
Submitted:
15 August 2024
Posted:
19 August 2024
You are already at the latest version
Abstract
Rift Valley fever (RVF) is a mosquito-borne zoonotic viral disease that infects both human and animals. This is a descriptive study summarizes investigation and response to RVF outbreak, using surveillance data. A RVF outbreak occurred in Berber locality in northern Sudan. We identified 246 cases of RVF including seven deaths among humans, 119 deaths and 82 abortions among Livestock. Our entomological surveillance confirmed the presence of Anopheles arabiensis, An. stephensi, Aedes aegypti, Ae. vexans, Culex pipiens, Cx. Quinquefasciatus, and Cx. theileri in the area during the outbreak. In a comparison with another outbreak of Rift Valley fever in nearby area while ago, a multisectoral One Health response strategy has resulted in strengthening the health system through re-innovating health facilities and centres and training about 200 healthcare and emergency responders. Additionally, it reduced cases and fatalities among humans by 78% and 63%, respectively, and loss in livestock due to deaths and/or abortions by 82%. The added-value of implementing One Health strategy was saving more lives and resources, while strengthening the health system. We recommend the systematic institutionalization of One Health strategy in the country as a core part of the national prevention and control strategy for zoonotic diseases epidemics and pandemics.
Keywords:
Zoonotic diseases
; Arboviruses
; Emerging Infectious Disease
; Epidemic
; Epizootic
; Haemorrhagic fevers
; Health security
; Pandemic preparedness
; prevention and response
1. Introduction
Arthropod-borne viruses (arboviruses) are group of viruses that are transmitted by diseases vectors, mainly mosquitoes, biting midges, sand flies, and ticks [1,2]. Most of arboviral diseases are zoonotic in nature, therefore they are readily causing a life-threatening illness to humans and animals, as well as reduction in meat and milk production by livestock leading to substantial health and socioeconomic burdens [3,4,5,6]. Arboviral diseases such as Rift Valley fever (RFV) are mainly emerging in form of health emergencies including epidemics among humans, epizootic among animals, or outbreaks that affect both human and animal populations [7,8,9,10]. These health emergencies usually overtaking health systems, particularly in under-resourced settings that lack early preparedness and response systems [11,6,12]. The geographical distribution, prevalence, morbidity, mortality, and related disability and socioeconomic burden of arboviral diseases are increasingly growing [8,13,14]. This growth is mainly driven by several risk factors including climate change, growing size of populations living in humanitarian crisis settings, change in land use and land cover, globalization, and unplanned urbanization [15,16,17,18,19,20,21].
Sudan is located in Northeastern Africa and has open borders with seven countries including Chad, Central African Republic, and Libya in the west, Egypt in north, South Sudan in south, and Eritrea and Ethiopia toward the east. Due to the large coastal area on the Red Sea, the country is considered one of the main coastal gates of Africa; therefore, there is high international travel and transportation dynamics of human and animals’ populations as well as goods. Additionally, due to the geo-political position and wide space, the country has a wide range of diversity in ecological zones, environmental suitability, disease vectors, and alternative hosts. Therefore, these characteristic altogether make Sudan an epidemic-prone country, particularly, for haemorrhagic fevers including RFV [12]. Furthermore, Sudan is endemic with several arboviral diseases including Chikungunya (CHIK) [22,23], Crimean-Congo haemorrhagic fever (CCHF) [5], dengue (DEN) [20], RVF [8], Zika and West Nile viruses [6]. RVF is endemic in the southern and central regions of Sudan and serological evidence about the local circulation of the virus there goes back to 1936 [24]. The disease has affected both human and animal populations in the country [25,26,27,28].
In this study, we report on the investigation and response to an outbreak of RVF in Berber locality, northern Sudan and highlight the added value of implementing One Health approach for the containment and control of the outbreak. We document best practices, success story, and we recommend additional measures to improve the prevention and control of RVF outbreaks.
2. Materials and Methods
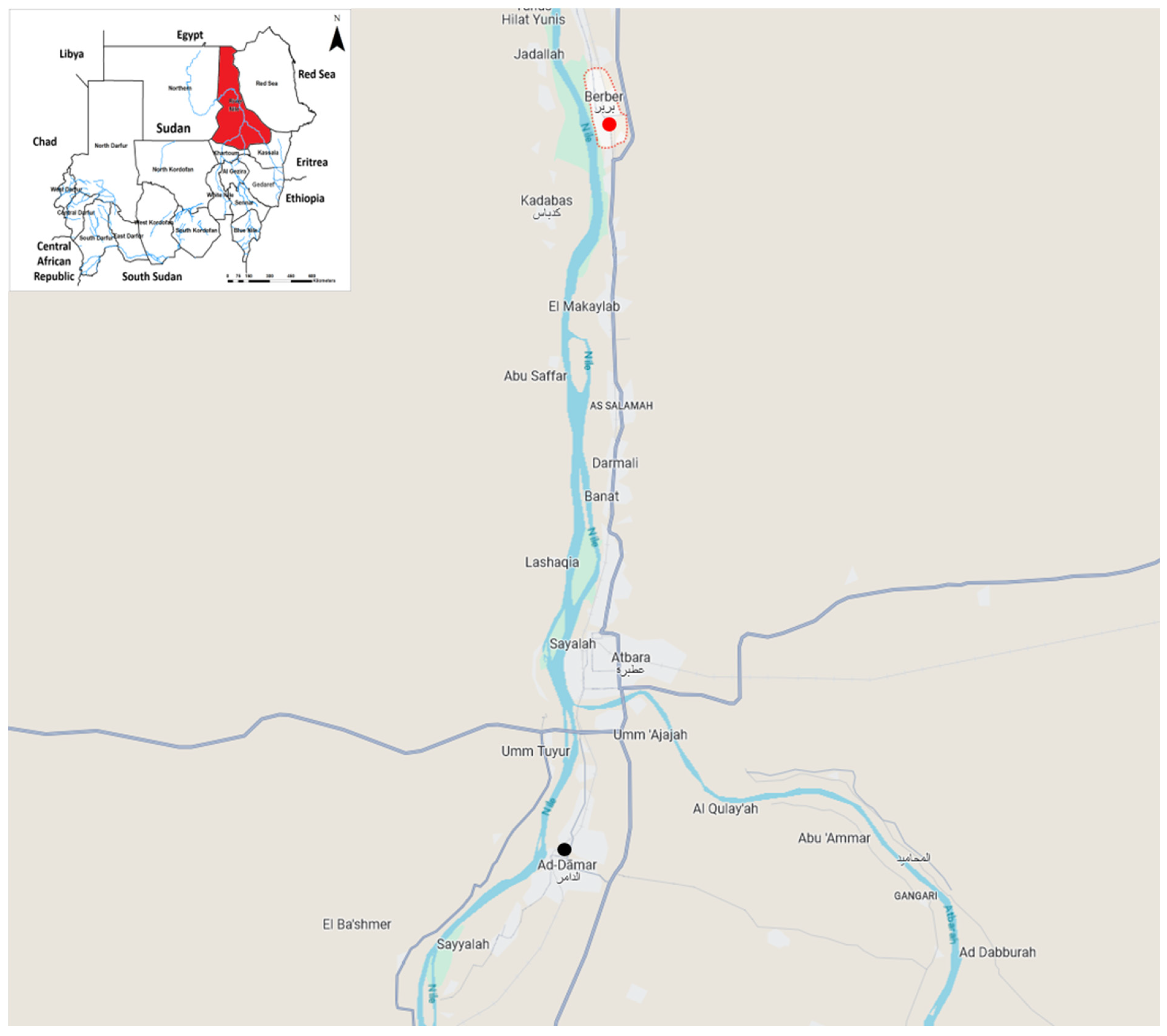
Here we analysed secondary anonymised data that was extracted from the outbreak report. Data was collected through the surveillance system. Additionally, we are documenting practices and actions were implemented throughout the investigation and response to the RVF outbreak in the area. In brief, in response to health alerts from the human and animal health authorities in Berber locality (Fig. 1), about unusual increase in non-malaria febrile illness among humans associated with high rate of abortion and deaths among livestock in September 2019, an emergency taskforce was deployed for investigation. This team was technically and logistically supported by the World Health Organization (WHO) to investigate a suspect epidemic of haemorrhagic fever in the area. Diagnostic analyses at the reference National Public Health Laboratory in Khartoum confirmed infections with RVFV among humans. Similarly, Central Veterinary Research Laboratory has confirmed infections with RVF were confirmed among livestock. The Integrated Vectors Management department at the directorate of Environmental Health and Food Control; Federal Ministry of Health has implemented additional investigations to determine the vector composition in Berber locality during the outbreak.
Figure 1.
Map indicates the study area highlighted with red sphere, and the place where the previous outbreak of RVF occurred marked with the black sphere.
Figure 1.
Map indicates the study area highlighted with red sphere, and the place where the previous outbreak of RVF occurred marked with the black sphere.
3. Results
3.1. Literature analysis:
The history of the epidemic in the area was established retrospectively by reviewing and analysing the epidemiological records and previous reports about similar health events in the area. This revealed that RVF virus has emerged in the capital city of the state; Eldamar locality (Fig. 1) over two month ago [7].
Upon increase in reported non-malaria febrile illness among humans and the local people reported increase in mortality and abortions among their domestic animals, sheep and goats in particular, investigations confirmed the emergence of RVF in the area (Table 1).
