
Submitted:
19 August 2024
Posted:
19 August 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
This study examines the association of sociodemographic risk factors and the comorbidities of COVID-19. Most COVID-19-related studies were conducted in inpatient settings among patients with severe infection during the first and second waves of the pandemic. The third wave with less severe Omicron variant presented a unique opportunity to observe the adult patients treated in outpatient settings. We conducted a cross-sectional study (117 patients aged > 40 years presented with symptomatic COVID-19). We employed the Charlson Comorbidity Index (CCI) to compute comorbidity burden, Medical Outcomes Survey Short form (SF-12) to measure general health, and Self-care Self- Efficacy Scale (SCSES) to assess self-care ability. Fisher’s exact test and analysis of variance (ANOVA) were used to compute the relationship between comorbidities and demographics. This study report focuses on the distribution of the comorbidities and its relationship to demographic variables. The top five comorbidities were hypertension (42%), diabetes (31%), pulmonary disease/asthma (19%), depression (14%), and cancer (11%). Depression was significantly higher among younger age groups (p<0.01) and women (p<0.05). Age (p<0.0001) and income (p<0.01) were the most significantly associated demographics with the comorbidity burden. Incidence of pulmonary disease showed a positive association to educational status (p=0.05). This was the first study to report a significant prevalence of depression among adults with symptomatic COVID-19.
Keywords:
COVID-19 positive adults
; Charlson Comorbidity Index
; Comorbidity burden and COVID-19
; Depression and COVID-19
; Comorbidities and COVID-19
; Social determinants of COVID-19
1. Introduction
The coronavirus disease 2019 (COVID-19) pandemic disproportionately affected the older adult population and inflicted significantly higher mortality among the older adult population with comorbidities. Pre-existing comorbidities heightened the older adult's vulnerability to COVID-19 infection and its complications. During the first two waves of COVID-19 infection, research documented cardiometabolic comorbidities such as diabetes mellitus, obesity, cardiovascular disease, and hypertension as the significant comorbidities contributing to greater fatalities among older adults with COVID-19. However, those studies were conducted in the inpatient settings because outpatient treatments were unavailable during that period [1,2]. The landscape of total comorbidity burden did not come to the forefront as a significant threat to the prognosis of a vulnerable adult fighting a COVID-19 infection and receiving treatment in an outpatient setting. With the emergence of multiple COVID-19 treatment modalities that can be provided in an outpatient setting, the paradigm for COVID-19 disease management is shifting to more outpatient care than hospitalization today. It is essential to understand the prevalent comorbidities to estimate the risk of poor prognosis among community-dwelling older adults with multiple comorbid conditions being treated in an outpatient setting [3]. Pre-existing comorbidities increase the risk of contracting the virus, lead to critical illness (i.e., admission to intensive care unit or death), and complicate recovery [4].
We conducted a cross-sectional study to assess the Influence of Comorbidities, General Health Status, and Self-Care Self-Efficacy on COVID-19 Symptoms severity among adults over 40 years of age during Omicron Wave [5]. The objective of the study was 1) to assess the prevalence of common comorbidities among adults with symptomatic COVID-19 disease and 2) to assess the impact of self-care, self-efficacy, and general well-being and the comorbidity burden on COVID-19 symptoms among adults treated in an outpatient clinic. This paper is describing the comorbidity burden and its relationship to sociodemographic factors among adults with symptomatic COVID-19 in an outpatient setting.
The Charlson Comorbidity Index (CCI) is reliable in predicting the impact of comorbidities in recovery from COVID-19 in the general population. Strong research evidence through rigorous studies conducted in multiple countries established that COVID-19 patients with pre-existing comorbidities were more likely to die, especially those with advanced age. This simple tool can be applied in the outpatient setting and the results obtained could help healthcare providers identify the most susceptible COVID-19 patients by comorbidities and age to assess their risk for mortality and morbidity and significantly reduce the number of fatalities from COVID-19 in an outpatient setting [4,6,7].
Multiple meta-analyses revealed that advanced age, comorbidities, and abnormal inflammatory biomarkers predicted poor outcomes. Cardiometabolic comorbidities contribute to higher mortality among patients with COVID-19 disease. Hypertension, diabetes, cardiovascular diseases, and chronic kidney disease were risk factors for patients with severe COVID-19 infection [1,2,8,9,10]. However, the list of comorbidities assessed was constructed based on clinical observations rather than structured instruments like the CCI, which can compute the compounding effect of multiple comorbidities in a person. Additionally, employing clinical observations alone might result in a possible bias towards physical health and exclusion of mental health in the list of relevant comorbidities.
