
Submitted:
17 August 2024
Posted:
19 August 2024
You are already at the latest version
Abstract
Minimum Inhibitory Concentration (MIC) measures the lowest concentration of antibiotic that inhibits in-vitro growth of microorganisms. Canine pyometra is a frequently occurring reproductive disorder where reliable antibiotics along with surgical excision of uterus predicts better prognosis. Scarce literature is available to facilitate proper antibiotic selection to avoid septicemia in clinical cases. The present study was conducted to determine sensitivity and potency of selected antibacterials based on MIC values against bacterial isolates obtained from Canine Pyometra in Kathmandu district, Nepal by Agar Dilution method. Isolates obtained from 63 intra-uterine samples after ovariohysterectomy were Enterococcus spp (n=41), Klebsiella spp. (n=7), Staphylococcus spp. (n=11) and Streptococcus spp. (n=4). Enrofloxacin and Amikacin were found highly sensitive (0% resistance) with a null hypothesis of resistance to all bacterial isolates and were significantly more potent than other antibacterials tested (p<0.05; Kruskal-Wallis test) based on lower MIC ranks. Similarly, ceftriaxone was found to be least potent and was highly resistant to Enterococcus spp. (75.61%) and completely resistant to other bacterial species tested (100%). Comparative results on sensitivity and potency in the study revealed Enrofloxacin and Amikacin to be better antibacterial of choice in pyometra innervation in in-vitro setting. Further clinical trials considering other equally important variables along with MIC should be conducted to predict actual clinical efficacy of antibacterials during therapeutic management of canine pyometra in Nepal.
Keywords:
Minimum Inhibitory Concentration (MIC)
; Canine Pyometra
; Antibiotic Sensitivity
; Potency
; Susceptibility
; Bacterial Isolates
; Agar Dilution Method
; Antimicrobial Resistance (AMR)
1. Introduction
Antibiotics have been documented to be used for medical purposes since 1500 BC; however, the development of salvasran to treat syphilis in 1910 has been considered the hallmark of antibiotic usage for chemotherapeutic purposes [1]. The selection of the most effective antibiotic regimen in a specific clinical case depends on various factors such as availability, cost, dosage, adverse effects, patient susceptibility, etc, however, the most critical considerations are good tissue penetration and low Minimum Inhibitory Concentration (MIC) values [2]. The MIC is the lowest concentration of a chemical that inhibits observable growth of a microorganism after incubating the media for 16-20 hours (longer for anaerobes) [3]. This concentration is typically determined through a complex process involving a series of antibiotic dilutions in agar or culture media, where microorganisms are inoculated, and their growth is assessed [4]. Previous studies have indicated that MIC, when analyzed in conjunction with Pharmacokinetic/Pharmacodynamic (PK/PD) parameters, is of paramount importance for clinicians and veterinarians in optimizing targeted antibiotic therapy [5,6].
Canine pyometra, also known as cystic endometrial hyperplasia complex, is a common reproductive issue that affects approximately 23% of intact middle-aged female dogs [7]. Studies show that in female dogs with pyometra, the major clinical findings include bacteremia, endotoxemia, and systemic inflammation, which can affect organs such as the heart, liver, kidneys, and bone marrow, sometimes leading to unexpected deaths in affected animals [8,9]. Escherichia coli is the most prevalent organism in canine pyometra, but Staphylococcus spp., Streptococcus spp., Pseudomonas spp., Proteus spp. can also be found [10,11,12,13].
The conventional treatment protocol for Canine pyometra, as outlined by ref. [14], typically involves ovariohysterectomy, administration of PGF2α, and broad-spectrum antibiotics. Ovariohysterectomy is widely acknowledged as the most effective treatment for pyometra, as emphasized by [15,16,17]. The use of antibiotics alongside surgical intervention is a matter of debate. Some experts advocate for the use of antibiotics in all cases of canine pyometra [18,19], while others recommend antibiotics only for dogs that are clinically unstable and at risk of developing septicemia [20,21]. However, there has been a growing consideration for alternative medical treatments with minimal side effects, such as the repeated administration of aglepristone with or without additional low doses of prostaglandins, as discussed by [22]. Amoxicillin, Ampicillin and Enrofloxacin are the most commonly used antibiotics during pre-surgical and post-surgical management of canine pyometra [23], however, some study insist that these antibiotics are highly resistance to bacteria isolated from canine pyometra [12].
Early recognition, diagnosis, and the implementation of an appropriate treatment plan are essential to avoid fatal consequences due to pyometra [24]. Therefore, identifying the causative agent through antibiogram testing and determining the effective antibacterial dosage prior to initiating treatment are considered more rational approaches in managing pyometra. This strategy also aids in the detection and prevention of potential drug resistance in common canine pathogens [12]. Given the frequent playful interactions between humans and their pets, the rising antibiotic resistance of commonly used human antibiotics against canine pathogens poses a significant and concerning threat to human health [25].
Several studies indicate that integrating MIC values with pharmacokinetic parameters such as Half-life (T1/2), Maximum Clearance (Cmax), and Area Under Curve (AUC) enhances targeted antibacterial therapy, with their effects on clinical efficacy well-documented [26]. The goal of determining MIC is to provide a more precise quantification of resistance, allowing for adjustments in antimicrobial concentrations to achieve effective serum or tissue levels based on pharmacokinetic or pharmacodynamic data [27]. Interpretive cut-points for MIC, set by the Clinical and Laboratory Standards Institute (CLSI) and the European Committee on Antimicrobial Susceptibility Testing (EUCAST), are primarily based on human data, and veterinary-specific criteria for interpreting MIC values for most antibacterials are limited and difficult to find [28]. Thus far, no published literature has been found on the Minimum Inhibitory Concentration (MIC) of antibacterials against bacterial isolates of Canine Pyometra in Nepal, with only a limited amount available globally.
According to ref.[29,30], the reliance on empirical therapy, irrational antibiotic use, poor drug selection, and inappropriate antibiotic dosing are leading causes of treatment failure and the emergence of resistant bacteria in many developing countries, including Nepal. Given this issue, our study aims to identify bacteria causing canine pyometra and determine the effective concentration and the most potent antibacterials against prevalent bacterial isolates based on MIC observations. Additionally, this study will also compare MIC of antibacterials for bacterial isolates with standard clinical breakpoints.
2. Materials and Methods
2.1. Study Period
The study took place between April 1, 2022, and April 30, 2023, and was organized into three main phases: collecting samples, conducting laboratory work, and interpreting and analyzing the data.
2.2. Study Design and Sampling
A cross-sectional study was carried out in five veterinary hospitals, clinics, and animal shelters in the Kathmandu Valley, selected at random. The sampling method was purposive, with a minimum of 10 samples collected from each location. Clinical cases of canine pyometra were diagnosed based on physical examination, blood tests, and radiographic evaluation, followed by referral for surgical ovariohysterectomy (OVH) under general anesthesia. A total of 81 intrauterine swabs were aseptically collected post-OVH from pyometra cases, following the method outlined by ref.[11]. The swabs were stored at room temperature before being transported to the laboratory for primary culture. Laboratory work was conducted at the Veterinary Diagnostic and Research Laboratory (VDRL), Tripureshwor. From these samples, individual bacterial colonies were isolated, resulting in the collection of 63 different bacterial species for the study.