3.2. The outbreak:
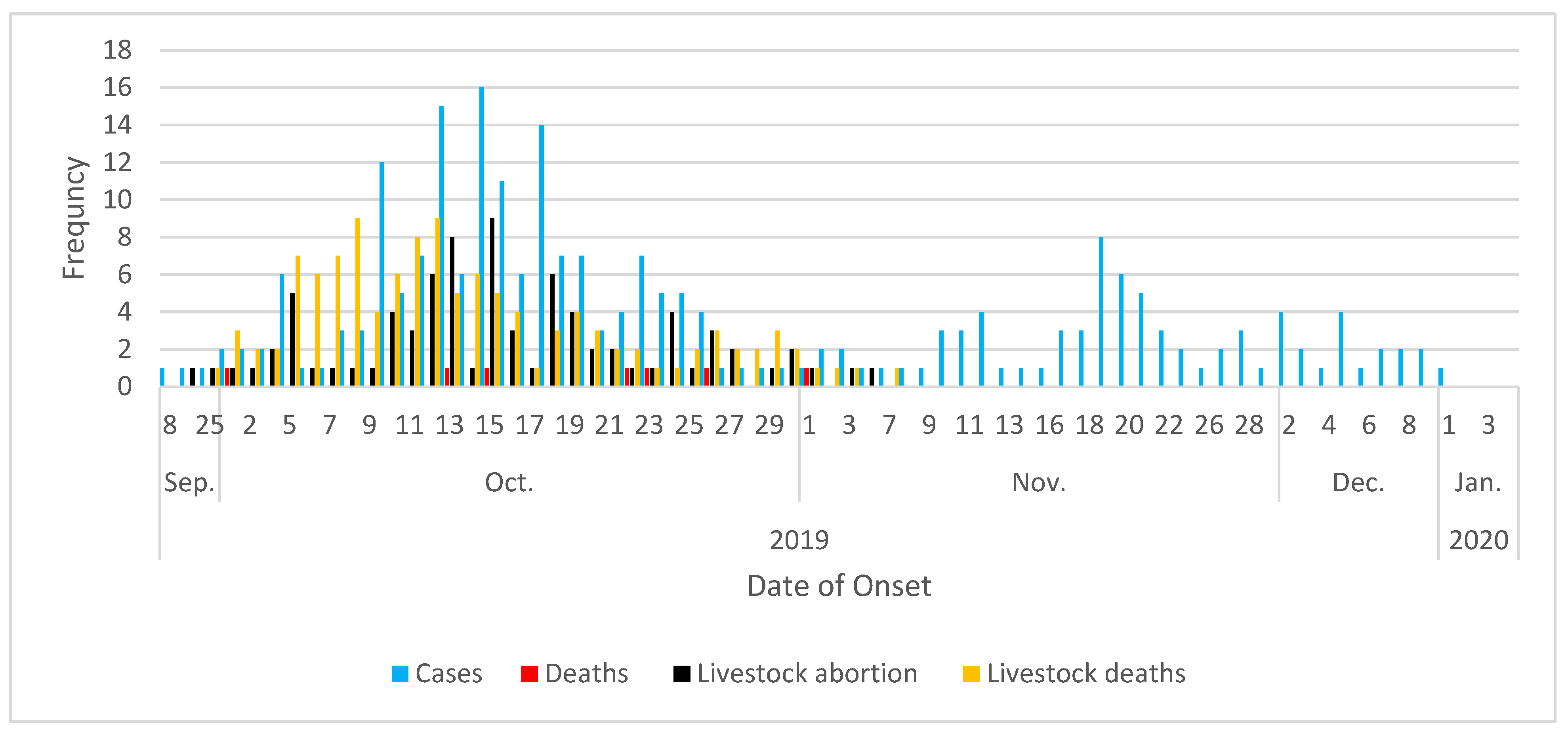
The development of this outbreak has started with the first index case that was reported in Berber locality on September 8th through January 1st 2020. In total, among humans, we identified 246 cases of RVF infection including seven deaths (Fig. 1). Additionally, 119 deaths and 82 abortions were reported among Livestock (Fig. 2). The outbreak peaked in October with 64% of cases and 86% of deaths among human were reported, also 96% and 94% of animal deaths and abortions respectively were reported during the same period (Fig. 2).
Figure 2.
Epicurve of RVF outbreak in Berber locality shows the temporal distribution of cases and deaths among humans as well as abortions and deaths among livestock between September 2019 and January 2020.
Figure 2.
Epicurve of RVF outbreak in Berber locality shows the temporal distribution of cases and deaths among humans as well as abortions and deaths among livestock between September 2019 and January 2020.
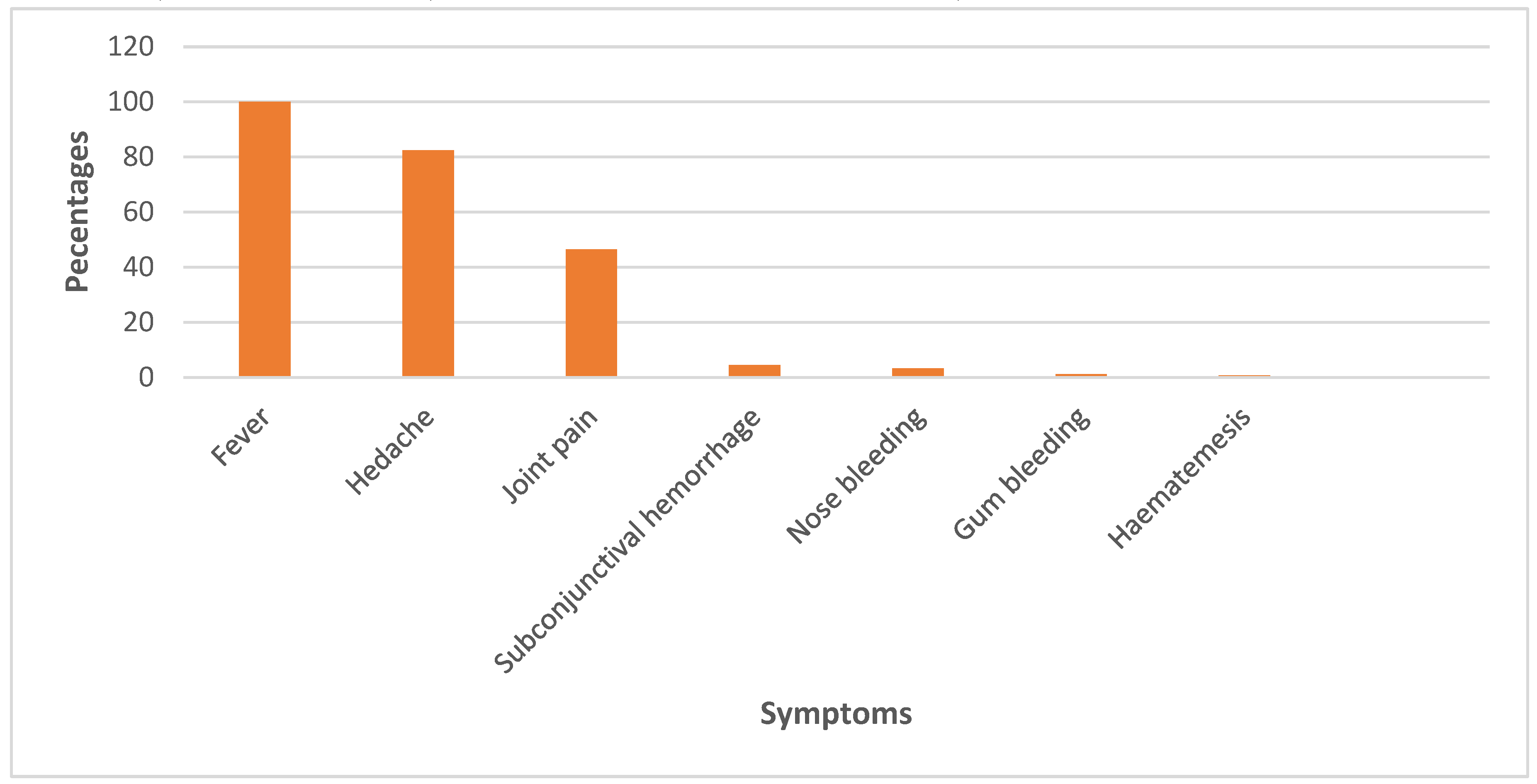
The major clinical presentation of RVF in human patients included fever (100%), headache (82%), joint pain (46%), and subconjunctival haemorrhage (5%). A few patients were presented with nose (3%) and gum (1%) bleeding as well as haematemesis (1%) (Fig. 3).
Figure 3.
The clinical presentations of Rift Valley fever patients during the outbreak in Berber locality between September 2019 and January 2020.
Figure 3.
The clinical presentations of Rift Valley fever patients during the outbreak in Berber locality between September 2019 and January 2020.
