
Submitted:
15 August 2024
Posted:
16 August 2024
You are already at the latest version
Abstract
Regular exercise has been shown to have a positive effect on the health outcomes of individuals with Type-2 diabetes mellitus (T2DM), however, it is still underutilised in developing countries. This study investigated diabetes-related knowledge, attitudes, and practice toward exercise and its benefits among individuals with T2DM. A total of one hundred and ninety-nine participants (male= 21.6% and female= 78.4%) with T2DM, aged between 18- 75, 43.77 (SD ±14.78) years participated in the study. A validated diabetes-related knowledge, attitude, and practice questionnaire, evaluated by true/false or unsure was utilised in the study. Descriptive and inferential statistics analysis was used to analyze data with the significance set at p<0. The study results demonstrated significantly poor diabetes-related knowledge of exercise (p<0.001). The majority of the study participants 163 (81.90%) with T2DM did not know that physical activity and exercise are different. Regarding the attitude of the individuals with T2DM, 158 (70.40%) of the study participants felt that their regular work was an adequate substitution for exercise. More than 50% of the study participants demonstrated a positive practice towards exercise and its benefits towards T2DM (p<0.001). The study revealed that participants’ knowledge and attitudes were poor towards exercise and its benefits, but their practice was good.
Keywords:
knowledge
; attitude
; practice
; physical activity
; Type-2 diabetes mellitus
1. Introduction
Diabetes mellitus is a metabolic disorder caused by insulin deficiency, which results in chronic hyperglycemia [24]. It is the most common metabolic disease that can lead to damaging effects on metabolic processes [28]. Statistically, about 9.3% of people worldwide suffer from metabolic syndrome [24], and this number is estimated to increase from 463 million to 700 million by the year 2045. Type-2 diabetes mellitus (T2DM) is one of the most common types of diabetes mellitus and is defined as a metabolic disorder characterized by hyperglycemia resulting from defects in insulin secretion, action, or both [4,11]. According to Grundling et al. [11], an estimated 24 million people are living with T2DM in Africa, and this number is predicted to increase by 129% to 55 million by 2045. The report further provided that more than half (54%) of people living with T2DM are undiagnosed in sub-Saharan Africa. The impact of T2DM in African countries has reached alarming proportions, hence, Northern Africa (driven by Egypt) and Southern Africa (driven by South Africa) appeared to have the highest number of people living with T2DM than the global average [9].
South Africa has approximately 4.58 million people living with T2DM [12] and is regarded as the second leading country in Sub-Saharan Africa that has high incidents of death cases caused by T2DM [26]. According to Grundlingh [12], the number of T2DM cases in South Africa has almost tripled from 4.5% in 2010 to 12.7% in 2019. Provincially, KwaZulu-Natal has the highest number of T2DM cases compared to other provinces [7]. The District Health Information System (DHIS) data showed that the prevalence of T2DM in KwaZulu-Natal (KZN) is 12.5% which increases to 34.1% when combined with patients with private medical aid [7]. This figure is, however, considered an underestimate as T2DM is frequently undiagnosed in the country [7]. According to Dessie et al.; Phoosuwan et al. [9,25], T2DM mainly affects older adults and is primarily caused by unhealthy eating habits, obesity, and physical inactivity due to notable changes in the diet caused by urbanization and industrialization [24].
One of the crucial steps towards reducing the T2DM burden and improving health outcomes is promoting lifestyle changes (i.e., healthy eating habits, and exercise) [23,27], education, adherence to medication as well as adequate knowledge, attitude, and practice. Lifestyle modifications are considered the cornerstone of the management of T2DM. According to Chiwungwe [8], understanding the disease and following appropriate measures by exercising for 60 minutes 2-3 days per week, may result in keeping blood glucose within its required range [24]. Furthermore, exercise leads to weight loss which is the primary goal for an individual with T2DM. Weight loss is thus a key determinant of energy expenditure, and this is vital for energy balance and body weight control [19]. Additionally, consuming correctly classified sources of carbohydrates, fats, as well as proteins, may result in good health and weight control. A study by Bradshaw et al. [6], reported that eating habits play a major role in managing T2DM and when coupled with exercise they are the determinants of weight control [24]. It is therefore important for individuals with T2DM to be well informed of appropriate measures to be followed regarding T2DM as well as to receive proper guidance from healthcare workers about the benefits of exercise [27]. This can help increase their motivation and confidence to engage in regular exercise, ultimately leading to better glycemic control and overall health outcomes.