2.3. Primary Culture, Isolation and Identification
Collected samples were transported to VDRL, Tripureshwor. Primary culture of samples were inoculated in nutrient agar and incubating at 37oC for 24 hrs. The primary colonies thus obtained were then subjected to secondary culture in Orientation Agar (®ChromAGAR of Hi-Media with 100% sensitivity and 98% specificity) using streak-plate method to obtain individual colonies as described by [31] for isolation and identification of bacterial species, which was further confirmed by the MALDITOF (Vitek®MS, Biomerieux, France).The final pure bacterial colonies were further stored at 0-4oC until MIC determination study.
2.4. Determination of MIC
Agar dilution method was used as guided by [32], which is in reference to the protocol developed by EUCAST. The procedure implemented in the study is as described below:
2.4.1. Selection of Agar
Mueller-Hinton Agar that meets Clinical and Laboratory Standards Institute’s standards [33] was selected as the reference medium.
2.4.2. Preparation of Stock Solution
Stock solutions for the panels of selected antibiotics to be tested were prepared following a standard method. The amount of antibacterial agent in the stock solution was calculated using the formula as adopted my [34]
where by, concentration of the solution was 10240 mg/L.
Thus prepared stock solution was stored in -20oC until further use.
2.4.3. Preparation of Working Solutions
Working solutions were prepared according to the guidelines specified in [35] using a two-fold serial dilution starting from 1 mg/L, as shown in (Table 1) below. To each solution, 19 ml of agar was added to complete the two-fold serial dilution. The prepared dilutions were then arranged in the corresponding wells of a microtiter plate.
2.4.4. Preparation of Bacterial Inoculum
Bacterial colonies’ suspension with concentration of 5 x 105 CFU/ml was prepared. 0.5 McFarland suspension was diluted 100× to a density of 106 CFU/mL (9.9 mL broth + 0.1 mL 0.5 McFarland suspension) and then poured to wells containing the appropriate antibiotic concentrations in the broth (10 µL inoculum to 100 µL diluted antibiotic).
2.4.5. Experimental Design
Antibiotics were selected based on their current usage preferences, ensuring that at least one antibiotic from each group was included. Bacterial isolates with a prevalence of more than 5% were included for MIC calculation.
A total of 8 antibiotics—Ampicillin, Ceftriaxone, Amikacin, Enrofloxacin, Azithromycin, Doxycycline, Clindamycin, and a Sulfadimidine-Trimethoprim (5:1) combination from Hi-Media—were selected for the study, provided by the Veterinary Diagnostic and Research Laboratory in Kathmandu. 10 ml working solution of antibiotics were prepared having concentration of 640 mg/l, 320 mg/l, 160 mg/l, 80 mg/l, 40 mg/l, 20 mg/l, 10 mg/l, 5 mg/l, 2.5 mg/l and 1.25 mg/l respectively in 20 ml test tubes.
Mueller Hinton Agar (®Hi-media) was prepared by adding 38 grams of agar in 1000 ml distilled water as per manufacturer’s instructions. The prepared agar was kept in hot water bath until use. 19 ml of agar was mixed in test tubes with 1 ml of respective working solutions of antibiotics and then poured to petri plates of diameter 9 mm such that the final concentration was achieved as shown in (Table 1). Two petri plates of same concentration were prepared in similar fashion. Antibiotic control plate was prepared by adding 1 ml of antibiotic solution of concentration 10240 mg/l in 19 ml of agar for each antibiotic Bacteria control plate was prepared by adding 1 ml of distilled water in 19 ml of agar. Petri plates were refrigerated until further use.
Bacterial inoculums were standardized for all the bacteria as mentioned above to obtain 104 colony forming units/ spot in agar. Replicator pins of diameter 2.5 mm was used to inoculate bacterial colonies from non-selective culture media to test plates. 63 strains of bacteria were inoculated to petriplates of each concentration of antibiotics. The inoculum was allowed to dry at room temperature and then incubated at 35oC for 24 hours.
2.4.6. Reading of Results
The Minimum Inhibitory Concentration (MIC) of antibiotics was visually determined as the lowest concentration at which bacterial growth was inhibited. A single colony or a faint haze within the inoculated area were disregarded. The MIC for trimethoprim-sulfamethoxazole was defined as the concentration that inhibited at least 80% of bacterial growth compared to the growth control.
2.5. Data Storage and Analysis
Data was tabulated and stored using MS-Excel v10. Statistical analysis was performed using SPSSv20. Descriptive statistics like median, mode, range, MIC50, MIC90, antibiotic susceptibility and Potency were used.
MIC50 and MIC90 was calculated according to the formula described by ref.[36]
where, graded series of MICs are arranged starting with the lowest values and n is the number of test strains.
Comparision of Antibacterials for each bacterial isolates was studied using Kruskal-Wallis test to determine the most potent antibacterial agent as stated by ref.[2]. Further Post-hoc Dunn’s test was performed to determine significant differences in between antibacterial agents.
3. Results
3.1. Prevalence of Bacterial Species
A total of 63 bacterial isolates were collected from infected canine uterus after ovariohysterectomy during the study period. Out of all the isolates, 65.08% of the isolates were Enterococcus (n= 41), 17.46% were Staphylococcus spp. (n= 11), 11.11% were Klebsiella spp. (n= 7) and only 6.35% were Streptococcus spp.(n=4). The data is represented in the (Figure 1) below:
3.2. Minimum Inhibitory Concentrations (MICs) of Different Antibacterials against Bacterial pyometra Isolates
The specific MIC ranges, MIC50s, and MIC90s values, Mean MIC ranks, CLSI breakpoints along with the resistance percentage for each bacterial species, are detailed in the (Table 2), providing a comprehensive overview of the antimicrobial profiles observed. Result showed that Enrofloxacin and Amikacin were found sensitive to all bacterial isolates. Ampicillin was found to be completely resistant against Staphylococcus spp. but effective against Enterococcus spp. and Klebsiella spp. Ceftriaxone was found completely resistant against Klebsiella spp. (100%) and Streptocoocus spp. (100%) and higher resistance was observed for Enterococcus spp. (75.61%). Little to no resistance was observed for Azithromycin against Klebsiella spp. (100%) and Enterococcus spp. (2.44%) however Staphylococcus and Streptococcus showed varying degree of resistance (27.27-50%). Doxycycline was completely resistant to Enterococcus spp. whereas no resistance was observed for Klebsiella spp. and Staphylococcus spp. Clindamycin was found highly sensitive for Staphylococcus spp.
