
Submitted:
19 August 2024
Posted:
20 August 2024
You are already at the latest version
Abstract
High-flow oscillatory ventilation (HFOV) is a common rescue treatment in infants and children with respiratory failure. This type of ventilation is an effective technique in numerous diseases that affect a child in the postnatal period, such as ARDS, meconium aspiration syndrome (MIS), postnatal pulmonary bleeding and idiopathic pulmonary hypertension (IPH). Although this ventilation technique is commonly recognized as a valuable therapeutic option in the general pediatric population, this is not the same for children with congenital cardiovascular diseases. The key mechanism of oscillatory ventilation is continuous positive pressure administered within the airways via a small tidal volume at high frequency. Tidal volumes are between 1 and 3 ml/kg delivered at 5 – 15 Hz equivalent to 300 – 900 breaths per minute. Few older studies conducted on humans and animals highlight that HFOV may be dangerous for congenital heart patients. According to these evidences, hemodynamic parameters such as blood pressure, wedge pressure, central venous pressure, heart rate and inotrope level can be dangerously changed for patients with congenital heart disease, therefore oscillatory ventilation should be avoided. Numerous retrospective studies have pointed out how oscillatory ventilation constitutes a valid therapeutic option in children with congenital heart disease. Recently, new evidences have highlighted how hemodynamic parameters are modified in a non-significant way by this type of ventilation, remaining beneficial as in the normal pediatric population. This narrative review aims to describe the mechanisms of oscillatory ventilation and collect all the available evidences to support its use in pediatric patients with congenital heart problems.
Keywords:
HFOV
; Pediatric Critical Care
; Congenital Heart Disease
; Acute Respiratory Distress Syndrome
; ARDS
; Pulmonary Hypertension
; Mechanical Ventilation
; Newborn
1. Introduction
High-frequency oscillatory ventilation (HFOV) is a rescue therapy in case of failure of conventional ventilation [1]. Oscillatory ventilation may require prolonged sedation and neuromuscular blockade to be effective, resulting in prolonged ICU requirement [2,3,4,5]. Cardiovascular complications include reduced venous return, decreased cardiac output, intraventricular hemorrhage and increased intrathoracic pressure [6,7]. Pneumothorax, pneumomediastinum, pneumopericardium, and interstitial emphysema may also occur during HFOV [8,9]. Various clinical studies have found that its use is safe and beneficial even in pediatric patients with univentricular physiology, as in the case of those undergoing Fontan surgery [10]. This type of ventilation has been effectively used in the treatment of ARDS as an early rescue ventilation after cardiac surgery performed in cardiopulmonary bypass or in the treatment of post-operative pulmonary hypertension [11,12,13]. This narrative review aims to highlight how and why using this ventilation mode is a valuable aid in the treatment of clinical conditions that may occur after cardiopulmonary bypass and how it is a safe and beneficial ventilation technique in pediatric patients suffering from congenital heart disease.
2. HFOV: How It Works
Oscillatory ventilation is a mode of invasive mechanical ventilation that requires the use of a particular ventilator called oscillator [14]. The mechanism of oscillatory ventilation is based on the generation of an oscillatory flow inside the airways creating a waveform that varies depending on the source of the oscillation, the attenuation of the waveform during the passage inside the airways and the pressure and efficiency of the volume delivered to the alveoli [15,16]. The HFOV then produces a biphasic pressure wave and diverts the new flow – called bias flow – to the patient with frequencies above 3 Hz [17]. The transmission frequencies of the oscillatory wave flow may vary from 5 to 15 Hz, equivalent to a range from 300 to 900 acts/minute, through a small tidal volume which oscillates between 1 – 3 ml/kg [18,19]. Through lung recruitment, the use of small tidal volumes reduces the incidence of atelectrauma determined by the process of opening and closing of the alveoli made by conventional ventilation, reducing the incidence of both volotrauma and barotrauma contemporarily [18,19]. The positive and negative deflections of the flow created by the oscillation lead to a fusion between the inspiratory and expiratory phases, which occur simultaneously. During conventional mechanical ventilation, gas transfer occurs by mass transport of gas molecules from the large central airways to the smaller peripheral airways. This requires the tidal volume to be greater than dead space ventilation. During HFOV this is not possible because the current ventilation delivered is less than the dead space [15,19,20]. Compared to conventional ventilation, the transport of gas in oscillatory ventilation occurs with a very different dynamic which involves the participation of multiple mechanisms simultaneously [21]. A well-known mechanism for gas transfer in HFOV is convective mass transfer, which may contribute to gas exchange in the proximal airways although it plays only a minor role in peripheral gas exchange [15,19,20]. Turbulence is another method of gas transfer, especially in larger airways. In this case, the different velocity profiles of the various asymmetric particles will lead to a net convective transport (Figure 1).