Type-2 diabetes mellitus is affected by numerous factors such as educational level, attitude towards the disease, and knowledge possessed by those who have to manage T2DM. Knowledge, defined as skills, information, and facts acquired through education or experience is a powerful tool in the fight against T2DM and maintaining normal blood glucose levels. Knowledge about bT2DM forms the basis for informed decisions about eating habits, exercise, weight control, blood glucose monitoring, and the use of medications [24,25]. Globally, knowledge related to understanding and management of T2DM is limited, despite how critical this disease may be [26]. Lack of sufficient diabetes knowledge frequently leads to poor self-care management skills and poor control of blood glucose, which consequently leads to poor compliance with both medication and lifestyle changes [23].
A study by Reid et al. [26] in the Free State province of South Africa, reported poor knowledge in individuals with T2DM in areas with high incidence of T2DM. The study reported limited information and managing intervention measures as the leading causes of the increased number of T2DM cases. People residing in rural areas often show poor diabetes-related knowledge because of their educational status which restricts them from being exposed and seeking important information. Researchers Moodley and Rambiritch; Reid et al. [17,26] added that individuals residing in rural are not well-educated and empowered to manage T2DM. Hence, poor awareness about T2DM observed might be due to the low level of education and the lack of organized diabetes education services in the diabetes clinic [16]. Traditionally, individuals from rural areas believe that being overweight or obese is indicative of health and a better socioeconomic state, however, this is untrue [15]. Obesity and overweight are associated with T2DM and heart disease [11]. Patient education is the cornerstone of care for patients with T2DM. Diabetes-related knowledge about exercise and its benefits is required to effectively manage T2DM. Sufficient diabetes knowledge enables people with T2DM to think positively and structure a mindset that enables a positive attitude toward behavioral change [5,8]
In this study, attitude is defined as an intention and ultimate practice related to T2DM as expressed by individuals with T2DM to internalize diabetes-related information and make good judgments about diabetes self-care and management [8]. Attitude plays a vital role in managing T2DM. A positive attitude displayed by individuals with T2DM may lead to a significant behavioral change towards T2DM. According to Belsti et al.; Chiwungwe [5,8], the attitude of an individual is largely influenced by numerous factors such as knowledge regarding the disease, family, educational status, residence, and how society defines a person with T2DM. Diabetes stigma can be a major challenge for individuals with T2DM by preventing individuals from seeking care and managing their health. Diabetes stigma may be due to the fear of being discriminated against and rejection [29]. Attitudes toward exercise among individuals with T2DM vary greatly [8]. Individuals with T2DM may perceive exercise as a burden or believe that their condition limits them from engaging in exercise [8]. Individuals with T2DM may fear injury from exercise or exacerbation of complications associated with T2DM and this can also contribute to negative attitudes towards exercise [8]. Alternatively, positive attitudes are evident among those who view exercise as an opportunity to improve their overall health and well-being [29]. Individual’s attitude toward T2DM is key in the adoption and maintenance of certain behaviors that are essential in treating and managing T2DM [8]. Having a positive attitude towards T2DM means being able to show a positive perception of health, and have a greater receptivity to treatment, favoring the reduction of stress associated with the disease as well as improvement of self-esteem and self-efficacy [29]. Knowledge, which is the central factor in managing T2DM, plays a vital role in an individual’s attitude towards T2DM.
Positive practice towards exercise and its benefits plays an equally important role in the management of T2DM through regular exercise. Maintaining consistent involvement in exercise requires overcoming common barriers such as lack of time, limited access to appropriate facilities or resources, social support deficiencies, and negative beliefs about personal abilities or the benefits of exercising [3,10]. Effective strategies for promoting active lifestyles among people with T2DM involve addressing these barriers by adopting tailored interventions based on individual needs and preferences. Therefore, the study aimed to determine an individual’s T2DM diabetes-related knowledge, attitude, and practice toward exercise and its benefits among individuals with T2DM.
