390. [Google Scholar] [CrossRef]
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology 2023, 78, 1966–1986. [Google Scholar] [CrossRef] [PubMed]
- Portincasa, P.; Baffy, G. Metabolic dysfunction-associated steatotic liver disease: Evolution of the final terminology. European journal of internal medicine 2024, 124, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Ratziu, V.; Boursier, J.; Fibrosis, A.G.f.t.S.o.L. Confirmatory biomarker diagnostic studies are not needed when transitioning from NAFLD to MASLD. Journal of hepatology 2024, 80, e51–e52. [Google Scholar] [CrossRef] [PubMed]
- Song, S.J.; Lai, J.C.; Wong, G.L.; Wong, V.W.; Yip, T.C. Can we use old NAFLD data under the new MASLD definition? Journal of hepatology 2024, 80, e54–e56. [Google Scholar] [CrossRef]
- Lee, C.M.; Yoon, E.L.; Kim, M.; Kang, B.K.; Cho, S.; Nah, E.H.; Jun, D.W. Prevalence, distribution, and hepatic fibrosis burden of the different subtypes of steatotic liver disease in primary care settings. Hepatology 2024, 79, 1393–1400. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.E.; Sookoian, S. From NAFLD to MASLD: updated naming and diagnosis criteria for fatty liver disease. Journal of lipid research 2024, 65, 100485. [Google Scholar] [CrossRef] [PubMed]
- Portincasa, P.; Khalil, M.; Mahdi, L.; Perniola, V.; Idone, V.; Graziani, A.; Baffy, G.; Di Ciaula, A. Metabolic Dysfunction-Associated Steatotic Liver Disease: From Pathogenesis to Current Therapeutic Options. International journal of molecular sciences 2024, 25, 5640. [Google Scholar] [CrossRef]
- Eslam, M.; Sarin, S.K.; Wong, V.W.; Fan, J.G.; Kawaguchi, T.; Ahn, S.H.; Zheng, M.H.; Shiha, G.; Yilmaz, Y.; Gani, R.; et al. The Asian Pacific Association for the Study of the Liver clinical practice guidelines for the diagnosis and management of metabolic associated fatty liver disease. Hepatol Int 2020, 14, 889–919. [Google Scholar] [CrossRef]
- Utz-Melere, M.; Targa-Ferreira, C.; Lessa-Horta, B.; Epifanio, M.; Mouzaki, M.; Mattos, A.A. Non-Alcoholic Fatty Liver Disease in Children and Adolescents: Lifestyle Change - a Systematic Review and Meta-Analysis. Annals of hepatology 2018, 17, 345–354. [Google Scholar] [CrossRef]
- Patel, K.R.; White, F.V.; Deutsch, G.H. Hepatic steatosis is prevalent in stillborns delivered to women with diabetes mellitus. Journal of pediatric gastroenterology and nutrition 2015, 60, 152–158. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Kinugasa, A.; Tsunamoto, K.; Furukawa, N.; Sawada, T.; Kusunoki, T.; Shimada, N. Fatty liver and its fibrous changes found in simple obesity of children. Journal of pediatric gastroenterology and nutrition 1984, 3, 408–414. [Google Scholar] [CrossRef]
- Wiegand, S.; Keller, K.M.; Robl, M.; L'Allemand, D.; Reinehr, T.; Widhalm, K.; Holl, R.W.; Group, A.P.-S.; the German Competence Network, A. Obese boys at increased risk for nonalcoholic liver disease: evaluation of 16,390 overweight or obese children and adolescents. International journal of obesity 2010, 34, 1468–1474. [Google Scholar] [CrossRef]
- Schwimmer, J.B.; Deutsch, R.; Kahen, T.; Lavine, J.E.; Stanley, C.; Behling, C. Prevalence of fatty liver in children and adolescents. Pediatrics 2006, 118, 1388–1393. [Google Scholar] [CrossRef]
- Welsh, J.A.; Karpen, S.; Vos, M.B. Increasing prevalence of nonalcoholic fatty liver disease among United States adolescents, 1988-1994 to 2007-2010. J Pediatr 2013, 162, 496–500 e491. [Google Scholar] [CrossRef]