This mode of gas exchange is most often observed in the bifurcation of the airways [15,19,20]. Taylor’s dispersion and molecular diffusion are one of the most essential mechanisms of gas exchange during HFOV [15,21]. Other mechanisms described include the Pendelluft effect, cardiogenic mixing and collateral ventilation [15,21]. Oscillatory ventilation is a rescue therapy in multiple clinical conditions such as refractory hypoxemia, severe “air leak” syndromes and cardiovascular failure [22,23,24].
3. Indications and Contraindications
There are many indications, contraindications and risks in the use of HFOV, as shown in Table 1.
For instance, HFOV is advantageous for patients with severe respiratory failure where conventional ventilation is set to parameters that can induce volotrauma, barotrauma and atelectrauma [1,3,15,25,26,27]. Oscillatory ventilation is advantageous in patients affected by Ventilation Induced Lung Injury (VILI) and ARDS [25,26,27]. Among newborns, HFOV is indicated for patients with neonatal air leak syndrome, persistent pulmonary hypertension, and meconium aspiration [18,28]. Even though there are no specific contraindications in the use of HFOV, however it is mandatory to consider any possible side effects. Increased airway resistance, hyperinflation and air-trapping must be considered as source of potential damage to the patient [8,9]. Therefore, aggressive ventilation parameters can determine lungs hyperinflation and hesitate in barotrauma, pneumomediastinum, pneumothorax, pneumopericardium and interstitial pulmonary emphysema as natural complications [8,9]. HFOV can reduce venous return, cardiac output, cause intraventricular hemorrhage due to the increase in intrathoracic positive pressure potentially worsening the hemodynamic status of the patient [6,7]. During oscillatory ventilation prolonged intubation might be required increasing the risk of infectious complications and length of stay in ICU [8]. Furthermore, it is essential to consider that the transportation of the patient is impossible and, because of the noisy piston pump, carrying out the clinical examination to detect any complications might be very difficult [1]. Airways aspiration maneuver could reveal changeling because of the strong alveolar de-recruitment. It is mandatory for the clinician to establish previously the methods and times based on the clinical condition of the patient [29]. The presence of plugs or mucous secretions could obstruct airways and hinder a correct thoracic oscillation compelling the clinician to practice suctioning maneuvers [24,30]. The use of a closed circuit for aspiration does not prevent alveolar de-recruitment. To maintain optimal alveolar function after a procedure, the clinician should resume performing ventilation while incorporating post-procedural recruitment maneuvers. These maneuvers are crucial for reopening and keeping alveolar structures expanded, ensuring adequate gas exchange and preventing atelectasis [3,30,31]. The disconnection of the patient from the ventilator should only be done if necessary [32].
4. Ventilator Settings
Figure 2 shows an example of ventilator that might be used for HFOV.
The most common technique for establishing initial ventilator settings is to start with a MAP between a range of 2-3 cmH2O above the mean airway pressure in conventional ventilation and a frequency between 10-12 Hz based on the age of the patient leaving the other parameters stable. Therefore, after determining the MAP and rate, the power APproximal setting is set between 70 and 90 cmH2O and the bias flow is typically 20 to 40 L/min with an inspiratory time of 33% [12]. There are no specific indications in the literature on the management of ventilatory settings, but the most common is the "open lung strategy" which is based on the judicious titration of MAP. The procedure consists of a progressive increase of 2 cmH2O on the MAP knob, evaluating the SpO2 every 2-3 minutes until there is no more gain in terms of peripheral saturation value. This pressure corresponds to “hyperinflation pressure”. Next, the knob is turned down by 2 cmH2O until the SpO2 decreases. The level of MAP obtained corresponds now to "de-recruitment pressure". Subsequently, the knob is raised by 2 cmH2O above the "de-recruitment pressure" obtaining the optimal MAP [33]. It is mandatory to check that the lungs are not hyperinflated with a chest x-ray or ultrasound: the lower edge must not exceed the ninth rib [34]. Furthermore, it is essential for the clinician to evaluate the stability of the patient's hemodynamic conditions. The other parameters must be adjusted reaching at least SpO2 value between 88-92% with a pH ≥ 7.20 tolerating permissive hypercapnia [12].