The comparison of MIC50 and MIC90 of different antibacterials against bacterial isolates in (Table 2) showed Enrofloxacin and Amikacin had the lowest value for both parameters i.e. MIC50 and MIC90. For Enterococcus, Enrofloxacin had the lowest MIC50 and MIC90 followed by Amikacin while Doxycycline had the highest MIC50 and MIC90. Similarly Enrofloxacin and Amikacin had the lowest MIC50 and MIC90 values while ceftriaxone had the highest MIC50 and MIC90 against Klebsiella spp. For Staphylococcus, Enrofloxacin had the lowest MIC50 and MIC90 followed by Amikacin while Ceftriaxone had the highest MIC50 and MIC90. Enrofloxacin and Amikacin had the lowest MIC50 and MIC90 values while ceftriaxone had the highest MIC50 and MIC90 against Streptococcus spp.
3.3. In Vitro Susceptibility and Potency Estimation of Bacteria pyometra Isolates to Different Antibiotics
(Table 3) presents the statistical comparison of in vitro susceptibility of the bacterial pyometra isolates to eight different antibiotics and their relative potency. The results showed that all four bacterial isolates—Enterococcus spp., Klebsiella spp., Staphylococcus spp., and Streptococcus spp.—were 100% susceptible to Enrofloxacin and Amikacin. In contrast, Ceftriaxone was the least effective against Klebsiella spp., Staphylococcus spp., and Streptococcus spp., while Doxycycline was the least susceptible for Enterococcus spp.
The potency of different antibiotics against each bacterial isolates was calculated using non-parametric Krushkal Wallis test using mean MIC rank. MIC were ranked from lowest to highest for antibiotics and variance of ranks were compared at 0.05 level of significance.
For Enterococcus spp, Enrofloxacin was significantly found to be most potent antibiotic followed by Amikacin and Clindamycin whereas Doxycycine and Ceftriaxone were found to be least potent (p<0.05; Kruskal-Wallis test). For Klebsiella spp, Amikacin was found to be significantly most potent followed by Enrofloxacin whereby Ceftriaxone and Sulfadimidine+Trimethoprim was found to be least potent (p<0.05, Kruskal-Wallis test). For Staphylococcus spp. Enrofloxacin was significantly the most potent antibiotic followed by Amikacin and Clindamycin whereas Ceftriaxone was found least potent (p<0.05, Kruskal-Wallis test). Similarly, for Streptococcus spp. Enrofloxacin was found to be significantly most potent followed by Amikacin whereby Ceftriaxone and Doxycycline were found to be least potent.
No significant differences was observed in between first two most potent antibiotics while significant differences was observed in between most potent and least potent antibacterials (p<0.05,Dunn’s test), which is shown in (Table 3).
4. Discussion
The MIC of an antibiotic is a key parameter for optimizing therapy when combined with various pharmacokinetic and pharmacodynamic factors. In this study, the MICs of eight antibiotics—Ampicillin, Ceftriaxone, Doxycycline, Azithromycin, Enrofloxacin, Clindamycin, Amikacin, and Sulfadimidine-Trimethoprim (5:1)—were determined against four bacterial isolates: Enterococcus spp., Klebsiella spp., Streptococcus spp., and Staphylococcus spp., all from canine pyometra, using the agar dilution method. To our knowledge, this is the first study that depicts MIC data of anti-bacterial agents from intrauterine bacterial isolates of Canine pyometra. The interpretive cut-off points provided by CLSI and EUCAST are based on human data and veterinary interpretation criteria of MIC value for most of the antibacterials are very scarce to find [28]. The above study may serve as a milestone in depicting MIC of antibiotics of various classes in veterinary pharmacology and microbiology studies.
Process of choosing proper antibiotic for therapeutic innervation during clinical management of canine pyometra induces dilemma in canine veterinary medicine practices due to conflicting data of pharmaceutical companies and research limitations in quantitative antibiotic susceptibility. Any apparent clinical advantage of one antibiotic over another is correlated to in-vitro descriptive statistics of antibiotics which in turn depicts better clinical management and prognosis of disease. The study hereby aims to develop a therapeutic protocol based on descriptive data analysis of antibiotics against bacterial species involved in canine pyometra rather than most commonly studied and used antibiotic disc diffusion tests.
Enterococcus, Klebsiella, Staphylococcus and Streptococcus were isolated from pyometra cases presented to different animal hospitals and clinics of Kathmandu valley which was similar to the findings reported by [21,37]. Enterococcus spp. was the most prevalent isolates obtained from 65.08% of the samples in our study which was different from the findings reported by ref.[38] and ref.[11] and ref.[12] Where E. coli was found to be the most prevalent bacteria in canine endometrial collection. Differences in findings might be attributed to differences in sampling individuals, study area and isolation methods used.
The MIC range for ampicillin against Enterococcus spp., Klebsiella spp., Streptococcus spp., and Staphylococcus spp. was 0.03-2 μg/ml, 0.03-2 μg/ml, 0.25-1 μg/ml, and 0.015-0.5 μg/ml, respectively. The MIC50 ranged from 0.06 to 0.5 μg/ml, with the lowest (0.06 μg/ml) for Staphylococcus spp. and the highest (0.5 μg/ml) for Enterococcus spp. and Klebsiella spp. The MIC values for Enterococcus and Streptococcus are below the CLSI sensitivity breakpoint [33], indicating high in-vitro efficacy of ampicillin against these bacteria. In contrast, the MIC values for Staphylococcus are above the CLSI breakpoint, suggesting intermediate efficacy. Our findings for Enterococcus sensitivity to ampicillin are consistent with [39], but differ from [40], which reported resistance linked to mutations in the PBP5 gene. The variation in MIC values may be due to differences in bacterial infection sites and strains. Additionally, the MIC50 and MIC90 for Staphylococcus in our study are double the values reported by [39]. For Enterococcus, the MIC50 was found lower than that reported by ref. [41] but MIC90 was higher in our study. Similar results were reported by ref. [42] for Streptococcus, where they highlighted that horizontal gene transfer of resistance genes such as bla (β-lactamase), erm (macrolide resistance), and van (vancomycin resistance), along with mutations in the bacterial genome and various environmental and host factors, contribute to the development and spread of antibiotic-resistant pathogens.
MIC range of Ceftriaxone was found higher than interpretative cut-points stated by CLSI for Klebsiella, Staphylococcus and Streptococcus spp. indicating resistance to Ceftriaxone in the strains isolated. The MIC50 and MIC90 of ceftriaxone for Streptococcus spp. were higher than those reported by [39,42,43]. This increase may be attributed to the overuse or misuse of ceftriaxone at the study site, leading to bacterial resistance. In contrast, the MIC values for ceftriaxone inhibiting 50% and 90% of Staphylococcus spp. were similar to those reported by [43]. Overall, the MIC90 values against all isolates exceeded the CLSI clinical breakpoints, indicating a higher prevalence of resistant strains.