Furthermore, most studies were conducted in inpatient settings among patients admitted with severe infection during the first and second waves of the coronavirus pandemic with most virulent alpha and delta strains of the COVID-19 virus. However, the third wave of COVID-19 infection, with predominantly less severe Omicron virus and its later variants, presented a unique opportunity to observe the elderly patients treated in the outpatient setting and to develop evidence-based risk assessment and risk-specific protocols to support the recovery of COVID-19 patients within the community cost-effectively. Along with pre-existing comorbidities, the lack of self-care self-efficacy, poor general health, and inadequate social support can be possible social determinants of mortality from COVID-19 disease. Still, these factors have not been systematically assessed using standardized instruments in a population with COVID-19 disease.
This study explored the impact of relevant risk factors such as comorbidities, general health status, and self-care practices on COVID-19 burden among at-risk adults who contracted COVID-19.
2. Materials and Methods
We employed a cross-sectional study to assess the role of selected sociodemographic and cardiometabolic risk factors in the burden of COVID-19 disease with a sample of 120 patients presenting for COVID-19 treatment at the "REGEN-COV" monoclonal antibody treatment centers. We recruited cognitively intact and hemodynamically stable COVID-19-positive adults aged 40 years and above who are not taking any other COVID-19 treatment for this study. Potential participants who met the eligibility criteria were screened with the Short Portable Mental Status Questionnaire (SPMSQ) to screen for cognitive impairment. Once the potential participant cleared the screening process, we collected self-reported data using standardized questionnaires presented in a preordered sequence. The questionnaire was available in English and Spanish and was completed by the participants in an electronic format using an iPad. Responses were scored and saved on the Research Electronic Data Capture (REDCap, Fort Lauderdale, US) software database. These factors include comorbidities, self-care self-efficacy, and available social support that can impact a person's ability to self-care to recover from COVID-19 illness.
We used the Charlson Comorbidity Index (CCI) to capture the weight of pre-existing comorbidities, the RAND Medical Outcomes Study Short-Form (SF-12) to assess general physical and mental health, the Self-Care Self-Efficacy Scale (SCSES) to measure the confidence of the participant in self-care, and the Social Support Survey (SSS) to gauge the available social support [11,12,13,14,15]. The CCI assigns differential weights to different comorbidities that reduce a patient's chance of survival. This instrument has been validated in diverse patient populations, including patients with COVID-19, and the reliability coefficient varies between 0.5 to 0.86 for predicting mortality based on comorbidities. The SF-12 taps eight health concepts: physical functioning, bodily pain, role limitations due to physical health problems, role limitations due to personal or emotional problems, emotional well-being, social functioning, energy/fatigue, and general health perceptions. It also includes a single item that indicates the perceived change in health. The reliability coefficient of SF-12 has been consistently above 0.7, demonstrating good reliability. The SCSES was newly validated as a self-report measure for self-care self-efficacy among adults with chronic illness (mean age ranging from 65-77 years) and found high reliability with Cronbach's alpha coefficients ranging from 0.89- 0.93. The SSS is a brief, self-administered instrument developed for patients in the Medical Outcomes Study, a two-year study of patients with chronic conditions and is reliable (all alphas > 0.91) and stable. The COVID-19 Symptom Severity Scale (COVID-SRS) was developed in this study for patients to rate their symptoms. This paper describes the incidence of comorbidities as measured by Charlson comorbidity index and its relationship to the sociodemographic factors of the study sample.
Data collection and storage were done using RedCap survey software. Data analysis was done using SAS software. A priori sample size calculation in the ANOVA model using four predictors with the alpha at 0.05 and medium effect size (f=.35), the sample size required was 94 to gain the power of 0.80. Providing for approximately 20% dropout after screening and incomplete data, we recruited 120 participants for this study. One hundred and seventeen participants completed the survey instruments to determine the role of selected sociodemographic risk factors in COVID-19 disease. After testing for the normal distribution and adjusting for missing data, we used nonparametric Fisher's exact test for categorical data in computing the relationship between the top five comorbidities and the major demographic variables queried in this study. Furthermore, we used Analysis of Variance (ANOVA) to quantify the compounding weight of comorbidities to estimate the relationship between the CCI score and the demographic variables
3. Results
The top five comorbidities among the population studied are shown in Table 1. The cardiometabolic disease spectrum was the most prevalent comorbidity among the COVID-19-positive adults presented for the COVID-19 antibody infusion therapy, including hypertension (42%) and diabetes without organ damage (31%). Other top comorbidities include pulmonary disease (19%), depression (14%), and cancer (solid tumor – 11%).