5. HFOV in Newborns and Children with Heart Disease
The main doubts regarding the use of HFOV concern the possible hemodynamic impact that this mode ventilation may have on children with congenital heart disease. Although, there is no evidence in the literature to imagine that this ventilation mode can be used in the same conditions that can occur in patients not affected by congenital pathologies [26,35,36]. Numerous clinical studies have demonstrated that the perception of the hemodynamic impact of HFOV is often overrated, both in normal and congenital heart disease populations. The actual impact on hemodynamics is frequently less significant than initially perceived. [37,38,39,40,41,42]. Two clinical studies conducted on a pediatric population showed how cardiac output was reduced when switching from conventional ventilation to HFOV in patients with ARDS, but they were very small single-center studies, composed of small preterm populations and in one of them the blood pressure was measured noninvasively [43,44]. Fort et al., in a study on an adult population, found an increase in pulmonary wedge pressure without significant alterations on other hemodynamic parameters such as cardiac output [45]. Clinical studies in adult populations have demonstrated that when switching from conventional ventilation to oscillatory ventilation in patients with ARDS, there is a significant increase in pulmonary wedge pressure and central venous pressure, without changes in heart rate, blood pressure and cardiac output [26,35]. Similar results have been found in studies on pediatric populations [41,42]. It was seen by Gutiérrez et al. in a single patient that a possible reduction in cardiac output and cardiac index may occur in the recruitment phase indicating possible alveolar overdistention, instead Goodman et al. observed an improvement in hemodynamic parameters such as cardiac index, cardiac output and oxygen transport accompanied only by a slight reduction in heart rate. This possible effect was explained by two contemporary mechanisms: the reduction of paCO2 and the reduction of transthoracic impedance. Correction of hypercapnia-induced acidosis and reduction of cardiac afterload improved patients' cardiovascular performance on both fronts [41,42]. While clinical studies on the hemodynamic effects of oscillatory ventilation in the pediatric population are rare, those on the pediatric population affected by congenital or acquired heart disease are even rarer. De Jager et al. recently conducted a retrospective analysis on 52 patients suffering from congenital and/or acquired heart disease with respiratory failure: no significant changes in hemodynamic parameters such as heart rate, blood pressure, central venous pressure and lactate level were measured. No significant changes were detected in the number of fluid boluses made when switching from one ventilatory mode to another, nor significant alterations in the administration of vasoactive drugs. Furthermore, an improvement in respiratory parameters such as paCO2 and paO2 was detected, associated with a simultaneous significant reduction in the dosage of muscle relaxants without any significant change in the dosage of sedatives. This monocentric and retrospective study is the only one in the literature that aims to analyze the hemodynamic effects of HFOV in this peculiar population of pediatric patients. It should also be underlined that the inclusion criteria were established not by considering clinical parameters, but by considering ventilatory parameters. The transition from the conventional to the oscillatory ventilation mode was carried out by adopting a protocol that was determined by the achievement of harmful ventilatory parameters, this was a cut off to use the HFOV regardless of the clinical condition and the underlying cardiac pathology. In this way it was possible to observe the effects of this ventilation mode on patients suffering from cardiac pathologies, including acquired or congenital ones [12]. HFOV has been used profitably in the treatment of post-cardiopulmonary bypass ARDS for more than a decade now [11,13,37,40,46,47,48]. Oscillatory ventilation has been shown to improve oxygen index, PaO2/FiO2 ratio, blood alveolar-arterial oxygen concentration gap, dynamic lung compliance, PaO2, PaCO2, pH, resulting in a positive impact on patient survival [13,40,48,49]. HFOV proved to be beneficial in controlling the production of inflammatory mediators during ARDS. Zheng et al. demonstrated that the use of oscillatory ventilation with protective parameters mixed with the “volume guaranteed” mode led to a significant improvement in the panel of proinflammatory mediators such as IL-6, IL-8 and TNF-α that are produced during the inflammatory response in ARDS. The reduction of these activators improved the blood gas analysis parameters significantly with a decrease in days of post-operative mechanical ventilation [50]. Oscillatory ventilation also represents a valuable aid in the treatment of pulmonary hypertension in cardiac newborns. The use of HFOV and inhaled nitric oxide therapy is now a consolidated therapeutic option for neonatal pulmonary hypertension. Its use is also finding its place in the pediatric population affected by congenital heart disease [39,50,51]. Huang et al. have demonstrated that, as in patients suffering from cardiac congenital disease, oscillatory ventilation associated with nitric oxide is a concrete and safe therapeutic option in the treatment of post-cardiac surgery pulmonary hypertension improving blood gas analysis parameters while determining a significant reduction in the days of post-operative mechanical ventilation [39].
6. Conclusions
Oscillatory ventilation has a role as a clinical option also in pediatric patients suffering from congenital heart disease. So far, there are no double-blind randomized controlled trials that prove its superiority over conventional ventilation in the clinical conditions for which it is indicated. Retrospective analyses have shown that it can also have a beneficial role in the treatment of pathologies such as ARDS and pulmonary hypertension in the pediatric population affected by congenital heart diseases. Given the rarity of this type of population, as well as the prejudice around this ventilatory modality, its diffusion is still limited. However, although rare and limited by the small size of the samples and by the prevalence of single-center retrospective studies, all publications for more than a decade have highlighted the benefit of HFOV in the pediatric population affected by congenital heart disease.