The MIC50 and MIC90 of Azithromycin were below CLSI breakpoint for Enterococcus, Klebsiella and Streptococcus strains indicating sensitivity to Azithromycin. The MIC90 of Azithromycin for Staphylococcus was found to be 8 mg/l which is greater than the breakpoint value indicating presence of resistant strains. The possible mechanisms by which staphylococci develop resistance to Azithromycin include (i) the modification of the 23S rRNA through methylation, (ii) the upregulation of Msr family efflux pumps, and (iii) the enzymatic inactivation of macrolides by phosphotransferases or esterases [44].
The MIC90 of enrofloxacin was 0.06 μg/ml for all bacterial isolates, lower than the value reported by [39]. This result is below the clinical breakpoint set by CLSI 2020 [33], showing that enrofloxacin is very effective against the bacteria found in canine pyometra. MIC range, MIC50 and MIC90 were found lower for Staphylococcus spp. than that reported by ref.[45] and ref.[46], which might be due to differences in sites of sample collection. The MIC parameters for Enterococcus were also found lower than the study conducted by ref.[41] and lower for Klebsiella than reported by [47].
Similarly the MIC range of Amikacin against all bacterial isolates were found ≤0.06 depicting high sensitivity of Amikacin against pyometra isolates. The result of our study is in contrast to the finding reported by ref.[48] who reported 50% sensitivity of Amikacin for bacterial isolates of Canine pyometra which might be due to difference in bacterial strains isolated and antibiotic sensitivity tests employed. The MIC range, MIC50 and MIC90 were found lower than that of ref.[47] for Klebsiella spp.
The MIC90 of Doxycycline against Enterococcus and Streptococcus was higher than CLSI breakpoints but were lower than CLSI breakpoints against Klebsiella and Staphylococcus spp. thus indicates efficacy of Doxycycline in Pyometra imposed by later bacterial isolates but not in former isolates. The MIC parameters were higher than that reported by ref.[41] for Enterococcus spp. in our study but lower than that reported by ref.[47] for Klebsiela spp.
MIC of Clindamycin was found to be within clinical breakpoints against Klebsiella, Streptococcus and Staphylococcus isolates but not for Enterococcus spp. since Enterococcus are intrinsically resistant to Clindamycin as supported by the findings of ref.[49] and ref.[50].
The MIC90 of Sulfadimidine-Trimethorim (5:1) for Klebsiella was found to be within the CLSI breakpoint indicating sensitivity of the drug against Klebsiella, whereby its MIC90 for other bacteria were found higher suggesting resistance to Sulfadimidine-Trimethorim. The results obtained are in contrast to the findings of ref.[43] where the drug was sensitive to Streptococcus and Staphylococcus spp. isolated from conjunctiva of dogs probably attributed to the difference in sample sites.
Potency studies among the 8 antibiotics tested for 4 bacterial isolates revealed Enrofloxacin to be significantly most potent antibiotic against Enterococcus, Staphylococcus and Streptococcus spp. and second most potent against Klebsiella spp. for which Amikacin was determined most potent and enrofloxacin being second most potent(p<0.05). Amikacin was found to be the second most potent antibiotic for Enterococcus, Staphylococcus and Streptococcus. Thus, Enrofloxacin and Amikacin can be concluded as having potency advantage in pyometra infections relating to studied bacterial isolates. There was no any significant differences among the potency of two antibacterials. Susceptibility studies based on MIC also revealed null resistance of bacterial strains against Enrofloxacin and Amikacin making the two drugs better antibacterial of choice in pyometra innervation.
Ceftriaxone was found to be significantly less potent than other antibiotics against all bacterial isolates (p<0.05), offering no potency advantage. Similar findings were observed in susceptibility studies, where ceftriaxone showed complete resistance to Klebsiella, Streptococcus, and Staphylococcus, and 75.61% resistance was observed in Enterococcus spp. The primary mechanism of resistance to ceftriaxone involves the production of AmpC β-lactamases, such as CMY and DHA, and extended-spectrum β-lactamases (ESBLs), including TEM, SHV, CTX-M, VEB, and GES enzymes [51]. These results suggest minimal efficacy of this antibiotic in clinical settings based on in vitro studies. The increasing resistance to ceftriaxone over time may be attributed to improper use of antibiotics and inadequate infection control practices, raising concerns for both public and animal health [52].
Doxycycline was found susceptible for Klebsiella, Staphylococcus whereas varying resistance (>50%) was observed in Enterococcus and Streptococcus spp. however, potency studies did not indicate any comparative advantage over other antibiotics. Similar results were obtained for sensitivity of Ampicillin to Enterococcus, Klebsiella and Streptococcus (75-100%) but were less potent in comparison to other antibiotics against the isolates. Azithromycin was highly sensitive to Klebsiella but was less potent than all antibacterials except Ceftriaxone and Sulfadimidine-Trimethoprim.
The study offers a preliminary guide for selecting antibiotics in the pre- and post-surgical management of pyometra and associated septicemia. However, further research is needed to test additional antibacterial agents and compare their potency against the bacterial isolates identified. Additionally, testing the susceptibility and potency of other bacterial isolates from canine pyometra is recommended to better inform treatment decisions. Clinical efficacy of an antibacterial agent depends on multiple factors beyond in vitro MIC studies, including drug concentration, serum levels, pharmacokinetics, pharmacodynamics, dosing, and safety margins. Therefore, no single parameter can determine superiority. Further clinical trials considering these factors for potent agents like Enrofloxacin and Amikacin could aid clinicians in successfully managing canine pyometra.
5. Conclusions
The study revealed that Enterococcus was the most prevalent pathogen associated with Canine pyometra, while Klebsiella, Streptococcus, and Staphylococcus species were also isolated. Enrofloxacin and Amikacin were found to be highly sensitivity against all isolates, indicating their effectiveness as treatment options. Ampicillin showed sensitivity towards Enterococcus and Klebsiella species but was ineffective against Streptococcus. Notably, Klebsiella and Staphylococcus strains exhibited high sensitivity to Doxycycline, whereas Enterococcus species were completely resistant. Ceftriaxone showed the highest resistance across all isolates, followed by Sulfadimidine-Trimethoprim (5:1). The findings highlight the superior potency of Enrofloxacin and Amikacin against the tested bacterial isolates, while Ceftriaxone was the least effective. These results provide critical guidance for the selection of antibiotics in the treatment and post-surgical management of Canine pyometra.
Author Contributions
Conceptualization, Avinash Chhetri. and Madhav Paudel; Methodology, Avinash Chhetri; Software, Avinash Chhetri; Validation, Avinash Chhetri, Madhav Paudel and Sharada Thapaliya; Formal Analysis, Avinash Chhetri; Investigation, Avinash Chhetri and Madhav Paudel; Resources, Avinash Chhetri and Madhav Paudel; Data Curation, Avinash Chhetri and Madhav Paudel; Writing – Original Draft Preparation, Avinash Chhetri and Madhav Paudel; Writing – Review & Editing, Avinash Chhetri, Madhav Paudel, Tulsi Ram Gompo and Sharada Thapaliya; Visualization, Madhav Paudel; Supervision, Sharada Thapaliya; Project Administration, Sharada Thapaliya; Funding Avinash Chhetri.