The distribution of the most prevalent five comorbidities across selected demographics (Table 2) showed a better picture of the pattern of comorbidities among at-risk adults who presented to receive COVID-19 infusion therapy. The prevalence of depression was higher among younger age groups (p=0.0019), with more women reporting depression than men (p=0.0183). Pulmonary disease/asthma prevalence was higher among those of higher educational levels (master/doctorate – p=0.0371). It is also notable that the prevalence of pulmonary diseases was reported by 50% of Asians, 24% of Hispanics and lesser in other races (p=0.0757). The prevalence of solid tumor cancers showed an insignificant increase with age (p>0.05). It is important to consider that many adults may suffer from multiple comorbidities, and the cumulative impact of comorbidities on an individual might be significantly different than the effect of a single comorbidity considered alone.
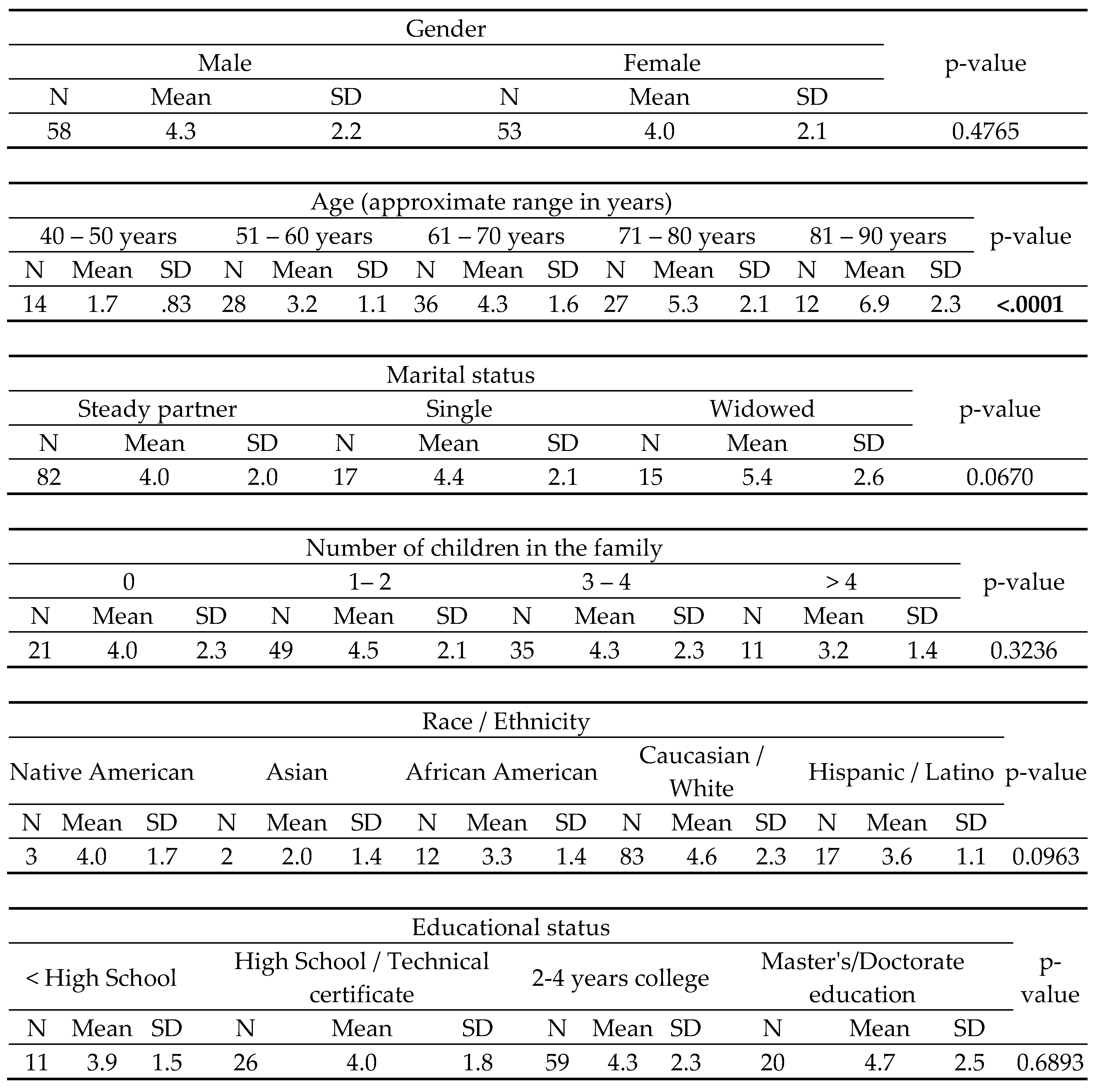
We used the CCI to measure the cumulative impact of comorbidities among selected demographics to the CCI (Table 3). Older age had the highest comorbidity burden in at-risk individuals who contracted COVID-19 and required COVID-19 antibody infusion therapy (p<0.0001), with their CCI almost doubling from age 51-60 years (mean 3.2 SD 1.1) to age 81-90 years range (mean 6.9 SD 2.3). Combined family income had the second highest comorbidity burden, especially among those with an income <$40,000 (mean 6.4 SD 3.6 - p<0.0089).
Considering race and ethnicity, the majority of the sample were Caucasians, and they had a higher comorbidity burden (mean 4.6 SD 2.3) compared to Native Americans (mean 4.0 SD 1.7), Hispanics (mean 3.6 SD 1.1) and African Americans (mean 3.3 SD 1.4), yet this difference did not mount to statistical significance (p=0.0963). Gender and education were not associated with the comorbidity burden in this analysis.
4. Discussion
This study explored the prevalence of selected comorbidities and the cumulative comorbidity burden among at-risk adults who contracted COVID-19 using Charlson Comorbidity Index. Recent studies found that higher CCI score can predict COVID+ pt with worse mental and physical health. But cannot predict control group for physical health. The research literature is scarce in assessing the comorbidity burden among COVID-19-positive older adults who received care in outpatient settings; hence, this study was initiated. It was conducted during the third wave of COVID-19, in which the OMICRON virus was the predominant strain. Though this strain