7. Future Directions
The future of HFOV in pediatric patients, particularly those with congenital heart disease, hinges on further rigorous research and refinement of clinical practices. While existing retrospective studies indicate that HFOV can be beneficial, there is a critical need for well-designed, multicentric, randomized controlled trials to establish robust evidence of its efficacy and safety compared to conventional ventilation. Research should focus on optimizing HFOV settings to minimize potential hemodynamic impacts and complications such as barotrauma and pneumothorax. Additionally, exploring the synergistic effects of combining HFOV with other therapeutic modalities, such as inhaled nitric oxide, could provide new avenues for enhancing patient outcomes. Future studies should also aim to develop tailored protocols that account for the unique physiological and pathological conditions in pediatric patients with congenital heart disease. Furthermore, advancements in technology and ventilator design could help mitigate some of the current limitations associated with HFOV, such as difficulties in clinical examination and airway management. By addressing these research gaps, we can better define the role of HFOV in treating severe respiratory conditions in this vulnerable patient population and potentially broaden its application in critical care settings.
Author Contributions
Conceptualization, S.S. and C.M.; methodology, L.L.V.; data curation, P.P.; writing—original draft preparation, S.S., L.L.V and C.M.; writing—review and editing, P.P., M.P. and G.C.; supervision, G.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created for this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Facchin, F.; Fan, E. Airway Pressure Release Ventilation and High-Frequency Oscillatory Ventilation: Potential Strategies to Treat Severe Hypoxemia and Prevent Ventilator-Induced Lung Injury. Respir Care 2015, 60, 1509-1521. [CrossRef]
- Sessler, C.N. Sedation, analgesia, and neuromuscular blockade for high-frequency oscillatory ventilation. Crit Care Med 2005, 33, S209-216. [CrossRef]
- Fessler, H.E.; Hess, D.R. Respiratory controversies in the critical care setting. Does high-frequency ventilation offer benefits over conventional ventilation in adult patients with acute respiratory distress syndrome? Respir Care 2007, 52, 595-605; discussion 606-598.
- Burry, L.D.; Seto, K.; Rose, L.; Lapinsky, S.C.; Mehta, S. Use of sedation and neuromuscular blockers in critically ill adults receiving high-frequency oscillatory ventilation. Ann Pharmacother 2013, 47, 1122-1129. [CrossRef]
- Gupta, P.; Green, J.W.; Tang, X.; Gall, C.M.; Gossett, J.M.; Rice, T.B.; Kacmarek, R.M.; Wetzel, R.C. Comparison of high-frequency oscillatory ventilation and conventional mechanical ventilation in pediatric respiratory failure. JAMA Pediatr 2014, 168, 243-249. [CrossRef]
- Squires, K.A.; De Paoli, A.G.; Williams, C.; Dargaville, P.A. High-frequency oscillatory ventilation with low oscillatory frequency in pulmonary interstitial emphysema. Neonatology 2013, 104, 243-249. [CrossRef]
- Bollen, C.W.; van Well, G.T.; Sherry, T.; Beale, R.J.; Shah, S.; Findlay, G.; Monchi, M.; Chiche, J.D.; Weiler, N.; Uiterwaal, C.S.; et al. High frequency oscillatory ventilation compared with conventional mechanical ventilation in adult respiratory distress syndrome: a randomized controlled trial [ISRCTN24242669]. Crit Care 2005, 9, R430-439. [CrossRef]
- Briggs, S.; Goettler, C.E.; Schenarts, P.J.; Newell, M.A.; Sagraves, S.G.; Bard, M.R.; Toschlog, E.A.; Rotondo, M.F. High-frequency oscillatory ventilation as a rescue therapy for adult trauma patients. Am J Crit Care 2009, 18, 144-148. [CrossRef]
- Mehta, S.; Lapinsky, S.E.; Hallett, D.C.; Merker, D.; Groll, R.J.; Cooper, A.B.; MacDonald, R.J.; Stewart, T.E. Prospective trial of high-frequency oscillation in adults with acute respiratory distress syndrome. Crit Care Med 2001, 29, 1360-1369. [CrossRef]
- Meliones, J.N.; Bove, E.L.; Dekeon, M.K.; Custer, J.R.; Moler, F.W.; Callow, L.R.; Wilton, N.C.; Rosen, D.B. High-frequency jet ventilation improves cardiac function after the Fontan procedure. Circulation 1991, 84, Iii364-368.