Funding
This research received no external funding.
Ethical consideration statement
This study adhered to ethical guidelines to ensure animal welfare. Sample collection from canine pyometra cases was conducted with minimal discomfort to the animals, following approval from Nepal Veterinary Council. Informed consent was obtained from dog owners, and antibacterial agents were used solely for research purposes. Data privacy and confidentiality were maintained throughout the study.
Acknowledgments
We extend our heartfelt gratitude to the Veterinary Diagnostic and Research Laboratory (VDRL) in Tripureshwor, Kathmandu, Nepal, for providing the necessary laboratory facilities for this research. We also deeply appreciate the respondents and all those who assisted from Kathmandu Metropolitan City. Our sincere thanks go to Dr. Rocksan Karmacharya, Dr. Rabindra Tiwari, and Dr. Subash Rimal for their invaluable support throughout this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Aminov, R.I. A Brief History of the Antibiotic Era: Lessons Learned and Challenges for the Future. Front. Microbiol. 2010, 1, 134. [Google Scholar] [CrossRef]
- Kowalski, R.P.; Yates, K.A.; Romanowski, E.G.; Karenchak, L.M.; Mah, F.S.; Gordon, Y.J. An Ophthalmologist’s Guide to Understanding Antibiotic Susceptibility and Minimum Inhibitory Concentration Data. Ophthalmology 2005, 112, 1987. [Google Scholar] [CrossRef] [PubMed]
- Andrews, J.M. Determination of Minimum Inhibitory Concentrations. J. Antimicrob. Chemother. 2002, 49, 1049–1049. [Google Scholar] [CrossRef]
- Kowalska-Krochmal, B.; Dudek-Wicher, R. The Minimum Inhibitory Concentration of Antibiotics: Methods, Interpretation, Clinical Relevance. Pathogens 2021, 10, 165. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.; Huang, L.; Hao, H.; Sanders, P.; Yuan, Z. Application of PK/PD Modeling in Veterinary Field: Dose Optimization and Drug Resistance Prediction. BioMed Res. Int. 2016, 2016, 5465678. [Google Scholar] [CrossRef]
- Rodríguez-Gascón, A.; Solinís, M.Á.; Isla, A. The Role of PK/PD Analysis in the Development and Evaluation of Antimicrobials. Pharmaceutics 2021, 13, 833. [Google Scholar] [CrossRef]
- Egenvall, A.; Hagman, R.; Bonnett, B.N.; Hedhammar, A.; Olson, P.; Lagerstedt, A.S. Breed Risk of Pyometra in Insured Dogs in Sweden. J. Vet. Intern. Med. 2001, 15, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Marretta, S.M.; Matthiesen, D.T.; Nichols, R. Pyometra and Its Complications. Probl. Vet. Med. 1989, 1, 50–62. [Google Scholar] [PubMed]
- Okano, S.; Tagawa, M.; Takase, K. Relationship of the Blood Endotoxin Concentration and Prognosis in Dogs with Pyometra. J. Vet. Med. Sci. 1998, 60, 1265–1267. [Google Scholar] [CrossRef]
- Bassessar, V.; Verma, Y.; Swamy, M. Antibiogram of Bacterial Species Isolated from Canine Pyometra. Vet. World 2013, 6, 546. [Google Scholar] [CrossRef]
- Liao, A.-T.; Huang, W.-H.; Wang, S.-L. BACTERIAL ISOLATION AND ANTIBIOTIC SELECTION AFTER OVARIOHYSTERECTOMY OF CANINE PYOMETRA: A RETROSPECTIVE STUDY OF 55 CASES. Taiwan Vet. J. 2020, 46, 67–74. [Google Scholar] [CrossRef]
- Paudel, M.; Kafle, S.; Gompo, T.R.; Khatri, K.B.; Aryal, A. Microbiological and Hematological Aspects of Canine Pyometra and Associated Risk Factors. Heliyon 2023, 9, e22368. [Google Scholar] [CrossRef] [PubMed]
- Robaj, A.; Sylejmani, I.; Hamidi, A. Occurrence and Antimicrobial Susceptibility of Bacterial Agents of Canine Pyometra. Indian J. Anim. Res. 2018, 52, 394–400. [Google Scholar]
- kumari Baithalu, R.; Maharana, B.R.; Mishra, C.; Sarangi, L.; Samal, L. Canine Pyometra. Vet. World 2010, 3, 340. [Google Scholar]
- Bartoskova, A.; Vitasek, R.; Leva, L.; Faldyna, M. Hysterectomy Leads to Fast Improvement of Haematological and Immunological Parameters in Bitches with Pyometra. J. Small Anim. Pract. 2007, 48, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Hagman, R. Pyometra in Small Animals 2.0. Vet. Clin. North Am. Small Anim. Pract. 2022, 52, 631–657. [Google Scholar] [CrossRef] [PubMed]
- Turkki, O.M.; Sunesson, K.W.; den Hertog, E.; Varjonen, K. Postoperative Complications and Antibiotic Use in Dogs with Pyometra: A Retrospective Review of 140 Cases (2019). Acta Vet. Scand. 2023, 65, 11. [Google Scholar] [CrossRef] [PubMed]
- Fossum, T.W.; Duprey, L.P.; O’Connor, D. Small Animal Surgery; 3rd ed.; Elsevier: Boston, MA, 2007; ISBN 978-0-323-04439-4.
- Tobias, K.M.; Johnston, S.A. Veterinary Surgery: Small Animal. No Title 2017. [Google Scholar]
- Textbook of Veterinary Internal Medicine: Diseases of the Dog and the Cat; Ettinger, S.J., Feldman, E.C., Côté, E., Eds.; Eighth edition.; Elsevier: St. Louis, Missouri, 2017; ISBN 978-0-323-31211-0.
- Hagman, R. Canine Pyometra: What Is New? Reprod. Domest. Anim. 2017, 52, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Fieni, F.; Topie, E.; Gogny, A. Medical Treatment for Pyometra in Dogs. Reprod. Domest. Anim. 2014, 49, 28–32. [Google Scholar] [CrossRef]
- Lavin, L.E.; Maki, L.C. Antimicrobial Use in the Surgical Treatment of Canine Pyometra: A Questionnaire Survey of Arizona-Licensed Veterinarians. Vet. Med. Sci. 2023, 9, 1124–1133. [Google Scholar] [CrossRef] [PubMed]
- Jeff, D.; Brian Lucas, H. Canine Pyometra: Early Recognition and Diagnosis. Available online: https://www.dvm360.com/view/canine-pyometra-early-recognition-and-diagnosis (accessed on 8 April 2024).