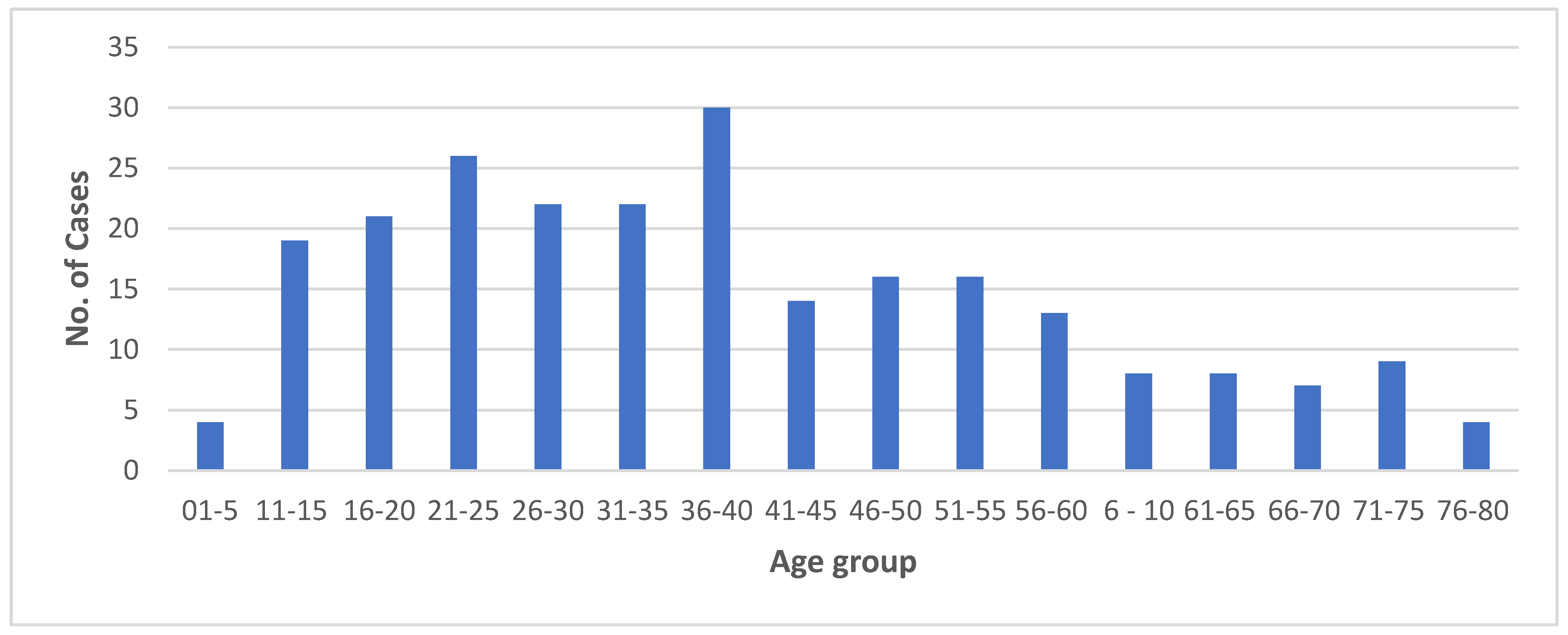
The demography of cases showed that 2% of patients were under five years old and 8% were children aged between 11 and 15 years old. The majority of patients (51%) were young adults aged between 16 and 40 years old and only 2% of patients were aged between 76 and 80 years (Fig. 4). The male to female sex ratio of cases was 1:1.
Figure 4.
The age structure of Rift Valley fever patients during the outbreak in Berber locality between September 2019 and January 2020.
Figure 4.
The age structure of Rift Valley fever patients during the outbreak in Berber locality between September 2019 and January 2020.
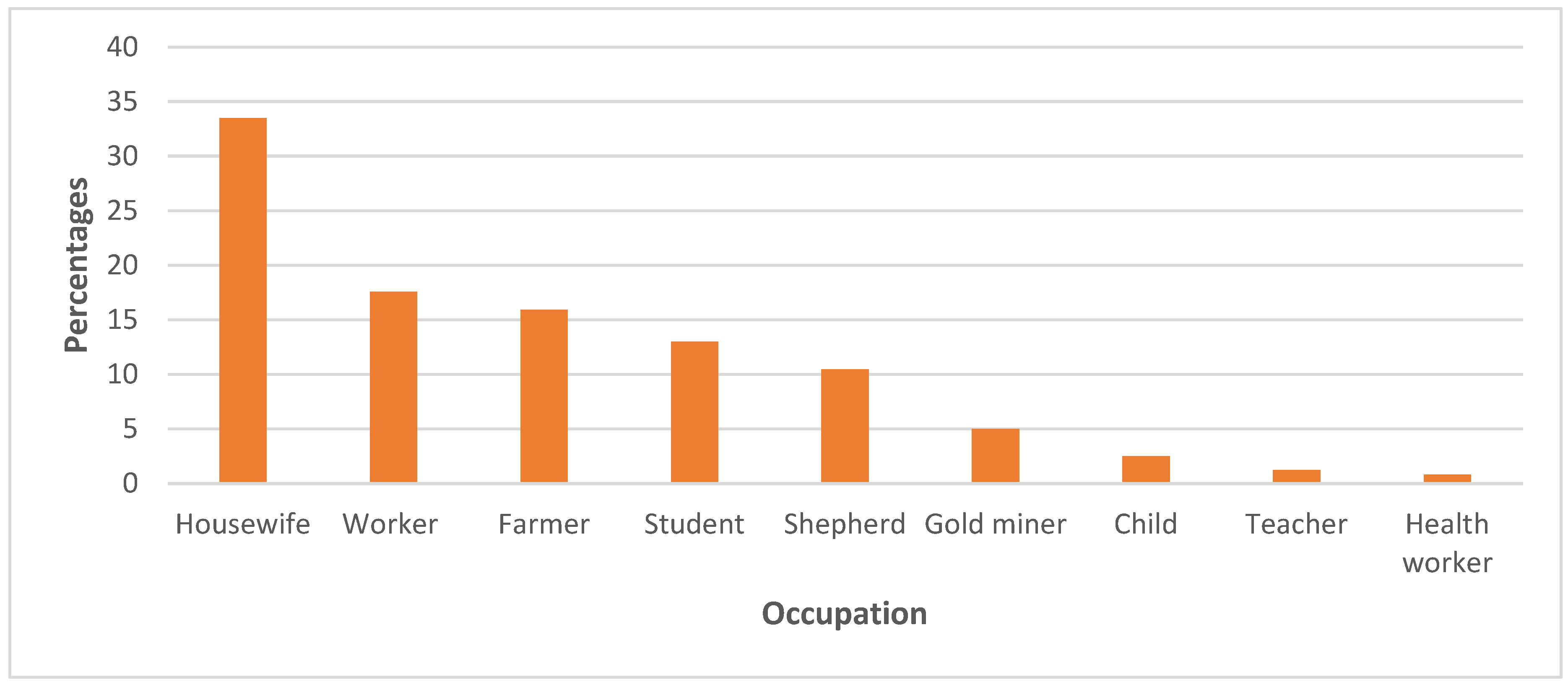
We further analysed the patients’ demographics to investigate any potential occupational hazard. Thirty-three percent of the patients were housewives followed by health workers (18%), farmers (16%). Interestingly, low proportions of the patients were animal breeders, children, and health workers, 10%, 3%, and 1% (Fig. 5).
Figure 5.
The distribution of the Rift Valley fever cases by occupation during the outbreak in Berber locality, River Nile state between September 2019 and January 2020.
Figure 5.
The distribution of the Rift Valley fever cases by occupation during the outbreak in Berber locality, River Nile state between September 2019 and January 2020.
3.3. The One Health response:
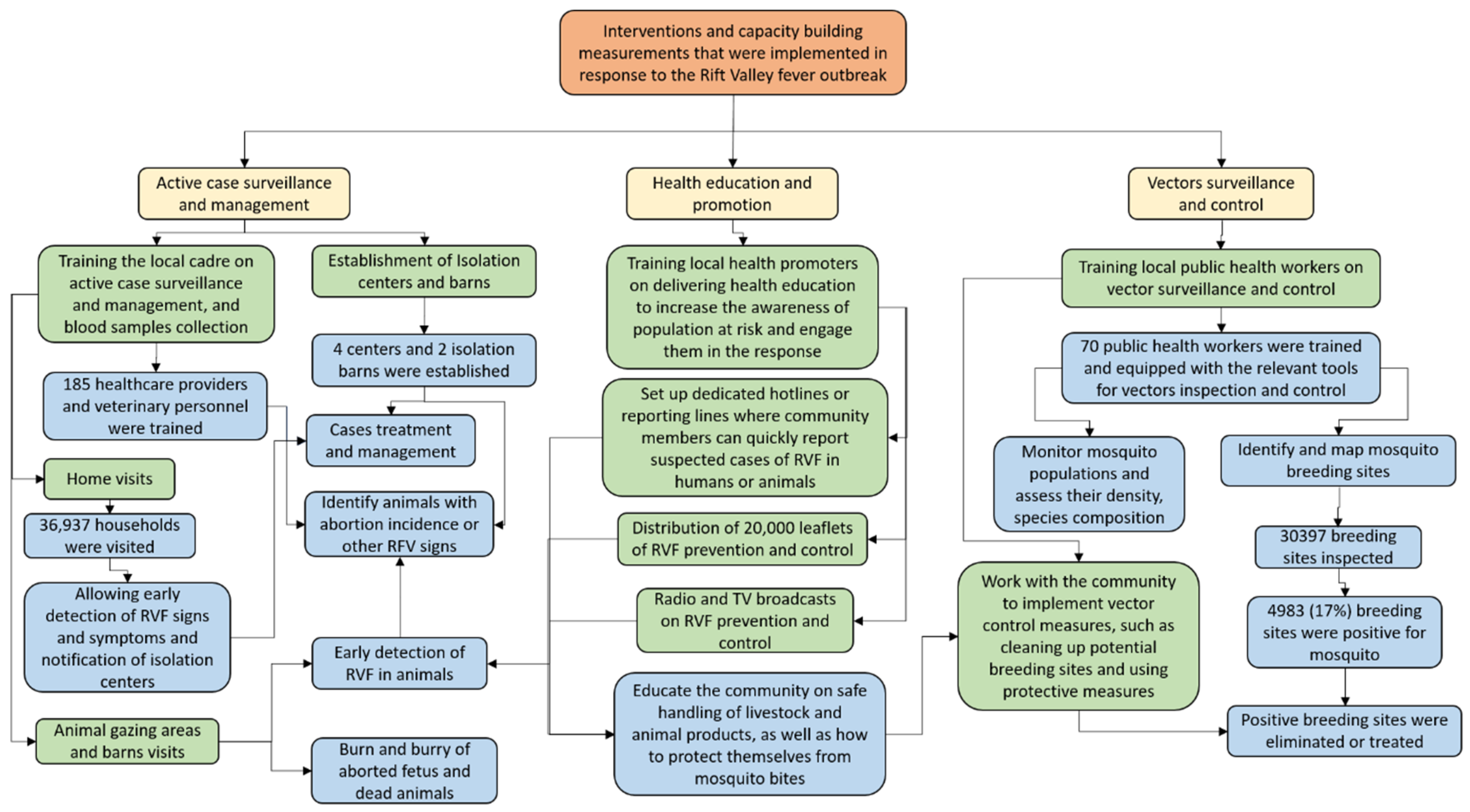
One hindered and eighty-five healthcare providers at the state Ministry of Health received a package of extensive and short training on the active case surveillance and effective management as well as blood samples collection, preservation, and shipment (Fig. 6). Also, 70 public health workers were trained and equipped for the vector inspection, collection, and control. Additionally, 110 health promoters were trained on the risk communication and outreach activities to engage communities at risk and raise their awareness about the risk, prevention and control measures, and what to do to handle infections among humans and animals (Fig. 6).