- Mischel, A.K.; Liao, Z.; Cao, F.; Dunn, W.; Lo, J.C.; Newton, K.P.; Goyal, N.P.; Yu, E.L.; Schwimmer, J.B. Prevalence of Elevated ALT in Adolescents in the US 2011-2018. Journal of pediatric gastroenterology and nutrition 2023, 77, 103–109. [Google Scholar] [CrossRef]
- Anderson, E.L.; Howe, L.D.; Jones, H.E.; Higgins, J.P.; Lawlor, D.A.; Fraser, A. The Prevalence of Non-Alcoholic Fatty Liver Disease in Children and Adolescents: A Systematic Review and Meta-Analysis. PloS one 2015, 10, e0140908. [Google Scholar] [CrossRef]
- Awai, H.I.; Newton, K.P.; Sirlin, C.B.; Behling, C.; Schwimmer, J.B. Evidence and recommendations for imaging liver fat in children, based on systematic review. Clin Gastroenterol Hepatol 2014, 12, 765–773. [Google Scholar] [CrossRef]
- Ciardullo, S.; Monti, T.; Perseghin, G. Prevalence of Liver Steatosis and Fibrosis Detected by Transient Elastography in Adolescents in the 2017-2018 National Health and Nutrition Examination Survey. Clin Gastroenterol Hepatol 2021, 19, 384–390 e381. [Google Scholar] [CrossRef]
- Liu, J.; Mu, C.; Li, K.; Luo, H.; Liu, Y.; Li, Z. Estimating Global Prevalence of Metabolic Dysfunction-Associated Fatty Liver Disease in Overweight or Obese Children and Adolescents: Systematic Review and Meta-Analysis. International journal of public health 2021, 66, 1604371. [Google Scholar] [CrossRef]
- Fernandes, D.M.; Pantangi, V.; Azam, M.; Salomao, M.; Iuga, A.C.; Lefkowitch, J.H.; Gill, J.; Morotti, R.; Lavine, J.E.; Mencin, A.A. Pediatric Nonalcoholic Fatty Liver Disease in New York City: An Autopsy Study. J Pediatr 2018, 200, 174–180. [Google Scholar] [CrossRef]
- Montinaro, F.; Busby, G.B.; Pascali, V.L.; Myers, S.; Hellenthal, G.; Capelli, C. Unravelling the hidden ancestry of American admixed populations. Nat Commun 2015, 6, 6596. [Google Scholar] [CrossRef]
- Yanai, H.; Adachi, H.; Hakoshima, M.; Iida, S.; Katsuyama, H. Metabolic-Dysfunction-Associated Steatotic Liver Disease-Its Pathophysiology, Association with Atherosclerosis and Cardiovascular Disease, and Treatments. International journal of molecular sciences 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, B.; Sultana, R.; Greene, M.W. Adipose tissue and insulin resistance in obese. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie 2021, 137, 111315. [Google Scholar] [CrossRef]
- Ziolkowska, S.; Binienda, A.; Jablkowski, M.; Szemraj, J.; Czarny, P. The Interplay between Insulin Resistance, Inflammation, Oxidative Stress, Base Excision Repair and Metabolic Syndrome in Nonalcoholic Fatty Liver Disease. International journal of molecular sciences 2021, 22. [Google Scholar] [CrossRef]
- Longo, M.; Zatterale, F.; Naderi, J.; Parrillo, L.; Formisano, P.; Raciti, G.A.; Beguinot, F.; Miele, C. Adipose Tissue Dysfunction as Determinant of Obesity-Associated Metabolic Complications. International journal of molecular sciences 2019, 20, 2358. [Google Scholar] [CrossRef] [PubMed]
- Alves-Bezerra, M.; Cohen, D.E. Triglyceride Metabolism in the Liver. Comprehensive Physiology 2017, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gong, J.; Tu, W.; Liu, J.; Tian, D. Hepatocytes: A key role in liver inflammation. Front Immunol 2022, 13, 1083780. [Google Scholar] [CrossRef] [PubMed]
- Deprince, A.; Haas, J.T.; Staels, B. Dysregulated lipid metabolism links NAFLD to cardiovascular disease. Mol Metab 2020, 42, 101092. [Google Scholar] [CrossRef] [PubMed]
- Bhat, N.; Mani, A. Dysregulation of Lipid and Glucose Metabolism in Nonalcoholic Fatty Liver Disease. Nutrients 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Fotbolcu, H.; Zorlu, E. Nonalcoholic fatty liver disease as a multi-systemic disease. World journal of gastroenterology : WJG 2016, 22, 4079–4090. [Google Scholar] [CrossRef]