- Bojan, M.; Gioanni, S.; Mauriat, P.; Pouard, P. High-frequency oscillatory ventilation and short-term outcome in neonates and infants undergoing cardiac surgery: a propensity score analysis. Crit Care 2011, 15, R259. [CrossRef]
- de Jager, P.; Curley, M.A.Q.; Cheifetz, I.M.; Kneyber, M.C.J. Hemodynamic Effects of a High-Frequency Oscillatory Ventilation Open-Lung Strategy in Critically Ill Children With Acquired or Congenital Cardiac Disease. Pediatr Crit Care Med 2023, 24, e272-e281. [CrossRef]
- Zheng, Y.R.; Xie, W.P.; Liu, J.F.; Wu, H.L.; Xu, N.; Huang, S.T.; Cao, H.; Chen, Q. Application of high-frequency oscillation ventilation combined with volume guarantee in infants with acute hypoxic respiratory failure after congenital heart surgery. Pediatr Pulmonol 2021, 56, 2621-2626. [CrossRef]
- Fan, E.; Brodie, D.; Slutsky, A.S. Acute Respiratory Distress Syndrome: Advances in Diagnosis and Treatment. Jama 2018, 319, 698-710. [CrossRef]
- Pillow, J.J. High-frequency oscillatory ventilation: mechanisms of gas exchange and lung mechanics. Crit Care Med 2005, 33, S135-141. [CrossRef]
- John, J.; Harcourt, E.R.; Davis, P.G.; Tingay, D.G. Dräger VN500's oscillatory performance has a frequency-dependent threshold. J Paediatr Child Health 2014, 50, 27-31. [CrossRef]
- Keszler, M., Pillow, J. J., and Courtney, S. E. Pediatric and Neonatal Mechanical Ventilation.; Springer: New York, 2015.
- Rettig, J.S.; Smallwood, C.D.; Walsh, B.K.; Rimensberger, P.C.; Bachman, T.E.; Bollen, C.W.; Duval, E.L.; Gebistorf, F.; Markhorst, D.G.; Tinnevelt, M.; et al. High-Frequency Oscillatory Ventilation in Pediatric Acute Lung Injury: A Multicenter International Experience. Crit Care Med 2015, 43, 2660-2667. [CrossRef]
- Miller, A.G.; Bartle, R.M.; Feldman, A.; Mallory, P.; Reyes, E.; Scott, B.; Rotta, A.T. A narrative review of advanced ventilator modes in the pediatric intensive care unit. Transl Pediatr 2021, 10, 2700-2719. [CrossRef]
- Miller, A.G.; Bartle, R.M.; Rehder, K.J. High-Frequency Jet Ventilation in Neonatal and Pediatric Subjects: A Narrative Review. Respir Care 2021, 66, 845-856. [CrossRef]
- Slutsky, A.S.; Drazen, F.M.; Ingram, R.H., Jr.; Kamm, R.D.; Shapiro, A.H.; Fredberg, J.J.; Loring, S.H.; Lehr, J. Effective pulmonary ventilation with small-volume oscillations at high frequency. Science 1980, 209, 609-671. [CrossRef]
- Ng, J.; Ferguson, N.D. High-frequency oscillatory ventilation: still a role? Curr Opin Crit Care 2017, 23, 175-179. [CrossRef]
- Aurilia, C.; Ricci, C.; Tana, M.; Tirone, C.; Lio, A.; Gambacorta, A.; Paladini, A.; Vento, G. Management of pneumothorax in hemodynamically stable preterm infants using high frequency oscillatory ventilation: report of five cases. Ital J Pediatr 2017, 43, 114. [CrossRef]
- Jarvis S, B.M., English W. High frequency oscillatory ventilation. Anaesthesia Tutorial of the Week. 2012, 261: 261–211.
- Clark, R.H.; Gerstmann, D.R.; Null, D.M., Jr.; deLemos, R.A. Prospective randomized comparison of high-frequency oscillatory and conventional ventilation in respiratory distress syndrome. Pediatrics 1992, 89, 5-12.
- Derdak, S.; Mehta, S.; Stewart, T.E.; Smith, T.; Rogers, M.; Buchman, T.G.; Carlin, B.; Lowson, S.; Granton, J. High-frequency oscillatory ventilation for acute respiratory distress syndrome in adults: a randomized, controlled trial. Am J Respir Crit Care Med 2002, 166, 801-808. [CrossRef]
- Vincent, J.L. High-Frequency Oscillation in Acute Respiratory Distress Syndrome. The End of the Story? Am J Respir Crit Care Med 2017, 196, 670-671. [CrossRef]
- Imai, Y.; Nakagawa, S.; Ito, Y.; Kawano, T.; Slutsky, A.S.; Miyasaka, K. Comparison of lung protection strategies using conventional and high-frequency oscillatory ventilation. J Appl Physiol (1985) 2001, 91, 1836-1844. [CrossRef]
- Johnson, A.H.; Peacock, J.L.; Greenough, A.; Marlow, N.; Limb, E.S.; Marston, L.; Calvert, S.A. High-frequency oscillatory ventilation for the prevention of chronic lung disease of prematurity. N Engl J Med 2002, 347, 633-642. [CrossRef]
- AARC Clinical Practice Guidelines. Endotracheal suctioning of mechanically ventilated patients with artificial airways 2010. Respir Care 2010, 55, 758-764.