2. Materials and Methods
2.1. Study Population, Sample Size and Sampling
This study used the descriptive cross-sectional design to collect data, where one hundred and ninety-nine participants (199) participated in the study. The study population was individuals with T2DM aged 18 years and above, attending church in KwaZulu-Natal-Durban, and community members from Chesterville. The participants were selected among the population based on the inclusion criteria, i.e., males or females diagnosed with T2DM, aged between 18- and above, and literate. Participants diagnosed with non-communicable diseases other than diabetes such as heart disease, individuals with mental limitations, and diagnosed with Type-1 diabetes mellitus were excluded from the study.
2.2. Procedure
The validated adapted South African Diabetes-related Knowledge, Attitude, and Practice questionnaire was used in the study. The questionnaire was designed based on a pre-validated and reliable questionnaire by Le Roux; Niroomand et al. [14,20] to collect data relevant to knowledge, attitude, and practice in individuals with T2DM about exercise and its benefits. The questionnaire consisted of KAP closed-ended structured questions about exercise and its benefits, evaluated by either true/false/unsure. The questionnaire was categorized into various sections: section A consisted of information on the socio-demographic distribution of variables of participants such as age, sex, and ethnic group. Section B covered 10 items on knowledge of T2DM towards exercise and its benefits, assessed with correct and incorrect responses. Knowledge was scored by summing the scores of all questions of the domain. The scores were then converted to percentages, and knowledge was determined by the number of selected correct/incorrect responses. A higher score of more than 50% was considered poor knowledge if more incorrect items were selected or good knowledge if more than 50% of correct knowledge items were selected. Section C covered 10 attitude questions on T2DM towards exercise and its benefits and Section D covered 10 practice questions on T2DM towards exercise and its benefits. Attitude and practice were assessed using a three-point scale, that is true, false, and unsure. Some items were reverse-coded because of their negative meanings of the items. A higher score of more than 50% was considered as either poor or good attitude/practice, depending on the question asked. A pilot study was conducted with 10 participants with T2DM, to test the effectiveness and validation of the questionnaire. The first author and a trained research assistant were responsible for collecting data to ensure uniformity.
2.3. Ethical Considerations
Ethical approval was obtained from the University of KwaZulu-Natal (UKZN) Biomedical Research Ethics Committee (BREC/000033892/2021) and permission to conduct the study was obtained from the church. Written informed consents were obtained from participants before enrolling in the study.
2.4. Data Analysis
The collected data was computed on an Excel spreadsheet and analyzed using SPSS version 23.3.1. Descriptive statistics such as percentages for categorical data, frequencies, means, and standard deviations (SD) were calculated and used to summarise the demographic profiles of the study participants. The results are presented in tables and graphs, and the association between variables was determined using appropriate statistical interpretations. The chi-square test was used to determine the association between knowledge and age. When conditions are not met Fisher’s exact test was used. Hence, the probability value(p-value) of less than 0.05 was accepted as statistically significant.
3. Results
3.1. Demographic Characteristics of the Participants
The demographic characteristics of the study participants are presented in Figure 1. A total of 199 individuals with T2DM met the inclusion criteria and were invited to partake in the study. The mean age of the study participants was 58.65 (SD± 12.04) years and more than half of the study participants aged between 60-69 (48.80 ± 16.64) participated in the study, with under 30, 57.50 (SD± 17.53), and 30-39, 42.50 (SD±13.89) being the lowest. 78.4%% were female and 21.6% were male participants. The majority of the study participants were black African (95.5%), followed by white participants (3.0%) and the Colored population made up only 1.5% of the study participants.
Table 1. showed that a significant 163(82%) of people with T2DM did not know that physical activity and exercise are different, (p<.001) followed by a significant 150(75%) that indicated that a person with T2DM cannot do strenuous exercise like weightlifting, cycling, and running, (p<.001). More than 50% of individuals with T2DM indicated 134(67%) that herbs make a person with T2DM healthier than if they use western medication, (p<.001). The majority 139(70%) believed that a person with T2DM using any type of medication can be cured of the disease, (p<.001) and a significant of 142(71%) did not know that diabetes medication may cause swelling of the feet, (p<.001).
The results (see Table 2 above) showed that a significant 158(79.4%) of people with T2DM felt that their regular work is an adequate substitution to exercise, (p<.001); followed by a significant 128(64.3%) of the study participants which indicated that they need someone to keep prompting them to do exercises, (p<.001). The majority 139(69.8%) indicated that they use mild pain or fatigue as an excuse to keep them away from exercising, (p<.001). Among 199 of the study participants, 125(68.3%) indicated that they do not look forward to doing exercises, (p<.001); with 137(68.8%) indicating that they felt that age is an influencing factor in motivating them to do exercises, (p<.001).