Figure 6.
Flowchart explain multisectoral One Health actions and measurements implemented in response to the Rift Valley fever outbreak in Berber locality in 2019.
Figure 6.
Flowchart explain multisectoral One Health actions and measurements implemented in response to the Rift Valley fever outbreak in Berber locality in 2019.
Entomological surveillance revealed that, the vector composition of mosquito species in Berber locality during the outbreak between September 2019 and January 2020, mainly included Anopheles arabiensis, An. stephensi, Aedes aegypti, Ae. vexans, Culex pipiens, Cx. Quinquefasciatus, and Cx. theileri. However, distribution and density of these species was very heterogeneous.
Comparing outcomes of two outbreaks of RVF in similar settings that occurred within less than three months gap in time highlights the added value of implementing multisectoral One Health in the surveillance, preparedness, and response to the disease outbreaks (Table 2). Through the implementation of integrated One Health strategy, about 78% more human case were averted and 63% lives were saved. On the animal side, over 80% loss in livestock resources were prevented (Table 2).
4. Discussion
Here we report a major RVF outbreak in Berber locality, River Nile state, northern Sudan between September 2019 and January 2020. We also document the first implementation of One Health strategy in response to an outbreak of zoonotic disease in Sudan. We identified 246 cases of RVF among humans including seven deaths in the River Nile state between September 2019 and January 2020. We also, detected 119 deaths and 82 abortions due to infections with RVF among livestock. Despite the apparently high number of infections among both, humans and animals, compared with a previous outbreak of RVF in a nearby locality around three months ago, this outbreak resulted in substantially less morbidity, mortality, and loss in livestock in comparison with other outbreaks of RVF in the country [7,29,30,31,32,33]. This underscore the added value of the jointly implemented One Health strategy with an integrated surveillance and response system [34,35,36]. Nevertheless, RVF outbreaks are serious threat to health and socioeconomic status particularly for poor populations that depend on livestock.
Up to recently, outbreaks of RVF were mainly occurring in the southern region of the country [6,27,30]. However, due to climate change that indicated by extreme weather events including the heavy rains and flash flooding, several vector-borne and zoonotic diseases are increasingly spreading and outbreaking throughout the country [21]. The country has recently suffered from major outbreaks of CCHF [5,37], CHIK [22], Cholera [38], DEN [39,40], hepatitis E [41], malaria [42], and RVF [7,8]. In addition to these challenges, the COVID-19 pandemic and increasing conflicts and humanitarian crisis have further weakened the already fragile health system, making it more difficult to effectively respond to these outbreaks [43,44,45].
Having the highest prevalence of RVF infections among housewives suggests household exposure and also the involvement of other modes of transmission of RVF such as exposure to raw meat and milk from infected animals [46]. This aligns with the WHO and Centers for Disease Control and Prevention (CDC) evidence that most of RVF infections result from contact with infected animals or their products and fluids [47,48]. The household exposure assumption is supported by the wide range of patients’ age, between less than 1 year old and over 80 years old. Nevertheless, this might be driven by the diverse species of vectors that were detected in the area during the outbreak. Particularly that evidence from other countries revealed that Cx. theileri was involved in the re-introduction of RVF virus following a long disappearance [49]. While, Anopheles arabiensis, An. stephensi, Aedes aegypti, Culex pipiens, and Cx. Quinquefasciatus are well known competent vector of RVF [26,50,51,52], Ae. vexans is known as anthropophilic and mammalophilic floodwater, is considered the initial vector of sporadic RVF outbreaks because of it is unique biology and breeding behaviour. Ae. vexans lays the eggs on the edge of waterbodies, the eggs need to dry first before it can hatch, therefore, it capable of withstanding draught for years while harbouring the RVF virus [53,54,55]. According to the Food and Agriculture Organization of the United Nations (FAO), once the infected eggs of Ae. vexan hatch after years, the emerging adults are readily capable to infects animals upon their first blood-meal [56]. This explains the sporadic nature of RVF outbreaks in endemic countries [57,58,59,60]. However, as commonly only small proportion of RVF infections develop symptoms and that most of the clinical presentation of RVF’s patients is closely similar to malaria and other prevalent diseases in endemic areas, low transmission and sporadic cases might be missed by the surveillance system or mistakenly identified as a different disease [39,61,62,63]. For instant, screening blood donated by seemingly healthy individuals for arboviral infections revealed high seroprevalence of arboviruses including Chikungunya, O'nyong'nyong, Zika, and West Nile virus, that was not captured through the routine surveillance and healthcare facility based diagnosis [64,65]. This calls for strengthening the diagnostic capacity and surveillance system for emerging infectious diseases including RVF [66,67,68]. Particularly in rural areas and humanitarian crisis settings, where populations are underserved and more vulnerable diseases outbreaks [7,42,69,70]. In Sudan, particular attention is urgently needed for the increasingly emerging and spreading invasive diseases vectors including An. stephensi and Aedes albopictus and the diseases they transmit, because little is known about their vectorial capacity and susceptibility to the locally implemented vector control interventions [23,71,72,73].
Changes in the land use and land cover due to climate change and human activities including deforestation, unplanned urbanization, conflicts and human-made humanitarian crisis are the major risk factors for disease outbreaks [21,74,75,76]. Unfortunately, the size of forcibly displaced population in the country is rapidly growing to over 10 million, this increases the vulnerability of communities to infectious diseases [40,41,76]. These risk factors increase humans and animals movements between endemic and disease-free areas [7,8,22], they also influence the spread of diseases vectors, particularly invasive vectors such as Aedes albopitcus and Anopheles stephensi [23,71,77,78].
Existed evidence confirms mother to child transmission in humans and animals, transovarial transmission in vectors, and the involvement of RVF in abortion among pregnant women [26,53,79,80,81]. RVF virus infects wide range of hosts including humans, wildlife and domestic animals particularly livestock, the disease has very devastating impacts on global security, health, socioeconomic, and food safety and security, particularly among poor communities in endemic countries including Sudan [27,30,30]. This underscores the need for implementing multisectoral One Health strategy for the surveillance, prevention, and control of RVF outbreaks [8,82,83]. Such strategy should capitalize on improving the diagnostic capacity and surveillance system, enhance case management and vector control, and more importantly strengthening preparedness, prevention, and response strategies and interventions.
More investment should be made on improving the early detection and surveillance through leveraging the use of diseases vectors as flying needles that naturally collect blood samples randomly from all different hosts in the area including human and livestock to monitor dynamics of diseases and pathogens through what is known as Xenosurveillance [84,85,86,87]. This will might offer a robust and cost-effective tool for the early detection of pathogens circulating in a specific area [23]. Integrating molecular Xenosurveillance, community-based syndromic surveillance for humans and animals, and the health facility-based passive surveillance enhanced with genomic analysis will create a powerful collaborative integrated surveillance [10,35,68,86,88]. Appreciating the potential challenges in the field for the implementation of molecular Xenosurveillance, it still could be leveraged as an early warning system that alert the health system to initiate more in depth investigations. Supporting this with a multisectoral One Health strategy for the early preparedness, prevention, and response strategy will substantially reduce the risk of future outbreaks and pandemics [89,90,91]. Interestingly, blood-fed mosquitoes were proven useful in tracking the community exposure to a non-mosquito-borne virus; namely SARS-CoV-2 in rural areas [92]. This underscores that, Xenosurveillance in addition to its cost-effectiveness in the early detection of vector-borne diseases before they emerge among human and/or animal populations and causing significant health and socioeconomic challenges, it offers a robust and non-invasive approach for tracking the community exposure to pathogens [84,93]. Nevertheless, the feasibility and effectiveness of this approach need to be explored in different settings and for different diseases [85,86].