- Ferguson, N.D.; Chiche, J.D.; Kacmarek, R.M.; Hallett, D.C.; Mehta, S.; Findlay, G.P.; Granton, J.T.; Slutsky, A.S.; Stewart, T.E. Combining high-frequency oscillatory ventilation and recruitment maneuvers in adults with early acute respiratory distress syndrome: the Treatment with Oscillation and an Open Lung Strategy (TOOLS) Trial pilot study. Crit Care Med 2005, 33, 479-486. [CrossRef]
- Stawicki, S.P.; Goyal, M.; Sarani, B. High-frequency oscillatory ventilation (HFOV) and airway pressure release ventilation (APRV): a practical guide. J Intensive Care Med 2009, 24, 215-229. [CrossRef]
- de Jager, P.; Kamp, T.; Dijkstra, S.K.; Burgerhof, J.G.M.; Markhorst, D.G.; Curley, M.A.Q.; Cheifetz, I.M.; Kneyber, M.C.J. Feasibility of an alternative, physiologic, individualized open-lung approach to high-frequency oscillatory ventilation in children. Ann Intensive Care 2019, 9, 9. [CrossRef]
- Sahin, O.; Colak, D.; Tasar, S.; Yavanoglu Atay, F.; Guran, O.; Mungan Akin, I. Point-of-Care Ultrasound versus Chest X-Ray for Determining Lung Expansion Based on Rib Count in High-Frequency Oscillatory Ventilation. Neonatology 2023, 120, 736-740. [CrossRef]
- Mehta, S.; Granton, J.; MacDonald, R.J.; Bowman, D.; Matte-Martyn, A.; Bachman, T.; Smith, T.; Stewart, T.E. High-frequency oscillatory ventilation in adults: the Toronto experience. Chest 2004, 126, 518-527. [CrossRef]
- Roosens, C.D.; Ama, R.; Leather, H.A.; Segers, P.; Sorbara, C.; Wouters, P.F.; Poelaert, J.I. Hemodynamic effects of different lung-protective ventilation strategies in closed-chest pigs with normal lungs. Crit Care Med 2006, 34, 2990-2996. [CrossRef]
- Li, S.; Wang, X.; Li, S.; Yan, J. High-frequency oscillatory ventilation for cardiac surgery children with severe acute respiratory distress syndrome. Pediatr Cardiol 2013, 34, 1382-1388. [CrossRef]
- Ayoub, D.; Elmashad, A.; Rowisha, M.; Eltomey, M.; El Amrousy, D. Hemodynamic effects of high-frequency oscillatory ventilation in preterm neonates with respiratory distress syndrome. Pediatr Pulmonol 2021, 56, 424-432. [CrossRef]
- Huang, S.T.; Lei, Y.Q.; Xie, W.P.; Zheng, Y.R.; Chen, Q.; Cao, H. Effect of postoperative administration of inhaled nitric oxide combined with high-frequency oscillatory ventilation in infants with acute hypoxemic respiratory failure and pulmonary hypertension after congenital heart surgery: A retrospective cohort study. J Card Surg 2022, 37, 545-551. [CrossRef]
- Zheng, Y.R.; Lin, S.H.; Chen, Y.K.; Cao, H.; Chen, Q. Rescue high-frequency oscillatory ventilation combined with intermittent mandatory ventilation for infants with acute respiratory distress syndrome after congenital heart surgery. Cardiol Young 2023, 33, 1165-1171. [CrossRef]