The overall results (Table 3 below) showed a significant positive practice towards exercise and its benefits among individuals with T2DM. The results in Table 3 showed that a significant 157(78.9%) participated in activities that make them sweat as they exercise, (p<.001); with a significant 141(70.9%) of the study participants which indicated that they found out how they can adjust their lifestyle to living with T2DM (p<.001). 124(62.3%) of the study participants check their blood pressure monthly, (p<.001); and 136(68.3%) keep asking therapists as to how they can perfectly learn exercises, (p<.001). 131(65.8%) of the study participants indicated that they ask their doctors if there are any medicines available, which will make them better, without doing exercise, (p<.001).
4. Discussion
The main finding of the study was that people with T2DM have a significantly unsatisfactory diabetes-related knowledge of exercise and its benefits. The study results showed a significant lack of knowledge among individuals with T2DM towards exercise and its benefits and this concurred with the results of Mwimo et al. [19] in Tanzanians, which reported minimal knowledge about exercise in managing T2DM. The inability of individuals to manage T2DM effectively contributes to the high rate of physical inactivity in the country. Studies have shown that individuals with T2DM often lack knowledge about their condition, leading to inadequate self-management practices, poor glycemic control, and an increased risk of complications. Lack of knowledge means poor adherence to medication and exercise and unawareness of the benefits of exercise in managing T2DM.
A study by Alaofe et al.; Okolie et al. [1,22] also reported poor knowledge among individuals with T2DM. Lack of knowledge may place these individuals at risk of doing things that may predispose them to complications. More than half (67%) of the study’s participants reported the use of herbs to cure T2DM and this concurred with the study Okolie et al. [22], which reported the use of herbs as a cure for T2DM, however, this may interfere with orthodox treatment. A study by Mukeshimana and Nkosi [18] on Rwandans added that most people especially the black population still believe that T2DM can be only treated using traditional medicine. The researchers argued that Rwandans believed that a person with TDM-related symptoms is bewitched, hence, consulting traditional healers and usage of traditional medicine were the best options for curing the disease. According to Odili et al. [21], a lack of knowledge about T2DM is associated with an increased rate of hospitalization. Similar findings were reported by Mohammadi et al. [16], in Ethiopia, where only 34% of T2DM patients demonstrated adequate knowledge about the importance of exercise for managing their condition.
The study also revealed that age had a significant association with knowledge of T2DM. The results showed that more than hundreds of participants from the age range of 60-69 years indicated to have a significant knowledge of 42.80 (SD±15.64) compared to other categories. This is mainly due to experience and increased information seeking. Older adults are more likely to seek out information about T2DM compared to young adults [2]. The study findings concurred with the results by Aljofan [2], which reported that older age groups are associated with high diabetes knowledge. With all the myths, disbelief, and lack of knowledge about T2DM, it is thus evidence that people still lack knowledge about exercise and its benefits. Knowledge about T2DM plays a significant role in enhancing the ability to cope and adjust to the disease. Therefore, individuals with T2DM must show greater understanding and knowledge about the disease.
Additionally, due to poor knowledge displayed by the study participants, the study results also demonstrated negative attitudes towards exercise and its benefits in individuals with T2DM. The results of the study concur with the study by Imam and Dharepgol [13] which found that 80% of individuals with T2DM had a negative attitude towards exercise practice. A study by Alaofe et al. [1] indicated a relatively negative attitude in individuals with T2DM. Individuals with T2DM reported that stigma contributed to their negative attitudes and impacted their psychological well-being. Moreover, factors such as not adhering to a healthier lifestyle and taking medication are contributing factors to negative attitudes. Similar findings have been described in an Ethiopian study undertaken in patients older than 50 years of age with T2DM [1]. There are numerous misconceptions displayed by participants with T2DM towards exercise and its benefits. More than 79.4% of the study participants indicated that their work can be used as a substitute for exercise and this is consistent with the findings of Sookan et al. [27], which indicated that participants viewed daily activity as similar to physical exercise, which is untrue. The majority of the study participants showed negative attitudes towards exercise because they believed it was not beneficial or were concerned about potential harm. Furthermore, only 29% practiced regular structured exercises as per international recommendations. These results indicate that there is a significant gap between knowledge and practice regarding the role of exercise in T2DM management.