- Targher, G.; Byrne, C.D.; Tilg, H. MASLD: a systemic metabolic disorder with cardiovascular and malignant complications. Gut 2024, 73, 691–702. [Google Scholar] [CrossRef]
- Speiser, P.W.; Rudolf, M.C.; Anhalt, H.; Camacho-Hubner, C.; Chiarelli, F.; Eliakim, A.; Freemark, M.; Gruters, A.; Hershkovitz, E.; Iughetti, L.; et al. Childhood obesity. The Journal of clinical endocrinology and metabolism 2005, 90, 1871–1887. [Google Scholar] [CrossRef] [PubMed]
- Baldridge, A.D.; Perez-Atayde, A.R.; Graeme-Cook, F.; Higgins, L.; Lavine, J.E. Idiopathic steatohepatitis in childhood: a multicenter retrospective study. J Pediatr 1995, 127, 700–704. [Google Scholar] [CrossRef] [PubMed]
- Rashid, M.; Roberts, E.A. Nonalcoholic steatohepatitis in children. Journal of pediatric gastroenterology and nutrition 2000, 30, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Phatak, U.P.; Pashankar, D.S. Obesity and gastrointestinal disorders in children. Journal of pediatric gastroenterology and nutrition 2015, 60, 441–445. [Google Scholar] [CrossRef] [PubMed]
- Molleston, J.P.; Schwimmer, J.B.; Yates, K.P.; Murray, K.F.; Cummings, O.W.; Lavine, J.E.; Brunt, E.M.; Scheimann, A.O.; Unalp-Arida, A.; Network, N.C.R. Histological abnormalities in children with nonalcoholic fatty liver disease and normal or mildly elevated alanine aminotransferase levels. J Pediatr 2014, 164, 707–713 e703. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.S.; Barlow, S.E.; Quiros-Tejeira, R.E.; Scheimann, A.; Skelton, J.; Suskind, D.; Tsai, P.; Uko, V.; Warolin, J.P.; Xanthakos, S.A.; et al. Childhood obesity for pediatric gastroenterologists. Journal of pediatric gastroenterology and nutrition 2013, 56, 99–109. [Google Scholar] [CrossRef]
- Franzese, A.; Vajro, P.; Argenziano, A.; Puzziello, A.; Iannucci, M.P.; Saviano, M.C.; Brunetti, F.; Rubino, A. Liver involvement in obese children. Ultrasonography and liver enzyme levels at diagnosis and during follow-up in an Italian population. Dig Dis Sci 1997, 42, 1428–1432. [Google Scholar] [CrossRef]
- Tazawa, Y.; Noguchi, H.; Nishinomiya, F.; Takada, G. Serum alanine aminotransferase activity in obese children. Acta paediatrica 1997, 86, 238–241. [Google Scholar] [CrossRef]
- Vos, M.B.; Abrams, S.H.; Barlow, S.E.; Caprio, S.; Daniels, S.R.; Kohli, R.; Mouzaki, M.; Sathya, P.; Schwimmer, J.B.; Sundaram, S.S.; et al. NASPGHAN Clinical Practice Guideline for the Diagnosis and Treatment of Nonalcoholic Fatty Liver Disease in Children: Recommendations from the Expert Committee on NAFLD (ECON) and the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN). Journal of pediatric gastroenterology and nutrition 2017, 64, 319–334. [Google Scholar] [CrossRef] [PubMed]
- Schwimmer, J.B.; Newton, K.P.; Awai, H.I.; Choi, L.J.; Garcia, M.A.; Ellis, L.L.; Vanderwall, K.; Fontanesi, J. Paediatric gastroenterology evaluation of overweight and obese children referred from primary care for suspected non-alcoholic fatty liver disease. Alimentary pharmacology & therapeutics 2013, 38, 1267–1277. [Google Scholar] [CrossRef]
- Lavine, J.E.; Schwimmer, J.B.; Molleston, J.P.; Scheimann, A.O.; Murray, K.F.; Abrams, S.H.; Rosenthal, P.; Sanyal, A.J.; Robuck, P.R.; Brunt, E.M.; et al. Treatment of nonalcoholic fatty liver disease in children: TONIC trial design. Contemporary clinical trials 2010, 31, 62–70. [Google Scholar] [CrossRef]