To strengthen future responses, it is essential to incorporate an animal vaccination program in regions endemic or vulnerable to RVF outbreaks [28]. This proactive measure will add significant value in preventing the recurrence of such outbreaks and minimizing their devastating impacts [94]. Effective preparedness, prevention, and response strategy in countries endemic with or at risk of RVF outbreaks like Sudan should consider vaccinating most at risk human populations using the currently leading candidate vaccine for human use, once it is approved [95]. To maximize the cost-effectiveness, there is a need to establish a coordinated mechanism for joint vaccination campaigns for humans and livestock, this might bring the disease eliminating at sight.
Due to the disease’s characteristics including virulence, devastating impacts on health, socioeconomic, and food insecurity, and global health security, RVF is on the high priority lists of Gavi; the Vaccine Alliance, the Coalition for Epidemic Preparedness Innovations (CEPI), and the WHO list for potential involvement of the next pandemic [89,96,97,98]. Therefore, the world will save more lives and resources by investing in improving the planning and implementation of effective measures of preparedness, prevention, and early responses through a multisectoral and integrated systems One Health strategy [35,90,99,100,101]. This must include increasing the awareness, engagement, and empowerment of communities at-risk to enhance the implementation of preparedness and prevention measures and facilitate the early notification through a community-based syndromic surveillance and increase the uptake of interventions and services including vaccination [68,102,103].
5. Conclusions
Here we reported an outbreak of Rift Valley fever in Berber locality in the northern region of Sudan. We identified 246 cases of RVF infection including seven deaths among humans, and 119 deaths and 82 abortions among Livestock in the area. Our entomological surveillance confirmed the presence of Anopheles arabiensis, An. stephensi, Aedes aegypti, Ae. vexans, Culex pipiens, Cx. Quinquefasciatus, and Cx. theileri in the area during the outbreak. In a comparison with another outbreak of Rift Valley fever in nearby area while ago, a multisectoral One Health response strategy has resulted in strengthening the health system through re-innovating health facilities and centres and training about 200 healthcare and emergency responders. Additionally, it reduced cases and fatalities among humans by 78% and 63%, respectively, and loss in livestock due to deaths and/or abortions by 82%.
This underscore the added value of implementing a One Health strategy including an integrated surveillance and response system for the containment and control of Rift Valley fever outbreak. We recommend the institutionalization of a comprehensive One Health strategy in countries endemic with devastating zoonotic diseases like Rift Valley fever. Such a multisectoral One Health strategy should capitalize on preparedness and prevention include improving the early detection, massive vaccination program for livestock, supporting the development of effective and safe vaccinations to human. This could be enhanced by the implementation of metagenomics-enhanced Xenosurveillance as an early warning system.
Author Contributions
Conceptualization, A.A.; methodology, A.A.; formal analysis, A.A., Y.A., E.E.S., and N.S.M.; investigation, A.A., Y.A., N.A.I., S.I.M., E.E.S., and N.S.M.; resources, Y.A. and C.M.M.; data curation, A.A. and Y.A.; writing—original draft preparation, A.A.; writing—review and editing, A.A., Y.A., N.A.I., S.I.M., J.Z., E.E.S., N.S.M., and C.M.M.; visualization, A.A., Y.A., E.E.S., and N.S.M.. All authors have read and agreed to the published version of the manuscript.
Funding
Please add: This research received no external funding.
Data Availability Statement
All data collected during this study is included in the published article.
Acknowledgments
We would like to thanks the World Health Organization Sudan Office for the technical and logistical supports, the local communities for their cooperation and our colleagues at the River Nile state Ministry of Health, and our colleagues at the National Public Health Laboratory for their help and support throughout the implementation of One Health strategy for the investigation and response to this outbreak..
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Weaver, S.C.; Barrett, A.D.T. Transmission Cycles, Host Range, Evolution and Emergence of Arboviral Disease. Nat Rev Microbiol 2004, 2, 789–801. [Google Scholar] [CrossRef] [PubMed]
- Sick, F.; Beer, M.; Kampen, H.; Wernike, K. Culicoides Biting Midges—Underestimated Vectors for Arboviruses of Public Health and Veterinary Importance. Viruses 2019, 11, 376. [Google Scholar] [CrossRef]
- Cleton, N.; Koopmans, M.; Reimerink, J.; Godeke, G.-J.; Reusken, C. Come Fly with Me: Review of Clinically Important Arboviruses for Global Travelers. Journal of Clinical Virology 2012, 55, 191–203. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.; Campo, J.M.D.; Constenla, D. A Review of the Economic Evidence of Aedes-Borne Arboviruses and Aedes-Borne Arboviral Disease Prevention and Control Strategies. Expert Review of Vaccines 2020, 19, 143–162. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Ali, Y.; Salim, B.; Dietrich, I.; Zinsstag, J. Epidemics of Crimean-Congo Hemorrhagic Fever (CCHF) in Sudan between 2010 and 2020. Microorganisms 2022, 10, 928. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Dietrich, I.; LaBeaud, A.D.; Lindsay, S.W.; Musa, A.; Weaver, S.C. Risks and Challenges of Arboviral Diseases in Sudan: The Urgent Need for Actions. Viruses 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Ali, Y.; Elduma, A.; Eldigail, M.H.; Mhmoud, R.A.; Mohamed, N.S.; Ksiazek, T.G.; Dietrich, I.; Weaver, S.C. Unique Outbreak of Rift Valley Fever in Sudan, 2019 - Volume 26, Number 12—December 2020 - Emerging Infectious Diseases Journal - CDC. Emerging Infectious Diseases 2020, 26, 3030–3033. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Mahmoud, I.; Eldigail, M.; Elhassan, R.M.; Weaver, S.C. The Emergence of Rift Valley Fever in Gedaref State Urges the Need for a Cross-Border One Health Strategy and Enforcement of the International Health Regulations. Pathogens 2021, 10, 885. [Google Scholar] [CrossRef] [PubMed]
- Remera, E.; Rwagasore, E.; Muvunyi, C.M.; Ahmed, A. Emergence of the First Molecularly Confirmed Outbreak of Rift Valley Fever among Humans in Rwanda, Calls for Institutionalizing the One Health Strategy. IJID One Health 2024, 4. [Google Scholar] [CrossRef]
- Nsengimana, I.; Juma, J.; Roesel, K.; Gasana, M.N.; Ndayisenga, F.; Muvunyi, C.M.; Hakizimana, E.; Hakizimana, J.N.; Eastwood, G.; Chengula, A.A.; et al. Genomic Epidemiology of Rift Valley Fever Virus Involved in the 2018 and 2022 Outbreaks in Livestock in Rwanda. Viruses 2024, 16, 1148. [Google Scholar] [CrossRef] [PubMed]
- Weaver, S.C. Prediction and Prevention of Urban Arbovirus Epidemics: A Challenge for the Global Virology Community. Antiviral Res 2018, 156, 80–84. [Google Scholar] [CrossRef]
- Pigott, D.M.; Deshpande, A.; Letourneau, I.; Morozoff, C.; Reiner, R.C.; Kraemer, M.U.G.; Brent, S.E.; Bogoch, I.I.; Khan, K.; Biehl, M.H.; et al. Local, National, and Regional Viral Haemorrhagic Fever Pandemic Potential in Africa: A Multistage Analysis. The Lancet 2017, 390, 2662–2672. [Google Scholar] [CrossRef]
- Kraemer, M.U.G.; Reiner, R.C.; Brady, O.J.; Messina, J.P.; Gilbert, M.; Pigott, D.M.; Yi, D.; Johnson, K.; Earl, L.; Marczak, L.B.; et al. Past and Future Spread of the Arbovirus Vectors Aedes Aegypti and Aedes Albopictus. Nat Microbiol 2019, 4, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Weaver, S.C.; Reisen, W.K. Present and Future Arboviral Threats. Antiviral Research 2010, 85, 328–345. [Google Scholar] [CrossRef]
- Coffey, L.L.; Forrester, N.; Tsetsarkin, K.; Vasilakis, N.; Weaver, S.C. Factors Shaping the Adaptive Landscape for Arboviruses: Implications for the Emergence of Disease. Future Microbiology 2013, 8, 155–176. [Google Scholar] [CrossRef]