Despite the higher level of poor knowledge and negative attitude towards exercise and its benefits among individuals with T2DM reported in this study, participants demonstrated good practice towards exercise and its benefits. The study participants showed good practices towards preventative measures against T2DM and this is consistent with the results Almousa et al. [3], which indicated the highest behavior displayed by Saudi Arabians was the commitment to take medication according to the doctor’s instructions This includes checking blood sugar every month (62.3%), seeking out information on how to live with T2DM (70.9%), and checking for feet injuries regularly (65.3%). The findings of the study are consistent with the results of the study by Reid et al. [26], which reported that patients with T2DM regularly take their medication.
5. Conclusions
The study revealed that participants’ knowledge and attitudes were poor towards exercise and its benefits, but their practice was good Alarmingly, the majority of the study participants still believed in traditional medicine in managing and preventing T2DM. These wrongful beliefs can too directly influence the T2DM management in our society. As the number of individuals diagnosed with T2DM continues to grow, it becomes increasingly important to understand and address the factors contributing to the effective management and prevention of complications associated with this condition.
Funding
This research received no external funding.
References
- Alaofè, H., Hounkpatin, W. A., Djrolo, F., Ehiri, J., & Rosales, C. (2021). Knowledge, attitude, practice and associated factors among patients with type 2 diabetes in Cotonou, Southern Benin. BMC Public Health, 21, 1-11. [CrossRef]
- Aljofan, M., Altebainawi, A., & Alrashidi, M. N. (2019). Public knowledge, attitude and practice toward diabetes mellitus in Hail region, Saudi Arabia. International Journal of General Medicine, 255-262. [CrossRef]
- Almousa, A. Y., Hakami, O. A., Qutob, R. A., Alghamdi, A. H., Alaryni, A. A., Alammari, Y. M., & Amlih, M. F. (2023). Knowledge, attitude, and practice toward diabetes mellitus and their association with socioeconomic status among patients with type 2 diabetes mellitus in Saudi Arabia. Cureus, 15(5).
- Amiriparsa, T., Attarzadeh Hosseini, S. R., Bijeh, N., & Nia, M. R. H. (2018). The Study of the Effect of a 16-Week Program of Resistance-Aerobic Training on BDNF, Hba1c, Pain, and Michigan Neuropathy Score Among Type 2 Diabetic Patients with Peripheral Neuropathy. Journal of Diabetes and Metabolism, 2(124),9.
- Belsti, Y., Akalu, Y., & Animut, Y. (2020). Attitude, practice and its associated factors towards Diabetes complications among type 2 diabetic patients at Addis Zemen District hospital, Northwest Ethiopia. BMC Public Health, 20, 1-11. [CrossRef]
- Bradshaw, D., Norman, R., Pieterse, D., & Levitt, N. S. (2007). Estimating the burden of disease attributable to diabetes South Africa in 2000. South African Medical Journal, 97(8), 700-706.
- Chetty, L., Govender, N., Govender, G. M., & Reddy, P. (2021). Demographic stratification of Type 2 diabetes and comorbidities in district healthcare in KwaZulu-Natal. South African Family Practice, 63(2). [CrossRef]
- Chiwungwe, F. (2017). Diabetes-related knowledge, attitudes and practices [KAP] of adult patients with type 2 diabetes in Maseru, Lesotho.
- Dessie, G., Mulugeta, H., Amare, D., Negesse, A., Wagnew, F., Getaneh, T., & Lebu, S. (2020). A systematic analysis on prevalence and sub-regional distribution of undiagnosed diabetes mellitus among adults in African countries. Journal of Diabetes & Metabolic Disorders, 19, 1931-1941. [CrossRef]
- Egede, L. E., & Ellis, C. (2010). The effects of depression on metabolic control and quality of life in indigent patients with type 2 diabetes. Diabetes technology & therapeutics, 12(4), 257-262. [CrossRef]
- ElSayed, N. A., Aleppo, G., Aroda, V. R., Bannuru, R. R., Brown, F. M., Bruemmer, D., & American Diabetes Association. (2023). 2. Classification and diagnosis of diabetes: standards of care in diabetes—2023. Diabetes care, 46(Supplement_1), S19-S40. [CrossRef]
- Grundlingh, N., Zewotir, T. T., Roberts, D. J., & Manda, S. (2022). Assessment of prevalence and risk factors of diabetes and pre-diabetes in South Africa. Journal of Health, Population and Nutrition, 41(1), 7. [CrossRef]
- Imam, A., & Dharepgol, P. (2023). Exploring knowledge, attitudes, and practices regarding diabetes mellitus among the general population: a cross-sectional investigation. Student’s Journal of Health Research Africa, 4(12), 7-7.