- Colantonio, D.A.; Kyriakopoulou, L.; Chan, M.K.; Daly, C.H.; Brinc, D.; Venner, A.A.; Pasic, M.D.; Armbruster, D.; Adeli, K. Closing the gaps in pediatric laboratory reference intervals: a CALIPER database of 40 biochemical markers in a healthy and multiethnic population of children. Clin Chem 2012, 58, 854–868. [Google Scholar] [CrossRef] [PubMed]
- Shannon, A.; Alkhouri, N.; Carter-Kent, C.; Monti, L.; Devito, R.; Lopez, R.; Feldstein, A.E.; Nobili, V. Ultrasonographic quantitative estimation of hepatic steatosis in children With NAFLD. Journal of pediatric gastroenterology and nutrition 2011, 53, 190–195. [Google Scholar] [CrossRef]
- Bohte, A.E.; Koot, B.G.; van der Baan-Slootweg, O.H.; van Werven, J.R.; Bipat, S.; Nederveen, A.J.; Jansen, P.L.; Benninga, M.A.; Stoker, J. US cannot be used to predict the presence or severity of hepatic steatosis in severely obese adolescents. Radiology 2012, 262, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Draijer, L.G.; Feddouli, S.; Bohte, A.E.; Vd Baan Slootweg, O.; Pels Rijcken, T.H.; Benninga, M.A.; Stoker, J.; Koot, B.G.P. Comparison of diagnostic accuracy of screening tests ALT and ultrasound for pediatric non-alcoholic fatty liver disease. European journal of pediatrics 2019, 178, 863–870. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Noureddin, M.; Bernstein, D.; Kwo, P.; Russo, M.; Shiffman, M.L.; Younes, Z.; Abdelmalek, M. Role of Noninvasive Tests in Clinical Gastroenterology Practices to Identify Patients With Nonalcoholic Steatohepatitis at High Risk of Adverse Outcomes: Expert Panel Recommendations. The American journal of gastroenterology 2021, 116, 254–262. [Google Scholar] [CrossRef]
- Schwimmer, J.B.; Middleton, M.S.; Behling, C.; Newton, K.P.; Awai, H.I.; Paiz, M.N.; Lam, J.; Hooker, J.C.; Hamilton, G.; Fontanesi, J. Magnetic resonance imaging and liver histology as biomarkers of hepatic steatosis in children with nonalcoholic fatty liver disease. Hepatology 2015, 61, 1887–1895. [Google Scholar] [CrossRef] [PubMed]
- Vajro, P.; Lenta, S.; Socha, P.; Dhawan, A.; McKiernan, P.; Baumann, U.; Durmaz, O.; Lacaille, F.; McLin, V.; Nobili, V. Diagnosis of nonalcoholic fatty liver disease in children and adolescents: position paper of the ESPGHAN Hepatology Committee. Journal of pediatric gastroenterology and nutrition 2012, 54, 700–713. [Google Scholar] [CrossRef]
- Ezaizi, Y.; Kabbany, M.N.; Conjeevaram Selvakumar, P.K.; Sarmini, M.T.; Singh, A.; Lopez, R.; Nobili, V.; Alkhouri, N. Comparison between non-alcoholic fatty liver disease screening guidelines in children and adolescents. JHEP Rep 2019, 1, 259–264. [Google Scholar] [CrossRef]
- Schwimmer, J.B.; Dunn, W.; Norman, G.J.; Pardee, P.E.; Middleton, M.S.; Kerkar, N.; Sirlin, C.B. SAFETY study: alanine aminotransferase cutoff values are set too high for reliable detection of pediatric chronic liver disease. Gastroenterology 2010, 138, 1357–1364 1364 e1351–1352. [Google Scholar] [CrossRef] [PubMed]
- Bussler, S.; Vogel, M.; Pietzner, D.; Harms, K.; Buzek, T.; Penke, M.; Handel, N.; Korner, A.; Baumann, U.; Kiess, W.; et al. New pediatric percentiles of liver enzyme serum levels (alanine aminotransferase, aspartate aminotransferase, gamma-glutamyltransferase): Effects of age, sex, body mass index, and pubertal stage. Hepatology 2018, 68, 1319–1330. [Google Scholar] [CrossRef] [PubMed]
- Shaw, J.L.; Cohen, A.; Konforte, D.; Binesh-Marvasti, T.; Colantonio, D.A.; Adeli, K. Validity of establishing pediatric reference intervals based on hospital patient data: a comparison of the modified Hoffmann approach to CALIPER reference intervals obtained in healthy children. Clinical biochemistry 2014, 47, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Sundaram, S.S.; Sokol, R.J.; Capocelli, K.E.; Pan, Z.; Sullivan, J.S.; Robbins, K.; Halbower, A.C. Obstructive sleep apnea and hypoxemia are associated with advanced liver histology in pediatric nonalcoholic fatty liver disease. J Pediatr 2014, 164, 699–706 e691. [Google Scholar] [CrossRef] [PubMed]