was not as virulent as the previous COVID-19 variants, at-risk older adults with comorbidities were still vulnerable to complications. They were receiving COVID-19 antibody infusions as an emergent therapy. During this time, most people were vaccinated with at least two doses of COVID-19, resulting in milder upper respiratory symptoms and making it possible to treat at-risk individuals in outpatient settings.
Diabetes, hypertension, pulmonary diseases, solid tumor cancers, and depression were the top five most prevalent comorbidities among COVID-19-positive older adults who received COVID-19 infusion in outpatient settings. It is documented that cardiometabolic risk factors such as diabetes, hypertension, cardiovascular diseases, and obesity ranked high among the list of comorbidities, leading to increased mortality within the first two waves of COVID-19 disease [16,17]. Consequently, it leads to prioritizing the lifesaving antibody treatment for older adults with cardiometabolic risk factors. Hypertension was not associated with higher mortality, but it often coexisted with diabetes, leading to increased comorbidity burden and higher mortality. Multiple studies also pointed out pulmonary disease was associated with higher mortality among COVID-19 patients [18,19].
Depression was one of the top five comorbidities, significantly associated with younger age and the female gender in this study. This was the first study to note a significant prevalence of depression among older adults with COVID-19 who presented for treatment. We also found that depression was more common among the lower spectrum of age group, alluding to the fact that depression is a burgeoning health problem with aging vulnerable populations who need to be specially cared for during future pandemics. In the United States (US), depression has a prevalence that ranges from 5% to 10%, usually, with numbers as high as 33.7% being reported during the pandemic. Findings show that the prevalence of depression in the U.S. increased over threefold during the pandemic compared to before it [20]. Also in this study, mental health status showed a stronger association with most COVID-19 symptoms than physical health status [5]. This finding needs to be further explored in future studies to understand the full impact of depression on dealing with COVID-19 among older adults. It should be noted that pulmonary disease was reported more by Asians and people of higher educational levels in this study, and the reasons for this finding are unclear and inconclusive due to the small sample size.