- Pomba, C.; Belas, A.; Menezes, J.; Marques, C. The Public Health Risk of Companion Animal to Human Transmission of Antimicrobial Resistance During Different Types of Animal Infection. In Proceedings of the Advances in Animal Health, Medicine and Production; Freitas Duarte, A., Lopes da Costa, L., Eds.; Springer International Publishing: Cham, 2020; pp. 265–278.
- Heffernan, A.J.; Sime, F.B.; Lipman, J.; Roberts, J.A. Individualising Therapy to Minimize Bacterial Multidrug Resistance. Drugs 2018, 78, 621–641. [Google Scholar] [CrossRef] [PubMed]
- Turnidge, J.; Paterson, D.L. Setting and Revising Antibacterial Susceptibility Breakpoints. Clin. Microbiol. Rev. 2007, 20, 391–408, table of contents. [Google Scholar] [CrossRef]
- de Boer, M.; Heuer, C.; Hussein, H.; McDougall, S. Minimum Inhibitory Concentrations of Selected Antimicrobials against Escherichia Coli and Trueperella Pyogenes of Bovine Uterine Origin. J. Dairy Sci. 2015, 98, 4427–4438. [Google Scholar] [CrossRef] [PubMed]
- Acharya, K.P.; Wilson, R.T. Antimicrobial Resistance in Nepal. Front. Med. 2019, 6, 105. [Google Scholar] [CrossRef] [PubMed]
- Cantón, R.; Morosini, M.-I. Emergence and Spread of Antibiotic Resistance Following Exposure to Antibiotics. FEMS Microbiol. Rev. 2011, 35, 977–991. [Google Scholar] [CrossRef] [PubMed]
- Alaidarous, M.; Alanazi, M.; Abdel-Hadi, A. Isolation, Identification, and Antimicrobial Susceptibility of Bacteria Associated with Waterpipe Contaminants in Selected Area of Saudi Arabia. BioMed Res. Int. 2017, 2017, 8042603. [Google Scholar] [CrossRef] [PubMed]
- Wiegand, I.; Hilpert, K.; Hancock, R.E.W. Agar and Broth Dilution Methods to Determine the Minimal Inhibitory Concentration (MIC) of Antimicrobial Substances. Nat. Protoc. 2008, 3, 163–175. [Google Scholar] [CrossRef] [PubMed]
- CLSI Clinical & Laboratory Standards Institute: CLSI Guidelines. Available online: https://clsi.org/ (accessed on 25 July 2024).
- Hasselmann, C. Determination of Minimum Inhibitory Concentrations (MICs) of Antibacterial Agents by Broth Dilution. Clin. Microbiol. Infect. 2003, 9. [Google Scholar]
- EUCAST Determination of Minimum Inhibitory Concentrations (MICs) of Antibacterial Agents by Broth Dilution. Clin. Microbiol. Infect. 2003, 9, ix–xv. [CrossRef]
- Schwarz, S.; Silley, P.; Simjee, S.; Woodford, N.; van Duijkeren, E.; Johnson, A.P.; Gaastra, W. Assessing the Antimicrobial Susceptibility of Bacteria Obtained from Animals. J. Antimicrob. Chemother. 2010, 65, 601–604. [Google Scholar] [CrossRef] [PubMed]
- Lopes, C.E.; De Carli, S.; Riboldi, C.I.; De Lorenzo, C.; Panziera, W.; Driemeier, D.; Siqueira, F.M. Pet Pyometra: Correlating Bacteria Pathogenicity to Endometrial Histological Changes. Pathog. Basel Switz. 2021, 10, 833. [Google Scholar] [CrossRef] [PubMed]
- Mateus, L.; Henriques, S.; Merino, C.; Pomba, C.; Lopes da Costa, L.; Silva, E. Virulence Genotypes of Escherichia Coli Canine Isolates from Pyometra, Cystitis and Fecal Origin. Vet. Microbiol. 2013, 166, 590–594. [Google Scholar] [CrossRef] [PubMed]
- Moyaert, H.; Morrissey, I.; de Jong, A.; El Garch, F.; Klein, U.; Ludwig, C.; Thiry, J.; Youala, M. Antimicrobial Susceptibility Monitoring of Bacterial Pathogens Isolated from Urinary Tract Infections in Dogs and Cats Across Europe: ComPath Results. Microb. Drug Resist. Larchmt. N 2017, 23, 391–403. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, C.-L.; Charlebois, A.; Masson, L.; Archambault, M. Characterization of Hospital-Associated Lineages of Ampicillin-Resistant Enterococcus Faecium from Clinical Cases in Dogs and Humans. Front. Microbiol. 2013, 4, 245. [Google Scholar] [CrossRef] [PubMed]
- Feßler, A.T.; Scholtzek, A.D.; Schug, A.R.; Kohn, B.; Weingart, C.; Hanke, D.; Schink, A.-K.; Bethe, A.; Lübke-Becker, A.; Schwarz, S. Antimicrobial and Biocide Resistance among Canine and Feline Enterococcus Faecalis, Enterococcus Faecium, Escherichia Coli, Pseudomonas Aeruginosa, and Acinetobacter Baumannii Isolates from Diagnostic Submissions. Antibiot. Basel Switz. 2022, 11, 152. [Google Scholar] [CrossRef] [PubMed]