- Rich, N.E.; Oji, S.; Mufti, A.R.; Browning, J.D.; Parikh, N.D.; Odewole, M.; Mayo, H.; Singal, A.G. Racial and Ethnic Disparities in Nonalcoholic Fatty Liver Disease Prevalence, Severity, and Outcomes in the United States: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol 2018, 16, 198–210 e192. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Gramlich, T.; Matteoni, C.A.; Boparai, N.; McCullough, A.J. Nonalcoholic fatty liver disease in patients with type 2 diabetes. Clin Gastroenterol Hepatol 2004, 2, 262–265. [Google Scholar] [CrossRef] [PubMed]
- Riekki, H.; Aitokari, L.; Kivela, L.; Lahti, S.; Hiltunen, P.; Vuorela, N.; Huhtala, H.; Lakka, T.A.; Kurppa, K. Prevalence and associated factors of metabolic-associated fatty liver disease in overweight Finnish children and adolescents. Front Endocrinol (Lausanne) 2023, 14, 1090344. [Google Scholar] [CrossRef]
- Kawamura, Y.; Arase, Y.; Ikeda, K.; Seko, Y.; Imai, N.; Hosaka, T.; Kobayashi, M.; Saitoh, S.; Sezaki, H.; Akuta, N.; et al. Large-scale long-term follow-up study of Japanese patients with non-alcoholic Fatty liver disease for the onset of hepatocellular carcinoma. The American journal of gastroenterology 2012, 107, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Pinhas-Hamiel, O.; Zeitler, P. Acute and chronic complications of type 2 diabetes mellitus in children and adolescents. Lancet 2007, 369, 1823–1831. [Google Scholar] [CrossRef] [PubMed]
- Di Bonito, P.; Licenziati, M.R.; Corica, D.; Wasniewska, M.G.; Di Sessa, A.; Del Giudice, E.M.; Morandi, A.; Maffeis, C.; Faienza, M.F.; Mozzillo, E.; et al. Phenotypes of prediabetes and metabolic risk in Caucasian youths with overweight or obesity. Journal of endocrinological investigation 2022, 45, 1719–1727. [Google Scholar] [CrossRef]
- Laffel, L.; Chang, N.; Grey, M.; Hale, D.; Higgins, L.; Hirst, K.; Izquierdo, R.; Larkin, M.; Macha, C.; Pham, T.; et al. Metformin monotherapy in youth with recent onset type 2 diabetes: experience from the prerandomization run-in phase of the TODAY study. Pediatric diabetes 2012, 13, 369–375. [Google Scholar] [CrossRef]
- Shah, A.S.; Zeitler, P.S.; Wong, J.; Pena, A.S.; Wicklow, B.; Arslanian, S.; Chang, N.; Fu, J.; Dabadghao, P.; Pinhas-Hamiel, O.; et al. ISPAD Clinical Practice Consensus Guidelines 2022: Type 2 diabetes in children and adolescents. Pediatric diabetes 2022, 23, 872–902. [Google Scholar] [CrossRef]
- Nobili, V.; Mantovani, A.; Cianfarani, S.; Alisi, A.; Mosca, A.; Sartorelli, M.R.; Maffeis, C.; Loomba, R.; Byrne, C.D.; Targher, G. Prevalence of prediabetes and diabetes in children and adolescents with biopsy-proven non-alcoholic fatty liver disease. Journal of hepatology 2019, 71, 802–810. [Google Scholar] [CrossRef]
- Newton, K.P.; Hou, J.; Crimmins, N.A.; Lavine, J.E.; Barlow, S.E.; Xanthakos, S.A.; Africa, J.; Behling, C.; Donithan, M.; Clark, J.M.; et al. Prevalence of Prediabetes and Type 2 Diabetes in Children With Nonalcoholic Fatty Liver Disease. JAMA Pediatr 2016, 170, e161971. [Google Scholar] [CrossRef]