- Esser, H.J.; Mögling, R.; Cleton, N.B.; van der Jeugd, H.; Sprong, H.; Stroo, A.; Koopmans, M.P.G.; de Boer, W.F.; Reusken, C.B.E.M. Risk Factors Associated with Sustained Circulation of Six Zoonotic Arboviruses: A Systematic Review for Selection of Surveillance Sites in Non-Endemic Areas. Parasites Vectors 2019, 12, 265. [Google Scholar] [CrossRef] [PubMed]
- Whiteman, A.; Loaiza, J.R.; Yee, D.A.; Poh, K.C.; Watkins, A.S.; Lucas, K.J.; Rapp, T.J.; Kline, L.; Ahmed, A.; Chen, S.; et al. Do Socioeconomic Factors Drive Aedes Mosquito Vectors and Their Arboviral Diseases? A Systematic Review of Dengue, Chikungunya, Yellow Fever, and Zika Virus. One Health 2020, 100188. [Google Scholar] [CrossRef]
- Huang, Y.-J.S.; Higgs, S.; Vanlandingham, D.L. Emergence and Re-Emergence of Mosquito-Borne Arboviruses. Current Opinion in Virology 2019, 34, 104–109. [Google Scholar] [CrossRef]
- Elaagip, A.; Alsedig, K.; Altahir, O.; Ageep, T.; Ahmed, A.; Siam, H.A.; Samy, A.M.; Mohamed, W.; Khalid, F.; Gumaa, S.; et al. Seroprevalence and Associated Risk Factors of Dengue Fever in Kassala State, Eastern Sudan. PLoS Negl Trop Dis 2020, 14. [Google Scholar] [CrossRef]
- Elduma, A.H.; LaBeaud, A.D.; Plante, J.A.; Plante, K.S.; Ahmed, A. High Seroprevalence of Dengue Virus Infection in Sudan: Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease 2020, 5, 120. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Mohamed, N.S.; Siddig, E.E.; Algaily, T.; Sulaiman, S.; Ali, Y. The Impacts of Climate Change on Displaced Populations: A Call for Actions. The Journal of Climate Change and Health 2021, 100057. [Google Scholar] [CrossRef]
- Ahmed, A.; Ali, Y.; Mohamed, N.S. Arboviral Diseases: The Emergence of a Major yet Ignored Public Health Threat in Africa. The Lancet Planetary Health 2020, 4, e555. [Google Scholar] [CrossRef]
- Ahmed, A.; Abubakr, M.; Sami, H.; Mahdi, I.; Mohamed, N.S.; Zinsstag, J. The First Molecular Detection of Aedes Albopictus in Sudan Associates with Increased Outbreaks of Chikungunya and Dengue. International Journal of Molecular Sciences 2022, 23, 11802. [Google Scholar] [CrossRef]
- Eisa, M. Preliminary Survey of Domestic Animals of the Sudan for Precipitating Antibodies to Rift Valley Fever Virus. J Hyg (Lond) 1984, 93, 629–637. [Google Scholar] [CrossRef]
- Abdallah, M.M.M.; Adam, I.A.; Abdalla, T.M.; Abdelaziz, S.A.; Ahmed, M.E.; Aradaib, I.E. A Survey of Rift Valley Fever and Associated Risk Factors among the One-Humped Camel (Camelus Dromedaries) in Sudan. Irish Veterinary Journal 2016, 69, 6. [Google Scholar] [CrossRef]
- Seufi, A.M.; Galal, F.H. Role of Culex and Anopheles Mosquito Species as Potential Vectors of Rift Valley Fever Virus in Sudan Outbreak, 2007. BMC Infectious Diseases 2010, 10, 65. [Google Scholar] [CrossRef]
- Aradaib, I.E.; Erickson, B.R.; Elageb, R.M.; Khristova, M.L.; Carroll, S.A.; Elkhidir, I.M.; Karsany, M.E.; Karrar, A.E.; Elbashir, M.I.; Nichol, S.T. Rift Valley Fever, Sudan, 2007 and 2010. Emerg Infect Dis 2013, 19, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Mansour, M.E.A.; Ahmed, A.; Kamal, S.; Elhassan, T.M.A.; Abdelgadir, A.E. Seroprevalence and Geographical Distribution of Rift Valley Fever in Livestock in Sudan. Journal of Applied Veterinary Science And Technology 2024, 5, 78–82. [Google Scholar] [CrossRef]
- de Glanville, W.A.; Allan, K.J.; Nyarobi, J.M.; Thomas, K.M.; Lankester, F.; Kibona, T.J.; Claxton, J.R.; Brennan, B.; Carter, R.W.; Crump, J.A.; et al. An Outbreak of Rift Valley Fever among Peri-Urban Dairy Cattle in Northern Tanzania. Trans R Soc Trop Med Hyg 2022, 116, 1082–1090. [Google Scholar] [CrossRef] [PubMed]
- Hassan, O.A.; Ahlm, C.; Sang, R.; Evander, M. The 2007 Rift Valley Fever Outbreak in Sudan. PLOS Neglected Tropical Diseases 2011, 5, e1229. [Google Scholar] [CrossRef]
- Lagare, A.; Fall, G.; Ibrahim, A.; Ousmane, S.; Sadio, B.; Abdoulaye, M.; Alhassane, A.; Mahaman, A.E.; Issaka, B.; Sidikou, F.; et al. First Occurrence of Rift Valley Fever Outbreak in Niger, 2016. Veterinary Medicine and Science 2019, 5, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Munyua, P.; Murithi, R.M.; Wainwright, S.; Githinji, J.; Hightower, A.; Mutonga, D.; Macharia, J.; Ithondeka, P.M.; Musaa, J.; Breiman, R.F.; et al. Rift Valley Fever Outbreak in Livestock in Kenya, 2006–2007. The American Journal of Tropical Medicine and Hygiene 2010, 83, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Youssouf, H.; Subiros, M.; Dennetiere, G.; Collet, L.; Dommergues, L.; Pauvert, A.; Rabarison, P.; Vauloup-Fellous, C.; Le Godais, G.; Jaffar-Bandjee, M.-C.; et al. Rift Valley Fever Outbreak, Mayotte, France, 2018–2019. Emerg Infect Dis 2020, 26, 769–772. [Google Scholar] [CrossRef] [PubMed]
- Zinsstag, J.; Hediger, K.; Osman, Y.M.; Abukhattab, S.; Crump, L.; Kaiser-Grolimund, A.; Mauti, S.; Ahmed, A.; Hattendorf, J.; Bonfoh, B.; et al. The Promotion and Development of One Health at Swiss TPH and Its Greater Potential. Diseases 2022, 10, 65. [Google Scholar] [CrossRef] [PubMed]
- Zinsstag, J.; Utzinger, J.; Probst-Hensch, N.; Shan, L.; Zhou, X.-N. Towards Integrated Surveillance-Response Systems for the Prevention of Future Pandemics. Infectious diseases of poverty 2020, 9, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Hassan, O.A.; Ahlm, C.; Evander, M. A Need for One Health Approach – Lessons Learned from Outbreaks of Rift Valley Fever in Saudi Arabia and Sudan. Infection Ecology & Epidemiology 2014, 4, 20710. [Google Scholar] [CrossRef]
- Ahmed, A.; Elduma, A.; Magboul, B.; Higazi, T.; Ali, Y. The First Outbreak of Dengue Fever in Greater Darfur, Western Sudan. Tropical Medicine and Infectious Disease 2019, 4, 43. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, N.S.; Ali, Y.; Abdalrahman, S.; Ahmed, A.; Siddig, E.E. The Use of Cholera Oral Vaccine for Containment of the 2019 Disease Outbreak in Sudan. Trans R Soc Trop Med Hyg 2022, 116, 763–766. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Eldigail, M.; Elduma, A.; Breima, T.; Dietrich, I.; Ali, Y.; Weaver, S.C. First Report of Epidemic Dengue Fever and Malaria Co-Infections among Internally Displaced Persons in Humanitarian Camps of North Darfur, Sudan. International Journal of Infectious Diseases 2021, 108, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Ali, Y.; Elmagboul, B.; Mohamed, O.; Elduma, A.; Bashab, H.; Mahamoud, A.; Khogali, H.; Elaagip, A.; Higazi, T. Dengue Fever in the Darfur Area, Western Sudan. Emerging Infect. Dis. 2019, 25, 2126. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Ali, Y.; Siddig, E.E.; Hamed, J.; Mohamed, N.S.; Khairy, A.; Zinsstag, J. Hepatitis E Virus Outbreak among Tigray War Refugees from Ethiopia, Sudan. Emerg Infect Dis 2022, 28, 1722–1724. [Google Scholar] [CrossRef]
- Mohamed, N.S.; Ali, Y.; Muneer, M.S.; Siddig, E.E.; Sibley, C.H.; Ahmed, A. Malaria Epidemic in Humanitarian Crisis Settings the Case of South Kordofan State, Sudan. The Journal of Infection in Developing Countries 2021, 15, 168–171. [Google Scholar] [CrossRef]
- El-Sadig, S.M.; Mohamed, N.S.; Ahmed, E.S.; Alayeib, M.A.; Tahir, L.H.; Edris, A.M.M.; Ali, Y.; Siddig, E.E.; Ahmed, A. Obstacles Faced by Healthcare Providers during COVID-19 Pandemic in Sudan. J Infect Dev Ctries 2021, 15, 1615–1617. [Google Scholar] [CrossRef] [PubMed]
- El-Sadig, S.M.; El-Amin, S.O.; El-Amin, R.O.; Siddig, E.E.; Ahmed, A. Humanitarian Crisis in Sudan: The Collapsed Health System Threats the Public and Global Health. QJM: An International Journal of Medicine 2023, 116, 810. [Google Scholar] [CrossRef]
- Ahmed, A.; Mohamed, N.S.; EL-Sadig, S.M.; Fahal, L.A.; Abelrahim, Z.B.; Ahmed, E.S.; Siddig, E.E. COVID-19 in Sudan. The Journal of Infection in Developing Countries 2021, 15, 204–208. [Google Scholar] [CrossRef]
- Grossi-Soyster, E.N.; Lee, J.; King, C.H.; LaBeaud, A.D. The Influence of Raw Milk Exposures on Rift Valley Fever Virus Transmission. PLOS Neglected Tropical Diseases 2019, 13, e0007258. [Google Scholar] [CrossRef] [PubMed]
- CDC: Centers for Disease Control and Prevention About Rift Valley Fever (RVF). Available online: https://www.cdc.gov/rift-valley-fever/about/index.html (accessed on 14 August 2024).
- The World Health Organization (WHO) Rift Valley Fever. Available online: https://www.who.int/news-room/fact-sheets/detail/rift-valley-fever (accessed on 27 January 2024).