The aging population often has to deal with multiple chronic illnesses, and the cumulative impact of these illnesses is often greater than a single disease condition. We used the Charlson comorbidity index to explore the cumulative burden of the comorbidities (among COVID-19-positive at-risk adults. It can compute the compounding effect of multiple comorbidities in a person). Each comorbidity category has an associated weight (from 1 to 6), based on the adjusted risk of mortality or resource use, and the sum of all the weights results in a single comorbidity score for a patient. A score of zero indicates that no comorbidities were found. The higher the score, the more likely the predicted outcome will result in mortality or higher resource use. The data from this study showed that higher age and lower income levels significantly compounded the comorbidity burden among COVID-19-positive at-risk adults. This finding concurs with previous study findings that older age and lower socioeconomic status make a person vulnerable to COVID-19 disease and its complications [21,22,23]. Comorbidity burden when measured exhaustively explains better than chronological age the increased risk of critical illness observed in patients hospitalized with COVID-19 [24]. This again attests to the need for targeted interventions to protect vulnerable populations during future COVID-19 and similar pandemics.
Self-care management in an outpatient setting is the cornerstone of managing comorbid conditions, and this becomes especially challenging amid a pandemic due to the constrained medical resources available at the clinics. A person's self-care seif efficacy is a major determinant in the odds of survival during a pandemic It is an important finding because the interventions aimed at boosting self-care self-efficacy concomitantly affect the mental health during a pandemic. These findings give insight into the inner struggles of vulnerable adult patients trying to maintain a stable health status at the expense of mental health and well-being. Again, targeted mental health support interventions are crucial to ensure positive health outcomes among vulnerable adults with comorbidities who are fighting a COVID-19 infection.
5. Conclusions
This study identified comorbidities in patients at risk for worsening COVID-19 disease in the outpatient settings. Our results inform the healthcare team to prioritize treatment of these individuals. Our data highlights comorbidities, self-care self-efficacy, and mental health as factors influencing health outcomes among adults with COVID-19 infection.
Author Contributions
Conceptualization, MMJ; methodology, HN, MMJ and BM.; software (REDCap), MMJ, BM and HN.; validation, MMJ and JF; formal analysis, HN, MMJ and JF; writing—original draft preparation, MMJ and JF; writing—review and editing, HSS, HS, JF, BM, HN, JT and PS ; project administration, MMJ. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (IRB) of the University of Texas Medical Branch (UTMB) (protocol code 21-0259 and date of approval was October 21, 2021).
Informed Consent Statement
Patient consent was waived due to the use of deidentified secondary data.
Data Availability Statement
The datasets analyzed during the current study are available from the primary author on reasonable request at mmjose@utmb.edu.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Fathi M, Vakili K, Sayehmiri F, Mohamadkhani A, Hajiesmaeili M, Rezaei-Tavirani M and Eilami O. The prognostic value of comorbidity for the severity of COVID-19: A systematic review and meta-analysis study. PLoS One. 2021;16:e0246190. [CrossRef]
- Figliozzi S, Masci PG, Ahmadi N, Tondi L, Koutli E, Aimo A, Stamatelopoulos K, Dimopoulos MA, Caforio ALP and Georgiopoulos G. Predictors of adverse prognosis in COVID-19: A systematic review and meta-analysis. Eur J Clin Invest. 2020;50:e13362. [CrossRef]
- Bentivegna M, Hulme C and Ebell MH. Primary Care Relevant Risk Factors for Adverse Outcomes in Patients With COVID-19 Infection: A Systematic Review. J Am Board Fam Med. 2021;34:S113-s126. [CrossRef]
- Khan MMA, Khan MN, Mustagir MG, Rana J, Islam MS and Kabir MI. Effects of underlying morbidities on the occurrence of deaths in COVID-19 patients: A systematic review and meta-analysis. J Glob Health. 2020;10:020503. [CrossRef]
- Jose MM, Feng J, Nguyen HT, Juneau C, Manakatt BM, Barnett J, Jones JL and Raji M. The Influence of Comorbidities, General Health Status, and Self-Care Self-Efficacy on COVID-19 Symptoms During the Omicron Wave. Curēus (Palo Alto, CA). 2023;15:e49176-e49176. [CrossRef]
- Martín-Martín J, Martín-Cazorla F, Suárez J, Rubio L and Martín-de-Las-Heras S. Comorbidities and autopsy findings of COVID-19 deaths and their association with time to death: a systematic review and meta-analysis. Curr Med Res Opin. 2022;38:785-792. [CrossRef]
- Preliminary Estimates of the Prevalence of Selected Underlying Health Conditions Among Patients with Coronavirus Disease 2019 - United States, February 12-March 28, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:382-386.