- Bardugo, A.; Bendor, C.D.; Zucker, I.; Lutski, M.; Cukierman-Yaffe, T.; Derazne, E.; Mosenzon, O.; Tzur, D.; Beer, Z.; Pinhas-Hamiel, O.; et al. Adolescent Nonalcoholic Fatty Liver Disease and Type 2 Diabetes in Young Adulthood. The Journal of clinical endocrinology and metabolism 2021, 106, e34–e44. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; Paik, J.M.; Henry, A.; Van Dongen, C.; Henry, L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology 2023, 77, 1335–1347. [Google Scholar] [CrossRef] [PubMed]
- D'Adamo, E.; Cali, A.M.; Weiss, R.; Santoro, N.; Pierpont, B.; Northrup, V.; Caprio, S. Central role of fatty liver in the pathogenesis of insulin resistance in obese adolescents. Diabetes care 2010, 33, 1817–1822. [Google Scholar] [CrossRef]
- Cali, A.M.; De Oliveira, A.M.; Kim, H.; Chen, S.; Reyes-Mugica, M.; Escalera, S.; Dziura, J.; Taksali, S.E.; Kursawe, R.; Shaw, M.; et al. Glucose dysregulation and hepatic steatosis in obese adolescents: is there a link? Hepatology 2009, 49, 1896–1903. [Google Scholar] [CrossRef] [PubMed]
- En Li Cho, E.; Ang, C.Z.; Quek, J.; Fu, C.E.; Lim, L.K.E.; Heng, Z.E.Q.; Tan, D.J.H.; Lim, W.H.; Yong, J.N.; Zeng, R.; et al. Global prevalence of non-alcoholic fatty liver disease in type 2 diabetes mellitus: an updated systematic review and meta-analysis. Gut 2023, 72, 2138–2148. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. Journal of hepatology 2019, 71, 793–801. [Google Scholar] [CrossRef]
- Xanthakos, S.A.; Lavine, J.E.; Yates, K.P.; Schwimmer, J.B.; Molleston, J.P.; Rosenthal, P.; Murray, K.F.; Vos, M.B.; Jain, A.K.; Scheimann, A.O.; et al. Progression of Fatty Liver Disease in Children Receiving Standard of Care Lifestyle Advice. Gastroenterology 2020, 159, 1731–1751 e1710. [Google Scholar] [CrossRef] [PubMed]
- Safar Zadeh, E.; Lungu, A.O.; Cochran, E.K.; Brown, R.J.; Ghany, M.G.; Heller, T.; Kleiner, D.E.; Gorden, P. The liver diseases of lipodystrophy: the long-term effect of leptin treatment. Journal of hepatology 2013, 59, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Sridharan, K.; Sivaramakrishnan, G.; Sequeira, R.P.; Elamin, A. Pharmacological interventions for non-alcoholic fatty liver disease: a systematic review and network meta-analysis. Postgrad Med J 2018, 94, 556–565. [Google Scholar] [CrossRef]
- Mantovani, A.; Byrne, C.; Scorletti, E.; Mantzoros, C.S.; Targher, G. Efficacy and safety of anti-hyperglycaemic drugs in patients with non-alcoholic fatty liver disease with or without diabetes: An updated systematic review of randomized controlled trials. Diabetes & metabolism 2020, 46, 427–441. [Google Scholar]
- Nobili, V.; Manco, M.; Ciampalini, P.; Alisi, A.; Devito, R.; Bugianesi, E.; Marcellini, M.; Marchesini, G. Metformin use in children with nonalcoholic fatty liver disease: an open-label, 24-month, observational pilot study. Clinical therapeutics 2008, 30, 1168–1176. [Google Scholar] [CrossRef]
- Nobili, V.; Manco, M.; Devito, R.; Di Ciommo, V.; Comparcola, D.; Sartorelli, M.R.; Piemonte, F.; Marcellini, M.; Angulo, P. Lifestyle intervention and antioxidant therapy in children with nonalcoholic fatty liver disease: a randomized, controlled trial. Hepatology 2008, 48, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Katsagoni, C.N.; Georgoulis, M.; Papatheodoridis, G.V.; Panagiotakos, D.B.; Kontogianni, M.D. Effects of lifestyle interventions on clinical characteristics of patients with non-alcoholic fatty liver disease: A meta-analysis. Metabolism: clinical and experimental 2017, 68, 119–132. [Google Scholar] [CrossRef]
- Spahis, S.; Alvarez, F.; Ahmed, N.; Dubois, J.; Jalbout, R.; Paganelli, M.; Grzywacz, K.; Delvin, E.; Peretti, N.; Levy, E. Non-alcoholic fatty liver disease severity and metabolic complications in obese children: impact of omega-3 fatty acids. J Nutr Biochem 2018, 58, 28–36. [Google Scholar] [CrossRef]