- Goodman, A.M.; Pollack, M.M. Hemodynamic effects of high-frequency oscillatory ventilation in children. Pediatr Pulmonol 1998, 25, 371-374. [CrossRef]
- Gutiérrez, J.A.; Levin, D.L.; Toro-Figueroa, L.O. Hemodynamic effects of high-frequency oscillatory ventilation in severe pediatric respiratory failure. Intensive Care Med 1995, 21, 505-510. [CrossRef]
- Simma, B.; Fritz, M.; Fink, C.; Hammerer, I. Conventional ventilation versus high-frequency oscillation: hemodynamic effects in newborn babies. Crit Care Med 2000, 28, 227-231. [CrossRef]
- Laubscher, B.; van Melle, G.; Fawer, C.L.; Sekarski, N.; Calame, A. Haemodynamic changes during high frequency oscillation for respiratory distress syndrome. Arch Dis Child Fetal Neonatal Ed 1996, 74, F172-176. [CrossRef]
- Fort, P.; Farmer, C.; Westerman, J.; Johannigman, J.; Beninati, W.; Dolan, S.; Derdak, S. High-frequency oscillatory ventilation for adult respiratory distress syndrome--a pilot study. Crit Care Med 1997, 25, 937-947. [CrossRef]
- Kneyber, M.C. High-frequency oscillatory ventilation and pediatric cardiac surgery: yes, we can! Crit Care 2011, 15, 1011. [CrossRef]
- Tripathi, R.S.; Stein, E.J.; Crestanello, J.A.; Papadimos, T.J. High-frequency oscillatory ventilation after cardiac surgery: a treatment for all ages. Crit Care 2012, 16, 405. [CrossRef]
- Kumar, A.; Joshi, A.; Parikh, B.; Tiwari, N.; Ramamurthy, R.H. High-frequency oscillatory ventilation for respiratory failure after congenital heart surgery: a retrospective analysis. Anaesthesiol Intensive Ther 2023, 55, 60-67. [CrossRef]
- Zheng, Y.R.; Chen, Y.K.; Lin, S.H.; Cao, H.; Chen, Q. Effect of High-Frequency Oscillatory Ventilation, Combined With Prone Positioning, in Infants With Acute Respiratory Distress Syndrome After Congenital Heart Surgery: A Prospective Randomized Controlled Trial. J Cardiothorac Vasc Anesth 2022, 36, 3847-3854. [CrossRef]
- Bizzarro, M.; Gross, I. Inhaled nitric oxide for the postoperative management of pulmonary hypertension in infants and children with congenital heart disease. Cochrane Database Syst Rev 2005, Cd005055. [CrossRef]
- Bizzarro, M.; Gross, I.; Barbosa, F.T. Inhaled nitric oxide for the postoperative management of pulmonary hypertension in infants and children with congenital heart disease. Cochrane Database Syst Rev 2014, Cd005055. [CrossRef]
Figure 1.
Gas Transport Mechanisms During High Frequency Oscillatory Ventilation (HFOV). Adapted from references: (Slutsky and Drazen, 2002; Pillow, 2005).
Figure 1.
Gas Transport Mechanisms During High Frequency Oscillatory Ventilation (HFOV). Adapted from references: (Slutsky and Drazen, 2002; Pillow, 2005).
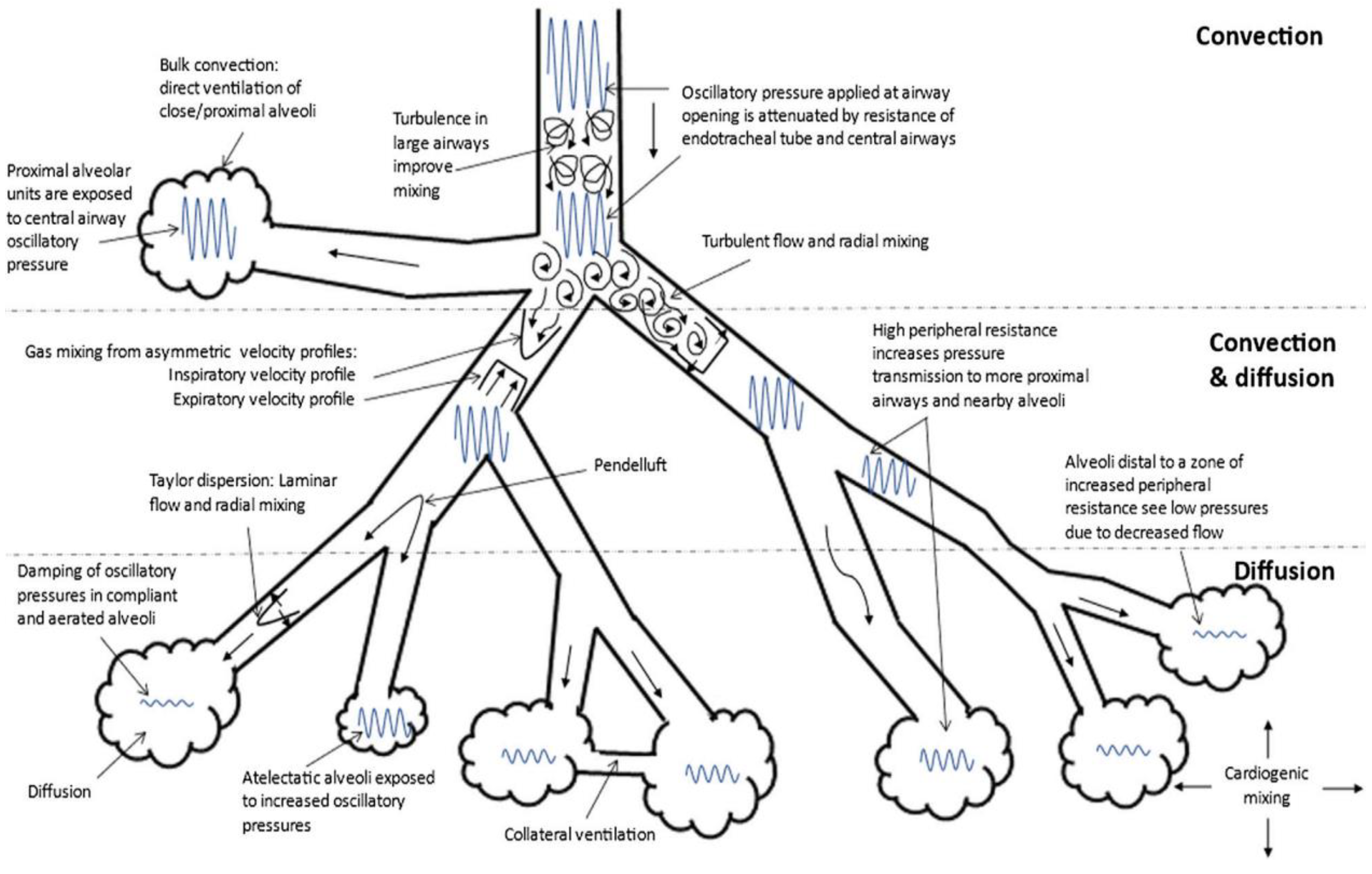
Figure 2.