- Le Roux, M. (2016). Diabetes-related knowledge, attitude and practices (KAP) of adult patients with type 2 diabetes in the Free State, South Africa (Doctoral dissertation, University of the Free State).
- Manafe, M., Chelule, P. K., & Madiba, S. (2022). The perception of overweight and obesity among South African adults: Implications for intervention strategies. International Journal of Environmental Research and Public Health, 19(19), 12335. [CrossRef]
- Mohammadi, S., Karim, N. A., Talib, R. A., & Amani, R. (2015). Knowledge, attitude and practices on diabetes among type 2 diabetic patients in Iran: a cross-sectional study. Science, 3(4), 520-4. [CrossRef]
- Moodley, L. M., & Rambiritch, V. (2007). An assessment of the level of knowledge about diabetes mellitus among diabetic patients in a primary healthcare setting. South African Family Practice, 49(10), 16-16d. [CrossRef]
- Mukeshimana, M. M., & Nkosi, Z. Z. (2014). Communities’ knowledge and perceptions of type two diabetes mellitus in Rwanda: a questionnaire survey. Journal of Clinical Nursing, 23(3-4), 541-549. [CrossRef]
- Mwimo, J. L., Somoka, S., Leyaro, B. J., Amour, C., Mao, E., & Mboya, I. B. (2021). Knowledge, attitude, and practice of physical activity among patients with diabetes in Kilimanjaro region, Northern Tanzania: a descriptive cross-sectional. study. BMJ open, 11(9): 046841. [CrossRef]
- Niroomand, M., Ghasemi, S. N., Karimi-Sari, H., Kazempour-Ardebili, S., Amiri, P., & Khosravi, M. H. (2016). Diabetes knowledge, attitude and practice (KAP) study among Iranian in-patients with type-2 diabetes: a cross-sectional study. Diabetes & Metabolic Syndrome: Clinical Research & Reviews, 10(1), S114-S119. [CrossRef]
- Odili, V. U., Isiboge, P. D., & Eregie, A. (2011). Patients’ knowledge of diabetes mellitus in a Nigerian city. Tropical Journal of Pharmaceutical Research, 10(5), 637-642.
- Okolie, V. U., Ehiemere, O. I., Iheanacho, N. P., & Kalu-Igwe, I. N. (2009). Knowledge of diabetes management and control by diabetic patients at Federal Medical Center Umuahia Abia State, Nigeria. International Journal of Medicine and Medical sciences, 1(9), 353-358.
- Owolabi, E. O., Goon, D. T., Ajayi, A. I., & Adeniyi, O. V. (2022). Knowledge of diabetes and associated factors in rural Eastern Cape, South Africa: A cross-sectional study. Plos one, 17(7), e0269811. [CrossRef]
- Peter, P. I., Steinberg, W. J., van Rooyen, C., & Botes, J. (2022). Type 2 diabetes mellitus patients’ knowledge, attitude and practice of lifestyle modifications. Health SA Gesondheid (Online), 27, 1-7. [CrossRef]
- Phoosuwan, N., Ongarj, P., & Hjelm, K. (2022). Knowledge on diabetes and its related factors among the people with type 2 diabetes in Thailand: a cross-sectional study. BMC Public Health, 22(1), 2365. [CrossRef]
- Reid, M., Roux, M. L., Raubenheimer, J., & Walsh, C. (2019). Diabetes-related knowledge, attitude and practices (KAP) of adult patients with type 2 diabetes mellitus in the Free State province, South Africa. South African Journal of Clinical Nutrition, 32(4), 20-27. [CrossRef]
- Sookan, T., Vaizie, A., Pillay, T., Moodley, S., Naidoo, S., & Naidoo, K. (2022). Exploring the role of the biokinetics in diabetes self-management: a survey of patients’ knowledge, attitudes and perceptions about exercise. Journal of Endocrinology, Metabolism and Diabetes of South Africa, 27(2), 70-74.