- Nobili, V.; Alisi, A.; Della Corte, C.; Rise, P.; Galli, C.; Agostoni, C.; Bedogni, G. Docosahexaenoic acid for the treatment of fatty liver: randomised controlled trial in children. Nutrition, metabolism, and cardiovascular diseases : NMCD 2013, 23, 1066–1070. [Google Scholar] [CrossRef]
- Schwimmer, J.B.; Lavine, J.E.; Wilson, L.A.; Neuschwander-Tetri, B.A.; Xanthakos, S.A.; Kohli, R.; Barlow, S.E.; Vos, M.B.; Karpen, S.J.; Molleston, J.P.; et al. In Children With Nonalcoholic Fatty Liver Disease, Cysteamine Bitartrate Delayed Release Improves Liver Enzymes but Does Not Reduce Disease Activity Scores. Gastroenterology 2016, 151, 1141–1154 e1149. [Google Scholar] [CrossRef]
- Della Corte, C.; Carpino, G.; De Vito, R.; De Stefanis, C.; Alisi, A.; Cianfarani, S.; Overi, D.; Mosca, A.; Stronati, L.; Cucchiara, S.; et al. Docosahexanoic Acid Plus Vitamin D Treatment Improves Features of NAFLD in Children with Serum Vitamin D Deficiency: Results from a Single Centre Trial. PloS one 2016, 11, e0168216. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.; Liang, S.; Ma, J.; Xiao, Y. Effect of growth hormone therapy on liver enzyme and other cardiometabolic risk factors in boys with obesity and nonalcoholic fatty liver disease. BMC endocrine disorders 2022, 22, 49. [Google Scholar] [CrossRef] [PubMed]
- Mosca, A.; Crudele, A.; Smeriglio, A.; Braghini, M.R.; Panera, N.; Comparcola, D.; Alterio, A.; Sartorelli, M.R.; Tozzi, G.; Raponi, M.; et al. Antioxidant activity of Hydroxytyrosol and Vitamin E reduces systemic inflammation in children with paediatric NAFLD. Dig Liver Dis 2021, 53, 1154–1158. [Google Scholar] [CrossRef] [PubMed]
- El Amrousy, D.; Abdelhai, D.; Shawky, D. Vitamin D and nonalcoholic fatty liver disease in children: a randomized controlled clinical trial. European journal of pediatrics 2022, 181, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Vos, M.B.; Van Natta, M.L.; Blondet, N.M.; Dasarathy, S.; Fishbein, M.; Hertel, P.; Jain, A.K.; Karpen, S.J.; Lavine, J.E.; Mohammad, S.; et al. Randomized placebo-controlled trial of losartan for pediatric NAFLD. Hepatology 2022, 76, 429–444. [Google Scholar] [CrossRef]
- Saneian, H.; Khalilian, L.; Heidari-Beni, M.; Khademian, M.; Famouri, F.; Nasri, P.; Hassanzadeh, A.; Kelishadi, R. Effect of l-carnitine supplementation on children and adolescents with nonalcoholic fatty liver disease (NAFLD): a randomized, triple-blind, placebo-controlled clinical trial. J Pediatr Endocrinol Metab 2021, 34, 897–904. [Google Scholar] [CrossRef]
- Goyal, N.P.; Mencin, A.; Newton, K.P.; Durelle, J.; Carrier, C.; Ugalde-Nicalo, P.; Noel, B.; Mouton, J.; Vargas, D.; Magrez, D.; et al. An Open Label, Randomized, Multicenter Study of Elafibranor in Children With Nonalcoholic Steatohepatitis. Journal of pediatric gastroenterology and nutrition 2023, 77, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Ostadmohammadi, V.; Namazi, M.J.; Rezasoltani, M.; Kheirkhah, D.; Rajabi, M.; Sharif, A.; Taghavi Ardakani, A.; Raygan, F.; Assareh, A.A.; Sharif, M.R. Effects of Zinc Supplementation on Inflammatory Status and Nonalcoholic Steatohepatitis in Overweight or Obese Children: a Randomized Clinical Trial. Biological trace element research 2024, 202, 3496–3503. [Google Scholar] [CrossRef]
- Zahmatkesh, A.; Sohouli, M.H.; Shojaie, S.; Rohani, P. The effect of orlistat in the treatment of non-alcoholic fatty liver in adolescents with overweight and obese. European journal of pediatrics 2024, 183, 1173–1182. [Google Scholar] [CrossRef]

Table 1.