- Imanishi, I.; Iyori, K.; Také, A.; Asahina, R.; Tsunoi, M.; Hirano, R.; Uchiyama, J.; Toyoda, Y.; Sakaguchi, Y.; Hayashi, S. Antibiotic-Resistant Status and Pathogenic Clonal Complex of Canine Streptococcus Canis-Associated Deep Pyoderma. BMC Vet. Res. 2022, 18, 395. [Google Scholar] [CrossRef] [PubMed]
- Jinks, M.R.; Miller, E.J.; Diaz-Campos, D.; Mollenkopf, D.F.; Newbold, G.; Gemensky-Metzler, A.; Chandler, H.L. Using Minimum Inhibitory Concentration Values of Common Topical Antibiotics to Investigate Emerging Antibiotic Resistance: A Retrospective Study of 134 Dogs and 20 Horses with Ulcerative Keratitis. Vet. Ophthalmol. 2020, 23, 806–813. [Google Scholar] [CrossRef]
- Fyfe, C.; Grossman, T.H.; Kerstein, K.; Sutcliffe, J. Resistance to Macrolide Antibiotics in Public Health Pathogens. Cold Spring Harb. Perspect. Med. 2016, 6, a025395. [Google Scholar] [CrossRef] [PubMed]
- Ganière, J.P.; Médaille, C.; Limet, A.; Ruvoen, N.; André-Fontaine, G. Antimicrobial Activity of Enrofloxacin against Staphylococcus Intermedius Strains Isolated from Canine Pyodermas. Vet. Dermatol. 2001, 12, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Awji, E.G.; Tassew, D.D.; Lee, J.-S.; Lee, S.-J.; Choi, M.-J.; Reza, M.A.; Rhee, M.-H.; Kim, T.-H.; Park, S.-C. Comparative Mutant Prevention Concentration and Mechanism of Resistance to Veterinary Fluoroquinolones in Staphylococcus Pseudintermedius. Vet. Dermatol. 2012, 23, 376–380, e68-69. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhang, L.; Dai, H.; Zhang, H.; Song, Y.; An, Q.; Wang, J.; Xia, Z. Multidrug-Resistant Klebsiella Pneumoniae Complex From Clinical Dogs and Cats in China: Molecular Characteristics, Phylogroups, and Hypervirulence-Associated Determinants. Front. Vet. Sci. 2022, 9, 816415. [Google Scholar] [CrossRef] [PubMed]
- Hadiya, H.D.; Patel, D.M.; Ghodasara, D.J.; Bhanderi, B.B. Canine Pyometra: Clinico-Diagnostic, Microbial, Gross and Histopathological Evaluation. Indian J. Vet. Sci. Biotechnol. 2021, 17, 41–45. [Google Scholar]
- García-Solache, M.; Rice, L.B. The Enterococcus: A Model of Adaptability to Its Environment. Clin. Microbiol. Rev. 2019, 32, e00058-18. [Google Scholar] [CrossRef] [PubMed]
- Sirichoat, A.; Flórez, A.B.; Vázquez, L.; Buppasiri, P.; Panya, M.; Lulitanond, V.; Mayo, B. Antibiotic Susceptibility Profiles of Lactic Acid Bacteria from the Human Vagina and Genetic Basis of Acquired Resistances. Int. J. Mol. Sci. 2020, 21, 2594. [Google Scholar] [CrossRef] [PubMed]
- McLeod, D.C.; Nahata, M.C.; Barson, W.J. Ceftriaxone: A Third-Generation Cephalosporin. Drug Intell. Clin. Pharm. 1985, 19, 900–906. [Google Scholar] [CrossRef]
- Shi, Q.; Ye, Y.; Lan, P.; Han, X.; Quan, J.; Zhou, M.; Yu, Y.; Jiang, Y. Prevalence and Characteristics of Ceftriaxone-Resistant Salmonella in Children’s Hospital in Hangzhou, China. Front. Microbiol. 2021, 12, 764787. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Prevalence of Bacterial isolates in Canine Pyometra (N=63).
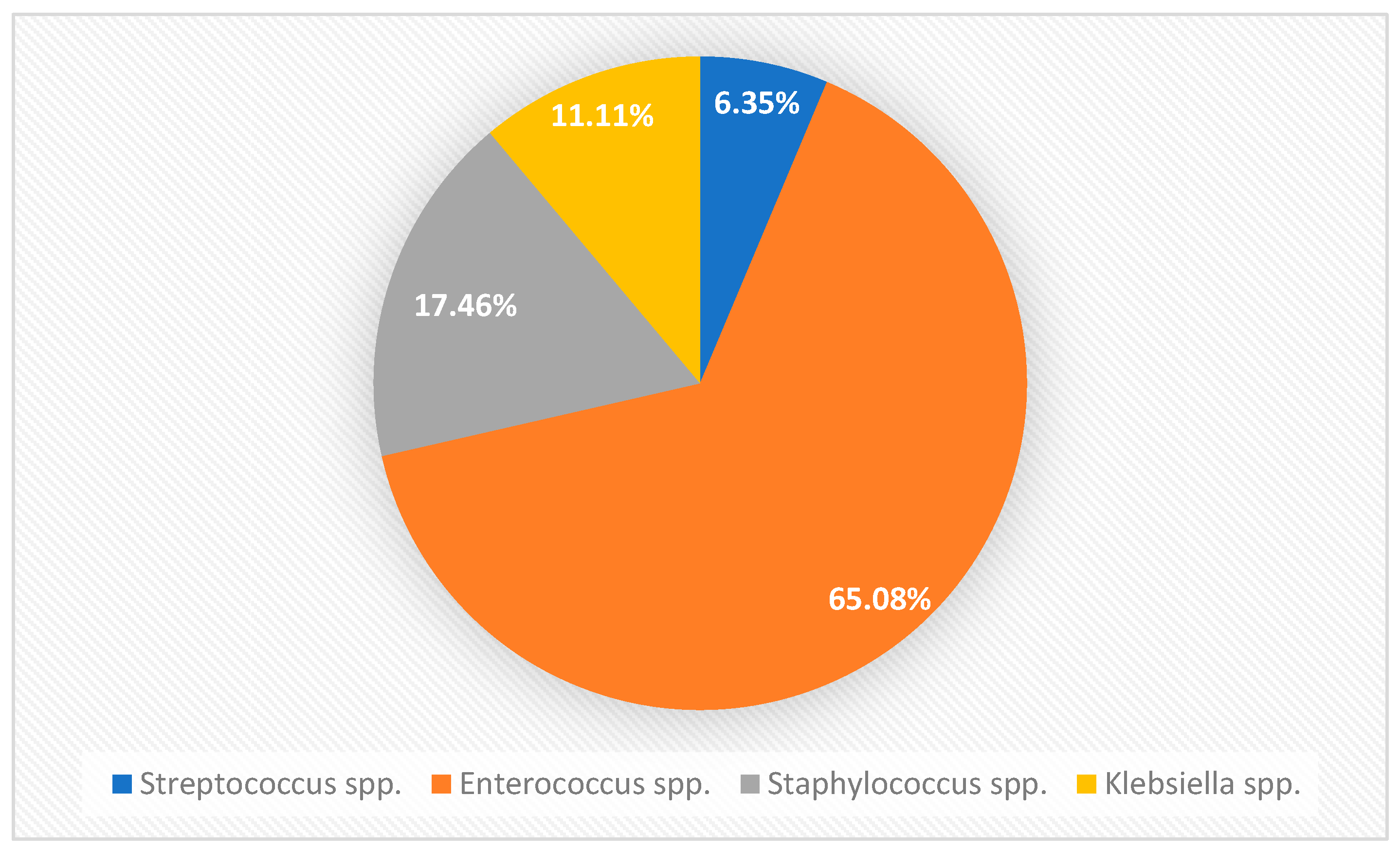

Table 1.
Preparation of dilution of antibiotics in agar dilution test.
| Antimicrobial conc. In stock solution |
Volume of stock solution |
Volume of distilled water |
Antimicrobial concn. Obtained (mg/L) |
Final concentration after adding. 19 ml Agar |
| 10240 | 1 | 0 | 10240 | 512 |
| 10240 | 1 | 1 | 5120 | 256 |
| 10240 | 1 | 3 | 2560 | 128 |
| 2560 | 1 | 1 | 1280 | 64 |
| 2560 | 1 | 3 | 640 | 32 |
| 2560 | 1 | 7 | 320 | 16 |
| 320 | 1 | 1 | 160 | 8 |
| 320 | 1 | 3 | 80 | 4 |
| 320 | 1 | 7 | 40 | 2 |
| 40 | 1 | 1 | 20 | 1 |
| 40 | 1 | 3 | 10 | 0.5 |
| 40 | 1 | 7 | 5 | 0.25 |
| 5 | 1 | 1 | 2.5 | 0.125 |
| 5 | 1 | 3 | 1.25 | 0.06 |
| 5 | 1 | 7 | 0.625 | 0.03 |
| 0.625 | 1 | 1 | 0.3125 | 0.015 |
| 0.625 | 1 | 3 | 0.1562 | 0.008 |
| 0.625 | 1 | 7 | 0.0781 | 0.004 |
Table 2.