- McIntosh, B.M. Rift Valley Fever: 1. Vector Studies in the Field. Journal of the South African Veterinary Association 1972, 43, 391–395. [Google Scholar] [CrossRef]
- Abdelgadir, D.M.; Bashab, H.M.M.; Elhadi Mohamed, R.A.; Abuelmaali, S.A. Risk Factor Analysis for Outbreak of Rift Valley Fever in Khartoum State of Sudan. Journal of Entomological Science 2010, 45, 239–251. [Google Scholar] [CrossRef]
- Abdo-Salem, S.; Tran, A.; Grosbois, V.; Gerbier, G.; Al-Qadasi, M.; Saeed, K.; Etter, E.; Thiry, E.; Roger, F.; Chevalier, V. Can Environmental and Socioeconomic Factors Explain the Recent Emergence of Rift Valley Fever in Yemen, 2000-2001? Vector Borne Zoonotic Dis 2011, 11, 773–779. [Google Scholar] [CrossRef]
- Linthicum, K.J.; Britch, S.C.; Anyamba, A. Rift Valley Fever: An Emerging Mosquito-Borne Disease. Annual Review of Entomology 2016, 61, 395–415. [Google Scholar] [CrossRef]
- Mohamed, R.; Abdelgadir, D.M.; Bashab, H.M. Transovarian Transmission of Rift Valley Fever Virus by Two Species of Mosquitoes in Khartoum State (Sudan): Aedes Vexans (Meigen) and Culex Quinquefasciatus (Say). Sudanese J Public Health 2013, 8, 164Á170. [Google Scholar]
- Outammassine, A.; Zouhair, S.; Loqman, S. Global Potential Distribution of Three Underappreciated Arboviruses Vectors (Aedes Japonicus, Aedes Vexans and Aedes Vittatus) under Current and Future Climate Conditions. Transboundary and Emerging Diseases 2022, 69, e1160–e1171. [Google Scholar] [CrossRef] [PubMed]
- Sanborn, M.A.; Klein, T.A.; Kim, H.-C.; Fung, C.K.; Figueroa, K.L.; Yang, Y.; Asafo-adjei, E.A.; Jarman, R.G.; Hang, J. Metagenomic Analysis Reveals Three Novel and Prevalent Mosquito Viruses from a Single Pool of Aedes Vexans Nipponii Collected in the Republic of Korea. Viruses 2019, 11, 222. [Google Scholar] [CrossRef]
- Food and Agriculture Organization of the United Nations (FAO) Rift Valley Fever: Vigilance Needed in the Coming Months. EMPRES WATCH. Rome 2012, 27.
- Birungi, D.; Aceng, F.L.; Bulage, L.; Nkonwa, I.H.; Mirembe, B.B.; Biribawa, C.; Okethwangu, D.; Opio, N.D.; Monje, F.; Muwanguzi, D.; et al. Sporadic Rift Valley Fever Outbreaks in Humans and Animals in Uganda, October 2017-January 2018. J Environ Public Health 2021, 2021, 8881191. [Google Scholar] [CrossRef]
- Nyakarahuka, L.; Whitmer, S.; Klena, J.; Balinandi, S.; Talundzic, E.; Tumusiime, A.; Kyondo, J.; Mulei, S.; Patel, K.; Baluku, J.; et al. Detection of Sporadic Outbreaks of Rift Valley Fever in Uganda through the National Viral Hemorrhagic Fever Surveillance System, 2017–2020. Am J Trop Med Hyg 2023, 108, 995–1002. [Google Scholar] [CrossRef]
- Nguku, P.M.; Sharif, S.K.; Mutonga, D.; Amwayi, S.; Omolo, J.; Mohammed, O.; Farnon, E.C.; Gould, L.H.; Lederman, E.; Rao, C.; et al. An Investigation of a Major Outbreak of Rift Valley Fever in Kenya: 2006–2007. Am J Trop Med Hyg 2010, 83, 05–13. [Google Scholar] [CrossRef]
- Sindato, C.; Karimuribo, E.D.; Pfeiffer, D.U.; Mboera, L.E.G.; Kivaria, F.; Dautu, G.; Bernard, B.; Paweska, J.T. Spatial and Temporal Pattern of Rift Valley Fever Outbreaks in Tanzania; 1930 to 2007. PLOS ONE 2014, 9, e88897. [Google Scholar] [CrossRef]
- Ali, Y.; Siddig, E.E.; Mohamed, N.; Ahmed, A. Rift Valley Fever and Malaria Co-infection: A Case Report. Clin Case Rep 2023, 11, e7926. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, M. c.; Haberberger, R. l.; Salib, A. w.; Soliman, B. a.; El-Tigani, A.; Khalid, I. o.; Watts, D. m. Evaluation of Arthropod-Borne Viruses and Other Infectious Disease Pathogens as the Causes of Febrile Illnesses in the Khartoum Province of Sudan. J. Med. Virol. 1996, 48, 141–146. [Google Scholar] [CrossRef]
- Watts, D.M.; el-Tigani, A.; Botros, B.A.; Salib, A.W.; Olson, J.G.; McCarthy, M.; Ksiazek, T.G. Arthropod-Borne Viral Infections Associated with a Fever Outbreak in the Northern Province of Sudan. J Trop Med Hyg 1994, 97, 228–230. [Google Scholar] [PubMed]
- Seruyange, E.; Ljungberg, K.; Muvunyi, C.M.; Gahutu, J.B.; Katare, S.; Nyamusore, J.; Gwon, Y.-D.; Evander, M.; Norder, H.; Liljeström, P.; et al. Seroreactivity to Chikungunya and West Nile Viruses in Rwandan Blood Donors. Vector-Borne and Zoonotic Diseases 2019, 19, 731–740. [Google Scholar] [CrossRef]
- Seruyange, E.; Gahutu, J.-B.; Muvunyi, C.M.; Katare, S.; Ndahindwa, V.; Sibomana, H.; Nyamusore, J.; Rutagarama, F.; Hannoun, C.; Norder, H.; et al. Seroprevalence of Zika Virus and Rubella Virus IgG among Blood Donors in Rwanda and in Sweden. Journal of Medical Virology 2018, 90, 1290–1296. [Google Scholar] [CrossRef]
- Cordes, K.M.; Cookson, S.T.; Boyd, A.T.; Hardy, C.; Malik, M.R.; Mala, P.; El Tahir, K.; Everard, M.; Jasiem, M.; Husain, F. Real-Time Surveillance in Emergencies Using the Early Warning Alert and Response Network. Emerg Infect Dis 2017, 23, S131–S137. [Google Scholar] [CrossRef] [PubMed]
- Bordier, M.; Delavenne, C.; Nguyen, D.T.T.; Goutard, F.L.; Hendrikx, P. One Health Surveillance: A Matrix to Evaluate Multisectoral Collaboration. Frontiers in veterinary science 2019, 6, 109. [Google Scholar] [CrossRef]
- Osman, Y.; Ali, S.M.; Schelling, E.; Tschopp, R.; Hattendorf, J.; Muhumed, A.; Zinsstag, J. Integrated Community Based Human and Animal Syndromic Surveillance in Adadle District of the Somali Region of Ethiopia. One Health 2021, 13, 100334. [Google Scholar] [CrossRef]
- Siddig, E.E.; Ahmed, A. When Parasites Stray from the Path: A Curious Case of Ectopic Cutaneous Schistosoma Haematobium. QJM: An International Journal of Medicine 2023, 116, 794–795. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Hemaida, M.A.; Hagelnur, A.A.; Eltigani, H.F.; Siddig, E.E. Sudden Emergence and Spread of Cutaneous Larva Migrans in Sudan: A Case Series Calls for Urgent Actions. IDCases 2023, 32, e01789. [Google Scholar] [CrossRef]
- Ahmed, A.; Abubakr, M.; Ali, Y.; Siddig, E.E.; Mohamed, N.S. Vector Control Strategy for Anopheles Stephensi in Africa. The Lancet Microbe 2022, 3, e403. [Google Scholar] [CrossRef]
- Ahmed, A.; Irish, S.R.; Zohdy, S.; Yoshimizu, M.; Tadesse, F.G. Strategies for Conducting Anopheles Stephensi Surveys in Non-Endemic Areas. Acta Tropica 2022, 236, 106671. [Google Scholar] [CrossRef]
- Hemming-Schroeder, E.; Ahmed, A. Anopheles Stephensi in Africa: Vector Control Opportunities for Cobreeding An. Stephensi and Aedes Arbovirus Vectors. Trends in Parasitology 2023, 39, 86–90. [Google Scholar] [CrossRef]
- AU PSC report, T.I. for S.S. Climate Change and Violence in Africa: No Time to Lose. Available online: https://issafrica.org/iss-today/climate-change-and-violence-in-africa-no-time-to-lose (accessed on 18 May 2021).