Example of ventilator with HFOV modality.
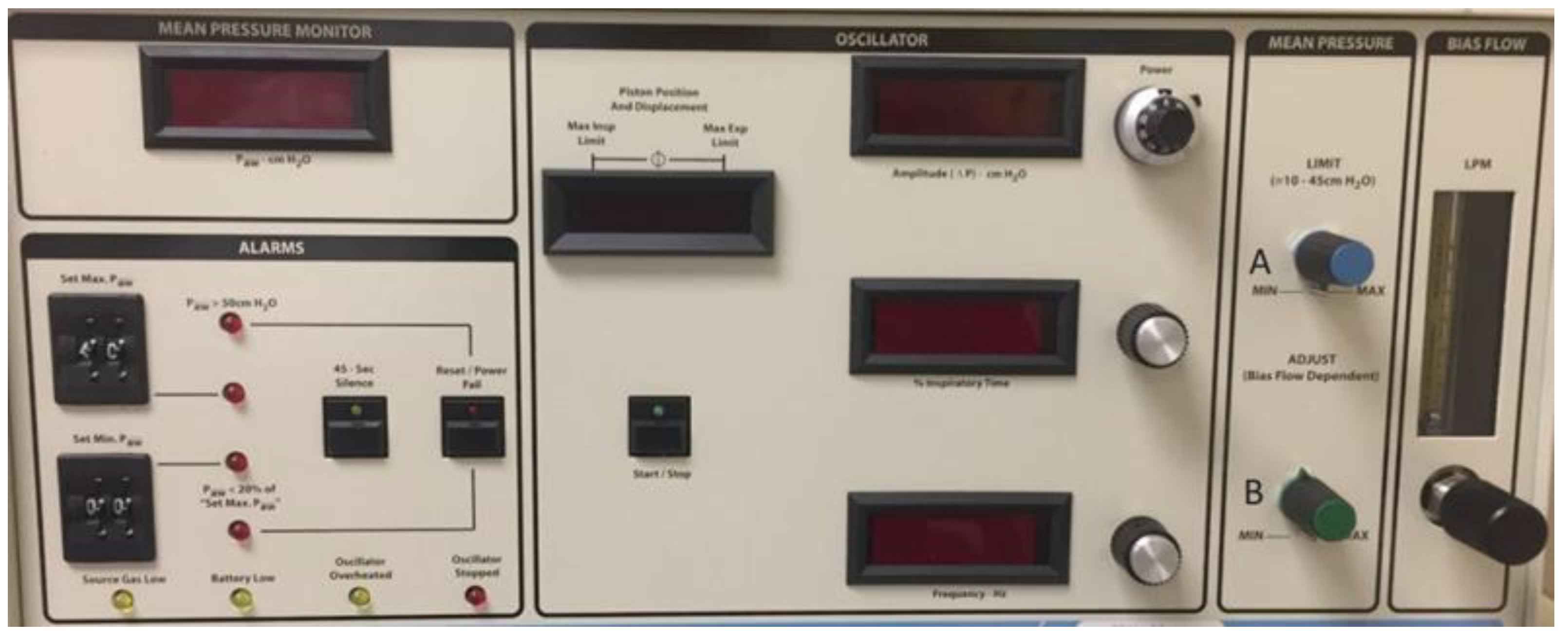

Table 1.
Indications and contraindications of HFOV.
| INDICATIONS | CONTRAINDICATIONS |
|---|---|
| Pulmonary issues | Pulmonary/thoracic complications |
|
|
| Cardiovascular diseases | Cardiovascular contraindications |
|
|
| Possible indications | Other contraindication |
|
|
ARDS: Acute Respiratory Distress Syndrome; ET: Endotracheal tube.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