Statistical Overview of Antibacterial MICs against Bacterial Isolates from Canine Pyometra.
Table 2.
Statistical Overview of Antibacterial MICs against Bacterial Isolates from Canine Pyometra.
| Sulfadimidine+Trimethoprim (5:1) | |||||||
|---|---|---|---|---|---|---|---|
| Bacteria | n | MIC Range | MIC50 | MIC90 | Mean MIC rank* | CLSI Breakpoint | Resistivity |
| Enterococcus | 41 | 0.25-64 | 2 | 8 | 200.34 | ≤1 | 23(56.10%) |
| Klebsiella | 7 | 1 to 4 | 2 | 2 | 41.50 | ≤2 | 2(28.57%) |
| Staphylococcus | 11 | 1 to 16 | 2 | 4 | 66.36 | ≤2 | 5(45.45%) |
| Streptococcus | 4 | 0.25-8 | 0.25 | 8 | 21.13 | N/A | NA |
| Ampicillin | |||||||
| Enterococcus | 41 | 0.03-2 | 0.5 | 2 | 200.34 | ≤8 | 0(0%) |
| Klebsiella | 7 | 0.03-2 | 0.5 | 2 | 26.71 | ≤8 | 0(0%) |
| Staphylococcus | 11 | 0.25-1 | 0.25 | 1 | 44.94 | ≤0.12 | 11(100%) |
| Streptococcus | 4 | 0.015-0.5 | 0.06 | 0.5 | 9.00 | ≤0.25 | 1(25%) |
| Ceftriaxone | |||||||
| Enterococcus | 41 | 0.25-32 | 8 | 32 | 237.18 | ≤1 | 31(75.61%) |
| Klebsiella | 7 | 8-32 | 16 | 32 | 52.00 | ≤1 | 7(100%) |
| Staphylococcus | 11 | 2-64 | 64 | 64 | 79.64 | N/A | 11(100%) |
| Streptococcus | 4 | 1-64 | 8 | 64 | 28.50 | ≤0.5 | 4(100%) |
| Azithromycin | |||||||
| Enterococcus | 41 | 0.06-32 | 1 | 4 | 164.02 | ≤16 | 1(2.44%) |
| Klebsiella | 7 | 0.25-4 | 1 | 4 | 36.43 | ≤16 | 0(0%) |
| Staphylococcus | 11 | 0.125-8 | 0.5 | 8 | 52.18 | ≤2 | 3(27.27%) |
| Streptococcus | 4 | 0.5-4 | 0.5 | 2 | 21.63 | ≤0.5 | 2(50%) |
| Doxycycline | |||||||
| Enterococcus | 41 | 8-128 | 32 | 64 | 294.61 | ≤4 | 41(100%) |
| Klebsiella | 7 | 0.25-1 | 1 | 1 | 29.36 | ≤4 | 0(0%) |
| Staphylococcus | 11 | 1 to 4 | 1 | 4 | 59.25 | ≤4 | 0(0%) |
| Streptococcus | 4 | 1 to 4 | 1 | 4 | 24.25 | ≤2 | 0(0%) |
| Enrofloxacin | |||||||
| Enterococcus | 41 | 0.015-0.125 | 0.03 | 0.06 | 47.91 | ≤2 | 0(0%) |
| Klebsiella | 7 | 0.03-0.06 | 0.06 | 0.06 | 9.86 | ≤2 | 0(0%) |
| Staphylococcus | 11 | 0.015-0.06 | 0.03 | 0.06 | 15.95 | ≤1 | 0(0%) |
| Streptococcus | 4 | 0.03-0.06 | 0.03 | 0.06 | 5.75 | N/A | 0(0%) |
| Amikacin | |||||||
| Enterococcus | 41 | 0.015-0.5 | 0.03 | 0.125 | 59.87 | ≤16 | 0(0%) |
| Klebsiella | 7 | 0.03-0.06 | 0.06 | 0.06 | 8.71 | ≤16 | 0(0%) |
| Staphylococcus | 11 | 0.015-0.06 | 0.03 | 0.06 | 17.27 | N/A | 0(0%) |
| Streptococcus | 4 | 0.03-0.06 | 0.06 | 0.06 | 7.13 | N/A | 0(0%) |
| Clindamycin | |||||||
| Enterococcus | 41 | 0.015-2 | 0.06 | 2 | 111.72 | N/A | NA |
| Klebsiella | 7 | 0.125-0.5 | 0.125 | 0.5 | 18.00 | N/A | NA |
| Staphylococcus | 11 | 0.03-0.06 | 0.03 | 0.06 | 17.77 | ≤0.5 | 0(0%) |
| Streptococcus | 4 | 0.06-0.5 | 0.25 | 0.5 | 14.63 | ≤0.25 | 2(50%) |
Notes: N/A indicates not available on CLSI guidelines MIC50 represents the antibiotic concentration required to inhibit the growth of 50% of the bacterial isolates tested, while MIC90 refers to the concentration needed to inhibit 90% of the isolates. * Indicates the using of non-parametric Krushkal Wallis test.
Table 3.
Comparative Analysis of In Vitro Antibiotic Susceptibility and Potency against Bacterial Isolates from Pyometra.
Table 3.
Comparative Analysis of In Vitro Antibiotic Susceptibility and Potency against Bacterial Isolates from Pyometra.
| Bacteria Isolated (n=tests) | Susceptibility | Potency |
|---|---|---|
| Enterococcus spp. (n=328) | E=AK=AP>AZ>ST>CR>D | E*>AK>C>AZ>AP=ST>CR>D* |
| Klebsiella spp. (n=56) | E=AK=AP=AZ=D>ST>CR | AK*>E>C>AP>D>AZ>ST>CR* |
| Staphylococcus spp. (n=88) | E=AK=C=D>AZ>ST>AP=CR | E*>AK>C>AP>AZ>D>ST>CR* |
| Streptococcus spp. (n=32) | E=AK>AP>C=D=AZ>CR | E*>AK>AP>C>ST>AZ>D>CR* |
Notes: E: Enrofloxacin, AK: Amikacin, AP: Ampicillin, C: Clindamycin, D: Doxycycline, ST: Sulfadimidine+Trimethoprim, AZ: Azithromycin, CR: Ceftriaxone. * Indicates significant difference (p<0.05,Dunn’s test) observed in between most potent and least potent antibacterials. The antibiotic susceptibility for each bacterial group was evaluated by comparing their MICs with the established CLSI breakpoints.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