- World Health Organization (WHO).2019). Classification of diabetes mellitus, World Health Organization, Geneva, viewed 20 June 2020, from https://www.who.int/publications/i/item/classification-of-diabetes-mellitus.
- Zhao, R., Zhang, X., Wang, S., Zhao, N., Li, D., & Fan, H. (2023). Factors affecting T2DM patients’ behaviors associated with integrated treatment and prevention services in China. International Journal for Equity in Health, 22(1), 223. [CrossRef]
Figure 1.
Distributions of socio-demographic characteristics of individuals with T2DM (n=199).
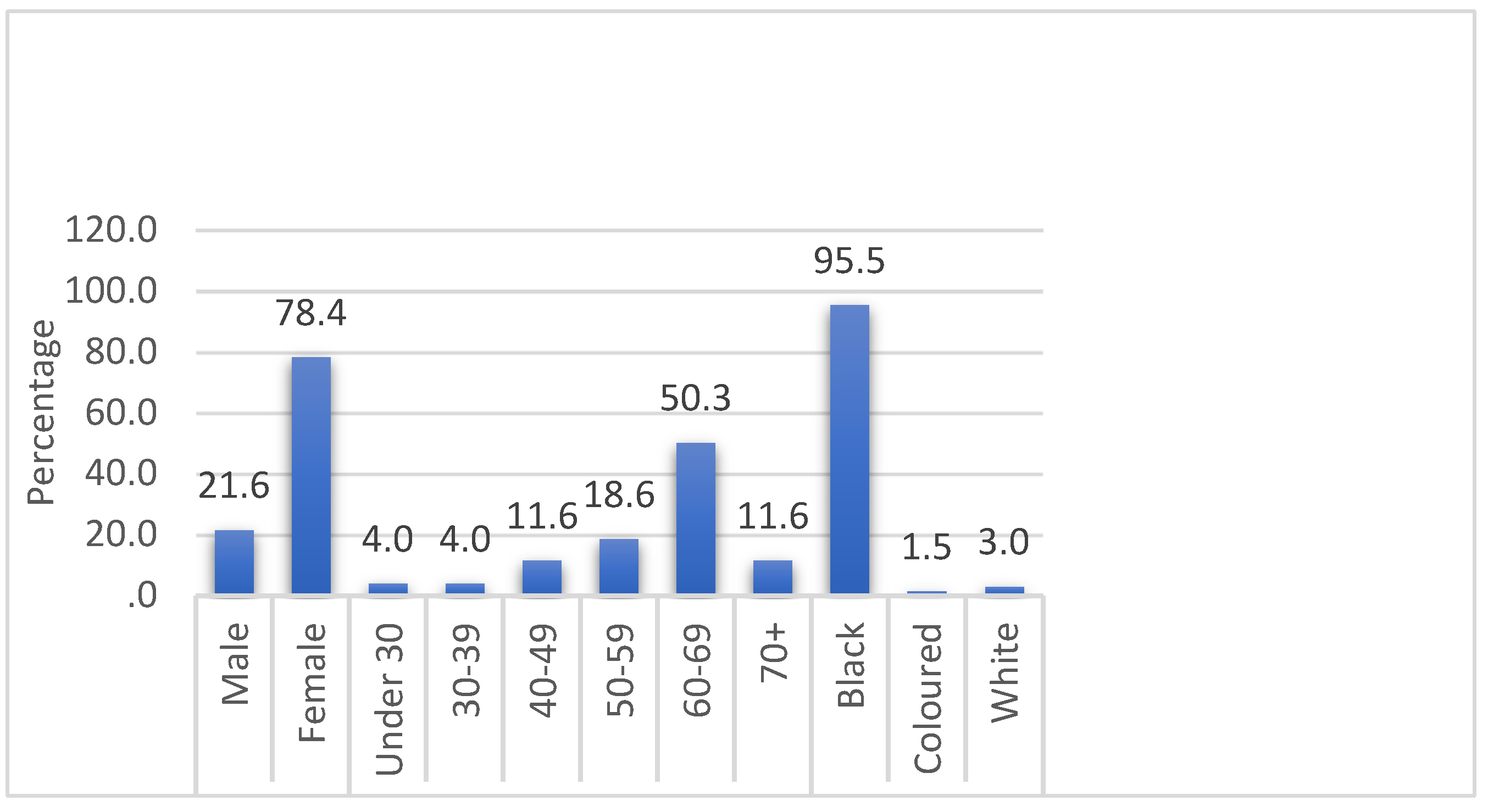

Table 1.