- Carlson, C.J.; Albery, G.F.; Merow, C.; Trisos, C.H.; Zipfel, C.M.; Eskew, E.A.; Olival, K.J.; Ross, N.; Bansal, S. Climate Change Increases Cross-Species Viral Transmission Risk. Nature 2022, 607, 555–562. [Google Scholar] [CrossRef]
- Gayer, M.; Legros, D.; Formenty, P.; Connolly, M.A. Conflict and Emerging Infectious Diseases. Emerg Infect Dis 2007, 13, 1625–1631. [Google Scholar] [CrossRef]
- Abubakr, M.; Sami, H.; Mahdi, I.; Altahir, O.; Abdelbagi, H.; Mohamed, N.S.; Ahmed, A. The Phylodynamic and Spread of the Invasive Asian Malaria Vectors, Anopheles Stephensi, in Sudan. Biology 2022, 11, 409. [Google Scholar] [CrossRef]
- Ahmed, A.; Khogali, R.; Elnour, M.-A.B.; Nakao, R.; Salim, B. Emergence of the Invasive Malaria Vector Anopheles Stephensi in Khartoum State, Central Sudan. Parasites & Vectors 2021, 14, 511. [Google Scholar] [CrossRef]
- Baudin, M.; Jumaa, A.M.; Jomma, H.J.E.; Karsany, M.S.; Bucht, G.; Näslund, J.; Ahlm, C.; Evander, M.; Mohamed, N. Association of Rift Valley Fever Virus Infection with Miscarriage in Sudanese Women: A Cross-Sectional Study. The Lancet Global Health 2016, 4, e864–e871. [Google Scholar] [CrossRef] [PubMed]
- Adam, I.; Karsany, M.S. Case Report: Rift Valley Fever with Vertical Transmission in a Pregnant Sudanese Woman. J. Med. Virol. 2008, 80, 929. [Google Scholar] [CrossRef] [PubMed]
- Adam, A.A.; Karsany, M.S.; Adam, I. Manifestations of Severe Rift Valley Fever in Sudan. International Journal of Infectious Diseases 2010, 14, e179–e180. [Google Scholar] [CrossRef]
- Bashir, R.S.E.; Hassan, O.A. A One Health Perspective to Identify Environmental Factors That Affect Rift Valley Fever Transmission in Gezira State, Central Sudan. Tropical Medicine and Health 2019, 47, 54. [Google Scholar] [CrossRef]
- Hassan, O.A.; Affognon, H.; Rocklöv, J.; Mburu, P.; Sang, R.; Ahlm, C.; Evander, M. The One Health Approach to Identify Knowledge, Attitudes and Practices That Affect Community Involvement in the Control of Rift Valley Fever Outbreaks. PLoS Negl Trop Dis 2017, 11. [Google Scholar] [CrossRef] [PubMed]
- Valente, A.; Jiolle, D.; Ravel, S.; Porciani, A.; Vial, L.; Michaud, V.; Kwiatek, O.; Pedarrieu, A.; Misse, D.; Ferraris, P.; et al. Flying Syringes for Emerging Enzootic Virus Screening: Proof of Concept for the Development of Noninvasive Xenosurveillance Tools Based on Tsetse Flies. Transboundary and Emerging Diseases 2023, 2023, 9145289. [Google Scholar] [CrossRef]
- Grubaugh, N.D.; Sharma, S.; Krajacich, B.J.; Iii, L.S.F.; Bolay, F.K.; Ii, J.W.D.; Johnson, W.E.; Ebel, G.D.; Foy, B.D.; Brackney, D.E. Xenosurveillance: A Novel Mosquito-Based Approach for Examining the Human-Pathogen Landscape. PLOS Neglected Tropical Diseases 2015, 9, e0003628. [Google Scholar] [CrossRef] [PubMed]
- Fauver, J.R.; Gendernalik, A.; Weger-Lucarelli, J.; Grubaugh, N.D.; Brackney, D.E.; Foy, B.D.; Ebel, G.D. The Use of Xenosurveillance to Detect Human Bacteria, Parasites, and Viruses in Mosquito Bloodmeals. Am J Trop Med Hyg 2017, 97, 324–329. [Google Scholar] [CrossRef]
- Cameron, M.M.; Ramesh, A. The Use of Molecular Xenomonitoring for Surveillance of Mosquito-Borne Diseases. Philosophical Transactions of the Royal Society B: Biological Sciences 2021, 376, 20190816. [Google Scholar] [CrossRef] [PubMed]
- The World Health Organization (WHO) Defining Collaborative Surveillance: A Core Concept for Strengthening the Global Architecture for Health Emergency Preparedness, Response, and Resilience (HEPR); World Health Organization, 2023; ISBN 92-4-007406-6.
- CEPI, T.C. for E.P.I. Priority Diseases. Available online: https://cepi.net/research_dev/priority-diseases/ (accessed on 19 January 2023).
- The World Health Organization (WHO) Ensuring Health Security in The African Region through Emergency Preparedness and Response Flagship Programmes in Rwanda; 2022.
- WHO Emergencies Preparedness, Response: Chikungunya in Sudan. Available online: http://www.who.int/csr/don/15-october-2018-chikungunya-sudan/en/ (accessed on 24 November 2018).
- Krajacich, B.J.; Samaké, D.; Dao, A.; Diallo, M.; Sanogo, Z.L.; Yaro, A.S.; Zeguime, A.; Poudiougo, J.; Cissé, K.; Traoré, M.; et al. Tracking SARS-CoV-2 Seropositivity in Rural Communities Using Blood-Fed Mosquitoes: A Proof-of-Concept Study. Front. Epidemiol. 2023, 3. [Google Scholar] [CrossRef] [PubMed]
- Brinkmann, A.; Nitsche, A.; Kohl, C. Viral Metagenomics on Blood-Feeding Arthropods as a Tool for Human Disease Surveillance. International Journal of Molecular Sciences 2016, 17, 1743. [Google Scholar] [CrossRef]
- Bird, B.H.; Nichol, S.T. Breaking the Chain: Rift Valley Fever Virus Control via Livestock Vaccination. Current Opinion in Virology 2012, 2, 315–323. [Google Scholar] [CrossRef]
- Jenkin, D.; Wright, D.; Folegatti, P.M.; Platt, A.; Poulton, I.; Lawrie, A.; Tran, N.; Boyd, A.; Turner, C.; Gitonga, J.N.; et al. Safety and Immunogenicity of a ChAdOx1 Vaccine against Rift Valley Fever in UK Adults: An Open-Label, Non-Randomised, First-in-Human Phase 1 Clinical Trial. The Lancet Infectious Diseases 2023, 23, 956–964. [Google Scholar] [CrossRef]
- WHO, T.W.H.O. Prioritizing Diseases for Research and Development in Emergency Contexts. Available online: https://www.who.int/activities/prioritizing-diseases-for-research-and-development-in-emergency-contexts (accessed on 1 July 2021).
- WHO, T.W.H.O. WHO | List of Blueprint Priority Diseases. Available online: http://www.who.int/blueprint/priority-diseases/en/ (accessed on 19 May 2019).
- GAVI, T.G.A. for V. and I. The next Pandemic: Rift Valley Fever? Available online: https://www.gavi.org/vaccineswork/next-pandemic/rift-valley-fever (accessed on 30 May 2021).
- Ali, Y.; Ahmed, A.; Siddig, E.E.; Mohamed, N.S. The Role of Integrated Programs in the Prevention of COVID-19 in a Humanitarian Setting. Transactions of The Royal Society of Tropical Medicine and Hygiene 2021. [Google Scholar] [CrossRef]
- Ali, Y.; Siddig, E.E.; Osman, M.; Mohamed, N.S.; Musa, A.; Ahmed, A. Preparedness, Prevention, Investigation, and Response to the Emergence of Mpox in Khartoum, Sudan in 2022. 2024.
- Lucey, D.R.; Gostin, L.O. The Emerging Zika Pandemic: Enhancing Preparedness. JAMA 2016, 315, 865–866. [Google Scholar] [CrossRef]
- Khairy, A.; Mahgoob, E.; Nimir, M.; Ahmed, M.; Jubara, M.; Eltayeb, D.; Ahmed, A. Acceptability of COVID-19 Vaccination among Healthcare Workers in Sudan: A Cross Sectional Survey. 2021.
- Ahmed, A.; Ali, Y.; Mohamed, N.S.; Zinsstag, J.; Siddig, E.E.; Khairy, A. Hepatitis E Virus Outbreak among Tigray War Refugees from Ethiopia, Sudan (Response). Emerg Infect Dis 2023, 29, 460–461. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Historical and current overview of the sequential events related to the epidemic development.
Table 1.
Historical and current overview of the sequential events related to the epidemic development.
| Date | Event or action taken |
| December 2018 | Violence escalated throughout the country and increased the dynamic of human and animal populations between RVF-endemic and disease-free areas. |
| January 2019 | Public services totally or partially paralyzed |
| August - October 2019 | Unexpected heavy rains and flash flooding occurred in River Nile |
| September 11th 2019 | Indexed case was reported from Berber locality, River Nile state |
| September 2019 | Alert from the state Ministry of Health |
| September 2019 | Investigation team was deployed and logistic and technical support was provided |
| September 2019 | RVFV infections in human and animal were confirmed |
| October 2019 | RVF epidemic and epizootic were officially declared |
| October 2019 | Ministry of Health, Ministry of Livestock, and WHO joint One Health response and containment mission was launched |
| January 2020 | Successful containment of the outbreak. |
Table 2.
A brief comparison between the outcomes of two different response strategies to two outbreaks of RVF in similar settings.
Table 2.
A brief comparison between the outcomes of two different response strategies to two outbreaks of RVF in similar settings.
| Outcomes | Routine intervention | Integrated One Health intervention | Added value of One Health strategy |
| Location | Eldamar locality | Berber locality | Health system strengthened |
| Period | May-July 2019 | September 2019-January 2020 | Less cases and deaths |
| Human cases | 1,129 | 246 | 78% less human cases |
| Human fatalities | 19 | 7 | 63% less human deaths |
| Death/abortion among animals | At least 1,104 deaths and/or abortions | 201 deaths and/or abortions | 82% less loss in livestock |
| Associated vector composition | Not identified | Anopheles arabiensis, An. stephensi, Aedes aegypti, Ae. vexans, Culex pipiens, Cx. Quinquefasciatus, and Cx. theileri | Implementation of vector species targeted interventions. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