Phase II, III, and IV clinical trials for MASLD treatment in children.
| Phases | ClinicalTrials.gov | Start Date of Trial (Year Month-Day) | Drug | Molecular Mechanism (Target) | Patients | Main Findings | Adverse Effect | References |
|---|---|---|---|---|---|---|---|---|
| II | NCT02201160 | 2009-01-01 | n-3 PUFA | anti-inflammatory, insulin metabolism regulator | NAFLD young male | FLI, ALT, and ALT/AST ratio reduction, lipid profile, and carotid intima-media thickness improvement | No | [97] |
| I-II | NCT00885313 | 2009-03-01 | Docosahexanoic Acid | anti-inflammatory | NAFLD children | improvement in liver steatosis by US | No | [98] |
| II-III | NCT01529268 | 2012-06-01 | cysteamine bitartrate | activators of PPARα | children with NAFLD activity scores ≥ 4 | AST, ALT, and lobular inflammation reductions | No | [99] |
| III | NCT02098317 | 2014-01-01 | Docosahexanoic Acid + Vitamin D | anti-inflammatory, immunity regulation | children and adolescents biopsy-proven NAFLD | improvement in IR, lipid profile, ALT, and NAFLD activity score | No | [100] |
| II | ChiCTRIPR-17011267 | 2017-03-01 | rhGH | stimulation of growth, IGF-1 production | NAFLD and obese boys | reduction in liver enzymes, CRP, BMI, LDL-C. Increase in HDL-C | No | [101] |
| III | NCT02842567 | 2017-04-01 | hydroxytyrosol + VitE | antioxidant, anti-inflammatory | children and adolescents biopsy-proven NASH | increase IL-10 | No | [102] |
| III | PACTR201710002634203 | 2017-10-19 | Vit D | anti-inflammatory and insulin-sensitizing effects | children with biopsy-proven NAFLD | improvement in hepatic steatosis, liver enzymes, cholesterol | No | [103] |
| III | NCT03467217 | 2018-10-02 | Losartan | angiotensin II receptor blocker | histologic NAFLD adolescents NAFLD activity score ≥ 3, and (ALT) ≥ 50 U/l. | Reduction of ALT | No | [104] |
| II | IRCT20170628034786N2 | 2019-01-16 | l-carnitine | Transport of fatty acids into mitochondria | NAFLD children | No impact on liver enzymes | No | [105] |
| II | NCT04165343 | 2020-02-01 | Elafibranor | Dual PPARα/δ agonist | NASH Children | ALT reduction | No | [106] |
| III | IRCT20200531047614N1 | 2020-09-01 | elemental zinc | anti-inflammatory and antioxidant | NASH overweight or obese children and adolescents | ALT, CRP reduction, HDL-cholesterolincrease | No | [107] |
| II | IRCT20220409054467N2 | 2022-05-13 | Orlistat | inhibiting pancreatic lipase, reducing the absorption of dietary fats | NAFLD amd overweight/obese adolescents | improvement in liver enzymes, steatosis, glucose/lipid metabolism | greasy stools, sleep problems, weakness, headache | [108] |
Legend: ALT, Alanine Aminotransferase, AST, Aspartate Aminotransferase, BMI, Body Mass Index, CRP, C-Reactive Protein, DHA, Docosahexaenoic Acid, FLI, Fatty Liver Index, HDL, High-Density Lipoprotein, IGF-1, Insulin-like Growth Factor 1, IL-10; Interleukin 10, IR, insulin resistance; LDL, Low-Density Lipoprotein, NASH, Nonalcoholic Steatohepatitis, NAFLD, Nonalcoholic Fatty Liver Disease, PUFA, Polyunsaturated Fatty Acids, PPAR, Peroxisome Proliferator-Activated Receptor, rhGH, Recombinant Human Growth Hormone; US, Ultrasonography.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