Participant’s diabetes-related knowledge (n=199).
| Item | Frequencies (%) | |
|---|---|---|
| Correct | Incorrect | |
| Physical activity & exercise are the same thing? | 36 (18) | 163 (82) |
| People with T2DM can safely perform exercise? | 140 (70) | 59 (30) |
| Exercise can be used in the management/treatment of T2DM. | 138(69) | 61(31) |
| A person with T2DM cannot do strenuous exercise like weightlifting, cycling, or running. | 49(25) | 150(75) |
| I am willing to engage in exercise to improve my health. | 131(66) | 68(34) |
| Type-2 diabetes mellitus management should include both exercise & a healthy diet. | 134(67) | 65(33) |
| A person with T2DM will often have high blood pressure. | 61(31) | 138(69) |
| A person with T2DM using herbs makes that person healthier than if they use Western medication. | 65(33) | 134(67) |
| A person with T2DM using any type of medication be cured of the disease? | 60(30) | 139(70) |
| Type-2 diabetes mellitus medication may cause swelling of the feet. | 57(29) | 142(71) |
Table 2.
Participants’ diabetes-related attitude (n=199).
| Item | Responses as frequency (%) | ||
|---|---|---|---|
| True | False | Unsure | |
| I feel that my regular work is an adequate substitute for exercise. | 158 (79.4) | 37 (18.6) | 4 (2.0) |
| I need someone to keep prompting me to do my exercises | 128 (64.3) | 58 (29.1) | 12 (6.0) |
| I use mild pain or fatigue as an excuse to keep away from my exercises. | 139 (69.8) | 55 (27.6) | 5 (2.5) |
| I will continue my exercises until I improve, regardless of how long it takes | 49 (24.6) | 145 (73,9) | 5 (2.5) |
| I believe I will improve with exercises as I have seen others improving | 59(29.6) | 129(68.4) | 11 (5.5) |
| I look forward to doing my exercises each day | 60 (30.2) | 125 (63.8) | 14 (7.0) |
| I feel that age is an influencing factor in motivating me to do my exercises | 137 (68.8) | 57 (28.6) | 5 (2.5) |
| I feel embarrassed doing exercise in front of others | 128 (69.3) | 63 (31.7) | 8 (4.0) |
| I feel that I have no time of my own and my daily exercises take away my valuable time | 130 (65.3) | 63 (31.7) | 6 (3.0) |
| I give up on exercises owing to the difficulty in sticking to a schedule | 128 (64.3) | 65 (37.7) | 6 (3.0) |
*Denotes significant results.
Table 3.
Participants’ diabetes-related practice of T2DM (n=199).
| Item | Responses as frequency (%) | ||
|---|---|---|---|
| True | False | Unsure | |
| I do activities that make me sweat as I exercise | 157 (78.9) | 38 (19.1) | 4 (2.0) |
| I find out how I can still adjust my lifestyle to living with T2DM | 141 (70.9) | 46 (23.1) | 12 (6.0) |
| I check my blood pressure monthly | 124 (62.3) | 58 (29.1) | 17(8.5) |
| I check my feet for injuries regularly | 130 (65.3) | 57 (28.6) | 12 (6.0) |
| I find it difficult to lose weight if I become overweight | 133 (66.8) | 57 (28.6) | 9(4.5) |
| I feel that my therapist is making tall claims when he explains to me the benefits of the exercise program | 136 (68.3) | 53 (26.6) | 10 (5.0) |
| I thought of asking my doctor, if there are any medicines available, which will make me better, without doing exercise | 131 (65.8) | 58 (29.1) | 10 (5.0) |
| I keep asking my therapist how perfectly I have learned the exercises or how better I could do it | 133 (66.8) | 55 (27.6) | 11 (5.5) |
| I am prompt in doing my exercises regularly as it keeps me alert and energetic throughout the day | 139 (69.8) | 55 (27.6) | 5 (2.5) |
*Denotes significant results.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