- Costa FF, Rosário WR, Ribeiro Farias AC, de Souza RG, Duarte Gondim RS and Barroso WA. Metabolic syndrome and COVID-19: An update on the associated comorbidities and proposed therapies. Diabetes Metab Syndr. 2020;14:809-814. [CrossRef]
- Gao F, Zheng KI, Wang XB, Sun QF, Pan KH, Wang TY, Chen YP, Targher G, Byrne CD, George J and Zheng MH. Obesity Is a Risk Factor for Greater COVID-19 Severity. Diabetes Care. 2020;43:e72-e74. [CrossRef]
- Gupta R, Hussain A and Misra A. Diabetes and COVID-19: evidence, current status and unanswered research questions. Eur J Clin Nutr. 2020;74:864-870. [CrossRef]
- Lu J, Yu Z, Zhang X, Wu M, Lin S, Zhu Y, Xu Z, You L, Wei F, Tang M, Jin M, Wang J and Chen K. Association between social health status and health-related quality of life among community-dwelling elderly in Zhejiang. Health Qual Life Outcomes. 2020;18:110. [CrossRef]
- Salomon RE, Crandell J, Muscatell KA, Santos HP, Jr., Anderson RA and Beeber LS. Two Methods for Calculating Symptom Cluster Scores. Nurs Res. 2020;69:133-141. [CrossRef]
- Twardzik E, Clarke P, Elliott MR, Haley WE, Judd S and Colabianchi N. Neighborhood Socioeconomic Status and Trajectories of Physical Health-Related Quality of Life Among Stroke Survivors. Stroke. 2019;50:3191-3197. [CrossRef]
- Ladha KS, Zhao K, Quraishi SA, Kurth T, Eikermann M, Kaafarani HM, Klein EN, Seethala R and Lee J. The Deyo-Charlson and Elixhauser-van Walraven Comorbidity Indices as predictors of mortality in critically ill patients. BMJ Open. 2015;5:e008990. [CrossRef]
- Riegel B, Barbaranelli C, Sethares KA, Daus M, Moser DK, Miller JL, Haedtke CA, Feinberg JL, Lee S, Stromberg A and Jaarsma T. Development and initial testing of the self-care of chronic illness inventory. J Adv Nurs. 2018;74:2465-2476. [CrossRef]
- Thakur B, Dubey P, Benitez J, Torres JP, Reddy S, Shokar N, Aung K, Mukherjee D and Dwivedi AK. A systematic review and meta-analysis of geographic differences in comorbidities and associated severity and mortality among individuals with COVID-19. Sci Rep. 2021;11:8562. [CrossRef]
- Zhang YJ, Sun XF, Xie B, Feng WJ and Han SL. Exploration of severe Covid-19 associated risk factor in China: Meta-analysis of current evidence. Int J Clin Pract. 2021;75:e14900.
- Lee SC, Son KJ, Han CH, Jung JY and Park SC. Impact of comorbid asthma on severity of coronavirus disease (COVID-19). Sci Rep. 2020;10:21805. [CrossRef]
- Rabbani G, Shariful Islam SM, Rahman MA, Amin N, Marzan B, Robin RC and Alif SM. Pre-existing COPD is associated with an increased risk of mortality and severity in COVID-19: a rapid systematic review and meta-analysis. Expert Rev Respir Med. 2021;15:705-716. [CrossRef]
- Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM and Galea S. Prevalence of Depression Symptoms in US Adults Before and During the COVID-19 Pandemic. JAMA Netw Open. 2020;3:e2019686. [CrossRef]
- Rahman MM, Bhattacharjee B, Farhana Z, Hamiduzzaman M, Chowdhury MAB, Hossain MS, Siddiqee MH, Islam MZ, Raheem E and Uddin MJ. Age-related risk factors and severity of SARS-CoV-2 infection: a systematic review and meta-analysis. J Prev Med Hyg. 2021;62:E329-e371. [CrossRef]
- Saragih ID, Advani S, Saragih IS, Suarilah I, Susanto I and Lin CJ. Frailty as a mortality predictor in older adults with COVID-19: A systematic review and meta-analysis of cohort studies. Geriatr Nurs. 2021;42:983-992. [CrossRef]
- Clark A, Jit M, Warren-Gash C, Guthrie B, Wang HHX, Mercer SW, Sanderson C, McKee M, Troeger C, Ong KL, Checchi F, Perel P, Joseph S, Gibbs HP, Banerjee A and Eggo RM. Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: a modelling study. Lancet Glob Health. 2020;8:e1003-e1017. [CrossRef]
- Valero-Bover D, Monterde D, Carot-Sans G, Cainzos-Achirica M, Comin-Colet J, Vela E, Cleries M, Folguera J, Abilleira S, Arrufat M, Lejardi Y, Solans O, Dedeu T, Coca M, Perez-Sust P, Pontes C and Piera-Jimenez J. Is Age the Most Important Risk Factor in COVID-19 Patients? The Relevance of Comorbidity Burden: A Retrospective Analysis of 10,551 Hospitalizations. Clin Epidemiol. 2023;15:811-825. [CrossRef]

Table 1.
Descriptive Statistics of the Studied Population.
| Comorbidity | Percentage |
|---|---|
| Hypertension | 42% |
| Diabetes | 31% |
| Pulmonary disease/ asthma | 18% |
| Depression | 14% |
| Cancer (solid tumor) | 11% |
| Myocardial infarction | 8% |
| Congestive heart failure | 8% |
| Renal disease | 6% |
| Peripheral vascular disease or bypass | 6% |
| Rheumatic or connective tissue disease | 5% |
| Mild liver disease | 4% |
| Cerebrovascular disease or transient ischemic disease | 3% |
| Lymphoma | 2% |
| Diabetes with end-organ damage | 1% |
| Severe liver disease | 1% |
| Gastric or peptic ulcer | 1% |
Table 2.
Demographics of the Top 5 Comorbidities.
| Demographics | Diabetes | Hypertension | Pulmonary disease / Asthma |
Depression | Cancer (solid tumor) |
|
|---|---|---|---|---|---|---|
| Age (approximate range in years) | 40-50 | 14% | 50% | 43% | 21% | 7% |
| 51-60 | 25% | 46% | 18% | 29% | 7% | |
| 61-70 | 44% | 33% | 14% | 11% | 6% | |
| 71-80 | 26% | 48% | 0% | 19% | 19% | |
| 81-90 | 33% | 33% | 0% | 17% | 25% | |
| p-value | 0.2212 | 0.6458 | 0.5176 | 0.0019 | 0.225 | |
| Gender | Male | 29% | 40% | 7% | 17% | 12% |
| Female | 32% | 43% | 23% | 19% | 9% | |
| p-value | 0.7522 | 0.6894 | 0.8238 | 0.0183 | 0.6552 | |
| Race and Ethnicity | Native American | 33% | 0% | 0% | 0% | 0% |
| Asian | 0% | 0% | 50% | 0% | 50% | |
| African American | 25% | 67% | 8% | 8% | 0% | |
| Caucasian | 34% | 42% | 12% | 25% | 12% | |
| Hispanic | 24% | 35% | 24% | 0% | 12% | |
| p-value | 0.8958 | 0.1572 | 0.0757 | 0.3045 | 0.3269 | |
| Education | < High School | 27% | 45% | 18% | 0% | 18% |
| High School /Technical |
23% | 42% | 12% | 8% | 4% | |
| College | 34% | 39% | 12% | 22% | 10% | |
| Master's/Doctorate | 35% | 45% | 20% | 35% | 20% | |
| p-value | 0.7494 | 0.9538 | 0.0371 | 0.7349 | 0.2462 | |
| Combined Family Income | < $25,000 | 17% | 42% | 17% | 8% | 0% |
| $25001-$40,000 | 45% | 73% | 27% | 18% | 27% | |
| $40,001-$50,000 | 44% | 44% | 22% | 0% | 0% | |
| $50,001-$75,000 | 25% | 19% | 25% | 25% | 13% | |
| $75,001-$100,000 | 30% | 43% | 4% | 13% | 13% | |
| >$100,000 | 24% | 44% | 12% | 21% | 15% | |
| p-value | 0.5542 | 0.1649 | 0.6423 | 0.2815 | 0.4278 | |
Table 3.
The Charlson Comorbidity Index (CCI) of Selected Demographics.
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



